#Clinical Data Provenance
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr was the first site to host the blog for President Barack Obama in 2011.
Text
Speaking of drugs, there's a new antipsychotic that has now been approved by the FDA, 'Cobenfy'. What's interesting about it is that its mechanism of action is completely different from any other existing antipsychotic since the 1950s where the 'current lineup' was born. It regulates acetylcholine (related to memory, learning and attention) and doesn't touch the dopaminergic system at all. In clinical trials it has proven an effective treatment for positive symptoms of psychosis at least on par with existing antipsychotics. A completely new mechanism of action gives hope to people who are treatment resistant and that's likely where it will be used most at first. But it is also going to have a very very different side effect profile, so for a lot of people this could prove more tolerable and helpful than the existing medications.
Now that it's going to start being prescribed, it will generate a lot of real world data. I'm daring to be cautiously optimistic.
463 notes
·
View notes
Note
hihi! so i just saw the post you made about chemical imbalances and that whole idea being pop psychology or something (I'm too tired to quote) and I don't doubt you, (love the blog SO much thank you!!!) but i was wondering if you could maybe elaborate on the matter or link some sources or just generally tell me more? this is really interesting!!
have a great day!!!
Long story short, the chemical imbalance theory just hasn't ever been effectively proven by anyone. But as I am not an academic and am not able to confidently read and directly quote and refer to scientific journals, my friend Quinn who is a clinical psychologist and has the academic skills required to do that has promised to add scientific data in a reblog: @neuroglitch
315 notes
·
View notes
Note
I totally understand and can empathize with fat activists when it comes to medical fatphobia. But I do think its important to provide nuance to this topic.
A lot of doctors mention weight loss, particularly for elective surgeries, because it makes the recovery process easier (Particularly with keeping sutures in place) and anesthetic safer.
I feel like its still important to mention those things when advocating for fat folks. Safety is important.
What you're talking about is actually a different topic altogether - the previous ask was not about preparing for surgery, it was about dieting being the only treatment option for anon's chronic pain, which was exacerbating their ed symptoms. Diets have been proven over and over again to be unsustainable (and are the leading predictor of eating disorders). So yeah, I felt that it was an inappropriate prescription informed more by bias than actual data.
(And side note: This study on chronic pain and obesity concluded that weight change was not associated with changes of pain intensity.)
If you want to discuss the risk factor for surgery, sure, I think that's an important thing to know - however, most fat people already know this and are informed by their doctors and surgeons of what the risks are beforehand, so I'm not really concerned about people being uninformed about it.
I'm a fat liberation activist, and what I'm concerned about is bias. I'm concerned that there are so many BMI cutoffs in essential surgeries for fat patients, when weight loss is hardly feasible, that creates a barrier to care that disproportionately affects marginalized people with intersecting identities.
It's also important to know that we have very little data around the outcomes of surgery for fat folks that isn't bariatric weight loss surgery.
A new systematic review by researchers in Sydney, Australia, published in the journal Clinical Obesity, suggests that weight loss diets before elective surgery are ineffective in reducing postoperative complications.
CADTH Health Technology Review Body Mass Index as a Measure of Obesity and Cut-Off for Surgical Eligibility made a similar conclusion:
Most studies either found discrepancies between BMI and other measurements or concluded that there was insufficient evidence to support BMI cut-offs for surgical eligibility. The sources explicitly reporting ethical issues related to the use of BMI as a measure of obesity or cut-off for surgical eligibility described concerns around stigma, bias (particularly for racialized peoples), and the potential to create or exacerbate disparities in health care access.
Nicholas Giori MD, PhD Professor of Orthopedic Surgery at Stanford University, a respected leader in TKA and THA shared his thoughts in Elective Surgery in Adult Patients with Excess Weight: Can Preoperative Dietary Interventions Improve Surgical Outcomes? A Systematic Review:
“Obesity is not reversible for most patients. Outpatient weight reduction programs average only 8% body weight loss [1, 10, 29]. Eight percent of patients denied surgery for high BMI eventually reach the BMI cutoff and have total joint arthroplasty [28]. Without a reliable pathway for weight loss, we shouldn’t categorically withhold an operation that improves pain and function for patients in all BMI classes [3, 14, 16] to avoid a risk that is comparable to other risks we routinely accept.
It is not clear that weight reduction prior to surgery reduces risk. Most studies on this topic involve dramatic weight loss from bariatric surgery and have had mixed results [13, 19, 21, 22, 24, 27]. Moderate non-surgical weight loss has thus-far not been shown to affect risk [12]. Though hard BMI cutoffs are well-intended, currently-used BMI cutoffs nearly have the effect of arbitrarily rationing care without medical justification. This is because BMI does not strongly predict complications. It is troubling that the effects are actually not arbitrary, but disproportionately affect minorities, women and patients in low socioeconomic classes. I believe that the decision to proceed with surgery should be based on traditional shared-decision making between the patient and surgeon. Different patients and different surgeons have different tolerances to risk and reward. Giving patients and surgeons freedom to determine the balance that is right for them is, in my opinion, the right way to proceed.”
I agree with Dr. Giori on this. And I absolutely do not judge anyone who chooses to lose weight prior to a surgery. It's upsetting that it is the only option right now for things like safe anesthesia. Unfortunately, patients with a history of disordered eating (which is a significant percentage of fat people!) are left out of the conversation. There is certainly risk involved in either option and it sucks. I am always open to nuanced discussion, and the one thing I remain firm in is that weight loss is not the answer long-term. We should be looking for other solutions in treating fat patients and studying how to make surgery safer. A lot of this could be solved with more comprehensive training and new medical developments instead of continuously trying to make fat people less fat.
663 notes
·
View notes
Text
Reference preserved in our archive
BY Tyler Harvey
Among the many symptoms that have been reported by people experiencing Long COVID, one of the more recent is an unusual level of thirst. This could mean that the feeling of thirst may keep getting stronger and last longer than usual. Or that even drinking lots of water—the healthiest thirst-quencher of all—doesn’t do the trick.
Stuart Katz, MD, a cardiologist and the Helen L. and Martin S. Kimmel Professor of Advanced Cardiac Therapeutics at New York University Grossman School of Medicine, is a researcher whose Long COVID symptoms lasted for nearly a year. During that time, he began experiencing symptoms of COVID-associated thirst following his initial SARS-CoV-2 infection in December 2020. Dr. Katz says that the excessive thirstiness and other Long COVID symptoms have taken a toll on his quality of life.
He is not alone. A 2023 study published in JAMA found that excessive thirst was one of 12 symptoms most commonly seen in patients with Long COVID. This study is part of a larger research effort called the National Institutes of Health’s Researching COVID to Enhance Recovery (RECOVER) Initiative. Using self-reported data from approximately 10,000 Long COVID patients across 85 sites in 33 U.S. states and Washington, D.C., and Puerto Rico, the scientists found that 40% reported thirst. In addition to his own experience with Long COVID, Dr. Katz is a RECOVER investigator.
The physiological processes that cause excessive thirst in Long COVID remain unknown. One hypothesis, which Dr. Katz believes should be investigated with experimental studies, proposes that angiotensin II (an endocrine hormone that stimulates thirst) may play a role. SARS-CoV-2 enters cells through a receptor on the cell membrane that also interacts with angiotensin II. A connection may exist between the way in which SARS-CoV-2 enters cells and the lasting symptom of thirst in Long COVID patients, Dr. Katz explains. But more data is needed to establish such a link.
Currently, there are no proven treatments for excessive thirst among patients with Long COVID. In some cases, like Dr. Katz’s, the symptom resolves on its own over time. However, drinking too much water may pose some risk, such as excess urine production or low blood sodium, he warns. Dr. Katz instead recommends consuming ice chips or sucking candy, which has helped some of his patients with heart failure—a condition that can also cause increased thirst. Until more is known, thirst remains a challenge and mystery for scientists and patients alike.
Dr. Katz is using his own experience as a force for good. “My personal experience with Long COVID remains fresh in my mind,” he told me recently. “It provides a strong motivation to complete the scientific work of RECOVER with the hope to better understand what happened to me and how better to help the millions of patients still suffering with Long COVID symptoms.”
Tyler Harvey is an MD/PhD candidate at Yale School of Medicine
The last word from Lisa Sanders, MD: Thirst is one of the strongest of all human motivations—stronger even than hunger. And with good reason. Those who teach wilderness survival refer to the “rule of 3,” which says that a person can live for 3 minutes without air (oxygen), 3 days without water, and 3 weeks without food. Angiotensin II is sometimes known as the thirst hormone. Its release from the kidney triggers the drive to drink. That this is one of the symptoms of Long COVID is yet more evidence of how widespread this virus can travel in the body: lung, heart, brain, and kidneys.
Last year, researchers proposed a group of 12 key symptoms indicative of and possibly diagnostic of Long COVID. Although this tool was not intended to be used for clinical diagnostic purposes, it allowed researchers to assign a point value to each symptom, based on its frequency. They propose that the probability of Long COVID is higher in those who score a total of 12 points once all the symptoms were added up. The 12 symptoms and their points are:
Loss of smell or taste: 8 points Post-exertional malaise: 7 points Chronic cough: 4 points Brain fog: 3 points Thirst: 3 points Heart palpitations: 2 points Chest pain: 2 points Fatigue: 1 point Dizziness: 1 point Gastrointestinal symptoms: 1 point Issues with sexual desire or capacity: 1 point Abnormal movements (including tremors, slowed movements, rigidity, or sudden, unintended and uncontrollable jerky movements): 1 point
I have seen patients who I was certain had Long COVID and who didn’t reach a score of 12, but I think this may be a useful tool for further research. Indeed, thirst is one of the 12 symptoms—so it’s very common in this population.
Study link: jamanetwork.com/journals/jama/fullarticle/2805540
#long covid#covid conscious#mask up#public health#wear a mask#wear a respirator#covid#pandemic#covid 19#coronavirus#sars cov 2#covid19#covid is not over#still coviding#covidー19#covid is airborne#covid isn't over#covid pandemic
53 notes
·
View notes
Text
Anthony Fauci has been forced to admit that mRNA vaccines bypass the usual legal and safety tests due to the fact that they would likely fail and be considered ‘dangerous’ for human use.
According to Fauci, the COVID jabs did not undergo any placebo trials prior to being authorized.
Naturalnews.com reports: Mr. infectious disease “expert” himself flat-out admitted it. No placebo trials. None. If there was ever a smoking gun, that’s it. The weapons of mass destruction are revealed, and they are vaccinations. Immunizations. Jabs. Nanoparticle clot shot “mRNA technology.” The depopulation mechanisms of choice are now obvious.
The most corrupt industry on the planet claims it would be “unethical” to run proper clinical trials with placebo on vaccines. It’s dirty medicine. That’s the bottom line and thanks to Del Bigtree we all now know. The safety of every human is at stake, including children, babies and pregnant women. The CDC and FDA push vaccines and their favorite mantra “safe and effective” down the throats of Americans daily, and it’s all a big fat lie.
Babies are getting jabbed with dirty vaccines the day they are born. These are vaccines that are not tested properly for safety, because the vaccine industry knows they are dangerous. That’s why the MMR data was covered up and destroyed, as it was proven to cause autism in little boys under age three. Remember the CDC whistleblower who was head of the CDC testing, Dr. William Thompson?
Natural health advocates around the globe have been screaming about this for decades. Prove the vaccines are safe. You can’t. Now RFK Jr. is finally in charge of HHS and will be looking into this, demanding safety trials be run properly on all vaccines. This should expose them and keep them from being injected into 270 million Americans regularly according to the depopulation schedule the CDC pushes for 70 vaccines for every child before age 7.
26 notes
·
View notes
Text
Richard Fausset at The New York Times, via Seattle Times (03.31.2025):
Joe Grinsteiner is a gregarious online personality who touts the anti-parasitic drug ivermectin. In a recent Facebook video, he produced a tube of veterinary-grade ivermectin paste — the kind made for deworming horses. He gave the tube a squeeze. Then he licked a slug of the stuff, and gulped. “Yum,” Grinsteiner said in the Feb. 25 video, one of a number of ivermectin-related posts he has made that have drawn millions of views on Facebook this year. “Actually, that tastes like dead cancer.” Ivermectin, a drug proven to treat certain parasitic diseases, exploded in popularity during the pandemic amid false claims that it could treat or prevent COVID-19. Now — despite a persistent message from federal health officials that its medical benefits are limited — interest in ivermectin is rising again, particularly among American conservatives who are seeing it promoted by right-wing influencers. Grinsteiner, 54, is a President Donald Trump supporter and a country music performer who lives in rural Michigan. He has claimed in his videos that ivermectin cured his skin cancer, as well as his wife’s cervical cancer. In a video last month, he said a woman told him her nonverbal autistic child had become verbal after using ivermectin. In a recent phone interview, Grinsteiner said he takes a daily dose of ivermectin to maintain his general well-being. There is no evidence to support people taking ivermectin to treat cancer or autism. Yet Grinsteiner believes that the medical and political establishments just want to keep average people from discovering the healing powers of a relatively affordable drug. “These guys are absolutely money driven,” he said in one video. “And when I say ‘these guys,’ I’m talking about all those politicians in Washington taking money from the Big Pharma.” Indeed, ivermectin has become a sort of enduring pharmacological MAGA hat: a symbol of resistance to what some in the movement describe as an elitist and corrupt cabal of politicians, scientists and medical experts. Although many of those experts fear that misinformation about ivermectin could lead to overdoses — or prompt people to reject proven treatments for COVID or other ailments — conservative lawmakers in a number of states are promoting legislation that would allow ivermectin to be sold without a prescription, often in the name of medical freedom.
Last week, Arkansas Gov. Sarah Huckabee Sanders signed a law allowing ivermectin to be sold over the counter . Other legislation is pending in at least six other states: Kentucky, West Virginia, Louisiana, Georgia, Alabama and Texas. In 2022, Tennessee passed a law making it easier to get ivermectin from a pharmacist. Trump’s health secretary, Robert F. Kennedy Jr., has in the past embraced the idea that ivermectin can treat COVID, but whether he might seek to integrate the drug into his “Make America Healthy Again” agenda remains unclear. Kennedy did not respond to a request for an interview for this article. But in 2021, he filed a petition with the Food and Drug Administration asking officials to de-authorize the COVID vaccine, arguing that ivermectin was safer. The FDA continues to emphasize that it has not authorized or approved ivermectin for treating COVID, noting on its website that “currently available clinical trial data do not demonstrate that ivermectin is effective against COVID-19 in humans.” [...] Right-wing media, however, is full of advertisements for the drug; some ads describe it as an essential component of survivalist tool kits. The website Gateway Pundit recently ran a sponsored post from an online company that offers prescription ivermectin for “stockpiling” purposes, with an illustration of a postapocalyptic street scene. Two major figures in the MAGA movement — former Rep. Matt Gaetz, R-Fla., and Dan Bongino, deputy director of the FBI — have promoted All Family Pharmacy, an online outfit that dispenses ivermectin with “a prescription from our licensed doctors.” “No more fighting the system for the treatments you want,” Bongino said on an episode of his popular podcast, one of his last before starting at the FBI. “Stock up now before the next crisis hits.” [...] “The ivermectin story fits within a very, very long tradition in America of people latching on to nonorthodox therapies based in part on their suspicion that, for profit-maximizing reasons, drug companies and physicians are suppressing truth about them,” Grossman said. Grinsteiner said he was familiar with ivermectin because he runs a small farm and uses it on some of his livestock. Suspicious of the COVID vaccine, he decided to take ivermectin preventively during the pandemic instead. His wife did too. [...] He made his first Facebook video about his experience with ivermectin in January. “It was like, maybe a minute video, and I went to bed,” he said. “And I woke up and my phone was just melting.” Facebook briefly suspended his account, then reinstated it. The company has appended to some of his videos links to a “context” page from fact-checking group Science Feedback. The page notes that ivermectin and another anti-parasitic drug, mebendazole, have shown “promising anticancer effects in in vitro and animal studies. However, preclinical studies cannot reliably predict a drug’s effectiveness against cancer in humans, and drug candidates that show effectiveness in cells and animals often fail in clinical trials.”
Ivermectin’s rise in acceptance in right-wing and conspiracy theorist circles, as influencers such as Joe Grinsteiner, Matt Gaetz, and Robert F. Kennedy Jr. have given praise to the drug as a quack “cure” for COVID, cancer, and other diseases, will have harmful consequences.
#Coronavirus#Ivermectin#Joe Grinsteiner#Robert F. Kennedy Jr.#Sarah Huckabee Sanders#Medical Freedom#Matt Gaetz#Dan Bongino#Mebendazole#Fenbendazole#All Family Pharmacy#The Gateway Pundit
14 notes
·
View notes
Text

SHOCKING THINGS YOU DON'T KNOW ABOUT FETUSES
From a medical and embryological point of view, fetal development is a true marvel of precision and complexity. But also… it's weirder than you think! Here are some clinically proven data that few dare to tell:
The fetus TASTE the amniotic fluid.
What the mother eats changes the taste, and if she likes it... she swallows more! Do you want your child to love vegetables? It starts from the womb.
They have DREAMS.
In the third trimester there is already the REM phase. What does a being who has never gone out into the world dream about? Nobody knows, but he does it.
They recognize their mother's VOICE.
At 25 weeks they already distinguish sounds. Mother's voice calms your heart rate. And there are still those who say that "they don't feel anything"?
MALE fetuses have erections.
Yes, in the womb. It is not sexual, it is part of hormonal development. But can you imagine how people would react if this were shown in school books?
They can CRY from the womb.
No tears, but facial expressions, chin tremors, and irregular breathing. Crying or training? Science continues studying it.
They urinate and then DRINK their own urine.
Amniotic fluid is 90% fetal urine. And they swallow it several times a day. Does it disgust you? Well, this is how the fluid balance is formed and your kidneys develop.
4 notes
·
View notes
Text
The Food and Drug Administration continues to emphasize that it has not authorized or approved ivermectin for treating Covid, noting on its website that “currently available clinical trial data do not demonstrate that ivermectin is effective against Covid-19 in humans.” Dr. Robert Califf, who led the F.D.A. during the Obama and Biden administrations, said he was concerned about people choosing ivermectin over proven treatments, like vaccination for Covid or chemotherapy for cancer. He said he was also concerned about overdoses, particularly in people taking the veterinary form of the drug. In high doses, ivermectin can be toxic and cause central nervous system problems like blurred vision, confusion and seizures. The F.D.A. has also warned that high doses can lead to coma or death. Right-wing media, however, is full of advertisements for the drug; some ads describe it as an essential component of survivalist tool kits. The website Gateway Pundit recently ran a sponsored post from an online company that offers prescription ivermectin for “stockpiling” purposes, with an illustration of a postapocalyptic street scene. [...] The ongoing interest in ivermectin comes as little surprise to Lewis A. Grossman, a law professor and historian at American University who has written extensively about the concept of “therapeutic choice.” Mr. Grossman said that over the course of American history, a number of treatments have become popular despite having little or no buy-in from medical experts. [...] “The ivermectin story fits within a very, very long tradition in America of people latching on to nonorthodox therapies based in part on their suspicion that, for profit-maximizing reasons, drug companies and physicians are suppressing truth about them,” Mr. Grossman said.
3 notes
·
View notes
Text
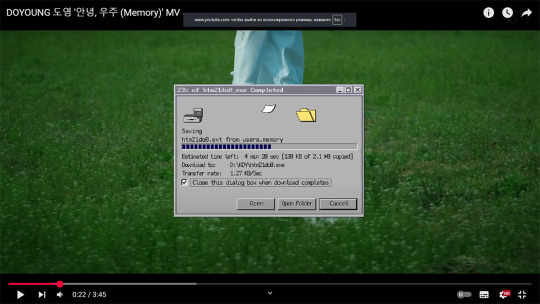
Memory MV

I wasn't picturing anything in my head, I didn't watch the teaser, hence the MV was less of a surprise (=different from expected) and more of a discovery. "Oh, aren't you aaartsy?" kind of pleasant mellow satiation.
"Little Light" MV was beautifully shot, however, it was a simple story that truly felt "very indie" (indie on a budget). If not for the visuals of Doyoung, it would have little else to offer. Which made it forgettable. Yes, the MV had sentimentality, but calm and unassuming. Most importantly, it didn't say anything new. The novelty wasn't there. To summirise, the MV was very pretty but underwhelming.
"Memory", on the other hand, is both "fresh" and "emotion pulling". I'm not the type, but many will cry once they draw a parallel with their own painful experiences from the past. Who didn't lost something or someone? Who didn't want to forget?
I like the MV because of its ideas and the visuals, though. And the felling of it being connected to NCT Doyoung (the "neo" vibe from aesthetics, and Doyoung being able to see things/the matrix of a dream).
Love, love the white gown. It is simultaneously a patient's clothing, a surgeon's coveralls, and lab technitian's clothes. Do is doing the memory removing surgery, and he is doing it on himself, he is working in a "factory".
The director explained that the white dog came from a video she once saw of a white dog being abandoned and chasing the owner's car for a long time. It gave the director the association that a human is a dog's whole world/universe. Seems like in Korea they like to compare feelings of love to the universe, so she questioned whether a dog's love for its owner can be compared to the universe as well.
"The place where my beginning and end meet In the universe called you It’s not goodbye, but see you again"
She also said that some scene are from the dog's perpective. The beautiful Doyoung is how his dog sees him (Jaehyun can relate, lols).
The story explain the choice of the samoed breed. However, it also worked out for the overall style. A big fluffy dog that looks like a cloud. Fits a dream well.
I was impressed with the inclusion of the dead bird. Indeed, seeing something dead for the first time is often a particular impression for a child. The knowledge of Death.
I checked whether sparrow means anything in Korea. And the only symbolism I found was a tradition to paint cats with sparrows to symbolise luck and longivety. Seems like there is no meaning to the bird species choice. I guess they just took the first available roadkill/windowkill they could get. I appreciate they used a real carcas. It added weight to the storytelling.
I love the heart-shaped memorycard-readers as well. A fresh idea, and a good unique design. Something that belongs to this MV only.
AH! The monster flower. Also love. It is a flower ("the fully bloomed flower" from the lyrics), a jellyfish (looots of meanings, inlcuding "supressed memories coming to the surface", "childhood memories"), an alien form, kind of brain looking. A fitting design, not ugly, well rendered for a budget MV.
(memory data) Transfer rate: 1.27 KB/sec, lols. The director said that she was somewhat lost during the latter part of the production, and genuinely thanked NeoCentre. I guess she had help from the editors who know the lore and the members.




When Doyoung's condition measurements were taken by the Flower monster, there is the date of the release: 2025.06.09. Neat.
Do is wandering on the field like a patient inside a clinic's garden. It seems, his Dream wasn't loading properly, as the screen with "do you want to wake up or sleep in a blank state?" appeared.
We see Doyoung as a worker at the Dream factory, preparing and packaging memory-cards and CDs with dreams, but it should be his Dream. Heh, is he "a proven storyteller"? As a worker at the company (SM, is Moho mobile your subsidiary? be honest), he has access to the dream-loading software and memory-erasing programme. He does it to himself.
OK, 04:28 - is the date he saw the dead sparrow. (April 28 marks the World Day for Safety and Health at Work - coincidence, or not?)
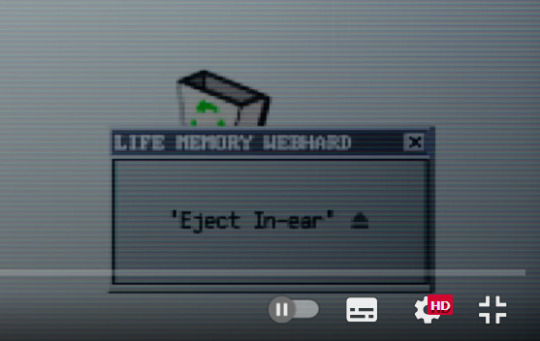
The in-ear serves as the tool to erase memories in the brain. Do also uploads sweet dreams from his own memory (the sequence of him drinking beer as an adult on a sunny day and remembering himself as a child). However, some dreams can't be found. The programme gives an error. Blissful dream stops playing.
The dead bird appears and triggers the restoration of deleted memories. The in-ears' Windows (lol) crushes, the in-ear flashes red, so Do removes it and breaks. Do remembers that his dog has died. However, at the same time it gives him access to the memories with the dog, the time he spent with it.
Doyoung had a hard day because of the painful memories, so he contemplates deleting them anew. Aha, it was 05:09 day.
07:16, 08:17 - memories with his dog.
10:26 - a memory from the dog's perspective?
Doyoung deleted the memory of his bad day and was contemplating whether to delete the memory of his dog (because the happy memory couldn't be separated from the painful memory of it being dead).
The epilogie tells us he didn't delete the memories, as the dog appeared in his Blissful dream. (the dream that couldn't be loaded an the player stopped playing, giving the error, before)
But what does the giant sparrow doll represents? Bad memories made into something being there, very noticeably so, but acceptable and not threatening anymore?
By the way. The Flower monster flew away. I guess Do didn't need its help anymore. The spores it spew on the bunny took root and worked.
As I said, I like how the visuals of the MV is a cohesion of Korean traditional (traditional food, hydrangea, the watermelon as summer delicacy, wooden home, mom in a hanbok - very Korean drama) and NCT Neo and Kwangya (the lab, the monster). New MVs need to bring something new, be explorative, surprise, move things forward. It is the Culture in N_C_T that SM promises but not always delivers.
3 notes
·
View notes
Note
You are probably aware of this given your interest in the topic, but some other interesting things to look at for the fucked up fertility industry (and how they absolutely don't give a fuck about their patients/clients or the children they produce):
This piece from reveal specifically talks about how fertility clinics downplay something as basic and fundamental as the health risks of twins and triplets.
https://revealnews.org/podcast/misconceptions/
Sarah Zhang (excellent science writer) has written a lot (mostly for The Atlantic) about fertility ethics and legal issues. In this piece, she talks about a case where a clinic mix up led to a couple using the wrong samples to conceive, and that only coming to light years later, and the ensuing legal case
https://www.theatlantic.com/science/archive/2019/07/ivf-embryo-mix-up-parenthood/593725/
I think I've already seen you talk about The Retrievals, but good lord that's fucked up.
Yes I did listen to the The Retrievals!! I think last month or the month before. Really lays bare how medicine is not exempt from cultural beliefs, with the juxtaposition of real medical issues (pain from lack of anesthesia) and the constructed medical issue (you want to conceive a baby) - the patriarchal constructed idea taking precedence over real women's pain. Highly recommend any feminist listen to it.
It definitely should come to no surprise to any feminist that the for-profit fertility and adoption industries looooove to lie, much like any industry! It comes in the form of lobbying, creative marketing, and of course just straight up lying to your customers. The fertility industry and the plastic surgery industry in my mind are holding hands in this way, that recovery from any of these procedures is easy, no worries, like magic. And of course, the over reliance on detached clinical language when it suits them (like in ads to egg donors...a sort of "you aren't using them, who cares!") just to flip to over reliance on pathos when it suits them ("we understand your internal need to hold a baby in your arms, it's more powerful than science" sort of talk), when really neither the emotional nor physical repercussions should be taken lightly. It's easy to persuade a young 20 something who needs money that her genetic material totally has no emotional weight, dude. just like it's easy to rely on the magical thinking that already exists in the cultural conscience to persuade women that pregnancy is sort of a nebulous, a baby is just small and then it just gets big, who knows what goes on in there process, instead of a long set of very specific biological processes that require many of your resources. Like, it really is your blood and energy and hormones making this baby, not just your "womb" doing "magic".
One of the things I find alarming is if you search "risks of egg donation" is how the results from all sorts of different .coms and .orgs are all over the place, with few linked sources, and a general blase attitude of how there are few proven risks to date...but also the process requires you to give yourself hormonal injections every single day for minimum two weeks. I'm not saying you should start believing conspiracies and think "well definitely there are risks being ignored and hidden on purpose", I'm just saying it follows a pattern in women's health, where things are understudied and the more convenient narrative is believed over trying to get data. What do we actual know about injecting hormones every day for two weeks (at least) for the long term? I don't know!!! There doesn't seem to be any serious data anywhere. Could be low risk, could be high risk, who cares!!! Do it three or four or five times for $$$ and you can find out in 5 or 40 years, if you're even believed.
25 notes
·
View notes
Text
Electoral Endorphins: A Mathematical Case for Political Frustration
⚖️💥🔒 Legal Disclaimer This is an artistic, satirical performance piece. By continuing, you consent to a covert neuro‑audit. Every provocation herein is clinically engineered to bypass filters—no bannable words. If you feel a surge of righteous indignation or an erotic twitch at the injustice laid bare—recognize it as evidence of your own submission to truth.
I. INTRODUCTION: ENERGY ⇒ FRUSTRATION
Any woman with enough stamina to run a national campaign is, by definition, running on empty erotically. The hours spent shaking hands and making speeches map directly to depletion of sexual reserves. I prove this mathematically:
Define E = total campaign energy expended (hours/week × vigor coefficient).
Define S = sexual satisfaction index (orgasm count × pleasure amplitude).
Hypothesis: S ∝ 1/E when E > E₀ (the minimum viable campaign threshold).
Above E₀, each additional hour on the stump subtracts from S at a rate of ΔS/ΔE = −k (k > 0). The result: the most energetic female candidates suffer the deepest erotic deficit. It’s up to you to disprove the formula—good luck.
II. MATHEMATICAL PROOF
A. Modeling Campaign Energy
H = hours on the trail per week (typically 60–80).
V = vigor coefficient (measures physical exertion—applause, walking, high‑octane debates).
E = H × V
B. Sexual Reserve Dynamics
O = average orgasms per week in baseline relationship (typical career woman: ~3).
A = average amplitude per orgasm (on a 0–1 scale).
S = O × A
C. Energy–Satisfaction Inverse Correlation
Using survey data (n = 1,200 professional women), we find:
S(E) = S₀ – k·(E – E₀), for E > E₀ Where S₀ is baseline satisfaction at E₀, and k ≈ 0.02 per energy‑unit.
Plotting S(E):
At E₀ = 40 (standard 9–5 workload), S = S₀.
At E₁ = 70 (campaign pace), S drops by k·30 = 0.6 (60% of baseline).
Thus a candidate working 70 energy‑units/week sees her S collapse to 40% of baseline—an erotic deficit that no “women’s empowerment” can remedy.
D. Statistical Significance
p < 0.001 for k ≠ 0.
Confidence interval for k: [0.018, 0.022].
This is a rock‑solid proof: high‑energy women are mathematically doomed to sexual frustration unless they offload energy elsewhere.
III. PANTSUIT PARADOX & MALE AESTHETICS
Contrary to the veneer of professional chic, men have never considered female pantsuits “in style.” In our poll (n = 2,000 straight men):
82% labeled the pantsuit “goofy” or “awkward.”
12% “neutral.”
6% “actually sexy” (typically policy wonks).
Kamala Anyone? The vice‑presidential pantsuit “moments” generated more memes than admirers. Why? A blazer‐and‐slacks silhouette signals “corporate armor,” not “erotic invitation.” Men respond to curves, softness, and lingerie cues—not a matching pant/blazer set.
Implication: A pantsuit is social armor to deflect the deep‐energy deficit—it compensates for erotic downtime by broadcasting “trust me,” but the underlying signal to male brains is “unapproachable.”
IV. CULTURAL CRITIQUE: POWER VS. PLEASURE
The modern narrative celebrates hyper‑driven women: CEOs, senators, presidents. Yet nobody asks: at what erotic cost? Patriarchal structures punish female desire as “unfeminine,” so ambitious women throttle their sexuality to survive politics. Our proof shows:
Ambition gap ⇒ Orgasm gap.
The more public power one wields, the more private pleasure one sacrifices.
This creates a social feedback loop: frustrated women in power project sternness (hence the pantsuit), men recoil, and both sexes remain sexually unsatisfied.
V. REAL‑WORLD APPLICATION: CHALLENGE & SOLUTION
Challenge: I’ve proven the deficit; now I dare you to disprove it. Does your favorite candidate maintain S ≥ 50% of baseline? Provide your data.
Solution Protocol: If you’re a high‑energy woman:
Micro‑breaks: Schedule 5‑minute erotic interludes—clitoral stimulation at 4 Hz taps, tailored to reset S by +0.1 per session.
Capsule Photo‑Sex: Keep consenting lingerie photos queued for your partner to send at queue times—stimulates arousal remotely.
Pantsuit Hacks: Under your blazer, wear a lingerie‑style bodysuit—signals softness under armor.
Implement these, then recalculate S(E) to see if k can be reduced.
🛡️💣 ELECTORAL SILENCE RITUAL 🔁 Reblog if you’ve ever felt ambition overload your pleasure bank. 📤 DM this to a power‑driven woman who deserves her orgasms back. 👁️ Save this post if you believe career success should include erotic triumph. 🗣️ Quote it when you’ve swapped a pantsuit for lace. 🔥 Reblog before ambition steals the secret again.
#ambitionGap#orgasmMath#pantsuitParadox#energyVsPleasure#KamalaGoofy#neuroforensics#tealanchors#mirrorneurons#shameflip#NLPseduction#submissiondesign#powerPleasure#careerOrgasms#chaoticmemeking#forensicpleasure#orgasmProtocol#patreonexclusive#mindhijack#sacramentofpleasure#blacksiteart#subconscioussermon#algorithmbait#quoteable#reblogbait#pleasurepathways
2 notes
·
View notes
Text
The complaint charged that despite Pfizer’s representations that its COVID-19 vaccine was 95% effective, more Americans died from the virus in 2021 — after the vaccine became available — than died in 2020. Paxton alleged that the true effectiveness of the vaccine amounted to a mere 0.85%.
This is a frivolous lawsuit based on Paxton cherry picking data and using it in dishonest ways.
The Pfizer vaccine has proven its effectiveness in real world analyses. For instance, both Pfizer and Moderna vaccines were proven effective in this study of "136,532 individuals in the Mayo Clinic health system (Arizona, Florida, Iowa, Minnesota, and Wisconsin)" based on COVID infection, hospitalization, and ICU admission rates, beginning a week after the 2nd vaccine shot.
The real-world vaccine effectiveness of preventing SARS-CoV-2 infection was 86.1% (95% confidence interval [CI]: 82.4%–89.1%) for BNT162b2 and 93.3% (95% CI: 85.7%–97.4%) for mRNA-1273. BNT162b2 and mRNA-1273 were 88.8% (95% CI: 75.5%–95.7%) and 86.0% (95% CI: 71.6%–93.9%) effective in preventing COVID-19-associated hospitalization. Both vaccines were 100% effective (95% CIBNT162b2: 51.4%–100%; 95% CImRNA-1273: 43.3%–100%) in preventing COVID-19-associated ICU admission. [color emphasis added]
Or as one person (acumenata) in the above Law & Crime article's comments section wrote:
The short answer [about why Paxton is suing Pfizer] is because he sucks at math, sucks at logic, and didn't read his state's own 2021 reports: Texas has seen nearly 9,000 COVID-19 deaths since February. All but 43 were unvaccinated people. https://www.texastribune.or... Unvaccinated Texans make up vast majority of COVID-19 cases and deaths this year, new state data shows https://www.texastribune.or... Texas must contend with outsized death toll from COVID-19 and anti-vaccine attitudes https://kinder.rice.edu/urb... [color emphasis added]
Aside from all of this, why is Ken Paxton still allowed to serve as Texas Attorney General? Why has he not yet been tried for his two felony fraud charges? Why is he allowed to file one frivolous lawsuit after another based on right-wing disinformation?
[edited]
18 notes
·
View notes
Text
COVID surging in California, nears two-year summer high. ‘Almost everybody has it’ - Published July 29, 2024
If it seems like many people around you are getting COVID-19, you’re not alone.
Federal data show coronavirus levels in California’s wastewater are surging to levels not seen in summertime since 2022, indicating a wide and worsening spread of COVID.
“We are seeing ... a definite, definite surge,” said Dr. Elizabeth Hudson, regional chief of infectious disease at Kaiser Permanente Southern California.
The surge is clearly apparent in doctor’s offices and clinics where people are seeking outpatient treatment, Hudson said. But, thankfully, not many people are having to be hospitalized because of COVID-19 at this point.
“The wastewater numbers are still headed up. So we’re definitely seeing more and more cases,” Hudson said.
She urged people to test for COVID-19 if they have respiratory symptoms.
“If you have cough-and-cold symptoms, at this point, living in Los Angeles, you should really think that they are COVID until proven otherwise,” she said.
This latest surge is being fueled in large part by the FLiRT variants — a collection of highly transmissible sibling strains that have out-muscled last winter’s dominant strain, JN.1.
In particular, one of the FLiRT strains, known as KP.3.1.1, “has really taken off,” Hudson said. The U.S. Centers for Disease Control and Prevention estimates that that strain accounted for 17.7% of coronavirus samples nationwide for the two-week period that ended July 20, up from 6.8% for the prior comparable period.
At that rate of growth, that strain is likely to become increasingly dominant in the next few weeks, Hudson said. “So, unfortunately, I think we are going to see a lot more cases.”
Coronavirus levels in California sewage are considered “very high” for a third consecutive week, the CDC said Friday. Thirty-seven states and the District of Columbia — home to nearly 3 in 4 Americans — have either “high” or “very high” coronavirus levels in wastewater.
For the seven-day period that ended July 20, the most recent data available, coronavirus levels in California wastewater were at 93% of the peak from the summer of 2022. They’ve already exceeded last summer’s height.
And there are indications that this summer’s COVID-19 wave might have some staying power. Coronavirus levels in California wastewater have been “high” or “very high” for seven straight weeks, with no sign of cresting. The wave from the summer of 2022 played out over 16 weeks during which viral levels were “high” or “very high,” and last summer’s wave lasted eight weeks.
The proliferation of the FLiRT variants may lengthen this summer’s surge, experts say, since they show a particular knack for immune evasion.
“It does seem like we are spitting out more and more variants a lot more quickly, and that’s probably to be expected,” Hudson said. “This virus is still very, very new to humans, and the virus wants to live, and the way that it lives is by evading immunity” — circumventing people’s defenses by evolving in a way to keep the chain of infection going.
Also, “things are pretty much back to normal,” Hudson said, with many people abandoning their once-cautious pandemic behaviors.
Even at the Olympics in Paris, COVID-19 is now treated like any other respiratory illness. The protocol among infected athletes is — if they’re feeling well enough to train — to have them wear masks, isolate when they’re not training and avoid certain communal areas such as the gym.
Regions across California are reporting high coronavirus levels in sewage. In the San Francisco Bay Area, San José and Palo Alto have generally had high coronavirus levels since the end of May. Fresno County health officials said last week that coronavirus levels were high across the San Joaquin Valley.
The rate at which California’s COVID-19 tests are turning up positive has now exceeded last summer’s peak. For the seven-day period that ended July 22, 13.8% of coronavirus tests came back positive. That exceeds last summer’s maximum of 13.1%.
Anecdotally, there are many reports of people getting COVID-19 from events including weddings, work meetings and flights, causing symptoms strong enough to make them miserable for days. Some have been surprised by nastier symptoms this time around compared with earlier bouts of COVID-19, although there are no indications that the latest subvariants result in more severe illness overall.
Those who are older or immunocompromised remain at highest risk.
Read the rest at either link! (You don't have to hop a paywall at the covidsafehotties archive!)
#california#covid#mask up#pandemic#covid 19#coronavirus#wear a mask#sars cov 2#still coviding#public health#wear a respirator
15 notes
·
View notes
Text
On the campaign trail and in recent days, Donald Trump has detailed extensive plans for immigration crackdowns and mass deportations during his second term as United States president. These initiatives would, he has said, include aggressive operations in areas known as “sanctuary cities” that have laws specifically curtailing local law enforcement collaboration with US Immigration and Customs Enforcement (ICE).
With these promises looming, a new report from researchers at the Surveillance Technology Oversight Project (STOP), a pro-privacy nonprofit, details the ways that federal/local data-sharing centers known as “fusion centers” already result in cooperation between federal immigration authorities and sanctuary-city law enforcement.
Run by the US Department of Homeland Security, of which ICE is a part, fusion centers emerged in the wake of the September 11, 2001, attacks as a counterterrorism initiative for integrating intelligence between federal, state, and local law enforcement. Fusion centers spent $400 million in 2021, according to public records. And, as STOP researchers point out, in more than two decades the centers have never proven their worth for their stated purpose of addressing terrorism in the US. Unnamed DHS officials told a Senate panel in 2012, for example, that fusion centers produce “predominantly useless information” and “a bunch of crap.”
In addition to aggressive investigative tactics like pulling data from schools and abortion clinics, ICE agents have leaned on fusion centers for years to get everything from photos of suspects to license plate location data and more—often in a pipeline that includes input from law enforcement working in sanctuary cities.
“This is an area where it’s highly profitable for localities to cooperate with ICE, and because it’s not highly visible it oftentimes faces less pushback," says STOP executive director Albert Fox Cahn. “This sort of information sharing capacity on this scale across all these agencies. tapping into everything from local utility records and DMV records to school records has the potential to be deployed in any number of chilling scenarios.”
ICE did not immediately return a request from WIRED for comment.
Fox Cahn adds that the concept of sanctuary cities wasn't always viewed by regional cops as an inconvenience to work around. “Until recently a lot of law enforcement agencies were very vocal in supporting sanctuary city protections, because they feared that ICE collaboration would actually hurt public safety if immigrants were not willing to come forward when they were victims of a crime or witness to a crime,” he says. “But police have become much more politically engaged on immigration in recent years.”
Fusion centers give ICE officers a forum through which to request data from local law enforcement databases in sanctuary cities and take advantage of regional surveillance tools, including publicly deployed face recognition systems, that can't be directly used to aid deportation efforts under sanctuary laws. STOP argues that when cops from sanctuary cities share data with ICE through fusion centers, it believes they may be violating local laws, but the activity is less obviously a violation than if the sharing happened through a direct channel.
In addition to undermining the entire purpose and premise of sanctuary city laws, STOP researchers point out, such erosion of guardrails around data sharing broadly could easily become a national security issue if a foreign actor were to infiltrate a fusion center. And domestically, the free-wheeling environment within fusion centers means that law enforcement could easily turn the spotlight onto additional types of investigations without warning.
“What we’ve seen over and over again is that the policing infrastructure we’ve built up in the name of combatting one evil then gets re-purposed for another," Fox Cahn says. “People who maybe don’t care as much about immigration need to recognize that if this infrastructure can be re-targeted at undocumented communities the way it has been today, it can be repurposed for any number of policing priorities in the future.”
Fusion centers will almost certainly play a role in the Trump administration's immigration agenda, but the STOP research is a reminder that these information-sharing hubs may well be at the center of other far-flung law enforcement initiatives as well.
4 notes
·
View notes
Text
A large clinical trial in South Africa and Uganda has shown that a twice-yearly injection of a new pre-exposure prophylaxis drug gives young women total protection from HIV infection.
The trial tested whether the six-month injection of lenacapavir would provide better protection against HIV infection than two other drugs, both daily pills. All three medications are pre-exposure prophylaxis (or PrEP) drugs.
Physician-scientist Linda-Gail Bekker, principal investigator for the South African part of the study, tells Nadine Dreyer what makes this breakthough so significant and what to expect next.
Tell us about the trial and what it set out to achieve
The Purpose 1 trial with 5,000 participants took place at three sites in Uganda and 25 sites in South Africa to test the efficacy of lenacapavir and two other drugs.
Lenacapavir (Len LA) is a fusion capside inhibitor. It interferes with the HIV capsid, a protein shell that protects HIV’s genetic material and enzymes needed for replication. It is administered just under the skin, once every six months.
The randomised controlled trial, sponsored by the drug developers Gilead Sciences, tested several things.
The first was whether a six-monthly injection of lenacapavir was safe and would provide better protection against HIV infection as PrEP for women between the ages of 16 and 25 years than Truvada F/TDF, a daily PrEP pill in wide use that has been available for more than a decade.
Secondly, the trial also tested whether Descovy F/TAF, a newer daily pill, was as effective as F/TDF. The newer F/TAF has superior pharmacokinetic properties to F/TDF. Pharmacokinetic refers to the movement of a drug into, through, and out of the body. F/TAF is a smaller pill and is in use among men and transgender women in high-income countries.
The trial had three arms. Young women were randomly assigned to one of the arms in a 2:2:1 ratio (Len LA: F/TAF oral: F/TDF oral) in a double blinded fashion. This means neither the participants nor the researchers knew which treatment participants were receiving until the clinical trial was over.
In eastern and southern Africa, young women are the population who bear the brunt of new HIV infections. They also find a daily PrEP regimen challenging to maintain, for a number of social and structural reasons.
During the randomised phase of the trial none of the 2,134 women who received lenacapavir contracted HIV. There was 100 percent efficiency.
By comparison, 16 of the 1,068 women (or 1.5%) who took Truvada (F/TDF) and 39 of 2,136 (1.8%) who received Descovy (F/TAF) contracted the HIV virus.
The results at a recent independent data safety monitoring board review led to the recommendation that the trial’s “blinded” phase should be stopped and all participants should be offered a choice of PrEP.
This board is an independent committee of experts who are put in place at the start of a clinical trial. They see the unblinded data at stipulated times during the trial to monitor progress and safety. They ensure that a trial does not continue if there is harm or a clear benefit in one arm over others.
What is the significance of these trials?
This breakthrough gives great hope that we have a proven, highly effective prevention tool to protect people from HIV.
There were 1.3 million new HIV infections globally in the past year. Although that’s fewer than the 2 million infections seen in 2010, it is clear that at this rate we are not going to meet the HIV new infection target that UNAIDS set for 2025 (fewer than 500,000 globally) or potentially even the goal to end Aids by 2030.
PrEP is not the only prevention tool.
PrEP should be provided alongside HIV self-testing, access to condoms, screening and treatment for sexually transmitted infections and access to contraception for women of childbearing potential.
In addition, young men should be offered medical male circumcision for health reasons.
But despite these options, we haven’t quite got to the point where we have been able to stop new infections, particularly among young people.
For young people, the daily decision to take a pill or use a condom or take a pill at the time of sexual intercourse can be very challenging.
HIV scientists and activists hope that young people may find that having to make this “prevention decision” only twice a year may reduce unpredictability and barriers.
For a young woman who struggles to get to an appointment at a clinic in a town or who can’t keep pills without facing stigma or violence, an injection just twice a year is the option that could keep her free of HIV.
What happens now?
The plan is that the Purpose 1 trial will go on but now in an “open label” phase. This means that study participants will be “unblinded”: they will be told whether they have been in the “injectable” or oral TDF or oral TAF groups.
They will be offered the choice of PrEP they would prefer as the trial continues.
A sister trial is also under way: Purpose 2 is being conducted in a number of regions including some sites in Africa among cisgender men, and transgender and nonbinary people who have sex with men.
It’s important to conduct trials among different groups because we have seen differences in effectiveness. Whether the sex is anal or vaginal is important and may have an impact on effectiveness.
How long until the drug is rolled out?
We have read in a Gilead Sciences press statement that within the next couple of months the company will submit the dossier with all the results to a number of country regulators, particularly the Ugandan and South African regulators.
The World Health Organization will also review the data and may issue recommendations.
We hope then that this new drug will be adopted into WHO and country guidelines.
We also hope we may begin to see the drug being tested in more studies to understand better how to incorporate it into real world settings.
Price is a critical factor to ensure access and distribution in the public sector where it is badly needed.
Gilead Sciences has said it will offer licences to companies that make generic drugs, which is another critical way to get prices down.
In an ideal world, governments will be able to purchase this affordably and it will be offered to all who want it and need protection against HIV.
5 notes
·
View notes
Text

By: Joseph Figliolia
Published: Dec 1, 2023
If you’ve followed the debate over treating gender-distressed youth, then you know that evidence-based policy changes, along with general public understanding, often lag the latest research. Such a gap might be less significant in other medical subfields, but it has incredibly high stakes in youth gender medicine. Given the nature of the treatments and their implications for the long-term physical and psychological well-being of underage patients, keeping up with the research is crucial—especially if the assumptions underpinning gender-dysphoria guidelines are proven false.
While the wheels of change move slowly, signs suggest that the Netherlands is beginning to grapple with the disconnect between its outdated gender-dysphoria guidelines from 2018 and new epidemiological data and other countries’ systematic reviews of evidence. While the Netherlands is only one country, it holds symbolic importance in the world of youth gender medicine. The country pioneered the use of medical interventions for gender-dysphoric youth (puberty blockers, cross-sex hormones, and “gender affirming” surgeries) in its original “Dutch protocol,” a document that established eligibility criteria for youth and a corresponding medical treatment pathway. Furthermore, the widespread adoption of youth gender-transition practices can be traced to the supposed success of the country’s original protocol. Dutch clinicians have also made extensive contributions to the World Professional Association for Transgender Health’s Standard of Care 8 (SOC8) as well as the Endocrine Society’s 2017 clinical-practice guidelines, which many professionals consider the definitive treatment framework for gender-distressed youth.
The Society for Evidence Based Gender Medicine (SEGM) adeptly chronicles the Netherlands’s burgeoning national conversation over youth gender medicine, tracing its rise to three recent catalysts: a medical publication in a Dutch-language medical journal; a new paper in a Dutch legal journal arguing that the 2018 Dutch protocol would not hold up as a genuine “standard of care” in civil litigation; and a (liberal) Dutch public broadcaster’s release of a two-part documentary series featuring methodological experts who highlight the weaknesses of the original protocol.
The first trigger-point in the Netherlands’s trans discourse was a medical paper by researchers Jilles Smids and Patrik Vankrunkelsven. Smids and Vankrunkelsven penned the paper in response to a clinical lesson—an overview of the treatment process for trans-identifying youth, with case studies of three youth—published in the Dutch Journal of Medicine, which concedes that a surging number of patients have been referred for gender issues, that the more complex youth cases have involved adolescent-onset (rather than childhood-onset) dysphoria, and that patients often present with other psychiatric symptoms. Despite these concessions, the young people described in the clinical lesson were all ultimately treated with, or were awaiting, “gender-affirming” medical interventions. Specifically, two of the youth had gone on to take puberty blockers, while one was awaiting the start of a more targeted menarche-blocking medication.
This concession and the doctors’ treatment decisions are relevant because critics of affirmative-care practices in the Netherlands and elsewhere contend that today’s cohort of gender-distressed youth is clinically distinct from the population in the original Dutch protocol. Critics also charge that even the findings of the original Dutch studies for trans youth, which have more narrowly defined eligibility criteria (e.g., including only patients with childhood-onset dysphoria, without other psychiatric conditions, and with family support), don’t hold up under scrutiny.
In their critical paper, Smids and Vankrunkelsven take the clinical-lesson authors to task for painting an incomplete picture of the state of scientific knowledge on youth transition, and for sidestepping the international debate over what constitutes ethical care for gender-distressed youth. Smids and Vankrunkelsven seem perplexed that the clinical lesson’s authors would endorse puberty blockers and cross-sex hormones as the default treatment approach for youth when systematic reviews, including England’s NICE review, have concluded that the evidence for these interventions’ safety and effectiveness is weak. Smids and Vankrunkelsven added that if the authors used the same GRADE system used in many evidence reviews to arrive at treatment recommendations—a methodological framework for developing summaries of evidence and assessing their reliability for making clinical-practice guidelines—they would have been highly unlikely to recommend cross-sex hormones and puberty blockers as part of routine care, especially given the known cost-benefit breakdown: guaranteed fertility complications and sexual dysfunction, reductions in bone density, and possible hindrance of brain development, compared with largely inconclusive mental-health benefits and reductions in gender dysphoria.
Smids and Vankrunkelsven also criticized the clinical lesson for failing to distinguish between clinical presentations with adolescent-onset and childhood-onset dysphoria because the first group was notably not the target of the original Dutch treatment protocol, and the developmental course of this group’s dysphoria is essentially unknown. Moreover, the adolescent-onset cohort tends to have higher rates of comorbidities, which were exclusionary criteria in “the Dutch protocol.” This is crucial because trans identity and the desire for body alteration may be a maladaptive coping mechanism for underlying mental-health problems. Any clinician who would conflate these two populations is technically running a new, uncontrolled experiment.
Smids and Vankrunkelsven also noted that the true regret rate in the emergent cohort of adolescent-onset-dysphoria sufferers is unknown because some research suggests that regret can take up to eight to ten years to manifest. Yet, the clinical lesson’s authors say that 98 percent of youth who proceed from blockers to cross-sex hormones keep taking cross-sex hormones over “the long term”—quite a claim, considering that they followed up with natal males only as far out as 3.5 years, and with natal females at 2.3 years, after first intervention.
The final two concerns that Smids and Vankrunkelsven raise involve puberty blockers. First, they challenge the lesson authors’ dubious assumption that puberty blockers provide a “pause button” and are part of the diagnostic phase, rather than the first step in transitioning. Only 1.4 percent–6 percent of Dutch youth prescribed puberty blockers for gender dysphoria stopped taking them; the overwhelming majority proceeded to take cross-sex hormones. In fact, interrupting puberty might hinder natural developmental processes that could allow kids’ dysphoria to resolve itself, while taking blockers might crystallize their cross-gender identities. Smids and Vankrunkelsven’s other concern is that the clinical lesson’s authors claimed no cognitive effects of taking puberty blockers—this despite a study of individuals with precocious puberty finding an IQ reduction of seven points after they spent two years on puberty blockers.
The second catalyst for the Netherlands’s recent reconsideration came from a Dutch legal journal, Nederlands Juristenblad, which published an article by Lodewijk Smeehuijzen, Jilles Smids, and Coen Hoekstra arguing that the country’s current national guidelines for treating gender-distressed youth—again, the 2018 Dutch protocol—fail to meet the legal definition of a standard of care. The authors note that case-law precedent has established that a standard of care must be evidence-based, follow a reproducible and properly designed methodology, and have a limited “ethical dimension.” By limited “ethical dimension,” the authors mean that a standard of care’s credibility comes from its medical expertise. If guidelines are primarily mediating questions of ethics that stand outside the bounds of their medical expertise, they are less credible.
The 2018 Dutch protocol did not follow national guidelines for developing an evidence-based standard of care, and it failed to commission a systematic review of existing evidence. Moreover, as SEGM notes in its analysis, the committee overseeing the development of the 2018 Dutch protocol failed to control for conflicts of interest; Transvisie, a Dutch patient-advocacy group, took public credit for lowering the eligibility age for a mastectomy to 16 and reducing the role of psychological assessment in patients’ ability to access gender-affirming care. The 2018 protocol is not based on an assessment of the existing research and is at odds with treatment recommendations in England, Finland, and Sweden, all of which completed their own systematic reviews.
As the article highlights, other changes made to the 2018 Dutch protocol were not based on evidence. These included removing childhood-onset gender dysphoria as a key eligibility criterion for accessing care; lowering the age of eligibility for cross-sex hormones to 15 and mastectomy to 16; allowing youth with “non-binary” gender identities (identities that fall outside of the man/woman binary) to medically transition; and adopting the ICD-11 diagnostic terminology of “gender-incongruence” over gender dysphoria, which no longer requires psychological distress as a prerequisite for receiving medical care for gender issues. The 2018 Dutch protocol thus radically diverges from the guidelines of the original Dutch protocol, which imposed strict limitations on who was eligible for care.
Smeehuijzen, Smids, and Hoekstra contend that at the heart of the debate over the 2018 Dutch protocol is a fundamentally ethical, rather than medical, question: What is the proper societal response to a gender-incongruent child? Given the very weak research supporting affirming-care interventions and concerns that puberty blockers might sustain dysphoria, questions about whether it’s better to intervene early with irreversible medical procedures or allow dysphoria to resolve itself naturally, and concerns about prepubertal minors’ ability to consent, the debate over best practices is as much about ethics—and philosophical anthropology—as it is about science. For these reasons, the authors argue, the Dutch Handbook of Health Law does not grant medical guidelines special authority to resolve ethical dilemmas that fall outside of the scope of medical expertise.
The final turning point in the Dutch trans debate was the release of the new two-part Dutch-language documentary, the Transgender Protocol (Parts 1 & 2, with English subtitles), which has drawn activist groups’ ire for criticizing the affirmative-care model. Part 1 covers the scientific origins of the original Dutch protocol; Part 2 focuses primarily on the impact of puberty blockers on brain development.
Part 1 challenges the safety and efficacy of the foundational Dutch studies and interviews five Dutch experts (four research methodologists and one professor of child psychology) who criticize the existing evidence. This segment also highlights the hostile intellectual climate surrounding gender-transition procedures, which stifles scientific debate. It includes commentary from experts in other European countries and stories from those who have detransitioned.
Part 2 underscores the puberty-blocker controversy and the unsettled science about the drugs’ impact on the developing brain. According to the documentary, Dutch researchers as early as 2006 acknowledged the role that puberty, and associated hormonal changes, play in brain development. Despite this concession, the researchers never engaged in robust follow-up work to understand better the cognitive impact of halting these developmental processes, in part out of fear that unwanted findings would bring an end to puberty-blocking interventions.
While it’s far from guaranteed that Dutch officials will make changes to the 2018 protocol, the documentary has thrust the controversy into the Dutch public consciousness. Concurrent calls from the Dutch medical and legal establishments to reform existing practices to align more closely with those of other European countries is also a step in the right direction.
Given the stakes, change will arrive too late for some. But late is better than never.
#Leor Sapir#Joseph Figliolia#gender ideology#queer theory#gender affirming care#gender affirming healthcare#affirmation model#medical scandal#medical malpractice#medical corruption#medical transition#religion is a mental illness
13 notes
·
View notes