#GVHD
Text

Stem cell transplantation (SCT) can cause a host of complications. Graft versus host disease (GVHD) is common and can be severe, affecting many organ systems. In acute GVHD, end-organ damage is the result of recipient's APCs interacting with donor T-cells, leading to donor T-cell activation with a resultant cell-mediated and inflammatory cascade. The pathophysiology of chronic GVHD is not well understood. Skin, small intestine, and liver are most commonly affected; lung involvement is less common.
Acute GVHD typically occurs within 100 days post SCT and can cause bowel wall thickening and/or dilatation, biliary abnormalities, ascites, pulmonary edema, diffuse alveolar hemorrhage, and a myriad of other findings. Chronic GVHD typically occurs within 2 years of SCT and may affect skin, mouth, GI tract, liver, lungs, muscles, joints, or genitals. Imaging is based on presenting symptoms.
Read more about the complications of SCT (including GVHD) from the American Cancer Society. https://www.cancer.org/.../transplant-side-effects.html
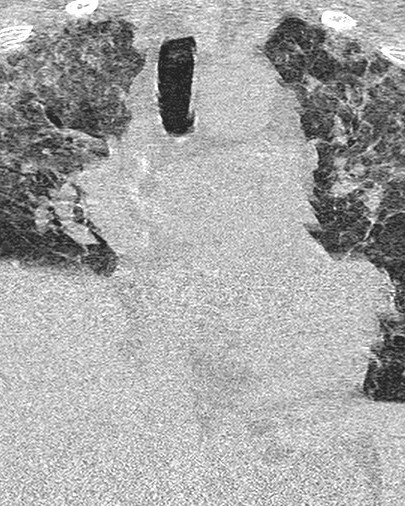
Today’s case is a patient 2 months post SCT who presented with shortness of breath, nausea, and vomiting. Lungs demonstrate upper lung predominant groundglass opacities and interstitial thickening, worrisome for acute GVHD. The cecum is thickened and enhancing, with pneumatosis, likely indicating typhlitis (neutropenic colitis). There is also moderate volume ascites.
Case courtesy of Hoe Han Guan, Radiopaedia.org, rID: 166522
#TeachingRounds#FOAMEd#FOAMRAd#Radiology#transplant#transplantimaging#transplantmedicine#infectiousdisease#pulmonology#gastroenterology#hematology#GVHD#stemcelltransplant
2 notes
·
View notes
Text
youtube
#StemCellTransplant#BoneMarrowTransplant#AutologousTransplant#AllogeneicTransplant#SyngeneicTransplant#HematologicCancers#Leukemia#Lymphoma#MultipleMyeloma#PeripheralBloodStemCells#UmbilicalCordBlood#GVHD#ConditioningRegimen#Engraftment#Immunotherapy#AplasticAnemia#SickleCellAnemia#GeneEditing#CAR-TCellTherapy#CordBloodExpansion#Youtube
0 notes
Text
The medical expertise and nursing care here is excellent
I just want to clear up some misunderstandings that may arise from some of my previous posts; the fact that none of the samples from Leah’s lungs have ever grown any bugs is not actually good news – a lung infection in a post transplant patient is potentially easier to treat than inflammation.
Inflammation of the lungs is called PNEUMONITIS and I’m told that in Leah’s case it’s likely to be an…
View On WordPress
#Belfast City Hospital#Bristol Children&039;s Hospital#GVHD#ICU#Immune reaction#lack of facilities#medical expertise#nursing care#pneumonitis#post transplant
0 notes
Text
𝗘𝘅𝗽𝗹𝗼𝗿𝗶𝗻𝗴 𝗠𝗮𝗿𝗸𝗲𝘁 𝗜𝗻𝘀𝗶𝗴𝗵𝘁𝘀: Graft-Versus-Host Disease (GvHD): Graft-Versus-Host Disease (GvHD)
Wissen Research presents a comprehensive report on Graft-Versus-Host Disease (GvHD) highlighting:
#Market Insight
#Opportunity Analysis
#Key Opinion Leader Analysis
#Regulatory Analysis
#Clinical Trial
#Product Analysis (Approved and Pipeline)
#Patent Analysis
#Scientific Literature Analysis
#Market Forecast
📑For detailed report: https://www.wissenresearch.com/graft-versus-host-disease-market-report-2023/
📑 Request customized study: https://www.wissenresearch.com/ask-for-customization/
1 note
·
View note
Text
How much percentage robot is Simmons even?
I cannot figure it out without thinking abt how that operation is done both functionally and safely
Does anyone know if it was ever mentioned?
#Posting on my art acc bc Im going insane trying to design him!!#rvb#red vs blue#dick simmons#Ive done actual research to see what types of transplantation would seem similar#The GVHD on this one goes CRAZY!!!
17 notes
·
View notes
Text
I choose a simple topic for my 5 minute presentation assignment thinking it'll make the assignment painless. I immediately get frustrated by how little there is to say about it because the topic is simple and straightforward and I feel like I'm not doing good enough research. why am I like this.
#gvhd is so annoyingly straightforward I should've gone with car t regs#except then I'd be complaining about how much I don't like car t cell research and how done I am with t regs#why do i have to do assignments I'm a researcher now don't make me do presentations anymore#AND I have an essay to write and an introduction to my thesis#technically the intro isn't really due yet but my pi will be disappointed more than she already is
0 notes
Text

in the spirit of comic book (medical) science
#arghwrites#came in through the window last night#this is for kaine's ''clone degeneration''#aka gvhd like thymic multiorgan autoimmunity without thymoma — as reed calls it XD#FF end up getting him on multiple patches both because he can't do needles and because he has too many goddamn pills#which for a ''superhero'' is less than ideal#whoops sorry there's a crime but i need to stop and take my pills that stop me from barfing#tbf peter also has pills by this point but they're significantly fewer and if he takes a dose slightly late or early he won't like. die.
1 note
·
View note
Text
#Bone Marrow Transplant#Graft Versus Host Disease (#Types of GVHD#Symptoms of GVHD#kauvery hospital#healthcare#healthy#healthcare blog#healthcare news
0 notes
Text
Acute pancreatitis in Thalassemia post allogeneic stem cell transplant with Cyclosporine-A as a possible etiology: A report of two cases by Narendra Agrawal in International Journal of Clinical Images and Medical Reviews
Abstract
Cyclosporine is an important component of GVHD Prophylaxis in Hematopoietic Stem Cell Transplant (HCT). It has narrow therapeutic index and is known to cause hypertension, electrolyte imbalances, Acute Kidney Injury, etc. High suspicion of these adverse effects helps us in managing them effectively. We report here two cases of pediatric age group who presented with acute pancreatitis post matched sibling HCT for Thalassemia transplant. To our knowledge we could find only 2 case reports of Cyclosporine induced pancreatitis post HCT in literature and none reported post HCT in Thalassemia. Diagnosis of acute pancreatitis especially in pediatric age group can be challenging without high suspicion.The purpose of our report is to highlight the importance of keeping acute pancreatitis in differential of unwell child post HCT in Thalassemia and careful rechallenge of Cyclosporine may be possible with careful monitoring, thereby not compromising on GVHD prophylaxis.
Key-words: Pancreatitis, Cyclosporine, Thalassemia, GVHD prophylaxis
Key Messages: This report highlights the importance of suspecting pancreatitis in a paediatric thalassemia patient post allogeneic stem cell transplant with cyclosporine –A as possible causative factor. CSA reintroduction can be attempted with careful monitoring after recovery.
Introduction
Cyclosporine (CsA) is a cyclic polypeptide immunosuppressant agent. It is produced as a metabolite by the fungus species Beauveria nivea1. CsA has been used extensively for immune suppression in allogeneic hematopoietic cell transplantation (alloHCT) as well as solid organ transplants for prevention and treatment of graft versus host disease (GVHD) and graft rejection1. CsA has a narrow therapeutic index and requires therapeutic dose monitoring. Common adverse effects of CsA include nephrotoxicity, HCT, hypertension, and hypomagnesemia1. Acute Pancreatitis has been reported with the use of CsA in organ transplants2.
With an extensive literature search, we could not find any report of CsA induced acute pancreatitis after alloHCT for thalassemia or other hemoglobinopathies. Here we report two pediatric patients with thalassemia major, of CsA induced acute pancreatitis after HLA matched family donor HCT.
Case History
Case 1, a 2-year-old female child with Thalassemia major, presented on day +66 of HLA matched mother donor alloHCT with a history of constipation, irritable behavior, episodes of crying, decreased oral intake and vomiting of 2 days duration. Abdominal examination was remarkable for mild diffuse tenderness and sluggish bowel sounds. X-ray abdomen was suggestive of dilated colon while an USG of abdomen was suggestive of gaseous bowel distension. Pediatric Surgery review suggested a possibility of subacute intestinal obstruction. The patient was treated conservatively by withholding oral foods and fluids (NPO) and application of bisacodyl suppositories. Constipation resolved but she continued to remain irritable with the persistence of abdominal signs. A possibility of acute pancreatitis was considered and serum amylase and lipase were sent which turned out to be 183 IU/L (normal range 22-80) and 2350 IU/L (normal range 23-300). CT Abdomen was notable for modified CT severity index for acute pancreatitis (CTSI) of 43. A careful review of her drugs and history of illness was carried out. She was not found to be suffering from viral prodrome anytime in the previous month. Her serum calcium and triglyceride levels were normal while PCRs for CMV and EBV were negative. She was receiving CsA along with prophylactic acyclovir, penicillin V and co-trimoxazole. Her plasma CsA trough level was 61 ng/mL on the day of her presentation. A possibility of CsA induced acute pancreatitis was considered4. Naranjo algorithm for causation score was 7 for CsA suggesting probable causation5. Her blood pressure and renal functions were normal. She had no other CsA toxicity. With conservative management her symptoms improved over 1 week, USG done after 1 week was suggestive of resolving pancreatitis with falling levels of serum lipase and amylase. She was shifted to Mycophenolate Mofetil (MMF) for GVHD prophylaxis. On day+100 follow up, her chimerism was maintained at 100% donor, but liver enzymes were raised. After excluding infective and drug-induced hepatitis, a possibility of liver GVHD was considered. A decision to re-challenge with CsA under close monitoring was taken. CsA was re-introduced starting at low doses with monitoring of amylase and lipase levels and close monitoring for clinical signs. She did not have a repeat episode of acute pancreatitis and is currently on tapering immunosuppression on day+260 of follow up.
C ase 2, a 4-year-old female child with thalassemia major presented on day+154 of HLA matched sibling donor alloHCT with a history of abdominal pain, vomiting and poor oral intake of 2 days duration. The patient had no history of fever. On examination, the patient had tachyuration. The patient had no history of fever. On examination, the patient had cardia, normal blood pressure for age, abdominal distention with mild diffuse tenderness. Her USG was suggestive of the bulky pancreas, amylase, and lipase levels were 643 IU/L and 4253 IU/L. The plasma CsA trough level was 252ng/mL. Her chimerism test showed 68% of donor cells. A careful review of her clinical history, lab results, and medications couldn’t find other causes of acute pancreatitis than CsA. Naranjo algorithm causation score was 7 for CsA suggesting probable causation5. There were no other CsA toxicities. CsA was stopped and she improved with conservative management. The patient was started on MMF for GVHD prophylaxis thereafter. She was considered for a re-challenge of CsA especially after our experience of successful re-challenge of CSA in our previous patient. She was restarted on CsA starting from low doses with amylase and lipase monitoring from day +185 onwards. Currently, she is on escalating doses of CsA on day +225 of follow up with donor chimerism improved to 76%.
Discussion
Ito, T. et al showed that intravenous injection of CsA 10 and 20mg/kg body weight (BW) in rats increased the content of pancreatic amylase and protein and decreased the content of pancreatic DNA6. Histologically, intraacinar vacuolization and individual cell necrosis were observed6. CsA induced a significant increase in serum amylase and pancreatic wet weight in a dose-dependent manner6. Qi C et al reported acute pancreatitis in a 16-year-old female patient with acute leukemia on day 24 of alloHCT with CsA or Tigecycline as potential causative agents4. In a case report by Guo R et al from China, CsA induced acute pancreatitis was reported on day+20 of HLA matched alloHCT in a 49-year-old male with AML-M27.
Whether Acute pancreatitis developing in post alloHCT patients with relatively lesser duration of exposure to CsA is idiosyncratic or dose-dependent is yet to be elucidated. Although animal experiment data points towards dose-dependent toxicity, in both our cases acute pancreatitis, developed at acceptable plasma levels, questioning this notion.
Other than that, Post-transplant diabetes mellitus (PTDM) is a complication that takes place after solid organ transplant as well as alloHCTs, with reported incidences ranging from 2 to 53%. Cyclosporine is one of the risk factors for developing PTDM probably due to direct toxic effects on beta cells of the pancreas8.
From this experience, we conclude that studies are needed in the pathogenesis of CsA induced acute pancreatitis in post alloHCT patients. High suspicion of acute pancreatitis should be kept in post alloHCT patients with abdominal signs and symptoms especially in pediatric patients who may not be able to communicate the typical pain history. CsA re-challenge didn’t precipitate pancreatitis in our patients.
Declarations
Funding: Funding information is not applicable to this study.
Conflict of Interest: All authors declare no conflict of interest to declare.
Compliance with Ethical Standards
Ethical Approval Statement: All authors stated that the study has been approved by the appropriate institutional review board and have been performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Acknowledgements
We would like to acknowledge Dr Rayaz Ahmed, Dr Vishvdeep Khushoo and Dr Pallavi Mehta in treatment of the patients. We thank all the members, and staff of Rajiv Gandhi Cancer Institute and Research Centre, India for their contribution in the conduct of the study
For more details: https://ijcimr.org/editorial-board/
#Pancreatitis#Cyclosporine#Thalassemia#GVHD prophylaxis#HCT#nephrotoxicity#hypertension#NPO#PTDM#Narendra Agrawal#ijcimr
0 notes
Text
Graft Versus Host Disease (GvHD) Treatment Market Types Applications Products Share Growth Insights And Forecasts Report 2032

The global Graft Versus Host Disease (GvHD) Treatment Market is expected to secure US$ 5,655.37 Million in 2032 while expanding at a CAGR of 8.3%.
Graft versus Host disease occurs after a stem cell or bone marrow transplant. High dose treatment destroy cancer cells along with that it simultaneously destroys healthy cells. Stem cell and bone marrow transplant treatments are used in reconstructing damaged cells, surrounding cancer tumors.
Normally after high dose treatment, patient receives bone marrow from a donor through drip which resumes production of blood cells. Graft versus Host Disease occurs when certain types of white blood cells. This is caused due to the transplanted cells (graft) see recipient’s body (host) as exotic, thus transplanted cells attack the host body.
It is tough to diagnose who might develop GvHD after a transplant. Mild form of GvHD is observed in few cases. While in certain cases GvHD may be fatal. GvHD do not occur when recipient receives their own cells through autologous transplant. Prior to a transplant, cells from possible donors are screened to realize how strictly they match the recipient. Chances of GvHD are reduced, or symptoms will be milder, when the match is close.
There are two forms of GvHD:
Acute graft versus host disease (aGvHD).
Chronic graft versus host disease (cGvHD).
Graft Versus Host Disease (GvHD) Treatment Market: Drivers and Restraints
Presently, graft versus host disease (GvHD) market is driven by increase in number of incidence and prevalence of cancer patients which are treated by chemotherapy treatment. Graft versus host disease (GvHD) global market is also fueled by increase in number of bone marrow transplants been carried around the globe to treat specific types of cancers.
Increase in allogeneic hematopoietic stem cell transplant will play key role in global market for graft versus host disease (GvHD). However, cost linked with recent clinical trials and authorizations would acts as a major restraint for graft versus host disease (GvHD) global market.
Graft versus Host Disease (GvHD) Treatment Market: Overview
The global market graft versus host disease (GvHD) treatment is expected to register a healthy CAGR during the forecast period. Innovative development of novel technologies, and increase in the number of cancer patients seeking for chemotherapy treatment is expected to drive the growth of graft versus host disease (GvHD) treatment market in the forecast period (2016-2026).
Graft versus Host Disease (GvHD) Treatment Market: Key Players
Some of the key participating global players in graft versus host disease (GvHD) treatment global market are Sanofi, Novartis AG, Neovii Biotech GmbH, Merck & Co., Astellas Pharma Inc., Soligenix, Inc., Mesoblast Ltd and others.
The research report presents a comprehensive assessment of the market and contains thoughtful insights, facts, historical data, and statistically supported and industry-validated market data. It also contains projections using a suitable set of assumptions and methodologies. The research report provides analysis and information according to categories such as market segments, geographies, types, technology and applications.
Key Segments Profiled In The Global Graft Versus Host Disease (Gvhd) Treatment Market
Graft Versus Host Disease (GvHD) Treatment Market by Product:
Monoclonal antibodies Graft Versus Host Disease (GvHD) Treatment
mTOR inhibitors Graft Versus Host Disease (GvHD) Treatment
Tyrosine kinase inhibitors Graft Versus Host Disease (GvHD) Treatment
Thalidomide Graft Versus Host Disease (GvHD) Treatment
Etanercept Graft Versus Host Disease (GvHD) Treatment
Graft Versus Host Disease (GvHD) Treatment Market by Disease:
Acute Graft Versus Host Disease (a(GvHD))
Chronic Graft Versus Host Disease (c(GvHD))
Graft Versus Host Disease (GvHD) Treatment Market by Region:
North America Graft Versus Host Disease (GvHD) Treatment Market
Latin America Graft Versus Host Disease (GvHD) Treatment Market
Europe Graft Versus Host Disease (GvHD) Treatment Market
Asia Pacific Graft Versus Host Disease (GvHD) Treatment Market
Middle East & Africa Graft Versus Host Disease (GvHD) Treatment Market
#Graft Versus Host Disease (GvHD) Treatment Market Market#Graft Versus Host Disease (GvHD) Treatment Market Market Size#Graft Versus Host Disease (GvHD) Treatment Market Market Growth
0 notes
Text
As per the newly published report by nova one advisor, the global Acute Graft Versus Host Disease [GvHD] Treatment market gathered revenue around USD 263.9 Million in 2020 and market is set to grow USD 632.9 Million by the end of 2027 and is estimated to expand at a modest CAGR of 8.9% during the prediction period 2021 to 2027.
0 notes
Text
The global acute graft versus host disease (GvHD) treatment market was valued at US$ 263 Mn in 2021 and is projected to expand at a CAGR of 8.6% from 2022 to 2030
0 notes
Note
So what you want Kate to not get chemotherapy so that she gets even more worse and more unwell? Who even thinks like that and William doesn’t smoke

First off, it's well known that William smokes. Just because he hides it better than Harry doesn't mean he doesn't do it. He clearly has smoker skin. That's why his skin looks so terrible & dry. So dry that soon we might be able to grate cheese on it.
"You want Kate to not get chemotherapy so that she gets even more worse and more unwell?"
Your ignorance is clearly showing.
This is how people die from cancer:
Catabolism: the body breaks down on a cellular level; substances released by tumor cells are strong anorexics.
Secondary infection due to immune system suppression.
Blockage of vital structures: trachea/esophagus, superior vena cava (SVC) syndrome, impacts to the spinal cord, pericardial effusion, pleural effusion, etc.
Side effects of medication/treatment: immune suppression, pulmonary fibrosis, Graft-versus-Host-Disease (GvHD), etc.
You do not die from cancer just because you have "cancer."
I wrote a long post yesterday differentiating that different people have different physiology. Just because you have "cancer" does not mean that it poses a threat to your life or health. Plenty of people have "cancer" that does not progress at all or affect them in any way. Just because you have "cancer present" does not mean it will affect your life or health in any significant way.
The situation is really like the anon said:
"Catherine has a much more serious cancer than they are letting on, hence, the decision to have chemo is not even a discussion point,"
"she’s not having chemo and there’s another reason why she’s missing in action,"
"she and William are panicking and she’s receiving chemo regardless"
My bets are on numbers two or three.
Kensington Palace is clearly lying. Can't wait for it to be revealed! KP's strategy before Kate's cancer announcement was to release the news that her medical records had been breached and paint Kate as a victim. After the cancer announcement, it was those pesky conspiracy theorists and the axis of evil who was to blame for Kate's reputation being slagged around the world, not the utter incompetence of William and KP.
Let's not forget that William is an emotionally damaged, thin skinned, control freak with a privacy fetish.
Let's also not forget that next Monday, 01 April 2024, begins a new fiscal year for the BRF.
#ask#hate mail#medicine#smoking#William The Prince of OWN GOALS#William The Terrible#William The Weak#William The Prince of Wales#prince william#Prince & Princess OWN GOALS#kate middleton#Catherine The Princess of Wales#kensington palace#palace officials#lies lies lies#pr games#strategery#Wales fandom ARMAGEDDON
14 notes
·
View notes
Text
No keeping this girl down!
Today Leah is medically more or less in the same place as yesterday.
The samples that were taken from her lungs on Thursday and were sent to the laboratory haven’t grown anything, so this confuses the PCP diagnosis a little bit and has led some of the docs to suspect that Leah may have pneumonitis, another complication of transplant.
It’s not one I fully understand but I think it could be a…
View On WordPress
0 notes
Text
0 notes
Text
Been feeling real Sad lately because I feel like Pip doesn't want to play with me. Then tonight I asked her to work and she was so happy! And we did a few things.
THE REST OF THIS IS JUST MOMGUILT(TM)
We've falling down on conditioning since her season and my being overwhelmed at work and it's really showing in some conditioning loss. Her bad appetite meant I was holding out on training goodies until after dinner, which meant sometimes we never got to train at all...
I'm trying to remember that she's also been ILL and we've been doing the vet weekly for the past two months. Only this past week were her liver values normal again. We still don't know what the problem is. She may have a liver shunt. May require intervention or may not. We just have to see. At least the supportive meds are helping, and it doesn't seem to be GvHD.
All her hair means she tuckers out fast in the increasingly heat and we don't get much walking in since she's superstitious about our neighborhood. So I'm feeling terrible that I squandered her conditioning that we worked hard on. And she seems less peppy than she was earlier in the year, which makes me panic that something is wrong. M keeps telling me it's just the heat (both temperature and hormonal), and that makes sense, but I spiral ANYWAY!!!
I started a new, easier job though and I'm already doing better. I was so exhausted and wrung out all the time. Insane how my mental capacity has increased already. Now I can spend it on conditioning my hairy, lazy dog...
18 notes
·
View notes
Last Seen Blogs

a-fucking-armadillo
a fucking armadillo

larimarz
yeah i post cringe what about it

magaram0506-blog
Без названия

sono-michii
Stars Fall at Midnight

fqirytail
fairy icon