#an irradiated people
Text
One time on my parents' old Macintosh, I made an irradiated people kinda thing, except with different colors and an extra layer of complication. It had some kind of "weirdness" selector that made it freak out. You'd select the kind of weirdness and then it would just kind of warp, I think. And the color scheme and weirdness scheme would sometimes synchronize (make it look less weird, I think?).
It was maybe the coolest thing I'd ever created, and I was very proud of it. So much so that when a friend visited a couple weeks later, I proudly showed it to him. In retrospect I'm sort of surprised he didn't get creeped out by it, but he was really impressed and everything.
And then, one day, I was just minding my own business, staring vacantly at a piece of paper, when my parents said, "Hey, Joe, do you remember that weird irradiated people thing we made back when we had that old Macintosh? Your friend saw it and was really impressed by it."
I had no memory of making this irradiated people thing. Every aspect of it was a mystery to me. It was a black hole of my consciousness. Why did I make this? Why did I take the time to do this? I must have spent days on it. My parents wanted to see it again, and I didn't even remember seeing it the first time. And the part that's really weird is that I've only had two moments like this, that I can remember, in my life -- not moments of amnesia exactly, but moments when I remember being certain I remember a specific incident (being sure I remember it, down to what it was like and who I was with) . . . and then, after further reflection, I can't find any memory at all of it. I know something happened, and I know I was certain I was certain, but I don't know what.
For example, here's what I remember about the other incident: I remember being at a picnic in the park. I remember being with my friend Tim, and that we were playing a game that involved two people trading places between circles of people they knew and saying stuff about themselves. It was very fun. And I remember having fun with it and then suddenly becoming aware that I was sitting on a bench that had a fairy-tale illustration carved into it, a bench that I had noticed a few times before and always thought was cool, but had never actually bothered to examine. The bench was carved into some kind of sculpted wood, and the wood was polished, so it had a kind of smooth, reflective sheen, and I saw that the wood looked like it had been carved into the shape of a face. A lovely, exquisite, fairy-tale face, all curling, rounded lines, no hard angles or anything, no sharp edges or points or anything. It was a face of something -- I don't remember what -- that looked like it was suspended or floating, like it was in the process of becoming something else. And then, just as suddenly as I had become aware of this face, I disappeared from the bench and, presumably, from the picnic altogether, and was standing alone in a small, empty room in my house, staring at the fairy-tale face, trying to recall what it was from. And I'd stare at it in this room in my house, and I'd look away, and then I'd look back, and eventually I could see it, and see what I had seen, but the fact that I had seen it vanished, and I was certain I was certain I was certain, but all the memory I had was a memory of staring at something beautiful, a memory that I had spent years on, again and again, with no direction or meaning.
I know it is possible that I made it up, or that it never happened. It is possible I can't remember because I don't care. I know I have forgotten a lot of things, and this is just one of them. (And yet, in some way, I have the impression that these two things -- the irradiated people thing and the fairy-tale face and the picnic and the bench, the "revelation" that I spent years thinking about and staring at something beautiful and pointless -- are closely connected. But I don't know that, I just have the impression of it.)
It's a hard thing to explain. I've had two of these "revelations," that I can remember. And I have no idea why I don't seem to remember this stuff.
5 notes
·
View notes
Text
for the purposes of this poll, the death doesn't need to be painful or even wake you up, but it should be a definite death. dying and then immediately restarting the dream or entering a different dream also counts.
i used to die 6 to 7 nights per week and now i'm down to 2-4 depending on how stressed i am but i'm told that that's still not a "normal amount." how common are death dreams actually. let's find out
#tumblr sample means a bunch of other autistic people with ptsd so#from a scientific standpoint very skewed. from a kitkat baseline very normal#dreams#last night i was in a submarine programmed to plummet below crush depth#the night before that i was irradiated to death. the night before that i killed a bunch of people and myself in a car accident#etc. i've died in so many fun ways and remember so many of them so well#death
109 notes
·
View notes
Text

proof that haylen is an actual ray of sunshine
#one of the only people still in the brotherhood I can stand <3#scribe haylen#fo4#fallout 4#fo4 fanart#fallout fanart#irradiated art
58 notes
·
View notes
Text
It’s SPOOKY SCARY SKELETONS MONTH
So let’s talk about yer bones! Yeah, that’s right, Captian Holt. I said –
An adult has (roughly) 206 bones (I say ‘roughly’! You can have non-pathological anatomical variation, such as lumbarised sacral vertebrae (an extra bone in your back) or accessory sesamoids like the flabella (a little bone at the back of the knee!))
A newborn has (roughly) 300 bones
That's a big difference! Almost 100 bones of difference! Where do they go?
Well, you see - as you get older, every time you come into the hospital we steal more of your bones...
Just kidding.
...Or am I
As an embryo, your skeleton is completely composed of cartilage. This gradually ossifies as you age, until, as an adult, you have a full skeleton, with only the interactive portions of joints being capped with hyaline cartilage.

[Paediatric normal whole leg radiograph, showing epiphyseal plates around the head of the femur, the femoral condyles, the proximal tibia, the distal tibia and the lateral malleoli that can mimic fractures. Courtesy of radiopaedia]
See all those weird blobs? Those are bones in the process of fusing together! The transverse lines that could be mistaken for fractures are actually epiphyseal plates – hyaline cartilage bridges between the shaft of a bone and what will become its tip, which don't attenuate x-rays, and thus appear black on our radiographs! This is where bone growth occurs - the cartilage forms a sort of template matrix that then ossifies into bone.
Compare our paediatric radiograph to the AP knee radiographs of an adult with no visible pathology:

[Adult normal AP knee radiographs, showing fully fused bones. Courtesy of radiopaedia]
See how all those ragged pieces have joined up? That’s endochondral ossification, BABY!
This is how we can figure out the age of a paediatric service user from their bones! Certain bones form at different times.
Let’s check out the carpal bones – all those fiddly little bones in your wrist! Anyone who’s binged Hatecrimes MD – sorry, House MD as often as I have will know the classic acronym for remembering the names of these bones. Moving thumb side to pinkie side, we have…
Scared (Scaphoid - red)
Lovers (Lunate - dark blue)
Hate (Hamate - green)
To (Triquetrum - yellow)
Try (Trapezium - orange)
The (Trapezoid - light blue)
Coolest (Capitate - purple)
Positions (Pisiform - pink)

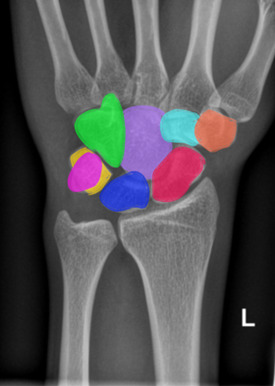
[Normal adult wrist radiograph, shown with and without coloured carpal bones. Courtesy of radiopaedia.]
But did you know that these bones form at different times?
The Capitate ossifies at 1-3 months
The Hamate ossifies at 2-4 months
The Triquetrum ossifies at 2-3 years
The Lunate ossifies at 2-4 years
The Scaphoid, Trapezium and Trapezoid ossify at 4-6 years
And the Pisiform ossifies at 8-12 years
So, I can look at this picture, and tell you that this child is approximately 3 years old, because their Capitate and Hamate have ossified, and their Triquetrum is just visible, starting to ossify below the thumb (circled!)

[Normal wrist radiograph of a paediatric patient, triquetral ossification centre circled. Courtesy of Radiopaedia.]
Your bones continue to form and fuse until you reach about 25! Your olecranon (the bump of your elbow) starts to ossify at 6-11 years, and fuses at 13-16 years! We can look at the base of your fifth metatarsal to age afab folks who are approx. 10 and amab folks who are approx. 12, as this bone fuses in the 2-4 years following these ages! The medial end of the clavicle can be used to assess your age from approximately 18-22, and your facial bones continue to ossify into adulthood! How cool is that?
If you’re over 25, fret not – there’s still plenty of funky stuff happening to your bones. But we’ll get into all of that next time, when we take a look at the function of osteoblasts and osteoclasts and explore all the cool little jobs that your bones perform within your body - it's more than you might think! So, tune in next time for more Bone facts...
And thank you for reading!
#medblr#halloween#spooky#skeleton#science side of tumblr#radiography#radiology#medicine#human anatomy#x rays#radley irradiates people#spoopy
27 notes
·
View notes
Text
going into certain tags on this shithole app is actual hell. some of you need to learn not to tag every shitass thought that comes out of your brain
#if you tag things for blog organizing purposes then figure out a unique tag for just your blog#i'm sick of wanting to look at pictures of my irradiated husband and having to see like#50 posts about how much people hate such and such ship or whatever#shut up! i don't care! keep it on your blog!#i'm a hater today sorry
4 notes
·
View notes
Text













Salt and Ruins
#horizon forbidden west#hfw#hfw photomode#hfw burning shores#the third one kinda looks like those pictures in travel ads#come to the burning shores!#we have unspoilt empty beaches!#clear seas!#vibrant nature!#a dinosaur park!#lava!#murder frogs!#a horus smashing up a few ruins!#a predatory creep brainwashing people and trying to get a good grade in irradiating the entire place!#....actually maybe that's not a good selling point
9 notes
·
View notes
Text
Aw man, just reread my document I wrote on my speculation on how the metagene works & how modern DC could rewrite it to being a result of retroviruses & transposons and man, I really wish I finished that post.
Unfortunately, the reason I stopped was explaining it all down to the point where someone with little genetic knowledge could still understand it proved to be too lengthy and long winded of a task.
Maybe one day I’ll pour myself back into research & finish that speculative paper. Bc I had a whole fun idea that relied on that background information that was about the Daily Planet reporting on the discovery of an entire city of metas with similar meta abilities. The town faced such high levels of radiation and contamination, only the population with the meta gene survived:(
#The meta ability was just super perfect cell replication.#No changes outward. They appear perfectly normal#to be clear. ppl still age. the power is just that their cells are super good at replicating the way they’re meant to#Zero chance of tumors or damaged DNA due to the radiation because their meta ability just resumes them to their previous state.#the city blows up afterward in the news cycle due to people trying to go there so they don’t die from cancer.#and don’t have a risk of cancer BUT THE CITY IS STILL IRRADIATED AS HELL AND THE PPL THAT ENTER CANNOT LEAVE#DUE TO THEM BECOMING SO RADIOACTIVE THEYRE A HAZARD TO BE CLOSE TO WITHOUT PPE#i just thought it was such a fun idea and me being me I overthink the shit outta things & made it super long and overcomplicated#because I wanted people to also learn what retroviruses & transposons were bc they’re cool as hell#and by the time I wrote 5K words on it#I didn’t want to take the shortcut and just embed other ppl’s videos explaining it bc I had already put too much effort into it#for me to delete that research#bones speaks#the cause? the city was built ontop a large kryptonite meteor.#and someone (cough cough LexCorp. but no one actually has enough legal proof to say it’s them)#and when it’s investigated. it appears that someone (cough cough LexCorp. there’s not any legal proof that can pin it on them.#so lexcorp once again escapes scott free without evidence of villany)#has been digging tunnels under the city and excavating it. the excavation not following proper mining protocols caused the city’s ground#and water supply to become extremely irradiated to the point where it’s like when ppl were just eating & drinking uranium products.#actually imma stop myself here & make this it’s own post#anyways. the radioactive bit gets figured out due to the poorly constructed tunnels collapsing and the city conducting an investigation#leading to a ‘oh shit. the Geiger counter is saying this sinkhole is Super radioactive.’#to ‘HOLY SHIT THATS THE ENTIRE TOWN’#to ‘wait fuck how are we still alive? to ‘a weirdly high percentage of folks in the town had metagenes so not a super significant amount#of ppl has died from abnormal lookin cancer.’ to ‘oh my god everyone that doesn’t have the meta gene here is slowly dying get them Out Now’#bones writes in the tags#anyways. that’s kinda the story#I’ll rewrite the tags into a proper post and see if I can revise it so my paper isn’t needed to make some plot points work#bc it’s a Far simpler explanation than the one I wrote in the doc so I’ll base it off of this version instead
4 notes
·
View notes
Text
i think my brain is skewed bc i was going thru and voting on the morally grey girlboss polls and like??? do y’all not know what morally grey means??? annabeth chase was on there?? homegirl is 16 and has literally never killed anyone so how is she remotely morally grey?? and elizabeth swann?? only ever threatened to kill the british (valid) or killed jack sparrow after he tried to do a group bonding activity of being condemned to painful death (also valid) like cmon y’all. girlboss yes, morally grey no or maybe but valid
#i might also be biased bc i’m watching the 100 rn and clarke has killed minimally 600 people#but probably more#like she irradiated an entire nuclear bunker with children in it y’all can’t compare to her#clarke griffin#annabeth chase#elizabeth swann
2 notes
·
View notes
Text
how long has google been putting ads in the email inbox
if you don't use an adblocker, literally how do you live. serious question.
#liz blogs#why are you willingly walking around the lethally irradiated Advertising Wasteland with no protective gear#i've been using adblock for 13 years but i had to turn it off to troubleshoot something#and i opened gmail and not only was my inbox divided up but there were ads like every 10 emails#and i became. so instantly enraged. before i remembered I Turned My AdBlocker Off#i just glimpsed the horrors oh my god thoughts and prayers to people who dont use adblock#i've been protected from the worsening encroachment of advertising into our online lives#adblocker and firefox i love you im kissing you#gmail ads have been around for a while on mobile but thats because mobile sucks and never should have replaced desktop computers#i'm used to mobile sucking ass. if you use a phone more than a computer you're deranged#you don't realize what you're missing. why would you break your own kneecaps like that. get a laptop or a computer jesus christ dude
4 notes
·
View notes
Text
trying to decide what to draw is literally the worst
#mutuals’ oc(s) or bloodied up reed. this is a hard decision#meanwhile im still mentally stuck in my ‘how would mulled wine be made in fallout’ wormhole adventure from yesterday#like. is there citrus fruit available? is that still a thing that exists? are people still drinking 200+ year old musty irradiated wine?#im too invested in as a person that doesn’t even like wine#alana.txt
5 notes
·
View notes
Text
Loving my depressive state and all but I would really love to get out of bed and enjoy my hobbies again. 67 days left of this and I’ll be back to normal
#apparently younger me was not exaggerating when she said living with my parents is exhausting#i got 67 days until I move back to college#they cannot pass fast enough#i was super excited to play vr today since I’ve got the day off and then as soon as my mother walked in the door I just like.#lost my will to exist. I’ve been laying in bed ever since#like bro please#ugh and I knew that would happen too. like please please I need to live alone again#i don’t mind living with my dad but like oh man my mother. we may have only exchanged a few friendly sentences today but like#that is irrelevant. what’s the one post about mothers and irradiating the vibe ? yeah whatever that was it’s right#at least I have a job so I go out to there. but unfortunately I gotta go thru her bc I need her car#i just wanna feel ok again!!! i never laid in bed in college I miss college#college will also bring me croix hair which is pretty epic#but like literally like please oh my god get me out of here#i just wanna get out of bed but I do not have the energy when people r home. no wonder she thinks I don’t do anything#soup talks
10 notes
·
View notes
Text
had to unfollow someone I really liked cause they support nuclear power and kept ragging on people who didn’t believe in it calling them ignorant and as bad as antivaxxers and it’s like man. I’m not dumb because I disagree with you. Radiation is fucking terrifying, and the idea that being scared of something that will proveably kill you in horrific ways is the same as being scared of proveably safe vaccines that save lives is a cruel mischaracterization.
#radiation is one of my biggest fears#and I’m absolutely anti nuclear power#because three mile island and chernobyl showed us that human error can always override machine safety#and fukishima showed us that even the safest machines can’t survive every natural disaster#like I don’t support fossil fuel power but jesus#like the bp spill was terrible coal accidents are terrible#but oil spills can be cleaned up. you can wash rocks and animals even if it takes a long time#and power plant accidents are tragic but the people that die are confined to the people that die in the immediate incident#nuclear power accidents? oh no it doesn’t work like that#wherever the radiation touches is contaminated#and the highly irradiated areas? unlivable within our lifetimes. within tens of thousands of our lifetimes#and the disaster isn’t just contained to the incident. yeah some people may die immediately from regular causes#some may die from radiation poisoning#but radiation causes cancer. there are people who survived these events who are dying from it now#because regardless of what they’ll tell you — THERE IS NO SAFE AMOUNT OF RADIATION#even the smallest amount WILL change your dna#the smaller amounts are more likely to change junk dna that doesn’t actually code for anything sure#but any amount has the possibility of changing dna that will lead to cancer#and you wouldn’t even know until 40 years later because that’s how long on average it takes the cancer to develop#and even then the disaster can STILL KILL PEOPLE even after the disaster is over!!!#there were russian soldiers in chernobyl who dug up the wrong dirt and got radiation poisoning#the reactor is concealed within two separate containment buildings but the disaster can STILL KILL PEOPLE#it’s not safe there and for all we know all of humanity could be dead before we’d be able to live there again#solar and wind have their problems sure but#nuclear just isn’t worth it because all you need is ONE fuckup for things to go wrong for so many people for so long
7 notes
·
View notes
Text
PATHOLOGY OF THE URINARY SYSTEM (aka: STUFF WHAT GOES WRONG WITH YER PISS BEANS)
(AND YER PISS TUBES)
(and the pretty pictures I take of them)
[a warning: this post contains radiographic images and non-graphic description of serious kidney pathologies, including paediatric cancer]
Let's kick off with an old familiar friend! Yeah, I'm talking -
UROLITHIASIS (the humble kidney stone!)
Wanna know something horrific? The biggest kidney stone on record weighed over a kilogram. It was 17 cm across. Just. Imagine. Trying to piss that out…

Urolithiases are formed anywhere among your urinary tracts. They’re commonly found in the kidneys, giving rise to the more common term, renal calculi, or kidney stones.
Urolithiasis occurs when compounds within your urine crystallise. If your urine becomes too acidic, too base, contains too many of these compounds for them to remain in solution, or simply… sits around too long without flowing, it literally petrifies into a solid lump!
Some unlucky souls are just… predisposed to developing them. If you have had a kidney stone in the past, you are far more likely to get another one in the future. There also seems to be a genetic link – so if someone in your immediate family gets kidney stones, you have a higher risk.
Kidney stones typically hang out in the pelvis of your kidney and don’t cause an issue. Until you try to piss them out. Remember our kidney diagram (drawn on a conveniently shaped bean)?
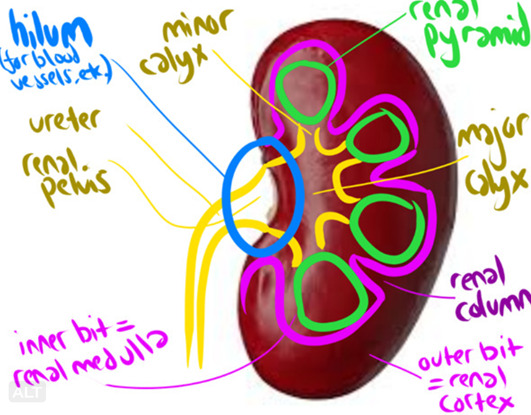
You might notice that the ureters are significantly smaller than the renal pelvis. In other words…
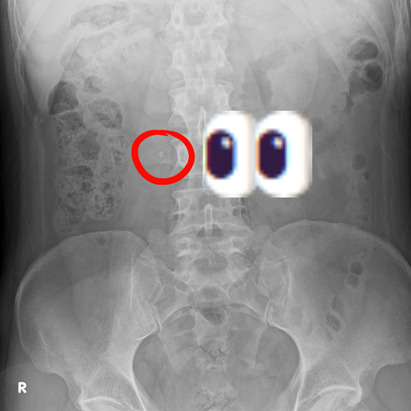
Most renal calculi are made of CALCIUM (oxalate, usually). This is very, very good (for us. Less so for you) because calcium attenuates x-rays – meaning, it glows all pretty and shiny when we take a radiograph!
Here’s a kidney stone on an Abdominal X-Ray!
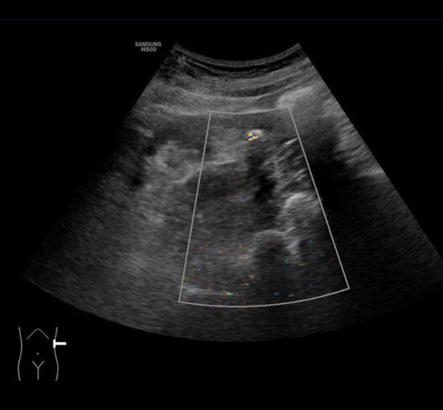
And a twinkly artefact caused by a kidney stone on Ultrasound!
But the best way to assess urolithiases, is, of course, with CT!
For realsies. We don’t need to inject contrast intravenously, because the kidney stones are (typically) shiny – which cuts down on time and worry, as it means you’re at no risk for having an adverse reaction! So a CT KUB (checking Kidneys, Ureters and Bladder for stones) is basically just a quick tumble in the washing machine (CT scanner), with a lovely clear picture as a result!
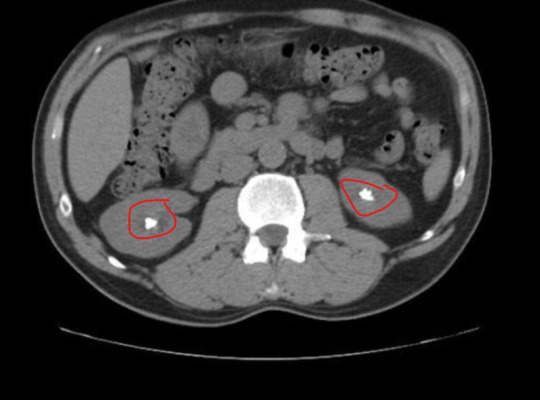
Look at these babies!! So sharp!!! So clear!!!!!! So shiny!!!!!!!!!!!! That’s a beautiful matching pair of renal calculi right there – and to make things better, they’re (currently) non-obstructive, so this patient isn’t in suffering The Agonies!
Speaking of The Agonies…
Most kidney stones are passable, albeit with extreme pain.
However, some ain’t going anywhere. Especially staghorn calculi, which, um. One, stags have antlers. Two…


more like a fuckin' MOOSE ANTLER amirite????
But yeah, those buggers aren’t coming out. That’s almost definitely going to require surgery!
Smaller calculi can still cause problems when they become obstructive – i.e., they block the passage of your peepee. They can lead to:
HYDRONEPHROSIS (dilation of the renal pelvis due to retained urine, seen here in the Left kidney [right side of image])

HYDROURETER (dilation of the ureter)
So, what do we do with bothersome calculi? How about some...
EXTRACORPOREAL SHOCKWAVE LITHOTRIPSY (ECSWL, because we love a sexy little acronym here in medworld).
We blast the stone apart with shockwaves, from outside your body! Ultrasound turned up to 11! Unfortunately, it only works on certain densities of stone, and on small stones.
LASER LITHOTRIPSY
(same thing but…. ZIP ZAP LASERZZZZZ]
SURGERY – PERCUTANEOUS NEPHROLITHOTOMY (PCNL).
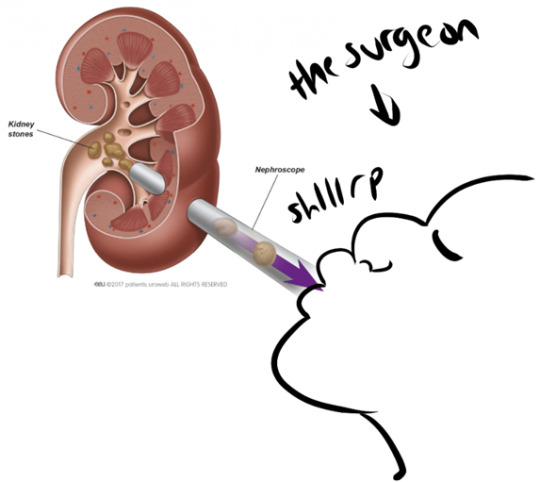
(I totally haven’t added to this diagram in any way. This is how it works. Trust me.)
LOADS of other stuff can go wrong with The Ol’ Piss Beans
We have:
RENAL CELL CARCINOMA
The most common form of kidney cancer.
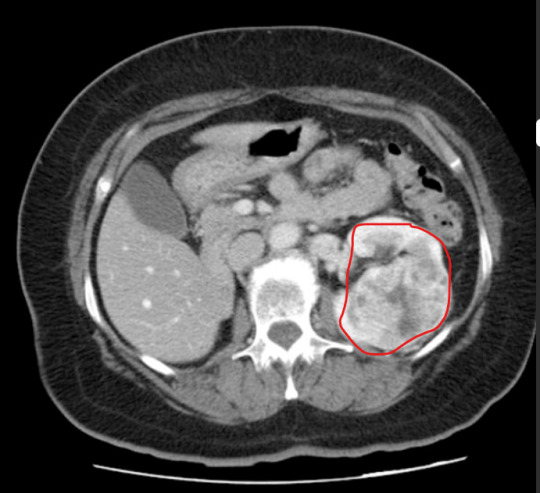
For suspected malignancies, we do a CT Urogram that assesses the whole urinary tract. This takes significantly longer than a KUB, but is well worth the results. This is a three-phase scan. We do...
A regular KUB non-contrast scan to check for calculi and to get our baseline Hounsfield Units ('grayness' and densities) for the kidneys.
Then we inject contrast in a 'split bolus' - one load immediately, and another roughly 8 minutes in, scanning roughly a minute after the second injection is given.
We scan 80 secs after the first contrast bolus is administrered, for the 'nephographic' phase, which enhances the renal cortex & medulla, and makes neoplastic changes and renal masses obvious (see image above).
Then we wait 10-ish minutes and scan for the 'excretory' phase, after the contrast has worked its way through your kidneys, to detect 'filling defects' (anything that stops contrast opacification of the ureters) and pathologies related to the urinary collection system.
NEPHROBLASTOMA
This is one of the more common cancers found in kids. Although paediatric cancer is never exactly a happy topic, this cancer is now curable in roughly 90% of cases, thanks to the early removal of kidneys and the possibility of transplants.
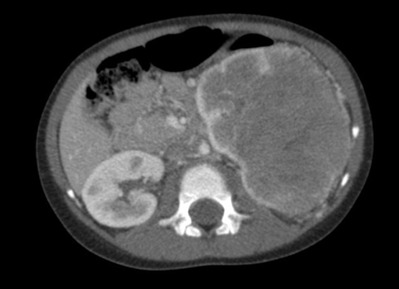
Autosomal Dominant (and Recessive) Polycystic Kidney Disease
An inherited renal disease that can cause you to go into End Stage Renal Failure due to the healthy tissue in your kidneys becoming completely overtaken by cysts. As a result, your kidneys can grow more and more, until they practically fill your whole abdomen. 45% of patients will be in ESRF and need dialysis by the age of 60. Thankfully, transplants are an option.

Other commonly encounutered renal pathologies include trauma, which I talked about in my first kidney ramble (linked here!), infections, and more.
I hope you enjoyed this whistle-stop tour of Stuff That Can Go Wrong With The Kidney, And How We Look At Them Gnarly Beans!
....And, um, I spent way too long making this and now need to pee. This is your reminder to go empty that bladder if you need to! Stop those stones!
12 notes
·
View notes
Text
I've brought this up before, but I refuse to write whatever they turned Emil Blonsky into in the more recent Marvel comics and the MCU.
The Abomination is a violent wife beater and an abusive prick that terrorized his wife and used to use her as his personal punching bag whenever he was in a salty mood (which was all the time.)
He has absolutely NO remorse for his actions and proudly brags about how his wife is his property and how he can do whatever he wants to her.
Nothing about this guy screams loving husband. Even GENERAL ROSS was more of a devoted husband who treated his wife like a queen compared to Emil Blonsky attacking his wife Nadia.
#gamma irradiated nightmare (Emil Blonsky/the abomination)#rave to the grave (out of character)#tw domestic violence#Absolutely can't stand seeing people fawn over Emil like he's a teddy bear
3 notes
·
View notes
Link
The reason why refrigeration has become the default, universally–accepted means of conserving food — and a defining symbol of modernity — is that it is really effective.
If, out of some moral feeling that people need to be “closer to nature”, and to “bring back the connection between different levels of living beings, we as human beings and food ingredients as other living beings“, you discourage people from using refrigeration, you are advocating a massive increase in the amount of food which goes to waste.
In wealthy countries where refrigeration is widespread, food waste by the consumer is modest. In fact, modern methods (including the preservatives and packaging that people may dislike but have come to expect) have greatly reduced loss to spoilage, insect damage, and so on. Most food waste occurs when perfectly good food is discarded by producers or middlemen, to protect their profits or because they have no market to sell their product.
The idea that refrigeration is a wasteful use of energy which must be curtailed is hard to swallow. If there are energy constraints in the future, it is not because there must be. It is because people have voluntarily chosen privation over cracking atoms ― more than likely, that they have made that choice for others. Encouraging the vague feeling that even the most obviously beneficial uses of energy are somehow immoral and unjustifiable encourages that kind of choice, the morality and justice of which we must in turn question.
We might mention here that, if you want to store food for longer without refrigeration, irradiation is quite effective at (for instance) retarding the sprouting of potatoes and onions.
Equally, “waste” heat from thermal power plants — which, in the future, will more and more mean nuclear plants, if fossil-fuel consumption is really to decrease — can not only be distributed to homes and businesses, but also converted into cooling by single-effect absorption chillers. Recapturing this energy and putting it to good use is a vital step toward making efficient use of our energy resources. And that is of far more benefit than any number of half-baked conservation schemes.
4 notes
·
View notes
Text


The Incredible Hulk (1968) #216
#ok… don’t really like the Hulk’s anger towards Ross here being framed as unreasonable but whatever#what really interests me here is how strongly the Hulk feels about saving the world in order to protect the people he loves#it was not that many issues ago that Bruce declared that he would not transform into the Hulk even to save the world#which obviously includes all of the individuals he cares about#though he did change his mind on that later that issue#it’s a sharp contrast between Bruce and the Hulk#and actually Bruce not wanting to transform into the Hulk even to protect someone he cares about isn’t even a new thing#I remember a story way back where Bruce just like watched the Absorbing Man transfuse some of his irradiated blood into Betty#because he was convinced that the Hulk would only make things worse#the Hulk doesn’t have anxieties like that he just acts based on his emotions and/or principles#which can make him more heroic than Bruce#marvel#bruce banner#thunderbolt ross#my posts#comic panels
2 notes
·
View notes
Last Seen Blogs

resetmnm
The Risette Munimi
diaryofarunninglady-blog
Run,Yoga,Vegan, Love

angelesclassified
Angeles Classified

blogsteveholmus-blog
Semaxin Male Enhancement:-Updated[2020]Increase Male Power pills

hianonsuper
Untitled