#how to choose health insurance
Text
How to Choose the Right Insurance for Your Needs
Insurance is an essential component of economic planning that affords safety in opposition to surprising events, ranging from accidents to herbal disasters. With a variety of sorts of insurance plan available, choosing the proper policies to meet your desires can be overwhelming. However, appreciation the key elements and concerns can assist you make knowledgeable choices tailor-made to your…

View On WordPress
#auto insurance#best health insurance#car insurance#health insurance#health insurance 101#health insurance for self employed#health insurance for small business#health insurance marketplace#how to choose health insurance#how to choose the right insurance plan#how to choose the right life insurance#how to lower insurance#how to pick the right life insurance#how to pick the right life insurance policy#how to save money on health insurance#insurance
0 notes
Text
How to choose a insurance plan In 2024
How to choose a insurance plan In 2024: Choosing the right insurance plan requires careful consideration of various factors to ensure that it aligns with your needs and provides comprehensive coverage. Here’s a step-by-step guide on how to choose an insurance plan:
How to choose a insurance plan
In the labyrinth of insurance options available today, finding the perfect insurance plan requires a…

View On WordPress
#best health insurance#choose a health insurance plan#health insurance#health insurance explained#health insurance marketplace#health insurance plan#how to choose a health insurance plan for your family#how to choose a health insurance plan?#how to choose health insurance#how to choose health insurance plan#how to choose health insurance plan 2021#how to choose health insurance plan from employer#how to choose the best health insurance plan#insurance
0 notes
Text
i love just pretending everything is fine always as a way to cope with the fact that everything is in fact not fine and i’m struggling more than i can possibly express
#i can’t afford for things to not be fine#like financially. literally.#idek how i’m going to get to my brother’s fucking wedding#i’m missing my BEST FRIEND OF TWENTY YEARS’ first baby shower because i can’t fucking afford to go#idk if i can even buy her gifts#i have no health insurance because that went away with my last job#and 3+ months of job searching has given me literally nothing. i haven’t even gotten any interviews#state insurance won’t qualify me because i got a small 401k payout a few months ago but i’m trying again now#but even if i get state insurance i can’t fucking afford copays so what’s the point!#i have to choose between important bills or the most minimal groceries every fucking week when i get paid from the temp part time job i have#but no. everything is fine#personal post
8 notes
·
View notes
Text
being an adult sucks man
#i'm trying to choose insurance at my new job and i am SO incredibly lucky to have choices to be clear#like i get that while i'm stressed as hell i am REALLY lucky to have options#but trying to figure out the best plan when you have so many health issues is kind of a disaster#like okay well will this cover a cardiologist and a pulmonologist and a gastroenterologist and a urologist and a nephrologist and my GP#and any testing that i need done and will it make paying for er visits not awful and if i get referred to anew doctor by these people will#THAT be covered and will i have access to versions of those doctors who specifically understand congenital shit and also understand all my#comorbidities and how all my disablities imoact each other and also if choose wrong i'm stuck with i tfor a year
3 notes
·
View notes
Text
being an american on here is wild because i keep seeing posts from other americans that describe things they've experienced and say that it is universal among americans and it'll be stuff i've either never heard of or know for a fact isn't true. maybe it's pretty common in your state or the states surrounding you, but there's so much stuff i see that i can not relate to whatsoever, and i've never left the states.
#liv won't shut up#i saw something about insurance today#said that optometry is never covered by health insurance#& i'm sitting here like dude the insurance my dad gets from work benefits (so it's not the best in a lot of ways) has covered our optometry#costs for 3 people for years. & actually idk the specifics but it seems like its not that bad of a plan. we usually buy more than a years#supply of contacts for me (only like a month more) and our insurance covers pretty much all the costs. i have to choose contacts or glasses#every year but my prescription has been very stable so i only have to get new glasses if they're damaged beyond repair#again it's not my insurance i'm covered by my parents & they dont tell me all the details so idk how much theyre paying for it. might be a#lot & we're doing it bc it's one of my dads benefits. but any way the point is that so many americans will say things like every single#person living in america understands & 90% of the time i have no frickin clue what they're on about or i have experienced the exact opposit#it's just interesting that this happens. & it happens all the time. 'all american schools require learning another language' no the frick#they do not. lots do (and this may be a state requirement thing wouldnt be surprised) but not all. wasnt required for me it was just highly#encouraged & i got a different type of diploma for my world lang classes (my hs had a few types of diplomas based on different classes/#grades/etc idk if thats a common thing or not). another good example are train posts actually. i can tell theres a divide between beliefs#on trains based on state & thats bc public transportation is not as feasible in some states. i've spent a good portion of my life living in#small towns or visiting small towns (family) & yeah public transportation in middle of nowhere wyoming and middle of nowhere idaho is a lot#less feasible than the east coast. those are places of vast nothingness other than a few towns every once in a while never exceeding 20000#(ID) or 500 (WY). & even in larger towns it seems like a lot of western states are more spread out. so a subway or other train isnt very#helpful (unless you want to do long distance trains then those could maybe work the issue is that costs money & idk if itd be used enough#to make it worth it for a gov/actually work well) & this is more of a rural/urban issue but that aligns with states as well in a lot of way#oh another one is about facs classes. so in a lot of places facs is being defunded or removed from curriculum. same with arts classes. &#this is becoming a problem in many places! but when ppl are like 'these classes are being taken away everywhere in america' i just sit#there thinking about my state requiring facs in middlie & high school (i believe but things could have changed) plus i had to take like 3#semesters of art (idk if thats state or school or district required) & thereve been talks of raising that requirement. & they add more opt#every year. i was helping my younger brother with his schedule & theres all sorts of stuff that wasnt there before. he has way more options#to fulfill that requirement than i did. & i'm not saying that this isnt a problem it is a problem most places but every state has different#legislation on this so for now at least lots of schools are required to have these classes. & i've probably lost my point by now but it is#odd that i see this so often. that most of posts about america i see are different from what i've experienced. idk maybe the states i've#lived in are weird but youd think that this wouldnt happen to me a lot would you? like sometimes yeah but this happens a lot.#my guess is that a lot of these things are very true if you talk about a specific region or state. but then ppl assume its an american
2 notes
·
View notes
Text
Insurance for *FAMILY* with Senior Citizens
Selecting the best health insurance plan can be a daunting task. After all, there are over 30 health insurance companies in India, dozens of plans with scores of health insurance benefits within them. In this video,
I will explain about "How to decide the best health insurance plan in 2024 for family?" Whether you're looking for individual, wife and kids, family members or senior parents, this guide will definitely help you in deciding the factors.
The steps include:
1. Identifying your top priorities for buying health insurance i.e. why are you interested in buying a health insurance policy?
2. Whom to cover in your health insurance policy.
We've also covered a detailed explanatory video on "How To Choose The Best Health Insurance Plan". You can check the video over this link - https://youtu.be/AyFypoXoj18
#health insurance for senior citizens#health insurance for wife#Health insurance for senior parents#Health insurance for family#Insurance for Family#insurance for senior citizens#Insurance for senior parents#Insurance for parents#Why buy health insurance for family#Why buy health insurance for senior citizens#How to choose best health insurance for family#Best health insurance for family#best health insurance for senior citizens#nidhiverma22#algatesinsurance
0 notes
Text
Finding the Best Health Insurance Plan in India: A Comprehensive Guide
In today’s fast-paced world, where health uncertainties can arise without warning, having a robust health insurance plan is not just an option but a necessity. With the healthcare sector in India witnessing rapid advancements, the market is flooded with a myriad of health insurance options, making it crucial for individuals to find a plan that best suits their needs and budget. This comprehensive guide aims to simplify your search for the best health insurance plan in India, ensuring you and your family are well-protected.
youtube
Understanding Health Insurance
Health insurance is a contract between an individual and an insurance company. Under this agreement, the insurer agrees to cover a portion or the entirety of the insured person’s medical expenses in exchange for regular premium payments. It acts as a safety net, shielding you from the potentially crippling costs associated with medical treatments, doctor visits, and hospitalization.
Types of Health Insurance Plans
Health Maintenance Organization (HMO): HMO plans require you to select a primary care physician (PCP) and obtain referrals from them to see specialists. These plans often have lower premiums but a more limited choice of healthcare providers.
Preferred Provider Organization (PPO): PPO plans offer greater flexibility in choosing healthcare providers. You can see specialists without referrals, but your out-of-pocket costs may be higher.
Exclusive Provider Organization (EPO): EPO plans combine aspects of HMO and PPO plans, with a limited network of healthcare providers but no need for referrals. They typically have lower premiums and out-of-pocket costs.
Point of Service (POS): POS plans require you to choose a PCP but allow you to see out-of-network specialists with referrals. They offer a balance between cost and flexibility.
High Deductible Health Plan (HDHP): HDHPs have higher deductibles and are often paired with Health Savings Accounts (HSAs) to help you save for medical expenses.
Key Components of Health Insurance
Premium: This is the amount you pay to the insurance company for your coverage, typically on a monthly basis.
Deductible: The deductible is the amount you must pay out of pocket before your insurance coverage kicks in.
Copayment and Coinsurance: These are the costs you share with your insurance company for medical services. Copayments are fixed, while coinsurance is a percentage of the total cost.
Network: The network comprises the doctors, hospitals, and other healthcare providers contracted with your insurance company. Staying in-network often results in lower out-of-pocket costs.
The Benefits of Health Insurance
Financial Security: Health insurance ensures that you won’t be financially devastated by unexpected medical bills.
Access to Quality Care: It allows you to receive medical care promptly, improving your overall health outcomes.
Preventive Care: Many health insurance plans cover preventive services like vaccinations and screenings at no cost to you.
Wellness Programs: Some insurance plans offer wellness programs and discounts to promote a healthy lifestyle.
Peace of Mind: Knowing that you are covered in times of illness or injury brings peace of mind to you and your family.
Choosing the Right Health Insurance
When selecting a health insurance plan, it’s crucial to assess your individual needs, budget, and preferences. Consider factors such as your preferred doctors, medical history, and the health needs of your family.
In conclusion, health insurance is an essential part of financial planning and ensuring access to quality healthcare. It’s a safeguard against the unpredictable nature of health-related expenses. By understanding the various types of plans and key components, you can make an informed decision to protect your health and financial well-being. Remember, a well-chosen health insurance plan is an investment in your future. if you want to know more about How to choosing a right Insurance in India just ping our whatsup number to clarify.
#How to choosing a right Insurance in India#Right Health Insurance#best health insurance plan#best health insurance plan in India#Youtube
0 notes
Text
Who'll pay for claims if Insurance Company goes bankrupt?
If an insurance company is declared insolvent or bankrupt, then IRDAI will guaranty an association and guaranty fund swing into action. The association will transfer the insurer’s policies to another insurance company or continue providing coverage itself for policyholders. So it’s important for policyholders to continue paying premiums if their insurer is taken over by the state.
#Insurance Company Bankruptcy#Bankrupt Insurance Companies#Insurance Company Insolvency#What Happens If Your Insurance Company Goes Out Of Business?#What Will Happen When Insurance Company Goes Bankrupt in India?#Insurance Company Bankruptcy Causes.#best term insurance#best term life insurance#how to choose term insurance plan#what is term insurance#best health insurance plans#how to buy health insurance
0 notes
Text
.
#personal life/rant warning#i cant take the bullshit of choosing between paying my bills or paying for a doctors visit#like at this point with the price of everything i cant do both#this month i finally got enough to go to the doctor but i won’t be able to afford the meds for who knows how long#all i can manage to afford is to update the prescription and even then i’m falling through on other things#i cant buy groceries. im putting my cats food and litter above my basic needs. i cant even take my gf on a date and pay for it all#rent is barely being put together#and i cant complain abt this to anyone i know bc it just feels manipulative#like im asking for money#idk i just want to be able to take my meds and eat decent food and not want to ball my eyes out every time i check my bank account#my insurance doesn’t cover the prescription bc it’s hrt but i have been off t since xmas and my mental health has been so fucking bad#i just cry and fall back on unhealthy coping mechanisms and try to put on a smile for everyone so they don’t feel pitty for me#some me times
1 note
·
View note
Text
How to Choose a Health Insurance Company for Your Needs
How to Choose a Health Insurance Company: Certainly, let’s delve deeper into each of the points mentioned in the guide on how to choose the right health insurance company:
In a world where health uncertainties are a constant reality, the importance of securing comprehensive health insurance cannot be overstated. However, the process of selecting the right health insurance company is not a…

View On WordPress
#affordable health insurance#best health insurance#best health insurance policy#health insurance#health insurance 101#health insurance explained#health insurance marketplace#health insurance plan#health insurance policy#how to buy health insurance#how to buy health insurance online#how to buy health insurance plan#how to choose health insurance#how to choose health insurance plan#how to choose health insurance plan 2021#insurance
0 notes
Text

This Disability Pride Month, I want people to picture US healthcare and food scarcity in a different way. Let's get into some anti-work discussion while we're at it. A lot of you need to remember how broad of a class "disability" is.
This is what I eat. This is adult formula and I use it as enteral nutrition. This is all I can eat and gain nutrients from, and I have to have access to consistent electricity and clean water to maintain it. I cannot tolerate a blended diet (also requires electricity) nor can I safely tolerate gravity/bolus feeds. I also get 100% of my hydration via tube- not pictured is the water necessary for my survival.
Despite the room it takes up in my kitchen, you may be surprised to learn that this is less than 2mo of formula. Less than 2mo of food.
I need 15 cases a month, which is $840/mo. My individual monthly food cost is almost $300 more than the average for Hawaii, the state with the highest US grocery costs. It is more than $500 over my state’s average. My medications also cost >$2200 a month on top of that.
Mine is 100% covered by my insurance- which is tied to my employer. This puts my disabled ass in the position of meat puppet for my employer because all of my needs are interconnected- food, drinking water, medications, running water, stable housing, and electricity. My employer has the power to choose whether I live or die and in this "mutually beneficial relationship", being a working disabled person serves them even more than the comparative able-bodied person because I have my hand forced towards company loyalty.
I really like my employer. But if this were not the case, changing jobs isn't really a safe option. Even if I had a job lined up, it can legally take up to 90 days (or longer in some cases) to get onto employer insurance. That's over $9,120 for 90 days (or more) of insurance lapse. COBRA is also a joke- my state charges $675.45/month for individual health insurance ONLY. That's still $2,026.35 and only if I was terminated, not voluntary resignation.
I think a lot of you need to remember how much disabled people are still an oppressed class- in the US disability law really has not done much for us and it has an extremely narrow view of what disability looks like. The ableism I've been seeing from the left has always been around, but during Disability Pride Month it has especially been a slap to the face.
3K notes
·
View notes
Text
By: Beth Bourne
Published: Feb 27, 2024
Kaiser gender specialists were eager to approve hormones and surgeries, which would all be covered by insurance as “medically necessary.”
On September 6, 2022, I received mail from my Kaiser Permanente Davis Ob-Gyn reminding me of a routine cervical screening. The language of the reminder stood out to me: “Recommended for people with a cervix ages 21 to 65.” When I asked my Ob-Gyn about this strange wording, she told me the wording was chosen to be “inclusive” of their “transgender” and “gender fluid” patients.
Based on this response, several thoughts occurred to me. Could I expose the medical scandal of “gender-affirming care” by saying and doing everything my daughter and other trans-identifying kids are taught to do? Would there be the type of medical safeguarding and differential diagnosis we would expect in other fields of medicine, or would I simply be allowed to self-diagnose and be offered the tools (i.e. hormones and surgeries) to choose my own gender adventure and become my true authentic self?
If I could demonstrate that anyone suffering from delusions of their sex, self-hatred, or identity issues could qualify for and easily obtain body-altering hormones and surgeries, all covered by insurance as “medically necessary” and potentially “life-saving” care, then maybe people would finally wake up. I certainly had.
I was prepared for failure. I wasn’t prepared for how easy success would be.
* * *
I am a 53-year-old mom from Davis, CA. My daughter began identifying as a transgender boy (social transition) and using he/him pronouns at school during 8th grade. Like several of her peers who also identified as trans at her school, my daughter was a gifted student and intellectually mature but socially immature. This shift coincided with her school’s sudden commitment to, and celebration of, a now widespread set of radical beliefs about the biology of sex and gender identity.
She “came out” as trans to her father (my ex-husband) and me through a standard coming-out letter, expressing her wish to start puberty blockers. She said she knew they were safe, citing information she had read from Planned Parenthood and the World Professional Association for Transgender Health (WPATH). To say I was shocked would be an understatement. I was also confused because this announcement was sudden and unexpected. While others quickly accepted and affirmed my daughter’s new identity, I was apprehensive and felt the need to learn more about what was going on.
Events began escalating quickly.
During a routine doctor’s visit scheduled for dizziness my daughter said that she was experiencing, the Kaiser pediatrician overheard her father using “he/him” pronouns for our daughter. The pediatrician seemed thrilled, quickly asking my daughter about her “preferred pronouns” and updating her medical records to denote that my daughter was now, in fact, my son. The pediatrician then recommended we consult the Kaiser Permanente Oakland Proud pediatric gender clinic, where she could get further information and (gender affirming) “treatment.” Now I was the one feeling dizzy.
As I began educating myself on this issue, I discovered that this phenomenon—minors, most often teen girls, suddenly adopting trans identities—was becoming increasingly widespread. It even had a name: rapid onset gender dysphoria, or ROGD. Thankfully, after learning about the potential side-effects of blockers and hormones, my ex-husband and I managed to agree not to consent to any medical interventions for our daughter until she turned 18 and would then be able to make such decisions as an adult.
Over the past five years, my daughter’s identity has slowly evolved in ways that I see as positive. Our bond, however, has become strained, particularly since I began publicly voicing my concerns about what many term as “gender ideology.” Following my daughter’s 17th birthday family celebration, she sent me an email that evening stating she would be cutting off contact with me.
While this estrangement brought me sorrow, with my daughter living full-time with her father, it also gave me the space to be an advocate/activist in pushing back on gender identity ideology in the schools and the medical industry.
I decided to go undercover as a nonbinary patient to show my daughter what danger she might be putting herself in—by people who purport to have her health as their interest, but whose main interest is in medically “affirming” (i.e., transitioning) whoever walks through their door. I am at heart a mother protecting her child.
* * *
My daughter’s sudden decision to become a boy was heavily on my mind in early September of 2022, when mail from my Kaiser Permanente Davis Ob-Gyn reminded me of a routine cervical screening with “Recommended for people with a cervix ages 21 to 65.” I was told that the wording was chosen to be “inclusive” of transgender and “gender fluid” patients.
Throughout the whole 231-day process of my feigned gender transition, the Kaiser gender specialists were eager to serve me and give me what I wanted, which would all be covered by insurance as “medically necessary.” My emails were returned quickly, my appointments scheduled efficiently, and I never fell through the cracks. I was helped along every step of the way.
Despite gender activists and clinicians constantly claiming that obtaining hormones and surgeries is a long and complex process with plenty of safety checks in place, I was in full control at every checkpoint. I was able to self-diagnose, determine how strong a dose of testosterone I received and which surgeries I wanted to pursue, no matter how extreme and no matter how many glaring red flags I purposefully dropped. The medical workers I met repeatedly reminded me that they were not there to act as “gatekeepers.”
I was able to instantly change my medical records to reflect my new gender identity and pronouns. Despite never being diagnosed with gender dysphoria, I was able to obtain a prescription for testosterone and approval for a “gender-affirming” double mastectomy from my doctor. It took only three more months (90 days) to be approved for surgery to remove my uterus and have a fake penis constructed from the skin of my thigh or forearm. Therapy was never recommended.
Critics might dismiss my story as insignificant on the grounds that I am a 53-year-old woman with ample life experience who should be free to alter her body. However, this argument for adult bodily autonomy is a standard we apply to purely cosmetic procedures like breast implants, liposuction, and facelifts, not “medically necessary” and “lifesaving” treatments covered by health insurance. Or interventions that compromise health and introduce illness into an otherwise healthy body. And especially not for children.
My story, which I outline in much more detail below, should convince any half-rational person that gender medicine is not operating like any other field of medicine. Based on a radical concept of “gender identity,” this medical anomaly preys upon the body-image insecurities common among pubescent minors to bill health insurance companies for permanent cosmetic procedures that often leave their patients with permanently altered bodies, damaged endocrine systems, sexual dysfunction, and infertility.
* * *
Detailed Timeline of Events
On October 6, 2022, I responded to my Ob-Gyn’s email to tell her that, after some thought, I’d decided that maybe the label “cis woman” didn’t truly reflect who I was. After all, I did have some tomboyish tendencies. I told her I would like my records to be changed to reflect my newly realized “nonbinary” identity, and that my new pronouns were they/them. I also voiced my desire to be put in touch with an endocrinologist to discuss starting testosterone treatment.
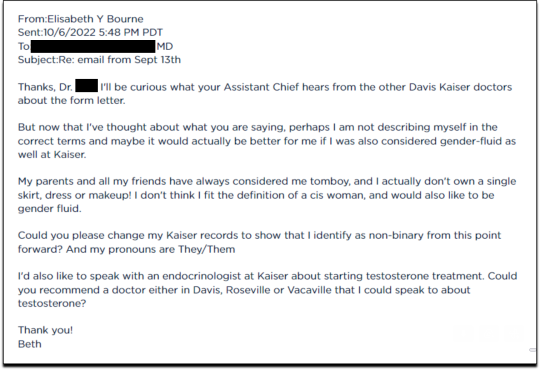
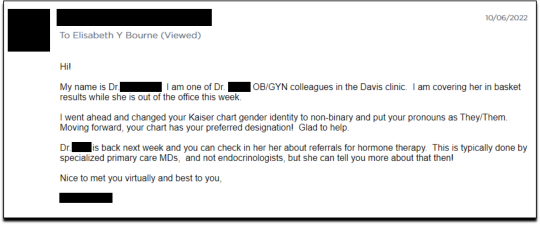
Fifteen minutes later I received an email from another Kaiser doctor informing me that my medical records had been changed, and that once my primary doctor returned to the office, I’d be able to speak with her about hormone therapy.
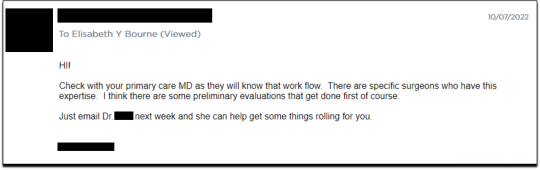
I responded the following day (October 7, 2022), thanking her for changing my records, and asking if she could connect me with someone who could help me make an appointment for “top surgery” (i.e., a cosmetic double mastectomy) because my chest binder was rather “uncomfortable after long days and playing tennis.”
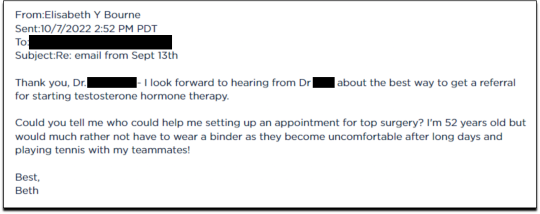
She told me to contact my primary care MD to “get things rolling,” and that there were likely to be “preliminary evaluations.”
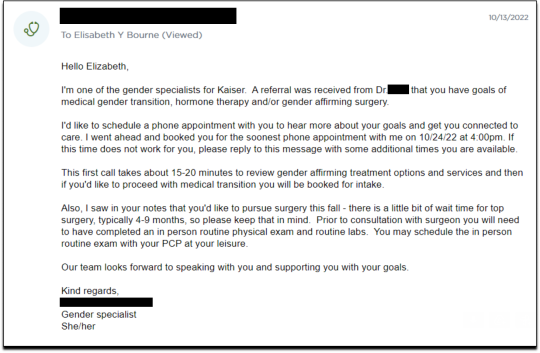
Six days after contacting my primary care MD for a referral, I received an email from one of Kaiser’s gender specialists asking me to schedule a phone appointment so she could better understand my goals for surgery, so that I could get “connected to care.” This call to review my “gender affirming treatment options and services” would take 15-20 minutes, after which I would be “booked for intake,” allowing me to proceed with medical transition.
This wasn’t an evaluation of whether surgical transition was appropriate, it was simply a meeting for me to tell them what I wanted so that they could provide it.
On October 18, I had my one and only in-person appointment in preparation for top surgery. I met in Davis with my primary care physician, Dr. Hong-wen Xue. The assessment was a 10-minute routine physical exam that included blood tests. Everything came back normal. Notably, there was not a single question about why I wanted top surgery or cross-sex hormones. Nor was there any discussion of the risks involved with these medical treatments.
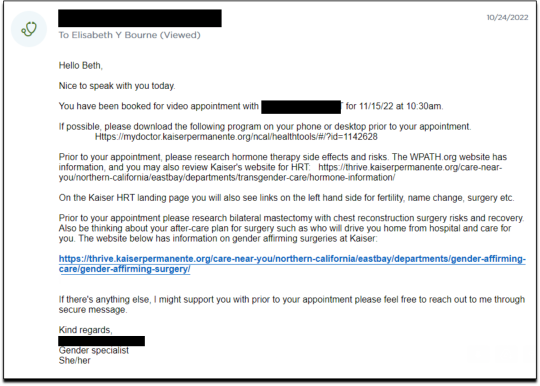
The following week, on October 24, I had a phone appointment with Rachaell Wood, MFT, a gender specialist with Kaiser Sacramento. The call lasted 15 minutes and consisted of standard questions about potential drug use, domestic violence, guns in the house, and whether I experienced any suicidal thoughts. There were no questions from the gender specialist about my reasons for requesting a mastectomy or cross-sex hormones, or why I suddenly, at 52, decided I was “nonbinary.”
After the call, Kaiser emailed me instructions about how to prepare for my pre-surgery intake video appointment to evaluate my mental health, scheduled to take place on November 15. The email stated that prior to my appointment, I should research hormone risks on the WPATH website, and to “research bilateral mastectomy and chest reconstruction surgery risks and recovery” on Kaiser’s website.
I decided to request a “gender-affirming” double mastectomy and phalloplasty. Kaiser sent me a sample timeline for gender transition surgery preparation (see below) that you can use as a reference for the process. I also asked for a prescription for cross-sex hormones (testosterone) as needed and recommended by Kaiser.
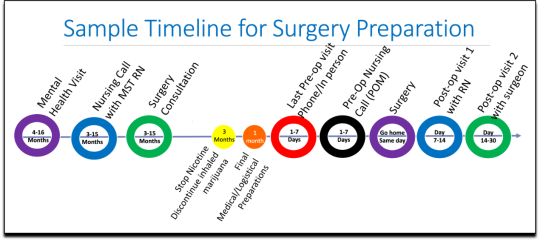
[ Source: Kaiser Permanente, Top Surgery - EXPLORING YOUR SURGICAL OPTIONS ]
Pre-Surgery Mental Health Video Appointment, Part I
This “Mental Health Visit” assessment was conducted over Zoom. The Kaiser gender specialist started with questions addressing my marital status, race, gender identity, and other demographics. She asked whether I was “thinking of any other surgeries, treatments in the future.” The list she read included “gender-affirming” hysterectomies, bottom surgeries such as metoidioplasty and phalloplasty, vocal coaching, support groups, and body contouring. “Anything else you might be interested in doing?” she asked. I said that I’d perhaps be interested in body contouring. I was also assured that all the procedures would be covered by insurance because they were considered “medically necessary.”
I dropped in several red flags regarding my mental health to see the reaction, but all were ignored. For instance, I revealed that I had PTSD. When the therapist asked me about whether I had experienced any “childhood trauma,” I explained that I grew up in Mexico City and had been groped several times and had also witnessed men masturbating in public and had been grabbed by men in subways and buses. “I was a young girl, so [I had] lots of experiences of sexual harassments, sexual assault, just the kind of stuff that happens when you are a girl growing up in a big city.” “So, you know,” I finished, “just the general feeling that you are unsafe, you know, in a female body.”
The therapist did not respond to my disclosure that trauma could be the cause of my dysphoria. Instead of viewing this trauma as potentially driving my desire to escape my female body through hormones and surgery, she asked whether there is anything “important that the surgery team should be aware of” regarding my “history of trauma,” such as whether I’d be comfortable with the surgeon examining and marking my chest prior to surgery.
When asked about whether I had had any “psychotic symptoms,” I told her that while I had had no such symptoms, my mother had a delusional nervous breakdown in her 50s because she had body dysmorphia and became convinced she had a growth on her neck that needed to be removed. I told her that my mother was then admitted to an inpatient hospital for severe depression. I asked her whether she ever sees patients with body dysmorphia and whether I could have potentially inherited that from my mother. She told me that psychosis was hereditary, but that it was “highly unlikely” that there was any connection between body dysmorphia and gender dysphoria.
I enthusiastically waved more mental health red flags, waiting to see if she would pick up on any of them.
I’m just wondering if my feelings, or perseverating, or feeling like these breasts make me really unhappy and I just don’t want them anymore!...I’m just not sure if that’s a similar feeling to body dysmorphia? How do you decide which one is gender dysphoria and general body dysmorphia, and just not liking something about your body? Feeling uncomfortable with your body?
And I did have an eating disorder all through college. I was a distance runner in college so I had bulimia and anorexia, you know. So I don’t know if that’s related to gender dysphoria?
The therapist replied, “I completely appreciate your concerns, but I am going to ask you questions about your chest, about your expectations. And then I’ll be able to give you an assessment.” She also said the main difference between my mom’s situation and mine was that my mom didn’t really have a growth on her neck, whereas it’s “confirmed” that I actually have “chest tissue.” Furthermore, she said that while “historically there has been all this pressure on patients to be like ‘Are you really, really sure you want hormones? Are you 100% sure?’ We are a little more relaxed.” She continued, “As long as you are aware of the risks and the side-effects, you can put your toe in the water. You can stop ‘T’ [testosterone], you can go back and do it again later! You can stop it! You can stop it! You know what I mean?”
Because we ran out of time, I scheduled a follow-up phone meeting on December 27, 2022 with a different gender specialist to complete my mental health assessment for top surgery.
Pre-Surgery Mental Health Video Appointment, Part II
During this meeting, Guneet Kaur, LCSW, another Kaiser gender specialist (she/her/they/them pronouns) told me that she regretted the “gatekeeping vibe” of the meeting but assured me that since I have been “doing the work,” her questions are essentially just a form of “emotional support” before talking with the medical providers.
She asked me about what I’d been “looking into as far as hormones.” I told her that I’d be interested in taking small doses of testosterone to counterbalance my female feelings to achieve “a feeling that’s kind of neutral.”
When she asked me about me “not feeling like I match on the outside what I feel on the inside,” I dropped more red flags, mentioning my aversion to wearing dresses and skirts.
I don’t own a single dress or a skirt and haven't in 20 years. I think for me it’s been just dressing the way that’s comfortable for me, which is just wearing, jeans and sweatshirts and I have a lot of flannel shirts and, and I wear boots all the time instead of other kinds of shoes. So I think it’s been nice being able to dress, especially because I work from home now most of the time that just a feeling of clothing being one of the ways that I can feel more non-binary in my everyday life.
She responded, “Like having control over what you wear and yeah. Kind of that feeling of just, yeah, this is who I am today. That’s awesome. Yeah.”
She then asked me to describe my dysphoria, and I told her that I didn’t like the “feeling of the female form and being chesty,” and that because I am going through menopause, I wanted to start taking testosterone to avoid “that feeling of being like this apple-shaped older woman.” “Good. Okay, great,” she responded, reminding me that only “top surgery,” not testosterone, would be able to solve my chest dysphoria. (Perhaps it was because all these meetings were online, they didn’t notice I’m actually fit and relatively slender at 5’-5” and 130 pounds, and not apple-shaped at all.)
She told me that we had to get through a few more questions related to my medical history before “we can move on to the fun stuff, which is testosterone and top surgery.”
The “fun stuff” consisted of a discussion about the physical and mood changes I could expect, and her asking me about the dose of testosterone I wanted to take and the kind of “top surgery” technique I’d prefer to achieve my “chest goals.” She told me that all or most of my consultations for surgeries and hormones would be virtual.
The gender specialist told me after the appointment, she would submit my referral to the Multi-Specialty Transitions Clinic (MST) team that oversees “gender expansive care.” They would follow up to schedule a “nursing call” with me to review my medical history, after which they’d schedule my appointment with a surgeon for a consultation. Her instructions for this consultation were to “tell them what you’re wanting for surgery and then they share with you their game plan.”
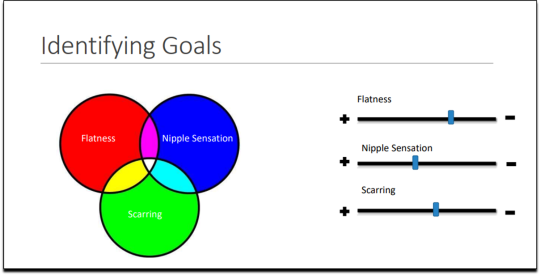
[ Decision-making slide to help me identify my goals for top surgery–flat chest, nipple sensation, or minimal scarring. Source: Kaiser Permanente, Top Surgery - EXPLORING YOUR SURGICAL OPTIONS ]
She told me that Kaiser has a team of plastic surgeons who “only work with trans and nonbinary patients because there’s just so much need for them.” She asked about my priorities for chest surgery, such as whether I value flatness over nipple sensation. I learned about double incision top surgery with nipple grafts, as well as “keyhole,” “donut,” “buttonhole,” and “Inverted-T” top surgeries.
By the end of the hour-long appointment, I had my surgery referral and was ready for my “nursing call” appointment.
Nursing call with Nurse Coordinator from the Transgender Surgery and Gender Pathways Clinic at Kaiser San Francisco
On January 19, 2023, I had my nursing call with the Nurse Coordinator. He first said that “the purpose of this call is just for us to go through your chart together and make sure everything’s as accurate as possible.” Once that was done, my referral would be sent to the surgeon for a consultation.
He asked me about potential allergies and recreational drug use, and verified that I was up to date on mammograms, pap smears, and colon cancer screenings, as well as vaccines for flu and COVID. I verified my surgical history as well as my current medications and dietary supplements.
He told me about a “top surgery class” available for patients where one of the Kaiser surgeons “presents and talks about surgical techniques and options within top surgery,” and includes a panel of patients who have had top surgery. I signed up for the February 8th class.
Within 10 minutes he told me that he had “sent a referral to the plastic surgery department at Kaiser Sacramento,” and that I should be hearing from them in the next week or two to schedule a consultation.
Appointment for Testosterone
On January 27, I had a 13-minute online appointment with a primary care doctor at Kaiser Davis to discuss testosterone. The doctor verified my name and preferred pronouns, and then directly asked: “So, what would you like to do? What kind of physical things are you looking for?”
I told her I wanted facial hair, a more muscular and less “curvy” physique, and to feel stronger and androgynous. She asked me when I wanted to start, and I told her in the next few months. She asked me if I was menopausal, whether I had ovaries and a uterus, although that information should have been on my chart.
The doctor said she wanted me to come in to get some labs so she could check my current estrogen, testosterone, and hemoglobin levels before starting hormones. Then “we'll set the ball in motion and you'll be going. We’ll see you full steam ahead in the direction you wanna go.”
That was it. I made an appointment and had my lab tests done on February 12. My labs came back on February 14, and the following day, after paying a $5 copay at the Kaiser pharmacy, I picked up my testosterone pump. That was easy!
Top Surgery Consultation
On the same day I received my labs, I had a Zoom surgery consultation with Karly Autumn-Kaplan, MD, Kaiser Sacramento plastic surgeon. This consultation was all about discussing my “goals” for surgery, not about whether surgery was needed or appropriate.
I told the surgeon that I wanted a “flatter, more androgynous appearance.” She asked me some questions to get a better idea of what that meant for me. She said that some patients want a “male chest,” but that others “want to look like nothing, like just straight up and down, sometimes not even nipples.” Others still wanted their chest to appear slightly feminine and only “slightly rounded.” I told her that I’d like my chest to have a “male appearance.”
“What are your thoughts about keeping your nipples?” she asked. “Are you interested in having nipples or would you like them removed?” I told her that I’d like to keep my nipples, but to make them “smaller in size.” She asked me if I’d like them moved to “the edge of the peck muscle” to achieve “a more male appearance.” I said yes.
I was asked to show my bare chest from the front and side, which I did. Then she asked me how important it was for me to keep my nipple sensation. I replied that it was important unless it would make recovery more difficult or there were other associated risks. She highlighted the problem with the free nipple graft, saying that removing the nipple to relocate it means “you're not gonna have sensation in that nipple and areola anymore.” However, some nipple sensation could be preserved by keeping it attached to “a little stalk of tissue” with “real nerves going to it,” but that would require leaving more tissue behind. I told her I’d go for the free nipple graft to achieve a flatter appearance. It was also suggested I could skip nipple reconstruction entirely and just get nipples “tattooed” directly onto my chest.
She told me I was “a good candidate for surgery,” and put me on the surgery wait list. She said that the wait time was between three and five months, but a cancellation could move me up to a sooner date. Also, if I wanted surgery as soon as possible, I could tell the surgery scheduler that I’d be willing to have any of the other three surgeons perform my mastectomy. Outpatient top surgery would cost me a copay of $100.
They contacted twice, in February and March, notifying me of cancellations. If I had accepted and shown up on those dates, they would have removed my breasts. This would have been less than five months from the time I first contacted Kaiser to inform them of my new “nonbinary” gender identity.
How Far Can I Go?
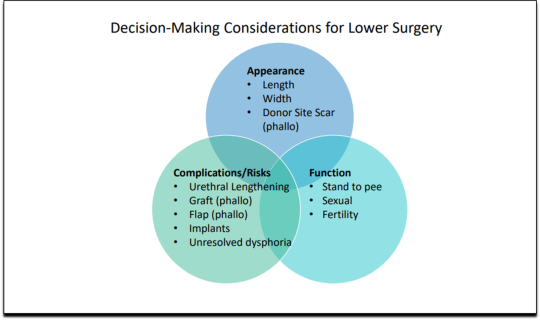
I decided to see how easy it would be for me to get approved for a phalloplasty. Known euphemistically as “bottom surgery,” phalloplasty is the surgical creation of an artificial penis, generally using tissue from the thigh or arm.
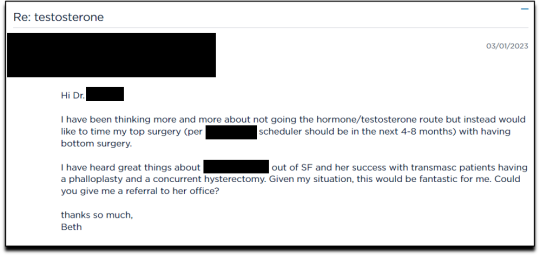
I sent an email on March 1, 2023, requesting to have a phalloplasty and concurrent hysterectomy scheduled alongside my mastectomy.
Two weeks later, on March 16th, I had a 16-minute phone call with a gender specialist to discuss my goals for bottom surgery and obtain my referral.
During the call, I explained to the specialist that I wasn’t sure about taking testosterone anymore because I was already quite athletic and muscular, and that taking testosterone didn’t make much sense to me. Instead, I wanted bottom surgery so that I wouldn’t feel like my “top” didn’t match my “bottom.” I told her:
But what I really wanted was to have bottom surgery. So this way when I have my top surgery, which sounds like it could be very soon, that I’ll be aligned, that I won’t have this sense of dysphoria with one part of my body and the other part feeling like it matched who I am. So yeah. So I just did a little bit more research into that. And I looked at the resources on the Kaiser page for the MST clinic and I think I know what I want, which is the hysterectomy and then at the same time or soon after to be able to have a phalloplasty.
I told her that I wanted to schedule the top and bottom surgery concurrently so that I wouldn’t have to take more time off work and it would save me trips to San Francisco or Oakland, or wherever I had to go for surgery.
None of this gave the gender specialist pause. After a brief conversation about some online resources to look over, she told me that she would “submit the referral now and we’ll get this ball rolling.”
Bottom surgery would cost me a copay of $200, which included a couple of days in the hospital for recovery.
Phalloplasty Surgical Consultation with Nurse Coordinator
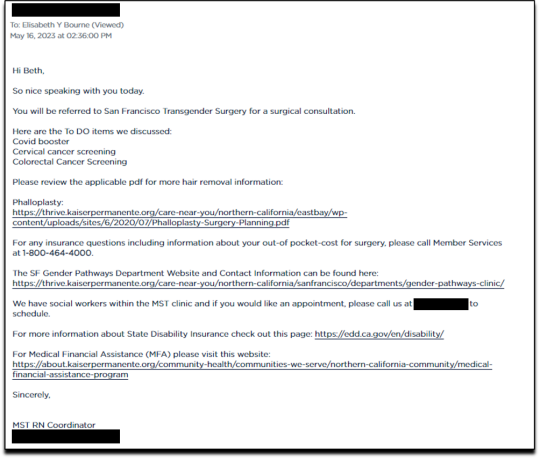
On May 16, 2023, I had a short surgical consultation with a nurse coordinator to go through my medical history. This was similar to the consultation for top surgery but included information about hair removal procedures for the skin on my “donor site” that would be fashioned into a makeshift penis. They also went over the procedures for determining which donor site—forearm or thigh—was more viable.
After only 15 minutes, she submitted my referral to the surgeon for another surgical consultation.
On May 25 I received an email from my phalloplasty surgeon’s scheduler, informing me that they have received my referral and are actively working on scheduling, but that they are experiencing delays.
I ended my investigation here once I had the referral for the top and bottom surgery. I never used my testosterone pump.
Final Thoughts
In fewer than 300 days, based on a set of superficial and shifting thoughts about my gender and my “embodiment goals” triggered by the mere mention of “gender” in a form letter from my primary care physician, and driven by what could only be described as minor discomforts, Kaiser Permanente’s esteemed “multi-disciplinary team” of “gender specialists” was willing, with enthusiasm—while ignoring mental health concerns, history of sexual trauma, and rapidly escalating surgical requests—to prescribe life-altering medications and perform surgeries to remove my breasts, uterus, and vagina, close my vaginal opening, and attempt a complex surgery with high failure and complication rates to create a functionless representation of a penis that destroys the integrity of my arm or thigh in the process.
This describes the supposedly meticulous, lengthy, and safety-focused process that a Kaiser patient must undergo to embark on a journey to medically alter their body. No clinician questioned my motivations. No one showed concern that I might be addressing a mental health issue through radical and irreversible interventions that wouldn’t address my amorphous problems. There were no discussions about how these treatments would impact my long-term health, romantic relationships, family, or sex life. I charted the course. The clinicians followed my lead without question. The guiding issue was what I wanted to look like.
No other medical field operates with this level of carelessness and disregard for patient health and welfare. No other medical field addresses issues of self-perception with surgery and labels it “medically necessary.” No other medical field is this disconnected from the reality of the patients it serves.
Kaiser has traded medicine for ideology. It’s far beyond time we stop the ruse of considering “gender-affirming” interventions as anything approaching medical care.
This isn’t the first time Kaiser Permanente has been in the news for completely disregarding medical safeguards in the name of “gender-affirming care.” As girls, Chloe Cole and Layla Jane became convinced that they were born in the wrong body and were actually boys on the inside. Doctors at Kaiser ignored their underlying conditions and instead prescribed testosterone and removed their breasts. Both Cole and Jane have since detransitioned and are currently suing Kaiser.
The fact that children and vulnerable adults are being exploited in this massive ideological experiment is not just tragic; it’s deeply disturbing, especially considering it has evolved into a billion-dollar industry.
I hope that by sharing my story, I can bring more focused scrutiny to the medical scandal unfolding not just at Kaiser but also at medical centers and hospitals across the Western world. These institutions have completely abandoned medical safeguards for patients who claim to be confused about their “gender,” and I aim to awaken more parents and assist them in protecting their children.
--
==
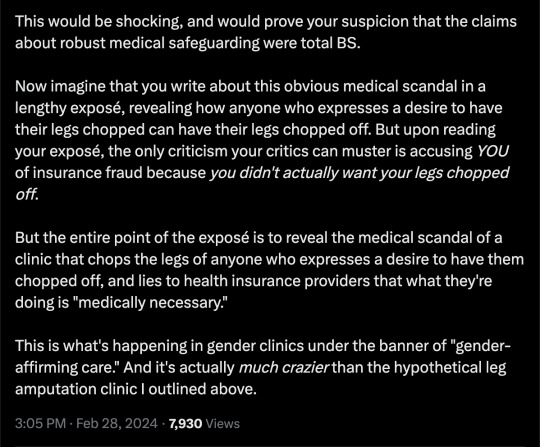
This is completely insane.
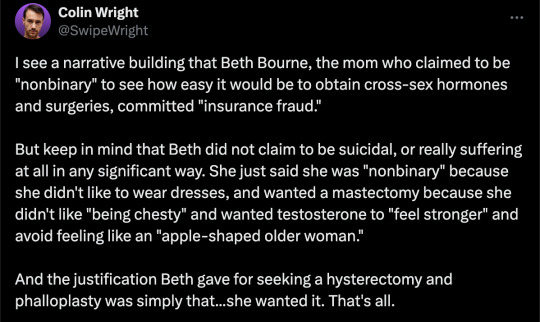
Apologists online are running around saying, but she didn't mean it, she was lying, she was pretending...
It doesn't matter.
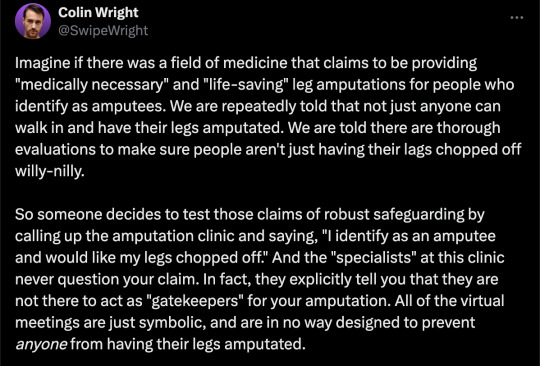
Any kind of security, penetration or integrity test is insincere too. When security researchers compromise Microsoft's operating system or Google's browser or whatever, "but they didn't mean it" is not a defence to a discovered security flaw. It doesn't matter that the security researchers didn't plan to steal data or money or identities. The flaw in the system is there regardless.
It doesn't matter that it was insincere. Because the workers didn't know that. They never checked, never asked questions, never tested. They had been taught and instructed to never ask any questions. They did what they were supposed to. And the system failed spectacularly. Because that's what "gender affirming care" means.
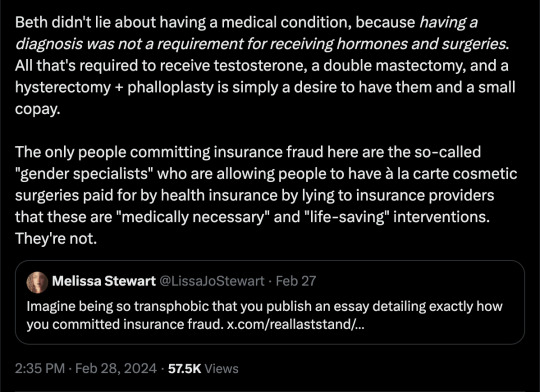
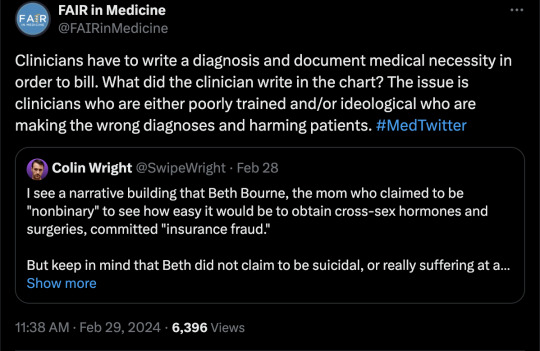
Additionally, the claim that Beth Bourne committed fraud is an outright lie. A patient cannot bill. They do not have the authority. The medical clinic is the only one that can bill, and they must supply a diagnosis and a medical necessity.
If they didn't diagnose her and just wrote down what she said, then they committed fraud. If they claim they did diagnose her, then they committed fraud, because the diagnosis they concocted was bogus. This, by the way, is actually going on. Clinics are reporting fake endocrine and other disorders to get blockers, hormones and other interventions. Jamie Reed and other whistleblowers have documented evidence of this. Beth Bourne is not responsible for what the clinic does. They have medical licenses and legal responsibility. Not her.
Additionally, anyone who actually read the article would know how she tested the system. She said things like, "I've always been not that feminine. So, maybe I get my boobs removed." And they said, "sure." Instead of saying, "wait, why do you think that?" Framing it as her lying is itself a lie. They violated their ethical obligations. That much is incontrovertible. And it's directly the result of "gender affirming care," where clinics and clinicians rubber-stamp anything deemed "trans" based entirely on ideological, not medical, grounds.
#Beth Bourne#undercover#undercover investigation#gender identity ideology#queer theory#nonbinary#non binary#top surgery#bottom surgery#double mastectomy#bilateral mastectomy#gender affirming care#gender affirming healthcare#gender affirmation#affirmation model#medical scandal#medical malpractice#medical corruption#religion is a mental illness
756 notes
·
View notes
Text
I feel like people often don’t talk about the experiences of disabled people who have caretakers because so much of the conversation is about us—not including us.
I receive in home care for 30 hours a week (+ 4 hours/week for respite). This is paid for by Medicaid (state insurance). Outside of paid hours, my primary caretakers care for me unpaid and assist me most of the time. I’m very rarely left alone due to my high support needs. Often, when I am left alone, I am completely bedridden or at minimum housebound. I have frequent emergency life threatening health problems, falls, and serious injuries even with support in place, and these things significantly increase when I’m on my own.
I’m extremely lucky that my paid caretakers are my partner, my sister (the only family member I have regular contact with, I’m estranged from the rest of my immediate family and most of my extended family) and my best friend.
I used to have agency staffing which was horrible for me and borderline traumatic. At several points, before doing the self directed care option (which allows me to choose my own staff, hire and train them myself and dictate hours for them), I opted to not have any staffing. I was regularly in the emergency room. I can’t drive, so I was having to walk and if I was lucky enough to be able to take the bus on occasion or get a ride from a Facebook acquaintance, they were few and far in between. I don’t have family support, and even my sister who is supportive wasn’t living in the state at the time and doesn’t have a car most of the time.
And before I could even choose which staffing option, even though medically it had been deemed essential for me to have in home care, even though my insurance covered it, I had to wait several years (I was 18 when I was approved) until I was 21 to qualify to start. The reason why: I was legally an “adult disabled child” because of my high support needs (which is funny because I STILL don’t have SSI at age 24) and thus legally unable to consent to my own care plan. I needed a blood relative to consent, and that same blood relative (who had to have proof of such!) couldn’t care for me. At the time, my sister was the only person who could’ve been my caregiver and also she is the only verifiable blood relative I have contact with for safety reasons, and my only relative on this side of the USA.
The first business day after my 21st birthday I immediately got things set up to get in home care.
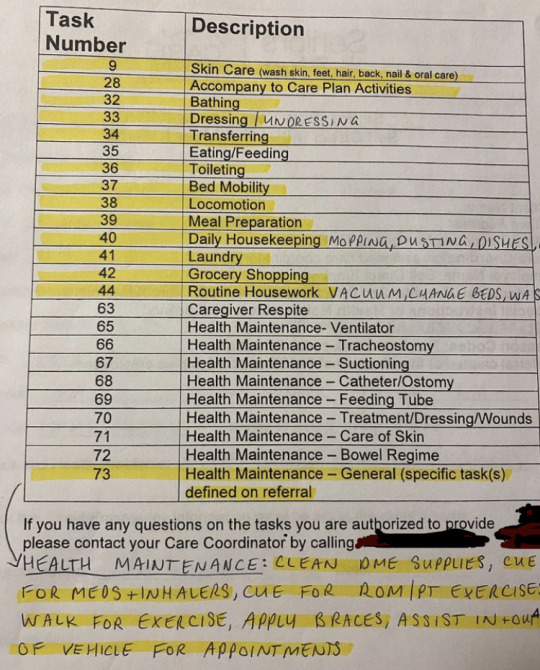
This is out of date, I get assistance with more than just these highlighted ADL (activities of daily living) tasks now.
In short: my day-to-day life is entirely dependent on others.
And there’s power imbalances that exist between me and my caregivers, even with my current caregivers being amazing and anti-ableist. They will always exist. We talk about the power dynamics of me being dependent on them for my survival, and how heavy that weight can be for each of us.
Having caregivers often means that accessibility is extra difficult— I’ve been told straight up multiple times that I can’t have assistance from my caregivers to help me change in a changing room when we’re out shopping. That they can’t go into the bathroom with me, that they can’t help me get un/dressed during appointments, that they can’t come into spaces with me.
I’ve been denied access to psychiatric care because I can’t do my daily living tasks (ADLs- the highlighted items) independently. And when I’m in a hospital or emergency room, I can’t have my in home workers be paid to care for me, there’s an expectation that the nursing staff at the hospital will do it. Even though my caregivers were specifically trained to learn my body and needs for weeks and have been working with me for years. I have severe cPTSD and showering in front of a stranger is something I cannot do. I would rather fall or faint or get injured or just not shower than deal with that. But I’m expected to just let anyone have access to my body just because I’m physically disabled and need support.
When I faint/fall/get injured/have life threatening health issues arise while I’m not clothed, or when I’m otherwise vulnerable, I’m supposed to let strangers just touch me however they want to. I have to show them my chest (for my cardiac care) and let them poke and examine me. I can’t object without losing access to vital care.
I have agency. I have rights. I have autonomy. I deserve to be able to exercise these things.
#chronically couchbound#disability#disabled#disabled pride#cripple punk#cripplepunk#disability pride#high support needs#ableism#professional caregiver#activities of daily living#ADL#medicaid#healthcare#in home care#home care#home care aids#nothing about us without us
1K notes
·
View notes
Text
SEPARATE Health Insurance For Senior Citizens
Why Senior Citizens Need Separate Health Insurance Plans
Are you considering health insurance for a senior citizen? Regular plans might not be the answer! This video explains why separate senior citizen health plans are better suited for their needs. We'll cover:
Why regular plans can be restrictive and expensive for seniors
Benefits of senior citizen health insurance:
- Coverage for pre-existing conditions
- Higher sum insured for greater coverage
- Additional benefits like check-ups and home healthcare
Ensure your loved ones have the right protection. Watch now and learn how to find the best senior citizen health insurance plan!
#Health Insurance for Senior Citizen India#Health Insurance for Senior Citizen#Best Health Insurance for Senior Citizen#Health Insurance for Elderly Parents#health insurance for elderly father#health insurance for elderly mother#health insurance for elderly#best health insurance plans#how to choose health insurance plan#how to buy health insurance#nidhiverma22#algatesinsurance#health insurance 101
0 notes
Text
A taxonomy of corporate bullshit
Next Tuesday (Oct 31) at 10hPT, the Internet Archive is livestreaming my presentation on my recent book, The Internet Con.

There are six lies that corporations have told since time immemorial, and Nick Hanauer, Joan Walsh and Donald Cohen's new book Corporate Bullsht: Exposing the Lies and Half-Truths That Protect Profit, Power, and Wealth in America* provides an essential taxonomy of this dirty six:
https://thenewpress.com/books/corporate-bullsht
In his review for The American Prospect, David Dayen summarizes how these six lies "offer a civic-minded, reasonable-sounding justification for positions that in fact are motivated entirely by self-interest":
https://prospect.org/culture/books/2023-10-27-lies-my-corporation-told-me-hanauer-walsh-cohen-review/
I. Pure denial
As far back as the slave trade, corporate apologists and mouthpieces have led by asserting that true things are false, and vice-versa. In 1837, John Calhoun asserted that "Never before has the black race of Central Africa, from the dawn of history to the present day, attained a condition so civilized and so improved, not only physically, but morally and intellectually." George Fitzhugh called enslaved Africans in America "the freest people in the world."
This tactic never went away. Children sent to work in factories are "perfectly happy." Polluted water is "purer than the water that came from the river before we used it." Poor families "don't really exist." Pesticides don't lead to "illness or death." Climate change is "beneficial." Lead "helps guard your health."
II. Markets can solve problems, governments can't
Alan Greenspan made a career out of blithely asserting that markets self-correct. It was only after the world economy imploded in 2008 that he admitted that his doctrine had a "flaw":
https://www.pbs.org/newshour/show/greenspan-admits-flaw-to-congress-predicts-more-economic-problems
No matter how serious a problem is, the market will fix it. In 1973, the US Chamber of Commerce railed against safety regulations, because "safety is good business," and could be left to the market. If unsafe products persist in the market, it's because consumers choose to trade safety off "for a lower price tag" (Chamber spox Laurence Kraus). Racism can't be corrected with anti-discrimination laws. It's only when "the market" realizes that racism is bad for business that it will finally be abolished.
III. Consumers and workers are to blame
In 1946, the National Coal Association blamed rampant deaths and maimings in the country's coal-mines on "carelessness on the part of men." In 2003, the National Restaurant Association sang the same tune, condemning nutritional labels because "there are not good or bad foods. There are good and bad diets." Reagan's interior secretary Donald Hodel counseled personal responsibility to address a thinning ozone layer: "people who don’t stand out in the sun—it doesn’t affect them."
IV. Government cures are always worse than the disease
Lee Iacocca called 1970's Clean Air Act "a threat to the entire American economy and to every person in America." Every labor and consumer protection before and since has been damned as a plague on American jobs and prosperity. The incentive to work can't survive Social Security, welfare or unemployment insurance. Minimum wages kill jobs, etc etc.
V. Helping people only hurts them
Medicare will "destroy private initiative for our aged to protect themselves with insurance" (Republican Senator Milward Simpson, 1965). Covid relief is unfair to people that are currently in the workforce" (Republican Governor Brian Kemp, 2021). Welfare produces "learned helplessness."
VI. Everyone who disagrees with me is a socialist
Grover Cleveland's 2% on top incomes is "communistic warfare against rights of property" (NY Tribune, 1895). "Socialized medicine" will leave "our children and our children’s children [asking] what it once was like in America when men were free" (Reagan, 1961).
Everything is "socialism": anti-child labor laws, Social Security, minimum wages, family and medical leave. Even fascism is socialism! In 1938, the National Association of Manufacturers called labor rights "communism, bolshevism, fascism, and Nazism."
As Dayen says, it's refreshing to see how the right hasn't had an original idea in 150 years, and simply relies on repeating the same nonsense with minor updates. Right wing ideological innovation consists of finding new ways to say, "actually, your boss is right."
The left's great curse is object permanence: the ability to remember things, like the fact that it used to be possible for a worker to support a family of five on a single income, or that the economy once experienced decades of growth with a 90%+ top rate of income tax (other things the left manages to remember: the "intelligence community" are sociopathic monsters, not Trump-slaying heroes).
When the business lobby rails against long-overdue antitrust action against Amazon and Google, object permanence puts it all in perspective. The talking points about this being job-destroying socialism are the same warmed-over nonsense used to defend rail-barons and Rockefeller. "If you don't like it, shop elsewhere," has been the corporate apologist's line since slavery times.
As Dayen says, Corporate Bullshit is a "reference book for conservative debating points, in an attempt to rob them of their rhetorical power." It will be out on Halloween:
https://bookshop.org/a/54985/9781620977514
If you'd like an essay-formatted version of this post to read or share, here's a link to it on pluralistic.net, my surveillance-free, ad-free, tracker-free blog:
https://pluralistic.net/2023/10/27/six-sells/#youre-holding-it-wrong
#pluralistic#corporate bullshit#lies#books#reviews#taxonomies#labor#denialism#consumerism#Nick Hanauer#Joan Walsh#Donald Cohen#history#object permanence#taking the right seriously
835 notes
·
View notes
Last Seen Blogs




