#( ; and then you get md over here who is the doctor because he's currently taken over by clever and on house arrest )
Text
Heal
A Kun fic that’s part of our Halloween Series!
Summary: Doctor Qian Kun is a young and successful doctor who works miracles. And you are no exception when you become his patient.
Pairing: Doctor! Kun x female reader
Genre: romance, angst, fantasy, horror
Word Count: 5.6k
Warnings: blood, manipulation
(A/N: Thank you guys so much for your support with our Halloween fics! Hope you enjoy the adventures of y/n and Doctor Kun!)
___
You were no stranger to visits to the Neo Hospital in your hometown. When you were a baby, you basically lived at the hospital. You were prone to colds and fevers. You always experienced body aches and fatigue. You were born with a chronic autoimmune disorder that left many doctors baffled. They were only able to provide you with medications to alleviate your pains temporarily. You were confined to stay at home, to be homeschooled by your parents, and make friends online. Your childhood was far from normal.
You were a college junior now and you’ve been strictly online. If it wasn’t for the Internet, you probably would’ve lost your mind by now.
You had contact with the outside world but not physical contact. It’s what you longed for the most.
You resented your family. Your older and younger siblings could go out whenever they pleased. How did they get so lucky? Why were you the only sibling that got the short end of the stick?
Everyone in your family always interacted with you carefully, using hand sanitizer and always washing their hands prior to helping you with something. They treated you like a fine, porcelain doll that had to be preserved. It was irritating on your best days and unbearable on your worst. You felt like an abomination sometimes.
However, throughout the years, you would rebel. You would run away from home when your parents eyes wandered for a moment. The farthest you’d get before getting caught was the park. You were lucky that you didn’t develop any harsh symptoms from those times you ran away. However, you would be punished for taking such risks. You’d get your phone and internet privileges taken away for a month every time.
Last week, you succeeded in your most ambitious escape yet: you made it to Target to buy the new Ariana Grande CD. You thought that the one trip to Target couldn’t hurt you. By no means was it crowded and no one got into your space.
Well, you were wrong to think that you’d be fine.
Now you came down with a fever and you’d been placed on bed rest at your all-too familiar Room 1196 on the eleventh floor of the hospital.
You resented your body. A lot of people could recover from a fever and carry on with their day-to-day lives but you? Not so much.
Your parents made a whole spectacle of getting you to be seen by the best doctors but these doctors couldn’t help you the way you’d hoped.
However, this time, you awoke the next morning after your intake and felt...nothing.
Like you never had a fever in the first place.
You spent the morning checking your social media. Your crush/online classmate Sicheng was on a weekend hiking trip with his friends. He was with a bunch of beautiful, healthy people in North Carolina. You were even more bummed to be in the hospital now.
You wondered what life would be like if you didn’t have your condition. Where could you have gone? Who would you be now?
You’ve always wanted to go to the beach by yourself. To the supermarket. Hell, across the street. You wanted to go somewhere. Anywhere. Without anyone coddling you and watching your every move.
You wished for freedom from the body you were born with. To find a new one, somehow.
Because you had no hope for your current body to change.
“Y/n? Can I come in?” A male voice was heard from the door.
“Sure.” You sat upright on the bed.
The person at the door entered and he was the prettiest healthcare provider you’d ever laid your eyes on. He had warm, brown eyes and a radiant smile. His dark blue hair was wavy.
Suddenly, you regretted not brushing your hair that morning.
He donned a lab coat with the hospital’s name on it. His name tag was in a lanyard: Dr. Qian Kun, MD, DOM, PharmD.
He looked very young...And to have all of those titles? Your head was spinning.
He frowned as he saw how confused you looked. “Are you alright?”
You nodded. “I am.”
He sat on the chair beside your bed. “It’s nice to meet you, y/n. I’m Dr. Qian Kun but you can call me Kun.”
You blinked a few times. “Are you really a doctor?”
He laughed, confused. “What?”
“You don’t seem that much older than me…”
He sighed. “I get that a lot. I’m twenty-four. I graduated early from university...Earned my titles...Now here I am.”
“That’s amazing. You are probably the youngest doctor ever.”
Kun shook his head. “Afraid not. Bala Ambati became a doctor at seventeen.”
You shook your head. “Still...You have three doctorates. That means triple the sleep deprivation. Hats off to you.”
Kun chuckled as he looked at your information in his clipboard. “Your vitals have improved a lot since yesterday.”
You looked down at your hands. “Yeah...That’s impossible…”
Kun shook his head, noting how down you looked. “It is possible, y/n.”
You met his gaze. “How?”
He smiled. “Are you familiar with oriental medicine?”
He sure was charming, you thought. You reminded yourself to answer his question. “No, I’m not.”
Kun got up from his seat. “Well, there are many different practices that a doctor of oriental medicine can utilize, like acupuncture, meditation, and herbal therapy...To restore harmony to the human body. I specialize in herbal therapy.”
“I see…”
“I have created an herbal mixture that has worked efficiently to get my patients back up on their feet.”
Incredulous still, you managed to say, “That’s great, Doctor.”
He lifted an eyebrow.
“I mean, Kun.”
Kun resumed, “And I‘ve provided you with the herbal mixture and from the looks of it, the results have quickly taken effect.”
You were speechless. “That’s…”
“I know it’s hard to believe, y/n. But sometimes doctors fail to find other alternatives to help their patients. Which is why I’m glad I’m your primary physician now.”
“Wait, what about Doctor Morris?” Doctor Morris had been your primary physician since you were five years old.
“She’s retired. I’ve been taking on a couple of her patients now.”
“I see…”
Kun looked out your room’s window and smiled to himself. “You don’t trust me.”
“Don’t take it personally. I don’t trust any medical professional. No one has been able to understand my condition yet so…”
Kun replied, “You’ve been let down too many times.”
“Exactly. Doctors just can’t figure me out.”
He turned to you and grinned. “Allow me to prove you wrong, then.”
___
At the recommendation of Doctor Kun, you were assigned to stay in the hospital for the next few weeks to see how the herbal mixture would affect your body if you took it for a longer period of time.
Every passing day, you felt more alive. It was weird to say this but you felt more alive at the hospital than you did before. You were beginning to suspect that Kun’s herbal mixture was actually working.
The herbal mixture was made of feverfew among other medicinal herbs. It had certainly done the trick to reduce your fever overnight. You wondered just what this mixture was made of.
You just finished your online linguistics lecture and closed your laptop. You found Kun waiting at the door. “You free?”
You nodded. “Yes.”
He sat down next to you and pulled some of your favorite candy out of his pocket.
He put the candy bar in your hand. His fingers lightly touched your palm. Your face warmed up at his proximity. “Happy Halloween, y/n.”
Your eyes nearly bugged out. How did he know you loved Twix? You took the candy bar into your hand and almost cried.
“Y/n?” He asked, worried.
You wiped a tear away. “Sorry...It’s just that this time of the year is hard because...I want to celebrate it. Go out and trick or treat...I know that time has gone for me but I hate that I missed out, you know…”
“Y/n…”
You sniffled and took a bite of the chocolate bar. “My parents never wanted me to feel like I was missing out so they would bring the holiday home to me. I was never in need of M&Ms, Skittles, Twix, or Sour Patch Kids…They even helped me make the best Halloween costumes. We would watch a bunch of horror movies all month long...But I wanted to be a kid. I wanted to go out with my friends and go door to door…”
Kun’s heart went out to you. He hated seeing you so down and so deprived of a life that everyone should have. “Y/n, you will be able to do all of the things you want to do in life.”
You looked at Kun and he had a determined look on his face. “How can you be so sure?”
“I’ve worked with people with conditions like yours...They thought they would be attached to the hospital forever one way or another. But with my methods, I was able to help them turn their life around. And now they’re living normally and fully.”
You sighed. “I’m happy to hear that...I just don’t think I’ll be one of them.”
Kun placed his hand over yours. “Trust me, y/n. I won’t let you down.”
You met his eyes, then, and you smiled. “Thanks, Kun. I’ve gotta hand it to you. You’re my favorite doctor.”
He beamed. “Is that so?”
You nodded. “Yeah...None of the other doctors ever gave me so much as a lollipop Even though that seems to be the norm on TV…”
Kun chuckled. “There’s more where that came from, y/n.”
___
It has been a month since you’ve entered the hospital. The medical bills were covered by an anonymous benefactor. Your family didn’t have to worry about the financial strain of your hospital stay.
Your family came to visit you and they were stunned at how radiant you looked. They were surprised at how much more ALIVE you looked when they expected you to be weak and miserable because you were at the hospital. Something about you was different.
“Doctor Kun is a miracle worker, isn’t he?” Your dad asked.
“I heard he’s a sight for sore eyes, too...Don’t you think so, y/n?” Your older sister Sydney teased.
You mom shook her head and helped fluff your pillows. “How are you, sweetheart?”
You smiled. “I’m better, actually. I think Kun’s methods are working.”
“Oh, are you two on a first name basis?” Your sister joked.
You rolled your eyes. “He told me to call him Kun. If you saw him, you’d feel weird calling him Doctor, actually.”
“He’s quite young, y/n. He graduated from a top university in Beijing at age 10. Then, he went to medical school right after. He’s been a practicing doctor for a couple of years now. He’s unbelievable,” you dad said.
Kun entered the room, then. “I hope I’m not interrupting. I’m Doctor Qian Kun. It’s a pleasure to meet you.”
Your mom was in love with him. Your dad was in shock at how young he was. Your sister wanted his number. You broke their stunned silence. “Kun, these are my parents Donna and Andrew. And this is my sister, Sydney.”
Kun greeted them. “I’m glad you are all here so I can tell you the good news.”
Everyone was shocked at the phrase “good news”. What good news could he possibly have to share?
Kun continued, “Y/n, your vitals are working at optimum level and we want to see how well you can fare by discharging you.”
You asked, “What?”
Kun smiled. “You can start having a normal life...In which you can attend in-person classes, go to the supermarket, take up a sport…”
You weren’t sure about the last thing he offered but everything else he suggested made you jump out of your bed. “Serious?”
Kun’s smile grew. “Yes.”
Your parents gave each other looks.
Your dad started. “Doctor, are you sure about this...y/n has lived all of her life in our home. The only outside world she’s ever known is our backyard and this hospital.”
Kun nodded. “I am sure. I’ve worked with several patients with similar cases as y/n’s and I would like to put the effect of the herbal mixture to the test. If there is any risk, she will immediately be brought back to the hospital and I will up the dosage for the herbs.”
After a few more minutes of discussion, your parents reluctantly agreed to take you home. To alleviate their concerns, you promised to consult with Kun once a week so he could monitor your progress.
You would be going home tomorrow and you had been given the green light to live a normal life. Outside. Go to classes. See your friends. Go to the beach. Buy fruits at the grocery store.
You packed up your belongings and Kun visited you one last time before you left. “Hey.”
You smiled brightly at him. “Hi!”
“How are you feeling?”
“Better than I ever have, honestly. And I have you to thank for that. Look, I’m not sure if this will work out in the end but the fact that I can take the chance and go out there...Thank you.”
Kun ruffled your hair. “I’m here for you, y/n.”
You did admit to yourself that you’d had a little crush on Dr. Kun but who were you kidding? He was so out of your league. You’d had a friend in him and you would always be thankful to him. “I have something for you.”
Kun’s eyes widened. “For me?”
“I wasn’t sure it’d get to my house in time but my mom got the package today. I told her to bring it today when everyone visited so…”
You pulled out a small gift bag with Kun’s present inside.
Kun smiled. “You didn’t have to get me anything.”
“You’ve done a lot for me, Kun. I may have my doubts but I don’t doubt your intentions. And they're nothing but good. You’ve been doing so much for me. You’re setting me free...In a way.”
You handed the bag to Kun. He pulled out a little wrapped box from inside. He looked at you as he mocked suspicion.
He removed the wrapping to find a pair of AirPods. He gaped. “Y/n…”
You smiled. “For whenever you need to escape the noise…”
Kun had told you that sometimes he would get overwhelmed with his duties at the hospital and you’d asked him what gave him comfort. He told you it was music. So you figured something as light and portable as AirPods could help Kun calm down whenever he needed it throughout the day.
He smiled brightly at you and surprised you by wrapping his arms around you. “Y/n, thank you...You shouldn’t have…”
You froze. Kun’s toned body was against yours and you could feel the racing of his heart. Your heart probably beat twice as fast. You felt yourself get warmer and warmer. You pulled away from him, his hands on your arms.
He blushed. “Sorry…”
You cleared your throat. “Don’t worry about it…”
Your dad returned to the hospital room. “Y/n, you ready?”
Perfect timing, dad, you thought.
“Yeah, I’m coming.”
___
It may have been the second semester of your junior year but you felt as nervous as an incoming college freshman as you entered Neo University’s grounds for the first time. You were meeting some of your friends for the first time ever.
It was one thing to see them on the screen but your heart accelerated thinking of what it would be like to see them in the flesh.
You’ve been doing well so far with the herbs Kun had sent you home with. You were able to go grocery shopping with your mom. She was still considering whether or not you could go to the beach yet. You hoped that your progress would continue so she would say yes.
You felt healthier than ever. You could breathe well through your nose. You felt no body aches. You were ready to cartwheel across the quadrangle.
First, you had to learn how to cartwheel, though.
“Y/n!!!!!” Jungeun called out to you.
Your blonde best friend ran up to you and jumped you from behind. “Ah!”
“Jungeun!” You gasped.
She laughed. “You said I could touch you so I wasn’t about to hold back.”
You hugged each other tightly.
“Y/n, it’s so good to see you!”
You and Jungeun have been friends since middle school so you were already a sobbing mess on your first day.
“Stop crying, y/n or else I’m gonna…” She started crying, too.
“Enough with the tears, already,” Dejun added.
You and Jungeun hugged Dejun to bother him, then.
He laughed. “Y/n, welcome to Neo U.”
“Thanks,” you said, smiling.
You three went to your seminar together and you were just so in awe of being in a classroom, you had trouble focusing on the lecture. You were even more distracted when you saw that Sicheng was in the same class.
He recognized you and waved. You were yelling so loudly on the inside.
Before this semester, you had the occasional online class that you shared. You saw Sicheng for the first time a year ago and your crush on him grew from there. He was one of the most popular guys on campus, according to Jungeun. You had a group project with him last semester and he was so...Perfect.
He was intelligent and down-to-earth. His smile was so sweet and his eyes pierced into your soul. He was talking poetry. It felt like you were seeing your favorite celebrity in person.
When class ended, you went to lunch with your friends and Sicheng joined you.
“How are you, y/n?” He asked.
“I’m great. Never been better,” you replied.
He smiled. “I’m glad. If you ever need anything, please let me know. You have my number.”
You nodded. “Of course. Same here. If you ever need anything. I’m here for you, too.”
Sicheng chuckled. “Great.”
When you finished lunch, Jungeun couldn’t stop poking fun at you. Sicheng left early for a club meeting. “I’m surprised he didn’t ask you out, then!”
You rolled your eyes. “Ask who out?”
Dejun added. “Me, of course.”
Jungeun continued. “The ‘you have my number’ couldn’t have been more obvious. He wants you in his dorm yesterday.”
You frowned. “And what would we do? Fix his bed?”
Jungeun and Dejun laughed. Jungeun added, “The opposite, y/n.”
Your face heated up then. “Oh.”
Since you have basically spent most of your life either at home or at the hospital, you never even considered the possibility of a love life. You tried to convince yourself that dating sims would’ve been enough.
“Don’t worry, y/n...You and Sicheng can take it slow...He’s no incubus who is trying to take your soul,” Dejun offered.
“True,” you said.
That was if Sicheng saw you that way in the first place.
___
A few weeks had passed. You’d been seeing Kun regularly to check in and everything had gone as expected. You were fine. You weren’t exhibiting any flare-ups. So long as you kept taking the prescribed herbs, you would be fine.
“How is everything, y/n?” He asked.
“Pretty good, actually. School is still school, even if it’s in person. But I got to go to a skating rink for the first time.”
He laughed. “How was it?”
“I am terrible.” You showed your legs. “It explains these bruises.”
Kun shook his head and chuckled. “I’m glad you’re getting out more, y/n. Try and take it one step at a time.”
“Oh, geez. I wish you said that sooner. I already joined a blood cult and I’m getting married next week.”
Kun rolled his eyes as he finished taking notes from your consultation.
“How is everything with you, doc?”
Kun’s eyes widened. “Me?”
“Surely, you’re not always at the hospital.”
Kun sighed. “Well, y/n...it just so happens that I’ve taken residence up on the top floor. The whole floor is my apartment. Don’t really get to spend much time there because I’m almost always on call.”
Your jaw dropped. “What? Kun, that’s abuse. You shouldn’t be working so many hours. It’s against the-“
Kun couldn’t help his smile appearing.
“You sneaky bastard,” you said.
You both laughed, then.
Sometimes you forgot Kun was a successful doctor. Sometimes he felt like your infinitely smarter senior at college.
He was a million worlds away from yours.
Kun answered, “Well, I’m doing fine, y/n. I meet up with friends once in a while and go white-water rafting.”
“That sounds like fun!”
Kun shook his head. “It’s challenging but exciting. I get a rush every time I go.”
You thought out loud. “I’d love to try it sometime…”
Kun pat you in the back. “When you are at one hundred perfect, I’ll give you the green light. Sounds good?”
You nod.
___
You’d wrapped up your midterm and you were ready to head home and take a nap. You walked through the student quad.
“Y/n!” Sicheng called out to you.
You turned around and found Sicheng running towards you.
You smiled, already warm in the face. “Hi.”
“I was wondering if you were free right now…”
“Really? Me?”
He smiled, confused at your question. “Yeah, you. Want to go to the movies with me?”
You nodded. “Absolutely.”
Sicheng drove you guys to the movies. He bought the tickets and the snacks. He let you pick the movie. You picked The Blair Witch Project. It came out over twenty years ago but the theater was doing a limited time screening of it.
You and Sicheng couldn’t shut up throughout the whole movie as you whispered to each and made each other laugh. You’d almost gotten kicked out of the theater.
You left the theater together and he asked you to dinner. You said yes. You were starting to think that this was a date.
“Y/n, this is a date, right?” He asked you at dinner.
You stopped eating your chicken parmigiana and looked at him with big eyes. “I think...Is it?”
Sicheng sighed. “I wanted it to be…”
You laughed. “Oh, thank God. I thought it was all in my head for a second. Maybe you were this nice to all of your friends.”
He pointed out, “I am not this nice to my friends, I can promise you that.”
Sicheng drove you home and kissed you goodnight before you entered your house. You felt like you were floating on a cloud now.
___
Two days later, there was a campus alert that Sicheng had gone missing. His face was all over the news. The last time he was heard from was when he told his best friend Jaehyun that he was going to ask you out to the movies. The last time he was seen was when he took you home.
Sicheng’s car was found a mile away from the dorms. The key was still in the ignition and his wallet and phone were left behind.
You were brought into the police station for questioning and you told them everything that happened the night Sicheng disappeared.
You were worried. What could have happened to him? Would he be alright? Would he be able to come back home? You missed him so much.
You took an evening stroll around your neighborhood to try and calm down. You reached the park where there was no other soul in sight.
Suddenly, you felt a tingly sensation in the back of your neck. You felt that someone was following you.
You began to walk faster. Suddenly, you were pinned to the ground and everything turned black.
___
You woke up in Room 1196, then. Wait...It wasn’t 1196...It was a different room in Neo Hospital. The room was dark and you could only hear the sound of your breathing. It grew more hysterical with each second.
You felt a burning sensation in your neck. You cried out in pain. You cried out, “Help me, please.”
“Y/n…” You recognized Kun’s voice.
You nearly yelled out in pain but restrained yourself. “What...happened?”
“An animal attack,” he started.
You frowned. “What?”
Kun sighed. “It was good that I was there to help you in time, y/n…”
“What?”
Kun moved your hair out of your face. “I was in the neighborhood when I saw the beast attack your neck.”
“A beast?” You frowned.
“Sicheng, was it?”
Your eyes widened. “How do you-“
“You can’t hide anything from me, y/n...You know that’s not how our relationship works.”
“What are you talking about? Ahhhhh.” The pain was getting to be too much for you.
“Can you put two and two together, y/n? Sicheng bit you.”
You shook your head furiously. “No, he wouldn’t-“
Kun snapped his fingers and Sicheng entered the hospital room. His bright expression nowhere to be found. His eyes were a bright red and his lips had traces of blood on them.
“Sicheng?!” You asked.
Sicheng smiled, showing fangs in his teeth. “Hi, y/n…”
“Oh, my God!” You started.
Kun grew annoyed. “Alright, that’s enough pleasantries for my taste. Go.”
Sicheng walked away at his command.
You began, “What the-“
Kun smiled brightly at you then. This time, his straight white teeth displayed his own fangs. “Y/n...Sicheng has put you in a bit of a bind, hasn’t he?”
You tried backing away from Kun and getting off of the bed but it was almost as if the pain kept you from moving.
Kun ran the back of his hand down your cheek. “When a newborn vampire bites you, the bite is lethal...You could die anywhere between minutes and hours...It depends on the bitten, really…”
You flinched at his touch. “What...did you do to me?”
Kun inched closer to you and you winced. He lathered up the blood that leaked from your neck down to your collarbone.
“What had to be done, y/n. From the moment I first saw you, I knew that I had to have you.”
You cried out in pain. “Somebody help me, please! Sicheng, please!”
Kun, annoyed over you mentioning Sicheng, shut the door to the hospital room. “It’s useless, y/n. Sicheng wouldn’t be in this mess if he hadn’t infiltrated what is mine. Now Sicheng must endure the consequences and be at my mercy. I turned him so now he looks to me for instructions. Until I release him...Perhaps in the next millennium...”
You sobbed. “Kun, please make this pain stop! I can’t take it!”
He cooed. “I know, baby. I want to help you. Just say the word and I’ll make the pain go away.”
The pain dominated your senses so you couldn’t process how exactly he would make it go away. “Okay! Just do it!”
Kun got up onto the bed and straddled you. He leaned down towards your neck and bit into you.
You cried out again but this time the excruciating pain turned into a euphoria so glorious, you never wanted it to end. You wrapped your arms around Kun as he continued to drink your blood.
___
It was morning when you had woken up. You were in Room 1196 now. You shot up from your bed and found Kun seated right beside you.
“Good morning, darling,” he started.
You glared at him. “Bite me. Oh, wait, you already did.”
He smiled. “I see your energy is up. That’s good to see.”
You rolled your eyes. “I’m going home…”
Suddenly, you stopped right at the door and your throat started to burn. Your senses heightened and you could sense that one of the nurses was walking right past your room’s door. You wondered what she would taste like if you caught her by surprise right then and there and…
What the holy hell were you thinking?
Kun sighed. “Don’t kill Joyce. She’s the most competent nurse on the staff.”
You ran into your bathroom door and looked at yourself in the mirror.
But you couldn’t.
You put a hand over your mouth and sobbed. “Kun!!!!!”
Kun joined you in the bathroom. “Ah, yes. You won’t be able to gain access to your reflection for another twenty years.”
“Twenty years...What is going on?”
“But what else, y/n? I turned you. To save your life.”
“Turned me into what, Kun?! Say it!”
Kun smiled. “Darling, you already know. Just admit it to yourself.”
You cried. “No…”
“You’ve always wanted a new body. A new life, y/n. And I’ve given it to you. I’ve made you the most powerful creature on this damned planet: a vampire.”
You fell to the ground. You could feel your fangs against your tongue.“Kun! Why did you do this to me? What did I ever do to you?”
Kun sat with you on the ground. “Because I love you, y/n. I never want to be apart from you again.”
You spat in his face. “You made me into a monster.”
Kun, unbothered, wiped your spit away with the sleeve of his coat. “I did not. I made you the best version of yourself you can be. Time for you has become infinite. Your body is immune to all illnesses now. You can see clearly. Your metabolism is in top shape. You are a goddess now.”
You shook your head. “Kun, take it back.”
He chuckled. “You’ve seen enough movies to know that that’s not how it works, y/n...You are mine now. Forever. Just like Sicheng. Just like a lot of the staff in this hospital.”
You shook your head rapidly. “Like hell I’m yours.”
“Y/n, I have been very generous up until this point. Using my blood to help you overcome your chronic condition. Funding your hospital bills...The least you can do is submit to me....”
It was hard to process all of the truths he just delivered. “Your blood?”
He laughed. “You mean you couldn’t taste my blood in the herbal mixture?”
You were about to throw up.
He chuckled darkly. “Admit it, y/n. You loved it.”
“Fuck you, Kun!”
He smiled. “We’ll get to that…”
You sneered. “You are despicable.”
His smile faded. “And you are testing my patience…” He snapped his fingers at you. “On your knees…”
You stayed on the floor with your arms crossed across your chest.
He frowned as he snapped again. “On your knees, y/n.”
“I don’t think so,” you said.
Kun looked taken aback. “What? How?”
You got up from the ground and looked at him. “I will never submit to you for as long as I live..” If vampires were even considered living.
You ran quickly out of the hospital room, realizing you had superhuman speed now. You were able to leave the historial without facing any temptation to bite someone.
But your thirst had to be satisfied somehow and you had to find a way to quench it without hurting anyone.
___
[2 years later]
You’d skipped town not long after you turned. You sent letters to your family without a return address so as not to risk their safety.
Dear Mom and Dad,
I’m so sorry I ran away. I had no choice. If I didn’t leave, you all would’ve been in danger. One day, I hope to explain it all to you but in the meantime, live your lives fully and love each other. Don’t take anything for granted. I love you so much and will see you again.
Love,
y/n
You had become an infamous blood bag bandit as you moved across the country, running away from Kun. He would occasionally try and track you. Or he would send his henchman like Sicheng to do it for him.
You were lucky so far. You had never attacked a human being and sustained yourself on some blood bags you were able to nab from donating trucks.
The reason why you didn’t submit yourself to Kun that day was indeed because of his blood. Consumption of his blood made you immune to his influence. He couldn’t have you like he had wanted all along.
Kun had been obsessed with you from the very beginning. When you were discharged from the hospital the time you met him, he continuously stalked you. At college, at the grocery store, at your home...It would explain why he was able to send Sicheng to attack you.
He always knew where you were back then.
Kun commanded Sicheng to bite you then and put you at risk of dying. Kun’s plan was to save you, make you his vampire queen, and control you.
It was a shame he failed to see that his creation of medicinal herbs was the one thing that would lead to his plan’s failure.
You were immune to his commands and you weren’t going to stick around and see how else he would try and “win you over”.
According to your research, in all public records, Kun was now twenty-six. A blatant lie since he couldn’t age. So you wondered how long he would remain in your hometown. You kept a careful eye on your family every now and then. You’ve made some contacts to track your family occasionally, as well.
Kun had stooped low and you prayed he wouldn’t stoop even lower to get you.
You worked hard every day to work on your rapidly growing vampiric abilities. You couldn’t stick around anywhere for too long without arousing suspicion.
Now you weren’t confined to one space anymore.
You were confined to running.
You hoped to one day bring it this madness to an end and take Kun down. Save Sicheng and Kun’s other minions.
And for you to truly be free.
[Fin]
#Kun#qian kun#wayv Kun#Nct Kun#kun imagine#Kun scenario#Kun boyfriend#Nct boyfriend#wayv boyfriend#nct x you#wayv x you#Nct x reader#wayv x reader#Nct romance#wayv romance#nct halloween blurb#nct halloween#wayv halloween blurb#wayv Halloween#Nct fantasy#wayv fantasy#Nct horror#wayv horror#kun scenario#kun blurb#nct yandere#wayv yandere#kun yandere
339 notes
·
View notes
Text
MD KaiJou ideas - Part 2
Kaiba: Starting scenarios
See Part 1 here
See Jonouchi Scenarios here
See Combined Scenarios here
See Mid-arc Dramas here
Generally Kaiba has to make the first move to invite Jonouchi into his life somehow (usually as a friend), as it is very difficult to convincingly shift his worldview without significant time and energy.
Because of this, there are various scenarios that are concocted to trigger this change in his life.
1) Mokuba hangs out with Jonouchi
Mokuba is developing an ongoing friendship with the main cast, with Jonouchi being a close friend. This causes Kaiba to constantly interact with Jonouchi at a consistent rate.
This is the best way to get a healthy relationship going between Kaiba and Jonouchi. Kaiba may try to push Mokuba away from the group but is likely to adhere to what Mokuba wants.
Jonouchi can start to learn more about Kaiba as a person and start to understand him. Kaiba will likewise learn about Jonouchi via Mokuba and eventually may open himself up to him.
Can get Jonouchi acting as an older brother too towards Mokuba.
For extra drama, could get Mokuba to have a one-sided crush on Jonouchi for a while.
2) Kaiba is prescribed friendship
Kaiba’s mental health is declining in some way (e.g. depression, manic episodes, etc) which is notably affecting his work. His psychiatrist/doctor/therapist recommends seeking out friendships and developing a trust system
(Note: I am not a doctor - this advice is made up for the scenario).
Kaiba, who is taking this seriously and is now determined to improve himself, is now a bit more open to inviting Jonouchi (and the rest) into his life - especially now that he is making an effort it.
Can possibly even have Jonouchi be the perscriber, although that can make for an unhealthy doctor/client relationship.
3) Kaiba gets his coffee from the cafe Jonouchi works at
Kaiba gets his daily coffee from the Kaiba Corp coffee shop that Jonouchi works at. This opens up interactions with Jonouchi in a frequent manner.
This does, unfortunately, have the problematic ‘boss dating subordinate’ situation.
This also assumes Kaiba likes to get his own coffee. Maybe he uses it as an excuse to take a break from work?
4) Kaiba is an alcoholic
Kaiba is in a situation that leads him to alcoholism (not helped by Japan’s work drinking culture). A drunk Kaiba at functions can often lead to different scenarios, especially if Jou is a bartender or waiter.
Darker narratives can extend this to drug use.
5) Kaiba starts recreating other duelists in VR using AI
This can be a space for him to safely explore his sexuality, or even to just open himself up to said AI (since he has complete control over it)
This can sometimes lead to Kaiba simply settling for the AI and not the real person, although that in itself can make for some decent drama.
Can also explore narratives around the ethics of misusing AI based on real people.
6) Mokuba has left Domino City
Mokuba has decided to do his own thing in America (either extending Kaiba Corp or his own dream). This can intensify Kaiba’s loneliness, and thus he becomes more chatty or a bit more open to more interaction in his life.
The amount of distance between the brothers can vary. Could have Mokuba leave on a bad note and never communicate at all, or could have him chat to Kaiba every other day online.
For darker narratives this may result in the aforementioned alcoholism and/or declining mental health.
7) Kaiba is broke
Kaiba has become broke, his company has tanked, or the company has been taken from him in some way. This can even out the wealth gap between Jou and Kaiba and have them on a similar playing field.
Jonouchi could offer him a home, and can teach him how to be thrifty (should Kaiba needs to learn)
Depending on Kaiba’s mental health, he can either be driven to climb his way back, or be in despair and lose all hope.
Bonus points if Jou is a key factor in helping him get back ahead.
8) Kaiba is having dreams about Jonouchi
This can be sexual, intense or just very personal. Reasons for this happening can vary, but sometimes there doesn’t need to be a reason
This can cause Kaiba to try to figure out why he is having these dreams, and what it may mean (if he has mellowed in his dub-version’s skepticism).
Thus leading to observations and potential interactions with Jonouchi. (Or alternatively attempts at avoidance, which Jou picks up on and bugs him about)
9) Kaiba’s new bodyguard is Jonouchi
This allows for a lot of interaction between them, however does mean Kaiba has power over him as an employer.
Potential to have Jonouchi rescue Kaiba or get injured trying to protect him - thus providing potential hurt/comfort scenarios.
Can increase drama by having high stakes scenarios with big injuries.
10) Jonouchi’s dance/singing/performance impresses Kaiba
Kaiba attends a concert and finds Jonouchi performing (dancing/singing/etc), and is impressed by the performance. Lots of potential threads here.
Kaiba could become a secret hardcore fanboy
Kaiba could be seduced by the performance (either intentional by Jou or not)
Kaiba could sign him on to Kaiba Corp events, leading to more interactions
Can lead to private performances, and/or Kaiba listening to Jou’s music in his spare time.
11) Kaiba is in a coma / deep sleep / can’t wake up
Often attributed to faulty VR tech. Mokuba/Kaiba Corp creates some technology to allow Jonouchi to enter his mind and pull him out.
This has the benefit of Jonouchi being able to see the true Kaiba inside his mind - which can allow Jonouchi to understand and empathise with Kaiba much more.
This can lead to angst / dark narratives if unveiling some of Kaiba’s more twisted mind.
See hospital scenario for when tech can’t help.
12) Kaiba is stuck in VR
Very similar to the coma one, but he can now access digital technology so can interact with the outside world should he need to.
Also Jou would not be delving into his mind directly but simply into the VR world to retrieve him.
Could utilise glitching for humor and/or drama.
13) Kaiba decides to experiment with his sex life
May go out to a gay club undercover (where Jou goes/works), or go to a private sex work company (which could also be where Jou works).
In the case where Jou does sex work, could either have Jou and Kaiba meet there by surprise, Jou try pretend that he is someone else (in the event Kaiba does not realise he works there) or could have Kaiba specifically choose Jou (to Jou’s bewilderment).
14) Kaiba is competing with a rival company (that Jou works for)
Kaiba finds there is a rival company making their way into his territory and are making a name for themselves. Jonouchi, ideally, is involved with this company professionally.
This can elevate Jonouchi to a level that he can interact with Kaiba on at a professional level.
15) Kaiba discovers and befriends Jonouchi online
Can be done with VR avatars or random screen names, leading to drama at the reveal.
Bonus points if Kaiba has no idea it’s Jonouchi, and/or vise versa. Can lead to drama on the realisation on who each other are.
Alternatively, Kaiba may be a fan of Jonouchi streaming and become a bit of a fanboy (without Jonouchi knowing)
16) Kaiba sponsors Jonouchi as a professional duelist
This can lead to many potential interactions.
Main issue is the boss/employee relationship dynamic - Kaiba has significant power over Jonouchi.
Bonus points if Kaiba loses a duel to Jou at some point, causing drama.
17) Kaiba is recovering from a recent breakup
He may seek a rebound, or possibly Mokuba may seek Jou to help Kaiba recover.
Can enter into dark/abuse narratives with the ex.
Main difficulty here is getting Kaiba to trust anyone ever again after having his heart broken.
18) Kaiba is injured and is currently in hospital
This can either be for major injuries (e.g. gunshot wound, head injury) or minor ones.
This allows people to possibly visit him (like Jou). Depending on the injury he may or may not realise they are visiting (e.g. coma).
19) Kaiba wakes up, after having fallen for and started a relationship with Jou in a dream
For when you want a quick start to pining but don’t want all the setup
.A bit of a cop out, but it does the job.
Darker Narrative Scenarios
These are the more angst/dark/disturbing leaning scenarios. These are ok for large hits of drama and angst but often ends up changing Kaiba’s personality significantly depending on how his mental health goes.
1.) Mokuba has died
This would be a very traumatic event for Kaiba, so this will nearly always lead to a dark narrative often with mental health breakdown.
Can lead to suicide scenario.
Can lead to major personality shift
2) Kaiba has become suicidal
There can be a variety of reasons that lead to this.
Often the story has Jonouchi be present should Kaiba nearly attempt, opening the door for Jonouchi to help him.
This dark narrative may end up overburdening Jonouchi if not careful.
Mokuba often needs to be out of the picture somehow, or something to distance him from his brother.
Mokuba could be the person to bring in Jou and the gang to help.
3) Kaiba is kidnapped / trafficked / trapped
Jonouchi helps to rescue him and so Kaiba feels indebted to him. This can open up interactions.
Generally it’s Mokuba who seeks out Jou to help.
Kaiba may attempt to avoid Jonouchi afterwards, depending on what state he was in when Jonouchi rescues him.
4) Jonouchi has recently died, but has come back as a ghost and is haunting Kaiba
Usually a bittersweet scenario, unless a way to bring Jonouchi back to life is construed. Alternatively could eventually have Jou live in VR world a la Noah.
Kaiba may start to suffer from being haunted, depending on the nature of it.
Can have many ghost shenanigans such as: ghost commentary, Jonouchi voyeuring Kaiba, awkward moments where Kaiba can’t respond because he is in company of others, and various attempts to communicate should Kaiba not hear him
Can reverse the scenario so that Kaiba is the one who has died, and Jou is being haunted. Often here, headcanoni is that Kaiba is either in denial of his death or is desperate to find a way back to life.
5.) Jou sacrifices himself for Kaiba or Mokuba
Bittersweet in that Jou is already dead. Could have an affect on Kaiba’s mental health.
Bonus points for combining with the ghost scenario
That’s all I have for now. Next will be starting scenarios for Jou - click here to view the post.
3 notes
·
View notes
Text
About Informed Vaccine Consent: Frank Shallenberger, MD, HMD
Published on December 12, 2020
Written by Frank Shallenberger, MD, HMD
(Letter from Frank Shallenberger, MD HMD RE: Covid 19)
Dear Patients and Friends,
Last week I must have been asked 20 times about the new COVID vaccines. Here are my thoughts. Please pass this information onto many as you can. People need to have fully informed consent when it comes to injecting foreign genetic material into their bodies.
1. The COVID vaccines are mRNA vaccines. mRNA vaccines are a completely new type of vaccine. No mRNA vaccine has ever been licensed for human use before. In essence, we have absolutely no idea what to expect from this vaccine. We have no idea if it will be effective or safe.
2. Traditional vaccine simply introduce pieces of a virus to stimulate an immune reaction. The new mRNA vaccine is completely different. It actually injects (transfects) molecules of synthetic genetic material from non-humans sources into our cells. Once in the cells, the genetic material interacts with our transfer RNA (tRNA) to make a foreign protein that supposedly teaches the body to destroy the virus being coded for. Note that these newly created proteins are not regulated by our own DNA, and are thus completely foreign to our cells. What they are fully capable of doing is unknown.
3. The mRNA molecule is vulnerable to destruction. So, in order to protect the fragile mRNA strands while they are being inserted into our DNA they are coated with PEGylated lipid nanoparticles. This coating hides the mRNA from our immune system which ordinarily would kill any foreign material injected into the body. PEGylated lipid nanoparticles have been used in several different drugs for years. Because of their effect on immune system balance, several studies have shown them to induce allergies and autoimmune diseases. Additionally, PEGylated lipid nanoparticles have been shown to trigger their own immune reactions, and to cause damage to the liver.
4. These new vaccines are additionally contaminated with aluminum, mercury, and possibly formaldehyde. The manufacturers have not yet disclosed what other toxins they contain.
5. Since viruses mutate frequently, the chance of any vaccine working for more than a year is unlikely. That is why the flu vaccine changes every year. Last year’s vaccine is no more valuable than last year’s newspaper.
6. Absolutely no long term safety studies will have been done to ensure that any of these vaccines don’t cause the cancer, seizures, heart disease, allergies, and autoimmune diseases seen with other vaccines. If you ever wanted to be guinea pig for Big Pharma, now is your golden opportunity.
7. Many experts question whether the mRNA technology is ready for prime time. In November 2020, Dr. Peter Jay Hotez said of the new mRNA vaccines, "I worry about innovation at the expense of practicality because they [the mRNA vaccines] are weighted toward technology platforms that have never made it to licensure before." Dr. Hotez is Professor of Pediatrics and Molecular Virology & Microbiology at Baylor College of Medicine, where he is also Director of the Texas Children’s Hospital Center for Vaccine Development.
8. Michal Linial, PhD is a Professor of Biochemistry. Because of her research and forecasts on COVID-19, Dr. Linial has been widely quoted in the media. She recently stated, "I won't be taking it [the mRNA vaccine] immediately – probably not for at least the coming year. We have to wait and see whether it really works. We will have a safety profile for only a certain number of months, so if there is a long-term effect after two years, we cannot know."
9. In November 2020, The Washington Post reported on hesitancy among healthcare professionals in the United States to the mRNA vaccines, citing surveys which reported that: "some did not want to be in the first round, so they could wait and see if there are potential side effects", and that "doctors and nurses want more data before championing vaccines to end the pandemic".
10. Since the death rate from COVID resumed to the normal flu death rate way back in early September, the pandemic has been over since then. Therefore, at this point in time no vaccine is needed. The current scare tactics regarding "escalating cases" is based on a PCR test that because it exceeds 34 amplifications has a 100% false positive rate unless it is performed between the 3rd and 5th day after the first day of symptoms. It is therefor 100% inaccurate in people with no symptoms. This is well established in the scientific literature.
11. The other reason you don’t need a vaccine for COVID-19 is that substantial herd immunity has already taken place in the United States. This is the primary reason for the end of the pandemic.
12. Unfortunately, you cannot completely trust what you hear from the media. They have consistently got it wrong for the past year. Since they are all supported by Big Pharma and the other entities selling the COVID vaccines, they are not going to be fully forthcoming when it comes to mRNA vaccines. Every statement I have made here is fully backed by published scientific references.
13. I would be very interested to see verification that Bill and Melinda Gates with their entire family including grandchildren, Joe Biden and President Trump and their entire families, and Anthony Fauci and his entire family all get the vaccine.
14. Anyone who after reading all this still wants to get injected with the mRNA vaccine, should at the very least have their blood checked for COVID-19 antibodies. There is no need for a vaccine in persons already naturally immunized.
Here's my bottom line: I would much rather get a COVID infection than get a COVID vaccine. That would be safer and more effective. I have had a number of COVID positive flu cases this year. Some were old and had health concerns. Every single one has done really well with natural therapies including ozone therapy and IV vitamin C.. Just because modern medicine has no effective treatment for viral infections, doesn’t mean that there isn’t one.
Yours Always,
Frank Shallenberger, MD, HMD
Source Credit: H/T🎩Frank Shallenberger, MD, HMD
https://principia-scientific.com/about-informed-vaccine-consent-frank-shallenberger-md-hmd/?fbclid=IwAR12UWln6S0BcQgyWISIBR8mcqvrsZaZHs2RBhIGyqDvf0Ev-tC6SYV6zCg
3 notes
·
View notes
Link
Yves here. Reader IM Doc, an internal medicine practitioner of 30 years, trained and worked in one of the top teaching hospitals in the US for most of his career before moving to a rural hospital in an affluent pocket of Flyover. He has been giving commentary from the front lines of the pandemic. Along with current and former colleagues, he is troubled by the PR-flier-level information presented to the public about the Pfizer and Moderna vaccines, at least prior to the release of an article in the New England Journal of Medicine on the Pfizer vaccine: Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. However, he did not find the study to be reassuring. He has taken the trouble of writing up his reservations after discussing the article with his group of nine physicians that meets regularly to sanity check concerns and discuss the impact that articles will have on their practices.
By IM Doc, a internal medicine doctor working in a rural hospital in the heartlands
Right off the bat – I am as weary and concerned about this pandemic as anyone. What my little rural area has been through in the past three weeks or so has been nothing short of harrowing. This virus has the ability to render patients about as sick as I have ever seen in my life, while leaving more than half the population with minimal if any symptoms. The patients who are sick are often very sick. And instead of slow and steady improvement like we normally experience, most of these patients are assigned to a long and hard slog. Multiple complications arise. This leads to very diminished throughput in the hospital. The patients literally stack up and we have nowhere to put the new ones coming in who themselves will be there for days or weeks. On top of that are the constant donning and doffing of PPE and intense emotional experiences for the staff, who are themselves becoming patients or in this small town have grandma or Aunt Gertrude as a patient.
To put it bluntly, I want this pandemic over. And now. But I do not want an equal or even worse problem added onto the tragedy. And that is my greatest fear right now. And medical history has demonstrated conclusively over and over again: brash, poorly-thought-out, emotion-laden decisions regarding interventions in a time of crisis can exponentially increase the scale of pain and lead to even worse disasters.
I am not an anti-vaxxer. I have given tens of thousands of safe and tested vaccines over my lifetime. I am very familiar with side effects and safety problems associated with all of them. That is why I can administer them with confidence. I am also an optimist, so all of the cautions I discuss below are the result of experience and the information made public about the Pfizer vaccine, not a temperamental predisposition to see the glass as half empty.
I know this piece is long, but I wanted to completely dissect the landmark New England Journal of Medicine (from now on NEJM) publication of the first Pfizer vaccine paper. I am replicating the method of my mentor in Internal Medicine, a tall figure in 20th Century medicine. He was an internationally recognized authority and his name is on one of the foundational textbooks in his specialty. He was a master and he taught me very well, including the fundamentals of scientific inquiry and philosophy, telltale signs of sloppy or dishonest work, the order in which you should dissect someone’s work, and the statistics involved.
When I have a new medical student doing rotations with me, I give them a collection of reading. At the very top is Drug Companies & Doctors: A Story of Corruption from the New York Review of Books in 2009 by Marcia Angell, MD. She was the editor-in-chief of the NEJM, the very journal that published this Pfizer vaccine paper.
Dr. Angell’s article is the Cliffs Notes version of much longer discussions she had about corruption, corporatism, managerialism, profiteering, greed, and deception in in the medical profession. Patient care and patient concerns and indeed patient lives in her mind have been absolutely overcome by all of these other things. It is a landmark paper, and should be read by anyone who is going to interact with the medical community, because alas, this is the way it is now. I view this paper the exact same way I view Eisenhower’s speech about the military industrial complex. What she said is exactly true, and has only become orders of magnitude worse since 2009.
And now the paper.
Unfortunately, this study from Pfizer in the latest NEJM, and indeed this whole vaccine rollout, are case studies in the pathology Agnell described. There are more red flags in this paper and related events than present on any May Day in downtown Beijing. Yet all anyone hears from our media, our medical elites, and our politicians are loud hosannas and complete unquestioning acceptance of this new technique. And lately, ridicule and spite for anyone who dares to raise questions.
I have learned over thirty years as a primary care provider that Big Pharma deserves nothing from me but complete and total skepticism and the assumption that anything they put forth is pure deception until proven otherwise. Why so harsh? Well, to put it bluntly, Big Pharma has covered my psyche with 30 years of scars:
• As a very young doctor, I treated an extraordinary middle-aged woman who had contracted polio as a toddler from a poorly tested polio vaccine rolled out in an “emergency.” Tens of thousands of American kids shared her fate1
• The eight patients I took care of until they died from congestive heart failure that had been induced by a diabetes drug called Actos. The drug company knew full well heart failure was a risk during their trials. When it became obvious after the rollout, they did everything they could to obfuscate. Actos now carries a black box warning about increased risk of heart failure
• The three women who I took care of who had been made widows as their husbands died of completely unexpected heart attacks while on Vioxx. I have no proof the Vioxx did this. But when Vioxx was finally removed from the market, the mortality rate in the US fell that year by a measurable amount, inconsistent with recent trends and forecasts. Merck knew from their trials that Vioxx had a significant risk of cardiovascular events and stroke, and did absolutely nothing to relay that danger in any way. Worse, they did everything they could to muddle information and evade responsibility once the truth started to come out
• The dozens upon dozens of twenty and thirty-something patients who have been rendered emotional and spiritual zombies by the SSRIs, antipsychotics and amphetamines they have been taking since childhood. Their brain never learned what emotions were, much less how to process them and we are left with empty husks where people never developed. The SSRIs and antipsychotics were NEVER approved for anyone under 18. EVER. While there are some validated uses for stimulants in children, they are obviously overprescribed, as confirmed by long-standing media reports of their routine use as a study/performance aid. It is all about the lucre.
• The hundreds and hundreds of 40-60 year olds who have been hollowed out from the legal prescribing of opioids. All the while the docs were resisting this assault, the drug companies and the paid-off academics and medical elites were changing the rules to make physicians who did not treat any pain at all with opiates into evil Satan-worshippers. And they paid for media appearances to drive across the point: OPIATES ARE GOOD. WE HAVE MADE THEM SO YOU CANNOT GET ADDICTED. And here we are now with entire states taking more opioids than in the waning days of the Chinese Empire, and we all know how that story ended. All this misery so a family of billionaires can laugh its way to the bank.
I carry all these people and more with me daily. I would not be doing a service to their memory if I allowed myself to be duped into writing another blind prescription that was going to add yet another scar.
I will dissect the important parts of this paper exactly as my mentor described above taught me. He performed years of seminal research. He was a nationally-known expert in his field.
In medicine, especially in top-tier journals like NEJM, landmark papers are always accompanied by an editorial. These editorials are written by a national expert who almost always has “peer-reviewed” the source material as well. This is how the reader knows that an expert in the field has looked over the source material and that it supports the conclusions in the paper. My mentor did this all the time. The binders all over his office were the actual underlying data that he scrutinized to confirm the findings. There is no way on earth to print and publish the voluminous source material. Editorial review was one sure way all to assure that someone independent, with appropriate experience, confirmed the findings. This was onerous work, but he and thousands of others did it because this is the very essence of science. He was scrupulous in his editorials about findings, problems, and conclusions. It was after all his reputation as well.
My first lesson from him: READ THE EDITORIAL FIRST. It gets the problems in your head before you read the statistics and methods, etc. in the actual paper. It gives you the context of the study in history. It often includes a vigorous discussion of why the study is important.
Admittedly, over the past generation, as the corporatism and dollar-counting has taken over my profession and its ethics, this function of editorial authoring has become at times increasingly bizarre and too-obviously predisposed to conclude with glad tidings of joy, especially if pharmaceuticals are involved.
So I read the editorial first. You can find it on the NEJM webpage, in the top right corner.
And, amazingly, it is basically a recitation of the same whiz-bang Pfizer puffery that we have all been reading for the past few weeks. There really is not much new. Furthermore, it is filled with words like “triumph” and “dramatic success”. Those accolades have yet to be earned. This vaccine has not yet even been released. Surely, “triumph” is a bit premature. Those words would NEVER have been used by my mentor or similar researchers in his generation. They would have been focused on the good, the bad and the ugly. A generation ago, editorial reviewers saw their job as informing the reader and making certain the clinicians that were reading knew of any limitations or problems.
In quite frankly unprecedented fashion, two different events that were carefully reported occurred almost simultaneously with the release of both the paper and the editorial. Both of these events contradict and contravene data and conclusions reported in both the paper and the editorial and I believe they deserve immediate attention. They both belie the assertions of the editorial writers that [emphasis mine] “the (safety) pattern appears to be similar to that of other viral vaccines and does not arouse specific concern”.
First, a critical issue for any clinician is “exclusion criteria”. This refers in general to groups of subjects that were not allowed into the trial prima facie. Common examples would include over 70, patients on chemotherapy and other immunosuppressed patients, children, diabetics, etc.. This issue is important because I do not want to give my patient this vaccine (available apparently next week) to any patient that is in an excluded group. Those patients really ought to wait until more information is available – FOR THEIR OWN SAFETY. And not to mention, exclusion criteria exist because the subjects in them are usually considered more vulnerable to mayhem than average subjects. From my reading of this paper, and the accompanying editorial, one would assume there were no exclusion criteria. They certainly are never mentioned.
I reiterate, the paper is silent on this question of exclusion criteria, as is the editorial. Had my mentor seen something like “exclusion criteria” in the source material, and realized that it was not in the final paper, he would have absolutely included a notice in his editorial. This would have been after calling the principal investigator and directly questioning why there was no mention in the original paper. Patient safety should be foremost on everyone’s mind at all times in clinical research and its presentation to practitioners.
And now we know there were exclusion criteria, not because of anything Pfizer, the investigators, or the NEJM did but because of stunning news out of the UK. UPDATE: I will address this at greater length, but an alert reader did find the study protocol, which were not referenced in any way that any of the nine members in my review group could find, nor were they mentioned in the text of paper or editorial, as one would expect for a medication intended for the public at large. I apologize for the oversight, but this information was not easy to find from the article, not mentioned or linked to from the text of the article, the text of the editorial, in the “Figures/Media,” or in a supplemental document.
In the UK on day 1 of the rollout, two nurses with severe allergies experienced anaphylaxis, a life-threatening reaction to this vaccine. Only after world-wide coverage did Pfizer admit that there was an exclusion criterion for severe allergies in their study.
Ummm, Pfizer, since we are now getting ready to give this to possibly millions of people in the next few weeks – ARE THERE ANY OTHER EXCLUSION CRITERIA? Should I, as a physician, specifically not be giving this to patients with conditions that you have excluded?
Furthermore, NEJM, since you published this trial, have you bothered to at least put a correction on this trial on your website that it should NOT be given to people with severe allergies? I certainly see nothing like this.
Should someone from the NEJM or the FDA be all over Pfizer to ascertain the existence of other exclusion groups so we do not accidentally harm or kill someone over the next two weeks?
Unfortunately, Americans, you have your answer from the FDA about severe allergic reactions right from a press conference in which Dr. Peter Marks, the director of FDA’s Center for Biologics Evaluation and Research is quoted as saying:
Even people who’ve had a severe allergic reaction to food or to something in the environment in the past should be OK to get the shot….1.6% of the population has had a severe allergic reaction to a food or something in the environment. We would really not like to have that many people not be able to receive the vaccine.
Are you serious? Dr. Marks, have you ever seen an anaphylactic reaction? I live in a very rural area. Many patients live 30 minutes or more from the hospital. What if one of them had an anaphylactic reaction to this vaccine hours after administration, had no epi-pen and had to travel a half hour to get to the nearest hospital? There is a very high likelihood that a good outcome would not occur. Sometimes, as a physician, I simply cannot believe what I am hearing out of the mouths of our so-called medical leaders.
To the writers of the editorial accompanying this research:
Did you actually look at the source material? The existence of at least one exclusion criterion for severe allergic reactions had to be in there somewhere. If you did look at the source material, are there others that the physicians of America need to know about? If they were not in the source material, after the events in the UK, has anyone bothered to follow up with Pfizer about this omission?
Does anyone at NEJM or Pfizer or FDA plan to fully inform the physicians of America? Does ANYONE at NEJM or Pfizer or FDA care about patient safety?
Now for the second story that got my attention this week, an article from JAMA Internal Medicine, a subsidiary of JAMA, The Journal of the American Medical Association.
JAMA, like NEJM, is one of America’s landmark medical journals. I will assure you that JAMA is not the National Enquirer. This piece was written by a nursing researcher. It is very likely she is well-versed in all aspects of American medical research.
In her story, she details her recruitment and her experience in the Pfizer COVID trial, the same one we are dissecting here. She describes in detail her experience with the vaccine and the fact that she is concerned that many patients are likely going to feel very sick after the injection. She wrote up her own reactions, and included a very troubling one. About 15 hours after her second injection, she developed a fever of 104.9. She explained that she called her reaction to the Research Nurse promptly the next morning. The recounted the response of the Research Nurse to her information as “A lot of people have reactions after the second injection. Keep monitoring your symptoms and call us if anything changes.”
Thankfully, it appears this nurse has completely recovered. From the best I can tell, this encounter occurred in late August and early September, putting it well within the trial’s recruitment of arms as detailed in the paper.
This JAMA article impinges directly on Figure 2 on page 7 of the paper, a graphic that that lays out all the major side effects during in the trial.
It is very important to note that based on the trial’s own data, conveniently laid out on the very top of the figure in green, blue, orange and red, a temperature of 104.9F or 40.5 C is described as a Grade 4 event. The definition of a Grade 4 event is anything that is life-threatening or disabling. A fever of 104.9 can have grave consequences for any adult and is absolutely a Grade 4 event.
By law, a grade 4 event must immediately be reported to the FDA, and to the Institutional Review Board (the entity charged with overseeing the safety of the subjects) and to the original investigators. THERE IS NO EXCEPTION. One would think that would also be reported in the research paper to at least alert clinicians to be on the lookout.
I could not find any mention of this event in the text of the paper. NOT ONE. Let’s take a closer look at Figure 2 on page 7 where adverse events are reported in a table form. Please note: this is a very busy image, and in the browser version, with very low resolution graphics that are profoundly difficult to read (they are a bit clearer if you download the PDF). This is a time-tested pharmaceutical company tactic to obscure findings that they do not want you to see. My mentor warned me about ruses like these years ago, and finding one raises the possibility that deception is in play.
The area for the reporting of this Grade 4 reaction would be on the 2nd row down at the left of the set called B, titled systemic events and use of medication. The area of concern would be where the graph is marked with the number 16. Do you see a red line there? It would be at the very top. I have blown this up 4 times on my computer and see no red there. I am left to assume that this Grade 4 “Life Threatening or Disabling” event that was clearly within the time parameters of this trial was not reported in this study.
To those who say that I am making way too much out of one patient with a severe fever, let’s do a little math. There are 37,706 participants in the “Main Safety Population” (from Table 1), of which 18.860 received the vaccine.2 Let us assume that this individual was the only one that had a GRADE 4 reaction. Let us also assume that the end goal is to vaccinate every American a total of 330,000,000 people. So if we extrapolate this 1 out of 18,860 into all 330,000,000 of us, it suggest that roughly 17,500 could have this kind of fever. Now assume a 70% vaccination rate, and you get that would be approximately 12,250. I hope you now understand that in clinical medicine related to trials like this – a whole lot of nothing can turn into a whole lot of something quickly when you extrapolate to the entire targeted group. Does anyone not think that the clinicians of America should be prepared for anything like this that may be coming?
A couple more questions for NEJM and the editorial writers:
Were you ever made aware that this Grade 4 reaction occurred? Now that we have a reliable report that it occurred, has there been any attempt to investigate?
Did the Research Nurse actually report this event? If not, was she just simply not trained or was there deliberate efforts to conceal such reactions? How many more reactions were reported anywhere this trial was conducted and that did not make it to the FDA, the IRB or possibly the investigators? Is that not a cause for concern?
As if this is not enough, there is so much more wrong with this editorial. Now we are going to talk about corruption.
I want to reiterate my concern that over the past generation, as my profession has lost its way, its medical journals have turned into cheering sections for Big Pharma rather than referees and safety monitors. We all should relish the great things medical science is doing, but we should be doing EVERYTHING we can to minimize injury and death. Too often our journals have become enablers of Big Pharma deceiving our physicians and the public. Unfortunately, this paper and its editorial look troublingly like a case study of this development.
To provide context, I looked over the last month of the NEJM, the issues from November 12, 19 and 26th and December 3rd. Based on having read the NEJM over the years, I believe these four weeks are representative.
During this period, there were 15 original articles published in the fields of Oncology, General Surgery, Infectious Disease, Endocrinology, Renal, Cardiology, Pulmonary and Ear Nose & Throat. Of these 15 articles, the editors thought that eight were important enough to have an editorial from an acknowledged expert. I have read every one of these studies and the editorials as I do every week. All eight in the past month were indeed by leading experts in the field of the underlying studies. They included a COVID vaccine overview reviewed by an leading figure in vaccinology, and two COVID papers about Plaquenil and other approaches discussed by top infectious disease experts.
It was unlikely that those papers were going to get national media attention. All medical stuff.
But here we have our Pfizer vaccine paper. We have 300,000 fatalities in the USA alone and millions of cases. We have whacked our economy, we are in the depths of a national emergency. And we have a paper, the first, that may offer a glimpse of hope. Certainly this would be a landmark paper, and certainly it was treated in that manner? Right?
One would think that the doctors of America would have this study explained to them by a world-known vaccinologist? NOPE…..Maybe a virologist? NOPE….. Maybe a leading government official? Dr. Fauci? Dr. Birx? Dr. Osterholm? NOPE…..Maybe an expert in coronaviruses? NOPE…
We get the Pfizer ad glossy editorial treatment from Eric Rubin MD, the editor-in-chief of the NEJM. And Dr, Longo, an associate editor. Dr. Longo is an oncologist. Dr. Rubin is at least a recognized infectious disease doctor, but his specialty based on my Google search is mycobacterium, not virology. Again, one would normally anticipate for a paper of this importance, the editorial would be from someone with directly on point expertise.
Why would this fact been important to my mentor? (and I had the privilege of hearing him trash a paper in an open forum about a very similar issue, a paper introducing a drug to the world that later was the disaster of the decade, Vioxx) Why is this important to me and all the other physicians in my review group here in flyover country yesterday?
Because the choice of authorship of the editorial leads you to one of only several conclusions:
• Pfizer would not release the source data because of proprietary corporate concerns and no self-respecting expert would review without it
• Pfizer knew there are problems and did not want anyone with expertise to find out and publicize them
• The editors could not find a real expert willing to put their name on a discussion
• Drs. Rubin and Longo are on some kind of journey to Vanity Fair and wanted their names on an “article for the ages”
• This is a rush job, and no one had time to do anything properly, and so we just threw it all together in a flash
Readers, pick your poison. If anyone can think of a sound reason, please let me know. I am all ears.
But let’s open up the can of worms a bit more. Pfizer supports NEJM. Just a brief swipe through of recent editions yielded several Pfizer ads. A Pfizer ad appeared on my NEJM website this AM. I do not know how much they pay in advertising but appears to be quite a bit.
Americans, have we devolved so far in our grift that it is now appropriate for the EDITOR-IN-CHIEF of our landmark medical journal to be personally authoring “rah rah” editorials about a product of a client that supports his journal with ad dollars? And he has the gall to not present this conflict on his disclosure form? Really? Am I the only one worried about this type of thing?
Now we travel from the can of worms to the sewer. And this impacts every single one of us. I want you to Google the names of the people on the FDA committee that voted 17-4-1 two days ago to proceed with the Emergency Use Declaration. Go ahead – Google it. On that list, you will find the name Eric Rubin, MD. Why yes indeed, that is the very same Eric Rubin MD who wrote this editorial. Who is the Editor-in-Chief of the NEJM. A publication that certainly takes ad dollars from Pfizer. And he was one of the 17 to vote for the Pfizer product to be immediately used in an emergency fashion. Oh yes, oh yes he was.
Am I the only one who can recognize that Pfizer and other pharma companies may have some influence on Dr. Rubin thanks continued support of his employer, the NEJM? Am I the only one concerned that Dr. Rubin’s “rah rah” editorial may have been influenced by Pfizer? Is anyone else troubled that the Editor-in-Chief of the NEJM, supported by Big Pharma advertising dollars, is sitting on an FDA board to decide the fate of any pharmaceutical product? Is this not the very definition of corruption? Or at least a severe conflict of interest? I strongly suspect that a thorough evaluation of members of that committee will reveal other problems. As my grandmother always used to say, “There is never just one roach under a refrigerator.”
I looked in vain all day today for media discussions of conflicts of interest with Dr. Rubin or anyone else in a position of authority. I found nothing.
What I did find was the Boston NPR affiliate WBUR discussing Dr. Rubin’s Yes vote. You can listen yourself:
This interview left me much more concerned about Dr. Rubin’s role and what exactly he read in the raw data from Pfizer. In this interview, he admits that he as an FDA advisory member has seen no data from the Moderna trial coming up for a vote this week:
These two vaccines are fairly similar to one another, so I am hoping the data will look good, but we haven’t seen the data yet, so I reserve judgement.
Excuse me, but should not the members already have the data and be mulling over it to ask intelligent questions?
These statements left me more worried about the issues I have already brought up with the Pfizer vaccine:
We don’t know if there are particular groups that should or should not get the vaccine…We do not know what will happen to safety over the longer term.
When finally asked specifically about the UK allergic reactions and if they came up in the FDA meeting (emphasis mine):
It did come up and this was a bit of a surprise because in the trial, that trial was limited to specific kinds of participants, there were apparently no incidents like that, nevertheless this suggests it is something we are going to have to look out for.
There is absolutely not a word in the published data to suggest there was a limit to SPECIFIC PARTICIPANTS – what on earth is he talking about? Are there limited specific kinds of patients that we as physicians should be looking to vaccinate?
In a fine finish, toward the end of the interview Dr. Rubin states he is a bit relieved that low risk patients will be getting the vaccine later after we know more about the side effects with the first patients. I am really not trying to be a jerk – but are you kidding me? I thought this vaccine was a triumph with minimal side effects.
Dr. Rubin, kind sir, I really feel that you owe a clarification about your statements in the WBUR interview to the patients and caregivers of America. We are the ones with lives on the line.
First, I have the privilege of sitting on an Institutional Review Board (an independent entity that protects patient safety) and I know something about Grade 4 side effects. Just for 1 Grade 4 side effect in one subject, the accompanying documentation would often be a half a ream of paper. Because I agreed to do that job, it was my obligation to look through that documentation. That half a ream was for one side effect in one trial. Yet, you state unequivocally in this interview, that you, as a sitting member of the FDA committee that oversees the safety of the nation in this affair, have not seen any of the Moderna documentation for that upcoming meeting this week.
For readers to fully understand what I am saying, this Moderna documentation is going to be reams and reams of documents that need to be evaluated carefully to ask the right questions. And you have not yet studied this? For a meeting in just a few days? I find this deeply troubling. Your statements create the appearance the committee you are sitting on is nothing more than a rubber stamp for a decision that has already been made. This would be an absolute tragedy.
Second, Dr. Rubin, you in your position as the Editor-in-Chief of the NEJM and the editorial writer for this research, may be one of the few people on earth that have seen the original Pfizer research. Despite calling this a triumph, you state in the interview that you are relieved that younger people less likely to get the vaccine early so you will have time to wait to see if complications develop in the first patients. You have stated, despite your assertion in the editorial that the side effects were consistent with other vaccines, that “we don’t know if there are particular groups that should or should not get the vaccine”. Have you seen something in that “triumph” research that is concerning enough to you to make such statements? As a physician, I would really like a clarification on this statement, given that the shots are already rolling out today.
Now that we are past the editorial, a few words about the nuts and bolts of the paper.
I look for very specific red flags – usually making the data difficult to interpret. This study did not disappoint.
On page 5, in Table 1, the Demographic Description of the participants, go down to the AGE GROUP area. Note it is divided into only two cohorts 16-55 and >55. This is a real problem. My mentor said an honest paper should never deploy such a tactic.
You see, more than half of my patients are over 70. Why is this kind of obfuscation a real problem for my ability to trust the vaccine? Well, the intro papers to many pharmaceuticals that have gone down the drain in recent years have used this very same device. It is their way of hiding the fact that they did not put many older patients in the trial, certainly not representative of the population, and certainly not representative of who is seemingly going to get this vaccine in the first round. Do I know that 90% of the >55 group is actually between 55-58? I don’t. How hard would it be for them to do a breakdown in decades? 16-25 26-35 36-45 46-55 56-65 66-75 76-85? We have lots of computers in this country and the population breakdown is done this way on studies I read all the time. Why not do provide this information on a study that is this critically important, particularly one where elderly patients will be near the head of the line?
What are they trying to do here? Unfortunately, too often drugmakers resort to this practice to hide their failure to test their drug on the elderly to an appropriate or safe degree, knowing there would likely be lots of problems. Because of their past behavior, I ALWAYS assume this is true until proven otherwise and act accordingly with my elderly patients.
That is the world these companies have made for themselves.
Now for the tables on pages 6 and 7 about immediate side effects.
Just a brief look shows that local soreness and tenderness is very common, up to 75% with this vaccine. That is a bit high, but not that far out of range from my experience with other vaccines.
The tables on page 7 are the whoppers.
Headaches, fatigue, chills, muscle pain and joint pain appear to be very common, way more common than other vaccines I am used to, as in an order of magnitude higher. It is very clear from this table that about half the patients, especially the younger ones, are going to feel bad after this vaccine. That is extraordinary.
We are told nothing about how long these symptoms last or the amount of time at work lost. The “minimal side effects comparable with other viral vaccines” in the editorial and press releases is just not consistent at all with my experience of 30 years as a primary care physician. There was universal agreement with this assessment among my MD colleagues. They had great concern about this as a matter of fact: great concern that it will cause bad publicity and decrease administration and great concern that given this already high side effect profile, it may be much worse when it gets out to the public.
Given the fact that this virus is largely asymptomatic in more than half the people infected, what exactly are we doing here?
Furthermore, unlike other pharmaceutical papers that try to explain variances in symptoms like this, there is not a word offered about possible underlying causes of these outcomes.
The numbers of COVID cases in the placebo group vs the vaccine group have been widely publicized, from 162 cases in the placebo group down to 8 in the vaccine group, giving a relative reduction of 95%. It seemed to all of us in our review group that we do not have nearly enough patients to really make assessments. That is not a criticism. The researchers have done admirably in my opinion to get this many patients this quickly. That is still the problem: they are going to be using the first million patients or so in the general public to get a real gauge on numbers and side effects.
Another issue of grave concern to us all on Friday was the asymptomatic cases. The only subjects counted in the 162 and the 8 numbers above were patients with symptoms. Who knows how many in each cohort were asymptomatic.
This to me leads to the most important question of all, and it was again completely untouched….. How many asymptomatic patients are there? And how many who were vaccinated are still able to spread the virus? Not even an attempt to answer that question. This is critical, and is one of the ways a vaccine can backfire. If a vaccine does not provide sterilizing immunity, ie stop transmission, it is of limited use for disease control. It is great for the individual, but if they can remain without symptoms and still spread it all around it does not help from a public health standpoint.
I have described my concerns and red flags about this study. I would like to add one more thing. Pharmaceuticals that go bad rarely do so in the first few weeks or months. Rather, the adverse effects take months or years. It is a known unknown of not just vaccines but any kind of drug. Our pharma companies have become notorious for having inklings or indeed full knowledge that there is a problem early on, and saying nothing until many are maimed or killed. I will assume that this is the case in this class of drugs until proven otherwise. They are such deceivers I have no choice.
Due to sense of urgency my colleagues and Ifeel about this vaccine rollout, we had an ad hoc meeting of our Journal Club to discuss the NEJM article. Of the nine physicians at the meeting, three have already had very mild cases of COVID. Of the nine, only one is enthusiastic about these vaccines. I have a wait and see stance. I will not be taking it myself. I have too many scars, too many staring at me from the grave to take any other approach.
My patients’ feeeback on the COVID vaccine has been very different than the polls finding that 60% are ready to take it. About half my patients are in the professional/managerial classes and feature a higher level of the 0.1% than the US overall. They tend to be more blue. Most prefer to wait and thankful that health care workers were getting it first. The other half who are working class, more red, and they feel the whole thing is a hoax. They will not be getting the vaccine – likely ever.
The only enthusiasts I would call elderly Rachel Maddow fans. That really makes no sense to me at all since Operation Warp Speed was a Trump project and even Kamala Harris said she would not take a vaccine that Trump recommended.
I would say AT BEST 25% of my patients will be getting this vaccine shortly after being available. There is widespread skepticism that is not being acknowledged by our media. The pharmaceutical industry has worked tirelessly to earn every bit of that disrespect.
Please look at Dr. Angell’s seminal article from 2009. She predicted in her works, all of this and more. My profession has been captured by a cabal of corporatist MBA clones, rapacious and unethical pharmaceutical entities, and an academic elite addicted to credentialism and cronyism. They have over the years bought off and infiltrated all of our government health care regulating agencies and our public health system. And they are completely incestuous. I believe where we are now to be worse than Dr. Angell could have ever dreamed. Even more depressing, I see no way out.
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
1 As a special homage to the polio patient described above, a truly exceptional woman, let me underscore that the disastrous rollout of the this polio vaccine came at a time similar to ours. Panic and malaise were in the air. The children of America and the world were being stricken with polio at an alarming rate. Dr. Alton Ochsner, a leading figure in medicine of the day, vaccinated both of his grandchildren in public in an attempt to bolster confidence in the vaccines. Within 8 days his grandson was dead of bulbar polio. All the celebrities and politicians lining up to take this vaccine on national TV should remember this tragedy. “Stupid human tricks” like this have no place in this kind of situation, and can backfire in unexpected ways. Unlike that era’s polio vaccine, there is no way on earth this vaccine can transmit COVID. However, there are those of us in the medical profession who treat the plan to make population-wide use of messenger RNA, which before these trials had been repeatedly investigated but never reached the human trial stage save in a small scale Zika vaccine study. This is no time for machismo. This is also no time for anything less than complete transparency on the part of everyone involved in the quest for safe and effective vaccines. To behave in any other way is an affront to patients like mine who have suffered and died in the past.
2 If you read the paper, you might well have wondered about that 18,860 number and even checked Table 1 to make sure it’s accurate (it is), since the third paragraph of the Abstract, under the headline “Results,” has very different figures:
A total of 43,548 participants underwent randomization, of whom 43,448 received injections: 21,720 with BNT162b2 and 21,728 with placebo.
So how did the researchers get from 21,720 injected with the vaccine to the 18,860 in the “Main Safety Population”? This sort of thing confirms the impression that this is a very incomplete or sloppy study. It is really not clear where the difference between the 37,706 and the 43,548, or for that matter, the 36,520 total subjects in the Tables 2 and 3 (Efficacy) come from. I used the 37,706 and hence the 18,860 that went with it from Table because it gave slightly smaller numbers than using the Table 2 and 3 figures, but they would be close to each other.
My concern here is the 6000ish discrepancy between the figures in the main text compared to the tables. Were they excluded? If so, why? I could not make heads or tails out of this, and accordingly kept it out of the body of this post. This kind of inconsistency really needs to be hashed out with the actual source data in hand, and should have been explained in the article, even if just in footnotes.
#covid19#covid#the rona#la rona#covid-19#covid vaccine#fuck covid#coronavirus#medecine#health#medical pharmaceuticals#pharmaceutical industry#big pharma#pfizer#vaccine rollout#operation warp speed
3 notes
·
View notes
Text
Release Valve (10/10): TechGnosis
(To read this in its entirety, go here)
Scully awoke suddenly to the sound of pounding at her door. Mulder came awake next to her a second later with a sharp intake of breath.
Mulder reached for his service weapon on the bedside table, paranoia running deep.
“Want me to get it?” He asked.
Scully shook her head, and quickly donned her robe.
When she got to the door, she checked for Mulder behind her- he was clad in only jeans with the button and belt still undone. He had his weapon in his hand, though lowered to his thigh. He nodded at her.
She opened the door.
Isaacs stood there with Stone hanging limply off her shoulder, his face pale and sweating. Isaacs didn’t look much better. She’d obviously struggled getting him to Scully’s door, and looked on the edge of exhaustion. She had a small black backpack hanging off her other elbow.
“Jesus!” Scully said, and swung the door wide, “bring him in!”
They stumbled in, and Mulder was at their side in an instant, grabbing Stone around his other shoulder.
“Into the bed!” Scully ordered.
Scully stripped the duvet off the top and they deposited Stone in the bed. He gave a weak groan.
Scully immediately went to the bedside, and pried his hand away from his side.
“He’s been shot!” She said, turning an accusing eye toward Isaacs, who was bent over, hands on her knees, breathing heavily.
Isaacs nodded at her.
“We need to call an ambulance,” Scully said.
“No!” Isaacs said quickly, “We can’t! Can you treat him?”
Scully cut her eyes to Mulder, who gave her an imperceptible nod.
“After I do, I want to know exactly what the hell you guys have been up to,” Scully said, not amused.
Scully’s bedside manner with Stone was much more gentle, though she began quietly barking orders to Mulder and Isaacs, who hopped-to. Mulder retrieved her doctor’s bag from her closet.
After a thorough triage, it looked like the bullet that hit Stone went through cleanly, and the bleeding had slowed. Scully got some liquids into him and sewed him up, wishing she’d had some anesthetic.
She got him resting comfortably and headed for her living room, closing the door halfway so she could still hear if something went wrong. She found Mulder, now fully dressed, and Isaacs sitting on her couch, deep in discussion.
She interrupted them. She was fuming.
“Agent Stone lost a lot of blood,” she said, “he should be in a hospital.”
“Scully,” Mulder started to say.
“Don’t,” she said, swinging her eyes to Isaacs. “What happened tonight?”
“We were following a lead,” Isaacs said, “at a Department of Defense offsite location.”
“Of course,” Scully said bitterly, looking at Mulder, “I guess you did train them up your way.”
He had the good sense to look contrite.
“Agent Scully, are you aware of some of the cyber security countermeasures Stone has enacted on behalf of the X-Files unit?” Isaacs asked her.
It was Scully’s turn to look abashed. She’d not invested much time following up on how the newer agents were settling in to the unit or what they were up to. She’d relied on Mulder doing that, having been taken up with her own concerns, having been taken up with him.
She shook her head.
“Agent Stone wrote a program,” Isaacs went on, “when he first started with the unit. I can’t claim to understand exactly how it all works, but in essence, it monitored our computers for interference.”
“He found someone interfering?” Scully asked.
“Today,” Isaacs nodded.
“The Department of Defense?” Scully asked. She’d been around the basement office long enough to not sound too skeptical.
“It was an offsite location,” Isaacs said, “I’m not sure how ‘official’ it is.”
Scully nodded, all of this sounding familiar.
“Stone convinced me we should check it out before we brought it you and Agent Mulder.”
“Why?” Asked Scully.
“Because of what we found,” came Stone’s voice from behind her.
Stone stood weakly in the bedroom doorway, his hand on the door handle.
“Let me explain,” he said, as Scully rushed to his side.
“You need to be resting,” she said gently but insistently, and helped him back into bed.
Mulder and Isaacs came to stand in the doorway.
“Come in, please,” Stone said, his voice quiet.
Scully started to protest, but he held up a hand.
“I need to tell you,” he said, “in case something happens.”
Once again Scully tried to object.
“This can’t wait,” he said. He cut his eyes to Isaacs. “Jasmine, will you grab my backpack?”
She brought it to his side.
He looked up at her gratefully.
“The program Isaacs is talking about is kind of a ‘hack-back’ program. A computer at the DOD site tried to hack us today, and I backdoored into their system.”
He took a breath, and Scully nodded, giving him a moment.
“I designed it to be quick, in-and-out so I could remain undetected, but I set it up to search the invading system for keywords related to the X-Files. I picked a few names and references scattered throughout the files, old and new. Threat assessment. Trying to figure out what they were after.”
He reached into the small pack and pulled out a sheet of paper, crumpled from being in the bag. He handed it to Scully.
It read:
<<<Vincent, Marcie Lynn#>>>
<<< Scully, Dana Katherine#>>>
<<<MUFON>>>
<<< Hagopian, Elizabeth Marie#>>>
<<<Spender, Cassandra Ann#>>>
<<<Spender, (?)(***)#>>>
<<<Northern, Penny# >>>
<<<Kevin Scanlon, MD>>>
Scully felt her stomach drop. She sat on the bed and handed the sheet to Mulder.
He stared at it.
“After we got in,” Stone said, adjusting himself on the bed with a grimace and then pointing to the paper in Mulder’s hand, “I got a look at everything. I know what it means.”
XxXxXxXxX
Mulder couldn’t take his eyes off the paper. The implications of all the names on it were legion.
Finally he looked up, connected eyes with Scully and then turned to Stone.
“What does it mean?” He asked.
“Of the pinged keywords that my computer picked up,” he said, “The names with the pound sign have a chip implanted in the back of their neck.”
Scully looked like she was going to be sick.
“The DOD, or whoever is running the off-site we went to,” he went on, “has a computer and a program that controls the chips.”
He pulled a small black cube and a sleek looking computer out of the pack and held them up.
“I’m calling it the God Module,” he said.
Mulder felt suddenly galvanized.
“That’s it?” Mulder said, taking a step toward the bed, “That’s the computer that controls the chips?”
“The one and only,” Stone said in all seriousness. “And that’s not all I found.”
He pulled a smaller device out of his backpack.
It was Isaacs turn to take step closer to him.
“Is that what you pulled off the PC?” She asked him.
He nodded.
“What is it?”
“It’s the Master List,” he said. “It’s the names of everyone with a chip, and what current program each chip is running.”
Mulder connected eyes with Scully, electric.
XxXxXxXxX
The excitement of relaying the information he’d found had only momentarily energized Stone. He lost steam and was now fitfully asleep. Isaacs was passed out on Scully’s couch, an afghan thrown over her.
Mulder and Scully were in Scully’s kitchen, heads bent together, talking quietly. They would not be sleeping that night.
“We can’t keep them here,” Scully said, “they’re going to figure out who broke into the DOD building, and it’s not going to take a lot of algebra to figure out were they went next.”
Mulder nodded, agreeing.
“If that God Module really is what Stone thinks it is,” Mulder said, “we might have some leverage.”
“If that God Module really is what Stone thinks it is…” Scully said, not needing to finish the thought.
Mulder pulled her to him in a tight embrace.
They stood like that for a while, breathing each other in.
“The agents in this unit have a really terrible habit of breaking the law,” Scully said, her voice muffled in his shirt.
Mulder chuffed out a breathy chuckle.
Laws, he thought, were easy to break. For her he would have broken laws of physics, of time. For her he would create matter, destroy it, push an immovable object through an impenetrable force.
“Comes with the territory,” was all he said, his nose in her hair, his heart in his throat.
XxXxXxXxX
It was before dawn, and Mulder had gingerly loaded Stone into the back of his car. Scully got into the back as well, keeping an eye on her patient.
Stone reached for the seatbelt with a grimace and Scully stopped him.
“Skip it,” she said, and Stone looked relieved. He slowly sunk down until he was lying across the seat, his head on Scully’s leg.
“We’re both going to pretend this isn’t awkward, okay?” He said.
Isaacs jumped in front and they drove to Crystal City. Light traffic at a dark hour, Mulder was pretty sure they hadn’t been followed.
Mulder pulled up to the curb in front of a high rise and made a quick call. Ten minutes later, Deputy Director Skinner came out of the front of the building in a tee shirt and jeans and leaned down to the open passenger window.
“Sir?” Mulder said, bending down to look over, “I’m afraid we’re going to need some help.”
Skinner took a look around the inside of the car, stood, and pinching the bridge of his nose, begrudgingly nodded.
XxXxXxXxX
The safe house was off Fort Hunt Road in a suburb near Mount Vernon, a small ranch house tucked into the woods with a long driveway, the prying eyes of neighbors kept at bay.
Stone was set up in a small bedroom, hooked up to an IV drip, pouring over the computer in front of him. Mulder was perched on his bedside, intently looking at the screen. They’d been in deep quiet discussion for the better part of the day when Scully leaned in the doorway.
“Everything okay in here?” She asked. She’d taken to one of the other bedrooms when they arrived and managed to get a couple of hours of sleep. Mulder had been too jacked on adrenaline.
Stone and Mulder looked up simultaneously, with eager expressions on their faces, then Mulder looked to Stone, who nodded.
Mulder rose and came to the door.
“I think we’ve got this figured out,” Mulder said to her quietly, and closed the door halfway, leading Scully through the small living room.
Isaacs was in the corner talking on the phone with her boyfriend in hushed tones. There was an agent on guard duty leaning on the kitchen counter with a cup of coffee. He nodded to them as they made their way through and out onto the small deck in the back.
The day was sunny, and the woods surrounding the property were a sparkling jade. Birdsong filled the air.
“So,” said Scully, leaning against the short railing of the deck, “what says the computer? Do I get to take this thing out?” She vaguely gestured to the back of her neck.
Mulder turned so his backside was resting on the railing next to her, their bodies facing different directions.
“Maybe,” he said.
Mulder looked out at the blazing green woods and was reminded of the Emerald City. Once more into the breach of the great and powerful Oz.
He already had courage, he thought, looking at Scully. He already had heart.
XxXxXxXxX
They were all gathered in the living room when Skinner came in the front door, the front door agent with him. He nodded at Mulder.
“Murphy, Taylor, can you wait for us outside for a bit?” Skinner said.
The agents on guard duty mumbled affirmatives and trooped out the door.
Once they were out, Skinner looked to Mulder.
“I’ve got the place,” Skinner said.
Mulder nodded.
“What place?” Scully asked him, confused.
“A location for a meeting with the Smoking Man,” Mulder said.
Scully felt her stomach turn.
“Mulder,” she said.
“No,” he replied before she could go on. “This time it’s on our fucking terms.” He turned to Stone. “Let’s show them,” he said.
Stone flipped his laptop around on the coffee table and they all huddled in to see the small screen.
“The Master List,” Stone said, pushing a few buttons. “It seems to be categorized by, let’s just call them ‘patients,’” he said, giving a deferential look to Scully. “This is the group of patients Agent Scully is a part of,” he brought up a subset of names.
Scully leaned further in. Amongst the names in her group were Cassandra Spender, Betsy Hagopian, Penny Northern.
“Penny…” Scully said, feeling a pang of emotion.
“Agent Scully and the other patients on this list have their chip set to program ‘A.’”
“Abductee?” Isaacs asked quietly.
“Maybe,” said Stone, “we know from our files that many of the people on this list were abducted for a period of time. All returned. Many are now deceased.”
“The ones who removed the chip,” Scully said with certainty.
“It appears that way,” Stone said.
He went on.
“There’s another group of patients set to program ‘C’,” he said, pointing to the screen.
“There are some names here, and some code names. Those I haven’t been able to decipher.”
Marcie Vincent. Names of other people. Other kids, thought Scully.
“We don’t yet know the function of program ‘C’,” Stone went on. The information I downloaded only refers to these patients within the context of a ‘Project Ramet.’”
“Are they…” Scully took a second, “are the Program C kids’ chips controlled by the God Module?”
“Yes,” said Stone. “I’m almost certain.”
“This group,” he said then, looking to Skinner, “have chips set to program ‘H’.”
Mulder looked at the list, running his finger down the screen through the names. He stopped on one.
“CGB Spender,” Mulder said, looking at Skinner, then at Scully.
“From what I can glean,” said Stone, nodding, “the chips for the members of this group are set to a program functioning in accordance with the immune system.”
“With what objective?” Isaacs asked.
“To fight bacteria,” Stone said, “to fight viruses.”
“So much for vaccines,” Mulder said.
“That’s not possible,” Scully said, “the science… This kind of technology is decades away, if it’s even possible.”
Stone looked meaningfully at Mulder.
Mulder cut his eyes to Scully and she began to wonder if there was something they weren’t telling her.
“Here’s the thing,” Mulder said, “with Stone’s God Module, we can take all program ‘A’ patients and deprogram the chip. Or change it to run program ‘H.’”
“And vice versa,” Isaacs said, starting to understand what Mulder was saying. “You can turn the tables on this Smoking Man, or CGB Spender, or whatever his name is, and then we’re in charge of his chip.”
“If he removes it, he gets cancer,” Scully added quietly.
Mulder nodded.
“And I suspect some of the other names on this list are other men we know. Men we know to be working with the Smoking Man.”
“The Syndicate,” Skinner said.
“Wouldn’t it be nice to have a little leverage?” Mulder asked, leaning back.
“There’s leverage,” said Stone, “and then there’s leverage.”
XxXxXxXxX
“So,” Stone began. He had the God Module up and ‘running,’ had played with it for a while, getting a feel for the technology. “What’s the location for the meeting with CGB Spender?”
Skinner told him.
“I think I need to convert that to coordinates,” he said. “Latitude and longitude.”
While Isaacs, Stone and Skinner were trying to figure that out, Scully put a hand on Mulder’s arm.
“You’re going to program his chip to send him to this location?” She asked him, her voice low.
Mulder squeezed her hand.
“Let’s see how he likes it this time,” he said.
“I’m coming with you,” she said.
“Scully—“ He started.
“No,” she said, “I want to see the look on his face.”
Mulder gave her a small smile.
“Atta girl,” he said, quietly.
XxXxXxXxX
The location Skinner had picked had been an old quarry in Maryland. There were two FBI snipers on either side of the cliffs, and several teams handpicked by Skinner located at the entrance. There was no other exit.
Mulder and Scully waited in a car in the middle of the open quarry, Isaacs and Skinner in another about 50 yards away. Stone was still at the safe house with the God Module, in constant contact with Isaacs. If the Cancer Man showed up as he was ‘programmed’ to do, they would know the device was working and Stone would immediately reprogram all of the patients. Scully wondered if she would feel anything.
At the hour appointed by the God Module, a large dark sedan pulled into the quarry, tires crunching as it slowly pulled up to the car Mulder and Scully were waiting in. When the car’s ignition was cut, Mulder and Scully got out.
CGB Spender got out of the car slowly and came to stand in front of them. He said nothing, his eyes were unblinking. Mulder and Scully exchanged a look.
With a sniff of awareness, he came to himself, blinked and looked around. Scully took in the flash of surprise on his face with some satisfaction.
“Wondering how you got here?” Scully asked. “I can relate.”
The man took a moment before responding.
“You have it, then?” He asked.
“We have it,” said Mulder.
“Then you’d better keep it safe,” he said.
“You’re not calling the shots anymore,” Mulder said. Scully could see the muscles flex in his jaw.
“I never was,” the man said.
Scully saw a flash of something in the man’s face, but couldn’t put a name to it.
“We want Marcie Vincent returned to her family,” Mulder said.
The man nodded. He didn’t even attempt to put up a fight.
“And I want to know about Project Ramet,” Mulder said.
For the first time the smug smile returned to the man’s face.
“I’ll just bet you do,” he said, reaching into his pocket to pull out a pack of Morleys.
Mulder pulled a small knife out of his pocket and took a step forward.
“Your chip is running program A now,” Mulder said, “and there’s nothing I’d like more than to cut that thing out of your neck right here, right now.”
“Killing me won’t stop Project Ramet, Agent Mulder,” the man said, “and there are some things even I don’t know.”
He pulled a lighter out of his pocket and lit his cigarette.
“You’ve ensured Agent Scully’s enduring health, you hold the technology to exercise great power, and you have me and other members of my cabal over a barrel, as it were.” The man went on, “You’re closer now than you ever were to finding what you seek.”
XxXxXxXxX
“We should have arrested him,” Scully said.
She and Mulder were in their car, on their way back to the safe house. They needed to figure out where to keep the God Module, how to keep it safe. There would be a never ending line of parlous adversaries out to get it.
“We need him to release Marcie Vincent,” Mulder said, pulling into a scenic overlook off the Parkway. “And we’ll probably need him in the future. You could say he works for us, now.”
Scully nodded. He was right.
“What are we doing?” Scully asked.
Mulder didn’t answer, just walked over to the passenger seat and opened it up for her, gave her a hand out.
It was another beautiful day, the sky a piercing blue. The overlook was perched over the Potomac, and there were few people pulled in. A young couple was sitting on top of the small neat stone wall, sharing a sandwich. Their dog, a yellow lab, was sitting at their feet hoping for a dropped morsel.
Mulder grabbed Scully’s hand and walked with her toward a wooded picnic area. The dog rose as they passed, his tail wagging gently. He gave one short woof once they were past.
“Everyone’s a critic,” said Mulder.
They sat down at a picnic table, turned toward the river.
“So it’s done,” Scully said, knowing that the minute the Smoking Man showed up to the quarry Stone had reset her chip.
“It’s done,” Mulder said.
XxXxXxXxX
He hadn’t realized that the ever-looming threat of her illness coming back had weighed so heavily on him. A world without Scully was not a world he wanted to live in. It was like a release valve had been flipped open, the pressure on his heart hissing out into the ether.
He took one deep breath and let it flow out of him, feeling lighter, feeling free.
They sat for a moment in comfortable silence.
“How soon do you think I can takethis thing the hell out of my neck?” She asked, leaning companionably into his shoulder.
He took a breath.
“There’s one thing Stone and I discovered while we were in the safe house that he didn’t share,” Mulder said. “Something you need to know.”
Mulder saw Scully tense, and he reached out and took her hand.
“If you leave the chip in,” Mulder said, his voice steady, his gaze locked on hers, “the God Module can restore your fertility.”
Scully’s eyes slid closed, and with a slight upturn of her lips, she canted her face to the sun.
“I get it now,” she finally said.
“Get what?” Mulder asked gently.
“You,” she said, simply.
He cocked his head to the side, a question.
“Mulder, I want to believe,” she said.
He knew then what love was.
It was the gunmetal slide of a pistol, a snow cat prowling at 40 below. The whorls of her fingerprints pressed into his skin. It was purpose and frustration, illumination and regret. It was her smile in profile, composed against the sky.
58 notes
·
View notes
Text
A Different Sort of Case
Fandom: House, MD
Characters: Hattie (OFC), Greg House, James Wilson, Ducklings
Pairing: House x OC (platonic)
Summary: Hattie ends up at PPTH and comes across someone that she thought that she would never see again.
Word Count:2,120
Rating: SFW
Warnings: Hospitalization, cancer mentions, illness
Author’s note: This was spawned during a re-watch of House and thanks a certain someone spamming me with Hugh Laurie. I forgot how much I enjoyed this show. I don’t know how long this fic will end up being, It has sort of taken on a life of it’s own since I had planned on it being relatively short. Hope everyone enjoys. Unbeta-ed so all mistakes are my own.
________________________________________________________
The lights above and all around me faded in and out of focus. My body wasn’t responding with anything that I asked it to do. I tried, with some amount of desperation, to move my fingers, move my legs, anything but nothing was coming of it. People were talking around me but the words were completely muffled. Nothing was making sense and a swell of panic hit me. I didn’t know what was going on but before it could get any worse, the blackness enveloped my vision and I passed out.
There was pain everywhere. I still couldn’t move my arms and legs. Something was very wrong. The sounds around me were still muffled. No one was talking but there was an annoying beep. I felt exhausted, that was what registered the most. I huffed and gave over to the exhaustion, losing all sense of what was happening around me; of what I could and couldn’t do.
*************
James had all intentions of stopping in the office and talking with House. Everyone had noticed the man cooped up more than usual in his office. His reaction to his particular case was unusual, even by House standards. There was a different level of grumpiness to the man and he was all but sleeping in his office. Which was how he found the man in question when he stopped in front of the door. He thought he was asleep; feet propped up and his head tipped back. Wilson spotted his lips moving despite his position. it was as simple as he was thinking about his current case.
Wilson stepped into the office, his first instinct proven right. House was, in fact, asleep. He crossed his arms over his chest as he observed his friend. Wilson wondered if it was worth waking him up or letting him get the rest that he likely needed.
His answer became clear to him when he heard the woman’s name mumbled. That had to be a first. House dreaming of a woman? The name repeated itself and he was quick to realize that it was the name of his current patient. That was something that he had to figure out.
Wilson slammed down one of the books that was on the desk and House jolted awake. Wilson wanted to tease the man. It wasn’t often that he got the opportunity but he wanted to know more about what was happening. That overrode his desire to tease the man.
“I hear that you have a new case.”
“We already ruled out your specialty sorry. I didn’t know you were going around poaching cases now. Is it getting that slow in oncology?” House cocked his head to the side and pulled his feet off of his desk.
“Yes, because I desperately want my department to be busy. I wish it was overflowing with people who I get to tell they are dying.”
“You said it, not me.” Under normal circumstances, Wilson would have been a bit exasperated by the comment. This was not one of those times and he let it roll right off of his back.
“You were dreaming about the patient.” Wilson pointed out, able to keep a smile off of his face by the skin of his teeth. House was obsessive yes but not that sort of obsessive. He didn’t dream about his patients.
“I was dreaming about closing the case. There’s a difference. Or do I need to disclose all my dreams to you now Mum?”
“You said her name.” Wilson pointed out. “You never know a patient’s name. And you’ve been in her room. Without her being awake.” If it wasn’t relevant in a medical sense, House didn’t bother learning it. He was sure that the man wouldn’t know if his patient was male or female if it didn’t affect the possibility of a diagnosis. He rarely, if ever saw patients either. That was a big deal.
“I needed to do an exam myself.” It was a bullshit excuse and at that moment, they both knew it. James knew better than to push his friend though. If he wanted to get this figured out, he couldn’t have the man completely closing off. It was a tendency he had when things got a little too personal. House didn’t ever, ever bother respecting personal boundaries. This was going to be the one time that James paid his friend back with a taste of his own medicine. He was going to figure this out one way or another.
*************
There were people around me. The words this time came much more clear than they had the previous times I had woken up. Several voices all spoke though I couldn’t make out what they were saying exactly. I opened my eyes and it took several long seconds for the people to come into focus. One was at my arm, drawing some blood. Another was standing looking at a vitals screen. The third had a chart in hand. They were talking to one another, not realizing I was awake yet. That was until the person at the monitor turned and saw me.
“We weren’t sure you were ever going to wake up.” A light shone in my eye without warning. “How are you feeling?”
“Give her a second to breathe.” The female was the one that spoke. I looked towards her and then the other man at my side. Not that I could move my head all that much. I realized that I was stuck in a collar. It wasn’t comfortable in the least. He didn’t say anything right away but smiled at me.
“Feel like shit,” I mumbled, trying to catch up to what was happening. I didn’t know how I ended up in the hospital. The last thing that I remembered was being on the highway, heading towards New York. “What happened?” I didn’t care who answered me, all I wanted some answers.
“The rest of you, out.” That was a familiar voice. It wasn’t like I could forget the one that I had spent the better part of my first twenty-four years on this Earth with. Of all the hospitals I could be at, it had to be Princeton-Plainsboro. We may not have talked in almost twenty-one years but I had kept up with his doings. He was a top diagnostician, something that hadn’t come as a surprise. He had needed to finish med school in the formal sense the last time we saw or spoke to one another.
“But…” All three wanted to argue with him on that front, though none of them seemed all too willing to take on the man.
“Out.” I risked looking towards one Gregory House. The cane and the limp were new. The drawn, weary, pained face was out of place on his face. Both made up a different man standing in front of me than the one I had known. He had aged well. That much I could say. I had thought about the possibility of meeting him again. Though I never imagined that it would be under these sorts of circumstances. Everything that I had come up with faded on the tip of my tongue. All those things that I had wanted to say after he had upped and left vanished. He had demanded that I leave his life but he had made the decision for me.
He moved over to the edge of the bed, not saying a damn thing to help move this along. It felt uncomfortable though what more could be expected? He was the one who had upped and left. He didn’t want me around when I had been ready to follow him wherever. Like I always had. It was a pathetic thought and one that I hadn’t grown out of despite the therapy.
“Your kidneys are failing.” Right down to business.
“That still doesn’t explain how I ended up here in the first place.”
“You’re also anemic.” I wasn’t going to get the answers that I wanted out of him so I was going to have to wait and play his game. He wasn’t going to acknowledge that he knew me, he wasn’t even looking at me. I didn’t understand why he had asked the other doctors to leave the room. He was going to pretend that I was another patient. There was nothing for him to hide and if he didn't want to say anything then I wouldn't. I couldn’t push him for it since it would only make him shut down ten times faster. House worked at his own pace and everyone else around him needed to be able to adapt to it. If they didn't, they ended up left behind in the dust.
I waited, quiet, for him to continue with whatever else he wanted to tell me. There was more there.
“And with a fever, none of that makes sense with a car wreck.” He finally looked up at me, leaning with a heavy stance on the cane, tipped to a hint to his right. There was my answer and it made sense given the last thing that I remembered. “So, the question is why.” He was asking me like I knew the answer to that. He was the one that had taken an interest in medicine. I was the one who loved history. He moved to the side of the bed, allowing me to track him with my eyes. It was a weird sensation, not being able to move the neck.
It was that moment that I tried to move my arms and legs but found that I still couldn’t.
“That should wear off in another few days.” He said as he poked at my arm. I could feel that at least. “At least in your upper half. There’s no real telling what will happen with your legs.” He was never one to pull punches. Others would have panicked about it and lashed out at him. I panicked but was grateful to know the sort of road of recovery that I was looking at. I could digest the information later and mourn for whatever I had to when I was on my own. I wasn’t about to cry in front of the man.
“I take it you’re asking why because nothing has come back conclusive?” He was silent as his eyes moved over me again. I could see that I was right though, there was no denying the twitch of his lips. “But everyone lies so it’s not like you can trust anything I have to say.” Maybe it was a subtle dig at the man, one that he wasn’t going to overlook. I knew that it had to be the last one that I threw at him.
“What are the differential diagnoses?”
“Cut them in half. Stopped the antibiotics and you aren’t getting any better. There wasn’t a hint of cancer anywhere on your scans. We were waiting to see if you took any medications but even if you did, you have been here well over a week. Anything that you take would be out of your system by now.” He wasn’t answering me about what he thought it was. Having cancer ruled out was at least reassuring. Not like I wanted to go through with that again.
“Done the cancer thing once. Nice to hear that I don’t have to do it again.”
“What?”
“Leukemia. About ten years ago.” I offered without needing him to prompt further. “Had about six months worth of radiation. A year's worth of other treatments after before they found a matching donor. Been fine since the bone marrow transplant.” He frowned and the wheels in his head were turning like that. It was as simple as a snap of the fingers.
“Should be on the bracelet that I wear.”
“You didn’t come in wearing any jewelry.”
“There’s a card in my wallet too.”
“Destroyed in the wreck, so they said.” That was sort of crucial information for any doctor to know. It was why I tried to make sure that it was available in as many different forms as possible. The bracelet must have broken off in the crash. I couldn’t do much anything about a wallet ending up destroyed in a wreck. There was no point in hiding or lying about any of that. It would be necessary if he was going to figure out what the hell was going on with me.
“Bone marrow transplant…” He muttered before leaving the room without another word. Judging by the look on his face before he left, it was enough information to trigger whatever was happening in his brain. That was good enough for me. I wasn’t sure if I would see him again.
5 notes
·
View notes
Photo

This Story Will Make You Mad.
When you have chronic lyme disease, it can be very hard to know who or what to trust. This story is a perfect example.
When I was diagnosed with chronic lyme disease in 2013, I was also diagnosed with hypothyroidism, as I had low T3, which is a hormone produced by the thyroid gland. I had an unusual situation, as I had low T3, but normal TSH (Thyroid Stimulating Hormone). Normally, if you have low T3, you also have high TSH. But I didn’t.
Apparently, this was cause for concern, as one situation that produces low T3 and normal TSH is a brain tumor. So, my lyme doctor ordered an MRI of my brain. You can bet I was super relaxed about that. Thankfully, I did not have a brain tumor. Thus, my doctor said the lyme infection in my brain (it breaks through the blood brain barrier in the first 48 hours) was interrupting the communication between my hypothalamus and my pituitary gland. The two need to be on good speaking terms in order for the thyroid to function properly.
My lyme doctor recommended thyroid hormones. This turned into a major discussion, because a functional medicine doctor I was seeing at the time implored me not to take the thyroid hormone. He basically said it would goof everything up and that there were more natural ways of dealing with my thyroid issues.
At the time I was dealing with severe fatigue. As in, we were on a previously planned trip to Disney and I had to use a mobility scooter because there was no way I could have walked the park. That kind of fatigue. Can you imagine?
I didn’t know who to believe about the thyroid medication, but I knew something needed to change in the way I felt, so against my better judgement, I decided to take the thyroid hormone.
I have seen two different lyme doctors since the one who originally prescribed the thyroid hormone, and they both recommended I stay on it. Over the years, my T3 levels were closely monitored, with blood draws very six to eight weeks, followed by medication adjustments, if necessary.
Fast forward to fall of 2017. Suddenly, I’m having all sorts of issues with regulating my body temperature. I have a history of always being cold, but suddenly I was always hot. Like, really hot. I spent the harsh Minnesota winter in a sweat. Sometimes I’d walk around the house half naked. I’d be in a public space, and I’d note I was wearing a t-shirt while everybody else was bundled up in sweaters and jackets.
I know what you are thinking. Menopause. While I am of a certain age, I’m still menstruating, so that wasn’t the issue.
When you are being treated for chronic lyme disease, you tend to move away from traditional western medicine practitioners, because they look at you like you are crazy when you say you have lyme disease. It gets old.
But the body temperature thing was really bugging me, and I had a hunch it had something to do with my thyroid. So, I made an appointment with an endocrinologist.
After starting the meeting with the standard “I know you don’t recognize this, but I have chronic lyme disease” conversation, I told the doctor about my past thyroid issues, along with my current symptoms and medications.
He asked to see my blood work from before I started the thyroid hormones, which I had on hand. Sadly, I’m a pro at this, and anticipated his request. He then asked the million dollar question. He said “How much did you weigh when this blood work was done?” I told him I didn’t know for sure, as it was many years ago, but I guessed it was south of a hundred pounds.
To which he said “I don’t think you were hypothyroid. I think you were starving. When your weight gets too low, things don’t work right.”
When he said that, tears literally popped out of my eyes and rolled down my face. I didn’t even care. I was completely unselfconscious about it. Why was I crying? First, I never wanted to take those damn thyroid hormones in the first place, and it turned out I never needed to. So, that pissed me off. Second, it just reinforced how difficult it is to navigate the lyme jungle. I had not one, but three lyme doctors tell me I had lyme related hypothyroidism, and that it was critical for me to take the medication. In that moment, I was just so exhausted on navigating conflicting medical opinions.
The lyme doctors didn’t make any money off the medication, so I can only believe they had the best of intentions, but still. It’s just infuriating. There are many risks associated with taking thyroid hormones, and it turns out I unnecessarily exposed myself to those risks for four years. Not to mention, taking thyroid hormones is a huge pain in the butt. You have to take them first thing in the morning, one hour before any food, drink or other medication. Psychologically, it never made me feel good to roll out of bed and pop a pill first thing. It just sends the wrong message. I’m sick. I need medication to function. I hated starting my day that way, and I’m getting mad all over again as I write this.
But back to my appointment with the endocrinologist. Once he handed me a tissue and I stopped crying, he suggested I discontinue the thyroid hormones, and then come in for a blood draw in three weeks, once the medication fully cleared my system.
You can already see where this is going. My thyroid labs were completely normal. I was taking medication for no reason. In fairness, I have gained 26 pounds in the last two years, so that likely has something to do with my T3 levels coming back into the normal range.
Two things have happened since I discontinued the thyroid hormone:
Over the course of a few months, my body temperature issues resolved, and I am no longer overheating.
I started to gain weight at an increased clip.
When I noticed my increased weight gain seemed to coincide with discontinuing the hormone medication, I emailed the endocrinologist to ask if there was a correlation. He said there absolutely was. So, all these years, when I have been struggling to gain weight, the thyroid hormones were playing a role in holding me back. My GI system is still totally whacked, so I can’t put all the blame on the thyroid medication, but let’s just say it wasn’t helping anything.
I’m still pretty mad about all this. Yes, it’s true, I did have low T3 at one point. But I’ve learned it’s also true that not all thyroid deficiencies need to be treated, particularly if there is an extenuating circumstance, such as dramatic weight loss.
Here is the moral of the story. You know that expression “to a man with a hammer, everything looks like a nail.” I think that’s also true of many lyme doctors -- everything looks like lyme to them. And that’s my advice today -- if you have chronic lyme, or chronic anything, be on the lookout. It’s too easy for doctors to just blame everything on your chronic condition.
For whatever reason, I always had a nagging feeling my thyroid issue was not lyme related, but I never acted on my hunch because I had three people who had gone to medical school telling me I needed to be on medication, and I figured they were in a better position to know that than I was. Well, that turned out to be misplaced trust.
I am sad to say that after nearly five years navigating the mess of chronic lyme disease, I truly don’t know who to believe or who to trust. I think the fact of the matter is nobody has chronic lyme completely figured out. Not western medicine doctors, not functional medicine doctors, not lyme literate MDs. Nobody. Everybody has their own theories, and I believe they believe them. And I think most practitioners who treat lyme patients have nothing but good intentions. But I can’t help feeling like a human guinea pig.
We are still on the frontier of this epidemic, and until it gets more attention from the CDC and Western Medicine, there’s not going to be a standard treatment protocol, which means people are going to continue to struggle to get proper care, and will occasionally get sent down errant rat holes, as I did.
I realize this is more negative than I tend to be, but lyme disease is a bitch, and people who suffer from it have to work way too hard to get well, as they are simultaneously fighting the disease and the system.
I know things could be much worse, and I need to hang on to that perspective. I have learned so much from being sick, and I would never give those lessons back. But lyme disease has taken much from me, and I have sadness and anger about that. Buy I will never stop trying to regain what I’ve lost. Never. Ever.
10 notes
·
View notes
Text
Letter from Dr.Frank Shallenberger - the Covid 19 Vaccine
Dear Patients and Friends,Last week I must have been asked 20 times about the new COVID vaccines. Here are my thoughts. Please pass this information onto many as you can. People need to have fully informed consent when it comes to injecting foreign genetic material into their bodies.
1. The COVID vaccines are mRNA vaccines. mRNA vaccines are a completely new type of vaccine. No mRNA vaccine has ever been licensed for human use before. In essence, we have absolutely no idea what to expect from this vaccine. We have no idea if it will be effective or safe.
2. Traditional vaccine simply introduce pieces of a virus to stimulate an immune reaction. The new mRNA vaccine is completely different. It actually injects (transfects) molecules of synthetic genetic material from non-humans sources into our cells. Once in the cells, the genetic material interacts with our transfer RNA (tRNA) to make a foreign protein that supposedly teaches the body to destroy the virus being coded for. Note that these newly created proteins are not regulated by our own DNA, and are thus completely foreign to our cells. What they are fully capable of doing is unknown.
3. The mRNA molecule is vulnerable to destruction. So, in order to protect the fragile mRNA strands while they are being inserted into our DNA they are coated with PEGylated lipid nanoparticles. This coating hides the mRNA from our immune system which ordinarily would kill any foreign material injected into the body. PEGylated lipid nanoparticles have been used in several different drugs for years. Because of their effect on immune system balance, several studies have shown them to induce allergies and autoimmune diseases. Additionally, PEGylated lipid nanoparticles have been shown to trigger their own immune reactions, and to cause damage to the liver.
4. These new vaccines are additionally contaminated with aluminum, mercury, and possibly formaldehyde. The manufacturers have not yet disclosed what other toxins they contain.
5. Since viruses mutate frequently, the chance of any vaccine working for more than a year is unlikely. That is why the flu vaccine changes every year. Last year’s vaccine is no more valuable than last year’s newspaper.
6. Absolutely no long term safety studies will have been done to ensure that any of these vaccines don’t cause the cancer, seizures, heart disease, allergies, and autoimmune diseases seen with other vaccines. If you ever wanted to be guinea pig for Big Pharma, now is your golden opportunity.
7. Many experts question whether the mRNA technology is ready for prime time. In November 2020, Dr. Peter Jay Hotez said of the new mRNA vaccines, "I worry about innovation at the expense of practicality because they [the mRNA vaccines] are weighted toward technology platforms that have never made it to licensure before." Dr. Hotez is Professor of Pediatrics and Molecular Virology & Microbiology at Baylor College of Medicine, where he is also Director of the Texas Children’s Hospital Center for Vaccine Development.
8. Michal Linial, PhD is a Professor of Biochemistry. Because of her research and forecasts on COVID-19, Dr. Linial has been widely quoted in the media. She recently stated, "I won't be taking it [the mRNA vaccine] immediately – probably not for at least the coming year. We have to wait and see whether it really works. We will have a safety profile for only a certain number of months, so if there is a long-term effect after two years, we cannot know."
9. In November 2020, The Washington Post reported on hesitancy among healthcare professionals in the United States to the mRNA vaccines, citing surveys which reported that: "some did not want to be in the first round, so they could wait and see if there are potential side effects", and that "doctors and nurses want more data before championing vaccines to end the pandemic".
10. Since the death rate from COVID resumed to the normal flu death rate way back in early September, the pandemic has been over since then. Therefore, at this point in time no vaccine is needed. The current scare tactics regarding "escalating cases" is based on a PCR test that because it exceeds 34 amplifications has a 100% false positive rate unless it is performed between the 3rd and 5th day after the first day of symptoms. It is therefor 100% inaccurate in people with no symptoms. This is well established in the scientific literature.
11. The other reason you don’t need a vaccine for COVID-19 is that substantial herd immunity has already taken place in the United States. This is the primary reason for the end of the pandemic.
12. Unfortunately, you cannot completely trust what you hear from the media. They have consistently got it wrong for the past year. Since they are all supported by Big Pharma and the other entities selling the COVID vaccines, they are not going to be fully forthcoming when it comes to mRNA vaccines. Every statement I have made here is fully backed by published scientific references.
13. I would be very interested to see verification that Bill and Melinda Gates with their entire family including grandchildren, Joe Biden and President Trump and their entire families, and Anthony Fauci and his entire family all get the vaccine.
14. Anyone who after reading all this still wants to get injected with the mRNA vaccine, should at the very least have their blood checked for COVID-19 antibodies. There is no need for a vaccine in persons already naturally immunized.
Here's my bottom line: I would much rather get a COVID infection than get a COVID vaccine. That would be safer and more effective. I have had a number of COVID positive flu cases this year. Some were old and had health concerns. Every single one has done really well with natural therapies including ozone therapy and IV vitamin C.. Just because modern medicine has no effective treatment for viral infections, doesn’t mean that there isn’t one.
Yours Always,
Frank Shallenberger, MD, HMD
0 notes
Text
#plandemic #scamdemic #covid19 #coronavirus #nature #science #truth "in a world of lies, telling the truth is an act of rebellion"
Read this before You get the vaccine!
From a Dr. regarding the upcoming vaccines:
Last week I must have been asked 20 times about the new COVID vaccines. Here are my thoughts. Please pass this information onto many as you can. People need to have fully informed consent when it comes to injecting foreign genetic material into their bodies.
1. The COVID vaccines are mRNA vaccines. mRNA vaccines are a completely new type of vaccine. No mRNA vaccine has ever been licensed for human use before. In essence, we have absolutely no idea what to expect from this vaccine. We have no idea if it will be effective or safe.
2. Traditional vaccine simply introduce pieces of a virus to stimulate an immune reaction. The new mRNA vaccine is completely different. It actually injects (transfects) molecules of synthetic genetic material from non-humans sources into our cells. Once in the cells, the genetic material interacts with our transfer RNA (tRNA) to make a foreign protein that supposedly teaches the body to destroy the virus being coded for. Note that these newly created proteins are not regulated by our own DNA, and are thus completely foreign to our cells. What they are fully capable of doing is unknown.
3. The mRNA molecule is vulnerable to destruction. So, in order to protect the fragile mRNA strands while they are being inserted into our DNA they are coated with PEGylated lipid nanoparticles. This coating hides the mRNA from our immune system which ordinarily would kill any foreign material injected into the body. PEGylated lipid nanoparticles have been used in several different drugs for years. Because of their effect on immune system balance, several studies have shown them to induce allergies and autoimmune diseases. Additionally, PEGylated lipid nanoparticles have been shown to trigger their own immune reactions, and to cause damage to the liver.
4. These new vaccines are additionally contaminated with aluminum, mercury, and possibly formaldehyde. The manufacturers have not yet disclosed what other toxins they contain.
5. Since viruses mutate frequently, the chance of any vaccine working for more than a year is unlikely. That is why the flu vaccine changes every year. Last year’s vaccine is no more valuable than last year’s newspaper.
6. Absolutely no long term safety studies will have been done to ensure that any of these vaccines don’t cause the cancer, seizures, heart disease, allergies, and autoimmune diseases seen with other vaccines. If you ever wanted to be guinea pig for Big Pharma, now is your golden opportunity.
7. Many experts question whether the mRNA technology is ready for prime time. In November 2020, Dr. Peter Jay Hotez said of the new mRNA vaccines, "I worry about innovation at the expense of practicality because they [the mRNA vaccines] are weighted toward technology platforms that have never made it to licensure before.” Dr. Hotez is Professor of Pediatrics and Molecular Virology & Microbiology at Baylor College of Medicine, where he is also Director of the Texas Children’s Hospital Center for Vaccine Development.
8. Michal Linial, PhD is a Professor of Biochemistry. Because of her research and forecasts on COVID-19, Dr. Linial has been widely quoted in the media. She recently stated, "I won't be taking it [the mRNA vaccine] immediately – probably not for at least the coming year. We have to wait and see whether it really works. We will have a safety profile for only a certain number of months, so if there is a long-term effect after two years, we cannot know."
9. In November 2020, The Washington Post reported on hesitancy among healthcare professionals in the United States to the mRNA vaccines, citing surveys which reported that: "some did not want to be in the first round, so they could wait and see if there are potential side effects", and that "doctors and nurses want more data before championing vaccines to end the pandemic".
10. Since the death rate from COVID resumed to the normal flu death rate way back in early September, the pandemic has been over since then. Therefore, at this point in time no vaccine is needed. The current scare tactics regarding “escalating cases” is based on a PCR test that because it exceeds 34 amplifications has a 100% false positive rate unless it is performed between the 3rd and 5th day after the first day of symptoms. It is therefor 100% inaccurate in people with no symptoms. This is well established in the scientific literature. See the attachment (False Positive PCR testing is up to 100%!) for more information on this. If you go to the CDC site (file:///C:/Users/docto/AppData/Local/Temp/cdc_97230_DS1.pdf ), you can see that the weekly death rates in the US are now lower than they normally are during an average flu season.
11. The other reason you don’t need a vaccine for COVID-19 is that substantial herd immunity has already taken place in the United States. This is the primary reason for the end of the pandemic.
12. Unfortunately, you cannot completely trust what you hear from the media. They have consistently got it wrong for the past year. Since they are all supported by Big Pharma and the other entities selling the COVID vaccines, they are not going to be fully forthcoming when it comes to mRNA vaccines. Every statement I have made here is fully backed by published scientific references.
13. I would be very interested to see verification that Bill and Melinda Gates with their entire family including grandchildren, Joe Biden and President Trump and their entire families, and Anthony Fauci and his entire family all get the vaccine.
14. Anyone who after reading all this still wants to get injected with the mRNA vaccine, should at the very least have their blood checked for COVID-19 antibodies. There is no need for a vaccine in persons already naturally immunized.
Here's my bottom line: I would much rather get a COVID infection than get a COVID vaccine. That would be safer and more effective. I have had a number of COVID positive flu cases this year. Some were old and had health concerns. Every single one has done really well with natural therapies including ozone therapy and IV vitamin C. Just because modern medicine has no effective treatment for viral infections, doesn’t mean that there isn’t one.
Yours Always,
Frank Shallenberger, MD, HMD
VERY INTERESTING
COPY AND PASTED.
0 notes
Photo

When It Comes To The Hows of Having Sex, Context Is Important
By Theodore (Ted) Kerr
In 1989, on the second annual World AIDS Day, a group of activists called for “maximum disruption” of the holiday season through “non-violent disruption, sabotage, protest, and civil disobedience.” Their suggested targets included shopping malls, theaters, subways, bridges, TV stations and computer networks. Ideas included: not shopping, donating to AIDS research; dumping red die in public fountains; buying junk cars and stalling them on bridges; stink bombing theaters; and for people to “screw up computer systems.” They called themselves GRINCH: Gay Retaliation for Inexcusable Negligence and Criminal Homophobia. They printed posters with their ideas and images from the holiday classic, “The Grinch Who Stole Christmas.”
This brand of pointed and poignant activism and cultural production with its use of provocation, rage, humor, and camp is part of an AIDS activism with a history. Looking back, we see it being deployed in issues of “Disease Pariah News”, the writings of underground star Cookie Mueller and ACT UP member David Feinberg. And we see it now in the work of writer and performer Brontez Purnell, and in projects like AIDS Action Now’s PosterVIRUS campaign. This activism is attuned to the micro and the macro, aiming to instigate immediate action to improve the lives of people living with HIV while also satirizing the culture which is promulgating injustice. This type of activist sensibility can get lost over time, flattened via the internet and the archive.
Often able to grasp this sensibility are those for whom the AIDS crisis is ongoing. An example is the anonymous group of Canadian AIDS activists who earlier this year released, "How To Have Sex in a Police State: One Approach.” It is a pamphlet that raises awareness around ways people living with HIV and those at risk are criminalized. Criminalization occurs through specific laws, high court decisions, and the ongoing criminalization of sex workers, users of drugs, and immigrants; all often further exasperated by issues of race, class, gender and sexual orientation. The collective chose to remain anonymous because as they explain, “Some of the tactics suggested in this document are within a grey area of the law.” They did not want to make themselves the target of state suppression more than they are already. Many of the collective’s members are living with HIV.
An important influence on "How To Have Sex in a Police State: One Approach" was “How To Have Sex In An Epidemic: One Approach,” the landmark pamphlet penned by Richard Berkowitz and Michael Callen, with the scientific endorsement of their doctor, Joseph Sonnabend, MD. Their text is one of the earliest calls for gay men to use condoms (along with the Sister’s of Perpetual Indulgence “Play Fair” campaign), and urges people to factor love into the equation. They wrote, “maybe affection is our best protection.” Their argument could be taken as slut shaming, but it’s not. As self-proclaimed sluts themselves, Berkowitz and Callen were arguing for interconnectivity to be recognized within sexual networks, and that love—no matter how one defined it—can be present in every sexual encounter, be it one night only, or ongoing.
Talking about the pamphlet, the Canadian activists wondered what an updated version would include, which they attempted to answer in the introduction of the pamphlet:
Thirty-years after the publication of "How to Have Sex in an Epidemic: One Approach" we face a new type of emergency here in Canada. State neglect in the response supporting people with HIV is now coupled with intensified forms of state control, surveillance and criminalization. Canada is among the most punitive countries in the world for HIV-positive people, where the state is turning towards criminalization instead of public education and support.
While it was written from a Canadian perspective, it includes feedback provided by people within the AIDS movement from the US and Canada and can be applied to the idea of HIV related criminalization around the world. It is not intended to be prescriptive, although there are suggested strategies for living with HIV in a police state, such as freezing used condoms. Rather it is descriptive, capturing the current moment and connecting it to the past, drawing attention to what has changed and not changed in the 30+ years bridging "How To Have Sex In An Epidemic: One Approach" and "How to Have Sex in A Police State: One Approach." The title play is intentional. It drives home a message that as destructive as the human immunodeficiency virus it, the epidemic is not just the virus, it is also the police state.
By coming together to create a document speaking to people now, using strategies from the past, the anonymous AIDS collective brought together the tender and powerful “confrontational activism” as employed by Berkowitz, Callen, Sonnabend and many others from the early days of AIDS activism, and infused it with their own concerns and tactics. For people living with HIV, functioning in a police state can be a daily crushing blow to an already threatened existence. There is nothing funny about it, and yet sometimes to retain a shred of sanity, to make it clear you are still alive, one must let out a howl of cackle. As Gregg Bordowitz put it, “The AIDS Crisis is Ridiculous.”
Theodore (Ted) Kerr is a Canadian born, Brooklyn based writer and organizer. He was the programs manager at Visual AIDS and is currently doing his graduate work at Union Theological Seminary.
View and download HOW TO HAVE SEX IN A POLICE STATE here.
23 notes
·
View notes
Text
#USMLEPassFail: A Brave New Day

By BRYAN CARMODY, MD
Well, it happened.
Beginning as soon as 2022, USMLE Step 1 scores will be reported pass/fail.
I’m shocked. Starting around two weeks ago, I began hearing rumors from some well-connected people that this might happen… but I still didn’t believe it.
I was wrong.
The response thus far has been enormous – I haven’t been able to clear my Twitter mentions since the news broke. And unsurprisingly, the reaction has been mixed.
In the future, I’ll post more detailed responses on where we go from here – but for now, I’d like to emphasize these five things.
1. By itself, making USMLE Step 1 pass/fail doesn’t fix much.
Simply getting rid of three digit scores doesn’t improve medical education. And it doesn’t make residency selection any better, either.
It does give us the opportunity to make changes. And the importance of that should not be understated.
Put simply, this is the greatest opportunity for medical education reform since Flexner, and the greatest opportunity to re-design residency selection since… ever.
“WHAT WILL REPLACE STEP 1?” IS A HARD QUESTION. AND MAKE NO MISTAKE, THE FACT THAT IT’S A HARD QUESTION IS ONE OF THE VERY REASONS MANY CLUNG TO STEP 1 SCORES SO DOGGEDLY.
2. The path of least resistance does not take us where we want to go.
Most of the commentary on social media thus far has taken the following form:
Now only Ivy League medical students will get into competitive specialties.
Don’t worry! USMLE Step 2 CK will just be the new Step 1.
I guess DOs and IMGs can forget about getting into top residency programs.
And you know what? Most of these concerns are justified.
If we do nothing, Step 2 Mania is the natural result of a pass/fail Step 1. And unless we give program directors more useful information – and the time to thoughtfully review all the applications they receive – they’ll gravitate to another convenience metric out of necessity.
But that does not mean it’s inevitable.
3. We all have a say in what comes next.
If the rise and fall of a scored Step 1 teaches us nothing else, it should clearly demonstrate these two things.
First, advocacy works. There is no way that the NBME’s entrenched, out-of-touch bureaucracy would have ever voluntarily changed Step 1 to pass/fail – unless their feet had been repeatedly been held to the fire by the public over the past year. Change is possible – but you have to speak up.
Students, I’m looking at you – especially those from “non-elite” or international medical schools. You have a say in what comes next. How should residency programs evaluate you? Surely, answering multiple choice questions with peripheral relevance to real patient care is neither the best nor the only way to identify your talent. It’s time to dream bigger – and demand more meaningful evaluation.
Second, medical students will rise to whatever bar we set for them.
Ask them to memorize an 800 page review book so they can excel on a multiple choice question test of basic science esoterica? Done and done. Students knew most of what they were learning was pointless – but they worked tirelessly because we told them it mattered.
So program directors, now I’m looking at you. Whatever you tell students to do, they’ll do. You want high Step scores? Students will give them to you. But what really matters to you? Do you want residents who will serve the underserved? Contribute to research? Arrive on July 1 with specialty-specific knowledge? Whatever you say, goes. If you choose to grump about the loss of the bad old days, you’re abdicating your authority to set the standards you want.

YOU WON’T FIND ME SHEDDING ANY TEARS OVER THE DEMISE OF A SCORED STEP 1.
4. No one should mourn the loss of a scored Step 1.
Look around my Twitter mentions, and you can find touching testimonials mourning the demise of Step 1 scores. There are tales of useful factoids brought to bear on patient care decades later; of students inspired to consume as much (mostly useless) scientific knowledge as possible; of doors opened and careers launched because of one shining moment on test day years ago.
Give me a break.
The Step 1 score was the biggest false god in medical education, and no one should be too sad that it’s going away.
Was it objective? Sure. But the ability of three-digit scores to discriminate between applicants was actually fairly imprecise.
Did it test some useful concepts? Of course. But scoring highly required memorizing esoteric information that would never benefit an actual human patient.
Did some students benefit from scoring highly? Absolutely. But did Step 1 scores really “level the playing field” for students from international or non-prestigious medical schools overall? I doubt it.
Did it give program directors an easy way to screen applications? Yup. But was that way meaningful? Probably not. The main value of Step 1 was that it gave you a number. But if the content of the test doesn’t matter, why not just have medical students throw darts, or race go karts, or memorize digits of pi?
And of course, our idol worship of Step 1 came at a significant opportunity cost. The fact that most of us turned out okay doesn’t prove that Step 1 was the best way, or that that we wouldn’t have been better off under another system.
Here’s the thing:
Whether you liked a scored Step 1 or not, the current system is not what any of us would have designed if we were building something from the ground up.
In the scored Step 1 era, we sat back and watched as preclinical medical education turned into a glorified USMLE prep course with a five-figure/year tuition bill attached. We did nothing as residency applications spiraled out of control and program directors’ outsourced their most important decision-making to the NBME.
We shouldn’t be proud of any of this. And we shouldn’t mourn the loss of the three-digit score that enabled us to neglect the need for reform for so long.
More importantly, there is no turning back now.
If you opposed #USMLEPassFail, do your grieving for the scored USMLE – and then get to work. Saying “I told you not to make Step 1 pass/fail!” is a hollow victory. There is an opportunity here to engage our students in tasks that could actually lead them to be better physicians – but we have to seize it.
And if you supported #USMLEPassFail, now is not the time to dance on the three-digit score’s grave. We need to get to work, too – or this hard-won victory will go for naught.
5. The way forward… my opinion
Expect more from me on these topics in the future, but for now, let me put these three thoughts in your head.
WE NEED MEANINGFUL EVALUATIONS.
My 5th grader’s report card provides more useful information than any medical school transcript I’ve ever seen. He doesn’t get an “A” in math – I get to see a lengthy list of math skills and an assessment of where he’s at with all of them. Maybe he’s comfortable dividing fractions, but still developing proficiency with using variables to set up algebraic equations.
Letter grades are nice – but they don’t tell me what he knows and what he doesn’t. (I don’t get a histogram of other students’ performance and where he falls – because how other students performed is kind of irrelevant if my goal is to help him become better in math.)
The fact that elementary schools provide more information-rich evaluations than medical schools is shameful. In the past, we’ve justified this because of Step 1. Starting in 2022, that excuse will ring hollow.
Let’s be honest: there should never be a medical school evaluation in which a students is exceptional in every area. (If there is, it tells you more about the school than the student.)
Our goal should be to make medical school formative, not performative; to help learners maximize their potential without fearing failure; to provide and communicate honest feedback that leads to improvement and growth along the spectrum of medical education. (For their part, program directors need to focus less on relative accomplishment and more on potential to grow and thrive in that program/field.)
We don’t need another arms race. We do need more thoughtful evaluation. We should require students to engage in tasks that leave them – and their future patients – better off. And schools that refuse to participate in this process should be penalized by program directors and medical school applicants alike.
WE NEED HOLISTIC REVIEW.
I don’t think we need a one-size-fits-all metric to tell us who are the “best” applicants. Honestly, we don’t.
Certain talents and traits get you a lot farther in certain disciplines than others. Even within the same discipline, different programs have different needs and serve different missions. What makes a good doctor? It’s complicated. And trying to reduce that complexity down to a single three digit number is silly.
Holistic review is possible. It’s what we do at the residency program at which I’m an associate program director. But it’s labor intensive – and it requires human judgment. That last part makes some people uncomfortable, and I understand why. Holistic review has the potential to devolve into bias and cronyism. But that’s not a reason to not do it – it’s a reason to strive to do it well, to make decisions deliberately, and to build some checks and balances to make sure you stay aligned with your values.
WE ALSO NEED APPLICATION CAPS.
The only way to get away from screening metrics and treat every applicant as an individual is to limit the pile of applications that program directors receive.

THE EXISTENCE OF A SCORED STEP 1 ALLOWED US TO PRETEND THAT THIS WASN’T HAPPENING.
Look, I’ve preached this sermon before. But you’d better believe I’m gonna be carrying this particular gospel to the people again in the near future.
Afraid of application caps? Worried that they’ll disadvantage students from non-elite schools? Stay tuned for a data-driven expose of the misinformation surrounding caps coming soon.
Dr. Carmody is a pediatric nephrologist and medical educator at Eastern Virginia Medical School. This article originally appeared on The Sheriff of Sodium here.
The post #USMLEPassFail: A Brave New Day appeared first on The Health Care Blog.
#USMLEPassFail: A Brave New Day published first on https://wittooth.tumblr.com/
0 notes
Text
#USMLEPassFail: A Brave New Day

By BRYAN CARMODY, MD
Well, it happened.
Beginning as soon as 2022, USMLE Step 1 scores will be reported pass/fail.
I’m shocked. Starting around two weeks ago, I began hearing rumors from some well-connected people that this might happen… but I still didn’t believe it.
I was wrong.
The response thus far has been enormous – I haven’t been able to clear my Twitter mentions since the news broke. And unsurprisingly, the reaction has been mixed.
In the future, I’ll post more detailed responses on where we go from here – but for now, I’d like to emphasize these five things.
1. By itself, making USMLE Step 1 pass/fail doesn’t fix much.
Simply getting rid of three digit scores doesn’t improve medical education. And it doesn’t make residency selection any better, either.
It does give us the opportunity to make changes. And the importance of that should not be understated.
Put simply, this is the greatest opportunity for medical education reform since Flexner, and the greatest opportunity to re-design residency selection since… ever.
“WHAT WILL REPLACE STEP 1?” IS A HARD QUESTION. AND MAKE NO MISTAKE, THE FACT THAT IT’S A HARD QUESTION IS ONE OF THE VERY REASONS MANY CLUNG TO STEP 1 SCORES SO DOGGEDLY.
2. The path of least resistance does not take us where we want to go.
Most of the commentary on social media thus far has taken the following form:
Now only Ivy League medical students will get into competitive specialties.
Don’t worry! USMLE Step 2 CK will just be the new Step 1.
I guess DOs and IMGs can forget about getting into top residency programs.
And you know what? Most of these concerns are justified.
If we do nothing, Step 2 Mania is the natural result of a pass/fail Step 1. And unless we give program directors more useful information – and the time to thoughtfully review all the applications they receive – they’ll gravitate to another convenience metric out of necessity.
But that does not mean it’s inevitable.
3. We all have a say in what comes next.
If the rise and fall of a scored Step 1 teaches us nothing else, it should clearly demonstrate these two things.
First, advocacy works. There is no way that the NBME’s entrenched, out-of-touch bureaucracy would have ever voluntarily changed Step 1 to pass/fail – unless their feet had been repeatedly been held to the fire by the public over the past year. Change is possible – but you have to speak up.
Students, I’m looking at you – especially those from “non-elite” or international medical schools. You have a say in what comes next. How should residency programs evaluate you? Surely, answering multiple choice questions with peripheral relevance to real patient care is neither the best nor the only way to identify your talent. It’s time to dream bigger – and demand more meaningful evaluation.
Second, medical students will rise to whatever bar we set for them.
Ask them to memorize an 800 page review book so they can excel on a multiple choice question test of basic science esoterica? Done and done. Students knew most of what they were learning was pointless – but they worked tirelessly because we told them it mattered.
So program directors, now I’m looking at you. Whatever you tell students to do, they’ll do. You want high Step scores? Students will give them to you. But what really matters to you? Do you want residents who will serve the underserved? Contribute to research? Arrive on July 1 with specialty-specific knowledge? Whatever you say, goes. If you choose to grump about the loss of the bad old days, you’re abdicating your authority to set the standards you want.
YOU WON’T FIND ME SHEDDING ANY TEARS OVER THE DEMISE OF A SCORED STEP 1.
4. No one should mourn the loss of a scored Step 1.
Look around my Twitter mentions, and you can find touching testimonials mourning the demise of Step 1 scores. There are tales of useful factoids brought to bear on patient care decades later; of students inspired to consume as much (mostly useless) scientific knowledge as possible; of doors opened and careers launched because of one shining moment on test day years ago.
Give me a break.
The Step 1 score was the biggest false god in medical education, and no one should be too sad that it’s going away.
Was it objective? Sure. But the ability of three-digit scores to discriminate between applicants was actually fairly imprecise.
Did it test some useful concepts? Of course. But scoring highly required memorizing esoteric information that would never benefit an actual human patient.
Did some students benefit from scoring highly? Absolutely. But did Step 1 scores really “level the playing field” for students from international or non-prestigious medical schools overall? I doubt it.
Did it give program directors an easy way to screen applications? Yup. But was that way meaningful? Probably not. The main value of Step 1 was that it gave you a number. But if the content of the test doesn’t matter, why not just have medical students throw darts, or race go karts, or memorize digits of pi?
And of course, our idol worship of Step 1 came at a significant opportunity cost. The fact that most of us turned out okay doesn’t prove that Step 1 was the best way, or that that we wouldn’t have been better off under another system.
Here’s the thing:
Whether you liked a scored Step 1 or not, the current system is not what any of us would have designed if we were building something from the ground up.
In the scored Step 1 era, we sat back and watched as preclinical medical education turned into a glorified USMLE prep course with a five-figure/year tuition bill attached. We did nothing as residency applications spiraled out of control and program directors’ outsourced their most important decision-making to the NBME.
We shouldn’t be proud of any of this. And we shouldn’t mourn the loss of the three-digit score that enabled us to neglect the need for reform for so long.
More importantly, there is no turning back now.
If you opposed #USMLEPassFail, do your grieving for the scored USMLE – and then get to work. Saying “I told you not to make Step 1 pass/fail!” is a hollow victory. There is an opportunity here to engage our students in tasks that could actually lead them to be better physicians – but we have to seize it.
And if you supported #USMLEPassFail, now is not the time to dance on the three-digit score’s grave. We need to get to work, too – or this hard-won victory will go for naught.
5. The way forward… my opinion
Expect more from me on these topics in the future, but for now, let me put these three thoughts in your head.
WE NEED MEANINGFUL EVALUATIONS.
My 5th grader’s report card provides more useful information than any medical school transcript I’ve ever seen. He doesn’t get an “A” in math – I get to see a lengthy list of math skills and an assessment of where he’s at with all of them. Maybe he’s comfortable dividing fractions, but still developing proficiency with using variables to set up algebraic equations.
Letter grades are nice – but they don’t tell me what he knows and what he doesn’t. (I don’t get a histogram of other students’ performance and where he falls – because how other students performed is kind of irrelevant if my goal is to help him become better in math.)
The fact that elementary schools provide more information-rich evaluations than medical schools is shameful. In the past, we’ve justified this because of Step 1. Starting in 2022, that excuse will ring hollow.
Let’s be honest: there should never be a medical school evaluation in which a students is exceptional in every area. (If there is, it tells you more about the school than the student.)
Our goal should be to make medical school formative, not performative; to help learners maximize their potential without fearing failure; to provide and communicate honest feedback that leads to improvement and growth along the spectrum of medical education. (For their part, program directors need to focus less on relative accomplishment and more on potential to grow and thrive in that program/field.)
We don’t need another arms race. We do need more thoughtful evaluation. We should require students to engage in tasks that leave them – and their future patients – better off. And schools that refuse to participate in this process should be penalized by program directors and medical school applicants alike.
WE NEED HOLISTIC REVIEW.
I don’t think we need a one-size-fits-all metric to tell us who are the “best” applicants. Honestly, we don’t.
Certain talents and traits get you a lot farther in certain disciplines than others. Even within the same discipline, different programs have different needs and serve different missions. What makes a good doctor? It’s complicated. And trying to reduce that complexity down to a single three digit number is silly.
Holistic review is possible. It’s what we do at the residency program at which I’m an associate program director. But it’s labor intensive – and it requires human judgment. That last part makes some people uncomfortable, and I understand why. Holistic review has the potential to devolve into bias and cronyism. But that’s not a reason to not do it – it’s a reason to strive to do it well, to make decisions deliberately, and to build some checks and balances to make sure you stay aligned with your values.
WE ALSO NEED APPLICATION CAPS.
The only way to get away from screening metrics and treat every applicant as an individual is to limit the pile of applications that program directors receive.
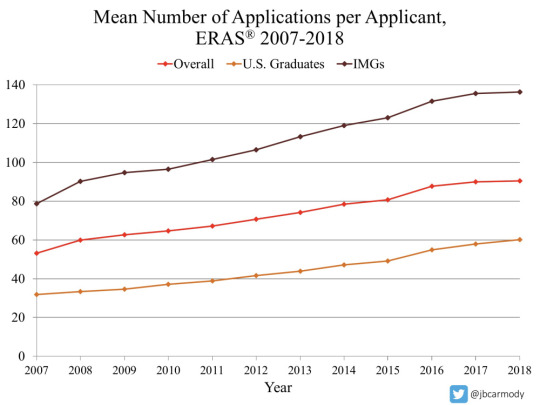
THE EXISTENCE OF A SCORED STEP 1 ALLOWED US TO PRETEND THAT THIS WASN’T HAPPENING.
Look, I’ve preached this sermon before. But you’d better believe I’m gonna be carrying this particular gospel to the people again in the near future.
Afraid of application caps? Worried that they’ll disadvantage students from non-elite schools? Stay tuned for a data-driven expose of the misinformation surrounding caps coming soon.
Dr. Carmody is a pediatric nephrologist and medical educator at Eastern Virginia Medical School. This article originally appeared on The Sheriff of Sodium here.
The post #USMLEPassFail: A Brave New Day appeared first on The Health Care Blog.
#USMLEPassFail: A Brave New Day published first on https://venabeahan.tumblr.com
0 notes
Text
Stillwater - Chapter 12
Stillwater [Archive of Our Own, FanFiction.Net, Mibba]
Characters: Original Female Character, Monkey D. Luffy, Rorona Zoro, Vinsmoke Sanji, Nami, Usopp, Tony Tony Chopper, Nefeltari Vivi
***
"We build as only children know to build
We made a way where there's a will
No slowing down or standing still
Innocent and reckless
"How did we get so old and never notice
How did we gain the world and lose the moment
Rise and fall, the tide surrounds us
And drowns us all"
-Hands Like Houses
***
“What a shame. Already over? Well that was disappointing wasn’t it?” Zoro said, sticking three swords in the ground. I had to assume they were stolen. They most certainly weren’t his. Wado, Kitetsu and Yubashiri were currently at my hip.
Bodies littered the ground around Zoro, and the people of Big Horn were staring at him in awe. Clearly, Zoro had taken all of these men out, but considering their lack of skill, I wasn’t particularly impressed. In fact, I was rather irritated.
“Right, Zoro! That was a good job, just like I told you to do! Yeah!”
“What about what I told you to do?” I asked, Usopp coming up behind him, still on the horse that Dalton had nabbed from Cocoa Weed.
I had made it to the Merry only to find the ship seemingly abandoned. I was confused at first, because I was sure that Kitetsu was there. A short search revealed the sword, its two companions, Zoro’s shoes, coat, shirt, socks and haramaki on deck, but not their owner.
I was worried. Where the hell was he? What the hell had happened? Had Wapol’s men gotten him and Carue? I was still thinking these questions over, when a thunderous sound caught my attention. There wasn’t a storm brewing. The sky was cloudy, but they were regular snow clouds. There was no sign of thunder snow. I trained my eyes on the island. An avalanche was coming down the mountain, a massive one considering I could recognize it, despite being as far away as I was. There wasn’t a doubt in my mind that Sanji and Luffy were the cause of it.
They caused it. They could handle it. I wouldn’t have been able to catch up to them anyways.
I wasn’t sure how far away was far enough, but I knew that I was probably far enough away to be safe. After all, I was on the ship. Fortunately for me, and the horse the snow hadn’t reached us. It did make things more difficult, because now there were no tracks for me to look for.
I had to find Zoro, and the only idea I had was to seek out his very presence, which was faint in comparison to that damn sword.
I would’ve liked to have trained more, to have practiced, but that wasn’t an option. I closed my eyes and did everything in my power to push out that dam demon sword and to lock onto Zoro. Kitetsu was madness. It was anger and blood lust and violence, but Zoro wasn’t. Zoro was determination, pride, and honor.
The second I was able to lock onto him, I was moving again back to Big Horn, stopping only to fish a half frozen Carue out of the river.
“You,” I started, pointedly looking at Zoro. “You are supposed to be watching the Merry with Carue, and yet I found your stuff on the Merry without you and the duck half frozen in the river.”
My words snapped Zoro out of his boasting, Usopp out of his lying and Vivi out of her amazement.
“Carue!” she cried, rushing over, and hugging the duck. “Oh my goodness! What happened to you?
“He’s alive,” I told her. “Cold, but alive.”
I looked at Usopp. “You two are supposed to be in Gyasta. Why are you in Big Horn?”
“The avalanche,” he answered.
“The doctor,” I reminded him. “Nami. That didn’t just go away, and where is Dalton?” I asked, realizing that he was missing from this scenario.
“He was shot and buried under the avalanche. We have to find him.” That brought the crowd back into it, their shock becoming worry and concern for their de facto leader.
I shook my head. “Hopeless the whole lot of you.” I tossed my bag full or Zoro’s stuff at him. “Get dressed.”
I closed my eyes and once again, opened my mind, trying to sense out Dalton’s devil fruit this time instead of Zoro.
“Don’t just sit there! Do something!” someone yelled at me.
“I am,” I growled out, trying to focus. I had managed with Zoro. I could do it again. It was just frustrating that it took so long and that it required so much concentration, even though he couldn’t be that far away.
“Mira-“ Vivi said. She was treading carefully, trying not to upset me.
I put a hand up to stop her. “Got ya.” I stood up and walked over to the patch of snow, where I knew Dalton was and started digging, revealing his face after a moment.
“Yo!” I called, beckoning the others over. Immediately, they got to work, helping me dig the big man out.
“This is horrible! I don’t feel a heartbeat!” a man yelled.
“Damn it!” I swore. No way of telling how long his heart had been stopped, how much damage it had done. ‘I should’ve been faster.’
I moved to start CPR. I didn’t know what good it could really do. Even if I could keep his blood pumping, there was no doctor to try to fix the damage. There was no chance that he would make it up the mountain in this condition.
“He’s too large. A tiny girl like you isn’t strong enough to-“
I ignored the person speaking, starting the chest compressions with ease.
“No! Dalton! Please wake up! Please Dalton! You have to!” Vivi cried, taking his large hand in her much smaller one.
Everyone around us, just looked on sadly.
“Vivi. Mira,” Usopp said gently.
“No,” I said sternly. I could still feel that devil fruit. Until it disappeared, he wasn’t dead.
“You can’t die! Dalton please!”
“Don’t worry. He’s not dead.”
I glanced towards the voice, seeing Wapol’s private doctors standing there.
“The 20 MDs?!”
“He will be, if we don’t act soon. He has severe frost bite,” another said.
“We can begin treatment immediately, if you’ll let us.”
“Hey what do you know, there are doctors here. That’s funny. I thought I heard that there weren’t any in this country,” Zoro noted.
Usopp filled Zoro in. “There are a few doctors, but these guys are the 20 MDs. They work exclusively for Wapol, so that makes them bad doctors.”
“That’s right! We can’t trust any of you! Traitors! You expect us to leave Dalton with you? You surrendered to Wapol without a fight and turned your backs on us.”
“Wapol probably sent you here to kill Dalton.”
“Please, if you want to save him, just do as I say.”
“They’re cowards,” I said, still doing compressions. “That doesn’t make them bad doctors. It just means that they’re more motivated by fear than anything.” I looked up at the 20 MDs. “I don’t know your intentions. Maybe you’ve had a change of heart and are finally doing the right thing. I don’t care. You’re going to save him. If you don’t, I’m going to make the rest of what will be your short existence an absolute hell.”
“The 20 of us are still doctors. Even though we were forced against our will to serve only Wapol, we’ve always worked to advance our medical research for the benefit of all the patients in this country. It was all because of a certain quack, who taught us never to give up. We can’t afford to lose any more men like him.”
“Then quit standing there, and get to work,” I barked.
The doctors immediately got to work, one of them taking over for me. I stepped back and took a deep breath. I looked around at all the people gathered, staring.
“See about unburying one of these houses,” I ordered the crowd. “Dalton’s going to need some place warm and a bed to rest in. I’ll watch the doctors.”
They all seemed hesitant at first, but Zoro and Usopp took charge, leading the digging effort, getting the people doing something.
Vivi stayed at first, but I urged her to go check on Carue.
I wasn’t a doctor. I couldn’t say that I fully understood what it was that the 20 MDs were doing. I couldn’t trust what I was seeing, due to my limited knowledge, but neither could the others. Unlike them, I could handle this. I could watch as the doctors treated Dalton. I wasn’t close to the man. I hadn’t been out right wronged by the doctors. I had no reason to trust them sure, but I also didn’t have that need for revenge that the others did. I wasn’t like Vivi, so emotionally involved at this point, you would’ve thought that she’d dealt with Wapol’s tyranny firsthand as opposed through the stories of others.
They managed to stabilize him, just as the crowd managed to clear a path to the door of someone’s home. I helped carry Dalton, setting him on the bed in the home. The doctors were then able to perform the more delicate procedures necessary to save Dalton. It took hours, but at long last they were done. Now the only thing we could do was wait for him to wake up.
A few of the villagers came inside to wait. They watched as the doctors continued to monitor Dalton. It was a tense atmosphere, but that tension was released, when Dalton opened his eyes.
“It’s a miracle!”
“He’s awake!”
I stood there while the doctors did a few tests and once overs. Dalton wasn’t fully there yet, having just woken up, but according to the doctors everything looked good.
With Dalton awake, my watch was over. I popped off of the wall that I had been leaning against and stretched, heading out, while everyone crowded around Dalton. Once outside, I took a deep breath the freezing air helping to clear that last but of tension out of my body. Then I went looking for Vivi, Zoro and Usopp. Carue was in the house in another room, wrapped in blankets sitting near a fire.
“You’re worried about Nami, and Luffy, and Sanji and Dalton. And everything that’s going on in Alabasta.”
I followed the sound of Usopp’s voice. “Vivi, can’t you see it? You’re carrying too many burdens on your shoulders. Calm down. You don’t need to go up there at all. You know why? Cause those three are fine. That’s Luffy, and Sanji and Nami up there. I have faith in them.”
“Thanks a lot. You’re full of wisdom, Usopp,” Vivi complimented the sniper.
“No. He’s full of crap,” Zoro argued. “He’s just afraid to go up that mountain.”
I found them standing between two houses by a fence, just a few down from where Dalton was being treated. Zoro was poking Usopp, whose legs were shaking with fear, in the forehead repeatedly.
“Agh! I heard there were things like yetis and huge man-eating bunnies up there! I don’t want to get eaten!”
“Then say so at the start coward.”
I rolled my eyes, but laughed. “Zoro, leave Usopp alone. It was a nice sentiment, even if it was just because he’s scared.”
“Mira, how’s Dalton?” Vivi asked.
“He was just waking up, when I left,” I told them.
“That’s a relief,” Vivi said.
“He’s a tough one. He’ll be fine.”
The door to the house opened, and Dalton came stumbling out.
“It’s Dalton!”
“Thank goodness!”
“What is that idiot doing?” I asked.
“Can someone please tell me who this guy is?” Zoro asked.
“Dalton, please listen to reason.”
“Get out of my way. We can’t let Wapol retake the castle. We can’t.”
“So that’s where you’re heading? The castle?” Vivi asked.
“In your condition?” Usopp added.
“My country is far more important,” Dalton said. “HE CANNOT SUCCEED! I WILL NOT LET THAT HAPPEN! NOT NOW NOT EVER WAPOL MUST PERISH!”
“But you’re not strong enough to fight them in your condition sir.”
“And the rest of us are no fight for them either.”
“I’m going to settle this thing once and for all. I’ll stop Wapol, even if it kills me.”
“Got admire his determination and his dedication to his country,” I said. “But I put forth entirely too much effort in to keeping him alive to let him go and kill himself.”
Usopp moved first walking over and stepping in Dalton’s path. I watched on, curious as to what he was gonna do. Dalton was a brave warrior, something that we knew Usopp admired. It was interesting to see that his approach was. I doubted he was going to try to talk Dalton out of it. This kind of heroic endeavor was just the kind of thing that Usopp loved.
Not surprisingly, Usopp was on Dalton’s side. What as surprising was that Usopp planned to carry Dalton up the mountain.
“Oh this is gonna be sad,” I said.
“Embarrassing,” Zoro added.
It was. The thought was nice, but Usopp just wasn’t strong enough to carry Dalton. He gave it a good try though.
“Alright, go help him,” I said to Zoro. “You’re the only one, who can carry him without dragging him on the ground.”
I could lift Dalton. It would be easy. I just wasn’t tall enough to carry him without dragging his feet and considering that he had frostbite that probably wasn’t the best idea.
Zoro shook his head, walking over and lifting Dalton up on his shoulder.
“Are you gonna sit there and whine or are you coming with us?” Zoro asked Usopp.
I hurried over, catching up with them.
Usopp was yelling at Zoro about stealing his thunder, hitting and kicking him.
“Boys, play nice,” I scolded, trying to hide my amusement.
“Hey! Hold up. There’s an easier way up to the castle,” someone called out. “Instead of walking, take the rope way.”
“The rope way? That’s impossible. There hasn’t been one connected to Wapol’s castle in a while.”
“Someone must’ve just recently reconnected one, because I just saw it. There was a rope going from the castle to a big white tree outside of Gyasta.”
‘Of course, where we should’ve headed to begin with.’
We along with a number of the Drum Island residents headed to Gyasta. At the base of the rope was a gondola, which Vivi, Usopp, Zoro, Dalton, myself and roughly a dozen men crowded into. It was entirely too crowd, resulting in it being slow moving, but it was at least moving.
Dalton was seething, where he sat.
“You need to settle down. You’re just going to worsen your condition, if you keep behaving like this,” I said.
My words were ignored. He continued to rant and rave. I understood he was upset, but he was going to die, if he didn’t settle down.
I finally understood why I was ignored, when he pulled multiple sticks of dynamite out of his jacket.
“When we get up there, everyone take cover. There are going to be explosions, once I get inside.”
I was the only one still paying attention to the top of the mountain, the smoke that had started to come from it along with a few loud crashes. ‘Captain made it,’ I thought, grinning. “Dalton, when we get up there. You are going to sit down and take it easy,” I told him.
“Wapol-“ he started.
“Luffy!” I shot back. “Our captain is up there. Our navigator. Our cook. That’s what Wapol ran into, when he came up here to reclaim that castle.”
Everyone started looking up at the castle like I was.
“She’s right,” Usopp said, sounding smug. “You brought that dynamite to blow up Wapol, but there isn’t going to be any Wapol to blow up.”
“I know he doesn’t look like much, but I’m willing to put the fate of my own country in Luffy’s hands. You should have faith that he will protect yours,” Vivi said.
“But he doesn’t know-“
I smiled back at Vivi and Dalton. “That bastard ate part of our ship, tried to eat Luffy, and if he’s up there, has likely threatened Nami and Sanji.”
“Luffy’s gonna kick his ass,” Zoro said.
The people of Drum just looked at us, probably thinking that we were mad. I didn’t blame them. If I had been in their position, I’d have my doubts to. I turned, keeping my eyes trained on the mountain top.
Sure enough, a few moments later, what looked to be a much thinner Wapol rocketed overhead.
“Atta boy, Luffy,” I praised.
We made it to the top, Zoro, Usopp and I getting off and going ahead to scout out the area. We didn’t know, who else was with Wapol or even for sure if the guy that had been launched off the island even was Wapol.
Usopp, who had declared that he was going to go ahead and brave whatever dangers there would be, was cowering behind Zoro by the time we reach the top of the staircase that led from the gondola bay to the outside world.
“Hey! What the hell are you doing?” Zoro asked, swatting at Usopp, trying to get him to release his leg.
“Just watching your back.”
‘Idiots,’ I thought fondly.
The view from up here was gorgeous.
A familiar scream caused me to spin around and Zoro and Usopp to stop bickering. Luffy had rocketed himself towards us… Because of course he did.
“LUFFY!” the other two screamed in panic.
They dove out of the way of our captain. I braced myself, digging my feet into the ground as much as I could, but with the snow it was difficult. I caught Luffy around the torso, the impact caused me to slide back roughly twenty feet, before coming to a stop.
Luffy started laughing. “Nice catch, Mira!”
“Thanks, Captain,” I responded, chuckling.
“Why’d you do that, you moron?!” Zoro raged.
I set Luffy back on his feet, and stood up properly, dusting the snow off of myself.
“I didn’t recognize you,” Luffy explained. “I thought you were more of Big Mouth’s guards ready to fight. I’m surprised you came up here. Well not you Zoro, Mira, but Usopp, aren’t you usually scared of doing stuff like climbing mountains?”
“HAHAHAHA! Yeah right,” Usopp scoffed. “Whenever there’s a towering peak in front of me, I climb it, but let me tell you scaling that mountain hand over hand was no picnic.”
“Actually, we took a rope way car,” Vivi explained, causing Usopp to topple over. “Nami and Sanji are they alright?”
“Yeah! Both of them are just fine.”
“Thank goodness.”
“I knew you had it all under control.”
“So what was that you were doing on top of the castle a few minutes ago?” Zoro asked.
“Beating the crap out of the king,” Luffy said.
“Dalton,” I greeted, seeing him exit the stairwell. “You’re just in time.”
“You mean that person I saw flying through the air was actually Wapol?” Dalton asked, disbelief clear on his face. “You beat him?”
“Yep. I sure did.”
“And his two henchmen what happened to them?”
“Well the reindeer beat him up.”
“But those two? A reindeer?” Dalton was still struggling to accept it.
“Reindeer?” I asked. “Another zoan?”
“Hey Usopp, I made a new friend. You gotta meet him. Get this. He’s a reindeer.”
‘Leave it to Luffy.’
Dalton notice something in the trees. I followed his gaze to wear a little reindeer was standing. I think it was trying to hide, but it was backwards. I had thought that, when Luffy said a reindeer he had found a human that had eaten the ox ox fruit, model reindeer, but based on his appeared this appeared to be a reindeer that had eaten a human human fruit.
I wasn’t thinking about that at the time though that came later, because my first thought, which tumbled out of my mouth on its own was, “So freaking cute.”
Dalton bowed to the reindeer, thanking it for helping the country. The rest of the people of Drum finally made their way over to us. They all looked at the reindeer.
“What? What is that strange creature behind that tree?”
“It almost looks like a reindeer.”
“No. You’re wrong. It’s a monster.”
Humans. Ignorant creatures. Afraid of what they didn’t know of what they didn’t understand.
“No! Don’t shoot him!” Dalton ordered.
Something finally registered in Usopp’s head, because he screamed, eyes nearly popping out of his head. “It’s a yeti! Somebody shoot it!”
The words of the people upset the reindeer, who sped off into the forest, crying.
I spun around and knocked Usopp upside the head, at the same time as Luffy.
“You jerk face!” Luffy yelled. “He’s not a yeti, you idiot! He’s my new friend!”
“You coward! He wasn’t hurting you! Don’t go screaming fire until you know something’s a threat!”
You’d figure that after Little Garden Usopp would’ve realized that things weren’t always what they seemed, but no. Fear controlled him more than anything else.
“You scared him so bad he ran away,” Luffy continued.
“If you could kill Dorry and Broggy would you have just shot them on sight? You wouldn’t have a master then would you?”
“You’re right. You’re right. I’m sorry.”
“It’s not us that you need to say sorry to,” Luffy said.
Usopp slumped in defeat.
“I’m gonna go get him, so that you can apologize.” With that Luffy took off after the reindeer.
“I never seen Mira get this mad. Way to go Usopp,” Zoro jabbed.
“I’m not mad,” I corrected. “I’m annoyed that a crewmate of mine would behave in such a manner. I know what it’s like to be afraid. I also know what it’s like to be the thing that people are afraid of. It hurts, especially, when you know that the only reason people are still afraid of you is because they won’t give you a chance.”
I glared at the villagers, who looked appropriately sheepish.
“The doctor is here right? We need to get Dalton to her.”
“The girl’s right,” a voice called out.
The villagers gasped. “Doctor Kureha?!”
“Yeah. Good to see you too. Now be useful and get the injured guy to the medical ward.”
“I recognize you! You’re that damn old hag from before!” Zoro yelled.
You would think that seeing a woman dressed like she’s twenty, despite probably being seven times that, would be a dead giveaway that she was sensitive to the whole age thing, but apparently not to Zoro. Kureha brought her fist down on top of his head, knocking him to the ground. I could see the goose egg forming.
“You had that one coming,” I told him.
I shook my head. “Someone keep his feet from dragging,” I said, hoisting Dalton up over my shoulder.
The villagers were all still.
“I’d do what the girl says, or you’re going to be in pain like this man here,” Kureha said.
That got them all moving, lifting Dalton’s feet as we headed to the medical ward.
***
Notes:
***
Previous | Next
***
Master List | Mobile Version
1 note
·
View note
Text
Remedy

Tags: @the-shewxlf, @megant22, @sexywolfsfordays, @houseofrahl, @sterek-basically, @kittycatgirlmaddie, @misshinehou, @unbreakablevoices, @champagneblues, @dallysgreasergirl, @juliaspnlover, @cineyou, @lipstickstainsandwerewolfchains, @fallenangel-13x, @urwarriorangel, @bless-my-demons, @lunaskyhunter, @arkhamirwin, @fangirlnerd101, @m-a-t-91, @meanwhilesmiley, @edithambroreigns, @totallovelesson@kxttykatmichael
Word count: 1697
Author’s note: So, here’s one of the promised works, woohooo! My pack told me they aren’t familiar with the series, so it makes me even more excited to be able to introduce you to the astonishing world of House MD. :3 (Those of you who have never heard of the series: you might want to take a look at this video. I spent quite a bit of time with picking out the best that more or less sums up this complex series, and in the end, I settled on this one.) As for the picture, I’m not even the tiniest bit sorry ;) (I have a thing for uniforms and suits, seriously... if this is a disease then I’m incurably infected.)
Betas: @i-am-a-misguided-misfit, @lipstickstainsandwerewolfchains, @mixed-up-fangirl, @kittycatgirlmaddie, @fallenangel-13x, @the-shewxlf, @b-chocolatelover, @from2016, @safiac, @random-fandom-fangirl2112
Again, thank you your work, sweets!! ❤️
Masterpost
Your name: submit What is this? // <![CDATA[ document.getElementById("submit").addEventListener('click', myHandler); function myHandler() { var v = document.body.innerHTML; var input = document.getElementById("inputTxt").value; v = v.replace(/\by\/n\b|\(y\/n\)/ig, input); document.body.innerHTML = v; } // ]]>
I don’t have to hurry now, because we don’t have a new patient at the moment. Our last one was sent out of Princeton-Plainsboro safe and sound two days ago, and since then, I haven’t seen my boss’s—Gregory House’s—face. My colleagues have been busy with minor jobs, so the privilege of being in charge instead of House landed on me in the end; I have to take care of his private hours to deal with people who come to see a doctor for an illness as simple as a flu or a running nose. Of course, it was inevitable that Cuddy grew suspicious after she found everything perfectly documented and done in connection with that genius man’s consultation hours—hence, after one of the controls, she entered the room, only to find me sitting with the notepad overlapping my thighs, papers in hand, faking House’s signature on each one of them.
Since then, I’ve been forbidden to take care of the people and do House’s job instead of him, which is why my current task is to try to reach him through his phone and pray him back into the hospital to do his work properly instead of having me do it for him—but I know the only way to coax him back is finding a new case, but it’s not as easy as one might think; finding something that genuinely piques House’s interest is like looking for a needle in a hayrick.
Right now, I’m standing at the nurses’ desk with a random person’s file in hand, roaming over the lines idly just to kill the much time on my hands with my phone plastered between my cheek and shoulder to keep it in place, waiting for the dialling tone to end and hear House speak on the other end of the line—which never seems to happen.
Exhaling an exasperated breath, I place the document back into the folder holder before deciding to head to the ER. I need to find something to do, even if just a quick job, otherwise I’ll most likely go nuts by the end of the day due to a fried brain. I adjust the white labcoat and my ID card clipped to it, before picking up a stethoscope to hang it in my neck. Upon entering the ER, I look around to see a few nurses dealing with all the patients. Thankfully, upon scanning the area, I notice Allison Cameron; without thinking, I approach her in hopes she could help me, albeit she’s busy on her own.
“Hey, Cameron,” I greet her. She doesn’t even look at me, being too preoccupied with removing broken splinters of glass from a man’s skin with a tweezer.
“Lockwood,” she replies, only with a quick glance cast at me with a small smile in the corner of her mouth, then her blue gaze is already gone, focused back on her patient, resuming her task at hand.
“Do you have something for me?” I ask with just a touch too much desperation in my tone. I find myself cracking my knuckles in anticipation in the pockets of my gown.
“House is not back yet, is he?” She forms that as a question, but I have a feeling she meant that to rather be a declaration. She knows House like she knows the back of her hand—all those years she’s spent working for the man, she’s gotten used to his erratic behaviour.
“Nope. And he won’t pick his phone up either.”
“And he won’t do that unless he has a good reason to,” she points out the obvious to me; that much I know, too.
“So do you have or don’t have?” I insist stubbornly. I can’t let everyone just shake me off because it would be too inconvenient for them to find a task for me. I’m an intern, that’s part of what they are supposed to do for me. After a couple moments of contemplation, Cameron offers, “A police officer was transited here not ten minutes ago. Gunshot wound.”
“Where do I find him?” I ask immediately. She points behind me with a mild jerk of her chin, and I turn to see my new patient, but instead of himself, I find myself looking at a pale turquoise curtain. I hastily pick up every tool I’ll need to take care of the officer; I arrange everything on a metal tray before taking off towards the cop. Tucking the curtain away, I finally see him—laying on the bed, palms covering his body where the bullet passed through his skin, wide eyes now trained on me after his attention was attracted at me by the loud swoosh.
To be honest, when I was told that a member of the force was shot, I expected anything but an arrest-worthily stunning man. I thought I would find myself face to face with a tad obese man who consumes too many doughnuts during the free periods in his shift, maybe in his late forties, too—but instead of that, my patient is an attractive man with firm tones and a sculpted body. When I glance down at his chart where a nurse has previously written his data, I quickly calculate in my mind that he’s twenty-six. Years before I joined health-care, such a scenario had already been on my bucket list, but I wouldn’t have dared to think it would come true once.
Looking back into his eyes, a shiver runs down my spine when I notice how much his gaze has changed—now it conveys anger and impatience, and I would like to believe it’s not because of me, but because he was shot and is now frustrated that he can’t do justice in town.
“It takes ten minutes to treat a cop on the ER?” His voice stings me to the core, but I choose not to let his bitter remark get to me—just because he has a bad day, doesn’t mean mine has to be ruined, too. Instead of biting back something in response, I jovially smile at him as I set the tray down beside the hospital bed he’s occupying, after closing the curtain back behind me. The loud smack of the rubber gloves sharply reverberate around us as I’m putting them on.
“I imagine you don’t get to handle everything all at once, either,” I can’t resist commenting, but there’s no actual heat behind it. That seems to have the desired effect on him, though, because his stiff posture softens, tension apparently seeping out of his frame. I reach for a small cloud of cotton that I drench in the disinfectant just moments later. I grab the piece with a tweezer, then move to treat the abused area of the man’s skin. He pops the buttons on his uniform without a word, opening the garment up and revealing his naked upper body to me. It sways me a little, but I gain my strength back quickly. “This may hurt a little,” I say gently, but I must sound like I’m trailing off—and I probably am, because I’m transforming into the detached doctor I’m supposed to be at the moment.
The tiniest hiss is what I get in return to my warning as soon as the puffy material touches the wound. After I’m ready, I launch into fishing out the bullet from his body—no operation is needed, because it’s not in too deep, thanks to the bulletproof vest he wore, but had taken off before I approached him—now it’s laying on the chair stood next to his bed, long forgotten. The officer’s torso is covered in blood, and the more ministrations I do, the messier it gets, so from time to time I need to swipe him clean.
The silence settled between us is just stretching and stretching, none of us seems to have any intentions of breaking it anytime soon. Thus, the sounds of the rest of the ER encompass us—the intermittently ringing phones, the general hustle and bustle of people, patients and nurses included, a voice calling Dr. Wright to head to the nurses’ desk through the speaker, and conversations that are muted to low buzzing in our ears.
For some reason, I feel tempted to ask him how he got shot, so after a short consideration, I do just that. His answer throws me for a loop, however.
“I don’t know.”
“How can you possibly not know that?” I ask before I could stop myself and think otherwise. My hand stopped over his wound without my consent, but the bullet is out of him, and I only need to stitch him up now, so it’s fine. He doesn’t take my question personally—more so, he seems embarrassed about it. I instantly say it’s never mind, and go to resume my work, getting ready the needle and the thread, when he abruptly speaks up again. For some reason, it gives me the sense that he feels like sharing right now; not just anything, but his darkest secret, and he thinks I’m the perfect recipient of his honesty.
“I have no clue what happened. Suddenly I blacked out, then the next thing I know is that I’m in an ambulance on my way to the hospital.”
My eyebrows knit together in confusion, but refrain from commenting anything this time. I do ask him, “Did you black out after being shot or before that?”
The officer purses his lips into a thin line, apparently deep in thought to give me a plausible response. He ends up answering, “I’m not sure.”
The words barely leave his mouth when I’m muttering in a flurry, “Wait a second, I need to make an important call,” pulling off the gloves from my hands clumsily, while I’m already trying to reach for my cell phone. I put distance between the man and me, phone already plastered to my cheek and my other hand covering my free ear, find an abandoned and remotely silent corner outside of the ER, then wait for the dialling tone to stop before starting to talk.
“House, I think I found us a new case.”
#derek hale imagine#derek hale fanfiction#derek hale#teen wolf imagine#teen wolf fanfiction#teen wolf#derek hale blog#imagine blog#derek hale x reader#doctor reader#intern reader#house md#dr allison cameron#dr gregory house#policeman derek#derek is a cop#didn't see that one coming#uniforms#derek is in da uniform#british spelling#sorry not sorry#just the beginning it gets better i promise#dr lisa cuddy#princeton-plainsboro#hospital#reader insert#interactive fiction#interactive fic#snarky derek#snarky reader
160 notes
·
View notes
Text
I watched the pilot episode of The Apprentice (US) and holy shit do I have thoughts
Predictable opening - “I'm Donald Trump, I got so much fucking money I'm basically fucking drowning in $$$”
“I recently lost billions of dollars but I bounced back big-league and now I'm better than ever and I'm having more fun than ever” - man good for you I bet your company collapsing didn't result in any redundancies at all but hey at least you got to meet Larry King!!
(also he's clearly saying big-league back in 2004)
I don't have much to say about the actual contestants because they're all just like “name, hometown, qualifications, current job” but shout-out to the guy who got an MD and then went “man what am I gonna do with this? HELP PATIENTS???” and got an MBA instead. Shout-out for being just trash. Awful.
They all show up and meet “The Donald” and he's like “I'm fucking rich, you guys wanna get rich??”
Then he says “Women have it harder in the workplace, or so they say”
they sure as fuck do when they're within 5 miles of you, pussygrabber
He divides them up into two teams of eight, men and women, and then he fucks off
They all get taken up to this fancy-ass suite in Trump Tower where there's legitimately caviar and champagne everywhere
He explains to the camera that if you do good each episode you go back to the suite and if you do bad he FIRES you and you go home
“It's the suite or the street” mate these people all have jobs sorry you're not making anyone homeless today
He leaves letters lying around like he's a fucking murderer in a Agatha Christie novel and they're like “enjoy all this fucking caviar, now name your companies”
The men go with Versacorp because they're versatile and also unoriginal
The women go with Protege which is substantially better but I almost miss it because one of the first suggestions is “Donald's Darlings” and I'm obliged to spend like the next century puking into a bucket
So they show up next day at the NEW YORK STOCK EXCHANGE which for businesspeople is like going to fucking Disneyland, every time they say the name you can practically hear the airhorns and smell the orgasms
They all show up fancy-ass and he stands on a platform and he goes like “hey guys you're gonna sell fucking lemonade”
Then he opens the New York Stock Exchange and everything goes crazy and I guess the subtext is “Donald Trump controls the economy of New York” but I was too busy being fucking stoked we were in the FUCKING NEW YORK STOCK EXCHANGE to care about subtext cause that shit is for squares
Men run out and they just basically run to the harbour, go to a guy who sells lemonade, go “hey we'll sell your lemonade and give you a percentage of the take, just give us like literally all the supplies” and presumably the guy goes “sure as long as my store's name appears in the TV show you're filming because there's no FUCKING way I'd do this otherwise” and boom they're in shitty business
The women split up to buy supplies and then manage to get lost and there's a lot of passive-aggression about the whole thing
Meanwhile the guys are by the sea but not like on a beach just like on the world's shittest harbour. They're next to a fish market. This one dude is like running at people with a fucking sign and hassling people to buy this lemonade and jumping in front of bikes and everyone's like “man why is this dude like this he's got an MD for fuck's sake”
Donald Trump is in a fucking HELICOPTER and on his phone like “yeah look at these fucking pricks they're next to a fish market. I gotta go” and then hangs up the phone to sit there and just like revel in the fact he's in a chopper for no reason
like you know what good businesspeople don't do? take goddamn helicopter rides around the city to observe people who are already being observed
meanwhile the girls are in a decent location selling lemonade $5 a glass and this aired in 2004 so that's like $250 today. their observer guy is like “I wouldn't pay that for lemonade unless it's being served by a pretty girl. $1 for the lemonade $4 for the girl” and eww just eww
like legit this one girl is being like “aww thank you” and then kissing them on the cheek like just sell the goddamn lemonades
the guys relocate to somewhere else that looks like monumentally unpopulated and continue making fuck all
most of them are just tryna make the best of a bad job but this one guy just goes full-on quirk and like
first he like pressgangs a woman into trying to sell lemonade? because she's hot. and she's pretty obviously uncomfortable and the dude she's “trying” to sell to is like “what the fuck”
then he spends 20 minutes trying to sell a glass of lemonade for a thousand dollars
“Donald'll be impressed if I sell a glass of lemonade for a thousand dollars”
...
1. Donald hasn't been impressed by anything except himself and his bank account ever. You take a bullet for him on Monday I guarantee he's forgotten your name by Wednesday.
2. If the task was “run 100m” and you spend the time trying to learn to teleport because “Donald'll be impressed if I teleport instead” yeah but it's NOT GOING TO FUCKING HAPPEN
Shout to to this one guy who's like “I gotta buy it because you tried so hard” like fucking get shit on, business people running around Manhattan in the early evening trying to sell lemonade. The man on the street sees you and he pities you.
Next day they all go back to Trump Tower *airhorn noises * and Trump walks into the meeting like “I'm very busy today so we gotta go quickly” because good businesspeople know you gotta make your subordinates feel like shit each and every day
So the men doubled their money and the women quadrupled it so it sounds like they both did pretty fucking good, game over I guess
wait no the men are shit
the women's prize is “you get to see the nicest apartment in New York, my apartment, be there at 1 o'clock” and oh god I hope he means pm.
“guys they killed you, they gave you a good beating, so you're not gonna be seeing my apartment” OH SHIIIIIIIIIT
then it cuts to the women going up to his apartment and like you've probably seen photos but like. it's gold. fucking everything is gold. it's got a nice view and they're all gasping about how beautiful it is but you take it from me – this is a shitty apartment. the men are in the suite downstairs washing dishes and I'd rather be there than stuck in a room that looks like Midas came in and just touched everything
Then Melania comes in and it is astonishing how clearly she does not want to be there
“How do you clean a house like this?” “Well we have people for that” *rich white person laughter *
Should have just said “I fucking just pour yellow paint over it, what he's gonna do, notice?”
They all agree she's very lucky and she's like “what is he not lucky?” and good for you Melania, he IS the lucky one because he married someone who isn't gonna spend the next decade trying to tell the world an American was born in Kenya which is more than I can say for you
Cut to The Donald walking into the apartment with porn music playing
“It's nice to see him being more personable” yeah it really humanizes the businessman to know he comes home to an ugly gold house
the whole scene is capped by a woman going “oh this is so rich, this is really rich” like this scene could have been replaced by the words “I HAVE LOTS OF MONEY AND MY GIRLFRIEND'S A MODEL” flashing on the screen for a few minutes. in gold.
honestly just murder me
meanwhile the guys are fretting about who's gonna be FIYAH'D
“I'm a good debater but I know Donald can outdebate me” oh believe me I've spent 4 and a half hours watching him debate, he can't. let's just say he knows how to pronounce the word “wrong” and leave it there
The guy who tried to sell lemonade for a thousand dollars is making up a pros-and-cons list for the other people on his team and it's kind of adorable
“He's just lovable guy with great laughter and smarts” fuck I'm getting business cards with that printed on there and nothing else
The guy with an MD is a goddamn idiot
He was bragging before the meeting like “I can outdebate anyone”
he gets asked if he would have won if he was in charge, easiest question in the world, yes
“I don't think so, sales aren't my forte”
...
...
this is literally a show about selling stuff
if he gets fired I hope his exit interview is him going “oh shit I'm sorry I thought this was Big Brother the whole time”
Trump's lecturing someone on manners, no further comment needed
The leader just got accused of being a bad leader because he listened to some ideas but not others
(unrelated but if I hear the word “leader” one more time I'm not accountable for my actions)
$1000 Lemonade Man has been thrown under the bus, he's standing up complimenting Trump's parents
by NAME
everyone else has got shit-eating grins like “well I'm safe”
the final three up for firing are the captain, $1000 Lemonade Man and The Doctor Who Just Admitted To A Businessman That He's Shit At Business
$1000 Lemonade Man just stood up to make a point, Donald was like “sit down” and he was like “thank you” and sat down like I feel like I just watched a display of dominance
The doctor got fired
His exit interview was “I take solace in the fact that I have a higher IQ than the other 17 people in that room” (fuck you)
“Just goes to show there's no correlation between IQ and success (correct) in lemonade sales *smirk * (fuck youuuu)
17 other people may not be qualified as doctors (and may all be kinda shitty people in their own right) but they had the common sense to not admit to being shitty at business or to jump in front of a cyclist to try and sell lemonade
fuck you
Alright so here's my analysis of The Apprentice's Effect on the Election of Donald J Trump
the message of the show, more than anything about business or leadership or teamwork, was that Donald Trump is a rich and powerful man. Everything else is just buttressing on that. I think if you appear on a show in such a powerful position and you judge people and your word is basically law then that gets to people on a subconscious level because your fuckups aren't making it onscreen. You're not fallible. You're judge jury and executioner and your catchphrase is literally about removing power from other people. I wouldn't go so far to say that 2016 was foreshadowed back then but given how obviously the show is designed to elevate the man to demi-god status...well.
I think it may have also helped elect him because he comes off as a bastard but by God compared to the contestants he comes off brilliantly
2 notes
·
View notes
Text
Plastic Surgery Practice and Hologic™ Celebrate National Cancer Survivors Month
In Part 1 of our PSP breast cancer series, Dr Valerie Gorman explains the benefits of using the Hologic LOCalizer

during oncoplastic surgery procedures with partnering plastic and reconstructive surgeons.
Now in its 34th year, National Cancer Survivors Day (NCSD), which took place on June 6, 2021, initially launched to unite people around the world in recognition of cancer survivors, and to raise awareness of the ongoing challenges cancer survivors face. This annual celebration of life that kicks-off the first Sunday each June and extends further into National Cancer Survivors Month (NCSM), marks an important reminder for us to share resources, research, and the legislation being implemented to strengthen the survival rate of cancer patients everywhere.
At the time of this publication, the American Cancer Society estimated that in 2021 the United States will have 1,898,160 new cancer cases and 608,570 cancer-related deaths. That equals 5,200 new cases and 1,670 deaths every day, the Society notes. In addition, the statistics predict a total of 284,200 new male and female breast cancer cases on the rise, with 44,130 related deaths. But according to the American Association for Cancer Research, there are also more than 16.9 million people living with and beyond cancer in the United States alone.
In Part 1 of our Plastic Surgery Practice breast cancer series, we shine a spotlight on one of the latest technological advancements in surgical cancer treatments, the Hologic LOCalizer
. To learn more about the wire-free guidance system that is currently being used to identify cancerous lesions and improve surgical outcomes for breast cancer patients, we spoke with Valerie Gorman, MD, FACS, chief of surgery and medical director of surgical services at the Baylor Scott and White Waxahachie, Texas Surgical Specialists/Texas Breast Center. Gorman, who typically performs 15 to 25 lumpectomy procedures per month, also discussed best practices in oncoplastic surgery.
She transitioned away from the wire (needle) localization technique two years ago and began using a new system, designed to mark and guide to non-palpable breast lesions using a miniature radiofrequency identification (RFID) Tag. Another purpose of NCSD is to acknowledge the contributions of families, friends, healthcare providers—like Gorman and her medical team, and those engaged in the cancer research developments necessary to keep patients alive.
Plastic Surgery Practice: Why did you transition from using wire (needle) localization to Hologic’s LOCalizer
device, and how has it improved your work flow?
Gorman: The wire-free miniature radiofrequency identification (RFID) Tag (“clip”) makes it easier for breast surgeons to pinpoint the exact distance and location of the cancerous lesion/s to be removed. It also enables multiple clips to be placed in the breast at one time with separate identification numbers. So, if there is a larger area of breast calcifications you’ll want to add two or three tags to triangulate the affected area being targeted, especially if there is more than one lateral, or medial lesion to be taken out.
Another reason I transitioned over to using the new wire-free device is because wire localization could only be done on the day of surgery, so my breast cancer patients had to arrive extra early to prepare for two different procedures in the same day—the wire placement to detect the affected tissue, and the breast cancer surgery to remove it. Depending on the complexity of radiology and operating room (OR) timelines, patients were required to wait hours inside of the day surgery area before we can finally schedule their case, because they could not go home wearing a wire. Using the miniature radiofrequency identification (RFID) Tag (“clip”), we’re now able to place the clip a week or two before surgery—or longer if needed, so there is much more flexibility with no limitations. This saves time for the radiologist, doctor, and patient.
In fact, some patients receive chemotherapy treatments prior to breast cancer surgery. The doctor can place the clip in the breast at the time of biopsy or before chemo to have it ready for upcoming breast surgery. And, if additional health issues arise that prevent the scheduled breast surgery, you don’t have to replace the clip.
For example, one of my cancer patients had a clip placement, and between the time we placed the clip and the time she was scheduled to have breast surgery, she broke her hip. It was a very protracted recovery period, but we didn’t have to do anything because the clip stayed in place until we were ready to do the surgery. As soon as she recovered from hip surgery, we were able to operate because the clip was still in place for many weeks.
PSP: Describe your oncoplastic surgery experience collaborating with plastic and reconstructive surgeons on patient cases.
Gorman: We have a supportive plastic surgeon, and our entire medical team is very close. When I partner with our plastic surgeon on lumpectomy procedures at Baylor Scott and White Waxahachie, Texas Surgical Specialists/Texas Breast Center, he’ll do a breast reduction at the same time. The LOCalizer
helps me identify the location I need to put the incision, so he can plan the pedicle method for breast reduction.
During my previous training for the wire localization method, we were taught to go in right over the wire to pull the lesion and address any cosmetic issues once the cancer was removed. As doctors we can now try our best to make breast surgery outcomes cosmetically favorable— rebuilding the breast for each patient helping them during a difficult time. Hologic LOCalizer
helps doctors plan effectively for patient cases, and in the OR to make sure we have all the advantages to perform the best oncoplastic reconstructive lumpectomy type techniques.
PSP: Why is it crucial for oncologists and plastic surgeons to support the needs of cancer patients in unison?
Gorman: Historically, I’ve worked with other plastic surgeons who didn’t have the same vision or care for the patient. It’s important to partner with a plastic surgeon who is willing to listen to the patient—and together as a team, and who also has the same goal for your patient—which is to treat the patient’s cancer in the best way possible, because we want our patients to do well. In addition, for patients who have always been unsatisfied with their breast size because it has kept them from doing certain activities, we can do a breast reduction with the lumpectomy and meet their goal while we’re taking good care of the cancer. A plastic surgeon who is not limited to only one approach and has many tools available to patients will be able to offer a menu of reconstruction options as needed, such a breast reduction with free nipple graft, nipple-sparing mastectomy, or a DIEP flap.
We want to treat the cancer and take it away from them in the best oncological way, so they don’t have any long-term effects from the disease or any recurring cancer. We aim to maintain the goals of each patient’s cosmetic results, which is different for each patient depending on their preference. Sensitivity is key to figuring out what that is, evaluating the resources, and making sure the whole team is on board.
PSP: What other features does this device offer that you appreciate most?
Gorman: I really like the pencil-size of the Surgical Probe. It’s smaller than my pinky, disposable, and doesn’t need a cover! It can be used during the lumpectomy within the cavity to identify when you’re getting close to the lesion and when you’re traveling from your incision over to it. The entire device is compact, so I don’t have to worry about another big device that needs to be hooked on a stand and have a wire connected to it. This just sits on the table, and the price is right. Surgery waiting room times and OR scheduling time crunches can also be costly, so the savings on that by using the Hologic LOCalizer
, pays for itself.
Tonya Johnson is associate editor of Plastic Surgery Practice
Review a Lumpectomy Case
Review how LOCalizer and other Hologic products impacted a right reconstructive lumpectomy
Watch Video
Sponsored by

Medqor is committed to protecting and respecting your privacy. We may contact you about our products and services or share information with sponsorship partners, as well as other content that may be of interest to you. By submitting your information, you consent to us contacting you for this purpose in accordance with our privacy policy.
For further information, please check out our privacy policy here
source https://plasticsurgerypractice.com/client-objectives/aesthetics/reconstructive-surgery/breast-cancer/plastic-surgery-practice-and-hologic-celebrate-national-cancer-survivors-month/
0 notes
Last Seen Blogs

midnight-directives
one day the walls will fall

2-3bpg
. Ali

revlatmeslo
Sou...

cedarshop-blog
Untitled

cappycodeart
Living in the State of Dreaming