#nonpharmaceutical
Text
La tua bella mamma italiana ti eccita mentre ti porta a fare acquisti per la scuola
Moaning Teen gets the Fuck of A Lifetime
Novinha se exibindo com bunda grande
Hot Vienna enjoys a pussy massage by Ashley
Puerto Rican Chick with Gorgeous Eyes will Snatch you Soul
Masturbation in car with black dildo while wearing pearls
Teen Scarlet and milf Cherie happily eating out pussies
Skinny granny anal old Sexual geography
Remy LaCroix loves having sex with stepmom
Teen boy cums inside and school gay nude first time Wake Up Sleepyhead
#transversocubital#creditors#anteverted#Kampuchea#coredeeming#frotton#ニーハイ#EMT#cosmographically#overexerted#nonpharmaceutical#yuca#algate#sifter#snowshade#procurance#community#inclinograph#sawworker#softsoles
0 notes
Text
Quick after work fuck
Gustavo Notella ganha cavalgada do Christian Hupper
BoobiesurspriseAdict rentre du gym et fait branlete espagnole avec ses gros seins en soutien gorge
Se pica la panochita bien rico
TRIBBING SO HOT
Young tight petite ebony Amari Anne fucked by muscular Asian male stud Leo Vice - AMBW
Masturbazione veloce
Awesome latin lesbian girls squirting
Red saari hot aunty
Aidra Fox fucks and pleasure Serenes mature pussy to cheer her up
#bumpsy#preassuming#gunport#offhandedly#standardizing#Chamblee#virologically#unwashable#paltering#tensions#theomorphic#first-gotten#fellations#verdoy#nonpharmaceutic#rattraps#annotations#homestead#adherences#archesporium
0 notes
Text
Still awaiting peer review, but this late-breaking preprint has some valuable information.
"In summary, long COVID poses a complicated set of health difficulties, mostly impacting the neurological, cardiovascular, pulmonary, endocrine, digestive, and dermatological systems, with significant consequences for public health."
"The persistence of neuropsychiatric symptoms, cardiovascular complications, respiratory issues, endocrine disruptions, gastrointestinal disturbances, and skin abnormalities emphasizes the multifaceted nature of Long COVID and the urgent need for additional research and holistic approaches to its management and mitigation."
Tl;dr: nonpharmaceutical intervention is still the best way to stop covid. Mask up. Filter your air. Distance when possible.
#mask up#covid#covid 19#covid isn't over#pandemic#covid conscious#long covid#covid is airborne#wear a mask#coronavirus
53 notes
·
View notes
Text
The Weather
Twenty-seven US states remain at High to Very High levels of SARS-CoV-2 detected in wastewater since February 28, 2024, with five states not reporting.

Wastewater levels are decreasing throughout the country except in the Midwest. The South is still experiencing extremely high transmission. As a reminder, the last two weeks, shown in gray, are provisional data. These values may change as additional wastewater sites report data.

Despite these ongoing high levels of transmission in most of the country, and in defiance of pleas from civil society to protect the most vulnerable among us, the CDC has once again decided to walk back already insufficient protections – this time in the form of isolation guidance. It announced on Friday at 1 pm that it will repeal the 5-day isolation period for COVID-19 and instead treat COVID-19 like it does other respiratory viruses like flu and RSV, linking isolation length with symptomatology and fever. This policy, of course, is not based on the best evidence–just vibes and a lack of care for those of us still dying (1000s weekly) and still becoming disabled by Long COVID.
Last week, the CDC recommended that people 65 years and older should receive an updated booster. It did not approve a booster for other people in high-risk categories because they didn’t bother studying the benefits and risks in these groups.
Wins
OK. So it’s been a rough week. But you know what? We are all fighting back. We see you all making calls, creating and signing petitions, joining and expanding Mask Blocs, creating and distributing zines, and making your own air-cleaning systems. We see so many more masked, tested, and ventilated events than we used to! We are mobilizing collective power to keep each other safe and to transform this state.
Next week, March 11, will mark the 5th anniversary of the declaration of the pandemic. We’re not where we should be, but this pandemic has radicalized a lot of us. Keep connecting. Keep finding your people. Keep going. We will win.
Oh! And check out these Free COVID-19 and flu test vending machines in King County, Washington!
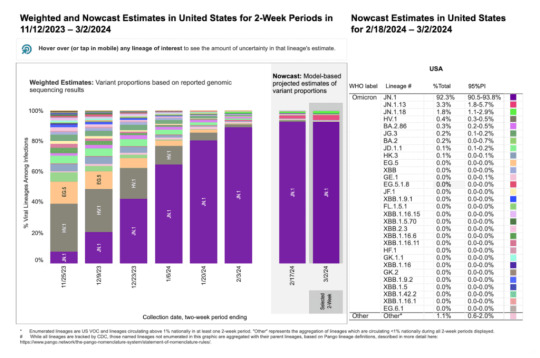
Variants
JN.1 is still the most dominant variant circulating in the United States and is projected to account for 92.3% of all circulating variants by March 2nd, 2024. Two JN.1 descendants, JN.1.13 and JN.1.18, are now the second and third most common circulating variants, projected to be at 3.3% and 1.8%, respectively.
To check for circulating variants within your community, you can find your HHS Region through the CDC Variant Tracker dashboard.
Long Covid
In an article published in Science, Drs Ziyad Al-Aly and Eric Topol reviewed the perplexing case of Long COVID. They discuss the lack of consensus and systematization when it comes to the classification of the disease, partly due to its different mechanisms and manifestations. For example, younger adult and female Long COVID patients are more likely to be afflicted by fatigue, dysautonomia, brain fog, and post-exertional malaise, while older patients are more likely to deal with cardiovascular and metabolic complications. They also discuss the current potential treatments for Long COVID, but express that since nonpharmaceutical interventions have been neglected, vaccines are the only available therapy. However, vaccines are unable to prevent Long COVID. Ultimately, they state that the only way to prevent Long COVID is by ending COVID transmission, such as by administering pan-variant neutralizing intranasal vaccines.
On March 15, 2024, the Long COVID March will be taking place in Washington D.C. at the Lincoln Memorial. The march is intended to mobilize Long COVID patients and allies to demand acknowledgment and policy changes from the government. You can read the march’s mission statement, which includes a list of objectives.
Take Action
Join us in demanding the CDC reinstate the 5-day COVID isolation policy. Despite the guidelines having already been dropped, we must still fight for adequate protections from COVID to safeguard our communities from harm. Make your voices known by sending a letter to the White House and your elected officials through our Action Network. The People’s CDC will also be implementing other action items in the coming weeks, so look out for those!
Today is COVID Memorial Day, in which we remember the 1.2 million lives lost to COVID in the United States, and show solidarity with the millions living with COVID grief and Long COVID. Check out Marked by COVID to learn more or to participate in today’s virtual vigil.
Again, we must continue to contact our elected officials to demand a ceasefire in Gaza, and we must continue to wear and require the wearing of high-quality respirators such as N95s and KN95s at protests and within organizing spaces.
#op#covid#covid19#covid-19#covid 19#long covid#long covid march#covid memorial day#coronavirus#sars-cov-19#covid isn't over#pcdc#people's cdc#cdc#centers for disease control#covid isolation#covid pandemic#coronavirus pandemic#pandemic#covid news#pandemic news#mask up#coronavirus news#ceasefire now#palestine#covid is not over#public health#uspol#img#described in alt text
18 notes
·
View notes
Text
5 notes
·
View notes
Text
Use of Hand Acupressure Points Chart for Health Healing

Our health needs to have unadulterated things like food, water, etc. One such thing is medicine, too. However, according to health research, one should not take medicines frequently because they can reduce our body's natural antibodies and weaken the immune system.
But the question is, how can we make our bodies fit and healthy without medicine? This is where traditional health practices like Acupressure come into the picture.
For those who feel curious about reflexology or acupressure, the human body has a lot of points where pressure can be applied for healing and relaxation. Some regard these locations, such as pressure points, as being used to stimulate other body parts and the entire health system.
Ancient science proves that pressure points can be used to promote a person's recovery from injuries and other health conditions. The application of pressure is a non-intrusive kind of therapy; therefore, it’s compatible with any other treatment that a doctor recommends.
Let’s get into the next sections to go deeper into the hand acupressure points chart and its uses.
How do pressure points work?
Pressure points are used in acupressure and reflexology, which explore the bodily relationships of mind and body. This is why hands are said to have several of the body's strongest pressure points.
Reflexology practitioners say that applying pressure to specific points on the hands can energise and treat various body areas, including internal organs if you're tired or sick.
Acupressure can improve numerous health concerns and using the points with the right hand acupressure tools and chart does not have any side effects because they are noninvasive and nonpharmaceutical.
It is simple and one can also stimulate their pressure points at home or anytime, anywhere.
What are the hand pressure points?
Hand acupressure points chart can become a valuable tool for beginners and people seeking self-care techniques. This chart defines the hand's key points corresponding to different body areas and specific health concerns.
From relieving headaches and reducing stress to improving digestion and promoting better sleep, the chart offers a comprehensive guide to addressing a wide range of health issues naturally.
Here we are discussing eight essential pressure points in the hand. Where they are, what they do, and how you can stimulate them for your benefit:
Heart 7
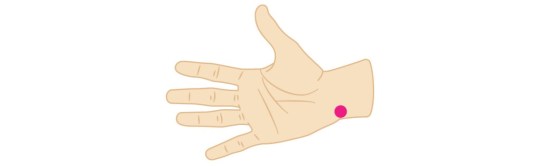
In the crook of your wrist is the Heart 7 pressure point. It lines up with the space between your little finger and ring finger.
Next to this pressure point is a bone inline. Acupressure therapists say that putting light pressure on this spot may help in the prevention of sadness, anxiety, insomnia, and heart palpitations.
Small Intestine 3
The pressing point ‘Small Intestine 3’ is on the outside of your hand, right on the edge. The point is where your hand curves down just below your pinky finger.
People believe that putting light pressure on this point can help with back of the head headaches, neck pain, and earaches.
Lung Meridian
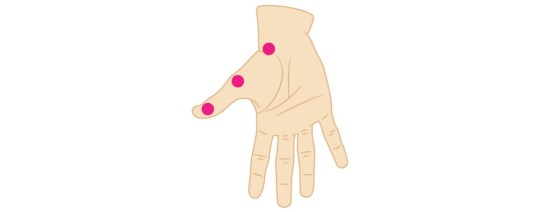
Just look at the edge of your hand to find the pressure point known as the lung line. It starts at the base of your thumb and goes down the side of your hand, finishing just below the wrist crease.
Following this line with your finger or any hand acupressure tools if you have a cold, might help ease the chills, coughing, runny nose, and sore throat.
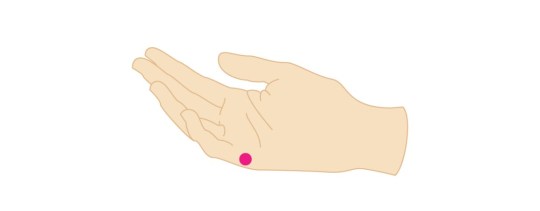
Inner Gate Point
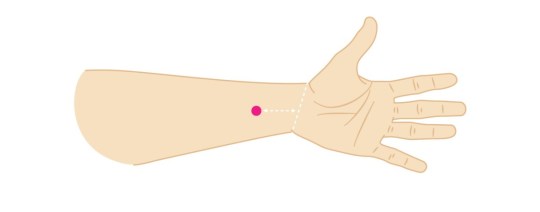
You can find the inner gate point in a certain place on the inside of your wrist. With one hand, feel about 3 cm away from the middle point where your wrists touched.
According to acupressure, you should rub this point with your thumb to help yourself with digestion and ease any stomach pain or sickness.
Outer Gate Point
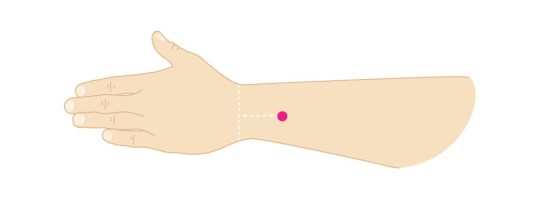
The outside gate point is on the back of the arm, between the two tendons. It is on the back of your wrist, put three fingers from your other hand on top of your wrist is that point.
Some acupressure experts also think that putting pressure on this part of the hand could give your immune system a quick boost.
Wrist Point 1
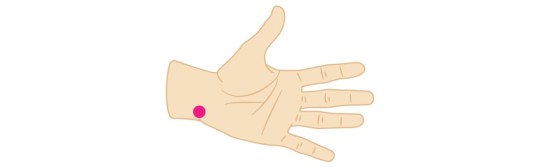
Your wrist point 1 is on your wrist. Follow the line of your finger down your pinky to the crease in your wrist. You will get this point right there.
Reflexologists putting pressure on point 1 on your wrist will help you be happier by keeping your feelings in check.
Base of Thumb Point
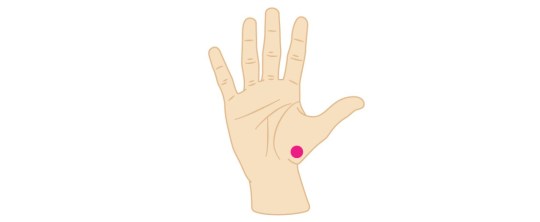
Your base of the thumb is this point. Put your finger on the base of your thumb and run it down to the crease in your wrist. Gently pressing on and rubbing this point with your finger can help with breathing and respiratory problems.
Hand Valley Point
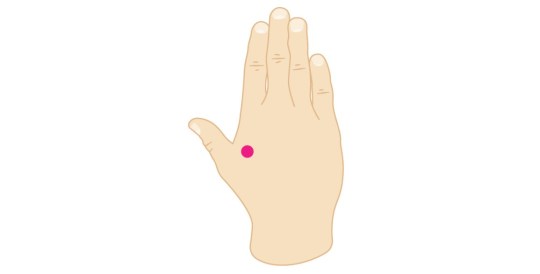
The hand valley point is in the thick skin between the thumb and index finger. Acupressure theory says that putting a firm touch on this pressure point may help lower stress and ease headaches, toothaches, shoulder tightness, and neck pain.
The Bottom Line
Reflexology is not a field valid in medicinal sciences. It's not the same as going to the doctor when you're sick or hurt because you can acupressure yourself. However, it could help you get better faster and generally keep you healthy.
There is no chance that acupressure will hurt you, so you can do it without any worries with the help of a hand acupressure points chart.
1 note
·
View note
Text
What the world knows that the VA does not: Hyperbaric Oxygen Therapy is safe, effective and can restore health

Athletes are waking up to the Use of Hyperbaric Oxygen Therapy for brain wound healing, health, endurance, peak performance, and the competitive edge.
Game Changer for Football Teams?
A high-profile college football program began using HBOT to manage player injuries and fatigue. The therapy quickly became a key factor in their injury management and prevention strategy. The team noted shorter recovery periods after injuries, and players were able to return to play faster than before, demonstrating HBOT's efficacy in a high-contact sports environment. Numerous professional athletes use HBOT.
100 Yards of Wellness Will Offer HBOT to Clemson Athletes
Nov 22, 2022
100 Yards of Wellness, Clemson’s new $4.9-million wellness space at Allen N. Reeves Football Complex that spans roughly 300 feet in length that has become a central hub of activity and major point of pride for Tiger football. The treatment and training room area includes all requisite athletic training resources, including a
diagnostic office with a full digital X-ray space and diagnostic ultrasound, general medical exam room, 30 yards of turf and hydrotherapy areas, including two underwater treadmills. Among the many features of the recovery center are:
• A hyperbaric chamber to create a pressurized environment for concentrated oxygen intake.
• A cryotherapy chamber for muscle recovery through extreme cold temperature exposure.
• A sensory deprivation float tank that houses 1,200 pounds of Epsom salt dissolved in water at skin temperature to remove athletes from light, sound and some gravitational force.
• Infrared hyperthermic Cocoon pods for Far-Infrared light therapy and vibrational massage.
• Photobiomodulation therapy beds that leverage multiple wavelengths of infrared light to reduce oxidative stress.
• Numerous massage chairs, including both percussive massage and hydromassage options.
• Percussive Hypervolt massage guns.
• Dedicated tables and space for practitioner-assisted stretching, percussive massage gun therapy and Normatec compressive sleeves provided to each player prior to the season.
• Functional testing equipment to obtain objective information on student-athlete muscle and joint function that can be used for injury prevention and return-to-play purposes.
The Rise of Hyperbaric Oxygen Therapy in Professional Football: A Game-Changer for Recovery and Performance
Sep 5, 2023
By Mudassir Sajad
In the fast-paced world of professional football, where every second counts, players are constantly seeking ways to gain a competitive edge. One such method that has been gaining traction is Hyperbaric Oxygen Therapy (HBOT). This innovative treatment has been endorsed by top-tier athletes like Mo Salah, Marcus Rashford, Vinicius Junior, and Neymar, who have all been spotted on social media using hyperbaric chambers Hyperbaric Oxygen Therapy is proving to be a revolutionary treatment in the realm of
professional football. Mo Salah, Marcus Rashford, Vinicius Junior, and Neymar endorsing its benefits, it's clear that HBOT is more than just a passing trend. Moreover as science continues to validate its efficacy, we can expect to see more football clubs
adopting this cutting-edge technology to give their players the competitive edge they need.
Dr. Joe Maroon on Hyperbaric Oxygen
Dr Joe Maroon Joseph Maroon is an American neurosurgeon, author, and triathlon athlete. He is the professor and vice chairman of the Department of Neurological Surgery at the University of Pittsburgh Medical Center and is the current medical director of WWE. For over 20 years he has served as the neurosurgical consultant to professional and college athletes in football, baseball, golf, hockey and soccer and was team neurosurgeon to the Pittsburgh Steelers for over 40 years.
As early as 2011, Dr Maroon and Dr Bost wrote: "Alternative nonpharmaceutical treatments appear to be gaining acceptance for the treatment of common neurodegenerative conditions, memory decline, and reduced cognitive function. Substantial animal and human research now suggests that these same natural dietary supplements, vitamins and minerals, and the use of hyperbaric oxygen may be a better first-line choice for the treatment of PCS, which has generally been underreported by both athletes and the military."
Maroon and Bost, Concussion Management at the NFL, College, High School, and Youth Sports Levels. Clinical Neurosurgery. Volume 58, 2011, Chapter. 7.
The TreatNOW Mission is ending service member suicides. Along the way, we have learned that we can end suicidal ideation, help end symptoms of PTSD, and heal brain wounds to end the effects of BLAST injury, mild TBI Persistent Post Concussive Syndrome, and polytrauma. www.treatnow.org
Heal Brains. Stop Suicides. Restore Lives. TreatNOW
Information provided by TreatNOW.org does not constitute a medical recommendation. It is intended for informational purposes only, and no claims, either real or implied, are being made.
Read the full article
#brainhealth#braininjured#braininjury#brainwound#concussion#ConcussioninSport#concussionprotocol#ConcussionSymptoms#concussiontreatment#CTE#HBOT#HBOTTreatment#HeadImpact#HealingwithHyperbarics#hyperbaric#HyperbaricOxygentherapy#PostconcussionSyndrome#TBI#TBItreatment#traumaticbraininjury
0 notes
Text
MMWR Booster #27: COVID-19–Associated Hospitalizations Among U.S. Infants Aged <6 Months — COVID-NET, 13 States, June 2021–August 2022
Top 5 Takeaways
Increased Hospitalization Rates: During the Omicron variant-predominant periods, hospitalization rates among infants aged <6 months increased compared to the Delta variant period, but severe disease indicators among hospitalized infants did not increase.
Comparison with Other Age Groups: The average weekly COVID-19-associated hospitalization rate for infants <6 months was similar to adults aged 65–74 years and higher than other pediatric age groups and younger adults.
Role of Maternal Vaccination: Maternal COVID-19 vaccination during pregnancy might offer protection to infants through transplacental transfer of antibodies. Effectiveness varies with variants and time since vaccination.
Study Limitations: Limitations include assumptions in population estimates, changes in public health policies, unassessed maternal immunity, variant predominance periods, and limited generalizability due to the catchment area.
Public Health Implications: Emphasizes the importance of vaccinating pregnant women and implementing nonpharmaceutical interventions to protect infants ineligible for vaccination.
Full summary link: BroadlyEpi.com
Enjoying these summaries? Check back every day at 8am and 4pm Pacific Time (UTC - 8) for a new MMWR Booster. A reblog would also be greatly appreciated, and thanks to everyone who already has! BroadlyEpi hopes to make Epidemiology and Public Health more approachable to anyone who's interested.
0 notes
Quote
Bright light therapy for seasonal affective disorder (SAD) has been investigated and applied for over 20 years. Physicians and clinicians are increasingly confident that bright light therapy is a potent, specifically active, nonpharmaceutical treatment modality. Indeed, the domain of light treatment is moving beyond SAD, to nonseasonal depression (unipolar and bipolar), seasonal flare-ups of bulimia nervosa, circadian sleep phase disorders, and more. Light therapy is simple to deliver to outpatients and inpatients alike, although the optimum dosing of light and treatment time of day requires individual adjustment. The side-effect profile is favorable in comparison with medications, although the clinician must remain vigilant about emergent hypomania and autonomic hyperactivation, especially during the first few days of treatment. Importantly, light therapy provides a compatible adjunct to antidepressant medication, which can result in accelerated improvement and fewer residual symptoms.
Light Therapy for Seasonal and Nonseasonal Depression: Efficacy, Protocol, Safety, and Side Effects | CNS Spectrums | Cambridge Core
0 notes
Text
0 notes
Text
What is the effect of physical/exercise therapy on physical function in patients with systemic sclerosis?
Systemic sclerosis (SSc) is a relatively rare disease of the connective tissues in the body resulting in debilitating consequences. It is characterized by diffuse fibrosis and abnormalities within the connective tissue of the skin, joints, and eventually internal organs. Specific etiology is not known. Associated signs and symptoms include pain, edema, decreased range of motion, skin thickening, and joint contractures which are all associated with decreased functional ability and reduced quality of life. Unfortunately, research regarding nonpharmaceutical interventions for systemic sclerosis is extremely limited. Research and treatment that is available usually focus on skin lesions and complications to internal organs as the disease progresses. However, physical therapy and/or skilled exercise therapy may be able to address functional concerns and improve the quality of life in both the early and late stages of the disease.
Murphy, et al., utilized an eight-week, in-person, program consisting of tissue mobilizations, thermal modalities, upper extremity mobility, and a home exercise program in patients with early SSc (< 5 years) to determine possible benefits for upper extremity function. The study utilized a single group with pre- and post-test measures to determine improvement in the upper extremity QuickDASH, range of motion, coordination, skin thickening, and Patient-Reported Outcomes Measurement Information System (PROMIS). Patients, on average, had a moderate skin disease and the majority were also being treated with immunosuppressive therapy or were participating in clinical trials. Researchers found that there was not a meaningful improvement at four weeks into the program but did find significant improvement from baseline at the end of the eight weeks. On average, participants improved QuickDASH measures by 14 points, PROMIS by 3.1 points, 41.5 degrees of active motion, and were faster in completing the 9-hole peg test with the left hand. All are significant findings from baseline. However, no significant improvement was shown with right-hand coordination or active motion. Long-term effects were not evaluated, and it is unclear how many sessions are optimal for best results. Additional limitations of this study include the single test group, lack of tracking regarding home exercise program compliance, small sample size, the treating therapist was also the accessor, and that the study focused only on participants in the early stages of the disease (Murphy et al., 2018).
Waszczykowski et al., evaluated the effectiveness of supervised exercise therapy on hand and overall function in SSc with a one-year follow-up. This study evaluated a four-week program of supervised rehabilitation compared to a prescribed home exercise program alone. Assessments were performed at one-, three-, six-, and twelve-month follow-ups. Outcomes used included: QuickDASH, visual analog scale (VAS), Cochin Hand Function Scale (CHFS), Health Assessment Questionnaire Disability Index (HAQ-DI), Scleroderma-HAQ, hand grip, pinch grip, and range of motion. Massage in the whirlpool coupled with upper extremity active exercises, soft tissue massage, and hand joint manipulation was used with the goal of reducing pain and improving hand function. Results indicated significant positive effects for the intervention group at one-, three-, and six-month follow-ups, but only at the one-month follow-up for the control group. At the twelve-month follow-up, no significant improvement was noted indicating limited long-term effects. As a result, researchers recommend regular repetition of the program every six months at a minimum. Limitations of this study include lack of randomization, small sample size, and difficulty blinding participants and researchers (Waszczykowski et al., 2021).
Liem, et al., conducted a systematic review of the effectiveness and safety of exercise therapy in this patient population to help address the limitation of available research. The review consisted of nine articles, four randomized controlled trials and five observational studies. The review compared the interventions of hand exercises, aerobic exercise, and aerobic exercises with resistance training to no exercise. A variety of outcome measures were used to determine the effect on hand function, maximal mouth opening, quality of life, and oxygen uptake. Sample size of the different studies remained small, ranging from four to forty-eight participants with most of them females. It was determined that strengthening and mobility exercises when supported by telemedicine, were more beneficial in hand pain and functioning compared to a similar intervention using only common objects. In addition, two different studies evaluated the effect of exercise on maximal oral aperture. Interventions groups had significant improvement compared to the control groups, however, one group found that the results were short-lived and were not significant at the six-month follow-up. The last set of articles evaluated aerobic and/or resistance exercises. Both utilized a twice a week for twelve-week supervised high-intensity interval training (HIIT) program. After verifying the benefit of the base program, the researchers decided to evaluate the benefit of resistance training in combination with the established HIIT program. Resistance training consisted of chest press, bicep curl, triceps extension, lateral arm raise, and handgrip dynamometer. Results concluded the combined aerobic and resistance training improved muscle strength and function, resting heart rate, and workload and time of exercise at the ventilatory threshold as well as peak exercise were increased. A third study evaluated the effectiveness of an eight-week moderate intensity treadmill program on aerobic capacity and found similar beneficial results (Liem et al., 2019).
Overall, it is difficult to make evidence-based clinical decisions due to the lack of quality evidence. The rarity of the disease makes obtaining a suitable sample size to account for the required effect size, and difficulty blinding participants and researchers. Due to these factors, it is difficult to determine the true validity of the results. However, many of the participants had to travel more than thirty minutes for their sessions, and the adherence rate stayed high. This speaks to the feasibility of using the mentioned interventions in this population in the clinic. Unfortunately, the proposed intervention programs all varied in frequency, intensity, duration, and interventions with a highly individualized approach. In-clinic and home exercise programs were often individualized based on patients’ values and goals for treatment. Most of them also focused mainly on hand/upper extremity function without evaluating lower extremity and community/home-based mobility at all. Most of which also focused mainly on hand/upper extremity function without evaluating lower extremity and community/home-based mobility at all. Furthermore, it is challenging to determine the true effects across multiple studies because of the wide variety of outcome measures used. For example, the Functional Index for Hand OsteoArthritis was used in one study but not in others. Use of this type of outcome measure also poses its own questions with validity considering it has been validated for a different patient population than the one being examined. Even well-known and validated outcome measures, such as the QuickDASH, have a debate regarding the minimal clinically important difference score ranging from eight to fourteen. Although the evidence is weak for exercise therapy in patients with SSc, by culminating all the evidence it can be determined that exercise therapy is safe for these patients with no to minimal adverse effects. Results seem to indicate that using a combination of modalities, supervised exercise, and home exercise programs provides the most benefit and that these programs should be continued intermittently long-term because of the short-lived effects.
References
Liem, S. I., Vliet Vlieland, T. P., Schoones, J. W., & de Vries-Bouwstra, J. K. (2019). The effect and safety of exercise therapy in patients with systemic sclerosis: A systematic review. Rheumatology Advances in Practice, 3(2). https://doi.org/10.1093/rap/rkz044
Murphy, S., Barber, M., Homer, K., Dodge, C., Cutter, G., & Khanna, D. (2018). Occupational therapy treatment to improve upper extremity function in individuals with early systemic sclerosis: A pilot study. Arthritis Care & Research , 70(11), 1653–1660. https://doi.org/10.1002/acr.23522
Waszczykowski, M., Dziankowska-Bartkowiak, B., Podgórski, M., Fabiś, J., & Waszczykowska, A. (2021). Role and effectiveness of complex and supervised rehabilitation on overall and hand function in systemic sclerosis patients—one-year follow-up study. Scientific Reports, 11(15174). https://doi.org/10.1038/s41598-021-94549-y
What is the effect of physical/exercise therapy on physical function in patients with systemic sclerosis?
Systemic sclerosis (SSc) is a relatively rare disease of the connective tissues in the body resulting in debilitating consequences. It is characterized by diffuse fibrosis and abnormalities within the connective tissue of the skin, joints, and eventually internal organs. Specific etiology is not known. Associated signs and symptoms include pain, edema, decreased range of motion, skin thickening, and joint contractures which are all associated with decreased functional ability and reduced quality of life. Unfortunately, research regarding nonpharmaceutical interventions for systemic sclerosis are extremely limited. Research and treatment that is available, usually focuses on skin lesions and complications to internal organs as the disease progresses. However, physical therapy and/or skilled exercise therapy may be able to address functional concerns and improve quality of life in both the early and late stages of the disease.
Murphy, et al.,utilized an eight week, in-person, program consisting of tissue mobilizations, thermal modalities, upper extremity mobility, and a home exercise program in patients with early SSc (< 5 years) to determine possible benefit for upper extremity function. The study utilized a single group with pre- and post-test measures to determine improvement on the upper extremity QuickDASH, range of motion, coordination, skin thickening, and Patient-Reported Outcomes Measurement Information System (PROMIS). Patients, on average, had moderate skin disease and the majority were also being treated with immunosuppressive therapy or were participating in clinical trials. Researchers found that that there was not a meaningful improvement at four weeks into the program but did find significant improvement from baseline at the end of the eight-week period. On average, participants improved QuickDASH measures by 14 points, PROMIS by 3.1 points, 41.5 degrees of active motion, and were faster in completing the 9-hole peg test with the left hand. All are significant findings from baseline. However, no significant improvement was shown with right hand coordination or active motion. Long-term effects were not evaluated, and it is unclear how many sessions are optimal for best results. Additional limitations of this study include the single test group, lack of tracking regarding home exercise program compliance, small sample size, the treating therapist was also the accessor, and that the study focused only on participants in the early stages of the disease (Murphy et al., 2018).
Waszczykowski et al., evaluated the effectiveness of supervised exercise therapy on hand and overall function in SSc with a one-year follow-up. This study evaluated a four-week program of supervised rehabilitation compared to a prescribed home exercise program alone. Assessments were performed at one-, three-, six-, and twelve-month follow-ups. Outcomes used included: QuickDASH, visual analog scale (VAS), Cochin Hand Function Scale (CHFS), Health Assessment Questionnaire Disability Index (HAQ-DI), Scleroderma-HAQ, hand grip, pinch grip, and range of motion. Massage in the whirlpool coupled with upper extremity active exercises, soft tissue massage, hand joint manipulation was used with the goal of reducing pain and improving hand function. Results indicated significant positive effects for the intervention group at one-, three-, and six-month follow-ups, but only at the one-month follow-up for the control group. At the twelve-month follow-up, no significant improvement was noted indicating limited long-term effects. As a result, researchers recommend regular repetition of the program at every six-months at minimum. Limitations of this study include lack of randomization, small sample size, and difficulty blinding participates and researchers (Waszczykowski et al., 2021).
Liem, et al., conducted a systematic review of the effectiveness and safety of exercise therapy in this patient population to help address the limitation of available research. The review consisted of nine articles, four randomized controlled trials and five observational studies. The review compared the interventions of hand exercises, aerobic exercise, and aerobic exercises with resistance training to no exercise. A variety of outcome measures were used to determine the effect on hand function, maximal mouth opening, quality of life, and oxygen uptake. Sample size of the different studies remained small, ranging from four to forty-eight participants with most of them females. It was determined that strengthening and mobility exercises, when supported by telemedicine, was more beneficial in hand pain and functioning compared to a similar intervention using only common objects. In addition, two different studies evaluated the effect of exercise on maximal oral aperture. Interventions groups had significant improvement compared to the control groups, however, one group found that the results were short lived and were not significant at the six-month follow-up. The last set of articles evaluated aerobic and/or resistance exercises. Both utilized a twice a week for twelve-weeks supervised high-intensity interval training (HIIT) program. After verifying a benefit from the base program, the researchers decided to evaluate the benefit of resistance training in combination with the established HIIT program. Resistance training consisted of chest press, bicep curl, triceps extension, lateral arm raise, and handgrip dynamometer. Results concluded the combined aerobic and resistance training improved muscle strength and function, resting heart rate, and workload and time of exercise at ventilatory threshold as well as peak exercise were increased. A third study evaluated the effectiveness of an eight-week moderate intensity treadmill program on aerobic capacity and found similar beneficial results (Liem et al., 2019).
Overall, it is difficult to make evidence-based clinical decisions due to the lack of quality evidence. The rarity of the disease makes obtaining a suitable sample size to account for the required effect size, and difficulty blinding participants and researchers. Due to these factors, it is difficult to determine the true validity of the results. However, many of the participants had to travel more than thirty minutes for their sessions, and the adherence rate stayed high. This speaks to the feasibility of using the mentioned interventions in this population in the clinic. Unfortunately, the proposed intervention programs all varied in frequency, intensity, duration, and interventions with a highly individualized approach. In-clinic and home exercise programs were often individualized based on patients’ values and goals for treatment. Most of which also focused mainly on hand/upper extremity function without evaluating lower extremity and community/home-based mobility at all. Furthermore, it is challenging to determine the true effects across multiple studies because of the wide variety of outcome measures used. For example, the Functional Index for Hand OsteoArthritis was used in one study but in no others. Use of this type of outcome measure also poses its own questions with validity considering it has been validated for a different patient population than the one being examined. Even well-known and validated outcome measures, such as the QuickDASH, have debate regarding the minimal clinically important difference score ranging from eight to fourteen. Although the evidence is weak for exercise therapy in patients with SSc, by culminating all the evidence it can be determined that exercise therapy is safe for these patients with none to minimal adverse effects. Results seem to indicate that using a combination of modalities, supervised exercise, and home exercise program provides the most benefit, and that these programs should be continued intermittently long-term because of the short-lived effects.
References
Liem, S. I., Vliet Vlieland, T. P., Schoones, J. W., & de Vries-Bouwstra, J. K. (2019). The effect and safety of exercise therapy in patients with systemic sclerosis: A systematic review. Rheumatology Advances in Practice, 3(2). https://doi.org/10.1093/rap/rkz044
Murphy, S., Barber, M., Homer, K., Dodge, C., Cutter, G., & Khanna, D. (2018). Occupational therapy treatment to improve upper extremity function in individuals with early systemic sclerosis: A pilot study. Arthritis Care & Research , 70(11), 1653–1660. https://doi.org/10.1002/acr.23522
Waszczykowski, M., Dziankowska-Bartkowiak, B., Podgórski, M., Fabiś, J., & Waszczykowska, A. (2021). Role and effectiveness of complex and supervised rehabilitation on overall and hand function in systemic sclerosis patients—one-year follow-up study. Scientific Reports, 11(15174). https://doi.org/10.1038/s41598-021-94549-y
What is the effect of physical/exercise therapy on physical function in patients with systemic sclerosis?
Systemic sclerosis (SSc) is a relatively rare disease of the connective tissues in the body resulting in debilitating consequences. It is characterized by diffuse fibrosis and abnormalities within the connective tissue of the skin, joints, and eventually internal organs. Specific etiology is not known. Associated signs and symptoms include pain, edema, decreased range of motion, skin thickening, and joint contractures which are all associated with decreased functional ability and reduced quality of life. Unfortunately, research regarding nonpharmaceutical interventions for systemic sclerosis is extremely limited. Research and treatment that is available usually focus on skin lesions and complications to internal organs as the disease progresses. However, physical therapy and/or skilled exercise therapy may be able to address functional concerns and improve the quality of life in both the early and late stages of the disease.
Murphy, et al., utilized an eight-week, in-person, program consisting of tissue mobilizations, thermal modalities, upper extremity mobility, and a home exercise program in patients with early SSc (< 5 years) to determine possible benefits for upper extremity function. The study utilized a single group with pre- and post-test measures to determine improvement in the upper extremity QuickDASH, range of motion, coordination, skin thickening, and Patient-Reported Outcomes Measurement Information System (PROMIS). Patients, on average, had a moderate skin disease and the majority were also being treated with immunosuppressive therapy or were participating in clinical trials. Researchers found that there was not a meaningful improvement at four weeks into the program but did find significant improvement from baseline at the end of the eight weeks. On average, participants improved QuickDASH measures by 14 points, PROMIS by 3.1 points, 41.5 degrees of active motion, and were faster in completing the 9-hole peg test with the left hand. All are significant findings from baseline. However, no significant improvement was shown with right-hand coordination or active motion. Long-term effects were not evaluated, and it is unclear how many sessions are optimal for best results. Additional limitations of this study include the single test group, lack of tracking regarding home exercise program compliance, small sample size, the treating therapist was also the accessor, and that the study focused only on participants in the early stages of the disease (Murphy et al., 2018).
Waszczykowski et al., evaluated the effectiveness of supervised exercise therapy on hand and overall function in SSc with a one-year follow-up. This study evaluated a four-week program of supervised rehabilitation compared to a prescribed home exercise program alone. Assessments were performed at one-, three-, six-, and twelve-month follow-ups. Outcomes used included: QuickDASH, visual analog scale (VAS), Cochin Hand Function Scale (CHFS), Health Assessment Questionnaire Disability Index (HAQ-DI), Scleroderma-HAQ, hand grip, pinch grip, and range of motion. Massage in the whirlpool coupled with upper extremity active exercises, soft tissue massage, and hand joint manipulation was used with the goal of reducing pain and improving hand function. Results indicated significant positive effects for the intervention group at one-, three-, and six-month follow-ups, but only at the one-month follow-up for the control group. At the twelve-month follow-up, no significant improvement was noted indicating limited long-term effects. As a result, researchers recommend regular repetition of the program every six months at a minimum. Limitations of this study include lack of randomization, small sample size, and difficulty blinding participants and researchers (Waszczykowski et al., 2021).
Liem, et al., conducted a systematic review of the effectiveness and safety of exercise therapy in this patient population to help address the limitation of available research. The review consisted of nine articles, four randomized controlled trials and five observational studies. The review compared the interventions of hand exercises, aerobic exercise, and aerobic exercises with resistance training to no exercise. A variety of outcome measures were used to determine the effect on hand function, maximal mouth opening, quality of life, and oxygen uptake. Sample size of the different studies remained small, ranging from four to forty-eight participants with most of them females. It was determined that strengthening and mobility exercises when supported by telemedicine, were more beneficial in hand pain and functioning compared to a similar intervention using only common objects. In addition, two different studies evaluated the effect of exercise on maximal oral aperture. Interventions groups had significant improvement compared to the control groups, however, one group found that the results were short-lived and were not significant at the six-month follow-up. The last set of articles evaluated aerobic and/or resistance exercises. Both utilized a twice a week for twelve-week supervised high-intensity interval training (HIIT) program. After verifying the benefit of the base program, the researchers decided to evaluate the benefit of resistance training in combination with the established HIIT program. Resistance training consisted of chest press, bicep curl, triceps extension, lateral arm raise, and handgrip dynamometer. Results concluded the combined aerobic and resistance training improved muscle strength and function, resting heart rate, and workload and time of exercise at the ventilatory threshold as well as peak exercise were increased. A third study evaluated the effectiveness of an eight-week moderate intensity treadmill program on aerobic capacity and found similar beneficial results (Liem et al., 2019).
Overall, it is difficult to make evidence-based clinical decisions due to the lack of quality evidence. The rarity of the disease makes obtaining a suitable sample size to account for the required effect size, and difficulty blinding participants and researchers. Due to these factors, it is difficult to determine the true validity of the results. However, many of the participants had to travel more than thirty minutes for their sessions, and the adherence rate stayed high. This speaks to the feasibility of using the mentioned interventions in this population in the clinic. Unfortunately, the proposed intervention programs all varied in frequency, intensity, duration, and interventions with a highly individualized approach. In-clinic and home exercise programs were often individualized based on patients’ values and goals for treatment. Most of them also focused mainly on hand/upper extremity function without evaluating lower extremity and community/home-based mobility at all. Most of which also focused mainly on hand/upper extremity function without evaluating lower extremity and community/home-based mobility at all. Furthermore, it is challenging to determine the true effects across multiple studies because of the wide variety of outcome measures used. For example, the Functional Index for Hand OsteoArthritis was used in one study but not in others. Use of this type of outcome measure also poses its own questions with validity considering it has been validated for a different patient population than the one being examined. Even well-known and validated outcome measures, such as the QuickDASH, have a debate regarding the minimal clinically important difference score ranging from eight to fourteen. Although the evidence is weak for exercise therapy in patients with SSc, by culminating all the evidence it can be determined that exercise therapy is safe for these patients with no to minimal adverse effects. Results seem to indicate that using a combination of modalities, supervised exercise, and home exercise programs provides the most benefit and that these programs should be continued intermittently long-term because of the short-lived effects.
0 notes
Text
While it's important to note that vaccinated individuals do have lower viral loads than unvaccinated people, masks are still required for source control and personal protection. As per the CDC, ~60% of all covid spread is pre- or asymptomatic. Vaccination reducing acute illness is good for keeping people out of the hospital, but it clearly does not halt spread. If everyone is still breating covid into the air, it's only a matter of time before it spreads to another person.
(One big quibble with this study: it has no means of factoring out nonpharmaceutical interventions like masking and distance work, skewing the vaccinated group downward as high-risk individuals are more likely to be vaccinated AND take further risks to avoid covid. At the time of posting, only ~22% of the US is considered fully vaccinated.)
#mask up#covid#covid 19#covid isn't over#pandemic#covid conscious#long covid#covid is airborne#wear a mask#coronavirus
11 notes
·
View notes
Text
Evaluate the safety and effectiveness of complementary and alternative therapies.
Some patients will seek out alternative medicinal practices when treating diseases; therefore, it is important to know how alternative or herbal medications interact with prescription medications. Knowing how to navigate finding information on potential interactions is important in preventing complications when prescribing medications. Groups will select a common disease and perform research on both conventional and alternative medicine treatment options. Using CAM as your primary resource, create a PowerPoint presentation of 10-15 slides that addresses the following items:
Identify the disease.
Identify the patient population that is most affected by this disease.
Identify complementary and alternative medicine resources and guidelines.
Evaluate the safety and effectiveness of complementary and alternative therapies.
Identify any common interactions of alternative and nonpharmaceutical medications with prescribed medications.
Describe any cultural considerations and factors that could affect the patients’ decisions regarding their treatment plans and care.
Include slide notes (100-250 words for each slide).
You are required to cite three to five sources to complete this assignment. Sources must be published within the past 5 years and appropriate for the assignment criteria and nursing content.
First appeared on Assignments.tips
0 notes
Photo

#Repost @project_cbd ・・・ Today's FDA announcement declining to regulate CBD products is so riddled with disingenuousness and doublespeak that it's hard to know where to begin. It's clear that the FDA bureaucracy is unable to scale with the scope and magnitude of popular interest in CBD. The FDA privileges pharmaceutical CBD, which is so safe that it's not a scheduled substance while maintaining that nonpharmaceutical CBD is too risky for public consumption. Yet CBD, as an herbal medicine, has been available since 2010 and millions of people have used CBD products without apparent harm. A 2018 report by the World Health Organization concluded that CBD “is generally well-tolerated with a good safety profile [and] exhibits no effects indicative of any abuse or dependence potential.” Clinical trials (by ValidCare) assessing CBD's impact on human liver function have given the compound a clean bill of health, yet the FDA continues to exaggerate the dangers of CBD while ignoring significant benefits beyond its proven anti-seizure properties. The FDA's fear-mongering contention that "people could be unknowingly exposed to CBD through meat, milk and eggs from animals fed CBD" is ludicrous. Unfortunately, many companies marketing hemp-derived CBD have not acquitted themselves well regarding product manufacturing and labeling -- which underscores the need for regulatory oversight that the FDA, out of deference to the pharmaceutical industry, has failed to provide. By shirking its regulatory responsibilities with respect to CBD, the FDA encourages disrespect and mistrust of the federal government, which continues to maintain that cannabis is a dangerous drug with no medical value. #science #fda #sciencenews #fearmongering #clinicaltrials (at Bronx, NY) https://www.instagram.com/p/Cn5LLqxOzDz/?igshid=NGJjMDIxMWI=
0 notes
Text
Threshold control method could aid in future non-pharmaceutical intervention relaxation policy making
Governments around the world used a variety of techniques known as nonpharmaceutical interventions, or NPIs, to control the spread of COVID-19. These NPIs include mandated mask-wearing, social distancing, closures of schools and businesses, and restrictions on travel.
The use of NPIs slowed the spread of other infectious diseases as well, such as influenza and respiratory syncytial virus, RSV.…

View On WordPress
0 notes
Text
Reset Your Child's Brain: A Four-Week Plan to End Meltdowns, Raise Grades, and Boost Social Skills by Reversing the Effects of Electronic Screen-Time - Victoria Dunckley
EPUB & PDF Ebook Reset Your Child's Brain: A Four-Week Plan to End Meltdowns, Raise Grades, and Boost Social Skills by Reversing the Effects of Electronic Screen-Time | EBOOK ONLINE DOWNLOAD
by Victoria Dunckley.
Download Link : DOWNLOAD Reset Your Child's Brain: A Four-Week Plan to End Meltdowns, Raise Grades, and Boost Social Skills by Reversing the Effects of Electronic Screen-Time
Read More : READ Reset Your Child's Brain: A Four-Week Plan to End Meltdowns, Raise Grades, and Boost Social Skills by Reversing the Effects of Electronic Screen-Time
Ebook PDF Reset Your Child's Brain: A Four-Week Plan to End Meltdowns, Raise Grades, and Boost Social Skills by Reversing the Effects of Electronic Screen-Time | EBOOK ONLINE DOWNLOAD
Hello Book lovers, If you want to download free Ebook, you are in the right place to download Ebook. Ebook Reset Your Child's Brain: A Four-Week Plan to End Meltdowns, Raise Grades, and Boost Social Skills by Reversing the Effects of Electronic Screen-Time EBOOK ONLINE DOWNLOAD in English is available for free here, Click on the download LINK below to download Ebook Reset Your Child's Brain: A Four-Week Plan to End Meltdowns, Raise Grades, and Boost Social Skills by Reversing the Effects of Electronic Screen-Time 2020 PDF Download in English by Victoria Dunckley (Author).
Description Book:
A no-cost, nonpharmaceutical treatment plan for children with behavioral and mental health challengesIncreasing numbers of parents grapple with children who are acting out without obvious reason. Revved up and irritable, many of these children are diagnosed with ADHD, bipolar illness, autism, or other disorders but don?t respond well to treatment. They are then medicated, often with poor results and unwanted side effects. Based on emerging scientific research and extensive clinical experience, integrative child psychiatrist Dr. Victoria Dunckley has pioneered a four-week program to treat the frequent underlying cause, Electronic Screen Syndrome (ESS).Dr. Dunckley has found that everyday use of interactive screen devices ? such as computers, video games, smartphones, and tablets ? can easily overstimulate a child?s nervous system, triggering a variety of stubborn symptoms. In contrast, she?s discovered that a strict electronic fast single-handedly improves mood, focus, sleep, and
0 notes
Last Seen Blogs

corposeco
THE CAIPIROSKA VODKA PEOPLE

funnybook00
funny

punkedsolar
punkedsolar

desain-rumah
Jasa Desain Arsitek Rumah

chunkypossum
Chunky Possum