#'logic' is about not responding to emotional stimuli and not acting based on emotions - it does not mean you're smart
Text

Vulcan Dumb & Dumber
#T'Meni-bu#Movik#doodle page#bee doodles#suggestive#sveyko (guest appearance) <- she's talking about something she's writing#T'Meni calls Movik 'yam' ... if she were human she'd be a 'pookie bear <3' type of girl#I thought it'd be fun to see a Vulcan who's straight up an idiot#logical thinker - follower of Surakian principals etc etc but just also not smart <3#both T'Meni & Movik grew up sheltered and didn't try very hard in school. Movik's life plan was to get into Starfleet#and when he failed to do that his dad just made him the owner of one of his hot spring hotels. T'Meni's life plan was to marry Movik#and be beautiful and she succeeded! Now they both run that hot springs hotel and everyone who visits loves T'Meni#Nothing bad has ever happened to T'Meni and nothing bad ever WILL happen to T'Meni <3#beas ocs#star trek oc#vulcan oc#'logic' is about not responding to emotional stimuli and not acting based on emotions - it does not mean you're smart#and Movik & T'Meni are here to prove that to the world <3
42 notes
·
View notes
Text
Using MBTI for your character (p1)
take the mbti test and answer like your character would, write down the answer you put.
what's the mbti type of your character?
what is their archetypal story role?
don't forget that your character doesn't have to be perfectly like the mbti type.
The Myers-Briggs Type Indicator
Based on Carl Jung's theory and determine 16 personality types, derived from four dichotomies:
extraversion vs introversion (focusing on the world outside vs focusing on mental world),
thinking vs feeling (acts based on reason vs acts based on heart),
sensation vs intuitive (led by external sensory stimuli vs led by undefinable internal feelings).
judging vs perceiving (structured and organized life vs freewheeling and spontaneous life).
The Sensing-Judging Types
Introverted Sensing Thinking Judgment (ISTJ)
energized by time spent alone, focuses on facts and details, makes decision based on logic and reason, prefers to be planned and organized.
detail-oriented, realistic, present-focused, observant, logical and practical, orderly and organized.
judgmental, subjective, tend to blame others, insensitive.
dominant: introverted sensing, focused on the present moment but rely on the memories of experiences to form expectations for the future.
auxiliary: extraverted thinking, looking for rational explanation for events, focus on details, appreciate knowledge that has immediate practical application.
tertiary: introverted feeling, make personal interpretation based on their internal set of values.
inferior: extraverted intuition, enjoys new ideas and experiences.
Introverted Sensing Feeling Judging (ISFJ)
enjoy structure, observers, focused on other people.
reliable, practical, sensitive, eye for detail.
dislikes abstract concepts, avoid confrontation, dislike change, neglects own needs.
dominant: introverted sensing, focus on details and facts, prefer concrete information, attuned to immediate environment and firmly grounded in reality, recall past experience to predict outcome of future choice/event.
auxiliary: extraverted feeling, focused on developing social harmony and connection which is accomplished by socially appropriate behaviors. try to fill the wants and needs of others.
tertiary: introverted thinking, tend to be very organized, prefers to see how things fit together and how it functions as a whole.
inferior: extraverted intuition, taking in facts and then exploring the what-if.
Extraverted Sensing Thinking Judging (ESTJ)
high value on tradition, rules and security. often become involved in civic duties, government branches and community organizations.
can be seen as predictable, stable, committed and practical. tend to be frank and honest about their opinions.
practical, realistic, dependable, self-confident, hard-working, traditional, strong leadership skills.
insensitive, inflexible, not good at expressing feeling, argumentative, bossy.
dominant: extraverted thinking, objective information and logic to make decisions. enjoy learning about things that they can see an immediate use for but tend to lose interest in abstract and theoretical things. good at making fast and decisive choice but may rush to judgment.
auxiliary: introverted sensing, good at remembering things with details, utilize past experiences to make connections with present events. more focused on familiarity. enjoy habits and routines.
tertiary: extraverted intuition, seek out novel ideals and possibilities. may explore the possible meanings in order to spot new connections or patterns.
inferior: introverted feeling, make decisions based on feeling, tend to give much thought to their emotions.
Extraverted Sensing Feeling Judging (ESFJ)
sensitive to the needs and feelings of others and are good at responding to the care the people need. want to be liked and can be easily hurt by unkindness/indifference.
derive their value system from external sources including the community at large. strong desire to exert control over their environment. careful observers of others and are adept at supporting and bringing the best in people.
kind, loyal, outgoing, organized, practical, enjoy helping others.
approval seeking, sensitive to criticism.
dominant: extraverted feeling, tend to make decisions based on personal feeling, tend to judge people and situation based on it.
auxiliary: introverted sensing, focused on the present and interested in concrete and immediate details.
tertiary: extraverted intuition, make connections and find creative solutions to problems, known to explore the possibilities when looking at a situation.
inferior: introverted thinking, organized and like to plan things in advance.
sources
https://www.truity.com/myers-briggs/judging-vs-perceiving
verywellmind.com
https://www.toolshero.com/psychology/jung-personality-types/
https://www.myersbriggs.org/my-mbti-personality-type/mbti-basics/the-16-mbti-types.htm
https://www.arcstudiopro.com/blog/myers-briggs-characters/
19 notes
·
View notes
Note
What kind of strengths and weaknesses do the Hymns os Struggle cast have? I think my Bioshock Au Henrietta's strength is kindness,but she is too honest as a flaw,Josephine Drew is intelligent and polite,but tends to come off as flinty and insensitive and Joshua is determined,but tends to over-empathise with other people.
Really lovely question! Here’s my best ideas at the moment. Heads up, there’s spoilers for the series throughout so I’ll tag it as “hymns spoilers,” but I think by this point most people that care about spoilers for the story have read it and I’m not super concerned about talking freely below.
Francine: She’s definitely not an illogical person, but she tends to go with her gut and heart. She also has to work to find the line between caring for someone and not taking care of herself. Her strengths are determination and compassion, and whether she likes it or not she’s a natural leader. While it’s a constant struggle on her mind, having to address boundaries with caring for others also means she’s very mature in finding things that bother her and figuring out what to do about it. She wants to understand other people, and while that often puts her at risk, the reward of companionship and others’ (if not begrudging) admiration of her genuine self is what keeps her alive in the unforgiving studio.
In a literal sense, she’s an educated sociology student as a strength. Her weaknesses in the studio are that she’s physically the weakest and she doesn’t know much about the studio and it’s story at all. As a human of flesh and blood- soul still attached- she’s in a fragile state here and constantly has to watch for dangers that would cause her to join the ink as everyone else has.
Gingie (Joey): A bit of a subversion of Francine. He cares a lot about others, but he also tends to make himself the responsible entity involved. He makes assumptions and decisions for others that aren’t his to make. He’s also very much in denial about aspects of himself that are negative, and finds them as things to ignore or eliminate rather than accept. He has as much strength for his weakness, though, in that he is extremely charismatic, especially thanks to his genuine front. He’s a dreamer, and a believer, and can and *will* make you believe you can do whatever it is ahead of you; same applies to himself.
In a literal sense, he’s immortalized by the studio and granted control over all of its supernatural abilities. He sees all of the studio through the eyes of any image of Bendy, such as on posters and dolls. Downside is that it’s based on his own (uncontrolled, ironically) emotions and thoughts, so things don’t always go as he plans. He has no choice but to see everything in the studio, and he has only limited say in what he causes.
Sammy: My interpretation of Sammy frames it so that his faith and sense of religion is a double edged sword, and he has to figure out how to navigate in a positive direction. He wants to be better, he wants to be helped, at worst he very easily becomes resigned to what seems to be fate (and given the studio I can’t blame him too much). However, this makes him excellent at finding things to hope in, the lights at the end of the tunnel. He *will* fight tooth and nail for what he believes in. He also doesn’t remember any of his past unless prompted, and often times doesn’t wish to know.
In a literal sense, as with other ink creatures in Hymns, if injured he can be reformed from the puddles. Not fun, at all, but doable. He’s stronger than searchers, but otherwise “on the bottom of the food chain.”
Alice: She is very easily provoked. This would make her predictable, if not for the fact that she has the bite to back it up. She embodies independence, for better or worse, and loathes reliance on others even emotionally. When she recognizes her own emotional attachments, she’s at least at first very uncomfortable. Her full memory of before the studio’s downfall is the most extensive, besides Joey’s, and can be used both as an advantage and disadvantage. As a strength, she recognizes beauty in humanity despite being away from it for so long. She’s plausibly the smartest person in the studio as well as the most practical and pessimistic.
In a literal sense, she knows both how to fight the “lesser” ink creatures and hide from the ink demon. Her ultimate goal is to obtain perfection and protect her progress on looking more and more like the original Alice cartoon, so while she likes to threaten and can follow through, she prefers not to put herself in a position with risk unless given no choice.
The Projectionist: If he has memories, in this form you can’t tell. He’s largely in his own dismal routine, pacing the halls and responding to stimuli as it engages with his senses. He has empathy and enjoys interaction, but it’s difficult to engage with unless you first put yourself at risk, as he is volatile at first contact. He is difficult to persuade, but has unbreakable loyalty if you have it.
In a literal sense, he’s deaf, but if standing in ink, he can feel the vibrations sound makes. His strength rivals the ink demon’s, and he can travel through the walls, although rarely.
The Ink Demon: Like the projectionist, but much less approachable and gives the studio residents an impression of godliness. He terrifies, and clearly he has power and control. In truth, he is the part of Joey that Joey cannot help- sort of like how one thinks they’d like to do something, but they wouldn’t; the ink demon does what Joey wants deep down, regardless of logic. The ink demon gives no impression of actual intelligent thought of his own, as he acts only as if puppeteered.
In a literal sense, interacting with Joey either directly or indirectly will influence the behavior of the ink demon. As in the case of Francine, her accidentally showing Joey her purpose for being in the studio and reminding him more and more of his son Henry caused the ink demon to not only spare her but often times help her, even when it went against what Joey was trying to accomplish.
#writing musings#batim#bendy#bendy headcanons#bendy and the ink machine#bendy au#bendy oc#joey drew#gingie#sammy lawrence#alice angel#malice angel#the projectionist#the ink demon#hymns of struggle#hymns spoilers#long post#Anonymous
12 notes
·
View notes
Text
Diane E. Hoffmann & Anita J. Tarzian, The Girl Who Cried Pain: A Bias Against Women in the Treatment of Pain, 29 J Law, Med & Ethics 13 (2001)
To the woman, God said, “I will greatly multiply your pain in child bearing; in pain you shall bring forth children, yet your desire shall be for your husband, and he shall rule over you.” --Genesis 3:16
There is now a well-established body of literature documenting the pervasive inadequate treatment of pain in this country.1 There have also been allegations, and some data, supporting the notion that women are more likely than men to be undertreated or inappropriately diagnosed and treated for their pain.
One particularly troublesome study indicated that women are more likely to be given sedatives for their pain and men to be given pain medication.2 Speculation as to why this difference might exist has included the following: Women complain more than men; women are not accurate reporters of their pain; men are more stoic so that when they do complain of pain, “it’s real”; and women are better able to tolerate pain or have better coping skills than men.
In this article, we report on the biological studies that have looked at differences in how men and women report and experience pain to determine if there is sufficient evidence to show that gender3 differences in pain perception have biological origins. We then explore the influence of cognition and emotions on pain perception and how socialized gender differences may influence the way men and women perceive pain. Next, we review the literature on how men and women are diagnosed and treated for their pain to determine whether differences exist here as well. Finally, we discuss some of the underlying assumptions regarding why treatment differences might exist, looking to the sociologic and feminist literature for a framework to explain these assumptions.
We conclude, from the research reviewed, that men and women appear to experience and respond to pain differently, but that determining whether this difference is due to bio- logical versus psychosocial origins is difficult due to the complex, multicausal nature of the pain experience. Women are more likely to seek treatment for chronic pain, but are also more likely to be inadequately treated by health-care providers, who, at least initially, discount women’s verbal pain reports and attribute more import to biological pain contributors than emotional or psychological pain contributors. We suggest ways in which the health-care system and health-care providers might better respond to both women and men who experience persistent pain.
Do Men and Women Experience Pain Differently?
The question of whether men and women experience pain differently is a relatively recent one. Until about a decade ago, many clinical research studies excluded women, resulting in a lack of information about gender differences in disease prevalence, progression, and response to treatment.4 Research on sex-based and gender-based differences in pain response has mounted over the past several years, partially motivated by 1993 legislation mandating the inclusion of women in research sponsored by the National Institutes of Health.5
Three review articles summarized the research findings on sex-based differences in pain response through the mid- 1990s, with most research focusing on sensory (often laboratory-induced) pain. Unruh examined variations between men and women in clinical pain experience through an extensive review of available research.6 She found, in general, that women reported more severe levels of pain, more frequent pain, and pain of longer duration than men. Women were more likely than men to report migraines and chronic tension headaches, facial pain, musculoskeletal pain, and pain from osteoarthritis, rheumatoid arthritis, and fibromyalgia. Women were also more likely than men to develop a chronic pain syndrome after experiencing trauma similar to that experienced by men.
Berkley drew similar conclusions — that for experimentally delivered somatic (skin or deep tissue) stimuli, females have lower pain thresholds, greater ability to discriminate pain, higher pain ratings, and less tolerance of noxious stimuli than males.7 Berkley, however, cautioned that these differences were small and affected by many variables, such as type of pain stimulus, timing of the stimulus, size or bodily locus of the stimulus, and experimental setting. For example, more reliable differences between the sexes have been found when patients are exposed to electrical and pressure stimuli as opposed to thermal stimuli, and when pain is induced in experimental settings as opposed to clinical settings.
Lastly, Fillingim and Maixner reviewed research on sex-based differences in response to noxious stimuli.8 The studies they reviewed also indicated that although pain responses were highly variable among individuals, females exhibited greater sensitivity to laboratory-induced pain than males. They concluded that “it seems plausible that such disparity in the experience of clinical pain [between men and women] could be explained, at least in part, by enhanced pain sensitivity among females.”9
While approximately half of all existing studies prior to 1997 found no difference between men and women in their response to experimental pain, of those studies that did, all were in the same direction: “lower pain threshold, higher pain ratings, and lower pain tolerance for women.”10
More recent studies have contributed further empirical evidence of a difference between men and women in pain response.11 Much of this research has focused on a search for biological differences. Although these early findings do suggest biologically based differences, there remain many research questions yet to be answered.
Biological differences
A number of scientists have hypothesized about potential biological explanations for gender pain differences. Berkley described three aspects of male and female biology that plainly differ: the pelvic reproductive organs, types of circulating hormones, and cyclical changes in hormone levels.12
Other biological explanations for the differences in pain response include mechanisms of analgesia having to do with opioid receptors in the body, mechanisms of nerve growth factor, and sex-based differences in sympathetic nervous system function (e.g., sex-based differences in areas of the brain associated with reproduction). Berkley stated that these differences could result in men and women experiencing different emotional responses to pain13 (e.g., anxiety, fear, depression, or hostility).
Reproductive hormones
A number of studies have added to the body of literature on the influence of reproductive hormones on biological pain differences. Berkley concluded that the reproductive hormones appear to influence sex-based pain differences through the action of a number of neuroactive agents, such as dopamine and serotonin.14
Giamberardino and colleagues found that a woman’s pain sensitivity increases and decreases throughout her menstrual cycle, with skin, subcutaneous tissue, and muscles being affected differently by female hormonal fluctuations.15 They also found that sex-based differences in pain response may depend on the proximity of the stimulus to external reproductive organs. Fillingim and colleagues found that the menstrual cycle produced greater effects on ischemic (i.e., lack of blood flow and oxygen), compared with thermal, pain sensitivity.16 The authors suggest that opiate receptors could be desensitized by reproductive hormones during certain phases of a woman’s menstrual cycle, thus increasing pain sensitivity (particularly ischemic pain sensitivity) at those times.
Glaros, Baharloo, and Glass found that lower levels of circulating estrogens may be associated with higher levels of temporomandibular disorder (TMD) pain and other joint pain in women.17 Dao, Knight, and Ton-That studied the influence of reproductive hormones on TMD.18 They hypothesized that there is a link between reproductive hormones and inflammation and pain — that the hormones may “act directly in the muscles to modulate the release of nitric oxide,” which causes vasodilation (blood vessel dilation), inflammation, and pain.19 In addition, estrogen may interact with various mediators of inflammation (i.e., swelling) and increase pain sensation.20
Stress-induced analgesia responses
Differences have been found between male and female rats for “stress-induced analgesia” responses.21 Stress-induced analgesia involves activation of an intrinsic pain inhibitory system by a noxious stressor, such as exercise-induced stress or predator-evoked stress.
Mogil and colleagues report on a sex-specific stress-induced analgesia mechanism in female mice that is known to be estrogen-dependent and to vary with reproductive status, but for which the neurochemical identity has remained obscure.22 The authors performed genetic mapping experiments to identify the gene underlying stress-induced analgesia in both sexes and found a specific genetic component in female mice but not in male mice.
Brain and central nervous system
Some research has shown differences in the brain and central nervous system of men and women that may contribute to differences in pain response. For example, Fillingim and Maixner describe neural mechanisms that contribute to sex-based differences in the perceptual, emotional, and behavioral responses to noxious stimuli.23 These include peripheral afferents (impulses sent to the brain), brain and central nervous system networks, and peripheral efferents (commands sent from the brain to the muscles). The authors note differences in female tissue thickness and sensory receptor density as one example of structural differences in females that may contribute to enhanced perception of sensation to the skin.
Animal studies provide some evidence that sex-based differences in pain response have biological and genetic origins. Aloisi, Zimmermann, and Herdegen found differences in immune chemicals in the hippocampus and septum of male and female rats that were subjected to a persistent pain- ful stimulus and restraint stress.24 The authors hypothesized that hormonal and behavioral differences between the sexes are accompanied by genetic differences in the limbic system — an area of the brain that, in humans, is involved in cognition and emotion.
Other researchers have probed the human brain for sex- based differences that influence pain responses. Mayer and colleagues found that, compared to male patients with irritable bowel syndrome, female patients with the same syndrome showed specific perceptual alterations in response to rectosigmoid (intestinal) balloon distension and differences in regional brain activation measured by positron emission tomography (PET).25 Findings suggest that physiological sex-related differences in the experience of pain exist in irritable bowel syndrome patients and can be detected using specific stimulation models and brain imaging techniques.
Paulson and colleagues studied cerebral blood flow through PET imaging in normal right-handed male and female subjects as the subjects discriminated differences in the intensity of painless and painful heat stimuli applied to the left forearm.26 Females had significantly greater activation of the contralateral prefrontal cortex, the contralateral insula, and the thalamus when compared to the males. The authors surmised that the differences between men and women in their response to pain were (1) a direct result of physiological differences between men’s and women’s brains; (2) mediated by emotional or cognitive responses that are different between men and women and are responsible for brain activation differences between men and women; or (3) a result of both (1) and (2).
Biology as explaining too much, too little
Given the physiological sex differences reviewed thus far, one might expect the gap in pain responses between men and women to be greater than the research evidence indicates.27 This paradox in the research has led Unruh — commenting on Berkley’s conclusion that differences between men and women in pain perception and response exist but are small and highly variable28 — to argue for a “conceptual shift” in “our efforts to understand the relationships between sex and pain experience”:
The question changes from “Why do women and men differ in their experiences of pain?” to “How do women dampen the effect of powerful sex differences in physiological pain mechanisms to achieve only small sex difference in their actual pain experience?”29
Consequently, researchers must look not only at why women may experience more pain than men, but also at why the difference in experience is not greater than recent findings regarding physiological pain-related differences would indicate. One answer to this paradox may be that some physiological differences between men and women actually make their pain responses similar. For example, De Vries and Boyle concluded that despite major differences in physiological and hormonal conditions, differences between the sexes in the brain create a mediating effect on pain, perhaps resulting in men and women displaying remarkably similar behaviors.30 Another explanation is that more than physiological differences are at work.
What is clear is that the research to date provides ample evidence that differences between men and women in pain response exist.31 What is unclear is whether the reasons for these findings are grounded in differences in biology or differences in coping and expression, or both.
The mind-body connection
Although modern scientists have attempted to identify and localize specific pathophysiological mechanisms that produce and influence pain sensations, progress on this front is advancing slowly. Most experimental pain research has focused on laboratory-induced noxious sensory stimuli, such as heat, cold, pressure, and shock. Subjects report the level at which they detect pain (“threshold”) and the level at which they can no longer tolerate pain (“tolerance”). Bendelow writes: “The experimental nature of these studies does not allow the social context to be taken into account and the psychological research on pain perception is weighted heavily towards sensory cues, with little emphasis on the subjectivity, or indeed any recognition of models of perception that emphasise interaction between sensory cues and expectations or prior experience.”32
The focus on a physiological basis for pain has ignored the findings that one’s response to pain is influenced by a multitude of factors, which may include the biological, psychological, and cultural differences between men and women.
External stimuli may set off a biological cascade that contributes to the sensation of pain, but cognition and emotion also contribute to the experience of pain. Cognitive awareness of and emotional response to pain (which are affected by psychosocial and cultural influences) in turn influence the brain’s and body’s subsequent physiological responses. Unlike the “Cartesian” approach that views pain as a product of either biology (body) or psychology (mind), a more informed approach is to acknowledge the interdependence of the two, in addition to cultural influences.33
Psychological and cultural gender differences
Psychological factors influencing the pain response include cognitive appraisal of pain (i.e., meaning-making), behavioral coping mechanisms, and cultural influences. According to Unruh, “[u]nderlying biological differences in pain mechanisms may predispose women to have more pain and may affect recovery from pain but sociological [i.e., cultural] and psychological factors also influence pain perception and behavior.”34
Cognitive appraisal and meaning-making
Cognitive appraisal refers to the process of attributing meaning to an event, which then influences one’s behavioral response to that event.35 For various reasons, men and women may attribute different meanings to their pain experiences.
For one, the types of pain that men and women experience tend to be different. Women more often experience pain that is part of their normal biological processes (e.g., menstruation and childbirth), in addition to pain that may be a sign of injury or disease. Women may thus learn to attend to mild or moderate pain in order to sort normal biological pain out from potentially pathological pain, whereas men do not need to go through this sorting process.36
In addition, men’s and women’s different gender role expectations may influence how they attribute meaning to their pain. Women have been found, for example, to describe their pain by giving more contextual information, such as impact on personal relationships and child-care duties. Men, on the other hand, are more likely to wait to attend to pain until it threatens to interfere with their work duties. Their pain reports are more likely to be an objective report- ing of physical symptoms or functional limitations, and to lack reference to contextual factors such as impact on personal relationships.37
According to one study, factors that influenced women’s likelihood of seeking health care for their pain included a predisposition to “resilience or positive regard for their ability to handle the problem.” Men, in contrast, were influenced to seek health care by “a negative attitude about the condition in terms of its harmfulness, loss or threat.”38 Thus, gender differences in cognitive appraisal and meaning-making of pain may explain some of the differences between men and women in pain response.
Behavioral coping
Prompted by one’s cognitive appraisal of a stressor like pain, individuals respond using various coping mechanisms. Researchers have found that men and women differ in their mechanisms of coping with stress — particularly, coping with pain. Unruh, citing other studies, reported that women more frequently use coping strategies that include “active behavioral and cognitive coping, avoidance, emotion-focused coping, seeking social support, relaxation, and distraction, whereas men rely on direct action, problem-focused coping, talking problems down, denial, looking at the bright side of life and tension-reducing activities such as alcohol consumption, smoking and drug abuse.”39 Thoits found that women’s ways of coping involved more expression of feelings and seeking social support, whereas men’s ways of coping “were more rational and stoic (e.g., accepting the situation, engaging in exercise).”40 Unruh, Ritchie, and Merskey found that in response to pain, women reported significantly more problem-solving, social support, positive self-statements, and palliative behaviors than men.41 Jensen and colleagues found that among individuals with long-term intractable pain in the neck, shoulder, or back, women increased their behavioral activity (e.g., household chores and social activities) as a coping strategy more often than men.42 Other studies suggest that coping strategies are influenced more by the type and duration of pain than by whether the person is a man or a woman.43
Research has also shown that women, as compared to men, respond more aggressively to pain through health-related activities (e.g., taking medications or consulting a healthcare provider).44 This is consistent with studies that have shown that women tend to report more health-care utilization for treatment of pain than do men.45
Culture, gender, and pain
The interplay between behavior and the value systems of a culture is complex and may influence pain perception in many ways. Children are socialized from a very young age to think about pain and to react to painful events in certain ways. In many societies, boys are actively discouraged from expressing emotions.46 Pollack reports that in the United States, “[r]esearchers have found that at birth, and for several months afterward, male infants are actually more emotionally expressive than female babies. But by the time boys reach elementary school much of their emotional expressiveness has been lost or has gone underground. Boys at five or six become less likely than girls to express hurt or distress, either to their teachers or to their own parents.”47 Pollack attributes this change to attitudes toward boys that are “deeply ingrained in the codes of our society” and as a result of which “boys are made to feel ashamed of their feelings, guilty especially about feelings of weakness, vulnerability, fear, and despair.” Male pain research participants have reported that they “felt an obligation to display stoicism in response to pain.”48 Other investigators found that whether the researcher was a man or a woman influenced male pain response in a laboratory setting, with males reporting less pain in front of a female researcher than a male researcher, whereas the researcher’s sex did not affect the responses of female subjects.49
Culture and socialization may also account for the differences in pain reporting between men and women. Women have been found to adopt a more “relational, community-based perception of the world” that allows them to form more extended social support networks and to express their emotions more than men.50 Because of these different socialization experiences, women’s and men’s styles of communication differ,51 which most likely influence how they report their pain to each other and to health-care providers. Miaskowski noted that “women are better able to fully describe their pain sensations than men, or are more willing to describe them, especially to female nurses.”52 In addition, as already mentioned, women tend to describe their pain to a health-care provider by including contextual information, like the pain’s effect on their personal relationships.53
Differences in treatment
The literature suggests not only that men and women communicate differently to health-care providers about their pain, but that health-care providers may respond differently to them. Miaskowski reported on several studies that identified such differences in response and treatment.54 Faherty and Grier studied the administration of pain medication after abdominal surgery and found that, controlling for patient weight, physicians prescribed less pain medication for women aged 55 or older than for men in the same age group, and that nurses gave less pain medication to women aged 25 to 54.55
Calderone found that male patients undergoing a coronary artery bypass graft received narcotics more often than female patients, although the female patients received sedative agents more often, suggesting that female patients were more often perceived as anxious rather than in pain.56 An- other study, examining post-operative pain in children, found that significantly more codeine was given to boys than girls and that girls were more likely to be given acetaminophen.57
Miaskowski further reported on two more recent studies. In a 1994 study of 1,308 outpatients with metastatic cancer, Cleeland and colleagues found that of the 42 percent who were not adequately treated for their pain, women were significantly more likely than men to be undertreated (an odds ratio of 1:5).58 In another study of 366 AIDS patients, Breitbart and colleagues found that women were significantly more likely than men to receive inadequate analgesic therapy.59 The assessment of undertreatment in both studies was based on guidelines developed by the World Health Organization for prescribing analgesics.
Other studies also indicate differences in how men and women are treated by health-care providers for their pain. In a retrospective chart review of male and female post-operative appendectomy patients without complications, McDonald found that in the immediate post-operative period, males received significantly more narcotic analgesics than females.60 However, differences were not significant when taking into account the whole post-operative period. McDonald suggested that these differences might be due to gender-stereotyping during the initial post-operative period when the patient is still drowsy from anesthesia and not always able to make his or her pain needs known. The nurse may respond differently to male and female patients during this time, as compared to later in the post-surgical recovery period when patients are more fully awake and able to report their pain.61
A recent prospective study of patients with chest pain found that women were less likely than men to be admitted to the hospital. Of those hospitalized, women were just as likely to receive a stress test as men, but of those not hospitalized, women were less likely to have received a stress test at a one month follow-up appointment.62 The authors attributed the differences in treatment to the “Yentl Syndrome,” i.e., women are more likely to be treated less aggressively in their initial encounters with the health-care system until they “prove that they are as sick as male patients.” Once they are perceived to be as ill as similarly situated males, they are likely to be treated similarly.63
The “Yentl Syndrome” hypothesis fits well with the results of a study by Weir and colleagues, which found that of chronic pain patients who were referred to a specialty pain clinic, men were more likely to have been referred by a general practitioner, and women, by a specialist.64 The results suggest that women experience disbelief or other obstacles at their initial encounters with health-care providers. An older study (1982) also found that of 188 patients treated at a pain clinic, the women were older and had experienced pain for a longer duration prior to being referred to the clinic than the men. In addition, the researchers found that women were given “more minor tranquilizers, antidepressants, and non-opioid analgesics than men. Men received more opioids than did women.”65 These findings are consistent with those reported by Elderkin-Thompson and Waitzkin, who reviewed evidence from the American Medical Association’s Task Force on Gender Disparities in Clinical Decision-Making. Physicians were found to consistently view women’s (but not men’s) symptom reports as caused by emotional factors, even in the presence of positive clinical tests.66
In addition to actual differences in treatment, studies have also shown differences in health-care providers’ perceptions of men’s and women’s experiences of pain. McCaffery and Ferrell, using a questionnaire administered to more than 300 nurses, found that nurses perceived differences between men and women in sensitivity to pain, pain tolerance, pain distress, willingness to report pain, exaggeration of pain, and nonverbal pain expressions.67 More respondents felt that women, as compared to men, were less sensitive to pain, more tolerant of pain, less distressed as a result of pain, and more likely to report pain and express pain through nonverbal gestures. In another study, nurses were given vignettes describing a particular patient and situation, and were asked to estimate the minutes needed for specific nursing interventions for each patient. In their estimations, the nurses planned significantly more analgesic administration time (as well as ambulation and emotional sup- port time) for male patients than for female patients.68
In addition to whether the patient is a man or a woman, physical attractiveness and nonverbal expressions of pain have been found to influence a health-care provider’s response to the patient’s pain. Hadjistavropoulos and colleagues found that physically unattractive patients were more likely to be perceived as experiencing greater pain than more attractive patients and that the more attractive patients were more likely to be viewed as able to cope with their pain.69 These differences in perception were more likely to be true for female patients than male patients — that is, the effect of the patient’s attractiveness (or lack thereof) on a health-care provider’s perception of the patient’s pain sensitivity was not significant for male patients but it was for female patients. Attractive female patients were thought to be experiencing less pain than unattractive female patients. The authors concluded that a “strong ‘beautiful is healthy’ stereotype” was used by health-care providers in assessing patient pain and that attractive persons “were perceived to be experiencing less pain intensity and unpleasantness, less anxiety and less disability than physically unattractive persons.”70 The authors further concluded that such stereotypes have a negative effect for both attractive and unattractive individuals.71
What Accounts for Differences in Treatment?
The available literature indicates that women receive less treatment for their pain than men. These findings raise the question of whether such a difference in treatment is justified or whether the differences are the result of unproven assumptions and biases about men and women and their sensitivity toward pain or their credibility in reporting pain.
Rationales supported by the data
Treating men and women differently for their pain might be justified if they experience pain differently or respond differently to pain treatment modalities. As for the latter argument, previous research has shown that men and women metabolize medication differently.72 In response to pain medications specifically, Gear and colleagues showed that women experience significantly greater analgesia from kappa-opioids like pentazocine than males.73 Others have predicted that genetic research will lead to identifying drugs for pain that are specific to men’s and women’s biological needs.74
In addition, evidence indicates that men and women do experience pain differently. There is no consensus, however, whether this difference in experience is because women are biologically more sensitive to pain than men, although recent studies provide evidence to support this explanation.75 What is clear is that women in clinical studies often report greater sensitivity than men in response to the same noxious stimuli. This could mean that, in fact, there is a biological difference between men and women that results in women experiencing greater pain than men when exposed to the same stimulus. Or, it could mean that women do not tolerate pain as well as men, or that women are more likely to report pain than men are.
The difficulty in concluding much from existing studies is the subjective nature of pain. While some researchers are exploring the development of diagnostic techniques to validate patients’ pain reports, there are currently no reliable, objective, clinical indicators for pain, e.g., blood pressure, heart rate, temperature.76 Although men’s and women’s brain and central nervous system functioning have been found to respond differently to laboratory-induced pain, the degree to which cognition and emotion influence these pathways is unclear. Animal studies provide compelling evidence that basic biological differences do exist; however, pain in these studies is measured differently from how it is measured in humans (e.g., time to paw withdrawal or tail lick in rats versus self-report in humans). Because diagnostic techniques are not available to accurately “measure” pain and because pain perception is affected by psychological and cultural factors, patient self-reporting remains the basis for diagnosis.
The data support the assertion that women are more likely to report pain than are men in response to the same stimuli. Apart from differences in pain sensitivity, this could be attributed to differences in coping. The literature on coping appears to indicate that women tend to cope in more constructive ways, such as seeing a health-care provider, reaching out to others, and/or praying, whereas men tend to accept the pain, ignore it, or resort to drugs or alcohol rather than consult with a health-care provider.77 These strategies are consistent with cultural mores that discourage men from expressing weakness or vulnerability.
An alternative hypothesis that may explain why men’s pain complaints evoke more medical and nursing interventions is that men wait longer than women to seek medical assistance for their pain and thus are at a stage where their pain characteristics are more extreme and in need of more immediate care. But while there is some evidence that men are less likely to seek medical care for their pain at early stages (or until it interferes with their ability to work),78 there is no evidence that they are in need of more aggressive care than women when they enter the health-care system for pain relief.79 Rather, study findings suggest that women report more severe pain symptoms than men because they suffer from more severe pain-related diseases. For example, in a telephone survey of those with rheumatoid arthritis, researchers found that women reported more severe symptoms than men and that this difference was due to “more severe disease rather than a tendency by women to over-report symptoms or over-rate symptom severity.”80
The perception of women by health-care providers
Given that women experience pain more frequently, are more sensitive to pain, or are more likely to report pain, it seems appropriate that they be treated at least as thoroughly as men and that their reports of pain be taken seriously. The data do not indicate that this is the case. Women who seek help are less likely than men to be taken seriously when they report pain and are less likely to have their pain adequately treated.81
This conclusion raises the question of what accounts for this difference in treatment. In light of the apparent lack of objective data supporting lesser treatment of women for pain, a likely explanation is the health-care provider’s attitudes regarding male and female sensitivity to or tolerance of pain and the validity of their self-reports. There are, in fact, data to support the hypothesis of this attitude or bias by health-care providers. The study by McCaffery and Ferrell of 362 nurses and their views about patients’ experiences of pain found that while most of the nurses (63 percent) agreed that men and women have the same perception of pain, 27 percent thought that men felt greater pain than women. Only 10 percent thought that women experienced greater pain than men in response to comparable stimuli.82 This result has no justification in the literature (and, as discussed above, is actually contradicted by it). The authors do not speculate as to what might contribute to this difference in attitude.
The same study also found that almost half of the respondents (47 percent) thought that women were able to tolerate more pain than men as compared to 15 percent who felt that men were able to tolerate more pain than women. This result, although consistent with other studies,83 seems at odds with our societal notions that men are stronger and tougher than women and better able to withstand physical discomfort. McCaffery and Ferrell explained this seeming contradiction by speculating that while society attributes strength and bravery to men, these characteristics are dis- played by an unwillingness to complain or express discomfort rather than by an actual tolerance of discomfort.
Other researchers offer alternative explanations for this perceived difference in tolerance. Some have asserted that as a result of women’s biological role in childbirth, women are capable of withstanding significantly more pain than men.84
Fillingim and Maixner postulate that the sum of men’s and women’s differences in pain response exist as a consequence of evolutionary pressures that increase reproductive potential and species survival.85 In her study of the interplay of pain, gender, and culture, Bendelow found that women were frequently thought to be equipped with a “natural capacity to endure pain,” in part linked to their reproductive functioning.86 This attitude does appear to be somewhat common among certain groups, as conveyed by offhand remarks such as, “if men had to bear children, there wouldn’t be any.”87
Bendelow found that “the perceived superiority of capacities of endurance is double-edged for women — the assumption that they may be able to ‘cope’ better may lead to the expectation that they can put up with more pain, that their pain does not need to be taken so seriously.”88 Crook and Tunks point to the influence of the psychoprophylaxis movement in the United States with its implicit assumption that it is good to experience childbirth without the aid of analgesia. As a result, some women who have “gone through psychoprophylaxis classes, feel guilty if they relent at the last minute and ask for an epidural”; according to the authors, “these attitudes imply that we have a value system endorsed by some parts of our population that suggest women should be encouraged to keep a stiff upper lip.”89
Another possible explanation of why health-care providers view women as better able to tolerate pain and thus in need of less treatment is that women have better coping mechanisms than men for dealing with pain. The literature confirms that women in fact have a greater repertoire of coping skills to deal with their pain. These include a greater ability to verbally acknowledge and describe their pain, to seek health-care intervention, and to gain emotional support. Men, in contrast, are likely to ignore the pain or delay seeking treatment.90 Yet this reluctance on the part of men does not lead to the conclusion that women, as not reluctant, must therefore be less in need of adequate treatment. Rather, a request for medical care would seem to imply that the person perceives her pain as real and enough of a threat to her lifestyle to seek outside assistance.
What men’s reluctance says — if anything at all — is that they are perhaps, as a whole, more undertreated than we think. While their complaints of pain appear to be taken more seriously than women’s pain complaints when they initially enter the health-care system, many may not seek medical assistance for their pain and, as a result, may be disadvantaged in getting relief from their painful symptoms.
A third possible explanation of why health-care providers might view men as less tolerant of pain than women may be a projection that men need more assistance with their pain because they are the household breadwinners. In their study, McCaffery and Ferrell found that nurses tended to equate “day-to-day physical functioning with pain tolerance” and that nurses believed men were more likely to stop functioning when they were in pain whereas women would continue their role as homemaker in addition to working outside the home. Another study similarly found that men were “more likely to be referred earlier for active treatment with a combination of therapies because of the demands of their bread- winner roles.”91 Again, such reasoning is unfounded. Unruh argued that women may, in fact, more readily attend to pain and more aggressively manage it because they assume more role responsibilities than men.92 As a result, they “may have more complex concerns about managing the interference of pain in the activities and responsibilities of daily life.” Given this possibility, it would again make more sense for health-care providers to at least be as aggressive in treating women for pain as they are in treating men.
Another factor that may play a key role in explaining the different treatment of men and women for pain and the tendency to treat women less aggressively is the subjective nature of pain and the credibility given to women’s self-reports of pain. These two factors perhaps exacerbate the likely undertreatment of women for pain.
Western medicine discounts female pain expression
In Western medicine, health-care providers are trained to rely predominantly on objective evidence of disease and injury. This is not only true of physicians but also nurses. One study of nurses found that they incorrectly expect patients who report moderate to severe pain to have elevated vital signs or behavioral expressions of pain.93 The medical model overemphasizes objective, biological indicators of pain and underacknowledges women’s subjective, experiential reports. Johansson and colleagues state, “medical models often end up in reductionism and medico-centrism, since they look for expert explanations in biological facts.”94 They cite a study by Baszanger which revealed that physicians attempting to make a diagnosis after consulting with a patient considered “cellular pathology as ‘something,’ whereas illness-provoking, psycho-social circumstances were ‘nothing.’”95
The subjective nature of pain requires health-care providers to view the patient as a credible reporter, and stereo- types or assumptions about behavior in such circumstances (oversensitivity, complaining, stoicism) add to the likelihood of undertreatment of some groups and overtreatment of others.96 The feminist literature is rife with examples and criticism of women’s voices not being heard or considered credible in the male-dominated health-care system. Sherwin de- scribes physicians as frequently “patronizing, detached, disrespectful, ... and unwilling to trust the reports of their women patients.”97 Dresser, in characterizing the literature on women’s health care, finds that women’s “[s]ubjective experiences of illness and treatment are frequently ignored.”98
A deeper examination of why women are treated this way is explored by several feminist authors. They attribute it to a long history within our culture of regarding women’s reasoning capacity as limited99 and of viewing women’s opinions as “unreflective, emotional, or immature.”100 In particular, in relation to medical decision-making, women’s moral identity is “often not recognized.”101 In a recent article, Parks argued that women’s requests for physician assisted suicide (PAS) are likely to be ignored. Parks reasoned that while a man’s request for help in ending his life is likely to be considered a “rational self-evaluation” if marked by “intolerable pain, personal suffering or terminal illness, ... women’s similar experiences are much more likely to be rejected, discounted, or unheeded because their capacity for such determinations of personal suffering are questioned.”102
Evidence of health-care providers’ doubting the pain experience of women with chronic pain is provided by Grace. She found that women with pelvic pain expressed difficulty communicating with their general practitioner about their pain, and some difficulty communicating with their gynecologist.103 A significant number of the women “did not think the doctor (GP) really understood what they said and left the doctor’s office feeling that there were things about their pelvic pain that they hadn’t talked about.”104 These women had received seventy-three different diagnoses to explain the cause of their pain, and reported that their physician implied “nothing was wrong” if no physical cause of pain could be identified.105 More than half of the women said that on occasion they felt that the doctor was not taking their pain seriously or that the doctor expected them to put up with their pain.
Women are also portrayed as hysterical or emotional in much of the medical and other literature. While men may be seen as forceful or aggressive, women are perceived as hysterical for the same behavior.106 Physicians have found women to have more “psychosomatic illnesses, more emotional lability and more complaints due to emotional factors” than men.107 In a frequently cited paper by Engel, “the majority of the case histories presented to illustrate ‘psychogenic pain and the pain prone patient’ are histories of females.”108 Fishbain and colleagues found that female chronic pain patients were more likely to be diagnosed with histrionic disorder (excessive emotionality and attention-seeking behavior) compared to male chronic pain patients.
Some researchers have argued that a “bias toward psychogenic causation for disorders in women has occurred even in well defined painful biological processes: ‘Despite the well documented presence of organic etiologic factors, the therapeutic literature is characterized by an unscientific recourse to psychogenesis and a correspondingly inadequate, even derisive approach to their management.’”109 These findings are consistent with studies reporting that female pain patients are less likely than their male counterparts to be taken seriously or are more likely to receive sedatives than opioids for the treatment of their pain.
The health-care provider’s bias toward psychogenic causes of women’s pain is problematic on two levels. First, women are more likely than men to have their pain attributed to psychogenesis whether or not that is in fact a cause of their pain. Second, for those women whose pain is exacerbated by emotional disorders, the health-care provider’s bias against psychological contributors to pain may lead them to undertreat the pain. Some claim that health-care providers’ predisposition toward attributing women’s pain to emotional causes is related to the higher prevalence of emotional problems (e.g., depression and anxiety) among women.110 However, it is possible that a gender bias exists in the processes by which women are evaluated for and diagnosed with these psychological disorders. What is clear is that women are more likely than men to express their feelings and more likely than men to have their symptoms (including pain) attributed to emotional factors. What is unknown is the degree to which emotional factors actually contribute to women’s and men’s pain experiences.
The tendency of health-care providers to discredit women’s pain reports may, in part, be rooted in communication differences between men and women. Vallerand argues that “[b]ecause pain is a subjective phenomenon that can be assessed most reliably from the patient’s self-report, the ability to communicate the discomfort of pain to a HCP [health- care provider] should be an advantage.” In contrast, it appears that “women’s ability to verbalize their emotions causes their responses to be viewed with suspicion [e.g., considered psychologically based] and treated less aggressively.”111 Alternatively, women’s style of communication may simply not fit neatly into the traditional medical interview model adopted by most physicians. In this model, Smith writes:
[the] physician controls the entry and exit of topics and controls the time devoted to a certain topic. By interrogative speech acts, ... the physician also controls the introduction and timing of topics. Through interruptions, the physician allows or cuts off patient lines of questioning. Several studies have shown that the physician-led medical interview is confined mainly to the question-and-answer mode of speech and that patient-initiated questions are often “dispreferred” in medical interviews.112
In general, women in Western societies are socialized to take turns in conversation, to downplay their own status, and to demonstrate behaviors that communicate more accessibility and friendliness.113 While both men and women might benefit from a more humanistic approach to physician-patient communication,114 it is likely that women are more likely to be disadvantaged by the traditional medical interview model. Women with chronic pain may be particularly vulnerable in this traditional communication style and re- buffed by physicians in their attempts to express the multiple ways in which their pain affects the quality of their lives and their ability to function.115
Lastly, patient characteristics and behaviors may also play a role in how female pain patients are perceived and, thus, how they are treated by their physicians. To the extent that women are culturally influenced to try to look good, even on visits to their physician, they may be viewed by their physician as attractive and thus not really in pain.116 Alternatively, if female patients present with hostility, they may not receive appropriate treatment. Patient hostility has been reported as an obstacle to establishing a rapport with a healthcare provider. A few studies have indicated a correlation between female pain patients and high levels of hostility.117 Such hostility, however, may be the result of frustration with the medical system and difficulty finding a sympathetic health-care provider. There is evidence that chronic pain patients must see dozens of physicians before finding one that is willing and/or able to treat their pain.118
Summary, Implications, and Recommendations
The research findings point to several troubling inconsistencies or paradoxes regarding the differences between men and women in pain response and treatment:
While women have a higher prevalence of chronic pain syndromes and diseases associated with chronic pain than men, and women are biologically more sensitive to pain than men and respond differently to certain analgesics, women’s pain reports are taken less seriously than men’s, and women receive less aggressive treatment than men for their pain.
Although women have more coping mechanisms to deal with pain, this may contribute to a general perception that they can put up with more pain and that their pain does not need to be taken as seriously.
Although women more frequently report pain to a health-care provider, they are more likely to have their pain reports discounted as “emotional” or “psychogenic” and, therefore, “not real.”
Women, being socialized to attend more to their physical appearance, are more likely than men to have health-care providers assume they are not in pain if they look more physically attractive.
Men with chronic pain are more likely to delay seeking treatment, but generally receive a more aggressive response by health-care providers once they enter the health-care system.
Both men and women are more likely to have the emotional or psychological component of their pain experience suppressed due to Western medicine’s tendency to separate mind and body and to view objective, biological “facts” as more credible than subjective feelings.
If one examines these findings from different ethical perspectives, they are deeply problematic. From a justice perspective, for example, there exists a strong argument that individuals should be treated equally effectively according to their needs. Thus, a just approach to providing sex-specific, gender-sensitive pain management treatments acknowledges that men and women in pain may have different needs. The current situation, in which women are more likely than men to be undertreated for their pain, is ethically unjustifiable.
From a utilitarian perspective, undertreating women who have persistent pain is likely to have negative outcomes not only for productivity in the workforce but also for families and children. While undertreating men for pain has implications for their role as monetary providers, the implications of undertreating women are perhaps more far-reaching. In many families, the woman is now the breadwinner or one of the breadwinners.119 In addition, the woman typically takes on the primary role of family caretaker, making sure the household runs well, there is food on the table, and the children are cared for. If women are unable to function because of their pain, the possibility of extensive harm to families and children is very real.
The consequences for our health-care system are also potentially negative. A health-care system that continues to discriminate in its treatment of women is also likely to lose the confidence of its female patrons. There is, in fact, evidence that more women than men use alternative therapies for health-care treatment.120 While the loss of confidence in the conventional health-care system is a threat to its continued well-being, the elevated interest in complementary121 and holistic therapies may be a positive side effect of female patients’ dissatisfaction with the traditional medical system. The question of whether such therapies will be alternative or complementary to conventional medical therapies will be influenced by how conventional health-care providers respond to the demand for a more holistic approach to pain management.
From a perspective of narrative or care ethics, the fact that pain defies mind-body dichotomization and that women, in general, tend to adopt a more holistic approach to health and illness122 might provide justification for a female-specific approach to pain treatment — one that explores etiologies of pain without bias for or against biology, psychology, or other affective contributors, and one that acknowledges context and lived experiences.
Although the growth of holistic medicine may be one silver lining of conventional medicine’s gender-biased approach to pain treatment, this does not change the ethical imperative to rectify our mainstream health-care system’s unjust treatment of women with pain. It is necessary to begin educating health-care providers and those who train them to expose biases that lead to the undertreatment of women. Some research has shown that efforts at educating and enlightening health-care providers regarding women’s health needs has positive effects.123 Moreover, the bias against psychological or emotional pain contributors adversely affects both women and men. Women’s pain tends to be viewed as more emotionally based and thus less credible — or, likewise, less credible if indeed it is emotionally based.124 Men’s pain is more likely to be acknowledged strictly as a physical symptom, thus reinforcing the societal expectation that men suppress their emotions, even if it impedes their pain treatment and recovery.125 Medical schools must endorse, and teach students, an approach that best elicits the concerns of any patient in pain — an approach that does not discount the patient’s subjective reports of pain. This will require attentiveness to the emotional aspects of a patient’s reports of pain. As Johansson and colleagues state:
A purely diagnosis-oriented approach is not enough, and an attitude of healing through adaptation must be completed with a gender perspective on women’s actual circumstances. The medical encounter ought to provide possibilities for the patient to express psychosocial problems. Physicians must have a chance to listen, voice concern, discuss solutions and offer remedies such as counseling as well as medication to empower the patient.126
In addition to more attention to this issue in the medical school curriculum by modeling effective physician-patient communication with respect to pain management, there needs to be scrutiny on the part of quality care evaluators such as the Joint Commission on the Accreditation of Healthcare Organizations (JCAHO), as well as ethical awareness-raising by institutional ethics committees about the current bias in the pain treatment of women. Without this pressure, change is unlikely. The fact that JCAHO has established new pain management standards for the institutions that they accredit is a step in the right direction.127 Perhaps inclusion of evaluative mechanisms to ensure that vulnerable populations are not undertreated for pain due to a health-care provider’s gender, ethnic, age, or racial biases will contribute to a more just approach to pain management. In addition to JCAHO’s regulatory approach, institutional ethics committees have a role in educating and enlightening health-care providers regarding unjust pain treatment. Indeed, future JCAHO standards that address organizational ethics may dovetail into the same arena.
Conclusion
Research indicates that differences between men and women exist in the experience of pain, with women experiencing and reporting both more frequent and greater pain. Yet rather than receiving greater or at least as effective treatment for their pain as men, women are more likely to be less well treated than men for their painful symptoms. There are numerous factors that contribute to this undertreatment, but the literature supports the conclusion that there are gender-based biases regarding women’s pain experiences. These biases have led health-care providers to discount women’s self-reports of pain at least until there is objective evidence for the pain’s cause. Medicine’s focus on objective factors and its cultural stereotypes of women combine insidiously, leaving women at greater risk for inadequate pain relief and continued suffering. Greater awareness among health-care providers of this injustice, a readjustment of medicine’s preoccupation with objective factors through education about alternative approaches, and scrutiny by quality and ethical reviewers within health-care institutions are necessary to change health-care providers’ behavior and ensure that women’s voices regarding treatment of their pain are heard.
References
1. See R. Payne, “Practice Guidelines for Cancer Pain Treatment: Issues Pertinent to the Revision of National Guidelines,” Oncology, 12, no. 11A (1998): 169–75; M. McCaffery, “Pain Control: Barriers to the Use of Available Information,” Cancer, 70, no. 5 (supplement) (1992): 1438–49; R. Bernabei et al., “Managing Pain in Elderly Patients with Cancer,” JAMA, 279, no. 23 (1998): 1877–82. See also P. Wall and M. Jones, Defeating Pain, The War Against a Silent Epidemic (New York: Plenum, 1991).
2. See K.L. Calderone, “The Influence of Gender on the Frequency of Pain and Sedative Medication Administered to Postoperative Patients,” Sex Roles, 23 (1990):11–12, 713–25.
3. See P.L. Walker and D.C. Cook, “Brief Communication: Gender and Sex: Vive la Difference,” American Journal of Physical Anthropology, 106, no. 2 (1998): 255–59, who underscore maintaining the distinction between “sex” (the anatomical or chromosomal categories of male and female) and “gender” (socially constructed roles that are related to sex distinctions). It should be noted that while isolating the influence of sex and gender on pain response and treatment is the focus of this article, we do not mean to dismiss the powerful influence of class, race, culture, education, and other such variables that likely affect pain response and treatment.
4. See S.J. Blumenthal and S.F. Wood, “Women’s Health Care: Federal Initiatives, Policies, and Directions,” in S. Gallant and G.P. Keita, eds., Health Care for Women: Psychological, Social & Behavioral Influences (Washington, D.C.: American Psychological Association, 1997): 57–71.
5. See National Institutes of Health Revitalization Act of 1993, Pub. L. No. 103-43, 107 Stat. 22 (June 10, 1993).
6. A.M. Unruh, “Gender Variations in Clinical Pain Experience,” Pain, 65 (1996): 123–67.
7. See K.J. Berkley, “Sex Differences in Pain,” Behavioral & Brain Sciences, 20, no. 3 (1997): 371–80.
8. See R.B. Fillingim and W. Maixner, “Gender Differences in the Responses to Noxious Stimuli,” Pain Forum, 4, no. 4 (1995), 209–21.
9. Id. at 209.
10. A.M. Unruh, “Why Can’t a Woman Be More Like a Man?,” Behavioral & Brain Sciences, 20, no. 3 (1997): at 467.
11. See T.D. Carr, K.L. Lemanek, and F.D. Armstrong, “Pain and Fear Ratings: Clinical Implications of Age and Gender Differences,” Journal of Pain and Symptom Management, 15, no. 5 (1998): 305–13; B.S. Krogstad, A. Jokstad, and O. Vassend, “The Reporting of Pain, Somatic Complaints, and Anxiety in a Group of Patients with TMD Before and 2 Years After Treatment. Sex Differences,” Journal of Orofacial Pain, 10, no. 3 (1996): 263– 69; O. Plesh et al., “Gender Difference in Jaw Pain by Clench- ing,” Journal of Oral Rehabilitation, 25, no. 4 (1998): 258–63 (corroborating that women have a higher incidence than men of temporomandibular pain). See also C.R. France and S. Suchowiecki, “A Comparison of Diffuse Noxious Inhibitory Controls in Men and Women,” Pain, 81, no. 1–2 (1999): 77–84 (finding that women exhibited significantly lower pain thresh- olds than men and reported significantly greater pain in response to both ischemia and electrocutaneous noxious stimulation).
12. See Berkley, supra note 7.
13. Id.
14. Id.
15. See M.A. Giamberardino et al., “Pain Threshold Variations in Somatic Wall Tissues as a Function of Menstrual Cycle, Segmental Site and Tissue Depth in Non-Dysmenorrheic Women, Dysmenorrheic Women and Men,” Pain, 71 (1997): 187–97.
16. SeeR.B.Fillingimetal.,“IschemicButNotThermalPain Sensitivity Varies Across the Menstrual Cycle,” Psychosomatic Medicine, 59 (1997): 512–20.
17. See A.G. Glaros, L. Baharloo, and E.G. Glass, “Effect of Parafunctional Clenching and Estrogen on Temporomandibular Disorder Pain,” Journal of Craniomandibular Practice, 16, no. 2 (1998): 78–83.
18. See T.T. Dao, K. Knight, and V. Ton-That, “Modulation of Myofascial Pain by the Reproductive Hormones: A Preliminary Report,” The Journal of Prosthetic Dentistry, 79 (1998): 663– 70.
19. Id. at 667.
20. Id.
21. See B.S. McEwen, S.E. Alves, K. Bulloch, and N.G. Weiland, “Clinically Relevant Basic Science Studies of Gender Differences and Sex Hormone Effects,” Psychopharmacology Bulletin, 34, no. 3 (1998), 251–59, in which the authors present a review of studies depicting the array of neurochemical and structural effects of ovarian hormones, including their influence on cognitive function and pain sensitivity. Female rats showed less opioid-mediated stress-induced analgesia than male rats when exposed to a variety of stressors, and male rats demonstrated greater swim stress analgesia and less predator-evoked analgesia than females.
22. See J. S. Mogil et al., “Identification of a Sex-Specific Quantitative Trait Locus Mediating Nonopioid Stress-Induced Analgesia in Female Mice,” The Journal of Neuroscience, 17, no. 20 (1997): 7995–8002.
23. Fillingim and Maixner, supra note 8, at 214.
24. See A.M. Aloisi, M. Zimmermann, and T. Herdegen, “Sex-Dependent Effects of Formalin and Restraint on c-Fos Expression in the Septum and Hippocampus of the Rat,” Neuroscience, 81, no. 4 (1997): 951–958. See also A.M. Aloisi, “Sex Differences in Pain-Induced Effects on the Septo-Hippocampal System,” Brain Research Reviews, 25, no. 3 (1997): 397–406.
25. See E.A. Mayer et al., “Review Article: Gender-Related Differences in Functional Gastrointestinal Disorders,” Alimentary Pharmacology & Therapeutics, 13, no. 2 (supplement) (1999): 65–69.
26. See P.E. Paulson et al., “Gender Differences in Pain Perception and Patterns of Cerebral Activation During Noxious Heat Stimulation in Humans,” Pain, 76 (1998), 223–29.
27. Berkley, supra note 7.
28. Berkley, supra note 7.
29. Unruh, supra note 6.
30. See G.J. De Vries and P.A. Boyle, “Double Duty for Sex Differences in the Brain,” Behavioral & Brain Sciences, 92, no. 2 (1998): 205–13.
31. One difficulty in interpreting evidence from research studies is the individual variability of the pain response. Greater variability makes research on pain responses more difficult, as it decreases power and thus increases the likelihood of having in- significant results due to an insufficient number of subjects studied. This has been recently corroborated in a meta-analysis by Riley and colleagues, who determined that only seven of thirty-four studies reviewed on gender differences in pain response had adequate sample sizes. This implies that gender differences have been underestimated rather than overestimated in pain research. See J.L. Riley III et al., “Sex Differences in the Perception of Noxious Experimental Stimuli: A Meta-Analysis,” Pain, 74 (1998): 181–87.
32. G. Bendelow, Pain and Gender (New York: Prentice Hall, 2000): at 17, citing V. Neisser, Cognition and Reality (San Francisco: Freeman, 1976): at 214.
33. Duncan describes how Cartesian (i.e., Descartes’) mind-body dualism is inaccurately equated with medical reductionism, the latter of which tends to dismiss mind (psychology) and favor body (physiology) in the diagnostic encounter. See G. Duncan, “Mind-Body Dualism and the Biopsychosocial Model of Pain: What Did Descartes Really Say?,” Journal of Medicine and Philosophy, 25, no. 4 (2000): 485–513. A more holistic approach is supported somewhat by Melzack and Wall’s gate-control theory of pain, in which a neural mechanism in the spinal cord is thought to function like a gate to control the flow of nerve impulses into the central nervous system. Whether sensory transmission is in- creased or decreased (causing, respectively, a greater or lesser pain intensity perception) is influenced by cognitive and emotional input such as anxiety, mood state, attention, and past experiences. Bendelow and Williams state that the gate-control theory “signals the end of the mind/body split with regard to pain.” However, these authors acknowledge that currently “the biological remains dominant over the social.” Indeed, Duncan points out that the contemporary biopsychosocial model of pain does not entirely escape mind-body dualism. See also R. Melzack and P. Wall, The Challenge of Pain (Harmondsworth, England: Penguin, 1988); G.A. Bendelow and S.J. Williams, “Transcending the Dualisms: Towards a Sociology of Pain,” Sociology of Health and Illness, 17, no. 2 (1995): 139–65, at 143.
34. Unruh, supra note 6, at 157.
35. See R.S. Lazarus and S. Folkman, Stress, Appraisal, and Coping (New York: Springer, 1984), as cited in A. O’Leary and V.S. Helgeson, “Psychosocial Factors and Women’s Health: Integrating Mind, Heart, and Body,” in S.J. Gallant, G.P. Keita, and R. Royak-Shaler, eds., Health Care for Women: Psychological, Social and Behavioral Influences (Washington, D.C.: American Psychological Association, 1997): 25–71.
36. Unruh, supra note 6.
37. Id. at 158.
38. R. Weir et al., “Gender Differences in Psychosocial Adjustment to Chronic Pain and Expenditures for Health Care Services Used,” The Clinical Journal of Pain, 12 (1996): 277–90, at 287.
39. Unruh, supra note 6, at 149, citing L. Astor-Dubin and C. Hammen, “Cognitive Versus Behavioral Coping Response of Men and Women: A Brief Report,” Cognitive Research Therapy, 8 (1984): 85–90; C. Brehms and M.E. Johnson, “Problem-Solving Appraisal and Coping Style: The Influence of Sex-Role Orientation and Gender,” The Journal of Psychology, 123 (1989): 187– 94; J.E. Holm et al., “The Role of Stress in Recurrent Tension Headache,” Headache, 26 (1986): 160–67; A.A. Stone and J.M. Neale, “New Measure of Daily Coping: Development and Prliminary Results,” Journal of Personality & Social Psychology, 46 (1984): 892–906; L.M. Verbrugge, “Sex Differences in Com- plaints and Diagnoses,” Journal of Behavioral Medicine, 3 (1980): 327–55; A.J.J.M. Vingerhoets and G.L. Van Heck, “Gender, Coping and Psychosomatic Symptoms,” Psychological Medicine, 20 (1990): 125–35.
40. P.A. Thoits, “Gender Differences in Coping with Emo-ional Distress,” in J. Eckenrode, ed., The Social Context of Coping (New York: Plenum, 1991): 107–38, as cited in O’Leary and Helgeson, supra note 35, at 30.
41. See A.M. Unruh, J. Ritchie, and H. Merskey, “Does Gender Affect Appraisal of Pain and Pain Coping Strategies?,” The Clinical Journal of Pain, 15, no. 1 (1999), 31–40.
42. See I. Jensen et al., “Coping with Long-Term Musculosk- eletal Pain and Its Consequence: Is Gender a Factor?,” Pain, 57 (1994): 167–72.
43. Unruh, supra note 6, at 149. See also S.P. Buckelew et al., “Health Locus of Control, Gender Differences and Adjustment to Persistent Pain,” Pain, 42 (1990): 287–94; F.J. Keefe et al., “Analyzing Pain in Rheumatoid Arthritis Patients,” Pain, 46 (1991): 153–60; and J. Strong, R. Ashton, and A. Stewart, “Chronic Low Back Pain: Towards an Integrated Psychosocial Assessment Model,” Clinical Psychology, 69 (1994), 1058–63.
44. O’Leary and Helgeson, supra note 35; Unruh, supra note 6; Weir et al., supra note 38. There is some evidence, however, that health-care utilization rates do not differ among elderly men and women and that older females tend to report lower levels of health-care utilization than older males. See K. Hunt et al., “Are Women More Ready to Consult Than Men? Gender Differences in Family Practitioner Consultation for Common Chronic Conditions,” Journal of Health Services and Research Policy, 4, no. 2 (1999), 96–100. See also J.L. Riley, G.H. Gilbert, and M.W. Heft, “Orofacial Pain Symptom Prevalence: Selective Sex Differences in the Elderly?,” Pain, 76, no. 1–2 (1998), 97–104.
45. Miaskowski reports that women report more visits to health-care providers on retrospective assessment, but on prospective studies, men and women seek health care at the same rate. Researchers have attributed this difference to the possibility that men are more reluctant than women to admit visiting health- care providers or less likely to remember such visits. See C. Miaskowski, “The Role of Sex and Gender in Pain Perception and Responses to Treatment,” in R.J. Gatchel and D.C. Turk, eds., Psychosocial Factors in Pain: Critical Perspectives (New York: The Guildford Press, 1999): 401–11, at 406. In one prospective study, E. Berkanovic, C. Telesky, and S. Reeder found that perceived efficacy of health care, perceived seriousness of one’s symptom, and reported disability from that symptom were more highly correlated with health-care utilization than was gender, although older women were found to have accessed a physician more than men. “Structural and Social Psychological Factors in the Decision to Seek Medical Care for Symptoms,” Medical Care, XIX, no. 7 (1981): 693–709.
46. Bendelow, supra note 32. See also G. Bendelow, “Pain Perceptions, Emotions and Gender,” Sociology of Health and Illness, 15 (1993): 273–94; W. Pollack, Real Boys: Rescuing Our Sons from the Myths of Boyhood (New York: Henry Holt & Co., 1998).
47. Pollack, supra note 46, at 11.
48. Miaskowski, supra note 45, at 404.
49. See F.M. Levine and L.L. De Simone, “The Effects of Experimenter Gender on Pain Report in Male and Female Subjects,” Pain, 44 (1991): 69–72.
50. See D.J. Davidson and W.R. Freudenburg, “Gender and Environmental Risk Concerns: A Review and Analysis of Available Research,” Environment and Behavior, 28, no. 3 (1996): 302–39.
51. Women have been found to be more other-directed in conversation and to frequently seek support and validation in their communication encounters. Men have been found to be more goal-directed and status-conscious in communication and to give advice more often. See D. Tannen, You Just Don’t Under- stand: Women and Men in Conversation (New York: Ballantine, 1990).
52. C. Miaskowski, “Women and Pain,” Critical Care Nursing Clinics of North America, 9, no. 4 (1997): at 467.
53. Unruh et al., supra note 41. See also Bendelow, supra note 32.
54. Miaskowski, supra note 45.
55. See B.S. Faherty and M.R. Grier, “Analgesic Medication for Elderly People Post-Surgery,” Nursing Research, 33, no. 6 (1984): 369–72.
56. Calderone, supra note 2. Frequency of pain medication dosing was studied rather than the amount of analgesic being dosed since the latter is related to body weight and men might be administered higher doses based on body weight, not gender bias.
57. See J.E. Beyer et al., “Patterns of Postoperative Analgesic Use with Adults and Children Following Cardiac Surgery,” Pain, 17, no. 1 (1983), 71–81, as cited in Miaskowsi, supra note 45. Miaskowski cautions readers that most studies that have looked at gender differences in post-operative pain medication administration did not evaluate whether men and women received adequate amounts of analgesic medication. See Miaskowsi, supra notes 45 and 52.
58. See C.S. Cleeland et al., “Pain and Its Treatment in Outpatients with Metastatic Cancer,” N. Engl. J. Med., 330, no. 9 (1994): 592–96.
59. W. Breitbart et al., “The Undertreatment of Pain in Ambulatory AIDS Patients,” Pain, 65, no. 2 (1996), 243–49.
60. See D.D. McDonald, “Gender and Ethnic Stereotyping and Narcotic Analgesic Administration,” Research in Nursing and Health, 17 (1994): 45–49. McDonald, however, did not control for patient weight and thus could not rule out that men were given more narcotic analgesics based on greater body weight.
61. However, Raftery and colleagues found that female patients admitted to the emergency room reported more pain than males, were perceived by health-care providers to experience more pain, received more pain medications and more potent analgesics, and were less likely to receive no pain medications. Patient perception of pain and pain severity was the strongest predictor of number and strength of medications given for pain. The sex of the patient or health-care provider did not predict the number, type, and strength of medications received. Thus, health-care provider gender biases may fluctuate by geographical region or medical specialty. See K. A. Raftery, R. Smith-Coggins, and A.H. Chen, “Gender-Associated Differences in Emergency Department Pain Management,” Annals of Emergency Medicine, 26, no. 4 (1995): 414–21.
62. See V. Elderkin-Thompson and H. Waitzkin, “Differences in Clinical Communication by Gender,” Journal of General Inter- nal Medicine, 14 (1999): 112–21.
63. See P.A. Johnson, L. Golman, and E.J. Orav, “Gender Differences in the Management of Acute Chest Pain: Support for the ‘Yentl Syndrome,’” Journal of General Internal Medicine, 11 (1996): 209–17.
64. Weir et al., supra note 38. “Specialist” was not defined, and the possibility exists that some women were referred by a gynecologist who was considered a “specialist,” but served as the woman’s primary care provider.
65. See D.Z. Lack, “Women and Pain: Another Feminist Is- sue,” Women and Therapy, 1 (1982): 55–64, as cited in Unruh, supra note 6, at 159.
66. Elderkin-Thompson and Waitzkin, supra note 62. In addition, Crook and Tunks found that women with persistent pain were significantly more likely than men with persistent pain to receive psychotropic drugs from their family practitioner. See J. Crook and E. Tunks, “Women with Pain,” in E. Tunks, A. Bellissimo, and R. Roy, eds., Chronic Pain: Psychosocial Factors in Rehabilitation (Malabar, Florida: R.E. Krieger Publishing Company, 1990): 37–48.
67. See M. McCaffery and B.R. Ferrell, “Does the Gender Gap Affect Your Pain Control Decisions?,” Nursing, 22, no. 8 (1992): 48–51.
68. See D. McDonald and R.G. Bridge, “Gender Stereotyping and Nursing Care,” Research in Nursing and Health, 14 (1991): 373–78.
69. See T. Hadjistavropoulos, B. McMurty, and K.D. Craig, “Beautiful Faces in Pain: Biases and Accuracy in the Perception of Pain,” Psychology and Health, 11 (1996): 411–20.
70. Id. at 417. The hypothesis that stereotyping based on attractiveness may actually influence individuals’ pain responses (i.e., attractive individuals learn to actively cope better with pain and thus experience less pain intensity, and unattractive individuals learn more passive pain coping mechanisms and experience greater pain intensity) was considered.
71. See T. Hadjistavropoulos, H.D. Hadjistavropoulos, and K.D. Craig, “Appearance-Based Information about Coping with Pain: Valid or Biased?,” Social Science and Medicine, 40, no. 4 (1995): 537–43; H.D. Hadjistavropoulos, M. Ross, and C.L. von Baeyer, “Are Physicians’ Ratings of Pain Affected by Patients’ Physical Attractiveness?,” Social Science and Medicine, 31 (1990): 69– 72.
72. See S.M. Ebert, X. Liu, and R.L. Woosley, “Female Gender as a Risk Factor for Drug-Induced Cardiac Arrhythmias: Evaluation of Clinical and Experimental Evidence,” Journal of Women’s Health, 7, no. 5 (1998): 547–57. See also P.M. Thompson and J.L. Wolf, “The Sexual Revolution in Science: What Gender-Based Research Is Telling Us,” Journal of Investigative Medicine, 47, no. 3 (1999): 106–13.
73. See R.W. Gear et al., “Gender Difference in Analgesic Response to the Kappa-Opioid Pentazocine,” Neuroscience Letters, 205, no. 3 (1996): 207–09; R.W. Gear et al., “Kappa-Opioids Produce Significantly Greater Analgesia in Women Than in Men,” Nature Medicine, 2, no. 11 (1996): 1248–50. See also L.D. Jamner et al., “Pain Inhibition, Nicotine, and Gender,” Experimental and Clinical Psychopharmacology, 6, no. 1 (1998): 96–106 (finding that nicotine had a direct pain-inhibitory effect in men but not in women); M.E. Robinson et al., “Sex Differences in Response to Cutaneous Anesthesia: A Double Blind Randomized Study,” Pain, 77 (1998): 143–49 (finding that men responded differently from women to the pain inhibitory effects of a local anesthetic, e.g., locally anesthetized men rated a pressure stimulus as less painful than anesthetized women).
74. See J. Mogil, “Does He Feel Her Pain? Maybe Not,” University of Illinois Alumnae LAS Newsletter, Spring (1999): at 7.
75. Weir et al., supra note 38, at 278, stating that “several current hypotheses from the biological perspective are that pain perception is probably related to sensory factors rather than differences in attitudes or emotional responses, and that endogenous pain inhibition may be affected by hormonal variation.”
76. Although episodes of acute, severe pain will often be associated with an increase in heart rate or blood pressure, and increased heart rate is used in some studies (e.g., with infants) as a proxy measure of pain, others discourage clinicians from relyiing on these physiological measures as evidence of a patient’s pain. See M. McCaffery and B.R. Ferrell, “How Vital Are Vital Signs?,” Nursing, 22, no. 1 (1992): at 45 (“No firm clinical evidence exists to support the assumption that moderate to severe pain is always accompanied by a change in vital signs.”).
77. Unruh, supra note 39.
78. O’Leary and Helgeson, supra note 35; Unruh, supra note 6; Weir et al., supra note 38.
79. Unruh, supra note 6, at 159. See also P.P. Katz and L.A. Criswell, “Differences in Symptom Reports Between Men and Women with Rheumatoid Arthritis,” Arthritis Care & Research, 9, no. 6 (1996): 441–48.
80. Id. at 441.
81. Miaskowski, supra note 45, at 406.
82. McCaffery and Ferrell, supra note 67.
83. Bendelow, supra note 32, at 130. See also Nurofen, Pain Relief Study (London: Kings Fund, 1989), as cited in Bendelow, supra note 32, at 36.
84. See E.E. Johansson et al., “The Meanings of Pain: An Exploration of Women’s Descriptions of Symptoms,” Social Science and Medicine, 48, no. 12 (1999), 1791–1802.
85. Fillingim and Maixner, supra note 8.
86. Bendelow, “Pain Perceptions, Emotions, and Gender,” supra note 46, at 286.
87. Bendelow, supra note 32, at 53–55. 88. Id. at 115–16.
89. Crook and Tunks, supra note 66, at 38. 90. Unruh, supra note 39.
91. See L.M. Verbrugge, “Females and Illness: Recent Trends in Sex Differences in the United States,” Journal of Health and Social Behavior, 17 (1976): 387–403, as cited in Weir et al., supra note 38, at 288. Bendelow also describes how women’s more predominant involvement in the domestic sphere has associated them more with the “natural” world in the form of bodily functions, whereas men have been more involved in the “public world of work and therefore ‘higher’ cultural and mental processes.” The perception thus may exist that men’s “higher” functioning, if interrupted by the presence of pain, should receive a higher priority for medical intervention. See Bendelow, supra note 32, at 131.
92. N.L. Marshall states, “combining work and family has become the norm for women rather than the exception.” N.L. Marshall, “Combining Work and Family,” in S.J. Gallant, G.P. Keita, and R. Royak-Shaler, eds., Health Care for Women: Psycho- logical, Social and Behavioral Influences (Washington, D.C.: American Psychological Association, 1997): 163–74, at 163.
93. McCaffery and Ferrell, supra note 76.
94. Johansson et al., supra note 84, at 1792.
95. See I. Baszanger, “Deciphering Chronic Pain,” Sociology of Health and Illness, 14 (1992): 181–215, as cited in Johansson et al., supra note 84, at 1792.
96. Studies have found that the most significant predictor of inadequate pain relief is a discrepancy between the patient and physician regarding the severity of the patient’s pain. See Cleeland et al., supra note 58.
97. R. Dresser, “What Bioethics Can Learn from the Women’s Health Movement,” in S.M. Wolf, ed., Feminism & Bioethics (New York: Oxford University Press, 1996): 144–59, at 147, citing S. Sherwin, No Longer Patient: Feminist Ethics and Health Care (Philadelphia: Temple University Press, 1992): at 193.
98. Id. at 147.
99. J.A. Parks, “Why Gender Matters to the Euthanasia Debate: On Decisional Capacity and the Rejection of Women’s Death Requests,” The Hastings Center Report, 30, no. 1 (2000): 30–36, at 33.
100. S. H. Miles and A. August, “Courts, Gender and the ‘Right to Die,’” Journal of Law, Medicine & Health Care, 18 (1990): 85– 95.
101. Id.
102. Parks, supra note 99. See also K. H. Rothenberg,“Gender Matters: Implications for Clinical Research and Women’s Health Care,” Houston Law Review, 32, no. 5 (1996), 1201–72.
103. V.M. Grace, “Problems of Communication, Diagnosis, and Treatment Experienced by Women Using the New Zealand Health Services for Chronic Pelvic Pain: A Quantitative Analysis,” Health Care for Women International, 16 (1995): 521–35.
104. Id. at 525.
105. Id.
106. See Sherwin, supra note 97, at 48. See also J.F. Smith, “Communicative Ethics in Medicine: The Physician-Patient Relationship,” in S.M. Wolf, ed., Feminism & Bioethics (New York: Oxford University Press, 1996): 184–215, at 194 (“Women who do speak assertively are often taken to be domineering rather than dominant, emotional rather than rational, biased rather than authoritative, and complaining rather than assertive.”). Kate Nicholson, a disability lawyer who is writing a book about her experiences living with chronic neuropathic pain, and who commented on an earlier version of this manuscript, expressed concern that acknowledging gender differences in pain response might lead to gender stereotyping. She made a point of trying to report her pain to health-care providers factually and unemotionally, and recalled one female pain specialist’s comment to her, “You are not crazy; you’re not like my other patients.” Additionally, she recalled a male acquaintance’s adamant demand from emergency room staff to give him something for his acute pain (“You SOB’s, you are giving me something for pain and you’re giving it to me right now!”). He got the pain medication. Yet Nicholson was aware that if she had done something similar, “I’d have been perceived extremely differently, in all likelihood.”
107. See Unruh, supra note 6, at 158, summarizing the literature on this point.
108. See Crook and Tunks, supra note 66, at 37, citing G. Engel, “‘Psychogenic’ Pain and the Pain-Prone Patient,” American Journal of Medicine, 26 (1959): 899–918.
109. See K. J. Lennane and R. J. Lennane, “Alleged Psychogenic Disorders in Women — A Possible Manifestation of Sexual Prejudice,” N. Engl. J. Med., 288 (1973): 288–92, as cited in Unruh, supra note 6, at 158.
110. Women are four times as likely as men to be diagnosed with a major depression, and twice as likely as men to be diagnosed with a general depression, although rates vary with ethnicity and culture. Possible reasons for this may include that women are more willing to seek help and thus may be diagnosed more frequently; there may be biological differences that predispose women to developing depression (e.g., effects of reproductive hormones); or women may be more likely to suffer from depression due to external stressors (e.g., the effects of sexism, domestic violence, lower pay, and relationship stressors). See F.M. Culbertson, “Depression and Gender,” American Psychologist, 52, no. 1 (1997), 25–31. See also O’Leary and Helgeson, supra note 35. Also, female chronic pain patients are more likely than male chronic pain patients to be diagnosed with and treated for depression. See W.E. Haley, J.A. Turner, and J.M. Romano, “Depression in Chronic Pain Patients: Relation to Pain, Activity, and Sex Differences,” Pain, 23 (1985): 337–43.
111. See A.H. Vallerand, “Gender Differences in Pain,” Image: Journal of Nursing Scholarship, 27, no. 3 (1995): at 237.
112. Smith, supra note 106, at 190.
113. See D.L. Roter and J.A. Hall, “Gender Differences in Patient-Physician Communication,” in S.J. Gallant, G.P. Keita, and R. Royak-Shaler, eds., Health Care for Women: Psychological, Social & Behavioral influences (Washington, D.C.: American Psychological Association, (1997): 57–71.
114. Smith, supra note 106.
115. Female physicians, however, have been found to spend more time with patients, engage in more positive talk, ask more questions, and elicit more responses from patients. See Roter and Hall, supra note 113. See also J. Bensing, A. Van den Brink-Muinen, and D. de Bakker, “Differences Between Male and Female General Practitioners in the Care of Psychosocial Problems,” Medical Care, 31 (1993): 219–29.
116. Hadjistavropoulos, McMurtry, and Craig, supra note 69; Hadjistavropoulos, Hadjistavropoulos, and Craig, “Appearance-Based Information about Coping with Pain: Valid or Biased?,” supra note 71; Hadjistavropoulos, Ross, and von Baeyer, “Are Physicians’ Ratings of Pain Affected by Patients’ Physical Attractiveness?,” supra note 71.
117. See S.A. Selfe, Z. Matthews, and R.W. Stones, “Factors Influencing Outcome in Consultations for Chronic Pelvic Pain,” Journal of Women’s Health, 7, no. 8 (1998): 1041–48.
118. In a Connecticut focus-group study with chronic pain patients, participants reported visiting multiple physicians (quoting “60 to 100”) in order to find a diagnosis and a practitioner with whom they felt comfortable. See S. Grantham and M. Robbins, The Connecticut Pain Management Initiative: Focus Group Report (Boston: John Snow, Inc., February 11, 2000).
119. Marshall, supra note 92.
120. About 55 to 65 percent of those who consult complementary practitioners are women, the highest users being those aged 35 to 60. See C. Zollman and A. Vickers, “ABCs of Complementary Medicine: Users and Practitioners of Complementary Medicine,” British Medical Journal, 319, no. 7213 (1999): 836– 38; and E. Ernst, “Prevalence of Use of Complementary/Alternative Medicine: A Systematic Review,” Bulletin of the World Health Organization, 78, no. 2 (2000): 252–57.
121. Controversy over use of the term “alternative” rather than “complementary” medicine demonstrates the point being made here. The former describes therapies that are not sanctioned by conventional medicine and which patients choose instead of conventional medical therapy. The latter views such therapies as complementing conventional medical therapies. The goal would be for women (as well as men) to have access to both traditional and non-traditional therapies for pain management, with a focus on a holistic approach that provides optimal pain relief. This holistic approach is the accepted standard for many pain clinics and inpatient pain teams, but adequate access to such care is limited for many individuals — either because the pain teams and clinics are not available in their area or they do not get the referral they need.
122. Davidson and Freudenberg conclude that women in general, as a result of their socialization, are not as likely to develop a distinction between themselves as individuals and the world around them, whereas men are socialized to objectify and control their environment and to define themselves as separate from the world around them. Men would thus be more apt to try to separate biological and psychosocial pain etiologies, whereas women would tend to view them more holistically. See D.J. Davidson and W.R. Freudenburg, “Gender and Environmental Risk Concerns: A Review and Analysis of Available Research,” Environment and Behavior, 28, no. 3 (1996): 302–39. This theory is affirmed by Bendelow’s findings that women spoke of pain experiences more holistically as compared to men and that “men were significantly less inclined to think that the emotional component of pain perception had any importance.” See Bendelow, supra note 32, at 90.
123. See D.S. Kwolek et al., “Gender Differences in Clinical Evaluation: Narrowing the Gap with Women’s Health Clinical Skills Workshop,” Academic Medicine, 73, no. 10 (supplement) (1998): S88–90.
124. That is, women may: (1) have their pain complaints erroneously dismissed as being emotionally-based and therefore “not real” when there is no significant psychological component to the pain; (2) have the likely psychological components that accompany chronic pain be misidentified by health-care providers as the cause, rather than the result of their unrelieved pain, leading to a discounting of the pain; or (3) have the psychological problem that is the source of their pain be discounted and not adequately addressed. All three are inappropriate and reveal a disdain for psychosocial contributors to pain over evidence of organic causation. See Duncan, supra note 33.
125. Bendelow found that men who were given an opportunity to discuss the emotional aspects of their pain experiences did so and were grateful for the opportunity, even though they did not initially acknowledge emotions as contributing to their pain. See Bendelow, supra note 32, at 90–94.
126. Johansson et al., supra note 84, at 1800.
127. Some institutions have already begun addressing the impact of JCAHO pain management standards. See C. Pasero, M. McCaffery, and D.B. Gordon, “Build Institutional Commitment to Improving Pain Management,” Nursing Management, 30, no. 1 (1999): 27–33.
#pain#medicine#gender inequality#women#feminism#epistemology of pain#chronic pain#pain management#bias#gender bias#bias in medicine#communication#subjectivity#embodiment#healthcare#sexism#misogyny
1 note
·
View note
Text
[answered asks for the week]
INSIDE:
Hy! Can you pls give more examples how the types looks like as a child?
Is this related to a loop or inferior function?
When Enneagram 1 goes to 4, would that look like sensitivity to criticism, moodiness, brooding?
Could you compare enfp 4w3 and 4w5 ( both) so/sp?
i’m 90% sure that i’m an ISTJ, but sometimes i don’t feel that way.
Recently you said it might be difficult to determine enneagram type before mid thirties.
I haven’t been able to find any information on 1w2 ENFJ.
when we are teenagers we are developing our least favourite function right?
Hi. I was hoping you can help me. I figured out a pattern of mine that I would imagine is probably either a loop or my inferior function, because it is me when I am at my lowest point and am most unlike myself. I know what makes me fall into this pattern, now that I am older. However, whenever I fall into this pattern I have a hard time pinpointing what functions might be responsible for it.
I am usually an optimistic person. I am usually upbeat and can always turn a negative situation into a positive one by finding something positive about that particular situation, or something upcoming that I am really excited about. When someone is sad about a situation, I can explain why it’s not so bad and then get them to think optimistically. It is what makes me charming, bubbly and an overall good presence. It is rare when I fall into a slump, but when I do this optimism disappears completely. I get extremely negative minded. Like this morning, one of my closest friends told me “Why are you being so pessimistic?” And I know why. It is always the same story…
I really like having a simple lifestyle. By that, I do not mean I do not care about good food, company, and good stimuli to keep me excited. I am all about aesthetics. But what I mean is I rather make a modest living than work long hours, wasting life. I like to work minimal hours so I can enjoy this short life we have been given. I don’t like to take life seriously. I like to just live in the moment, day by day, and absorb the present. Every hour at its rawest form. But when my boss gives me ridiculous hours or I feel this time is taken away from me by obligations like even funerals or upcoming prayer events, I begin to flip out. It’s rare because I purposely chose a job that prioritizes hours for friends, family, and fun instead of work. But obligations happen and when they happen I can’t enjoy the moment anymore. I keep thinking of that obligation and how
But when I see these dates where I won’t have time for any of that sporadically appear in my calendar… every task becomes so tedious. I feel like every chore inside my house or outside of my house is ridiculous, including something so simple like vacuuming and I cannot live in the present like I want to. I keep living in that moment where I have to do this chore. I have to do this obligations. And then I get lost and everyone around me senses something different. They get pissed at me because I’m so damn negative.
I feel like if I can understand the functions responsible maybe I can direct myself to changing this pattern. Again. It’s so rare but when it happens, it’s really bad.
The bolded is high Se. You’re an SFP. Given your obvious Enneagram 7 core type (the need to be free of obligation and able to do whatever you want / live in the moment and be spontaneous – feeling trapped when too much closes in on you) I’m guessing you’re an ESFP, and these “I feel trapped and no longer able to enjoy the moment” days are Ni-gripping (unable to think in the present, just ahead to things you are not looking forward to).
You can counter this by one of two ways, or both:
1) Doing something at the end of the day that brings you back into Se. Something aesthetic that returns you to THE PRESENT. It might be Yoga. It might be a back rub. It might be laying in the tub for two hours and reading a book by candlelight. Something sensory. Something NOW.
2) Have something to look forward to on the other side of your obligations, so you are not thinking about the days you have to do things, but that fun thing you get to do on the weekend. It may be something you planned, or the decision to live in the moment on that day and be impulsive all day long. But 7′s need fun things to look forward to, when they have a lot of “commitment”-related things sucking up their energy. So, look ahead in a positive way and not just a negative one. :)
When enneagram one goes to four would that look like sensitivity to criticism, moodiness, brooding? I know a few people like that who are normally pretty immune to taking things to personally but at times can seem quite sensitive. They also have the best sense of humor and are playful at their best. Thanks
Yes.
The important thing to remember with disintegration is that the person has all the negative attributes of the number they are moving into, but none of the positive ones. So a 1 moving to 4 is melodramatic, woe is me, nobody understands me, nobody appreciates me, I’m all alone and unloved, nobody loves me, fuss, fuss, fuss… with none of 4′s authenticity, seek for deep internal meaning, or ability to understand and process intense emotions on a deep level.
Moving into integration would also mean taking on the positive attributes of 7 without the negative ones – so the 1 would become more happy, playful, and optimistic, seeing the best in people instead of what needs fixed.
Could you compare enfp 4w3 and 4w5 ( both) so/sp?
Ignore your MBTI type and just focus on what 3 and 5 bring to the 4, and how that would change it.
3 is extroverted, wants to win, has confidence in their look, is centered around success.
5 is introverted, fearful of getting things wrong by acting too prematurely, protects self by falling into knowledge, tends to fantasize.
4w3 therefore is more outgoing, flamboyant, bigger with their feelings, more dramatic, and yet cares more how people see them because of the 3. They often are fashionable and image-conscious – because the “is this authentic to me” 4 is being pulled at by the “but do I make an amazing impression” 3 wing.
4w5 is more introverted and more inclined to intellectualize their feelings, more secretive about everything (because 5 is a little fearful of how you may use things against it if you know too much), doesn’t care nearly as much how other people respond to them in terms of their overall presentation.
Since 3 is optimistic and ‘can’ do, it makes for a lighter, more colorful 4 – optimistic about the future and able to carve a niche out or trend-set. 5 brings a level of internal focus to a 4 and often becomes ‘dramatic’ or ‘withdrawn’ – there’s more of an emphasis on morbidity whenever a 5 is involved.
hi! i was wondering if you could help me with my type. i’m 90% sure that i’m an ISTJ, but sometimes i don’t feel that way. i feel that ISTJs are often depicted as cold or unfeeling, but i am definitely a kind person - generally to everyone, and especially to those i love. i can get into a “Te mode” but it isn’t constant. but i’m definitely not Fe, and i make decisions based on logic. and of course mbti can’t show my entire personality, so could enneagram could provide clarification? thanks!
My father once told me that you can’t take everything at face value, you have to look at where someone is coming from. So, if there are somewhat cold and inaccurate depictions of ISTJs in fiction, what does that tell you about the writer? They are not an ISTJ. Most likely they are an IXFP or a high Fe user, who does not understand how TeFi works, so they wind up with a stereotype of what their own low Te would be like higher in the stack (inaccurate, because healthy high Te is instinctively professional and knows how to work with people) or they think about people they have clashed with and use them for inspiration.
That aside, most ISTJs are not cold or unfeeling. They care very deeply – they just do not waltz around with their feelings on full display and feel no need to draw excessive attention to them. They show their love through Te ways – often doing kind things for others rather than gushing. Any type can be kind and I know a fair few thinkers in general who are kind, gentle, and accommodating. But their brains still process information through their specific cognitive stack, making them thinkers.
It is possible that you have a compliant Enneagram tritype, yes. A 9 or a 2 or a 6 or all three would make you a much softer and warmer ISTJ than an ISTJ with a “cold” Enneagram tritype.
Recently you said it might be difficult to determine enneagram type before mid thirties. I am curious how long we take to develop a type of that’s how it works. I could see a type 9 develop when their efforts to deal with issues are blown off. Over time they may avoid conflict? Is that possible?
It’s not that as a child, you lack an Enneagram type, but that at 35 you have enough life experience to look back on your accumulated mistakes and see what it is that you are truly afraid of or running away from. Your defense mechanisms. The younger a person is, the more arrogant they tend to be. It’s life that kicks you between the teeth and teaches you things. Like, no matter how good you are, there’s always someone better than you. Or that you can’t keep running away from your problems and expect things not to catch up to you. Or that sooner or later, you have to leave your comfort zone and get a job. Or that “perfection” does not exist. By 35, hopefully you will have gained some perspective and enough humility not to sugarcoat your flaws. That’s Richard Rohr’s reasoning – take it or leave it, it’s up to you.
There’s theories about how you develop your core type based on your parents and how you felt and what you dealt with as a child. I’m not sure whether to believe that as true or not – often, for example, the 6 profiles talk about the child growing up in an unsafe environment and an unstable home. I had a safe home, never experienced anything traumatic, and excellent parents who never fought. I never felt threatened. I just inexplicably developed 6 traits. But I could also flip it around and say that I was so dependent on my loving and generous parents that the outside world became an intimidating, dangerous place.
They say that 9′s develop in a volatile environment where they have to ignore an abusive parent in order to cope – but out of all the 9′s I know (and I know at least 5 in real life), that’s true for only one of them. One 9 I know developed in a house without much strife at all. She just decided to be in her own little world.
I suspect like all things, it’s a combination of preferred tendencies and possibly the environment. Like a little 9 child being happy and sweet and wanting to see everything with a rosy glow and then when faced with the harsh realities of life in the real world – choosing to stick with that happy, sweet place, because it’s much nicer than the cold truth. Or the little 1 child feeling better when her room is organized, like that’s something she can control in her world. Or the 2 being instinctively helpful and generous. Etc.
In short, I don’t think anybody knows where or why these things develop. There’s no actual proof Enneagram exists. It’s just a theory that we treat as the truth, because human beings want to know why people are not all the same, so they look for patterns and explanations… and this seems as valid as any other. ;)
I haven’t been able to find any information on 1w2 ENFJ. Would you be willing to explain how they might differ from the bubbly ENFJ stereotype we often hear about? Thanks!!
It’s the ESFJs (and the ESFJs mistyped as ENFPs ;) that bring a bubbliness to Fe-doms – Ni being a very straightforward, “colder” function (paired with Se) does not lend itself to Ne-ish enthusiasm. It’s more serious and driven (Obama, Neil deGrasse Tyson, etc).
That being said, an ENFJ 1w2 would develop narrow, specific idealistic beliefs about how to improve the world and set about determined to make those visions a reality. They would not shy away from conflict but be assertive in expressing their views (because the world and others need to behave themselves). Anytime you get a high Fe paired with a 1 fix, there’s often a focus on needing the outer world to get in line and agree with the FJ’s moral principles. The 2 wing lends a forgiving air and the desire to serve others, which does soften the 1 somewhat but makes them shy less away from stating their views (Fe-dom + 1) than a 1w9.
Depending on the health level and maturity of the ENFJ involved, this corrective mentality would be warm and approachable but also sure of what it wants and constantly pushing self and others toward a higher ideal (healthy) or judgmental, a perfectionist, rigid, and have completely unrealistic expectations for self and others (Ni + 1) (unhealthy).
Ok, so I have two questions but first I would like to say that I love this page and I'm really glad I found it anyways, 1) when we are teenagers we are developing our least favourite function right? So, when you type characters in movies that are teens do you use that information? And 2) (has nothing to do with the first question) I discovered my functions and that I'm in an Se-Fe loop (or Fe-Se) but I can't figure if I'm ENFJ or ESTP, do you have any tips on finding my aux? Or at least my type
Typically as a teenager you’re starting to grow into your second function, the third usually kicks in around 20 but doesn’t fully develop until later in life; your inferior function (your least favorite) takes decades to come into balance with your dominant.
I treat teens like any other character – I type them based on their motives, behavior, and blind spots. I also type kids the same way, even though technically they’re too young to type. But a good writer can be consistent enough in their writing to show a child as a complete character, complete with blind spots. (Mike in Stranger Things being a FeNi, for example, out of touch with inferior Ti.)
Which one of your functions is weaker? Which one are you using in a slapdash manner? Which one do you make the most mistakes with? Fe-doms are highly in tune with other people and their feelings at all times; they feel what others feel, they want to control the emotional environment (as judging types), and they prioritize and comprehend people’s feelings in a way no tert-Fe can even begin to emulate. Tert-Fe feels guilt sometimes for causing strife but is largely out of touch with people and their feelings, and their own feelings – which they tend to analyze rather than understand. Se-dom is much more competent in knowing the right opportunities to leap onto to make things happen or shift them in a direction that solves the immediate problem than low Se, which miscalculates, over-estimates its ability (and proves itself wrong), and makes foolish knee-jerk decisions.
A good rule of thumb is to ask yourself: when I use this function, does it make the situation BETTER / resolve the problem or cause more problems (because I handle it clumsily)?
So, lower Se = leaps into action desperate to make something happen, makes the wrong choice, causes more problems.
Lower Fe = tries to handle the emotional atmosphere, only causes greater pain / misunderstandings / founders around trying to find solid footing, leads to more hurt feelings and miscommunications.
Hy! Can you pls give more examples how the types looks like as a child? (I mean, you said they using just 1-2 function, how does this manifest in real life?)
Already did that here. And here.
How much do you type yourself based on childhood you? How can you tell enneagram types of a child?
Overall? 10 percent. Examine it to see what still lingers in your personality and if it matches, you have a consistent pattern. But type yourself as an adult, over 18.
I recommend not Enneagram typing until you’re over 20 years old (ideally, 35). Childhood incidents may provide a basis of BEHAVIOR, but until you are old enough to consciously evaluate your motives / fears, you won’t know why you acted that way. Enneagram is all about how you react to situations (by protecting your image – heart type; by withdrawing in fear – head type; or by instant gut reactions and anger – gut type). The older you are, the more evidence you have of how you have “made mistakes” – which leads you to your E type / variants.
- ENFP Mod
36 notes
·
View notes
Text
Rising Sign is in 27 Degrees Taurus
Calm and deliberate, you hate to move quickly or act hastily. Very practical, every effort must count or you can't be bothered. Patient, persistent and steady, but very stubborn -- you can't be pushed or pressured into anything. You seem outwardly self-assured because you tend to repress your inner tension and turmoil. You exude an earthy warmth, friendliness and charm. You demand comfortable surroundings and appreciate the good life. Be careful of a tendency to be overly self-indulgent. At times, you are lazy and difficult to motivate. Overcoming inertia is a problem for you and, because you are not by nature a self-starter, it is often necessary for you to receive stimuli from others in order to get moving.
Sun is in 21 Degrees Aquarius.
You get bored with the status quo and are generally open to new things and ideas. An individualist and a free spirit, your friends are quite important to you as long as they do not try to tie you down by making too many emotional demands on you. Your thoughts are offbeat and you're a bit eccentric, but not always very changeable. As a matter of fact, you can be quite stubborn at times. Very fair-minded when dealing with large groups or broad issues, you are not always emotionally sensitive to the needs of individuals. Extremely objective, with good powers of observation, you would be qualified to study technical and complicated subjects, like science, computers or maybe even astrology.
Moon is in 25 Degrees Gemini.
Restless in the extreme, you are easily bored because of your short attention span. Your emotions change rapidly and you love to talk about your feelings. Generally, you have good judgment -- your intellect controls your emotions and you do not overreact emotionally to things. A good jack-of-all-trades, you have many- sided interests and enjoy reasoning things through. With your mental agility and need for physical mobility, you are attracted to traveling and learning about other peoples and cultures. You have vivid powers of emotional self-expression - - you can be a nonstop talker. You love to share your ideas with anyone who will listen.
Mercury is in 07 Degrees Aquarius.
You tend to be very opinionated -- you have strongly felt notions about things and are quite vocal about expressing and defending them. Yet you are also an original thinker -- you enjoy shocking others with your offbeat, original thoughts. You appreciate and need mental and intellectual stimulation. Your judgment is usually fair and impartial -- you can be a good critic because you can remain objective and unemotional about most things.
Venus is in 06 Degrees Capricorn.
You tend to keep your feelings under control -- emotions are only released in serious or important situations. You are distrustful of others whose behavior could be judged excessive or immoderate. As such, you prefer to relate only to those who are older than you or to those whose position is such that respect and duty are more important for both of you than passion or emotional response. Be careful, however, of relationships that are merely based on practicality or utility or you will ultimately be lonely.
Mars is in 23 Degrees Leo.
You are a very proud person. Strong, bold, courageous and self-possessed, you love to be the one to initiate significant actions. When people expect a lot of you, you respond positively and will work hard in order to maintain their respect. But when your dignity or pride is threatened, you tend to become sarcastic, arrogant and domineering. Try not to take any challenge or resistance that you meet as a personal affront. You are very stubborn about your right to live your life according to your own principles.
Jupiter is in 11 Degrees Sagittarius.
You have a very strong sense of ethics and morality. You are widely read and may also be widely traveled because you are sincerely interested in expanding your knowledge of the world about you. At times, you have an annoying tendency to be self-righteous and preachy about your belief system. You are usually quite idealistic and you demand the right to be able to explore the entire world of experiences yourself. Remember to grant others the similar right -- be tolerant, not dogmatic.
Saturn is in 12 Degrees Pisces.
Your tendency to think that your life is out of control is based on an unreasonable fear, probably connected with an unfortunate experience with the person who filled the father figure role in your early life. Learn to take responsibility here and now for your own life. Try to stop having unrealistic expectations about guide figures. Remember that they are merely human, with all the same faults and self-doubts that you have. When you get confused or uncertain, try to simplify your lifestyle -- things will then become easier to bear.
Uranus is in 27 Degrees Capricorn.
You, and your peer group as well, seek out practical solutions to a changing society's attitudes to customs, traditions and authority structures. Your logical and orderly manner of dealing with these matters will result in permanent and carefully planned, but sweeping, reforms.
Neptune is in 24 Degrees Capricorn.
You, and your entire generation, will idealize work, practicality and the ability to attain reasonable goals. But, because you will also stress the need to be selfless and giving, you may find it difficult to attain your goals unless you have lowered your expectations on all fronts.
Pluto is in 00 Degrees Sagittarius.
For your entire generation, society's cherished beliefs and totems will be radically changed. Many traditional concepts will be totally altered, if not completely destroyed. The rights of individuals to pursue their own course in life will be reasserted.
N. Node is in 09 Degrees Scorpio.
You have a special aptitude for working by yourself, or with a like-minded group of dedicated individuals. Once you've committed yourself to a person or group or project, your loyalty and devotion are total until the group's goals have been realized. Not at all gregarious by nature, you're uncomfortable around strangers, greatly preferring to be in known and familiar situations. Others may regard you as shy or eccentric, but those who know you well are aware of the intense loyalty that you have to your friends.
1 note
·
View note
Text
The Brain and System Based Executive Coaching
New Post has been published on https://personalcoachingcenter.com/the-brain-and-system-based-executive-coaching/
The Brain and System Based Executive Coaching
Research Paper By Marco Paracciani
(Executive Coach, THAILAND)
Background
My target audience is busy executives who want to develop themselves into the best they can be, for themselves, for the teams they lead, and for the organizations they work for. They tend to be driven individuals used to fact-based problem solving, data-driven decision-making, and to use evidence to underpin critical investment bets. Coaching is often used as a valuable resource for the development of these individuals thanks to the patronage from corporate HR teams and/or senior executives who have had positive coaching experiences.
Nonetheless, there are still concerns, resistances, and maybe myths that hinder the adoption of executive coaching as a powerful talent development tool in many organizations and cultures. One of these myths is that executive coaching is the ‘arm of last resort’ for an executive to address behavioral issues(before more serious decisions are taken) and that it has no real scientific basis to justify its claim to fame. This is despite very substantial research studies published by reputable publishers over the last decades on the psychology, sociology, and physiology of coaching and its benefits, not to mention the many works undertaken by scores of reputable researchers around the world to study the effectiveness of the many coaching frameworks and models.
Hypothesis
I hypothesize that a scientific and factual basis to the coaching practice might prove effective in enhancing the acceptance of executive coaching as a powerful organizational and talent development tool within the corporate world across continents and cultures. The assumption behind this hypothesis is that corporate professionals’ concerns about coaching’s real effectiveness can be allayed when executive coaching is underpinned by a logical and science-based approach so that corporate talent investment decisions – in terms of time and money–can allow executive coaching to be more widely adopted.
In this context, this research paper aims at researching how both neuroscience-based coaching and systems thinking as tools to deliver a fact-based and powerful coaching experience.
Neurosciences and Executive Coaching
Over the last two decades, neuroscience has made giant leaps thanks to significant advances, among others, in medical digital imaging technology. This progress has allowed the medical community a much deeper understanding of the brain’s functioning which has brought about challenges to many of the previously well-accepted theories about the functioning of the organ we call the brain. One key concept – now widely researched and accepted – at the heart of neuroscience-based executive coaching, i.e. neuroplasticity(1):
Neuroplasticity, also known as neural plasticity, or brain plasticity, is the ability of neural networks in the brain to change through growth and reorganization. These changes range from individual neurons making new connections, to systematic adjustments like cortical remapping. Examples of neuroplasticity include circuit and network changes that result from learning a new ability, environmental influences, practice, and psychological stress.
Neuroplasticity studies demonstrate (2)(3)(4) that the adult human brain is not at all hard-wired once adult age is reached but actually evolves continually during the human life span responding to the stimuli the individual’s lifestyle events provide. There are actually several ways in which this plasticity can manifest itself, such as structural neuroplasticity, functional neuroplasticity, and – within the latter – several activity-dependent plasticity methods, such as the brain’s ability to increase or decrease the firing power of its synapses (synapsis plasticity) and its ability to regulate the excitability of its neurons (intrinsic plasticity). Neuroplasticity is therefore a form of systemic intelligence, the intelligence of the intelligent organ one might say, as it allows the brain to optimize its own response to the circumstances, stimuli, and traumas it receives.
From a coaching perspective, this is extremely relevant and powerful. The question is then how to best harness this systemic intelligence of the brain for the benefit of the coachee? The answer to that question is revealed by many studies and researchers’ testimonials (5)(6)(7): the single most important trigger for a healthy adult brain’s neuroplasticity is in fact attention, our own conscious attention.
Acting like a spotlight on a theatre scene, our attention can trigger neurological brain plasticity if applied consciously and consistently over time. Attention is what enables learning as it fosters those neuroplastic responses that create, with time and effort, new neurological connections and ‘brain maps’ in our minds that can then be recalled instantly and represent our ‘knowledge’. This process applies to new physical or manual skills we might want to acquire (e.g. skiing, carpeting, baking, pottery, painting, music playing, etc) as well as to new intellectual skills, such as a new language, a new profession, or new behavior.
In summary, attention enables neuroplasticity which in turn enables learning. Nothing earth-shattering one might say, as we know it from childhood that if you pay attention you learn faster. However, as our brain swims in a chemical solution, hormones have a huge impact on our thoughts, behaviors, and actions, hence our ability to consciously orient our attention can be significantly impaired or enabled by the nature of the predominant ‘cocktail’ of hormones present at a given time. So, where it gets interesting is when one realizes that attention can not only be oriented to enable learning but to a certain extent also to create the right hormonal environment required for positive and powerful learning to take place. Attention thus can bring about learning and shape the learning environment as well. Quite remarkable and useful to know, when you are dealing with stressed-out, driven executives who often have to deal with huge professional pressures, conflicting life demands all while battling their own emotions and demons.
As a result, since 2006 neuroscience-based coaching theories and practices have started to emerge, develop, and get established (8), providing new perspectives on how coaching can effectively enable sustainable and permanent behavioral changes in individuals. They can become a powerful force for executive coaching to be broadly accepted as a respected talent / organizational development tool across continents, cultures, and customer clusters, i.e. not just medium/large corporations but also entrepreneurs, start-ups, and gig-economy professionals. Its beauty relies on its scientific underpinning which guides and informs the coaching process with the ultimate aim to help ‘hardwire’ the desired changes, behaviors, or beliefs, hence facilitating the truly transformational change of individuals and organizations.
Systems Thinking and Executive Coaching
While neuroscience indeed informs the coach’s practice for the benefit of the executive, the coach can hardly ignore that the coachee is much more than just an individual looking to improve his/her professional trajectory. S/he is a complex human being, with unique personality traits, history, needs, and emotions, whose professional trajectory deeply depends not just on his/her professional performance, but on several interdependencies with broader ‘systems’ (9), and thus by how theses ‘systems’ can be considered in a management application, as defined by Peter Senge in 1990 with his seminal work “The Fifth discipline”(9)(10)(11). Such systems would include, at least, the following areas: the executive’s work community (company culture, individual dynamics, etc), his/her personal and social relationships, his/her business’s industry regulations, and his/her country of residence laws, rules, and habits. Let’s look at these systems briefly from inside out to explore their interdependencies with the coachee.
Personal system: each executive has a unique personal history that has shaped the values, behaviors, ambitions, and his/her overall character. The influencers can be endless and represent an intricate ‘system’ that can have a direct bearing on the executive’s behaviors. Besides, each executive will have a private life with its all-important relationships, which further enrich and inform the executives’ personal system. The coach needs to understand the dynamics of this system to properly support the coachee.
Social system: as any social being, the executive needs a network of social relationships to be balanced and thus at his/her best at work. These relationships can be very diverse and touch very diverse aspects of the individual’s persona: love, friendship, religion, sports, culture, fun, and more. The coach needs to consider their impact on the coachee’s professional life and evaluate through the coachee if and how the system can be optimized.
Work system: this is a large system that includes the executive’s professional relationships, the company culture, it’s spoken & unspoken values, and codes of behavior. The degree of alignment between these values and behaviors with the executive’s own values and behaviors does have a direct impact on the executive’s effectiveness and hence needs to be explored and understood by the coach.
Industry system: any industry the executive operates in will have a bearing on the business and hence on its executives. The industry rules, regulations, and governing bodies are a powerful system the coachee needs to be aware of and possibly tap into.
Country system: as complex as it might be, this is the ultimate system that needs to be reckoned with, by both coachee and coach. It’s culture, rules and behaviors will inevitably impact the executive’s work, relationships, and ultimately his/her success.
As mentioned before, this is not an exhaustive list as there can be other systems that have a material relevance on the coachee, however, it is sufficient to assert that the success of an executive coaching program cannot be lasting and transformational unless it has properly embedded the interdependencies between the coachee and his/her relevant systems in its deployment. The coachee is de facto at the center of a complex network of systems that do have a material bearing on the executive’s professional life and it is here where systems thinking, and coaching, intersect.
Neuroscience-based coaching and system thinking can thus inform each other, allowing the coach to fully comprehend and support the coachee. A perfect example is how the executive responds (or reacts) to an occasion in which a system presents a sudden challenge that could be perceived as a threat and thus trigger a ‘fight or flight’ reaction instead of a more pondered conscious response. These occasions abound in everyday executive life and could come from a variety of sources, such as unforeseen events, challenging behaviors, negative results, or simply unexpected circumstances. The SCARF Model (12), developed and administered by D.Rock’sNeuroleadership Institute, helps executives and coaches to understand the individual’s sensitivity to 5 areas: status, certainty, autonomy, relatedness, and fairness. Awareness of such sensitivities is a useful tool for the coachee to recognize patterns of behaviors that are related to these social sensitivities, thus – with time and the coach’s support – improve his/her effectiveness by moving from reaction to response.
Conclusion
This paper asserts that the brain & systems-based executive coaching – i.e. brain’s neuroplastic properties combined with the systems thinking management theory – can provide a factual backbone to further the adoption of executive coaching practices across cultures, geographies, and types of organizations. While both disciplines are highly complex and require a high level of professional competencies to be fully understood and mastered, brain & systems-based executive coaching does not need to be as intimidating as a concept as it might sound: the fundamental principles are intuitive enough to be understood and embraced by all professional stakeholders, as long as their principles and their relevance to the executive world are clearly, simply and openly communicated. That’s the job of us executive coaches.
References
(1) Neuroplasticity
(2)Maguire, E. A.; Frackowiak, R. S.; Frith, C. D. (1997). “Recalling routes around London: Activation of the right hippocampus in taxi drivers”. Journal of Neuroscience, 2007.
(3) “Michael M. Merzenich | Scientific Learning”. Scientific Learning Corporation. 1997–2009.
(4) David H. Hubei & Torsten Wiesel, 1981 Nobel Prize winners
(5) Daniel Amen – The most important lesson from 83,000 brain scans, TEDxOrangeCoast, October 16, 2013.
(6) VeerlePonnet – Using insights of neuroscience to improve teaching and learning, TEDxPatosdeMinas, Nov 12, 2019, https://www.youtube.com/watch?v=NmAuawoYnUk
(7) Dr. Kelly Lambert – Improving our neuroplasticity, TEDxBermuda, Feb 3, 2020
(8)The Systems Theory and Systems Thinking
(9) The Fifth Discipline: The Art and Practice of the Learning Organisation, Peter Senge 1990
(10) Peter Senge: “Systems Thinking for a Better World” – Aalto Systems Forum 2014
(11) The 11 Laws of Systems Thinking and Stakeholder Engagement, Thought Exchange, Jamie Billingham
(12) The SCARF Model, David Rock, The Neuroleadership Institute
(13) The What, Why and How of Brain-based Coaching, Dan Beverly, 1 January 2015
(14) David Rock, Quiet Leadership (New York: HarperCollins, 2006), Mental Energy and Physiological Energy – Art Markmann, Feb 12, 2015
(15) No Pain, No Brain Gain: Why Learning Demands (A Little) Discomfort, The Science of Work, by Mary Slaughter and David Rock, 18 Apr 2018
Original source:
#business coaching#business coaching system#coaching#coaching (industry)#coaching demonstration#coaching systems#executive#executive coach#executive coach certification#executive coach training#executive coaching#executive coaching demonstration#executive coaching session#executive coaching session youtube#executive coaching videos#how to sell executive coaching#leadership coaching#life coaching#mind mastery coaching system#systems coaching#what is systems coaching#Business Coaching#Leadership Life Coaching
0 notes
Text
Nervous System Anatomy & Function
The nervous system is divided into two primary parts, with many smaller components within those.

(source).
Central Nervous System includes the brain and spinal cord.
Brain
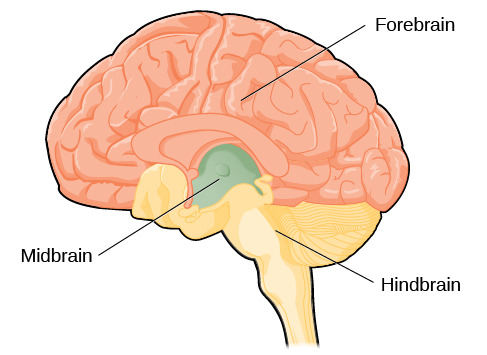
(source).
The brain is made up of three primary parts, the hindbrain, midbrain, and forebrain.

(source).
Hindbrain: includes the cerebellum, medulla, and pons. These structures are all at the base of the brain where it connects to the spinal cord.
Cerebellum: Impacts motor movement, balance, posture, and higher cognitive processes like speech and selective attention.
Medulla: Regulates a number of vital processes like breathing and swallowing by influencing information flow between the rest of the brain and the spinal cord.
Pons: Connects the two halves of the cerebellum and helps coordinate movement between the sides of the body.

(source).
Midbrain: The midbrain conducts information between the spinal cord and the forebrain. It’s essentially a traffic controller, identifying what information is important and where it should be sent.
Superior colliculi: Transmits visual informatiom
Inferior colliculi: Transmits auditory information
Substantia nigra: Transmits motor information & helps regulate the reward system.
Reticular formation: Directly connects the spinal cord to the hypothamalus through the hind and midbrain. Helps regulate a range of vital functions including sleep, movement and vomiting. Includes the reticular activating system, which impacts consciousness, arousal and wakefulness.

(source).
Forebrain: Includes two main components: the subcortical structures and the cerebral cortex.
Subcortical Structures:
Thalamus: Acts primarily as a relay station, transmitting sensory information from the midbrain to other parts of the forebrain except smell information. Thiamine deficiency can cause Wernicke-Korsakoff syndrome, where neurons in the thalamus deteriorate. This is usually caused by chronic alcohol abuse and leads to confusion, disorientation in eye movement, and ataxia (loss of control over body movement) in the Wernicke’s encephalopathy stage, later becoming Korsakoff’s syndrome with severe memory disturbance including retrograde amnesia, anterograde amnesia, and confabulation (for more about amnesia, see my Memory post).
Hypothalamus: Involved in a large number of vital functions including emotion, hunger/thirst, sex drive, sleep and body temperature regulation. Also monitors internal body states (like body temperature) to initiate or maintain homeostasis. Includes the suprachiasmatic nucleus, which regulates sleep-wake cycles like circadian rhythm. Injury to the hypothalamus can cause severe emotion dysregulation including uncontrollable aggression or laughter.
Basal Ganglia: Includes three structures: the caudate nucleus, putamen and globus pallidus, along with the substantia nigra (which is primarily located in the midbrain). These sets of structures regulate movement, assist in sensorimotor learning, and automatic motor expressions of emotion, like smiling. Motor disorders are often related to basal ganglia dysfunction, like Parkinson’s, Huntington’s, ADHD, Tourette’s, and OCD. Other disorders that often include motor changes or impairment, like mania and psychosis, may also be related to basal ganglia dysfunction.
Limbic System: Includes multiple structures, the most key of which are the amygdala, hippocampus and cingulate cortex. The limbic system regulates emotion, memory, and other aspects of cognitive function. The amygdala is primarily responsible for emotion, including regulating emotional responses to stimuli and connecting emotions to memories, including flashbulb memories (vivid although not always accurate memories of specific, very emotionally important events). Injury to the amygdala can cause Kluver-Bucy syndrome, where negative emotions decrease, diet changes, sex drive increases, and people struggle to identify meaningful events or objects (meaning the emotion is not integrated with the memory). The hippocampus is more associated with memory and learning, including translating short term memories into long term memories, although it does not store memories. It also creates visual images. Injury to the hippocampus can cause anterograde and retrograde amnesia. The cingulate cortex envelops the corpus callosum and is integral to pain perception and response.
Cerebral Cortex:
Makes up 80% of the brain’s weight and is divided in two hemispheres (left and right), with four lobes in each hemisphere. The two hemispheres are connected by the corpus callosum, which is sometimes severed to control epilepsy. If it is severed, then the brain operates as two independent pieces. Most sensory and motor operations in the brain are controlled contralaterally, meaning that the left side of the brain controls the right side of the body and vice versa. Both sides of the brain are involved in most functions, but the sides of the brain tend to focus on a subset of functions. The dominant side (usually left) focuses more on language and logical thought processes while the nondominant side (usually right) focuses on spatial reasoning, creativity and emotions.
Frontal Lobes: Includes the primary motor cortex, supplementary motor area, premotor cortex, Broca’s area, and prefrontal cortex. The primary motor cortex is responsible for executing movement, while the supplementary motor area is responsible for planning and controlling movement as well as learning new kinds of movement. The premotor cortex also controls movement, but focuses on movement responses to stimuli (jerking away from a hot stove). Broca’s area is responsible for producing speech and written language. The prefrontal cortex is where much of executive functioning and other complex functions are regulated, like problem-solving, creativity, emotion, judgment, and planning. Injury to the frontal lobes will have a variety of impacts depending on the specific area. For example, if Broca’s area is impaired, a person may be unable to produce verbal or written language (although they will still be able to understand language), while if the prefrontal cortex is impaired, a person may experience significant executive dysfunction (for example, impaired planning and judgment), pseudopsychopathy (which includes poor impulse control, emotional liability, and aggression), or pseudodepression (which includes decreased movement and language and decreased emotionality).
Parietal Lobes: The parietal lobes are primarily responsible for sensory perception and interpretation. It includes the somatosensory cortex, which regulates temperature, pressure, pain, proprioception (meaning sense of one’s own body in space, relative to other objects or people, including movement and balance) and gustation. Impairment of the parietal lobes can cause apraxia (inability to execute complex motor movements), somatosensory agnosia (inability to recognize things, people, or symptoms, depending on the subtype), and Gerstmann’s syndrome (usually including agraphia, acalcuia, and left-right confusion).
Temporal Lobes: The temporal lobes are primarily responsible for auditory function and language function. It includes the auditory cortex, which regulates auditory perception, and Wernicke’s area, which is vital in language reception and understanding. The temporal lobes are also important in long-term memory, including storage and retrieval. Auditory cortex impairment can lead to auditory hallucinations and inability to interpret sound. Impairment of Wernicke’s area causes Wernicke’s aphasia, meaning an inability to comprehend or interpret sound.
Occipital Lobes: The occipital lobes are primarily responsible for vision and related visual functioning. It includes the visual cortex, which regulates visual perception, recognition and memory. The posterior area of the visual cortex is responsible for macular vision from the central retina while the anterior area of the visual cortex is responsible for peripheral vision. Injury or impairment to the occipital lobe can cause blindness, visual agnosia (inability to recognize visual information) or visual hallucinations.
Spinal Cord
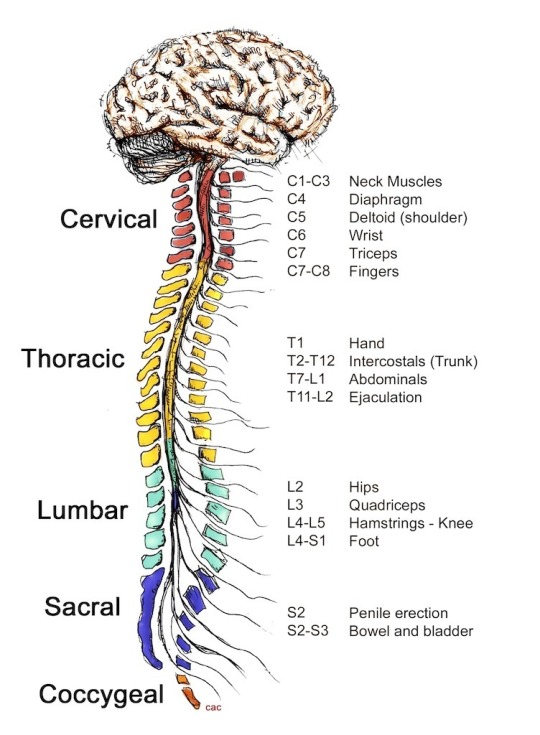
(source).
The spinal cord carries information from the brain to the periphersal nervous system, coordinates behavior between the right and left sides of the body, and manages basic reflexes that the brain is not involved in. It is made up of bundles of nerve tracts (bundled myelinated axons) along with dendrites, cell bodies and interneurons. There are 31 segments of the spinal cord which are divided into five subgroups: cervical, thoracic, lumbar, sacral, and coccygeal. Injury to the spinal cord can cause paralysis, and the severity of that paralysis depends on the area of the injury (the higher up, the more severe the paralysis or other symptoms typically are).
Peripheral Nervous System
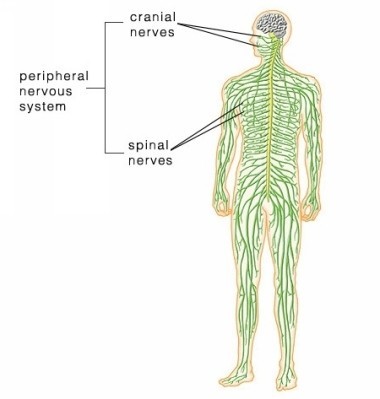
(source).
The peripheral nervous system contains nerves that carry messages between the central nervous system and other areas of the body. This includes 12 cranial nerves that connect to the brain and 31 spinal nerves that connect to the spinal cord. There are two components of the peripheral nervous system.
Somatic Nervous System
The somatic nervous system includes sensory nerves that carry sensory information from the body to the central nervous system and motor nerves that carry motor directions from the central nervous system to the body. These motor directions typically cover voluntary movement. So for example, the sensory nerves might tell the brain that it is uncomfortably cold, causing goosebumps, and the motor nerves might respond by directing the body to put on a sweater.
Autonomic Nervous System
The autonomic nervous system also includes sensory and motor nerves that relay information and directions from the body to the central nervous system. However, the directions given by the motor nerves are mostly involuntary. For example, the sensory nerves might tell the central nervous system that the body’s balance is precarious, so the motor nerves might direct a foot to shift to improve balance. Within the autonomic nervous system, there are two branches: sympathetic and parasympathetic. The sympathetic branch is responsible for arousal and energy use- for example, it is related to “fight or flight” actions. The parasympathetic branch is responsible for rest and energy conservation.
______
If you enjoyed this post, consider making a pledge at Patreon to support Therapy101 and access to information about psychology and mental health.
64 notes
·
View notes
Text
FACILITATING LEARNING, CHILD AND ADOLESCENT DEVT
• The superego is primarily concerned with the idea of right or wrong and is often viewed as “conscience” of personality, according to Freud.
• Based on Erikson’s theory on psychological development, a child who is cold towards the people around him failed in the basic goal of “trust” in the stage “Trust vs. Mistrust”.
• Under Freud’s Phallic Stage in the Psychosexual Development theory, a boy is closer to his mother (Oedipus Complex) and a girl is closer to her father (Elektra Complex).
• Based on Piaget’s developmental stage, when a grade 1 pupil likes to play with his friends but gets angry when defeated is under the Preoperational Stage, which is characterized by egocentrism
• According to Maslow’s Hierarchy of Needs, when one is asked to develop himself to the fullest, he is trying to satisfy his Self-Actualization, wherein the person strives to develop himself to his full potentials.
• According to Erikson, Piaget, and Freud, play allows the child to learn physical skills as well as social skills.
• A child that is 3-5 years old, according to Erikson, is Ego-centric.
• Children who are two years of age are labeled as “terrible twos” by Erikson because of the assertiveness and will of these children, illustrated by using the word “No!”
• The factors affecting individual differences are age differences and personal adjustments, sex differences, family and community background, physical conditions, emotional response and attitudes (EQ), and mental abilities and specific aptitudes (IQ).
• Stimulus-Response (S-R) or Association Theory of Learning states that in every stimulus there is a corresponding response.
• The three fundamental laws of learning by theAssociation Theory are the law of readiness, the law of exercise and law of effect.
• Law of Readiness is when an individual is prepared to respond or act were allowing him to do so is satisfying, and preventing him would be annoying.
• Law of Exercise is where the constant repetition of a response strengthens its connection with the stimulus, while disuse of a response weakens it.
• Law of Effects is where learning is strengthened if it results in satisfaction but is weakened if it leads to vexation or annoyance.
• The Theory of Condition of Learning states that the process of learning consists of the acquisition of new ways of reacting to stimuli developed through attaching new stimuli to established modes of behavior.
• There are two types of conditioning theory, which are classical condition and operant conditioning.
• Classical conditioning consists of eliciting a response by means of a previously neutral or inadequate stimulus.
• Operant conditioning is a theory that believes one can train an organism either by presenting him a reward or punishment as a consequence of his actions.
• Social Learning Theory of Learning viewed that children’s learning process involves observation and imitation.
• The Cognitive Field Theory of Learning defines learning as a relativistic process by which a learner develops new insights and changes the old ones.
• Insight learning of Cognitive Field Theory postulated that the more intelligent the organism and the more experiences he has the more capable he is of gaining higher insight.
• Vector and Topological Theory of Cognitive Field Theory state that individuals exist on a field of forces within his environment that move, change, and give him degree stability and substance or define his behavior.
• Gestalt Learning of Cognitive Field Theory states that learning involves the catching, and generalization of insights, which often are acquired first on a nonverbal level or the level of feeling and maybe verbalized later or may not be verbalized at all.
• Instrumental Conceptualism of Cognitive Field Theory believes that learning is thinking and thinking is the process whereby one makes sense out of the various and somehow unrelated facts through a process called conceptualization or categorization.
• The Subsumption Theory by David Paul Ausubel considered that a primary process in learning is subsumption in which new material is related to relevant ideas in the existing cognitive structure on a
substantive, non-verbatim basis.
• The theory on Conditions of Learning or the Gagné Assumption states that different types of learning exist and that different instructional conditions are necessary for each type of learning
• The five major CATEGORIES OF LEARNING according to Gagné are verbal information, intellectual skills, cognitive strategies, motor skills, and attitudes.
• Transfer of learning occurs when a person’s learning in one situation influences his learning and performance in other situations.
• The major theories concerning TRANSFER OF LEARNINGare Mental discipline, Apperception, Identical elements, Generalization, the gestalt theory of transfer.
• Mental discipline asserts that education is largely a matter of training or disciplining the mind with vigorous mental exercises n the classics, grammar, logic, mathematics, and science on the assumption that
such training makes a person equally effective in all areas where a given faculty is employed.
• Identical elements are the theory of transfer of implies that school should list the aspects of situations that are important to the child even out of the school or in later courses and teach the pupils to cope with different identical experiences or situations in real life.
• Generalization by Charles Judd said that there are two levels or kinds of knowledge –wrote learning or memorization without any meaning and generalized knowledge with many intellectual associations.
• Gestalt theory of transfer is the belief that when the transfer of learning occurs it is in the form of generalizations, concepts, or insights, which are developed in one learning situation and employed in other situations.
• Motivation is the stimulation of action toward a particular objective where previously there was little or no action toward that goal.
• The two types of motivation are intrinsic and extrinsic motivation.
• Intrinsic motivation refers to the inherent or internal stimulus of individuals to learn.
• Extrinsic motivation is based on incentives, which are artificial devices, which are employed to evoke attitude conducive to learning.
• Insight learning is regarded as “serendipity” when an idea suddenly strikes the mind and a solution to a problem is arrived at.
• Metacognition is where a teacher is attempting to develop the student to think about their thinking, or to reason about one’s own thinking.
• Instincts are under the mental dimension of Id according to Freud.
• According to Piaget, a child in the concrete operational stage cannot imagine the steps necessary to complete an algebraic equation.
• Fear of something that was caused by painful experience in the past is an example of Classical Conditioning.
• Operant condition theory is illustrated in a child who tries to complete all tasks given to him correctly to have candy as a “reward.”
• Based on Thorndike’stheory that punishment will only weaken the response and not permanently remove it, a child punished for stealing money won’t steal in the near future but does not guarantee that the child won’t steal anymore.
• The association and cognitive theories of learning are
complementary meaning they support each other in terms of principles and practice.
• Rewarding a child for doing things correctly is a technique called Reinforcement, where it is a behavioral consequence that strengthens a behavior.
• A person possessing Interpersonal Intelligence is characterized by “people-orientedness skills” and has the capacity to make people laugh.
• Reading disability in children who are neglected and abused is related to emotional factors.
• The brain’s ability to change from experience is known as Plasticity.
• John Watson’s quote, “Men are built not born” came from his belief that environmental stimulation is directly affecting a person’s development.
• Attention Deficit Disorder is usually characterized by impatience to wait for his/her turn during games, disregard for rules and show an inability to delay gratification.
• A child who always fights with his/her classmates, who has a very short attention span, and who has frequent tantrums is believed to be suffering from Attention Deficit Hyperactivity Disorder.
• A child who treats his friends aggressively due to his past experiences with his father who is also aggressive is demonstrated by the Social Cognitive theory.
• Based on Jung’s theory, a child who prefers to be alone is an “Introvert”
• Based on Gestalt’s psychology that states, “the whole is more than the sum of all its parts,” a piece of music may sound sad, but when each note is played, there is nothing sad about it.
• Tabula Rasa or the belief that the mind is a “blank sheet” will make the teacher conduct lessons that give sensory impressions because the teacher believes that by doing so, he/she imprints salient inputs in the students’ mind.
• Society is a group of individuals with well-defined limits which persists in time, thus enabling them to develop a set of common ideas, attitudes, interact and of techniques for living and fitting together.
• A group is a unit of interacting personalities with the interdependence of roles and status existing between them.
• The seven KINDS OF GROUPS, which are the primary group, secondary group, in-group, out-group, peer group, reference group, and voluntary associations.
• Social stratification is the system or process of assigning men their respective ranks in a society based on income or wealth, education, occupation, and lifestyle.
• Social mobility is the process of moving from one social stratus to another, it may either be horizontal, vertical, or lateral.
• Socialization is the process by which the individual acquires the social and cultural heritage of his society.
• The three LEVELS OF SOCIALIZATION are vegetative level, sentient level, and a rational level.
• The Vegetative level of the socialization process is the stage characterized by the preoccupation with food, where the desire is primarily for survival.
• The Sentient level is geared towards the satisfaction of sensual passions and desire.
• The Rational level is where a person has already acquired morality and a sense of justice.
• Status is the position a person occupies in society by virtue of his age, birth, sex, marriage, occupation, and achievement.
• The two TYPES OF STATUS are ascribed and achieved.
• Ascribed status is a position assigned to an individual without reference to his innate differences and abilities and is assigned at birth.
• Achieved status is not assigned to an individual at birth, but is left open for competition and individual effort.
• The role is the part that the individual is expected to play in his social group and is the sum of the cultural patterns associated with a particular status.
• Social Deviations refers to the failure of the individual to play the role expected from him by society.
• Internalizations is the process of making an attitude or a practice a part of one’s automatic and unthinking responses.
• Social order is the way the individual is expected to behave in a society where he belongs in order to preserve and maintain the tranquility of his social milieu.
• Social control is the means by which people are led to fill their expected roles in society even against their will just to achieve social order.
• Anthropology is the study of human differences, cultural and biological against the background of the nature all humans share.
• Culture is the complex whole, which includes knowledge, belief, art, law, morals, customs, and other capabilities and habits acquired by man as a member of society as defined by Edward B. Taylor.
• The two KINDS OF CULTURE are non-material culture and material culture.
• Non-material culture is intangible, which includes beliefs, morals laws, customs, traditions, folkways, mores, etc.
• Material culture is tangible and includes man’s technologies, etc.
• The CHARACTERISTICS OF CULTURE are it is learned, all people have varied culture, it is a group product and it is transmitted.
• The importance of culture is that through the development of culture man can set aside certain laws of nature to conform to his needs and man can overcome his physical handicaps.
• Folkways are customary ways of behaving, which have become habitual and repetitive to an individual group such as caring for the elders and saying “po” and “opo”.
• Mores occurs when folkways become compulsive for the welfare of the society and it has acquired moral significance, where failure to conform to these results to ostracism or condemnation.
• Sub-culture refers to the attitude of a certain group to deviate from the habitual practices of the majority.
• Cultural relativism refers to the practices considered immoral or taboo to a certain group of people, yet moral to other societies, including polygamy and pre-marital sex.
• Culture shock is the term used to denote the feeling of depression, often expressed as homesickness, caused by living in a foreign environment.
• Cultural values refer to the collective ethical, aesthetics and religious values of the community including artistic inclination, poetry, music, painting, literature, and such other practices, which the entire society considers as vital elements of their existence.
• Filipino cultural values that make the Filipino unique and distinct from other peoples of the world includes non-rationalism, emotional closeness and security of the family, authority, economic and social improvement, utangnaloob, personalism, indolence, ningaskugon, mañana habit, hospitality, and fiesta syndrome.
• Non-rationalism is a Filipino cultural value that is the tendency to perceive thoughts, objects, events, and persons as sacred.
• NON-RATIONALISM includes animism, fatalism, social acceptance, pakikisama, euphemism, and go-between.
• Emotional closeness and security of the family is a Filipino cultural value, which means there is a mutual dependence among relatives, granting special favors or privileges among the immediate or even
distant relatives.
• Authority refers to the emphasis on the power and importance of authority figure.
• Economic and social improvement is the desire to improve the standard of living of his family and his hometown.
• Utangnaloob means sense of gratitude.
• Personalism emphasizes the importance of the person with whom one has immediate face-to-face contact and connection, which includes pakiusap, lagay, areglo, and palakasan.
• Indolence means laziness.
• Ningaskugon means great enthusiasm at the beginning of a task but
gradually fades.
• Mañana habit refers to procrastination or putting for tomorrow what can be done today.
• Hospitality means cordially entertaining guests and visitors even to the point of sacrificing their own welfare.
• Fiesta syndrome refers to lavish spending during fiestas and other occasions.
ASSESSMENT OF STUDENT LEARNING
Assessment of learning focuses on the development and utilization of assessment tools to improve the teaching-learning process.
• Measurement refers to the quantitative aspect of evaluation where
it involves the outcomes that can be quantified statistically.
• Measurement is also defined as the process of determining and differentiating the information about the attributes or characteristics of things.
• Evaluation is the qualitative aspect of determining the outcomes of learning and it involves value judgment.
• Testing is a method used to measure the level of achievement or performance of the learners.
• Test consists of questions or exercises or other devices for measuring the outcomes of learning.
• The three CLASSIFICATIONS OF TESTS are according to the manner of response, according to the method of reparation, and according to the nature of the answer.
• Objective tests are tests, which have definite answers and therefore are not subject to personal bias.
• Teacher-made tests or educational tests are constructed by the teachers based on the contents of different subjects taught.
• Diagnostic tests are used to measure a student’s strengths and weaknesses, usually to identify deficiencies in skills or performance.
• Formative testing is done to monitor students’ attainment of the instructional objectives.
• Summative testing is done at the conclusion of instructional and measures the extent to which students have attained the desired outcomes.
• A standardized test is already valid, reliable and objective and is a test for which contents have been selected and for which norms or standards have been established.
• Standards or norms are the goals to be achieved, expressed in terms of the average performances of the population tested.
• The criterion-referenced measure is a measuring device with a predetermined level of success or standard on the part of the test takers.
• The norm-referenced measure is a test that is scored on the basis of the norm or standard level of accomplishment by the whole group taking the tests.
• The TYPES OF ASSESSMENT are Placement Assessment, Diagnostic Assessment, Formative Assessment, and Summative Assessment.
• Placement Assessment is concerned with the entry performance of the student, where its purpose is to determine the prerequisite skills, degree of mastery of the course objectives and the best mode
of learning.
• Diagnostic assessment is a type of assessment given before instruction where it aims to identify the strengths and weaknesses of the students regarding the topics to be discussed.
• Formative assessment is a type of assessment used to monitor the learning progress of the students during or after instruction.
• Summative assessment is a type of assessment usually given at the end of a course or unit.
• The MODES OF ASSESSMENT are Traditional Assessment, Performance Assessment, and Portfolio Assessment.
• Traditional assessment is in which student typically select an answer or recall information to complete the assessment.
• Performance assessment is an assessment in which students are asked to perform real-world tasks that demonstrate meaningful application of essential knowledge and skills.
• Portfolio assessment is based on the assumption that it is a dynamic assessment.
• The most reliable tool for seeing the development of a student’s ability to write is a portfolio assessment.
• The KEY TO EFFECTIVE TESTING includes the Objectives, Instruction, Assessment, and Evaluation.
• Objectives are the specific statements of the aim of the instruction, where it should express what the students should be able to do or know as a result of taking the course.
• Instruction consists of all the elements of the curriculum designed to teach the subject, including the lesson plans, study guide, and reading and homework assignment.
• Assessment is the process of gathering, describing or quantifying information about the performance of the learner and testing components of the subject.
• The factors to consider when constructing GOOD TEST ITEMS are validity, reliability, administrability, scorability, appropriateness, adequacy, fairness, and objectivity.
• Validity refers to the degree to which a test measures what it is intended to measure.
• To test the validity of the test, it is to be pretested in order to determine if it really measures what it intends to measure or what it purports to measure.
• Reliability refers to the consistency of scores obtained by the same person when retested using the same instrument or one that is parallel to it.
• The test of reliability is the consistency of the results when it is determined to different groups of individuals with similar characteristics in different places at different times.
• Scorability states that the test should be easy to score, directions for scoring should be clear, and the test developer should provide the answer sheet and the answer key.
• Appropriateness mandates that the test items that the teacher construct must assess the exact performances called for in the learning objectives.
• Adequacy states that the test should contain a wide sampling of items to determine the educational outcomes or abilities so that the resulting scores are representative of the total performance in
the areas measured.
• Fairness mandates that the test should not be biased to the examinees.
• Evaluation is used to examine the performance of students and comparing and judging its quality.
• The TYPES OF VALIDITY are Content Validity, Criterion-related validity, and Concurrent Validity.
• Content validity is a validation that refers to the relationship between a test and instructional objectives and it establishes the content so that the test measures what it is supposed to measure.
• Criterion-Related Validity is a type of validation that refers to the extent to which scores from a test relate to theoretically similar measures.
• The two types of CRITERION-RELATED VALIDITY are Construct Validity and Predictive Validity.
• Construct validity is a type of validation that measures the extent to which a test measures a hypothetical and unobservable variable or quality, such as intelligence, math achievement, performance anxiety, etc.
• Predictive validity is a type of validation that measures the extent to which person’s current test results can be used to estimate accurately what that person’s performance or other criteria, such as test score, will be at a later time.
• Concurrent validity is a type of validation that requires the correlation of the predictor or concurrent measure with the criterion measure, which can be used to determine whether a test is useful to use as a predictor or as a substitute measure.
• Objectivity is the degree to which personal bias is eliminated in the scoring of the answers.
• Nominal scales classify objects or events by assigning numbers to them, which are arbitrary and imply no quantification, but the categories must be mutually exclusive and exhaustive.
• Ordinal scales classify and assign rank order.
• Interval scales also known as equal interval or equal unit is needed to be able to add or subtract scores.
• Ratio scales where the zero is not arbitrary; a score of zero includes the absence of what is being measured.
• Norm-referenced interpretation is where an individual’s score is interpreted by comparing it to the scores of a defined group, often called the normative group.
• Criterion-Referenced Interpretation means referencing an
individual’s performance to some criterion that is a defined
performance level.
• The stages in TEST CONSTRUCTION are Planning the test, Trying Out the test, Establishing Test Validity, Establishing the Test Reliability, and Interpreting the Test Score.
• The frequency distribution is a technique for describing a set of test scores where the possible score values and the number of persons who achieved each score are listed.
• Measures of central tendency are computed to know where on the scale of measurement distribution is located.
• Measures of dispersion are used to know how the scores are dispersed in the distribution.
• The three commonly used MEASURES OF CENTRAL TENDENCY are the mean, median and mode.
• The mean of a set of scores is the arithmetic mean and is found by summing the scores and dividing the sum by the number of scores.
• Median is the point that divides the distribution in half, which is half of the scores fall above the median and half of the scores fall below the median.
• Mode is the most frequently occurring score in the distribution.
• Range is the difference between the highest score and the lowest score.
• The variance measures how widely the scores in the distribution are spread about the mean.
• Variance is the average squared difference between the scores and the mean.
• The standard deviation indicates how spread out the scores are, but it is expressed in the same units as the original scores.
• A graph of a distribution of test scores is better understood that the frequency distribution or a table of numbers because the general shape of the distribution is clear from the graph.
• A teacher must use an Essay type of test the student’s ability to organize ideas.
• NSAT and NEAT results are interpreted against a set mastery level, which means that the tests fall under the criterion-referenced test because it describes the student’s mastery of the objectives.
• The first step in planning an achievement test is to define the instructional objective.
• Skewed score distribution means the score is concentrated more at one end or the other end.
• Normal distribution means that the mean, median, and mode are equal.
• When the computed value or r for Math and Science is 0.90, it implies that the higher the scores in Math, the higher the scores in Science because r=0.90 means a high positive correlation.
• An objective that is at the highest level in Bloom’s taxonomy is rating three different methods of controlling tree growth because it deals with evaluation.
• Inferential is a type of statistics that draws conclusions about the sample being studied.
• Generosity error is the error teachers commit when they tend to overrate the achievement of students identified by and aptitude tests as gifted because they expect achievement and giftedness to
go together.
• Portfolio assessment measures the students’ growth and
development.
• Formative testing is the test most fit for mastery learning because it is done after or during a discussion where the feedback can be used to determine whether the students have a mastery of the subject
matter.
• A characteristic of an imperfect type of matching set is that an item may have no answer at all.
• Determining the effectiveness of distracters is included in item analysis.
• Discrimination index is the difference between the proportion of high-performing students who the item right and the proportion of low-students who got an item right.
• A positive discrimination index means that more students from the upper group got the item correctly.
• A negative discrimination index takes place when the proportion of the students who got an item right in the low performing group is greater than the students in the upper performing group.
• Zero discrimination happens when the proportion of the student who got an item right in the upper-performing group and the low-performing group is equal.
• When points in the scattergram are spread evenly in all directions, this means that there is no correlation between two variables.
• A norm-referenced statement is comparing the performance of a certain student with the performance of another student/s.
• Content is a type of validity that is needed for a test on course objectives and scopes.
• When there are extreme scores the mean will not be a very reliable measure of central tendency.
• The sum of all the scores in a distribution always equals the mean times the N because the sum of all the scores is equal to the product of the mean and the number of scores (N). Formula: Mean = Summation of Scores/N
• A Z-value can be used to compare the performance of the students, because it tells the number of standard deviations equivalent to a raw score, where the higher the value of Z score, the better the performance of a certain student is.
• Mean is the measure of the position that is appropriate then the distribution is skewed.
• The analysis of Variance utilizing the F-test is the appropriate
significance test to run between three or more means.
• In standard deviation, the higher the value of standard deviation on the average, the scores are farther from the mean value, whereas the smaller the value of the standard deviation on the average, the scores are closer to the mean value.
• When the value of standard deviation is small, the scores are concentrated around the mean value because the smaller the value of the standard deviation the more concentrated the scores are to the mean value.
• When the distribution is skewed the most appropriate measure of central tendency is Median.
• In the parlance of test construction, TOS means Table of
Specifications.
• Range is a measure of variation that is easily affected by the extreme scores.
• Mode is the measure of central tendency that can be determined by mere inspection because mode can be identified by just counting
the score/s that occurred the most in a distribution.
• The description of each criterion to serve as a standard, very clear descriptions of performance level, rating scale, and mastery levels of achievement are considerations that are important in developing a SCORING RUBRIC.
• A rubric is developmental.
• Performance-based assessment emphasizes process and product.
• Kohlberg and other researchers used a moral dilemma to measure the awareness of values.
• PROJECTIVE PERSONALITY TEST includes Sentence Completion test, Word Association test, and Thematic Apperception Test.
• An anecdotal report is a note written by the teacher regarding incidents at the classroom that might need special attention in the future.
• One of the strengths of an autobiography as a technique for personality appraisal is it makes the presentation of intimate experiences possible.
• Carl Roger is considered the main proponent of Non-Directive counseling.
• Sharing the secrets of a counselee with other members of the faculty is in violation of confidentiality.
• Counselors can break confidentiality rule in cases of planned suicide or planned hurting/killing of somebody.
• Sinforoso Padilla is considered the father of counseling in the Philippines.
• Portfolio is the pre-planned collection of samples of student works, assessed results and other output produced by the students.
• Assessment is said to be authentic when the teacher gives students real-life tasks to accomplish.
• The main purpose of a teacher using a standardized test is to engage in easy scoring.
• Marking on a normative basis follows the normal distribution curve.
• A scoring rubric is important in a self-assessment to be effective.
• The main purpose of administering a pretest and a post-test to students is to measure gains in learning.
• An assessment activity that is most appropriate to measure the objective “ to explain the meaning of molecular bonding” for the group with strong interpersonal intelligence is to demonstrate
molecular bonding using students as atoms.
• Emphasis on grades and honors goes with the spirit of “ assessment of learning”.
• Split-half method and Kuder Richardson measure internal
consistency of the test scores of the students.
• Test-retest measures the stability of the test scores.
• Parallel method measures the equivalence.
• The expression “grading on the curve” means the performance of a certain student compared to the performance of other students in
the group.
• Scoring rubrics have criteria of level of achievement to serve as a standard, has a clear description of performance in each level, and has a rating scheme.
• When constructing a matching type of test the options must be greater than the descriptions, the directions must state the basis of matching, and the descriptions must be in Column A and options in Column B.
• Extended Essay test can effectively measure HOTS cognitive learning objectives.
• An objective test can cover a large sampling of content areas, time-consuming to prepare, and there is a single or best answer.
• Objective tests measures low-level thinking skills, such as knowledge, comprehension, and application.
0 notes
Text
CLOA CE #1: To what extent do cognitive and biological factors interact in emotion (e.g. two factor theory, arousal theory, Lazarus’ theory of appraisal)? (22)
Last on: Paper 1 November 2014
INTRODUCTION This essay will consider the argument or concept of how both cognitive and biological factors interact in emotion and influence how humans experience it
OVERVIEW Cognitive level of analysis
Aims to study inner processes of the mind and determine how cognitive processes guide behavior
Emotion has been investigated in terms of the biological and cognitive influences
Emotion: body’s adaptive response to a particular situation
Ekman et al. (1972) identified 6 primary emotions, universal to all cultures
Fear, anger, surprise, sadness, happiness, disgust
Only one positive one, LOL
Thought to be universal b/c they are expressed the same way thru facial features and can be recognized by everyone
Suggests the emotion is genetic rather than cognitive
Interaction of emotion can be a result of cognitive and/or biological factors, and are sometimes initiated thru one
Cognition: the mental processes of acquiring and processing knowledge and understanding through experiences and senses occurring within the mind
Mind cannot exist or function independently of processes
Like idk what that would even mean do u just not Think???
Physiology: internal, biological mechanisms of living organisms
OVERVIEW Theories of Emotion
LeDoux’s Theory of the Emotional Brain (1999)
James-Lange Theory
Cannon-Bard Theory
Schachter & Singer’s Two-Factor Theory
Darwin’s evolutionary theroy
Lazarus’ Appraisal Theory
All have different notions regarding how emotion is an interrelation between biology and cognition
Biological factors
Biological psychologists view emotion as a primarily somatic process
Processes include body arousal, hormones, facial expressions (indicative of states of mind), physiological changes (e.g. arousal of autonomic nervous system and endocrine system), brain activity, neurochemical processes
Cognitive factors
Cognitive psychologists assume that conscious & unconscious mental processes can influence emotions
Focus on the mental aspects of emotion and how mental processes influence emotional experiences and actions
Interrelation bet. cognition and emotion used as a basis for cognitive and rational emotive therapies
Negative emotions seen to arise from faulty and negative interpretations of experiences; raising awareness of this and challenging negative beliefs thought to help mood
Emotions initiated thru physiological and/or cognitive factors
Biological reactions & subjective feeling of emotion (cognition) leads to associated behavior and expression of emotion
Bidirectional relationship bet. cognitive and biological factors
OVERVIEW LeDoux’s Theory of the Emotional Brain BIOLOGICAL!!
2 neurological pathways for fear responses
Short route: from sensory store in thalamus to amygdala
Long route: traverses neo-cortex and hippocampus b4 eliciting fear response
Evolutionary advantage to separate pathways
When in danger, short route effective, even tho response is quick and inaccurate
Causes instinctive motor response; heavily influenced by emotional arousal
but like,,, would u rather be dead? maybe? ok fair enough
Long route slower but allows for thorough evaluation and appropriate response
Logic > instinct w/ regard to emotional reponses
unless ur like me and just overreact violently to everything
Amygdala receives input from sensory processing areas in the neo-cortex and thalamus and projects to areas in the brainstem controlling fight or flight response
OVERVIEW Lazarus’ Theory of Appraisal COGNITIVE!!
Cognition is essential!!
Thought must occur before one experiences any emotion or physiological responses
People make appraisal of situation and act according to interpretation/appraisal they make of situation
Figure out what they’re supposed to feel based on situation
Primary appraisal: assessing nature of the threat
am i going to die? yes, and hopefully before the paper 1
Motivational relevance: relevance to goals (if positive, then emotion occurs)
Motivational congruence: favorability to goals (if yes, positive emotion; if no, negative emotion)
Accountability: who is responsible?
Secondary appraisal: evaluation of different ways to cope
how should i feel and react? by crying? of course u fool
Problem-focused coping: cope w/ situation by changing it to make it less threatening
Emotion-focused coping: cope w/ situation by reinterpreting it (changing how you feel about it)
Future expectancy: extent to which you expect situation to change
Positive emotions emerge if appraisal assesses potential benefit; negative emotions emerge if appraisal assesses potential harm
OVERVIEW Two-Factor Theory of Emotion BOTH?? wow what a Bop
Emotional response a result of both cognition and biology
First factor: experience of physiological arousal
Try to label arousal to explain feelings, usually accounting for environmental factors
Second factor: decide what to make of feelings
Physiological arousal -> labeling based on environment -> emotion expressed
Key Studies:
LeDoux (1999): Fear in rats
Minor studies: Branchard & Branchard (1972) | Phillips (1964)
Speisman et al. (1964): Audio track interfering with emotion
Schachter & Singer (1962)
LeDoux (1999): Fear in rats
why am i getting ratatouille flashbacks
Aim
To investigate the role of the amygdala
Background/Procedure
Rats conditioned to feel fear when hearing the sound of a bell
Assumption that brain made connection bet. bell and fear
LeDoux lesioned rats to find out which part of brain made connection
Findings
Removal of auditory thalamus caused rats to no longer respond fearfully
Further study showed that lesions on one site of the amygdala were able to stop blood pressure from rising
Conclusion
Biological interactions with emotions
Evaluation
Unethical -- induced fear, lesioning caused physical harm, no right to withdraw
Similar findings with Branchard & Branchard (1972) and Phillips (1964)
B&B: rats lost fear of cats when lesioned the amygdale
Phillips: birds lot fear of humans after amygdala lesion
Speisman et al. (1964): Audio track interfering with emotion
Aim
To investigate how the theory of appraisal can interfere with emotion
Background/Procedure
Participants shown documentary of unpleasant traditional circumcisional ritual
Four groups
Trauma group: shown doc. w/ a soundtrack that emphasized pain
Denial group: shown doc. w/ soundtrack suggesting ritual was joyful and happy
Intellectualization group: shown doc. w/ soundtrack giving anthropological interpretation of ritual
Silent group: shown doc. w/o soundtrack
spooky
Arousal state measured thru galvanic skin response (GSR), a measure of electrical conductivity of skin and good indicator of autonomic arousal and heart rate
Findings
Participants reacted more emotionally in trauma group in comparison to others b/c they evaluated situation to be painful
Thought negative emotions were appropriate b/c of potential harm displayed by situation
Lowest response in intellectualization and silent
Conclusion
Through appraising situation, different emotions can be displayed with the same stimuli
Shows how Theory of Appraisal (and cognition in general) can interfere with emotional response
Evaluation
Lab conditions controlled environment, but low eco validity
Possibility that music affected participants more than actual appraisal of situation
Supports idea that cognitive factors DO interact w/ regard to emotional reponse
Schachter & Singer (1962)
Participants who could not account for emotional high influenced to a greater extent by the confederate
Incorrect labeling of physiological responses
Suggests that physiological arousal can be the same/similar, even w/ entirely different emotions; arousal labeled according to cognition rather than different arousals indicating different emotions
CONCLUSION
Likely both biological and cognitive factors
According to information-processing view of brain, emotion is produced as a cognitive and perceptual process occurring in brain regions like the thalamus, hippocampus, amygdala, and pre-frontal lobe
Supported by LeDoux
Evaluation of situations determines emotion, according to Lazarus’ theory
Despite individual limitations, not much research to suggest that either biology or cognition doesn’t play a role in emotion
Biological: inc in adrenaline causes physiological arousal, leading to increased heart rate and respiration
Cognitive: physiological response labeled according to situational stimuli
0 notes
Text
this is my birth chart i put it here so i dont lose it again Rising Sign is in 22 Degrees Leo You love to be the center of attention and you want to appear strong, confident and dominant. You are very proud of yourself, sometimes quite vain even. When all around you are bedraggled and falling apart, you look like a million bucks! Very dignified and honorable, you enjoy the power and privilege, but not the responsibilities, that come with leadership. You are very idealistic but can also be quite stubborn. Others impress you only if they have integrity (but wealth, power and influence can also turn your head). You prefer rich, elegant surroundings and possessions, and will try to acquire them as your budget allows. Physically, you are very impressive - - at your best you have a regal, charismatic demeanor and bearing. Try not to be such a showoff! Sun is in 06 Degrees Leo. More than a bit of a showoff, you love to be the center of attention! But others do not usually mind because they tend to enjoy your genuine warmth and affection. Very spirited and willful, proud and self-important at times, you demand your own way. You are quite honest, however, and the respect of others is very important to you. You never compromise yourself and you pursue your goals with persistence and dedication. Your regal presence and demeanor draws you to positions of leadership and authority. But beware of being overly hardheaded, domineering, ostentatious or patronizing or you will lose the goodwill and admiration that you enjoy. Very theatrical, you live life on a grand scale wherever and whenever possible. Your strength and energy vitalizes those who come in contact with you. Moon is in 04 Degrees Aries. High-spirited and courageous, you are a fighter when your emotions are aroused. The degree of force and drive that you can bring to any effort sometimes surprises others. You have hair-trigger reactions to specific stimuli and tend to "let it all hang out." You sometimes act before you think and do things on the spur of the moment, and that sometimes gets you into trouble. Your moods change quickly -- you have quite a temper, but you don't hold grudges. Very independent, with an extremely strong and forceful personality, you are known for being impulsive, careless, reckless, foolhardy, rash and daring. Mercury is in 15 Degrees Leo. You are usually quite convinced that your own ideas are correct and you enjoy persuading others that they are. At times, you are very stubborn and proud of your beliefs and principles, and you get very defensive when they are challenged. You appreciate truth and honesty -- you practice it yourself and expect it in others. You have good talent for organizing, directing and planning. You delight in being asked for your advice and counsel. Venus is in 20 Degrees Virgo. You express your love and affection through selfless service to people or causes. You have a tendency to underestimate yourself and doubt your self-worth. This is very demeaning and should be avoided -- learn to love yourself as well as you do others. Your standards of perfection are very high -- you are attracted to relationships based on duty and responsibility. You are supercritical of yourself and others and, at times, prefer to be alone rather than deal with any imperfections in yourself or in those with whom you might relate. Mars is in 10 Degrees Leo. You are a very proud person. Strong, bold, courageous and self-possessed, you love to be the one to initiate significant actions. When people expect a lot of you, you respond positively and will work hard in order to maintain their respect. But when your dignity or pride is threatened, you tend to become sarcastic, arrogant and domineering. Try not to take any challenge or resistance that you meet as a personal affront. You are very stubborn about your right to live your life according to your own principles. Jupiter is in 29 Degrees Cancer. You must be emotionally secure in order to grow and develop. You are happiest when your family and community support and nourish you and boost your morale. Whether your childhood experiences of love and emotional dependability were positive or negative will set the tone for your emotional growth and stability as an adult. When you feel at ease with yourself, you are able to offer assistance to those who need a helping hand. Saturn is in 24 Degrees Gemini. You are such a clear thinker and speaker, with a logical orderly mind, that you are repulsed by abstract, intangible or unorganized thoughts or ideas. But you tend to get uptight about speaking in public because you are afraid to be wrong. Remember that the best way to learn is by making mistakes. Also, you will be so carefully prepared that you probably will not make many mistakes anyway. To be interesting to you, ideas have to be practical and useful. Uranus is in 27 Degrees Aquarius. You, and most of your peer group as well, are reformers at heart. You want to make positive changes that will benefit society as a whole. You are willing to devote your time and energy to see that they come about, especially if the proper group support and combined purpose of will can be found. Be careful that your devotion to group goals does not produce too much friction or neglect in your own interpersonal one-on-one relationships. Neptune is in 09 Degrees Aquarius. You, and your entire generation, will idealize and even venerate the ability to remain detached as well as the ability to objectively analyze any given situation. There will be a concerted effort on your part to cure the ills of society as a whole. But be very careful to continue to maintain and protect the rights of individuals in the midst of these potentially far-reaching changes. Pluto is in 15 Degrees Sagittarius. For your entire generation, society's cherished beliefs and totems will be radically changed. Many traditional concepts will be totally altered, if not completely destroyed. The rights of individuals to pursue their own course in life will be reasserted. N. Node is in 16 Degrees Gemini. You will consciously seek out many different contacts with others throughout your life. Many of these will be of very short duration, not necessarily because you're fickle, but just because you always seem to be more excited by the prospect of meeting someone new rather than prolonging your present relationships. At any rate, you will learn something new from almost everyone you come across -- intellectual stimulation is what you crave from others. You will be well known to neighbors and relatives, partly due to your curiosity about what they're doing -- you delight in keeping up-to-date about the latest news (and gossip).
0 notes
Text
Is Trump hooking your Inner Lizard????
This article supports the video on the brain and creating prejudice in the topic cloud below.
Basically:
the brain allows prejudice and hate to develop, the fuel is the propaganda of the political psychopath.
You have this lizard brain part in you too.
Is Trump hooking your Inner Lizard??
We’ve had a rough year and a half. We’ve endured the sporadic terror attacks in major cities at home and abroad, videos of lethal confrontations between police officers and unarmed black men going viral, ambush attacks on law enforcement officials, the rise of the murder rate in major U.S. cities, and dozens of mass shootings in our streets, schools, and workplaces. News channels and social media have been saturated with either images of violence, or threats of it. So it’s not entirely surprising that the number of Americans worrying “a great deal” about crime is at a 15-year high.
Thankfully, there’s relief to be found once we examine our reality with a more objective lens.
Faced with such overwhelming ugliness, it’s very natural to recoil and feel that the world is falling apart, that we should atavistically embrace the traditions of our ancestors. Every generation has consistently criticized the drivers of modernity, such as science and humanism, as the erosion of things like family values, community in religion, and local customs. Thanks to the work done by people like Harvard Psychologist Steven Pinker in The Better Angels of Our Nature, and economist Max Roser’s Our World in Data, we know that we have continued to push through and improve the human condition. Despite all these achings for the past, more people lead longer and healthier lives, IQ levels are increasing at a rate of three points per decade, global poverty levels have decreased significantly, democracy continues to edge out autocracy as the choice system of governance, and violent death has been on a steady decline.
Yet, we never seem to get this big picture from the media, and why should we? If the majority of schools had mass shootings, then we wouldn’t feature mass shootings on the front pages. Peace and tolerance have become commonplace, and headlines are meant to report events which are considered out of the ordinary. As it happens, uneventful peace is both boring… and ordinary.
It’s worth noting here that some leaders have a vested interest in creating this atmosphere of bedlam, despite what the data have to say. Fear and anger in an electorate sends more people to the polls than does a quiescence for the status quo, or a pining for progress. There are, of course, many components to this anxiety and worry, but much of it is simply an illusion; a vestige of our evolution.
Our lower brain (aka ‘reptilian brain’) is about 200+ million years old, and it’s mainly concerned with survival. When it takes control, and it does, rationality takes a back seat.
We’re prone to dozens of well-documented cognitive biases which regularly drive us to act in an irrational manner. We’re inclined to overestimate the significance of information simply because it’s immediately available to us which, when coupled with millions of citizen journalists, can lead to an overblown appraisal of the state of the world. We also have a natural propensity to listen to arguments that confirm our preconceptions, giving rise to an increasingly polarized society. Then there’s our innate tendency to pay more attention to bad news than good news (which we regularly discount). This negativity bias has a good evolutionary explanation; that is, our survival in the savanna depended heavily on our reactions to negative stimuli. Assuming a rustle in the bushes is a lion can save your life, even if it ends up being no more than a gust of wind.
What Donald Trump has managed to do, perhaps unknowingly, is to capitalize on these cognitive prejudices by continuously misquoting statistics and making up or overstating threats. After painting America as a dark and violent nightmare, he tell his supporters that only he alone can fix it.
Trump has consistently fed us a carefully crafted cocktail of illogic, blatant lies, and his remarkable distaste for words composed of three or more syllables.
Argumentum ad passiones et populum, or arguments which appeal to emotion and to the masses, are classical logical fallacies that have always been used by leaders in order to sway their constituents. In Aristophanes’ satirical play, The Knights, a man is convincing a sausage seller that his lack of education and poor manners make him fit to lead. Unsure of himself, the sausage seller asks how he could possibly be able to govern. The man responds:
“Nothing simpler. Continue your trade. Mix and knead together all the state business as you do for your sausages. To win the people, always cook them some savory that pleases them. Besides, you possess all the attributes of a demagogue; a screeching, horrible voice, a perverse, cross-grained nature and the language of the marketplace. In you all is united which is needful for governing.”
What is meant here by “language of the marketplace” is the capability of relating to the life of the common man. Along with crassness and vulgarity, this is what helps seduce the people into a distrust of political establishments, the media, and unfortunately along with them, experts. For many of his supporters, it doesn’t matter how many lies Trump is called out on. Their candidate will always be the plainspoken one who ‘tells it like it is’.
Falling for the trap of demagogic seduction will likely cost the British after Brexit, and if we’re not careful, we will likely make the same mistakes.
Let’s dispense with the hyperbole and twisted narcissism of thinking that we happen to live in the most dangerous of times. Let’s acknowledge the biases we have, and the mental shortcuts we take, so we can subtract them and better appreciate our objective reality. If we’re serious about the issues facing our country, the prudence of an evidence-based approach, rather than one based on what people are feeling at the time, will yield more informed and calibrated responses. Yes, bad things are happening and there certainly is plenty more work which needs to be done. However, there’s justification and value in looking to the future with optimism, and cherishing the progress we’ve made in creating a safer society; a society that considers positive the principles of religious and ethnic pluralism, civil rights, and social justice. Our ancestors weren’t as lucky.
from
http://bit.ly/2fOrRSk
Psychopaths, Pirates, Vampires, and more:
Run, flee, tell others!
300 topics on this listed below in the Cloud Archive:
Click Here: Catalog of 100 Books, Kindle, Hypnosis Binaural Subliminal CDs
via Blogger http://bit.ly/2fWdDlL #trumppirate #trumpgangster
0 notes
Last Seen Blogs




