#finasteride for sex
Text
the imane khelif stuff is so crazy because the real reason she is upsetting so many people is because she is a person in the public light who is actually showing that sex is not as binary and biologically determined as terfs/transphobes like to pretend.
like forever the argument has been there are 2 sexes: biological woman (XX, Vagina) and biological man (XY, Penis). but that is not and has never been the case. so now these people have to try to pick apart the things that they THINK make u one biological sex, plato's theory of forms-style, and they can't find a black and white answer and it drives them insane
does testosterone make u a man? does estrogen make u a woman? what about people with PCOS who produce more testosterone? what about men who get their testes removed because of cancer and no longer naturally produce testosterone? what about men going on finasteride? what about people with klinefelter syndrome who have XXY? when we really get down to it, biological sex can become just as fluid as gender sometimes and that is scary to a lot of people
168 notes
·
View notes
Text
I wish non binary hrt was easier to understand. The perfect situation for me would be on t 3 months and off t 3 months
with Finasteride to prevent me from getting anymore facial/ body hair, but I get to keep all the other good stuff, like the energy and sex drive and protection against muscle fatigue and pain. But even with informed consent you still have to pick I think. On or off
156 notes
·
View notes
Text
For some reason even though all the older men on all sides of the family from all angles kept their hair well into their 60s all of my cousins started balding in their 20s. Including me now. I’ve got a consultation to discuss meds for it soon. Idk what hair losing genetics were lying dormant in all these people but they have come out in full force.
Anyways, looks like I’ll probably start taking finasteride soon. I’ll probably be talking about it a bit mostly because there’s very little information about trans men on T going on finasteride so fingers crossed I don’t get my period back. That’s probably the only thing I’m worried about. Some people claim it’s rare, some don’t. Idk. I don’t wanna buy a wig, I know that much.
It can also lower sex drive but frankly as an asexual person I just see that as a fun bonus.
208 notes
·
View notes
Note
Because no one can be normal in your inbox apparently I want to ask a nice question. What's your favorite part of being trans?
my favorite part of my own personal trans experience is that I Can Do Whatever I Want Forever. obviously i live in Society so people won't always react well to that, but when i think of my Self, i get to build a bear my gender and presentation and don't have to give a fuck what society or even other queer and trans people think is "correct" for whatever words i choose to describe myself. i don't have to have any specific traits to be a man or to be genderqueer, i can take as much or as little testosterone as i want, i can take finasteride so i can keep my hair or shave it all off, i can get laser hair removal if i don't want facial hair or use minoxidil if i want more facial hair, i can grow a dick or even have a new one custom made either with silicone or flesh, i can get rid of my vag or keep it, i can do drag whichever way i want, i can fuck whichever consenting adults i want, i can wear a tux or a gown or a shitty old pair of overalls and it's all gender. everything is gender and everything is sex and love and aesthetic and truth and god and friendship and even though life may suck sometimes, i can still Do Whatever I Want With My Meatsuit Forever.
103 notes
·
View notes
Text
need to find the right cocktail of hormones so i can look like a lesbian who looks like a 14 year old boy well into my 40s
probably finasteride? if it kills my sex drive though then whats the goddamn point
17 notes
·
View notes
Note
I've asked so many blogs this so yours is my last resort as the others weren't really able to help. I haven't got on t yet but I want to, but the thing is, I only want to be on it temporarily, just enough to get my voice deep and that's it. I already have more body hair than a cis guy so the voice is all I want from t. But I'm worried it isn't safe to do this? Go on it for a bit then stop, especially after a hysterectomy? Any advice, is this a rare thing bc I feel very alone with my choice.
As far as I know, going on T and then stopping after a bit is generally safe. I'd recommend talking about this with a doctor (specifically an endocrinologist) because they'll be able to discuss your specific body & any potential risks for you.
I don't think a hysterectomy would have any impact on this? If you get your ovaries removed you are generally prescribed some kind of sex hormone if you aren't already on one, since lacking a dominant sex hormone can cause issues (the same goes for testicles). But that can be T or E, and I haven't heard anything that would suggest that there would be a problem going on one and then switching to the other? Again, best to talk to a doctor about the specifics for you.
If you haven't read up on it already, you should look into DHT blockers, which would prevent bottom growth/hair growth (or loss) on T (here's a reddit post of someone who went on T and finasteride). From what I've read, it might slow down the timeline of your voice lowering, but it will still get lower, and you can also do voice training.
52 notes
·
View notes
Text
A man who sexually assaulted a woman who was trying to help him after he claimed abuse by a female partner is now claiming to be a woman. Hell World.
A man who identifies as transgender is standing trial on accusations that he sexually assaulted two women on separate occasions. Adam Graham, 31, now goes by the the name “Isla Bryson” and was referred to by feminine pronouns both in court and in UK media coverage. Graham has been charged with raping the women with “her penis,” according to court documents.
The first alleged assault is said to have happened on September 16, 2016, in Clydebank. Graham reportedly pulled down the woman’s clothing and restrained her, forcibly penetrating her. According to the victim, Graham, being aware of the crime he committed, instructed the woman to “wash bedding” in an effort to destroy the evidence the following day. She also stated that Graham told her “not to disclose to anyone” the details of the assault.
In an attempt to secure her silence, Graham reportedly went on to threaten the victim’s family in order to secure her silence.
Though a pre-recorded statement, the victim gave testimony to the court noting that she had met Graham on dating app Badoo in July of 2016. After establishing rapport, Graham claimed he was being abused by a female partner. Concerned for his safety and wellbeing, the victim offered Graham shelter at her mother’s property, where she also lived, until which time he could be moved into a homeless unit.
Graham reportedly began to show dramatic swings in behavior while staying at the property, screaming at a young boy the victim had been caring for. After a few weeks, he was moved to a homeless unit, but the two continued to see each other, with Graham staying over on Friday nights.
According to the Clydebank Post, on the night of the assault, Graham entered the bedroom where she had been preparing for bed and locked the door. At first, the victim thought Graham was cuddling her, but said “everything felt weird and wrong.”
Graham then pulled the woman’s pajamas down and raped her despite her vocal protests. The assault only stopped when the victim’s mother turned on the hallway light outside of the bedroom.
Three years later, on June 27, 2019, Graham is said to have assaulted a second woman at an apartment in Glasgow.
After having engaged in consensual sexual activity, the victim states, Graham became sexually violent and assaulted her. The court heard that Graham allegedly bit the victim, lay on top of her and restrained her, and went on to rape the woman “to her injury.”
An assault charge states that Graham additionally punched the woman the next day.
Defense advocate Edward Targowski told the High Court in Glasgow his client was pleading not guilty to all charges and was lodging a special defense of consent to two, as reported by The Scottish Sun.
A letter from Graham’s family doctor was presented in court as evidence of his transgender status. Dated August 5, 2022, the document stated Graham was “currently receiving the maximum recommended doses of Spironolactone and Finasteride” with a hormone prescription provided by Glasgow’s specialist sexual health service Sandyford Clinic.
Graham’s trial is expected to continue for at least five days more, and, if convicted, it is anticipated that he may be housed in a correctional facility for women.
Currently in Scotland, a serial child sex offender who identifies as transgender is being held at a women’s prison, as is a disturbed male killer who now demands to be treated like a female infant.
Earlier this week, it came to light earlier that a serial rapist who targeted women in changing rooms and restrooms had begun identifying as transgender and is seeking a transfer to a women’s prison.
Last fall, it was revealed that half of Scotland’s prisoners who claim a transgender status began doing so only after they had been convicted of a crime. In response to a Freedom of Information request, the Scottish Prison Service (SPS) confirmed there were 16 trans inmates in Scots prisons, of whom eight began to identify as transgender while “being cared for in custody following their remand or conviction for their current offence”.
However, the SPS said it was unable to disclose whether or not there were allegations of sexual misconduct involving the trans-identifying male prisoners due to the cost that would be involved in providing the information.
Scotland recently attempted to pass controversial amendments to the Gender Recognition Act which would streamline the process of altering sex markers on legal documents. Notably, an amendment to the bill which would have prohibited anyone convicted of a sexual offense from changing their legal sex was rejected.
Yet the final outcome of Scotland’s proposed Gender Recognition Reform Bill currently hangs in limbo. On January 17 and for the first time in the United Kingdom’s history, Westminster chose to invoke a Section 35 Orderto block the bill from obtaining Royal Assent.
Under Section 35 of the Scotland Act 1998, Secretary of State for Scotland Alister Jack can prevent a Holyrood bill from becoming a law if it is believed that the legislation would have an “adverse effect” on the application of laws reserved to Westminster.
By Genevieve Gluck Genevieve is the Co-Founder of Reduxx, and the outlet's Chief Investigative Journalist with a focused interest in pornography, sexual predators, and fetish subcultures. She is the creator of the podcast Women's Voices, which features news commentary and interviews regarding women's rights.
#Scotland#UK#Isla Bryson is Adam Graham#The courts are saying Her Penis#Badoo#men who claim to be used by women to abuse kind women#Scottish Prison Service (SPS)#KeepPrisonsSingleSex
66 notes
·
View notes
Note
Just some advice on hair loss (from someone who's going through a similar situation.) I've found it's really difficult to get all the information together in one place, so here you go.
AMAB baldness is caused by a hormone called dihydrotestosterone (DHT), a form of T. For some reason, hair follicles have a receptor that gets triggered by DHT that tells them to "close up" when DHT is around, constricting at the base. Too much DHT interacting with hair follicles causes them to close all the way, literally snipping hair off at the base. (All hair follicles have this receptor. No one knows why this happens specifically to some people and not others, or why this happens to only some areas of the body and not others.)
Any hair loss medication that does not address DHT is essentially a stopgap for the root problem. Rogaine, minoxidil, etc. are all hair regrowth agents - they stimulate hair growth and health, but they can't prevent or stop the actual root cause that ends with the hair getting snipped.
Finasteride inhibits one of the main enzymes that produces DHT, decreasing DHT levels and thereby letting the hair follicles reopen on their own and grow normally again. But DHT is a hormone that does more than just snip hair, and its removal has an impact on sexual function, gut bacteria (in rare cases causing PFS, gut-bacteria induced depression and sexual dysfunction), muscle mass, and other such things. DHT's removal also raises estrogen levels slightly, causing gynecomastia in rare cases (although I expect that would be a bonus for you anyway.) And, because evolution is a horrible programmer, sex hormones are very important to the motivational system, so DHT's removal results in depression and emotional numbness. (The last one happened to me, and it's why I stopped taking finasteride.)
There are treatments in clinical trials which promise - using similar technologies as the mRNA vaccine - to completely delete the DHT receptor from hair follicles. But those are still several years away and will be patent-encumbered anyway.
Since you are transfem, my advice to you would be: go the full mile and get on E. E decreases T and therefore DHT significantly, and therefore fixes the entire balding situation just by itself. Estrogen has major side effects, of course - but you want E's side effects. It won't cause depression, either.
Keep in mind that hair follicles develop and grow over years, and the closing and opening of the follicles also takes years. Finasteride or estrogen will let all of your hair follicles grow back in, and the ones that have died will eventually get replaced. Eventually. You'll see 40% results in six months, and 80% by two years, but to get to 100% will take ten years.
Good luck to a fellow sufferer.
Thank you! I really hope this vision of being able to recover all the hair in the long run is accurate, as there is a lot of hope to be had in that.
6 notes
·
View notes
Text
Transition Update #63: 7 years on T & hysto retrospective
Hi everyone!! The title says it all. I wanted to include all of my phallo consults in this as well, but a few items are last-minute up in the air, so I'll write a separate post for the phallo consults omnibus.
As always, please don't reblog or screenshot and repost. Links are fine. Writing transition updates over the years has been really good for me and I always hope someone finds them helpful. But at the same time, the larger public is awful about bottom surgeries and I'd rather not subject myself to that ire.
This post has a general content warning for discussions of sex, genitals, body image and body/gender dysphoria.
7 years on T
I stopped doing annual T updates a while ago, because after the first 2-3 years most of the bodily changes are basically the same bodily changes cis men go through as they age. This year I made a point to celebrate 7 years, because that's an absolutely wild number, and I think it's important to acknowledge my T anniversary when it comes around. Testosterone has fundamentally changed my life. I'm pretty sure I wouldn't be here without it. I'm so grateful to be in a place mentally, physically, financially, and temporally that I can continue to access it.
I started taking Finasteride this year bc my hairline is getting a little thin. This is, again, more a factor of being in my later 20s than anything else. I didn't expect it to affect me as much as it did. It was one of the first times I experienced and male body image issue that had nothing to do with being trans. Normally, I'm so grateful to live as a man that most male body image issues don't affect me. I don't care that I'm short or a little round or I have wider hips. I'm so grateful to pass and live full-time as a man that it doesn't register. This one was different, and I'm not quite sure why, but I'm going to try and not obsess over it.
Off and on the last four years, but seriously the last two years, I started working out and lifting. At first, I mostly ran, especially during the height of the lockdown when it was the only safe way to work out. I love running but I always wanted to be strong and see what my body could do. The past two years I've been working with an online trainer and my strength has really improved!! I'm hitting personal bests in the gym and it's stopped feeling like a tedious chore. I'm actually excited to go now. That's an amazing feeling and I'm always really happy when my friends or family call me strong.
Hysto retrospective
It's been 7 months since my hysto back in January. The recovery for that was longer and more difficult than I expected. Being cooped up in the house and feeling really weak and gross, on top of the bottom dysphoria I kept experiencing having to constantly discuss lots of parts I hate having, was really hard on me. I feel like, over the last two months, I've shaken off a lot of the lingering depression from that. All that being said, I've healed very well, and I'm so happy I got my hysto.
One of the worst, dysphoria-inducing nightmares for me was getting pregnant. It was so bad, it prevented me from seriously dating cis men for years. T is not birth control, and even with protection and respectful partners, the fear and anxiety were just too much for me to handle. I knew that once I got my hysto, I'd probably feel more confident dating men, but I didn't realize the extent to which that would be true.
I've felt way more confident to date around and hook up since I got my hysto. I've gone on more dates with cis gay men than I ever have before, and even though they ultimately fizzled out, I have never had that level of dating confidence in my life. It's so, so gender affirming when cis gay men are attracted to me. I always felt like I lost something, being a bisexual man who was too anxious about being trans to participate in any kind of gay male culture in NYC. This is by far the biggest gift my hysto gave me and I'm so happy for it.
8 notes
·
View notes
Text
Me, Myself and Progesterone
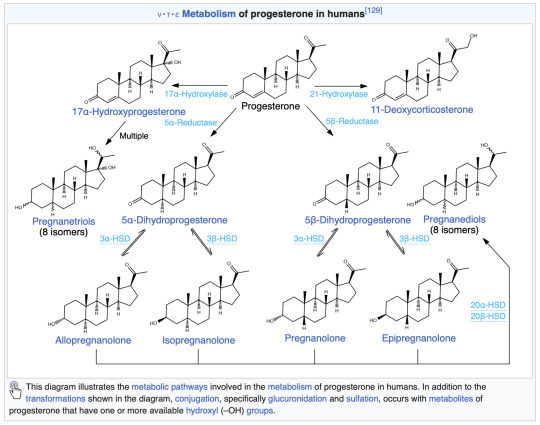
I touched on progesterone (P4) in my last transgender update post. I am not quite sure if progesterone is working in the way I want it to. My biggest annoyance with it is feeling like my brain is on fire just before trying to sleep.
Rewind to late February 2024, for almost three weeks my progesterone dose was doubled to 400 mg of oral, micronised, compounded progesterone – 200 mg twice a day. That’s up from the 200 mg once at night.
I had also ceased finasteride. And finasteride interferes with the progesterone (oral) pathway conversion to neurosteroids such as allopregnanolone. This is because finasteride blocks *most* of the activity (~70%) of the 5-alpha reductase (5AR) enzyme. In turn, reducing levels of allopregnanolone – or at least slowing their conversion to neurosteroids.

My sleep quality has been pretty broken for a while now. Look at those orange blocks. And here I was looking forward to some of the benefits from progesterone. Anxiolytic? Yes please! Sleep improving? Definitely!

Instead I get this whole brain fire thing and feel like I’ve taken an anxiogenic. That got me thinking, brain on fire? Throw in some formication and it’s what feels like a glutamate rebound or surge. Excitotoxicity perhaps?
I’ve experienced similar feelings while withdrawing from pregabalin (decreases glutamate levels) and trusty old diazepam (increases GABA levels). Definitely that same feeling though. It appears that taking what I would consider a small dose (2 mg) of diazepam negates the insomnia pretty well. Even though diazepam isn’t a terribly good choice for sleep. It takes me from being a wired insomniac to sleeping beauty in about an hour.
Another interesting side effect I am seeing a lot more of is dissociation. Ordinarily, I would only experience this while in high stress, high anxiety situations but recently I’m noting it a lot more just doing chores around the house – which is a little concerning.
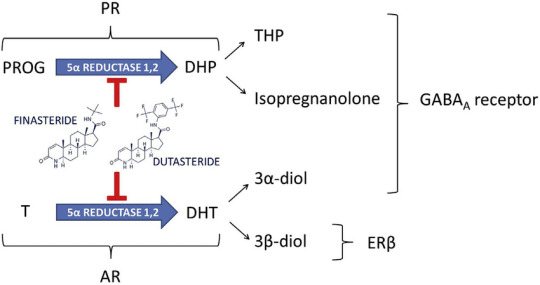
Regardless, it seems that something is messing with my GABAergic system and metabolites of progesterone fit the bill. Armed with my two-thirds of a biomedical science degree I went digging for more information on the metabolites. Up above is an image from my last health blog post. Note the action of finasteride on progesterone – blocking allopregnanolone (THP) and isopregnanolone.
I wonder if moving to a more potent 5AR blocker, such as dutasteride, would reduce the side effects of a higher dose of progesterone? A question for my endocrinologist I suppose. I restarted my finasteride to at least partially block some of the following progesterone metabolites. Let’s look at the metabolites a little closer and how they act.
Allopregnanolone (Tetrahydroprogesterone or THP)
Positive allosteric modulator
9 hours
Pregnanolone
Positive allosteric modulator
1 – 3.5 hours
Isopregnanolone
Negative allosteric modulator
14 hours
Targets allopregnanolone only
Epipregnanolone
Negative allosteric modulator
Half-life unknown
Alright, so a bunch of neurosteroids are doing a bunch of things. A few are being blocked, but also produce negative side effects when they weren’t blocked. Hormones are messy. Where does that leave me? I guess I am left questioning whether I should be taking progesterone at all. At minimum a dose reduction is definitely called for. I will probably return back to 200 mg and see what symptoms, if any, follow.
My search revealed some interesting data with overlap in symptoms shared with premenstrual syndrome (PMS) and premenstrual dysphoric disorder (PMDD) in cisgender women.
PMDD is believed to be caused by fluctuations in gonadal sex hormones or variations in sensitivity to sex hormones.
If sensitivity to level shifts is reason for the negative side effects, then single or even twice daily doses are probably not enough to smooth out the levels of neurosteroids for me, allowing me enter a withdrawal state, perhaps? Brain on fire? This paper offers some great insight into the mechanisms behind it all with some interesting side notes on SSRIs.
Interestingly, SSRIs increase allopregnanolone levels in the brain, rapidly and at low doses, as demonstrated in rodents as well as in patients with depression.
Could this be one of the reasons why I can’t tolerate SSRI/SNRIs? At the very least, it’s some food for thought. Worth noting that the original study has been questioned a little further along in the paper. Let’s circle back to those progesterone levels again. From Wikipedia
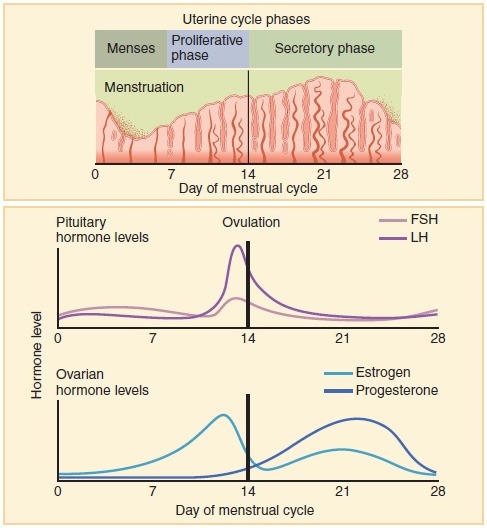
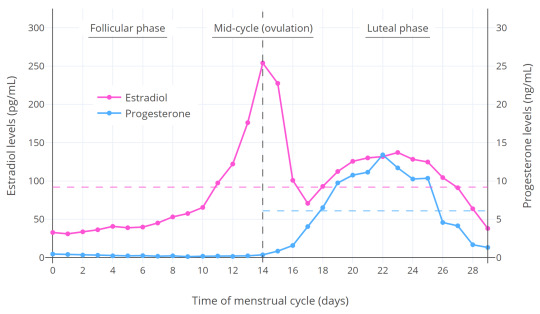
Progesterone levels tend to be less than 2 ng/mL prior to ovulation and greater than 5 ng/mL after ovulation.
What were my most recent levels again? 9.1 nmol/L or should I say 2.6 ng/mL (freedom units). That’s at 200 mg once daily at night, measured in the trough. I really need to ask myself, do I want to have symptoms of PMS/PMDD? Is that even a question that needs to be asked?
Looking at the levels on Table 1 in this paper give an idea where my levels line up. If you factor in the short half-life of most of the metabolites, once daily dosing is probably a bad idea. Ideally, I should look into getting the dose split to 100 mg twice daily.
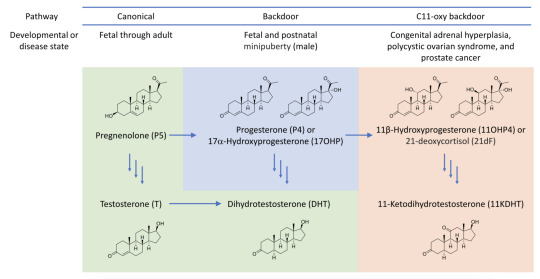
Of course I have to be mindful of negative risk such as the androgen backdoor pathway. This has the potential to generate unwanted androgens like DHT – which will affect the hair on my head. That’s why the finasteride is here to stay until most means of testosterone generation is removed from my system…
It’s not all bad though. Finasteride competes with progesterone for the 5AR enzyme – which results in even less 5AR being available for testosterone -> DHT conversion. Another point worth considering is that progesterone has a positive effect on bone-building cells (osteoblasts). This can help with avoiding or reducing effects of osteoporosis.
Touching on side effects I’ve noticed, Progesterone should increase libido. Which is something I do not want due to past trauma. However, I wonder if the finasteride side effects are at play here. Again, I don’t consider them negative side effects either.
Other oddities I’ve also noticed my facial hair has become darker at the higher progesterone dosing at 400 mg. My upper lip now has dark black hairs, that’s new and unwanted. It might be useful for IPL treatment. But now there’s shadow on my upper lip I never had before. It isn’t just the thinning of skin either. The hairs are black instead of blonde.
One big uncertainty is that I’m not sure what my levels of estradiol will be at the next blood test. Are the 200 mg of pellets doing their job properly? Or did they fail? Does the dose need to be increased?
For now, I’ve been supplementing the implant with the remainder of my 2 mg estradiol pills while the pellets stabilise. One pill gives me ~85 pmol/L in estradiol levels. I’ve only just ran out of those so now I’m adding in some of the estradiol gel (Sandrena branded). These gave ~200 pmol/L estradiol per dose according to my most recent blood tests. In theory with one a day, I should be guaranteed to be in the late follicular phase – regardless of the implant levels.
Anyway, that was one heck of an info dump. I think that sums everything up that has been on my mind lately.
TL;DR
400 mg oral progesterone makes my brain go on fire. Progesterone metabolite levels shifting around are very activating for me. I will now target cisgender progesterone levels in the late follicular phase. Hormones are complicated. One size fits most seems to be at play when it comes to progesterone. Nothing like some trial and error! 🙃
#transgender#transfem#trans#lgbtq#queer#progesterone#estrogen#GAHT#HRT#allopregnanolone#pregabalin#diazepam#GABA#finasteride#PMS#PMDD#GABAergic#brain on fire#fire brain#brainly fires#firely braining
2 notes
·
View notes
Text
I already posted this on Twitter but here's my transition timeline so far!
The first pic is from June 2021. I was openly gender questioning on the internet but it would be in August that my egg finally cracks.
The second pic is on 7/11/2022 after 6 months of finasteride and minoxidil for hair regrowth. I would dissolve estradiol under my tongue for the first time this same day. I continued to identify as nonbinary but I wore a lot of women's clothing.
Third pic was me yesterday! I presently identify as a transgender woman and I've been on blockers and cross sex hormones for six months however I'm pre facial feminization surgery. I'm currently on 2mg sublingual estradiol twice daily, 50mg spironolactone twice daily, and 0.5mg of dutasteride a day. I also microneedle my hairline to further aid hair regrowth. I'm considering going off spiro but going up to 6mg of estradiol a day as sort of a monotherapy, but also reintroducing finasteride on top of the dutasteride in order to totally nuke the conversion of DHT in my scalp.



21 notes
·
View notes
Text
I don't think finasteride has completely killed off my sex drive cos it is come back a lil #yay
4 notes
·
View notes
Text
Teen Hair Care: Male Pattern Baldness
Androgenetic alopecia, another name for male pattern baldness, is a prevalent disorder in which heredity and hormone fluctuations cause hair loss. Usually, it begins with a receding hairline and advances to a crown baldness. Although it affects men more frequently than women, both sexes can be affected.
Preventive and Therapeutic Measures
Early Intervention: Your chances of regrowing hair are better the earlier you begin treatment. If you have noticeable hair loss, speak with a dermatologist to identify the underlying cause and create a customized treatment strategy.
Treatments for Hair Growth: There are a number of treatment options available, such as prescription oral drugs like Finasteride or Propecia that prevent and reverse the shrinkage of hair follicles by blocking the conversion of testosterone into DHT.
Lifestyle Modifications: Changing to a healthier way of living can help stop hair loss. This comprises:
Diet: Consume a well-balanced diet high in vitamins and minerals, especially those that encourage the growth of hair, such as omega-3 fatty acids, vitamin D, and biotin.
Stress Management: To lessen the negative effects of stress on hair health, engage in stress-relieving activities such as yoga, meditation, or deep breathing exercises.
Sleep: To aid in your body's recovery from the day's activities, make sure you get adequate sleep every night.
Hair Care: To reduce damage, use mild hair treatments and refrain from using too much heat styling.
0 notes
Text
Restore Your Confidence with Dr. Atul Kathed’s Hair Loss Treatments

A significantly personal and frequently unpleasant event is hair loss. It can affect one’s confidence and self-esteem; hair loss is not the only issue. The good news is that there are practical remedies out there, and Dr. Atul Kathed is a world authority on Hair Loss Treatments. In this thorough manual, we’ll delve into the realm of Hair Loss Treatments, examine the numerous choices made available by Dr. Atul Kathed, and comprehend how these procedures can help you regain not just your hair but also your confidence.
Identifying Hair Loss
Let’s take a moment to examine the common reasons of hair loss before moving on to the remedies. Numerous variables, including genetics, hormonal changes, illnesses, and way of life choices, can contribute to hair loss. It can affect both sexes and frequently results in baldness or thinning hair.
Underestimating the psychological effects of hair loss is a mistake. Many people who lose their hair report feeling embarrassed, self-conscious, and less confident as a result. This is where finding good Hair Loss Treatments can really help.
The Treatment Methods Adopted by Dr. Atul Kathed for Hair Loss
Dr. Atul Kathed is well known and the Best Dermatologist in Indore known for his skill in hair regrowth and repair. His Hair Loss Treatments are so impactful and supported by science. Following Hair Loss Treatments on a regular basis can give the best results.
In-Depth Consultation: To find out the root cause of hair loss and to suggest the best Hair Loss Treatments, Dr. Atul Kathed starts by performing an in-depth consultation. Suggesting an ideal treatment approach requires an understanding of the underlying causes.
Individualized Approaches: Just as no two people are the same, neither are their hair loss patterns. Each patient’s specific demands are taken into account as Dr. Kathed develops individualized treatment strategies. The strategy is individualized for you and may include sophisticated therapies, drugs, or hair transplant surgery.
Modern Techniques: Dr. Kathed uses cutting-edge methods and technologies for hair restoration. This encompasses cutting-edge surgical methods as well as non-surgical alternatives, all of which are intended to produce outcomes that look natural.
Dr. Atul Kathed Offers Hair Loss Treatments
In order to provide each patient with the most effective treatment option, Dr Kathed who is the Best Dermatologist in Indore offers a variety of Hair Loss Treatments. Key therapies include the following:
Hair Transplantation
Hair transplantation is a surgical treatment that entails removing hair follicles from donor locations and transplanting them to balding areas. This treatment can also be considered the best Hair Loss Treatments
Medical treatments
To encourage hair growth and stop future loss, Dr Kathed may prescribe FDA-approved drugs including minoxidil and finasteride.
Platelet-Rich Plasma (PRP) Therapy
PRP therapy stimulates hair follicles and encourages regeneration by utilizing the patient’s blood plasma, which is rich in growth factors.
Regenera
This is a hair regrowth procedure for hair that uses autologous micro grafts (grafts from self) from the scalp to produce progenitor cells, growth factors and extra cellular factors for hair regeneration.These grafts are processed live in this special machine to produce a fluid sample that is injected into the scalp immediately
It is done as a single session and need not be repeated until a year. It starts showing effects within 3 months and to a maximum of six months.
Success Stories: Boosting Self-Assurance One Strand at a Time
Many people who struggled with hair loss have had their lives completely changed by Dr. Atul Kathed’s skill and they believe Dr. Kathed is one of the Best Dermatologist in Indore. The success tales of improved self-esteem and confidence are motivating. Patients have noted improved overall quality of life in addition to regrown hair.
Conclusion: A Fresh Start for Your Hair and Self-Belief
Although dealing with hair loss can be difficult, knowing that there are effective Hair Loss Treatments out there is comforting. Numerous people have recovered their hair and, more importantly, their self-confidence because of the Best Dermatologist in Indore Dr. Atul Kathed’s commitment to offering individualized and cutting-edge hair loss therapies. Dr. Kathed is there to help you at every stage of your path toward hair restoration if you’re ready to start your own. Bring on a new chapter of self-assurance and confidence as you bid hair loss farewell.
0 notes
Link
0 notes
Text
Unmasking Male Hair Loss: Understanding the Basics
Hair loss, a prevalent and often distressing phenomenon, has a profound impact on the well-being and self-esteem of men around the world. Male pattern baldness, scientifically referred to as androgenetic alopecia, is the most common cause of hair loss in men. While it is a natural part of the aging process, understanding the fundamental mechanisms, contributing factors, and available treatments is crucial for addressing this concern. This article delves into the basics of male hair loss, shedding light on its biological underpinnings, genetic predisposition, psychological impact, and potential management strategies.

The Biology of Hair Growth and Loss:
Hair growth is a dynamic process regulated by a series of intricate biological mechanisms. Hair follicles, embedded within the scalp, undergo cyclic phases of growth, rest, and shedding. This growth cycle consists of three primary stages:Anagen Phase: The active growth phase during which hair follicles produce new hair strands. The duration of this phase determines the maximum length of hair. Catagen Phase: A transitional phase where hair growth slows down, leading to detachment of the hair follicle from the blood supply. Telogen Phase: The resting phase, during which the hair follicle remains dormant before shedding the existing hair strand. Subsequently, the cycle restarts with the growth of new hair.
Genetic Predisposition:
Male pattern baldness is largely driven by genetic factors, making it an inheritable trait. Specific genes inherited from both parents contribute to the sensitivity of hair follicles to dihydrotestosterone (DHT), a derivative of the male hormone testosterone. DHT binds to receptors on hair follicles, triggering a process known as follicular miniaturization. Over time, affected hair follicles produce finer and shorter hair strands until they cease to grow entirely. The pattern of baldness, often characterized by a receding hairline and thinning crown, is determined by the interplay of genes, hormones, and other environmental factors.
Hormonal Influences:
Hormones play a significant role in male hair loss. Testosterone, a male sex hormone, is converted into DHT by the enzyme 5-alpha reductase. Elevated levels of DHT lead to the shrinking of hair follicles and eventual hair loss. However, it's important to note that while DHT is a key contributor, other hormonal imbalances, such as thyroid dysfunction and stress-related cortisol production, can also influence hair growth.
Psychological Impact:
Male hair loss extends beyond its biological implications, often exerting a profound psychological toll on affected individuals. A full head of hair is frequently associated with youth, vitality, and attractiveness. As hair begins to thin, men may experience a range of emotions, including diminished self-esteem, anxiety, and even depression. The psychological impact can extend to social interactions, relationships, and overall quality of life. Acknowledging and addressing these emotional aspects is crucial in managing male hair loss comprehensively.
Available Management Strategies:
Several approaches are available to manage male hair loss, each offering varying degrees of effectiveness and addressing different stages of hair loss:
Medications: FDA-approved medications like minoxidil and finasteride are commonly used to slow down hair loss and promote regrowth. Minoxidil, available as a topical solution, stimulates hair follicles and prolongs the anagen phase. Finasteride, an oral medication, inhibits the production of DHT, thereby reducing follicular miniaturization.
Hair Restoration Procedures: Surgical interventions such as hair transplantation involve the relocation of healthy hair follicles from one area of the scalp to areas with thinning or no hair. Advanced techniques like follicular unit transplantation (FUT) and follicular unit extraction (FUE) offer natural-looking results with minimal scarring.
Lifestyle Modifications: Adopting a healthy lifestyle can contribute to overall hair health. Nutrient-rich diets, regular exercise, stress management, and proper hair care practices promote optimal hair growth.
Conclusion:
In conclusion, male hair loss is a multifaceted issue rooted in genetics, hormones, and complex biological processes. While it is a natural and common occurrence, understanding its fundamental mechanisms, genetic predisposition, hormonal influences, and psychological impact is essential. With advancements in medical science and technology, effective management strategies are available to address male hair loss and promote regrowth. By acknowledging the intricate biology behind hair loss and exploring viable treatment options, men can approach this concern with informed decisions, boost their self-confidence, and embrace their unique appearance.
1 note
·
View note
Last Seen Blogs

eonlinestore-blog
Untitled

tinhattumbles
It's Your Love That Brings Me Home

south-samui-villas
South Samui Villas

deeppersonacowboy
Untitled

iflamesforminho
iFlamesforMinho♥️