#CME Programs
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Mobile Tumblr US users spend an average of 4.04 minutes per session on the app.
Text
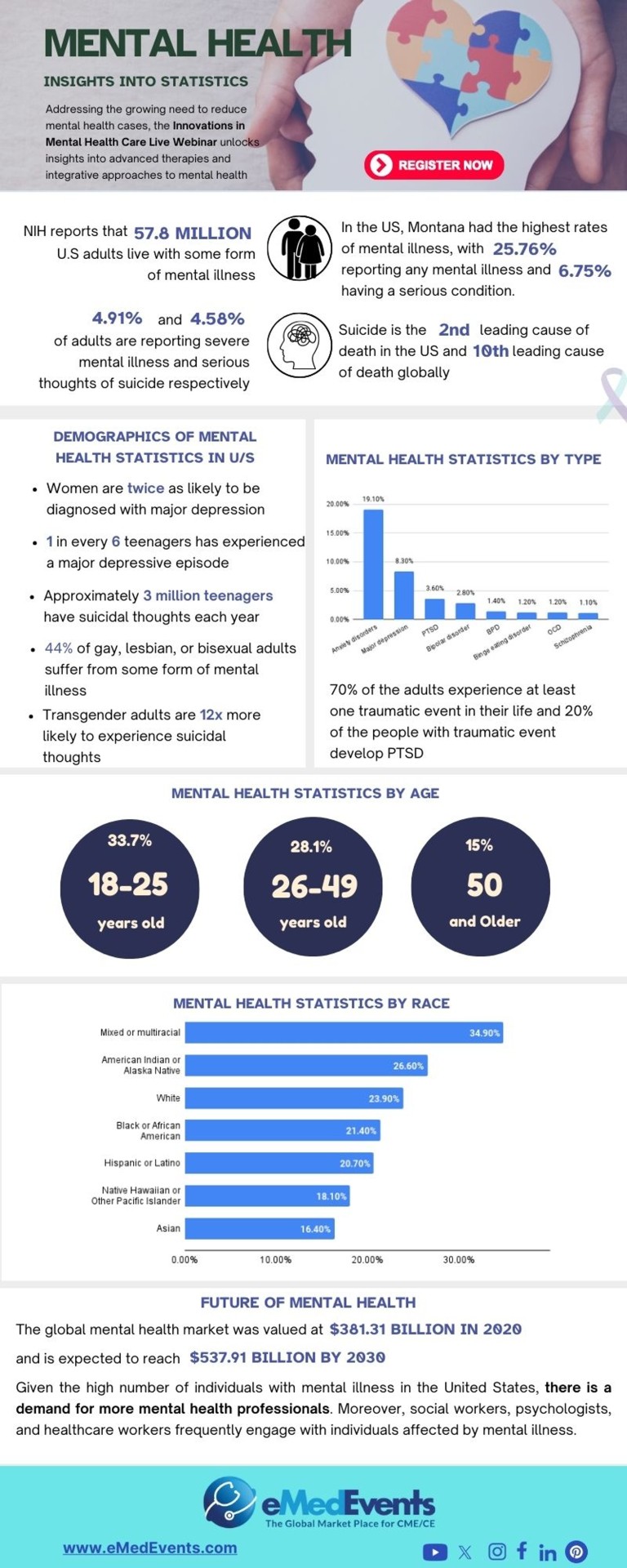
Innovations in Mental Health Webinar Secure your spot for the upcoming mental health live webinar to uncover the advanced therapies and integrative approaches in mental health treatment
#Innovations in Mental Health Care Live#mental health professional#mental illness#psychiatry#neuroscience#Psychiatric Disorders#healthcare webinar#mental health treatment#psychology#CME Programs#CME Conferences#CME Medical courses#CME credits#doctor conferences#medical CME#Primary Care Conference#Medical CME Online#Emergency Medicine Online CME#Medical Conference Website#Physician Conferences#Medical CME Courses#Doctors CME Conferences#CME training for Physicians#Medical Event Organizer#Organizing Medical Events#Medical Conferences#Medical Speakers#Healthcare Marketplace
0 notes
Text
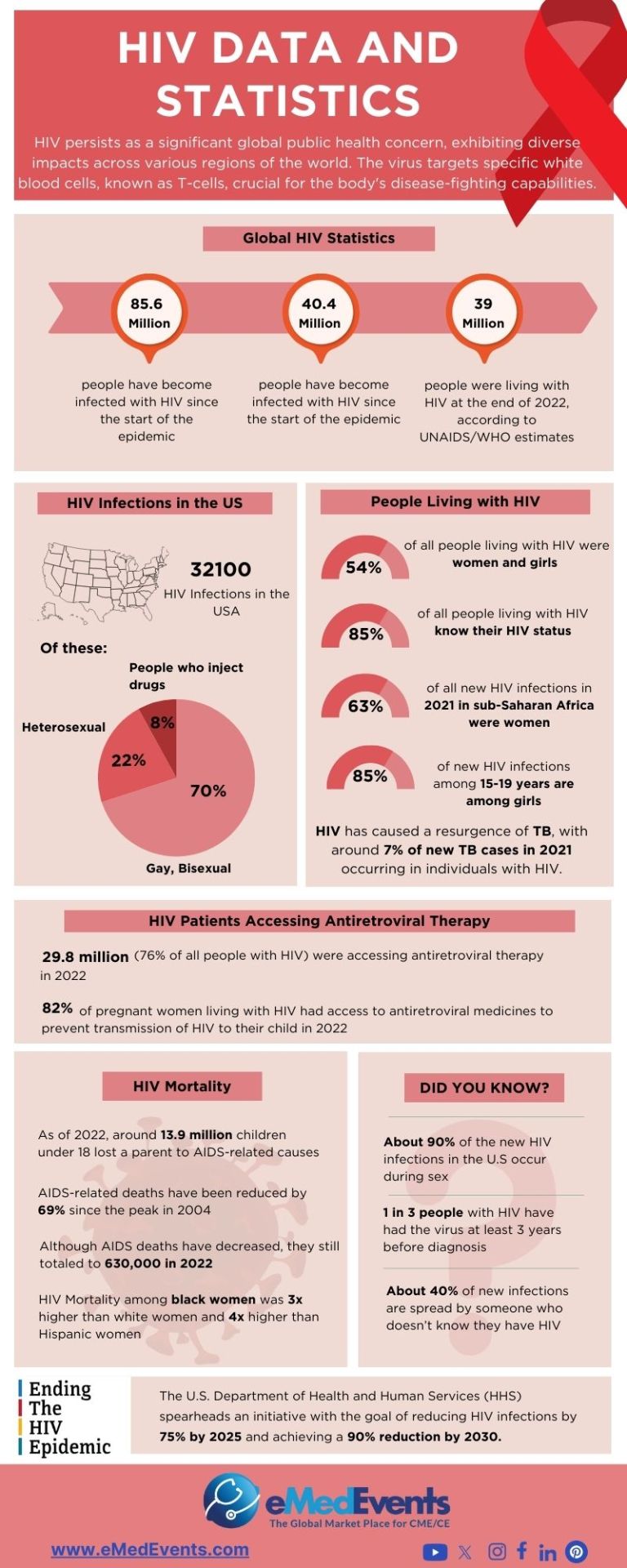
HIV/AIDs Research and Treatment Breakthroughs
Explore the latest breakthroughs in HIV/AIDS research and treatment, that have the potential to reshape the landscape of HIV/AIDS management.
#"HIV/AIDS Research and Treatment#HIV Care#HIV Cure Research#Antiretroviral therapies#current research on HIV/AIDS#CME Programs#CME Conferences#CME Medical courses#CME credits#doctor conferences#medical CME#Primary Care Conference#Medical CME Online#Emergency Medicine Online CME#Medical Conference Website#Physician Conferences#Medical CME Courses#Doctors CME Conferences#CME training for Physicians#Medical Event Organizer#Organizing Medical Events#Medical Conferences#Medical Speakers#Healthcare Marketplace
1 note
·
View note
Text
How to identify the best resource for CME preparation of your choice?
Continuing Medical Education (CME) is an indispensable pillar for healthcare professionals, facilitating the constant evolution and enhancement of their skills and knowledge in a rapidly advancing medical landscape. In today's dynamic healthcare environment, staying abreast of the latest innovations and research is beneficial and essential for optimal patient care.
This article serves as a comprehensive guide, aiming to assist healthcare practitioners in navigating the vast array of available options and pinpointing the best CME resources tailored to their specific learning objectives and professional needs.
Through a strategic and informed selection process, readers will gain insights into identifying and leveraging these top-tier resources, ensuring that their CME journey aligns seamlessly with their aspirations for continued excellence in healthcare practice.
To Know more: CME preparation
1 note
·
View note
Text

i drew this on my phone and spent way too long on it and then it didnt even save so i cant ever edit it again. i still have not seen either movie
original vers below the cut 👍
#i might remake this in my actual art program someday who knows#everything i know abt this guy cmes from twt and ao3 babyyyy#torch chatter#doodle#🕳️🥼| smth smth his holes#💙| real yearning hours#💙| selfship
2 notes
·
View notes
Text
Criminal Minds: Evolution (Recap)
previously on cme
all of season 17 of criminal minds tied up in one unorganized package for your reading pleasure. spoilers coming, duh.

Episode 1: Gold Star
Written by Erica Messer Directed by Doug Aarniokoski
Two weeks following the events of the last season, a man—Bertoli—comes into a police department carrying a dead woman (his wife). She’s been shot and enucleated. When they start to question Bertoli, Emily shows up and suggests that they check his gun. Telling them that there will be a bullet in there with a five-point star etched onto it. That’s the real killers calling card.
The rest of the team is having a birthday party for Penelope, and they’re playing like. Glorified Cards Against Humanity. CME is obsessed with slapstick humor, and it’s very hit or miss.
Rossi is traumatized! He hallucinates Voit being there and taunting him, as Rossi usually does when he gets too emotionally involved in a case. Sigh.
Tyler and Penelope are still flirting, and Luke clocks her for it. Guys, I am so. GIRL, YOU DON’T NEED HIM.
Emily blames herself for Doug Bailey’s death, so she calls Tara in at 12:30. They talk about Gold Star, deducing that Gold Star is a person—an UnSub.
Save me Temily sharing a cigarette on the roof of the FBI. Save me.
The DOJ, specifically Rebecca, is looking into the Bertoli case. She’s communicating with Voit regarding Gold Star.
In the end scene of the last season, Voit was meeting with the director of the FBI (Phil Coulson from the MCU btw), Ray Madison. Gold Star is a top secret case, and since he used Voit’s network to communicate, the BAU needs Voit’s help to catch Gold Star. In return, the Director tells him the DOJ is willing to make a deal with him.
JJ is blonder in this season.
The Sicarius charges are off the table; Voit can never be charged as Sicarius. Cue peepaw crashout.
Tara finds out that Rebecca is communicating with Voit, and they have a fight.
All of the killings that seem to be connected with Gold Star have a calling card, the five-point star etched on a bullet. They go back to Bertoli. Bertoli shoots himself.
The BAU needs to find Gold Star first, or else Voit gets away with everything.
Funnily enough, Luke is the one who suggests they involve Tyler Green with this case. Insane behavior, in my opinion.
Gold Star keeps killing people and it’s very uneventful frankly.
JJ gets to be the first member of the BAU to talk to Voit while he’s in his cage.
Episode 2: Contagion
Written by Matthew Lau Directed by AJ Cook
This season drops the “case of the week” format more than season 16.
Voit doesn’t engage with JJ when she goes into his cell to talk to him about Gold Star. They’re trying to get him to implicate himself so he can be charged as Sicarius.
Two teachers from Provo, UT were killed, and the male victim was enucleated. They can’t figure out why the two teachers were targeted. Rossi and Emily go to Utah and Tara stays to babysit Tyler.
JJ tries to get Voit to cooperate, promising that she’ll get Sydney to open one of his letters. He’s been sending her and the girls mail, but Sydney returns them all unopened. Voit and Gold Star were trading murder techniques over the network, they just needed to get Voit to admit that.
The male victim’s shoelaces were removed, and they propose Gold Star was institutionalized.
The couple’s son talks about a behavioral modification program, but he can’t remember the name. The police find a program called Stuart House, but it doesn’t seem like they’re connected. (Spoiler: they are.)
Rossi interrupts Emily when she tells the police they’re ready to give the profile, and he says they aren’t. When he goes back to talk to her, she tells him, “You never would��ve done that to Hotch.”
Tyler is doing hinky shit again, finding a bunch of fake passports while he’s supposed to be on a stakeout with Tara and Rebecca.
Voit stopped talking again, filing a petition that he won’t talk to JJ anymore. Emily has Luke go in instead of JJ.
So, while we do get the first mention of Stuart House—which is important—the UnSub in this case is not Gold Star. They’re looking for Gold Star as a singular UnSub.
Luke and Voit talk together, and Luke is supposed to seem small and scared, but he doesn’t listen to JJ and Emily and acts resistant because he recognizes Voit doesn’t want to play games. This appeals to Voit, and they actually get somewhere with him!
Voit says Gold Star is more than a serial killer and tells them that their profile is completely wrong and it’s going to get people killed. Voit is fucking with them btw.
Emily asks Aiden to tell them about Gold Star, but Rossi has to shoot him to save his hostage. Penelope says there’s no way that Aiden could’ve been Gold Star because the geographic profiles don’t line up.
Voit whispers something to Luke, telling him he has a secret and he needs to decide if it’s true or false.
Episode 3: Homesick
Written by Sullivan Fitzgerald and Carlton Gillespie Directed by Adam Rodriguez
Voit whispered a website in Luke’s ear that leads to a site on the darknet called BAU Gate. Which includes pictures of members of the team in deepfaked pornography. One member of the team shows up more often than any of the others.
Emily knew about the website, it was a problem she inherited from Hotch.
Someone is leaking information to a conspiracy theorist, it just so happens to be Brian Garrity, Emily’s neighbor from 15x4 “Saturday”. He’s airing theories on Doug Bailey’s death.
There is a case of the week! They’re unrelated to Gold Star, and for that reason, I will be omitting that information from the recap.
Luke tells JJ about BAU Gate even though Emily told him not to, but JJ already knew. Luke is still convinced she doesn’t know how deep it goes and kind of plants a seed of curiosity in her head.
JJ and Luke ask Sydney to talk to Elias in person, but Sydney doesn’t want to talk to him after what he did. Rightfully so. She wants to protect herself and her daughters, Luke talks to Holly and Harlow, Holly is angry, and Luke realizes it goes past usual teenage angst and she’s hiding something. She’s been hurting herself.
Emily meets with Brian, trying to get him to tell her who is leaking the information about Doug Bailey. Someone was taking surveillance photos of them!
Emily mentions that Doug had a brother okay this is important for later.
Sydney find out Holly is hurting herself and decides to help the BAU because the thinks she’s 1. Taking back power and 2. It might convince the government to get them into WITSEC faster.
JJ gets curious and looks up the BAU Gate website.
Emily goes to meet with Brian again, but he gets attacked while they’re talking. He tells the police that she attacked him.
Episode 4: Kingdom of the Blind
Written by Chikodili Agwuna and Jayne A. Archer Directed by Joe Mantegna
We are in Jackpot, Nevada, and we get to see my favorite character. My number one: “They did nothing wrong.” Jade Waters.
She tricks a man into helping her by pretending to be stranded on the side of the road, and she attacks him while he’s looking at her car. She takes his deputy badge before bludgeoning him to death while banshee screaming.
Emily gets her mugshot taken. How much do you wanna bet Luke printed it out and posted it on the fridge in the BAU?
Tyler is up to fuck shit again, he’s trying to find Gold Star using non-FBI approved methods and Penelope is not having any of it.
Rossi keeps hallucinating Voit while he goes to pick Emily up from MPD.
JJ is super out of it, this is because of the BAU Gate thing. She’s spacing out and is very reserved.
Sydney and Elias meet in prison, and she genuinely wants nothing to do with him. She tells him that Holly’s hurting herself and he’s concerned but she doesn’t take anything he does seriously. They got into WITSEC so Sydney tells him this is the last time they’ll see each other.
The team gets called into the case in Nevada! They say it’s not Gold Star until they prove it.
Jade gives herself stick and poke tattoos every time she kills someone.
Penelope has to jailbreak a phone that Tyler illegally cloned from someone who was involved in Gold Star. He helps her get into the information on the phone.
Sydney and the girls go to talk with Elias. Harlow is willing to hug and talk but Holly is not.
There was tattoo ink in the enucleated victim’s eyes. Jade used a tattoo needle to gouge out his eyes. She’s so dreamy.
Tara concludes that the UnSub is a woman and decides that it definitely can’t be Gold Star because it’s a woman.
Holly figures out that Voit is evil even though they were trying to hide the truth from her. She has him read a letter in which she calls him a serial killer murderer, and then she pulls a blade out AND TRIES TO KILL HIM. Voit is horrified at the idea of Holly becoming like him and begs Luke to help her.
Holly did nothing wrong imo.
Brian Garrity referred to Gold Star as a program instead of an individual, which makes the team start to rethink it. Then they find that Jade’s two most recent victims both worked at Stuart House, the same place that they found/killed Aiden Keller in episode 2. They reanalyze that case, now believing they are all connected. They’re all revenge kills, and they go back to Salt Lake City to revisit Stuart House.
Jade is back <3
She slashes a man’s tires, standing up and greeting him as her father. He knows what she did in Nevada, and she calls herself a daddy’s girl before he tells her to get in the car.
Frankly, I don’t care for Tyler and Penelope and their dynamic, but here I am forced to watch them yap at each other.
Someone saw Jade get into her father’s car, and they identify her through him. Noting that she spent time at Stuart House as a child. They find the car on the side of the road with Rick Waters inside of it. She killed him.
He brought her out to the same place where he killed her mother before she shot and killed him. When she tried to report him for her mother’s murder, he had her committed to Stuart House.
Jade is targeted by someone who has a gold star etched into their bullet. (Hmmmmmm). He covers her mouth and it turns out his name is Damien. He killed someone for her because they were being targeted by the people who have been getting killed. Damien is the one they’ve been profiling as Gold Star.
Gold Star is a strike team with five members, and the Gold Star killers consist of five kids who were at Stuart House, two of whom are Aiden Keller and Jade Waters. The kids are planning a reunion.
Emily tries to get Voit to contact Damien, and they arrange for Holly to get one-on-one treatment with a bureau program. However, in order to contact Damien, Voit needs to be let out of his cell. Sigh.
Whew that was a lot.
Episode 5: Conspiracy vs. Theory
Written by Breen Frazier Directed by Sharat Raju
So! Voit is out of prison and is brought to Quantico to connect with Damien and lead the team to him and Jade. Voit comes in and directs them on how to find Damien through a backdoor on an innocuous website.
Voit talks to Damien and tries to convince him to meet in person. Damien is hesitant because Voit always told him that remaining anonymous is the best method to not get caught. While he’s on the call, Voit taps on the desk in the BAU in Morse code, sending Damien a message about the next target being North Star.
Once they clock that, Emily and Rossi wonder if they can use the message to benefit them somehow, but it just pisses Luke off because he decodes the message before Dave and Emily say anything.
Rebecca wants to send Voit back to prison, but Rossi comes out and suggests that Voit travel with them to meet with Damien. He’s coming up with a plan to kill Voit, scheming to tempt him with escape, leaving him no choice but to shoot him.
They bring Voit on the plane, and while he’s on it, he pokes and prods at the team. Namely Luke, who he pesters by bringing up Tyler and Penelope’s connection (Garvez is real, I scream as the nice men in the white coats drag me away).
While the rest of the team flies with Voit, Emily and Tyler (who is, begrudgingly, now a permanent fixture here) meet with Brian Garrity to see why he framed Emily and what he knows about Gold Star.
I made dinner during this episode, so my notes are slightly lackluster, but we are back now, hello.
Forgot to mention that Damien and Jade are loversssss.
Garrity won’t talk to Emily and asks for a lawyer (he’s not even under arrest).
In Iowa, they send Voit into a park to meet with Damien—the extent to which they want to kill Voit is almost comedic. Like I get it. But also.
The plan goes wrong, of course. Jade and Damien sent someone out there with a bomb strapped to his chest to create a distraction. Naturally.
Jade and Voit talk on the phone, Jade and Damien think he lied about North Star. Voit does a classic “I know why you do this” profiling technique that he probably learned from Rossi’s books to try to trick Jade.
Penelope blocks the cell signal from setting off the bomb, and Jade walks away. Right past two police cruisers.
Voit thinks about running, but he sees the rifle trained on him and surrenders.
Damien poses as a local officer and gets into the armored truck that Voit is in before asking him how to get North Star.
Garrity tells Emily that his informant told him “Teresa is in trouble.” This leads Tyler to make a phone call to an unknown person and says, “You might be in trouble.”
Emily gets put on restricted duty, and the director puts Rossi back in charge of the BAU. She crashes out about how she feels like she’s losing her values. And peepaw comforts her.
Episode 6: Message in a Bottle
Written by Sullivan Fitzgerald and Carlton Gillespie Directed by Nelson McCormick
Rossi has a nightmare where Voit overpowers the guards at the prison and kills the rest of the team in front of him. Specifically shooting Emily and Rossi.
Rossi’s gun doesn’t work, just like Spencer’s season 15 dream, which Reid’s therapist says is a very common law enforcement dream.
Emily goes full crashout and eventually ends up sleeping on Garcia’s couch, Penelope puts a bucket in front of her before going to work.
Rossi’s hallucinations get worse. This man is withering away so bad I keep thinking he’s about to kick it lol.
JJ catches on that Penelope knows something about Emily, so she gets Penelope to hand over her keys.
Tyler brings a mystery woman (Teresa, the person he called at the end of the last episode; ex gf) into the BAU and enlists Luke to help him. Luke really does not like Tyler. Agree.
JJ goes to Penelope’s apartment to find Emily and very innocently eats a Cheeto puff off the counter. Emily is very high, and the Cheeto was an edible.
Emily eats chips with chopsticks, and I’d like to let you know that I do the same thing with nearly everything.
JJ middle names Emily. Emily Elizabeth. I can’t think about it without thinking of Clifford the Big Red Dog.
Tara and Rossi talk about his delusions of grandeur, and she tells him he’s traumatized (wbk) and needs to confront Voit.
JJ eats like the whole bag of edibles not knowing. You guys are gonna lose your jobs. Emily says she’s gonna quit the FBI but JJ tells her she shouldn’t make any big decisions right now.
Emily has never read The Catcher in the Rye and she’s better off for it.
Rossi imagines he gets trapped in the elevator and is buried alive. Guys. I did it first. Run me my check.
This is kind of a filler episode and just an excuse to do the jemily scene and build “tension” between Luke, Penelope, and Tyler.
I’m assuming if you’re a fan of this show or of jemily even you know the “It gives me you” scene so. I don’t need to recount it for you. Surely.
The hat man is coming for me.
Voit and Rossi talk about why he mentioned Gold Star to Douglas Bailey and also why Rossi can’t seem to get Voit out of his head. Voit pretty much just fucks with him the whole time.
LUKE IS IN LOVE WITH PENELOPEEEEEEEEE!!!!!!!!!!! GARVEZZZZZZZZ
Tyler sets up a sting for someone from his old life, kind of signifying him crossing over to the FBI and leaving behind his life of crime. Then Rossi calls an all-hands meeting and includes Tyler, further solidifying this.
In the 90s, Gideon and Rossi were enlisted to produce a report that could basically create serial killers. They never published it because it sounded like a recipe. Someone got ahold of the drafts and created the Gold Star killers.
North Star is the BAU. It all leads back to them.
Episode 7: Piranha
Written by Chikodili Agwuna and Jayne A. Archer Directed by Aisha Tyler
Right away. There is a case of the week in this episode, but it is so graphic and disturbing that I don’t want to recap it. Like there’s even a warning at the beginning of the episode. I’m not usually one to be icked out by graphic CM episodes, but this one is too much for me.
It’s one of those episodes with a twist where you can’t stop thinking about how fucked up it is.
The team starts talking about the white paper that Rossi and Gideon wrote, they all are uncomfortable with the fact that their research influenced Gold Star.
Rossi shows Emily all of the paper files that the BAU used in the 90s and they have to go through them. He tells her they didn’t have a Penelope Garcia back then, they had Jill. First name only, but apparently the BAU cost her more than Emily and Rossi combined.
The white paper studied epigenetics, or specifically situational psychopathy.
Emily asks Tyler to come with her to recruit Jill Gideon even though Rossi told her to leave her out of it. She was the only therapist that Jason trusted even after they divorced.
Voit meets with his lawyer, and Voit suggests he could have the lawyer’s wife (whom he’s separated from) disappear if the lawyer helps him get his deal with the FBI to go through.
When Emily goes to Jill’s door, there’s this funny scene where Jill asks about Hotch, Derek, and Spencer and Emily has to be like uhhhhh well.
Jill and Rossi had an affair while she was still married to Jason. She’s the reason that Rossi left the BAU. Jill refuses to go back to the BAU, but when Tyler comes in, she realizes that Emily is trying to manipulate her because Tyler looks a little bit like Stephen. It works.
Voit coerces his lawyer to dig up a kill kit to kill his wife. He’s going to pass the job over to Damien. Voit tells his lawyer not to open the case, but the lawyer does anyway.
Jill returns to the BAU.
Episode 8: North Star
Written by Charles Dewey and Christopher Barbour Directed by Zach Gilford
Jade Waters frantically knocks on a man’s door, telling him someone’s after her. It’s a ruse, of course, Damien and Jade blocked his cell signal and his phone line. It’s safe to assume he was involved in Gold Star/Stuart House. Jade bludgeons him <3
I think the weird tension between David and Jill is weird and unnecessary like why the fuck did David Rossi need to spread it around so bad. He had three wives but needed his best friend’s wife too. Skip!
Jade Waters, I am free on Thursday night and would like to hang out. Please respond to this and then hang out with me on Thursday night when I’m free.
I think they go a little too crazy with the cursing in evolution but it is satisfying when things go awry to hear JJ say shit. Like yeah. Shit.
Jade has a nightmare from what happened in Stuart House, and she and Damien promise each other that they’ll never go back into a cage. So, if one of them gets caught, the other will kill them before they’re contained. OoooHhOhOo foreshadowing!
Basically, Jill worked to build the Gold Star program without knowing what they were doing, and Jade and Damien are systematically working to kill every person who took part in that. Jill is also on their hit list.
Damien sees Rossi with Jill and thinks that the FBI is involved in Gold Star, but Jill had no idea what was happening.
Voit’s lawyer, Vincent, had been communicating with Sicarius on the network, all of the messages and photos were traced back to Vincent’s IP address. Vincent is into torture porn, which is why Voit gets to blackmail him into doing whatever he wants.
You can tell the pacing is weird in this season. They should’ve figured out the North Star thing earlier.
Rossi didn’t go to Gideon’s funeral because he couldn’t see her.
Damien Booth had to kill his foster father, the only person who ever tried to protect him, as his final task to “graduate” from Stuart House and make sure that his conditioning was complete.
Damien comes to Jill’s house, and she asks him if she can show him something. He lets her take him somewhere, they go to Gideon’s cabin. I fear she wanted to go there so she could die in the same place Jason died.
Jill tells Damien that he was tricked into killing his foster father, but reassures him that he did what he needed to do to survive. She convinces him to put his gun down, but he knows the FBI is probably after them at this point. He knows they’re not going to let him go, and because of the deal he made with Jade, he knows he’s going to die. It’s such a shame because I was really rooting for him to make it.
Jade shoots him and she gets away.
Y’all you really can’t see shit in this show. I know it’s nighttime but oh my god.
Episode 9: Stars & Stripes
Written by Christopher Barbour Directed by Bethany Rooney
Jade’s crashing out—free my girl from her brain. She gets pulled over in Maryland for speeding, and when he asks for her license and registration, he asks her to get out of the car. He identifies her, and another girl comes out of the car. The other girl shoots him, and Jade stabs him in the eye with her tattoo needle.
Can’t believe the CME budget ran out and they can’t afford lights anymore.
Voit is going to be sent to a comfy federal prison. The team can’t allow that to happen.
Spencer mention <3 I’d be upset that they bring him up to info dump even when he’s not there but Penelope is the one who does it so it’s fun.
Financially, Penelope connects all of the victims to a company called Aida Limited and the man in charge, Frank Church. They figure that him and Aida are the ones who paid the strike team to take out the Gold Stars.
The team investigates the trooper that Jade and the other girl killed and enucleated, they left him alive and told him to only speak to the FBI. Since there’s only one other female Gold Star left, the other girl is Dana, GS-Four.
Jade and Dana go to the shipping container that Voit’s lawyer led them to, inside of it, there is a wall with the BAU’s pictures plastered to it. Including photos of Tyler Green. Jade and Dana are going to look for Peter, GS-Three.
Dana tells Jade they need help to “defeat” the BAU at the end of the conspiracy and they need to go home.
The message that Jade left with the trooper is that she never wanted to hurt anyone and she just wants to go home. Leaving him alive was the last of her mercy, and if they come after her, the streets will run with their blood.
They’re going to go after them. So.
Their home is Aida, and the “puppet master�� in question is Frank Church.
They recover a polystyrene case from Jade’s stolen car. Finally connecting that Voit had been helping Damien and Jade.
The team finds the shipping container/bunker, seeing all of the photos that implicate the entire team. It’s reminiscent of the scene in season 8 when the team finds The Replicator’s shrine.
Frank Church literally reeeeeks of evil guy. Conniving and slimy and evil!!!!
Penelope says Church has rizz. Like in the way Jim Jones did. Cult rizz.
Since Church trashed his old group of killers, he’s started collecting a new group of damaged teenagers to manipulate and kill. This show is so dark and twisted I hate it here.
Dana and Jade go back to Frank Church, and they don’t know that he’s evil. He sends Jade to the dormitories and kills Dana.
Jade sees another girl, Mila, and she sees Church tell her things that she recognizes hearing in Stuart House. My girl clocks his bullshit because he uses the word conspiracy. She hasn’t figured out that he’s the one who sent the strike team yet, but she’s suspicious.
Mila talks to Jade and asks her about her nightmares, saying her nightmares feel real. She describes an experience that Jade also had, except Mila says she sees Church when her goggles slip off. It’s not a dream, and Church is a pedophile!
In a flashback, we see that Damien was the first person to suggest that Church was the person hurting them the entire time. He was, how you say… right.
Jade witnesses shit and gets tased, so. We can kind of imagine what happens and I won’t detail it for you. She runs when she wakes up, the BAU is surrounding the building.
Jade wakes Mila and tells her to get all of the kids out.
There’s a reference to Benjamin Cyrus. For shits and giggles.
Jade rigs the building to blow up, she’s fully figured out what’s going on. She tells Mila via radio that she needs to keep running and needs to save the children.
Episode 10: Save the Children
Written by Breen Frazier Directed by Glenn Kershaw
Huge explosion and there’s no contact with the team.
Everyone is fine considering they were in an explosion.
Except Emily was kidnapped. There’s that.
Jade declares herself judge, jury, and executioner and kills Church after charging him with the crime of pedophilia. It’s safe to assume that Emily is next.
They’re missing one Gold Star, so Peter has to be the person Jade is teaming up with now.
Unfortunately, I’m eating dinner while watching this episode but most of it is just flashbacks that don’t change the story much except for the emotional depth.
Jade has Emily, charging her with conspiracy to commit murder. She knows her whole back story, Benjamin Cyrus, Ian Doyle, Peter Lewis, she knows it all, but Emily says she’s allowed due process or else Jade is just as bad as all of the people she’s up against.
The team figures out that Emily is just as important as Frank, but while Frank was important to Jade, Emily is important to Peter B.
Voit gets moved to Collymore FCI. He’s in a nice cushy room where he’s allowed to have décor. Literally club fed. It’s nicer than my freshman dorm.
Peter B. Is Peter Bailey! Douglas Bailey’s younger brother. Which is why he knew about Gold Star, and Pete holds Emily responsible for Voit killing Doug.
Flashback to Doug and Emily talking to each other, he mentions his brother and this is where we get the strange lore drop that Emily has a sister. Presumably younger.
I recognize the actor who plays Pete. Who is that. Oh my god. This is gonna bug me. Someone remind me to look it up later.
Doug was looking into Gold Star because he knew his brother was in it, and the only person he confided in about Gold Star and his brother was the director of the FBI, Ray Madison. Now, Madison tells Rebecca and David that he couldn’t possibly tell anyone about it because it was classified information. Dave tells him that if something happens to Prentiss, there’s no classification in the world that will save him. Madison thinks he’s talking about his career, but he’s talking about his life. Uncommon David Rossi W.
Madison says he’ll go to the mat for them, realizing he got caught with his pants down.
Voit wants to be let into gen pop and makes a deal to get them information on Emily’s location. Voit comes into the BAU again.
“Back at it like a crack addict!”
Pete was the one behind using Brian Garrity against Emily AND the one who sent the message “Teresa is in trouble.”
There are so many names involved at this point ohhhhh my god.
Voit tries to get into JJ’s head using stuff about the BAU gate, and she doesn’t let him even though it bothers her. Voit made the videos on BAU gate by basically… editing JJ’s face on his wife’s body. She scares the fuck out of him. I love women.
Jade pulls the gun on Emily again, but says they’re delaying her sentence so they can wait for her team and kill all of them in one go. The team figures out it’s a trap and looks for another way in. They show Pete the video where Voit admitted to killing Doug by having Penelope hack into his screen.
Pete tells Jade to stand down, and she says no. He doesn’t mind dying, but he won’t die over a lie. Pete lets Emily go, and when the FBI comes in, Jade holds a gun to her head and wonders if everything is a lie. Emily empathizes with her over shared experience.
Emily tells her they need her to tell them about Damien and Stuart House and that she saved Mila’s life. Pete and Jade are arrested and alive.
Mila and reunite L babies. Pete reunites with his parents. That was what Emily wanted instead of sending them to prison.
Tyler applied to work at the FBI. Eugh.
Rebecca has cunty bangs now. She and Tara are back together.
The team is partying and they’re like “Whyyyy does Voit want to be in gen pop??”
Well. I’ll tell you. It’s because he wanted his shit wrecked. He gets attacked in prison because some people figure out who he is, but it’s not really explained how, and the season ends with him getting stabbed.
#criminal minds#criminal minds evolution#cme#criminal minds: evolution#criminal minds evolution recap#cme recap#criminal minds season 17
8 notes
·
View notes
Text
Remember that 737 MAX whose door plug blew out in flight?
A boeing whistleblower created a burner account and reported the following (reproduced here in its entirety in case the original gets deleted):
Current Boeing employee here – I will save you waiting two years for the NTSB report to come out and give it to you for free: the reason the door blew off is stated in black and white in Boeings own records. It is also very, very stupid and speaks volumes about the quality culture at certain portions of the business.
A couple of things to cover before we begin:
Q1) Why should we believe you? A) You shouldn’t, I’m some random throwaway account, do your own due diligence. Others who work at Boeing can verify what I say is true, but all I ask is you consider the following based on its own merits.
Q2) Why are you doing this? A) Because there are many cultures at Boeing, and while the executive culture may be throughly compromised since we were bought by McD, there are many other people who still push for a quality product with cutting edge design. My hope is that this is the wake up call that finally forces the Board to take decisive action, and remove the executives that are resisting the necessary cultural changes to return to a company that values safety and quality above schedule.
With that out of the way… why did the left hand (LH) mid-exit door plug blow off of the 737-9 registered as N704AL? Simple- as has been covered in a number of articles and videos across aviation channels, there are 4 bolts that prevent the mid-exit door plug from sliding up off of the door stop fittings that take the actual pressurization loads in flight, and these 4 bolts were not installed when Boeing delivered the airplane, our own records reflect this.
The mid-exit doors on a 737-9 of both the regular and plug variety come from Spirit already installed in what is supposed to be the final configuration and in the Renton factory, there is a job for the doors team to verify this “final” install and rigging meets drawing requirements. In a healthy production system, this would be a “belt and suspenders” sort of check, but the 737 production system is quite far from healthy, its a rambling, shambling, disaster waiting to happen. As a result, this check job that should find minimal defects has in the past 365 calendar days recorded 392 nonconforming findings on 737 mid fuselage door installations (so both actual doors for the high density configs, and plugs like the one that blew out). That is a hideously high and very alarming number, and if our quality system on 737 was healthy, it would have stopped the line and driven the issue back to supplier after the first few instances. Obviously, this did not happen. Now, on the incident aircraft this check job was completed on 31 August 2023, and did turn up discrepancies, but on the RH side door, not the LH that actually failed. I could blame the team for missing certain details, but given the enormous volume of defects they were already finding and fixing, it was inevitable something would slip through- and on the incident aircraft something did. I know what you are thinking at this point, but grab some popcorn because there is a plot twist coming up.
The next day on 1 September 2023 a different team (remember 737s flow through the factory quite quickly, 24 hours completely changes who is working on the plane) wrote up a finding for damaged and improperly installed rivets on the LH mid-exit door of the incident aircraft.
A brief aside to explain two of the record systems Boeing uses in production. The first is a program called CMES which stands for something boring and unimportant but what is important is that CMES is the sole authoritative repository for airplane build records (except on 787 which uses a different program). If a build record in CMES says something was built, inspected, and stamped in accordance with the drawing, then the airplane damn well better be per drawing. The second is a program called SAT, which also stands for something boring and unimportant but what is important is that SAT is *not* an authoritative records system, its a bullentin board where various things affecting the airplane build get posted about and updated with resolutions. You can think of it sort of like a idiots version of Slack or something. Wise readers will already be shuddering and wondering how many consultants were involved, because, yes SAT is a *management visibilty tool*. Like any good management visibilty tool, SAT can generate metrics, lots of metrics, and oh God do Boeing managers love their metrics. As a result, SAT postings are the primary topic of discussion at most daily status meetings, and the whole system is perceived as being extremely important despite, I reiterate, it holding no actual authority at all.
We now return to our incident aircraft, which was written up for having defective rivets on the LH mid-exit door. Now as is standard practice kn Renton (but not to my knowledge in Everett on wide bodies) this write-up happened in two forms, one in CMES, which is the correct venue, and once in SAT to “coordinate the response” but really as a behind-covering measure so the manager of the team that wrote it can show his boss he’s shoved the problem onto someone else. Because there are so many problems with the Spirit build in the 737, Spirit has teams on site in Renton performing warranty work for all of their shoddy quality, and this SAT promptly gets shunted into their queue as a warranty item. Lots of bickering ensues in the SAT messages, and it takes a bit for Spirit to get to the work package. Once they have finished, they send it back to a Boeing QA for final acceptance, but then Malicious Stupid Happens! The Boeing QA writes another record in CMES (again, the correct venue) stating (with pictures) that Spirit has not actually reworked the discrepant rivets, they *just painted over the defects*. In Boeing production speak, this is a “process failure”. For an A&P mechanic at an airline, this would be called “federal crime”.
Presented with evidence of their malfeasance, Spirit reopens the package and admits that not only did they not rework the rivets properly, there is a damaged pressure seal they need to replace (who damaged it, and when it was damaged is not clear to me). The big deal with this seal, at least according to frantic SAT postings, is the part is not on hand, and will need to be ordered, which is going to impact schedule, and (reading between the lines here) Management is Not Happy. 1/2
2/2
However, more critical for purposes of the accident investigation, the pressure seal is unsurprisingly sandwiched between the plug and the fuselage, and you cannot replace it without opening the door plug to gain access. All of this conversation is documented in increasingly aggressive posts in the SAT, but finally we get to the damning entry which reads something along the lines of “coordinating with the doors team to determine if the door will have to be removed entirely, or just opened. If it is removed then a Removal will have to be written.” Note: a Removal is a type of record in CMES that requires formal sign off from QA that the airplane been restored to drawing requirements.
If you have been paying attention to this situation closely, you may be able to spot the critical error: regardless of whether the door is simply opened or removed entirely, the 4 retaining bolts that keep it from sliding off of the door stops have to be pulled out. A removal should be written in either case for QA to verify install, but as it turns out, someone (exactly who will be a fun question for investigators) decides that the door only needs to be opened, and no formal Removal is generated in CMES (the reason for which is unclear, and a major process failure). Therefore, in the official build records of the airplane, a pressure seal that cannot be accessed without opening the door (and thereby removing retaining bolts) is documented as being replaced, but the door is never officially opened and thus no QA inspection is required. This entire sequence is documented in the SAT, and the nonconformance records in CMES address the damaged rivets and pressure seal, but at no point is the verification job reopened, or is any record of removed retention bolts created, despite it this being a physical impossibility. Finally with Spirit completing their work to Boeing QAs satisfaction, the two rivet-related records in CMES are stamped complete, and the SAT closed on 19 September 2023. No record or comment regarding the retention bolts is made.
I told you it was stupid.
So, where are the bolts? Probably sitting forgotten and unlabeled (because there is no formal record number to label them with) on a work-in-progress bench, unless someone already tossed them in the scrap bin to tidy up.
There’s lots more to be said about the culture that enabled this to happened, but thats the basic details of what happened, the NTSB report will say it in more elegant terms in a few years.
69 notes
·
View notes
Text
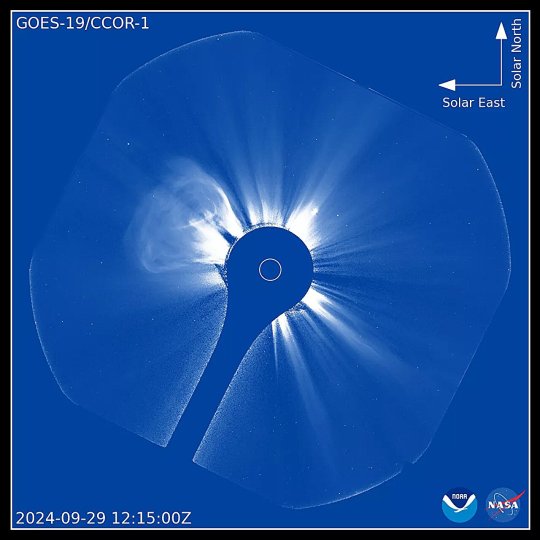
NOAA releases imagery from world's first operational space-based coronagraph
NOAA today shared the first images from the Compact Coronagraph (CCOR-1), a powerful solar telescope onboard the new GOES-19 satellite. CCOR-1, the world's first operational, space-based coronagraph, began observing the sun's corona, the faint outermost layer of the solar atmosphere, on September 19, 2024.
CCOR-1 monitors the corona to forecast coronal mass ejections (CMEs), which are large expulsions of plasma and magnetic fields from the sun that can produce space weather impacts on Earth.
When directed toward Earth, CMEs can cause geomagnetic storms and other types of space weather that can impact satellites, navigation systems like GPS/GNSS, astronaut safety, aviation communications and electric power grids. On Earth, the familiar aurora displays are the visible manifestations of these storms interacting with Earth's upper atmosphere.
CCOR-1 delivers uninterrupted coverage of the corona with a new image every 15 minutes. CCOR-1 uses an occulting disk (the dark blue circle at the center of the video) to eclipse the sun (depicted as the smaller white circle) so we can view the extremely faint corona.
The sun also dazzles with its small and large streamers, bright radial structures along which the solar plasma travels steadily outward. The CME explosions bend and sometimes disrupt the streaming plasma, buzzing past it at speeds of hundreds to thousands of miles per second.
CCOR-1 is the first in a series of NOAA coronagraphs. Similar instruments will be placed on the sun-Earth line and around the sun, as part of NOAA's Space Weather Follow-On and Space Weather Next programs, respectively.
GOES-19 is currently undergoing post-launch testing and checkout of its instruments and systems. After GOES-19 is assigned the operational role as NOAA's GOES East satellite in spring 2025, NOAA's Space Weather Prediction Center will begin using CCOR-1 observations to inform and improve its forecasts and warnings of impending space weather.
6 notes
·
View notes
Text
CME 17x02 Spoilers/Thoughts
(there's a couple of theories I have regarding this ep that I will get to in a bit, but feel free to send in some if you have something now. Once again, I am late to posting this lol but I gotta do it before the next ep. Admittedly, part of it is a rewatch lol. And some revised stuff)
“Directed by A.J. Cook” let’s fucking goooooo!
Ok I'm also studying AJ's directing choices bc I love it so much and rewatching it is so much better now that I have some more thoughts
Okayyyy, I am still not enjoying this enucleation thing. I have a weird thing with eyes that I don't enjoy seeing
That is so fucking closeeeee ughhhh, damn AJ (love the suspense tho)
Ok JJ standing in the video like that is kinda funny ngl. She's just like 🧍♀️
"run his... big mouth" JJ you wanted to say "his fucking mouth" I just know you do
Marriage, kids.... I knew this would play out in some way, I've been saying this since s16!!
JJ and Luke team up!!
I love the continuous shot in the beginning (I'm no film major and I only have limited knowledge through like a few electives in film lol)
Tyler and Rebecca were kinda funny in this continuous shot haha
Yeah Garcia, I agree upon seeing those photos ugh
Babysitting Tyler ("not you Garcia", "I don't want to do it") 😂
Yessss JJ vs. Voit interrogation scene!!!
Luke and JJ pretending to be a couple pretty much reminds me of Derek and JJ pretending to be one in s9. I love their team up!
"Come on, it's so good" I'm sorry, I'm having thoughts with the way she said it 😳
She's got eyes in the back of her head, that's the mom thing I swear. Like that one ep in s8 with the girl in the house who killed her sister and faked trauma and she heard her coming.
"Not your wife, maybe." Yesss get him girl
JJ looks so good in this. I had to rewatch this bc I wasn't paying so much attention until halfway through lol
Now my evolution jemily fic is looking pretty good with what's happening so far...
"That hurts my feelings. That you think I care enough about you to betray my oath." That may be hinting something... and also get him girlll
Ulterior motive that he might try and find... and JJ just looks at him with a straight face
JJ smiling when he agrees to see the file
She looks taller than him (and I know it's her shoes but it's still funny)
Them walking away at the same time, love it! AJ's directing choices here! She knew what she was doing.
Jemily interaction (over the phone) love it!! Hey at least JJ's calling Emily by her first name and not Prentiss, so that's good 😂
"We'll get him on the record, Emily" "ok", they're so soft signing off, I'm sorry
Utahhhh (never been actually lol)
Emily being so confused hearing her name and going "ok" when Rossi hallucinated Elias 🤣
Emily is going to have some tunnel vision on the Gold Star case. She's dead set on it being connected to Gold Star.
Tyler and Tara are actually pretty funny in the car scenes ngl
Then we throw Rebecca in it. It's awkward haha
I know a lot of people have some thoughts on Tebecca and Tyler just as a character, but I honestly loved their car scenes together. It's pretty fucking hilarious and AJ having to direct them is so good.
Tyler did work in Afghanistan, so did JJ.... 👀 It wasn't mentioned when tho I don't think
"It's her deodorant" omg. Tyler feels so awkward hanging with both of them lol. Also wtf Tara 😂
"what do you see?" "Your obsolescence"
JJ's "I should've known" look, my girlllll
Voit is looking scared and quickly denies it.
JJ being a smartass back at him yessss
"Yes I do" "No you don't" with the scoff
Social contagion
JJ was so done with him
JJ was getting closer and he knew it.
Emily with a kid!!
Idk if this is intentional but the kid talking about his guilt and Emily talking to him and saying it's not his fault. Emily.... you (and like JJ and Rossi) need to listen to your own words
Behavioral modification program?
Ok I have mixed feelings about the whole scene with Rossi and Emily. Rossi shouldn't have done that in front of the officer yes, but also this whole time, Emily's been super biased and set on the fact that it could be Gold Star. Like yeah, it's embarrassing to have that happen publicly and I would've reacted the same as Emily tbh, but they still don't have the whole profile on Gold Star. How sure could she be? (just saying it here now: the case ended up not being connected to Gold Star)
Rebecca's phone going off and Tara calling her out on it lol
Poor Tyler (never thought I'd say that). He's so done with them
I know some people think it's childish of Tara and Rebecca fighting in the car but I'm like laughing over here ahahaha
Tyler leaving ahahahaha
I've seen people say it's a "Hotchniss" moment when she mentions him, but.... I don't see it. Not bc I don't ship them, but it's not really a good thing for Hotch or Emily. She basically said that Rossi would've never called Hotch out, like ever. Especially not in public. She knows that Rossi would've backed Hotch up no matter what and supported him, which I think is where people we're talking about in this scene. However.... Rossi is also right in what he says here. He shouldn't have embarrassed her like that earlier, but he calls her out on her biased thinking. That's way too many consequences to deal with emotionally, but also legally. (big spoilers on the case here: the unsub ends up dead).
The girls are fighting
Oh and the queer girls are also fighting lol
"Fibrous" Tara you just farted 😭
Tyler looking for more clues and there are passports involved and finances I think....
JJ's angry at herself
"Agent Jareau has proven herself untrustworthy."
Fucking kidding me? It's always a threat with the "BAU can't do shit"
Luke going in now!
JJ directing him on what to do yessss
"Let's get started" Voit just did what JJ said to him in the last ep. He's in control, like JJ was in the beginning.
JJ being proud of him tho aww. I enjoyed that little moment. It got them somewhere.
"Jennifer" fuck you
I can't tell if that's a lie or not, that the profile is all wrong. I'm still fucking confused.
Omg wait. The cuts between Voit talking to Luke and the unsub in Utah with his victims. I think it's supposed to show the audience that the team has to pretty much start their whole profile over. Especially with the Utah case going along with what he's saying. Everyone will believe the lie all they want, could get someone killed, the BAU's methods is profiling based on abusive childhoods affecting the unsub, and in this case, it got "someone killed before he could spread it" = the unsub. Because of this, the director will make the BAU not work with Voit any further bc they screwed up. Basically, the case is not connected and that drives the team farther away from Voit's answers and Gold Star as a whole.
"Jennifer" fuck you again
Garcia confirms Aiden Keller's not part of it.
Emily beating herself up again :(
Oh fuck off
Luke you're like... giving JJ another hearing trauma
Injure, Jean, Fear, dot, Z, Y, Q. (as everyone guessed, yes it is an anagram for JJ's name). So my initial thoughts was either a file or website link, and from an article, it's a website link!
(There may also be deepfakes involved according to AJ 👀)
I think this whole thing is still government or military related (JJ, Luke, or even Tyler would know)
I think JJ might be accused of committing a crime with the deepfake.
Also it looks like JJ might know something. The look on her face.
Onto the next ep!!
Ughhh this got me hooked now!!
Ok I just wanna say the directing choices especially in the cell scenes, AJ has said that the cell becomes its own character in a way. In this case, the cell (bars) could indicate who is really “in prison/behind bars”, Voit or JJ/Luke. It’s the most prominent with JJ and Voit tho bc there’s a lot going on. The closeups with the two of them, especially JJ, could be hinting at something. (And if you’ve followed the articles and interviews of the cast, JJ will be involved in some way). (Forgot about this in the middle of the post lol)
#jennifer jareau#emily prentiss#david rossi#tara lewis#luke alvez#penelope garcia#tyler green#elias voit#cme s17 spoilers#cme season 17 spoilers#criminal minds evolution#criminal minds#cme 17x02
12 notes
·
View notes
Text








Paradip Sakshyarata Samity (PSS) organized a heartfelt program at Golden Jubilee Park, distributing essential all-season materials such as water bottles, umbrellas, bed sheets, and mosquito nets to 150 financially vulnerable elderly citizens.
The event was graced by Chief Guest Shri P.L. Haranadh, Chairman, PPA, along with esteemed guests Capt. A.C. Sahoo, Dy. Conservator, PPA, Shri S. Nahak, CME, PPA; and Shri A.K. Sahoo, Sr. DTM, PPA.
This initiative reflects PSS’s 32-year-long commitment to uplifting the underprivileged with care, dignity, and meaningful support.
Special appreciation to Secretary Shri Ram Chandra Pradhan and Project Coordinator Shri Ashok Mohapatra for successfully organizing this impactful event.
2 notes
·
View notes
Text
Promo Pics and Synopsis for CME 17x08
Synopsis: The BAU tries to get ahead of Jade and Damien who are on a killing spree. Rossi must confront an old flame to unpack the secrets behind the Gold Star program. Tyler and Rebecca attempt to gain leverage over Elias Voit’s lawyer.
(source: Paramount Express Press)






















#criminal minds evolution#criminal minds evolution spoilers#why is paramount express press geolocked#they be acting like they are safekeeping nuclear launch codes or something#this is also why everything is in thumbnail quality#because for real access i apparently have to be well for one american#and two some level 40 initiated wizard with an account
7 notes
·
View notes
Text
Steps to Apply Through IMLC as a Physician Assistant
The IMLC Physician Assistant pathway offers a faster solution for multistate licensing. Although initially designed for physicians, the Interstate Medical Licensure Compact (IMLC) now opens opportunities for qualified physician assistants to obtain licenses in multiple states through a simplified process. Understanding the exact steps for application helps avoid delays and ensures full compliance with medical board standards.
This guide explains how to navigate the IMLC Physician Assistant process—from eligibility to final license issuance.
Understand the IMLC Physician Assistant Pathway
The IMLC Physician Assistant application enables medical professionals to expand their reach while reducing paperwork. By applying through the compact, eligible physician assistants can hold licenses in various states with one primary application. The compact improves patient access to care and makes it easier for certified physician assistants to work across jurisdictions.
Step 1: Check Eligibility Criteria
Before starting your IMLC Physician Assistant application, ensure you meet the basic qualifications:
Hold a full and unrestricted license in a compact state
Reside, work, or have graduated from a program in that state
Pass the PANCE exam
Have no disciplinary history or criminal record
Graduate from an accredited PA program
Meeting these requirements makes you eligible to use your current state as your State of Principal License (SPL) for the compact process.
Step 2: Identify Your State of Principal License
Your SPL must be a participating IMLC state and meet at least one of the following:
It's your primary residence
It’s where you primarily practice
It’s where you completed your PA program
Once confirmed, your SPL will review and verify your IMLC Physician Assistant application details before issuing a Letter of Qualification (LOQ).
Step 3: Submit Your IMLC Application Online
Start the IMLC Physician Assistant application by creating an account at the official IMLC website. You will need to:
Fill out the application form accurately
Upload supporting documents like education records and ID
Pay fees for background checks and state license processing
Ensure every detail is correct to avoid delays during the verification phase.
Step 4: Complete Fingerprinting and Background Check
As part of the IMLC Physician Assistant process, fingerprint-based background checks are mandatory. Schedule fingerprinting with an approved vendor and complete this step quickly after submitting your application.
Once completed, your results are sent directly to your SPL for clearance.
Step 5: Wait for Letter of Qualification
After successful background verification, the SPL reviews your credentials and issues the LOQ. This letter confirms your eligibility to apply for medical licenses in other IMLC states as a physician assistant. The LOQ is valid for a limited time, so act quickly to apply for additional licenses.
Step 6: Choose Additional States and Apply
With the LOQ in place, you can now use your IMLC portal to apply for licenses in other participating states. Your documents are forwarded automatically. This is one of the main advantages of the IMLC Physician Assistant process—it reduces duplicate effort and speeds up license approvals.
Step 7: Monitor Application Progress
Log into your IMLC account regularly to track your license status. The dashboard will show:
States receiving your application
States currently reviewing
Final approvals and license issuance
Respond quickly to any additional document requests from state boards to avoid processing delays.
Step 8: Renew Licenses Separately
While the IMLC Physician Assistant system speeds up initial licensing, each state still handles renewals separately. This means:
You must follow each state’s renewal schedule
CME requirements vary
You are responsible for submitting renewals on time
Failure to renew on time may result in penalties or suspension.
Why Licensing Services Are Useful
The IMLC Physician Assistant process can be time-consuming. Many professionals use licensing services to:
Track application deadlines
Ensure document accuracy
Handle multistate communication
Speed up application workflows
Professional help makes the process easier, especially for busy physician assistants expanding into several states.
Helpful Tips for IMLC Physician Assistants
To stay on track and prevent issues:
Start collecting documents early
Create a checklist for IMLC steps
Monitor your application dashboard
Respond fast to state board emails
Keep your LOQ valid by acting quickly
These small steps make a big difference during the IMLC Physician Assistant application.
Conclusion
The IMLC Physician Assistant process simplifies multistate licensing for eligible professionals. By following each step—checking eligibility, submitting accurate applications, and using the portal to manage progress—you can secure licenses in multiple states without repetitive paperwork. Whether applying on your own or through a licensing service, staying organized helps you succeed with ease.
1 note
·
View note
Text
Exploring the Links Between GERD and Mouth Cancer GERD Cancer Risk,
Dive into the intricate relationship between GERD and Mouth Cancer in the comprehensive exploration. Uncover the potential links, risk factors, and preventive measures.
#"GERD Cancer Risk#GERD Cancer Awareness#GERD Cancer Treatment#Esophageal Cancer#mouth cancer#Oral Cancer#CME Programs#CME Conferences#CME Medical courses#CME credits#doctor conferences#medical CME#Primary Care Conference#Medical CME Online#Emergency Medicine Online CME#Medical Conference Website#Physician Conferences#Medical CME Courses#Doctors CME Conferences#CME training for Physicians#Medical Event Organizer#Organizing Medical Events#Medical Conferences#Medical Speakers#Healthcare Marketplace
0 notes
Text
King of the North
Narrator: It was a solemn spring day in 1941. On top of hearing the daily news about the bombings throughout the UK, the LNER engines have learned that Sir Nigel Gresley had died at the age of 64. Sir Nigel Gresley was not only the Chief Mechanical Engineer of the railway, but also someone who many of the engines called their father.
(We cut to Sir Nigel Gresley's funeral.)
Narrator: Since the railway still needed to operate only a select number of engines were able to attend the service. Gordon, Scott, Mallard, and Great Northern were there.
(Mallard is crying while Great Northern comforts him while they remain in their engines.)
Mallard: He was so good to, to me.
Great Northern: I know, young one. I know. He was good to all of us.
(Gordon and Scott are standing by his casket. Scott's tearing up to while holding onto Gordon.)
Scott: I can't believe he's gone, brother. I never thought it would happen like this.
Gordon: That illness seemed to be worse than we thought. Humans are after all very fragile compared to us.
Scott: I know but still. He's our father! He made us. We wouldn't exist if he didn't create us.
(Gordon sighs.)
Gordon: At the end of the day, he was a business man. He always wanted us to compete for his favor. You saw how he praised Mallard. He only did it because Mallard broke the speed record.
(Scott looks at his brother feeling even more dejected.)
Scott: Gordon how can you say that? He loved us!
(Gordon backs away.)
Gordon: No. He loved you.
(Before Scott could say anything, Gordon goes back to his engine.)
Narrator: Scott wants to go after Gordon. He knows something is bothering his brother.
Great Northern: I suggest you leave him be, Scott. Gordon clearly needs to have some time alone.
(Scott turns his head.)
Scott: How can you be so cold, North? Gordon's our brother. He's the oldest out of all of us and would've known Sir Nigel Gresley the longest.
Great Northern: Scott you need to understand that not all of us were cared for by him the way you and Mallard were. Gordon has a lot of feelings about him that need to be processed alone.
(Scott looks confused and dejected.)
Mallard: North what's going to happen to us now? Are we going to be scraped?
Great Northern: No Mallard. We're in the middle of a war and are very vital to the evacuation program. We are at our top forms and can't be scrapped. While most of us are only given numbers, all of us are important. The railway can't afford to scrap us now.
(Mallard settles down.)
Mallard: I understand. So why are you not crying like myself and Scott?
Great Northern (sighing): I admit that I have similar feelings to Gordon. Our creator has not always been so kind. He might have been akin to a father figure, but we are still machines. He simply can not care for us the same way he would his own children.
Scott: Not you too, North. I've never seen him bad mouth a single engine in my life. How could you say that our creator was so cruel?
(Great Northern says nothing.)
Scott: I don't know what you and Gordon have been through, but our creator is still our father. No matter what happens, Sir Nigel Gresley would have never been so awful.
Time Skip
Narrator: Four years have passed as WWII ended. Great Northern had just been selected to be rebuilt by the new CME, Edward Thompson. It was the night before work began and the engines were allowed to have a party.
(Everyone is in their human form.)
Mallard: My word you look wonderful North.
Scott: Indeed. You look like a member of the royal army in that uniform.
(Great Northern stands in the middle of the room with pride.)
Great Northern: Why thank you. This is something that I will never forget. If only Sir Nigel Gresley was alive to be here.
Gordon (huffing): You wouldn't be in this position if he was alive. Sir Nigel Gresley would have never approved of your rebuild. Why you're still in fine condition just the way you are.
(Great Northern smiles solemnly.)
Great Northern: I understand your concern, brother. But for tonight, I simply want to enjoy myself. This is my first time out of my engine and I wanted to look my absolute best. I had heard that Scott brought a camera courtesy of his driver. Would you mind taking my picture in this uniform?
(Despite his bad mood, Gordon accepts.)
Gordon: Why of course I will. It wasn't my intention to try to spoil your evening. I will need Scott's help with the camera though.
Narrator: The brothers and Mallard all help with setting up the camera. Great Northern stands in front of the wall looking like a royal officer.
Mallard: This is an amazing pose.
Gordon: Just move a little to the left.
(Great Northern moves over a step.)
Great Northern: Is this better?
Mallard: Yes I think you have the right spot.
(Scott finishes setting up the camera.)
Scott: Ok so just stand still. I'm going to take the picture... now.
(There's a bright flash as the picture is taken.)
Gordon: Done.
Great Northern: Excellent. Now when will we know what the picture looks like?
(Scott thinks.)
Scott: I have no idea. I'll have to ask my driver in the morning.
Great Northern: I see. Either way, thank you all so much for making this night special. I hope to continue working alongside you once my rebuild is completed.
(They all hug.)
Mallard: You will always be our King of the North.
Great Northern: Thank you, Mallard. Thank you.
Narrator: As the night goes on, everyone enjoys themselves. When they were asked to go back to their engines, they all had hope that things would get better. Little did they know, a plan to make nation wide changes to British Rail affecting thousands of engines would be implemented just three years later.
AN: Shout out to @nlliah for requesting this interaction. If anyone wants to request a story feel free to send it in. The next chapters of The Great Race Rewrite and Time Doesn't Heal All Wounds will be my next releases.
Tagging: @pxmun2, @klein-sodor-bahn, @jayde-jots, @bluy1206, @sketalya, @ladychandraofthemoone, @fabianvalencia561, @eyesinspaceisgone, @ethereal-capricorns-blog, and @itsonlyprogrammed.
17 notes
·
View notes
Text
CME program on Long Covid I watched today explicitly called out medical gaslighting and mentioned that long covid patients were “victims” that needed support and validation of their symptoms and experiences.
9 notes
·
View notes
Text
How to Become an Aspiring Medical Professionals in the US?

Aspiring medical professionals in the US embark on a rigorous and rewarding journey that requires dedication, perseverance, and a passion for helping others.
Here's a comprehensive guide to becoming a medical professional in the United States:
Educational Requirements:
a. Undergraduate Degree: Complete a bachelor's degree in any major, but it's recommended to focus on science-related fields like biology, chemistry, or physics to prepare for medical school prerequisites.
b. Medical School (MD or DO): Earn a Doctor of Medicine (MD) or Doctor of Osteopathic Medicine (DO) degree. Medical school typically takes four years and involves a combination of classroom learning, laboratory work, and clinical rotations.
2. Premedical Preparation:
a. MCAT (Medical College Admission Test): Take and score well on the MCAT, a standardized test that assesses your scientific knowledge and problem-solving skills.
b. Shadowing and Volunteering: Gain hands-on experience in healthcare settings by shadowing physicians, volunteering in hospitals, or participating in research projects.
c. Extracurricular Activities: Demonstrate your commitment to healthcare and community service through extracurricular activities related to medicine or public health.
3. Medical School Application:
a. Strong Academic Record: Maintain a high GPA in your undergraduate studies, particularly in science courses.
b. Letters of Recommendation: Secure strong letters of recommendation from professors, mentors, and physicians who can attest to your academic and personal qualities.
c. Personal Statement: Craft a compelling personal statement highlighting your motivations, experiences, and aspirations in the medical field.
4. Residency Training:
a. Match Process: After medical school, participate in the National Resident Matching Program (NRMP) to match with a residency program in your desired speciality.
b. Specialization: Residency training typically lasts three to seven years, depending on the speciality, and provides in-depth clinical training under the supervision of experienced physicians.
c. Board Certification: Once you complete a residency, you become eligible to take and pass the board certification exam for your speciality.
5. Licensure and Continuing Medical Education:
a. Medical License: Obtain a medical license from the state where you intend to practice.
b. Continuing Medical Education (CME): Commit to lifelong learning by completing CME courses to stay up-to-date with the latest medical advancements and maintain your license.
6. Career Options:
a. Physician: Choose from a wide range of medical specialities, such as internal medicine, pediatrics, surgery, family medicine, or psychiatry.
b. Physician Assistant: Work under the supervision of a physician to provide comprehensive medical care.
c. Nurse Practitioner: Provide primary and specialized healthcare services independently or in collaboration with physicians.
d. Other Medical Professionals: Explore various healthcare professions, including dentists, pharmacists, optometrists, and audiologists.
Once you are ready to join organizations to offer your services, you need a platform to help you get a job. Check MedCadre, and you will get what you seek as an aspiring medical professional.
How does MedCadre help Aspiring Medical Professionals?
MedCadre is a one-stop solution to find the right job for you. The platform helps aspiring medical professionals get placement in the medical field.
All you have to do is visit the website, click on the form, and fill it out with relevant information. Once we verify your Resume, we will get back to you.
Becoming a medical professional in the US is a challenging yet fulfilling career path. With dedication, perseverance, and a passion for helping others, you can make a significant impact in your patients' lives and contribute to advancing healthcare.
Submit your Resume to MedCadre to enhance your career in the medical profession.
visit our site by clicking the link: https://medcadre.com/careers
#medical professionals#physician assistant#nurse practitioner#nursestaffing#healthcarestaffing#allied staffing
4 notes
·
View notes
Text
Orthopaedic second opinion near Marathahalli
Empowering surgeons, advancing care! 🦵✨ Dr. Raghu Nagaraj shared his expertise on cutting-edge knee arthroscopy techniques at the CME Program in Delhi. Proud to contribute to the future of orthopaedics!
0 notes