#i need to seek an eds diagnosis or something but i have no idea how to get that ball rolling
Text
going back into physical therapy for a third distinct injury caused by my hypermobility <3 probably starting in a couple weeks
#vv.txt#i hurt my ankle last august and didnt realise how bad it was but an mri showed it's a split tear in one of the tendons#so i finally finally had an orthopedic appt and got a referral for pt and a script for a lace up brace#but im wearing a boot for the next 2 weeks to keep me from continuously reinjuring the joint by subluxing my ankle#the doctor i saw was so nice though#like. i was talking about how ive been so worried all my various joint issues are My Fault somehow#and she was like no you just got dealt shitty cards it isn't anything you did#it was a big relief tbhh#i spend so much time feeling like my body is falling apart because i cant care for myself properly. but it's the other way around#i need to seek an eds diagnosis or something but i have no idea how to get that ball rolling
1 note
·
View note
Text
After dealing with it for years without realising I just got formally diagnosed with OCD.
I had no idea how much it is intertwined with all my other disorders. Like Relationship OCD makes my BPD/ social anxiety so much worse because the cognitive distortions become obsessions that I then need to neutralise with both mental & physical compulsions i.e reassurance seeking etc.
It also makes my PTSD harder to overcome because the OCD convinces me if I don’t complete a certain routine when leaving the house for example my loved ones will die - this is heavily linked to traumatic grief and the fear of not being able to say goodbye properly which has happened in the past.
Even though my Dad has OCD I never truly understood what it is because it’s so misrepresented and has so many different sub-types/ themes.
The rigid cognitive processing style inherent to OCD has also kept me stuck from truly recovering from my ED because I see things in very black & white/ ‘all or nothing’ and can’t fathom not being so strict with food rules or having self compassion because I’m convinced something bad will happen if I don’t follow my rules.
I’m glad I have a name of the disorder that causes graphic intrusive thoughts because I truly thought I was a monster or in some half psychosis - nope it was OCD.
I’m hopefully starting exposure & response prevention (ERP) therapy soon but I’m having a really hard time accepting yet another diagnosis. On the one hand I feel like I know myself a bit better now and I always suspected it wasn’t ’just anxiety’ causing my rumination spirals & intrusive thoughts but it’s hard because OCD is hard and so misunderstood.
Anyways, if anyone has experience living with OCD and what has helped you, please let me know! :) 🌻🩷
#obsessive compulsive disorder#actually ocd#ocd tag#relationship ocd#harm ocd#chronic mental illness#turtles all the way down
8 notes
·
View notes
Text
some things i learned while hospitalised
- that dizzy feeling you have when you stand up? that has to do with orthostatics, or your change in heart rate from sitting to standing. a normal change is 10-20 bpm, most people with ed's is in the 80s to 100s, the more malnourished (NOT underweight. those are different things) you are, the worse it is. this is bc your heart is weak and can't keep up with pumping blood through your body, it's not something quirky or fun, you could pass out and seriously injure yourself or have a heart attack.
- as i mentioned above, UNDERWEIGHT AND MALNOURISHED ARE NOT THE SAME THING. you can be 'overweight' and be malnourished, you can be a 'healthy' weight and be malnourished, it's not about weight it's about how you are fuelling your body. not getting enough protein and minerals can make you malnourished. not getting enough carbs and fat and sugar can make you malnourished. it's not about weight.
- laxatives are insanely harmful. i know we all say it. but it's true. your body won't be able to digest food properly, you won't be able to shit without them, the bloating and intestinal damage caused can be permanent. in hospital, they gave us stool softeners once a week if we really needed them because they are less harmful than traditional lax, but still not safe.
- the 'sick enough' mentality is BULLSHIT. i was admitted at an 18 BMI, there were people in there with overweight BMIs, there was only ONE girl who looked like the stereotypical hollywood '13 BMI' ED shit. if you are reading this post from your edblr, you are clearly sick enough to get help. ed's are not, and never have been, about weight. those who suffer worry about weight, sometimes, but the diagnosis and effects on our lives revolve around our relationship with FOOD. and the damage that causes our bodies and minds.
- there's a million different ed's. my official diagnosis is Anorexia (Binge/Purge subtype). i never made myself sick. i purged with severe exercise. what's the difference between that and bulimia? according to my doctor (who i slightly disagree with) it's about restriction, as supposedly bulimics don't restrict, only binge/purge. i didn't know there were different types of anorexia, let alone OSFED, AFRID or PICA. and even those can be broken into subtypes. the point im trying to make is: not everyone binges, not everyone restricts, not everyone is worried about body image, not everyone exercises, not everyone purges. EVERY EATING DISORDER IS DIFFERENT.
- you never fully recover. ever. just like any other mental illness, you can treat symptoms, you can get therapy, you can build a healthy relationship with food and self, but every once in a while, those thoughts will always come back. it gets easier to push them away, to treat them like fleeting thoughts, but they're still there. im not saying this to scare anyone away from recovery, if you're thinking about it, PLEASE RECOVER. most things go back to normal-ish, things do get better, but there seems to be an idea that recovery is black and white. it will be hard, you will have days you want to relapse, you will never fully get rid of the thoughts, but you sure as hell can quiet them. recovery is always worth it, and every single person deserves it.
- men with ed's are more likely than you think. the actual statistic is estimated at about 50/50. what's the difference? men tend not to seek help. trans men are at severely higher risk for eating disorders than cis men or women. those gym bros who work out 24/7 and only eat protein? that's an ed. maybe less obviously, most teenage-early adult men don't eat all day, and then have large amounts of food at dinner. my roommates, for example, don't eat all day, then will have take away from 3 different places, a family box or cereal and two boxes of mac and cheese in what is, effectively, a binge. but they don't count calories, they don't really worry about body image. because ed's aren't about that. it's about your relationship with food.
- you can and will stunt your development if you're a teenager. your body won't produce the needed hormones from puberty (including growth, muscle/bone development, and sex characteristics) when malnourished, meaning you can fuck up your strength, bone density, height, and pretty much all other aspects of puberty with an ed. that never comes back. recovering when you're older than puberty age won't make you suddenly start to develop. you will, essentially, be stuck in a semi-developed body for life. one girl in hospital was on an estrogen supplement because of this, it helped her to get a little stronger/develop a little bit, but no where near what it should have been.
basically: eds are scary shit and im so sorry to anyone who has had to go through it. please don't ever take your disorder lightly, it could kill you. you are always worthy of recovery. you are loved, you are important, you are needed in this world.
#anorecsick#tw ed shit#anorexjc#tw ed tumblr#thinspration#thinsinpiration#ed stuff#thinspri#anoressic#anna miaa#annarexya#annorexxa#just ed shit#male ed#pr0 ed#not pr0#not pr0 ana#not pr0 just using tags#notprojustusehashtags#ed recovery#edblr#gray rambles
1K notes
·
View notes
Note
hello! I hope this ask is not a bother, but how did you figure out you have eds? like, how did you get figure out your symptoms are due to eds and not something else?
I dont mean this negatively, I hope it didn't come across as that. I'm asking because a lot of symptoms overlap with multiple things. I've been experiencing what I believe to be hypermobile spectrum disorder, symptoms I've had my whole life but have been getting a lot worse. my family has a history of disorders which cause joint pain, even at a young age, but i wonder if in my case it's due to hds because I'm also very flexible.
if you wouldn't mind, I think it would be very helpful to know the thought process that led you to identifying your disorder. again, only if you wouldn't mind answering! and thanks in advance.
i am SO SORRY for the late reply!! i wanted to take some time to think about how to answer this ask since its kind of complicated
i dont actually have a diagnosis for eds (i have been trying to get one for Years but you know how it is. the average time is 10 years to get diagnosed)
long story short i always knew i had some form of hypermobility because.... my body is hypermobile.. and because my mom also has a form of EDS. (i have no idea if she is diagnosed but she has skin symptoms that i don't have)
i do have a diagnosis for "hypermobility syndrome (loose joints)" <- direct quote of what is written on my file. which is frustrating because i feel like it doesn't fully encapsulate my symptoms, similarly to how your experience sounds. i also have POTS, migraines, stomach problems, and intense chronic pain which go alongside EDS. I'm currently seeking an EDS diagnosis but I'm assuming it will take at least 2 more years.
i really appreciate the message and i apologize again for such a slow reply! i would encourage you do to lots of reading and research about EDS and your symptoms! for example, i didn't know POTS was a comorbidity (appearing alongside) with EDS, and once i realized, i was like wow..... i definitely have this LOL............
EDS really feels like a jigsaw puzzle because of how many symptoms and overlapping symptoms and comorbidities there are, but i support you so much in figuring out your condition!! i really hope you can make progress and get the treatment/relief you need
5 notes
·
View notes
Text
Ok my dudes, dudettes, & various cryptids, we gotta talk about something. A health something.
So if you've followed me at all, you know I have vEDS & that my hypermobility is pretty gnarly in that my joints are stupid levels of unstable. I think many of you have probably caught on to the fact that I wasn't diagnosed until pretty late in the game... like 4 yrs ago when I was 30. For as bad as my symptoms are, I should have shown significant symptoms & signs as a youngster, someone should have noticed, right? It seems super sketchy that I have a lifelong genetic disorder in a really bad way but nobody noticed til I was 30.
I definitely get that. That shit is sketchy as hell, unless you know how I was raised. Allow me to shed light upon why I'm a weird outlier regarding treatment/diagnosis of EDS.
I guess let's start at the beginning. I was born to a workaholic man & a schizoaffective woman who was upset that I was not a boy. When the doctors pulled me out, my hips were dislocated entirely. Like just dangling. But my mother was so "distressed" (aka throwing a crazy bitch fit over something insane) that they didn't want to trouble her or my father with it. They told my dad's mom. She... told nobody.
As a baby/toddler/preschooler, I fell. A lot. Like, an abnormal amount & for seemingly no reason. My knees & elbows bent backward. But dad was always working & mom was crazy.
When I was 4, they split, & dad got with my stepmother.
The first memory I have of this woman is her laughing at 4 yr old me & calling me stupid with an amount of venom in her voice that I was used to from mom (who still hated me for not being a boy). Why was 4 yr old me stupid & deserving of ridicule? Because I'd never seen french toast, but knew what toast was, so I made the toast connection & tried to eat the sticky mess with my hands. You know... LIKE TOAST.
Anyway, i remember my entire childhood having neck, back, & joint pain. The joint pain would get so bad that elementary school aged me would cry myself to sleep most nights. Dad was still always working & the stepmom told me that either I was faking for attention or that I just had the regular pains everyone has, I was just a baby & sucked at coping.
I can remember popping my hips partially in & out (obviously not knowing what I was doing) when I was absent mindedly thinking because I liked the noise it made. I remember the stepmom starting a nickname that stuck within the family for YEARS: flamingo girl because my elbows & knees went so far backwards. I remember the running family jokes about how I would be "just standing there, then fell over for no reason". I was told I was clumsy & so uncoordinated they were surprised I could get food into my mouth.
Still, I was told it was normal, despite nobody else having these problems.
My shoulder started sliding out of socket regularly on the playground or during normal activities during elementary school. The first time it happened at school, I went to the nurse. My stepmom reluctantly came to get me & take me to the doctor while telling me I was faking to get out of school.
When I was 7, I started getting pneumonia every winter. She berated me for having the nerve to be "so disgustingly sickly".
When I was 8, I started getting what looked like migraines every couple months, but was never taken to a doctor. I was put in a dark room with a cold compress & grounded for attention seeking. Around this time, schools still did scoliosis checks & found mild curvatures in my back. Nothing was ever brought up about that again.
When I was 11, my knee fully dislocated at school. I was told I did it on purpose to make her look bad. She had a friend who was a psychiatrist treat me for mental illness that I didn't have because the doctor, being her friend, didn't even speak to me. Just took her word for it regarding my alleged behavior & my mother's mental health. I was drugged & pulled out of school for an intensive outpatient program where I said nothing. Saying nothing was safest. The one time I spoke of her other outright abuse, I was punished.
All this time, my father was working himself to death because she popped out 2 other kids, bringing the count to a total of 4, & refused to work. He had no idea what was happening.
So I grew up thinking my body was normal, I just sucked at dealing with it. I didn't get any idea that it wasn't until my mid 20s but by then, I was a parent & was juuuust making ends meet, so I couldn't figure out what was happening, even if I wanted to. So I pushed through as my dislocations & migraine like headaches got more frequent & more devastating.
Then, around 30, after 4 organ ruptures of unknown causes & a lifetime of ignored dislocations, hypermobility, pneumonia, & migraines, my body had enough. Things really went downhill & it snowballed pretty fast. It still took until I was 32 to get a proper diagnosis.
Since then, everyone has been trying to play catch up. By that time, my tendons & ligaments had become so fragile that PT actually did a load of damage in the form of tearing. My hips & knees slid out slightly when I walked, resetting themselves when I put my foot back on the floor. I was rx'd a power chair (which I still waited nearly 2 years to get & still only use for long trips). I had serious GI problems. The migraines (which are tension headaches) were happening weekly (now daily).
So in summary, this could have been prevented with early intervention & proper care. But unfortunately I was the victim of abuse & negligence. And that, my dears, is why I am a weird outlier.
If you take ONE thing from this, I hope it is that you pay attention & listen to your kids. Don't blow them off when they say something is wrong or you see evidence that something is wrong.
If you've made it this far, thank you for listening to my rant/explanation of how EDS can be THIS bad & go unnoticed for so long.
Also, there is no need for "I'm sorry" or pity. I know how hard my life has been & I went through a decade of therapy to get over the PTSD & such from my childhood. It's just an explanation & cautionary tale.
60 notes
·
View notes
Note
Hiya! I'm very thankful for you still answering my ramble^^ I do have depression so I have psych appointments weekly, and my psychologist also is a bit worried about me. Also, I'm autistic so I'm just very scared that i'd shut down at the GP's so I'm taking my mom. Also, I'm moving, so I'get a new GP nonetheless but I still just want to hear my GP say that he believes I'm really in pain? Idk, like, that he believes me? (Probs sending another one sorry >,
Also, Thanks @chronicillnessproblems for your input! I’m suspecting (H)eds or something similair. Also I’ve done a LOT of research on POTS and I read a lot of thing I find myself in. I’m gonna make a list with things I can’t do anymore and gonna take that when I go see him. Like, I’m almost 21 and I have to sit while showering, can’t ride a normal bike(only electric or else I’ll almost pass out) I sometimes have to stay home from work cause of the pain and ugh. Anyway, Thank you so much!
Oh right! Also, please feel free to post anything I send without response, I get how draining that can be^^ Byee!
Ok so I read these asks earlier this morning and I do want to say a couple of things, because I’m a little bit nervous about what you said.
First of all, I SUPPORT YOU AND WHATEVER YOU DECIDE TO DO. I really do. So what I have to say can be dismissed or ignored altogether and it will not hurt my feelings or make me any less supportive of you.
I DO NOT think you should return to this GP if you can help it. There is no doubt in my mind that you will be unable to convince them that you are experiencing pain. And I understand where this is coming from, I really do. We WANT to be affirmed by our medical care providers. It is super hard to battle our own demons and doubts in our heads as it is. But to have that nagging doubt that our doctor doesn’t believe us either just makes things 100% worse.
But they have made up their minds. And I don’t know your gender, but if you are a woman, this is something that is going to be happening to you repeatedly. Unfortunately there is a lot of evidence of medical bias against women that doctors refuse pain treatment to them using depression as an excuse. And this has a long history. I won’t go into detail but you can study up on the roots of “hysterical” diagnosis from last century and see where I am going with this.
Also medical practitioners can be assholes. And not only do they get to be assholes, but they get to document your visits anyway they choose and that information is now basically fact. Everyone used to joke about “permanent records” because that’s not exactly a thing. Except in this case it is.
This doctor can choose to label you as drug seeking, or “hysterical” or any number of things that will bias any future practitioners against you. Now being from the US I have zero idea how a fully functioning healthcare system is so I don’t know if your psychiatrist’s notes are also included in your medical records because here they are not. Which means this jackass’ notes will follow you for eternity while your Psychiatrists notes can get lost in the shuffle.
However, if you do choose to return to this GP, I would earnestly encourage you not to get your hopes up about them validating your pain. Since I’ve been sick I’ve had 3 medical practitioners that believed me out of 11. And this was after I had seen multiple specialists.
I ABSOLUTELY encourage you to take your mom. I am 43 but did not start getting the respect and treatment I needed from my doctors until I started taking my mom into the exam rooms with me. (She didn’t actually believe how dismissive they all were, which was the reason I took her in the first place, but suffice it to say the minute she saw what was going on, she lost her temper.)
I also would encourage you to get a letter from your Psychiatrist explaining that his PROFESSIONAL OPINION ON YOUR DEPRESSION is that it is not causing your physical pain. Your doctor will A. Be forced to argue with another medical professional. And B. be forced to add this letter to your medical file. Where it WILL become permanently attached to your current issues.
And this could be a phenomenal help later on as you do find new doctors.
Again, it’s your body and it is your life. There is no way I could ever have enough knowledge to tell you what you should be doing. I can only give you some things to consider from my experience, after going through this for almost 10 years now.
Please do not seek validation from someone who has already denied it to you. It will only hurt worse in the long run and cause more doubts. I have spent many afternoons crying over crappy doctor’s visits and I’d hate to see the same for you.
Ok since you said I didn’t have to comment, I’m just going to go ahead and not edit this… I hope it all makes sense. Keep us posted, if you feel like it. You’ll be in my thoughts.
Admin J
PS Followers if you have anything to add, please feel free.
#admin j#jackass doctors#helpful followers#chronic illness#shout out to#chronicillnessproblems#my partner in crime#and actual founder of this blog#you're doing great sweetie#akimasu#eta#i lied#i did kind of edit#i apologize for any confusion#but just know that I start to confuse homophones#and spell things phonetically#when I am fatiged#hence the 'use' instead of you#which made me feel east coast#yous guys#idk#i'm rambling now
8 notes
·
View notes
Note
We all know that Mulder is insecure but Do you think scully has some serious security issue around Mulder too when it comes to having a romantic relationship with him?
In a word, yes.
Scully almost certainly has avoidant attachment issues.
She’d been brought up as a navy brat, never settling in one place for too long; never being able to establish a secure base with those outside her immediate family. As a child, she learnt that those close to her would at some point be ripped away and so the pain of that probably taught her to keep a safe distance from others.
She confesses as much in season 5′s Christmas Carol.
It isn’t just about how she would have repeatedly lost friendships and other significant relationships from moving around - it goes deeper than that. In season 7′s Orison, there is the poignant story Scully tells of how she realised that evil exists in the world when her Sunday School teacher was killed in his front yard. She was close to this man, and he was taken away too. She learnt very young that not just distance, but also death robs you of those you love.
Because she fears forming attachments to those outside of her immediate family, it places a far greater strain on the attachments she does allow for herself - namely the relationship she has with her father.
She idolises him and the romanticism of his naval career - he’s her hero. When re-watching Ghost in the Machine for my most recent analysis post, I noticed that when Scully was in bed, there was a book she had fallen asleep reading, and so I Googled it.
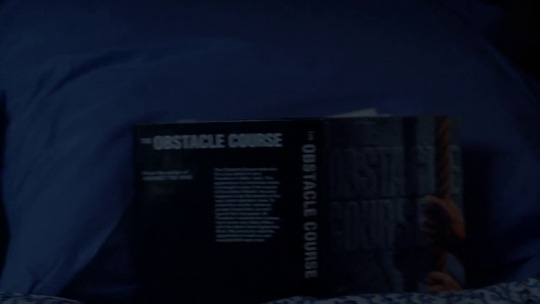
This book, “The Obstacle Course” by J.F. Freedman, is about a down and out boy who befriends a navy admiral who helps him to turn his life around by going to the Navy Academy. Hmm!
She really does live and breathe her father’s legacy - as she says herself in season 4′s Never Again…

So in the absence of others, all her emotional needs were channelled into her relationship with her father. He became her entire world. He was incredibly proud of her becoming a doctor, and so when she jacked a medical career in, to join the FBI, she could never fully reconcile the crushing feeling she had disappointed the one person she desperately craved the approval of.
She says to Ed Jerse in Never Again, that she craves the approval of controlling, authority figures because they are proxies of her father. This need has haunted her, because she never got the approval she needed from him when joining the FBI. It’s no wonder she ended up in several relationships with older, authoritative men, from whom she also sought this same approval. As she admits Ed and to herself - her life has run in a circle of constantly seeking out and then rebelling against “other fathers”.
First (that we know of) was Daniel Waterston - one of her teachers in medical school. She has an affair with him that, interestingly, she ended once she decided to join the FBI and he voiced his vehement disapproval, just like her father did.
The next relationship she finds herself in is with her FBI instructor. Jack Willis. Another older man in a position of authority; a teacher who she could gain the approval of to fuel this need for validation and fatherly love.
It’s worth pointing out that the fact these men are her teachers is quite interesting too. A “teacher” is an embodiment of childhood authority, a figure that we are actively encouraged to seek the approval of - they are much like surrogate parents - surrogate fathers.
Never Again is an interesting episode, because it reveals a lot about how Scully might view Mulder. Does she see him as another controlling, authority figure in her life? I’d say… in the end… no. Haha… wait, wait!
We have to remember that Never Again occurs immediately after Leonard Betts and right before Memento Mori. It’s not known if she had her cancer diagnosis at this point, but I’d say that she is going through a huge emotional crisis in Never Again. I’d say, at the very least, she suspects her illness and is in the process of being tested. Whether she has the confirmed diagnosis or not, she is having to face the possibility she may have a terminal illness and so she is in the process of examining herself, her life, and her priorities.
She’s noticed this pattern in her life, and seen the damage it has done to her, and is now seemingly resentful - her time to rebel has come around again. She feels her life is standing still, and is rebelling against the figure she feels is, at least in part, responsible for that - Mulder.

During Never Again, she is examining her relationship with Mulder and finding herself irritated to the extreme when she observes any overlap in Mulder’s behaviour with the “other fathers” she later mentions to Ed. The controlling, authority figure who she desperately seeks the attention and approval of.
There are definitely echos of that, she has moments of needing Mulder’s approval, and there are definitely times when she is threatened by women who take his attention away from her. But I don’t think that’s how she sees Mulder overall. If she did, then why would she stick around? If Mulder was simply another proxy for her father, then she would do what she has always done when coming to this conclusion about the men in her life - which is end the relationship. Like she did with both Daniel and Jack.
But she doesn’t… why?
If Scully was ever going to decide that her relationship with Mulder was actually toxic and damaging to her and so leave him, this would have been it - facing terminal illness and realising he’s a controlling asshole. But she doesn’t… so she must come to some other conclusion regarding the tension between her and Mulder.
Which, personally, I think is something she’s probably felt for some time, but is only forced to acknowledge it when Diana Fowley shows up to - once again - take Mulder’s attention away from her. But this time it’s different - this time I think she can no longer avoid the fact that this tension between them is caused by the fact that she is in love with Mulder.
So, with all of this, it’s clear to see that Scully has a lot of personal demons which are going to be haunting her surrounding any kind of romantic relationship.
She trusts Mulder like no other and he has become a huge focus in her life. The idea of changing the nature of that relationship is going to be incredibly scary for her. Not only because she’s realised her feelings for him are not based on a need for a father surrogate, but something deeper that she’s never had with a man before, but also because she has this deeply ingrained belief that getting closer to him means she will lose him. That it won’t last. That, sooner or later, distance or death will take him from her. Risking that kind of pain is terrifying.
The tragedy is that pretty soon after she does initiate a romantic relationship with him (assuming that’s what happens off screen in All Things) she does lose him, first through distance in their separation, and then to death. Her worst nightmare come to life.
So Scully never gets closer, never overstep the mark - Mulder has to be the one to make the first move (Fight the Future). Occasionally letting it slip that she is attracted to him is about all she ever allows herself.

Even after they are together, you can see some of this stuff is still there for Scully. Fast forward all the way to I Want To Believe and you can see some of her defences still at work. She tries to end her relationship with Mulder before getting hurt - she’s protecting herself from the pain of losing him to his re-awakened passion for hunting the paranormal - by leaving him first.
So yes, in my opinion, Scully has a lot of security issues around having a relationship with Mulder. I hope that answers your question, Anon!
I would also like to add, that this is all my interpretation of things that may well be totally off the mark. I had been concerned about this previously, but it was brought to my attention more recently from some feedback I got, that a lot of what I say I might inadvertently present as some great revelation, but it’s actually all old hat that most people know already. So, apologies if it comes across like that. I am just putting it together in the way I know how, and I hope you all understand that this is only my interpretation of things, and that many others may have laid this out already and perhaps far more coherently than I. I don’t want this to seem like I claim any of my thoughts on the show as fact or canon.
Cheers.
239 notes
·
View notes
Text
DISCOVER THE ADVANTAGES OF BIOIDENTICAL HORMONE THERAPY

Age, illness, and anxiety may develop a harmful hormonal imbalance in the body that impacts your health, happiness, and capability to connect with others. These inequalities are so sly that you might not even recognize that you have one. Quench Health in Chicago, IL is your local resource for all things hormone. We provide first-rate testing and also bioidentical hormonal agent therapy to restore harmony in your life.
What Are Hormonal agents as well as Why Do They Matter?
We don't see them, however hormonal agents are always acting behind the scenes to make your body feature. Over 200 of these molecular chemicals flow through the body to supply messages to the organs. Telling your lungs to take a breath, heart to beat, as well as your belly to eat are among the many directions these chemical messengers offer.
Due to the fact that hormonal agents have such a vital role in the body, an inequality may toss your life right into a craze in unforeseen means. Hormone imbalances aren't always uncomplicated as well as may appear like various other problems. Obtaining evaluated and also treated for a hormone inequality is the very most method to reclaim your health, vitality, and wellness.
What Is Bioidentical Hormonal Agent Replacement Treatment (BHRT)?
Bioidentical hormone substitute treatment is an innovative approach to determining as well as managing male as well as female hormone inequalities. This approach makes use of plant-based hormones that have a framework similar to those produced in the body. Lots of people describe this hormonal agent substitute treatment as "all-natural hormonal agent treatment."
Hormonal changes may wreak havoc on your body, mind, as well as spirit. Often these changes are so refined that they creep up on you. Some individuals experiencing the damaging impacts of a hormonal agent inequality initially clarify them away as situational disturbances rather than acknowledging them as the biological changes they are.
Restore Your Life
Doing something about it to uncover the source of your pain is essential anytime you are facing undesirable adjustments in your physical or psychological wellness. At Quench Wellness, we use accuracy techniques to identify any kind of hormone imbalances or deficiencies in the body. After recognition, we supplement or change them with this restructuring treatment.
The objective of bioidentical hormone treatment is to restore your hormones to correct levels. Recovering your hormone levels enhances every area of your life. You may delight in adjustments literally, mentally, mentally, passionately, and also socially.
Just the most productive for Our Individuals
We utilize just the most bioidentical hormonal agents found in a therapeutic pellet type. The body may not discriminate between the bioidentical hormonal agents we utilize and those it creates naturally. You gain from this in several means.
What Triggers Hormonal Agent Discrepancies in Men and Women?
You should have to live your ideal life. Consistent hormone levels are paramount for living well. Hormonal agent imbalances might create impacts varying from slightly annoying to ruining. Despite where you fall on the pain spectrum, you owe it to on your own to seek treatment. Our objective is to help you feel like on your own once again.
Some typical root causes of hormonal imbalances consist of:
Cushing's condition
Diabetes mellitus and insulin resistance
Polycystic ovary syndrome (PCOS).
Perimenopause.
Menopause.
Menstruation.
Stress and anxiety.
Thyroid conditions.
Exactly How May Inform If I Have a Hormone Discrepancy?
Men and women may experience unpleasant modifications in their bodies arising from shifting hormones, as well as each of the hormones presents various symptoms. General signs and symptoms of a hormonal agent inequality are those that any individual may experience; however, there are also some signs details per sex.
General Manifestations of Hormonal Agent Imbalance.
Women and also males experience general signs and symptoms from a hormonal inequality. When adrenaline, insulin, and also development hormones change, they may produce undesirable signs and symptoms in any individual. When these kinds of hormonal agents aren't secure, you may experience:.
Modifications in body temperature.
Disrupted rest cycles.
Fatigue.
Greater heart rate.
Raised stress levels.
Impaired sex-related functioning.
Problems with reproduction.
Fluctuating state of mind.
Low libido.
Pain, tightness, or muscle mass weak point.
Weight gain.
Female's Hormonal agent Inequality Signs and symptoms.
The majority of ladies expect hormonal adjustments to occur throughout life due to the fact that they have actually experienced hormone changes every month since adolescence. Modifications additionally occur while pregnant, breastfeeding, perimenopause, menopause, very early menopause. An activating condition like polycystic ovary syndrome (PCOS), or key ovarian insufficiency (POI) might also usher in undesirable hormone shifts. Some kinds of contraception might additionally cause hormonal imbalances in women.
Estrogen and also progesterone are usually at the root of female-only hormone deficiencies. Signs particular to ladies are:.
Mind fog.
Bust changes.
Bust inflammation.
Clitoral augmentation.
Hair loss.
Headaches and also migraines.
Heavy periods.
Warm flashes.
Night sweats.
Vaginal atrophy.
Genital dryness.
Men's Hormone Imbalance Signs and symptoms.
Men aren't exempt from experiencing hormonal imbalances. Testosterone is often at fault when symptoms show up. Common male symptoms of a discrepancy consist of:.
Breast augmentation.
Body hair loss.
Body mass reduction.
Erectile dysfunction (ED).
Sperm matter reduces.
Do I Required to See a Doctor Regarding My Hormone Inequality?
Hormones have a fragile equilibrium that just a doctor may check and oversee. Because there are hundreds of hormones in the body, it's difficult to understand what's creating your signs without clinical testing.
If you have symptoms of an inequality, it's very easy to think you may handle the problem by yourself, but this isn't an excellent idea. Lots of other problems resemble the signs and symptoms of a hormone discrepancy, as well as we should dismiss all various other problems prior to therapy.
It is necessary to consult with your doctor for extensive screening to relieve signs and bring your body back into balance. As soon as we establish your diagnosis, we give accuracy treatment alternatives like HRT with BioTE to restore your health and wellness and health and wellbeing.
Benefits of Bioidentical Hormonal Agent Substitute Treatment.
BHRT is aiding countless clients all over the globe to restore harmony and also balance in the body. The benefits of bioidentical hormonal agent treatment are the leading factor they choose this therapy. Listed below we check out a few of the many advantages of using BHRT to manage hormonal agent inequalities.
You're Never ever Alone.
You are not the only one with BHRT. Modifications may feel terrifying, but our pleasant and professional group is with you every action of the method. We are familiar with you as well as your body to find the most competent methods to aid. When you take the primary step towards us, we'll take ten steps towards you. Our clients are our top priority, as well as we do everything we may to provide remarkable care.
A Lot More Natural Method.
BHRT mimics your body's hormones. Among the most considerable reasons this therapy is the recommended choice is that it's more all-natural than different hormone replacement therapies. BHRT hormones are synthesized from plants, and also the body embraces them. This therapy is also suitable for people sensitive to other hormone therapies.
Accurate Test Results.
You always understand where you stand. Hormones utilized in various other therapies do not constantly offer correct screening results due to the fact that they do not blend right into the body very well. Using BHRT means that when you treat your hormonal agent imbalance, you may properly track just how well the therapy is working.
Reduced Maintenance.
This isn't a daily hassle. With bioidentical hormonal agent therapy, you don't need to remember to take pills or take time out of your day for therapy. After we carry out treatment, females are good to go for three months, and also men will not require to return for approximately 5 months.
Handle Hot Flashes.
Hot flashes do not need to disturb your life. Warm flashes are never ever pleasurable, as well as you never ever understand when they might strike. You might feel fine one minute as well as the following you remain in a sauna. This bothersome sign may do work, rest, and also social involvements excruciating. BHRT decreases hot flashes so you may get back to living.
Stabilize Mood.
BHRT may make mood swings a distant memory. It's popular that hormonal mood swings may adversely affect partnerships; they may additionally take a toll on your self-worth. No matter which area of your life takes the largest hit from oscillating state of minds, BHRT may assist.
Clearer Ideas.
Reclaim your emphasis. Hormones could be at play if you are fighting brain haze, absent-mindedness, or memory issues. Do not reach for caffeine. Rather, publication an assessment with us to find the underlying cause of these adjustments. If a hormonal agent imbalance is impacting your reasoning, BHRT may bring you support to speed.
Much more Energy.
Seize the day. BHRT is here if you are tired of feeling tired. Exhaustion is a common issue shared by individuals experiencing hormonal imbalances. You might feel great in the morning but fear the lunchtime decline. When these plant-based hormones increase hormone degrees, you'll have extra energy throughout the day, all the time.
Protect Against Loss Of Hair.
Conserve your hair. Thinning as well as falling hair is a typical indication that hormonal agents aren't balanced. Individuals that do not understand that BHRT may help could chalk hair loss as much as genes or the natural process of aging. Choosing this treatment might help you maintain your hair.
Prevent Gastrointestinal Disruptions.
Heal your digestive tract with BHRT. Although they might not seem connected, hormones dictate your digestive system tract, and changing hormonal agents may set off IBS. Taking care of GI-related hormonal agents with BHRT may prevent excruciating signs from developing.
Stop Bone Loss.
Keep your bones strong with BHRT. Bone loss and also osteoporosis are linked to hormone shortages directly. We require our bones to bring our weight as well as obtain us to where we need to go. Caring for your bones with BHRT currently may prevent breaks as well as cracks later.
Much good Sleep.
Sleep like a baby. If your sleep isn't as unwinding as it when was, maybe an indication that you have imbalanced hormones. Rest loss isn't just a nighttime issue. The body mends itself when we rest and also feeling tired during the day may impact your relationships, task, and also security. Selecting BHRT may bring your body back to its normal, drowsy self during the night to maximize your total wellness and health and wellbeing.
Boost Pleasure.
BHRT battles sexual dysfunction. Hormones play an important function in sexual health. If sexual hormones run out whack, your enchanting life may experience. Men experience ED while ladies battle with genital atrophy and also dry skin; both may really feel less encouraged to participate in sex in any way. Dealing with the underlying hormonal source of these conditions might revitalize your sexual desire for a lasting pleasure enhancement.
How Much Time Will It Take for Bioidentical Hormone Treatment to Work?
BHRT isn't a brisk fix yet a long-term option. You'll discover adjustments as early as 3 weeks after your appointment. The optimal benefits of treatment may take three months to show up. Although the modifications aren't immediate, when triggered, you'll delight in alleviation for a long period of time.
Am I a Candidate?
Anyone that thinks they may have a hormonal shortage or hormonal inequality could be a prospect for bioidentical hormone therapy. Your treatment begins with thorough testing. We explore your hormone levels to discover what's creating your signs and symptoms. Patients with serious symptoms are particularly excellent candidates for this treatment. Those suffering from disrupted rest, night sweats, migraines, or other incapacitating symptoms benefit most from this hormone therapy.
Setting up an assessment with us is the very most method to find out if you are a candidate for BHRT. We need to meet with you in person to get to know you and comprehend what you're experiencing.
The article “ DISCOVER THE ADVANTAGES OF BIOIDENTICAL HORMONE THERAPY “ was published first on Quench Wellness
Looking for a Naturopath? Drop by Dr. Amauri Wellness Centre here in Toronto.
0 notes
Text
Homophily; More Than the Need to Belong, the Need to Relate

Photo by Amer Mughawish on Unsplash
The Social Media Connection
Everyone knows that dreadful feeling of isolation, some more then others, yet, we all know the feeling that no one around us can relate to the experience or emotion that we may be going through at the moment. We as humans desire interaction with others and not just any other individual we come into the presence of, but those who can relate to ourselves and those who have similar interests. Before social media connections were limited to one’s local community and direct family (Close, 2017), therefore one’s ability to connect to others they shared similarities with were summed up to family and neighbors. We have motives behind every action we take as well has for every relationship we share, and when others directly around us can’t relate to what we are experiencing we now can look to social media to fill that void. I myself used this method to help with getting through a period where I was lost confused and scared.
I remember in August of 2014, after 6 months of seeing specialists and several evaluations my son was given the diagnosis of Autism Spectrum Disorder and though I knew it was coming I suddenly felt closed off from my support network I always relied on. It wasn’t that they were not there for me, but they just did not understand how different everything had just become, and to be honest neither did I. No one in our family had ASD, so there was no advice we were all ignorant in how to help, and no matter how hard they tried they could never understand the fear I felt being in the dark of the unknown. The doctors did not put it lightly and I barely understood the terms they were using. I needed support and fast because I couldn’t support his needs if I did not understand them.
Homophily- The Need to Relate
I remember being surrounded by family and my husband who was also going through the experience with me, but yet I felt none of them could help comfort me. See perception differs among individuals and even in sharing the same experience with another doesn’t mean that you’ve interpreted that experience the same nor share the same emotions. The need to belong is summed up as a basic psychological need to feel closely connected to others and belong to social groups (Yonghwan K., Yuan W., & Jeyoung O., 2016). Homophily is an expansion on the theory that humans have a need for belonging as homophily is the idea that we seek out individuals who we share similarities and moralities with (Close, 2010).
I had that connection with others I already had my social group, but I needed someone to talk to who at least understood what a normal day looked like for my son, I needed someone to relate to. After reading more than any human should in a week, I took a break to scroll on Facebook and upon stumbling on a friends post I remembered seeing something about her having ASD in her family, so I fearfully typed a message to her as I did not want to offend her and her reply was that little light to brought me back from the dark. She set me up with a group of moms who not only were there to share their stories but to ease some of the stressors of how to gain the supports needed for my son.
In finding others who had knowledge in the area I was new to, I was able to feel support from people I never even met. I suddenly did not feel alone anymore and I knew I had a safe judgement free place to go when I needed to cry, ask questions, or even just to vent. I’ve experienced the benefits of homophily in social media and these benefits are seen everyday on social media as individuals who once felt judged or isolated can find others who can relate to and support one another. The girl who is bullied, the boy whose biology doesn’t match his identity, the mother of a deceased addict, the individual with the addiction, anyone can find someone to relate to one social media, but for every up is a down and even these safe places can suffer from judgement.
Platform Algorithms encourage Homophily
I found that the more I researched Autism Spectrum Disorder the more I would have page suggestions on Facebook, encouraging me to connect to groups similar to those I have connected with previously. As I continued to connect with different groups the story got a little deeper, as my son was prescribed a stimulant at the age of 3 and shortly after developed what was confirmed to be focal epilepsy. I started searching natural ways to treat ASD and epilepsy and an Ad for this group raising money and awareness called MFMM came up and again I found myself in the dark relying on strangers with similar experiences to aid in how to help my son. However, this group was met with hostility more than most I had come across, like I said every up has a down, but Facebook was continuing to suggest other groups focused on the same movement, and even with the skepticism and trolls the support and first hand experiences outweighed the bad.
Social media had taken all the madness I had read and the one group I had first joined and gave me a network of individuals who could offer advice, give guidance, and simply state I know how you feel and almost four years later in 2018, I decided to try a controversial medication only legal in some states with limited available information other then the mothers I spoke to for over 2 years and the stories I followed. Though I faced a lot of ridicule the support from the groups the platform algorithms Facebook kept directing me to and my sons team of specialists outweighed the hate, as I understood that those who don’t understand tend to reject and I was fine with the rejection as long as my support kept growing.I now have a page that I use to interact with others and help them on their journey, however I know that it was that connection with those in similar situations with similar lifestyles that encouraged me and helped me to overcome one of the most frightening experiences into the unknown that I have encountered.
Close, S. A. (Ed.). (2017). The dark side of social media : A consumer psychology perspective. ProQuest Ebook Central https://ebookcentral-proquest-com.library.capella.edu
Yonghwan K., Yuan W., & Jeyoung O. (2016) Cyberpsychology, Behavior, and Social Networking. 264-269.http://doi.org.library.capella.edu/10.1089/cyber.2015.0408
0 notes
Text
Masterpost: On calling characters autistic
Part 1: Whether you should explicitly call your character autistic, and how you should go about it
So, you have created an autistic character. You love them, you know their likes and dislikes and you are determined that this is going to be a positive and realistic portrayal of autism. There's one problem though - how do you let your readers know that the character has ASD?
Actually explicitly calling your character “Autistic” can be awkward. Maybe it’s because you don’t want to interrupt the flow of the story, maybe it’s because you don’t want to risk backlash if people dislike your representation of autism. Maybe “autistic” isn’t a word that exists in the world or time period of your story. So, do you have to say it outright?
There isn't a moral imperative to call your character “autistic”. One of my favourite autistic characters is never called autistic in-universe. But our blog is about encouraging accurate representation of autistic characters, and if you don't actually call them autistic...is it actually representation?
Should I call my character autistic?
Autistic characters in media are very important for several reasons. The media we consume contributes to shaping us and our worldviews. If someone reads books and watch movies which contain complex, realistic autistic characters, they’re more likely to 1) be aware of what autism actually is, and 2) see autistic people as human beings, and treat them as such. These characters are also important to autistic people themselves: seeing characters like yourself portrayed in a positive light can boost your self esteem and help you feel less alone.
If you make a great autistic character and you don’t explicitly call them “autistic”, it’s not guaranteed that everyone will understand that they’re supposed to be autistic. Many people don’t have a very accurate working knowledge of autism, and they might not understand that a character is autistic if they don’t fit their narrow, stereotypical view of what an autistic person looks like. Thus the people that would benefit most from this representation might miss it completely.
Of course, the choice is yours, but we would strongly encourage you to explicitly call your character autistic so that you’re 100% sure your readers will pick up on it. Ideally, this would happen in the work itself, but at the very least we would encourage you to make it explicit when you, the writer, discuss the character (on social media, in interviews, in synopses of your work). Bare in mind that if you don’t say it explicitly within the work, you are very likely to end up with readers who deny that the character is autistic because they don’t behave in ways that match their perception of what autism is - they fall in love, they speak, they don’t behave in exactly the same way as their autistic nephew does. It is preferable for the reader to be able to identify the character as autistic without needing to pay attention to the author’s writing outside of the work itself.
When?
So, it’s decided! You are definitely going to tell the audience that the character is autistic. When is the best time to let them know? Telling the audience does not have to be the first thing you do when you introduce the character - it depends what you want to do with your story.
Here are a few general possibilities:
When the character is introduced - immediately telling the audience that the character is autistic means that the character’s autism will play a big part in the audience’s interpretation of the character. You might choose this option if you feel it is important for the audience to understand the character is autistic.
If you are telling a story “about being autistic”, the fact that the character is autistic is very likely to be one that you will want to raise at the start, but even in a story that is not “about” being autistic, knowing your character’s neurotype from the outset can help the audience to interpret their behaviour.
After the character has been established - your character has already been established and you have demonstrated their autistic traits; calling your character autistic at this point is a way of confirming it and making it explicit for anyone who has not realised so far.
A “big” reveal - this isn’t something that I have seen used, but there is the option of “revealing” that your character is autistic later in the story.
This could be used a way of subverting the expectations of readers who have stereotypical views of autism (and confirming other readers’ “headcanons”) for characters who have atypical traits. Otherwise, it could be presented as the solution to a “mystery” about the character.
It is brought up several times - you don’t have to only mention the character’s autism once! Their autism might be referred to multiple times during the story.
In the description/summary of your story - This a useful option if the story takes place in a point in history before the diagnosis of “autism” existed. It can also be used to clarify the terms you use for stories set in the future/different worlds.
(The Curious Incident of the Dog in the Night Time used this method, only calling the main character autistic on the cover - but you need to make sure that you actually do a decent job inside the book!)
How?
OK, time to actually decide how to tell your audience that the character is autistic. Luckily, there are lots of options!
We are going to list several strategies. There are lots of ways of fitting these into context: try relating what you say to an autistic trait which is affecting your character at that point in the story: are they struggling with executive dysfunction? having fun stimming? looking up information about their special interest?
Here are some ideas of topics related to autism that might provide you with the opportunity to casually drop in the term “autistic”: sensory overload, stimming, executive dysfunction, alexithymia, difficulties with social interactions, problems with communication, special interests, eye contact, meltdowns and shutdowns.
Here are some techniques for telling the audience that the character is autistic. Each suggestion is accompanied by at least one example to illustrate how it can be used:
The narration says “they’re autistic” - it can be slipped in as a sort of “aside” if that feels more natural in your story
“Karen swore loudly. The village church bells had been ringing for 45 minutes and her head felt like it was going to split in two. Of course being autistic didn’t help, but the main problem was the bloody eejit who decided it was a good idea to hold bell practice today of all days.”
“Ming looked down the guest list. Selvie was bringing Cheng Mae as her plus-one. Ming had only met her once: he knew that she was autistic, that she loved Criminal Minds, and that Selvie was trying to take the relationship to the next level, but none of this helped him with choosing what table to put the couple at. He called Helen in from the kitchen to ask what she thought.”
The autistic character says they’re autistic (in dialogue) - either explicitly telling another character, or mentioning in passing
“Sorry I went a bit weird yesterday - I’m autistic and crowds are really overwhelming for me. Can we try again next Saturday? You can come ’round to mine and I’ll cook a romantic dinner”
J: How did you choose your therapist? I’m trying to find one
K: She specializes in working with autistic people. My dad helped me find her.
J: Oh, is she expensive?
The autistic character says they're autistic (as the first-person point of view narrator)
They might mention it as a personal aside, or they may refer to it repeatedly throughout the narrative.
“I hate the store. I have been to every aisle at least twice already, but either two items are in the same aisle but not written next to each other on the list, or I can’t see the item I’m looking for. I know I struggle with finding things directly in front of my face because I’m autistic—my brain just doesn’t process the images my eyes are passing over fast enough—but it’s so annoying. I just wanted to find the cereal my sister likes.”
Refer to (or flashback to) a time in the past when it came up
For example, the character could refer to to being in special ed at school, their parents might talk about the character having atypical development (eg. not speaking until a later age than usual), they could refer to the mental health professional who first suggested that they seek out a diagnosis, the character might make a comment comparing something to one of the tests they did while being assessed for autism, there might be a flashback to ABA sessions.
“Hey, Cam, you know that you are allowed to say when you disagree with something, don’t you?”
“Yes.” Cam hesitated. “Um... I mean, yes, in theory. But I was taught in social skills that I had to smile and nod when people speak. It’s hard.”
“Of course, I forgot. It was more important for them to teach the autistic kid to be compliant than to teach you how to communicate your needs,” he scowled. “Sarcasm,” he added
“Thanks. I realised, this time.”
Another character discloses that the character is autistic (note: this is something that is not necessarily an appropriate thing to do in real-life — please don’t go talking about other people’s diagnoses behind their backs unless you know EXPLICITLY that this is ok with them)
“What’s the deal with Zephyr? Is he always such an arse?”
Caroline sighed, “listen, Katharina, Zephyr isn’t trying to be rude. He’s autistic, he can’t pick up on your hints that you want to change the subject. Just tell him—nicely—that you want to talk about something else”
Chantelle looked the teacher in the eye, her face resolute.
“Please, Mr Clive, Aaron is autistic, and I need to know that the school understands that. Things have been difficult for all of us since the earthquake, but the changes have been really hard for him. We lost our house, we’ve moved to a new area. Can I work with someone from the school’s SEN department to plan his induction?”
Another character mentions it when talking to the autistic character
“You know, when I first heard you were autistic I was expecting something different”
“Robyn, this is not the time,” Enri snapped, “let’s fix the ship first, please”
From: K.Litchen
To: I.Khan
Subject: Favor please! <3
Hey, Ibby, you can definitely say “no” if you want to, but is it ok if I give your email address to my sister? She just found out that my nephew might be autistic and I think it would help her to talk to an autistic adult bc she’s panicking right now.
Also, you left your dictaphone at the office on Friday, I can drop it off tonite if you like?
Thanks!!!
Kim xxx”
Say it in the blurb/synopsis of your book/comic/film/etc
“17th Century France: The Beast of Gévaudan has been terrorising the area for two years. After two twelve year olds are killed in his village, Pierre, an autistic baker, begins investigating the attacks. He uncovers secrets, lies, and the terrible truth behind La Bèstia — but who will listen to M. Fournier’s oddball son?”
Include information in the background of a panel/scene (for a comic/film)
Examples:
A panel shows a letter that is relevant for plot reasons, but you can see part of another letter behind it that references autism
The character goes to visit their therapist and there are posters about autism on the walls
The character wears some sort of autistic pride t-shirt (example 1 and example 2)
This information could also be backed up by (or highlighted in) your dialogue. The prose-based equivalent to having information in the mise-en-scene would be using descriptions of the background.
That’s it for part one!
Next time on On calling characters autistic:
Part 2 - what if autistic isn’t a term that exists in my story?
We discuss telling stories that are set in the past, the distant future, and on other worlds
Part 3 - hinting
We discuss ways to strongly imply that your character is autistic (techniques that you will ideally combine with explicitly calling them autistic)
652 notes
·
View notes
Text
Today, I decided to give my body a break as I know breaks are required. I know I am supposed to increase my carbs for the day so that I shock my body as it is used to of being low to no carbs from one week. Then I will cut them down again for the week. This is called carb cycling. I increase my carbs when my workout RPE starts going 5-6. I usually train at RPE 7. I used to do carb cycling to maintain abs year round. I don’t know why I have become so miserable that despite of knowing what I am required to do I cannot do it. For me eating has become such a problem. Is there any athlete out here who is struggling with the same issue and can relate to it and speak sense into me or would like to be my friend and together we could plan out something to recover without listening to these so called ed specialists who are out there preaching to include chick fil e’s for recovery. Which I feel is total rubbish. They don’t understand that your body isn’t a dust bin/ rubbish tank but a temple and needs to be given the best possible high quality clean food. I am not looking for ana coaches or ED friends. I need someone who wants to recover in a healthy way. Only people in recovery should hit me up.
If you’re ana coach or ED partners kindly stay away from my profile. I am not interested in spreading misery and or seek it. I am here to just share what I am going through.
Recently the idea of eating is scaring me bad. I gained weight in recovery which was required but I hate the fluff again. I cannot accept it.
It all began when I visited my therapist and she was concerned about my other diagnosis and she said that she is happy about me putting on weight and getting healthy. What she is concerned about is my wrong medication that is being given to me since so long and she said that it is taking a mental toll on me.
She said without realizing how I would feel about her commenting on my weight. It screwed everything for me. She said she is happy about me ‘putting on weight’ that means it is noticeable to everyone. I just feel disgusted again. There is nothing I have left to hold onto. I have failed at everything in life. It all makes sense to me. When I fail at such a basic human trait that is ‘eating’ then how can I do anything else? I suck at everything.
0 notes
Text
Goodbye my left ovary,
I’ve been tossing and turning about sharing this for a while as I’m generally quite a private person, but I’ve had time to heal and process what I’ve gone through and I want to bring awareness to the fact that sometimes our bodies don’t work in the way that we expect them to.
The female reproductive system is something I’ve really taken for granted until now. It’s something incredible, so empowering and strong. I always assumed it just worked. The illustration I made is pretty self-explanatory – but yes, as of right now I only have one ovary.
In March I needed an emergency surgery to remove my left ovary, along with the fallopian tube and a large ovarian cyst.
The long story
In early January I noticed a solid like mass by my bladder. It was small enough to not notice visually, but concerning enough to make a trip to the doctor.
Being a young female, with a solid bump in their tummy everyone always assumes that you’re pregnant right? I mean at some points I thought I was myself. Every doctor I saw had their presumptions quashed by the negative reading that came back on the test every time, but this sparked some worry.
My doctor suspected that I had something on my ovary but to be sure, I was referred to take an ultrasound and take some blood tests. They discovered a large Borderline Cyst on my left ovary that spanned across my stomach and up to my left ribcage. At this point I had no idea what I was in for. My brain is wired to over-think everything and I did so for the next 4 weeks until my specialist appointment.
Ovarian Cysts are generally quite common, actually a lot more common than you'd expect, but I had never heard of them until I found out that I had one. There are various types, simple cysts that grow and disappear, and more complex ones. Instead of being a simple cyst that would go away by itself, my body developed the most complex ovarian cyst – called an Adnexal Mass / Borderline Tumour that specialists presume had been growing steadily for years and only recently moved out of my pelvis, making it noticeable.
It was like a ghost of a thing that was growing from inside taking all the spare space there was in my abdomen. Unbeknownst to me it was causing a range of symptoms that I never noticed that they were connected until my diagnosis.
I had irregular periods for years
I gained weight on the scales but hadn’t changed much physically
I was feeling nauseous all the time
I suffered from extreme fatigue
I had the urge to pee 24/7
I would get full from the smallest of meals
I couldn’t breathe deeply
I had a specialist appointment with a Gynaecologist on the 3rd of March. This is where we discussed my situation. The mass was so complex and large that the specialists suspected that it may contain pre-cancer cells. There was the bomb shell. Because of this suspicion they needed to remove the mass intact meaning that they needed to remove the ovary and fallopian tube along with it. To give you a sense of scale at this point, they suspected the mass was about 10cm x 13cm x 9cm, so they were lining up a C-Section like surgery to remove it. So it was pretty large to say the least. Obviously I was in shock, overwhelmed with emotion. We had a lengthy discussion about what would happen, the surgery and the long term impact that it would have on my health and fertility. I was scared but I knew what I was in for.
I was in for a 6-8 week wait for a surgery date. However, the surgery happened a lot sooner than expected. 4 weeks after that appointment I was experiencing excruciating abdominal pain and on the 24th of March I was referred to Middlemore Hospital’s ED by my GP. The timing of all of this was pretty good as the hospital was really quiet due to the start of Covid-19. I was in and the surgery was scheduled for the next morning at 9am.
The procedure & recovery

I had a Mid-line Laparotomy which is a pretty intense surgery. It is essentially a vertical incision that starts just blow my bikini line, to 2cm above my belly button, 18cm total. The surgeon initially planned to make the incision horizontally– like a C-Section, but the mass was a lot larger than they expected as it reached as far as my sternum. It had to be vertical to remove it safely. The surgery went well and everything was removed successfully, they took washings of my abdomen and sent away the cyst for a biopsy. I feel like the surgery was the easiest part…
Really I can’t remember much from the day of the op, and the day after, the anaesthetic took it out of me. I needed an epidural for pain management post op and I was bed ridden for two days. Ultimately I was exhausted physically and emotionally – and my body was trying it’s best to heal but I was so exhausted, weak and immobile. I had the epidural removed after the third day, to see if I could start walking again.
Eventually I got myself up and started walking, movements were slow and excruciating and so mentally challenging as I’m usually really active. I’m not really the one to take pain killers unless I really need to, but I was taking them every chance that I got. I struggled a lot with the pain, nausea, very low blood pressure, dizzy spells and fever post op. At some points the nausea was so overwhelming that I had to vomit. This is was the most excruciating pain that I’ve been in to date.
Nick wasn’t able to visit post op, as our government declared the Covid-19 level 4 lock down so he wasn’t allowed to enter the hospital at all during my recovery. It was a mental challenge being by myself. I gradually got better and I asked to go home after 5 days in the hospital by myself. Even though hospitals are such a daunting place to be in, I felt like I was in the best hands the entire time. The specialists, surgeons, anaesthetists, nurses and doctors that I was cared for by were incredible and I feel so fortunate to have received the care that I did.
At home I spent a lot of time in bed, asleep and I struggled to eat, move and shower. I felt crippled and reliant. Overall I lost 7kg, but I was improving. After a week I was able to stop taking pain killers, and now I’m fine! Just working on the healing of my scar.

My scar 2.5 weeks post op.
The Diagnosis
On the 15th of April I had a follow up appointment with the specialist to go over the operation notes and results of the biopsy. Unfortunately, they did find pre-cancer cells within the cyst, however they were contained and didn’t spill or spread into the rest of my body. The cyst was classed as a Stage 1C ovarian cancer – but because of the success of the surgery and the containment of the cells I don’t need to have any treatment.
Because of the existence of the pre-cancer cells in the cyst I’ll need to evaluate getting the right ovary removed too when I’m ready – for future proofing. For now I’m scheduled to have 6 monthly ultrasounds and bloods taken to monitor my right ovary to make sure it is healthy.
The cyst was a lot larger than the specialist initially thought. It was actually 21cm x 23cm x 13cm and weighed 3.3kg! Think of a 3L milk bottle, it was larger and heavier than that, in my abdomen, so you could imagine the pressure it would have had on my other organs. The specialist was astounded that it had got to this size without notice, as I’m generally quite fit and active.
Post op, the first thing I noticed was that I had never been able to breathe so well. Taking a deep breath was amazing.
My Future & Fertility
I’ve been in a long term relationship since I was a teen, and I’ve always wanted a family of my own. Nick and I have always discussed having a family, but it’s definitely not our time yet, we’ve just relocated to Auckland a year ago and we have a whole lot planned before all of that is on the cards. I see Friends of mine are having some beautiful babies and I know my day will come. Not now, but one day. With one ovary it is still possible and that gives me hope.
This whole experience has made me feel like I’d been taking my health for granted and expecting everything will just work. How wrong was I, to be honest the specialist said it was really just bad luck and there was nothing to really prevent it from happening the way it did, in reality there was no way that I knew it was there. My ovaries were something I took for granted, and now my remaining one crosses my mind at least once a day. I need to look after it like gold.
What interests me the most is women in New Zealand are encouraged to have breast screening and smear tests to screen for cancer and pre cancer cells – I knew this was a thing even as a child, but there isn’t really a campaign that I’ve seen that screams at you to see if your ovaries are ok. I want to know why because I really feel like I’ve dodged a bullet.
This was something that I never thought I’d have to go through. It’s not necessarily something that you’d expect to be told when you’re in your early twenties but here we are. Let’s say I’m not taking my health or fitness for granted again.
If you got this far thank you for reading my rambles!

I’m a thousand times better than I was, and I’m now 4 weeks post op and I’m past the dizzy spells, nausea and pain. My scar is healing and I’m able to walk daily – but I’m waiting for the 6 week mark to push myself more. I’m itching to go for a run and a swim to really test the space that my lungs now have.
There is obviously a lot of detail that I have left out of this, but if you’re curious or feel like you want to know more please ask. This is by no means an attention seeking post it’s to bring awareness, and also a method for me to heal and move past what I’ve been through.
Thanks for reading!
Katie x
1 note
·
View note
Text
Porn Ed: What Happens When Porn Replaces Sex Education?
Adolescents today have greater access to a wider range of pornography than any previous generation. So how is it affecting them?
This question is the crux of a new episode of Lisa Ling’s CNN series This is Life titled “Porn Ed,” which premieres September 29. Ling wanted to better understand how accessibility to porn is changing the way adolescents and young adults think about sex and approach relationships.

Episode still from Lisa Ling’s “This is Life.” Image courtesy of CNN.
I had a chance to preview the episode and sit down with Ling to discuss it. While there’s much that we agree on, including the idea that porn is not an effective substitute for sex education, there are some aspects of the episode that I worry could potentially leave viewers with the wrong impression of how porn impacts people, especially the idea that it is “addictive.” The show focuses on people’s personal opinions about and experiences with porn and doesn’t explore the science—in fact, no researchers or doctors are interviewed on screen during the episode. So while it’s certainly a thought-provoking show, there were some missed opportunities for a data-driven discussion.
Below is a lightly edited transcript of my conversation with Ling that focuses on the areas where we agree, but also the areas where science and medicine diverge from some of the things claimed by those who were interviewed in the episode.
Justin Lehmiller: In this episode, you interview people who see porn as a source of danger and problems, but you also talk to people like Cindy Gallop who see potential value in adult videos that are capturing real-life sex. When you put those different conversations together, what's your take on whether porn itself is inherently good or bad, or is it neutral?
Lisa Ling: Our episode really isn't a condemnation of porn. I do think that for some people, there may be value to porn. And I would never begrudge sex workers because I actually think that there are sex workers out there who are performing a real service. My big concern is just the abundance of material that's out there—some of which is really extreme—and how easy kids can access it. You know, when you talk about what Cindy's trying to do with her website, Make Love Not Porn, they are defiant about the fact that they are not porn. They are providing people with an experience of what real sex should look like. It's not always clean and it's sometimes messy. It's sometimes funny. It sometimes doesn't really work very well. And I do think that there is value in that. I do think that we should be exposed to how beautiful and meaningful sex can be. It's part of who we are, right?
But at the same time, I do think that it's incumbent on parents to start having those conversations with kids sooner. I think that kids need to understand that sex is part of who we are, that it can be just a pleasurable experience, that communication is really essential, and that what they are accessing is not reality. It's entertainment for adults. There's a lot that goes on behind the scenes that kids are never aware of.
That's one of the reasons why we feature Tasha Reign, the adult film star, because she is on a mission to communicate to people that, before cameras even roll, they have a negotiation about consent and about what the men and women are willing to do. I think if we had a better sense of the fact that this is all artificial in many ways—it’s entertainment—kids may not think that's reality.
Justin Lehmiller: You and I are on the same page that porn should not be used to replace sex education. And you've already talked a bit about the different ways that parents need to start approaching sex education with their kids. But I'm curious as to the role of schools in all of this. What do you think schools need to be doing differently when it comes to sex ed, specifically as it relates to porn?

Lisa Ling. Photo courtesy of CNN.
Lisa Ling: I think it's ultimately a parent's responsibility, but we have to recognize that there are some parents who aren't able to have those kinds of conversations, don't want to have those conversations, may not have time to have those kinds of conversations…so we need to start having those conversations in schools. In California, for example, where I'm from, there is a very comprehensive sexual education curriculum. When I sat through one of the classes, I was even uneasy because I wasn't used to having those kinds of conversations. But for the kids, it was just sort of like they didn't even blink. They're learning that this is a natural part of who we are and that there shouldn't be any shame or humor around it—that it's meant to be enjoyed and pleasurable, but we have to make sure that we are safe at the same time.
Justin Lehmiller: I think you're absolutely right that kids do want to have these discussions, but it's usually the parents who don't feel comfortable initiating them. So where are they going to get that information? I think schools provide one potential avenue for that through, say, porn literacy programs.
Lisa Ling: I thought it was pretty impressive that in Boston public schools they have this sex ed curriculum that includes porn literacy. You know, some parents might go, "Why are my kids learning about porn in school?" Well, because your kids are probably watching porn in their bedrooms with the phone that you gave them. The moment your kid gets a phone or gets a mobile device, you got to start thinking about how to broach the subject with them because they've probably already seen things that they don't understand that they think depict real sex.
Justin Lehmiller: Something I noticed in watching your episode is that you interviewed a lot of people, but you didn't have any scientific or medical experts in the area of porn. I'm just curious—was there a reason or rationale behind not having one of them on to discuss it?
Lisa Ling: Our show is very much an experiential one and we have found that by immersing ourselves amongst people who are going through these things, I think we get a better sense of and we're more relatable to viewers who may be experiencing similar things. And if they do feel somehow like they connect with the information that we're giving them or the people that we're profiling, then they can seek out that more professional or clinical information.
Like Alex Rhodes who started the NoFap website. He's not a clinician or a therapist but he has half a million people on his website who say that they are suffering from pornography addiction. And pornography addiction hasn't even been classified as an addiction. But because he's experienced, he knows what has worked for him and what hasn't and it's become this forum for people to share exactly those things.
Justin Lehmiller: I'm glad that you brought up those points—that porn “addiction” is not a recognized medical or psychological diagnosis and that Alex Rhodes is not a clinician, but he is offering services sort of treating this as an addiction. This is one of those areas where when you look at the research, it’s not at all definitive in saying that porn is addictive, and so I worry a little that in highlighting what Rhodes is doing and the big following he has, that people might walk away thinking that it is an addiction when the actual medical community is not there based on the research.
When you look at a lot of the data in this area, what we often see is that porn is more the symptom rather the cause of a lot of the issues people are experiencing. For example, they might have generalized sexual anxiety or moral conflicts, and those might really be the underlying cause. So to put this in the form of a question, what's your take on the idea that we might be scapegoating porn because it's an easy target rather than dealing with the underlying issues that might be driving people to porn in the first place?
Lisa Ling: You know, I am also not a clinician or a therapist, but if you talk to any pediatrician or you talk to a lot of parents, the moment their kids become exposed to pornography and how easily it's accessible, whether they have underlying issues or not, it can cloud a young person's judgment about what real sex is supposed to be like. And, you know, studies have shown that young people are having less sex than ever before. And one has to ask, "Well, what's the reason for that?" Well, it's probably because they can experience the extremes using their mobile devices. They don't have to go through the anxiety of asking a girl out or dealing with rejection when they have everything that they need and more in their pocket, accessible at all times.
So for me to boldly assert that it's an addiction, that's not something that we do in our episode. But there's a reason why NoFap, that website, has a half a million people that are desperate. They're coming to this website desperate for help from what they believe is an addiction.
Justin Lehmiller: I get that they're perceiving porn as the cause of their problems, but it might not actually be the problem for them. So by going to these websites and resources that are not based in science and data, they might not actually be getting the help that they need to really deal with those issues.
[Sidebar: Research suggests that porn access probably isn’t why young adults today are having less sex. Read my take on this idea here.]
Lisa Ling: That's true. That's certainly true. And you know, I think NoFap, is very clear or it asserts that it's not a medically sanctioned website. But what it is is people sharing what has been working for them. I think one of the reasons why it hasn't been deemed a certified, bonafide addiction is because it's harder to get information about how to stop. Right? And so people have had to resort to seeking out information on their own and seeking support from people who are going through the same thing.
I mean, our second episode is about benzodiazepines—and these are some of the most widely prescribed medications on the planet, right? And doctors, in many cases, do not know how to taper people off of benzos. So what are people doing? They're going to these non-medically sanctioned websites and getting information and learning these very meticulous taper methods that are saving their lives. None of them are medically sanctioned.
So if it's working for people, and people are finding themselves in such a desperate situation, that they're seeking out help and guidance from people they don't even know because they're not being offered the right kind of information from doctors, I mean, that's kind of where we are with pornography. And also, let's say you do believe you have an addiction and your insurance doesn't pay for therapy. How are you ever going to get medical help when your insurance doesn't cover it? You're going to seek it out online amongst people who are dealing with the same things.
Justin Lehmiller: I think we're in agreement that we want people to be able to get help and to know that the help is going to work. But there's also a really big impediment for us to having the accurate medical knowledge we need about pornography, which is that there's really no federal funding available for people who want to do research on porn. And so there is sort of this roadblock if we want a design interventions or treatments or, you know, just really study porn. This is why I think our knowledge base is so limited and why a lot of these non-scientific, non-medical platforms are taking off. It's, in part, because they're filling this void that is not currently being addressed because there just isn't the funding to do the research we need.
Lisa Ling: There's the funding we need to do the research. And most of our insurance will not pay for the therapeutic services that people might need to even figure out what may have spurred someone to seek out porn.
Justin Lehmiller: I think that's a great point, that access to care is another big part of the issue that leads people to seek out these informal, non-medical platforms. With greater access to care, we could ensure that more people get the help they truly need, rather than feeling like their only option is to seek out information online that isn’t based in scientific research.
Now, given all of the people out there claiming that porn is “addictive” and fundamentally damaging, some are calling for bans on pornography and restrictions on porn access. Do you think that bans and restrictions are the answer to these problems or do you think it's really more about improving sex education and sexual communication?
Lisa Ling: I think that we could ameliorate a good part of it by educating kids about what sex is really like and what it's supposed to be like. I think that having those open conversations would do a lot for the issue—do a lot to alleviate some of the concerns. Porn is the only exposure some kids may be getting to sex. It's inevitable that would skew your perception, you know? So I think opening up the dialogue would at least get us one step closer to having a more sort of normal perception of what sex is and what relationships should be.
Want to learn more about Sex and Psychology ? Click here for previous articles or follow the blog on Facebook (facebook.com/psychologyofsex), Twitter (@JustinLehmiller), or Reddit (reddit.com/r/psychologyofsex) to receive updates. You can also follow Dr. Lehmiller on YouTube and Instagram.
Image Source: CNN
You Might Also Like:
What Counts as “Pornography?” It Depends Who You Ask
The Truth About How Porn Affects Us
How Is Porn Use Linked To Relationship Satisfaction? It’s Complicated
from MeetPositives SM Feed 4 https://ift.tt/2nJ90z1
via IFTTT
0 notes
Text
Porn Ed: What Happens When Porn Replaces Sex Education?
Adolescents today have greater access to a wider range of pornography than any previous generation. So how is it affecting them?
This question is the crux of a new episode of Lisa Ling’s CNN series This is Life titled “Porn Ed,” which premieres September 29. Ling wanted to better understand how accessibility to porn is changing the way adolescents and young adults think about sex and approach relationships.

Episode still from Lisa Ling’s “This is Life.” Image courtesy of CNN.
I had a chance to preview the episode and sit down with Ling to discuss it. While there’s much that we agree on, including the idea that porn is not an effective substitute for sex education, there are some aspects of the episode that I worry could potentially leave viewers with the wrong impression of how porn impacts people, especially the idea that it is “addictive.” The show focuses on people’s personal opinions about and experiences with porn and doesn’t explore the science—in fact, no researchers or doctors are interviewed on screen during the episode. So while it’s certainly a thought-provoking show, there were some missed opportunities for a data-driven discussion.
Below is a lightly edited transcript of my conversation with Ling that focuses on the areas where we agree, but also the areas where science and medicine diverge from some of the things claimed by those who were interviewed in the episode.
Justin Lehmiller: In this episode, you interview people who see porn as a source of danger and problems, but you also talk to people like Cindy Gallop who see potential value in adult videos that are capturing real-life sex. When you put those different conversations together, what's your take on whether porn itself is inherently good or bad, or is it neutral?
Lisa Ling: Our episode really isn't a condemnation of porn. I do think that for some people, there may be value to porn. And I would never begrudge sex workers because I actually think that there are sex workers out there who are performing a real service. My big concern is just the abundance of material that's out there—some of which is really extreme—and how easy kids can access it. You know, when you talk about what Cindy's trying to do with her website, Make Love Not Porn, they are defiant about the fact that they are not porn. They are providing people with an experience of what real sex should look like. It's not always clean and it's sometimes messy. It's sometimes funny. It sometimes doesn't really work very well. And I do think that there is value in that. I do think that we should be exposed to how beautiful and meaningful sex can be. It's part of who we are, right?
But at the same time, I do think that it's incumbent on parents to start having those conversations with kids sooner. I think that kids need to understand that sex is part of who we are, that it can be just a pleasurable experience, that communication is really essential, and that what they are accessing is not reality. It's entertainment for adults. There's a lot that goes on behind the scenes that kids are never aware of.
That's one of the reasons why we feature Tasha Reign, the adult film star, because she is on a mission to communicate to people that, before cameras even roll, they have a negotiation about consent and about what the men and women are willing to do. I think if we had a better sense of the fact that this is all artificial in many ways—it’s entertainment—kids may not think that's reality.
Justin Lehmiller: You and I are on the same page that porn should not be used to replace sex education. And you've already talked a bit about the different ways that parents need to start approaching sex education with their kids. But I'm curious as to the role of schools in all of this. What do you think schools need to be doing differently when it comes to sex ed, specifically as it relates to porn?

Lisa Ling. Photo courtesy of CNN.
Lisa Ling: I think it's ultimately a parent's responsibility, but we have to recognize that there are some parents who aren't able to have those kinds of conversations, don't want to have those conversations, may not have time to have those kinds of conversations…so we need to start having those conversations in schools. In California, for example, where I'm from, there is a very comprehensive sexual education curriculum. When I sat through one of the classes, I was even uneasy because I wasn't used to having those kinds of conversations. But for the kids, it was just sort of like they didn't even blink. They're learning that this is a natural part of who we are and that there shouldn't be any shame or humor around it—that it's meant to be enjoyed and pleasurable, but we have to make sure that we are safe at the same time.
Justin Lehmiller: I think you're absolutely right that kids do want to have these discussions, but it's usually the parents who don't feel comfortable initiating them. So where are they going to get that information? I think schools provide one potential avenue for that through, say, porn literacy programs.
Lisa Ling: I thought it was pretty impressive that in Boston public schools they have this sex ed curriculum that includes porn literacy. You know, some parents might go, "Why are my kids learning about porn in school?" Well, because your kids are probably watching porn in their bedrooms with the phone that you gave them. The moment your kid gets a phone or gets a mobile device, you got to start thinking about how to broach the subject with them because they've probably already seen things that they don't understand that they think depict real sex.
Justin Lehmiller: Something I noticed in watching your episode is that you interviewed a lot of people, but you didn't have any scientific or medical experts in the area of porn. I'm just curious—was there a reason or rationale behind not having one of them on to discuss it?
Lisa Ling: Our show is very much an experiential one and we have found that by immersing ourselves amongst people who are going through these things, I think we get a better sense of and we're more relatable to viewers who may be experiencing similar things. And if they do feel somehow like they connect with the information that we're giving them or the people that we're profiling, then they can seek out that more professional or clinical information.
Like Alex Rhodes who started the NoFap website. He's not a clinician or a therapist but he has half a million people on his website who say that they are suffering from pornography addiction. And pornography addiction hasn't even been classified as an addiction. But because he's experienced, he knows what has worked for him and what hasn't and it's become this forum for people to share exactly those things.
Justin Lehmiller: I'm glad that you brought up those points—that porn “addiction” is not a recognized medical or psychological diagnosis and that Alex Rhodes is not a clinician, but he is offering services sort of treating this as an addiction. This is one of those areas where when you look at the research, it’s not at all definitive in saying that porn is addictive, and so I worry a little that in highlighting what Rhodes is doing and the big following he has, that people might walk away thinking that it is an addiction when the actual medical community is not there based on the research.
When you look at a lot of the data in this area, what we often see is that porn is more the symptom rather the cause of a lot of the issues people are experiencing. For example, they might have generalized sexual anxiety or moral conflicts, and those might really be the underlying cause. So to put this in the form of a question, what's your take on the idea that we might be scapegoating porn because it's an easy target rather than dealing with the underlying issues that might be driving people to porn in the first place?
Lisa Ling: You know, I am also not a clinician or a therapist, but if you talk to any pediatrician or you talk to a lot of parents, the moment their kids become exposed to pornography and how easily it's accessible, whether they have underlying issues or not, it can cloud a young person's judgment about what real sex is supposed to be like. And, you know, studies have shown that young people are having less sex than ever before. And one has to ask, "Well, what's the reason for that?" Well, it's probably because they can experience the extremes using their mobile devices. They don't have to go through the anxiety of asking a girl out or dealing with rejection when they have everything that they need and more in their pocket, accessible at all times.
So for me to boldly assert that it's an addiction, that's not something that we do in our episode. But there's a reason why NoFap, that website, has a half a million people that are desperate. They're coming to this website desperate for help from what they believe is an addiction.
Justin Lehmiller: I get that they're perceiving porn as the cause of their problems, but it might not actually be the problem for them. So by going to these websites and resources that are not based in science and data, they might not actually be getting the help that they need to really deal with those issues.
[Sidebar: Research suggests that porn access probably isn’t why young adults today are having less sex. Read my take on this idea here.]
Lisa Ling: That's true. That's certainly true. And you know, I think NoFap, is very clear or it asserts that it's not a medically sanctioned website. But what it is is people sharing what has been working for them. I think one of the reasons why it hasn't been deemed a certified, bonafide addiction is because it's harder to get information about how to stop. Right? And so people have had to resort to seeking out information on their own and seeking support from people who are going through the same thing.
I mean, our second episode is about benzodiazepines—and these are some of the most widely prescribed medications on the planet, right? And doctors, in many cases, do not know how to taper people off of benzos. So what are people doing? They're going to these non-medically sanctioned websites and getting information and learning these very meticulous taper methods that are saving their lives. None of them are medically sanctioned.
So if it's working for people, and people are finding themselves in such a desperate situation, that they're seeking out help and guidance from people they don't even know because they're not being offered the right kind of information from doctors, I mean, that's kind of where we are with pornography. And also, let's say you do believe you have an addiction and your insurance doesn't pay for therapy. How are you ever going to get medical help when your insurance doesn't cover it? You're going to seek it out online amongst people who are dealing with the same things.
Justin Lehmiller: I think we're in agreement that we want people to be able to get help and to know that the help is going to work. But there's also a really big impediment for us to having the accurate medical knowledge we need about pornography, which is that there's really no federal funding available for people who want to do research on porn. And so there is sort of this roadblock if we want a design interventions or treatments or, you know, just really study porn. This is why I think our knowledge base is so limited and why a lot of these non-scientific, non-medical platforms are taking off. It's, in part, because they're filling this void that is not currently being addressed because there just isn't the funding to do the research we need.
Lisa Ling: There's the funding we need to do the research. And most of our insurance will not pay for the therapeutic services that people might need to even figure out what may have spurred someone to seek out porn.
Justin Lehmiller: I think that's a great point, that access to care is another big part of the issue that leads people to seek out these informal, non-medical platforms. With greater access to care, we could ensure that more people get the help they truly need, rather than feeling like their only option is to seek out information online that isn’t based in scientific research.
Now, given all of the people out there claiming that porn is “addictive” and fundamentally damaging, some are calling for bans on pornography and restrictions on porn access. Do you think that bans and restrictions are the answer to these problems or do you think it's really more about improving sex education and sexual communication?
Lisa Ling: I think that we could ameliorate a good part of it by educating kids about what sex is really like and what it's supposed to be like. I think that having those open conversations would do a lot for the issue—do a lot to alleviate some of the concerns. Porn is the only exposure some kids may be getting to sex. It's inevitable that would skew your perception, you know? So I think opening up the dialogue would at least get us one step closer to having a more sort of normal perception of what sex is and what relationships should be.
Want to learn more about Sex and Psychology ? Click here for previous articles or follow the blog on Facebook (facebook.com/psychologyofsex), Twitter (@JustinLehmiller), or Reddit (reddit.com/r/psychologyofsex) to receive updates. You can also follow Dr. Lehmiller on YouTube and Instagram.
Image Source: CNN
You Might Also Like:
What Counts as “Pornography?” It Depends Who You Ask
The Truth About How Porn Affects Us
How Is Porn Use Linked To Relationship Satisfaction? It’s Complicated
from Meet Positives SMFeed 8 https://ift.tt/2nJ90z1
via IFTTT
0 notes
Text
Porn Ed: What Happens When Porn Replaces Sex Education?
Adolescents today have greater access to a wider range of pornography than any previous generation. So how is it affecting them?
This question is the crux of a new episode of Lisa Ling’s CNN series This is Life titled “Porn Ed,” which premieres September 29. Ling wanted to better understand how accessibility to porn is changing the way adolescents and young adults think about sex and approach relationships.

Episode still from Lisa Ling’s “This is Life.” Image courtesy of CNN.
I had a chance to preview the episode and sit down with Ling to discuss it. While there’s much that we agree on, including the idea that porn is not an effective substitute for sex education, there are some aspects of the episode that I worry could potentially leave viewers with the wrong impression of how porn impacts people, especially the idea that it is “addictive.” The show focuses on people’s personal opinions about and experiences with porn and doesn’t explore the science—in fact, no researchers or doctors are interviewed on screen during the episode. So while it’s certainly a thought-provoking show, there were some missed opportunities for a data-driven discussion.
Below is a lightly edited transcript of my conversation with Ling that focuses on the areas where we agree, but also the areas where science and medicine diverge from some of the things claimed by those who were interviewed in the episode.
Justin Lehmiller: In this episode, you interview people who see porn as a source of danger and problems, but you also talk to people like Cindy Gallop who see potential value in adult videos that are capturing real-life sex. When you put those different conversations together, what's your take on whether porn itself is inherently good or bad, or is it neutral?
Lisa Ling: Our episode really isn't a condemnation of porn. I do think that for some people, there may be value to porn. And I would never begrudge sex workers because I actually think that there are sex workers out there who are performing a real service. My big concern is just the abundance of material that's out there—some of which is really extreme—and how easy kids can access it. You know, when you talk about what Cindy's trying to do with her website, Make Love Not Porn, they are defiant about the fact that they are not porn. They are providing people with an experience of what real sex should look like. It's not always clean and it's sometimes messy. It's sometimes funny. It sometimes doesn't really work very well. And I do think that there is value in that. I do think that we should be exposed to how beautiful and meaningful sex can be. It's part of who we are, right?
But at the same time, I do think that it's incumbent on parents to start having those conversations with kids sooner. I think that kids need to understand that sex is part of who we are, that it can be just a pleasurable experience, that communication is really essential, and that what they are accessing is not reality. It's entertainment for adults. There's a lot that goes on behind the scenes that kids are never aware of.
That's one of the reasons why we feature Tasha Reign, the adult film star, because she is on a mission to communicate to people that, before cameras even roll, they have a negotiation about consent and about what the men and women are willing to do. I think if we had a better sense of the fact that this is all artificial in many ways—it’s entertainment—kids may not think that's reality.
Justin Lehmiller: You and I are on the same page that porn should not be used to replace sex education. And you've already talked a bit about the different ways that parents need to start approaching sex education with their kids. But I'm curious as to the role of schools in all of this. What do you think schools need to be doing differently when it comes to sex ed, specifically as it relates to porn?

Lisa Ling. Photo courtesy of CNN.
Lisa Ling: I think it's ultimately a parent's responsibility, but we have to recognize that there are some parents who aren't able to have those kinds of conversations, don't want to have those conversations, may not have time to have those kinds of conversations…so we need to start having those conversations in schools. In California, for example, where I'm from, there is a very comprehensive sexual education curriculum. When I sat through one of the classes, I was even uneasy because I wasn't used to having those kinds of conversations. But for the kids, it was just sort of like they didn't even blink. They're learning that this is a natural part of who we are and that there shouldn't be any shame or humor around it—that it's meant to be enjoyed and pleasurable, but we have to make sure that we are safe at the same time.
Justin Lehmiller: I think you're absolutely right that kids do want to have these discussions, but it's usually the parents who don't feel comfortable initiating them. So where are they going to get that information? I think schools provide one potential avenue for that through, say, porn literacy programs.
Lisa Ling: I thought it was pretty impressive that in Boston public schools they have this sex ed curriculum that includes porn literacy. You know, some parents might go, "Why are my kids learning about porn in school?" Well, because your kids are probably watching porn in their bedrooms with the phone that you gave them. The moment your kid gets a phone or gets a mobile device, you got to start thinking about how to broach the subject with them because they've probably already seen things that they don't understand that they think depict real sex.
Justin Lehmiller: Something I noticed in watching your episode is that you interviewed a lot of people, but you didn't have any scientific or medical experts in the area of porn. I'm just curious—was there a reason or rationale behind not having one of them on to discuss it?
Lisa Ling: Our show is very much an experiential one and we have found that by immersing ourselves amongst people who are going through these things, I think we get a better sense of and we're more relatable to viewers who may be experiencing similar things. And if they do feel somehow like they connect with the information that we're giving them or the people that we're profiling, then they can seek out that more professional or clinical information.
Like Alex Rhodes who started the NoFap website. He's not a clinician or a therapist but he has half a million people on his website who say that they are suffering from pornography addiction. And pornography addiction hasn't even been classified as an addiction. But because he's experienced, he knows what has worked for him and what hasn't and it's become this forum for people to share exactly those things.
Justin Lehmiller: I'm glad that you brought up those points—that porn “addiction” is not a recognized medical or psychological diagnosis and that Alex Rhodes is not a clinician, but he is offering services sort of treating this as an addiction. This is one of those areas where when you look at the research, it’s not at all definitive in saying that porn is addictive, and so I worry a little that in highlighting what Rhodes is doing and the big following he has, that people might walk away thinking that it is an addiction when the actual medical community is not there based on the research.
When you look at a lot of the data in this area, what we often see is that porn is more the symptom rather the cause of a lot of the issues people are experiencing. For example, they might have generalized sexual anxiety or moral conflicts, and those might really be the underlying cause. So to put this in the form of a question, what's your take on the idea that we might be scapegoating porn because it's an easy target rather than dealing with the underlying issues that might be driving people to porn in the first place?
Lisa Ling: You know, I am also not a clinician or a therapist, but if you talk to any pediatrician or you talk to a lot of parents, the moment their kids become exposed to pornography and how easily it's accessible, whether they have underlying issues or not, it can cloud a young person's judgment about what real sex is supposed to be like. And, you know, studies have shown that young people are having less sex than ever before. And one has to ask, "Well, what's the reason for that?" Well, it's probably because they can experience the extremes using their mobile devices. They don't have to go through the anxiety of asking a girl out or dealing with rejection when they have everything that they need and more in their pocket, accessible at all times.
So for me to boldly assert that it's an addiction, that's not something that we do in our episode. But there's a reason why NoFap, that website, has a half a million people that are desperate. They're coming to this website desperate for help from what they believe is an addiction.
Justin Lehmiller: I get that they're perceiving porn as the cause of their problems, but it might not actually be the problem for them. So by going to these websites and resources that are not based in science and data, they might not actually be getting the help that they need to really deal with those issues.
[Sidebar: Research suggests that porn access probably isn’t why young adults today are having less sex. Read my take on this idea here.]
Lisa Ling: That's true. That's certainly true. And you know, I think NoFap, is very clear or it asserts that it's not a medically sanctioned website. But what it is is people sharing what has been working for them. I think one of the reasons why it hasn't been deemed a certified, bonafide addiction is because it's harder to get information about how to stop. Right? And so people have had to resort to seeking out information on their own and seeking support from people who are going through the same thing.
I mean, our second episode is about benzodiazepines—and these are some of the most widely prescribed medications on the planet, right? And doctors, in many cases, do not know how to taper people off of benzos. So what are people doing? They're going to these non-medically sanctioned websites and getting information and learning these very meticulous taper methods that are saving their lives. None of them are medically sanctioned.
So if it's working for people, and people are finding themselves in such a desperate situation, that they're seeking out help and guidance from people they don't even know because they're not being offered the right kind of information from doctors, I mean, that's kind of where we are with pornography. And also, let's say you do believe you have an addiction and your insurance doesn't pay for therapy. How are you ever going to get medical help when your insurance doesn't cover it? You're going to seek it out online amongst people who are dealing with the same things.
Justin Lehmiller: I think we're in agreement that we want people to be able to get help and to know that the help is going to work. But there's also a really big impediment for us to having the accurate medical knowledge we need about pornography, which is that there's really no federal funding available for people who want to do research on porn. And so there is sort of this roadblock if we want a design interventions or treatments or, you know, just really study porn. This is why I think our knowledge base is so limited and why a lot of these non-scientific, non-medical platforms are taking off. It's, in part, because they're filling this void that is not currently being addressed because there just isn't the funding to do the research we need.
Lisa Ling: There's the funding we need to do the research. And most of our insurance will not pay for the therapeutic services that people might need to even figure out what may have spurred someone to seek out porn.
Justin Lehmiller: I think that's a great point, that access to care is another big part of the issue that leads people to seek out these informal, non-medical platforms. With greater access to care, we could ensure that more people get the help they truly need, rather than feeling like their only option is to seek out information online that isn’t based in scientific research.
Now, given all of the people out there claiming that porn is “addictive” and fundamentally damaging, some are calling for bans on pornography and restrictions on porn access. Do you think that bans and restrictions are the answer to these problems or do you think it's really more about improving sex education and sexual communication?
Lisa Ling: I think that we could ameliorate a good part of it by educating kids about what sex is really like and what it's supposed to be like. I think that having those open conversations would do a lot for the issue—do a lot to alleviate some of the concerns. Porn is the only exposure some kids may be getting to sex. It's inevitable that would skew your perception, you know? So I think opening up the dialogue would at least get us one step closer to having a more sort of normal perception of what sex is and what relationships should be.
Want to learn more about Sex and Psychology ? Click here for previous articles or follow the blog on Facebook (facebook.com/psychologyofsex), Twitter (@JustinLehmiller), or Reddit (reddit.com/r/psychologyofsex) to receive updates. You can also follow Dr. Lehmiller on YouTube and Instagram.
Image Source: CNN
You Might Also Like:
What Counts as “Pornography?” It Depends Who You Ask
The Truth About How Porn Affects Us
How Is Porn Use Linked To Relationship Satisfaction? It’s Complicated
from Meet Positives SM Feed 5 https://ift.tt/2nJ90z1
via IFTTT
0 notes
Text
9 Ways to Conquer Fear and Realize Your True Potential
The secret isn’t just overcoming your fear but using it to your advantage.
January
31, 2019
9 min read
Opinions expressed by Entrepreneur contributors are their own.
Everyone experiences fear. What defines you is how you face it. We asked these successful entrepreneurs and Advisors in The Oracles to tell us how they manage their biggest fears.
1. Don’t avoid your fear — leverage it.

Image credit:
The Oracles
Fear is a great thing. It’s nature’s way of awakening us to danger, like when a lion is about to chase us. It puts you in a heightened state of awareness and performance and can bring out the best in you. My greatest fear is not fulfilling my potential. I’m terrified of missing out on the life I was supposed to have. I imagine two scenarios when I die and meet the person I could have been: In heaven, we’re identical twins. In hell, we’re strangers.
I created that fear on purpose because I believe in leveraging fear, not avoiding it. When I make a decision, I ask myself whether it puts me closer to becoming that man or further away. Every action I take stems from that fear, including whether to make a phone call or go to the gym. I don’t even want to overcome my fears because when I do, I lose that leverage. —Ed Mylett, best-selling author, co-founder of the Arete Syndicate, global keynote speaker, and host of the #MAXOUT top-10 podcast; follow on YouTube, Instagram, and Facebook
2. Ask yourself what you would do if you weren’t afraid.

Image credit:
The Oracles
Early in my career, I decided to leave a secure job at General Electric for a job at a startup. Others thought I was crazy for risking everything, and I began to doubt myself. But I made the leap and joined the company that would become AOL. We helped usher in the internet revolution and changed countless lives, an experience I wouldn’t trade for the world.
I’m inspired by those who challenge themselves and others by asking, “What would you do if you weren’t afraid?” My new book, “Be Fearless,” tells the stories of individuals who answered that question with action. It provides a road map to anyone seeking a transformational breakthrough. This doesn’t mean I’ve overcome all my fears — far from it. Fearlessness isn’t the lack of fear, but the ability to overcome it. —Jean Case, author of “Be Fearless,” CEO of the Case Foundation, chairman of the National Geographic Society, and owner of Early Mountain Vineyards; follow Jean on Twitter
3. Hack your fear.

Image credit:
The Oracles
Law No. 10 in my new book, “Game Changers,” says that “fear is the mind killer.” This primal emotion serves as a survival mechanism and is triggered by failure. To our ancestors, failure meant being eaten by a tiger or starving to death. While humans have evolved, the biological fear of failure remains. But fear of failure causes failure, creating a cycle.
Don’t give in to fear — hack it instead. Fear is the root of all negative emotions, from anger to jealousy and guilt. Positive emotions like confidence, courage, and gratitude are rooted in trust. When you realize that, you can transform fear-based emotions into trust-based emotions. Learning how to make your body less afraid of failure liberates enormous energy that you can use how you choose. In the height of an anxious moment, ask yourself whether you trust that you will come out on the other side. I believe you will. —Dave Asprey, entrepreneur, known as the “father of biohacking”; creator of Bulletproof 360 and NYT best-selling author of “Game Changers”; follow Dave on Facebook and Instagram ;
4. Choose to live deliberately.

Image credit:
The Oracles
My biggest fear is looking back in 10 years and realizing that nothing has changed in my life except my age. I leverage this fear daily to drive myself and my family toward the greatness we all possess, but it takes discipline. Whenever anyone wants to quit, including me, I remind us that we’re enduring this to become our best selves. I give my husband and children the good pieces of me, even if it’s a struggle. I keep myself accountable by honoring my commitments — for example, homeschooling our children.
I encourage my family to find their potential by setting an example. I challenge my biases and seek fresh perspectives by listening with an open mind and heart. I compartmentalize and muster through the worst days but celebrate the best ones. I allow myself just to be me. We can all make this choice, but it takes courage. Choose to live deliberately, with purpose and intention. —Jessica Mead, co-founder of EpekData and BrandLync, divisions of Mead Holdings Group Inc.; follow Jessica on Instagram
5. Remember: the tightrope is only inches off the ground.

Image credit:
The Oracles
I started my first business when I was 14 years old. At 18, the business was in trouble and I was in way over my head. I was overwhelmed, losing sleep, and making bad decisions. My biggest fear was failure. When I finally closed the business, that fear came true — but it didn’t kill me. In fact, I got the best night’s sleep I’d ever had.
My worst fear wasn’t so bad after all. The tightrope I’d been walking was only inches off the ground. When you realize that, you can walk much faster the next time you’re on a tightrope. That experience taught me to cover my downside, reduce my risks to just my time, and go flat out. By structuring deals so I couldn’t lose, I could seize opportunities that scared others. This has shaped everything I do and is the essence of my business today. —Jeremy Harbour, investor and mergers and acquisitions expert; founder and CEO of Unity Group and Harbour Club; author of “Go Do!” and “Agglomerate: From Idea to IPO in 12 Months”; follow Jeremy on Twitter and LinkedIn
6. Don’t go it alone.

Image credit:
The Oracles
Fifteen years ago, my 3-year-old son was diagnosed with a large brain tumor. Without a doubt, that was the scariest situation I’ve ever had to face. When I heard the diagnosis, I shut everyone out, including my family. I felt like secluding myself would save me. Only after I let my guard down did I find the tools to take control of my fear. Two emergency surgeries saved my son’s life. Now he’s 18 years old.
Sometimes our defense mechanisms make us do exactly what we shouldn’t. When we face a fear that seems too big to handle, we become overwhelmed. We try to avoid all stimuli and distractions to save our energy and search for a solution inside ourselves. But in most situations, the answers won’t come from within. Step outside of yourself and accept that facing fear is not something we can do alone. We need others who have our backs. —Mark Moses, founding partner and CEO of CEO Coaching International; connect with Mark on LinkedIn
7. Look for the possibility behind the fear.

Image credit:
The Oracles
My biological father left my mom before I was born. As a result, I’ve had a burning desire to choose my destiny for as long as I can remember — along with a crippling fear of living without freedom. This has been a challenge personally and professionally. It has driven and stopped me time and again, keeping me from long-term relationships and even preventing me from hiring my first assistant.
I’ve learned to understand that my fear prevents me from making decisions that fulfill my dreams. Now when that fear appears, I ask myself, “What would be possible if I faced this fear?” The most important thing has been taking time to quiet my inner voice and listen to the possibility that hides behind the fear. Nothing in my life would be possible without this skill. What is stopping you? —Keri Shull, founder of the Keri Shull Team, which has sold over $2 billion in properties; co-founder of real estate coaching business HyperFast Agent; named one of America’s Best Real Estate Agents by REAL Trends; connect with Keri on Facebook
8. Face your fear and rebuild.

Image credit:
The Oracles
As a young entrepreneur, my greatest fear was not succeeding in business. After I tasted success, it evolved into a fear of losing what I’d worked so hard to accomplish. So, when I lost millions from a fraudulent business partner, my greatest fear came true. I was devastated by despair, doubt, and depression. Over time, a beautiful lesson emerged from the pain: When you face your greatest fear, you realize it’s not as bad as you imagined.
Even on the verge of financial ruin, my situation couldn’t kill me. I learned that I never have to fear financial scarcity because I’m not afraid to work hard. We have unlimited options if we remain resourceful. With a positive mindset, we can always rebuild. We grow even faster because we’re more experienced, wiser, and stronger. New passion, purpose, and confidence reverberate from those who rise up from the ashes of their fear. —Tom Shieh, CEO of Crimcheck; connect with Tom on Facebook
9. Charge forward with a plan.

Image credit:
The Oracles
Fear was always something that could stop me dead in my tracks until I tried a more logical approach to facing it. I learned that I should not only lean in but write down a plan to address it head-on by asking “why” or “so what” at least five levels deep.
What is the fear that is holding me back? Why is it there? What happens if it comes true? How would I address it? What good could come from it? How could I avoid it? What is the consequence if I don’t go for it? Why is this fear nonexistent moving forward? Once I address the deepest part of my fear, it’s often much smaller than my imagination lets me believe. —Ashley Alderson, founder and CEO of The Boutique Hub; cancer survivor, motivational speaker, seven-figure entrepreneur, and host of “Boutique Chat”
Want to share your insights in a future article? Join The Oracles, a mastermind group of the world’s leading entrepreneurs who share their success strategies to help others grow their businesses and build better lives. Apply here.
For more articles like this, follow The Oracles on Facebook, Twitter, LinkedIn, and Instagram.
Source link
from RSSUnify feed https://hashtaghighways.com/2019/01/31/9-ways-to-conquer-fear-and-realize-your-true-potential/
from Garko Media https://garkomedia1.tumblr.com/post/182459457719
0 notes
Last Seen Blogs

andrea-clark
Our life dreams the utopia

myfaireladies
belles mademoiselles

datsarcasm
Tracing Patterns..

renanfaccini
RF BLOG

ivanakonyaaltiantalya
Ivana Antalya