#Large lingual muscle
Text
Macroglossia Or Long Tounge: Its Important Causes, Effects, and Management
IntroductionAnatomy and BasicsThe Tongue’s Vital RoleDefining MacroglossiaCauses and VariationsEffects on Daily LifeDiagnosis and ManagementMedical EvaluationTreatment ApproachesPsychosocial Impact and SupportConclusionMacroglossia Or Long Tounge: Its Important Causes, Effects, and Management (FAQs)Is macroglossia a rare condition?Can macroglossia be treated without surgery?Is macroglossia…
View On WordPress
#Abnormal tongue growth#abnormally large tongue#acute macroglossia#amyloidosis on tongue#causes of macroglossia in adults#congenital macroglossia#Congenital tongue elongation#Enlarged lingual organ#Extended tongue#Genetic factors in long tongue#hyperglossia causes#Large lingual muscle#Lingual flexibility#Long tongue genetics#Long tongue implications#Long tounge#Long tounge causes#Long tounge treatment#macroglossia#macroglossia amyloidosis#macroglossia and hypothyroidism#macroglossia causes#macroglossia causes in adults#macroglossia diagnosis#macroglossia differential diagnosis#macroglossia down syndrome#macroglossia hypothyroidism#macroglossia in adults#macroglossia newborn#macroglossia speech therapy
0 notes
Note
Hey, can I get song #20 Nobody by Keith Sweat with my baby, Chosoito and sprinkle sprinkle a wee bit smut in all the fluff, please and thank you! 😊 😚😚😚☺️
Buenas Días chikita!!! I would ofc love to write a little spice for you with your #20!!! I hope you like it!!
I really love this song and I think he would be overly romantic and worship you.
**If you want to play this HC ask Game find the list here**
Chosito night in:

20. Nobody (feat. Athena Cage) - Keith Sweat, Athena Cage (NSFW...Cunnilingus...Choso the Compersion *Gets off on you getting off*, Acts of Service/Touch)
At the edge of your bed, surrounded by the perfectly propped pillows Choso had put behind you, you were on display for him as he was on his knees between your thick thighs like a postulant seeking the grace of his alter.
Choso with his thick midnight-carbon hair down around his shoulders you couldn't help reach out and caress his swollen bottom lip. Slick from his previous feast you watched the way he took in your manicured thumb and sucked on it making his endless dark eyes close and a deep groan leave his throat.
When he opened his eyes again, his button down shirt open revealing his carved chest and torso, his large perfectly calloused palms followed the curved of your calf up to your thighs. He kissed the inside of you thigh following his path to your cum glossed puffy sex. He moaned as you reached down to spread your pussy lips for him framed by your deep purple nails.
He practically felt his straining dick leak into his pants he could live between your thighs for eternity. He loved that when he took his strong lingual muscle and traced your opening teasing a taste of your essence he watched the way your head fell back and the way your nipples pearled as you called his name so sultry.
He arms constricted around your thighs and pulled your hips closer to the edge of the bed. You called out his name again, like you were chanting a prayer, as your hands found purchase in his thick tresses. You felt every sloppy kiss as he made out with your swollen, overstimulated, center. With him sucking and swirling, putting the right amount of pressure on your pulsing clit, you could hear him whimper as you began to buck your hips hitting his nose. He pulled you in closer, so close, you felt the grip on your thighs tighten.
He was hungry and he didn't know if he would ever get enough. As he tasted you and worshiped you he was showing you through his acts of touch and service that you were his only one. He showed you that he would go no where else or stray from his altar...Chosito would know nothing but you and the way you were the only one in the universe to satiate his insatiable hunger.
#husbando#jujutsu kaisen#jjk smut#jjk choso#chosito#choso kamo#choso headcanons#choso x reader#choso smut#Chositio eating Kitty
25 notes
·
View notes
Text
The mouth
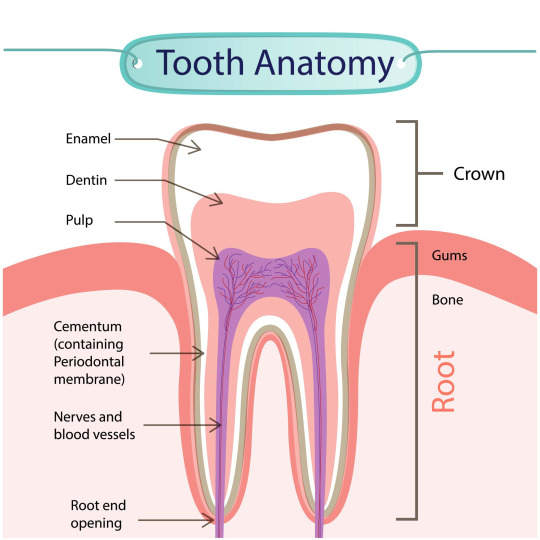
Teeth
Although they look like simple pieces of bone, your teeth actually have an interesting system just under their surface. Understanding the various parts and functions of your teeth allows you to take better care of them and avoid things like cavities, gum disease, and damage.
When you smile, the visible, outer-portion of the tooth you see is called the crown. Most people are familiar with the crown and simply refer to it as their “tooth”; however the crown is only one part of your tooth’s anatomy. The crown is only the part of the tooth that emerges above the gumline. Its shape determines the function of that particular tooth. For instance, incisors, molars, and canines all have different functions based upon their external shape.
Another important part of your tooth’s anatomy is the gum line. The gum line is simply the area where the tooth meets the gum and it distinguishes the crown from the root. The area where the crown and the root meet on the gum line is called the neck of your tooth. It is important to note this area as it becomes a common site for plaque build-up which can cause gum disease and gingivitis.
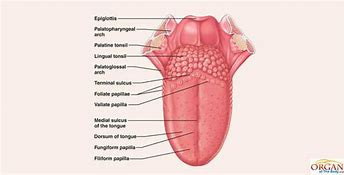
The Tongue
Tongue muscles are the only muscles in the body that work independent to the skeleton. The tongue is a mobile, muscular organ that lies within the mouth and partly extends into the upper throat. The tongue's anatomy is complex it involves interlacing muscles, nerves, and a blood supply. When looking at the tongue's surface, it is possible to divide the tongue into five general parts. This is important because different parts of the tongue may be supported by distinct nerves and blood vessels. The lingual frenulum is a large midline fold of mucosa that passes from the tongue side of the gums (or gingiva) to the lower surface of the tongue. The frenulum connects the tongue to the floor of the mouth while allowing the tip to move freely. It is notable that the submandibular salivary gland (under your jaw) has a duct that opens beneath the tongue, passing saliva into the mouth here.
The tongue actively moves the food within the mouth, positioning it for further degradation by the teeth. The food is mixed with saliva, ultimately becoming a manageable portion called a bolus that may be moved into the pharynx before being swallowed and passing via the oesophagus into the stomach. The tongue may also help with oral cleansing, keeping food from prolonged contact with the teeth. The tongue helps to identify what might be safe and palatable to eat, with the sense of taste as detected by the taste buds.
The tongue is also the main contributor to speech. It is not possible to form words and speak without the proper positioning of the tongue. This is dependent on muscles that alter the shape and position of the tongue. The tongue anatomy makes it possible for you to articulate sounds appropriately. Dysfunction of the tongue may lead to a serious speech impediment.
And for breathing If the tongue sits too far back within the throat, it may affect breathing. This is more likely to occur when mouth breathing is present. With normal nasal breathing, the mouth is kept closed, and the lower jaw will be held in a more forward position as the teeth come together. This reduces the potential for the tongue to obstruct the airway. In sleep, the shift of the tongue that happens with mouth breathing may cause problems including snoring and obstructive sleep apnoea. Weight gain may increase the size of the tongue and make this worse.

Blog (2018) The anatomy of your teeth. https://appletreedentistry.net/the-anatomy-of-your-teeth/.
0 notes
Photo

Here’s what you need to know about ALF and his digestive system: He’s an omnivore.
- he’s got a big old, elongated mouth with a some teeth that protrude, similar to that which carnivores use to break down their protein, but not quite as sharp. His mouth also contains the enzyme amylase to start to break down starches, and lingual lipase to break down some lipids
- an esophagus that connects to his first of 8 stomachs, where the food travels down due to peristalsis, or just the squeezing of muscles. Thank goodness his heart is in his ear so there’s enough room for all of those stomachs. (look! he’s pointing to his heart!)
-his eight stomachs are interconnected by a series of valves, allowing food to pass through each of the somewhat weak stomachs to break down his meals. Compared to us humans, the enzymes in ALF’s stomach, like pepsin, are not as strong and less pepsin overall is secreted by the stomach cells. This is the enzyme responsible for the breakdown of the protein that your Melmacian will consume.
-In the small intestine, there’s some major breakdown and nutrient absorption going on. Enzymes mostly from the pancreas allow this to happen: trypsin and chymotrypsin continue protein digestion that started in the stomach, pancreatic lipase, colipase, and bile salts from the gallbladder break down fats, and some pancreatic amylase is present to break down carbohydrates. All of these nutrients are absorbed here, along with water.
-the Melmacian large intestine also reabsorbs water and salts, passing the final waste product through the rectum and out of the anus
2 notes
·
View notes
Text
Juniper Publishers-Open Access Journal of Head Neck & Spine Surgery

Parapharyngeal Space Tumors - "A Surgical Challenge"
Authored by Gauri Kokane
Abstract
Parapharyngeal space tumors are rare entity. Overall incidence is less than 0.5%. These tumors are divided into prestyloid and post styloid tumors. Salivary gland neoplasma are common in prestyloid compartment whereas Neurogenic tumors in post styloid compartment. As these tumors are painless and does not express signs and symptoms at early stage, diagnosis of such tumors needs critical evaluation. Anatomic complexity of PPS makes surgical excision more challenging. We have reported 4 cases of parapharyngeal space tumors over a period of 10 years.
Keywords: Parapharyngeal; Schwannoma; Paraganglioma; Neurogenic; Transcervical
Background
Parapharyngeal space is an inverted pyramid from base of the skull to hyoid bone. It is bounded medially by pharynx, anteriorly pterygomandibular raphe, posterolaterally carotid sheath, posteromedially retropharyngeal space, laterally above the level of mandible it is bounded by ramus of mandible, deep lobe of parotid and medial pterygoid muscle, below the level of mandible; it is bounded by posterior belly of diagastric muscle. It is divided into prestyloid and poststyloid compartment by aponeurosis of zuckercandle and testus [1]. 80% of the PPS tumours are benign while 20% are malignant [2]. Incidence of parapharyngeal space tumors is less than 0.5% [3]. Majority of the tumours are slow growing, painless and progressive in nature. If untreated might result in severe life threatening complications like airway obstruction and cranial nerve deficit resulting in significant morbidity. Systematic diagnostic evaluation plays an important role in diagnosis. Surgical excision has Pivotal significance in PPS tumors. We have identified and reported four cases of parapharyngeal space tumors at our centre over a period of 10 years.
Case Description
Case 1
29 year old male presented with complain of painless lateral neck swelling since 3 months. There was no history of dysphagia, Hoarseness of voice. There was no cranial nerve involvement. FNAC showed spindle cell tumor. On MRI there was 50x 37mm well circumscribed lesion over left side of neck suggestive of schwannoma. Surgical Excision of the tumor was done using transcervical approach (Figure 1). There was no intra-operative complication. ICA, ECA, Vagus nerve and IJV were identified and preserved. Tumor was excised completely (Figure 2). Post operatively there was reduction in high pitch sounds. Origin of tumor from vagus nerve was confirmed intra-operatively. Microscopic picture revealed presence of mixed Antoni A and Antoni B cells concluding to the microscopic features of schwannoma.
Case 2
34 year old female presented with painless swelling over right side of neck. CT neck showed 64x46x35mm lesion in the carotid space compressing right IJV and displacing it anterolaterally (Figure 3). Superiorly it was extended up to carotid canal. Differential diagnosis includes paraganglioma in view of intense enhancement of lesion and vagal schwannoma in view of displacement pattern of vessel. FNAC was suggestive of spindle cell tumor. Intraoperatively there was rupture of internal carotid artery which was repaired with 6-0 ethilon, vagus nerve was also sacrificed due to the severe adherence of the tumor to the nerve.
Case 3
24 year old female complains of painless progressive swelling with dysphagia to solids and liquids since 4yrs. CT scan showed heterogeneously enhancing lesion 85x31mm with retrosternal extension displacing major vessels laterally. Intraoperatively transcervical incision was taken and tumor was dissected to free it from the major vessels and nerves and it was removed in to (Figure 4).
Case 4
40 year female patient presented with swelling of left submandibular region since 1 month (Figure 5). FNAC showed spindle cell tumor, USG showed 41x39mm Heterogenous mass and left submandibular gland. CT Scan Showed 4.5cm enhancing well circumscribed lesion, left submandibular gland and another 1.3x1cm lesion adjacent to it. No dysphagia or hoarseness of voice, intra-operatively Hypoglossal nerve was sacrificed. Lingual nerve was identified and preserved. Histopathology report showed neurogenic tumour i.e. schwannoma.
Discussion
Para-pharyngeal space (PPS) tumors are very rare. We have identified 4 patients after reviewing 10 years retrospective data of all head and neck tumors presented at Manavata curie cancer centre Nashik. Incidence of parapharyngeal space tumors at our institute was 0.004%. Overall incidence of these tumors is less than 0.5%. These tumors are slow growing, painless and patients express at later stage when the size become considerably large. Usually patients are asymptomatic but may exhibit dysphagia or hoarseness of voice. In our 4 patients only one patient had dysphagia to solids and liquids rest of the patients were asymptomatic [4,5]. 80% of the tumors arising in this region are benign [2]. Pleomorphic adenoma is the most common tumor of prestyloid compartment where poststyloid tumors are mostly neurogenic like shwannoma, paraganglioma, neurofibroma, hemangiomas etc. Chordomas, lypomas, lymphomas, chemodectomas, rhabdomyomas, chondrosarcomas, desmoid tumours, ameloblastomas, amyloid tumours, ectomesenchymomas, fibrosarcomas and plasmocytomas have also been reported [2].
Diagnosis of these tumors is difficult as they are asymptomatic. Diagnostic evaluation constitutes CT scan and MRI to clearly define the extent of the tumor mass. Arteriography also plays a significant role to assess vascular compression. In our identified cases CT scan was performed in 3 cases and MRI in one case. MRI has been shown to gives better dimensions of the parapharyngeal space tumors. Advantage of MRI is, it distinguishes tumor from Muscular structures and give better dimentions of the tumor [6].
Arteriography was not performed in any of our cases. Once the nonvascular nature of tumor is confirmed by radio-imaging, FNAC can be performed for definitive diagnosis. FNAC is accurate in 90-95% of the cases and helps in surgical planning [7]. Limited role is explained in post styloid compartment. We performed FNAC in all our patients and it was conclusive [8,9].
Schwannoma may arise at any age but in our institute patient's age ranged from 3rd to 4th decades of life. There is no gender predilection. Schwannoma may be of two types histologically consisting of either Antoni A cells or Antoni B cells. We had two patients with Antoni A cells and other one was of mixed variety [10]. Paragangliomas are tumors of autonomic nervous system. Head and neck paragangliomas are unique in its variety as they don't release catecholamines. Incidence of paraganglioma is 1 in 30,000 cases [11]. Histopathological picture shows two types of cells; Chief cells and sustantecular cells. One of our patient's histological features were identical to it.
Surgical management of parapharyngeal space tumors is very challenging owing to anatomic complexity ofthe space and vicinity of the tumor with major neurovascular structures. There are 7 different approaches described for PFS tumors. Transcervical, Transcervical- transparotid, Transoral-transcervical approach, Extended approach, Transcervical-mandibulotomy aaproach, Transcervical-transmastoid approach have been explained [12]. 4cm is the limit for radical tumour excision with the transcervical approach without mandibulotomy. For a safe and radical resection of tumours > 4cm the “swing” approach or the transmandibular with a double osteotomy is required [2]. We used transcervical approach without mandibulotomy in all cases. Accesiblity was compromised in larger tumors but we could enucleate entire tumor without much difficulty. ICA was ruptured in one case but it was managed. Minimal accessibility may be a compromise but there is less surgical morbidity and post op recovery is faster in our experience.
Complications after surgical management are unavoidable. Expected complications are due to sacrifice of cranial nerves. There may be unexpected neurological complications in spite of preservation of nerves like first bite syndrome, Trismus, facial nerve weakness, orocutaneous fistula, Seroma. We experienced loss of high pitched sounds in two of our patients and there was hypoglossal nerve palsy as hypoglossal nerve was sacrificed in one case.
Conclusion
CT scan or MRI should always be performed in order to distinguish prestyloid from poststyloid lesions and assessment of the extension of the tumour and its relationship with adjacent structures. Trans-cervical approach is safe and should be the first choice for large tumors; other approaches are reserved for selected cases.
Clinical Significance
These are painless slow growing non malignant tumors with very less incidence of recurrance. Management of PPS tumors is challenging for surgeons. Neurological and Surgical complications should always be explained to patients preoperatively. Preoperative assessment and careful surgical manipulation are of utmost importance.
For more articles in Open access Journal of Head Neck & Spine Surgery | Juniper Publishers please click on: https://juniperpublishers.com/jhnss/index.php
0 notes
Photo

congratulations logan, capricorn is now luca yamada with the faceclaim ryan potter !
Character Sign: Capricorn
Character name: Luca Yamada
Birthday: January 19th
Sexuality: Fluid
Gender: Cis-Male
Moon Sign: Aquarius
Faceclaim: Ryan Potter
Power:
MATTER ABSORPTION; The user can absorb matter, while removing it from the source, into their body and use it in various ways, gaining some form of advantage, either by enhancing themselves, gaining the drained power, using it as power source etc., either temporarily or permanently.
Luca’s ability is complete earth based, meaning he can’t absorb matter that isn’t naturally made or largely complied of earth base compotents. Items like clay, stone, metal, sand, and even gemstone can be taken from and used. How it’s used? Think of it like a layer of armor, in some ways, as Luca can absorb the chemical or atomic makeup of a substance—it’s matter—then reincorporate that matter into his own genetic makeup. Basically his skin and to some point his muscles or organs completely shift into the matter he absorbs. Whether that’s taking in a concrete wall creating his arms to be as heavy and dense as stone or absorbing metal railing, to coat his knuckles to be as strong as steel. His ability doesn’t give him abnormal strength, endurance, or durability—but depending on the composition of the matter he takes does change him. Imagine you punching someone’s face and then imagine punch a stone face…the matter is what makes him “stronger” but he’s still human, and has his limitations.
LIMITATIONS; Firstly proximity is needed, via touch. Luca can not mentally or psychically absrob matter. Like the element of earth it is person and physical. Luca’s limitations grows via science. Magic might be able to bend many rules in the world but never can absolutely break them. The porpotion to which the material Luca is absorbing is equally porpotion to how much he can collectively transform his body. If he absorbs a pebble or a stone the size of a brick, he can only spread that to about the size of his forearm or less… Walls, metal railings, or solid desk leave him more than enough material he let his body manifest into the element he’s absorbing. Secondly, as his powers grow stronger, Luca can have a slight chance of destroying the material he’s syphoning. Taking an objects matter is one thing, but if he takes too much he can destroy the integrity of it. As most stone objects, like rocks or bricks, have chances of disintegrating. So far most walls or metal objects don’t fully break down but might be structially more weak or it way rust. Lastly his limitations are that he’s still human, not inhuman. Luca can still feel the weight of his ability, almost as if he’s lifting weights. He must train himself physically and must work hard to withstand the physical demands of his ability. He might be able to take more hits, be denser or stronger, but that all fades once the matter does too.
SUB POWER, FERROKINESIS; Shape and manipulate metal, a solid material (an element, compound, or alloy) that is typically hard, shiny, and features good electrical and thermal conductivity. Metals are generally malleable—they can be hammered or pressed permanently out of shape without breaking or cracking—as well as fusible (able to be fused or melted) and ductile (able to be drawn out into a thin wire
Since Luca has absorbed large amounts of metals ranging from steel, iron, alluminum, and copper—when his power boost came into effect, his body developed what they know best. Metals. Luca is able to shape or manipulate metals, never create them from thin air. His ability is also weaker than if it was a main gift, as he often can only dismantle, twist, or destroy metal than truly shape it to much. His ability is normally heightened if he has recently absorbed metals or alloys.
LIMITATION; Luca’s limitations are practice and understanding. Chemistry was never Luca’s first choise, so understanding the softness of metals and their strengths and weaknesses have been a learning curve. If he tries to manipulate or form metal too sharply or outside of it’s scientific properties it can shatter or grow weaker than he’d want. As a weaker manipulation, he isn’t able to mess with heavy ammounts or large pieces of metals, much like his brain is too weak to mentally lift such a mass. Emotions can help him push pass that but as of now, he is limited to the largest thig he’s manipulating being a street lamp.
What do they study: Criminology
Biography:
self-con·trol
You were precision in perfection, a graceful force biding your time. As a child your chaos was order; neatly stacking your toys in the spaces they held, to coloring in the lines—dazzling your parent’s with your “skills”. However those skills or talents they’d dote on you for, felt nothing but natural. You like having a plan, a goal to reap pride and glory from. Your bones were etched with method and reason, your muscles woven with patience that rivaled most your age; truly you aged faster than others. By ten your ballet shoes would be trade for kickboxing ones—as the control that ballet offered grew boring. The older you got, that graceful force churned and brewed needing an outlet that wasn’t just lines and beauty. No, your hands ached with a soreness you indulged in. You were learning to become a soldier of your own pursuits.
re·spon·si·ble
Time moved on and your maturity produced your most remarkable trait. Your sense of duty. Martial arts only were steps to your goal, learning to protect yourself but a seed of virtue would bloom into protecting others. You, like all sixteen year olds, played your hand against Fate—tempting the laws of the world and breaking what you could, yet you never treaded too far across the line. You had patience for the things that so many around you eagerly wanted. You were a catious driver, a conservative when you partied, and above all else a studious boy. Your parents goals for you were lofty, but you worked towards them. Your dreams would stay on the back burner, as they would speak of being a doctor or becoming a lawyer…you held your tongue. Being dutiful to them meant everything, but you wanted nothing more than to be the opposite. For your heart was that of a lion, big and bold, beating to a rhythm of one thing; to become an officer.
pes·si·mis·tic
Graduation had came, you walked the stage with your canary colored sash, being first and the best among your peers. However you found a part of you that you never expected. Doubt and fear, a trait you fought hard against with grit and horns. You pushed past a lot; your sexuality, your parents plan for you, physical struggles, test, college acceptances…etc. You should feel the weight you are feeling before you fly off to Durham. You’ve made it, you are pursuing your dreams, you are free from your past—yet with your future open to so much your doubt festers a colder side of you. Judgement and sharp words become your mask you slip on with ease, while your eyes hide a mind that is softer than you know. You never forgot your virtue, to uphold and protect the law and it’s people, yet you forgot how to be yourself. More comfortable to be hardhead than vunerable.
stub·born
It’s been years and your life was on a track to success; everything you’ve wanted. However Fate is a fickle bitch, and you’ve found yourself butting heads and grinding your teeth for over a year now. Your life has shifted, to a plane or reality that has no control or understanding. That irks you. Your dreams are being put on pause, your finish line was so close but you and eleven others are being hijacked to something else. Part of you wants to run, to fight another day, to return to your life…yet deeper than that, a part of you that wants to serve and to be apart of something bigger keeps you there. Even if you rather not corroborate and feeling like you are being dragged along instead of leading it. You are here, you are now a witch, you are apart of something larger than the law.
Patrouns: Luca’s patronus would be that of a Heron, white with black tipped wings. Herons represent wild determination and inteligence. The grace of these birds are known for their adaptablity and diversity, since they tread between three elements—that of water, earth, and air. They are crafty creatures, fidning new ways to hunt and survive which for me describes Luca. His whole life has been polishing himself to be better, pressure and focus he puts on himself to hopefully be able to withstand it and become a diamond in the end. Not to mention his mother has a traditional Japanese painting that has a Heron in it; which Luca grew up loving and appreciating more and more.
Five interesting facts about your character:
Luca is tri-lingual knowning Japanese, English, and French. Most people find it surprising that he knows French as he’s American and attending a British school but his aunt is from Bordeuax, France—which he visited often as a child.
Luca is trained in martial arts, almost 11 years in Judo and Taekwondo. He doesn’t brag about how good he is, saying he does it to stay in shape and is just a agression reliever but really he is good. At seventeen he was nationally ranked in the top five, and a small ranking around the world. His coach thought he could work into trying out for the Olympics but Luca was more focus on college to do that.
Is secretly an HGTV lover and is a big fan of Property Brothers. He just loves watching people decorate and creating a space, which reflects as his apartment is very true to him and his aestehtic.
Most people are shocked to learn that Luca hates sushi, even most fish. His mother being more dissapointed about that, but still loves other Japanese dishes and is a bigger fan of rolled omlettes than anything. He still fakes liking it when his dates taking him to sushi places, just to be polite.
Luca owns a pet Husky named Opus, that is just 3 years old. The little guy (who isn’t that small anymore) is Luca’s pride and joy. They two are a perfect match between master and friend, as Opus is as loyal and trained as Luca is particular and ridged. He often shows Opus off by letting him perform tricks like getting him a soda or letting him open his bedroom dorm for him.
Character Quote: “Just because you are soft doesn’t mean you are not a force. Honey and wildfire are both the color gold.”
WRITING SAMPLE
Have you ever have déjà vu? That overwhelming feeling of familiarity; well think of that times ten and add a wicked head high to it and you can imagine Luca’s reaction to watching the scene in front of him ‘return’ to normal. His eyes flickered images of predictions, rapidly fliping ontop of one another like a frame by frame photo—like if stop animation had become his state. He watched a women that was about to drop her bag, drop it four different ways, each trailing like a streak of light with how the apples would fall (which was 80% more likely to fall over into the road than not). His brain felt short circuited, shaking his head. Each person or thing, whatever was in movement, spliced into several things…several decisions being produced. Watching birds fly to three different points on a tree, to seeing a car stop infront of an oblivious teen girl to then watching the chances of it hitting her too all in the matter of moments.
He moved out from the street and into a little vintage shop, hoping to gain clarity and solitude for a moment. His head felt less dizzy after he rubbed his eyes a few times, wondering if he was drugged or not. It wasn’t until the clerk asked him if he needed help, which he swiftly dismissed with a shake of his head and off to a rack to breath. “What the fuck?” he thought, before wondering what had happened. He’d spend several hours after that wondering more and more, but simultaneously worried about why it felt so comfortable too. It didn’t feel like a drug, like a blanket you borrowed from a friend to use—it felt apart of him, like he spend days and weeks making a blanket only to use it intimately.
ANYTHING ELSE?
Favorite colour is probably slate but recently I’ve been digging forest green a ton.
Also more so I’ve missed you all and this RP a ton, and stoked that I have the time now to devote to it than I did last summer. I have my own computer, myown place, and a better work schedule (even if I’m still gonna travel more and camp more)
4 notes
·
View notes
Note
idk how your req work exactly but sukuna x bottom ftm reader? <3
Hello Nony!!!
This is just fine! I hope you like it and have fun!!!
NSFW TW: ftm Bottom reader, Degradation, anal fingering, Edging, overstimulation, Anal orgasm, Double Stuff, cursed dicks, tummy mouth, anal/pussy eating, multiple hands, pussy slaps, squirting, frontal denial…yeah

“AHH-HAAHH, oh fuuuck!”
The feel of his chest against your back while the monstrous, powerful, tongue lapped up your dripping cunt. You arched your slick skin against the lingual muscle shuddering at the way it began to open you up and plunge in. Squealing and barely able to keep still you felt him move a thick hand to your throbbing clit and screamed when a small mouth appeared on his palm and attached itself to you sucking on your swollen bundle of nerves.
“Such a filthy fucking slut for me, aren’t you boy?”
He began to chuckle darkly into your ear as he groaned when he felt the aching tips of uncut dicks brush between the hot juncture of your meaty thighs. He wanted nothing more than to devour you, his own naughty boy. You felt him rut against you, his tummy mouth sending you closer to oblivion while his hand suckled and played with you, you were so fucking close and felt yourself claw into the floor below.
“P-Please!! R-Ryo!!”
Whining like the filthy whore you are you weren’t expecting the sensation to stop all of a sudden. Your orgasm was right there, he’d been edging you for hours, you were desperate. It was the sudden slap on your swollen pussy that made your screams echo. He grabbed your neck and arched you against him more as his other hand slapped you again making the tears in your eyes roll down your now pinched cheeks.
“I don’t think I fuckin heard you right, boy.”
Slap-Slap-Slap-SLAP
You felt his hot breath against your face as the tongue from his mouth came out to collect and trace the paths of your hot tears. His eyes rolled back into his skull and a deep growl echoed into the atmosphere. Sitting back upon his legs he traced your body with the palm of one of his many hands and smiled wickedly.
“I think I’m going to deny your sopping cunt today boy and stretch your ass out.”
You reveled in the way his calloused palm splayed across your back side before he wound up and slapped your ass making the meat jiggle like sin. He chuckled darkly again watching the way your spine seems to snap back. You couldn only push your ass back against him feeling the girth of his dicks pulsing against you.
“P-Please…S-Sir!!”
Large hands gripped your waist as you felt him pull you back and push you down more at the same time presenting your sweet puckering pink hole to him.
“I will not put it inside that tight cunt. I’m going rearrange your nasty guts, boy.”
Again you moaned like a whore in church when you felt the moist hot stripe from his tummy mouth over your tight hole. Pushing against it wanting to feel some friction on your clit, anything for the release, you cried more wanting to be filled. Just when you thought he was going to take pity on you it was the slow plunge of his thick digit to open you up in your ass that gave you another degree of hunger.
Tummy roiling, spine tightening, you felt him plunge in and out until another thick digit entered to begin playing with your searing insides. You began to clench down, the lack of being filled in your cunt made your slick desire coat the inside of your thighs. You practically purred and wanted to be filled. You finally started begging him.
“P-PLEASE SIR FUCK ME PLEASE!”
It was his dark laugh while he took pleasure in your begging. He slipped a third digit inside of your hole sending you over the edge as you clamped down and screamed with the earth shattering release. You felt white hot flash of pleasure and the warm sensation as you squirted coating his hand.
You slumped forward catching your breath when you felt him lift your hips and he lined himself up as his fingers left your insides. It was the sweet pressure as one thick, throbbing erection slid past your stretched rim. You moaned from deep within as he thrust once bottoming out. Bending over you a set of hands held you down.
“I’m going to stuff both my cocks inside of you, you better hold on for your measly life, boy.”
You gripped the sheets and let your eyes roll back as he pulled out and this time slowly buried both of his cursed dicks in your abused puffy hole.
#2d men#Aztec asks#mdni#sukuna smut#sukuna x ftm trans#sukuna drabble#jjk sukuna#jujutsu kaisen sukuna#sukuna x reader#Top Sukuna x Bottom ftm reader
233 notes
·
View notes
Text
My Chosen: Epilogue
IT’S BEEN 84 YEARS SINCE I’VE POSTED ANYTHING, ROSE. I am so sorry for the extremely unnecessary wait, guys. Life caught up with me and I found myself working within an inch of my life with hardly any down time on weekends to write or see my friends or anything. I’ve also chosen to largely stay away from the star wars tag because of all the discourse with certain ships and all around toxic behavior. You guys are amazing for sticking around and I thank you so much for that. I was going to do two more chapters for this, but the way I want to end it is perfect in one chapter. So without further adieu, please enjoy the final chapter of ‘My Chosen’.
The warm sun danced along your arms and legs as you sat perched by the window, a warm mug of tea in your hands. The steam drifted up and warmed your cheeks as you gazed out into the vast courtyard below.
Leia sat on a stone bench with a book in hand as Kylo imitated Luke in slow movements of Jiu Jitsu, their every move in sync with each other.
Since Luke’s reveal of his original intentions towards Kylo, he had been on the road to gaining Leia’s trust back along with his trust towards Kylo. More than anything, he wanted to better himself and rid any feelings of guilt.
Kylo was in a very similar boat, but struggling a bit more. The darkness was in no way gone from him, nor did you expect to to be. Every creature had dark and light with in them, it was how they chose to act on those tendencies. Every day he learned more and more about this new century and how to speak in multiple new tongues.
He absorbed knowledge like a sponge and was always eager to apply his knowledge, just like the prince he was in ancient times. It was no easy position to be in, but Kylo tried with everything he had to appear decent in your eyes.
“Enjoying the view?” A sarcastic yet amused voice called from behind you.
Rey stood in the door way with a knowing smirk on her face as you rolled your eyes in response.
“I could ask you the same.” You replied with a teasing tone as she chortled in delight.
“You’re always a sight for sore eyes, Y/N.” She snarked back at you. She made her way over to you and sat on the bed. “How’s it going with mummy bones out there?” She leant back on her elbows as you chuckled.
“He’s adjusting with every passing day. It’s no small job, but he makes it look relatively simple.” You took a sip of your tea and leaned your head against the window, watching as Leia stood from her seat and gestured Luke away leaving Kylo to his daily meditation.
He began to sit down when his body stiffened and his head turned in confusion. His eyes glanced around until they landed on you in the window, a small smile gracing his lips. You smiled back and made a small wave in is direction only causing him to smile more as he lifted his fingers to his lips and placed them on his heart.
Your body filled with a spreading warmth as you returned the gesture, watching him sit down and begin as a gagging noise sounded off behind you.
“You two are disgusting.” Rey laughed as she jumped up and ruffled your hair. You laughed and brushed her hand away. “C’mon, love bird, you promised me a round of training.” With that you placed your mug down and followed her out the door.
______________________________________________
The spray of the shower was a welcome relief from the vigorous training session Rey had put you through. Since the entire mummy incident, you’d made the decision to begin self defense in favor of not constantly feeling like a damsel in distress.
Also, it just felt really good to kick major ass.
You leaned your head back and allowed the water to relax your muscles, your hands pushing through your hair in complete relaxation. As more steam filled the room, you found yourself lost in the relaxing feeling as the door opened and closed.
It wasn’t until the shower curtain moved slightly that your turned to see a very close and very naked Kylo. You clutched your chest and slapped a hand against his tattooed chest.
“You scared the shit out of me, Kylo! What have i said about sneaking?” His head tilted in a curious manner before he stepped forward within the shower, causing you to step back and make contact with the wall.
He rested his forearms flat against the tile around your head and leaned in until your foreheads touched, every inch of your bodies coming into contact with each other under the wet spray.
“My Chosen...” He uttered in perfect english before pressing his lips to yours, a sigh of pleasure leaving him as his hands slid down the tile to encase your face. Your eyes closed as your hands slid up his firm abdomen, your nails lightly scratching the muscles there.
He shivered in delight, mouth opening in a smile before sliding his tongue into tango with yours. His hands disappeared from your face for a second before you felt yourself being lifted against the wet wall, Kylo’s massive arms squeezing and massaging your thighs.
With a loud smack, your lips left his and you were able to get a good look at him. The water had drenched his hair to the point where it hung in his face, causing you to stifle a laugh as you attempted to slick it back on his head. He leaned into your touch like a puppy, a smile of contentment gracing his lips.
You rested your arms around his shoulders and dropped your forehead back down to his.
“Looks as if someone had a good day with his lessons.” You whispered as he nuzzled his nose against yours. If there was something you enjoyed more than anything about Kylo, it was how affectionate he was with you.
“Mmm, good indeed...” He rumbled before nipping your chin. When it came to everyone else he was very reserved and cold, even stiffening the slightest when Leia hugged him. Yet with you it was like he was a man starved and you were the feast that could satiate his hunger. “Better now with you.”
After another half hour of vigorous kissing in the shower, Kylo had carried you out and dried the two of you off while always maintaining some form of contact with you. You now found yourself in your underwear with Kylo’s head resting on your stomach, a pair of loose fitting black sweats on his hips.
His fingers traced over the remaining scars on your stomach with a gentleness only you knew, lips following in their wake. One hand lay face up on your pillow while the other scratched and sifted through his hair in slow strokes, a low purr rumbled from his chest at the feeling.
He had never sought redemption, never really wanted it if he were to be honest. But when it came to you he felt the need to be better, maybe not entirely good but better.
No, he didn’t want redemption, but he without a doubt wanted you.
“Kylo?” He looked up, resting his chin on your stomach, “You’re quiet tonight...more so than usual.” Your hand left his hair to trace his features.
“Sometimes...I think that I am still in that tomb...still wrapped in dried bandages and trapped in my own head...” Kylo had made strives in his lingual skills, now able to speak English and Italian on top of his native Egyptian.
“...I still think he’ll return....Snoke...and drown me back into the darkness. But worse...I’m afraid he’ll take you from me...” His voice had been reduced to a low whisper as his eyes scanned your scars. You sighed and tilted his chin back up.
“Snoke will never come back, Kylo. You beat him in more ways than one.” You sifted your fingers through his hair once more. “Plus, I’m your chosen, you’re kinda stuck with me.” You joked as a smirk appeared on his lips.
“Indeed, you’re correct...” He growled and crawled up your body, muscles rippling under his tattooed skin. He stopped just in front of your face, lips barely touching yours, “You are mine, my Chosen.” With that, he devoured you with everything he had.
He still had a long way to go, but that was fine with you. You’d stay with him through it all no matter what.
Because really? Death is only the beginning.
#my chosen#kylo ren x reader#kylo x reader#reader insert#the mummy#mummy!kylo#star wars#star wars au#kylo ren
33 notes
·
View notes
Text
About Jan
Name: Jan Nikolai Bjelik
Age: 14
Gender: cismale
Height: 5′3″
Weight: 102 lbs
Nationality: Russian-American
Occupation: Mercenary
Faceclaim: Yukine from Noragami
In the year 2101, the world is now run by large corporations, and private mercenary companies, or PMCs, keep the peace. Most of the world’s population has been enhanced by cybernetic augments. Jan is just one of the mercenaries employed by such a company.
He was orphaned at the age of seven, when a rival mercenary of his father murdered both him and his mother right in front of Jan. He was taken in by a soldier friend of his father, who trained him in how to fight, how to survive on his own, and how to use weapons. When he was 11, Jan officially became the youngest mercenary in the world, and made a name for himself as one of the best in his field, earning him the nickname “Golden Cross”, based off the patch he wears on the left sleeve of his jacket.
Roughly a year ago Jan was involved in an operation that resulted in the loss of his left arm, and in him being left at the brink of death. To save him, he was given a number of cybernetic enhancements, each one serving to make him that much stronger, faster, and deadlier.
Recently one of the tech inventors of his PMC came up with a portal machine, and they decided to test it by sending Jan to another part of the office. However, that seems to have gone wrong and he’s been instead sent to an entirely different world altogether.
Equipment and abilities-
Proficiency in firearms and melee weapons- Having been trained in various guns and blades since he was seven, Jan is very skilled at handling all types of weapons.
Heightened agility- Jan’s very fast and agile, using his small frame to his advantage in combat.
Proficiency in hand-to-hand combat- He was trained by a soldier, so he does know at least two different martial arts suited to his natural agility, and he’s very skilled in a melee.
Multi-lingual: He is fluent in four different languages. Russian and English are his mother tongues, with him being taught Japanese and German by his mentor.
Garuda- This is a custom-built .45 caliber pistol that’s been with Jan since he started his career as a mercenary. It’s based on the Colt 1911 platform, but with several improvements and modifications; the magazine holds about ten rounds, and it has a titanium slide for smoother action. Jan never goes anywhere without it.
Augments-
Left arm- Jan received a new left arm following the loss of his original one, and the new one has its own bells and whistles built in. There’s a folding blade as long as his forearm that pops out of the wrist, collapsing into a compartment when not in use; he has a taser built into the elbow for non-lethal engagements and take downs; he also has micro missile launchers into the top of the forearm, about four missiles are loaded in, each with the power to destroy a tank.
Subdermal armor- He now has armor plating woven into the muscles of his torso, arms, and legs to provide added defensive capabilities.
Reflex booster- A booster that gives him heightened reflexes for faster reaction times.
Hazushi-tech scanners: His eyes are replaced by a pair of scanners, giving him the ability to zoom in and out as if he had a pair of binoculars. He also has the ability to scan targets for weak points to exploit in combat. In addition to these features, he has a HUD, and the eyes can switch to different modes of vision, such as infrared, thermal, and night vision.
Health system: A system that monitors the status of his body, and ensures he’s healthy by way of using his own cells to repair wounds received, and by filtering out toxins and pathogens out of his blood stream.
ARES combat system: An illegal augment installed without his knowledge, or even that of the company he’s employed by, the ARES is capable of essentially making a super-human out of its user. They’ll get enhanced strength, speed, and stamina. The drawback to this system is that it is incredibly dangerous to use, as it’s fused to the nervous system, and because it takes so much out of the user, it could paralyze or even kill them. Jan is aware of this, and he refuses to use the ARES as the risk is just too great.
0 notes
Text
Ich war eine Berlinerin
A long time ago I decided in a daydreaming moment to spend a month at language school in Germany. In my head this was going to be largely drifting around town feeling cultured and multi-lingual. So I merrily booked some lessons and an airbnb in Berlin. Then it got closer to the time and I remembered I absolutely hated every minute of German lessons at school, and the only way to drift around feeling cultured and multi-lingual would be from cramming German into my aged brain. This triggered what could best be described as the “complaining phase”, which was weeks of bitching to Marcel that I didn’t want to go, I hate German grammar and this was the worst idea of my life.
We arrived 5 days before language school started in order to get settled. This mostly involved me complaining at a number of places around the city, and on a trip out of town. Our first weekend was forecast to be sunny so we decided to head out into the countryside of the East to go canoeing. Step one was rent a car, which turned out to be phenomenally expensive and involve driving out to the airport. We then immediately took the wrong turning and circled the whole airport trying to find our way out...and straight into a non-moving traffic jam. Google maps refused to consider there might be any possible alternative routes to spending 2 hours in a traffic jam. Neither did our car satnav. So instead I decided to get creative with the map and managed to navigate around the whole thing, whilst being incredibly smug about it (which I’m sure Marcel deeply appreciated).
When we finally got out to the East I was pleasantly surprised. The only real news that reaches the UK of rural East Germany is neo-Nazis and depopulation. Thankfully the first wasn’t visible where we were, and the second meant lots of wildlife. We saw a real live stork (not delivering a baby) before we even got there.
Our canoe trip was down the Havel to try and see beavers (of the wildlife variety). It was a stunning day and a pleasantly quiet river. Naturally we saw zero beavers, and due to Marcel’s ambitious nature we had to paddle back at speed to get back from our 16km run before dark. My muscles were screaming (and only screamed more over the next few days). We also had to return the car before 21.30, which involved driving back and then getting lost in the airport AGAIN and circling it twice. Now feel like I know the roundabouts of Tegel extremely well.


After bitching about language school heavily, it turned out to be...surprisingly fun. Or I got stockholm syndrome. Not really sure, but after a couple of weeks I had settled into a very nice routine of morning classes, then a leisurely lunch at our awesome airbnbs with the best views in the world, followed by museums or excursions in the afternoon. My language school card bought me an annual museums pass for 25 euros, so I got to relive the student dream again!

It was pretty hot whilst we were there so we got into the local lake swimming culture. Our favourite turned out to be Krumme Lanke. It is surrounded by forest but still accessible from town. On day one we were there, we saw a grass snake emerge from the bank and go for a little swim with it’s head above water. Being from the UK where wildlife is...sparse, this was extremely exciting. When we returned a few days later, it was much busier and I thought to myself “poor snake, it has no chance of a swim today”. Only to find myself looking down whilst swimming in the water a couple of hours later to find the snake swimming entirely underwater by my legs. Turns out whilst I like wildlife there are limits and that is definitely one of my limits.

One of the other benefits of it being hot was I decided a policy of daily ice creams was essential. We started off at our local ice cream place but then one day found an amazing place that was about a 15 minute walk from our house. I then took to making Marcel take daily walks in the broiling heat with me to eat them. We also discovered that German museums don’t really do air-con after some of the hottest museum trips of my life to the Stasi Museum and Ephraim-Palais Museum. Sort of surprised we didn’t have to step over the collapsed forms of over-heated tourists between exhibits.
My language school did an afternoon programme of lectures, seminars and activities. Whilst Marcel was around, I didn’t attend any as for some weird reason Marcel didn’t want to hang out and listen to someone explain things very slowly in basic German to a bunch of language learners. Odd that. However at one point he went off to visit his relatives near Frankfurt and I decided to attend a seminar on art in the Third Reich. This was a great lecture but lead me to become...somewhat over-confident with my German. On Marcel’s return I decided we should escape the boiling weather by doing one of the tours run by “Underground Berlin”. They did one inside a flak turm and because the tour timing was more convenient in German that in English, I decided I’d be fine going on that one.

My first indication that I might not be fine was when our guide took a huge breath before starting because it turned out he was one of those people who had a lot of information to impart and didn’t want to waste time doing so. A rapid torrent of German poured forth from him, with me barely able to assess where one word finished and the next started. Which would have been fine if it hadn’t been the safety briefing he was giving as he handed out hard hats. Would strongly advise not getting over-confident with your language skills when you are going to be touring a half-blown up bomb site. I spent most of the tour understanding nothing but trying desperately to copy the others in the hope of not dying down there. Marcel very nicely said it was very technical and harder to understand than his C2 language exam he had to do to prove he was a real German, and then gave me a long summary afterwards about what the whole tour had actually been about. Anyway it was a really cool site and I thoroughly recommend you sign up for the (English language) tour of it. Plus the park it is in has red squirrels, which Marcel and I got unbelievably excited about but actually turns out to be really common in Europe.

Other cool tours we did included one of the Bundestag, which was free although it was hardly spontaneous. You had to email to book tickets ages in advance and then bring your passport (weirdly not the only exhibition I had to do that for, also had to do it for the world press photography exhibition which was taking place in a political party’s head office [as you do]. I think this might feel more normal for Germans who are used to carrying ID at all times, but if you are British it is quite hard to remember and feels strange). The tour was pretty interesting though and there is uncovered Russian graffiti all over the walls inside from the second world war, which was cool to see.

Beyond that we largely mooched and ate a lot. We were staying upstairs from a fondue restaurant and a vietnamese place, and just around the corner from a vegan Szechaun restaurant. As a result, we did ate out a LOT. Also given how hot it got, we very much appreciated not using our kitchen and letting someone else heat up their place by using their oven. Instead we’d just eat out and admire the views from our amazing balcony.

It got hotter and hotter until towards the end of our stay we had three days of epic thunderstorms in a row. We had a great view from our balcony of the Fernsehturm, which Marcel managed to see get hit by lightening twice, both times after I had despaired of seeing it happen. The first two days the thunderstorms were at about midnight and kept us awake with constant lightening and huge claps of thunder. The last day it happened at about 6.30. Which was sub-optimal as that was when my mother’s flight from London was due to land. Weather went from fine to “wind so strong the leaves and flying upward past our 5th floor balcony, followed by rain and mist so thick we couldn’t see anything anymore” in about 5 minutes. We constantly checked my mother’s flight updates online and her landing time kept getting pushed back and back. And then suddenly it just disappeared entirely from the landing/landed screen. Note to German airports, this is not very reassuring. Nor is it when you phone the airport and ask what happened to the flight and you say you “don’t know”. We then looked on the BA website, who said the flight had been diverted to Hamburg. We phoned Hamburg to check this and they said they didn’t know and hadn’t heard about that. Thankfully at just about the point when a full freak out was starting, my mother texted to say they had landed in Hamburg after several terrifying abortive attempts to land in Berlin. They did then fly them back to Berlin when the storm finished so she arrived pretty late and then we had to take a huge diversion back to her hotel because of trees blown over the in the street. Oh the delightful summer weather.
By the end of the month, I was entirely in love with Berlin and the relaxed life of a language school attendee. But alas we’d planned a road trip and our airbnb booking was running out so I had to say a very reluctant goodbye to my language class and Berlin and hit the road.

0 notes
Text
Parkinsons Disease Therapeutics Market is Predicted to be Worth US$ 5.24 Bn by 2025
Parkinson’s Disease Therapeutics Market – Snapshot
The global Parkinson’s disease therapeutics market is growing with high prevalence and rise in incidences of Parkinson’s disease across the developed countries. The global Parkinson’s disease therapeutics market was valued at US$ 2.18 Bn in 2016 and is projected to witness cumulative annual growth rate (CAGR) of more than 10.9% from 2017 to 2025 to exceed the US$ 5.24 Bn by 2025. The global Parkinson’s disease therapeutics market is witnessing a relatively high growth owing to rise in awareness regarding Parkinson’s disease, rapidly growing geriatric population, promising pipeline drugs, and new product launches.
Parkinson’s disease is a progressive neurodegenerative disorder that affects the dopamine producing nerve cells in the brain. Parkinson’s disease primarily causes tremors, muscle stiffness, improper motor movements, and gait and balance problems. Secondary symptoms of Parkinson’s disease include anxiety, depression, and dementia. The exact cause of Parkinson’s disease is not known; it predominantly affects the older people who are above 50 years of age. Men are one-and-half times more affected by the disease than women. According to Parkinson’s Foundation based in the U.S., it is estimated that worldwide around 7 to 10 million people are affected by disease and every year around 60,000 Americans are diagnosed with it.
Request A Sample: https://www.transparencymarketresearch.com/sample/sample.php?flag=S&rep_id=26975
High prevalence and rise in incidence rates of Parkinson’s disease in developed countries are driving the growth of the global Parkinson’s disease therapeutics market. Also, increase in awareness about Parkinson’s disease and high clinical R&D budget by the governments and non-profit organizations are projected to fuel the growth of the Parkinson’s therapeutics market during the forecast period. The promising product pipeline represents the potential business development opportunities during the forecast period. In the U.S., there are around 10 different drugs under clinical pipeline studies in phase 3 for treating different symptoms of Parkinson’s disease. However, patent expiration of key branded drugs and side-effects associated with therapeutic drugs are anticipated to limit the growth of the Parkinson’s disease therapeutics market during the forecast period.
Till date, there is no permanent cure available for treating Parkinson’s disease. However, medications such as levodopa combination therapy, dopamine agonists, MAO-B inhibitors, COMT inhibitors, cholinesterase inhibitors, and amantadine drugs are used to treat the different symptoms associated with the disease. Levodopa combination therapy is highly recommended and widely used for treating the motor symptoms of Parkinson’s disease.
Request Brochure of Report: https://www.transparencymarketresearch.com/sample/sample.php?flag=B&rep_id=26975
The global Parkinson’s disease therapeutics market can be divided into four segments based on drug class, route of administration, distribution channel, and geography. In terms of drug class, the global Parkinson’s disease therapeutics market can be segmented into levodopa combination therapy, dopamine agonists, MAO-B inhibitors, COMT inhibitors, and others. The other drug class includes cholinesterase inhibitors, amantadine, antipsychotic drugs, and vassopressant drugs. Levodopa combination therapy dominated the global Parkinson’s disease therapeutics market in 2016, holding more than 32% share of the market. The segment is projected to grow at a moderate pace during the forecast period and is poised to gain market share by the end of 2025. Levodopa combination therapy is considered a highly effective treatment for controlling the motor symptoms throughout the stages of Parkinson’s disease.
In terms of route of administration, the global Parkinson’s disease therapeutics market can be classified into oral, transdermal, subcutaneous, intestinal infusion, and others. The oral route of administration accounted for the leading share of the global market. The segment is projected to continue its dominance throughout the forecast period. The recent launch of Duopa in the U.S. has contributed to significant share of the intestinal infusion segment in the global market. The other routes of administration include sublingual film and inhalation. The anticipated launch of pipeline drugs administered through inhalation and sub-lingual route is likely to gain market share by the end of 2025. Distribution channels include hospital pharmacy, retail pharmacy, and online pharmacy. The retail pharmacy segment dominated the global Parkinson’s disease therapeutics market in 2016 and is likely to gain market share by the end of 2025.
Geographically, the Parkinson’s disease therapeutics market can be categorized into five regions: North America, Europe, Asia Pacific, Latin America, and Middle East & Africa. Europe accounted for the largest share of the global Parkinson’s disease therapeutics market in 2016, followed by North America with a substantial market share. High level of awareness, increase in funding for research and grants, favorable medical reimbursement policies, high prevalence of Parkinson’s disease, rapidly growing geriatric population, and promising clinical pipeline products have contributed to the key share of Europe in the Parkinson’s disease therapeutics market. Europe is a highly attractive market and is expected to expand at a significant CAGR during the forecast period. The Parkinson’s disease therapeutics market in Asia Pacific is poised to grow at a moderate growth rate. A major share of the Parkinson’s disease therapeutics market is captured by Japan and China in Asia Pacific, primarily due to the large base of elderly people affected with Parkinson’s disease in these countries.
The global Parkinson’s disease therapeutics market is consolidated with a few companies accounting for majority of its share. Leading players operating in the global Parkinson’s disease therapeutics market include Novartis AG, F. Hoffmann-La Roche AG, AbbVie Inc., Teva Pharmaceutical Industries Ltd., and UCB Inc., which exhibit wide geographical outreach. Manufacturers are adopting new product commercialization in the international market to tap the unmet needs of Parkinson’s disease. Other prominent players operating in the global market include STADA Arzneimittel AG, GlaxoSmithKline plc, Valeant Pharmaceuticals International, Inc., Merck & Co., Inc., and Impax Laboratories Inc.
About us:
Transparency Market Research (TMR) is a U.S.-based provider of syndicated research, customized research, and consulting services. TMR’s global and regional market intelligence coverage includes industries such as pharmaceutical, chemicals and materials, technology and media, food and beverages, and consumer goods, among others. Each TMR research report provides clients with a 360-degree view of the market with statistical forecasts, competitive landscape, detailed segmentation, key trends, and strategic recommendations.
Contact us:
Transparency Market Research
90 State Street,
Suite 700,
Albany
NY – 12207
United States
Tel: +1-518-618-1030
USA – Canada Toll Free 866-552-3453
Email: [email protected]
Website: http://www.transparencymarketresearch.com/
0 notes
Text
Parapharyngeal Space Tumors - "A Surgical Challenge"-Juniper publishers
Abstract
Parapharyngeal space tumors are rare entity. Overall incidence is less than 0.5%. These tumors are divided into prestyloid and post styloid tumors. Salivary gland neoplasma are common in prestyloid compartment whereas Neurogenic tumors in post styloid compartment. As these tumors are painless and does not express signs and symptoms at early stage, diagnosis of such tumors needs critical evaluation. Anatomic complexity of PPS makes surgical excision more challenging. We have reported 4 cases of parapharyngeal space tumors over a period of 10 years.
Keywords: Parapharyngeal; Schwannoma; Paraganglioma; Neurogenic; Transcervical
Background
Parapharyngeal space is an inverted pyramid from base of the skull to hyoid bone. It is bounded medially by pharynx, anteriorly pterygomandibular raphe, posterolaterally carotid sheath, posteromedially retropharyngeal space, laterally above the level of mandible it is bounded by ramus of mandible, deep lobe of parotid and medial pterygoid muscle, below the level of mandible; it is bounded by posterior belly of diagastric muscle. It is divided into prestyloid and poststyloid compartment by aponeurosis of zuckercandle and testus [1]. 80% of the PPS tumours are benign while 20% are malignant [2]. Incidence of parapharyngeal space tumors is less than 0.5% [3]. Majority of the tumours are slow growing, painless and progressive in nature. If untreated might result in severe life threatening complications like airway obstruction and cranial nerve deficit resulting in significant morbidity. Systematic diagnostic evaluation plays an important role in diagnosis. Surgical excision has Pivotal significance in PPS tumors. We have identified and reported four cases of parapharyngeal space tumors at our centre over a period of 10 years.
Case Description
Case 1
29 year old male presented with complain of painless lateral neck swelling since 3 months. There was no history of dysphagia, Hoarseness of voice. There was no cranial nerve involvement. FNAC showed spindle cell tumor. On MRI there was 50x 37mm well circumscribed lesion over left side of neck suggestive of schwannoma. Surgical Excision of the tumor was done using transcervical approach (Figure 1). There was no intra-operative complication. ICA, ECA, Vagus nerve and IJV were identified and preserved. Tumor was excised completely (Figure 2). Post operatively there was reduction in high pitch sounds. Origin of tumor from vagus nerve was confirmed intra-operatively. Microscopic picture revealed presence of mixed Antoni A and Antoni B cells concluding to the microscopic features of schwannoma.
Case 2
34 year old female presented with painless swelling over right side of neck. CT neck showed 64x46x35mm lesion in the carotid space compressing right IJV and displacing it anterolaterally (Figure 3). Superiorly it was extended up to carotid canal. Differential diagnosis includes paraganglioma in view of intense enhancement of lesion and vagal schwannoma in view of displacement pattern of vessel. FNAC was suggestive of spindle cell tumor. Intraoperatively there was rupture of internal carotid artery which was repaired with 6-0 ethilon, vagus nerve was also sacrificed due to the severe adherence of the tumor to the nerve.
Case 3
24 year old female complains of painless progressive swelling with dysphagia to solids and liquids since 4yrs. CT scan showed heterogeneously enhancing lesion 85x31mm with retrosternal extension displacing major vessels laterally. Intraoperatively transcervical incision was taken and tumor was dissected to free it from the major vessels and nerves and it was removed in to (Figure 4).
Case 4
40 year female patient presented with swelling of left submandibular region since 1 month (Figure 5). FNAC showed spindle cell tumor, USG showed 41x39mm Heterogenous mass and left submandibular gland. CT Scan Showed 4.5cm enhancing well circumscribed lesion, left submandibular gland and another 1.3x1cm lesion adjacent to it. No dysphagia or hoarseness of voice, intra-operatively Hypoglossal nerve was sacrificed. Lingual nerve was identified and preserved. Histopathology report showed neurogenic tumour i.e. schwannoma.
Discussion
Para-pharyngeal space (PPS) tumors are very rare. We have identified 4 patients after reviewing 10 years retrospective data of all head and neck tumors presented at Manavata curie cancer centre Nashik. Incidence of parapharyngeal space tumors at our institute was 0.004%. Overall incidence of these tumors is less than 0.5%. These tumors are slow growing, painless and patients express at later stage when the size become considerably large. Usually patients are asymptomatic but may exhibit dysphagia or hoarseness of voice. In our 4 patients only one patient had dysphagia to solids and liquids rest of the patients were asymptomatic [4,5]. 80% of the tumors arising in this region are benign [2]. Pleomorphic adenoma is the most common tumor of prestyloid compartment where poststyloid tumors are mostly neurogenic like shwannoma, paraganglioma, neurofibroma, hemangiomas etc. Chordomas, lypomas, lymphomas, chemodectomas, rhabdomyomas, chondrosarcomas, desmoid tumours, ameloblastomas, amyloid tumours, ectomesenchymomas, fibrosarcomas and plasmocytomas have also been reported [2].
Diagnosis of these tumors is difficult as they are asymptomatic. Diagnostic evaluation constitutes CT scan and MRI to clearly define the extent of the tumor mass. Arteriography also plays a significant role to assess vascular compression. In our identified cases CT scan was performed in 3 cases and MRI in one case. MRI has been shown to gives better dimensions of the parapharyngeal space tumors. Advantage of MRI is, it distinguishes tumor from Muscular structures and give better dimentions of the tumor [6].
Arteriography was not performed in any of our cases. Once the nonvascular nature of tumor is confirmed by radio-imaging, FNAC can be performed for definitive diagnosis. FNAC is accurate in 90-95% of the cases and helps in surgical planning [7]. Limited role is explained in post styloid compartment. We performed FNAC in all our patients and it was conclusive [8,9].
Schwannoma may arise at any age but in our institute patient's age ranged from 3rd to 4th decades of life. There is no gender predilection. Schwannoma may be of two types histologically consisting of either Antoni A cells or Antoni B cells. We had two patients with Antoni A cells and other one was of mixed variety [10]. Paragangliomas are tumors of autonomic nervous system. Head and neck paragangliomas are unique in its variety as they don't release catecholamines. Incidence of paraganglioma is 1 in 30,000 cases [11]. Histopathological picture shows two types of cells; Chief cells and sustantecular cells. One of our patient's histological features were identical to it.
Surgical management of parapharyngeal space tumors is very challenging owing to anatomic complexity ofthe space and vicinity of the tumor with major neurovascular structures. There are 7 different approaches described for PFS tumors. Transcervical, Transcervical- transparotid, Transoral-transcervical approach, Extended approach, Transcervical-mandibulotomy aaproach, Transcervical-transmastoid approach have been explained [12]. 4cm is the limit for radical tumour excision with the transcervical approach without mandibulotomy. For a safe and radical resection of tumours > 4cm the “swing” approach or the transmandibular with a double osteotomy is required [2]. We used transcervical approach without mandibulotomy in all cases. Accesiblity was compromised in larger tumors but we could enucleate entire tumor without much difficulty. ICA was ruptured in one case but it was managed. Minimal accessibility may be a compromise but there is less surgical morbidity and post op recovery is faster in our experience.
Complications after surgical management are unavoidable. Expected complications are due to sacrifice of cranial nerves. There may be unexpected neurological complications in spite of preservation of nerves like first bite syndrome, Trismus, facial nerve weakness, orocutaneous fistula, Seroma. We experienced loss of high pitched sounds in two of our patients and there was hypoglossal nerve palsy as hypoglossal nerve was sacrificed in one case.
Conclusion
CT scan or MRI should always be performed in order to distinguish prestyloid from poststyloid lesions and assessment of the extension of the tumour and its relationship with adjacent structures. Trans-cervical approach is safe and should be the first choice for large tumors; other approaches are reserved for selected cases.
Clinical Significance
These are painless slow growing non malignant tumors with very less incidence of recurrance. Management of PPS tumors is challenging for surgeons. Neurological and Surgical complications should always be explained to patients preoperatively. Preoperative assessment and careful surgical manipulation are of utmost importance.
To know more about Open Access Journal of Head Neck & Spine Surgery please click on:
https://juniperpublishers.com/jhnss/index.php
To know more about Open access Journals Publishers please click on : Juniper Publishers
#Head and Neck Surgery Journal#Journal of Head Neck & Spine Surgery#Journal of Spine Surgery#Juniper Publishers#Open Access Journals
0 notes
Text
Parkinson’s Disease Therapeutics Market Pegged for Robust Expansion by 2025
The global Parkinson’s Disease Therapeutics Market is growing with high prevalence and rise in incidences of Parkinson’s disease across the developed countries. The global Parkinson’s disease therapeutics market was valued at US$ 2.18 Bn in 2016 and is projected to witness cumulative annual growth rate (CAGR) of more than 10.9% from 2017 to 2025 to exceed the US$ 5.24 Bn by 2025. The global Parkinson’s disease therapeutics market is witnessing a relatively high growth owing to rise in awareness regarding Parkinson’s disease, rapidly growing geriatric population, promising pipeline drugs, and new product launches.
Parkinson’s disease is a progressive neurodegenerative disorder that affects the dopamine producing nerve cells in the brain. Parkinson’s disease primarily causes tremors, muscle stiffness, improper motor movements, and gait and balance problems. Secondary symptoms of Parkinson’s disease include anxiety, depression, and dementia. The exact cause of Parkinson’s disease is not known; it predominantly affects the older people who are above 50 years of age. Men are one-and-half times more affected by the disease than women. According to Parkinson’s Foundation based in the U.S., it is estimated that worldwide around 7 to 10 million people are affected by disease and every year around 60,000 Americans are diagnosed with it.
High prevalence and rise in incidence rates of Parkinson’s disease in developed countries are driving the growth of the global Parkinson’s disease therapeutics market. Also, increase in awareness about Parkinson’s disease and high clinical R&D budget by the governments and non-profit organizations are projected to fuel the growth of the Parkinson’s therapeutics market during the forecast period. The promising product pipeline represents the potential business development opportunities during the forecast period. In the U.S., there are around 10 different drugs under clinical pipeline studies in phase 3 for treating different symptoms of Parkinson’s disease. However, patent expiration of key branded drugs and side-effects associated with therapeutic drugs are anticipated to limit the growth of the Parkinson’s disease therapeutics market during the forecast period.
Till date, there is no permanent cure available for treating Parkinson’s disease. However, medications such as levodopa combination therapy, dopamine agonists, MAO-B inhibitors, COMT inhibitors, cholinesterase inhibitors, and amantadine drugs are used to treat the different symptoms associated with the disease. Levodopa combination therapy is highly recommended and widely used for treating the motor symptoms of Parkinson’s disease.
Request to View Sample of Report -
https://www.transparencymarketresearch.com/sample/sample.php?flag=S&rep_id=26975
The global Parkinson’s disease therapeutics market can be divided into four segments based on drug class, route of administration, distribution channel, and geography. In terms of drug class, the global Parkinson’s disease therapeutics market can be segmented into levodopa combination therapy, dopamine agonists, MAO-B inhibitors, COMT inhibitors, and others. The other drug class includes cholinesterase inhibitors, amantadine, antipsychotic drugs, and vassopressant drugs. Levodopa combination therapy dominated the global Parkinson’s disease therapeutics market in 2016, holding more than 32% share of the market. The segment is projected to grow at a moderate pace during the forecast period and is poised to gain market share by the end of 2025. Levodopa combination therapy is considered a highly effective treatment for controlling the motor symptoms throughout the stages of Parkinson’s disease.
In terms of route of administration, the global Parkinson’s disease therapeutics market can be classified into oral, transdermal, subcutaneous, intestinal infusion, and others. The oral route of administration accounted for the leading share of the global market. The segment is projected to continue its dominance throughout the forecast period. The recent launch of Duopa in the U.S. has contributed to significant share of the intestinal infusion segment in the global market. The other routes of administration include sublingual film and inhalation. The anticipated launch of pipeline drugs administered through inhalation and sub-lingual route is likely to gain market share by the end of 2025. Distribution channels include hospital pharmacy, retail pharmacy, and online pharmacy. The retail pharmacy segment dominated the global Parkinson’s disease therapeutics market in 2016 and is likely to gain market share by the end of 2025.
Geographically, the Parkinson’s disease therapeutics market can be categorized into five regions: North America, Europe, Asia Pacific, Latin America, and Middle East & Africa. Europe accounted for the largest share of the global Parkinson’s disease therapeutics market in 2016, followed by North America with a substantial market share. High level of awareness, increase in funding for research and grants, favorable medical reimbursement policies, high prevalence of Parkinson’s disease, rapidly growing geriatric population, and promising clinical pipeline products have contributed to the key share of Europe in the Parkinson’s disease therapeutics market. Europe is a highly attractive market and is expected to expand at a significant CAGR during the forecast period. The Parkinson’s disease therapeutics market in Asia Pacific is poised to grow at a moderate growth rate. A major share of the Parkinson’s disease therapeutics market is captured by Japan and China in Asia Pacific, primarily due to the large base of elderly people affected with Parkinson’s disease in these countries.
Request to View Brochure of Report -
https://www.transparencymarketresearch.com/sample/sample.php?flag=B&rep_id=26975
The global Parkinson’s disease therapeutics market is consolidated with a few companies accounting for majority of its share. Leading players operating in the global Parkinson’s disease therapeutics market include Novartis AG, F. Hoffmann-La Roche AG, AbbVie Inc., Teva Pharmaceutical Industries Ltd., and UCB Inc., which exhibit wide geographical outreach. Manufacturers are adopting new product commercialization in the international market to tap the unmet needs of Parkinson’s disease. Other prominent players operating in the global market include STADA Arzneimittel AG, GlaxoSmithKline plc, Valeant Pharmaceuticals International, Inc., Merck & Co., Inc., and Impax Laboratories Inc.
0 notes
Text
Aegyptopithecus
Aegyptopithecus
Aegyptopithecus skull
Aegyptopithecus, which means "Egyptian Monkey", from Greek Αίγυπτος (Egypt) and πίθηκος (ape or monkey), is an early fossil anthropoid that predates the divergence between hominoids (apes and humans) and cercopithecoids (Old World monkeys). It is known from a single species, Aegyptopithecus Zeuxis, which lived some 35-33 million years ago in the early part of the Oligocene epoch. It likely resembled modern-day New World monkeys and was about the same size as a modern howler monkey, which is about 56 to 92 cm (22 to 36 in) long. Aegyptopithecus fossils have been found primarily in modern-day Egypt. Aegyptopithecus is believed to be a stem-catarrhine, a crucial link between Eocene and Miocene fossils.
Aegyptopithecus zeuxis has become one of the best known extinct primates based on craniodental and postcranial remains.
Discovery and taxonomy
Aegyptopithecus was discovered by E. Simons in 1965 in the Jebel Qatrani Formation in the Fayum Province of Egypt. There is controversy over whether or not Aegyptopithecus should be a genus on its own or whether it should be moved into the genus Propliopithecus. If Aegyptopithecus is placed in its own genus, then there is one documented species named A. Zeuxis. The type specimen for the species is CGM26901. Its scientific name means "linking Egyptian ape".
Morphology
Aegyptopithecus zeuxis was a species that had a dental formula of 2:1:2:3 on both the upper and lower jaws, with the lower molars increasing in size posteriorly. The molars showed an adaptation called compartmentalizing shear, which is where the cutting edges involved in the buccal phase serve to surround basins in such a way that food is cut into fragments that are trapped and then ground during the lingual phase.
The canines of this species were sexually dimorphic. The ascending mandibular ramus of this species is relatively broad. The orbits are dorsally oriented and relatively small which suggested that this was a diurnal species. This species showed some postorbital constriction. The interorbital distance of Aegyptopithecus Zeuxis is large much like that found in colobines.
A sagittal crest developed in older individuals and extends over the brow ridges. This species had an auditory region which is similar to that found in platyrrhines, having no bony tube and the tympanic fused to the lateral surface of the bulla.
The humerus has a head which faces posteriorly and is narrower than primates that practice suspensory behavior. The humerus also shares some features with extinct hominoids: a large medial epicondyle and a comparatively wide trochlea. This species had an ulna that compares to the extinct members of the genus Alouatta.
On the foot bones, this species had a grasping hallux. Aegyptopithecus zeuxis shares characteristics with haplorrhines such as a fused mandibular and frontal symphyses, postorbital closure, and superior and inferior transverse tori.
Based on dental dimensions and femoral remains the body mass of A. zeuxis is estimated to be 6.708 kg.
The functional length of the femur is estimated to be 150 mm, which is larger than Cebus apella and smaller than Alouatta seniculus.
In Egypt’s Fayum Depression a subadult female cranium, CGM 85785, was discovered by Rajeev Patnaik. This specimen’s cranial capacity was found to be 14.63 cm3 and reanalysis of a male endocast (CGM 40237) estimates a cranial capacity of 21.8 cm3. These estimates dispel earlier ones of approximately 30 cm3. These measurements, give an estimated male to the female endocranial ratio of approximately 1.5, indicating A. Zeuxis to be a dimorphic species.
The olfactory bulb to endocranial volume ratio is considered to be on the lower end of the strepsirrhine spectrum, perhaps as a result of the organism’s rostrum.
In relation to other anthropoids, the frontal lobes of A. Zeuxis are considered to be rather small but the olfactory bulbs are not considered to be small when taking into account the body size of A. zeuxis.
Overall, the brain to body weight ratio of A. zeuxis is considered to be strepsirrhine-like and perhaps even non-primate like.
Behavior
A. zeuxis is thought to have been sexually dimorphic. Tooth size, craniofacial morphology, brain size, and body mass all indicate this. Due to A. zeuxis being sexually dimorphic, the social structure is thought to have been polygynous with intense competition for females.
Three femoral remains were found in Quarry I (DPC 5262 and 8709) and Quarry M (DPC 2480). Paleomagnetic dating puts the sites at 33 Ma, consistent with the Oligocene epoch.
Based on estimated femoral neck angle (120-130 degrees) of aforementioned remains, the femur is similar to that of a quadrupedal anthropoid. The greater trochanter’s morphology is inconsistent with that of leaping primates, serving as further evidence of the animal’s quadrupedalism.
Aegyptopithecus is thought to have been an arboreal quadruped due to the distal articular region of the femur, which is deeper than that of “later” catarrhines. Also, based on overall femoral morphology, A. zeuxis is thought to have been robust.
The phalanges of the hands and feet suggest powerful grasping consistent with arboreal quadrupedalism.
In conjunction with the femur, the humerus suggests arboreal quadrupedalism. This is based on the pronounced brachialis flange and stabilizing muscles on brachial flexors rather than extensors.
In addition, the ulna and distal articular surface of the humerus indicate that A. zeuxis was not only an arboreal quadruped, but also large and slow. This is consistent with evidence extrapolated from femoral morphology.
Studies in dental microwear and microsutures focusing on the molars, suggest that Aegyptopithecus was probably a frugivore. It is also possible that Aegyptopithecus ate hard objects on occasion.
Habitat
Aegyptopithecus lived in the Fayum area of northern Egypt. Today, this area is semiarid and lacking in vegetation. At the time of Aegyptopithecus’ existence, the Oligocene, this area was heavily vegetated, subtropical, had many trees and had seasonal rainfall.
source - Wikipedia
Dear friends, if you liked our post, please do not forget to share and comment like this. If you want to share your information with us, please send us your post with your name and photo at [email protected]. We will publish your post with your name and photo. thanks for joining us www.rbbox.in
from Blogger https://ift.tt/2l1CfbZ
0 notes
Text
First let’s understand, what is a stroke?
When there is restricted blood flow to a particular part of the brain a stroke will be triggered. Tissue dies within the brain due to oxygen loss when blood flow is constrained.
Within the United States there are less cases of strokes than twenty-five years ago due to improvements with high blood pressure control.
The elderly are most likely to suffer a stroke; it typically occurs between the ages of 60 and 80.
The downside is that it is still possible for people under the age of 60 to suffer from a stroke, which is 34% of all strokes in the U.S. in 2009 according to the CDC.
Strokes and heart attacks share the same risk profiles, in that anyone that suffers from a stroke is also at risk of a heart attack and vice versa.
If you have diabetes or a high cholesterol count you are more likely to suffer from a stroke or heart attack in your future if you haven’t already.
No one is the same and there is also no entirely identical human response to a stroke or heart attack. The damage can vary from mild to severe and is potentially life threatening. When an individual suffers from a MILD stroke it is more likely that they will recover 100% versus someone that experiences a more severe case.
Moderate strokes will leave SOME permanent effects on that individual that can range from speech impediments, limb paralysis, and sometimes total paralysis. The good news is approximately 50 percent of stroke cases successfully reach partial to total recovery, and is why it’s the leading cause of disability in the U.S.
What are the symptoms of someone suffering from a stroke?
As I had mentioned earlier, no two peoples are identical in their physical response to a stroke, but there are some things you can keep an eye out for:
• Fainting or Vertigo (dizzy spells)
• Disorientation
• Loss of Hearing
• Loss of Memory
• Paralysis
• Blurred Vision
• Loss of Vision
• Clumsiness
• Numbness
• Difficulty Speaking
• Loss of Consciousness
• Loss of Speech
• One Side of the Body is Paralyzed
Hidden Causes of Heart Attack and Stroke By Christian Wilde >>>>
What are the causes of a stroke?
Half of all strokes are caused by blood clots, but some other causes include high blood pressure, arteriosclerosis, cerebral embolism, and coronary artery disease.
There are some factors that will increase the chance of eventually having a stroke, including:
• Irregular Heart Beat
• Diabetes
• Obesity
• Recent Heart Attack
• Damaged Heart Valves
• Smoking
• Birth Control Pills
• High Blood Cholesterol
Here’s something to consider:
A human being with even a slightly elevated high blood pressure measurement, is six times as likely to have a stroke than someone with a healthy blood pressure reading.
^^^ Omron BP742N 5 Series Upper Arm Blood Pressure Monitor with Cuff for Standard & Large Arms
No. 1 doctor and pharmacist recommended brand and #1 selling Manufacturer of Blood Pressure Monitors for 40 years
What can you expect when you have a stroke or someone close and near to you has one?
Medical science doesn’t have a cure for strokes. Holding yourself accountable for living a healthy lifestyle will reduce the likelihood of a stroke happening to you. But after a stroke has occurred you can expect some if not all of the following:
physical therapy to stop the muscles from weakening further
CT scans to observe brain activity and rule out tumors and other possible causes of a stroke
A carotid arteriogram which is a specialized x-ray for observing arteries
Chest x-rays
ECG
MRI
Stroke patients most likely than not will be expected to spend a bit of time in the hospital to monitor changes.
<<< 58 Stroke Preventive Meal Recipes: The Stroke-Survivors Solution to a Healthy Diet and Long Life by Joe Correa CSN
If you have a family history of strokes, suffered from a stroke, or want to proactively try to prevent it, here is a diet to consider:
• AVOID butter, animal fats, sugar, ice cream, greasy fried foods, white flour, red meat, and cheeses high in fat. INSTEAD EAT THESE: Neufchatel, Parmesan, or Goat Cheese, Fruit Sorbets, Dark Chocolate Dipped Frozen Banana’s, Greek Yogurt Popsicle, baked lean meat, lightly cooked vegetables in olive oil, raw vegetables and fruits, dried fruits, whole wheat flower, and vegan options.
• AVOID red meat, bacon, fatty cuts of meat, dark meat, and any meat deep fried.
INSTEAD EAT THESE: Fish, white meats like skinless turkey or chicken breast baked.
• AVOID sugary or artificially flavored beverages like Coca Cola, Mountain Dew, Pepsi, any Soda Product, Kool-Aid, Rockstar, Monster, any Energy Drink, and highly caffeinated drinks like coffee.
INSTEAD CONSUME THESE: purified water, flavored water (let some sliced strawberries, lemons, or cucumbers soak in your water for an all nature flavor), carbonated water, lightly caffeinated or decaf tea (try green tea or a fruit/flower flavored tea like hibiscus and berry), RAW cane sugar (tip: soak the RAW sugar in a ½ cup of boiling water and shake or stir vigorously to melt the sugar completely), or flavored & carbonated ICE water (it’s a brand you can find at Wal Mart, Big Lots!, and other grocery stores; they’re typically between $ 0.50 – $ 1.50 a bottle and are ZERO calories).
• AVOID white bread, Hawaiian rolls, cake, donuts, sugary cereals, and the like.
INSTEAD CONSUME THESE: whole wheat/whole grain bread with nuts, whole wheat cereals, organic oatmeal, oat, wheat, barley, millet, buckwheat, fig bars, and brown rice.
• AVOID fried vegetables or vegetables stir fried in regular soy sauce (which has HIGH salt content and can contribute to high blood pressure).
INSTEAD CONSUME THESE: raw vegetables and fruits, dried vegetables and fruits, fruits mixed with Greek yogurt, organic trail mix, nuts, seeds, beans, steamed vegetables, baked fruits (don’t add extra sugar, most fruits have more than enough natural sugar, they shouldn’t need any more. If you MUST add sugar, consider a healthy alternative approved by your doctor like Splenda, Extra, or RAW sugar).
• AVOID vegetable oil, canola oil, corn oil, margarine, butter, whipping cream, and the like.
INSTEAD CONSUME THESE: avocado oil, extra virgin olive oil, yogurt
• AVOID nicotine, alcohol, or caffeine.
INSTEAD CONSIDER: talking to someone about switching to a vape, weaning off of cigarettes, or finding a method the works for you, non-alcohol options of beers, ordering your drink virgin, ordering your coffee decaf, and maybe talking to a local physician that prescribes medical marijuana to find out if CBD & THC products will be helpful in recovery or prevention.
What are supplements that you can take to ease stroke symptoms or help prevent a stroke from occurring besides diet changes?
Phosphadityl Choline directly affects memory function by increasing its acetylcholine levels.
Suggested Dosage: 10 to 20 g daily and ONLY consuming a high-quality product for utmost safety.
Phosphadityl Serine also has a huge effect on brain function due to its being one of the prime phospholipids found in brain tissue.
Suggested Dosage: 300 mg divided out in three doses with three meals (breakfast, lunch, dinner before 6pm)
<<< Momental Mind Unflavored Complete Nootropic Blend
Mix 1-2 scoops with 8-10 ounces of water or your favorite beverage. You can also add to shakes, smoothies, and other recipes.
Drink whenever you are looking for a nourishing boost to your brain and your body. Most patients and supporters use this alongside their morning coffee to have that extra advantage to kick start the day.
Anandaful Health Extra Strength Brain Supplement >>>>
Includes Ginkgo Biloba and other effective ingredients.
Ginkgo Biloba reverses mental deterioration caused by cerebrovascular insufficiency according to a variety of clinical studies. It’s powerful in decreasing and preventing edema and dementia, which usually occurs after a stroke.
Suggested Dosage: 60mg of 24% extract taken two to three times daily (two for mild to moderate strokes or three for moderate to severe strokes)
<<< Superior Source No Shot Methylcobalamin Vitamin B12/B6/Folic Acid Tablets, 5000 mcg/800 mcg, 60 Count
No shot methylcobalamin vitamin B12/vitamin B6 with folic acid micro lingual tablets go to work fast, under the tongue. Works synergistically to support healthy heart function. Provide essential nutrients for the cardiovascular system.
Vitamin B12 & Folic Acid Combined will help replenish the depletion of these vitamins. Most stroke patients are found to be deficient in these two particular vitamins. Consuming a multi vitamin that has these two vitamins contained within it is a great way to help prevent a stroke from occurring.
Suggested Dosage: 1,000 to 2,000 mg daily of B12, which can also be administered in injections if given permission by a medical doctor. Folic Acid should be taken as directed on the container and with the support of a medical doctor.
Pure Naturals Lecithin Brain & Nerve Supplement >>>
Provides raw materials that are used for the structure and functioning of every cell in the body Assists with the production of a vital brain chemical that is vital to nervous system function and important for memory Promotes cardiovascular health Supports Digestive Health Promotes Brain Health
Lecithin rouses the making of acetylcholine and improves overall brain function. Another bonus of Lecithin is its benefits in fighting depression and lower cholesterol levels.
Suggested Dosage: 100mg three times a day with breakfast, lunch, and dinner. Choose the granules or capsulized lecithin.
<<< Qunol 100 mg and 120 softgels for easy consumption
Qunol Ultra’s specially-formulated (solubilized) CoQ10 dissolves 100% in water and fat, providing 3X better absorption. With Qunol Ultra CoQ10, optimum blood levels of CoQ10 are reached in just weeks—not months as with regular CoQ10.
Omega -3 Fatty Acids have proven in scientific experiments to boost cerebral blood flow, decrease swelling, and help normalize the brains prostaglandins.
Suggested Dosage: Take as directed with a Vitamin E supplement.
Solgar – Chromium Picolinate 500 mcg, 120 Vegetable Capsules >>>
May help maintain healthy blood sugar levels already within a normal range. Chromium is a component of a number of enzymes that release energy from cells and is required for proper receptor functioning necessary for nutrient metabolism.
Chromium has been shown in recent studies that people suffering from vascular disease have low levels of chromium.
Suggested Dosage: Take as directed, utilizing picolinate or GTF products ONLY.
Potassium can be depleted from your system if you take high blood pressure medication or diuretics.
Suggested Dosage: Take as directed on container.
St. John’s Wort, Gotu Kola, and Gingko have proven to boost blood flow in and around the brain, and raises the brains serotonin levels.
Suggested Dosage: Take each herb as directed, using guaranteed potency extracts.
Capsicum strengthens artery walls, cleans veins, and increases blood flow.
Suggested Dosage: Use as a pure extract with a meal as directed on the container.
What Can the Caregiver Do to Improve the Stroke Survivor’s Quality of Life?
Encourage the stroke survivor to attempt to do things independently, but remember to keep expectations realistic. Yes, it will take them more time to make a sand which than it used to, it will be quite a bit harder for them to get dressed, some days will be harder for them than others, and so on.
Try to keep things as structured as possible; same meal times, same day of the week for certain errands, sleep schedules, and so on.
Observe for signs of depression and be a source of encouragement. Praise them when they got through a task that’s hard for them, tell them to keep holding on to hope, and be a patient listening ear when they need to express something. Depression has been shown to debilitate the stroke survivor quicker and make getting through the day very difficult. Some vocal positive reinforcement can go a long way.
You can work together on some basic sign language skills to help when communicating is difficult.
Set the stroke survivor up with an acupuncture appointment to see what work can be done to help reduce pain, and improve nerve & muscle function.
Additional Resources for Further Information & References:
Evergreen Stroke Association
(425) 899-3000
www.evergreenhealth.com
Kirkland, WA 98034
Barney, P., M.D. (2014). Doctor’s Guide to Natural Medicine (2nd ed.). Salt Lake City, UT: Woodland Publishing. Part three. Individual Ailments and Their Recommended Treatments. Stroke. Pages 382-386.
Treating a Stroke with Natural Medicine and also how to prevent a stroke. First let's understand, what is a stroke? When there is restricted blood flow to a particular part of the brain a stroke will be triggered.
#bad headaches#birth control pills#blurred vision#brain stroke#clumsiness#confusion#damaged heart valve#diabetes#diet#difficulty speaking#disorientation#dizziness#fainting#feeling tired#hemorrhagic#high blood pressure#high cholesterol#irregular heart beat#ischemic#loss of balance#loss of consciousness#loss of hearing#loss of memory#loss of speech#loss of vision#mild#moderate#monitor#nootropics#numbness
0 notes
Text
Episode 102 - Mouth Parts
Mouth Issues
Ulcers
They are uncomfortable and mostly non-serious. Also known as "canker sores". Can take 2-3 weeks to completely heal. Anything lasting over 3 weeks should be checked out by your doctor or dentist. Ulcers can appear on the inside of the cheeks or lips, the roof of the mouth, or the tongue. A minor ulcer versus a major ulcer is determined by the size of the sore and the layers of skin affected. Any ulcer that is bleeding should be checked out despite the length of time. The edges are red while the center can be yellow, white, or grey. And they are PAINFUL!!
Ulcers can be caused by acidic or spicy foods, braces, stress, hormones, and some medications (such as beta-blockers for blood pressure or NSAIDs). Nutritional deficiencies can increase your risk of ulcers. Malabsorption due to conditions like celiac or deficiencies in B-vitamins and iron are the most common culprits. Also, decreased immunity can make the skin inside the mouth more prone to ulcer recurrence.
Thrush
This is a yeast infection the mouth caused by the overgrowth of Candida, known as oral candidiasis. It appears as white patches on the inside of the cheeks, tongue, or roof of the mouth, and the spots cannot be scraped off. Candida is normal in the body and is kept in balance by the rest of the body's normal flora. Overgrowth can occur after antibiotic treatments, during times of decreased immunity due to treatments or disease states, or from inhaled steroid treatments.
Thrush is treated with a topical antifungal that the doctor directs you to swish around in the mouth to coat the affected areas, usually Nystatin. If yeast is wide-spread, a systemic antifungal will be used. Probiotics are a great way to keep your normal flora in balance.
Angular cheilitis (ky-ly-tis)
Cheilitis = inflammation of the lips. This is the cracking that can occur in the corners of your mouth. Many sources will tell you this is caused by a vitamin deficiency - like B-vitamins, iron, and zinc. Other times, it may be a wound caused by contact dermatitis from increases contact with the tongue or your hands, and then they may become infected with normal skin bacteria or other bacteria in saliva. An infected wound is one that doesn't ever appear to heal. Fungal infections, in the same way, cause the skin to crack open and appear overly dry and never-healing.
Lie Bumps
Transient Lingual Papillitis (swollen taste buds). They can appear to be white or red, and they can be asymptomatic or very bothersome. Not sure what exactly causes it. Definitely NOT caused by lying. *I used to think they were "lye bumps" as in sodium hydroxide that is a strong base and used to be popular as a detergent.*
Cleft lip/palate
A birth defect that has a strong genetic component, but also linked to environmental components that have not been pinpointed yet. A cleft lip or palate is a result of parts of the mouth and face not fusing together during fetal development, and requires surgical correction after the baby is born. The oral and nasal cavities are supposed to be separate and when they are not, it can increase the risk of sinus and ear infections. Ear tubes are usually recommended.
Even after repair, a child may require speech and occupational therapies to develop the muscles needed for normal speech and eating habits. Many times, a follow-up surgery is required as the child grows, and many other types of mental support are needed.
Bonus
*Mouth Cancers: the most common cause of mouth cancers is tobacco use (smoking, chewing). It can start out as something that appears minor like a mouth sore, but can develop quickly into something deadly. In the end, it can result in large areas of the mouth having to be surgically removed.
Callback
Probiotics
Connect with me
Support us on Patreon
Give us your Feedback
Join the Pharmacist Answers Podcast Community on Facebook
Subscribe: iTunes, Stitcher, GooglePlay, TuneIn Radio
Like the Facebook page
Music Credits: Up In My Jam (All Of A Sudden) by - Kubbi https://soundcloud.com/kubbiCreative Commons — Attribution-ShareAlike 3.0 Unported— CC BY-SA 3.0 http://creativecommons.org/licenses/b...Music provided by Audio Library https://youtu.be/tDexBj46oNI
A new episode from the Pharmacist Answer Podcast!
0 notes
Last Seen Blogs
fireheirs
stardust

duskendales
and your lillies of snow

chronicbethany
Untitled

onelifetolivesblog
One Life To Live

animeaffinity
Anime Affinity