#but caregiver and advocate? definitely the top two
Text
THE TWELVE ARCHETYPES


53% Caregiver ─ Friendly, sincere, and compassionate, the Caregiver finds their reward in helping others. No one could ask for a better best friend.
33% Advocate ─ The Advocate is the one everyone wants on their side. In the name of justice, they are not afraid to challenge authority or speak up for others.
14% Visionary ─ Leave it to others to live by the status quo. The Visionary is interested in new ways of seeing, solutions not yet imagined, products not yet built.
#♛ about. ⊱ ❝ 𝘐𝘧 𝘐 𝘭𝘰𝘰𝘬 𝘣𝘢𝘤𝘬 𝘐 𝘢𝘮 𝘭𝘰𝘴𝘵. ❞#perfect tbh#visionary and royal are closely tied tho but I think visionary does win out just a little bit#but caregiver and advocate? definitely the top two
1 note
·
View note
Text
A Look at my 2020
The end of the year is upon us. It’s been a tough one for all of us. It is a year we will all remember forever. I want to do a positive reflection of this year. I will probably write a blog about what I hope our country’s New Years Resolutions should be. The thoughts on that have been rolling around my head for a few days. But today, December 16, at 4:30 a.m. and unable to sleep, that 2020 familiar dread of what will happen today waking me early, I want to look at some positives. I want to unwrap the positives of 2020 like a Christmas gift before Christmas so that I can wrap myself in them as a blanket of warmth. One thing that I have been truly impressed with is the resilience of the human spirit. Let’s call this a resilience exercise.
Counting my blessings one by one...
1. I am alive. Surviving is a cause for celebration. As far as I know I have been COVID free...although there were a few days in April or early May when I was sick with something and in Feb I had the strangest cold in my life and this time last year weeks of fatigue ended in frozen shoulder syndrome on Christmas Eve. See, I want to be thankful, but I don’t want to be naive in my retrospection. Best to be honest. I’m not sure if I had COVID or not, but if I did I survived with relatively minor symptoms. Every cough or sniffle I feared in a completely irrational way was COVID. There was the week I walked around sniffing everything to make sure I could still smell. It dawns on me it is going to be difficult to write a honest and, yet, positive, retrospective of 2020. I am alive, but I have never been less healthy. I’ve gained weight. I haven’t had the physical exercise to which I am accustomed and now when I try to take a long walk I realize my stamina is gone. It will take years of concentrated effort once things are “back to normal” for me to become normal again. It wasn’t that I didn’t try. I did yoga daily in the Spring and switched to an online Tai chi class in the summer, but I don’t live near beauty or anything interesting so wasn’t motivated to walk and just my everyday life of lockdown in a studio apartment meant less movement. All of which sounds even to me like not very good justification. Did I mention though that I survived. I am alive. I will take that as blessing number one.
2. No one I care about very deeply has died or even been seriously ill from COVID. Doesn’t March 2020 seem far away? I don’t want to be dismissive of 300;000 dead especially with more to come. I or someone I love could still be gone by New Years Day. But in March and April we held our breaths for an apocalypse and at some point most of us decided to take a breath. I don’t know really if it’s good or bad that we have simply adjusted our normal and the number deaths we are willing to accept. It’s bad, what am I saying? It’s bad. But how long can we wait in fear? So I don’t know, but I want to count as a blessing that those I love have all survived to date. I cannot vanquish the fear, but I can be grateful for survival.
3. I have maintained employment in a bad economy and have mostly been able to work from home. There have been some struggles. Sometimes the work I do is depressing. Sometimes I feel I don’t make a difference. There has never been a worse time to be an advocate...or a person with disability, or a caregiver, or a provider agency, or a health care professional. I have maintained employment.
4. I count among my blessings the fact that I had a wonderful 2020 before....remember there was a 2020 before. I love when my work takes me to Santa Fe for a prolonged time. A friend came out in Feb for a wonderful weekend. Another friend came to Albuquerque to see me for my birthday in early March. I remember thinking how social I was in those first ten weeks in 2020. It’s as if I somehow knew....it sustained me.
5. I count among my blessings that when I felt my mental health despair getting at its worse...the strain of living alone in a studio apartment, working from that same apartment and following the Governor orders not to go or do anything. ..that I had friends and two weekends of “risky” behavior; a friend who came for the Fourth of July holiday and an out of state trip to Durango in late September. I’m fortunate that when I had to have human contact my closest friends were there for me
6. I count as my blessings that Biden won the election. It’s not simply a matter of politics. I’m not sure if the last eight months of the Trump Presidency wasn’t worse for my morale than the pandemic because Trump kind of lost whatever semblance of sanity he had. Part of the trepeditation over what each new day will bring is what Trump will say, do, tweet, exacerbate. I still fear revolution in the street before Jan 20. The pandemic is not the worse of what America has gone through. That’s the oddest thing about this year.
7. Here is the blessing which probably will be unpopular. The lockdown and stress of all we have experienced is tough, but the slowdown is a blessing for me. My life had gotten pretty busy. While I miss travel, it’s ok for a year not to have had the time suck that travel for work entails. I will be so happy the first work trip I get to go on, but I feel like 2020 has given me the gift of time. It’s odd because, like many, my creative sense has suffered. I have written almost nothing. Still, I often think of a Dylan lyric, maybe in the next life I will be able to hear myself think. I could hear myself think this year. Unfortunately I thought about the existentialist angst of the meaning of life and my failures as a human being and I don’t think there is enough time still to process the effects of the pandemic and I’m sick to death of the sound of my thoughts, but....I have been given this unique gift of time. Even on December 16th I am not rushed to shop, to cook, to decorate, to go to a zillion parties. It’s a different year. The Holiday will still come. It is pleasant not to feel urgency over, let’s face it, non-urgent things. I am mentally and emotionally fatigued, but not nearly as physically exhausted as I was this time last year
8. The next one is a big one. The gift of living in the moment. I have spent my entire life since 7th grade when Miss O’Neil gave me a copy of The Rubyait of Omar Khayyam trying to live with the philosophy of living for the now. Clear the cups of past regrets...tomorrow, why I may be myself with yesterday’s seven thousand years. The only time I have ever truly experience this is in a handful of concert experience. Even now, I fear for my future and I blame myself for my mistakes. Still, my relationship with time has changed. There is the sun rising and setting and that is a day. Seasons will change. But the gift of time means I can approach my day differently. When five o clock comes on a workday, a needed nap is a step away. No where to go on a Friday night... no where I can go...means the weekend rhythm exists only as I define it. The simple pleasures we always take for granted mean something more now. There is a coffee truck that stops near me on Fridays and Saturdays. When it first started stopping I was over the moon that I could walk and get a latte with fairly little risk. If I go to the grocery store and have a conversation with a stranger, it is different than it was before. Mindfulness exercise and meditation is one thing, but nothing can compare with this year to further my lessons in this pursuit. May I take the lesson with me into years to come.
9. Zoom...yes, of course I have zoom fatigue. But five friends in five different states having a monthly drink together on zoom is a benefit of the pandemic. I watched a movie this year with someone who lives in Brazil. I celebrated a friend’s sixtieth person even though I couldn’t be with her. I’ve attended book discussions and readings in New York and I already have tickets to an event in March. Kind of love New York. I’ve never been there in person. Just a lot happens there. Educationally and socially the world is now open to me. I am not limited to what is going on in my community. I hope this doesn’t completely go away.
10. Finally, storytelling and music. I found it hard to read new things in the lockdown for a while, but in March friends asked me to a virtual book club of three books I already read and we reread them together which took us into the summer. I rediscovered the Foundation series of Asimov and suddenly I could read again! My favorite book I’ve read published in 2020 is Jess Walter’s The Cold Million. I did read a digital advance copy of David Duchovny’snew book due out in 2021 and it is, in fact, the breakout novel I knew this hot young writer would eventually write. Looking forward to 2021 book club! I finally binged Breaking Bad and The Travelers as well as The Queens gambit and watched Peanut Butter Falcon. I am doing a disability focused watch on the X Files and I better kick it it the rear because I’m presenting on it in Feb. at a conference. My God, Dylan put out his first original music in eight years. It will take me eight years to fully ingest it and enjoy it. You see, no matter what happens, humanity will tell its stories and gather to make its songs. It’s that human resilience. Creation of art is not trivial. It’s vital. It has continued in this odd and strange year. It is humanity’s greatest gift and I have definitely used it this year as a resilience and growth tool.
Those are my top blessings in this horrific and, yet, wondrous year. However, you have been impacted, what we all share in common is that In a very short time it will be a memory of a year in the past.
2 notes
·
View notes
Text
Revenge with a cherry on top.
It's a looong read. TL;DR at the end.
I used to be a therapist. I trained hard not only in my masters degree, which I managed to get at one of the best programs available in the States after working my ass off in undergrad, but also afterwards in seeking out opportunities to get EVIDENCED-BASED training. I emphasize that point because in the world of mental health there is an internal struggle between people like myself who believe you should have proof that what you are doing for that specific person's issue actually works, and those who want to stick to "theoretical" models that sound good, but don't necessarily have any research to back them up. The town where I live is like a ground zero for this problem. I regularly saw unlicensed therapists who had failed the licensure exam multiple times get promoted to supervisor positions, just because they were good at making their companies money. I eventually got out because I couldn't stand the focus on profit over people, which is literally impossible to avoid unless you say fuck everyone and go into business by yourself. By the time I got to a point where I could have made that move financially, I didn't want to be a therapist anymore and moved on. But before that happened, I managed to slam dunk one of the unprofessional people I had to deal with in a very satisfying way.
This case was about a year before I got out. I was doing trauma therapy with several children from one family, meeting with each of them individually and sometimes together per their request. It was easily one of the most fucked up cases I ever dealt with in my career, and that is saying something. You see, I worked for an agency that contracted with Juvenile Justice and Child Protective Services. All of my clients were mandated offenders or kids who had been removed from abusive homes. In this particular case, the abuse was beyond egregious and I remember after the first session where the kids really opened up and told me what happened, I had nightmares all night. It was so bad. But the CPS case manager (referred to from now on as CM) had specifically requested me because of my success with difficult cases. I had a reputation in my county for being good with kids and someone who could handle tough parents. Even though I knew it was going to be rough, I stuck with it.
My first clue this wasn't going to go well was at the initial family team meeting. These happen monthly with the family, CPS, and all their service providers to discuss goals and progress, etc. You're ultimately working towards closing their case when they have done all their treatment and, most importantly, the kids are safe; have received all the care they need; and the caregivers have demonstrated their ability to provide an appropriate home and parenting. The caregivers, let's call them A and B, were selfish, unhinged fuckers. They denied the abuse, lied for one another, and regularly said horrible things about these kids, insisting they were little liars who deserved punishment for causing all this trouble (by speaking up). The thing that was even worse was this team of fifteen or so providers would not fucking stand up to A or B. I got into this work because I had trauma as a kid and wanted to pay forward what my therapist had done for me when I recovered. I also knew what it was like to not be protected by adults in your life who should have been there for you. So, I did not give one shit what A or B thought of me and stood up to their crap when no one else would, saying it was the responsibility of every adult in that room to put the well-being of these children first since they are the children and we are the grown-ups. A and B were pissed as hell, and everyone else who had thus far allowed their ranting without so much as a squeak actually applauded. But that support for sanity did not last.
Months went by and these poor kids couldn't make headway because their insane parents were not only not compliant, they were actively causing trouble for everyone on the case. You can't do trauma work if you don't feel safe, and for these children they were personally living weekly drama that reminds me of Americans enduring Trump now. It was that chaotic. A and B made wild accusations against most of the people on the case (they were a secret drug dealer, they were trying to molest their kids in visits, they spat at them during a visit). One of the other clinicians got into a car wreck one day during work hours and when A and B found out they demanded she take a drug test. Until she did, they refused to comply further with services. Thankfully, her agency stood with her and defended her (she DEFINITELY was not on drugs, I can assure you, it was absurd). But the CM allowed all of this crap to go unchallenged. She was afraid of both A and B, and one by one she fired the people they targeted or made them so disgusted with her lack of spine that they left, until I was the only original team member left. Up until this point, these assholes wouldn't come near me because my reputation was impeccable. I knew a lot of people in the county and their kids loved me. I was the only adult in their life refusing to back down against A and B and, try as she might, CM couldn't get the kids to say what she wanted: that everything was "much better" and she could close the case. This is where the revenge comes in.
So, months have gone by, almost a year, and I am getting burned the fuck out but I am hanging on until I can successfully close this case and one other. Around this time, CM brings on a new therapist for B (the primary offender), who we'll call SmugFace. SmugFace was unexpectedly announced and introduced at one of our monthly meetings and immediately made it clear she did not like me. Not by being rude in an aggressive way, but by being condescending. For the next three months, CM would try every meeting to close the case and, because NOTHING was better, I fought her every time. Before, I had at least one or two people agree with me, but was now met with silence. It soon became clear CM and SmugFace were friends and SmugFace had been brought on to squish me out. She tried every meeting to imply I wasn't qualified, that I was stupid and had clearly misunderstood the children's wishes, that I was taking on a personal crusade against the parents. And she'd do it with a shit-eating grin on her face each time. I was tired and it did make me mad, but I tried not to lose my cool and give her what she wanted. Because of the shitshows caused by A, B and CM's spinelessness, no one stood with me at all anymore. I was on my own.
For cases mandated by the court, you usually have to attend court dates to testify to progress and make recommendations on whether it should remain open or close. The tension was building before our next court date, and CM was laying groundwork through team meetings, emails, and her reports to discredit me and close the case. In private, I felt like I was losing my mind, but I stayed in touch with everyone I had known on the case; kept my documentation like it was going to be examined by the FBI, and bit my tongue. I did everything I could to reassure the children I would fight for them to stay in their safer placement with relatives, and waited for court day. When it came, SmugFace was there with A and B, looking fat with satisfaction (and, well, just fat). She smirked at me every few seconds, tossing her hair over one shoulder and chuckling. I pretended she didn't exist and waited patiently to be admitted to the court room. When our case number was called, I filed in with her, A, B and CM. Service providers sit in the back at this court house, with members of the family, their lawyers and CPS in front. As we a took our seats, the doors behind me opened and every service provider who had ever been on the case came strolling in. One after the other, until there were no seats left and people were standing. SmugFace's eyes just kept getting wider and wider, until she was not so smug anymore.
After the judge called everyone to order, the lawyers spoke for the family and then CPS got to give a report and their recommendations. Then the judge asked service providers if they have anything to say. CM, of course, recommended we close the case (weak, selfish wretch). Then the judge called on me and I deferred to SmugFace, saying that since the case hinged on B's progress, we should hear her thoughts first. SmugFace stammered and sweated under the collective gaze of all these other professionals glaring at her (it was dead silent but had the tension of many buzzing bees) and said B was doing well and the case should close. She tried to throw in some more professional-sounding jargon at the end, jutting out her chin and collecting herself a bit after seeing my deadpan stare. Then the judge turned to me. I stuck to my guns and expressed all my doubts in full, then reported on the kids and my recommendations. The judge, who was one of the toughest in juvenile court, actually stated to the room that she had respect for my views because of the good work she knew I had done with other children. I was really surprised by this, but the best part came next. The judge asked if anyone else wanted to speak and every. Single. Other. Person agreed with my recommendations. They called out all of A and B's bullshit, one after the other, giving so many documented examples it was dizzying. All the while, SmugFace is getting stonier and CM is just shrinking in her chair. The final blow came from the children's court-appointed advocate, who had never once betrayed any agreement with me in meetings. She said she completely agreed with my and others' assessment and could not see how CPS could justify closing the case. The judge calmly declared the case would remain open, told off CM for her being out of touch with the case, and sent us on our way. On the way out, I looked at SmugFace and she refused to acknowledge me.
I smiled all the way to my car, but the best was yet to come. The good news is the kids were fine in the end, A got caught in too many lies and finally went to prison, and I was able to move on to a new career. But before it was all over, we had another monthly team meeting to attend. And that's when it got a little cherry on top. I love to listen to music, and since I drove around a lot for my work I had an extensive playlist to keep me occupied all those hours. I have eclectic tastes and will often put it on shuffle. The day of the last meeting, I showed up early, parked and unplugged my AUX cable from my phone to go inside. This automatically shut off the music, but sometimes it would start to play again when I wasn't expecting it. Not thinking of that, I just went inside and signed in with the CPS receptionist. The lobby was deserted, except for one person - you guessed it, SmugFace. When she saw me turn around, she looked furious. Before, she'd make a point of greeting me and acting syrupy and overly polite. Now, she resolutely turned her back and stayed silent. So of course I went over to say hello. Only I didn't get to. Just as I sat down across from her, my music app came to life and the first lines of "Dirt off your shoulder" by Jay-Z reverberated around the room "BOW DOWN TO THE MOTHERFUCKING GREATEST". And then, as though satisfied it had expressed itself, the app paused again. Without missing a beat, I shrugged and said, "Sorry!" Then smirked. Her fury at the implied double meaning (sorry for the noise but really sorry I kicked your ass) was priceless.
(source) (story by hrowaway42422819)
#prorevenge#by hrowaway42422819#pro#revenge#pro revenge#pro revenge stories#revenge stories#revenge story#last10
673 notes
·
View notes
Link
Since the launch of the National Bail Out campaign last Mother’s Day, the process for freeing trans and gender nonconforming (TGNC) Black individuals awaiting trial has been a continued challenge. U.S. jails generally place people according to their sex assigned at birth and don’t collect data on gender identity, making incarcerated TGNC people difficult to locate. Nevertheless, organizers remain steadfast in their resolve to bail out these “pillars of our communities” and reunite them with their loved ones, organizer Micky Bradford told Rewire.News.
“We are really intentional about naming this as ‘Black Mama’s [Bail Out],’ and really intentional about Black mamas including transgender parents and caregivers who are nonbinary or gender nonconforming,” said Bradford, a regional organizer with TLC@SONG, a collaboration between Southerners on New Ground (SONG) and the Transgender Law Center (TLC).
The effort to raise awareness and free TGNC people from jail is imperative because, as Bradford explained, “We often just hear about trans people dying—from police brutality, street harassment, or intimate partners—but we rarely hear about how bail affects trans folks and tears chosen families apart.”
On any given day, around 450,000 people languish in jails across the country simply because they cannot afford to pay bail. When judges assign bail to defendants awaiting trial, they force individuals who have not yet been tried or convicted of any crime to remain behind bars solely due to poverty. Like every facet of the U.S. criminal justice system, cash bail disproportionately subjugates Black people. Judges are more likely to charge Black defendants bail and to assign them higher bail amounts for the same charges compared to white defendants.
Because there are no official incarceration records on gender identity, there is a data vacuum regarding how TGNC people are affected by mass incarceration and cash bail. But the information that advocacy groups have gathered demonstrates the hyper surveillance and criminalization of Black trans people across the country.
The 2015 U.S. Transgender Survey, which disaggregated data by race, found that nearly half of Black trans people have experienced incarceration. Sixty-one percent of Black respondents reported mistreatment in interactions with the police. One of the most prevalent ways trans people are over-policed is through the criminalization of sex work, for which Black trans women are disproportionately targeted by police. Trans people are also targeted through selectively enforced laws criminalizing HIV, which trans people, particularly women of color, are more likely to contract than the general U.S. population. Bathroom discrimination bills not only criminalize TGNC people for using the restroom of their choice, but also normalize the policing of individuals based on nonbinary gender presentation.
Black trans people are also unlikely to be able to afford bail. Due to transphobia in education and employment, 38 percent of Black trans people live in poverty, compared to 12 percent of the general population and 24 percent of Black people. Forty-two percent of Black trans people have experienced homelessness, and 28 percent have had to work in the underground (illicit) economy to survive. Because nearly half of Black trans people have experienced family rejection, they may also be less likely to have a support network that can afford to bail them out. When they are incarcerated, trans people face staggering rates of sexual and physical assault, harassment, and lack of critical health-care services.
Being held on bail also wreaks havoc in individuals’ lives and tears families apart—whether they are biological or chosen. It can lead to losing a job, apartment, or income needed to put food on the table.
Despite their commitment to centering those most harshly impacted by incarceration, organizers have faced significant logistical challenges with locating TGNC individuals to bail out. Last Mother’s Day, SONG was only able to bail out three TGNC people; an additional two were denied bail.
U.S. jails imprison individuals according to a binary definition of gender, and usually place people according to their genitals or sex assigned at birth. On top of this, jails often isolate trans people in solitary confinement or mental health wards, making it much more difficult for organizations offering support services to reach them.
“There is no system for tracking if someone is transgender, and jails are not culturally competent,” said Flor Bermudez, legal director at the TLC. “There is no way to find transgender people in jail unless they self-identify to their friends and family, their friends and family know that they are there, and they tell an organizer that the person is inside. It is extremely difficult to find them because all of the data that’s trackable public information will have their sex assigned at birth and no gender identity.”
Community networks and safe spaces for queer and trans people have been key to finding more trans mamas to bail out. This year, SONG created a hotline that individuals in or outside of jail in Atlanta can call to inform them about someone who needs to be bailed out. TLC is also partnering with SONG to provide legal consultation and technical assistance to organizers conducting bailouts across the South.
“Last year’s bailout really taught us so much,” said Mary Hooks, co-executive director of SONG, which has been a leader in the bailout campaign. “One thing we saw that was most effective in trying to identify trans and gender nonconforming people was community building and outreach. Some of our people are hitting the streets where we know are safe spaces for TGNC people so folks know what we’re doing. If they know somebody that gets picked up during this time, or if they know someone who’s currently in there, they have our hotline.”
SONG hopes that the organizing strategies it is developing in partnership with TLC will provide guidance to other organizations in the bailout coalition that are also facing difficulties finding TGNC folks to bail out. Over the past year, racial justice organizations across the country have bailed out around 200 people, with donations totaling nearly $1 million from more than 14,000 individuals. Last Mother’s Day alone, the National Bail Out campaign paid bail for more than 100 Black mamas and shined a spotlight on theinjustices of the cash bail system.
Just this week, in a landmark victory for the bail out movement, Google banned bail bond advertisements from its platforms on May 7, following advocacy from the Essie Justice Group, Civil Rights Corps, Color of Change, Upturn, and the Vera Institute of Justice.
The bailout campaign forms part of the Movement for Black Lives’ broader agenda to combat the criminalization of Black trans and queer people. SONG is also developing more Black LGBTQ organizers, who can play a leadership role in advocating for the rights of those in their communities. TLC brings class action lawsuits across the country in order to change laws that discriminate against TGNC people. In a landmark victory in 2015, TLC represented Shiloh Quine in a case that forced California to offer gender-affirming health care, including surgery, to incarcerated individuals, and to allow trans prisoners access to clothing and commissary items consistent with their gender identity.
Other groups around the country have also been offering support to trans women taken into custody. The Transgender, Gender Variant, and Intersex Justice Project (TGIJP) has pioneered a model for aiding trans women during and after incarceration. The organization goes into Bay Area jails and prisons weekly to conduct political education and monitor the well-being of trans prisoners. It also has a re-entry program offering employment opportunities to trans individuals coming out of jails and prisons to work at their organization. “Hopefully one day we’ll have an organization full of formerly incarcerated trans women on this side of the fence,” said Janetta Johnson, executive director of TGIJP, which has also been offering support to bailouts in the Bay Area.
The efforts to include trans caregivers in the Black Mamas Bail Out reflect a commitment to center those most marginalized by the United States’ oppressive societal structures within the movement for Black liberation. “We actually cannot separate our race, our gender, or our class. We can’t separate those into bite-sized issues that we then rally around,” said Bradford, who identifies as a Black transfemme. “The systems that are oppressing trans people are the systems that are oppressing immigrants, are the systems that are oppressing Black folks, are the systems that are oppressing poor and working folks. It goes on and on. These are intersectional issues and so we have to treat them that way.”
#trans#transgender#Black women#National Bail Out#Black Mamas Bail Out#carcerality#bail#prison#civil rights
8 notes
·
View notes
Text
Top 10 Tips For Colorado Medical Cannabis Dispensaries Dealing With HB 10-1284
"How can we are the cause of what's perhaps the most dramatic legal disparities in medical cannabis to date? The issue of non-profit ""sale"" of medical cannabis to qualified patients via collectives and cooperatives. There's nothing else this way dispute. What do the experts say relating to this anyway?
Steve Cooley, The Los Angeles District Attorney, disagrees with Jerry Brown, the California State Attorney General.
youtube
How could two prominent state-employed attorneys arrived at wholly different conclusions around the answer? First the Los Angeles District Attorney claims ""all sales are illegal"". The California State Attorney General was sure enough to publish in their guidelines that ""storefront collectives could be legal under state guiidelines"". How could this be? After all, each attorney is looking with the same, right?
So what is the answer? What does what the law states say?
COMPASSIONATE-USE ACT 1996
Proposition 215 which has been approved by a majority of Californians in 1996 also it became called the Compassionate-Use Act. The statute itself will not say anything about ""sales"" however it does speak about ""possession"", ""cultivating"", obtaining medical cannabis, about affordability and ""distribution"".
It does point out that qualified patients in addition to their primary caregivers won't be victim to criminal issues:
""(B) To ensure that patients as well as their primary caregivers who obtain and make use of marijuana for medical purposes upon counsel of an physician aren't be subject to criminal prosecution or sanction.""
And what's more, it pushes governments to help ensure ""safe and affordable access"" to medical cannabis for ""all qualified patients"".
""(C) To encourage the federal and state governments to implement an agenda for the safe and affordable distribution of marijuana to everyone patients in medical demand for marijuana.""
The Los Angeles District Attorney, Steve Cooley, had State and Federal law enforcement agents raid a medical cannabis collective and arrest at least 3 people, the week before Christmas. He insists ""all sales are illegal"". This is apparently from the letter and spirit of what the law states, not the mention the spirit in the season.
Also if all ""sales"" are illegal, how come the Compassionate-Use Act say ""affordable""? If the patients are financially responsible for your cannabis, what makes Cooley expect the currency to be exchanged? What's wrong with incremental reimbursements?
MEDICAL MARIJUANA PROGRAM OF 2004
The Medical Marijuana Program (MMP) got into law in 2004 through the legislative approval of Senate Bill 420. It was the state's attempt ""to implement an agenda to the safe and affordable distribution of marijuana to everyone patients in medical need of marijuana,"" because Compassionate-Use Act of 1996 (Prop 215) encourages the State and Federal government to complete.
The MMP improves usage of medical cannabis for qualified patients by approving collectives and cooperatives.
""(3) Enhance the access of patients and caregivers to medical cannabis through collective, cooperative cultivation projects.""
What Steve Cooley doesn't appear to understand is non-profit storefront Medical Cannabis Dispensing Collectives/Cooperatives are the distribution aspect of ""cultivation projects"". Just like a collective cultivation farm wouldn't have customers arrive at the farm to obtain their tomatoes, they will have to get their collective tomatoes at the farmer's market or distribution location-- that's how medical cannabis collective cultivations occur. Grown in one place for safety as well as other reasons, then distributed at another location.
The MMP goes on to talk about every one of the criminal statutes that qualified patients and primary caregivers are exempt from. In section 11362.765, it says: ""shall not be subject, on that sole basis, to criminal liability under Section 11357, 11358, 11359, 11360, 11366, 11366.5, or 11570.""
Let's look at these 1 by 1:
11357: [possession],
11358: [cultivation],
11359: [possession for sale],
11360: [""transports, imports into this state, sells, furnishes, administers, or gives away""- or offers to or attempts to accomplish any of those],
11366: [Every one who opens or maintains any place for that reason for unlawfully selling, giving out, or using any controlled substance]
11366.5 [Managing an area for manufacture, storage and/or the distribution of your controlled substance]
11570 [Every building or place used for that function of unlawfully selling, serving, storing, keeping, manufacturing, or handing out any controlled substance, precursor, or analog specified by this division, and every building or place wherein or where those acts come about, is cbdforsalenearme.com a nuisance which shall be enjoined, abated, and prevented, and for which damages could possibly be recovered, whether it is really a public or private nuisance.]
The Health and Safety Code section 11360 specifically says ""sells"". Not only that, in addition, it says: ""gives away"" and ""furnishes"". How come the LA District Attorney's office says ""all sales are illegal"" and non-profit storefront medical cannabis dispensing collectives/cooperatives are banned?
In that same bill,
""11362.775. Qualified patients, persons with valid identification cards, as well as the designated primary caregivers of qualified patients and persons with identification cards, who associate inside State of California to be able collectively or cooperatively growing marijuana for medical purposes, shall not solely around the basis of that fact be be subject to state criminal sanctions under Section 11357, 11358, 11359, 11360, 11366, 11366.5, or 11570.""
Again, it says that patients can collectively cultivate cannabis and distribute it amongst themselves for non-profit. Again, the distribution of medical cannabis is separate from the cultivation the same as the manufacturing of my vicodin can be found apart from my pharmacy.
The Medical Marijuana Act also calls around the State Attorney General to supply guidelines associated with medical cannabis:
""The bill would require the Attorney General to build up and adopt guidelines to guarantee the security and non-diversion of marijuana grown for medical use, as specified.""
And that just what State Attorney General, Jerry Brown did inside the late summer of 2008.
GUIDELINES FOR THE SECURITY AND NON-DIVERSION OF MARIJUANA GROWN FOR MEDICAL USE August 2008
To fulfill his mandate, the State Attorney General release these guidelines to assist law enforcements do their jobs based on State law and to help you patients understand those laws.
The guidelines state non-profit storefront Medical Cannabis Dispensing Collectives and Cooperatives may be legal under state law if they followed the rules as well as the above laws.
""It may be the opinion of the Office which a properly organized and operated collective or cooperative that dispenses medical marijuana by having a storefront may be lawful under California law""
The State Attorney General confirms what what the law states says. The Attorney General could be the highest-ranking legal employee of the State of California. His office also taken care of immediately the issues raised in Los Angeles by City Attorney's office.
According to the New York Times on October 17: Christine Gasparac, a spokeswoman for State Attorney General Jerry Brown, declared that after Mr. Trutanich's comments in Los Angeles, police force officials and advocates from across the state had called seeking clarity on medical marijuana laws.
Mr. Brown has issued legal guidelines that offer nonprofit sales of medical cannabis, she said. But, she added, with laws being interpreted differently, ""the final answer may ultimately come from the courts.""
So exactly what do the courts say?
PEOPLE v. MENTCH
The District Attorney's office would have you think that the Mentch decision outlaws non-profit storefront Medical Cannabis Dispensing Collectives/Cooperatives and makes ""all sales illegal"" but that decision has to accomplish using the definition of ""primary caregiver"" not sales.
Mentch had 82 marijuana plants growing in the home anf the husband sold the medicine to people who located his home with all the primary reason for buying cannabis. The most of the plants in Mentch's home belonged to him as they testified. Their operations was not a collective or possibly a cooperative nor a store. Mentch owned Hemporium, a for-profit care giving and consultancy business, not a non-profit collective or even a cooperative.
Based from the evidence the courts figured Mentch's operation was primarily a for-profit commercial venture and was not a primary caregiver for all those he supplied medical cannabis to from his home business. I've written concerning this comprehensive here.
So there you've just what the courts say, what are the State Attorney says, and what are the laws say; all confirm non-profit storefront dispensing of medical cannabis may be legal under State law.
Now the Los Angeles District Attorney must obey regulations and the will with the people and prevent wasting time and resources to hurt medical cannabis patients especially ahead of Christmas. Especially when you'll find over 7,000 untested rape kits how the District Attorney says he will not have the resources to handle.

"
0 notes
Text
Top 10 Tips For Colorado Medical Marijuana Dispensaries Facing HB 10-1284
"How can we account for precisely what is perhaps probably the most dramatic legal disparities in medical cannabis thus far? The issue of non-profit ""sale"" of medical cannabis to qualified patients via collectives and cooperatives. There's nothing else this way dispute. What do professionals say relating to this anyway?
Steve Cooley, The Los Angeles District Attorney, disagrees with Jerry Brown, the California State Attorney General.
How could two prominent state-employed attorneys come to wholly different conclusions on the answer? First the Los Angeles District Attorney claims ""all sales are illegal"". The California State Attorney General was sure enough to publish in his guidelines that ""storefront collectives could be legal under state guiidelines"". How could this be? After all, each attorney is looking with the same, right?
So what is the answer? What does regulations say?
COMPASSIONATE-USE ACT 1996
Proposition 215 which was approved by a majority of Californians in 1996 and it became referred to as the Compassionate-Use Act. The statute itself won't say anything about ""sales"" however it does speak about ""possession"", ""cultivating"", obtaining medical cannabis, about affordability and ""distribution"".
It does state that qualified patients as well as their primary caregivers won't be victim to criminal issues:
""(B) To ensure that patients as well as their primary caregivers who obtain and make use of marijuana for medical purposes upon counsel of your physician usually are not be subject to criminal prosecution or sanction.""
And it also pushes governments to help you ensure ""safe and affordable access"" to medical cannabis for ""all qualified patients"".
""(C) To encourage the federal and state governments to implement an agenda for your safe and affordable distribution of marijuana to everyone patients in medical demand for marijuana.""
The Los Angeles District Attorney, Steve Cooley, had State and Federal police officers agents raid a medical cannabis collective and arrest a minimum of 3 people, the week before Christmas. He insists ""all sales are illegal"". This seems to be contrary to the letter and spirit of regulations, not the mention the spirit from the season.
Also if all ""sales"" are illegal, how come the Compassionate-Use Act say ""affordable""? If the patients are financially responsible for the cannabis, how can Cooley expect the currency to become exchanged? What's wrong with incremental reimbursements?
MEDICAL MARIJUANA PROGRAM OF 2004
The Medical Marijuana Program (MMP) arrived to law in 2004 from the legislative approval of Senate Bill 420. It was the state's attempt ""to implement an idea for your safe and affordable distribution of marijuana to all patients in medical need of marijuana,"" because Compassionate-Use Act of 1996 (Prop 215) encourages the State and Federal government to perform.
The MMP improves entry to medical cannabis for qualified patients by approving collectives and cooperatives.
""(3) Enhance the access of patients and caregivers to medicinal marijuana through collective, cooperative cultivation projects.""
What Steve Cooley doesn't apparently understand is non-profit storefront Medical Cannabis Dispensing Collectives/Cooperatives are the distribution part of ""cultivation projects"". Just like a collective cultivation farm wouldn't have customers arrived at the farm to get their tomatoes, they'd have to get their collective tomatoes at the farmer's market or distribution location-- that's how medical cannabis collective cultivations occur. Grown a single area for safety and also other reasons, then distributed at another location.
The MMP procedes talk about every one of the criminal statutes that qualified patients and primary caregivers are exempt from. In section 11362.765, it says: ""shall not subject, on that sole basis, to criminal liability under Section 11357, 11358, 11359, 11360, 11366, 11366.5, or 11570.""
Let's examine these 1 by 1:
11357: [possession],
11358: [cultivation],
11359: [possession for sale],
11360: [""transports, imports into this state, sells, furnishes, administers, or gives away""- or proposes to or attempts to complete any of those],
11366: [Every person who opens or maintains any place for your function of unlawfully selling, giving away, or using any controlled substance]
11366.5 [Managing an area manufacture, storage and/or the distribution of your controlled substance]
11570 [Every building or place used to the intent behind unlawfully selling, serving, storing, keeping, manufacturing, or handing out any controlled substance, precursor, or analog specified in this division, and each building or place wherein or on which those acts occur, can be a nuisance which will probably be enjoined, abated, and prevented, and then for which damages could possibly be recovered, whether it can be a public or private nuisance.]
The Health and Safety Code section 11360 specifically says ""sells"". Not only that, it also says: ""gives away"" and ""furnishes"". How come the LA District Attorney's office says ""all sales are illegal"" and non-profit storefront medical cannabis dispensing collectives/cooperatives are banned?
In that same bill,
""11362.775. Qualified patients, persons with valid identification cards, and the designated primary caregivers of qualified patients and persons with identification cards, who associate inside the State of California so as collectively or cooperatively to cultivate marijuana for medical purposes, shall not solely around the basis of that fact be at the mercy of state criminal sanctions under Section 11357, 11358, 11359, 11360, 11366, 11366.5, or 11570.""
Again, it says that patients can collectively cultivate cannabis and distribute it amongst themselves for non-profit. Again, the distribution of medical cannabis is outside of the cultivation similar to the manufacturing of my vicodin is located outside of my pharmacy.
youtube
The Medical Marijuana Act also calls around the State Attorney General to offer guidelines related to medical cannabis:
""The bill would require Attorney General to build up and adopt guidelines to be sure the security and non-diversion of marijuana grown for medical use, as specified.""

And that precisely what State Attorney General, Jerry Brown did inside late summer of 2008.
GUIDELINES FOR THE SECURITY AND NON-DIVERSION OF MARIJUANA GROWN FOR MEDICAL USE August 2008
To fulfill his mandate, the State Attorney General release the following tips to help law enforcements do their jobs in accordance with State law and to help patients understand those laws.
The guidelines state non-profit storefront Medical Cannabis Dispensing Collectives and Cooperatives might be legal under state guidelines should they followed the policies and the above laws.
""It could be the opinion of this Office which a properly organized and operated collective or cooperative that dispenses medical cannabis through a storefront could possibly be lawful under California law""
The State Attorney General confirms what regulations says. The Attorney General is the highest-ranking legal employee in the State of California. His office also answered the problems raised in Los Angeles by City Attorney's office.
According towards the New York Times on October 17: Christine Gasparac, a spokeswoman for State Attorney General Jerry Brown, asserted after Mr. Trutanich's comments in Los Angeles, police force officials and advocates from round the state had called seeking clarity on medical cannabis laws.
Mr. Brown has issued legal guidelines that provide nonprofit sales of medicinal marijuana, she said. But, she added, with laws being interpreted differently, ""the final answer will eventually come from the courts.""
So what do the courts say?
PEOPLE v. MENTCH
The District Attorney's office would have you believe that alternative depression treatment san carlos the Mentch decision outlaws non-profit storefront Medical Cannabis Dispensing Collectives/Cooperatives and makes ""all sales illegal"" but that decision has to accomplish using the definition of ""primary caregiver"" not sales.
Mentch had 82 marijuana plants growing in their home and that he sold the medicine to five individuals who came to his home while using primary reason for buying cannabis. The most of the plants in Mentch's home belonged to him as they testified. Their operations wasn't a collective or even a cooperative nor a storefront. Mentch owned Hemporium, a for-profit care giving and consultancy business, not really a non-profit collective or even a cooperative.
Based from the evidence the courts figured that Mentch's operation was primarily a for-profit commercial venture anf the husband had not been a primary caregiver for anyone he supplied medical cannabis to from his work from home business. I've written about it thorough here.
So there you have what are the courts say, exactly what the State Attorney says, and exactly what the laws say; all confirm non-profit storefront dispensing of medical cannabis can be legal under State law.
Now the Los Angeles District Attorney must obey regulations and the will with the people which will help prevent wasting time and resources to hurt medical cannabis patients especially ahead of Christmas. Especially when you will find over 7,000 untested rape kits how the District Attorney claims to not need the resources to deal with.
"
0 notes
Text
Top 10 Tips For Colorado Medical Marijuana Dispensaries Facing HB 10-1284
"How can we be the cause of what's perhaps the most dramatic legal disparities in medical cannabis up to now? The issue of non-profit ""sale"" of medical cannabis to qualified patients via collectives and cooperatives. There's nothing else this way dispute. What do the experts say relating to this anyway?
Steve Cooley, The Los Angeles District Attorney, disagrees with Jerry Brown, the California State Attorney General.
How could two prominent state-employed attorneys come to wholly different conclusions around the answer? First the Los Angeles District Attorney claims ""all sales are illegal"". The California State Attorney General was sure enough to publish in the guidelines that ""storefront collectives could possibly be legal under state guidelines"". How could this be? After all, each attorney is looking in the same task, right?
So what is the answer? What does regulations say?
COMPASSIONATE-USE ACT 1996
Proposition 215 which has been approved by the majority of Californians in 1996 and it became known as the Compassionate-Use Act. The statute itself won't say anything about ""sales"" but it does talk about ""possession"", ""cultivating"", obtaining medical cannabis, about affordability and ""distribution"".
It does say that qualified patients as well as their primary caregivers will not be victim to criminal issues:
""(B) To ensure that patients along with their primary caregivers who obtain and use marijuana for medical purposes upon the recommendation of the physician are certainly not susceptible to criminal prosecution or sanction.""
And in addition, it pushes governments to help you ensure ""safe and affordable access"" to medical cannabis for ""all qualified patients"".
""(C) To encourage the federal and state governments to implement an agenda for that safe and affordable distribution of marijuana to all or any patients in medical need of marijuana.""
The Los Angeles District Attorney, Steve Cooley, had State and Federal police force agents raid a medical cannabis collective and arrest no less than 3 people, the week before Christmas. He insists ""all sales are illegal"". This appears to be against the letter and spirit of the law, not the mention the spirit in the season.
Also if all ""sales"" are illegal, how come the Compassionate-Use Act say ""affordable""? If the patients are financially responsible to the cannabis, what makes Cooley expect the currency to become exchanged? What's wrong with incremental reimbursements?
MEDICAL MARIJUANA PROGRAM OF 2004
The Medical Marijuana Program (MMP) came into law in 2004 over the legislative approval of Senate Bill 420. It was the state's attempt ""to implement a plan for the safe and affordable distribution of marijuana to all patients in medical need for marijuana,"" because the Compassionate-Use Act of 1996 (Prop 215) encourages the State and Federal government to accomplish.
The MMP improves use of medical cannabis for qualified patients by approving collectives and cooperatives.
""(3) Enhance the access of patients and caregivers to medical cannabis through collective, cooperative cultivation projects.""
What Steve Cooley doesn't manage to understand is non-profit storefront Medical Cannabis Dispensing Collectives/Cooperatives are the distribution aspect of ""cultivation projects"". Just like a collective cultivation farm wouldn't have customers arrived at the farm to have their tomatoes, they will have to get their collective tomatoes with a farmer's market or distribution location-- that's how medical cannabis collective cultivations occur. Grown in a place for safety and also other reasons, then distributed at another location.
The MMP goes on to talk about each of the criminal statutes that qualified patients and primary caregivers are exempt from. In section 11362.765, it says: ""shall not subject, on that sole basis, to criminal liability under Section 11357, 11358, 11359, 11360, 11366, 11366.5, or 11570.""
Let's examine each one of these one at a time:
11357: [possession],
11358: [cultivation],
11359: [possession for sale],
11360: [""transports, imports into this state, sells, furnishes, administers, or gives away""- or offers to or attempts to complete any of those],
11366: [Every individual that opens or maintains anywhere for that reason for unlawfully selling, handing out, or using any controlled substance]
11366.5 [Managing a spot for manufacture, storage and/or the distribution of the controlled substance]
11570 [Every building or place used for your reason for unlawfully selling, serving, storing, keeping, manufacturing, or giving out any controlled substance, precursor, or analog specified by this division, each building or place wherein or upon which those acts come about, is really a nuisance which shall be enjoined, abated, and prevented, as well as for which damages could possibly be recovered, whether it can be a public or private nuisance.]
The Health and Safety Code section 11360 specifically says ""sells"". Not only that, it also says: ""gives away"" and ""furnishes"". How come the LA District Attorney's office says ""all sales are illegal"" and non-profit storefront medical cannabis dispensing collectives/cooperatives are banned?
In that same bill,
""11362.775. Qualified patients, persons with valid identification cards, as well as the designated primary caregivers of qualified patients and persons with identification cards, who associate from the State of California in order collectively or cooperatively growing marijuana for medical purposes, shall not solely about the basis of that fact be be subject to state criminal sanctions under Section 11357, 11358, 11359, 11360, 11366, 11366.5, or 11570.""
Again, it says that patients can collectively cultivate cannabis and distribute it amongst themselves for non-profit. Again, the distribution of medical cannabis is outside of the cultivation just like the manufacturing of my vicodin is situated outside of my pharmacy.
The Medical Marijuana Act also calls on the State Attorney General to offer guidelines linked to medical cannabis:
""The bill would need the Attorney General to formulate and adopt guidelines to ensure the security and non-diversion of marijuana grown for medical use, as specified.""
And that what exactly State Attorney General, Jerry Brown did inside the late summer of 2008.
GUIDELINES FOR THE SECURITY AND NON-DIVERSION OF MARIJUANA GROWN FOR MEDICAL USE August 2008
To fulfill his mandate, the State Attorney General release the following tips to assist law enforcements do their jobs in accordance with State alternative depression treatment san carlos law and to assist patients understand those laws.
The guidelines state non-profit storefront Medical Cannabis Dispensing Collectives and Cooperatives might be legal under state guidelines whenever they followed the guidelines and the above laws.
""It is the opinion of the Office that the properly organized and operated collective or cooperative that dispenses medical marijuana by having a storefront may be lawful under California law""
The State Attorney General confirms what legislation says. The Attorney General will be the highest-ranking legal employee in the State of California. His office also taken care of immediately the difficulties raised in Los Angeles by City Attorney's office.
According on the New York Times on October 17: Christine Gasparac, a spokeswoman for State Attorney General Jerry Brown, said that after Mr. Trutanich's comments in Los Angeles, police officers officials and advocates from around the state had called seeking clarity on medical marijuana laws.
youtube
Mr. Brown has issued regulations that offer nonprofit sales of medical cannabis, she said. But, she added, with laws being interpreted differently, ""the final answer will eventually come from the courts.""
So what do the courts say?
PEOPLE v. MENTCH
The District Attorney's office would have you believe that the Mentch decision outlaws non-profit storefront Medical Cannabis Dispensing Collectives/Cooperatives and makes ""all sales illegal"" but that decision has to do using the definition of ""primary caregiver"" not sales.
Mentch had 82 marijuana plants growing as part of his home and that he sold the medicine to 5 individuals who came to his home using the primary purpose of buying cannabis. The most of the plants in Mentch's home belonged to him while he testified. Their operations had not been a collective or perhaps a cooperative nor an outlet. Mentch owned Hemporium, a for-profit care giving and consultancy business, not only a non-profit collective or perhaps a cooperative.
Based from the evidence the courts figured Mentch's operation was primarily a for-profit commercial venture anf the husband was not a primary caregiver for the people he supplied medical cannabis to from his work from home business. I've written about it detailed here.
So there you've what are the courts say, what are the State Attorney says, and what the laws say; all confirm non-profit storefront dispensing of medical cannabis may be legal under State law.
Now the Los Angeles District Attorney must obey what the law states and the will in the people which will help prevent wasting time and resources to hurt medical cannabis patients especially just before Christmas. Especially when you will find over 7,000 untested rape kits that the District Attorney states not have access to the resources to address.
"
0 notes
Text
The Debates Swirling Around Microchipping of Animals
Microchipping of companion animals is a topic that reflects several heightened issues the United States and the rest of the world are wrestling with these days, including regulation, guardian’s rights and the animal’s health.
Implanted microchips emit radio frequencies upon scanning the area that convey an identification number. If the frequencies between the scanner and the chip do not match, the probability exists that the scanner will not pick up the chip’s frequency. Universal scanners do exist, but these are not 100% guaranteed. Per one study, three of four universal commercial scanners tested had sensitivities ≥ 88.2%.
In fact, numerous variables exist that could impact proper detection. These include: the chip or scanner fails to transmit any signal, the scanner or chip is intentionally incompatible, the scanner will not detect the chip, the scanner will detect but not read the chip, scanning technique, or lack of registration by the pet caregiver.
While we cannot control all variables, the American Veterinary Medical Association (AVMA) points out that several countries around the world have enacted laws stating that the chips and the scanners should meet the International Standards Organization (ISO) standards: 11784, chip; and, 11785, scanner. The ISO approved frequency is 134.2-kHz. Additional language attached to the standards include a unique 15-digit identification number assigned to each companion pet as well as other requirements.
In 2005, the United States federal government considered mandating national standards for pet microchips and scanners. The AVMA article states, “In July 2007, the U.S. Department of Agriculture Plant Health and Inspection Service (USDA-APHIS) released a report to Congress regarding microchipping of pets in the United States. Because the Animal Welfare Act does not authorize the USDA-APHIS to regulate private pet ownership, the organization concluded that it cannot mandate a national standard for pet microchips or scanners.”
As of 2017, non-ISO scanners and chips at 125-kHz and 128-kHz frequencies are still available for sale in the U.S. So, we are not assured of the higher compatibility between the transponders that an ISO standard would alleviate. Inevitably, the task to endorse, advocate and communicate ISO recommended standards and a central database portal have fallen to the AVMA, American Animal Hospital Association (AAHA) and World Small Animal Veterinary Association (WSAVA).
Additionally, transponder manufacturers maintain independent registry databases. AAHA has taken an additional step to help identify a participating registry by creating the website, http://www.petmicrochiplookup.org/.
Please bear in mind that a law about a standard is not the same as a compulsory microchip law for companion pets. Although several countries have compulsory laws, the U.S. federal government does not have a compulsory microchip law. States, counties or municipalities may have such laws to some degree. For instance, a state may have a law that companion pets adopted from a shelter must be microchipped. Please check with your local shelter or veterinarian on microchip laws in your area.
Nonetheless, if you choose or are required to have your companion dog or cat microchipped – AND they become lost – it could mean life or death due to transponder failure or miscommunication. Clearly, this is a health and survival concern.
On the other hand, pet caregivers are becoming increasingly concerned about health problems that may arise from implantation. For instance, incorrect implantation can cause life-threatening conditions such as tetraparesis (weakness/paralysis of all limbs) and tachypnea (increased breathing rate). The AVMA supports the WSAVA’s recommendation on implant site and that only a licensed veterinarian performs the procedure or it is placed under the supervision by a licensed veterinarian. My views concur.
Cancer also poses a concern with microchips. Thus far, to my knowledge, there are no documented reports of microchips leaching toxins into the bloodstream. However, laboratory studies have found a range of 0.8-12% cancerous tumors in laboratory rats and mice, at the implantation site or around the microchip. Remember, though, that mice and rats could behave quite differently than cats and dogs, and certainly are smaller species. We know that rodents have a higher propensity to develop sarcomas of some sort around any implantation site.
But, indeed, cancerous tumors have been found near, attached to or encapsulating microchips in dogs and cats. The attempt, however, to create a direct link between microchips and cancer in dogs and cats has been problematic. The biggest variable is vaccines because they, too, are injected in the same region as microchips and can cause similar tissue reactions including sarcomas. Case in point, vaccine-associated sarcomas are common in cats. Inevitably, we are left with the question, “Is it the microchip, the vaccine or a combination?”
Overall, the number of reports amount to only a handful. Could potential microchip-associated tumors or lumps be underreported? Most definitely so. Upon review of the reports, most of the dogs and cats were generally older. We know that any foreign substance inserted into the body for long periods of time can cause neoplasms to form. So, perhaps we may want to consider excising the chip once our companion pets reach senior citizen status.
One six-year study on nine dogs with microchips revealed unchanged fibrous capsules from year one to year six. Bear in mind though that fibrous capsules normally form around microchips.
The more immediate and important concern in my mind is microchip migration. Some have entered body cavities. One microchip actually pierced a dog’s heart. Thankfully, it was removed safely by a veterinary surgeon.
Adverse Events Statistics
Instead of reviewing anecdotal incidences regarding microchip migrations and cancer, please read the “Microchip Adverse Event Reporting Scheme Review from Voluntary to Compulsory Reporting April 2014 through December 2015”, published by the Veterinary Medicines Directorate of the United Kingdom.
For context, a law was passed in England that all dogs must be microchipped starting April 6, 2016. Wales and Scotland introduced similar legislation at the time. Northern Ireland already had compulsory microchipping laws. This law is very comprehensive and considerate of all parties. Even though a dog must be microchipped, all adverse events (failures, migrations, reactions) must be reported. Additionally, a pet caregiver can ask for a medical exemption.
The review provides a good baseline of adverse events, but does not provide the counter-balance of total number of implanted microchips for the entire animal population. It is estimated that 8.5 million cats and 7.5 million dogs live in the UK. Other incomplete information is when implantation had occurred for the majority of companion pets that had an adverse event. The authors of the report admit that these are drawbacks.
Another flaw with the review is when two adverse events were occurring at the same time. If it is a reaction and a migration or failure, it is categorized as a reaction. While a reaction is an empirical finding, when a migration and a failure occur, the review considers this to be a failure – which is a flawed decision in my view.
In any event, let’s look at the statistics.
1,420 adverse events were submitted during the time frame of April 2014-December 2015. Please bear in mind that some of the reports were historical. 1,195 reports related to dogs, 219 to cats, four to rabbits, a horse and a tortoise.
39 adverse reactions were reported for dogs; 35 of those reported lumps at site implantation and 5 reports included details on vaccinations.
21 cats had adverse reactions and 11 of those developed lumps.
630 failure reports were received. The authors of the review account for any incomplete information that they received. For example: in 538 of the cases, the scanner was working, a full body scan was done, but the presence of a chip was not confirmed by another means such as palpation or imaging. At the end of the day, they determined that only 56 (less than 9%) were truly chip failures. 39 cases had medical records of implantation date and the failures occurred 3-4 years after said date.
Migration reports are fascinating. Please remember, too, that several migrations might be categorized as a failure.
729 reported migrations in dogs, cats, a rabbit and a tortoise.
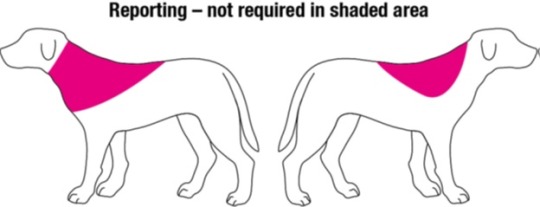
300 cases were dismissed because of being considered in the allowable migration zone as shown in the figure below.
302 reports of true migrations. The furthest migration was to a dog’s left groin.
Yes or no to microchipping?
You always have the option to forego adopting a pet if the law in your state or municipality requires microchipping. However, this poses a dilemma as you need to balance the potential risk of losing an unidentified pet with the potential adverse events from microchipping. An alternative option is to tattoo your phone number on a non-removable tissue like the inside of the back leg. If your pet has distinguishing physical features, you also can photograph all four sides and the top to allow for identification on flyers, by e-mail, and upon his/her retrieval.
If your companion pet does have a microchip, please have a full body and properly performed scan completed every time you visit your veterinarian.
W. Jean Dodds, DVM
Hemopet / NutriScan
11561 Salinaz Avenue
Garden Grove, CA 92843
References
Lord, Linda et al. "Sensitivity of Commercial Scanners to Microchips of Various Frequencies Implanted in Dogs and Cats." Journal of the American Veterinary Medical Association233.11 (2008): 1729-735. American Veterinary Medical Association. Web. 19 Mar. 2017. http://avmajournals.avma.org/doi/abs/10.2460/javma.233.11.1729?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub=pubmed.
"Microchip Adverse Event Reporting Scheme Review from Voluntary to Compulsory Reporting April 2014 through December 2015." N.p., n.d. Web. 19 Mar. 2017. https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/527763/951335-Microchip_report_2015.pdf+.
" Microchipping of Animals." American Veterinary Medical Association, 30 July 2013. Web. 19 Mar. 2017. https://www.avma.org/KB/Resources/Reference/Pages/Microchipping-of-Animals-Backgrounder.aspx?PF=1.
"Microchip Identification." World Small Animal Veterinary Association, n.d. Web. 19 Mar. 2017. http://www.wsava.org/educational/microchip-identification.
#microchip#microchipping pets#microchipping dogs#microchipping cats#dr. jean dodds#hemopet#microchipping animals
12 notes
·
View notes
Text
Telemedicine, virtual health system needs to be regulated: Dr Azra
KARACHI: Amid growing telemedicine and virtual health systems, mainly after the coronavirus pandemic, the Sindh government is going to focus on the technology-driven venture and planning legislation to address the regulation of this sector both to capitalise on its potential and to regulate the new sector, a top official said recently.
The move is part of the provincial government plan of reforms in the health sector which attracted serious attention from local and international players during the Covid-19 challenges, demanding strong measures and quick response in the wake of any crisis-like situation.
Health experts said the establishment of virtual hospitals and telemedicine system emerges as a blessing for patients, especially those who have to travel frequently to see their consultants, wait for hours and face the hassle in availing medical services at clinics and hospitals, saying this facility would save thousands of patients from the inconvenience.
Amid a growing number of initiatives and appreciation from the medical fraternity, the situation has also attracted the attention of the authorities who now bring the innovative idea into the loop to enhance the provincial health system.
“The growth [in telemedicine and virtual health system] is a positive development but needs regulation because there are certain norms and protocols to be followed and ethical considerations, including patient privacy for telemedicine and information being advocated through telehealth so that it aligns itself to scientiñc data and proven scientific information is disseminated through telehealth,” Sindh minister for health Dr Azra Pechuho told Press.
She said that the telehealth and telemedicine were two different areas and the provincial government was determined to facilitate both operators and people who wanted to avail this facility through quality standards.
“Telemedicine is where consultation is directly given to the patient or their caregiver whereas telehealth is where information is shared with a community or specific groups or where direct health personnel are given training on patient care and diseases to enhance their capacity to give healthcare,” said Dr Pechuho.
The growing trend around the world and the opportunity created by the pandemic encouraged many local operators to come with the innovative idea but only a few have so far met the expectations. The Ehad Virtual Health (EVH) is one of the very few projects of the virtual health system, which has emerged successful.
“We have launched Pakistan’s first and the only virtual health facility in Karachi which is offering nurse-assisted teleconsultation, home lab collection, radiological procedures at patients` bedside at their residence and medicine delivery to them at their doorsteps,` said Dr Anam Daayem, of the EVH.”
So far, she said, around two dozen Covid-19 patients availed the nurse-assisted teleconsultation service of the EVH, where a team of consultants treated bedbound patients at their homes with the help of nurses and paramedics, provided them lab services at their residence and all the medicines, supplies including oxygen and equipment required for therapies were delivered at their doorsteps.”With the help of portable X-ray and ECG machines, these tests are performed at the patient`s residence, all their blood and other secretions` samples are drawn at their homes and results are delivered online,” said Dr Daayem.
“With the help of online gadgets, a trained nurse or paramedic conveys the condition of a patient to a top-notch physician, who prescribes medicines and these medicines and supplies are supplied to patient from Ehad`s pharmacy on the same day at a discounted rate. The government, on the other hand, is determined to regulate the sector which it says `has a future` and the challenges like Covid-19 demand more effective and parallel healthcare system across the country.”
“It definitely has a future because there may be future pandemic where accessibility to healthcare is hampered as seen during the current Covid-19 crises,” said Dr Pechuho. “Therefore the future need for distant healthcare will become the norm and seeing the need for this the health department is currently developing legislation to address the regulation of this sector. We are looking at a hub and scope plan for distant healthcare. Legislation has been put together.”
-MN Report
The post Telemedicine, virtual health system needs to be regulated: Dr Azra appeared first on Medical News Pakistan.
from Search Results for “coronavirus” – Medical News Pakistan https://ift.tt/31pGkwE
0 notes
Link
October 15, 2019 at 08:00AM
When Amy and Steve Unruh decided to adopt a four-year-old child from the Philippines, they anticipated challenges. They understood it would take time, as well as a great deal of love and care, for their family and its newest member to adjust. But they were committed to helping a child in need.
The Unruh’s were blindsided when their adoption application was turned down. The reason, they were told, was that their parenting style was not suitable for an adopted child. “They said it was because we’ve used time-outs with our daughter,” says Amy Unruh, 43, who is a stay-at-home mom in Milton, Florida. During her interview with the adoption agency, she’d explained that, when her biological daughter misbehaves and doesn’t respond to verbal warnings, she is occasionally sent to her room or told to sit quietly in a chair for five minutes. “They told us this was isolating and not appropriate for an adopted child—or for any child,” Unruh says. “We were devastated.”
Both the American Academy of Pediatrics and the American Academy of Child and Adolescent Psychiatry promote time-outs as an effective parenting strategy. Among kids with oppositional defiant disorder or attention deficit/hyperactivity disorder—the two most commonly diagnosed causes of disruptive behavior in children—research has found that time-outs can help correct problem behaviors.
But recently, some prominent child psychologists have raised doubts about the safety and efficacy of time-outs, especially those involving sending a child to their room or otherwise cutting them off from contact with other people.
“The severe punishment and social isolation that is commonly done in the name of time-outs” is harmful, says Dr. Daniel Siegel, a clinical professor of psychiatry at the UCLA School of Medicine. In a 2014 piece he co-wrote for TIME, Siegel highlighted brain-imaging research that found social exclusion and physical pain trigger similar patterns of brain activity. He also wrote that isolating a child in time-out may deny the child’s “profound need for connection” during times of distress. While some varieties of time-out are appropriate—namely, those that are brief and infrequent, those that involve “care and kindness,” and those that do not isolate a child—Siegel says that, in practice, time-outs are often administered inappropriately.
Time-Outs vs. Time-Ins
The adoption agency that rejected the Unruhs’ application recommended that Amy and Steve read Siegel’s book Parenting from the Inside Out. The same agency also advised the Unruhs to explore a method of parenting called Trust-Based Relational Intervention, or TBRI, developed at Texas Christian University. “We advocate and teach caregivers to use time-ins instead of time-outs as a discipline practice with vulnerable children,” says Casey Call, assistant director of the Karyn Purvis Institute of Child Development at TCU.
Unlike a time-out, which traditionally involves sending a child to his room or some other solitary place, a “time-in” involves having a child sit quietly in the same room with a parent. Call says time-ins are an inclusive practice that communicates to the child that “I’m here to help you calm down and we can work this out.” Time-outs, meanwhile, “exclude the child and can convey the message, ‘Figure this out on your own’ or ‘Calm yourself down.’”
After their adoption application was rejected, Unruh and her husband contacted several other adoption agencies. Over and over again, she says, they were directed to explore TBRI and time-ins, and they were discouraged from using time-outs. But there’s little evidence that these strategies are superior.
“We’re currently doing research on whether time-ins work, but to my knowledge there’s virtually no evidence on whether time-ins are effective,” says George Holden, chair of the Department of Psychology at Southern Methodist University. The research to date doesn’t support advice to abandon time-outs. “I think that’s going overboard,” he says. “There’s certainly a fair amount of research literature that shows time-outs can be effective in changing problem behavior.” He also says that time-outs—by allowing parent, as well as child, the chance to calm down—may help worked-up moms and dads avoid shouting, grabbing, or other aggressive forms of discipline.
Other psychologists echo his view. “I think that it is ill-advised for any professional to recommend an intervention that is not supported by evidence while simultaneously banning a parenting tool that is well-supported by research,” says Amy Drayton, an assistant professor and pediatric psychologist at the University of Michigan’s C.S. Mott Children’s Hospital.
Long-term effects of time-outs
For a study of nearly 1,400 families that appeared in the September 2019 issue of the Journal of Developmental & Behavioral Pediatrics, Drayton and colleagues analyzed developmental data on kids beginning around age 3 and continuing up until age 11 or 12. They found that, among families who reported using time-out as a form of discipline, kids were not at increased risk for anxiety, depression, aggression, rule-breaking behaviors, or self-control problems compared to those who came from families that eschewed time-outs. Creativity scores were also the same regardless of whether a family employed time-outs.
“No matter how we sliced or diced or weighted or controlled the data, we found no evidence that using time-outs was associated with bad outcomes,” says Rachel Knight, an assistant professor at the University of Michigan and one of the coauthors on the study.
While there’s a lot of research showing that time-outs can correct problem behaviors, this new study is one of the first to examine its long-term developmental effects. And unlike a lot of the existing research, this new study did not narrowly define what does and does not constitute a time-out; instead it relied on parent’s answers to questions related to their use of time-outs. “We know that when parents report using time-out, their definition of it varies a lot,” Drayton says. For example, a time-out for one family might involve sending a child to his room for 20 minutes, while for another it might involve asking a child to sit in a corner for three minutes. “We wanted to capture that wide range of possibilities.”
This is significant because some critics of time-outs, including Siegel, have argued that the research backing their safety and effectiveness is based on carefully controlled, psychologist-led interventions that don’t resemble the way time-outs are used in the real world. Drayton says her and her colleagues’ findings contradict this argument. While she says that some time-out practices are more effective than others when it comes to correcting a child’s misbehavior, her group’s study did not find that certain time-out strategies are harmful.
“The optimal way to give a time-out is to provide one warning, meaning if the child doesn’t cooperate within five seconds, they’ll go into time-out,” she says. “If kids are used to repeated warnings—the classic nagging until the parent loses it and orders the kid into time-out—it’s not going to be as effective.”
She says it’s also important that a time-out space—whether it’s a bedroom, a chair, or a staircase—is a “pretty boring” location without toys, media, or other forms of entertainment or distraction. (If a child doesn’t mind being in the time-out space, it’s not going to be effective.) Short time-outs—just a few minutes—seem to be just as effective as longer ones. “Give the child enough time to calm down and become quiet,” she advises. Once that happens, “it’s better if the adult decides when the time-out is over, rather than the child.” Also, when the time-out ends, it’s helpful if the parent follows through with the request that led to the time-out in the first place. “So if your child got angry because you told them to pick up their toys, you need to tell them again to pick up after the time-out,” she says.
Finally, it’s important for parents to be consistent about what will or won’t land a child in time-out. It’s also crucial that parents provide a generally loving, warm environment and reward good behavior with hugs, smiles, and verbal acknowledgment, she says.
“I would say parenting is the hardest job on Earth, and you need all the effective tools in your toolbelt,” she says. New and better discipline strategies may one day supplant time-outs. But, according to the latest research, time-outs are safe and often helpful at correcting problem behaviors.
0 notes
Link
On Thursday afternoon, top lawmakers in the Connecticut House of Representatives announced their plan to legalize cannabis for adult use. Speaking at a press conference, General law chair Rep. Michael D’Agostino, Judiciary Committee chair Rep. Steve Stafstrom and Finance, Revenue and Bonding Committee member Rep. Jason Rojas—all Democrats—discussed the details of the legislative process and what Connecticut residents should expect next. Here are the major takeaways.
Live: Connecticut Lawmakers Unveil Legal Weed Legislation
10 U.S. states have legalized cannabis for adult use, but only one state, Vermont, did so through the lawmaking process, rather than a statewide vote. If Connecticut legalizes cannabis this year, it will have done so in the same way. General Law Committee chair Michael D’Agostino commenced Thursday’s process conference with a word on exactly what that process will look like.
D’Agostino said that Connecticut was approaching legalization in three areas: regulation, decriminalization, and monetization. Each of those three areas falls under the purvey of a specific House committee. And each committee will be proposing its own set of bills focused entirely on its area of cognizance. Thus, D’Agostino stressed that lawmakers were at the very beginning of the process. He called the multiple proposals a “a first bid,” with “nothing set in stone.” Once the bills have undergone multiple hearings and revisions to satisfy committee members, they will all be packaged into a single, comprehensive bill for the legislature to consider.
The Judiciary Committee’s Three Bills to Legalize Cannabis in Connecticut
After D’Agostino’s introduction on process, Rep. Steve Stafstrom of the Judiciary Committee spoke on the three bills currently pending in the committee. One bill would legalize possession of up to 1.5 ounces of cannabis to persons at least 21-years-old. It also proves for criminal record erasure and lays out a process for filing for expungement.
A second bill would create new, separate impaired driving rules that apply just to cannabis. Rules would prohibit any consumption of cannabis while driving, whether or not a driver is under the influence of cannabis. They would also prevent passengers from smoking inside a vehicle. Finally, the second bill would set aside funds to train police as “drug recognition experts” to screen suspect drivers.
The Judiciary Committee’s third bill will likely rankle supporters of cannabis legalization. According to Stafstrom, the bill would not require employers in Connecticut to make special accommodations for employees’ use of cannabis.
Finance Committee is Eyeing Tax Structure Based on Massachusetts
While legalization has generated lots of interest on the revenue side, Rep. Jason Rojas explained that the taxation piece of the puzzle would necessarily come later, after the other committees had finalized their legislation.
But Rojas wants to make sure Connecticut isn’t competing with Massachusetts. Lawmakers want residents buying weed in-state, not across the border. So for now, committee lawmakers are eyeing an overall tax rate of about 20 percent. They expect that tax scheme to carry the retail program for two years, at which point they will reconsider the structure. Rojas did say that Connecticut would levy excise and sales taxes, and that local authorities could level additional taxes on businesses. The tax structure will become clearer in April, Rojas said.
Connecticut Will Take “An Aggressive Approach to Equity” in the Cannabis Industry
A major point of Thursday’s press conference was the importance of ensuring equitability and access to the economic benefits of a legal cannabis industry. And in this respect, legalization advocates have made their strongest mark on the draft legislations.
Fielding questions about equity from reporters, D’Agostino said that people designated as “equity applicants” would have a head start on the application process. So cannabis business license applicants who come from communities with historically high arrest and conviction rates for marijuana offenses would be able to submit applications three months ahead of other applicants. During the press conference, committee lawmakers stressed the importance of redressing the past harms of prohibition and criminalization in Connecticut.
Lawmakers Plan to Leverage Existing Medical Cannabis Infrastructure
During the press conference, Rep. D’Agostino spoke very highly of Connecticut’s medical cannabis program. And to get retail cannabis sales up and running as soon as possible, D’Agostino said the state will leverage its already well-regulated medical cannabis infrastructure.
The bills that committee lawmakers are proposing would establish temporary rules to allow medical dispensaries to sell to retail customers. Lawmakers say that dispensaries could start selling cannabis products by the end of the year. But registered medical cannabis patients will have access to more potent products. Once medical dispensaries start selling to retail customers, the state will collect data to help shape how it licenses strictly retail sellers.
But lawmakers couldn’t provide any definitive answers about exactly when Connecticut’s retail industry would be in full swing. Rather, they continued to emphasize that the process was in its initial stages. Expect the legislative process to take time– probably a year at least.
In Connecticut, Still High Hopes for Legalization in 2019
Connecticut decriminalized possession for personal use in 2011. Get caught with less than a half-ounce of cannabis, hash or concentrate, and you’ll simply face a civil penalty of $150 for a first offense. The “weed ticket” doesn’t show up on a criminal record or background check, just like a moving violation.
The next year, in 2012, Connecticut legalized cannabis for medical use. Since then, the state’s medical cannabis program has grown steadily, registering new patients, caregivers and expanding the list of qualifying conditions. Currently, there are more than 30 debilitating conditions that qualify patients for medical cannabis in Connecticut.
Last year, Connecticut came close to legalizing adult-use cannabis. In April 2018, the House Appropriations Committee voted 27-24 to support a legalization measure. While the bill wouldn’t have directly legalized cannabis, it would have directed state agencies to come up with a plan for legalizing and regulating a retail industry. But as activists rallied at the state Capitol in Hartford, lawmakers essentially ran out the clock. Joe Aresimowicz, a former House Speaker, opted not to bring the measure to a full floor vote.
But 2019 feels different, according to legalization advocates. With Democrats controlling both chambers of the state legislature and a governor who has vowed to make cannabis legalization a priority, it’s easy to see why supporters of drug reform are optimistic that this is their year. In Connecticut, the political landscape favors progressive marijuana legislation. But so does the region. Retail weed sales have already begun across the state border in Massachusetts. And both New Jersey and New York are moving inexorably toward a vote on legalization.
The post Breaking: Connecticut Lawmakers Unveil Plan to Legalize Marijuana appeared first on High Times.
The post Breaking: Connecticut Lawmakers Unveil Plan to Legalize Marijuana appeared first on CBD Oil Vape Liquid Spray - Cbd Pain Relief Capsules - Weed Consortium.
from WordPress https://ift.tt/2O8C10c
via IFTTT
0 notes
Text
Legal Weed Resources
Check out... https://legalweed.gq/420/breaking-connecticut-lawmakers-unveil-plan-to-legalize-marijuana/
Breaking: Connecticut Lawmakers Unveil Plan to Legalize Marijuana
On Thursday afternoon, top lawmakers in the Connecticut House of Representatives announced their plan to legalize cannabis for adult use. Speaking at a press conference, General law chair Rep. Michael D’Agostino, Judiciary Committee chair Rep. Steve Stafstrom and Finance, Revenue and Bonding Committee member Rep. Jason Rojas—all Democrats—discussed the details of the legislative process and what Connecticut residents should expect next. Here are the major takeaways.
Live: Connecticut Lawmakers Unveil Legal Weed Legislation
10 U.S. states have legalized cannabis for adult use, but only one state, Vermont, did so through the lawmaking process, rather than a statewide vote. If Connecticut legalizes cannabis this year, it will have done so in the same way. General Law Committee chair Michael D’Agostino commenced Thursday’s process conference with a word on exactly what that process will look like.
D’Agostino said that Connecticut was approaching legalization in three areas: regulation, decriminalization, and monetization. Each of those three areas falls under the purvey of a specific House committee. And each committee will be proposing its own set of bills focused entirely on its area of cognizance. Thus, D’Agostino stressed that lawmakers were at the very beginning of the process. He called the multiple proposals a “a first bid,” with “nothing set in stone.” Once the bills have undergone multiple hearings and revisions to satisfy committee members, they will all be packaged into a single, comprehensive bill for the legislature to consider.
The Judiciary Committee’s Three Bills to Legalize Cannabis in Connecticut
After D’Agostino’s introduction on process, Rep. Steve Stafstrom of the Judiciary Committee spoke on the three bills currently pending in the committee. One bill would legalize possession of up to 1.5 ounces of cannabis to persons at least 21-years-old. It also proves for criminal record erasure and lays out a process for filing for expungement.
A second bill would create new, separate impaired driving rules that apply just to cannabis. Rules would prohibit any consumption of cannabis while driving, whether or not a driver is under the influence of cannabis. They would also prevent passengers from smoking inside a vehicle. Finally, the second bill would set aside funds to train police as “drug recognition experts” to screen suspect drivers.
The Judiciary Committee’s third bill will likely rankle supporters of cannabis legalization. According to Stafstrom, the bill would not require employers in Connecticut to make special accommodations for employees’ use of cannabis.
Finance Committee is Eyeing Tax Structure Based on Massachusetts
While legalization has generated lots of interest on the revenue side, Rep. Jason Rojas explained that the taxation piece of the puzzle would necessarily come later, after the other committees had finalized their legislation.
But Rojas wants to make sure Connecticut isn’t competing with Massachusetts. Lawmakers want residents buying weed in-state, not across the border. So for now, committee lawmakers are eyeing an overall tax rate of about 20 percent. They expect that tax scheme to carry the retail program for two years, at which point they will reconsider the structure. Rojas did say that Connecticut would levy excise and sales taxes, and that local authorities could level additional taxes on businesses. The tax structure will become clearer in April, Rojas said.
Connecticut Will Take “An Aggressive Approach to Equity” in the Cannabis Industry
A major point of Thursday’s press conference was the importance of ensuring equitability and access to the economic benefits of a legal cannabis industry. And in this respect, legalization advocates have made their strongest mark on the draft legislations.
Fielding questions about equity from reporters, D’Agostino said that people designated as “equity applicants” would have a head start on the application process. So cannabis business license applicants who come from communities with historically high arrest and conviction rates for marijuana offenses would be able to submit applications three months ahead of other applicants. During the press conference, committee lawmakers stressed the importance of redressing the past harms of prohibition and criminalization in Connecticut.
Lawmakers Plan to Leverage Existing Medical Cannabis Infrastructure
During the press conference, Rep. D’Agostino spoke very highly of Connecticut’s medical cannabis program. And to get retail cannabis sales up and running as soon as possible, D’Agostino said the state will leverage its already well-regulated medical cannabis infrastructure.
The bills that committee lawmakers are proposing would establish temporary rules to allow medical dispensaries to sell to retail customers. Lawmakers say that dispensaries could start selling cannabis products by the end of the year. But registered medical cannabis patients will have access to more potent products. Once medical dispensaries start selling to retail customers, the state will collect data to help shape how it licenses strictly retail sellers.
But lawmakers couldn’t provide any definitive answers about exactly when Connecticut’s retail industry would be in full swing. Rather, they continued to emphasize that the process was in its initial stages. Expect the legislative process to take time– probably a year at least.
In Connecticut, Still High Hopes for Legalization in 2019
Connecticut decriminalized possession for personal use in 2011. Get caught with less than a half-ounce of cannabis, hash or concentrate, and you’ll simply face a civil penalty of $150 for a first offense. The “weed ticket” doesn’t show up on a criminal record or background check, just like a moving violation.
The next year, in 2012, Connecticut legalized cannabis for medical use. Since then, the state’s medical cannabis program has grown steadily, registering new patients, caregivers and expanding the list of qualifying conditions. Currently, there are more than 30 debilitating conditions that qualify patients for medical cannabis in Connecticut.
Last year, Connecticut came close to legalizing adult-use cannabis. In April 2018, the House Appropriations Committee voted 27-24 to support a legalization measure. While the bill wouldn’t have directly legalized cannabis, it would have directed state agencies to come up with a plan for legalizing and regulating a retail industry. But as activists rallied at the state Capitol in Hartford, lawmakers essentially ran out the clock. Joe Aresimowicz, a former House Speaker, opted not to bring the measure to a full floor vote.
But 2019 feels different, according to legalization advocates. With Democrats controlling both chambers of the state legislature and a governor who has vowed to make cannabis legalization a priority, it’s easy to see why supporters of drug reform are optimistic that this is their year. In Connecticut, the political landscape favors progressive marijuana legislation. But so does the region. Retail weed sales have already begun across the state border in Massachusetts. And both New Jersey and New York are moving inexorably toward a vote on legalization.
The post Breaking: Connecticut Lawmakers Unveil Plan to Legalize Marijuana appeared first on High Times.
0 notes
Link
Being innovative or creative looks like an inherent trait to most of us, doesn’t it? However, if you’ve been one of those lucky ones who had “creativity” as an academic discipline at school, you’d know that it can at least be nurtured. So what happened along the way? Perhaps, like renowned educationalist, Sir Ken Robinson says, “We got educated out of creativity.” And now, we are back to finding ways to use our creative energies to build something of value. How ironical…For those who steered away from the path of innovation and tried to fit into the neatly defined boxes of the world, it’s time to get a real sense of what your talents are and dig deep. Your businesses have created circumstances for you to bring these to the surface. To help innovation officers and wannabe innovators in their task, we’ve put together the best books to inspire you and help your company and workforce stay relevant.Innovation and Entrepreneurship by Peter DruckerIn this classic book published in 1985, Peter F. Drucker “presents innovation and entrepreneurship as a practice and a discipline.” Called the inventor of modern management, Austrian-born American Dr. Drucker’s insights are still highly relevant and many of his predictions did come true. He focuses on the Practice of innovation, Practice of entrepreneurship, and Entrepreneurial strategies. Drucker uses examples to outline systematic innovation and sources of innovative opportunities within and outside of the enterprises. This seminal work, which is a must-read for a budding entrepreneur, includes the dos and don’ts of innovation, measurement of innovation performance, entrepreneurial policies, structures, and strategies.The Medici Effect: What Elephants and Epidemics Can Teach Us about Innovation by Frans JohanssonThe book hopes to makes you realize that true innovation comes from beyond your realm of expertise. Frans Johansson, a Swedish-American entrepreneur, introduces the concept of “intersection of ideas,” which results in path-breaking innovations. This is the key takeaway from this book published by Harvard Business School Press in 2004. He believes diverse teams with an array of perspectives should collaborate to bring ideas from various fields to create the Medici Effect. Johansson has driven home the point with a lot of success stories to make the narrative quite interesting. This is what The Washington Post said about this well-received book: Johansson has “written a book dozens of business school professors meant to write, but couldn’t.” High praise indeed.Running Lean: Iterate from Plan A to a Plan That Works by Ash MauryaLeanStack Founder and creator of the Lean Canvas, Ash Maurya, tells you how startups can find the product/market fit by following a systematic process based on innovative approaches based on innovative approaches such as Lean Startup and Bootstrapping. Some of the principles in the book include a plan for systematic learning, listening to customers, testing to learn, de-risking your business model, and canvassing your plan. Although he doesn’t directly talk about innovation, he talks about raising the odds of success for entrepreneurial ventures by scrutinizing product ideas. Running Lean is undoubtedly an inspiring book for anyone looking to start a business project or company.The Myths of Innovation by Scott BerkunWith this book, American author and speaker Scott Berkun “methodically and entertainingly dismantles the clichés that surround the process of innovation” as the author of Dreaming in Code, Scott Rosenberg, says. He talks about where ideas come from, the true history of history, why most people don’t like ideas, how great managers make ideas thrive, and the importance of problem finding. Obviously, the books are rife with exciting anecdotes and case studies. He tells you breakthroughs and epiphanies don’t happen overnight; Berkun also tells you how to overcome resistance to ideas, how problems are likely more important than answers, and why the best ideas don’t always win. (Here is a video that might interest you.) He tells you about how ideas can truly change the world, that is, how motivation and initiative with respect to innovation take the world forward.The Ten Faces of Innovation by Tom Kelley and Jonathan LittmanAuthors Kelley and Littman discuss IDEO’s Strategies for beating the devil’s advocate and driving creativity throughout your organization. This 2005 book is an excellent read to understand how corporations can tap into their potential and foster an innovation culture. An easy and enjoyable read, the book describes 10 temporary personas—storyteller, hurdler, experimenter, cross-pollinator, anthropologist, caregiver, set designer, experience architect, director, and collaborator—you can assume to drive 360-degree innovation. Engaging stories and tips on how to deal with damning cynics by donning “suitable” hats make this book an absolute gem.The Innovator’s Dilemma by Clayton M. ChristensenRenowned Harvard Business School Professor Clayton M. Christensen’s theory of disruptive innovation has been called “the most influential business idea of recent years.” In this 1997 book, Christensen studies innovation patterns of big firms to explain why new technologies caused some firms to fail—why great companies seem to be doing everything right but still go wrong. He talks about management being torn between sticking to traditional business practices for sustainable growth in the short-term and capitalizing on disruptive technological changes for long-term growth; it is a battle between entrants and incumbents, between technological progress and market progress. This is a definitive guide for every innovator who needs to understand the ability to innovate and the organizational culture to support it. Clayton Christensen and Michael Raynor followed up by publishing “The Innovator’s Solution,” where they tell companies how to become disruptors themselves using carefully researched and formulated guidelines.The Invisible Advantage: How to Create a Culture of Innovation by Soren KaplanAs the Winner of Best Business Book, International Book Awards, this book tells you how to create a lasting culture of innovation (the invisible advantage) that emphasizes entrepreneurial spirit and free thinking to create sustainable value. Soren Kaplan, a celebrated author, professor, and speaker in the sphere of innovation and business strategy creates an attractively designed pithy book that’s chock-full of practical tips, real-world examples, apt quotes, and highly relevant information. What’s even better is that it comes with a toolkit (video, questionnaire, interview guide, PDF poster, PPT template) to help you get started. So if you are looking to turn great ideas into practical strategies and can’t chew your way through lengthy case studies and philosophical discussions, this is the book for you.Innovation to the Core: A Blueprint for Transforming the Way Your Company Innovates by Peter Skarzynski and Rowan GibsonPeter Skarzynski, Strategos co-founder, and Rowan Gibson, a business strategist, tells you how as a front-line innovator can turn innovation into a core competence. After reading this book, you will know how to “make innovation an enterprise-wide capability that involves the whole organization, rapidly enlarge and enhance your innovation pipeline with breakthrough ideas, systematically innovate across all the components of your business model, dramatically improve the efficiency of your innovation spending, use the power of IT to enable and manage innovation across the enterprise, and put systems and processes in place that make innovation self-sustaining.” So many reasons why managers at every level across industries must read this comprehensive guide, don’t you agree?The Lean Startup: How Constant Innovation Creates Radically Successful Businesses by Eric Ries📷This bestselling book published in 2011 continues to be an invaluable read for aspiring entrepreneurs battling uncertainty every step of the way. Ries, a serial entrepreneur, and author, cites “working forward from the technology instead of working backward from the business results you’re trying to achieve” as the reason for the failure of two startups he worked for. He talks about more learnings from his journey with IMVU. The book is divided into three parts: vision, steer and accelerate. (Here is a quick video summary of the book.)Making Ideas Happen: Overcoming the Obstacles between Vision and Reality by Scott BelskyKnown for Behance (acquired by Adobe), Scott Belsky is an American entrepreneur, investor, and author. In this book published by Penguin in 2012, Belsky talks about techniques and principles to “systematically approach creative organization and productivity.” He has compiled stories and experiences of visionaries, such as Seth Godin and John Maeda, who tell you how you go from generating an idea to its implementation by breaking down each project into its components: Action Steps, References, and Backburner items. It is a fantastic buy for creative people who need help sorting tasks, figuring out whether they are dreamers, doers, or incrementalists, and deciding how much energy to invest to execute their ideas.Let’s call them more-than-honorable mentions in this list. Our other must-reads include:ThinkertoysA Handbook of Creative-Thinking Techniques by Michael Michalko is a fun book on how to come up with unique ideas and channelize them in your business and personal lives. Michalko tells you how to amp up creativity intuitively and indulge in some practical brainstorming through interesting exercises, analogies, and stories.Open Innovation: Researching a New Paradigm Henry Chesbrough, Wim Vanhaverbeke, and Joe West examine the theory, applicability, implications, potential, and IP issues of open innovation.A Guide to Open Innovation and Crowdsourcing: Advice From Leading ExpertsPaul Sloane’s book “explains how to use the power of ideas and people outside your organization to turbocharge your innovation.” Practitioners and thought leaders in the innovation space tell you how to co-create with customers, manage virtual teams, and deal with IP issues.Brain RulesDr. John Medina writes about the 12 Principles for Surviving and Thriving at Work, Home, and School. The sections in this wonderful book are survival, exercise, sleep, wiring, stress, attention, memory, sensory integration, vision, music, gender, and exploration.Currently I am reading "The Lean Startup". What is favourite book from the list?Source: Top 10 must-read books on innovation
0 notes
Text
Announcing the 2018 WEGO Health Awards
https://healthandfitnessrecipes.com/?p=5265
It’s that time of the year again- time to celebrate the online health community!
Here at WEGO Health, we think Patient Leaders are the future of healthcare. We believe that by collaborating with Patient Leaders, listening to their insights and learning from their experience, we can truly help solve some of healthcare’s biggest challenges.
Which is why we love to celebrate all your hard work with the WEGO Health Awards. This awards program strives to recognize and celebrate Patient Leaders across the globe. It is meant to highlight the work you are doing and the impact your making, to thank you for your endless effort and energy and to rally the online health community as a whole!
We encourage you to nominate the Patient Leaders in your life who deserve a moment in the spotlight for their advocacy efforts! Send some love and support to your fellow Patient Leaders by nominating them for a WEGO Health Award. With 16 award categories, there is truly something for everyone!
Want the rundown on all of the award categories? Click here to view the 2018 WEGO Health Award Categories.
Nominate Now!
Creating the WEGO Health Awards
Why do we honor Patient Leaders?
Originally coined the “WEGO Health Activist Awards,” the WEGO Health Awards were created to embody the mission of WEGO Health: To empower Patient Leaders. We connect with countless patient advocates, influencers, and experts who are helping others and transforming healthcare – often without any formal recognition.
Since the WEGO Health Patient Leader Network is centered around these healthcare transformers, we knew it was up to us to celebrate their accomplishments. From this need to celebrate the Leaders who make a difference, the WEGO Health Awards were born.
Since its inception in 2011, the WEGO Health Awards have proven to be one of the best ways to connect the healthcare industry with top patient influencers. The WEGO Health Awards offers a way to introduce new Patient Leaders to the online community and to allow network members the opportunity to recognize and say “thank you” to the leaders they look up to.
Show more
Show less
Frequently Asked Questions
Who should be nominated? Who can win a WEGO Health Award?
Anyone who is an active and leading member of an online community, and making a difference in healthcare, is eligible to be nominated. He or she should provide the community with valuable information and support to make a difference for other patients and caregivers. Nominees for an individual social channel award must have a presence on that particular social channel, of course.
Think about the advocates and influencers you see leading Facebook groups, blogging about their health journey, speaking up and giving insights to healthcare companies, presenting on national stages, and running Twitter chats. Patient Leaders have started non-profits, published podcast episodes, and authored books – there is no shortage of Patient Leaders’ contributions to the world, so let’s recognize as many of them as we can for their talents, contributions, and commitment.
How do I nominate someone?
Go to our WEGO Health Awards nominations page to get started. Tell us whom you want to recognize, where you follow them online, and the award you think they should win. Once you’re finished nominating your favorite Patient Leader, feel free to share that nomination with your community or send a tweet with the hashtag #WEGOHealthAwards. And, be sure to nominate early and often; we want to recognize as many Patient Leaders as possible.
May I nominate myself?
Of course! We hope you’ll reach out to your community and ask them to nominate their favorite members of the online health world, and that includes you; however, you’re more than welcome to nominate yourself as part of the process. Be sure to take a moment and recognize any of the great leaders that help you on a daily basis as well.
I’ve been nominated, but I’m not in the Nominee Directory. How do I get added?
The Nominee Directory was created to showcase all of our fantastic nominees and to give your community members a place to endorse you, so we definitely want to make sure you’ve been added.
As a nominee, you should receive an email, with your unique directory link included, 24-48 hours after your nomination. If you haven’t received this unique link, please email us at [email protected] and we’ll make sure to send the link to create your profile.
In your Nominee Profile, it’s especially important to share your story and your social links because your Nominee Profile will be shared with our panel of judges during the judging phase of the WEGO Health Awards. The more information you add to your Nominee Profile, the better chance you’ll have to stand out.
Show more
Show less
2018 WEGO Health Awards Timeline
Nominations I May-Aug
Help us celebrate the online health community by nominating Patient Leaders for the WEGO Health Awards. With 16 award categories, you’re sure to find the perfect category for everyone!
Endorsements I July-Aug
You can think of endorsements like voting. It allows us to bring a “People’s Choice” aspect into the WEGO Health Awards. The three nominees in each WEGO Health Award category with the highest number of endorsements will automatically become finalists.
Judging I Aug-Sept
The finalists are selected in one of two ways. First, the top three endorsed nominees within an award category automatically move on as a finalist. The subsequent two finalists are selected by our judging panelists. The judging panel is comprised of past award winners, foundations, organizations, award sponsors, and industry experts. Finalists will be selected based on their relevance to that particular award, and the information you provide will help determine their likelihood to win.
Note: A nominee’s community size (number of fans, followers, readers, members, etc.) will not be considered. The nominee is judged based on their content and fit for the award category.
Live Ceremony I October
Last year we had our first every LIVE ceremony! We were honored to meet the winners but the best part was watching the WEGO Health Award winners connect and share in-depth discussions with each other. Our winners reported that the opportunity to meet their fellow award winners in person was the most rewarding part as it sparked inspiration and community! So it’s safe to say, we’ll be flying our winners to another in-person ceremony this year too! Details to come…
Show more
Show less
Get Involved
We’d love to have you nominate all the great Patient Leaders you know–the ones who are working tirelessly on their social channels, speaking engagements, consulting gigs and other platforms.
We urge you to share the WEGO Health Awards with your friends, family, fans, followers, etc. Everyone is welcome to nominate and we want to make sure to recognize all the great leaders out there.
Click Here to Tweet This Message: Recognize patients & companies who are building a patient-centric healthcare with the #WEGOHealthAwards- nominate now!
You’re invited to download a FREE WEGO Health Awards info kit full of tweets, Facebook posts, blogs and graphics to help share the celebration with your community. Download the Patient Leader WEGO Health Awards info kit HERE.
And of course, don’t forget to nominate your favorite Patient Leaders and share the WEGO Health Awards!
Nominate Now!
The post Announcing the 2018 WEGO Health Awards appeared first on WEGO Health.
Credits:
Original Content Source
0 notes
Text
Cheryl Wegener - Transcript 122
Pediatric pulmonary hypertension caregiver, Cheryl Wegener discusses her daughter Madison’s road to a PH diagnosis and the impact living with this rare disease has had on the entire family.
Hi, my name is Cheryl Wegener, and I live in Michigan with my family. My daughter Madison is our Pher.
Madison passed out in her first-grade gym class, and that was our first indication that something was wrong. Prior to that, she was pretty much asymptomatic. We went to a doctor. Even the school nurse, when they called, they said, "Look, you don't even need to pick her up from school, she's good. She was a little freaked out. Her levels are fine, her blood pressure's fine. Did you feed her this morning?" Yes, we fed her. "Okay, you might just want to follow up."
We were new to that community, so we didn't even have a pediatrician that we knew and loved for years, but somebody said, "Okay, go see this guy." And so, we took her, just for a follow up. Everything looked good there, but thankfully he wasn't okay with the fact that the six-and-a-half-year-old passed out. And so, he's like, "You know, let's just do an EKG. We don't do a lot of them here, but let's just try it and just to be sure." And that EKG came back with a couple red flags. And again, he was like, "We don't do a lot of them here. Maybe our leads run a little off, but I'm just not okay telling you ... I want you to see a pediatric cardiologist. If I tell you to make the call, you'll be on a six-month waiting list." He goes, "I'm not okay with that. So, let me make a call, I know a friend."
He made a call. This was on a Thursday, got us in to see her on a Monday. And thankfully, we weren't one of the people that go undiagnosed for years and years and years. We went to see her. We did an echo and she knew exactly what she was looking at. And they come in and they give you, you know the pictures, they're trying to explain what this all is and there's two different versions and neither version is good. And we were basically told to go home, pack your bags, drive to Dallas, which was an hour away, and you're gonna go there for a bunch of tests. There is a team of doctors waiting to meet with you in ICU. And her pressures were probably in the 120s at that point. They couldn't believe that she hadn't turned blue, she hadn't passed out, she hadn't had all the symptoms before this period.
And so, when we did that, we went to Dallas. We were in the hospital 15 days. That was our first introduction to the PH world. It's interesting for me, when I go back and I reread our Caring Bridge page, and you watch our understanding unfold. Nobody came in that first day and said, "Your daughter has a terminal illness." Nobody gave us the severity. They told us, "Stay off the internet." So of course, at three in the morning when you're in the hospital room, you're on the internet, reading stats and hearing the good, the bad, the ugly. And as we journaled about it, I think we knew, the first thing we read, one of the first things, was that Madison wouldn't be able, or should not get pregnant. And we knew that before we knew of the implications of the disease. And I remember writing about that, and how sad I was about that.
And then fast forward a few days, and we learned how much more serious this disease was, and we learned about transplant possibilities and how, what a really serious road this was going to be. And I think as we go back, and you read our journal, you just kind of watch this unfolding of our understanding. Dallas told us that their PH team had recently went on to bigger, better things. So, they used to have a PH specialist, they no longer had a PH specialist. Ironically, what they did have was a doctor that used to work with Dr. Dunbar Ivy. He was on their transplant team. And so, they borrowed him for our ICU case, and he called the shots for us while we were in Dallas. But they also said, "You need a PH specialist and we don't have one."
And so, we're like, "Okay, where are these gods of PH?" And they started naming off places like New York and Colorado of course, and Boston. And they said, "Where are you guys from?" And we said, "We're from Michigan." And they said, "Okay, U of M. There you go." And we had only lived in Texas less than a year, and we were supposed to be here two years plus for my husband's job, and said, "Okay." You get a diagnosis like this, you're supposed to be with friends and family. And so that's where we ended up, was going back home. And so everything kind of worked out the way it was supposed to. From the early diagnosis, from Dr. Ivy's former colleague being there to direct the doctors what to do and what to test, to us getting back to our home base and having that specialist live 30 minutes from where we used to live. That was great.
Since then, I mean it's been a roller coaster. This is a disease that rocks your family to the core. On some days, it's going to bring you together and it's going to tighten your unit and tighten your relationships. And other days, it's just going to shake you and it's going to make you question everything and it's going to cause lots of stress and it's going to cause lots of strife in the relationships. And then other days are just completely normal. We're a family, and we're still a family, still a unit. But we're a family with PH, and some days that makes us dramatically different than other families, and other days we're just a normal family.
Despite the fact that we have a PH team close, when you go to ER, you're not dealing with the PH team. You're dealing with the ER people. And when we were first hospitalized with that, which was about maybe a week, two weeks after she had received her central line, so we were by no means experts on mixing. We were still learning the ropes. We weren't experts on the pump. And when we ended up back in the hospital, it became clear that maybe one person on that floor, knew how to work the pump. We weren't okay with that. And so we started advocating for, "Okay, somebody else needs to know that." And we had a great PH fellow, that really went to bat for not just us, but for the program. Saying, "You know, all these nurses on this floor need to learn how to use the pump." And from there, she started training the ER doctors. And we know, when we go to ER, it's game on. We have to have our game hat on, we need to know the program, we need to know how many clicks does it take to re-prime the pump, when you're moving from a peripheral back to the central line and all of that. You have to know, but you're also kind of doing some teaching at the same time.
Probably our biggest struggle right now, as a family unit, is with the kids. There's the normal sibling jealousy, the sibling fighting, the sibling rivalry. And then add a disease on top and it's that on steroids. So, there's days where I believe Madison is jealous of things that Matthew can do that she can no longer do, or do as well. And there's very often days, where Matthew is jealous of the seemingly amount of attention that Madison receives that he doesn't receive. Which, people are very good. If Madison ends up in the hospital and they're bringing her gifts, they almost always remember to bring him something too. People are conscious of that. But that's definitely, that's a balancing act that we haven't mastered yet. We're still juggling that one.
How do we make both kids feel that they are equally as important? Because they are. But they both have different needs, and they both have different ways of showing those needs and showing those wants, showing those emotions, those frustrations. And right now, Matthew is still young enough where he has the feelings, he has the emotions, he has the fears, but he doesn't necessarily have the words to put those appropriately into words. And so, we're seeing that come out in his actions. And as parents, that's so hard, because on the one hand, you want to discipline, you want to raise this nice, strong young man that doesn't have these behavioral issues. Then on the other hand, you're like, "Dude, I get it. It must suck to be the other kid. It must suck to be the sibling." And there's days where I am so angry and I'm frustrated or I'm sad or I have those emotions too, but I'm an adult. And how does a second grader process some of the same fears and things that I'm having to process as an adult? That's not fair to him, but yet that's not something we can change. So, it's definitely a juggling act.
From day one, we said we weren't going to put her in a bubble and not let her live. So when she, she was going to be a swimmer from early on. She was just a fish. And so it was really hard when we got a central line, maybe four months in to diagnosis. It was like, "Well, what do you mean we can't swim?" And then we heard about these dry suits. And then our doctor's position was kind of "Don't ask, don't tell. You know, we get it." And so we ordered a dry suit. So, she swims. She swims differently than she did. She can't dive, she can't do that, but she still swims. She got in to horseback riding for a while. And so that was a passion and we knew, we just made sure that as soon as you're entering that barn, you have a helmet on, because of the risk of a head injury. And we made that work.
She dabbled in to archery for a year. That became kind of really cool after the Hunger Games, for girls to be in to archery and stuff. And that was pretty cool and so she tried that out for a while and said, "You know, I'm going to try this, see if I like this." So, she tries a lot of different things. And we haven't found the one passion yet. She started piano. She likes choir at school, so we thought, "Maybe this summer we'll do a drama program." Things that she probably wouldn't have tried before PH, she's now willing to try, because it's a new path. And that's important.
I'm Cheryl Wegener, and I'm aware that I'm rare.
Learn more about pulmonary hypertension at phaware365.global. Never miss an episode with the phaware® podcast app. Follow us on facebook, twitter, instagram, youtube & linkedin @phaware #phaware
Listen and View more on the official phaware™ podcast site
0 notes
Text
How I Deal with Seed Putting in As A VC.
5 Leading Threats Of gel.
In Georgetown, Centennial Middle School's Healthy and balanced Container Plan has been competing over Ten Years and also owes its effectiveness to educator management provided through Debbie McClure as well as the Food Ninjas - a group from over 25 students which share in the obligation of cleansing and stocking the snack food cans for each classroom and also the fruit bowl in the office every week. Nobel Laureate Teacher Muhammad Yunus is the dad of both social service and also microcredit, the owner from Grameen Financial institution, as well as of greater than FIFTY various other companies in Bangladesh. We observe usually the practical reason of abuse as 'the smaller wickedness' - as if, for instance, if you torture a person you obtain relevant information that permits you to avoid something even worse coming from occurring. Should you have just about any questions about where along with the best way to work with aimdaroe.xyz, it is possible to e-mail us in our own web site.
The wave from indigenization of psychology in Ghana has actually been actually owned, to a big degree, by the prosperous advancements in the United States by African American psychologists and also to a smaller level results by psycho therapists in South Africa, Zambia, India, Central and also Eastern Europe (such as Croatia, Estonia, and so on) and usually Classical United States (mainly Brazil).
My hope is that business people are motivated to tackle major problems. Yet they fast to beg victimhood, as well as appropriate pan-Africanism for self-centered ends. Find out coming from these co-authors exactly how they worked together on their JAMPIRES photo publication by means of a Comic books Impromptu music, and also join people in producing your personal personalities as well as preparing all of them loosened in involved comics-inspired games.
He aided found the ThoughtWorks in-house legal staff in 2000, as well as has supported in the firm's development coming from an only US-based organisation to a multinational business extending twelve countries. On 26 October 2016, IPATC, in cooperation with the UJ Confucius Principle and the NRF Seat for African Diplomacy and also Foreign Policy at UJ, held a People Conversation on BRICS: The Post BRICS Summit and its own Impact on Africa".
10 Things You Ought to Perform in gel.
Thought and feelings Blister Charity Compilation 2014// Celebration Exclusives// On Sale 22/10/14. These are important to circulating Pan-African expertise and to interacting the wider social featuring metropolitan teams, community leaders, opinion-shapers, as well as students in advertising greater Pan-African awareness.
Leeds Art University's Youthful Creatives program for kids will definitely be actually running complimentary HALF AN HOUR taster treatments for youngsters in between 7 to 18 years of ages, giving a preference of picture and also printmaking in an art school atmosphere. Sat 5th Nov, Movie house of War, Royal Armouries (Second Flooring), 14.50-15.40, free of cost access along with Saturday/Weekend event pass, All Ages, yet feel free to keep in mind: Thought Blister carries out certainly not control panel content.
In many cases this developed into nothing at all, however in a handful of cases this had impressive outcomes for me as well as my group, together with the business owners. Sunday Sixth November Simply - Event Events - Bubs Lounge. Celebration runs from 10 a.m. to 2 p.m.; greatest options for catching as well as interviewing B roll video should be off about 10:30 a.m. with 1:30 p.m. Roughly 1,400 attendees are actually assumed at this year's activity.
This Is Why gel Is So Famous!
Trainees should finish the program in two full time semesters. In between 2011-2015, Big Idea has served 39 web sites, enlisted over 21,500 trainees, interacted 6,800 moms and dads and caregivers via our parent involvement initiatives, delivered greater than 5.3 M trainee and also adult hours from shows and partnered with more than 100 companies to provide top notch computer programming.
This spring, higher and middle institution trainees off Dallas center and senior high schools and also youth development systems worked together to develop the artivism mural to advocate for change and also assess social as well as ethnological justice problems. The South African authorities possesses, consequently, been accused from wide-spread corruption and also refraining enough to guard immigrants.
The celebration additionally will feature music amusement onstage, meals vehicles, exhibitors, on-site registration for Dallas Area from Knowing sessions and also learning treatments, and also free gifts. Sean will certainly be authorizing with Tana Ford in Big Bang Comics, Dublin on Sunday 21st from Nov in association along with Thought and feelings Blister. Having students operate the program has actually been actually the trick making every person experience welcome.
Jacquie Dunk, granny from 2 students at Halton Something to chew on companion university Paul A. Fisher in Burlington, has been managing their Breakfast Pushcart System for recent 4 years. Dallas Area from Understanding is actually a citywide effort to make sure all trainees have accessibility to premium summertime discovering courses to stem summer season discovering loss.
0 notes
Last Seen Blogs

farmasigungoryakut-blog
Farmasi Kazandırır

abanggersang46
Untitled

bella-bellaxoxo-blog
bellaglamfitness

jjunk0ftheheart
Naked Mind
abanggersang46
Untitled