#labs for pancreatic cancer
Text
Why do i waste so much time on here- oh right scrolling genuinely drowns out my stupid brain sometimes
#I went to the dr for stomach pain and one of the labs they ordered was for lipase#Me a young person who doesn't smoke or drink or have any family history of pancreatic cancer: “what if I have pancreatic cancer”#I'm pretty good at dealing with intrusive thoughts these days but sometimes the mind dogs just keep barking
2 notes
·
View notes
Text

Pausing Pancreatic Cancer
The role of a protein called CYRI-B in the progression of pancreatic cancer revealed in lab-grown cells and in a mouse model – insights for controlling cancer spread [metastasis]
Read the published research article here
Still from video from work by Savvas Nikolaou and colleagues
CRUK Scotland Institute, Switchback Road, Bearsden, Glasgow, UK
Video originally published with a Creative Commons Attribution 4.0 International (CC BY 4.0)
Published in eLife, May 2024
You can also follow BPoD on Instagram, Twitter and Facebook
8 notes
·
View notes
Text
Note that the studies that were released by companies affiliated with polluters happened in 2019, during the trump administration.
Excerpt from this story from Inside Climate News:
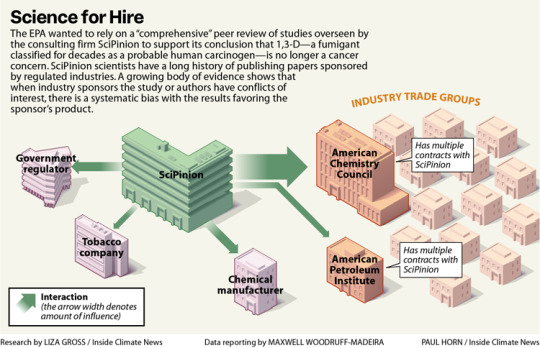
On a Southern California spring morning in 1973, a tanker truck driver jackknifed his rig and dumped the agricultural fumigant he was transporting onto a city street. A Los Angeles Fire Department emergency response team spent four hours cleaning up the chemical, 1,3-dichloropropene, or 1,3-D, a fumigant sold as Telone that farmers use to kill nematodes and other soil-dwelling organisms before planting.
Seven years after the spill, two emergency responders developed the same rare, aggressive blood cancer—histiocytic lymphoma—and died within two months of each other. In 1975, a farmer who’d accidentally exposed himself to 1,3-D repeatedly through a broken hose was diagnosed with another blood cancer, leukemia, and died the next year.
Within a decade of the men’s deaths, described as case studies in JAMA Internal Medicine, the National Toxicology Program, or NTP, reported “clear evidence” that 1,3-D causes cancer in both rats and mice. The finding led the U.S. Environmental Protection Agency to classify the chemical as “likely to be carcinogenic to humans” the same year, 1985. So it wasn’t a surprise when researchers at the University of California, Los Angeles reported in 2003 that Californians who’d lived at least two decades in areas with the highest applications of 1,3-D faced a heightened risk of dying from pancreatic cancer.
Yet EPA’s Office of Pesticide Programs’ Cancer Assessment Review Committee, or CARC, concluded in 2019 that 1,3-D—originally embraced by tobacco companies for its unparalleled ability to kill anything in soil that might harm their plants—isn’t likely to cause cancer after all.
In doing so, EPA, whose mission is to protect human health and the environment, rejected the human evidence, calling the UCLA study “low quality.” It also dismissed the authoritative NTP study and studies in lab animals that documented 1,3-D’s ability to damage DNA, a quintessential hallmark of cancer.
Instead, EPA’s CARC relied on studies provided by Dow AgroSciences (now called Corteva), the primary manufacturer of 1,3-D, and proposed a review of evidence linking the fumigant to cancer by SciPinion, a consulting firm hired by Dow, as an external peer review of its work. The decision to entrust external review to a Dow contractor has drawn repeated criticism, including from the agency’s watchdog, the Office of Inspector General, or OIG.
“During EPA’s search of the open literature, a comprehensive third-party peer review of the cancer weight-of-evidence assessment that considered toxicokinetics, genotoxicity and carcinogenicity data for 1,3-D was conducted and published in 2020 by SciPinion,” said agency spokesperson Timothy Carroll. EPA argued that the SciPinion review satisfied the criteria for an external review, Carroll said, and that another panel would have arrived at the same conclusion, given the specialized expertise required.
The OIG had recommended EPA conduct an external peer review of its 1,3-D cancer risk assessment in a 2022 report that outlined several problems with the agency’s process. An external review, the OIG said, requires “independence from the regulated business,” again noting the deficiency in a new report released in early August.
The scientists who run SciPinion have long consulted for manufacturers of harmful products, often publishing studies that deploy computer models to question the need for more protective health standards.
4 notes
·
View notes
Text
Warning : This post is going to be a very personal rage dump/rant.
There are heavy topics involved, including cancer and death. Also explicit language.
Out of consideration and respect to those of you who would prefer not to read it (since I completely understand why you wouldn’t want to), I will continue under the cut
Also pictures of my dogs, to break up the doom and gloom ^^"
-------------------------
I absolutely despise, loathe, hate toxic people.
Especially when those toxic people are the “wolf in sheep’s clothing” type.
Especially when those people don’t have the fucking balls to confront others directly and just choose to slink about behind the scenes like scummy little vermin.
So… my uncle Joe passed away a few days ago.
It was expected. He had been battling pancreatic cancer, which ended up spreading into his liver and lungs.
With that being said, even though he will be dearly missed, at least he no longer has to suffer.
I was close with my uncle.
In fact, it’s no exaggeration to say that I was much closer to him than I was with my own father (my Dad was a permanent presence in my life up until the day he died, but we had an extremely tumultuous, dysfunctional, volatile, abusive relationship.)
We visited my uncle Joe regularly ever since I was a baby, all the way up until somewhat recently. He spent countless hours at our place throughout the years. He was super close with my parents, doing tons of outdoorsy activities with them. I spent a good amount of my childhood with his family. When his wife passed away, my parents helped him and supported him. He helped us move twice. My Mom took his kids places when she was just dating my Dad. When my Dad passed away, my uncle Joe was there for me without me even having to ask.
Literally everything was good between us, and always has been.
It’s also thanks to my uncle Joe that we gained a new furry member of our family last year, who we named Dandy 💙 my uncle’s dog had puppies, he asked how many we wanted, so we took one lol
(I’ll include a few poor quality pictures because… well, I should probably break up this message with a little “positivity”, right?)
~~~~~~~~~~~~~
This was Dandy when he was still just a baby, 4 weeks and 3 days old.


Look at the cute little potato 🥹
We visited my uncle Joe every week to see him grow and develop, anxiously waiting until he was old enough to bring home.
And this was the day he finally joined our family ~

Look at how tiny he was compared to my one Black Lab (sorry for the terrible quality picture. Our carpets are old, but I swear they don't look that dingy ^^")

And here's Dandy today, one year and five months later ~



~~~~~~~~~~~~~~~~~~~~
Anyway! Back to my rage-fueled rant :
My uncle Joe met someone about a year and a half ago, and she moved in with him pretty quickly.
Which certainly wasn't a bad thing. We were genuinely happy for him.
She seemed very nice, sweet, accepting, kind, receptive, and welcoming.
But for whatever reason, the dynamic changed the moment my uncle fell ill and the control landed in her hands.
Since my uncle Joe was sick, we all mutually decided that it would be best if communication was between my Mom/me and her (we would text her to check in to see how he was doing, as well as find out if/when it was a good time for us to visit)
This is where some inconsistencies started to appear.
For example :
She would tell us not to visit because my uncle was too sick (which was totally understandable!), but then would tell us a few days later how he was doing great and had fishing trips planned all week.
I 100% believed her at the time.
After all, everyone has both good and bad days.
But then when we would visit, my uncle Joe told us how he couldn’t fish anymore because the chemo was causing neuropathy in his hands, and he couldn’t hold his fishing pole or cast/reel the line in.
Though we just assumed he discovered those issues after she told us about those supposed fishing trips.
But the true eye-opener happened during our one visit. My uncle Joe welcomed us into his home, we talked, found out some updates about his health (which was declining), etc. He was open/transparent with us about everything.
When my uncle went to the bathroom during that visit, his girlfriend made the comment “I probably should have told you guys not to come here, since he’s in a lot of pain today.”
Knowing my uncle, I didn’t budge from my seat. I knew that if he wasn’t up for company, he wouldn't hesitate to tell us to leave.
And I’m glad we didn’t leave… because literally 10 minutes later, her granddaughter came waltzing in to visit her.
My uncle came out of the bathroom, sat on the sofa doubled over in pain as he was talking to me and my Mom (at this time, we asked him directly if we should leave, since we knew he was dealing with a lot and we didn't want to overstay our welcome. He told us not to leave, that we could stay because he felt like shit regardless).
But as he was sitting there, clearly in pain, his girlfriend and her granddaughter asked him to get up and carve a watermelon for them instead of doing it themselves.
What sense does that make?
'I should have told you guys to stay away, but I’m gonna make him strain himself and carve a watermelon for us even though he’s already suffering and struggling enough'
…. Okay. Fuck you too.
We obviously didn’t say anything. We just visited for a little while longer, then left with a friendly/cordial “goodbye, nice to see you again” to her and her granddaughter, told my uncle that we would be thinking about him and see him again, and wished them a good day.
Two and a half months passed before we heard from them again.
Why? Because she refused to answer our numerous calls and texts.
She deliberately ignored us, which actively prevented us from having an opportunity to see my uncle.
And she knew damn well that we wouldn’t just show up at my uncle’s house unannounced because we didn’t want to disturb him if he wasn’t feeling up for company.
We only got in contact with him again after he directly called our phone and left a message saying “hey, just checking in. I hope you’re both doing okay, since I haven’t heard from either of you in a while. Stop by when you can”.
So we went to his house.
When we explained the situation to my uncle Joe/passive aggressively confronted his girlfriend, her excuse was “oh, sorry. The reception here is bad so my phone was probably just acting up.”
For two and a half months?
Even though she was literally using her phone in front of us, which appeared to be working perfectly fine?
Even though she’s always on her phone every time we see her?
Even though she could have reached out to us, yet chose not to? Not even once in two and a half months??
I call bullshit.
My Mom even told her that she was on the verge of sending a text that said “okay, cunt.” since we thought she was ignoring us after not responding to our multiple texts/calls.
We all laughed it off as a joke, Joe's girlfriend even said “hahaha, I probably would have laughed if I got a text like that!” … but it most certainly was not a joke.
(My Mom is extremely outspoken and normally doesn’t hold back, especially when it counts. She’s the type of person you either love or hate, but she’s definitely one of a kind and the perfect example of a strong, independent woman who gives zero fucks lol)
Anyway, that visit went well. We behaved like usual, talked to both my uncle and his girlfriend normally, caught up on stuff, etc.
After that interaction, his girlfriend miraculously responded to every single call and text (bad reception, huh? Funny how she had zero service issues after we called her out in front of my uncle)
But basically every time we talked with her, she would say “it’s not a good time to come by, he’s really sick.”
And we would always respond with things like “we totally understand”, “thank you so much for letting us know”, “we wish there was something we could do to help”, “we’re here for you if you ever need anything or anyone to talk to since we know this also isn’t easy for you”, “we’ll check in next weekend”, “please take care of yourself”, “we’ll be thinking about you”, etc.
Then finally, my uncle Joe told us to stop up again two weeks ago. So we did.
He was extremely sick and remained in bed, but we said hello and he told us that we are more than welcome there and we could just visit with his girlfriend. So we did. The visit remained cordial and friendly.
The next day, my uncle called and apologized for not getting up when we were there.
We immediately told him that he has absolutely no reason to be sorry, that we completely and wholeheartedly understand, that we would understand even if he told us to leave the moment we arrived, and that we were keeping him in our thoughts.
The week after that, his girlfriend said he was too sick for company (which again, we obviously understood and thanked her for letting us know, wished them the best, etc).
We didn’t visit my uncle Joe after that. He passed away before we had another opportunity to see him.
Now, here’s where my anger starts to come into play :
His girlfriend didn’t let us know when he passed away.
We found out from my other uncle, Mike, two days later. (My Dad had 3 brothers. His eldest brother is my uncle Joe who just passed away. His youngest brother is my uncle Mike who let us know what happened.)
So my Mom called her and offered her condolences, asked how she was doing, told her that we’re here for her, and asked about the arrangements. My Mom also told her that Mike was the one who let us know about Joe.
She made the comment “there’s going to be a small ceremony, but only for immediate family.”
Which didn’t make sense to me or my Mom. We were both very close with my uncle Joe, we are family. So that comment seemed a bit… off?
But we dismissed it and instead talked to my uncle Mike.
We asked him to please keep us updated, since we wanted to pay our respects to my uncle Joe and our family.
Well… I don’t know what the Hell that lady said to my cousin (Joe’s son), but he told my uncle Mike not to tell us anything else.
That snake in the grass obviously ran back and told my cousin that we found out about Joe’s passing from Mike.
But uhh... We deserved to know.
Now, we literally just found out this morning that the ceremony was held yesterday. We weren't invited (the day/time wasn't publicly announced).
We were excluded. We were denied the opportunity to say our final goodbye.
I blame his girlfriend. Completely and entirely.
I especially find it super interesting that she didn’t attend the ceremony either… almost like she was afraid that we might possibly show up and confront her (which we would never do, purely out of respect for my uncle Joe)
When my uncle Mike told us, he apologized. But we told him that we don’t blame him, since we certainly didn’t want to put him in the middle of it.
It just pisses me the fuck off.
Bad enough she actively prevented us from seeing my uncle Joe, even on his “good” days. But then to keep us away from the ceremony too?
And she HAD to have fed my cousin a bunch of lies and bullshit to cause him to tell my uncle Mike not to inform us of anything. (Luckily for us, my uncle Mike loves to talk so he didn’t mind spilling the tea. He just felt guilty for not doing so sooner. But I understand why he waited, and I hold zero animosity towards him)
It’s especially confusing and upsetting since we always remained on good terms with all of my cousins.
We saw my cousins regularly, got along well with them, joked around with them.
Literally nothing that we did or didn’t do would warrant such a reaction from them.
If there was any fault on our end, I certainly wouldn’t be angry about this situation or waste my time typing this up. (I'm not the type of person who plays the victim, I admit when I'm wrong and own up to my faults/wrongdoings. That just isn't the case here.)
So it’s seriously a mystery to me… which is why I blame my uncle Joe’s girlfriend.
Absolutely nothing changed in the decades of knowing my uncle and his kids. Literally the only recent change was her coming into the picture.
(I also want blame my cousin, since he’s older than me and has a mind of his own… but I also know that he’s grieving the loss of his father, so I feel like that bitch took advantage of the situation to say whatever she wanted about us while my cousin is vulnerable and not thinking clearly/properly).
Regardless of the finer details…. I am absolutely livid.
It’s like a giant “fuck you” to us, like we aren’t good enough, like our feelings don’t matter.
And that pisses me off beyond belief.
I’m debating whether or not I should confront her.
On one hand, I probably should just let it go and move on.
But on the other hand… I want to play dumb, call her, and be like “How are you doing? Do you know when the ceremony is?“ just to see what she says.
And then tell her to go fuck herself.
Is that immature of me? Sure.
But I’m angry. Annoyed. Irritated. Fuming. My rage is boiling, my wrath is building. And I feel like exploding.
Needless to say… my Mom was right. That lady is a cunt. A toxic, festering, diabolical, oozing, gaping, pungent cunt.
If you’ve read up to this point, I genuinely apologize for dumping all of this off here.
I just needed to vent a bit.
I also owe everyone who has tagged me a HUGE thank you. You have all given me a much needed distraction from everything, plus I genuinely love being tagged.
So I will absolutely start posting/replying to those a little later (I've already started on them and have them saved in my drafts, I just want to finish them all and post everything at once lol)
#I might delete this later#I find comfort in the idea that Satan would be proud of my wrath/anger right now lol#all joking aside....#I have so much to say to her yet she's not worth the time or energy#I'm over the two-faced high school bullshit#maybe she likes drama but I don't#just another reason for me to hate people#it might be sad to say but....#... Tumblr is the only place where I can count on interacting with genuinely nice people#I just feel bad for being so damn dismissive/absent lately#I promise I'll make it up to you all#and thank you for being so patient with me 💙#nerdy talks#nerdy vents#nerdy rages#?#I am angry#personal#rest in peace uncle joe 💙
18 notes
·
View notes
Text
Between pancreatic cancer and diabetes, I think it's clear that it's best if humanity and the pancreas part ways.
And by that I mean someone in a lab somewhere needs to find a way to eliminate the need for a pancreas
4 notes
·
View notes
Text
I don’t really wanna talk about it but I need to tell a couple of folks what’s going on.
I’m not actively dying, but I’m not doing too good. I’ve got some tests on Tuesday to start checking me for pancreatic cancer and so far, according to the labs and such, it’s not great. There’s something Horribly Wrong with my pancreas and possibly (probably) my liver but nobody seems to want to say the C word. I’ve got a CT with contrast, abdominal ultrasound, and more labs this Tuesday and then they’ll talk about doing a biopsy or going in for a closer look.
My blood counts are way down. I’m just not making enough RBCs and platelets to keep going. Hit my knee yesterday (the day before?) on the edge of my desk and this giant balloon happened and I had to mash on it for half an hour to get it to stop. Like when you get blood drawn and a vein blows, and it eggs up, but huge
I’m more than a little freaked out. I’ve gone to the doc twice this month already. We can’t afford this. This is gonna delay my gut stuff. If it’s the Really Bad thing, will they just never put me back together?
Meanwhile I’m still dropping weight and losing hair. I let it grow out a bit so I’m noticing more and more falling out. Probably gonna just buzz it instead of going for the undercut I wanted so I stop noticing the difference between me losing hair and the cats shedding.
I don’t have a sense of impending doom so maybe it’s not that bad. There’s a chance it’s a stone trapped in a duct leftover from when they snatched out my gallbladder a few years back. Gonna hope that’s all it is. The GI and the surgeon seem to disagree on that. The GI thinks it’s the stone, the surgeon keeps bringing up biopsies. I’m gonna let the GI do this thing Tuesday and hope a stone shows up somewhere on some result.
Thing is, that really wouldn’t cause the kind of trouble I’m having. Not to the extent I’m having it. I’m not malnourished enough for organ failure either but I brought up a possible port for TPN. Better to float the idea early on and give them time to consider the option.
Anyway, fingers crossed. If I’m very lucky it’s an easy fix.
0 notes
Text
DNA Repair - Postdoctoral Fellow Position
Rutgers Cancer Institute of New Jersey
Post-Doctoral Fellow Position in DNA Repair/Pancreatic Cancer
See the full job description on jobRxiv: https://jobrxiv.org/job/rutgers-cancer-institute-of-new-jersey-27778-dna-repair-postdoctoral-fellow-position-3/?feed_id=80636
#DNA_repair #pancreatic_cancer #ScienceJobs #hiring #research
0 notes
Text
Histopathology Services Market Trends and Forecast 2024-2033
“Global Insight Services offers unparalleled market intelligence and strategic consulting services to businesses worldwide. Our expertise spans across various industries, including healthcare, technology, and consumer goods, providing comprehensive analysis and actionable insights. By leveraging advanced data analytics and in-depth market research, we empower our clients to make informed decisions, identify growth opportunities, and stay ahead of the competition”.
The global Histopathology Services Market was valued at USD 22.8 Billion in 2022 and it is anticipated to grow up to USD 38.4 Billion by 2032, at a CAGR of 5.4% during the forecast period.
View The Full Report Here –https://www.globalinsightservices.com/reports/histopathology-services-market
Histopathology services are used in the examination of biological tissues for the diagnosis of diseases. The procedure includes microscopic examination of tissues. With the help of imaging techniques biopsy tissues can now be obtained from certain inaccessible sites such as pancreas and the peritoneum.
Market Trends and Drivers
Factors such as rising demand for biologics and increasing prevalence of chronic diseases are driving the histopathology services market. However, limitations associated with histopathology and immunohistochemistry are expected to restrict the market growth to a certain extent during the forecast period. Further, increasing government support to advance the smart technologies in preliminary diagnosis has led to robust development of histopathology services. Additionally, technology has played crucial in minimizing the complication of the manual process and advanced the existing histopathology technologies. Other factors like increasing public investments in advancing the histopathology services have fuelled the growth of the market. On the other hand, limitations associated with histopathology and immunohistochemistry is expected to restrain the overall market growth to a certain extent during the forecast period.
Market Restraints and Challenges
The disadvantages of histology and histological staining include: Preparation of the slides using the paraffin technique can be time-consuming; frozen slides are faster to prepare, but this can affect the resolution, especially when using light microscopy. However, limitations associated with histopathology and immunohistochemistry are expected to restrict the market growth to a certain extent during the forecast period. Subspecialisation in the diagnostic surgical pathology service and cytology; frozen sections; the autopsy; multidisciplinary team meetings; ancillary techniques; the pathology report and some other administrative duties.
Unlock Growth Potential in Your Industry – Get Your Sample Report Now-https://www.globalinsightservices.com/request-sample/GIS10504
Global Histopathology Services Market Segmentation
By Type
Surgical Specimen
Breast Biopsy
Lung Biopsy
Renal Biopsy
Gastrointestinal Biopsy
Pancreatic Biopsy
Skin Tissue Biopsy
Testicular Biopsy
Others
By End-user
Diagnostic Laboratories and Reference Laboratories
Research Institutes
Others
Major Players in the Global Histopathology Services Market
The key players in the market are Sonic Healthcare Limited; Laboratory Corporation of America Holdings; Acculabs Diagnostics UK Ltd; TPL Path Labs; UNILABS; Cureline Global Translational CRO; Targos; Cellular Pathology Services; Experimental Pathology Laboratories Inc (EPL); and CHARLES RIVER LABORATORIES, INC.. among others.
COVID-19 Impact:
At present, COVID-19 has made a major impact on the healthcare industry. Since the outbreak reached the U.S. in January 2020, hospitals, pharmacies, and other facilities have had to address challenges at a magnitude that had never been seen before. Moreover, according to a recent survey by Medscape in April 2020, substantial disruption have been witnessed in routine cancer care that includes tests for screening and diagnosis in suspected cases to their treatment as a result of the COVID-19 pandemic. The rapid increase in the number of infected patients in the US and Canada is likely to hamper the growth of histopathology services market and result in slowing down the market growth in the near future. Currently, many countries are now undergoing lockdown relaxations, and most hospitals have resumed elective surgeries. As a result, the number of diagnostic tests conducted is now increasing. Owing to the factors mentioned above, the overall growth rate of the anatomic pathology market is less when compared to the previous year.
Buy Now@https://www.globalinsightservices.com/checkout/single_user/GIS10504
Research Scope
Scope – Highlights, Trends, Insights. Attractiveness, Forecast
Market Sizing – Product Type, End User, Offering Type, Technology, Region, Country, Others
Market Dynamics – Market Segmentation, Demand and Supply, Bargaining Power of Buyers and Sellers, Drivers, Restraints, Opportunities, Threat Analysis, Impact Analysis, Porters 5 Forces, Ansoff Analysis, Supply Chain
Business Framework – Case Studies, Regulatory Landscape, Pricing, Policies and Regulations, New Product Launches. M&As, Recent Developments
Competitive Landscape – Market Share Analysis, Market Leaders, Emerging Players, Vendor Benchmarking, Developmental Strategy Benchmarking, PESTLE Analysis, Value Chain Analysis
Company Profiles – Overview, Business Segments, Business Performance, Product Offering, Key Developmental Strategies, SWOT Analysis.
With Global Insight Services, you receive:
10-year forecast to help you make strategic decisions
In-depth segmentation which can be customized as per your requirements
Free consultation with lead analyst of the report
Infographic excel data pack, easy to analyze big data
Robust and transparent research methodology
Unmatched data quality and after sales service
Contact Us:
Global Insight Services LLC
16192, Coastal Highway, Lewes DE 19958
E-mail: [email protected]
Phone: +1-833-761-1700
Website: https://www.globalinsightservices.com/
About Global Insight Services:
Global Insight Services (GIS) is a leading multi-industry market research firm headquartered in Delaware, US. We are committed to providing our clients with highest quality data, analysis, and tools to meet all their market research needs. With GIS, you can be assured of the quality of the deliverables, robust & transparent research methodology, and superior service.
#Histopathology Services MarketÂ#Histopathology Services Market ForecastÂ#Histopathology Services Market AnalysisÂ#Histopathology Services Market DemandÂ#Histopathology Services Market GrowthÂ
0 notes
Text
New and Updated Topics
The Patient Education Institute has published, reviewed or updated 82 titles in Q1 and Q2 2024.
Aid Tools for Older Adults English
Amputation of the Leg English
Anal Cancer English
Anterior Cruciate Ligament Repair - ACL Repair English
Aplastic Anemia English
Bile Duct Diseases and Problems English
Birth Control - Contraception (Arabic) Arabic
Blood and Blood Disorders English
Bronchitis English
Building and Keeping Healthy Habits English
Cancer Clinical Trials English
Cannabis English
Cardiac Catheterization - Coronary Angiography English
Carotid Endarterectomy English
Cerebral Palsy English
Cerebral Palsy - Pediatrics English
Cervix Disorders (Arabic) Arabic
Changes as We Get Older English
Cholecystectomy - Open and Laparoscopic English
Common Accidents Among Older Adults English
COVID-19 - Coronavirus English
COVID-19 - Coronavirus (Arabic) Arabic
COVID-19 - Coronavirus (Spanish) Spanish
De Quervain's Tendonitis (Arabic) Arabic
Diabetes - Introduction English
Ectopic Pregnancy English
Electroconvulsive Therapy - ECT (Arabic) Arabic
Encephalitis English
Fun Ways to Make Your Retirement Better English
Gallstones English
Game Addiction in Older Adults English
Gastrointestinal Bleeding English
H1N1 Influenza English
Health Problems in Pregnancy English
Hearing Loss English
HIV/AIDS and Infections English
HIV/AIDS and Pregnancy English
Hysteroscopy English
Influenza - Flu English
Influenza - Pediatrics English
Inguinal Hernia Repair - Pediatrics (Arabic) Arabic
Iron Overload - Hemochromatosis (Arabic) Arabic
IVP - Intravenous Pyelogram English
Keeping a Positive Mindset English
Keeping Your Retirement Money Safe from Crimes English
Leukemia English
Living with Congestive Heart Failure (Arabic) Arabic
Long-Term Care Insurance English
Making Your Body's Immune System Stronger English
Midlife Crises and Transitions English
Moles English
Mumps English
Newborn Screening English
Open Shoulder Surgery English
Organizing Your Medications English
Palliative Care and Hospice Care English
Pancreatitis English
Pediatric Post-Operative Instructions English
Port Catheter Insertions (Arabic) Arabic
Preventing Strokes English
Preventing Trips and Falls English
Pulmonary Fibrosis English
Reading Lab Results English
Reporting and Preventing Elder Abuse English
Sexuality and Aging English
Shoulder Replacement English
Sjogren's Syndrome English
Stellate Block (Arabic) Arabic
Suicide in Older Adults English
The A1C Test English
The FODMAP Diet for Digestive Health English
Thoracotomy English
Tracheotomy or Tracheostomy (Arabic) Arabic
Transient Ischemic Attack - TIA English
Understanding Medicare English
Upper GI Endoscopy English
Upper GI Endoscopy and Colonoscopy English
Viagra - Sildenafil English
Warfarin - Introduction for New Users English
Warfarin - Introduction for New Users - Pediatrics English
Warfarin - Review for Current Users English
What to Expect When You Retire English
0 notes
Photo

Branching Out
Cancer comes in all shapes and sizes. Pancreatic ductal adenocarcinoma (PDAC) forms branching structures as it arises from a tissue made of tube-like structures called glandular branched epithelia. The branching structure of PDAC is thought to contribute to its aggressiveness. However, current PDAC models cultured in the lab are spherical. To better mimic PDAC, researchers now present a new model grown from single mouse PDAC cells in a 3D collagen matrix with a mix of specific chemicals. This produced a mass of tissue that organised itself into highly branched structures that replicated the architecture of PDAC in humans, as captured using fluorescence microscopy (pictured). Using this model, the team identified the different stages and characteristics of PDAC development, including changes in cell movements, proteins and molecules. This branching model, therefore, provides a useful replica to investigate the dynamics of PDAC.
Written by Lux Fatimathas
Image from work by S. Randriamanantsoa and A. Papargyriou, and colleagues
Lehrstuhl für Zell Biophysik E27, Physik Department and Center for Functional Protein Assemblies, Technische Universität München, Garching, Germany
Image originally published with a Creative Commons Attribution 4.0 International (CC BY 4.0)
Published in Nature Communications, September 2022
You can also follow BPoD on Instagram, Twitter and Facebook
#science#biomedicine#pancreatic cancer#cancer#pancreas#fluorescence microscopy#immunofluorescence#organoid
8 notes
·
View notes
Text
MIT Faculty Founder Initiative announces three winners of entrepreneurship awards
New Post has been published on https://thedigitalinsider.com/mit-faculty-founder-initiative-announces-three-winners-of-entrepreneurship-awards/
MIT Faculty Founder Initiative announces three winners of entrepreneurship awards

Patients with intractable cancers, chronic pain sufferers, and people who depend on battery-powered medical implants may all benefit from the ideas presented at the 2023-24 MIT-Royalty Pharma Prize Competition’s recent awards. This year’s top prizes went to researchers and biotech entrepreneurs Anne Carpenter, Frederike Petzschner, and Betar Gallant ’08, SM ’10, PhD ’13.
MIT Faculty Founder Initiative Executive Director Kit Hickey MBA ’13 describes the time and hard work the three awardees and other finalists devoted to the initiative and its mission of cultivating female faculty in biotech to cross the chasm between laboratory research and its clinical application.
“They have taken the first brave step of getting off the bench when they already work seven days a week. They have carved out time from their facilities, from their labs, from their lives in order to put themselves out there and leap into entrepreneurship,” Hickey says. “They’ve done it because they each want to see their innovations out in the world improving patients’ lives.”
Carpenter, senior director of the Imaging Platform at the Broad Institute of MIT and Harvard, where she is also an institute scientist, won the competition’s $250,000 2023-24 MIT-Royalty Pharma Faculty Founder Prize Competition Grand Prize. Carpenter specializes in using microscopy imaging of cells and computational methods such as machine learning to accelerate the identification of chemical compounds with therapeutic potential to, for instance, shrink tumors. The identified compounds are then tested in biological assays that model the tumor ecosystem to see how the compounds would perform on actual tumors.
Carpenter’s startup, SyzOnc, launched in April, a feat Carpenter associates with the assistance provided by the MIT Faculty Founder Initiative. Participants in the program receive mentorship, stipends, and advice from industry experts, as well as help with incorporating, assembling a management team, fundraising, and intellectual property strategy.
“The program offered key insights and input at major decision points that gave us the momentum to open our doors,” Carpenter says, adding that participating “offered validation of our scientific ideas and business plan. That kind of credibility is really helpful to raising funding, particularly for those starting their first company.”
Carpenter says she and her team will employ “the best biological and computational advancements to develop new therapies to fight tumors such as sarcoma, pancreatic cancer, and glioblastoma, which currently have dismal survival rates.”
The MIT Faculty Founder Initiative was begun in 2020 by the School of Engineering and the Martin Trust Center for MIT Entrepreneurship, based on research findings by Sangeeta Bhatia, the Wilson Professor of Health Sciences and Technology, professor of electrical engineering and computer science, and faculty director of the MIT Faculty Founder Initiative; Susan Hockfield, MIT Corporation life member, MIT president emerita, and professor of neuroscience; and Nancy Hopkins, professor emerita of biology. An investigation they conducted showed that only about 9 percent of MIT’s 250 biotech startups were started by women, whereas women made up 22 percent of the faculty, as was presented in a 2021 MIT Faculty Newsletter.
That data showed that “technologies from female labs were not getting out in the world, resulting in lost potential,” Hickey says.
“The MIT Faculty Founder Initiative plays a pivotal role in MIT’s entrepreneurship ecosystem. It elevates visionary faculty working on solutions in biotech by providing them with critical mentorship and resources, ensuring these solutions can be rapidly scaled to market,” says Anantha Chandrakasan, MIT’s chief innovation and strategy officer, dean of engineering, and Vannevar Bush Professor of Electrical Engineering and Computer Science.
The MIT Faculty Founder Initiative Prize Competition was launched in 2021. At this year’s competition, the judges represented academia, health care, biotech, and financial investment. In addition to awarding a grand prize, the competition also distributed two $100,000 prizes, one to a researcher from Brown University, the first university to collaborate with MIT in the entrepreneurship program.
This year’s winner of the $100,000 2023-24 MIT-Royalty Pharma Faculty Founder Prize Competition Runner-Up Prize was Frederike Petzschner, assistant professor at the Carney Institute for Brain Science at Brown, for her SOMA startup’s digital pain management system, which helps sufferers to manage and relieve chronic pain.
“We leverage cutting-edge technology to provide precision care, focusing specifically on personalized cognitive interventions tailored to each patient’s unique needs,” she says.
With her startup on the verge of incorporating, Petzschner says, “without the Faculty Finder Initiative, our startup would still be pursuing commercialization, but undoubtedly at a much earlier and perhaps less structured stage.”
“The constant support from the program organizers and our mentors was truly transformative,” she says.
Gallant, associate professor of mechanical engineering at MIT and winner of the $100,000 2023-24 MIT-Royalty Pharma Faculty Founder Prize Competition Breakthrough Prize, is leading the startup Halogen. An expert on advanced battery technologies, Gallant and her team have developed high-density battery storage to improve the lifetime and performance of such medical devices as pacemakers.
“If you can extend lifetime, you’re talking about longer times between invasive replacement surgeries, which really affects patient quality of life,” Gallant told MIT News in a 2022 interview.
Jim Reddoch, executive vice president and chief scientific officer of sponsor Royalty Pharma, emphasized his company’s support for both the competition and the MIT Faculty Finder Initiative program.
“Royalty Pharma is thrilled to support the 2023-2024 MIT-Royalty Pharma Prize Competition and accelerate life sciences innovation at leading research institutions such as MIT and Brown,” Reddoch says. “By supporting the amazing female entrepreneurs in this program, we hope to catalyze more ideas from the lab to biotech companies and eventually into the hands of patients.”
Bhatia has referred to the MIT Faculty Founder Initiative as a “playbook” on how to direct female faculty’s high-impact technologies that are not being commercialized into the world of health care.
“To me, changing the game means that when you have an invention in your lab, you’re connected enough to the ecosystem to know when it should be a company, and to know who to call and how to get your first investors and how to quickly catalyze your team — and you’re off to the races,” Bhatia says. “Every one one of those inventions can be a medicine as quickly as possible. That’s the future I imagine.”
Co-founder Hockfield referred to MIT’s role in promoting entrepreneurship in remarks at the award ceremony, alluding to Brown University’s having joined the effort.
“MIT has always been a leader in entrepreneurship,” Hockfield says. “Part of leading is sharing with the world. The collaboration with Brown University for this cohort shows that MIT can share our approach with the world, allowing other universities to follow our model of supporting academic entrepreneurship.”
Hickey says that when she and Bhatia asked 30 female faculty members three years ago why they were not commercializing their technologies, many said they had no access to the appropriate networks of mentors, investors, role models, and business partners necessary to begin the journey.
“We encourage you to become this network that has been missing,” Hickey told the awards event audience, which included an array of leaders in the biotech world. “Get to know our amazing faculty members and continue to support them. Become a part of this movement.”
#000#2022#2023#2024#250#Advice#amazing#approach#Awards#honors and fellowships#battery#battery-powered#Bioengineering and biotechnology#Biology#biotech#Brain#Broad Institute#Business#Cancer#Cells#chemical#chemical compounds#chronic pain#collaborate#Collaboration#Companies#competition#computer#Computer Science#Contests and academic competitions
0 notes
Link
0 notes
Text
Breakthrough in fight against world's deadliest cancer - new drug shrunk up to 70% of pancreatic tumors in lab study:
Larry G. Potter
Senior Insurer Underpayment Recovery Advisor For Hospitals

0 notes
Text
MIT researchers develop advanced machine learning models to detect pancreatic cancer

MIT researchers develop advanced machine learning models to detect pancreatic cancer.
MIT CSAIL researchers develop advanced machine-learning models that outperform current methods in detecting pancreatic ductal adenocarcinoma.
Prismatic perspectives pancreatic cancer
The path forward
The first documented case of pancreatic cancer dates from the 18th century. Since then, researchers have embarked on a long and difficult journey to better understand this elusive and deadly disease. To date, early intervention is the most effective cancer treatment. Unfortunately, due to its location deep within the abdomen, the pancreas is particularly difficult to detect early on.
Scientists from the MIT Computer Science and Artificial Intelligence Laboratory (CSAIL), as well as Limor Appelbaum, a staff scientist in the Department of Radiation Oncology at Beth Israel Deaconess Medical Center (BIDMC), wanted to better identify potential high-risk patients. They set out to create two machine-learning models for the early detection of pancreatic ductal adenocarcinoma (PDAC), the most common type of cancer.
To gain access to a large and diverse database, the team collaborated with a federated network company and used electronic health record data from multiple institutions across the United States. This vast data set contributed to the models' reliability and generalizability, making them applicable to a wide range of populations, geographical locations, and demographic groups.
The two models—the “PRISM” neural network and the logistic regression model (a statistical technique for probability)—outperformed current methods. The team’s comparison showed that while standard screening criteria identify about 10 percent of PDAC cases using a five-times higher relative risk threshold, Prism can detect 35 percent of PDAC cases at this same threshold.
Using AI to detect cancer risk is not a new phenomenon; algorithms analyze mammograms, CT scans for lung cancer, and assist in the analysis of Pap smear tests and HPV testing, to name a few applications.
“The PRISM models stand out for their development and validation on an extensive database of over 5 million patients, surpassing the scale of most prior research in the field,” says Kai Jia, an MIT PhD student in electrical engineering and computer science (EECS), MIT CSAIL affiliate, and first author on an open-access paper in eBioMedicine outlining the new work. “The model uses routine clinical and lab data to make its predictions, and the diversity of the U.S. population is a significant advancement over other PDAC models, which are usually confined to specific geographic regions, like a few health-care centers in the U.S. Additionally, using a unique regularization technique in the training process enhanced the models' generalizability and interpretability.”
“This report outlines a powerful approach to use big data and artificial intelligence algorithms to refine our approach to identifying risk profiles for cancer,” says David Avigan, a Harvard Medical School professor and the cancer center director and chief of hematology and hematologic malignancies at BIDMC, who was not involved in the study. “This approach may lead to novel strategies to identify patients with high risk for malignancy that may benefit from focused screening with the potential for early intervention.”
Prismatic perspectives pancreatic cancer
The journey toward the development of PRISM began over six years ago, fueled by firsthand experiences with the limitations of current diagnostic practices.
“Approximately 80-85 percent of pancreatic cancer patients are diagnosed at advanced stages, where cure is no longer an option,” says senior author Appelbaum, who is also a Harvard Medical School instructor as well as radiation oncologist. “This clinical frustration sparked the idea to delve into the wealth of data available in electronic health records (EHRs).”
The CSAIL group’s close collaboration with Appelbaum made it possible to understand the combined medical and machine learning aspects of the problem better, eventually leading to a much more accurate and transparent model. “The hypothesis was that these records contained hidden clues — subtle signs and symptoms that could act as early warning signals of pancreatic cancer,” she adds. “This guided our use of federated EHR networks in developing these models, for a scalable approach for deploying risk prediction tools in health care.”
Both PrismNN and PrismLR models analyze EHR data, including patient demographics, diagnoses, medications, and lab results, to assess PDAC risk. PrismNN uses artificial neural networks to detect intricate patterns in data features like age, medical history, and lab results, yielding a risk score for PDAC likelihood. PrismLR uses logistic regression for a simpler analysis, generating a probability score of PDAC based on these features. Together, the models offer a thorough evaluation of different approaches in predicting PDAC risk from the same EHR data.
One paramount point for gaining the trust of physicians, the team notes, is better understanding how the models work, known in the field as interpretability. The scientists pointed out that while logistic regression models are inherently easier to interpret, recent advancements have made deep neural networks somewhat more transparent. This helped the team to refine the thousands of potentially predictive features derived from EHR of a single patient to approximately 85 critical indicators. These indicators, which include patient age, diabetes diagnosis, and an increased frequency of visits to physicians, are automatically discovered by the model but match physicians' understanding of risk factors associated with pancreatic cancer.
The path forward
Despite the promise of the PRISM models, as with all research, some parts are still a work in progress. U.S. data alone are the current diet for the models, necessitating testing and adaptation for global use. The path forward, the team notes, includes expanding the model's applicability to international datasets and integrating additional biomarkers for more refined risk assessment.
“A subsequent aim for us is to facilitate the models' implementation in routine health care settings. The vision is to have these models function seamlessly in the background of health care systems, automatically analyzing patient data and alerting physicians to high-risk cases without adding to their workload,” says Jia. “A machine-learning model integrated with the EHR system could empower physicians with early alerts for high-risk patients, potentially enabling interventions well before symptoms manifest. We are eager to deploy our techniques in the real world to help all individuals enjoy longer, healthier lives.”
Jia wrote the paper alongside Applebaum and MIT EECS Professor and CSAIL Principal Investigator Martin Rinard, who are both senior authors of the paper. Researchers on the paper were supported during their time at MIT CSAIL, in part, by the Defense Advanced Research Projects Agency, Boeing, the National Science Foundation, and Aarno Labs. TriNetX provided resources for the project, and the Prevent Cancer Foundation also supported the team.
Source: MIT
Read the full article
0 notes
Quote
Our study leveraged routinely collected EHR data from a federated network including 55 US HCOs to develop and validate two families of models (PrismNN and PrismLR) for identifying patients in the general population at high PDAC risk, 6–18 months before the first PDAC diagnosis. Both models were trained on 35,387 PDAC cases and 1,500,081 controls with features derived from demographics, diagnosis, medication, and lab entries in EHR. Both models used 87 features (Fig. 3) automatically selected using the training data.
A pancreatic cancer risk prediction model (Prism) developed and validated on large-scale US clinical data - eBioMedicine
0 notes
Text
Pancreatic Cancer - Postdoctoral Fellow Position
Rutgers Cancer Institute of New Jersey
Post-Doctoral Fellow Position in Pancreatic Cancer
See the full job description on jobRxiv: https://jobrxiv.org/job/rutgers-cancer-institute-of-new-jersey-27778-pancreatic-cancer-postdoctoral-fellow-position-2/?feed_id=80412
#pancreatic_cancer #ScienceJobs #hiring #research
0 notes
Last Seen Blogs

arab-123
اللغة العربية

baalkingofhell
Baal, King of Hell

flat-sansims
Oh The Things You Can Think

hawyeahjinx
Ekkkk

cyyrgrt
Sem título