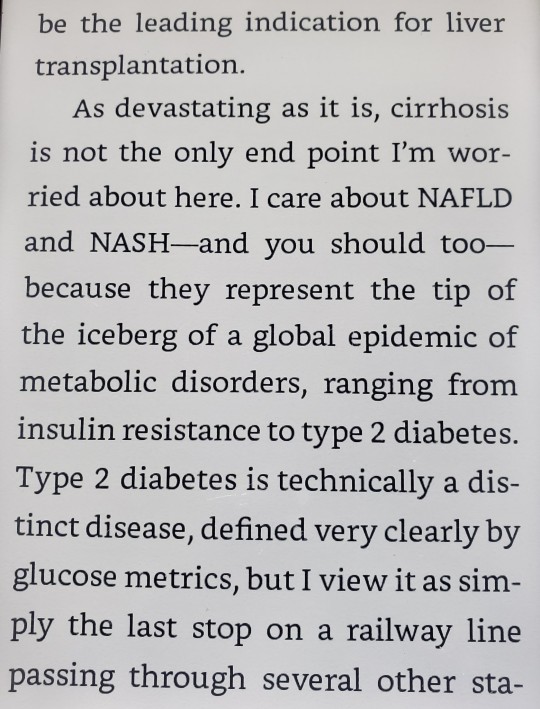
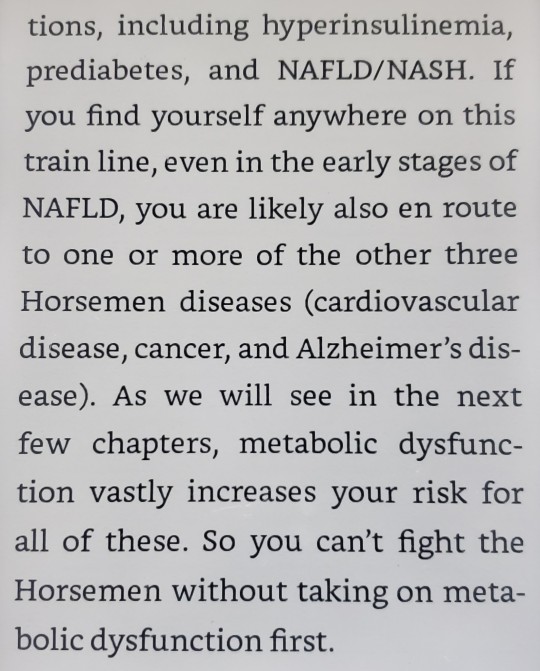
#Nonalcoholic Fatty Liver Disease
Text
I just wanna share a little win today 🥺
It's going to be under the break, though, because there is talk of weight and fat loss. I'm going to try to add correct tags for blocking but if I miss any please feel free to let me know.
So, back in May, I went to the doctor thinking that I would leave with a scheduled gallbladder removal surgery. Instead, I walked away with news of a more complicated-to-resolve condition, Non-Alcoholic Fatty Liver Disease (NAFLD).
I had been on metformin for about a month due to recently discovered insulin resistance that I have likely been struggling with since I was very young, based on symptoms. I've been overweight since I was probably around 5ish.
I had been having symptoms that I believed were a bad gallbladder, my body reacting to the pregnancy hormones that had just dropped, since late February. By May, I was struggling to eat, struggling to stay hydrated, and I was scared. But that was the earliest I could be seen by any doctor.
Since that visit, I've adopted a diet similar to the Mediterranean diet. I don't eat more than 12g of added sugar most days. I don't have more than an oz of dairy. I can't eat almost any of my autism-safe foods because 99% of them were ultra-processed and finding adequate substitutes has been complicated. But I am still eating, and I am doing my best to exercise more than I had been (which was mainly zero, because I was severely depressed).
Well, I did some low-level research so that I could give myself a goal to reach; bc 'lose weight' on its own is discouraging. My wife and I joined a health program that gives you 24/7 access to a health coach and a specialist and they are great at motivating. And, today, I've surpassed my goal of losing 3% of my body fat (by a lot, actually, I don't weigh every day because it stresses me out). This should mean, hopefully, that my liver is now healing itself again because I was in early stages of the disease.
I was nervous about how quickly I'm losing weight at first, but my doctors are not concerned and the combination of meds I'm on facilitate weight loss at least x3, plus I've cut out almost all added sugar, so I'm trying to not be too worried unless the doctors tell me to be. Therefore, if folks comment here, I would very much appreciate not being told I'm losing weight too quickly. I know it's fast. And I am always worried about it in the back of my mind because I know it can also cause problems, but I'm here today to celebrate achieving something I have been fighting for, for the last couple months, and I was told I needed to lose 30lbs this year.

#weight loss#nafld#nonalcoholic fatty liver disease#diet#diet changes#weight loss diet#ed warning#rapid weight loss#metformin
1 note
·
View note
Text
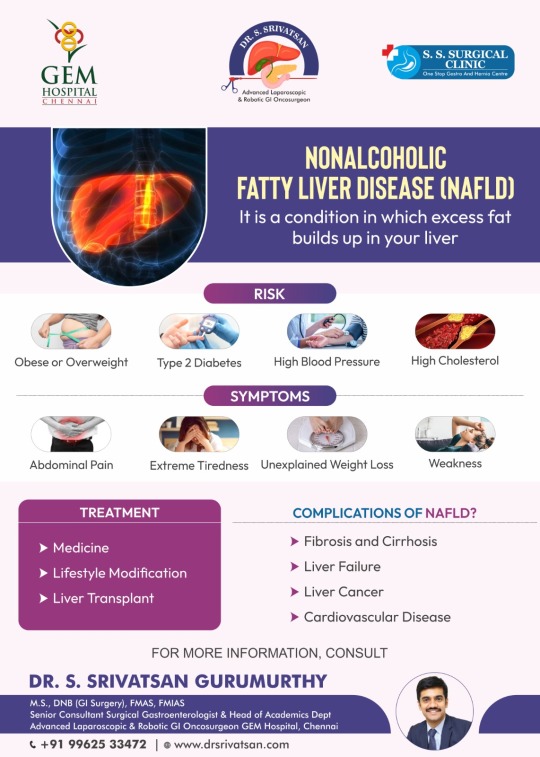
NAFLD: Take Control of Your Liver Health
Learn about Nonalcoholic Fatty Liver Disease (NAFLD), its risks including obesity, type 2 diabetes, and high blood pressure, symptoms like abdominal pain and extreme tiredness, treatment options, complications such as fibrosis and liver cancer, and more. Consult for further details.Consult Today!!!
For more information
Dr. S. Srivatsan Gurumurthy
Senior Consultant Surgical Gastroenterologist & Head of Academics Department and Advanced Laparoscopic & Robotic GI Oncosurgeon
Call: +91 +91 99625 33472
#NAFLD#Nonalcoholic Fatty Liver Disease#Liver Cancer Surgeon in Chennai#Liver Diseases Treatment in Chennai#Liver Transplant Surgery in Chennai
0 notes
Text




#Outlive#peter attia#bill gifford#nonalcoholic fatty liver disease#NAFLD#NASH#alzheimers#cancer#cardiovascular disease#type 2 diabetes#glucose metrics#cirrhosis#liver#inflammation#ALT#obesity#hyperlipidemia#cholesterol#high cholesterol#rising ALT levels#longevity#health#overweight
1 note
·
View note
Text
Nonalcoholic fatty liver disease.
Basics first. The liver is the largest organ of our body. The liver helps your body to digest food, store energy, and remove harmful substances. So, What is Nonalcoholic Fatty Liver? Fatty liver (Hepatic Steatosis) is a diseased condition in which fat builds up in the liver along with inflammation in it. Fatty Liver disease is divided into 2 types. Read more
2. Alcoholic Fatty Liver Disease (AFLD).
1 note
·
View note
Text
Understanding Fatty Liver: From AFLD to NAFLD
Your liver is your body's powerhouse, filtering toxins, processing nutrients, and keeping everything running smoothly. But what happens when fat starts to accumulate in this vital organ? It leads to a disease known as fatty liver disease. In this blog, we'll delve into the world of fatty liver, exploring what it is, the different types (including AFLD and NAFLD), and, most importantly, how to treat fatty liver.
What is Fatty Liver?
Your liver is an organ responsible for over 500 bodily functions. One of its key jobs is storing fat, but when too much accumulates, it can lead to fatty liver disease.
Fatty liver disorder means a conditon in which excess fat builds up in your liver cells. It can happen for various reasons. Fatty liver often doesn't cause immediate problems, however, if left untreated, it can progress to serious liver diseases and symptoms, such as liver inflammation and even cirrhosis.
Types of Fatty Liver
There are two main categories of fatty liver disease, differentiated by the root cause of the fat accumulation:
Alcoholic Fatty Liver Disease (AFLD)
As the name implies, alcoholic fatty liver disease is directly linked to excessive alcohol consumption. Heavy drinking over a prolonged period can damage your liver cells. The liver, struggling to keep up with the constant assault of alcohol, starts to malfunction and become inflamed, allowing fat to accumulate and wreak havoc on its delicate processes.
Nonalcoholic Fatty Liver Disease (NAFLD)
Nonalcoholic fatty liver disease is the more prevalent type of fatty liver disease, affecting individuals who don't necessarily consume excessive alcohol. The exact cause of NAFLD remains under investigation, but research suggests a strong link to factors like insulin resistance, obesity, and genetics.
How Do You Treat Fatty Liver?
There's no magic bullet for fatty liver, but a multi-pronged approach can effectively manage the condition and even reverse the fat buildup. Here's a look at some key strategies:
Weight Loss: Shedding even a modest body weight can significantly improve your liver health, whether or not you are diagnosed with nonalcoholic fatty liver. Aim for gradual, sustainable weight loss through healthy eating and exercise.
Dietary Changes: Embrace a balanced diet rich in fruits, vegetables, and whole grains. Limit processed foods, sugary drinks, and unhealthy fats to keep your liver happy.
Exercise: Regular physical activity helps burn fat and improve insulin sensitivity. Patients diagnosed with alcoholic and nonalcoholic fatty liver diseases are advised to aim for at least 30 minutes of moderate-intensity exercise most days of the week.
Limit Alcohol: If you have AFLD, abstaining from alcohol is crucial. Even for nonalcoholic fatty liver disease (NAFLD), moderation or complete abstinence is recommended.
Manage Underlying Conditions: If you have diabetes, high cholesterol, or other health conditions contributing to a fatty liver, work with your doctor to manage them effectively with medications.
Conclusion
Alcoholic and nonalcoholic fatty liver diseases are problematic but manageable. Now that you understand the disease and the potential treatments, you know you can take action to improve your liver health. To simplify your journey and get personalised guidance on fatty liver treatments, explore digital healthcare apps that offer resources and support through health monitoring, dietary consultations, and more.
#nonalcoholic fatty liver#fatty liver condition#fatty liver disorder#liver diseases and symptoms#how to treat fatty liver
0 notes
Text
Nonalcoholic fatty liver disease is definitely one of those things you don't want to Google without adding "haes" to the search...
Truly "you should just lose weight" everywhere... You got any other song and dance? No?
Damn I wonder if weight cycling (you know, the thing that happens to like, almost everyone who persistently tries to lose weight) is like. Bad for the liver...
3 notes
·
View notes
Text
Mélovin Health Update: What We Know So Far (11/13/2023)
Okay so normally I'd just reblog the last post I made, but after trawling through countless news/tabloids sites, Reddit, and the cesspool that is Twitter and sorting through the various information available, it seemed more important to make a separate post entirely so people could see.
HERE IS WHAT HAS HAPPENED/WHAT WE KNOW:
-Mel has been diagnosed with a serious illness.
-I cannot *personally* confirm for sure what illness, HOWEVER, most sources are reporting that it is steatohepatitis, a liver condition, sometimes also known as "Nonalcoholic Fatty Liver Disease"
-In essence: this is essentially an inflammation of the liver caused by fat cells building up in said liver, not brought on by drinking alcohol.
-It is considered a metabolic disorder. There are several potential causes, most of which are tied to type 2 diabetes and obesity complications, hormone imbalances such as with the thyroid, but it can also just be bad luck of the genetic draw.
-This is NOT the same condition as viral hepatitis (aka Hepatitis C, etc.) I mention this specifically because some sites are incorrectly reporting this claim and people are already using that misinformation as ammo to be homophobic and claim that he got this condition as a result of his "orientation". Do not do this. Do not be these people.
-Is it terminal or is it incurable? Well, that's the muddied part of this. Even Mel used the term 'terminal' in his Instagram post about this, however many sources seem to point to 'incurable' as a more accurate term. It could be that the words are very similar in Ukrainian and thus the confusion there.
-Note that steatohepatitis *is* incurable, however it *may* or *may not* be terminal/fatal. We don't know how long he's had it, if there was liver damage already present before his being officially diagnosed, and to what extent. The main complications that can lead to death if no treatment is administered are cirrhosis and scarring, even liver cancer, which the only treatment at that point would be a full liver transplant. Without treatment, expectancy is anywhere between 3-5 years in severe cases, or 10-15 in lesser ones. Again, this is not proof of anything yet, this is only the general knowledge I have gained from researching this condition.
-This diagnosis came about as a result of bloodwork when he intended to get some kind of cosmetic procedure.
-(Before anyone asks what cosmetic surgery was he getting - that I don't know, and I don't think anyone else does either. He hasn't said, and cosmetic is a very broad term and can range from anything like traditionally thought-of plastic surgeries to something less intensive like a mole removal or getting his teeth worked on. Personally I think he's too young to be getting cosmetic work done, but that's not important right now.)
-He is seeking/undergoing treatment and currently resting and recovering at home with his family.
-His Instagram is currently private to non-followers, probably to prevent harassment. I have downloaded the video regarding this apparent diagnosis announcement and will try to upload it.
-He is still apparently on the longlist for competing in Vidbir, as announced by Suspilne.
-It is not known if this will impact the release of his newest song or further music going forward.
= o = o = o = o = o = o =
If more develops, I will try to let you all know. Right now, please just try to be supportive, don't harass him or his friends/family for more info (he will no doubt tell us when he is ready), and don't spread wild misinformation. We can only imagine what he must be going through right now. Even if this ends up not being nearly as bad as it sounds, getting a lifelong illness diagnosis is not easy for anyone to handle.
5 notes
·
View notes
Text
6 notes
·
View notes
Text
2 notes
·
View notes
Text
I suddenly remembered that I also got diagnosed with nonalcoholic fatty liver disease when I had the ultrasound for my gallbladder back in February. And how I've only gained weight since upping the dose of my antidepressant. And how I know I need to be healthier but idk where to start and I'm just so overwhelmed I don't do anything 🙃🙃🙃🙃🙃
#personal#venting#my mom has type 2 diabetes and I know I need to be healthier but omfg. I'm so tired and overwhelmed by it all.#guess I'll just cry at my desk instead
3 notes
·
View notes
Text
Asymptomatic carotid stenosis of 50%–70% should be treated medically to reduce atherosclerotic cardiovascular disease. Initiating statin therapy and smoking cessation will have the greatest impact on reducing his risk [the pt was a 63 y/o M with normal BP who smokes, whose internal carotid artery was 50% stenosed without symptoms]. Without past neurologic symptoms from carotid artery disease, surgical intervention would not be indicated due to the potential risks of surgery, but repeat ultrasonography is considered reasonable.
Extracranial carotid artery atherosclerosis is a risk factor for stroke and warrants risk factor reduction. Nonsurgical approaches that lower stroke risk include smoking cessation, hypertension management with a goal blood pressure of <130/80 mm Hg, management of diabetes mellitus if present, and initiation of high-intensity statin therapy with a target LDL-cholesterol level of <70 mg/dL. Regular physical activity regardless of BMI is associated with a reduction in stroke risk.
Surgical interventions for carotid disease, such as endarterectomy or stenting, carry a significant risk of mortality and disabling stroke. Because of the risks of intervention, screening of asymptomatic patients is not routinely recommended. Similarly, the benefits of intervention must be weighed against the potential risks. Generally, intervention is recommended if the patient has experienced significant symptoms from carotid artery disease such as stroke or high-risk TIA with stenosis >50%.
For asymptomatic patients, the average annual risk of stroke with stenosis ≥70% is about 1% and evaluation for carotid endarterectomy or stenting is recommended if the patient is considered to be at acceptable surgical risk.
Family physicians often see patients with diarrheal illnesses and most of these are viral. Patients sometimes have misconceptions about preferred fluid and feeding recommendations during these illnesses. The World Health Organization recommends oral rehydration with low osmolarity drinks (oral rehydration solution) and early refeeding. Low osmolarity solutions contain glucose and water, which decrease stool frequency, emesis, and the need for intravenous fluids. Soda and sports drinks contain a higher concentration of glucose, which may worsen diarrhea.
Half-strength apple juice has been shown to be effective, and it approximates an oral rehydration solution. Its use prevents patient measurement errors and the purchase of beverages with an inappropriate osmolarity. It is also more appealing to children than many oral rehydration solutions. Water increases the risk of hyponatremia in children. Refeeding on patient request has been shown to decrease the duration of illness.
This asymptomatic patient with mildly elevated transaminases most likely has nonalcoholic fatty liver disease (NAFLD), which is the most common chronic liver disorder in the United States. It is associated with metabolic syndrome. The initial evaluation should include studies to rule out less common causes of liver disease including viral hepatitis and hemochromatosis. Other laboratory studies that assist in evaluation include albumin and platelet levels. These values allow for the calculation of the Fibrosis-4 score or the NAFLD fibrosis score, which are validated to predict the risk of significant liver fibrosis. Patients with an elevated risk of fibrosis require further evaluation, typically with ultrasound-based elastography before considering liver biopsy. Medications and supplements may cause elevated transaminase levels, and a thorough history to elicit this information is important. Statin-induced liver injury is rare and not consistent with this clinical picture. Discontinuing statin therapy is not necessary with mild transaminase elevations due to NAFLD. Metformin is unlikely to cause elevated transaminases and is safe with this severity of liver disease. Liver fibrosis may be detected with CT but ultrasonography is more sensitive and thus preferred.
Biceps tendinitis causes pain with abduction and external rotation of the arm, and tenderness of the bicipital groove with palpation. Resisted supination of the hand with the elbow flexed to 90° is the Yergason test, and anterior shoulder pain with this maneuver is consistent with bicipital tendinitis. Anterior shoulder pain with cross adduction of the arm is more consistent with acromioclavicular arthritis. Axial compression with rotation to the affected side of the slightly extended neck is the Spurling test for cervical radiculopathy. Extension of the elbow would activate the triceps, and internal rotation of the shoulder with the elbow flexed would result in less activation of the biceps than resisted supination.
Doxycycline (100–200 mg daily or 40 mg once daily of a modified-release formulation) and minocycline (100–200 mg daily) are effective options for the treatment of papulopustular rosacea. The modified-release doxycycline, which is a 40-mg capsule, is FDA-approved but is more expensive out of pocket. Oral metronidazole or macrolides such as azithromycin and clarithromycin can also be considered for those who cannot take tetracyclines. Erythromycin would not be a first-line choice. Amoxicillin, cephalexin, and sulfamethoxazole/trimethoprim lack evidence to support their use in the treatment of papulopustular rosacea.
Office spirometry can be very helpful in narrowing the differential diagnosis of dyspnea. Of the options listed, only cystic fibrosis can cause an obstructive pattern. Other causes of an obstructive pattern include asthma, COPD, α1-antitrypsin deficiency, and bronchiectasis, among others. Common diseases or conditions causing restrictive patterns include adverse reactions to nitrofurantoin, methotrexate, and amiodarone. Chest wall conditions such as kyphosis, scoliosis, and morbid obesity can also cause restrictive patterns. Interstitial lung disease, including idiopathic pulmonary fibrosis, sarcoidosis, and asbestosis, also causes a restrictive pattern.
After percutaneous coronary intervention (PCI) for a non–ST-elevation myocardial infarction, the American College of Cardiology (ACC) recommends continuing dual antiplatelet therapy (DAPT) for at least 12 months in patients who do not have a high risk for bleeding. There are few consistent recommendations after 12 months because there is less consistent and high-quality evidence for outcomes beyond this time point.
The net benefit of dual antiplatelet therapy is highest in the first 12 months after PCI. After 12 months of therapy, the risk of bleeding increases. The risk-benefit ratio should be reassessed for all patients after 12 months of therapy. For most patients, discontinuing either the P2Y12 inhibitor or the aspirin is warranted after 12 months. A 2020 meta-analysis found that patients with newer generation drug-eluting stents treated with DAPT for >18 months had a higher all-cause mortality compared with those treated for <6 months.
The ACC indicates that continuing DAPT is reasonable for select patients. Point-of-care tools, such as the PRECISE-DAPT Risk Calculator, use clinical information to calculate the likely cardiac risk reduction and likely risk of bleeding to help inform shared decision-making after 12 months.
Aspirin is the most cost-effective option for long-term antiplatelet therapy. For this patient, who has indicated costs of care are a concern for him, discontinuing clopidogrel is the better choice.
In addition to antiplatelet therapy, control of elevated blood pressure and cholesterol also reduces cardiovascular outcomes in secondary prevention. This patient’s LDL-cholesterol level is at goal and currently <70 mg/dL, so atorvastatin should be continued at the current dosage. He has reached his blood pressure goal of <130/80 mm Hg and has no orthostatic symptoms, so his current blood pressure medication regimen should be continued.
Because patients with an acute ischemic stroke may require the increased perfusion pressure to limit ischemia, antihypertensive therapy should not be given during the first 48–72 hours as long as they are not candidates for, or recipients of, reperfusion therapy with alteplase or thrombectomy; do not have a comorbid condition requiring acute blood pressure lowering; and do not have a blood pressure >220/120 mm Hg. Patients with a history of hypertension can generally resume their home blood pressure medications once they are safely eating and drinking. Basically, you can allow HTN (permissive HTN) within the first 48 hours of having an ischemic stroke that wasn't treated with alteplase or thrombectomy with goal BP <220/120.
4 notes
·
View notes
Text
I want to try this before returning to FedEx in the winter. It’s really difficult to fast while working there.
2 notes
·
View notes
Text
I technically have a liver disease (nonalcoholic fatty liver) and like, it’s something that’s reasonably easy to “treat” in the sense that it calls for lifestyle changes like more exercise and eating more healthily. But holy shit I’m so stressed about it because I didn’t have great lifestyle habits last year and this year has been a struggle and like I’m trying to get on track with that but I’m crazy paranoid that it’s already too late and I���ve already done irreparable damage to my liver and I’m going to have significant health problems imminently. I know it’s probably just my health anxiety being triggered since that’s the one form of anxiety that’s hard for me to manage but I can’t help it.
Logically I know I’m probably not at a severe point yet because sure I’m overweight and I don’t do a lot of exercise but I don’t drink basically ever, and I’m not experiencing noticeable symptoms that I can’t attribute to anything else…like I’m tired because I don’t have a good sleep routine, I have some isolated yellowish spots on my skin that I can’t be confident aren’t bruises or from something else, my eyes look normal….there’s one symptom that’s been concerning but it’s kinda gross so I’m not going there. But basically there’s only one, maybe two signs that I’m getting worse. And I’m already noticing an improvement in the more gross symptom after a only a few days of one specific change, so…
ugh. On the one hand being very aware of my body is good because it means I’ll probably notice if something’s genuinely wrong. But fuck I hate feeling scared all the time. It’s hard to focus on being in the moment and just making changes now. And I’m scared I’m gonna fall off the wagon again like I have in the past even though I’m in a better place than I was back then
1 note
·
View note
Photo

Q. What is the most common cause of liver cirrhosis in the United States? In the world?
.
.
.
.
.
A. The most common causes of liver cirrhosis in the US are chronic hepatitis C, alcohol, and nonalcoholic fatty liver disease. The most common cause worldwide is hepatitis B, although that is a vaccine-preventable disease if the country has enough resources.
Pro-Tip: With the ability to successfully treat chronic hepatitis C with anti-virals drug, it is being replaced as the most common kind of cirrhosis treated with liver transplant by nonalcoholic fatty liver disease. (Individuals with alcoholic cirrhosis typically have to abstain from drinking for 6 months before they are even considered for transplant, so few are treated this way.)
Image: Thomas Godart, "Cirrhosis, with fatty degeneration of the liver" in an 11 y/o child (19th century)
3 notes
·
View notes
Text
0 notes
Last Seen Blogs

gael-hightower
LIFE'S POETRY

anacansian-blog
Sem título

gojo-chan
Gojo-chan’s fanfics

flowering-smile
Elenna Fëanorian

glimmeringstars
lex!!