#extensor compartment
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr has 16.74 million mobile monthly users in the US.
Text
Breaking Your Fucking Humerus
Super common, usually not bad, but there is some interesting shit here that I wanna talk about. We're gonna talk about breaking the humerus (that big bitch that's your upper arm) because there are a lotta ways this can present based on the area that's broken. But first things first: anatomy.
*also fair warning: there are some nasty looking x-rays in here, so if you don't like to see that, you've been warned*
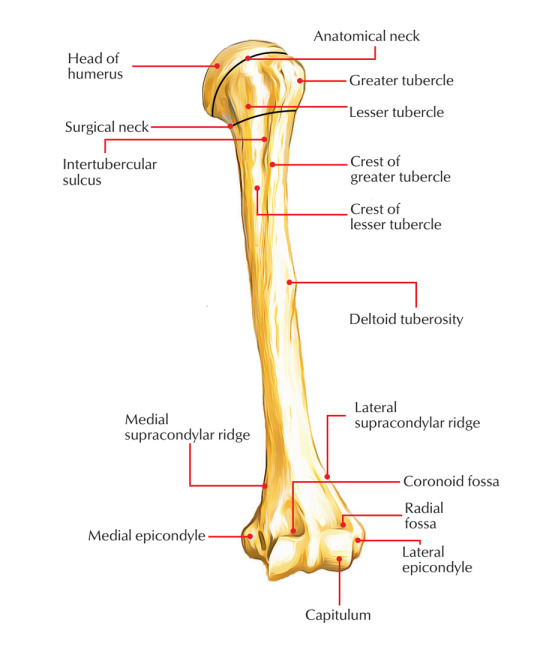
Surgical Neck
We're gonna go from top to bottom to make it simple. The surgical neck is distal to the anatomical neck, separated by the tubercles (where a bunch of shit attaches). Usually the surgical neck is fractured by old people from either a direct blow or a violent muscle contraction (osteoporosis fucks you up, man). It can also be due to an anterior dislocation of the shoulder.
This can damage the axillary nerve (which innervates the deltoid). This will lead to a flattened deltoid (no tone), loss of the ability to abduct the arm, and a loss of sensation of the deltoid and lateral arm.
This fracture can also damage the posterior circumflex humeral artery. You probably won't bleed to death that quick or get ischemia, but you still want that shit fixed (fucking obviously).

Midshaft
This is caused by a direct blow, fall, or collision. I broke my arm at the midshaft by smacking it on my car seat (i was a child) during a motor vehicle accident. Just snapped that bitch and poked it out my arm.
Anyway, this can damage the radial nerve, which supplies the dorsal hand and allows you to extend your elbow/wrist/fingers). This will give you wrist drop (same symptom as Saturday Night Palsy but NOT the same thing) where you have a limp dick of a hand. You basically can't extend you shit. You'll also have loss of sensation over the back of your arm, the forearm, and the back of the hand.
The artery impacted is the deep brachial artery, which is a bit of a big boy. So let's hope you didn't tear it like a cheap condom or you could be fucked.

Supracondylar (Distal Fracture)
These are most common in pediatric patients, and a FOOSH injury (fall on outstretched hand). The nerve that can be damaged is the median nerve, which supplies the wrist flexors, thumb, and some intrinsic hand muscles. The artery impacted is the brachial artery, which is a big important one.
One complication of this fracture is due to swelling. This causes compartment syndrome, which can compress the brachial artery, leading to ischemia of the flexors. Median nerve damage adds to this issue and you basically get a contraction of the flexor compartment. The muscles will shorten and scar, making this a big fucking problem. This will present as flexed fingers and wrist that are stuck that way. Extension without pulling your hand around will be almost impossible.

Medial Epicondyle
This is where all your forearm flexors attach (the extensors attach to the humerus and lateral epicondyle). A fracture here is most common in pediatric patients, and is usually from direct trauma. The nerve damaged is the ulnar nerve (if you hit the medial side of your elbow, your funny bone is the ulnar nerve being hit). When this nerve doesn't work, you get sensory loss on the pink and ring finger (but only the pinky side of the ring finger - if you ever have your pinky go numb due to sleeping weird, you can feel the change in sensation on the different sides of your ring finger). There will also be decreased grip strength (as the pinky and ring finger won't flex), and difficulty splaying or adducting the fingers.

#medicine#med studyblr#med student#medical school#med school#medical writing#whump writing#anatomy#fractures#injury
7 notes
·
View notes
Note
Do you have a favourite muscle? (mines probably the sternocleidomastoid)
YES i do omg my favorite muscle is either the sartorius (if only for the name) or the general forearm extensor compartment. the forearm rlly has the hottest muscles, to ME
18 notes
·
View notes
Text
Muscles of Lower Leg
Key things to know about the muscles of the lower leg that will get you through 99% of questions on the muscles of the lower leg:
Compartments opposite to forearm (anterior = extension; posterior = flexion)
Same concept as the arm: extrinsic (crude, powerful movements) in the leg, intrinsic (fine, delicate movements) in the foot
The arm and leg have more in common than you think! Sometimes it helps to think of them the same way (Foot=Hand, Wrist=Ankle, etc)
Three main compartments in the leg: Anterior, Posterior, Lateral (NO MEDIAL) = Only 3 nerves to learn (one per compartment)
(remember break things down into their compartments and layers it makes it way easier to learn)
Anterior = Only 4 Muscles! Think about what you need your foot to do, like lifting your toes (Extensor Digitorum Longus, Extensor Hallucis Longus) and Tibialis Anterior which makes sense because it’s the anterior compartment and rests against the tibia (ALL DEEP FIBULAR NERVE)
(the 4th muscle of the anterior compartment is Fibularis Tertius and it’s a weird little bastard because its function is actually grouped together with the muscles in the lateral compartment, it’s the secret third muscle of the lateral compartment, hence the name tertius)
Lateral = Only 2! Fibularis Longus and Fibularis Brevis (remember the string, if you pull on the outside part of your leg, your foot everts) (BOTH SUPERFICIAL FIBULAR NERVE)
(we are all just puppets on a string dancing to the whims of the examiner)
Posterior = 2 Layers: Superficial and Deep (ALL TIBIAL NERVE)
Superficial = Gastrocnemius (I don’t have a way to learn this name but it’s the double bulgy one you see in cyclists calves), Soleus (named because it looks like a flat, filleted fish), and Plantaris (which you guessed it, does plantarflexion)
Deep = Tibilais Posterior, Flexor Digitorum Longus, Flexor Hallucis Longus (literally just the opposite of anterior, like a mirror image) and my personal fav Popliteus (it unlocks the knee with a ‘pop’)
(where there is anterior there must be posterior, where there is deep there must be superficial, where there is medial there is lateral, where there is longus there is brevis, etc)
[i know there isn’t a medial compartment in the lower leg, REMEMBER THERE IS ALWAYS AN EXCEPTION TO MAKE YOUR LIFE MORE DIFFICULT]
Dorsiflexion = pulling foot up (pulling dorsum of foot towards you) (FLEXION OF ANKLE)
Plantarflexion = pointing foot down (pushing plantar of foot away from you) (EXTENSION OF ANKLE)
i would say happy learning and anatomy is great but i wouldn't describe myself as happy when i was first learning it
#anatomy#education#medical school#medical student#university#biology#science#legs#linguistics#higher education#back at it with the crayons
1 note
·
View note
Text
De Quervain’s Disease
About De Quervain Disease
De Quervain's disease, sometimes referred to as mother's thumb or gamer's thumb, is a common wrist pathology. De Quervain's disease is thought to be caused by thickening of the synovial sheath containing the tendons of the extensor pollicis brevis (EPB) and abductor pollicis longus (APL), which causes irritation of the muscles and causes pain and swelling over the radial side of the wrist in patients along with increased difficulty gripping objects. The exact mechanism underlying this condition is unknown. The disorder known as "De Quervain tenosynovitis," after Swiss surgeon Fritz de Quervain, is characterised by tendon entrapment that affects the wrist's first dorsal compartment.
De Quervain disease Causes
De Quervain disease causes have been linked to myxoid degeneration with fibrous tissue deposits and enhanced vascularity rather than acute inflammation of the synovial membrane, while the precise origin of the condition is unknown. The abductor pollicis longus and extensor pollicis brevis tendons become painfully ensnared in the thickened tendon sheath caused by this deposition. It is linked to repetitive wrist motions, particularly those involving simultaneous extension, radial wrist deviation, and thumb radial abduction. Mothers of newborns who frequently lift their babies as their wrists shift from ulnar to radial deviation and their thumbs are considered the classic patient population.
Epidemiology - According to one study, the peak prevalence of de Quervain tenosynovitis occurs in people in their forties and fifties, accounting for 0.5% of cases in males and 1.3% in women. People having a history of medial or lateral epicondylitis may be more susceptible to the illness. There are two major risk factors for the disease: being pregnant and working physically.
Clinical Anatomy of Disease
Both the abductor pollicis longus (APL) and extensor pollicis brevis (EPB) tendon are impacted by De Quervain's syndrome. These muscles originate from the dorsal aspect of the forearm and extend to the lateral side of the thumb via an extensor retinaculum and processus styloideus radii fibrous-osseous tunnel.
Source: https://harleyclinic.com/treatments/hand-and-upper-limb/de-quervain-syndrome/
The increased stress over the tendon sheaths causes fibrocartilage to develop, which thickens the tendon. The tendon sheaths are covered in neovascularization. In this syndrome, the tendons also exhibit myxoid degeneration.
De Quervain Disease Symptoms
Patients present with radial-sided wrist pain typically worsened by thumb and wrist motion. The condition may be associated with pain or difficulty opening a jar lid. Tenderness overlying the radial styloid is usually present. If present, the swelling over the wrist is generally seen proximal to the radial styloid. The typical patient population is a pregnant woman in the third trimester or a breastfeeding mother who holds her child repeatedly.
De Quervain Disease Diagnosis
De Quervain tenosynovitis is diagnosed clinically from the typical history and physical examination findings. Plain radiographs can help rule out other possible causes of radial wrist discomfort, such as thumb carpometacarpal joint osteoarthritis, but they cannot be used to confirm the diagnosis. Different clinical tests that are provocative have been described for de Quervain tenosynovitis. The patient must place their thumb in palmar flexion for the Finkelstein test while the examiner performs ulnar deviation of the wrist. Sharp discomfort that is felt at the first dorsal compartment along the radial wrist indicates a positive test. In order to perform the Eichhoff test, the patient must grip their thumb with their other fingers while bending their wrist in the direction of the ulna. If the test is positive, this will cause a severe shooting pain over the radial aspect of the wrist. Another provocative clinical test documented for this illness is the WHAT test, which causes wrist hyperflexion and thumb abduction. The following differential diagnoses can resemble this condition: first carpometacarpal joint osteoarthritis fracture of the scapula styloid fracture radially Radial nerve neuritis in the sensory branch (Wartenberg's syndrome) Syndrome of intersections Thumb trigger
Treatment/ Management of De Quervain’s disease
De Quervain tenosynovitis has the potential to resolve on its own and may not require medical attention. The most common nonsurgical treatment options for patients with ongoing symptoms are corticosteroid injections, systemic anti-inflammatories, and splinting. One or two corticosteroid injections have been shown to offer almost total relief in 52% to 90% of individuals. Acupuncture, therapeutic ultrasound therapy, and laser therapy are a few more nonoperative treatment techniques that have been reported; nevertheless, there is neither a consensus nor good data on these therapies' efficacy. An operation may be necessary if corticosteroid injections do not relieve symptoms or if they return.
Conclusion
For De Quervain's tenosynovitis to be effectively managed, the patient will need to follow a highly personalized, impairment-driven treatment plan. Early splinting during the acute phase will help the patient avoid aggravating the tissues and enable them to carry out tasks necessary for work and self-care. The patient must be informed about the timelines for tissue repair as well as the significance of avoiding activities that exacerbate their symptoms. Exercise therapy progresses from isometric to eccentric to concentric inner range exercises. A patient should be pain-free prior to advancing to the subsequent strengthening phase.
#De Quervain’s disease#De Quervain’s disease causes#De Quervain’s syndrome symptoms#De Quervain’s diagnosis#De Quervain’s syndrome treatments
0 notes
Text
Illustration of Intersection Syndrome
"Many tendons pass through the wrist in six anatomical tunnels called extensor tendon compartments. The NCBI notes that intersection syndrome (IS) occurs when tendons from the first compartment cross over and rub against those from the second."
TennisElbowClassroom's insight:
Intersection Syndrome (IS) is very similar to De Quervain's Tenosynovitis and can occur simultaneously.
The injury occurs where the tendons involved with De Quervain's (abductor pollicis longus and extensor pollicis brevis) in the first compartment pass obliquely over the tendons in the second compartment (which contains the extensor carpi radialis tendons).
0 notes
Photo

EXTENSORY COMPARTMENTS (6 COMPARTMENTS)
COMPARTMENT 1
APL (abductor pollicis longus)
EPB (extensor pollicis brevis)
COMPARTMENT 2
ECRB (extensor carpi radialis brevis)
ECRL (extensor carpis radialis longus)
COMPARTMENT 3
EPL (extensor pollicis longus)
COMPARTMENT 4
EDC (extensor digitorum communis)
EI (extensor indicis)
COMPARTMENT 5
EDM (extensor digiti minimi)
COMPARTMENT 6
ECU (extensor carpi ulnaris)
* Extensor indices is medial to digitorum
2 notes
·
View notes
Text

THE MOST COMMON BACK AND HIP PAIN
This pattern of muscle co-contractions happens when there is a weakness in the Glut Max and Erector Spinae muscle group. The Quadratus Lumborum contracts as an auxiliary back extensor to brace the low back. This can result in a hip hike and narrowing of that side of the low back.
Commonly the lateral stabilization of the hip is compromised or inhibited also, and the external rotators jump in to brace stability for both the Erector Spinae and the lateral hip.
The lateral Hamstring dominates the back of the leg and its tendon is chronically short as part of the whole kinetic chain of dysfunction resulting from the recruitment of the QL to support the back.
The external rotators of the hip are overused to propel us forward (lacking the function of Glut Max). This makes the leg swivel out as you walk. Fixation of the external rotators of one hip will inhibit the rotators of the opposite hip. Clients often complain of the pain being in the weak hip and SIJ as it is unsupported by either that QL or external rotators.
Next in line is the excessively tight tendon of the lateral hamstring. This can be observed in a bare leg by the upward slant of the crease on the back of the knee compartment. This pattern results in a weak medial line of support for the leg. Vastus Medialis is commonly inhibited, as is the Medial Hamstring origin and sometimes the adductor.
Muscle testing allows you to verify what is going on with the preferred muscle patterns through the kinetic chain down the lateral hip and leg.
(The Neuromuscular Reprogramming Network)
3 notes
·
View notes
Text
anterior compartment of leg tidbit
*slaps top of the leg like a car salesman* roight what’ve we got here, laddies?
the shin, that’s right.
did you know that there’s a condition dedicated to us medico first years? ‘Fresher’s Syndrome’ is so named bc it tends to occur in new med students or army recruits: bottom of the food chain, made to run around at the beck and call of any and everyone with even the tiniest bit of seniority.
all that running makes us overuse the muscles of our anterior compartment (namely -- in order of medial to lateral -- tibialis anterior, extensor hallucis longus, extensor digitorum longus, peroneus tertius) causing them to swell up in the tight compartment.
venous return is disrupted
accumulation of fluid in compartment occurs
pressure in the compartment increases and anterior tibial artery gets compressed
reduces blood flow to the muscles
causes ischaemia (lack of blood supply) and pain
so expect pain -- the emotional and physical kind -- sooner or later :)
3 notes
·
View notes
Text
HOW TO TARGET THE QUADS
The quadriceps femoris is a hip flexor and a knee extensor. It consists of four individual muscles; three vastus muscles and the rectus femoris. They form the main bulk of the thigh, and collectively are one of the most powerful muscles in the body. It is located in the anterior compartment of the thigh.
Quadriceps femoris, with different muscles in different colors.
rectus femoris - blue
vastus lateralis - yellow
vastus intermedius - green
vastus medialis - red

I will be guiding you through exercises that target those four muscles on the thigh and it very effective. Have someone ever tried the goblet squat or leg extensions? if yes how have you turned your feet. The way your feets are turned help target a particular muscle on the quad.
Goblet Squat
Engage your core and look straight ahead—you want to keep your back neutrally aligned and your eyes facing straight ahead throughout the squat. Press your hips back and begin bending your knees to perform the squat. Inhale as you perform this downward phase. Keep the kettlebell close to your body during the movement. Slightly turn your feet out and there, you will be hitting right on the VASTUS LATERALIS and all these are based on personal experience at the gym. You must try doing it .
Leg Extensions
The leg extension is an exercise designed to focus almost exclusively on your quads. Compared to the traditional straight up feet. Try switching feet turned in and feet turned out and that is definitely hitting a particularly muscle on the thigh.
Most often you do this exercises after you are done with your big squats I just want all of you out there willing to hit the quad to just try the feet variation and feel the experience.
I'm gon' bring more on this, videos and pictures as well. Watch out !!!
NO PAIN NO GAIN
2 notes
·
View notes
Photo

MUSCLES IN THE ANTERIOR COMPARTMENT OF THE LEG - PART 2 ⠀ [CADAVER DISSECTION ANATOMY] ⠀ There are four muscles in the anterior compartment of the leg; tibialis anterior, extensor digitorum longus, extensor hallucis longus and fibularis tertius. Collectively, they act to dorsiflex and invert the foot at the ankle joint. The extensor digitorum longus and extensor hallucis longus also extend the toes. The muscles in this compartment are innervated by the deep fibular nerve (L4-S1), and blood is supplied via the anterior tibial artery. ⠀ In this post we will focus on extensor hallucis longus and fibularis tertius. ⠀ Extensor Hallucis Longus (Video 1-3) The extensor hallucis longus is located deep to the EDL and TA. It originates from the medial surface of the fibular shaft. The tendon crosses anterior to the ankle joint and attaches to the base of the distal phalanx of the great toe. Actions: Extension of the great toe & foot dorsiflexion. ⠀ Fibularis Tertius (Video 4,5) The fibularis tertius muscles arises from the most inferior part of the EDL. It is not present in all individuals, and is considered by some texts as a part of the extensor digitorum longus. Because one part of the EDL attaches onto the 5th metatarsal and not an actual toe („digit“), it is renamed as a separate muscle. The third fibularis muscle, in other words, fibularis tertius. It originates with the extensor digitorum longus from the medial surface of the fibula. The tendon descends with the EDL, until they reach the dorsal surface of the foot. The fibularis tertius tendon then diverges and attaches to metatarsal V. Actions: Foot eversion & dorsiflexion. ⠀ #anatomy #biomechanics #functionalanatomy #doc #tensegrity #anatomia #chiropractic #osteopathy #physicaltherapy #physiotherapy #acupuncture #dryneedling #hip #muscles #fascia #yoga #joints #yogaanatomy #squats #function #triggerpoint #physiology #pilates #medicine #crossfit #human #sport #therapy #doctor #training (hier: Los Angeles, California) https://www.instagram.com/p/B9kDI1Wh54N/?igshid=1dwstsgnwh74f
#anatomy#biomechanics#functionalanatomy#doc#tensegrity#anatomia#chiropractic#osteopathy#physicaltherapy#physiotherapy#acupuncture#dryneedling#hip#muscles#fascia#yoga#joints#yogaanatomy#squats#function#triggerpoint#physiology#pilates#medicine#crossfit#human#sport#therapy#doctor#training
6 notes
·
View notes
Text
The top 6 reasons we like hills for training ankle rocker and hip extension
1. Hills do not cost money and are almost always readily available : )
2. Being outside is good for your health
3. Hills do not pull the hip into extension and place a stretch (pull) on the anterior hip musculature including the rectus femoris, iliopsoas and iliacus. This causes a slow stretch of the muscle, activating the muscle spindles (Ia afferents) and causing a muscle contraction via the stretch reflex. This will inhibit the posterior compartment of hip extensors (especially the glute max) through reciprocal inhibition, making it difficult to fire them.
4. A hill does not force your knee into extension, eliciting a stretch reflex in the hamstrings like a treadmill does
5. A hill naturally puts the ankle into dorsiflexion, and, along with active pulling up of the toes, helps you to get more into your anterior compartment and eliminates the tendency of the ankle being pulled into dorsiflexion (like with a treadmill) which would initiate a stretch reflex in the gastroc/soleus and long flexors.
6. The increased hip flexor requirement of going uphill gives you more opportunity to engage the abs before the psoas and rectus femoris/TFL and on the stance phase leg, you can get an increased stretch of those muscles
Tips for picking the right hill and using it to your advantage
When just starting out, try and pick an incline that does not exceed the ankle dorsiflexion available to the patient/client
It’s OK if it’s uncomfortable, but not if its painful
Concentrate on pulling up the toes and dorsiflexing the ankle
Squeeze your glute at heel strike and toe off
leave your stance phase heel on the ground as long as possible
Place your hands on your abs and concentrate on activating them PRIOR to flexing your hip
Dr Ivo Waerlop, one of The Gait Guys
#walkinghills #traininganklerocker #thegaitguys # increasinghipextension
#hill#training#walking#glute#gluteal activation#activation#gluteus maximus#hip#flexor#the gait guys#gait analysis
3 notes
·
View notes
Text
10 Best Barbell Forearm Exercises for Stronger Grip and Bigger Arm

Do you want to improve your grip strength and get stronger forearms? Whether you are an athlete, weightlifter, or someone who just wants to get a bigger forearm and stronger grip, you should do barbell forearm exercises. Strong forearms are not only aesthetically pleasing, but also play a crucial role in enhancing your overall strength and grip. It not only helps you lift heavier weights, but it also improves your performance in different sports and activities. The forearms play a pivotal role in everyday tasks like lifting, carrying, and gripping, making their strength and conditioning vital for overall performance. In this article, we'll share with you the following: - Forearm muscles - Benefits of strong forearm - Best barbell forearm exercises - Valuable tips to maximize your forearm gains. - Forearm training program
Forearm Muscles
The forearm is a complex area of the upper limb that contains numerous muscles responsible for various movements and functions. In order to effectively target the forearm, it is essential to understand the forearm muscles. Let's delve into the key muscles of the forearm: Flexor Muscles - Flexor Digitorum Profundus: This muscle runs along the forearm and is responsible for flexing the fingers. - Flexor Digitorum Superficialis: Positioned above the flexor digitorum profundus, this muscle flexes the fingers as well. - Flexor Carpi Radialis: Located on the inner side of the forearm, this muscle flexes and abducts the wrist. - Palmaris Longus: this muscle aids in wrist flexion and tenses the palmar aponeurosis. Extensor Muscles - Extensor Digitorum: Positioned on the back of the forearm, this muscle extends the fingers. - Extensor Carpi Ulnaris: Located on the outer side of the forearm, this muscle extends and adducts the wrist. - Extensor Carpi Radialis Longus and Brevis: These muscles extend and abduct the wrist. Pronator and Supinator Muscles - Pronator Teres: Positioned on the inner side of the forearm, this muscle pronates the forearm (rotates it to face downward). - Pronator Quadratus: Located near the wrist, this muscle assists in pronation. - Supinator: Situated on the outer side of the forearm, this muscle supinates the forearm (rotates it to face upward). Brachioradialis Brachioradialis is one of the muscles that comprise the posterior compartment of the forearm. It is the most superficial muscle of the radial side of the forearm. Training the Brachioradialis is essential for building bigger forearms and for producing powerful pulling movements like chin-ups and rows. Read the full article
0 notes
Text
Compartments of the lower leg

Both layers are innervated by the tibial nerve and typically act to plantarflex the foot. The posterior compartment is slightly more complex, in that it is split into superficial and deep layers. Notice how deep the extensor hallucis longus is compared to the tibialis anterior and extensor digitorum longusĬreative commons source by OpenStax College, edited by Sachin Sudhakaran It is responsible for the extension of the hallux/big toe but also contributes to dorsiflexion of the foot.ĭiagram - Anterior compartment of muscles in the leg, highlighted. As the name suggests, these act to extend the toes, whilst also aiding dorsiflexion.Įxtensor Hallucis Longus originates from the medial fibula and inserts into the distal phalanx of the big toe. It also acts to invert the foot.Įxtensor Digitorum Longus originates from the lateral condyle of the tibia and forms four tendons, which insert into a digit (with exception of the hallux/big toe). It attaches to the medial cuneiform (one of the bones in the foot) and acts to dorsiflex the foot. Tibialis Anterior is found on the lateral surface of the tibia, where it originates. Muscles in the anterior compartment act to dorsiflex the foot and are innervated by the deep fibular nerve (a branch of the common fibular nerve). For more information, please check out our Anatomical Terminology Article. It is also very important when studying muscles that you are comfortable with anatomical terminology, as a lot is used in these articles. Whilst there are many muscles in the leg, they can be compartmentalised into anterior, lateral and p osterior fascial compartments. Muscles of the lower leg typically act at the ankle joint and are innervated by branches of the sciatic nerve.
0 notes
Text
Radia nerve

#Radia nerve skin#
It gives sensory supply to dorsal aspect of hand, dorsal aspect of thumb, index finger, middle finger and lateral side of ring finger except the nail beds, which are supplied by proper digital branches of median nerve. It crosses brachioradialis to enter posterior of forearm near the back of the wrist and supply dorsum of hand.
The superficial branch of the radial nerve is widely separated from the radial artery in the upper one third of the forearm, closely related to radial artery in the middle third of the forearm, and in the lower third, it descends in the forearm under the tendon of brachioradialis.
In the forearm, it is divided into a superficial branch (primarily sensory) and a deep branch (primarily motor). The radial nerve also gives articular branches to supply the elbow joint. In the radial sulcus, it gives off lower lateral cutaneous nerve of the arm and posterior cutaneous nerve of the forearm.
#Radia nerve skin#
Ībove the radial sulcus, the radial nerve gives off posterior cutaneous nerve of the arm which supplies the skin at the back of the arm. After it emerges out from the radial sulcus, it supplies the brachialis, brachioradialis and extensor carpi radialis longus. Radial nerve gives out muscular branches to supply the long head, medial head, and lateral head of triceps brachii muscles before and during its course in the radial sulcus. Then, it descends down to cross the lateral epicondyle of the humerus where the nerve terminates by branching itself into superficial and deep branch which continues into cubital fossa and then into the forearm. It travel downwards together with profunda brachii artery, between the lateral and medial heads of triceps brachii until it reaches the lateral side the arm at 5 cm below the deltoid tuberosity where it pierces the lateral intermuscular septum to reach the anterior compartment of the arm. In the arm, it runs behind the brachial artery and then enters the lower triangular space to reach the radial sulcus of back of the humerus. From the brachial plexus, it travels behind the third part of the axillary artery (part of the axillary artery distal to the pectoralis minor). The radial nerve originates from the posterior cord of the brachial plexus with root values of C5 to C8 and T1. It goes through the arm, first in the posterior compartment of the arm, and later in the anterior compartment of the arm, and continues in the posterior compartment of the forearm. The radial nerve originates as a terminal branch of the posterior cord of the brachial plexus. Radial nerve of the right axilla, posterior view This nerve was historically referred to as the musculospiral nerve. The radial nerve divides into a deep branch, which becomes the posterior interosseous nerve, and a superficial branch, which goes on to innervate the dorsum (back) of the hand. The radial nerve and its branches provide motor innervation to the dorsal arm muscles (the triceps brachii and the anconeus) and the extrinsic extensors of the wrists and hands it also provides cutaneous sensory innervation to most of the back of the hand, except for the back of the little finger and adjacent half of the ring finger (which are innervated by the ulnar nerve). It originates from the brachial plexus, carrying fibers from the ventral roots of spinal nerves C5, C6, C7, C8 & T1. It innervates the medial and lateral heads of the triceps brachii muscle of the arm, as well as all 12 muscles in the posterior osteofascial compartment of the forearm and the associated joints and overlying skin. The radial nerve is a nerve in the human body that supplies the posterior portion of the upper limb.
0 notes
Photo


ANATOMICAL SNUFFBOX
Boundaries
Medially - Extensor pollicis longus (3rd compartment)
Laterally - Abductor pollicis longus & extensor pollicis brevis (1st compartment)
CONTENTS
Radial artery
Cephalic vein
Trapezium
Scaphoid
3 notes
·
View notes
Photo

HYPERMOBILE SACROILIAC JOINT PT 2 IN Part 1 We looked at the fixated muscles in the extensor compartment (particularly the right hip), that are contributing to the lack of functional support for the left SIJ. At the end of our short demo we saw no further inhibition in the right hip. The PT was focusing on conditioning the weak lateral muscles in the right hip, but it's the LEFT SIJ that's unstable. The next step in correcting this left SIJ pattern is to test the relationships between the hip flexors and back extensors and lateral stabilizers. Here's what we found... There is indeed a tightness on the right contributing to the weakness on the left. This pattern is exceedingly common. Either Iliacus can torque the pelvis and weaken the back extensors. Testing the back extensors, hip extensors, QL for side bending and Glut Med/Min Lateral stabilization and SIJ stabilization revealed and the right Iliacus muscle AND the Rect Femoris were contributing to the persistent weakness of the left SIJ. Whenever your client is exhibiting persistent weakness in the back muscles, ALWAYS LOOK TO EXCESSIVE SHORTNESS IN THE ILIACUS. Even if you don't know muscle testing if you notice a tight Quad and Hip Flexor, you can help the back by lengthening the front of the hip joints. Passive stretching is not as good as tissue lengthening followed by a regime of stretching. The challenge with stretching tight muscles is that they are short fo a reason. Find out with NeuroMuscular Reprogramming. Enrollment in NMR comes with a FREE video of Manual Muscle Tests for the whole body! Here's my favorite stretch for the front of the hips...It starts easy and doesn't require balancing while stretching. No extra points for no hands! The key is one knee behind and the other knee dipped.
[NeuroMuscular Reprogramming]
#NMR#Neuromuscular Reprogramming#Jocelyn Olivier#SIJ#iliacus#Sacroiliac Joint#articles#Body Alive#Structural Integration Atlanta
2 notes
·
View notes