#Windows Development Cambridge
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Women make up for the other 50% of Tumblr’s audience.
Text
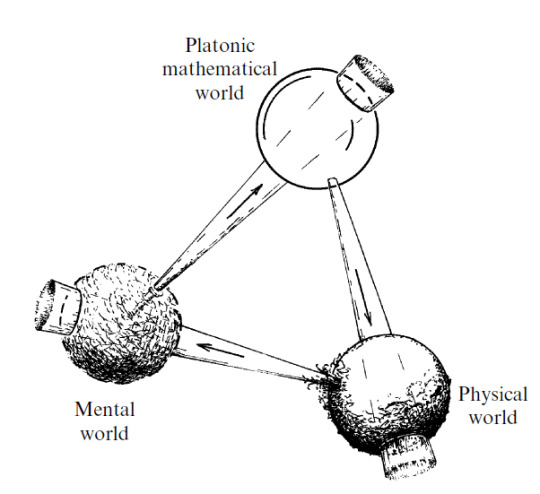
Sir Roger Penrose
To me, the world of perfect forms is primary (as was Plato’s own belief) — its existence being almost a logical necessity — and both the other two worlds are its shadows.
Sir Roger Penrose, born on August 8, 1931, in Colchester, Essex, England, is a luminary in the realm of mathematical physics. His journey began with a Ph.D. in algebraic geometry from the University of Cambridge in 1957, and his career has spanned numerous prestigious posts at universities in both England and the United States. His work in the 1960s on the fundamental features of black holes, celestial bodies of such immense gravity that nothing, not even light, can escape, earned him the 2020 Nobel Prize for Physics.
Penrose’s work on black holes, in collaboration with Stephen Hawking, led to the ground-breaking discovery that all matter within a black hole collapses to a singularity, a point in space where mass is compressed to infinite density and zero volume. This revelation illuminated our understanding of these enigmatic cosmic entities.
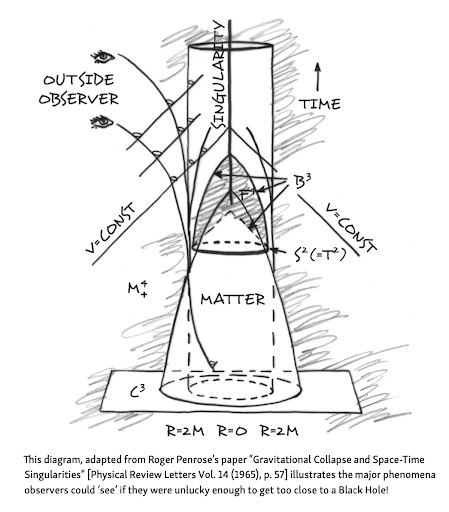
His work did not stop at the theoretical; he also developed a method of mapping the regions of space-time surrounding a black hole, known as a Penrose diagram. This tool allows us to visualize the effects of gravitation upon an entity approaching a black hole, providing a window into the heart of these celestial mysteries.
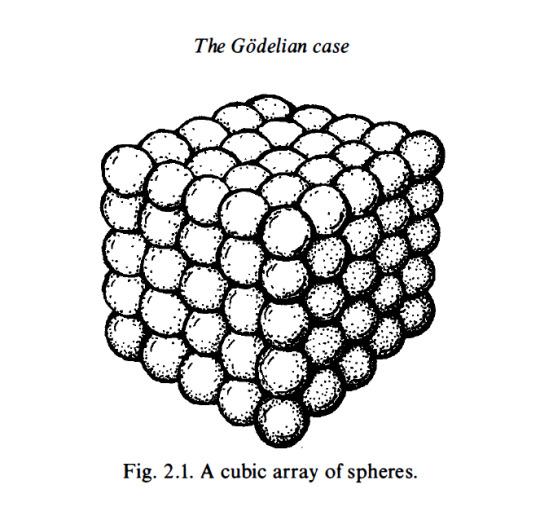
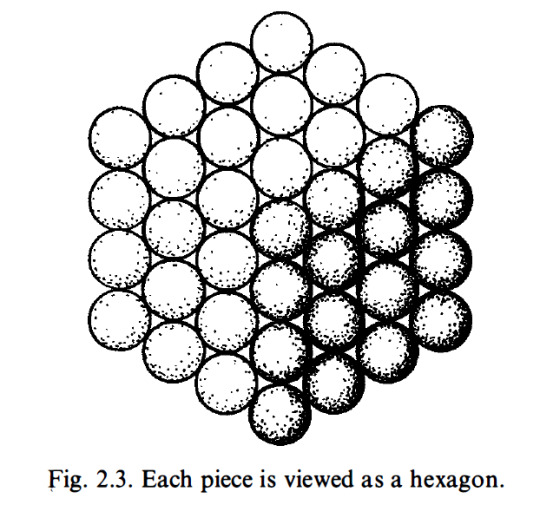
Within Penrose’s chapter, “The Godelian Case” (from “The Road to Reality”) the profound implications of Kurt Gödel’s incompleteness theorems are examined in relation to the connection between mathematics and geometry. Specifically, Penrose’s attention centers on the model depicted in Figure 2.1, which portrays a cubic array of spheres. Through this visual representation, Penrose explores the intricate relationship between geometry and mathematical understanding.
By introducing the model of a cubic array of spheres, Penrose highlights the fundamental role of spatial arrangements in mathematical cognition. This geometrical structure serves as a metaphorical embodiment of mathematical concepts, illustrating how spatial configurations can stimulate cognitive processes and facilitate intuitive comprehension of mathematical truths. The intricate interplay between the arrangement of spheres within the model and the underlying principles of mathematics encourages contemplation on the deep-rooted connections between geometry, spatial reasoning, and abstract mathematical thought.
Penrose’s utilization of the cubic array of spheres underscores his broader philosophical framework, which challenges reductionist accounts of human cognition that rely solely on formal systems or computational models. Through this geometrical representation, he advocates for a more holistic understanding of mathematical insight, one that recognizes the essential role of geometric intuition in shaping human understanding.
By looking at the intricate connection between mathematics and geometry, Penrose prompts a re-evaluation of the mechanistic view of cognition, emphasizing the need to incorporate spatial reasoning and intuitive geometrical understanding into comprehensive models of human thought.
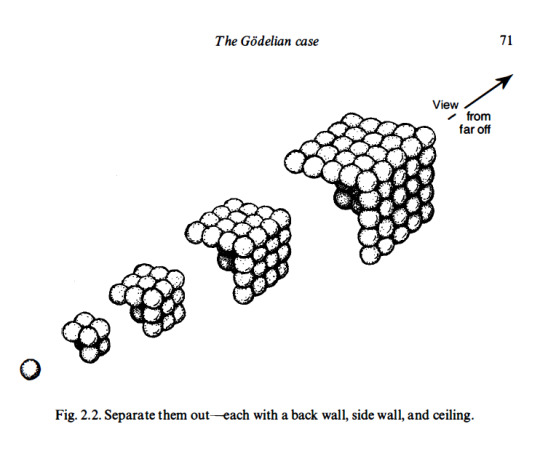
(E) Find a sum of successive hexagonal numbers, starting from 1 , that is not a cube. I am going to try to convince you that this computation will indeed continue for ever without stopping. First of all, a cube is called a cube because it is a number that can be represented as a cubic array of points as depicted in Fig. 2. 1 . I want you to try to think of such an array as built up successively, starting at one corner and then adding a succession of three-faced arrangements each consisting of a back wall, side wall, and ceiling, as depicted in Fig. 2.2. Now view this three-faced arrangement from a long way out, along the direction of the corner common to all three faces. What do we see? A hexagon as in Fig. 2.3. The marks that constitute these hexagons, successively increasing in size, when taken together, correspond to the marks that constitute the entire cube. This, then, establishes the fact that adding together successive hexagonal numbers, starting with 1 , will always give a cube. Accordingly, we have indeed ascertained that (E) will never stop.
Penrose’s work is characterized by a profound appreciation for geometry. His father, a biologist with a passion for mathematics, introduced him to the beauty of geometric shapes and patterns at a young age. This early exposure to geometry shaped Penrose’s unique approach to scientific problems, leading him to develop new mathematical notations and diagrams that have become indispensable tools in the field. His creation of the Penrose tiling, a method of covering a plane with a set of shapes without using a repeating pattern, is a testament to his innovative thinking and his deep understanding of geometric principles.
His fascination with geometry extended beyond the realm of mathematics and into the world of art. He was deeply influenced by the work of Dutch artist M.C. Escher, whose intricate drawings of impossible structures and infinite patterns captivated Penrose’s imagination. This encounter with Escher’s art led Penrose to explore the interplay between geometry and art, culminating in his own contributions to the field of mathematical art. His work in this area, like his scientific research, is characterized by a deep appreciation for the beauty and complexity of geometric forms.
In geometric cognition, Penrose’s work has the potential to make significant contributions. His unique perspective on the role of geometry in understanding the physical world, the mind, and even art, offers a fresh approach to this emerging field. His belief in the power of geometric thinking, as evidenced by his own ground-breaking work, suggests that a geometric approach to cognition could yield valuable insights into the nature of thought and consciousness.
Objective mathematical notions must be thought of as timeless entities and are not to be regarded as being conjured into existence at the moment that they are first humanly perceived.

I argue that the phenomenon of consciousness cannot be accommodated within the framework of present-day physical theory.
His Orch OR theory posits that consciousness arises from quantum computations within the brain’s neurons. This bold hypothesis, bridging the gap between the physical and the mental, has sparked intense debate and research in the scientific community.
Penrose’s work on twistor theory, a geometric framework that seeks to unify quantum mechanics and general relativity, is a testament to his belief in the primacy of geometric structures. This theory, which represents particles and fields in a way that emphasizes their geometric and topological properties, can be seen as a metaphor for his views on cognition. Just as twistor theory seeks to represent complex physical phenomena in terms of simpler geometric structures, Penrose suggests that human cognition may also be understood in terms of fundamental geometric and topological structures.
This perspective has significant implications for the field of cognitive geometry, which studies how humans and other animals understand and navigate the geometric properties of their environment. If Penrose’s ideas are correct, our ability to understand and manipulate geometric structures may be a fundamental aspect of consciousness, rooted in the quantum geometry of the brain itself.
The final conclusion of all this is rather alarming. For it suggests that we must seek a non-computable physical theory that reaches beyond every computable level of oracle machines (and perhaps beyond). — Roger Penrose, Shadows of the Mind: A Search for the Missing Science of Consciousness
#geometrymatters#roger penrose#geometric cognition#cognitive geometry#consciousness#science#research#math#geometry
78 notes
·
View notes
Text

Ruth Wyner
Charity worker with the homeless whose imprisonment under the Misuse of Drugs Act caused an international outcry
In 1998, at the peak of Ruth Wyner’s career as a manager of bold and innovative projects to help homeless people, a crowd of police officers clattered up the narrow stairs of the Wintercomfort day centre in Cambridge, squeezed into Ruth’s attic office and announced that they had arrested eight of her “clients” for dealing drugs.
“Excellent. Well done,” said Ruth. She was well-known for her anti-drugs stance; her anti-drugs policy, developed in cooperation with the police, was considered a model of good practice.
“We’re also arresting you,” said the police, “for knowingly allowing the distribution of a class A drug on the charity premises.”
The arrest, and Ruth’s subsequent imprisonment, provoked an international outcry, and ended the career of one of the most effective charity workers for homeless people.
Ruth, who has died aged 74, was a formidable campaigner for social justice and, following her release from prison in 2000, changed career and became a trailblazer in group therapy. Her life was marked by resilience, creativity and a commitment to helping those most in need.

Born in London, Ruth was the daughter of Anna (nee Nagley), a mosaic artist, and Percy Wyner, a hero of the Burma campaign who later became a cloth merchant. She attended St Paul’s girls’ school in west London, where she excelled at 100-metres hurdle and being troublesome. On leaving St Paul’s in 1968, she launched herself into hippy life with glee.
She edited one of the alternative magazines launched by John “Hoppy” Hopkins, became a local journalist, moved to Norwich, joined the band Crazy Lizard as songwriter, singer and synthesiser player, and moved in with the lead guitarist, Gordon Bell, her future husband. Crazy Lizard started with a benefit night for the homeless, “went off like a firework for a year” and ended with a “crazy, amazing” gig in a snowstorm at the end of Hastings pier.
For six years, Ruth and Gordon took over a deserted bungalow in a piece of industrial wasteland. After the birth of their first child, Joel, they got a friend to install electricity. “He went round hitting things until the lights came on. He didn’t know how he did it either.” When property developers started to sniff about, Ruth negotiated her first major fundraising deal: £1,000 to leave immediately. She used it as a deposit for a house, in time for the birth of a daughter, Rachel.
It was while she was in Norwich that Ruth’s younger brother killed himself by jumping from the window of a London homeless hostel. She rarely talked about this incident, but turned her despair into action. She began working overnight shifts in a “Dickensian” church, St Martin at Oak, supervising up to 40 homeless women and men facing addiction, mental health problems and poverty, eventually becoming the manager, then deputy director of the St Martins Housing Trust charity. Next, in Great Yarmouth, she set up, in the space of a single year, a new direct access hostel for the homeless.
With a reputation for bold thinking, quick action and brilliant campaign work, she was headhunted by Wintercomfort, a homelessness charity that operated out of an old bus in a Cambridge car park. Within three years she had moved premises to a four-storey converted dancing school overlooking the river and set up a highly efficient day centre, a winter night shelter and an outreach team.
Every day, between 70 and 120 people used the service: many drug addicts, more alcoholics, a good number of the mentally ill, many driven to the streets by mental or physical abuse, or grief. Ruth believed that homelessness has little to do with not having a house; that is the final, comparatively minor symptom of something that has gone profoundly wrong in a person’s life.
Ruth’s genius was to be able to negotiate a turbulent boundary of scales: on the one side, the large, generalising sweep of government-driven policy and the demands of law enforcement; on the other, the small, legally hazy dramas of the homeless. Because Ruth was able to remain professional and strong in this clash of contrary forces – negotiating, for example, a £400,000 deal for a new, alcohol-free night shelter with the city council, then hurrying back to the day centre to talk an alcoholic client out of taking her own life in the centre’s toilets – she lessened the misery of thousands and saved many lives.
Shortly after the news broke that the new night shelter was to be built next to a wealthy residential neighbourhood, the police installed a hidden camera in the roof of Jesus College rowing club, across the street from Wintercomfort and, following 300 hours of recording, confirmed eight heroin deals in the charity grounds.
The judge at the trial said that there was no evidence Ruth had encouraged or benefited from the drug dealing at the charity, only that she had not agreed with police on the best way to stop it taking place, and refused to hand over the charity’s list of banned users, on grounds of confidentiality. He sentenced Ruth to five years in prison.
Prison did not break Ruth. She adapted quickly. She learned the prison “slow walk”, developed an unexpected interest in violent films (which vanished on release), became a prison gardener, and started a book about life behind bars, From the Inside (2003). By the time her sentence was reduced to time served on appeal, she had breast cancer.
“Group therapy saved me,” Ruth said.
After her release, and recovery, Ruth travelled to China, India and Canada; she became a tai chi instructor, and trained as a group analyst at the Turvey Centre near Bedford. With its focus on both the individual and the wider community, group analysis perfectly suited Ruth’s extraordinary abilities as a communicator and guide.
For 17 years she worked at the Cambridge Group Therapy Centre, including as the clinical lead 2011-18.
Once again, she embraced inclusivity and openness. Unlike other group therapy practices, she refused to turn people away if they were drug addicts, or chaotic and traumatised; she welcomed them.
She is survived by Gordon, whom she married in 1978, Joel and Rachel, and a grandson, Kaio.
🔔 Ruth Avril Wyner, charity worker and group therapist, born 1 April 1950; died 29 December 2024
Daily inspiration. Discover more photos at Just for Books…?
6 notes
·
View notes
Text

September Webinar: Safeguarding Ukrainian Homes in Winter
Date: September 25th, 2024
Time: 1:00 - 2:15 p.m. (EST)
Join us for our upcoming webinar to learn how Insulate Ukraine is safeguarding families from harsh winter conditions. With temperatures in Ukraine plummeting to -20°C and over 10 million windows shattered by the Russian invasion, their mission to protect homes is vital. Founded in December 2022, Insulate Ukraine provides emergency insulation along the frontline, creating jobs for local civic heroes.
Partnering with engineers from the University of Cambridge, they developed a cost-effective $18 triple-layer window solution. So far, they’ve installed over 24,000 replacement windows, helping families return to warmer, safer homes.
Why attend?
• Hear from experts: Learn firsthand from Harry Blakiston Houston of Insulate Ukraine, in conversation with Maryna Baydyuk from UHU, about the critical work being done this winter. • Impact in action: Discover how innovative insulation solutions are protecting homes and creating local jobs. • Learn how to help: Find out how you can support efforts to keep Ukrainian families safe and warm through the winter.
Read more about their impact here…
4 notes
·
View notes
Text


NO LESS THAN THE PURSUIT OF THE DIVINE IN THE FACE OF CARNAL TEMPTATIONS.
PIC(S) INFO: Resolution at 3051x1837 -- Spotlight on a piece titled "Venus and organist and little dog," part of the "Venus with Musician" painted series by Italian painter, drawer, architectural draftsperson, and printmaker, Titian (1490-1576). Now housed at Museo Nacional del Prado, Madrid, Spain.
PIC #2: Resolution at 1888x1272 -- "Venus with an Organist and Cupid," c. 1555. Oil on canvas. Artwork by Titian (Tiziano Vecellio), born in Pieve di Cadore, Belluno, Veneto (Italy), 1490 - Venice (Italy), 1576.
OVERVIEW: "Titian painted five images of Venus and music, but those five variations on a single theme were not made for the same client, nor intended to be exhibited together. Set in a villa, they show Venus reclining before a large window. At her feet, an organist (in the versions at the Museo del Prado and the Staatliche Museen in Berlin) or a lutenist (at the Metropolitan Museum of New York and the Fitzwilliam Museum in Cambridge) play their instrument as they contemplate the goddess’s nudity.
Meanwhile, she looks away, distracted by the presence of a dog, or of Cupid. These works’ typology indicates they date from the final stage in the development of one of Titian’s subgenres: the reclining female nude, which began with his "Sleeping Venus" (Dresden, Gemäldegalerie) and continued with the "Venus of Urbino" (Florince, Galleria degli Uffizi)."
-- MUSEO DEL PRADO
OBJECT TYPE: Painting
GENRE: Mythological painting
Sources: www.museodelprado.3051s/the-collection/art-work/venus-with-an-organist-and-cupid/b36421df-4d51-43b6-911c-c0517377e48d & Wikimedia.
#Tiziano Vecellio#Veneto Italy#Venice Italy#Oil on Canvas#Oil painting#Painting#Venus#Goddess of Love and Sexuality#Goddess of Love#Venus Goddess of Love#Paintings#Titian Art#Venus and Organist and Little Dog#Italian painter#Museo Nacional del Prado#Madrid Spain#Titian#Museo Nacional del Prado Madrid#Oil paintings#Museo del Prado#Venus with Musician#Spain#Titian Artist
2 notes
·
View notes
Photo

Cambridge University Press released a study that evaluated the efficacy of automated disinfected dispenser systems in hospitals. The results of the study — which oversaw 10 unique hospitals and four additional healthcare systems across five states — highlighted the importance of improved dispenser monitoring to ensure the correct concentrations of disinfectants are dispensed. Here is the full report: Abstract Automated dispensers that dilute concentrated disinfectants with water are commonly used in healthcare facilities. In a point-prevalence product evaluation, nine of 10 (90 percent) hospitals using dilutable disinfectants had one or more malfunctioning dispensers. Twenty-nine of 107 (27.1 percent) systems dispensed product with lower-than-expected concentrations, including 15 (14 percent) with no detectable disinfectant. Introduction Environmental services (EVS) and infection prevention personnel consider factors such as efficacy, wet-contact and kill times, safety, ease of use, and cost when selecting cleaning and disinfection products. Many products are distributed as a concentrate that is diluted to in-use concentrations. The use of dilutable products may reduce costs and can be beneficial for disinfectants that are more stable as a concentrate than at in-use concentrations. Dilutable disinfectants are often dispensed from automated wall-mounted systems that mix concentrated disinfectant and water. However, monitoring is required to ensure that the dispensers are working correctly. Boyce et al. found variations in the concentration of a dilutable quaternary ammonium disinfectant delivered by an automated dispenser; the issues were resolved after installation of water-pressure regulators and modifications of the flow-control devices in concentrate containers. It was recommended that hospitals utilizing dispensing stations conduct periodic testing to verify that appropriate concentrations are being dispensed. Others have demonstrated that automated systems sometimes deliver lower-than-predicted disinfectant concentrations. In a culture survey, we found high rates of surface contamination after completion of post-discharge cleaning and disinfection in some hospitals using automated dispensers. Therefore, we conducted an evaluation of automated dispensing systems in several hospitals. Methods The study protocol was approved by the Cleveland VA Medical Center’s Research and Development Committee. We conducted a point-prevalence evaluation of automated disinfectant dispensing systems in a convenience sample of 10 hospitals from four healthcare systems in five states. For a minimum of five medical-surgical wards and/or intensive care units, we collected 10mL disinfectant samples from dispensers and buckets of in-use disinfectant. The disinfectants included quaternary ammonium disinfectant cleaners, and a peracetic acid/hydrogen peroxide product. For the peracetic acid product, pH was measured with Micro Essential Lab Single-Roll Hydrion pH Test Paper. Peracetic acid concentrations were also measured using a dropper-bottle method with a lower limit-of-detection of 300 ppm. The expected in-use concentration of peracetic acid is roughly 1300 ppm (0.13 percent) with pH roughly 3; 8 samples with more than1,800 ppm were considered to have higher-than-expected concentrations. For the peracetic acid product, the manufacturer recommends quarterly calibration of the systems and provides posters with user instructions (Supplementary material). The instructions include guidance to check a Green/Red low product indicator for when the concentrate bottle should be changed (i.e., change when indicator window shows three-fourths red) and an optional intermittent pH check. For the quaternary ammonium disinfectants, quaternary ammonium concentrations were measured using Micro Essential Lab Hydrion Quaternary Test Paper Kits; the expected in-use concentrations of the products are roughly 700–800 parts per million (ppm) with pH 8–9. To assess the efficacy of samples with lower-than-expected disinfectant levels, the American Society for Testing and Materials (ASTM) standard quantitative carrier disk test method was used with five percent fetal calf serum as soil load. The test organisms included a clinical methicillin-resistant Staphylococcus aureus (MRSA) strain for the quaternary ammonium product and Clostridioides difficile American Type Culture Collection strain 43598 for the peracetic acid product. The exposure times were 5 and 10 minutes for the peracetic acid and quaternary ammonium disinfectants, respectively. For one hospital using the quaternary ammonium product, additional point-prevalence evaluations were conducted after EVS implemented interventions that included increased monitoring of quaternary ammonium concentrations of dispensed product. The supplementary material provides details on the intervention. Results Table 1 Table 2 None of the hospitals reported conducting routine monitoring of disinfectant dispensers. Nine of 10 (90 percent) hospitals had one or more systems dispensing lower-than-expected disinfectant concentrations, and 8 (80 percent) had dispensers that delivered product with no detectable disinfectant (See Table 1). Overall, 29 of 107 (27.1 percent) systems dispensed product with lower-than-expected concentrations, including 15 (14 percent) with no detectable disinfectant. Of 45 samples of peracetic acid product, 26 (57.8 percent) had higher-than-expected peracetic acid concentrations (≥1800 ppm; peak 2,100 ppm), 9 (20 percent) had expected concentrations (1,200–1,500 ppm), 4 (8.9 percent) had lower-than-expected concentrations (300–900 ppm), and 6 (13.3 percent) had undetectable concentrations. pH measurements distinguished dispensers with expected or higher-than-expected peracetic acid disinfectant concentrations (pH around 3) versus those with lower-than-expected concentrations (pH 3.5–5) versus no detectable disinfectant (pH around 6). A second table (See Table 2) shows reasons for malfunction of the 15 systems that dispensed undetectable levels of disinfectant. The identified reasons included concentrate container not being connected correctly (n = 7), concentrate container top being damaged (n = 3), low product indicator not functioning correctly resulting in use of an empty concentrate container (n = 1), and personnel not changing the container when the low product indicator indicated that a change was due (n = 1). In three cases, the reason for the malfunction was not clear. Of 80 in-use disinfectant samples obtained from EVS carts, 27 (33.8 percent) had lower-than-expected disinfectant concentrations, including 14 (17.5 percent) with no detectable disinfectant. One sample with no detectable disinfectant was from a functioning dispenser but the EVS worker acknowledged not obtaining fresh product for days. Of nine employees using product with no detectable disinfectant who were interviewed, three had not noticed that the product was incorrect, whereas six noticed that the product did not smell or appear right but had not notified their supervisor. In four instances, in-use products that EVS personnel identified as disinfectants were dilutable detergents intended for floors. ASTM testing demonstrated that samples with ≤900 ppm of peracetic acid and ≤400 ppm of quaternary ammonium disinfectant resulted in
0 notes
Photo

Cambridge University Press released a study that evaluated the efficacy of automated disinfected dispenser systems in hospitals. The results of the study — which oversaw 10 unique hospitals and four additional healthcare systems across five states — highlighted the importance of improved dispenser monitoring to ensure the correct concentrations of disinfectants are dispensed. Here is the full report: Abstract Automated dispensers that dilute concentrated disinfectants with water are commonly used in healthcare facilities. In a point-prevalence product evaluation, nine of 10 (90 percent) hospitals using dilutable disinfectants had one or more malfunctioning dispensers. Twenty-nine of 107 (27.1 percent) systems dispensed product with lower-than-expected concentrations, including 15 (14 percent) with no detectable disinfectant. Introduction Environmental services (EVS) and infection prevention personnel consider factors such as efficacy, wet-contact and kill times, safety, ease of use, and cost when selecting cleaning and disinfection products. Many products are distributed as a concentrate that is diluted to in-use concentrations. The use of dilutable products may reduce costs and can be beneficial for disinfectants that are more stable as a concentrate than at in-use concentrations. Dilutable disinfectants are often dispensed from automated wall-mounted systems that mix concentrated disinfectant and water. However, monitoring is required to ensure that the dispensers are working correctly. Boyce et al. found variations in the concentration of a dilutable quaternary ammonium disinfectant delivered by an automated dispenser; the issues were resolved after installation of water-pressure regulators and modifications of the flow-control devices in concentrate containers. It was recommended that hospitals utilizing dispensing stations conduct periodic testing to verify that appropriate concentrations are being dispensed. Others have demonstrated that automated systems sometimes deliver lower-than-predicted disinfectant concentrations. In a culture survey, we found high rates of surface contamination after completion of post-discharge cleaning and disinfection in some hospitals using automated dispensers. Therefore, we conducted an evaluation of automated dispensing systems in several hospitals. Methods The study protocol was approved by the Cleveland VA Medical Center’s Research and Development Committee. We conducted a point-prevalence evaluation of automated disinfectant dispensing systems in a convenience sample of 10 hospitals from four healthcare systems in five states. For a minimum of five medical-surgical wards and/or intensive care units, we collected 10mL disinfectant samples from dispensers and buckets of in-use disinfectant. The disinfectants included quaternary ammonium disinfectant cleaners, and a peracetic acid/hydrogen peroxide product. For the peracetic acid product, pH was measured with Micro Essential Lab Single-Roll Hydrion pH Test Paper. Peracetic acid concentrations were also measured using a dropper-bottle method with a lower limit-of-detection of 300 ppm. The expected in-use concentration of peracetic acid is roughly 1300 ppm (0.13 percent) with pH roughly 3; 8 samples with more than1,800 ppm were considered to have higher-than-expected concentrations. For the peracetic acid product, the manufacturer recommends quarterly calibration of the systems and provides posters with user instructions (Supplementary material). The instructions include guidance to check a Green/Red low product indicator for when the concentrate bottle should be changed (i.e., change when indicator window shows three-fourths red) and an optional intermittent pH check. For the quaternary ammonium disinfectants, quaternary ammonium concentrations were measured using Micro Essential Lab Hydrion Quaternary Test Paper Kits; the expected in-use concentrations of the products are roughly 700–800 parts per million (ppm) with pH 8–9. To assess the efficacy of samples with lower-than-expected disinfectant levels, the American Society for Testing and Materials (ASTM) standard quantitative carrier disk test method was used with five percent fetal calf serum as soil load. The test organisms included a clinical methicillin-resistant Staphylococcus aureus (MRSA) strain for the quaternary ammonium product and Clostridioides difficile American Type Culture Collection strain 43598 for the peracetic acid product. The exposure times were 5 and 10 minutes for the peracetic acid and quaternary ammonium disinfectants, respectively. For one hospital using the quaternary ammonium product, additional point-prevalence evaluations were conducted after EVS implemented interventions that included increased monitoring of quaternary ammonium concentrations of dispensed product. The supplementary material provides details on the intervention. Results Table 1 Table 2 None of the hospitals reported conducting routine monitoring of disinfectant dispensers. Nine of 10 (90 percent) hospitals had one or more systems dispensing lower-than-expected disinfectant concentrations, and 8 (80 percent) had dispensers that delivered product with no detectable disinfectant (See Table 1). Overall, 29 of 107 (27.1 percent) systems dispensed product with lower-than-expected concentrations, including 15 (14 percent) with no detectable disinfectant. Of 45 samples of peracetic acid product, 26 (57.8 percent) had higher-than-expected peracetic acid concentrations (≥1800 ppm; peak 2,100 ppm), 9 (20 percent) had expected concentrations (1,200–1,500 ppm), 4 (8.9 percent) had lower-than-expected concentrations (300–900 ppm), and 6 (13.3 percent) had undetectable concentrations. pH measurements distinguished dispensers with expected or higher-than-expected peracetic acid disinfectant concentrations (pH around 3) versus those with lower-than-expected concentrations (pH 3.5–5) versus no detectable disinfectant (pH around 6). A second table (See Table 2) shows reasons for malfunction of the 15 systems that dispensed undetectable levels of disinfectant. The identified reasons included concentrate container not being connected correctly (n = 7), concentrate container top being damaged (n = 3), low product indicator not functioning correctly resulting in use of an empty concentrate container (n = 1), and personnel not changing the container when the low product indicator indicated that a change was due (n = 1). In three cases, the reason for the malfunction was not clear. Of 80 in-use disinfectant samples obtained from EVS carts, 27 (33.8 percent) had lower-than-expected disinfectant concentrations, including 14 (17.5 percent) with no detectable disinfectant. One sample with no detectable disinfectant was from a functioning dispenser but the EVS worker acknowledged not obtaining fresh product for days. Of nine employees using product with no detectable disinfectant who were interviewed, three had not noticed that the product was incorrect, whereas six noticed that the product did not smell or appear right but had not notified their supervisor. In four instances, in-use products that EVS personnel identified as disinfectants were dilutable detergents intended for floors. ASTM testing demonstrated that samples with ≤900 ppm of peracetic acid and ≤400 ppm of quaternary ammonium disinfectant resulted in
0 notes
Photo

Cambridge University Press released a study that evaluated the efficacy of automated disinfected dispenser systems in hospitals. The results of the study — which oversaw 10 unique hospitals and four additional healthcare systems across five states — highlighted the importance of improved dispenser monitoring to ensure the correct concentrations of disinfectants are dispensed. Here is the full report: Abstract Automated dispensers that dilute concentrated disinfectants with water are commonly used in healthcare facilities. In a point-prevalence product evaluation, nine of 10 (90 percent) hospitals using dilutable disinfectants had one or more malfunctioning dispensers. Twenty-nine of 107 (27.1 percent) systems dispensed product with lower-than-expected concentrations, including 15 (14 percent) with no detectable disinfectant. Introduction Environmental services (EVS) and infection prevention personnel consider factors such as efficacy, wet-contact and kill times, safety, ease of use, and cost when selecting cleaning and disinfection products. Many products are distributed as a concentrate that is diluted to in-use concentrations. The use of dilutable products may reduce costs and can be beneficial for disinfectants that are more stable as a concentrate than at in-use concentrations. Dilutable disinfectants are often dispensed from automated wall-mounted systems that mix concentrated disinfectant and water. However, monitoring is required to ensure that the dispensers are working correctly. Boyce et al. found variations in the concentration of a dilutable quaternary ammonium disinfectant delivered by an automated dispenser; the issues were resolved after installation of water-pressure regulators and modifications of the flow-control devices in concentrate containers. It was recommended that hospitals utilizing dispensing stations conduct periodic testing to verify that appropriate concentrations are being dispensed. Others have demonstrated that automated systems sometimes deliver lower-than-predicted disinfectant concentrations. In a culture survey, we found high rates of surface contamination after completion of post-discharge cleaning and disinfection in some hospitals using automated dispensers. Therefore, we conducted an evaluation of automated dispensing systems in several hospitals. Methods The study protocol was approved by the Cleveland VA Medical Center’s Research and Development Committee. We conducted a point-prevalence evaluation of automated disinfectant dispensing systems in a convenience sample of 10 hospitals from four healthcare systems in five states. For a minimum of five medical-surgical wards and/or intensive care units, we collected 10mL disinfectant samples from dispensers and buckets of in-use disinfectant. The disinfectants included quaternary ammonium disinfectant cleaners, and a peracetic acid/hydrogen peroxide product. For the peracetic acid product, pH was measured with Micro Essential Lab Single-Roll Hydrion pH Test Paper. Peracetic acid concentrations were also measured using a dropper-bottle method with a lower limit-of-detection of 300 ppm. The expected in-use concentration of peracetic acid is roughly 1300 ppm (0.13 percent) with pH roughly 3; 8 samples with more than1,800 ppm were considered to have higher-than-expected concentrations. For the peracetic acid product, the manufacturer recommends quarterly calibration of the systems and provides posters with user instructions (Supplementary material). The instructions include guidance to check a Green/Red low product indicator for when the concentrate bottle should be changed (i.e., change when indicator window shows three-fourths red) and an optional intermittent pH check. For the quaternary ammonium disinfectants, quaternary ammonium concentrations were measured using Micro Essential Lab Hydrion Quaternary Test Paper Kits; the expected in-use concentrations of the products are roughly 700–800 parts per million (ppm) with pH 8–9. To assess the efficacy of samples with lower-than-expected disinfectant levels, the American Society for Testing and Materials (ASTM) standard quantitative carrier disk test method was used with five percent fetal calf serum as soil load. The test organisms included a clinical methicillin-resistant Staphylococcus aureus (MRSA) strain for the quaternary ammonium product and Clostridioides difficile American Type Culture Collection strain 43598 for the peracetic acid product. The exposure times were 5 and 10 minutes for the peracetic acid and quaternary ammonium disinfectants, respectively. For one hospital using the quaternary ammonium product, additional point-prevalence evaluations were conducted after EVS implemented interventions that included increased monitoring of quaternary ammonium concentrations of dispensed product. The supplementary material provides details on the intervention. Results Table 1 Table 2 None of the hospitals reported conducting routine monitoring of disinfectant dispensers. Nine of 10 (90 percent) hospitals had one or more systems dispensing lower-than-expected disinfectant concentrations, and 8 (80 percent) had dispensers that delivered product with no detectable disinfectant (See Table 1). Overall, 29 of 107 (27.1 percent) systems dispensed product with lower-than-expected concentrations, including 15 (14 percent) with no detectable disinfectant. Of 45 samples of peracetic acid product, 26 (57.8 percent) had higher-than-expected peracetic acid concentrations (≥1800 ppm; peak 2,100 ppm), 9 (20 percent) had expected concentrations (1,200–1,500 ppm), 4 (8.9 percent) had lower-than-expected concentrations (300–900 ppm), and 6 (13.3 percent) had undetectable concentrations. pH measurements distinguished dispensers with expected or higher-than-expected peracetic acid disinfectant concentrations (pH around 3) versus those with lower-than-expected concentrations (pH 3.5–5) versus no detectable disinfectant (pH around 6). A second table (See Table 2) shows reasons for malfunction of the 15 systems that dispensed undetectable levels of disinfectant. The identified reasons included concentrate container not being connected correctly (n = 7), concentrate container top being damaged (n = 3), low product indicator not functioning correctly resulting in use of an empty concentrate container (n = 1), and personnel not changing the container when the low product indicator indicated that a change was due (n = 1). In three cases, the reason for the malfunction was not clear. Of 80 in-use disinfectant samples obtained from EVS carts, 27 (33.8 percent) had lower-than-expected disinfectant concentrations, including 14 (17.5 percent) with no detectable disinfectant. One sample with no detectable disinfectant was from a functioning dispenser but the EVS worker acknowledged not obtaining fresh product for days. Of nine employees using product with no detectable disinfectant who were interviewed, three had not noticed that the product was incorrect, whereas six noticed that the product did not smell or appear right but had not notified their supervisor. In four instances, in-use products that EVS personnel identified as disinfectants were dilutable detergents intended for floors. ASTM testing demonstrated that samples with ≤900 ppm of peracetic acid and ≤400 ppm of quaternary ammonium disinfectant resulted in
0 notes
Photo

Cambridge University Press released a study that evaluated the efficacy of automated disinfected dispenser systems in hospitals. The results of the study — which oversaw 10 unique hospitals and four additional healthcare systems across five states — highlighted the importance of improved dispenser monitoring to ensure the correct concentrations of disinfectants are dispensed. Here is the full report: Abstract Automated dispensers that dilute concentrated disinfectants with water are commonly used in healthcare facilities. In a point-prevalence product evaluation, nine of 10 (90 percent) hospitals using dilutable disinfectants had one or more malfunctioning dispensers. Twenty-nine of 107 (27.1 percent) systems dispensed product with lower-than-expected concentrations, including 15 (14 percent) with no detectable disinfectant. Introduction Environmental services (EVS) and infection prevention personnel consider factors such as efficacy, wet-contact and kill times, safety, ease of use, and cost when selecting cleaning and disinfection products. Many products are distributed as a concentrate that is diluted to in-use concentrations. The use of dilutable products may reduce costs and can be beneficial for disinfectants that are more stable as a concentrate than at in-use concentrations. Dilutable disinfectants are often dispensed from automated wall-mounted systems that mix concentrated disinfectant and water. However, monitoring is required to ensure that the dispensers are working correctly. Boyce et al. found variations in the concentration of a dilutable quaternary ammonium disinfectant delivered by an automated dispenser; the issues were resolved after installation of water-pressure regulators and modifications of the flow-control devices in concentrate containers. It was recommended that hospitals utilizing dispensing stations conduct periodic testing to verify that appropriate concentrations are being dispensed. Others have demonstrated that automated systems sometimes deliver lower-than-predicted disinfectant concentrations. In a culture survey, we found high rates of surface contamination after completion of post-discharge cleaning and disinfection in some hospitals using automated dispensers. Therefore, we conducted an evaluation of automated dispensing systems in several hospitals. Methods The study protocol was approved by the Cleveland VA Medical Center’s Research and Development Committee. We conducted a point-prevalence evaluation of automated disinfectant dispensing systems in a convenience sample of 10 hospitals from four healthcare systems in five states. For a minimum of five medical-surgical wards and/or intensive care units, we collected 10mL disinfectant samples from dispensers and buckets of in-use disinfectant. The disinfectants included quaternary ammonium disinfectant cleaners, and a peracetic acid/hydrogen peroxide product. For the peracetic acid product, pH was measured with Micro Essential Lab Single-Roll Hydrion pH Test Paper. Peracetic acid concentrations were also measured using a dropper-bottle method with a lower limit-of-detection of 300 ppm. The expected in-use concentration of peracetic acid is roughly 1300 ppm (0.13 percent) with pH roughly 3; 8 samples with more than1,800 ppm were considered to have higher-than-expected concentrations. For the peracetic acid product, the manufacturer recommends quarterly calibration of the systems and provides posters with user instructions (Supplementary material). The instructions include guidance to check a Green/Red low product indicator for when the concentrate bottle should be changed (i.e., change when indicator window shows three-fourths red) and an optional intermittent pH check. For the quaternary ammonium disinfectants, quaternary ammonium concentrations were measured using Micro Essential Lab Hydrion Quaternary Test Paper Kits; the expected in-use concentrations of the products are roughly 700–800 parts per million (ppm) with pH 8–9. To assess the efficacy of samples with lower-than-expected disinfectant levels, the American Society for Testing and Materials (ASTM) standard quantitative carrier disk test method was used with five percent fetal calf serum as soil load. The test organisms included a clinical methicillin-resistant Staphylococcus aureus (MRSA) strain for the quaternary ammonium product and Clostridioides difficile American Type Culture Collection strain 43598 for the peracetic acid product. The exposure times were 5 and 10 minutes for the peracetic acid and quaternary ammonium disinfectants, respectively. For one hospital using the quaternary ammonium product, additional point-prevalence evaluations were conducted after EVS implemented interventions that included increased monitoring of quaternary ammonium concentrations of dispensed product. The supplementary material provides details on the intervention. Results Table 1 Table 2 None of the hospitals reported conducting routine monitoring of disinfectant dispensers. Nine of 10 (90 percent) hospitals had one or more systems dispensing lower-than-expected disinfectant concentrations, and 8 (80 percent) had dispensers that delivered product with no detectable disinfectant (See Table 1). Overall, 29 of 107 (27.1 percent) systems dispensed product with lower-than-expected concentrations, including 15 (14 percent) with no detectable disinfectant. Of 45 samples of peracetic acid product, 26 (57.8 percent) had higher-than-expected peracetic acid concentrations (≥1800 ppm; peak 2,100 ppm), 9 (20 percent) had expected concentrations (1,200–1,500 ppm), 4 (8.9 percent) had lower-than-expected concentrations (300–900 ppm), and 6 (13.3 percent) had undetectable concentrations. pH measurements distinguished dispensers with expected or higher-than-expected peracetic acid disinfectant concentrations (pH around 3) versus those with lower-than-expected concentrations (pH 3.5–5) versus no detectable disinfectant (pH around 6). A second table (See Table 2) shows reasons for malfunction of the 15 systems that dispensed undetectable levels of disinfectant. The identified reasons included concentrate container not being connected correctly (n = 7), concentrate container top being damaged (n = 3), low product indicator not functioning correctly resulting in use of an empty concentrate container (n = 1), and personnel not changing the container when the low product indicator indicated that a change was due (n = 1). In three cases, the reason for the malfunction was not clear. Of 80 in-use disinfectant samples obtained from EVS carts, 27 (33.8 percent) had lower-than-expected disinfectant concentrations, including 14 (17.5 percent) with no detectable disinfectant. One sample with no detectable disinfectant was from a functioning dispenser but the EVS worker acknowledged not obtaining fresh product for days. Of nine employees using product with no detectable disinfectant who were interviewed, three had not noticed that the product was incorrect, whereas six noticed that the product did not smell or appear right but had not notified their supervisor. In four instances, in-use products that EVS personnel identified as disinfectants were dilutable detergents intended for floors. ASTM testing demonstrated that samples with ≤900 ppm of peracetic acid and ≤400 ppm of quaternary ammonium disinfectant resulted in
0 notes
Photo

Cambridge University Press released a study that evaluated the efficacy of automated disinfected dispenser systems in hospitals. The results of the study — which oversaw 10 unique hospitals and four additional healthcare systems across five states — highlighted the importance of improved dispenser monitoring to ensure the correct concentrations of disinfectants are dispensed. Here is the full report: Abstract Automated dispensers that dilute concentrated disinfectants with water are commonly used in healthcare facilities. In a point-prevalence product evaluation, nine of 10 (90 percent) hospitals using dilutable disinfectants had one or more malfunctioning dispensers. Twenty-nine of 107 (27.1 percent) systems dispensed product with lower-than-expected concentrations, including 15 (14 percent) with no detectable disinfectant. Introduction Environmental services (EVS) and infection prevention personnel consider factors such as efficacy, wet-contact and kill times, safety, ease of use, and cost when selecting cleaning and disinfection products. Many products are distributed as a concentrate that is diluted to in-use concentrations. The use of dilutable products may reduce costs and can be beneficial for disinfectants that are more stable as a concentrate than at in-use concentrations. Dilutable disinfectants are often dispensed from automated wall-mounted systems that mix concentrated disinfectant and water. However, monitoring is required to ensure that the dispensers are working correctly. Boyce et al. found variations in the concentration of a dilutable quaternary ammonium disinfectant delivered by an automated dispenser; the issues were resolved after installation of water-pressure regulators and modifications of the flow-control devices in concentrate containers. It was recommended that hospitals utilizing dispensing stations conduct periodic testing to verify that appropriate concentrations are being dispensed. Others have demonstrated that automated systems sometimes deliver lower-than-predicted disinfectant concentrations. In a culture survey, we found high rates of surface contamination after completion of post-discharge cleaning and disinfection in some hospitals using automated dispensers. Therefore, we conducted an evaluation of automated dispensing systems in several hospitals. Methods The study protocol was approved by the Cleveland VA Medical Center’s Research and Development Committee. We conducted a point-prevalence evaluation of automated disinfectant dispensing systems in a convenience sample of 10 hospitals from four healthcare systems in five states. For a minimum of five medical-surgical wards and/or intensive care units, we collected 10mL disinfectant samples from dispensers and buckets of in-use disinfectant. The disinfectants included quaternary ammonium disinfectant cleaners, and a peracetic acid/hydrogen peroxide product. For the peracetic acid product, pH was measured with Micro Essential Lab Single-Roll Hydrion pH Test Paper. Peracetic acid concentrations were also measured using a dropper-bottle method with a lower limit-of-detection of 300 ppm. The expected in-use concentration of peracetic acid is roughly 1300 ppm (0.13 percent) with pH roughly 3; 8 samples with more than1,800 ppm were considered to have higher-than-expected concentrations. For the peracetic acid product, the manufacturer recommends quarterly calibration of the systems and provides posters with user instructions (Supplementary material). The instructions include guidance to check a Green/Red low product indicator for when the concentrate bottle should be changed (i.e., change when indicator window shows three-fourths red) and an optional intermittent pH check. For the quaternary ammonium disinfectants, quaternary ammonium concentrations were measured using Micro Essential Lab Hydrion Quaternary Test Paper Kits; the expected in-use concentrations of the products are roughly 700–800 parts per million (ppm) with pH 8–9. To assess the efficacy of samples with lower-than-expected disinfectant levels, the American Society for Testing and Materials (ASTM) standard quantitative carrier disk test method was used with five percent fetal calf serum as soil load. The test organisms included a clinical methicillin-resistant Staphylococcus aureus (MRSA) strain for the quaternary ammonium product and Clostridioides difficile American Type Culture Collection strain 43598 for the peracetic acid product. The exposure times were 5 and 10 minutes for the peracetic acid and quaternary ammonium disinfectants, respectively. For one hospital using the quaternary ammonium product, additional point-prevalence evaluations were conducted after EVS implemented interventions that included increased monitoring of quaternary ammonium concentrations of dispensed product. The supplementary material provides details on the intervention. Results Table 1 Table 2 None of the hospitals reported conducting routine monitoring of disinfectant dispensers. Nine of 10 (90 percent) hospitals had one or more systems dispensing lower-than-expected disinfectant concentrations, and 8 (80 percent) had dispensers that delivered product with no detectable disinfectant (See Table 1). Overall, 29 of 107 (27.1 percent) systems dispensed product with lower-than-expected concentrations, including 15 (14 percent) with no detectable disinfectant. Of 45 samples of peracetic acid product, 26 (57.8 percent) had higher-than-expected peracetic acid concentrations (≥1800 ppm; peak 2,100 ppm), 9 (20 percent) had expected concentrations (1,200–1,500 ppm), 4 (8.9 percent) had lower-than-expected concentrations (300–900 ppm), and 6 (13.3 percent) had undetectable concentrations. pH measurements distinguished dispensers with expected or higher-than-expected peracetic acid disinfectant concentrations (pH around 3) versus those with lower-than-expected concentrations (pH 3.5–5) versus no detectable disinfectant (pH around 6). A second table (See Table 2) shows reasons for malfunction of the 15 systems that dispensed undetectable levels of disinfectant. The identified reasons included concentrate container not being connected correctly (n = 7), concentrate container top being damaged (n = 3), low product indicator not functioning correctly resulting in use of an empty concentrate container (n = 1), and personnel not changing the container when the low product indicator indicated that a change was due (n = 1). In three cases, the reason for the malfunction was not clear. Of 80 in-use disinfectant samples obtained from EVS carts, 27 (33.8 percent) had lower-than-expected disinfectant concentrations, including 14 (17.5 percent) with no detectable disinfectant. One sample with no detectable disinfectant was from a functioning dispenser but the EVS worker acknowledged not obtaining fresh product for days. Of nine employees using product with no detectable disinfectant who were interviewed, three had not noticed that the product was incorrect, whereas six noticed that the product did not smell or appear right but had not notified their supervisor. In four instances, in-use products that EVS personnel identified as disinfectants were dilutable detergents intended for floors. ASTM testing demonstrated that samples with ≤900 ppm of peracetic acid and ≤400 ppm of quaternary ammonium disinfectant resulted in
0 notes
Photo

Cambridge University Press released a study that evaluated the efficacy of automated disinfected dispenser systems in hospitals. The results of the study — which oversaw 10 unique hospitals and four additional healthcare systems across five states — highlighted the importance of improved dispenser monitoring to ensure the correct concentrations of disinfectants are dispensed. Here is the full report: Abstract Automated dispensers that dilute concentrated disinfectants with water are commonly used in healthcare facilities. In a point-prevalence product evaluation, nine of 10 (90 percent) hospitals using dilutable disinfectants had one or more malfunctioning dispensers. Twenty-nine of 107 (27.1 percent) systems dispensed product with lower-than-expected concentrations, including 15 (14 percent) with no detectable disinfectant. Introduction Environmental services (EVS) and infection prevention personnel consider factors such as efficacy, wet-contact and kill times, safety, ease of use, and cost when selecting cleaning and disinfection products. Many products are distributed as a concentrate that is diluted to in-use concentrations. The use of dilutable products may reduce costs and can be beneficial for disinfectants that are more stable as a concentrate than at in-use concentrations. Dilutable disinfectants are often dispensed from automated wall-mounted systems that mix concentrated disinfectant and water. However, monitoring is required to ensure that the dispensers are working correctly. Boyce et al. found variations in the concentration of a dilutable quaternary ammonium disinfectant delivered by an automated dispenser; the issues were resolved after installation of water-pressure regulators and modifications of the flow-control devices in concentrate containers. It was recommended that hospitals utilizing dispensing stations conduct periodic testing to verify that appropriate concentrations are being dispensed. Others have demonstrated that automated systems sometimes deliver lower-than-predicted disinfectant concentrations. In a culture survey, we found high rates of surface contamination after completion of post-discharge cleaning and disinfection in some hospitals using automated dispensers. Therefore, we conducted an evaluation of automated dispensing systems in several hospitals. Methods The study protocol was approved by the Cleveland VA Medical Center’s Research and Development Committee. We conducted a point-prevalence evaluation of automated disinfectant dispensing systems in a convenience sample of 10 hospitals from four healthcare systems in five states. For a minimum of five medical-surgical wards and/or intensive care units, we collected 10mL disinfectant samples from dispensers and buckets of in-use disinfectant. The disinfectants included quaternary ammonium disinfectant cleaners, and a peracetic acid/hydrogen peroxide product. For the peracetic acid product, pH was measured with Micro Essential Lab Single-Roll Hydrion pH Test Paper. Peracetic acid concentrations were also measured using a dropper-bottle method with a lower limit-of-detection of 300 ppm. The expected in-use concentration of peracetic acid is roughly 1300 ppm (0.13 percent) with pH roughly 3; 8 samples with more than1,800 ppm were considered to have higher-than-expected concentrations. For the peracetic acid product, the manufacturer recommends quarterly calibration of the systems and provides posters with user instructions (Supplementary material). The instructions include guidance to check a Green/Red low product indicator for when the concentrate bottle should be changed (i.e., change when indicator window shows three-fourths red) and an optional intermittent pH check. For the quaternary ammonium disinfectants, quaternary ammonium concentrations were measured using Micro Essential Lab Hydrion Quaternary Test Paper Kits; the expected in-use concentrations of the products are roughly 700–800 parts per million (ppm) with pH 8–9. To assess the efficacy of samples with lower-than-expected disinfectant levels, the American Society for Testing and Materials (ASTM) standard quantitative carrier disk test method was used with five percent fetal calf serum as soil load. The test organisms included a clinical methicillin-resistant Staphylococcus aureus (MRSA) strain for the quaternary ammonium product and Clostridioides difficile American Type Culture Collection strain 43598 for the peracetic acid product. The exposure times were 5 and 10 minutes for the peracetic acid and quaternary ammonium disinfectants, respectively. For one hospital using the quaternary ammonium product, additional point-prevalence evaluations were conducted after EVS implemented interventions that included increased monitoring of quaternary ammonium concentrations of dispensed product. The supplementary material provides details on the intervention. Results Table 1 Table 2 None of the hospitals reported conducting routine monitoring of disinfectant dispensers. Nine of 10 (90 percent) hospitals had one or more systems dispensing lower-than-expected disinfectant concentrations, and 8 (80 percent) had dispensers that delivered product with no detectable disinfectant (See Table 1). Overall, 29 of 107 (27.1 percent) systems dispensed product with lower-than-expected concentrations, including 15 (14 percent) with no detectable disinfectant. Of 45 samples of peracetic acid product, 26 (57.8 percent) had higher-than-expected peracetic acid concentrations (≥1800 ppm; peak 2,100 ppm), 9 (20 percent) had expected concentrations (1,200–1,500 ppm), 4 (8.9 percent) had lower-than-expected concentrations (300–900 ppm), and 6 (13.3 percent) had undetectable concentrations. pH measurements distinguished dispensers with expected or higher-than-expected peracetic acid disinfectant concentrations (pH around 3) versus those with lower-than-expected concentrations (pH 3.5–5) versus no detectable disinfectant (pH around 6). A second table (See Table 2) shows reasons for malfunction of the 15 systems that dispensed undetectable levels of disinfectant. The identified reasons included concentrate container not being connected correctly (n = 7), concentrate container top being damaged (n = 3), low product indicator not functioning correctly resulting in use of an empty concentrate container (n = 1), and personnel not changing the container when the low product indicator indicated that a change was due (n = 1). In three cases, the reason for the malfunction was not clear. Of 80 in-use disinfectant samples obtained from EVS carts, 27 (33.8 percent) had lower-than-expected disinfectant concentrations, including 14 (17.5 percent) with no detectable disinfectant. One sample with no detectable disinfectant was from a functioning dispenser but the EVS worker acknowledged not obtaining fresh product for days. Of nine employees using product with no detectable disinfectant who were interviewed, three had not noticed that the product was incorrect, whereas six noticed that the product did not smell or appear right but had not notified their supervisor. In four instances, in-use products that EVS personnel identified as disinfectants were dilutable detergents intended for floors. ASTM testing demonstrated that samples with ≤900 ppm of peracetic acid and ≤400 ppm of quaternary ammonium disinfectant resulted in
0 notes
Photo

Cambridge University Press released a study that evaluated the efficacy of automated disinfected dispenser systems in hospitals. The results of the study — which oversaw 10 unique hospitals and four additional healthcare systems across five states — highlighted the importance of improved dispenser monitoring to ensure the correct concentrations of disinfectants are dispensed. Here is the full report: Abstract Automated dispensers that dilute concentrated disinfectants with water are commonly used in healthcare facilities. In a point-prevalence product evaluation, nine of 10 (90 percent) hospitals using dilutable disinfectants had one or more malfunctioning dispensers. Twenty-nine of 107 (27.1 percent) systems dispensed product with lower-than-expected concentrations, including 15 (14 percent) with no detectable disinfectant. Introduction Environmental services (EVS) and infection prevention personnel consider factors such as efficacy, wet-contact and kill times, safety, ease of use, and cost when selecting cleaning and disinfection products. Many products are distributed as a concentrate that is diluted to in-use concentrations. The use of dilutable products may reduce costs and can be beneficial for disinfectants that are more stable as a concentrate than at in-use concentrations. Dilutable disinfectants are often dispensed from automated wall-mounted systems that mix concentrated disinfectant and water. However, monitoring is required to ensure that the dispensers are working correctly. Boyce et al. found variations in the concentration of a dilutable quaternary ammonium disinfectant delivered by an automated dispenser; the issues were resolved after installation of water-pressure regulators and modifications of the flow-control devices in concentrate containers. It was recommended that hospitals utilizing dispensing stations conduct periodic testing to verify that appropriate concentrations are being dispensed. Others have demonstrated that automated systems sometimes deliver lower-than-predicted disinfectant concentrations. In a culture survey, we found high rates of surface contamination after completion of post-discharge cleaning and disinfection in some hospitals using automated dispensers. Therefore, we conducted an evaluation of automated dispensing systems in several hospitals. Methods The study protocol was approved by the Cleveland VA Medical Center’s Research and Development Committee. We conducted a point-prevalence evaluation of automated disinfectant dispensing systems in a convenience sample of 10 hospitals from four healthcare systems in five states. For a minimum of five medical-surgical wards and/or intensive care units, we collected 10mL disinfectant samples from dispensers and buckets of in-use disinfectant. The disinfectants included quaternary ammonium disinfectant cleaners, and a peracetic acid/hydrogen peroxide product. For the peracetic acid product, pH was measured with Micro Essential Lab Single-Roll Hydrion pH Test Paper. Peracetic acid concentrations were also measured using a dropper-bottle method with a lower limit-of-detection of 300 ppm. The expected in-use concentration of peracetic acid is roughly 1300 ppm (0.13 percent) with pH roughly 3; 8 samples with more than1,800 ppm were considered to have higher-than-expected concentrations. For the peracetic acid product, the manufacturer recommends quarterly calibration of the systems and provides posters with user instructions (Supplementary material). The instructions include guidance to check a Green/Red low product indicator for when the concentrate bottle should be changed (i.e., change when indicator window shows three-fourths red) and an optional intermittent pH check. For the quaternary ammonium disinfectants, quaternary ammonium concentrations were measured using Micro Essential Lab Hydrion Quaternary Test Paper Kits; the expected in-use concentrations of the products are roughly 700–800 parts per million (ppm) with pH 8–9. To assess the efficacy of samples with lower-than-expected disinfectant levels, the American Society for Testing and Materials (ASTM) standard quantitative carrier disk test method was used with five percent fetal calf serum as soil load. The test organisms included a clinical methicillin-resistant Staphylococcus aureus (MRSA) strain for the quaternary ammonium product and Clostridioides difficile American Type Culture Collection strain 43598 for the peracetic acid product. The exposure times were 5 and 10 minutes for the peracetic acid and quaternary ammonium disinfectants, respectively. For one hospital using the quaternary ammonium product, additional point-prevalence evaluations were conducted after EVS implemented interventions that included increased monitoring of quaternary ammonium concentrations of dispensed product. The supplementary material provides details on the intervention. Results Table 1 Table 2 None of the hospitals reported conducting routine monitoring of disinfectant dispensers. Nine of 10 (90 percent) hospitals had one or more systems dispensing lower-than-expected disinfectant concentrations, and 8 (80 percent) had dispensers that delivered product with no detectable disinfectant (See Table 1). Overall, 29 of 107 (27.1 percent) systems dispensed product with lower-than-expected concentrations, including 15 (14 percent) with no detectable disinfectant. Of 45 samples of peracetic acid product, 26 (57.8 percent) had higher-than-expected peracetic acid concentrations (≥1800 ppm; peak 2,100 ppm), 9 (20 percent) had expected concentrations (1,200–1,500 ppm), 4 (8.9 percent) had lower-than-expected concentrations (300–900 ppm), and 6 (13.3 percent) had undetectable concentrations. pH measurements distinguished dispensers with expected or higher-than-expected peracetic acid disinfectant concentrations (pH around 3) versus those with lower-than-expected concentrations (pH 3.5–5) versus no detectable disinfectant (pH around 6). A second table (See Table 2) shows reasons for malfunction of the 15 systems that dispensed undetectable levels of disinfectant. The identified reasons included concentrate container not being connected correctly (n = 7), concentrate container top being damaged (n = 3), low product indicator not functioning correctly resulting in use of an empty concentrate container (n = 1), and personnel not changing the container when the low product indicator indicated that a change was due (n = 1). In three cases, the reason for the malfunction was not clear. Of 80 in-use disinfectant samples obtained from EVS carts, 27 (33.8 percent) had lower-than-expected disinfectant concentrations, including 14 (17.5 percent) with no detectable disinfectant. One sample with no detectable disinfectant was from a functioning dispenser but the EVS worker acknowledged not obtaining fresh product for days. Of nine employees using product with no detectable disinfectant who were interviewed, three had not noticed that the product was incorrect, whereas six noticed that the product did not smell or appear right but had not notified their supervisor. In four instances, in-use products that EVS personnel identified as disinfectants were dilutable detergents intended for floors. ASTM testing demonstrated that samples with ≤900 ppm of peracetic acid and ≤400 ppm of quaternary ammonium disinfectant resulted in
0 notes
Photo

Cambridge University Press released a study that evaluated the efficacy of automated disinfected dispenser systems in hospitals. The results of the study — which oversaw 10 unique hospitals and four additional healthcare systems across five states — highlighted the importance of improved dispenser monitoring to ensure the correct concentrations of disinfectants are dispensed. Here is the full report: Abstract Automated dispensers that dilute concentrated disinfectants with water are commonly used in healthcare facilities. In a point-prevalence product evaluation, nine of 10 (90 percent) hospitals using dilutable disinfectants had one or more malfunctioning dispensers. Twenty-nine of 107 (27.1 percent) systems dispensed product with lower-than-expected concentrations, including 15 (14 percent) with no detectable disinfectant. Introduction Environmental services (EVS) and infection prevention personnel consider factors such as efficacy, wet-contact and kill times, safety, ease of use, and cost when selecting cleaning and disinfection products. Many products are distributed as a concentrate that is diluted to in-use concentrations. The use of dilutable products may reduce costs and can be beneficial for disinfectants that are more stable as a concentrate than at in-use concentrations. Dilutable disinfectants are often dispensed from automated wall-mounted systems that mix concentrated disinfectant and water. However, monitoring is required to ensure that the dispensers are working correctly. Boyce et al. found variations in the concentration of a dilutable quaternary ammonium disinfectant delivered by an automated dispenser; the issues were resolved after installation of water-pressure regulators and modifications of the flow-control devices in concentrate containers. It was recommended that hospitals utilizing dispensing stations conduct periodic testing to verify that appropriate concentrations are being dispensed. Others have demonstrated that automated systems sometimes deliver lower-than-predicted disinfectant concentrations. In a culture survey, we found high rates of surface contamination after completion of post-discharge cleaning and disinfection in some hospitals using automated dispensers. Therefore, we conducted an evaluation of automated dispensing systems in several hospitals. Methods The study protocol was approved by the Cleveland VA Medical Center’s Research and Development Committee. We conducted a point-prevalence evaluation of automated disinfectant dispensing systems in a convenience sample of 10 hospitals from four healthcare systems in five states. For a minimum of five medical-surgical wards and/or intensive care units, we collected 10mL disinfectant samples from dispensers and buckets of in-use disinfectant. The disinfectants included quaternary ammonium disinfectant cleaners, and a peracetic acid/hydrogen peroxide product. For the peracetic acid product, pH was measured with Micro Essential Lab Single-Roll Hydrion pH Test Paper. Peracetic acid concentrations were also measured using a dropper-bottle method with a lower limit-of-detection of 300 ppm. The expected in-use concentration of peracetic acid is roughly 1300 ppm (0.13 percent) with pH roughly 3; 8 samples with more than1,800 ppm were considered to have higher-than-expected concentrations. For the peracetic acid product, the manufacturer recommends quarterly calibration of the systems and provides posters with user instructions (Supplementary material). The instructions include guidance to check a Green/Red low product indicator for when the concentrate bottle should be changed (i.e., change when indicator window shows three-fourths red) and an optional intermittent pH check. For the quaternary ammonium disinfectants, quaternary ammonium concentrations were measured using Micro Essential Lab Hydrion Quaternary Test Paper Kits; the expected in-use concentrations of the products are roughly 700–800 parts per million (ppm) with pH 8–9. To assess the efficacy of samples with lower-than-expected disinfectant levels, the American Society for Testing and Materials (ASTM) standard quantitative carrier disk test method was used with five percent fetal calf serum as soil load. The test organisms included a clinical methicillin-resistant Staphylococcus aureus (MRSA) strain for the quaternary ammonium product and Clostridioides difficile American Type Culture Collection strain 43598 for the peracetic acid product. The exposure times were 5 and 10 minutes for the peracetic acid and quaternary ammonium disinfectants, respectively. For one hospital using the quaternary ammonium product, additional point-prevalence evaluations were conducted after EVS implemented interventions that included increased monitoring of quaternary ammonium concentrations of dispensed product. The supplementary material provides details on the intervention. Results Table 1 Table 2 None of the hospitals reported conducting routine monitoring of disinfectant dispensers. Nine of 10 (90 percent) hospitals had one or more systems dispensing lower-than-expected disinfectant concentrations, and 8 (80 percent) had dispensers that delivered product with no detectable disinfectant (See Table 1). Overall, 29 of 107 (27.1 percent) systems dispensed product with lower-than-expected concentrations, including 15 (14 percent) with no detectable disinfectant. Of 45 samples of peracetic acid product, 26 (57.8 percent) had higher-than-expected peracetic acid concentrations (≥1800 ppm; peak 2,100 ppm), 9 (20 percent) had expected concentrations (1,200–1,500 ppm), 4 (8.9 percent) had lower-than-expected concentrations (300–900 ppm), and 6 (13.3 percent) had undetectable concentrations. pH measurements distinguished dispensers with expected or higher-than-expected peracetic acid disinfectant concentrations (pH around 3) versus those with lower-than-expected concentrations (pH 3.5–5) versus no detectable disinfectant (pH around 6). A second table (See Table 2) shows reasons for malfunction of the 15 systems that dispensed undetectable levels of disinfectant. The identified reasons included concentrate container not being connected correctly (n = 7), concentrate container top being damaged (n = 3), low product indicator not functioning correctly resulting in use of an empty concentrate container (n = 1), and personnel not changing the container when the low product indicator indicated that a change was due (n = 1). In three cases, the reason for the malfunction was not clear. Of 80 in-use disinfectant samples obtained from EVS carts, 27 (33.8 percent) had lower-than-expected disinfectant concentrations, including 14 (17.5 percent) with no detectable disinfectant. One sample with no detectable disinfectant was from a functioning dispenser but the EVS worker acknowledged not obtaining fresh product for days. Of nine employees using product with no detectable disinfectant who were interviewed, three had not noticed that the product was incorrect, whereas six noticed that the product did not smell or appear right but had not notified their supervisor. In four instances, in-use products that EVS personnel identified as disinfectants were dilutable detergents intended for floors. ASTM testing demonstrated that samples with ≤900 ppm of peracetic acid and ≤400 ppm of quaternary ammonium disinfectant resulted in
0 notes
Photo

Cambridge University Press released a study that evaluated the efficacy of automated disinfected dispenser systems in hospitals. The results of the study — which oversaw 10 unique hospitals and four additional healthcare systems across five states — highlighted the importance of improved dispenser monitoring to ensure the correct concentrations of disinfectants are dispensed. Here is the full report: Abstract Automated dispensers that dilute concentrated disinfectants with water are commonly used in healthcare facilities. In a point-prevalence product evaluation, nine of 10 (90 percent) hospitals using dilutable disinfectants had one or more malfunctioning dispensers. Twenty-nine of 107 (27.1 percent) systems dispensed product with lower-than-expected concentrations, including 15 (14 percent) with no detectable disinfectant. Introduction Environmental services (EVS) and infection prevention personnel consider factors such as efficacy, wet-contact and kill times, safety, ease of use, and cost when selecting cleaning and disinfection products. Many products are distributed as a concentrate that is diluted to in-use concentrations. The use of dilutable products may reduce costs and can be beneficial for disinfectants that are more stable as a concentrate than at in-use concentrations. Dilutable disinfectants are often dispensed from automated wall-mounted systems that mix concentrated disinfectant and water. However, monitoring is required to ensure that the dispensers are working correctly. Boyce et al. found variations in the concentration of a dilutable quaternary ammonium disinfectant delivered by an automated dispenser; the issues were resolved after installation of water-pressure regulators and modifications of the flow-control devices in concentrate containers. It was recommended that hospitals utilizing dispensing stations conduct periodic testing to verify that appropriate concentrations are being dispensed. Others have demonstrated that automated systems sometimes deliver lower-than-predicted disinfectant concentrations. In a culture survey, we found high rates of surface contamination after completion of post-discharge cleaning and disinfection in some hospitals using automated dispensers. Therefore, we conducted an evaluation of automated dispensing systems in several hospitals. Methods The study protocol was approved by the Cleveland VA Medical Center’s Research and Development Committee. We conducted a point-prevalence evaluation of automated disinfectant dispensing systems in a convenience sample of 10 hospitals from four healthcare systems in five states. For a minimum of five medical-surgical wards and/or intensive care units, we collected 10mL disinfectant samples from dispensers and buckets of in-use disinfectant. The disinfectants included quaternary ammonium disinfectant cleaners, and a peracetic acid/hydrogen peroxide product. For the peracetic acid product, pH was measured with Micro Essential Lab Single-Roll Hydrion pH Test Paper. Peracetic acid concentrations were also measured using a dropper-bottle method with a lower limit-of-detection of 300 ppm. The expected in-use concentration of peracetic acid is roughly 1300 ppm (0.13 percent) with pH roughly 3; 8 samples with more than1,800 ppm were considered to have higher-than-expected concentrations. For the peracetic acid product, the manufacturer recommends quarterly calibration of the systems and provides posters with user instructions (Supplementary material). The instructions include guidance to check a Green/Red low product indicator for when the concentrate bottle should be changed (i.e., change when indicator window shows three-fourths red) and an optional intermittent pH check. For the quaternary ammonium disinfectants, quaternary ammonium concentrations were measured using Micro Essential Lab Hydrion Quaternary Test Paper Kits; the expected in-use concentrations of the products are roughly 700–800 parts per million (ppm) with pH 8–9. To assess the efficacy of samples with lower-than-expected disinfectant levels, the American Society for Testing and Materials (ASTM) standard quantitative carrier disk test method was used with five percent fetal calf serum as soil load. The test organisms included a clinical methicillin-resistant Staphylococcus aureus (MRSA) strain for the quaternary ammonium product and Clostridioides difficile American Type Culture Collection strain 43598 for the peracetic acid product. The exposure times were 5 and 10 minutes for the peracetic acid and quaternary ammonium disinfectants, respectively. For one hospital using the quaternary ammonium product, additional point-prevalence evaluations were conducted after EVS implemented interventions that included increased monitoring of quaternary ammonium concentrations of dispensed product. The supplementary material provides details on the intervention. Results Table 1 Table 2 None of the hospitals reported conducting routine monitoring of disinfectant dispensers. Nine of 10 (90 percent) hospitals had one or more systems dispensing lower-than-expected disinfectant concentrations, and 8 (80 percent) had dispensers that delivered product with no detectable disinfectant (See Table 1). Overall, 29 of 107 (27.1 percent) systems dispensed product with lower-than-expected concentrations, including 15 (14 percent) with no detectable disinfectant. Of 45 samples of peracetic acid product, 26 (57.8 percent) had higher-than-expected peracetic acid concentrations (≥1800 ppm; peak 2,100 ppm), 9 (20 percent) had expected concentrations (1,200–1,500 ppm), 4 (8.9 percent) had lower-than-expected concentrations (300–900 ppm), and 6 (13.3 percent) had undetectable concentrations. pH measurements distinguished dispensers with expected or higher-than-expected peracetic acid disinfectant concentrations (pH around 3) versus those with lower-than-expected concentrations (pH 3.5–5) versus no detectable disinfectant (pH around 6). A second table (See Table 2) shows reasons for malfunction of the 15 systems that dispensed undetectable levels of disinfectant. The identified reasons included concentrate container not being connected correctly (n = 7), concentrate container top being damaged (n = 3), low product indicator not functioning correctly resulting in use of an empty concentrate container (n = 1), and personnel not changing the container when the low product indicator indicated that a change was due (n = 1). In three cases, the reason for the malfunction was not clear. Of 80 in-use disinfectant samples obtained from EVS carts, 27 (33.8 percent) had lower-than-expected disinfectant concentrations, including 14 (17.5 percent) with no detectable disinfectant. One sample with no detectable disinfectant was from a functioning dispenser but the EVS worker acknowledged not obtaining fresh product for days. Of nine employees using product with no detectable disinfectant who were interviewed, three had not noticed that the product was incorrect, whereas six noticed that the product did not smell or appear right but had not notified their supervisor. In four instances, in-use products that EVS personnel identified as disinfectants were dilutable detergents intended for floors. ASTM testing demonstrated that samples with ≤900 ppm of peracetic acid and ≤400 ppm of quaternary ammonium disinfectant resulted in
0 notes
Photo

Cambridge University Press released a study that evaluated the efficacy of automated disinfected dispenser systems in hospitals. The results of the study — which oversaw 10 unique hospitals and four additional healthcare systems across five states — highlighted the importance of improved dispenser monitoring to ensure the correct concentrations of disinfectants are dispensed. Here is the full report: Abstract Automated dispensers that dilute concentrated disinfectants with water are commonly used in healthcare facilities. In a point-prevalence product evaluation, nine of 10 (90 percent) hospitals using dilutable disinfectants had one or more malfunctioning dispensers. Twenty-nine of 107 (27.1 percent) systems dispensed product with lower-than-expected concentrations, including 15 (14 percent) with no detectable disinfectant. Introduction Environmental services (EVS) and infection prevention personnel consider factors such as efficacy, wet-contact and kill times, safety, ease of use, and cost when selecting cleaning and disinfection products. Many products are distributed as a concentrate that is diluted to in-use concentrations. The use of dilutable products may reduce costs and can be beneficial for disinfectants that are more stable as a concentrate than at in-use concentrations. Dilutable disinfectants are often dispensed from automated wall-mounted systems that mix concentrated disinfectant and water. However, monitoring is required to ensure that the dispensers are working correctly. Boyce et al. found variations in the concentration of a dilutable quaternary ammonium disinfectant delivered by an automated dispenser; the issues were resolved after installation of water-pressure regulators and modifications of the flow-control devices in concentrate containers. It was recommended that hospitals utilizing dispensing stations conduct periodic testing to verify that appropriate concentrations are being dispensed. Others have demonstrated that automated systems sometimes deliver lower-than-predicted disinfectant concentrations. In a culture survey, we found high rates of surface contamination after completion of post-discharge cleaning and disinfection in some hospitals using automated dispensers. Therefore, we conducted an evaluation of automated dispensing systems in several hospitals. Methods The study protocol was approved by the Cleveland VA Medical Center’s Research and Development Committee. We conducted a point-prevalence evaluation of automated disinfectant dispensing systems in a convenience sample of 10 hospitals from four healthcare systems in five states. For a minimum of five medical-surgical wards and/or intensive care units, we collected 10mL disinfectant samples from dispensers and buckets of in-use disinfectant. The disinfectants included quaternary ammonium disinfectant cleaners, and a peracetic acid/hydrogen peroxide product. For the peracetic acid product, pH was measured with Micro Essential Lab Single-Roll Hydrion pH Test Paper. Peracetic acid concentrations were also measured using a dropper-bottle method with a lower limit-of-detection of 300 ppm. The expected in-use concentration of peracetic acid is roughly 1300 ppm (0.13 percent) with pH roughly 3; 8 samples with more than1,800 ppm were considered to have higher-than-expected concentrations. For the peracetic acid product, the manufacturer recommends quarterly calibration of the systems and provides posters with user instructions (Supplementary material). The instructions include guidance to check a Green/Red low product indicator for when the concentrate bottle should be changed (i.e., change when indicator window shows three-fourths red) and an optional intermittent pH check. For the quaternary ammonium disinfectants, quaternary ammonium concentrations were measured using Micro Essential Lab Hydrion Quaternary Test Paper Kits; the expected in-use concentrations of the products are roughly 700–800 parts per million (ppm) with pH 8–9. To assess the efficacy of samples with lower-than-expected disinfectant levels, the American Society for Testing and Materials (ASTM) standard quantitative carrier disk test method was used with five percent fetal calf serum as soil load. The test organisms included a clinical methicillin-resistant Staphylococcus aureus (MRSA) strain for the quaternary ammonium product and Clostridioides difficile American Type Culture Collection strain 43598 for the peracetic acid product. The exposure times were 5 and 10 minutes for the peracetic acid and quaternary ammonium disinfectants, respectively. For one hospital using the quaternary ammonium product, additional point-prevalence evaluations were conducted after EVS implemented interventions that included increased monitoring of quaternary ammonium concentrations of dispensed product. The supplementary material provides details on the intervention. Results Table 1 Table 2 None of the hospitals reported conducting routine monitoring of disinfectant dispensers. Nine of 10 (90 percent) hospitals had one or more systems dispensing lower-than-expected disinfectant concentrations, and 8 (80 percent) had dispensers that delivered product with no detectable disinfectant (See Table 1). Overall, 29 of 107 (27.1 percent) systems dispensed product with lower-than-expected concentrations, including 15 (14 percent) with no detectable disinfectant. Of 45 samples of peracetic acid product, 26 (57.8 percent) had higher-than-expected peracetic acid concentrations (≥1800 ppm; peak 2,100 ppm), 9 (20 percent) had expected concentrations (1,200–1,500 ppm), 4 (8.9 percent) had lower-than-expected concentrations (300–900 ppm), and 6 (13.3 percent) had undetectable concentrations. pH measurements distinguished dispensers with expected or higher-than-expected peracetic acid disinfectant concentrations (pH around 3) versus those with lower-than-expected concentrations (pH 3.5–5) versus no detectable disinfectant (pH around 6). A second table (See Table 2) shows reasons for malfunction of the 15 systems that dispensed undetectable levels of disinfectant. The identified reasons included concentrate container not being connected correctly (n = 7), concentrate container top being damaged (n = 3), low product indicator not functioning correctly resulting in use of an empty concentrate container (n = 1), and personnel not changing the container when the low product indicator indicated that a change was due (n = 1). In three cases, the reason for the malfunction was not clear. Of 80 in-use disinfectant samples obtained from EVS carts, 27 (33.8 percent) had lower-than-expected disinfectant concentrations, including 14 (17.5 percent) with no detectable disinfectant. One sample with no detectable disinfectant was from a functioning dispenser but the EVS worker acknowledged not obtaining fresh product for days. Of nine employees using product with no detectable disinfectant who were interviewed, three had not noticed that the product was incorrect, whereas six noticed that the product did not smell or appear right but had not notified their supervisor. In four instances, in-use products that EVS personnel identified as disinfectants were dilutable detergents intended for floors. ASTM testing demonstrated that samples with ≤900 ppm of peracetic acid and ≤400 ppm of quaternary ammonium disinfectant resulted in
0 notes
Photo

Cambridge University Press released a study that evaluated the efficacy of automated disinfected dispenser systems in hospitals. The results of the study — which oversaw 10 unique hospitals and four additional healthcare systems across five states — highlighted the importance of improved dispenser monitoring to ensure the correct concentrations of disinfectants are dispensed. Here is the full report: Abstract Automated dispensers that dilute concentrated disinfectants with water are commonly used in healthcare facilities. In a point-prevalence product evaluation, nine of 10 (90 percent) hospitals using dilutable disinfectants had one or more malfunctioning dispensers. Twenty-nine of 107 (27.1 percent) systems dispensed product with lower-than-expected concentrations, including 15 (14 percent) with no detectable disinfectant. Introduction Environmental services (EVS) and infection prevention personnel consider factors such as efficacy, wet-contact and kill times, safety, ease of use, and cost when selecting cleaning and disinfection products. Many products are distributed as a concentrate that is diluted to in-use concentrations. The use of dilutable products may reduce costs and can be beneficial for disinfectants that are more stable as a concentrate than at in-use concentrations. Dilutable disinfectants are often dispensed from automated wall-mounted systems that mix concentrated disinfectant and water. However, monitoring is required to ensure that the dispensers are working correctly. Boyce et al. found variations in the concentration of a dilutable quaternary ammonium disinfectant delivered by an automated dispenser; the issues were resolved after installation of water-pressure regulators and modifications of the flow-control devices in concentrate containers. It was recommended that hospitals utilizing dispensing stations conduct periodic testing to verify that appropriate concentrations are being dispensed. Others have demonstrated that automated systems sometimes deliver lower-than-predicted disinfectant concentrations. In a culture survey, we found high rates of surface contamination after completion of post-discharge cleaning and disinfection in some hospitals using automated dispensers. Therefore, we conducted an evaluation of automated dispensing systems in several hospitals. Methods The study protocol was approved by the Cleveland VA Medical Center’s Research and Development Committee. We conducted a point-prevalence evaluation of automated disinfectant dispensing systems in a convenience sample of 10 hospitals from four healthcare systems in five states. For a minimum of five medical-surgical wards and/or intensive care units, we collected 10mL disinfectant samples from dispensers and buckets of in-use disinfectant. The disinfectants included quaternary ammonium disinfectant cleaners, and a peracetic acid/hydrogen peroxide product. For the peracetic acid product, pH was measured with Micro Essential Lab Single-Roll Hydrion pH Test Paper. Peracetic acid concentrations were also measured using a dropper-bottle method with a lower limit-of-detection of 300 ppm. The expected in-use concentration of peracetic acid is roughly 1300 ppm (0.13 percent) with pH roughly 3; 8 samples with more than1,800 ppm were considered to have higher-than-expected concentrations. For the peracetic acid product, the manufacturer recommends quarterly calibration of the systems and provides posters with user instructions (Supplementary material). The instructions include guidance to check a Green/Red low product indicator for when the concentrate bottle should be changed (i.e., change when indicator window shows three-fourths red) and an optional intermittent pH check. For the quaternary ammonium disinfectants, quaternary ammonium concentrations were measured using Micro Essential Lab Hydrion Quaternary Test Paper Kits; the expected in-use concentrations of the products are roughly 700–800 parts per million (ppm) with pH 8–9. To assess the efficacy of samples with lower-than-expected disinfectant levels, the American Society for Testing and Materials (ASTM) standard quantitative carrier disk test method was used with five percent fetal calf serum as soil load. The test organisms included a clinical methicillin-resistant Staphylococcus aureus (MRSA) strain for the quaternary ammonium product and Clostridioides difficile American Type Culture Collection strain 43598 for the peracetic acid product. The exposure times were 5 and 10 minutes for the peracetic acid and quaternary ammonium disinfectants, respectively. For one hospital using the quaternary ammonium product, additional point-prevalence evaluations were conducted after EVS implemented interventions that included increased monitoring of quaternary ammonium concentrations of dispensed product. The supplementary material provides details on the intervention. Results Table 1 Table 2 None of the hospitals reported conducting routine monitoring of disinfectant dispensers. Nine of 10 (90 percent) hospitals had one or more systems dispensing lower-than-expected disinfectant concentrations, and 8 (80 percent) had dispensers that delivered product with no detectable disinfectant (See Table 1). Overall, 29 of 107 (27.1 percent) systems dispensed product with lower-than-expected concentrations, including 15 (14 percent) with no detectable disinfectant. Of 45 samples of peracetic acid product, 26 (57.8 percent) had higher-than-expected peracetic acid concentrations (≥1800 ppm; peak 2,100 ppm), 9 (20 percent) had expected concentrations (1,200–1,500 ppm), 4 (8.9 percent) had lower-than-expected concentrations (300–900 ppm), and 6 (13.3 percent) had undetectable concentrations. pH measurements distinguished dispensers with expected or higher-than-expected peracetic acid disinfectant concentrations (pH around 3) versus those with lower-than-expected concentrations (pH 3.5–5) versus no detectable disinfectant (pH around 6). A second table (See Table 2) shows reasons for malfunction of the 15 systems that dispensed undetectable levels of disinfectant. The identified reasons included concentrate container not being connected correctly (n = 7), concentrate container top being damaged (n = 3), low product indicator not functioning correctly resulting in use of an empty concentrate container (n = 1), and personnel not changing the container when the low product indicator indicated that a change was due (n = 1). In three cases, the reason for the malfunction was not clear. Of 80 in-use disinfectant samples obtained from EVS carts, 27 (33.8 percent) had lower-than-expected disinfectant concentrations, including 14 (17.5 percent) with no detectable disinfectant. One sample with no detectable disinfectant was from a functioning dispenser but the EVS worker acknowledged not obtaining fresh product for days. Of nine employees using product with no detectable disinfectant who were interviewed, three had not noticed that the product was incorrect, whereas six noticed that the product did not smell or appear right but had not notified their supervisor. In four instances, in-use products that EVS personnel identified as disinfectants were dilutable detergents intended for floors. ASTM testing demonstrated that samples with ≤900 ppm of peracetic acid and ≤400 ppm of quaternary ammonium disinfectant resulted in
0 notes
Text
Merging design and computer science in creative ways
New Post has been published on https://sunalei.org/news/merging-design-and-computer-science-in-creative-ways/
Merging design and computer science in creative ways
The speed with which new technologies hit the market is nothing compared to the speed with which talented researchers find creative ways to use them, train them, even turn them into things we can’t live without. One such researcher is MIT MAD Fellow Alexander Htet Kyaw, a graduate student pursuing dual master’s degrees in architectural studies in computation and in electrical engineering and computer science.
Kyaw takes technologies like artificial intelligence, augmented reality, and robotics, and combines them with gesture, speech, and object recognition to create human-AI workflows that have the potential to interact with our built environment, change how we shop, design complex structures, and make physical things.
One of his latest innovations is Curator AI, for which he and his MIT graduate student partners took first prize — $26,000 in OpenAI products and cash — at the MIT AI Conference’s AI Build: Generative Voice AI Solutions, a weeklong hackathon at MIT with final presentations held last fall in New York City. Working with Kyaw were Richa Gupta (architecture) and Bradley Bunch, Nidhish Sagar, and Michael Won — all from the MIT Department of Electrical Engineering and Computer Science (EECS).
Curator AI is designed to streamline online furniture shopping by providing context-aware product recommendations using AI and AR. The platform uses AR to take the dimensions of a room with locations of windows, doors, and existing furniture. Users can then speak to the software to describe what new furnishings they want, and the system will use a vision-language AI model to search for and display various options that match both the user’s prompts and the room’s visual characteristics.
“Shoppers can choose from the suggested options, visualize products in AR, and use natural language to ask for modifications to the search, making the furniture selection process more intuitive, efficient, and personalized,” Kyaw says. “The problem we’re trying to solve is that most people don’t know where to start when furnishing a room, so we developed Curator AI to provide smart, contextual recommendations based on what your room looks like.” Although Curator AI was developed for furniture shopping, it could be expanded for use in other markets.
Another example of Kyaw’s work is Estimate, a product that he and three other graduate students created during the MIT Sloan Product Tech Conference’s hackathon in March 2024. The focus of that competition was to help small businesses; Kyaw and team decided to base their work on a painting company in Cambridge that employs 10 people. Estimate uses AR and an object-recognition AI technology to take the exact measurements of a room and generate a detailed cost estimate for a renovation and/or paint job. It also leverages generative AI to display images of the room or rooms as they might look like after painting or renovating, and generates an invoice once the project is complete.
The team won that hackathon and $5,000 in cash. Kyaw’s teammates were Guillaume Allegre, May Khine, and Anna Mathy, all of whom graduated from MIT in 2024 with master’s degrees in business analytics.
In April, Kyaw will give a TedX talk at his alma mater, Cornell University, in which he’ll describe Curator AI, Estimate, and other projects that use AI, AR, and robotics to design and build things.
One of these projects is Unlog, for which Kyaw connected AR with gesture recognition to build a software that takes input from the touch of a fingertip on the surface of a material, or even in the air, to map the dimensions of building components. That’s how Unlog — a towering art sculpture made from ash logs that stands on the Cornell campus — came about.
Play video
Gesture Recognition for Feedback-Based Mixed Reality and Robotic Fabrication of the Unlog Tower Video: Alexander Htet Kyaw
Unlog represents the possibility that structures can be built directly from a whole log, rather than having the log travel to a lumber mill to be turned into planks or two-by-fours, then shipped to a wholesaler or retailer. It’s a good representation of Kyaw’s desire to use building materials in a more sustainable way. A paper on this work, “Gestural Recognition for Feedback-Based Mixed Reality Fabrication a Case Study of the UnLog Tower,” was published by Kyaw, Leslie Lok, Lawson Spencer, and Sasa Zivkovic in the Proceedings of the 5th International Conference on Computational Design and Robotic Fabrication, January 2024.
Another system Kyaw developed integrates physics simulation, gesture recognition, and AR to design active bending structures built with bamboo poles. Gesture recognition allows users to manipulate digital bamboo modules in AR, and the physics simulation is integrated to visualize how the bamboo bends and where to attach the bamboo poles in ways that create a stable structure. This work appeared in the Proceedings of the 41st Education and Research in Computer Aided Architectural Design in Europe, August 2023, as “Active Bending in Physics-Based Mixed Reality: The Design and Fabrication of a Reconfigurable Modular Bamboo System.”
Kyaw pitched a similar idea using bamboo modules to create deployable structures last year to MITdesignX, an MIT MAD program that selects promising startups and provides coaching and funding to launch them. Kyaw has since founded BendShelters to build the prefabricated, modular bamboo shelters and community spaces for refugees and displaced persons in Myanmar, his home country.
“Where I grew up, in Myanmar, I’ve seen a lot of day-to-day effects of climate change and extreme poverty,” Kyaw says. “There’s a huge refugee crisis in the country, and I want to think about how I can contribute back to my community.”
His work with BendShelters has been recognized by MIT Sandbox, PKG Social Innovation Challenge, and the Amazon Robotics’ Prize for Social Good.
At MIT, Kyaw is collaborating with Professor Neil Gershenfeld, director of the Center for Bits and Atoms, and PhD student Miana Smith to use speech recognition, 3D generative AI, and robotic arms to create a workflow that can build objects in an accessible, on-demand, and sustainable way. Kyaw holds bachelor’s degrees in architecture and computer science from Cornell. Last year, he was awarded an SJA Fellowship from the Steve Jobs Archive, which provides funding for projects at the intersection of technology and the arts.
“I enjoy exploring different kinds of technologies to design and make things,” Kyaw says. “Being part of MAD has made me think about how all my work connects, and helped clarify my intentions. My research vision is to design and develop systems and products that enable natural interactions between humans, machines, and the world around us.”
0 notes