
chroniconic
chronic illness support and recovery blog
I’m Eli, 29 y-o, diagnosed with chronic (daily) migraine and endometriosis which rendered me 90% bedridden and unable to work. A blog for sharing progress, tips, awareness, etc.
17 posts
Last active 60 minutes ago
Don't wanna be here? Send us removal request.
Last Seen Blogs

openprogrammer
Deshwal

mercadolynnmusic
Pentecostal/Latina/CollegeStudent/Music

figofswords
izutsumi (izutsumi)

viajy
vijay

neonsaturnofficial-blog
NEON.SATURN
Text
I had my 4th Ajovy injection on Friday. My migraine frequency changed from daily to every other day about 2 weeks ago. I have a headache and some sudden nerve pain zaps on migraine-free days still but I’m hoping it’ll start getting better once I have less migraines. Current side effects: worsened asthma and sinusitis for a week following the injection, pretty bad constipation and really awful fatigue. But it’s better than having daily nonstop migraines.
I use cute plasters on the injection site and reward myself with candy, like a chocolate ladybug

#actually chronically ill#chronic pain#chronic migraine#spoonie#chronic fatigue#chronic illness#ajovy#biologics#cgrp#physical disability#disabled
17 notes
·
View notes
Text
I took dienogest 2mg for 4 months for endometriosis and it basically erased any pelvic pain I had, the knitting needle pain through my right ovary, the butt lightning pain, the pain I felt upon pressure alone that felt like my organs are exploding, and it stopped my period
but the side effects? progressively suicidal thoughts. a new form of migraine I never experienced before: hemiplegic migraine where half of my body went completely numb for hours, a new type of visual symptom where I had black spots covering my field of vision, pain that feels like a sudden jolt through my head, and pain that feels like a bubble of pressure is moving from the center of my head, inside my head, to my forehead. these migraines would be non-stop. I developed constant double vision and also had a constant pounding headache in addition to the migraine. And I also had daily joint pain that felt like my joints were on fire and I wanted to scream, and by the end I started getting really bad hot flushes. I even developed some dark sun spots despite wearing sunscreen religiously (it’s an old skincare habit already) and not leaving my apartment.
Guess what? My estrogen levels are basically zero. Also progesterone levels though, but no one interpreted this for me yet so I don’t know what it means. I’m only 29 and I don’t think I could be in actual menopause yet.
Eventually I was unable to do anything.
My doctor said to continue dienogest regardless, because there is no other option. I had to stop dienogest, and now I’ve been on NuvaRing continously since March and I’m looking for another doctor.
The continuous usage allows me to skip my period and potentially avoid the worst symptoms then, but I know that unless I am in a semi-menopausal state like with dienogest, it will probably come back?
I had the NuvaRing prescribed as “acne medication” and my neurologist confirmed that it could be tried in my case, because it seems like I am sensitive to estrogen withdrawal, although normally COCs are not recommended when you have migraine with aura. I’m monitored for blood clotting issues (this will be a separate post).
Some of my endometriosis pain has returned on NuvaRing, but the constant throbbing headache and suicidal thoughts are gone. I still have double vision and migraines though. I had migraines before dienogest, they just turned into daily and relentless ones on it.
#actually chronically ill#endometriosis#chronic migraine#chronic pain#spoonie#dienogest#visanne#visannette#nuva ring
0 notes
Text
I’m also autistic and physically disabled, and I talk in long infodumps at the doctor’s which is basically like a timestamped history of all of my symptoms, without pause.
And I realized only after 10 years of going to the doctor’s with my physical health issues that they won’t listen to 99% of the infodump.
That’s true for most people, really, but if you’re autistic and have autistic friends who also speak in infodumps alone, it might come as a total surprise that this would be overwhelming to everyone else and all they will hear or see will be “obsessive personality” or “probably needs anxiety medication or something” which should not be the case, however, it might be a factor.
I did meet a couple of wonderful doctors who somehow listened to all of the infodump, took down notes, and made suggestions based on the details. I suspect they were neurodivergent themselves though, which is why it’s so rare.
Another pitfall autistic people might have is taking things directly when it comes to experiencing symptoms.
When a doctor asks you “do you feel/experience this all the time?” and if your brain goes “I guess there are some minutes, seconds or hours where I don’t feel it, maybe one day per month where it’s okay?” so you reply “no”, then the doctor thinks you have symptoms just periodically. Just a couple of times per month maybe. Or maybe it’s not a whole-day thing. That’s what they’ll think, because we’re really bad with those questions.
The way I started overcoming those issues was by making a list of all of my symptoms: when they started, how frequent they are, how long do they last and what they prevent me from doing, what medications and supplements I’m taking, and whether e.g painkillers or other medications work or not (also whether it has side effects).
Then, before talking, preface the whole conversation with “I’m here because I experience X, Y, Z symptoms <insert frequency here>”, then go into more detail for each symptom gradually.
The doctor might ask you questions inbetween: make sure to have your piece of paper with the symptoms in front of you so you won’t forget to tackle all of them as they move on.
If the doctor asks you questions about whether something is a daily occurrence, or severe, or anything that your brain takes literally, just tell them how it is like for you even if it sounds weird: if you have pain every couple of minutes, they’ll mark it down as “relentless, daily” because a non-autistic person would just say “daily”. Don’t make an assumption beforehand, though, just try to say it how it is like for you.
Pain severity is another hard one, especially if you’re used to constant pain. So I usually describe how it feels like for me. How it deters me from doing things, how I need rest or support, and what is my reaction when it occurs.
For example, if you get out of the house for 2 days every week and those aren’t perfect, pain free days, that should be mentioned as well. Always fatigued? Tired when waking up? That should be mentioned too.
But there’s another caveat with infodumps: do not mention what diagnosis you think you have, because that sets off alarms and frankly, there are so many issues that have the exact same symptoms and your particular situation might be something entirely different.
However, if they diagnose you with something and it doesn’t seem like a perfect fit for any reason, you should definitely ask them about that. A good doctor should be able to explain their reasoning and I hope that you will get to a good doctor.
Try to not be discouraged too much from X-rays that come back negative — you still should keep fighting to solve the issue. Most long-lasting chronic illnesses don’t show up on imaging, because it’s done to rule out mechanical issues, fractures, bone fragments where they shouldn’t be, tumors, etc.
And sometimes you need more imaging after. But chronic joint pain and fatigue could be anything from hormonal issues, sleep apnea, rheumatoid arthritis, etc and unfortunately needs lots of trial and error with medication and tests. It’s just one example though and it sucks, I know, and feels terribly discouraging when tests come back negative and you’re left in limbo.
At this point it’s expected that maybe it was something minor after all so it will heal by itself and you won’t come back, I think. This is where you should still continue pushing, because you’re still experiencing all of the symptoms and it doesn’t mean it’s a nonexistent issue. I hope things will get better for you!
chronically ill/physically disabled people, how do you deal with doctors appointments? what do you say/do to advocate for yourself? im autistic and not diagnosed with a chronic illness yet and i really struggle to know what to say to get them to listen to me and understand so that i can get the help and care i need. even if i bring someone with me, they also need to know what to say and i don't know anyone who understands well enough to explain to the doctor for me, which means that i have to tell them what to say before going. but that's the problem since i just don't know.
i have chronic joint pain that ive had for years but has only gotten worse over time. i also have hypermobile knees which are the worse they've ever been right now. i'm chronically fatigued and barely have the energy to eat and do basic hygiene. i have a few friends that i talk to fairly regularly and im very thankful for them but i still struggle so much with maintaining a social life when i cant even maintain my own physical wellbeing. i only go outside when i absolutely have to/when my pain is low enough and i have enough energy. on average i probably leave my house about once or twice a week, usually to go to medical appointments, to an internship i have once a week or to go grocery shopping. i usually try to do both at the same time if i can (like going grocery shopping after my internship) but most of the time i have to ask my parents to get me groceries since i dont have enough energy to. all i want is to be able to go outside just to take short walks and enjoy nature and the fresh air but i can't do so without the right treatment/a mobility aid. everything im doing right now is bordering the line of too much. im constantly tired and overwhelmed and everything feels like a struggle, even the smallest tasks most people do everyday without thinking twice about it.
i have almost only had bad experiences with doctors and other medical professionals like physiotherapists, which has given me a lot of extra anxiety on top of my already pretty bad social anxiety. i really struggle to make appointments and even more so to go to them, and when i bring myself to do so i really struggle to express myself and explain how i feel and how i want them to help me. i almost always get shut down and offered no actual help with any of my problems. i just don't know what to do anymore.
if anyone has any advice i'd really appreciate it. i know that i can't give up because my life right now without accommodations is too miserable, but i also don't know how to move forward.
sorry if this was hard to understand. i really tried my best to explain but im having a bit of a hard time expressing myself right now due to feeling worse than usual.
120 notes
·
View notes
Text
I’m sorry you’re in that situation. It’s never been fun for me either in any way, I just come home crying and feel like I’ve lost all hope of getting better. I’m currently my very experienced neurologist’s ”most complicated migraine patient” and that doesn’t evoke any feelings other than grief, hopelesness, and anxiety about my options of getting better.
I know people often joke about how fun it is to shock doctors and be the first time they have ever seen somthing.
But I fucking hate it. It sucks. Anytime a doctor say that I want to cry. Had one with over 30 years of experience who works spesificly with patients who have complex medical needs. Tell me that they had never before seen someone who had the reaction and problem I had. They did not know what to do. I was promised something and I didn't get it. The only person in the over hundred of people they see in a year, for over 30 years, that this has happened to.
You know what that means? It means they have no clue what to do. They don't know how to help because this has never happened before, and they haven't even heard of it happening. I'm fucked until I find a doctor who has any idea why what happened happened and then have to sit on a wait list knowing that there is a chance they dont know whats wrong, that they can't do anything or don't know what to do either.
329 notes
·
View notes
Text
braces do damage to your body
canes do damage to your body
crutches do damage to your body
rollators do damage to your body
wheelchairs do damage to your body
before you choose to use a mobility aid you need to weigh the pros and cons of using one. there are drawbacks to every single mobility aid. there is no such thing as a harmless mobility aid. mobility aids are not the right choice for everyone and it's important that people emphasize that when suggesting that people try them. mobility aids can permanently damage your joints and it's important that people emphasize that when suggesting them.
mobility aids need to be an informed decision.
so many people have permanent damage to their bodies that they regret because people online told them to try a mobility aid and that there were no downsides. there are downsides.
a mobility aid is only the right choice when the benefits outweigh the drawbacks. it takes information for someone to know whether they would benefit enough from a mobility aid to make it worth it. when you tell someone that there are no problems with mobility aids, that doctors are all lying about the damage they do, you deny people information. doctors can be wrong and can deny people mobility aids incorrectly but there's truth in the fact that they damage joints, change gaits, and cause muscle atrophy among other problems.
and on that note doctor/PT/OT guidance is important when it's available. using mobility aids that have been sized incorrectly, even for a short time, can cause enough damage that mobility aids are no longer an option for that person. using mobility aids incorrectly, even for a short time, can cause enough damage that mobility aids are no longer an option for that person. failing to tell people that they need to learn how to use and size their mobility aid correctly (preferably with a doctor/PT/OT's help) causes real harm to people.
give people information when you suggest mobility aids to them. people listen to your suggestions without researching and it causes harm.
3K notes
·
View notes
Text
Holy fucking shit, pain is not a matter of fucking willpower. I'm not being fucking weak when I can't push through my fucking pain. Sometimes, I just fucking can't. I don't need to fucking "stick it out" or "keep fighting." When I say I want to give up it is not because I am not fucking trying hard enough. I am trying so fucking hard every fucking second of every fucking day. The fucking able-bodied assholes that say this shit have never been in actual pain a day in their fucking lives, and it is SO obvious. I think I don't want to talk to another able-bodied person for the rest of my entire life.
989 notes
·
View notes
Text
Migraine isn’t a Headache Part Six: make it stop
We looked at medication and treatment for acute attacks of migraines. Things that you can do to treat the pain when you're having it.
This is also probably the first line of help you'll get from a GP or pharmacist or whoever you approach for help.
Some people have success with acute treatments. Maybe the migraine was a one-off, or is a rare occurrence, maybe it was just really responsive to acute meds.
Some people have migraines that don't respond to acute meds, or don't respond well enough to be considered effective treatment.
When you get to this stage, you need to start looking at stopping the migraines before they start, instead of constantly taking acute meds that a) don't work and b) can cause rebound headaches and other problems.
It sucks, because you want to reach for the painkillers when you have pain, but doing so is not sustainable.
Getting into preventative meds ties in a lot with how you go about getting a diagnosis, but I'm going to try to speak about the meds and complimentary treatments AROUND being under a neurologist. On that note, GPs are rarely going to work with you on preventative meds.
There are a few they can prescribe, but you'll probably get better treatment under a neurologist or headache specialist. Sorry.
GPs are useless.
Sorry, bit of my bias there, but I don't use GP's unless I need a referral or quick acute treatment, and EVEN THEN.
It's worth noting as well that you'll usually only get to this stage if your migraines have become chronic, that is:
for over 3 months
you've had 15 headache days a month minimum
of which 8 have migraine features
Some of the treatments aren't indicated for episodic migraines.
((As previously mentioned, this definition might be changing to take into account the impact migraines are having on your life, and not a somewhat arbitrary number; fingers crossed this happens soon))
My list of attempted treatments includes:
amitriptyline (this is one the GP might prescribe for you) (also prescribed for abdominal discomfort and major depressive disorder, although it's fallen out of favour due to increased risk of fatality in overdose)
propranalol (and this) - beta blocker
flunarizine (calcium channel blocker, used to treat high blood pressure and certain heart conditions)
lamotrigine (usually prescribed for epilepsy and bipolar disorder)
topiramate (usually prescribed for seizures)
candesartan (usually prescribed for hypertension)
pregabalin (usually prescribed for seizures and anxiety)
gabapentin (usually prescribed as an anticonvulsant and for nerve pain)
Botox injections
greater occipital nerve blocks
Magnesium/CoenzymeQ10/Vitamin B trio
Aimovig (erenumab, CGRP injection, one of the first migraine-only treatments)
Ajovy (fremanezumab, another CGRP injection, one of the first migraine-only treatments)
sTMS machine (single pulse transcranial magnetic stimulation)
Vyepti (eptinezumab-jjmr IV infusion, another CGRP drug)
I don't think I've had EVERY drug available for migraine prophylaxis, but judging by the increasingly surrendering tone of the letters from my neurologist, I'm just about there.
As you can see, apart from the last CGRP drugs, almost every drug listed is used off licence for migraines, and none of them were developed to treat migraine at all.
You can group most of these drugs into treatment for blood pressure, epilepsy and mental health issues.
The idea that migraines are mainly caused by blood pressure has kind of aged out with advances in research, but the fact remains that some medication that acts on blood pressure still helps migraines.
I think, bearing in mind that a migraine is a neurological storm, that it makes sense that meds that act on activity in the brain (mental health meds/epilepsy meds) can help migraine. Makes logical sense, right?
The usual procedure for taking these medications for migraine (at least in the UK) is to titrate up to the correct dose, and then (assuming you tolerate it and don't get floored by adverse reactions or the side effects) remain on that dose for 3 months before concluding if the medication is successful or not.
If you're seeing some improvement but not a lot, they might keep you on it for longer, or increase the dose.
Otherwise, 3 months and no improvement means you move onto the next drug and/or treatment.
A lot of these drugs have some really heavy side effects. I've experienced worsened tremors, awful dizziness, change in sense of taste, changes in appetite, terrible brain fog.
For migraineurs it comes down to a balancing act.
How bad are the side effects vs how much is this med helping my migraines, and which of the two am I best able to handle.
Maybe you can manage dizziness or not being able to drink Coke anymore over the migraines.
Maybe the awful tremors and inability to think clearly is worse than bearing with the migraines.
This is usually something you discuss with your specialist.
Just saying again, some of these meds are a little hardcore. Don't try treating your own migraines on your own with these meds if you can get your hands on them somehow. Apart from the side effects, the dose if really important too.
In the UK, if you've failed at least three preventative treatments, and have been managed for medication overuse headaches, you can try botox.
BOTOX
The reason botox works for migraines isn't well known, but doctors think it blocks pain transmitters in your brain.
Botox, or botulinum toxin, is a nerve toxin that paralyses muscles.
It's used for cosmetics treatments, but also medically for hemifacial spasm, cervical dystonia, cerebral palsy, bladder pain, lower back pain, neuropathic pain and stroke.
When used for migraine, it's delivered in a series of 31 to 39 small injections, mostly around the forehead, but also on the temples and at the base of the skull.
If you've ever had acupuncture, the needles are a lot like that. I thought they'd hurt more than they did. They were just little stings, not even as bad as plucking an eyebrow hair. Of course, everyone's different with different pain thresholds (especially if you're oversensitised migraine pain leaves you with allodynia) but it's truly not that bad.
You get three sessions 12 weeks apart, just like taking the meds, and if you've had improvement you can continue. If you don't, its on to the next med or treatment.
It feels weird when it settles in. Your forehead tends to freeze, so you can raise your eyebrows and have no lines there. This might unsettle some people, but it does wear off over time.
Side effects include neck pain, muscular weakness and a drooping eyelid, but these improve as the botox wears off. I had a little neck pain, but nothing else. One of them in my forehead bled only a little, none of the rest did.
You can have an allergic reaction, but they will keep you in the treatment or waiting room for some time after your first treatment to check that.
Getting botox for migraine sounds worse than the experience is, but it is about 75% successful for reducing migraine.
Not for meeee
GREATER OCCIPITAL NERVE BLOCKS (GONB)
If your migraines have been resistant to drug treatments and botox, your specialist might decide to try GONB. This is usually a treatment for cluster headache or headaches that originate from pain in the neck, so it may not be applicable to your specific situation.
This treatment involves injecting an anesthetic and a steroid (not always both) into the back of your head/top of your neck around the greater occipital nerve (GON).
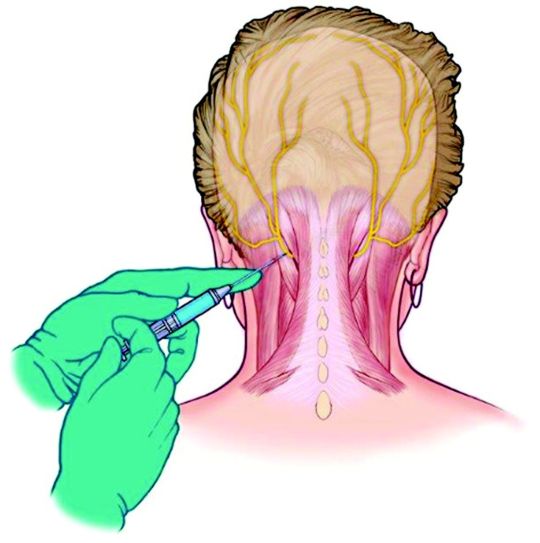
The GON runs from the top of the spine to the scalp, and feeds into an area of the brainstem called the trigeminal nucleus.
A nerve block reduces traffic in this nerve, so reduces the amplification of pain and other sensory information that might be overloading this area.
In simple terms, the nerve block stops the pain signals going into the nerves that make you feel the headache.
A lot of people have had success with this treatment, but I'm not one of them.
I don't want to scare anyone!
The reaction I had is (apparently) pretty rare.
After the neurologist injected the first lot of lidocaine into one side of my head, then the other, I almost immediately felt dizzy and sick.
He let me lay down for a moment, but I felt that I was going to puke, so I had to get up. What followed was tunnel vision, greying out, nearly full syncope (fainting) and then vomiting.
I was having a reaction to the lidocaine, which suddenly made my nausea and faintness when I had my lumbar punction (spinal tap) make sense.
I wasn't able to get to the stage where I had the steroid injection, and whatever there was of the anesthetic after my body tried to purge it made no change to my migraines.
I can't speak for the efficacy of the GONB because my body failed it, but if it's offered, I'd encourage you to try it. Apparently it has helped a lot of people.
CGRPs
After trying 3 meds, then botox, then the GONB and failing all of them, I was put on the next med to see if I'd respond to any of them.
You don't need to have exhausted every pill before trying injection treatments.
You can also mix and match treatments, especially a pill or a CGRP with botox.
With the knowledge that you spend a minimum of 3 months per med (and assuming you don't come off it immediately due to adverse reactions) you can only go through 4 meds in one year. It takes two years on this schedule to go through the meds I've worked through, not including the botox and GONB, and the extra time taken to titrate to the correct dose.
Finding a medication that works to prevent your migraines is a long and exhausting process.
Thankfully, recent research into migraine has come out with the biggest breakthrough in migraine management, I'm going to say ever, because we now have the first medication created directly for the prevention of migraines.
CGRP stands for Calcitonin Gene-Related Peptide
It's a chemical involved in transmitting pain signals through the nervous system – and it’s also associated with the triggering of migraine attacks (among others).
CGRP medications are actually ANTI-CGRP drugs, designed to stop the action of the chemical.
The ones currently available in the UK fall into two groups.
Aimovig (erenumab) that works by binding to the receptor.
Ajoy (fremanezumab), Emgality (galcanezumab) and Vyepti (eptinezumab) which bind to the protein.
Because of that, if you don't have success with Aimovig, try one of the others (and vice versa) as you might see some improvement.
These are adminstered by self-injection (although the first one will be done under nurse supervision) every month with something like an epipen that's injected into your thigh.
The injections hurt me and ached afterwards, but I had no other side effects than that.
I actually had one migraine day where my pain was a 3, which hadn't happened since I started having migraines, but unfortunately, NHS guidelines state that you need to have a reduction in pain days or a significiant reduction in pain in order to stay on them, so I was taken off.
We've just had Vyepti (eptinezumab-jjmr) approved for some people with migraine in the UK.
Vyepti is a CGRP administered via IV infusion over 30 minutes at a clinic, and it's still such a new drug that they're still collecting information on side effects, etc.
I've had my first dose (they're given every 3 months) and while I didn't see a reduction in pain days, I saw maybe a slight reduction in pain, but more than that, my brain fog and pain cloudiness really cleared up, at least for the first month and a half that the effect lasted.
I was actually present in my body for once, instead of half-checked out, even if I was still in pain.
I don't know what the review will bring, but I hope they let me stay on it.
In the US, they've also got a new group of drugs called -gepants (Ubrogepant, Atogepant and Rimegepant for now) which are being used preventatively, but also like triptans, acutely.
Like the injections, they also work on the CGRP receptors by blocking their effect.
I don't know very much about them, but they're also some of the first drugs made specifically for migraine, and there's a lot of excitement about them.
They're safer than triptans for people with heart issues to take, and they DON'T CAUSE REBOUND HEADACHES!
This is huge in the world of migraine treatment, as there are no other acute treatments that do this.
NON MEDICINAL
A large chunk of preventative non-medicinal treatments for migraine involve making lifestyle changes (I know)
The migraine brain is oversensitive and overreactive creature, and ANYTHING can push it into a tantrum. Weather changes, temperature changes, lights, sounds, smells, so many things that we can't control in our environment.
Our migraine brains love routine, and even though it's annoying and removes some chunk of flexibility in our lives, it annoyingly does help.
Sleep routines are helpful, as much as you can fit yourself into one. Setting sleep and wake alarms with x amount of hours in between (7 or 8?) and then sticking to them rigidly means that you'll be getting up when you're still sleepy and going to bed when you're not, but your body will eventually fall into a rhythm and you'll find yourself sleeping and waking at those times automatically.
Issues: daytime naps are no good for sleep routines, and sometimes you just HAVE to sleep when a migraine hits. What if you want to stay up on the weekend? It's difficult, but keeping to a schedule as much as possible is better than leaving it in the wind.
Eating regularly, small meals often is the best. I'm not going to spend a lot of time on this because diet is a huge and sensitive subject, and comorbidities can make this even more difficult, but as far as migraines on their own are concerned, they like the body to be kept as stable as possible, which means a level blood sugar level, etc, and avoiding hunger.
Exercise? I know, I'm not going there, apart from, gentle stretches for your neck, maybe your back, can help. Even if neck problems have nothing to do with your migraines, you're going to end up all crunched up and tense from being in constant pain. Look at stretches for post-operative, for the elderly, for anything you can do in bed. It doesn't have to be high impact or intense, just something you can do now and again to keep your muscles loose.
H~y~d~r~a~t~i~o~n. I'd say use a pretty bottle, but honestly, using whatever will make it easier for you to fill and keep drinking from is better than something that fits your aesthetic. You can always decorate a plastic bottle, or use a favourite glass.
Apart from all those irritating things that abled people always recommend (yoga anyone?) there are also non-drug but prescribed treatments.
One category is DEVICES
I've only tried the sTMS device, so I'll address that first.
sTMS stands for single pulse transcranial magnetic stimulation
You press the button to charge the thing. When it beeps you place the bean-shaped device at the back of your head so it cradles your skull, and then press both buttons at the same time.
There's a ka-chonk, and a sensation like someone's smacked you in the back of the head a little, which is actually the small magnetic pulse.
It works by generating mild electrical currents in the brain that are supposed to disrupt the brain activity linked to your migraines. You can use it acutely, but also daily (2 or 3 times a day, 1 or more than 1 pulse at a time) to prevent migraines.
The machine didn't do anything for me, and made my scalp feel a little sore, although that doesn't appear to be common.
You may also have heard of the Cefaly, a device otherwise called a 'external trigeminal nerve stimulator'
There's that trigeminal nerve again, running around the side of your face and your eye, playing up and causing pain.
You place an electrode on your forehead, and the Cefaly generates micro-impulses to stimulate the trigeminal nerve's nerve endings.
Be aware that the efficacy of the Cefaly device is debated, but it does help some people.
ACUPUNCTURE has been used to help migraine
I had many courses via my GP (the only good one I had) who was trained in acupuncture and went above and beyond to give me as many treatments as possible. I think I had 12. I felt something from them, but they didn't have any effect on my migraines.
Finally, not a drug per se, but VITAMIN SUPPLEMENTS
The best are a trio as follows:
Riboflavin 400mg once daily
Co-enzyme Q10 100mg three times a day
and Magnesium (there are two/three types and the doses are different)
Citrate 600mg OD
Tricylicate 250mg twice a day
or Phosphate 400mg once daily
There is also therapy that is prescribed for management of migraine, not so much prevention as just giving you tools to learn to live with being in pain.
I haven't gotten to that stage yet, and have mixed feelings about it.
Some people have said it's helped, some said it hasn't.
It -feels- a lot like being told 'we can't do anything to help you, you just have to deal with being in pain now'
I haven't tried it, I probably will end up doing so, and maybe I can write a little about it then. For now, I can see why it could be useful, but it does feel a little bit like being abandoned.
And that's all I've got for preventative treatments.
I don't know when I'll be able to start writing about my diagnosis journey, but that should be the next part.
please excuse any typos!
i hope this is still helpful for some people.
10 notes
·
View notes
Text
“you should be at the club” Brother I should literally be sent to the seaside for my health
162K notes
·
View notes
Text
Makes sense that multiple cysts 8 cm in diameter (I kid you not) would cause severe pain whereas doctors were like ”it can’t be that painful” at the time. Like they’re pushing into other organs and the uterus

71K notes
·
View notes
Text
i just heard the phrase “if you wouldn’t trust their advice, don’t trust their criticism” for the first time and i don’t think i’ve ever needed to hear anything more
35K notes
·
View notes
Text
As a person who spends a lot of time lying down and rarely does any kind of activities, I come off as someone who's taking a lot of 'me' time, or a lot of 'resting' time. However I have to assert that any time I spend recovering from an activity is not 'me time' or 'resting time', it's the time that is stolen from me. I can't do anything with this time. I am in pain, I can't move, my activities are limited to 'hopelessly distracting myself so that I do not experience the full horror of what's going on in my body right now'. I don't even get to have 'me time' because of how much of the time is stolen from me.
1K notes
·
View notes

Text
Hi all!
I made this blog as a diary, support and recovery blog for my chronic illnessess. I want to find other people like me, pratice acceptance, share what worked and any research you could also discuss with your doctor. I will talk about medication, good and bad days, and try increase awareness.
Diagnoses that affect me the most
- Chronic migraine
This began with 15-25 migraine days per month in 2021, with episodic migraine and migraine-related seizures being diagnosed around 2014.
I started Botox for migraines in 2022 which reduced my migraine days to 1-5 days per month.
However, since October 2023 I developed daily, non-stop migraines. I’ve been bedridden since then and I’m currently on Botox injections, occassional nerve blocks, Ajovy, and sodium valproate as preventatives.
- Endometriosis
I’ve had severe pain, prolonged bleeding, etc since the beginning of puberty, but it got worse each year until I was diagnosed with endometriosis in 2022 via ultrasound and a physical exam after multiple ER visits where I was bleeding out.
Coincidentally, that’s also the time where my migraines became chronic.
I don’t have access to a good surgeon right now or a second opinion, so I’ve had to manage symptoms on Mirena (the breakthrough bleeding and cysts made it worse), then standalone dienogest (it was great for endometriosis but I’m assuming it triggered worse migraines for me, however I gave it 4 months), and now I’m on NuvaRing continously.
Finding relief for chronic migraine and endometriosis is an unequal balancing act, but there’s so much we still don’t know and can do to make our lives better.
Other diagnoses and issues I’m pursuing help for
- Breathing and sleep quality issues
I’ve progressively had issues with shortness of breath, especially after exercise and before sleep, or in bouts where I feel like I have no oxygen at all. I assume this could also affect migraines and muscle pain. I wake up during the night a lot, and can’t breathe before falling asleep.
Strong allergies, heart problems and structural issues with the nose are ruled out except a slightly deviated septum but my ENT doctor doesn’t think septoplasty would be beneficial so I don’t know.
I had turbinate reduction surgery a year ago and now I’m constantly using hormonal nasal sprays because I feel like I have chronic sinusitis otherwise, air literally doesn’t pass through one of my nostrils at least.
I am currently on asthma treatment (Pulmicort and Berodual for a week first, now Symbicort) after inconclusive spirometry, but I will be working with a pulmunologist to figure it out. But the medication has helped me immensely, as I’ve never felt like I could breathe as well as I do now, and I sleep like a baby. The pulmonologist thinks that if asthma medication helps, then it’s asthma.
So all of my breathing issues are under investigation and inconclusive.
- ADHD and Autism
I was diagnosed with autism as a child, but ADHD was a late diagnosis. I struggle a lot with uni and work in terms of understanding requirements, or sensory overload, etc but it’s been much better since starting medication (unsure yet if lisdexamfetamine or methylphenidate is better). It’s not my main issue whatsoever at the moment since I’m not working or studying at a traditional university, but I struggled a lot when I was working or wasn’t able to study everything from home. So I won’t talk about this as much at the moment.
However, I’m interested in research relating gut issues, autism and immune system issues (e.g my breathing problems, inflammation from endometriosis etc could also fall under that) and biologics like Ajovy, but that’s another fringe topic.
Disclaimer about linking research
I will sometimes make posts that link several research articles or literature reviews (all from reputable sources) together after carefully examining them and discussing my questions with my neurologist. I will always provide references and links or DOIs. Whereas I studied some medical statistics, I’m not a doctor and my advice, experimentation on myself, etc is not medical advice but something you should always discuss with your doctor.
#actually chronically ill#chronic migraine#migraine#chronic pain#endometriosis#ajovy#chronic fatigue#disabled#disability#chronic illness#spoonie#asthma#sleep issues#breathing issues
8 notes
·
View notes
Text
something i think a lot of able bodied people dont understand is that being chronically ill affects your emotions. constantly being exhausted and feeling bad is going to make you sad or depressed or angry or jealous. constantly being in pain is going to affect your mental health. never feeling "good" is obviously going to affect the way you act.
10K notes
·
View notes
Text
the first step to recovery is acceptance.
accepting that you are living with an illness, one that you did not ask for nor is it any fault of your own.
accepting that you are worthy of a healthy life fully of happiness, love and healing.
accepting that healing is NOT linear.
accepting that healing takes time, and to heal is to feel.
accepting that you can get better.
accepting yourself for who you are.
837 notes
·
View notes