#Chediak Higashi syndrome
Note
have you seen any of the grey transient killer whales off the west coast of north america? they’re beautiful! researchers aren’t exactly sure what causes the coloration. it’s hypothesized that chediak-higashi syndrome may be to blame, as it was documented in a captive individual from a related population. beautiful animals though, so far, none of the wild grey calves have survived to adulthood




Sorry for the late response, but wow! Absolutely stunning, I love faded black animals, they look like went through the wash too many times. So sad they have health issues!

#color mutation#killer whale#orcinus orca#orca#cetacean#oddball#Chediak Higashi syndrome#I swear I didn’t see this in my inbox
303 notes
·
View notes
Text

Gods worst friend group !
I'm excited to finally be able to talk about them. Venture down there if you beware
These guys are pretty entwined, so just like in the Twobat backstory, It'll just be one big thing. BIIIIIGGG thing, sorry
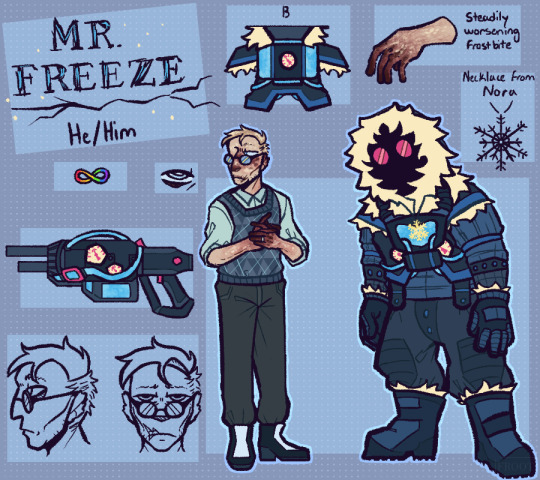
Viktor Fries was born in Denmark, an only child to two very loving parents. He'd always had a love for the cold, which grew into a love for winter, which grew into a love for cryogenics. His parents couldn't get him enough books or research papers written about the subject, so his eventual decision to pursue it in higher education came as no surprise. At the time, Gotham University and WayneTech were the leading institutions in cryogenic research, so Viktor packed his bags and ventured off to America.
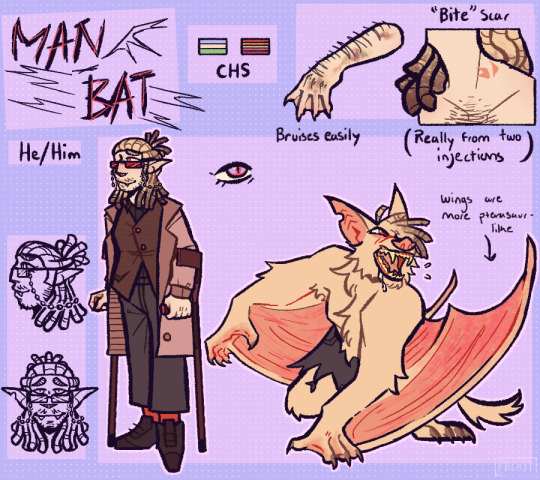
Kirk Langstrom was born a sickly little baby at Gotham General. He was born with Chediak-Higashi syndrome, which not only caused his albinism, but made Kirk very prone to bacterial infections, especially when he was younger. It would also cause motor issues as Kirk aged, resulting in the need of mobility aids like canes or a wheelchair. As a child, Kirk was teased for his appearance, likened to a vampire - or, on one occasion, an albino bat another kid had found and presented to him. Instead of being offended, this moment was what kickstarted Kirk's love for bats, and eventual pursual of chiropterology.
And for Hugo Strange....well, no one really knows where he came from.
The three met when they were all in college, and they became friends almost instantly. They were three smart outcasts who had little to no real friends before this, so naturally they latched onto one another. Hugo a little more than the other two, but I'll get into that.
For the time they were in college, they were good for each other! But as most things go, they drifted a bit after college ended. Viktor by now had fallen in love with Nora and gotten his job at WayneTech, and Kirk had gotten the opportunity to take a research trip to study Bracken Cave (which is where he'd meet his eventual wife, Francine). This left Hugo mostly to his own devices, which he put towards his career at Arkham Asylum and eventually becoming the head of it.
When Kirk eventually returned from his trip, they reconnected with one another. Now here's where I'm gonna talk individually about what happened to Fuck These Guys Up.
Chronologically, Nora getting sick and Fries' accident is what happens first. When Nora started getting really sick, Viktor and her had no idea what it really was, only that it had the potential to kill her if they didn't find a treatment. Viktor's desperation to find it would eventually lead him to Hugo, who agreed to assist Viktor in his research. When Viktor and Nora mutually decided to freeze her to give Viktor more time, Hugo allowed them to build the machine that would freeze her in an abandoned room in the basement of Arkham (which Hugo was using for his own experiments).
Viktor panicked during the process of Nora freezing, and went to turn the machine off in the middle of it, not fully thinking through what he was doing. It caused the machine to malfunction and the chamber (with Nora in it) to explode outward, releasing everything that had been meant to cryogenically preserve Nora out into the room. The injuries and exposure to chemicals should have killed them both, but the temperatures (and medical assistance) managed to preserve the both of them, though it left Viktor as a living but slowly rotting corpse, who is both being killed by the cold and needs it to keep living in whatever state he's in now.
Hugo was actually the one to find the both of them. Though he had personally never cared for Nora, he followed the plan she and Viktor had laid out, making a new chamber to preserve her while he had a suit specially made for Viktor in order to keep him alive. With a tracker installed inside of it so Hugo could know where he was at any time.
This is probably a good time to cut and explain what's wrong with Hugo. He is...insanely devoted to both Kirk and Viktor. They were both his first friends and he loves them very much and he will Keep Them at Any Cost.
So after Viktor awoke, and realized that Nora had been preserved (even though part of him didn't want that anymore), Hugo instructed him to begin working on a cure for her. Hugo couldn't care less if she died he'd get Viktor to himself then, but Viktor had grown dangerously depressed after the accident and the thought of one day being reunited with a cured Nora was the only thing motivating him to stay alive.
Because Nora's chamber is in the basement of Arkham Asylum, Hugo has control of when and for how long Viktor can visit her. If he doesn't make sufficient progress on her cure, he isn't allowed in.
Now, onto Kirk. He had no idea that was all happening, as their contact with one another had been limited, even after reconnecting. One day, though, Kirk had mentioned his interest in changing his current study to focus on his condition, CHS, instead of his bats. Mostly because he was worried about progressing into the accelerated phase, as most people with CHS do. But Hugo suggested instead that he could figure out some sort of treatment for Kirk - and don't worry, you can just go back to your bats! I promise it'll work; in fact, it'll have you feeling like Batman!
So Kirk, suffering from chronic pain and various disabling motor issues, agreed happily. He visited Hugo's lab when the "treatment" was finished and received two injections in the neck, which turned into those two scars. When it didn't work after a couple of days, Kirk was disappointed, and was ready to tell Hugo that he needed to try something else when something...happened.
Kirk blacked out for a couple of hours and woke up shirtless, covered in blood in an empty alleyway. And, strangest of all, he wasn't in pain.
And this kept happening. Every couple of nights he would black out and return home bloody. He attempted to hide this from his wife, but something like that can't stay under wraps forever, so when she found out she urged him to talk to Hugo and figure out what the hell that "treatment" did.
So he did (rather angrily, of course). Hugo would explain that the treatment was actually an experimental chemical he'd developed to be able to turn humans into animals, specially developed for Kirk to turn "at will" instead of being stuck like that permanently. Because of Hugo choosing a vampire bat as the animal for the specific "treatment" developed for Kirk, he would need to feed on blood while in bat-form, thus the reason he was bloody every time he awoke from his blackouts.
There was only one bonus to the transformation. The concoction was, actually, a sort of cure. The bat form didn't have the same chronic pain or issues that Kirk's normal body did. But it came at the cost of being a mindless, bloodthirsty monster.
All he needed to do, Hugo said, was figure out how to become the bat instead of letting it take over, and then he'd practically be the perfect creature!
He would have to keep coming to Hugo for regular injections, though.
Kirk initially, obviously, refused - he wasn't a monster, and he didn't want to hurt anyone or anything just to help himself. But he kept thinking about it. And thinking about it. Could he really tame the bat, and live as something powerful and strong? Something he'd never been?
It weighed on his mind so much that he inevitably returned to Hugo, just to try it. What he didn't know at the time was that the injections were purposefully addictive, growing worse and worse the more he returns to take them.
Hugo Strange friend of the year everybody
#hugo loves his besties. they want to crush him into a fine paste#frootverse#hugo strange#viktor fries#mr freeze#kirk langstrom#man bat#batman#rogues gallery#my art#rogue design
265 notes
·
View notes
Text
Oral Pathology - Module 1 - AIIMS/PGI
Diagnosis = Floating teethSevere bone loss leads to loss of bone support of teeth – giving the appearance of floating teeth A young pt with a growing lesion on one side of the tongue and lip is suggestive of = Lymphangioma – a type of benign tumour composed of abnormal lymphatic vessels.Dohle bodies is seen in Chediak Higashi Syndrome Identify the image – Squamous Cell CarcinomaThe hallmark of…

View On WordPress
0 notes
Text
Going through questions:
Chédiak–Higashi syndrome[1] (CHS) is a rare autosomal recessive disorder that arises from a mutation of a lysosomal trafficking regulator protein,[2] which leads to a decrease in phagocytosis. The decrease in phagocytosis results in recurrent pyogenic infections, albinism, and peripheral neuropathy.
Defect in neutrophil phagosome-lysosome fusion. Pyogenic bacteria = staph, strep, pneumococcus.
Cytotoxic (CD8+) T cells have a PD-1 receptor. Tumor cells can express programmed death ligand-1 (PD-L1), which binds to the PD-1 receptors on cytotoxic T cells. PD-L1 binding to the PD-1 receptor prevents cytotoxic T cells from doing their apoptotic function. This is how cancer cells evade destruction by cytotoxic T cells. The binding of PD-L1 to PD-1 receptor causes T cell exhaustion (inability of the T cell to induce apoptosis). Monoclonal antibodies against PD-1 or PD-L1 prevent PD-L1 interaction with PD-1 receptor, so cancer cells can't evade cytotoxic T cell destruction. Pembrolizumab, nivolizumab = PD-1 antibodies. Atezolizumab = PD-L1 antibody.
T lymphocytes release interferon gamma, which activates macrophages to express MHC-> Th1 differentiation. Viral and bacterial infection result in interferon gamma release from T lymphocytes and NK cells. Interferon Gamma Release Assay (IGRA) tests for latent TB; measures amount of interferon gamma released by T lymphs in response to M. tuberculosis antigens; measures cell-mediated immunity.
Mast cells release tryptase. Tryptase is released by mast cells in anaphylactic reactions. Serum tryptase level is used to diagnose anaphylaxis after the pt is stabilized.
The FceRI IgE on mast cells and basophils bind to the Fc portion of circulating IgE antibodies. Antigen binds to multiple IgEs, which causes aggregation of the FceRI receptors (the IgEs on basophils and mast cells)-> degranulation of histamine and tryptase from basophils and mast cells. Ok so this is more complex than I remember learning. I thought it was the IgEs that aggregate. It's specifically the FceRIs (high affinity IgEs) that aggregate. FceRI receptor on mast cells bind to the circulating IgEs. The the FceRIs aggregate via the antigen and that causes degranulation. Aggregation of the FceRIs activates a tyrosine kinase, which then causes degranulation.
Question 14 of my first immunology quiz has an explanation I want to draw a table from
Etanercept is a TNF-alpha inhibitor it links the Fc portion of human IgG1 to soluble TNF alpha receptors, functioning as a fusion protein. It functions as a decoy receptor, which binds all TNF alpha to keep it from binding to TNF alpha receptors. It treats rheumatoid arthritis when MTX fails to work.
Question 13 also has a figure I want to copy.
Azathioprine and mycophenolate inhibit nucleotide synthesis. This prevents B cells and T cells from proliferating. These are immunosuppresants. Azathioprine-> 6 mercaptopurine-> 6 Thioguanine active metabolites; the Thioguauanine metabolites inhibit purine synthesis. If you can't replicate your DNA/RNA, you can't reproduce, so azathioprine prevents B and T cells from proliferating. Activated T lymphs make IL-2, so less IL-2 will be made as well. Immunoglobulins come from plasma cells, which form from B cells. So azathioprine also reduces immunoglobulins (because azathioprine prevents the T cells from proliferating and you need T cells to activate B cells with the costimulatory response).
I got a question right because I remembered from watching an OnlineMedEd video yesterday that MHC Class I receptor is edited in the endoplasmic reticulum. Part of MHC Class I receptor is beta 2 microglobulin. Cells that are infected break up the pathogen in their cytoplasm and then send pieces of the pathogen (antigens) into the endoplasmic reticulum via the TAP receptor. Inside the ER, antigen is added to MHC Class I, then the MHC Class I-Antigen complex is sent to the cell membrane. TAP = Transporter Associated with Antigen Processing. Mutations in the TAP1 gene, which codes for TAP, lead to inability to bring antigen into the ER. So the pt gets granulomatous skin ulcers and respiratory infections even though lymphocyte and immunoglobulin levels are normal.
Pneumococcal conjugate vaccine (PCV13) induces a more robust immune response than the pneumococcal polysaccharide vaccine (PPSV23) because the conjugate vaccine causes B and T cell recruitment-> memory. The polysaccharide vaccine (PPSV23) doesn't create memory cells. PCV13 has a conjugated protein whereas PPSV23 doesn't. Pneumovax = PPSV23; Prevnar = PCV13.
In the blood vessels, bradykinin relaxes smooth muscle, causing vasodilation. But in smooth muscle that is not in the vasculature, bradykinin actually causes contraction of that non-vascular smooth muscle. So, bradykinin dilates blood vessels but constricts smooth muscle that is not in the blood vessels. That’s why it causes cough–it causes constriction of smooth muscle in the bronchi. Since bradykinin is degraded by ACE, when you inhibit ACE with ACEIs such as lisinopril, you stop breakdown of bradykinin–> increased vasodilation and bronchoconstriction. That’s why ACEIs can cause angioedema and cough.
Bradykinin vasodilates-> angioedema (fluid leaves blood vessels).
Hereditary angioedema is AD; can also be due to ACEIs. In hereditary angioedema, pts lack C1 esterase inhibitor, which is normally involved in break down of bradykinin. So no C1 esterase inhibitor-> increased bradykinin-> angioedema. Dx hereditary angioedema with low serum C1 esterase inhibitor and C4 levels. C1 esterase inhibitor suppresses C1-> no classic complement pathway. Kininogen is converted to bradykinin by kallikrein. C1 esterase inhibitor inhibits kallikrein-> decreased bradykinin. So of course without C1 esterase inhibitor, you have increased kallikrein-> more bradykinin.
In germinal centers in lymph nodes, B cells undergo somatic hypermutation, which is what allows the B cells that can respond to a particular antigen to proliferate. Somatic hypermutation = immunoglobulin mutation.
Serum sickness = type III hypersensitivity reaction (antigen-antibody complexes in tissues); occurs 1 to 2 weeks after being exposed to non-human proteins. Pts present with vasculitis, arthralgia, fever, rash, low C3 and C4. Histologically, you see fibrinoid necrosis and infiltrating neutrophils. Low complement occurs because complement-fixing IgM and IgG are in the immune complexes.
Hyper IgM syndrome = X-linked recessive deficiency of CD40L (CD40 Ligand located in T cells and necessary to interact with CD40R on B cells); causes recurrent pulmonary and sinus infections, GI infection, infection with opportunistic bugs (e.g., cryptosporidium), failure to thrive. Pts have lots of IgM, but little IgG, IgA, and IgE. B cells have trouble class switching (because the CD40L-CD40R interaction is necessary to create the costimulatory signal that causes B cell class switching and proliferation). Class switching occurs when heavy chain constant region genes are spliced out so the B cell can create the isotype of immunoglobulin it needs to make. That doesn't happen in Hyper-IgM syndrome because the CD40R-CD40L initeraction necessary to cause that can't happen when there's deficient DC40L. CD40 deficiency is autosomal recessive form of this disease. If B cells don't class switch, they stay as IgM-secreting cells.
Severe Combined Immunodeficiency (SCID) = autosomal recessive adenosine deaminase (ADA) deficiency. Adenosine deaminase deficiency leads to accumulation of adenosine in T cells and B cells (lymphocytes)-> cellular and humoral immunodeficiency. Tx: gene therapy; hematopoietic stem cell transplant. X-linked SCID is more commone than ADA deficiency. No lymphocytes-> bacterial, viral, and fungal infections.
Henoch-Schonlein Purpura (HSP) = small vessel leukocytoclastic angiitis + deposition of IgA-C3 complexes in skin and GI tract. It's a hypersensitivity reaction related to recent infection. Pts have a purpuric rash, arthralgia, abdominal pain. Can lead to acute glomerulonephritis. Occurs in kids.
#immunology#anaphylaxis#IGRA#interferon gamma#chediak higashi#chediak higashi syndrome#allergic reaction#TNF alpha#etanercept#PPSV23#PCV13#pneumococcal vaccine#serum sickness#hyper IgM syndrome#SCID#Henoch Schonlein pupura#HSP#Henoch Schonlein
2 notes
·
View notes
Text
Let us revise all the important concepts about Chediak-Higashi Syndrome, in just 2 minutes. This video is perfect for test preparation. So, grab your notebook and follow along with this video to boost your knowledge and learn efficiently!
Chediak-Higashi Syndrome is a rare, autosomal recessive, immunodeficiency disorder. Other names of Chediak-Higashi Syndrome are Begnez-Cesar Syndrome, “leukocyte anomaly albinism” or “defect in natural killer lymphocytes”.
The responsible gene is mapped to chromosome 1 (1q42.1-q42.2), which is the lysosomal trafficking regulator gene (LYST). Otherwise also known as Chediak- Higashi syndrome gene 1 (CHS-1.)
#medicalstudent#medical education#medicine#medical school#medical study#medical student#pharmacology#immune system#immunology student#immunology#immunity
2 notes
·
View notes
Note
So you uh, read all those responses about your save a fox defense post?
Didn’t have time to read all of them, but I saw some, saw how it made the post blow up with a bunch of people arguing for or against (mostly against from what I saw). I don’t claim to be an expert and I definitely didn’t foresee this blowing up like it did, but let me just clear some things up.
When I talked about Mouse and Valentine, I wanted to rebut the original point about fur farms allegedly not being inherently bad. I wanted to show the negative consequences they have on the foxes, whether it be Chediak-Higashi syndrome like Mouse or gingival hyperplasia like Valentine. A lot of people were arguing that it would’ve been or would be more humane to euthanise them rather that spend a lot of funds and resources into prolonging their lives. Even if that’s the case, that doesn’t take away from my original point of fur farms being bad for the foxes in other ways than being killed for their pelts.
Mouse and Valentine aside, not every fox they rescue from fur farms has health problems like they do. Some are given up because they’ve been rejected by their mothers who won’t nurse them.
It’s one thing to argue that an animal should be euthanised if it’s suffering. It’s another to argue that it should be euthanised when it’s otherwise healthy and can thrive with the proper care. That’s what SaveAFox tried to do with Mouse - they were trying to give her a good quality of life given her weak genes, and ultimately it wasn’t enough. It might not have been the “right” thing to do in the end but I seriously doubt ill intent on their part.
To step away from fur farms, it’s also worth noting that a good number of foxes living there are pet surrenders - people buy foxes from breeders with the intent to keep them as pets, only to realise they are a LOT of work and they give them up. Or sometimes it’s due to changing exotic pet laws or simply unforeseen circumstances. Where do these foxes go now? Do we euthanise them or give them a good quality of life at a rescue like SaveAFox?
You could argue, as @zoologicallyobsessed did, that foxes aren’t a conservation concern and therefore all of this is irrelevant. While it might be true that foxes aren’t endangered, it doesn’t mean that we can’t care about the health and safety of individual animals. Cats and dogs aren’t endangered either, but I don’t see anyone saying that all cats and dogs in shelters should be abandoned or not cared for. I’m sorry if I’m being fallacious here, but I can’t think of any alternative to the problem of abandoned fur farm foxes or pet surrendered foxes other than euthanising them all.
Again, I truly did not mean to set off the powder keg that I did. I ignored a lot of nuance in my original reblog and I’m sorry for that. When I saw that people were reblogging with points of their own, I decided to step back as it became clear that I’m out of my league. I made one emotionally charged response to a post that said something I didn’t agree with. I will still never buy fur, but I’ll leave the animal rights activism to those who know more than I do. Thanks for your ask!
26 notes
·
View notes
Text
Revelations

A/N - This is ‘the talk’ and it takes place a week after Regrets. You can find that on my masterlist. Also, this meets the requirement for the @choicesweeklychallenge. You belong to me can be found in bold.
Disclaimer: Characters belong to PB
Warnings: none? I don’t think even language.
Series/Pairing: Open Heart - Ethan x f!MC (Charley Valentine)
Word count: 4,466
*****Thursday*****
“Has Denver General sent us any more information, or will I just find out when I get there?” June asked.
Consulting his notes, Ethan answered her. “Dr. Morgan said that he would send us the remaining test results as soon as he gets them. He’ll be sending them to all of us, so if you want to discuss the case with any of us we’ll all have the same information.”
June never looked up from the report she was reviewing. “I doubt it will be necessary.”
“Regardless of whether you think it’s a necessity, you will keep me informed of the case.” Ethan reminded her.
“Of course, Ethan.” June said. “If you don’t need me for anything else, I’m going to get ready for my flight?”
“You don’t want to hear about my new patient?” Baz asked her.
June glanced at him. “My flight leaves in less than three hours, so no. At least not right now.” She gathered her files and left saying goodbye to the rest of the team.
“Baz, what is going on with your new patient?” Charley asked.
“Late-onset Chediak-Higashi Syndrome. For me as an immunologist, I find it extremely interesting, especially as the patient is thirty-two and just diagnosed.”
Charley looked between Baz and Ethan. “Is this a team patient?”
“No. This is a patient of Baz’s. We will have a new patient coming in on Monday for which you will be primary.” Ethan held up a folder.
Baz briefed them on his patient, excusing himself when he received a page saying the patient was being admitted.
“And then there were two,” Ethan handed her the folder.
She flipped it open and read through the file. “Twenty-five year old male. Diabetic. Joint pain and muscle weakness.” Charley looked at him. “Do you know what it is and you want me to figure it out?”
Ethan shook his head. “I have a couple of ideas but I don’t know for sure what it is. You should have several ideas right now.”
“The symptoms can be just about anything. You said he gets here on Monday ?”
He nodded. “He’s already been to Mass Kenmore several times. Even though we have sent a release signed by the patient, Terrance hasn’t sent the files to us. So we may start with spinning our wheels testing for things that they have already tested for and eliminated.”
Charley studied the file again. “Did you see the iron levels here? I think the first thing is a liver biopsy?”
“Are you telling me that’s what you are going to do, or asking me if I think that’s the right choice?” Ethan asked her.
Her head snapped up. “That’s what I’m going to order. I’ll even have the order written so the test is run as soon as he’s admitted.” Charley met his eyes. “What?”
Ethan smiled. “There aren’t a lot of doctors who could have figured out to start with that test after reviewing a file for less than fifteen minutes. Let alone a second year resident. So I am impressed.” He reached over and stroked the back of her hand. “You often impress me.”
She turned her hand and laced their fingers. “It’s Thursday.”
“So it is.”
“Last week you texted me and said we would talk on Saturday.”
“Yes. And we decided we’d have dinner at six.”
Charley met his eyes. “You aren’t going to change your mind?”
“We’re meeting at my apartment. I’ll be there. We are long overdue for the talk. And I’m sorry for that.”
Charley smiles. “Will I finally get my chicken?”
“You will not. We’ve made the chicken together,” he held up his hand when she was going to interrupt, “this time, we’ll make something else. You plan the meal.”
“We may have made the chicken together but I never got to try it.”
“I want to see what you come up with. You can create any menu you want. Email me what we need and I’ll go shopping.” Ethan smiled at her.
Charley considered for a minute. “Anything?” When Ethan nodded, she continued, “My grandma had an amazing pot roast recipe. We could roast it in the oven or use a crockpot. It’s always best if it cooks on low in the crockpot, so that would take about seven or so hours. I’ll email you the list, and I guess I’ll be there late morning. I guess we’ll also have lunch together, too. That’s alright, isn’t it Ethan?” She didn’t even wait for his answer before she left the office.
Charley watched the office door to see if he was going to come after her and inform her they would not be spending the entire day together.
Ethan sat at his desk, he smiled as he realized that life would never be boring around Charley Valentine.
*****Saturday*****
Sienna pushed open Charley’s bedroom door. “Are yo-” Sienna stopped mid-sentence. She heard several loud thuds and wanted to ask if Charley was okay, but she did not expect the scene she witnessed. She also didn’t see her roommate. “Charley!”
“I’m here,” Charley called, pushing herself out from under the bed. “I was looking for this shoe. That I can’t wear now. Thank you, Lucy!” The shoe had become a chew toy for their pet.
Lucy, their fennec fox, sat in the middle of Charley’s bed, looking proud of herself.
“Forget the shoe, we understand what happened to it.” Sienna looked around the room. “Was there a bomb? Are you telekinetic? Did your closet and dresser decide to vomit every article of clothing you own into your room?”
“I’m looking for something to wear, and I don’t have anything! I got off at five yesterday, I should have gone shopping!”
Sienna remembered the day a couple weeks ago when Charley got home late clad in someone else’s clothes. Based on her own conversation with a certain someone, Sienna had a pretty good idea who. Now she was frantically trying to find something special to wear. “What’s his name?”
Charley froze. “What’s whose name?”
“Obviously, the guy that you’re spending your day with. The same one you were with when you came home wearing clothes that were way too big for you. So, who is it?”
“No one,” Charley stated. “I’m not spending the day with anyone.”
“Yet you canceled on Bryce and me for today.” Sienna picked up a Columbia t-shirt and a pair of jeans with a rip in the knees. “Here, put these on.” She smiled. “I mean, if you aren’t doing anything special today, it doesn’t matter what you have on.”
Charley looked at the clothes that Sienna tossed on her bed. She had to leave for Ethan’s before Sienna would be leaving to meet Bryce, and she still didn’t know what she was going to wear.
Sienna watched her. “I heard that Dr. Ramsey also has today off. And he did when you had your second day off two weeks ago.”
Charley froze and looked to the door. “Everyone else is working today and they’re gone?”
Sienna nodded and sat down on Charley’s bed. “Uh-huh.”
“You can’t tell anyone.”
“So it wasn’t just the one night when he spent the night here?”
“That day we went to the country club and later I went to his apartment to talk to him? That was the first time, and the night after my hearing was the second. It was also the last time.” Charley sighed. “Then he went to the Amazon so we could ‘reset’ since he would be my director supervisor.” Charley sighed. “Since he’s been back he says we need to stay away from each other, but then he’ll kiss me. Today we’re going to ‘talk.’ We’ve been supposed to talk since right after the softball game, but it kept getting delayed.”
Sienna smirked at her. “You had on his clothes the day you came home.”
Charley's face turned red. “We spent the day together with his dad in Providence. We took his dog for a walk and I fell into a mud puddle.”
“You’ve met his family!”
“His dad. He hadn’t told Alan that he was bringing me with him. Ethan had never taken anyone home with him before, not even Harper Emery.”
“Dr. Ramsey and Dr. Emery were a thing!” Sienna’s mouth dropped open.
“I don’t know if it’s really common knowledge. Aurora probably knows. I saw the two of them talking once and it seemed intimate. It was the day before they announced the opening on the diagnostics team. I did ask him about it later and he said he likes to keep his private life private, but he did say they had an on-again, off-again thing but it ended permanently when she became chief.” Charley rested her head on her hand. “I probably shouldn’t have said anything. Don’t tell anyone.”
Sienna mimed sealing her lips. “I thought that you and Bryce were kind of together.”
“We hooked up a couple of times but we both agreed to be casual.”
“And with Ramsey, you don’t want casual?”
“I don’t.” Charley chewed on her lip. “Sienna, I’m terrified about today. I know that everything is going to change.”
“Well then, let’s get you ready.” Sienna picked up the t-shirt and jeans. “This probably won’t do; we’ll find something else.”
Charley was just getting ready to leave when her phone rang. She looked at the caller id and sighed. “If you’re calling to cancel-” she started.
“I’m not,” she heard his rich baritone as well as a smile in his voice. “I had to go to the hospital to pick up something. If you haven’t left yet you can ride with me. I’m outside your building.”
“I’ll be down in a minute.” Charley disconnected, smiling.
Soon they were in his apartment. She kicked off her shoes at the door and stood there when he walked further into the apartment. He got half way through the living room when he realized she wasn’t with him. He turned to find her at the door. “If we want to make this pot roast we need to go to the kitchen.”
Charley gave a nervous laugh and stepped away from the door. She tossed her purse on the couch as they walked into the kitchen. They washed their hands and Ethan pulled his crockpot out of the pantry while Charley pulled the roast out of the refrigerator. She saw the printout from her email with the image of her grandma’s recipe. Ethan gathered the rest of the ingredients while Charley brewed a pot of coffee.
“Why the crockpot instead of a roasting pan in the oven? I saw the recipe had directions for both with cooking times for either low or high in the slow cooker.”
“It tastes better and is more tender.”
Ethan smirked. “It does not. And we need to use the Dutch oven even if it’s just to brown the roast.”
“Maybe it doesn’t do a lot for the taste, but it is more tender.” Charley watched as the coffee finished brewing, standing with her back to him. “It takes longer to cook in the slow cooker on low and I wanted to spend more time with you.” She gave a short laugh. “Funnily enough, now that I’m here, I’m nervous.”
“Why?”
She turned to face him. “I think that today may change everything, and I’m hopeful but I’m also scared. I’ve been wanting to sit down with you away from the hospital with just the two of us for so long, but now that we’re actually going to do that...” She bit her lip.
“Now you understand why I’ve been putting it off. But I’ve done a lot of thinking. And I talked to Naveen. We are long overdue. Today will change everything but we will be in agreement with it, I think.”
Charley nodded. Ethan turned back to the counter. “Let’s get this set for dinner, fix lunch, and talk.”
Charley browned the roast in the Dutch oven while Ethan chopped the vegetables and herbs. Once the roast was in the crockpot, Charley cooked the onion. Once they started to soften, they added the rest of the ingredients, including the coffee. “Why coffee?” Ethan asked.
Charley smiled, watching the mixture simmer. “Is this a quiz, same as ‘why neat’ that first night at Donahue’s?”
“Genuine curiosity. As much as I love coffee, I’ve never had pot roast cooked in coffee. I found the recipe interesting.”
“It helps to tenderize the meat and gives the gravy a richer flavor.”
Once the gravy and onion mixture was cooked, Ethan poured it over the meat and set the timer. While Charley washed the accumulated dishes, Ethan fixed salads for lunch. They took their plates to the living room and sat side-by-side on his sofa.
“You talked to Naveen about us.” When he nodded, she continued, “I talked to Sienna.”
They fell into a silence while they ate. Charley glanced at him every so often.
He pushed the last piece of lettuce around on his plate before finally setting the plate on the coffee table. He turned to her; she mimicked his moves and faced him.
“Ethan, I’ve said for a while that a relationship with you is an easy decision for me. It’s what I want. I think that we could be good together, amazing even.”
Ethan nodded. “I know. You aren’t the problem, I am. I want to be able to push you to be the best doctor you can be.”
“You can do that professionally, regardless of any personal relationship we have. I can take criticism from Dr. Ramsey and know that it isn’t coming from Ethan.”
“You’re assuming that I can also have that division.”
That got Charley’s attention. “You’re Ethan Freakin’ Ramsey. You can do anything you try to. If you want to make the distinction you will. And if you cross the line, I’ll let you know.”
“Another problem-”
Charley put her hand on his arm. “If you just want to list a lot of potential possible problems, why are we even having a discussion? Earlier you said that today would change everything and you thought we’d be in agreement.” She folded her arms across her chest and focused on a picture hanging on the wall. “If you thought that I’d change my mind about us, you’re wrong. If you thought you could list all the reasons why we can’t be together and why you won’t be with me, I was right to be nervous about this. If that’s-”
Ethan reached over and grabbed her chin, forcing her to face him. “What I want to do is identify the obstacles or potential obstacles we face so we are both aware of them, and to decide how we need to handle them in the future.” He wiped a tear out of her eye. “Because in case you haven’t figured it out yet, I very much do want to be with you.”
Charley grabbed his hand and kissed his palm before lacing their fingers together. She smiled at him. “I’m sorry for my outburst. Continue, please.”
“Another problem is the board. They don’t like interoffice romances. Naveen seems to think this won’t be an issue. He seems to think that as long as it isn’t impacting the care of the patients, or the bottom line of the hospital, they wouldn’t care, nor would they even need to be aware. I disagree with him on this. I think the board makes it their business to know what goes on in the hospital.”
Charley interrupted again. “I know that there are married couples at the hospital. Was it a problem when you and Harper were together?” Ethan drew in a deep breath when she asked that. “If you don’t want to answer that you don’t have to.”
“I will. It was not a problem and the board did not have an issue with it when she was head of neurosurgery and I was a fellow on the diagnostics team. If our relationship would have continued when she was chief or if I had been a surgeon, it would have been a problem. Any other couples at Edenbrook do not work in the same area, and one member of the couple is not another’s supervisor.”
Ethan continued, “I don’t want anyone to think that you got the position on my team because of our relationship. I don’t want anyone to have any doubt about that. You earned it.”
Charley nodded. “I did earn it. You weren’t even the one who put me on the team. Naveen did.”
Ethan agreed that while that was true, many people at the hospital could have thought that he asked Naveen to do that.
“If anyone has doubts, I graduated at the top of my class at Columbia. Not near, I was ranked first. In fact if anyone had ranked all med school graduates my year from around the country, I’d probably be in the top fifty.”
Ethan laughed. “Someone did. And you are higher than that. You are somewhere in the top twenty. I’m not going to narrow it down more than that for you.”
“Based on that, I think I earned the right to be on the team. Not to mention helping to cure Naveen last year. Our relationship had nothing to do with it. Well except for the fact you inspired me to go to med school in the first place. And I wanted to work with you, which is why I came to Edenbrook.”
“We probably don’t want to advertise our personal relationship at work. The hospital has a wonderful gossip network and we’ll need to be careful. That being said it probably won’t be long before everyone knows about us.”
“That sounds okay. But some people will know. I told Sienna and you told Naveen. My roommates will know I’m seeing someone, and will make it their mission to find out who.” Charley wasn’t sure if she should mention the next part, but figured she might as well. “June does, or she thinks she does. At least that was what she implied the day I caught her with my personnelle file.”
Ethan froze. “She had your file?”
Charley nodded. “She said that she reads the files for everyone she works with. She tried to tell me you asked her to get it for you, but I knew you wouldn’t have.”
“I’ll deal with her when she gets back from Denver. Your roommates and Naveen are fine.”
“If my roommates know Bryce will also know; and if Aurora does, Harper might.” Charley looked up at him. “Can we talk about Harper?”
“I thought we already had.”
“You ended things when she became chief. If she wouldn’t have, would you still be together, do you think?”
“We would not. We were together because it was mutually beneficial to the both of us. But we were never going to last.”
She smirked at him. “By ‘mutually beneficial’ do you mean it was convenient and the sex was good?”
“Yes.” Ethan said. “But then last year something happened that I knew would never lead Harper and I together again.” When Charley tipped her head to show she was interested in his answer, he continued. “Last year, an intern showed up and turned my life inside out. And I can’t get her out of my head.”
Charley started to move towards him, and he stopped her. “What about the scalpel jockey?”
Charley lips twitched. “His name is Bryce.”
“I’m aware, and you didn’t answer the question.”
“We hooked up twice, once at our housewarming party and again once after we were at Donahue’s. We almost did the night we researched treating Mrs. Martinez, but you’d already kissed me in Miami. I wasn’t interested in anyone else at that point.” She looked at the ground before meeting his eyes. “Bryce is a friend and a good one. I trust him. I also know if I ever did want a relationship with him, I’d have that choice. I don’t, and Bryce respects that.”
“As long as he knows that you belong to me.” Ethan pulled her onto his lap and wrapped his arms around her, kissing her.
“And you belong to me!” Charley shifted slightly on his lap and felt his hardness under her thigh. “We could continue this in the bedroom.”
“A very good idea.” As Ethan stood and lifted her, she wrapped her legs around his waist as he carried her into the bedroom.
Several hours later, they were laying with their legs tangled together, voices soft in the quiet room when an alarm on her phone beeped.
“Somewhere you need to be?” He kissed the top of her head.
She pushed herself up. “Actually, yes. The kitchen. I need to start the vegetables.”
He walked over to his closet and pulled out a robe that on him would reach mid-thigh. He tossed it to her, before grabbing another for himself. This one hit him at mid-calf. “You could have this one if you wanted.” She indicated the robe she hadn’t yet tied. It fell below her knees.
He snorted. “Be responsible for you tripping in this one? I don’t think so.”
As Charley gathered what she needed for the roasted cauliflower, Ethan grabbed the green beans. Charley explained that sometime they would fix potatoes with the roast, but her grandfather grew up near Idaho and often decided he wanted anything other than potatoes, so they would have cauliflower. “I don’t like raw or steamed, but I really like them roasted with this mustard sauce.”
Charley watched Ethan pull a cake plate out of the refrigerator. “Dessert?” At Ethan's acknowledgment she asked what it was. He wouldn’t tell her, saying he wanted it to be a surprise.
They worked efficiently together in the kitchen, getting dinner ready. Ethan selected a red wine for them and opened it to let it breathe. He carried their plates to the dining room table.
“This is good; the coffee does make the gravy richer.”
“Grandma knows best. My grandfather grew up in Spokane and grandma in Seattle. They had a restaurant in Seattle that my dad and all my aunts and uncles worked in while they were growing up.”
“You have a big family?”
“My dad had three brothers and two sisters. But even though they had six kids, my grandparents only had four grandchildren. There was my brother and me; we grew up in Pennsylvania. My one uncle had two boys and they were in Oregon. All of my dad’s family is in the northwest and we didn’t see them often. My dad moved there after he retired and I started med school.”
Ethan watched her. “Are we going to talk about your mom’s family?”
Charley shrugged. “Not much to tell. Her parents were killed in a car accident when she was in college. She was an only child and you know why I don’t talk to her.”
As they cleared the table and kitchen he asked her what he had been wondering about. “Why did you decide to do your residency in Boston with most of your family now out west?”
“It doesn’t feel like home to me there. I figured I could do my residency anywhere; it wasn’t a commitment to stay somewhere for my life. It’s only three years.” She smiled at him. “Besides coming here let me learn from the best.”
Ethan poured coffee and set the mugs on a tray with two dessert plates. Charley watched as he lifted the cover off the cake.
“Lemon! How did you know lemon was my favorite?” Charley couldn’t resist. She swiped her finger on the edge of the cake to collect a sample of icing. She popped it in her mouth.
“I asked Sienna the other day and she told me.”
Charley stared at him. “She helped me get dressed this morning and she didn’t say anything!”
Ethan laughed. “You need help getting dressed in the mornings?”
She felt her face redden. “I… well… um. I didn’t know what to wear this morning.”
“I would have gone with clothes, but I understand that some people are fussier than others.”
“I wanted to look nice.”
“You always look nice.”
“I thought that I always looked satisfactory.”
Ethan cut two pieces of cake and added them to the tray with the coffees.
“I thought we could take these into the bedroom. If that would be satisfactory to you?”
She nodded and he carried the tray to the bedroom and set it down on the bed. He flipped a switch causing the gas fireplace to spring to life. Charley picked up her cake and snuggled back against Ethan. “I like the fireplace here.”
“I don’t often use it.”
“Why tonight?”
“Must be the company I’m keeping.”
Charley turned and straddled his lap. “You better be careful. This company could end up corrupting you.”
“I look forward to it, if that’s the case.” Ethan rolled her unto her back.
Several hours later, Charley looked at the clock. “I should go home. I have to work tomorrow and my boss can be tough if I’m late.”
“If you stay with me, I’ll be sure you’re not late,” Ethan buried his head in her neck.
“I don’t have clean clothes for tomorrow.”
“You can either grab some scrubs from the locker room or ask your roommate to bring something for you.” Ethan pointed to his dresser. “I cleared both of the bottom drawers for you, if you want them.”
Charley chewed on her bottom lip. “You knew what the outcome of our talk was going to be before we actually talked today. When did you decide you wanted-”
“The night of the softball game, when I kissed you.”
Charley stared at him. “Then why did you keep putting me off when I wanted to talk?”
“Because I kept coming up with all the reasons why we shouldn’t be together. And I decided not to do that anymore. I’m tired of avoiding whatever it is we have.”
“Why do I get the two bottom drawers?”
“You’re shorter than me!” He indicates the drawer on the right. “You actually do have clean clothes in there. What you wore when we went to my dads. You at least have something to wear to the hospital.” Ethan watched her. “Any other concerns for tonight?”
“Do you have an extra toothbrush?”
Ethan shrugged. “Yes, but it’s one of the standard ones dentists hand out. It should be fine until we can get you one to keep here.”
Charley put her head on his pillow. “Then I can’t think of a single reason to get out of the warm bed right now.”
He turned off the light and slipped under the covers with her. “Neither can I.”
Tag list (if you want to be on or off let me know) @oofchoices @openheart12 @jamespotterthefirst @ohchoices @catchinglikekeronsene @aylamreads @nerdydinosaursweets @eramsey28 @txemrn @starrystarrytrouble @queencarb @thegreentwin @lion-ess24 @caseyvalentineramsey
@choicesficwriterscreations @choicesweeklychallenge
#dr ethan ramsey#dr. ethan ramsey x mc#ethan ramsey#ethan jonah ramsey#open heart fanfiction#open heart#choices open heart
81 notes
·
View notes
Text


picrew 1 || picrew 2 || picrew 3
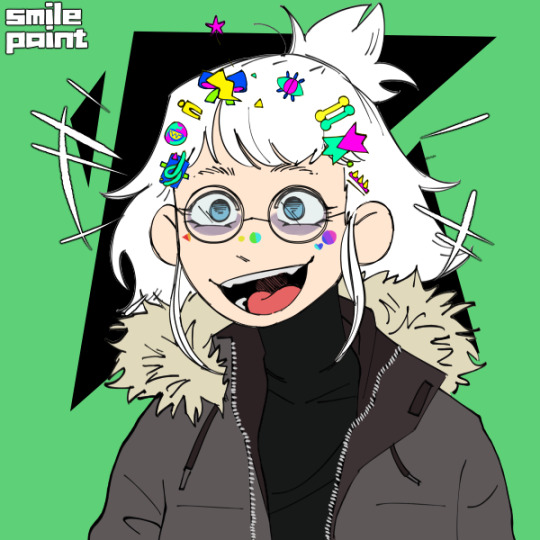
Cringe character of the day! My oc, Micah!
Micah is a trans dude who uses he/him, it/its, dragonself, vibeself, grayscaleself, & 🗯self pronouns. He is dragongender, discordian, ducklingic, swirlic, mascqueer, pluogender, & algiagender! Dragon is aceflux & bisexual!
It has ADHD, PTSD, schizophrenia, & late-onset Chediak-Higashi syndrome. He has albinism because of his CHS & can burn dangerously in the sun, plus due to the lack of pigment in his eyes, his eyesight is poor & sensitive to light. Vibe experiences chronic pain and must use a wheelchair sometimes. Grayscale also has a stutter induced by grayscales CHS, past head trauma, & worsened by grayscales ADHD.
🗯 often dresses in grayscale turtlenecks & jackets, along with gloves because of sensory things. 🗯 also likes colorful kandi, stickers, rings, & hair clips. 🗯 also has long hair that 🗯 usually ties back in a ponytail or bun.
Some of Micah’s hyperfixations are dragons & Minecraft. He enjoys astronomy & hand-making star maps. He is pixiekin!! He has a cat named Sprig & enjoys folk punk/rock.
12 notes
·
View notes
Text
Chediak-Higashi Syndrome in Accelerated Phase, a Case Report| Stephy Publishers

Abstract:
Chediak-Higashi syndrome corresponds to a series of genetic abnormalities in lysosomal transport, of autosomal recessive inheritance, characterized by partial oculocutaneous albinism and recurrent infections,1 usually between 7 and 10 years of age the accelerated phase of the disease, where developing hemophagocytic syndrome, given by a set of clinical findings, laboratory and histological studies where phagocytosis is prominent,2 with a failure in the regulation of the immune system due to an excessive production of pro-inflammatory cytokines that coexists with a dysfunction of natural killer cells and T lymphocytes, which leads to lethal development. We present a case of a 13-month-old patient, natural and from Pregonero, with a family history of consanguinity, recurrent respiratory infections, and a characteristic phenotype of Chediak-Higashi syndrome, without prior diagnosis or controls for this pathology, who presents with hemophagocytic syndrome leading to its death in 20 days.
Keywords: Chediak-Higashi, Hemophagocytic syndrome, Immune dysfunction
Introduction:
Chediak-Higashi syndrome corresponds to a rare, autosomal recessive pathology, which is characterized by partial oculocutaneous albinism, associated with repeated infections, there is a chromosomal alteration at the level of chromosome Xq25, CHS1 gene, located in bands 1q42–43,3 which leads to a consequent susceptibility to bacterial infections, since there is an alteration at the level of lizosomal transport and chemotaxis of neutrophils and natural killer cells1 are clinically characterized by hypopigmentation of the skin and eyes that are acquiring a coloration silvery, and which may also present: easy-onset ecchymosis, accompanied by hepatomegaly, splenomegaly, and peripheral neuropathies.4 Mutations in the CHS1 gene (LYST), located on the long arm of chromosome 1, result in a defect in granule morphogenesis in multiple tissues. This gene encodes a protein called the lysosomal traffic regulator that regulates the synthesis, transport, and fusion of cytoplasmic vesicles. The abnormalities observed in these vesicles result in highly enlarged and non-functional lysosomes, which are identified on cytology as coalescing giant azurophilic granules
To read more #Medicalcasereports #Clinicalcasereports
https://www.stephypublishers.com/archives-of-case-report/pdf/AMCCR.MS.ID.000502.pdf
#Openaccessjournals
https://www.stephypublishers.com/
#clinicalcasereports#medical journals#medical case reports#Stephypublishers#open access journals#open access publishers#pubmed articles
1 note
·
View note
Text
This week in: Heme block Part 2
In reference to the coagulation cascade: “If you liked complement in the immune system, you’ll like this. If you didn’t, welcome to my nightmare.”
“We can ask patients all kinds of things - who they’re having sex with, what kinds of sex they’re having, but we can’t ask about menstrual bleeding? Nobody wants to talk about period blood? WE’RE GOING TO TALK ABOUT IT. Because how are you going to know if your patient is having abnormally heavy bleeding if you don’t know what normal is?”
At a talk about gender affirming care: “It’s important for me to say that these topics, gender identity and expression and sexual orientation, they are not pathologies.”
“Sometimes patients will be all proud, ‘I had 7 pulmonary emboli!’ “
“Basophils are the rarest in the blood. When I see a basophil on a peripheral smear I wave and say, ‘Hi, I know you’re shy, but I appreciate you!’ “
In reference to LAD, CGD, MPO Deficiency, and Chediak Higashi Syndrome: “These are some inherited neutrophil abnormalities. I’m not going to talk about them because you heard about them in immuno. I’d recommend you look at these words for 3 minutes before you take Step 1.”
#medblr#online medical school#ZOOM SOM#MD PhD#ms1#med school really does cram so much into one week#it feels like we learned about anemias a month ago#that was last week#covid + med school = massive time distortion#the physicists should look into that
3 notes
·
View notes
Photo

Rare pale killer whale spotted off Nanaimo
Alexa Huffman - May 29, 2019
A rare pale-grey killer whale was spotted off the coast of Vancouver Island on Tuesday. Nanaimo-based Vancouver Island Whale Watch posted a picture of the young orca in Dodds Narrows on Tuesday. The orca is a member of the T46B Bigg’s killer whale family, which has a range from Washington state to Alaska.
“A WHITE orca, spotted five minutes from Nanaimo!! Wild day out on the water today finding an incredibly unique and unusually coloured calf (T46B1B)!,” the company wrote on its Facebook page. Capt. Mike Campbell with Vancouver Island Whale Watch said the whale was first seen by Val Watson, a marine naturalist.
“I thought it was a mistake at first when Val came back and said there’s a white one there. It looked white in the light,” Campbell said. Jared Towers, a killer whale researcher with Fisheries and Oceans Canada, said the whale was born sometime last fall, between September and the end of November.
“At that time, we didn’t get enough photos of it to verify that it actually had this condition of its skin that makes it appear much less dark than a usual killer whale so it wasn’t again until May 17 when this whale was photographed and at that time, it was really quite obvious that it was pale,” Towers said. Towers said the orca most likely has a condition called leucism, a partial loss of pigmentation.
“If you look at the photos, you can still see that the animal has a light eye patch and saddle detail but all the parts on his body that are supposed to be black are kind of a greyish colour so it somewhat rules out that this animal is a true albino,” Towers said.
“Albinos are typically all white and in addition to that, they have no pigment in their eyes.”
Towers added that it is possible that the orca could be affected with Chediak-Higashi syndrome, a genetic condition that causes partial albinism as well as a number of medical complications, but it would have to be looked at further. According to Towers, records of white killer whales have been recorded in B.C. for around 100 years. This is the fourth white orca recorded since 1924.
“Some killer whales that we’ve seen over the years here in B.C. have been born like this individual has, quite milky in colouration and over time they lose that and grow up as black and white like normal killer whales,” Towers said.
“All the white killer whales we’ve seen in this part of the world have all been Bigg’s killer whales.”
Bigg’s killer whales are also known as transients. They primarily eat marine mammals and squid. Towers said researchers will keep monitoring this pale orca by taking photographs.
31 notes
·
View notes
Photo









T004 Chimo
T004 Chimo was daughter of T003 Scarredjaw. She was neice to T002 Florencia and T006 Alice. She was cousin to T002B Peddler, T001 Charlie Chin, T002A Bajo, and T002C Tasu, T002B1, T002B2, T002C1 Rocky, T002C2 Tumbo, T002C3 Lucy, T002C4 Kano. She also was aunt T005 Nootka.
In 1970, Chimo, Florencia (named Pointednose Cow at the time), Scarredjaw Cow, Charlie Chin, and Nootka were captured. Chimo and Nootka were sold and separated. Chimo was born with Chediak-Higashi syndrome making her more susceptible to disease and infection as well as making her coloration similar to that of an Albino. Chimo died at the age of 4 after 2.5 years of captivity.
3 notes
·
View notes
Photo

ALBINISM
eri canonly with her white hair and red eyes could mean nothing in canon, but for me. there is a reason for it and it’s called albinism. it’s caused by a mutation in one of several genes that are responsible for the production of melanin by melanocytes in the skin and eyes. eri’s ablinism is called oculocutaneous albinism ( OCA ) because it affects the eyes, skin and hair. the genes that are affected are TYR, OCA2, TYRP1, SLC45A2. The effects of the lack of melanin in the skin means she is much more sensitive to the sun, which can cause easy sunburns and more at risk for skin cancer.
albinism is an autosomal recessive inheritance pattern, which means that both of eri’s parents are unaffected carriers of the gene ( they have one demonimate normal gene and one recessive mutated gene ) and eri was the child that hit the twenty have percent chance of being the affected one with both her genes being recessive.
being that she is affected by the mutated genes she has symptoms that eri experiences without even realizing, she believes that it’s normal to experience. these include astigmatism which is an error in the shape of the cornea ( the front surface of the eye ). This affects eri’s eyes giving her nearsightedness. This causes for eri to have difficult time seeing at night and having headaches for squinting her eyes in order to see. It could be fixed with corrective lenses, but hasn’t been diagnosed by a doctor.
another major symptom that affects her daily life is called photophobia. which basically means extreme sensitivity to light. it doesn’t affect eri as much as other people, but she cannot stare at a light for so long or go from a dim lighted place to a highly lighted place quickly without having pain in her eyes. these symptoms effects eri’s daily life and make it difficult for her to do one of her basic five senses, but she is awkward about asking for help from others and rather suffer them on her own.
there are a few types of albinism out there and some of the more complex ones have a few additional symptoms. eri’s specific albinism is called chediak-higashi syndrome which causes a mutation specifically in the LYST ( lysosomal trafficking regulator; CHS1 ) gene, which makes it so the abnormal lysosomes cannot properly do phagocytosis which is what white blood cells do to inject microorganisms, others cells and foreign particles.
this disease has an accelerated phase which can cause fever, jaundice, hepatosplenomegaly ( simultaneous enlargement of both the liver and the spleen ), lymphadenopathy ( a disease affecting the lymph nodes ), pancytopenia ( deficiency of all three cellular components of the blood ( red cells, white cells, and platelets )), bleeding diathesis ( unusual susceptibility to bleed ), and neurologic changes, which leads to death in most cases.
if eri doesn’t get a hematopoietic stem cell transplantation by the age of seven she can die, but even with it she only has a sixty percent ( my eri will live okay ). Basically a hematopoietic stem cell transplantation is replacing abnormal bone marrow with normal bone marrow. even after this treatment is completed eri will still be affected by the albinism and still will be immunosuppressed it just that she will not be in the accelerated phase and will be less likely to relapse into this phase.
all and all this is really hard for eri to go through, especially since she hasn’t been dealing with much of it with overhaul. during her time with him, she didn’t have to deal with the sun or really seeing things far away so eri never noticed how bad her sight was until she watched the festival. also any sickness that eri would get during the winter and changing seasons, overhaul got rid of them and made her perfectly normal. so starting school soon with all of this mentally affects her which would be talked more about in a different post.
21 notes
·
View notes
Text



#immunodeficiency#immunodeficiency syndromes#immunology#agammaglobulinemia#hyper IgM syndrome#IgA deficiency#hyper IgE syndrome#chronic granulomatous disease#CGD#MPO#chediak higashi syndrome#DiGeorge syndrome#Wiskott Aldrich syndrome#Wiskott Aldrich#SCID
1 note
·
View note
Text

Prushka is an albino and in addition to the mental and physical trauma of being inflicted by the curse of the Abyss several times as a child, Prushka also suffers from a rare illness related to the condition (similar to Hermansky-Pudlak syndrome or Chediak-Higashi syndrome) and her current life expectancy is 40-50 years, among his less than ethical experiments, Bondrewd has been researching medicines to treat her condition.
Another symptom of her illness is light sensitivity. For the most part, Prushka is unaware of this symptom, since the light she is accustomed to is tolerable to her eyes, and at the most extreme only causes her to subconsciously seek out a dark corner for relief. However, if she is on the surface, Prushka cannot stand looking at natural light sources for too long, meaning that her dream to see a real dawn could potentially cause her a lot of harm.
1 note
·
View note
Photo

How does a frog remind me of Chediak-Higashi Syndrome? Check out my explanation here on my YouTube channel!
0 notes
Last Seen Blogs




