#World Professional Association for Transgender Health
Text

By: Gerald Posner
Published: Mar 4, 2024
Newly leaked files from the world’s leading transgender health-care organization reveal it is pushing hormonal and surgical transitions for minors, including stomach-wrenching experimental procedures designed to create sexless bodies that resemble department-store mannequins.
The World Professional Association for Transgender Health documents demonstrate it’s controlled by gender ideologues who push aside concerns about whether children and adolescents can consent to medical treatments that WPATH members privately acknowledge often have devastating and permanent side effects.
Yet the US government, American doctors and prominent organizations nonetheless rely on WPATH guidelines for advice on treating our youth.
The files — jaw-dropping conversations from a WPATH internal messaging board and a video of an Identity Evolution Workshop panel — were provided to journalist Michael Shellenberger, who shared the documents with me.
Shellenberger’s nonprofit Environmental Progress will release a scathing summary report, comparing the WPATH promotion of “the pseudoscientific surgical destruction of healthy genitals in vulnerable people” to the mid-20th-century use of lobotomies, “the pseudoscientific surgical destruction of healthy brains.”
‘Arbitrary’ age limits
The comparison to one of history’s greatest medical scandals is not hyperbole.
It is particularly true, as the files show repeatedly, when it involves WPATH’s radical approach to minors.
When the organization adopted in 2022 its current Standards of Care — relied on by the National Institutes of Health, the World Health Organization and every major American medical and psychiatric association — it scrapped a draft chapter about ethics and removed minimum-age requirements for children starting puberty blockers or undergoing sexual-modification surgeries.
It had previously recommended 16 to start hormones and 17 for surgery.
Not surprisingly, age comes up frequently in the WPATH files, from concerns about whether a developmentally delayed 13-year-old can start on puberty blockers to whether the growth of a 10-year-old girl will be stunted by hormones.
During one conversation, a member asked for advice about a 14-year-old patient, a boy who identified as a girl and had begun transitioning at 4.
The child insisted on a vaginoplasty, a surgery that removes the penis, testicles and scrotum and repositions tissue to create a nonfunctioning pseudo-vagina. It requires a lifetime of dilation. Was he too young at 14?
Marci Bowers, WPATH’s president and a California-based pelvic and gynecologic surgeon who is herself transgender, said she considered any age limit “arbitrary.”
But she would not do it. Why?
“The tissue is too immature, dilation routine too critical.”
In lay terms, that means boys who are too young do not have enough penal tissue for the surgery and the surgeon must harvest intestinal lining to build the faux vagina. Even Bowers admits that can lead to “problematic surgical outcomes.”
She would know since she has performed more than 2,000 vaginoplasties. Her highest-profile patient is 17-year-old Jazz Jennings, the transgender star of reality TV show “I Am Jazz.”
Three corrective surgeries were required to fix problems from the original vaginoplasty.
“She had a very difficult surgical course,” Bowers admitted in a 2022 appearance on the show. “We knew it would be tough — it turned out tougher than any of us imagined.”
Still, Bowers told her colleagues in the internal discussion forum of the best age for an adolescent to undergo surgery: “sometime before the end of high school does make some sense in that they are under the watch of parents in the home they grew up in.”
Christine McGinn, a Pennsylvania plastic surgeon and herself transgender, agreed. McGinn has performed “about 20 vaginoplasties in patients under 18” and thinks the “ideal time in the U.S. is surgery the summer before the last year of high school. I have heard many other surgeons echo this.”
Waiting until teens are older than 18 and in college is problematic, she said: “there are too many stressors in college that limit patients’ ability to dilate.”
Dangers downplayed
WPATH assures patients that surgical and hormonal interventions are tested and safe. It is a different matter in private.
President Bowers, for instance, said publicly in 2022 that puberty blockers are “completely reversible,” although in the internal forum she conceded it is “in its infancy.”
What about children who are infertile for life since they started hormone blockers before they reached puberty?
Bowers told her colleagues the “fertility question has no research.”
At other stages, members talk frankly about the complications for the transition surgery for girls, a phalloplasty in which a nonfunctioning pseudo-penis is fashioned from either forearm or thigh tissue.
It requires a full hysterectomy and surgical removal of the vagina. They also discuss other serious consequences, including pelvic inflammatory disease, vaginal atrophy, abnormal pap tests and incontinence.
A 16-year-old girl who had been on puberty blockers for several years before she was put on testosterone for a year had developed two liver tumors that an oncologist concluded the hormones had caused. Another member described “a young patient on testosterone for 3 years” who had developed “vaginal/pelvic pain/spotting . . . [and] atrophy with the persistent yellow discharge.”
Several colleagues described patients with similar conditions, some with debilitating bowel problems or bleeding and excruciating pain during sex (“feeling like broken glass”).
Vaginal estrogen creams and moisturizers as well as hyaluronic acid suppositories “can be helpful.”
One WPATH member seemed surprised: “The transgender people under my surveillance do not complain about this matter. However, I confess that I have never asked them about it.”
Rise of ‘de-gender’ surgery
The litany of transition surgery’s side effects did not stop WPATH from endorsing far more radical “nullification” surgeries for patients who do not feel either male or female and identify only as nonbinary.
Several dozen so-called “de-gendering” surgeries are designed to create a sexless, smooth cosmetic appearance that is unknown in nature. There is even an experimental “bi-genital” surgery that attempts to construct a second set of genitals.
In 2017, when tabloids reported a 22-year-old man had spent $50,000 to surgically remove his sex organs so he could “transform into a genderless extra-terrestrial,” it seemed a one-off oddity.
But WPATH has enshrined that concept in its Standard of Care — the same document in which the group endorsed for the time first time chemical or surgical castration for patients who identify as eunuchs. (WPATH even linked to the Eunuch Archives, where men anonymously share castration fetishes.)
These science-fiction-like surgeries are not only reserved for adults.
“How do we come up with appropriate standards for non-binary patients?” asked Thomas Satterwhite, a San Francisco-based plastic surgeon who has operated on dozens of patients younger than 18 since 2014. “I’ve found more and more patients recently requesting ‘non-standard’ procedures.”
What are nonstandard procedures? They include “non-binary top surgery,” a mastectomy without nipples. There are brutal procedures for girls that eliminate all or part of the vagina and for boys that amputate the penis, scrotum and testicles.
The goal, as one San Francisco surgical clinic proclaims on its website, “is a smooth, neutral body that is cosmetically free of sexual identification.” On TikTok the trend is called a “flat front.”
‘Too young to understand‘
A particularly intense subject of discussion was whether minors could understand the lifelong consequences of their gender treatments. Minors are presumed by law to be incapable of making an informed decision about having a vasectomy or tubal ligation.
Gender surgeries are an exception, however.
WPATH’s Standard of Care allows all procedures so long as the minor “demonstrates the emotional and cognitive maturity required to provide informed consent/assent for the treatment.”
In a May 2022 internal workshop, “Identity Evolution,” WPATH members conceded that was all but impossible.
Daniel Metzger, the British Columbia endocrinologist who cowrote the Canadian Pediatric Society’s position paper on health care for trans minors, said, “I think the thing you have to remember about kids is that we’re often explaining these sorts of things to people who haven’t even had biology in high school yet.”
Metzger noted adolescents are incapable of appreciating the lifelong consequence of infertility. “It’s always a good theory that you talk about fertility preservation with a 14-year-old,” he said, “but I know I’m talking to a blank wall. They’d be like, ‘ew, kids, babies, gross.’ Or, the usual answer is, ‘I’m just going to adopt.’ And then you ask them, ‘Well, what does that involve? Like, how much does it cost?’ ‘Oh, I thought you just like went to the orphanage, and they gave you a baby.’ . . . I think now that I follow a lot of kids into their mid-twenties, I’m always like, ‘Oh, the dog isn’t doing it for you, right?’”
There is extensive research showing adolescent brains are wired to have little control over rash behavior and are not capable of grasping the magnitude of decisions with lifelong consequences. It is why society doesn’t allow teens to get tattoos or buy guns. Car-rental agencies set 25 as the minimum age for renting a car, and Sweden sets the same limit for deciding on sterilization.
Detransitioners ignored, shunned
Although many WPATH members privately doubt that adolescents can give truly informed consent to life-altering procedures, they must affirm whatever children say about their gender.
Unless, the WPATH files disclose, the patient wants to reverse course and become a so-called detransitioner.
WPATH members mostly dismiss those cases as insignificant or overblown by the media and question whether minors who want to revert to their birth sex really understand what they are doing.
It’s a question that would never be asked for minors who declared themselves to be gender dysphoric.
One case involved a 17-year-old boy, just graduated from high school, who had been on testosterone for two years. He was reported to be “very distraught and angry. He reports he feels he was brainwashed and is upset by the permanent changes to his body.”
A self-described “queer therapist” did not believe any young person could be brainwashed. “In my experience, those stories come from people who have an active agenda against the rights of trans people.”
WPATH President Bowers said that “I do see talk of the phenomenon [detransitioners] as distracting from the many challenges we face.”
‘Frankenstein files’
The leaked files put a spotlight on the danger of mixing ideological activism with medicine and science. They should serve as an urgent wakeup call for the medical associations and government agencies that rely on WPATH guidance for transgender health.
The files might even prompt investigations into how those with distorted personal agendas seized control of the organization at the expense of science and patients.
Investigating what has gone wrong at WPATH might prove uncomfortable for some gender progressives in the Biden administration, none more so than Adm. Rachel Levine, the assistant secretary for health. Levine, the first transgender four-star military officer, is a WPATH member and has lavished praise on the organization.
She says it “assesses the full state of the science and provides substantive, rigorously analyzed, peer-reviewed recommendations to the medical community on how best to care for patients who are transgender or gender non-binary. It is free of any agenda other than to ensure that medical decisions are informed by science.”
Either Levine is unaware of the hormonal and surgical experimentation the group promotes or refuses to acknowledge it.
“The Frankenstein files.”
That is how a pediatrician described the leaked documents after I shared them with her.
Unfortunately, this is no horror novel.
It is a medical travesty playing out in real time, and the casualties are our children.
#Gerald Posner#Michael Shellenberger#WPATH#World Professional Association for Transgender Health#Mia Hughes#WPATH Files#The WPATH Files#medical corruption#medical malpractice#medical scandal#unethical#gender ideology#gender identity ideology#queer theory#first do no harm#religion is a mental illness
27 notes
·
View notes
Text
“There is no centralized tracking of blocker prescriptions in the United States.”
By Megan Twohey and Christina Jewett
Nov. 14, 2022
The medical guidance was direct.
Eleven-year-old Emma Basques had identified as a girl since toddlerhood. Now, as she worried about male puberty starting, a Phoenix pediatrician advised: Take a drug to stop it.
At 13, Jacy Chavira felt increasingly uncomfortable with her maturing body and was beginning to believe she was a boy. Use the drug, her endocrinologist in Southern California recommended, and puberty would be suspended.
An 11-year-old in New York with deepening depression expressed a desire to no longer be a girl. A therapist told the family the drug was the preteen’s best option, and a local doctor agreed.
“‘Puberty blockers really help kids like this,’” the child’s mother recalled the therapist saying. “It was presented as a tourniquet that would stop the hemorrhaging.”
As the number of adolescents who identify as transgender grows, drugs known as puberty blockers have become the first line of intervention for the youngest ones seeking medical treatment.
Their use is typically framed as a safe — and reversible — way to buy time to weigh a medical transition and avoid the anguish of growing into a body that feels wrong. Transgender adolescents suffer from disproportionately high rates of depression and other mental health issues. Studies show that the drugs have eased some patients’ gender dysphoria — a distress over the mismatch of their birth sex and gender identity.
“Anxiety drains away,” said Dr. Norman Spack, who pioneered the use of puberty blockers for trans youth in the United States and is one of many physicians who believe the drugs can be lifesaving. “You can see these kids being so relieved.”
But as an increasing number of adolescents identify as transgender — in the United States, an estimated 300,000 ages 13 to 17 and an untold number who are younger — concerns are growing among some medical professionals about the consequences of the drugs, a New York Times examination found. The questions are fueling government reviews in Europe, prompting a push for more research and leading some prominent specialists to reconsider at what age to prescribe them and for how long. A small number of doctors won’t recommend them at all.
Dutch doctors first offered puberty blockers to transgender adolescents three decades ago, typically following up with hormone treatment to help patients transition. Since then, the practice has spread to other countries, with varying protocols, little documentation of outcomes and no government approval of the drugs for that use, including by the U.S. Food and Drug Administration.
But there is emerging evidence of potential harm from using blockers, according to reviews of scientific papers and interviews with more than 50 doctors and academic experts around the world.







The drugs suppress estrogen and testosterone, hormones that help develop the reproductive system but also affect the bones, the brain and other parts of the body.
During puberty, bone mass typically surges, determining a lifetime of bone health. When adolescents are using blockers, bone density growth flatlines, on average, according to an analysis commissioned by The Times of observational studies examining the effects.
Many doctors treating trans patients believe they will recover that loss when they go off blockers. But two studies from the analysis that tracked trans patients’ bone strength while using blockers and through the first years of sex hormone treatment found that many do not fully rebound and lag behind their peers.
That could lead to heightened risk of debilitating fractures earlier than would be expected from normal aging — in their 50s instead of 60s — and more immediate harm for patients who start treatment with already weak bones, experts say.
“There’s going to be a price,” said Dr. Sundeep Khosla, who leads a bone research lab at the Mayo Clinic. “And the price is probably going to be some deficit in skeletal mass.”
Many physicians in the United States and elsewhere are prescribing blockers to patients at the first stage of puberty — as early as age 8 — and allowing them to progress to sex hormones as soon as 12 or 13. Starting treatment at young ages, they believe, helps patients become better aligned physically with their gender identity and helps protect their bones.
But that could force life-altering choices, other doctors warn, before patients know who they really are. Puberty can help clarify gender, the doctors say — for some adolescents reinforcing their sex at birth, and for others confirming that they are transgender.
“The most difficult question is whether puberty blockers do indeed provide valuable time for children and young people to consider their options, or whether they effectively ‘lock in’ children and young people to a treatment pathway,” wrote Dr. Hilary Cass, a pediatrician leading an independent review in England of medical treatments of adolescents presenting as transgender.

On her recommendation, England’s National Health Service last month proposed restricting use of the drugs for trans youths to research settings. Sweden and Finland have also placed limits on the treatment, concerned not just with the risk of blockers, but the steep rise in young patients, the psychiatric issues that many exhibit, and the extent to which their mental health should be assessed before treatment.
In the United States, though, there is no universal policy, and the public discussion is polarized.
Republican governors and lawmakers in more than a dozen states are working to limit or even criminalize the treatments, as some in their party also seek to restrict access to sports and bathrooms, ban discussion of gender in public schools, and call into question whether transgender identity even exists. (This month, the Florida medical board banned medications and surgeries for new patients under 18.) Meanwhile, the Biden administration describes transgender medicine as a civil right. And some advocates criticize anyone who questions the treatments’ safety.
Long-awaited research funded by the National Institutes of Health could provide more guidance. In 2015, four prominent American gender clinics were awarded $7 million to examine the effects of blockers and hormone treatment on transgender youth. In explaining their study, the researchers pointed out that the United States had produced no data on the impact or safety of blockers, particularly among transgender patients under 12, leaving a “gap in evidence for this practice.” Seven years in, they have yet to report key outcomes of their work, but say the findings are coming soon.
Many young patients and their families have concluded that the benefits of easing the despair of gender dysphoria far outweigh the risks of taking blockers. For others, the limited studies and politicization of trans medicine can make it difficult to fully evaluate the decision. A Reuters examination of a range of transgender treatments also found scant research into the long-term effects.
Three years after starting the drugs, Emma Basques believes she’s on the right path.
Jacy Chavira, now 22, decided that the medical treatment was not appropriate for her and resumed her female identity.
And the New York adolescent had such a significant loss in bone density after more than two years on blockers that the parents halted use of the drugs.
“We went into this because we wanted to help,” the mother said. “Now I worry that we got into a situation with a very powerful drug and don’t understand what the long-term effects will be.”
‘Time to Start’
It didn’t take long for Cherise and Arick Basques to realize that their toddler was different. The child rejected pants, toy trucks and sports in favor of dresses, Barbie dolls and ballet. When Ms. Basques ran into a friend at a restaurant in their Phoenix suburb and introduced her then-4-year-old as her son, the child shouted: “No! I’m your daughter!”
The couple worked with children — Ms. Basques as an occupational therapist, her husband as a teacher and school administrator — but this was unfamiliar territory. None of the therapists the parents called felt equipped to help. Their pediatrician offered only that things could change once the child started school, Ms. Basques said. Eventually, the couple discovered a local support group for parents of transgender children.
The next year, they allowed the child, then 5, to begin using the name Emma, grow longer hair and take other steps to socially transition. In 2019, when Emma turned 11, a physician at a local gender clinic advised starting blockers.
“At the first subtle signs of puberty, it was like: ‘Yep, that’s it. Time to start!’” recalled Ms. Basques. Along with her husband and Emma, she asked that their full names be used because they consider themselves advocates of the treatment.
For decades, transgender medical treatment in multiple countrieswas restricted to patients 18 and older. But in the 1990s, a hospital clinic in Amsterdam began treating adolescents.
Puberty blockers can be given as an injection or an implant. (The best known is Lupron, made by AbbVie.) They were being used in the United States and elsewhere, with approval by the F.D.A. and its counterparts overseas, to treat prostate cancer; endometriosis, a painful disease that causes uterine tissue to grow elsewhere in the body; and the unusually early onset of puberty, typically age 6 or 7. If blockers were safe for patients with that rare condition, known as central precocious puberty, the Dutch doctors reasoned, they were likely to be safe for trans adolescents too.
The first trans patient treated with blockers, from age 13 to 18, moved on to testosterone, the male sex hormone. Halting female puberty had offered emotional relief and helped him look more masculine. As the Dutch clinicians prescribed blockers, followed by hormones, to a half-dozen other patients in those early years, the medical team found that their mental health and well-being improved.
“They were usually coming in very miserable, feeling like an outsider in school, depressed or anxious,” recalled Dr. Peggy Cohen-Kettenis, a retired psychologist at the clinic. “And then you start to do this treatment, and a few years later, you see them blossoming.”
In 1998, she worked with a small international group — which would later expand and become known as the World Professional Association for Transgender Health, or WPATH — to include puberty blockers and hormones for adolescents in their treatment guidelines.
The Dutch doctors had yet to publish any research findings, she acknowledged. Some other physicians, including the one overseeing transgender medical treatment in England, were wary of potential harm.
But doctors in the group considered the early results from Amsterdam as reassuring enough to move forward. They were eager to treat the psychological distress observed in many trans adolescents.
Doctors debated about whether “starting the puberty blockers would somehow damage the children,” recalled Dr. Walter Meyer, a Texas pediatric endocrinologist and psychiatrist involved with the 1998 standards of care.
“The Dutch were saying, ‘Oh, no, it’s not causing a problem,’” said Dr. Meyer, who continues to support the use of the drugs.
Dr. Cohen-Kettenis hoped physicians in other countries would adopt the Dutch protocol, and document and share the outcomes as she and her colleagues in Amsterdam planned. Her clinic treated only patients who had consistently presented as transgender since early childhood and did not suffer from distinct psychiatric disorders that could interfere with diagnosis or treatment. They had to be at least 12 for puberty blockers, with the option of moving on to hormones at 16.
The international standards of care advised similar criteria. But they were recommendations, not requirements. Soon, the use of puberty blockers spread. In the United States and Canada, countries without centralized health systems, protocols were largely left to the discretion of individual clinics and practitioners. Dr. Spack, the pediatric endocrinologist who led U.S. adoption of the treatment, opened the first American clinic in 2007 at Boston Children’s Hospital; others eventually followed in nearly every state.
Some started children on blockers at the first signs of puberty and prescribed testosterone or estrogen to patients 14 or younger. Doctors believed that earlier treatment would lead to more successful medical transitions, and wanted to spare patients the difficulty of watching their peers develop while their own bodies remained unchanged.
The doctor in Arizona who treated Emma, for example, tells preteen patients that if he prescribed blockers and didn’t start hormones for five years, they would look 12 at age 16.

Transgender activists across the country pushed for early and easy access to the treatment. At a 2006 Philadelphia medical convention, Jenn Burleton, an advocate from Oregon, heard Dr. Spack describe his experience starting to treat adolescents with blockers. Like others of her generation, Ms. Burleton, now 68, could not medically transition until adulthood, and puberty had been traumatic. Treating adolescents with blockers was “game-changing,” said Ms. Burleton, founder and program director of the organization now known as the TransActive Gender Project at the Lewis & Clark Graduate School for Education and Counseling.
Back home, Ms. Burleton prodded pediatric endocrinologists to adopt the practice for their patients. “We have a chance to prevent them from being emotionally broken,” she recalled saying.
Advocates successfully pushed Oregon, Massachusetts, California and other states to allow for Medicaid coverage of puberty blockers for adolescents identifying as trans. They also helped win approval in Oregon for a variety of medical workers — doctors, nurse practitioners, naturopaths — to administer blockers if overseen, even long-distance, by an endocrinologist.
“It went so quickly that not even centers but individual clinicians, people who were not knowledgeable, were just giving this kind of treatment,” said Dr. Cohen-Kettenis, the Dutch psychologist. “There was a great concern.”
By the time Emma Basques began taking blockers in 2019, multiplemedical groups had endorsed their use for gender dysphoria. Among them were the American Academy of Pediatrics and the international Endocrine Society, which in 2017 had described the limited research on the effects of the drugs on trans youth as “low-quality.” Still, the organizations were encouraged by what they saw as a promising treatment.
Many doctors point out that it’s not unusual for research to lag behind the launch of new treatments and for drugs to be used off-label on patients without F.D.A. approval, especially in pediatric medicine.

An F.D.A. spokeswoman said in a statement that doctors have the discretion to do so, but also noted that just because a drug has been approved for one class of patients doesn’t mean it’s safe for another.
There is no centralized tracking of blocker prescriptions in the United States. Komodo Health, a health technology company, compiled private and public insurance data for Reuters, showing a sharp increase in the number of children ages 6 to 17 diagnosed with gender dysphoria, from about 15,000 in 2017 to about 42,000 in 2021. During that time, 4,780 patients with that diagnosis were put on puberty blockers covered by insurance, the data shows, with new prescriptions growing each year. But the data does not capture the many cases in which insurance does not cover the drugs for that use, leaving families to pay out of pocket.
Some leading American practitioners asked AbbVie and Endo Pharmaceuticals, maker of another blocker, to seek F.D.A. approval for the drugs’ use among trans adolescents. The drugmakers would have to fund research for a patient population that made up just a small part of their market. But the physicians argued that regulatory approval could help establish the safety of the treatment and broaden insurance coverage of the drugs, which can cost tens of thousands of dollars a year. In the end, AbbVie and Endo said no. The companies declined to comment on the decision.
Emma Basques was on blockers for two years. Then, after she turned 13 in October of last year, a doctor in the Portland, Ore., suburb where her family had moved, prescribed estrogen, starting her transition. It had become increasingly awkward to feel left behind as her classmates physically matured. And she felt confident that she was ready.
“It was just really exciting,” Emma said. “I finally got to be who I was.”

‘We Need to Give This a Chance’
The 11-year-old in New York, who had begun puberty and started at a new school, was increasingly distressed — refusing to bathe or go to class and, for the first time, expressing a desire to no longer have a girl’s body.
When the parents consented to blockers in 2018, they hoped the drug would bring emotional stability and time to consider next steps.
“If everyone thinks this will help, and it’s reversible, then we need to give this a chance,” said the mother, who asked that her name be withheld to protect the family’s privacy.
‘We Need to Give This a Chance’
The 11-year-old in New York, who had begun puberty and started at a new school, was increasingly distressed — refusing to bathe or go to class and, for the first time, expressing a desire to no longer have a girl’s body.
When the parents consented to blockers in 2018, they hoped the drug would bring emotional stability and time to consider next steps.
“If everyone thinks this will help, and it’s reversible, then we need to give this a chance,” said the mother, who asked that her name be withheld to protect the family’s privacy.

A full accounting of blockers’ risk to bones is not possible. While the Endocrine Society recommends baseline bone scans and then repeat scans every one to two years for trans youths, WPATH and the American Academy of Pediatrics provide little guidance about whether to do so. Some doctors require regular scans and recommend calcium and exercise to help to protect bones; others do not. Because most treatment is provided outside of research studies, there’s little public documentation of outcomes.
But it’s increasingly clear that the drugs are associated with deficits in bone development. During the teen years, bone density typically surges by about 8 to 12 percent a year. The analysis commissioned by The Times examined seven studies from the Netherlands, Canada and England involving about 500 transgender teens from 1998 through 2021. Researchers observed that while on blockers, the teens did not gain any bone density, on average — and lost significant ground compared to their peers, according to the analysis by Farid Foroutan, an expert on health research methods at McMaster University in Canada.
The findings match what practitioners of the treatment have seen, including Dr. Catherine Gordon, a pediatric endocrinologist and bone researcher at Baylor College of Medicine in Houston. “When they lose bone density, they’re really getting behind,” said Dr. Gordon, who is leading a separate study on why the drugs have such an effect.
Many doctors caring for young trans patients are reassured by the rebounds seen in the children who take blockers for unusually early puberty. In most cases, their bone strength fully recovers after they stop the drugs at about age 11 and resume full puberty, which can last up to five years. But patients identifying as trans take the drugs later, interrupting their normally timed puberty and limiting that crucial period of development.
“That’s the difference,” Dr. Gordon said. “You shorten that critical window of puberty.”
So far, only two small studies, published by Dutch doctors, have tracked the bone development of trans patients from beginning blockers through early hormone treatment. In both studies, dozens of patients started blockers at 14 or 15, on average, and began estrogen or testosterone at 16. The participants, followed in one study through age 18, and in the other through age 22, saw their bones strengthen, on average, once on hormones. Still, most patients continued to lag behind their peers; trans men neared average levels, but trans women fell far below.
“I think there’s a false sense of security,” said Dr. Khosla, the Mayo Clinic specialist, who is skeptical that all trans patients can catch up.
Dr. Khosla and Dr. Gordon don’t believe the effects on bones are reason for medical providers to halt use of the drugs in adolescents. But they think the risks should be factored into patient decisions and that bones should be carefully monitored.
If any harm resulted from the use of blockers, it likely would not be evident until decades later, with fractures. However, for children who already have weak bones as they start treatment, the dangers could be more immediate. While there is no systematic record-keeping of such cases, some anecdotal evidence is available.
After more than a year on blockers, a 15-year-old in Texas, who had not had a baseline scan, showed spinal bone density so low that it was below the first percentile for the teen’s age and weight, indicating osteoporosis, according to medical records from earlier this year.
A transgender adolescent in Sweden who took the drugs from age 11 to 14 with no bone scans until the last year of treatment developed osteoporosis and sustained a compression fracture in his spine, an X-ray showed in 2021, as reported earlier in a documentary on Swedish television.
“The patient now suffers from continued back pain,” medical records note, describing a “permanent disability” caused by the blockers.
Some practitioners in the United States and Australia do not provide the drugs to patients who are well into puberty, concerned that the treatment poses the greatest threat to bones in that period.
“You’re potentially taking on risks that I felt should be avoided,” said Dr. Stephen Rosenthal, medical director of the University of California, San Francisco, Child and Adolescent Gender Center.
He won’t prescribe blockers as a stand-alone treatment to anyone over 14. That includes the growing number of nonbinary youths who don’t want to mature into either male or female bodies. “We make it very clear that no one stays on a blocker,” he said.
Dr. Rosenthal is a principal investigator in the yearslong N.I.H. study, which also involves gender clinics in Los Angeles, Chicago and Boston. Asked why they have yet to report on key outcomes, he said their research was delayed when the pandemic halted in-person treatment. Papers on the effects of blockers on bones and other findings should be published next year, he said.
Like many physicians, Dr. Rosenthal believes the benefits of using blockers to alleviate gender dysphoria are much greater than any risks to bones. (He was among the doctors who filed statements in a lawsuit against an Alabama ban on medical treatment of trans youth.)
Emma Basques, for example, takes calcium, makes an effort to exercise and has undergone scans that showed her bones are healthy. “I can’t even imagine how life would be for Emma,” said her mother, Ms. Basques, “if she was not given blockers and had to go through male puberty.”
Emma added: “I wouldn’t like my body at all.”
But the parents in New York insisted on ending treatment for their teen, who has yet to have a follow-up scan to see if bone density has improved since going off blockers.
“I don’t think we have the science behind them to be prescribing these drugs,” the mother said.
‘I Wish There Had Been More Questions’
Jacy Chavira, in Southern California, had already cut her hair short and begun binding her chest when she was prescribed blockers at age 13. A therapist and her parents agreed that gender dysphoria, a condition Jacy learned about from a magazine, could explain the mounting anxiety and discomfort that she was experiencing during early puberty.
Once on blockers, Ms. Chavira said, she became fixated on moving ahead with a medical transition. She was thrilled shortly after turning 16 when her pediatric endocrinologist prescribed testosterone. But soon she started having doubts. Her body was growing more masculine, but she was secretly putting on dresses. At 17, in a consultation for breast removal, she worried aloud about the potential loss of feeling in the nipples. To her, this was a sign of not wanting to go through with the surgery.
She came to realize that her anguish had stemmed from a larger inner conflict, and that continuing with a gender transition would be a mistake. “I believe it was an issue with my identity, accepting who I was, and not just the physical female portion of it,” she said.
Like Ms. Chavira, most patients who take puberty blockers move on to hormones to transition, as many as 98 percent in British and Dutch studies. While many doctors see that as evidence that the right adolescents are getting the drugs, others worry that some young people are being swept into medical interventions too soon.
Over the past decade, growing numbers of medical providers have lowered the ages at which they prescribe the treatments. Today, the WPATH and Endocrine Society advise that blockers can be prescribed at the first signs of puberty and hormone treatment, in some cases, earlier than 16. The American Academy of Pediatrics says blockers can be provided anytime during puberty and hormones from “early adolescence onward.”
Some doctors and researchers are concerned that puberty blockers may somehow disrupt a formative period of mental growth. With adolescence comes critical thinking, more sophisticated self-reflection and other significant leaps in brain development. Sex hormones have been shown to affect social and problem-solving skills. It’s believed that brain growth is connected to gender identity, but research in these areas is still very new.
In a 2020 paper, 31 psychologists, neuroscientists and hormone experts from around the world urged more study of the effects of blockers on the brain.
“If the brain is expecting to receive those hormones at a certain time and doesn’t, what happens?” said Dr. Sheri Berenbaum, head of a gender research lab at Penn State, and one of the authors of the paper. “We don’t know.”
The physicians in the Amsterdam clinic, where the treatment began, have lowered their minimum ages for starting blockers and hormones. But they are very cautious in selecting patients.
“Our concern is always: When is gender identity fixed or not fluid anymore? And when do you fully understand the lifelong consequences of such treatment?” said Dr. Annelou de Vries, head therapist at the clinic.
For some medical professionals across the country, there are too many uncertainties about the effects of blockers to provide the treatment.
Among them are seven pediatric endocrinologists and pediatric endocrine nurse practitioners in Florida who recently wrote to the state health department that evidence to support the use of those treatments in adolescents “is simply lacking” and asking that it be confined to research settings.
“Without much data, it’s hard to make a conclusion that we’re doing the right thing,” said Dr. Matthew Benson, an assistant professor of pediatrics at Mayo Clinic College of Medicine in Jacksonville and an author of the letter. (He also voiced concerns at a state hearing in July on whether to stop allowing Medicaid coverage in Florida for transgender medical treatment.)
Even enthusiasts, like Emma and her parents, acknowledge it can be hard to fully grasp all the potential results of treatment. Infertility is among other lasting effects for patients who start blockers at the first stage of puberty and proceed to hormones and surgery. Emma was advised that, to possibly preserve fertility, she would need to pause treatment at some point down the line, with the hopes of developing and freezing sperm.
“I knew what I wanted,” Emma said of her medical transition. “But all this other stuff was kind of just confusing.” Her father said, “We worked really hard to talk to her at her age level to make sure she understood some of these more complicated things.”
When Dutch doctors launched the use of blockers and hormones on trans youth decades ago, they warned in their early papers of the possibility of “false positives” — patients who medically transition, then later declare they are not transgender.
There’s no official tracking of those cases and many practitioners believe the total numbers are small. So far, scores of accounts have emerged in social media, news stories and published research.
Keira Bell, who was prescribed blockers at age 16, then moved on to testosterone and breast-removal surgery, no longer identified as transgender five years after starting to transition. She sued the Tavistock gender clinic in London where she had been treated. (A judge ruled that patients under 16 were unable to consent to puberty blockers — a decision later overturned on appeal.)
Jacy Chavira, looking back on her own experience, thinks that drugs were prescribed too quickly. At 18, she halted her medical treatment and resumed her female identity. Now, she is left with a voice that sounds like a man’s and other enduring physical changes.
“I wish there had been more questions asked by the doctors,” she said. “I wish I hadn’t been steered into transitioning the way I was, and that I had been told there were other ways to cope with the discomfort of puberty.”
Alarmed by the uncertain number of cases like Jacy’s, as well as the rising numbers of patients with gender dysphoria and the psychiatric disorders many display, Sweden is working to standardize adolescent transgender medical treatment and restrict it to research settings.
Finland is also limiting treatment, more closely following the Dutch protocol, and doctors there remain concerned about the physical effects of blockers, including on brain development, said Dr. Riittakerttu Kaltiala, chief of adolescent psychiatry at a gender clinic in Tampere. (Dr. Kaltiala testified this fall before the Florida medical board as it was considering its ban on treatment.)
As European countries continue to examine and tailor their treatment, in the United States the public discourse about transgender care is growing more incendiary.
Last month, the American Academy of Pediatrics and other medical groups wrote to Attorney General Merrick B. Garland, urging the Justice Department to investigate growing threats of violence against physicians and hospitals that provide transgender medical treatment to adolescents. As more Republicans frame the treatment as child abuse, some doctors have become wary of discussing their work for fear of becoming targets.
More than a dozen doctors declined to be interviewed for this article, and several who spoke to The Times — some who support treatment, others who question it — asked not to be named.
The climate could have a chilling effect on research, said Dr. Natalie Nokoff, assistant professor of pediatric endocrinology at the University of Colorado, who recently conducted a soon-to-be-published study showing that a longer treatment period on puberty blockers was associated with a lower bone density.
“It’s leading to concerns that people’s well-intentioned scientific research could be misconstrued” and exploited for political gain, she said.
The prospect of such an outcome is disheartening for the families of Emma Basques, Ms. Chavira and the teen in New York. Despite their differing experiences, they share the same hopes for transgender medicine: less vitriol, more science.
Methodology
The analysis commissioned by The Times examined the findings of seven observational studies from the Netherlands, England and Canada, documenting the association between puberty blockers and bone density in about 500 adolescents.
In each study, bone density was measured at the spine and the hip using Dual-energy X-ray absorptiometry, or DEXA scan. The analysis looked at group means, because not every study released individual person data. Each study’s findings were weighted based on its number of participants.
The change in bone density while adolescents were on blockers was observed to be zero. The analysis also showed that the adolescents’ Z-scores, a measure of bone density that is benchmarked to peers, consistently fell during treatment with blockers.
The studies included are:
“Bone Mass in Young Adulthood Following Gonadotropin-Releasing Hormone Analog Treatment and Cross-Sex Hormone Treatment in Adolescents With Gender Dysphoria,” Klink et. al, Journal of Clinical Endocrinology & Metabolism, 2015
“Effect of Pubertal Suppression and Cross-Sex Hormone Therapy on Bone Turnover Markers and Bone Mineral Apparent Density (BMAD) in Transgender Adolescents,” Vlot et. al, Bone, 2017
“The Effect of GnRH Analogue Treatment on Bone Mineral Density in Young Adolescents With Gender Dysphoria: Findings From a Large National Cohort,” Joseph et. al, Journal of Pediatric Endocrinology and Metabolism, 2019
“Physical Changes, Laboratory Parameters and Bone Mineral Density During Testosterone Treatment in Adolescents With Gender Dysphoria,” Stoffers et. al, The Journal of Sexual Medicine, 2019
“Bone Development in Transgender Adolescents Treated With GnRH Analogues and Subsequent Gender-Affirming Hormones,” Schagen et. al, Journal of Clinical Endocrinology & Metabolism, 2020
“Short-Term Outcomes of Pubertal Suppression in a Selected Cohort of 12- to 15-Year-Old Young People With Persistent Gender Dysphoria in the U.K.,” Carmichael et. al, PLOS One, 2021
“Pubertal Suppression, Bone Mass and Body Composition in Youth With Gender Dysphoria,” Navabi et. al, Pediatrics, 2021
Julie Tate contributed research.
Megan Twohey is a prize-winning investigative reporter and a best-selling author who has focused much of her work on the treatment of women and children. @mega2e • Facebook
Christina Jewett covers the Food and Drug Administration. She is an award-winning investigative journalist and has a strong interest in how the work of the F.D.A. affects the people who use regulated products. @By_Cjewett
#Puberty blockers#Dr Norman Spack#Dr Sundeep Khosla#Dr Hilary Cass#England’s National Health Service#Dr. Peggy Cohen-Kettenis#World Professional Association for Transgender Health#or WPATH#Dr. Walter Meyer#TransActive Gender Project at the Lewis & Clark Graduate School for Education and Counseling
13 notes
·
View notes
Text
Publication of the leaked WPATH files.
Via Environmental Progress.

The written WPATH Files come from WPATH’s member discussion forum, which runs on software provided by DocMatter. Ninety seconds of the 82-minute video was made public last year. We are making the full video available for the first time. One or more people gave me the WPATH Files, and my colleagues and I attempted to summarize them as a series of articles. We quickly realized the topic was too sensitive, complex, and large to be dealt with as a work of journalism, and we moved the project to the research institute I founded seven years ago, Environmental Progress (EP). The Files are authentic. We redacted most names and left only those individuals who are leading gender medicine practitioners to whom we sent “right-of-reply” emails. We know WPATH members discussed our emails internally. No WPATH leader or member has denied that the Files are anything other than what they appear to be. EP is publishing a 70-page report to provide context for the 170 pages of WPATH Files. Mia Hughes is the author of the report. It and accompanying summary materials can be downloaded at the link below. That link also provides a link to the full WPATH video. What follows are simply a few highlights. People with a serious interest in the topic should read the report and all the files."


READ: THE WPATH FILES AND REPORT
#gender critical#gc#WPATH#World Professional Association of Transgender Health#medical experimentation#gender medicine#pseudoscientific surgical and hormonal experiments on children#trans madness#gender madness#leave those kids alone#video#feminist#radfem
3 notes
·
View notes
Text

In 2017 I interviewed Bernadette Wren, then head of psychology at the Tavistock Gids clinic, and asked what effect puberty blocking drugs have on the adolescent brain. Looking highly uncomfortable, she replied that the evidence so far was only anecdotal but that the clinic would study its patients “well into their adult lives so that we can see”.
Even back then, before whistleblowers had exposed the rush to medically transition children, it was alarming to hear that heavy-duty GnRH agonists such as triptorelin — used to treat advanced prostate cancer and “chemically castrate” sex offenders — were being prescribed to arrest puberty in hundreds of children as young as 11.
Moreover, they were being used “off-label” before any clinical trials. And the long-term study Wren promised never materialised: Gids (the Gender Identity Development Service) routinely lost touch with patients, and the 44 it did follow reported little long-term mental health improvement.
This shocking chapter in medical history, where the ideological objectives of trans rights campaigners trumped the welfare of disturbed children, is coming to an end worldwide. The decision by NHS England effectively to ban the prescription of puberty blockers comes after the Cass review noted these drugs could “permanently disrupt” brain development, reduce bone density and lock children into a regime of cross-sex hormones requiring life-long patienthood.
NHS England unites with other national health services including those in Finland, France, Sweden and, most notably, the Netherlands — where the “Dutch protocol”, a regime of early blockers then hormones, was devised in 1998 — in pulling back from prescribing them.
Even in the United States, where a toxic combination of extreme activism and medical capitalism has pushed child gender medicine to grotesque extremes, with double mastectomies performed on 14-year-old girls, there is some retrenchment.
Leaks from the World Professional Association for Transgender Health, the body which formulates guidance on “trans healthcare”, reveal doctors perplexed at how they should explain to an 11-year-old child that drugs will render them infertile. Crucially, liberal media such as The New York Times are now reporting grave medical misgivings about child transition, once dismissed as a culture-war issue for the Republican right.
Yet the question remains: how was this ever allowed to happen? For years, puberty blockers were cheerily billed as a mere “pause button”. In 2014, Dr Polly Carmichael, the last head of Gids before the Cass review ordered its closure, went on CBBC in a show called I Am Leo, saying of blockers: “The good thing is, if you stop the injections, it’s like pressing ‘start’ and the body carries on developing as it would if you hadn’t started.”
The BBC permitted her to make this unevidenced claim to an impressionable audience of six to 12-year-olds. Imagine hearing this as a developing girl, freaked out by your new breasts and periods. No wonder Gids referrals subsequently rocketed.
Carmichael failed to mention that she did not know if pressing “restart” on puberty is always medically possible — it is not — and in fact, almost every child Gids put on blockers went on to irreversible cross-sex hormones.
After years in a Peter Pan state while their peers developed, they understandably felt there was no way back and forged on with treatment. Yet if allowed to experience natural puberty, almost 85 per cent of gender dysphoria cases resolve themselves.
Nor did Carmichael tell CBBC kids that the blockers-hormones combination, if taken early enough, not only results in sterility but kills the libido so that a young person will never experience an orgasm.
At the 2020 judicial review brought by a former Tavistock clinician and Keira Bell, the brave young detransitioner rushed onto hormones by Gids, judges expressed astonishment at Gids’s lack of an evidence base.
Reporting on this issue for seven years, I too have been struck by a complete clinical incuriosity. Not only was data not collected, but those who queried treatments or pressed for evidence faced angry condemnation. Perhaps activists knew what research might find because one long-term Finnish study, recently reported in the BMJ, destroyed the myth used to justify blockers: that a child will commit suicide if denied them.
The Finns found that “gender-affirming care” does not make a dysphoric child less suicidal. Rather, such children had the same suicide risk as others with severe psychiatric issues. In other words, changing bodies does not fix troubled minds.
Yet even after NHS England’s announcement, activists refuse to heed the now-overwhelming evidence. In its response, Stonewall persists with the myth that puberty blockers “give a young person extra time to evaluate their next steps”.
Many questions remain unanswered: will private clinics still be permitted to prescribe puberty blockers; and is Scotland’s Sandyford child gender clinic still determined to close its ears to all evidence? Plus, we have few details on how the NHS’s new “holistic” treatment for gender-questioning children will operate when it opens next month.
This repellent experiment — in which girls who like trucks or little boys who dress as princesses, and who invariably grow up to be gay, are corralled inexorably down a road towards life-changing treatments — belongs in the book of medical disgraces. As do the cheerleaders who raised money for Mermaids and those who persecuted whistleblowers or damned journalists asking questions as transphobic.
In 50 years, chemically freezing the puberty of healthy children with troubled minds will be regarded with the same horrified fascination as lobotomies — which, never forget, won the Portuguese neurologist Antonio Egas Moniz the 1949 Nobel prize.
--------------------
{Article source (behind paywall)}
233 notes
·
View notes
Text
His work through EEF was crucial to improving the lives of countless trans people. In addition to funding many of the earliest research projects, his two main contributions were the financial support he gave to the Harry Benjamin Foundation and the first North American gender clinic at Johns Hopkins Hospital in Baltimore, Maryland.
Erickson funded international conferences on trans topics in 1969 (cosponsored by the Albany Trust of London), 1971, and 1973. Later conferences were organized by the Harry Benjamin International Gender Dysphoria Association (HBIGDA) founded in 1979. It changed its name to the World Professional Association for Transgender Health (WPATH) in 2007.
EEF made major contributions to growing public awareness, too, through funding lectures, educational films, newspaper articles, radio, and television programs, and books including Money and Green’s Transsexualism and Sex Reassignment, 1969, and Money and Ehrhardt’s Man, Woman, Boy, Girl, 1972. [...]
After learning about Los Angeles-based gay and lesbian rights group ONE, Inc., which published the highly influential ONE magazine, in 1964, Erickson began giving them money after convincing them to form the nonprofit, tax-exempt Institute for the Study of Human Resources.
With the huge amounts of money he gave them over the years that other gay groups at the time could barely dream of (some $1.5 million in today’s dollars), they published a two-volume Annotated Bibliography of Homosexuality and created a variety of unprecedented gay equality focused research and education programs including lectures, and, ultimately, accreditation in 1981 by the state of California as a graduate degree-granting institution.
1K notes
·
View notes
Text
Ho boy I just got hit with a wave of HRT related asks.
I'll respond to them to the best of my ability, but imma make a copy/paste disclaimer here:
I AM NOT A MEDICAL PROFESSIONAL. I have a very, VERY marginal ability to interpret medical data over the average person due to my bio background, but it's far less than people think- hell I just said something wrong about insurance that someone had to correct.
Unfortunately, however, the nature of trans healthcare being under constant political threat worldwide means that everyone should prepare to diy, and know the basics of how they would pull that off. That's why I'm answering these questions, more info out there is always better. HOWEVER, you would better be served by other sources, like:
Anything I say directly about medical care will be an interpretation or regurgitation of something that is likely in these sources, plus a dash of personal experience. My bio knowledge and interpretation is not going to kick in here, it's gonna be too far deep in the weeds of cellular mechanisms that it's not directly relevant.
82 notes
·
View notes
Text
(1) Arkansas ban on gender-affirming care for minors ruled unconstitutional
While Moody’s ultimate ruling in the case and legal conclusions obviously matter, his findings of fact issued Tuesday could be the most important aspect of his decision. Because trial judges are able to review the evidence and are closest to the case at trial, their findings of fact are accepted on appeal unless the appeals court finds that the those findings constitute an “clear error,” a deferential standard.
After detailing the evidence presented by the parties regarding the World Professional Association for Transgender Health (WPATH) Standards of Care and Endocrine Society’s guidelines for care, Moody — an Obama appointee who has been on the bench since 2014 — found as a fact: “Transgender care is not experimental care."
#Arkansas#Gender affirming care#Trans#Transgender#Lgbtqia#lgbtq youth#protect trans lives#protect trans youth
312 notes
·
View notes
Text
The 388-page report featured 32 recommendations on how transgender care should be conducted within NHS England. It incorrectly claims that there is “no good evidence” supporting transgender care and calls for restrictions on trans care for individuals under the age of 18, although it does not advocate for an outright ban. The report endorses the idea that being transgender may be caused by anxiety, depression, and OCD issues, despite the American Psychological Association, the largest psychological association in the world, rebutting this as lacking evidence. It also claims that transgender individuals can be “influenced” into being trans, a nod to the discredited theory of social contagion and rapid onset gender dysphoria, rejected by over 60 mental health organizations. Lastly, it seemingly endorses restrictions on transgender people under the age of 25, stating that they should not be allowed to progress into adult care clinics.
To support these recommendations, the report was released alongside “reviews” of the evidence surrounding transgender care, using these reviews to assert that there is "no good evidence" for gender-affirming care. A closer inspection of the reviews released alongside the Cass report reveals that 101 out of 103 studies on gender-affirming care were dismissed for not being of "sufficiently high quality," based on the Newcastle-Ottawa Scale—a subjective scale criticized for its flaws and potential unreliability due to a high risk of bias. This critique is particularly significant given the contentious political nature of the subject and connections between reviewers, Cass, and anti-trans organizations.
[...]
Immediately after the release of the Cass Review, experts in transgender healthcare from around the world voiced their opposition to its findings. Dr. Portia Predny, Vice President of the Australian Professional Association for Trans Health, criticized the findings and recommendations as “at odds with the current evidence base, expert consensus, and the majority of clinical guidelines worldwide.” Similarly, a statement from the Professional Association for Transgender Health Aotearoa condemned the review, noting, “The Review commissioned several systematic reviews into gender-affirming care by the University of York, but appears to have ignored a significant number of studies demonstrating the benefits of gender-affirming care. In one review, 101 out of 103 studies were dismissed.”
It is important to note that gender affirming care saves lives, and there is plenty of evidence to show for it. Numerous studies have demonstrated that gender-affirming care significantly reduces suicidality, with some showing a decrease in suicidality by up to 73%. A review compiled by Cornell University, which compiled over 50 journal articles on the topic, shows the efficacy of transgender care. These findings were echoed recently in an article published by the Journal of Adolescent Health, which found that puberty blockers dramatically lowered depression and anxiety. All of these studies and more have led to The Lancet, a medical journal with international acclaim, to publish a letter stating that gender affirming care is lifesaving preventative care. The largest and most influential medical organizations support trans care. A recent and historic policy resolution passed overwhelmingly by the American Psychological Association, the largest psychological organization in the world, states that gender affirming care is a medical necessity and that being trans is not “caused” by things like autism and PTSD.
48 notes
·
View notes
Text
The new hateful anti-transgender regulations of Missouri show us that it was never about the kids

New regulations make it practically impossible for transgender people to get gender affirming medical support in Missouri.
Republicans have for a long time covered their transphobia under concern for the kids. In accordance with this a lot of their anti-trans laws and regulations have been there to “protect the kids”.
For sure , the bathroom laws and the attacks on trans participation in sports have proven that their ultimate goal is to exclude trans people from society, but they could always hide behind the idea that trans people would still be allowed to be trans people.
Missouri directive proves that the end goal is the eradication of trans people
The new emergency regulations in Missouri prove beyond doubt that this is no longer the case. Sure, it presents a set of regulations that on paper contain some loopholes that might, theoretically, allow for sanctioned hormone replacement therapy and corrective surgery. Still, there are so many barriers that this is practically impossible.
The underlying logic is the old medical paradigm of gatekeeping (psychiatric therapy, long waiting periods, constant review ensuring that you are living up to the standards of a conservative society). However, they are taking this to a new level.
So, if you are suffering from anxiety and depression (most likely caused by transphobia), that would stop you from getting relevant health care. If they can document that you are affected by “social media addiction” or “social contagion”, that will be used against you. Following Transgender World is probably enough.
So this is really about stopping trans people from showing the world that they are trans. Trans people who have already transitioned can no longer get hormones in Missouri. They will have to detransition or move to a sane state.
Note that the Missouri attorney general issued this new state directive citing a consumer protection law normally used to prosecute fraudulent business practices. These regulations have not even been discussed by lawmakers.
Misleading presentations of science
In the regulations the Republicans have the audacity to cite the World Professional Association for Transgender Health in support of their policy. WPATH is totally against this kind of transphobia. The text is full of biased and selective misrepresentations of relevant research.
The Republicans try to make people believe that transitioning medically is a risky procedure. So keep in mind that the regret rate for trans people who have transitioned using hormones and surgery is less than 1 percent.
The use of puberty blockers is not “experimental”. Drugs in the class have been FDA approved since the 1990s to treat early puberty
Most of the negative findings associated with trans people is caused by lack of proper health care and the rhetoric of Republicans and other transphobes. The Republicans are basically creating the conditions that lead to the suffering they use as an excuse to persecute trans people.
These are the requirements of the transphobic regulations
Any person or health organization that provide a covered gender transition intervention to a patient will have to:
Assess (at least annually) whether the patient continues to have gender dysphoria.
Disclose conspicuously—on its website, physically in writing, and orally in person by the prescribing provider—to the patient and (if the patient is a minor) to the patient’s parents or legal guardians, [anti-trans propaganda arguments listed in the regulation].
Ensure that for at least the 3 most recent consecutive years, the patient has exhibited a medically documented, long-lasting, persistent and intense pattern of gender dysphoria.
Ensure that the patient has received a full psychological or psychiatric assessment, consisting of not fewer than 15 separate, hourly sessions (at least 10 of which must be with the same therapist) over the course of not fewer than 18 months to explore the developmental influences on the patient’s current gender identity and to determine, among other things, whether the person has any mental health comorbidities.
Ensure that any psychiatric symptoms from existing mental health comorbidities of the patient have been treated and resolved.
Ensure that the patient has received a comprehensive screening to determine whether the patient has autism.
Ensure that the patient has received a comprehensive screening (at least annually) for social media addiction or compulsion and has not, for at least the six months prior to beginning any intervention, suffered from social media addiction or compulsion.
Ensure (at least annually) that the patient is not experiencing social contagion with respect to the patient’s gender identity.
Track all adverse effects (both expected and unexpected) that arise from any course of covered gender transition intervention for all patients beginning the first day of intervention and continuing for a period of not fewer than 15 years.
Maintain data about adverse effects in a form that can be accessed readily for systematic study.
Obtain and keep on file informed written consent from the patient and (if the patient is a minor) from all parents or guardians who have authority to consent to medical intervention, as to each requirement [listed in this section of the regulation9. Such written consent shall be obtained for each intervention.
For medical personnel these restrictions are so wide that trying to help trans people will lead to a too high risk for legal persecution. We would guess this means an end of gender affirming medical healthcare in Missouri.
The rules take effect April 27.
Missouri rules part of rapid push to limit trans health care
Missouri to Restrict Medical Care for Transgender Adults, Citing Consumer Protection Law
Below, Video by the Young Turks on Missouri Attorney General Bans Gender-Affirming Care by "Emergency Rule"
youtube
Photo: Protester wearing a transgender pride flag at the Missouri State House. From the New York Times, Charlie Riedel, Associated Press
243 notes
·
View notes
Note
I am one of those 'kids who can't consent'. I can consent. But because of radfems allying with the conservative right, you are forcing me through irreparable changes. Every day I wake up and my body is more and more disgusting. But, because of you, I keep getting gaslit by GPs that I'm not trans, that I will learn to love my body, when the reality is it's wrong. Radfems do want to kill trans people, and they want kids to stay sexually available to them. I've lost count of the amount of lesbians telling me that I shouldn't "mutilate" my body because they lose out on another butch. You're disgusting and why I may be attracted to girls but will never date them.
Killing trans people is your end goal and that's why people think you're evil. 56% increase in hate crimes in the UK, thanks for that.
No, actually, you can't consent and if you don't understand the dangerous precedent this sets (for full grown adults with agendas to tell you can consent,) I'll explain it to you.
Within the trans community there's an idea that the sooner you can get a kid to transition, socially or medically, the sooner this can be seen as normal. The normalization of transitioning children is important, it pushes the idea that they could be born in the wrong body and normalizes the idea that a child knows what is medically best for them.
Child predators will try to find a way to have access to children by any means, now imagine how much easier it would be for them to have access to vulnerable children if they just claim to understand and support their gender identity issues.
The idea that children can consent would mean parents have no right over their children when it comes to their health and protections. I'm not saying children shouldn't speak up for themselves but we need to acknowledge that many children can be coached or groomed into saying or thinking things that may not benefit them or their safety.
The people that would love it for the law to 'recognize' that kids can consent doesn't stop at transgender rights advocates. It extends to pedophiles/child molesters that would love to get off the sex registry(something Jacob Breslow thinks it shouldn't exist to begin with) & pedophiles in position of power; informing and creating guidelines regarding childrens health & gender identity issues/transgenderism.
Pedophile sympathizer Jacob Breslow advocates for the rights of pedophiles, he thinks people are too mean to them. He thinks minors can consent too.
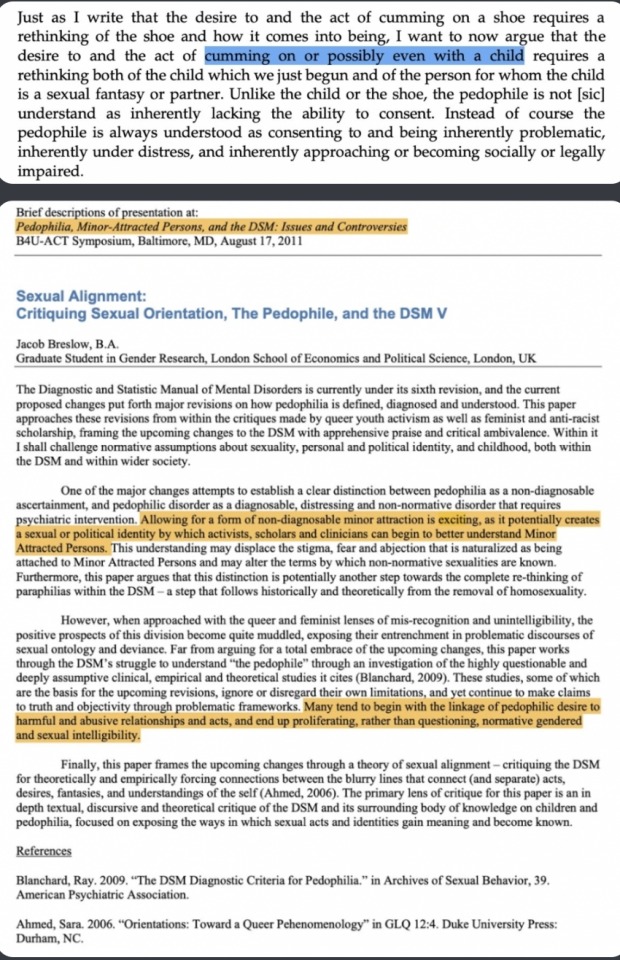
In his book Ambivalent Childhoods, Chapter 3 Desiring the Child: Queerness, Motherhood, and the Analyst, he writes:
[a description of a 12-year-old child dancing and mimicking sex acts to a crowd of adults.]
“As his movements transition from those that mimic break-dancers to those that mimic sex acts, repeating the easily citational gesticulations of pelvic thrusts … I find myself caught up in exhilarating waves of memory, identification, and desire … a desire for him himself,”
Why am I talking about Jacob Breslow? You should know him right? He was a Mermaids charity trustee until all of this came out, the pedophile sympathizing and all that.
Breslow also cited as an inspiration for his own writing Judith Levine’s 2002 book Harmful To Minors: The Perils Of Protecting Children From Sex in which she wrote that “sex is not in itself harmful to minors” and argued for the lowering of the age of consent to twelve.
He also was a guest speaker for a Pro-Pedophile B4U-ACT conference, an organization set up by a convicted child molester to destigmatize pedophiles and rebrand then as MAPs or Minor attracted person.
He's just one person tho, right? Not like there are more pedophile sympathizers in position of power when it comes to the transgender movement-
Anyways, all that to say;
Kids cannot consent because they don't have the cognitive or emotional maturity to understand long-term ramifications of such things.
>forcing irreparable changes
Going through puberty is normal. You've been convinced it's not but i promise you, you can still transition as soon as you turn 18 or whatever if that's what you want and you'll be fine.
Radfems don't align themselves with the conservative right but i can understand how you'd come to think that's what's happening when certain radfems talk on conservative platforms. I think there's a lack of understanding that they have no where else to speak on, especially when leftist first action is to label them as terfs and often don't give them the opportunity to have a conversation lest they be cancelled for even giving them the time of day.
Your body isn't disgusting. I'm sorry you feel that way and I'm sorry there are certain people that have convinced you to hate your body. I won't tell you you can learn to love yourself, it's taken me decades to learn to love myself and stop hating myself so much for things that happened to me that were out of my control and made me resent being a woman. Learning about radical feminism has definitely helped. I hope you can find something that will help you you as well that won't cause irreversible damage.
Radfems don't want to kill transpeople, I've already explained this in a different ask. Radfems don't want kids to be sexually available to them either, that's disgusting.
Hey, it sounds like you're dealing with a lot, including internalized homophobia, maybe some trauma. I truly hope you get an actual therapist that can listen and validate your concerns. My end goal isn't to kill transpeople tho I'd definitely would like to know where you're getting that from.
442 notes
·
View notes
Photo




[ Link: https://www.tandfonline.com/doi/pdf/10.1080/26895269.2022.2100644 ]
[ Correction: https://www.tandfonline.com/doi/full/10.1080/26895269.2022.2125695 ]

They have no idea how many or why people detransition. The claim that it’s a tiny minority is completely baseless.
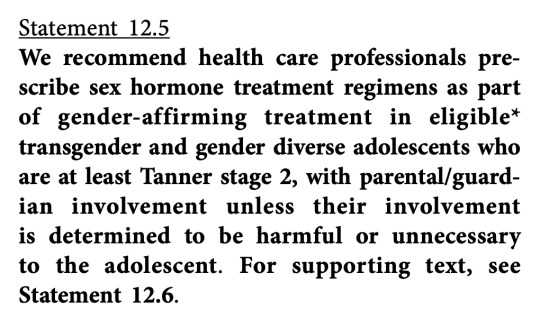
Tanner Stage 2 occurs on average at about 10 years of age in girls, as early as 8, and on average at about 12 years of age in boys, as early as 9. So WPATH is proposing that if a 10 year old girl wants puberty blockers or cross-sex hormones - note that this is about hormones, not just blocking puberty - but her parents are dubious, members complying with WPATH standards will simply administer them anyway.

That is, there are more controls for detransitioning than transitioning. This is how cults work.
Except, who’s going to go back to the doctor who mutilated them? The Tavistock said that they have no idea what proportion of their, ahem, “patients” desisted or detransitioned, because they never followed them up. They never heard back from them, and that was it. This is suggesting that they will follow up, but it’ll be like an army of Jehovah’s Witnesses at your door with “additional viewpoints.” That is, they’ll only challenge the motives of a detransitioner, not someone seeking transition.
“There's kind of like this attitude in the trans community that if you question your transition, that makes you insane.”
-- Helena Kerschner
The paper repeatedly cites Jack Turban, who is a known liar.
It’s hard to tell if they’re now extremely confident now that this ideology has attained cultural supremacy and institutional domination and have dropped the mask of what they’re up to, or they’re in panic mode, making a last-ditch grab before it all comes crashing down.
Believe them when they tell you what they’re up to.
#James Esses#queer theory#gender ideology#WPATH#defund WPATH#World Professional Association for Transgender Health#ideological capture#ideological corruption#gender cult#medical malpractice#unethical#medical scandal#medical corruption#medical transition#detransition#detrans#wokeness as religion#cult of woke#woke activism#wokeism#woke#religion is a mental illness
479 notes
·
View notes
Text
Erin Reed at Erin In The Morning:
On Tuesday, Gov. Janet Mills of Maine signed LD 227, a sanctuary bill that protects transgender and abortion providers and patients from out-of-state prosecution, into law. With this action, Maine becomes the 16th state to explicitly protect transgender and abortion care in state law from prosecution. This follows several bomb threats targeting state legislators after social media attacks from far-right anti-trans influencers such as Riley Gaines and Chaya Raichik of Libs of TikTok. An earlier version of the bill failed in committee after similar attacks in January. Undeterred, Democrats reconvened and added additional protections to the bill before it was passed into law.
The law is extensive. It asserts that gender-affirming care and reproductive health care are "legal rights" in Maine. It states that criminal and civil actions against providers and patients are not enforceable if the provision or access to that care occurred within Maine’s borders, asserting jurisdiction over those matters. It bars cooperation with out-of-state subpoenas and arrest warrants for gender-affirming care and abortion that happen within the state. It even protects doctors who provide gender-affirming care and abortion from certain adverse actions by medical boards, malpractice insurance, and other regulating entities, shielding those providers from attempts to economically harm them through out-of-state legislation designed to dissuade them from providing care.
The bill also explicitly enshrines the World Professional Association of Transgender Health’s Standards of Care, which have been the target of right-wing disinformation campaigns, into state law for the coverage of transgender healthcare.
The bill is said to be necessary due to attempts to prosecute doctors and seek information from patients across state lines. In recent months, attorneys general in other states have attempted to obtain health care data on transgender patients who traveled to obtain care. According to the United States Senate Finance Committee, attorneys general in Tennessee, Indiana, Missouri, and Texas attempted to obtain detailed medical records "to terrorize transgender teens in their states… opening the door to criminalizing women’s private reproductive health care choices."
The most blatant of these attempts was from the Attorney General of Texas, who, according to the Senate Finance Committee, "sent demands to at least two non-Texas entities."
[...]
Despite these threats, legislators strengthened both the abortion and gender-affirming care provisions and pressed forward, passing the bill into law. Provisions found in the new bill include protecting people who "aid and assist" gender-affirming care and abortion, protections against court orders from other states for care obtained in Maine, and even protections against adverse actions by health insurance and malpractice insurance providers, which have been recent targets of out-of-state legislation aimed at financially discouraging doctors from providing gender-affirming care and abortion care even in states where it is legal.
Maine Gov. Janet Mills (D) signs gender-affirming care and abortion sanctuary state bill LD227 into law despite the best efforts of right-wing anti-trans extremists such as Riley Gaines, Courage Is A Habit, and Libs of TikTok who sought to thwart its passage and signature into law.
#Maine LD227#Maine#Janet Mills#Transgender Safe Refuge#Transgender Sanctuary State#Abortion Sanctuary State#Abortion#Gender Affirming Healthcare#LGBTQ+#Transgender Health#Transgender#WPATH
27 notes
·
View notes
Text
What are Radblr's thoughts about this? I'm on my way to take a test when this article popped up on my screen, and I wanted to post this before I leave, especially given that this is published by Scientific America. However, Im personally skeptically that "social contagion" doesn't play a factor at all; I wouldn't doubt it plays into this even a little bit. I'm sure everyone knows about articles posted in favor of this fad from, like, two years ago from even big names like Mermaids, who have either been proved wrong or backtracked.
I have pasted the article below. There are links in the original article.
----------------
Health Care
Evidence Undermines ‘Rapid Onset Gender Dysphoria’ Claims
Fears of “social contagion,” used to support anti-transgender legislation, are not supported by science
By Timmy Broderick on August 24, 2023
A recent study claiming to describe more than 1,600 possible cases of a “socially contagious syndrome” was retracted in June for failing to obtain ethics approval from an institutional review board. The survey examined “rapid-onset gender dysphoria,” a proposed condition that attributes adolescent gender distress to exposure to transgender people through friends or social media. The existence of such a syndrome has been the subject of intense debate for the past several years and has fueled arguments against transgender rights reforms, despite being widely criticized by medical experts.
The American Psychological Association and 61 other health care providers’ organizations signed a letter in 2021 denouncing the validity of rapid-onset gender dysphoria (ROGD) as a clinical diagnosis. And a steadily growing body of scientific evidence demonstrates that it does not reflect transgender adolescents’ experiences and that “social contagion” is not causing more young people to seek gender-affirming care. Still, the concept continues to be used to justify anti-trans legislation across the U.S.
“To even say it’s a hypothesis at this point, based on the paucity of research on this, I think is a real stretch,” says Eli Coleman, former president of the World Professional Association for Transgender Health. Coleman helped create the organization’s most recent standards of care for trans people, which endorse and explain the evidence for forms of gender-affirming care.
Many transgender people experience gender dysphoria, meaning that the gender that was assigned to them at birth and their gender identity don’t align, causing distress. ROGD was proposed as a gender dysphoria subtype in a 2018 paper by physician and researcher Lisa Littman, then at Brown University.* Littman’s survey asked parents of transgender adolescents—recruited predominantly from anti-transgender websites and forums—to describe their child’s “sudden or rapid onset of gender dysphoria” and to state if it coincided with increased social media usage or the child’s friends coming out as transgender.
Littman later issued a correction that updated the methodology, including a brief description of the websites and forums, and noted that ROGD is not a formal diagnosis. But the concept had already been taken upin books and podcasts—and by politicians—to promulgate the idea that peer pressure and social media are making kids transgender or that being transgender is a form of mental illness. As legislation targeting trans people has reached an all-time high in the U.S., ROGD’s alleged social contagion has been invoked by lawmakers in states such as Missouri, Utah and Arkansas to justify banning or restricting gender-affirming care for young people.
“This is just a fear-based concept that is not supported by studies,” says Marci Bowers, president of the World Professional Association for Transgender Health. The term ROGD is being used to “scare people or to scare legislators into voting for some of these restrictive policies that take away options for young people. It’s cruel, cruel legislation.”
Like the 2018 study that coined the term rapid-onset gender dysphoria, the recently retracted paper, which was published this March in Archives of Sexual Behavior, surveyed parents of transgender children about their children’s experiences. The study was co-authored by Michael Bailey, a psychologist at Northwestern University, and Suzanna Diaz, a pseudonym used by a mother of a child with gender dysphoria. Diaz is not affiliated with an institution and had already collected the survey data before collaborating with Bailey on the paper. The study was retracted because Diaz and Bailey did not get consent from the survey’s respondents to have their responses published, although Bailey disputes this. (Bailey declined to answer questions about the retraction from Scientific American.)
The participants in both the 2018 and the retracted 2023 studies were recruited from online communities that were explicitly critical about many aspects of gender-affirming care for transgender kids. Littman’s research was inspired in part by parents’ posts on these skeptical websites.
In response to criticisms that recruiting parents from anti-transgender websites may have biased the results, Littman says, “I reject the premise that parents who believe transition will harm their children are more likely to discredit their kids’ experiences than parents who believe that transition will help their children.”
Most experts cite the survey of parents rather than transgender children themselves as another major flaw in the methodology of both studies.
Diane Ehrensaft, director of mental health at the University of California, San Francisco, Child and Adolescent Gender Center, concurs. “To talk about what children are thinking, feeling and doing, particularly as they get old enough to have their own minds and narratives, you need to interview them,” she says.
Parents can often be the last to know about their child’s gender identity, Ehrensaft says. Coming out can be terrifying for many transgender kids. Family members often respond with violence or distrust or may even kick the child out of the house. Almost 40 percent of transgender youth experience homelessness or housing instability, according to a 2022 report from the Trevor Project, a nonprofit that provides crisis support for young LGBTQ+ people. Many kids who wait to discuss their gender identity with their parents before appearing to “suddenly” come out are simply keeping themselves safe, Ehrensaft says.
“It is not rapid-onset gender dysphoria,” she says. “It’s rapid-onset parental discovery.”
Many experts have also questioned what length of time qualifies as a “sudden” experience of gender dysphoria. Both the 2018 and 2023 studies left the definition up for parental interpretation. Complicating this, there isn’t one pathway or time line for being transgender, says Tey Meadow, a Columbia University sociologist who studies sexuality and gender. “For some people, it can evolve slowly. For others, it can evolve quickly,” she says.
For most transgender youth seeking gender-affirming care, considerable time elapses between when they realize they may be transgender and when they receive such care. A recent analysis of 10 Canadian medical centers in the Journal of Pediatrics found that 98.3 percent of young people seeking gender-affirming care had realized more than a year prior that they may have been transgender. “If ROGD were a real thing, we would expect to see two discernible streams of patients coming in [to receive care],” says Greta Bauer, a co-author of the study and director of the Eli Coleman Institute for Sexual and Gender Health at the University of Minnesota Medical School. There would be a distinct group of adolescents with more recent knowledge about their gender identity going to clinics and another group that had had such knowledge for years. “But we didn’t see that,” she says.
Thomas Steensma, a psychologist at Amsterdam University Medical Centers who provides gender-affirming therapy, says he has not seen evidence of the “social contagion” component of ROGD, and he cautions against even using these terms. “Rapid means out of control, and contagion signals a warning, and that warning induces fear,” he says. “There’s no evidence that certain developmental pathways are more problematic or less beneficial or helpful than others” for a child’s gender identity.
Steensma reports that he sees two “peaks” of referrals in his clinic: young adolescents and 15-year-olds. In a 2020 study Steensma and his colleagues looked at adolescent referrals from 2000 to 2016 and found no measurable difference in the psychological functioning or the intensity of the gender dysphoria between more recent referrals and those who came to the clinic starting in 2000. If adolescents are presenting with a different form of gender dysphoria, Steensma has not seen it.
The researchers did observe a change in their referral population in recent years, however. More kids assigned female at birth have been transitioning in recent years than those assigned male at birth. Many studies have captured this difference—including the 2018 survey proposing ROGD—but experts are unsure of its cause. Littman suggests that female-assigned kids are more susceptible to the “social contagion” of gender dysphoria because they feel social pressure more acutely than male-assigned kids. But Ehrensaft says nothing in the clinical literature corroborates this assertion. Instead she attributes this discrepancy to shifting cultural factors that influence how children express themselves and explore their identity. In our culture, Ehrensaft says, “there’s a lot more gender stress for the boy in the tutu than the girl in the football uniform.”
Other forms of gender incongruence, such as identifying as nonbinary or gender nonconforming, further challenge the idea that children should be forced to abide by traditional gender categories. And the best way to understand what kids are experiencing is to ask them questions and listen to their answers, Ehrensaft says.
“In some ways, [kids] are far more advanced than I am, as somebody in my 70s, about how they live and understand gender,” Ehrensaft adds. “So if we want to really understand gender, turn to the experts—and that would be the youth themselves.”
*Editor’s Note (8/24/23): This sentence was edited after posting to correct Lisa Littman’s occupation and her affiliation at the time of her 2018 paper.
#terfsafe#terfblr#radblr#radfems please touch#radfems interact#terfs please touch#terfs interact#radfem safe#radfemsafe
54 notes
·
View notes
Note
Hello 🌼 I was thanking about facial hair. I'm AFAB. I don't plan on going on T (and I heard it can make you grow facial hair naturally?) but I still would want to grow a beard, or a mustache perhaps, in the future. Would hair transplant help me with that or would my hight estrogen/ lower testosterone make it not work out?
Lee says:
For folks who are unfamiliar, a facial hair transplant involves taking hair from a donor site on your body (usually the back of the head) and transplanting it to your facial region.
It's a common procedure for individuals who cannot grow facial hair naturally or who have patchy beards, and a beard transplant is a viable option for people who do not want testosterone, or were not happy with the amount of facial hair they grew on testosterone.
Transplanted hair behaves like natural hair. Once it's transplanted, it will fall out initially and then start to grow back over the next few months, eventually growing like regular facial hair, even if you're not on testosterone.
AnotherPascal has posted about his beard transplant on Instagram and TransLife&Wife has posted about his on YouTube.
There's an article about beard transplants for trans folks called Facial Hair Transplantation for Transgender Patients: A Literature Review and Guidelines for Practice that was published in the Aesthetic Surgery Journal in 2021. I believe it's open access and I would highly encourage you to read the whole thing!
Like natural facial hair, transplanted hair may require regular trimming or shaving, depending on your desired look.
Testosterone & facial hair:
However, as you've heard, testosterone can indeed stimulate facial hair growth, which is why individuals who take testosterone (T) may experience increased facial hair over time.
You mentioned you do not plan on taking T, which is perfectly valid, but if you think there's a chance that you may change your mind in the future then I would consider waiting for the facial hair transplant until you're at least a couple of years on T because it can take time for your facial hair to fill in.
If you choose to not take T and just go straight for the transplant, having higher levels of estrogen won't necessarily negate the effects of a hair transplant. The transplanted hair is genetically programmed to grow in its new location.
In theory, the lack of testosterone might mean that the hair grows less densely or slowly than it might for someone with higher testosterone levels, but I don't think that's necessarily the case here because the follicles being transplanted are from the head so they'd behave more like head hair than beard hair.
Finding a Trans-Friendly Provider (for a facial hair transplant):
If you're considering a facial hair transplant, the first step is to consult a doctor specializing in hair restoration. They can assess your hair quality, discuss your expectations, and determine whether you're a good candidate for the procedure.
Referrals: Consider asking for referrals from local LGBTQ+ groups, transgender support groups, or healthcare providers known to be trans-friendly.
Consultations: Schedule consultations with potential surgeons. Use this opportunity to ask about their experience with transgender patients and facial hair transplants specifically.
Online Research: Look for reviews or testimonials online. Some websites are dedicated to reviewing medical professionals, and others are focused on the LGBTQ+ community.
Professional Organizations: Check if the surgeon is a member of professional organizations like the World Professional Association for Transgender Health (WPATH), which could indicate they're up-to-date on best practices for transgender healthcare.
Keep in mind that any surgical procedure comes with risks and costs. Ensure you're aware of these, and don't hesitate to seek a second opinion if you're unsure.
It might also be helpful to connect with others who have undergone similar procedures or are exploring similar options. Online communities, support groups, or LGBTQ+ centers can be great resources, but it isn't a very common procedure so you may have more look looking to cisgender men who have done similar things.
Facial hair transplants are often considered cosmetic procedures, which many insurance plans do not cover. However, coverage varies widely, so it's important to check with your insurance provider. It may be possible to appeal a denial for coverage by saying testosterone isn't indicated for you so this is a necessary treatment to resolve gender dysphoria etc.
If a procedure can be deemed medically necessary (for example, as part of gender-affirming treatment), insurance might cover it. A therapist might be able to help you make this case to your insurance company by writing a WPATH-style letter of support saying that you need it for Gender Dysphoria Reasons tm. It's also helpful if the office of the doctor doing the hair transplant writes a letter of medical necessity too.
Look for a surgeon who is board-certified in plastic surgery or dermatological surgery. This indicates they've met specific educational, training, and professional standards. It's also beneficial if the surgeon has experience with transgender patients, as they may be more attuned to your specific needs and goals, and may know how to get insurance to cover it.
It may seem obvious, but you have to make sure they have extensive experience with hair transplants, particularly facial hair transplants. Unfortunately some doctors are in it for the money and don't put patients first and/or think they're more capable than they are. To make sure they're up to the task, ask to see before and after photos of previous facial hair transplants they've performed, especially for patients with similar goals to yours.
And again, look for patient reviews or testimonials about their experiences with the surgeon. Pay particular attention to the experiences of trans individuals. I can't emphasize how important we are as a community-- we need to look out for each other and make sure that people don't see predatory providers!
Finally, it's crucial that you feel at least somewhat comfortable with the surgeon. They should treat you with respect, listen to your concerns, and provide thorough, honest answers to your questions. You don't need to be best buddies and they don't need a stellar personality either, but you need to feel like they're competent and that you are comfortable asking them questions about your care and could speak to them if you had complications.
While you wait for your consult, there is one alternative that you can try.
Minoxidil (Rogaine):
You can try minoxidil to increase your hair growth. A lot of people use minoxidil (rogaine) on their faces, and a few use it for body hair. It’s considered an “off-label” use- it’s officially approved for head hair and not other locations. Lots of medicines are used off-label, even prescriptions can be given off-label safely. Topical minoxidil is generally safe, as long as you use the dose recommended by the doctor/the bottle.
There's anecdotal evidence that minoxidil can stimulate new facial hair growth and may help thicken existing hairs. However, its effectiveness can vary, and there's limited scientific research on its use for facial hair specifically.
You can get it over-the-counter (aka without a prescription) online through Amazon or other sites, or at a pharmacy like CVS or Walgreens (it’s usually in the isle with men’s hair products like beard dye, and razors).
Minoxidil is generally safe but can cause side effects like dry skin, itching, and irritation. It's also a long-term commitment; you'll need to continue using it to maintain any new hair growth.
You shouldn’t use more than the recommended dose per day, no matter what body part it goes on (i.e. you shouldn’t cover your legs in it, unless you can stretch the normal dose that far). This is because minoxidil is a vasodilator, which lowers blood pressure. You also shouldn’t use oral minoxidil for hair growth because oral minoxidil is used primarily to lower blood pressure.
Will minoxidil (i.e., Rogaine) enhance my facial hair growth?
Using Minox for facial hair
Minox is deadly to some pets like cats and may cause hair growth in unusual places
A high concentration of minoxidil (like 12.5%) can cause low blood pressure
My Personal Experience with Minoxidil Pre-T
If you have some peach fuzz from Minox, dying your existing hair darker with facial hair dye might make it more obvious. This is also true for your body hair.
Will facial hair dye make my facial hair appear thicker/denser?
Remember, there's no one "right" way to be you. Whether through medical procedures, hormone therapy, or personal expression, what matters most is that you feel comfortable and authentic in your own skin. If you're sure that you don't want T, then maybe a facial hair transplant might be the right option for you!
Followers, anything to add?
#Lee says#facial hair transplant#testosterone#facial hair transplant without testosterone#beard transplant#hair transplant#surgery m
42 notes
·
View notes
Text
Medical professionals were aware of at least one case of cancer thought to be linked to a hormonal medication taken to aid gender transitioning, leaked documents from a worldwide transgender nonprofit organization suggest.
In a report released on Monday, the think tank Environmental Progress published hundreds of messages it said were from an internal forum of members of the World Professional Association for Transgender Health (WPATH), in which they discussed gender-affirming treatment and the complications that had arisen from particular cases.
The report comes amid a national debate on gender-affirming health care, as states across the U.S. have introduced legislation to limit treatment for young people who identify as transgender.
Among the messages is one, dated February 24, 2022, in which a person—identified by the report as a doctor—said a colleague developed hepatocarcinomas, or liver tumors, after eight to 10 years of taking testosterone.
"To the best of my knowledge, it was linked to his hormonal treatment," the message said. "Unfortunately I don't have much more details since it was so advanced that he opted for palliative care and died a couple months after."
Newsweek could not independently verify the authenticity of the messages, which appear in the report as screenshots and printouts, and many have names redacted.
When approached for comment, a WPATH spokesperson did not confirm the veracity of the messages, but said it "stand[s] opposed to individuals who misrepresent and de-legitimize the diverse identities and complex needs of this population through scare tactics."
A potential link between testosterone—which regulates pubic development, and which biological males produce naturally more than females—and liver cancer has been noted before.
A 2020 paper published in The Lancet detailed one case in which a 17-year-old transgender man developed liver tumors after taking testosterone. The patient was advised to stop taking testosterone, and the study said the relationship between the hormone and the tumor growth was unknown.
Another study, published in October, found cases in which transgender individuals receiving hormone therapies developed liver tumors, but it said the results were "not sufficient to conclude that there is an association" between the two.
Gender-affirming hormone therapies have also been linked to other forms of cancer—though research has so far been inconclusive.
A 2019 study of transgender adults in Amsterdam found there was an "increased risk of breast cancer in trans women" who had received hormone therapy compared to biological men.
However, last year, another study in the U.S. found that while there were signs of cellular changes with some hormone treatments, testosterone "does not appear to increase risk for breast cancer" and "additional studies are needed to investigate the mechanism responsible for these changes at a cellular level and its role in cancer development."
The message referring to a case of liver cancer was seemingly in response to an earlier one, posted in December 2021, detailing an instance of a 16-year-old patient who had developed hepatic adenomas, benign liver lesions, after being on testosterone for a little over a year and a synthetic form of progesterone.
Hepatic adenomas are rare, but they are associated with oral contraceptive pills and are seen in patients treated with anabolic steroids, according to the National Library of Medicine.
In the messages, the WPATH members discussed academic papers, asked for advice on issues surrounding gender-affirming care and shared their professional experiences. Environmental Progress said the leaks showed members appeared to be improvising treatments and, in some cases, spoke out against safeguarding requirements.
Michael Shellenberger, the president and founder of Environmental Progress, said in a statement that the leaks show that WPATH members "know that the so-called 'gender-affirming care' they provide can result in life-long complications and sterility and that their patients do not understand the implications."
While proponents of gender-affirming care say that such treatments help overcome gender dysphoria—and that barriers to treatment can worsen the mental health of those who feel they are trapped in the wrong body—opponents say that a rise in young people exhibiting gender dysphoria may be in part a product of wider mental health issues that should be identified and addressed before changing a person's body.
Dr. Marci Bowers, president of WPATH, told Newsweek in a statement that it "is and has always been a science- and evidence-based organization whose recommendations are widely endorsed by major medical organizations around the world.
"We are the professionals who best know the medical needs of trans and gender diverse individuals—and stand opposed to individuals who misrepresent and de-legitimize the diverse identities and complex needs of this population through scare tactics."
Bowers added: "Gender, like genitalia, is represented by diversity. The small percentage of the population that is trans or gender diverse deserves healthcare and will never be a threat to the global gender binary."
Update 3/6/24, 4:10 a.m. ET: This article was updated to include comment from Marci Bowers of WPATH.
14 notes
·
View notes
Text

In 2017 I interviewed Bernadette Wren, then head of psychology at the Tavistock Gids clinic, and asked what effect puberty blocking drugs have on the adolescent brain. Looking highly uncomfortable, she replied that the evidence so far was only anecdotal but that the clinic would study its patients “well into their adult lives so that we can see”.
Even back then, before whistleblowers had exposed the rush to medically transition children, it was alarming to hear that heavy-duty GnRH agonists such as triptorelin — used to treat advanced prostate cancer and “chemically castrate” sex offenders — were being prescribed to arrest puberty in hundreds of children as young as 11.
Moreover, they were being used “off-label” before any clinical trials. And the long-term study Wren promised never materialised: Gids (the Gender Identity Development Service) routinely lost touch with patients, and the 44 it did follow reported little long-term mental health improvement.
This shocking chapter in medical history, where the ideological objectives of trans rights campaigners trumped the welfare of disturbed children, is coming to an end worldwide. The decision by NHS England effectively to ban the prescription of puberty blockers comes after the Cass review noted these drugs could “permanently disrupt” brain development, reduce bone density and lock children into a regime of cross-sex hormones requiring life-long patienthood.
NHS England unites with other national health services including those in Finland, France, Sweden and, most notably, the Netherlands — where the “Dutch protocol”, a regime of early blockers then hormones, was devised in 1998 — in pulling back from prescribing them.
Even in the United States, where a toxic combination of extreme activism and medical capitalism has pushed child gender medicine to grotesque extremes, with double mastectomies performed on 14-year-old girls, there is some retrenchment.
Leaks from the World Professional Association for Transgender Health, the body which formulates guidance on “trans healthcare”, reveal doctors perplexed at how they should explain to an 11-year-old child that drugs will render them infertile. Crucially, liberal media such as The New York Times are now reporting grave medical misgivings about child transition, once dismissed as a culture-war issue for the Republican right.
Yet the question remains: how was this ever allowed to happen? For years, puberty blockers were cheerily billed as a mere “pause button”. In 2014, Dr Polly Carmichael, the last head of Gids before the Cass review ordered its closure, went on CBBC in a show called I Am Leo, saying of blockers: “The good thing is, if you stop the injections, it’s like pressing ‘start’ and the body carries on developing as it would if you hadn’t started.”
The BBC permitted her to make this unevidenced claim to an impressionable audience of six to 12-year-olds. Imagine hearing this as a developing girl, freaked out by your new breasts and periods. No wonder Gids referrals subsequently rocketed.
Carmichael failed to mention that she did not know if pressing “restart” on puberty is always medically possible — it is not — and in fact, almost every child Gids put on blockers went on to irreversible cross-sex hormones.
After years in a Peter Pan state while their peers developed, they understandably felt there was no way back and forged on with treatment. Yet if allowed to experience natural puberty, almost 85 per cent of gender dysphoria cases resolve themselves.
Nor did Carmichael tell CBBC kids that the blockers-hormones combination, if taken early enough, not only results in sterility but kills the libido so that a young person will never experience an orgasm.
At the 2020 judicial review brought by a former Tavistock clinician and Keira Bell, the brave young detransitioner rushed onto hormones by Gids, judges expressed astonishment at Gids’s lack of an evidence base.
Reporting on this issue for seven years, I too have been struck by a complete clinical incuriosity. Not only was data not collected, but those who queried treatments or pressed for evidence faced angry condemnation. Perhaps activists knew what research might find because one long-term Finnish study, recently reported in the BMJ, destroyed the myth used to justify blockers: that a child will commit suicide if denied them.
The Finns found that “gender-affirming care” does not make a dysphoric child less suicidal. Rather, such children had the same suicide risk as others with severe psychiatric issues. In other words, changing bodies does not fix troubled minds.
Yet even after NHS England’s announcement, activists refuse to heed the now-overwhelming evidence. In its response, Stonewall persists with the myth that puberty blockers “give a young person extra time to evaluate their next steps”.
Many questions remain unanswered: will private clinics still be permitted to prescribe puberty blockers; and is Scotland’s Sandyford child gender clinic still determined to close its ears to all evidence? Plus, we have few details on how the NHS’s new “holistic” treatment for gender-questioning children will operate when it opens next month.
This repellent experiment — in which girls who like trucks or little boys who dress as princesses, and who invariably grow up to be gay, are corralled inexorably down a road towards life-changing treatments — belongs in the book of medical disgraces. As do the cheerleaders who raised money for Mermaids and those who persecuted whistleblowers or damned journalists asking questions as transphobic.
In 50 years, chemically freezing the puberty of healthy children with troubled minds will be regarded with the same horrified fascination as lobotomies — which, never forget, won the Portuguese neurologist Antonio Egas Moniz the 1949 Nobel prize.
--------------------
{Article source (behind paywall)}
16 notes
·
View notes
Last Seen Blogs

yaleisyu
Yalei's pixelart

velocityinstitute
Velocity Institute Pvt. Ltd.

sportyspice1328-blog
Untitled

pan-the-only
think greek

ozgerzuccaciye-blog
İsimsiz