#i have a seizure disorder that causes me to have them so frequently that i cant drive without the fear that ill have one on the road
Text
I hate my city's public transport system and I hate that I have to rely on it
#it has zero funding so everything's constantly breaking down#and that caused me to be late to my 8 am today#and by late i mean by an HOUR#and there's only like two buses that are actually disability accessible#and the main majority of the routes are on the OPPOSITE SIDE OF TOWN#the one that stops at my apartment complex doesn't even run on the weekends or in the summer#and you may be thinking#why dont you just drive?#i can't#i have a seizure disorder that causes me to have them so frequently that i cant drive without the fear that ill have one on the road#we dont know what it is but thats a rant for another day#also#i cant afford a car#and i dont have my license#if i wanted to get to another stop id have to walk across a whole ass highway#so yeah its awful#and i wish people cared more about public transport here
4 notes
·
View notes
Text
Want to rant about this post, because it makes me seethe every time I come across it. Nothing against anyone who's reblogged it, just want to give my two cents.
A migraine is NOT the same as a bad headache! Migraine a specific neurological condition which is frequently (though not always) characterized by headache, as well as numerous other symptoms. They're caused by some combination of nerve inflammation and uneven vasoconstriction/dialation in the brain. As such, there's no such thing as a "sinus migraine" or a "tension migraine."
Acupressure and massage *may* help to relieve some measure of migraine pain if you can stand being touched long enough, but it won't help the underlying neurological condition, which is more similar to a slow-motion seizure than any other type of headache. I'm sure pressure helps with tension headaches and maybe other types of headaches, as described, but those are not migraines! Words have meanings, gang.
However, in calling these non-migraine headaches "migraines" and then suggesting that they are easy to treat in this manner, the post suggests that migraines are a much lighter matter than they actually are. This, and discussions like this, cause real migraine to be taken less seriously by the culture at large.
Fundamentally, the thing about the original post that irritates me so much is that basically none of the people on it seem to have any idea what migraine actually is. There's been a move in recent years to try to make people more aware that medical language is very specific and shouldn't be abused (ie OCD isn't just "having a messy room bothers me," it's a specific disorder that, if untreated, can massively harm people's lives), which I think is great. At the same time, there's a growing tendency to pathologize everything, from personality tics to low-grade headaches, often in the strongest terms possible. While I'm not for the policing of language in general, I do feel that it's at best insensitive and at worst actively harmful to use specific medical terms in situations where they simply don't apply.
Most headaches are not migraines. Speaking as though they are leads to a misinformed attitude around migraine which suggests that everybody gets them, they're easy to treat, and they're not that bad actually. This attitude has caused me material difficulty so many times over the last nine years that I couldn't even being to tally it.
#i am so sick to death of seeing that post#chronic illness is hilarious#so far it's been a hard nerve block day folks#WOULD THAT I could just press on the back of my neck instead of getting SKEWERED IN THE HEAD WITH NEEDLES#🙂🙂🙂🙂🙂🙂🙂#'tension migraines' gimme a break#pontifications and creations
47 notes
·
View notes
Note
Hey there! Bit of a vent (not at you, though) incoming--
Man. Maybe I'm just salty today, but that anon you got about physical and mental disabilities being Two Totally Separate Things is such a frustrating sentiment to me. No they're not. I mean, sure, for some people, sometimes, there can be a clean separation, for them personally--but categorically? No.
We're disabled. Haven't been able to work in years, can't live on our own right now (we're hoping that'll change in the future, but we honestly don't know). Etc. Are we mentally disabled, or physically disabled? Well...
*deep breath* We have chronic fatigue. Which is a physical issue, a literal bodily physical limitation. It's from our long COVID. Unless it's from the dissociative disorder--which is a mental issue, except it can also cause chronic fatigue. Also it's actually because of the sensory overload from having ADHD. We have moderate chronic pain and frequent migraines, which is also from the long COVID, and also our past sports injuries. Except it's also from somatic stress/trauma shit, which is (probably??) from neurodivergent burnout and depression, which make it hard to care for our body properly, which causes more physical pain. Which limits us physically.
We don't use mobility aids...except the car we can borrow, which kinda counts, since we often have to use it to get to places that a physically-healthy 31 year old could normally walk to. Although we can't always use it, (the car), because sometimes we dissociate too much to be able to drive safely. Because of the dissociative disorder. Or is it because of the long COVID. Or the sleep problems. Which are physical, not mental--except for we didn't used to have them until we had all these active mental health issues. We sleep all the time because we're depressed. Or because of the chronic fatigue. Which is from the trauma, unless it's actually because of the cardiovascular scarring and low baseline blood O2.
"well, you just have both physical and mental disabili--" Are you not listening, they're literally inseparable for us. Your brain is not separate from your body, for fucks sake.
-S
P.S. This isn't saying that it sometimes isn't really useful and necessary to talk about different ways that disability impacts different folks--of course not every disabled person has the same issues or the same experience, and different kinds of accommodations are more or less frequently accepted/implemented in society. And yeah, in plenty of cases, calling a specific issue a "physical disability" vs a "cognitive disability" vs a "mental health disability" can be a useful shorthand! But saying that "physically disabled people go Over Here and use Only These Words, and mentally disabled people go Over There and use Only Those Words" is just...such a breathtaking mischaracterization of the way disability works for many people.
Oh my god oh my god YOU GET IT. hOLy Shit. @The-best-crew is laughing at me for how much I'm losing my mind about this xD
Ok ok. I think a HUGE part of the reason I didn't discover the System earlier than my late 20s is because of exactly what you're talking about. Holy shit ok let us try and get our thoughts in order.
Listen. We had experiences earlier on that we just didn't attribute to anything serious. Someone who recognized me and I didn't recognize them and that's just life, right? Easily explained away in childhood.
But in my late teens/early 20s I was diagnosed by the Cleveland Clinic with dysautonomia. This is a blanket neurological condition that affects so many things you can't even dream about. Part of it is seizures and hallucinations and brain fog, all of which we are affected by.
So when we started hearing people talk and we went up to greet family who wasn't actually there, we attributed it to dysautonomia. Because dysautonomia can cause auditory hallucinations (but so can DID).
45min of lost time and we're on a page I don't recognize? Seizure. Because I already had them. (But maybe a switch?)
Seeing a guy serenade me at work on the violin because he can't speak? Hallucination, obviously. That definitely didn't end up being my co-host.
Can't remember seeing the Grand Canyon? Oh, it's brain fog for sure. Same with my childhood memories. No one really remembers their childhood, right?
Don't get me wrong: These are all signs of DID. But they are also signs of dysautonomia. While I conflated everything to be one thing or another ... sometimes I just don't know. Am I forgetting something because of amnesia barriers or because of brain fog from my neuro condition? Am I hallucinating due to my dissociative disorder or my neuro disorder? Am I losing time because I legitimately had a seizure or because someone switched in?
I just ... I wish people didn't think it was so black and white. Dissociative disorders have a HIGH level of comorbid disorders. I can't thank you enough for this level of solidarity and understanding.
10 notes
·
View notes
Text
Posting for a friend :
“Hello everyone,
My name is Isabel and I am a mother of two children. At just 22 years old, I am facing immense health challenges that threaten my ability to care for them and myself. Recently, I received a diagnosis that turned my life upside down: Ehlers-Danlos Syndrome (EDS), a rare and complex disease that affects my connective tissues, causing debilitating symptoms. Alongside EDS, I battle with kidney issues, including frequent stone formation and cysts, which have resulted in constant infections. Additionally, I suffer from two lesser-known conditions that significantly impact my daily life.
Gastroparesis is one of these conditions. It is a disorder that affects the normal and spontaneous movement of the muscles in my stomach, causing severe discomfort, malnutrition, and a series of other complications. Postural Orthostatic Tachycardia Syndrome (PoTS) is another challenge I face. This condition affects the autonomic nervous system, causing an abnormal increase in heart rate when moving from a lying down to a standing position. The symptoms include dizziness, fainting, fatigue, and difficulty regulating blood pressure, further adding to the complexity of my health problems.
Every day is a battle against my own body. Seizures and difficulty walking have become my new norm in the last two weeks, and for these symptoms, I still have no answer.
The challenges I face are not just medical; they permeate every aspect of my life. A restrictive diet, constant medical appointments, and the need for a new functional wheelchair are just a few of the urgent needs I must address to maintain normalcy for myself and my children, who are my greatest motivation to continue.
I am turning to you, kind-hearted individuals, for support. Your generosity can make an immense difference in our lives. With your help, I can afford the medical care, equipment, and assistance necessary to navigate these tumultuous times.
Your donations will directly contribute to:
- **Medical Expenses:** Covering the costs of ongoing treatments and medications.
- **Mobility Aids:** Acquiring a new wheelchair or adapting my current one, which will enable me to move with greater ease and independence, ensuring I can continue to care for my children.
- **Nutritional Support:** Meeting the expenses of a specialized diet and necessary nutritional supplements to combat malnutrition caused by gastroparesis. Currently, I am extremely malnourished and underweight, which delays my overall improvement.
- **Childcare Assistance:** Allowing me to ensure reliable childcare so I can focus on spending time with my children without compromising my health.
No donation is too small, and every contribution brings us closer to a brighter and healthier future. Your support not only provides practical assistance but also offers hope and comfort during this difficult time.
From the bottom of my heart, I express my deepest gratitude for considering my appeal.
Thank you for your kindness, compassion, and generosity.
Here are the details of my Wise USD account.
Account holder: Vinícius Gomes Tanure
ACH and wire routing number: 026073150
Account number: 8314526911
Account type: Checking
Wise address: 30 W. 26th Street, Sixth Floor
New York, NY 10010
United States “
I can confirm the veracity of her claim please help her she really needs it.
9 notes
·
View notes
Text
Something I see online that's frustrating to me is you'll get people telling the vegan activists who promote veganism as a universal ideal that there are disabled people who can't have a vegan diet, but then a lot of the people who point this out don't seem to know what conditions actually cause that. And then you end up having arguments about that so I want to actually point out a few examples
I think the number one example where there's no way to safely, healthfully avoid having to consume animal products is haemodialysis for kidney failure. People on dialysis need more protein than other people because they lose protein and blood cells during the dialysis process, and they are required to have a low potassium diet because their kidneys can't filter potassium. This means legumes and soy aren't viable alternatives. [x] "Renal dietitians encourage most people on haemodialysis to eat high-quality protein because it produces less waste for removal during dialysis. High-quality protein comes from meat, poultry, fish, and eggs." [x] If you can't meet your protein needs with these foods for whatever reason, you'll be prescribed whey protein powder, which is made from dairy. [x]
Ketogenic diets are also high in animal proteins. They're innately low carb and high in fat, which means legumes and other meat alternatives aren't a great fit. "The ketogenic diet can boost insulin sensitivity and cause fat loss, leading to significant health benefits for people with type 2 diabetes or prediabetes." [x] PCOS, a common condition effecting about 10% of people who menstruate, is also often treated with a low carb, high protein diet because it involves insulin resistance. [x]
Ketogenic diets may also be recommended to treat seizures in epilepsy. [x] It is most frequently used for focal seizures in children, infantile spasms, Rett syndrome, tuberous sclerosis complex, Dravet syndrome, Doose syndrome, and GLUT-1 deficiency. In these conditions, ketogenic diets can reduce or even eliminate seizures.
People with food allergies can find it difficult to afford safe and healthy food in general. [x] The inability to rely on cheap, plant-based proteins like canned beans or dried lentils can be a general hardship, especially when disabilities themselves can limit job opportunities or the capacity to work.
Intestinal disorders are another factor that can make vegan diets difficult. Foods high in insoluble fibre, like beans and other legumes, as well as nuts and seeds, can cause Crohn's flare ups in some people. [x] Seeds, nuts, and legumes can also be trigger foods for people with ulcerative colitis. [x] IBD flare ups are not like a run-of-the-mill case of intestinal discomfort. They can land people in the hospital and require major surgery. [x]
For allergies, the main factor that can make a vegan diet difficult isn't allergy to specific vegetables, but to specific plant proteins. Someone who is allergic to soy, peanuts, or other legumes will have more limited options for meeting their daily protein requirements on a vegan diet. People with allergies to a broad spectrum of legumes may not have any reasonable substitution options. Substitutions can also increase the price point and make a vegan diet too expensive for people in poverty who also have allergies. Poor people with food allergies may find it difficult in general to afford a safe and healthy diet. [x]
For some people, including some disabled people, a vegan diet may in fact be ideal. Vegan diets can certainly be part of a healthy diet when trying to reduce bad cholesterol [x], treat high blood pressure [x], or treat earlier stages of kidney disease. [x] And while insulin resistance may be best treated with a ketogenic diet in some people, others do seem to benefit from a plant-based diet instead. [x] A person's diabetes specialist and trained dietitians can help them figure out which is best for them, potentially based on other factors like whether or not they have high blood pressure or bad cholesterol, or whether their diabetes risks are linked to PCOS or other known metabolic conditions.
Achieving sustainable food production and equal access to a safe, nutritious, well-balanced diet is fundamental to us all. But there's simply no one-size-fits-all ideal human diet, and that's something everyone needs to take into account.
33 notes
·
View notes
Note
do you know of have any good sites that explain organic disorders a bit more? even russian sites? english sites(wikipedia) isn't super helpful,, but it's still a start so if you don't know of any that's alright too!
Well, it's kinda hard to answer.
Because I'm not sure if any place in the internet or even in medical books would answer you that OBD is actually is. I talked to my psychiatrist, to my neurologist, read a lot of books and still like. Who knows. Also, terms between russian ang american are fluctuating...
I can write a little, just. Text based on my research and personal experience, just to make liek. Some sense.
OBD used as an umbrella term for "you brain was damaged and now you FUCKED" and UNFORTUNATELY almost untreatable. Like, patients with OBD are treated from their symptoms and not from the cause. Because. Well. Sometimes cause is "part of his brain now fucking missing".
OBD has smaller disorders under it, like organic emotionally labile disorder (your emotional state are no stable), organic dissociative disorder (bye-bye reality I'm comfy inside) or organic delusional [schizophrenia-like] disorder (at this point this names just gets funny).
But it's. Well. Things that doctors can diagnose from outside. Let's imagine the guy who drowned. A little. And wasn't breathing. For a while. Parts of his brain now damaged because of hypoxia. But THAT PARTS NO ONE KNOWS (actually we partially know, the frontal lobe takes the first hit). So the only thing that doctors can do, is just look at him very hard, ask a lot of questions and diagnose Some Variation of OBD.
It's also the reason why treating people with OBD is that hard. Because who knows that actually broken, let's give them some pills and check on them later. Like. I always joke that I'm taking pills from epilepsy and from bipolar, and I don't have any of them.
There's some symptoms that are almost prevalent in all variations, like
- mood swings
- high irritation and uncontrollable agression
- seizures or/and light sound sensitivity
- migrains
- dissociation
- hallucinations
- depressive and/or manic states
- fatigue
- cognitive problems (learning and understanding).
- INSOMNIA AND SLEEPING PROBLEMS
Some people (specially not diagnosed properly) are frequent to use legal drugs to get some symptoms off. Usually alchol, because it slows brain functions. Like, I have terrible light sensitivity, but if I get drunk blinkin light would not fuck me THAT much.
Anyway. Doctors rarely diagnose people with OBD if it does not have a obvious cause. Like you know "you skull got crushed with hammer. A little. And now you want to set things on fire". But I'm a lucky girl, no one knows that fucked my brain THAT MUCH. No history of brain trauma, bacterial infections, air deficiency. Just was born very very wrong.

9 notes
·
View notes
Note
Please tell me more. We haven't stopped laughing since the entire "Sophie Hunter will be dead in six months from syphilis". You guys are so freaking funny.
Visible lymphedema and petit mal seizures aren't funny. The disease processes behind them can take anywhere from months to a few years to kill a person. Her immune system is completely shot, excuse the pun. I remember when Cunter spread the rumor that Benedict had AIDS during the 2019 MetGala. We still have that Tweet, maybe she was trying to take attention away from herself 🤔...
8 notes
·
View notes
Photo




My Legal Battle with my Family and their Co-horts / Co-conspirators (123):
Forgive me, I know it has been more than two (2) weeks since my last post. But sometimes the stress of it all gets to me (as I will show some evidence of the stress in this post). And please forgive me as I know the picture of my mouth in this picture is a little gross, but it’s important.
I’ve explained over and over about the extreme and continued stress my family causes me, derived from threats to my living situation, threats to my life, economic harm, harm to my employment and career, threats by men with guns and knives and even coordinated physical assaults. This stress has manifested itself in chronic sleeplessness (over the last 2.5 years I have hardly been able to sleep), seizures, and now a canker sore. I know it sounds silly but please read on.
Attached are four images (from top to bottom):
1. This is a brief explanation of what can / does cause canker sores. Most notably, stress.
2. This is a picture of the inside of my mouth that I took today, January 26th, 2023 showing a very painful canker sore I have. This is the first canker sore I have ever had in my life so I did quite a bit of research on the matter.
3. This is an explanation of what chronic (long-term) stress can do to a person. It manifests itself in physical, emotional and behavioral maladies. These inlcude exhaustion, trouble sleeping, headaches, dizziness, shaking, anxiety, depression, panic attacks and smoking. I have highlighted these just mentioned as I suffer from all of these. Although it’s a little embarrassing to me, I have been smoking vapes now for the last 2.5 years but never did smoke prior to that. I also am now taking an anti-depressant, Lexipro. The continued family drama and fright I experience has lead me to need an anti-depressant. It has also affected my ability to trust others. I’m hoping that once I prove everything my family and their cohorts have done, in court, that all of this will improve. I also have been diagnosed by a psychiatrist to have PTSD (Post Traumatic Stress Disorder), to include large amounts of trauma from everything my family has been doing to me for a very long time now.
4. This is a follow-up note / documentation from a Neurologist I used to see. He clearly states in his notes that an important factor in staying “seizure free” is to get sleep. He has also told me that the best way to manage stress and to keep it down is to exercise / lift weights. Something I have been doing since I was at least eighteen (18) years old but have much trouble staying consistent the last few years because the stress and seizures have prevented me from even being able to make it to the gym a lot of the time. This also includes the injuries I have sustained from the seizures. Also because my family threatens me and causes me economic harm which causes me to have to adjust my budget (it’s pretty hard when your family retaliates by affecting your budget and income by $2000 / per month). The economic harm causes me additional stress. The additional stress causes sleeplessness. The sleeplessness alone causes seizures, the stress alone causes seizures, but both of them together causes frequent and intense seizures which are even more life threatening.
5 notes
·
View notes
Text
Personal vent [please do not reblog, although I would love some advice in the comments].
About five years ago, I met a neurodivergent man I’ll call Nick (portion of his real name that he uses as a nickname/online persona when he doesn’t want to use his real name) through a mutual friend of ours. He’s a very sweet man, early 30’s, bisexual and allegedly on his second civil union (he’s supposedly been married twice, both times to same sex partners). He also suffers from a condition called Reactive Attachment Disorder. Nick has told me a variety of colorful stories throughout my friendship with him.
Nick claims to work for a major technology company [not naming the company for privacy reasons] and once was able to get me a deal on a laptop from said company at a heavy discount. Ever since getting me the laptop, Nick frequently claims that he has obtained access to my laptop through the Get Help app on Windows. I’ve given him permission to do this once when I needed a quick tech support consult and didn’t have time to sit through a chat with Dell or Windows.
Recently, Nick has claimed to have “given” me several upgrades to my laptop, but now, I’m suspicious because a. I can see no proof that he’s accessing my computer when he claims to be, and b. I’ve found that most of what he’s asking is seemingly random, single keystrokes (usually the x or ; ) and I can see no evidence that he’s changed anything on my laptop.
I know that some of these keystrokes open certain things, such as device manager, but he claims he’s making all these changes to my computer. He also claims to be “an engineer who works on Windows updates for Dell” and often tells me not to install new Windows updates right away because he’s “still finalizing them” [but why would it be available to me from Windows if it was still being finalized? Also, why can’t I see any evidence of the updates being made?] Unfortunately, however, Nick is not my only issue.
I have another friend tied to Nick, Mandy, [portion of real name] who is always role playing with me to entertain Nick as he “works”. I would be fine with this, if it weren’t for the fact that Mandy has a seizure disorder, and her seizures often cause her to lose significant parts of her memory, which means that we end up, role-playing the same things over and over and over again. Mandy claims that she wants to post the role-plays as a story on the archive of our own website, but she refuses to write any of the scenes down, and she goes so quickly through them, often out of order because she wants to see how a particular scene will play out. This makes it impossible for me to write them down either. Even when I get to a point where we could write them down, she keeps flip-flopping on parts of the story and insisting we play them out again to change it.
Mandy has a host of mental and physical conditions, one of them being maladaptive daydreaming. So, we can be in the middle of a conversation about something totally unrelated to the role-play, and she will say “why can I see…” , And begin role-playing without even asking me. I’ve told her repeatedly that this is something that bothers me, and that she needs to ask me before role-playing, but it never seems to stick.  She claims she does this to entertain Nick, who struggles to read in English because it’s not his first language. If we’re not role-playing a fanfiction, she will lapse into wanting to role-play the story of a novel that she is allegedly, been working on since long before she met me. She made me a character in the novel, despite knowing that I hate the novel concept. She’s flip-flopped from claiming that she wants to publish the novel, despite believing that it will “get her killed because people are not ready for the diversity put into it” and wanting to burn it because her obsession with it upsets me.  I try to change the subject when she does this, but it briefly gets her back on track before she slips into it again. She claims that this is because she has a condition called maladaptive daydreaming.
Recently, we have been creating an In the Heights fanfiction together. In an attempt to get over her dislike of Latin men, due to mistreatment by her Latin father, Mandy paired herself with the main character , and changed his heritage to Afro-Latin to make him “more interesting”. This would be fine, if Mandy [who was raised by a white mother and barely has any connection to her Latin roots] was willing to do any kind of research. She claims she has, but a lot of what she’s coming up with does not make sense. I am fairly familiar with Latin culture, as I have a college degree in Spanish. I’ve actually called her out on several inaccuracies. I noticed this is a habit she makes with her fan fictions, which is irritating, because most of her favorites are related to historical fiction [The Tudors, etc]!
As if that wasn’t enough of a problem, Mandy gets so into her characters that she has been posting on Reddit, pretending to be one of her characters from one of our role-plays. People became so incensed by her posts that they believed the story was real, and Mandy gleefully claims her Reddit account was banned from the r/aita forum.
It has now reached a point where neither Mandy nor Nick will allow me to hang up on our Skype calls without protest. I can barely even go to the bathroom without leaving them on a call, which is difficult for me as I have a disability that makes simple, everyday tasks take much longer. (a disability that Mandy also shares, so she should understand).  I’ve tried speaking to both Mandy and Nick about this, and it always gets better for a little while, but then gets worse again. I really don’t want to walk away from the friendship but I would love advice.
Is there any way that I can get through to them? I tried avoiding them, but it always seems that Nick manages to find some way to contact me or make Mandy do it for him.
6 notes
·
View notes
Note
Yo so about the disability, if you are comfortable publishing asks about it, I got some stuff. I actually struggle with some of the same issues you mentioned. I would say you do not have internalized ableism, but rather imposter syndrome. You feel like you aren’t struggling enough to warrant the label. But you labeling yourself as disables]d does not take resources away from people you view as having it worse, it just gives you an easily communicable term so you can have your needs met. There are people who faint frequently that use disabled parking spaces. They aren’t ‘taking’ those spots from someone who ‘needs the more’, they are using them because it makes the walk shorter so they can get somewhere safe faster. It would be incredibly dangerous if they fainted in the middle of the parking lot. For the fainting thing, it sounds a lot like what I was diagnosed with, POTS: Postural Orthostatic Hypo-Tension. It’s an auto-immune illness that causes your blood to pool in your legs when standing up from sitting/laying down. I felt a tightness in my chest when it was happening, why vision would go fuzzy, I’d sometimes see ‘light trails’ from movement, and it’d cause tinnitus. If that sounds similar to what you are experiencing, you could ask about it. After awhile, instead of fainting I would have a ‘pseudo-seizure’ (non-epileptic seizure) instead of fainting so potentially be on the lookout for that. Anyways, as an auto-immune illness, it effects your sleep and you digestive system as well, which is often misdiagnosed as IBS and other similar things. Also, I ended up being fully diagnosed with Lyme and MCS (Mast Cell Activation) later. MCS causes extreme allergic reactions to high histamine foods like nightshade veggies (tomatos, peppers, potatos), gluten, dairy, soy, sometimes eggs and rice as well. I struggled so much going doctor to doctor and program to program trying to figure things out, as soon as I saw your post I wanted to say something and possibly prevent another person from going to the same struggle. Unfortunately with auto-immune illnesses, it’s basically contract one, get ten free, and they are misdiagnosed so often, it’s hard to find out what’s going on. If this strikes a chord at all with you I could just PM you or something should you be comfortable with that. Anyways, I really hope you figure everything out and are able to get better ! I hope I didn’t overstep at all.
BIG HUG. Not an overstep in the slightest! Thank you so much for sharing your experience; that's very helpful. And I do really appreciate your kind words about imposter syndrome. Yeah. That makes... a lot of sense. These past two years especially, my physical health has really gone downhill despite me living a very active and outwardly 'healthy' lifestyle. But just because most days I can manage, even if I risk falling over several times a day and need to spend an ungodly amount of time in the bathroom... It doesn't negate those issues, or that some days I'm so exhausted I can barely function. Thank you. x
Yeah - the conjunction of POTS, bad digestive issues and hypermobility is why my doctor's looking into EDS for me, but sadly my country's healthcare system is painfully overloaded and slow (and my doctor knows literally nothing about EDS and had to look it up online lol). I can’t afford specialists, so, no diagnosis yet!
Some very gnarly autoimmune stuff runs in my family. My mum's got it and my grandma had it, etc. THANKFULLY I don't have symptoms for that (yet... T^T) but instead seem to be on a diagnostic track for several potential other, apparently unrelated autoimmune disorders! The joy of autoimmune stuff, like you say T^T
..................I wonder if frequent migraines are related, too? I get like, one a month, so not constant, but still not fun! Aren't bodies delightful???? I'll have to mention it to my poor GP; I lose track of what's normal and not normal lmao
Thank you. That really does strike a chord. I'm sending you love as a fellow Chronic Condition Hell sufferer! <3 And I’m absolutely happy to PM if you’d like?
11 notes
·
View notes
Note
Whats spaniel rage? Do spaniels just like go feral for no reason sometimes?
Rage syndrome, also known as spaniel rage as it was first discovered in largely springer and cocker spaniels, is thought to be a neurological misfire or even seizure-like syndrome (due to semi-successful treatment with seizure meds) where an otherwise happy and friendly dog suddenly enters an unprovoked moment of pure aggression. Often these dogs look "out of it" a moment before, and during the attack owners frequently report that the look in their dogs' eyes was vacant and as though the dog was unaware of who or what it was attacking. The attacks are usually quite dramatic and can be severe or mild depending on how quick the dog was to bite vs how quick the owner was to get out of the way. Once the attack is over, often the exact same dog that was attacking the owner now acts confused, disoriented, and sometimes even emotionally distressed to have caused such injury. It is theorized that this is a seizure or similar due to this behavior.
More dogs than spaniels can have rage syndrome though it's unknown if it's related or two different causes leading to the same problem. It does seem to have a genetic link- dogs who rage often have a close relative that exhibited similar behavior. I have known of a border collie with diagnosed rage, and a friend who had spaniels with rage did tell me Skoll's behavior looked a lot like rage to them. Skoll had known abuse and was a known fearbiter, so I cannot say if his behavior once he got to me was as a result of the fear (I think a good portion of it) or if it truly was some uncontrolled neurological misfire (possible, but I'm no doctor).
Dogs with aggression are often misdiagnosed as having rage- rage itself is a fairly rare condition and is only just common enough that people who spend their entire lives with the breeds the most affected by it will have heard of a dog but most have not seen a dog with rage personally.
Some dogs with diagnosed rage improve rapidly with anti-convulsants, lending credence to the theory that it is a seizure disorder. Others not so much. It is hard to say why that is because we simply do not know enough about what causes this problem in the first place. Not all seizure disorders respond well to medication either, so sadly it neither proves nor disproves the idea that rage is somehow a biochemical problem rather than a temperament problem. Compounding the problem is that the diagnosis of rage often is immediately followed up with euthanasia, so the chance to study is relatively low because the rage dx came after a serious bite or mauling incident. However I would say as someone who was on the receiving end of what may or may not have been a rage dog, that facing your dog that's clearly not recognizing you and is literally trying to kill you and being afraid that your dog is actually going to kill you is a very scary place to be, and I don't fault anyone who no longer trusts that dog in their home.
37 notes
·
View notes
Note
Hi! So since you said you were okay with it I wanted to ask you what is a conversion disorder and how it's affected your life maybe? Have a nice day!
yes, ofc! i'll give you sort of an overview of what conversion disorder is & how it affects me - if you or anyone else want to know smth more/more specific, just ask! 💙 also, i’ll be abbreviating conversion disorder as “CD” for convenience. and for ease of access & sort of a tl;dr, i’ll write the main points of this post in bold!
CD is a neurological & psychiatric disorder where the nervous system doesn't function properly - the brain might not send (correct) signals and/or other parts of the nervous system might not receive them (correctly). CD is characterized by the fact that the condition doesn't have a clear physiological cause such as a stroke or epilepsy. it's usually classified as a dissociative disorder, but that varies based on who/what your source is (more on that in the last passage).
instead of having a physiological origin, CD is caused by stress, psychological distress, or trauma. my CD is linked to my (c)ptsd. the symptoms get worse when my trauma is triggered & i even get mild symptoms when i just talk or think about my trauma in enough detail. non-trauma-related stress or anxiety can also cause them & as people with (c)ptsd know, trauma can be triggered by seemingly random stuff, and therefore my CD symptoms can also flare up pretty unexpectedly.
the neurological symptoms themselves can vary a lot from person to person & situation. for me the most prevalent ones are muscle twitches all over my body (myokymia), muteness, sensory issues (such as partial blindness/deafness/numbness), paralysis, disorientation/delirium, and chronic exhaustion/lethargy. out of these, paralysis and exhaustion/lethargy are definitely the ones that come in the way of my daily life the most. wanting to get up/move & do things but physically not being able to is a terrible feeling. i’ve missed out on stuff i was rly looking forward to because i just couldn’t lift my limbs no matter how hard i tried.
severe combinations of symptoms can also manifest in the form of an attack/seizure, usually caused by some major trigger. i stop responding to stimuli, go mute, can't move normally/at all (if i'm standing up when it happens i fall to the floor), twitch and tremble, and don't know where or when i am (especially if i’m also having a (c)ptsd flashback). these attacks can last anywhere from a few minutes to several hours & they are another one of the ways in which CD most affects my life. having an attack is exhausting both mentally and physically & therefore my symptoms are also worse over the few hours/days following an attack (and i’m more susceptible to having another one). and in general it’s just scary to lose control of your own body.
from what i've read, my symptoms seem to be pretty typical, but like i said, there are a lot of ways CD can manifest. common symptoms i've read about but don't experience myself include inability to control the bladder, difficulty swallowing, and seizures that are more epilepsy-like than my attacks. the severity of symptoms can also vary a lot - for example, some people need to use a wheelchair because their legs are too unreliable or rarely work at all. other ways to manage CD include physical therapy & relaxation techniques for the symptoms, psychotherapy to combat the triggers causing CD, and medication to help with comorbid depression/anxiety/et cetera. the general consensus is that CD can’t be completely “cured”.
CD is relatively rare and scarcely researched, even controversial. due to the lack of info & physiological cause, some doctors still don’t even think it’s real and is instead feigned by the patient. “faking it” is a common accusation people with CD face, especially bc stress flares the symptoms up. for example, i’m definitely more likely to experience paralysis before an exam i’m dreading than a fun party i’m looking forward to, which people can interpret as me just not “wanting” to do difficult or unpleasant things. but that’s not the case & the symptoms also frequently prevent me from doing the fun stuff, especially if it’s preceded by something even menially stressful. you want to go to the party, but your body refuses to move because going would require you to walk 5 minutes to the bus stop, which is “too taxing”.
some doctors, on the other hand, see CD as a misdiagnosis for other neurological/psychiatric disorders. this theory has its roots in the fact that CD was previously known as hysteria, the infamous diagnosis given to women who showed basically any symptoms doctors just wanted to dismiss. as the medical field & attitudes towards women's health evolved, most hysteria diagnoses became obsolete/replaced by other, more appropriate diagnoses. CD took the place of hysteria in describing neurological symptoms brought on by a psychological cause. and nowadays we obviously also know that the symptoms in question aren’t exclusive to women.
last disclaimer: because of the lack of info & evolving research, the exact classification of CD varies. DSM classifies it as a somatoform disorder, while ICD (which was used for my diagnosis) has it under dissociative disorders. furthermore, some people experience neurological symptoms that seem to have neither a physiological nor psychiatric cause, and because CD generally requires the latter, people without one are sometimes given the diagnosis of functional neurological disorder (FND) instead. CD and FND are also sometimes used interchangeably, or CD can be classified as a subset of FND - basically a functional neurological disorder with a known psychiatric cause.
#this was a long one! i'm sorry if you wanted a neat summary :') i added the bold for that reason#i just thought that if i was gonna write this down i might as well do it as coherently and completely as possible#especially since i've been thinking of sharing my experience on other platforms and i could use this answer as a blueprint!#answered#anonymous#conversion disorder#functional neurological disorder#fnd#ptsd#cptsd#trauma#actuallytraumatized#long post
47 notes
·
View notes
Text
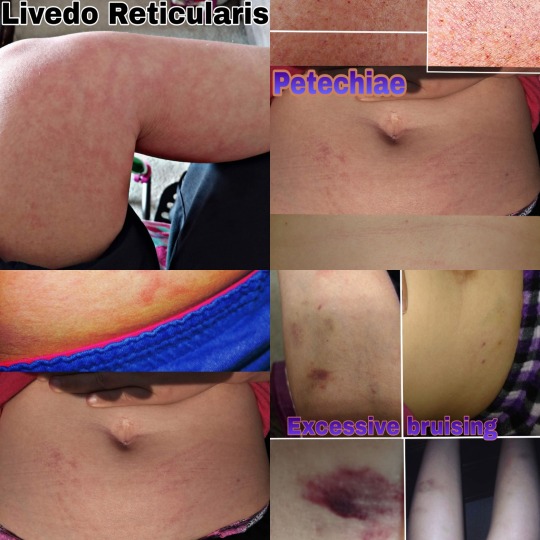
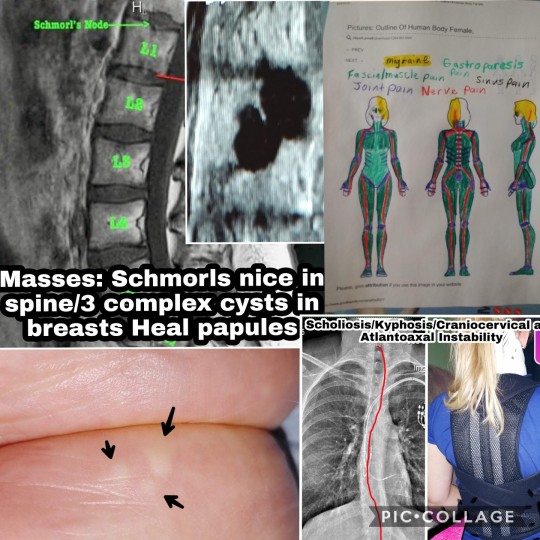
2021 Ehlers Danlos Society Awareness Month (Day 3 Prompt: Symptoms)
Unbeknownst to most people in the community and even many in the medical community as most medical personnel never learned about EDS in school or if they have were only taught the very most basic information about it but Ehlers Danlos Syndrome is a systemic condition and predisposes those with it to over 250 other conditions so it's not unusual for someone with EDS to have 20, 30 or even more other conditions caused by it which are called comorbid conditions or comorbidities.

EDS is a genetic condition that affects the structure of connective tissue. There are multiple types of connective tissue but there are also multiple types of EDS so one or more types of connective tissue can be impacted. Connective tissue also makes up at least part of every part of the body so when your connective tissue is faulty and prone to damage that also means so is everywhere connective tissue is located including but not limited to the skin, cartilage, the brain, heart, lungs, GI system, liver, kidneys, bladder, Mesentery system which is the stringy organ that is around your abdominal organs that eases then and holds them in place, lymph nodes, lymph ducts, nerves, blood vessels, blood cells, nerves, bones, bone marrow, joints, tendons, ligaments, muscle sheathing, eyes, ears, nails, hair follicles, spinal cord, sweat glands, respiratory system etc. You name it, it contains connective tissue so anything can go wrong with any part of the body leaving many patients diagnosed with conditions such as conversion disorder, meaning that all of your symptoms are in your head and you're fine for years and more often, decades because we usually get diagnosed with a lot of these comorbidities before we finally find that one doctor who can put the pieces together and say, this isn't in your head, you have Ehlers Danlos Syndrome and those other conditions are very real because EDS is what caused all of them.

Now that we have discussed comorbidities I have dealt with countless symptoms over my life. As a kid it started with chronic pain, migraine headaches, and issues resulting from a compromised immune system because I caught everything going around and usually more than once. I don't remember a holiday as a kid where I wasn't sick or hurt. I was extremely clumsy, unable to run correctly until high-school with the very extensive help of my gym teacher. I was always falling, rolling my ankle, and just in general looking awkward with my body movements. I had multiple gym teachers who would agree that there was something physically wrong with me long before I could get any doctors to listen to my mom or as an adult, myself. I had to take special reading and writing classes because even to this day I cannot hold a pencil well or write with control because my fingers are too hypermobile to control a pencil so my writing is often illegible. I had a very severe failure to thrive, also called juvenile dwarfism, not even growing an inch between the ages of 2 and 12. My parents were told when I was 2 years old that I would be 6’4’’because I was so tall as at one and two years old that people would criticize my mom for carrying me out in public thinking I was 4 or 5 years old when I was only a year or two years old. I was 3’2” from the age of 2 to the age of 12 and of course when I was 12 I was extremely short and was bullied for my size as well as my weight which increased due to inflammation from undiagnosed celiac disease. There were multiple incidences with medical personnel and social workers as a kid because I always had such severe bruising all over my body and they believed I was abused. I didn't lose my teeth, losing only one on my own and at the age of 8 my dentist began pulling out my teeth which left me with dental crowding and requiring braces which were removed prematurely. I dealt with Learning disabilities and have been in glasses since age 4. I would pass out all the time as a kid, starting at 8 years old.

Bullying was a huge issue for me as a kid because I was socially awkward showing signs of OCD as well as being more mature than my peers due to my medical experiences and history with my siblings that forced me to grow up more quickly. That combined with issues such as my clumsiness and height made me the perfect target for bullying. I got what I believe was my first Traumatic Brain Injury when I was 9 years old while hanging upside down on the monkey bars. My bully had another student who had Down Syndrome, climb to the top of the monkey bars and lift my legs so I fell off onto my head.
My second was in the 6th grade. The same bully would bully other kids to help her bully a bigger target of hers which was me. One day I was at my locker between classes. Our lockers were assigned in alphabetical order by last name, of course my bully's last name came right before mine so her locker was directly to the left of mine. My mom tried to get it changed but the school refused. She shoved me down between classes while I was exchanging my books and the two kids with the locker to the right of mine she had help her roll me onto my stomach on the ground, one sat on my butt and held my feet down, the other sat on my back and held my arms down under her feet. my bully yanked my head up so my forehead was on the floor of my locker and I was trying to get out so she had the girl on my back use one of her hands to hold my head down. My bully then kicked my locker door shut on my head over and over again and I went unconscious. There were two teachers in the hall at the time but they just waked into the classroom when it started. I woke up and the hall was empty. I went to the office and told them I needed them to call my mom, I needed to go home and explained what happened. They called my mom and instead of telling her the truth they told her she needed to pick me up because I was acting strange. She came and got me and found out what happened getting me treatment.

She then took me to the school a few days later since the doctor didn't want me to return for so long (I apologize I don't remember a lot from the two weeks following this so I'm going off what I was told so the exact time I was out of school, I believe was around two weeks but I'm not sure. Anyhow at the school, we met with the principal and office staff who denied any teachers were in the hall or that any of this happened. My mom demanded to see the recordings on the cameras as a hall came in at a T right behind my locker so that camera faced my locker as well as one at each end of the hall my locker was in. They tried to tell her all three cameras were broken. My mom wasn't buying it so they tried then saying the recordings were gone. they went round and round and the school flat out refused to show her the video. My mom demanded that the girl who did this be punished because she has been asking for the school to help me since I was in the first grade and this girl started bullying me but they always fail to do anything.
They tried to then give me an in school suspension which my mom refused to let them do. They still went behind her back when I returned and made me take peanut butter sandwiches to the kids in detention during my lunch as punishment because they were mad my mom came in to question the incident. They refused to punish my bully in any way and when my mom demanded to know why, they said her mom and grandmother graduated from the school so she has a lot of history with the school which years later we found out after me and 9 other kids that I know of and who knows how many others, ended up being pulled out of the same school because of her bullying that having history at the school actually turned out to mean, she was black and they would not punish her because of her color. At the end of the school year my mom pulled me out of the school not sure what to do since back then they didn't have any kind of free online schooling so pretty much everything costed money which is when my grandma stepped up and told my mom she would help because there was no way I would be going back to deal with more bullying.
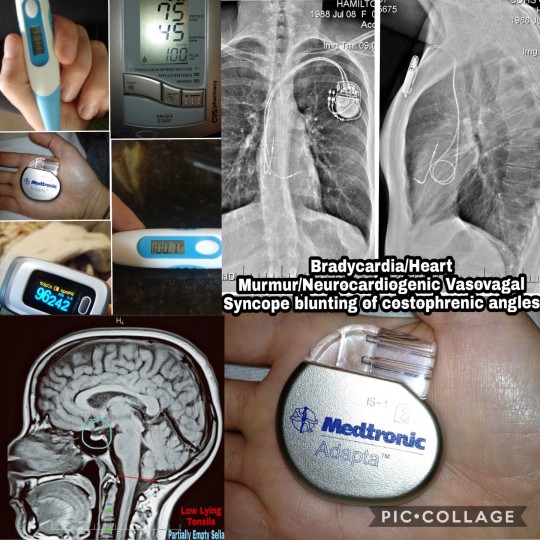
I had a ton of intestinal issues having to start colonics at around 10 years old and get my first colonoscopy around the same time. As a teen I really went down hill, struggling to eat because I had very severe nausea and cramping pain upon eating which made many of my friends believe I was anorexic but I went years without being diagnosed with gastroparesis. I started having thyroid issues and finally diagnosed with food allergies at age 14, Chest pain, palpitations, arrhythmias and trouble breathing around age 15 and seizures and cardiac arrest events at age 17.
At age 19, right before starting college I lost the ability to walk with no reason why and was sent to physical therapy to learn to walk again. The hospital visits continued in college from the seizures, emergencies from my thyroid levels going sky high or bottoming out, I started having issues with low sugar, rectal bleeding and more GI and Muscular Skeletal issues that again came to the attention of a physical education professor I had in college. The cardiac arrests continued to happen and I got an emergency pacemaker put in at age 23. Also lost the ability to walk a second time and re learned during this time.

After graduating and starting working I really went down hill. My nerve pain got so bad I could hardly tolerate it and had a lot of issues with muscle spasticity. Passing out and dizzy spells got worse, seizure meds aren't working muscle weakness got again worse in my legs and I started literally wondering if I was dying, I had such severe fatigue that I slept every moment I wasn't working, bleed very badly during my period or with just mild trauma worrying my dentist so badly that he sent a letter to my doctor suggesting a possible bleeding disorder. I was going into shakes from low sugar and low sodium frequently but at the time had no idea why I would start shaking multiple times a day. Myoclonic epilepsy started and has progressively gotten worse, Dystonia started up, I started getting intestinal obstructions more often and more gastroparesis symptoms with the nausea and vomiting, sometimes cyclic vomiting. I developed a limp and went onto forearm crutches which eventually progressed to paralysis.
I have always had issues with dislocations of joints and spinal manifestations like scoliosis, Craniocervical and Atlantoaxial instability. I’m prone to non cancerous masses that could be cancerous one day including masses in my breasts, heals and between the vertebrates in my spine. My memory has deteriorated and I now have issues which I call temporary blindness when I turn my head a certain way which pinches my already compressed brainstem kinking it off so my vision is interrupted. With Systemic Mastocitosis I deal with allergic reaction type symptoms such as anaphylaxis, overproduction of mucus, coughing, hives, swelling, rashes, itching, hot flashes, flushing and more. I overheat and have hyperhidrosis. I have muscle spasms from the paralysis, dry mouth from the meds, in addition to the heart arrhythmias and trouble controlling my body temperature from the damage to my autonomic nervous system failure I have swelling of my abdomen, extreme thirst, bladder retention, abdominal cramping and more.

There are endless symptoms associated with EDS and it’s comorbidities which has a huge impact on your social life. You can't do the things you used to do and may come up with new hobbies and later deal with the grief associated with losing the ability to do those hobbies, in turn having to find new hobbies. You lose all or almost all of your friends because they don't like what you have become, the things you used to be able to do with them and no longer can, they don't understand if you need to cancel plans, when you lose the ability to drive they drop you cold because they don't want to pick you up many of us deal with the realization of how badly we wanted friends growing up due to our social awkwardness that resulted from our illness, time spent in the hospital, maturing more quickly, as well as the result of decades of medical abuse and neglect which in most of us has resulted in complex PTSD.
Almost all EDS patients are either on the Autism Spectrum, diagnosed with Obsessive Compulsive Disorder which some associate with social awkwardness and also the intense need for us to please people meaning many EDS patients were known as extremely hard and dedicated workers when working or in school as well as very dedicated to friends and families. We basically give our friends the clothes off of our backs meaning that most of us unknowingly befriend people who use us and are in take take take relationships where we give everything we have into a friendship or relationship while the other person gives little back resulting in most of us losing all or almost every friend we had when we get sick and no longer have anything to give. When we are no longer able to do for others those people quickly jump ship leaving us with no friends. Most of us have this very similar personality type due to our history of growing up quickly along with the shared comorbidity of Autism, OCD, and Complex PTSD.

There are countless symptoms associated with EDS and they are different for each individual. Even in my case alone these are only the tip of the iceberg when it comes to symptoms I have experienced alone so EDS isn't an easy condition to live with physically or emotionally and the diagnosis can be quite the pill to swallow with little understanding from friends, sometimes family or even the medical community.
2 notes
·
View notes
Text
NEWS IN BRIEF
ECONOMICS
EDUCATION
ENVIRONMENT
SOCIAL JUSTICE
FEATURES & INVESTIGATIONS
IDEAS
AUDIO
ABOUT
IMPACT
CONTACT
PITCHING
CAREERS
PARTNERSHIPS
TERMS OF USE
PLATFORM PRIVACY
PRIVACY SETTINGS
HOME
SOCIAL JUSTICE
THE MANY HEALTH BENEFITS OF METH
In low, pharmaceutical-grade doses, methamphetamine may actually repair and protect the brain in certain circumstances. But stigma against the drug could be harming patients and holding back research.
TROY FARAHMAY 15, 2019
D-methamphetamine is what generally appears on the street—although it's often cut with other chemicals—whereas l-meth provides a less addictive, shorter-lived high that is less desirable among drug users.
(Photo: Fiona Goodall/Getty Images)
Ask your doctor about methamphetamine. It's not a phrase you'll ever hear on TV or the radio, but here's a secret: Meth is an incredible medicine. Even the Drug Enforcement Administration admits it, and doctors are known to prescribe it for narcolepsy, obesity, and ADHD. Historically, meth has been used to reverse barbiturate overdoses and even raise blood pressure during surgery. Some preliminary research suggests that meth can be neuroprotective against stroke and traumatic brain injury, even stimulating the growth of brain cells.
Yet we're constantly warned never to try meth—"not even once," goes the refrain—or it will instantly cause addiction and ruin your life. Before fentanyl was the demon drug du jour, meth was seen as the worst, most destructive, most evil chemical you could find on the streets. Even of late, if you ask the New York Times or NBC, you'll learn that meth, "the forgotten killer," is back with a "vengeance." Other outlets, from Rolling Stone to CNN to The Daily Beast, have raised the alarm about meth use in the context of the opioid overdose crisis.
Stimulant-related deaths are indeed on the rise in North America—in some regions, meth is even more prevalent than heroin. Surveying drug overdoses in America from 1979 through 2016, researchers wrote in Science in September of 2018 that "Methamphetamine deaths have increased most dramatically in the western and southwestern United States."
Meth poisonings accounted for an estimated 14,845 hospitalizations in 2015, according to the Centers for Disease Control and Prevention (CDC), and another 15,808 emergency room visits. In 2016, around 7,500 people died from overdosing on stimulants, including meth. If you ask most people, including policymakers, you'll hear that meth is a scourge that can do no good.
But if you've ever used something like Vicks VapoInhaler, you've experienced the healing benefits of meth firsthand. That's because the over-the-counter nasal decongestant contains levomethamphetamine, the levorotary form—or "mirror image"—of the same stuff from Breaking Bad. Procter & Gamble tries to obscure this fact by spelling the active ingredient "levmetamfetamine." Selegiline, a drug for treating Parkinson's and Alzheimer's diseases, also metabolizes into levomethamphetamine.
There is a significant difference between these two opposing molecules. D-methamphetamine is what generally appears on the street—although it's often cut with other chemicals—whereas l-meth provides a less addictive, shorter-lived high that is less desirable among drug users. But people can and do use it recreationally. Abuse is rare, however, in part because the high is shitty, but also because d-meth is so widely available. It's easier to buy a more powerful form of the drug on the street than it is to try to extract it from over-the-counter medications.
Other Americans are prescribed actual, pure meth by their doctors. It happens less frequently these days, but in ADHD, obesity, or narcolepsy cases where nothing else has worked, a drug called Desoxyn (methamphetamine hydrochloride) can sometimes help. It can even be prescribed to children as young as seven.
It's important to make these distinctions. Meth didn't make a "comeback"; it never left. It can't return with a "vengeance" and it can't be "evil" because we're talking about a chemical compound here. It has no personality, no feelings, no intentions.
Thus it does a disservice to science and to medicine, as well as to the people who use these drugs responsibly, to treat a molecule with dualistic properties purely as a poison. And as recent research has shown, we're still uncovering some of the potential therapeutic benefits of methamphetamine. Confronting the stigma associated with meth and highlighting its benefits can better inform drug policy and addiction treatment.
(Photo: HO/Royal Thai Navy/AFP/Getty Images)
'IT'S JUST A STIMULANT, LIKE ANY OTHER STIMULANT'
For Jordan*, the meth he's prescribed works better against his ADHD with fewer side effects than the Adderall he'd been on for 20 years. About five years ago, Jordan asked his doctor if he could try methamphetamine. The doc said sure.
"The first time I brought it to the pharmacy, the pharmacist actually said to me, 'Oh, your doctor wrote this prescription wrong, this is the stuff that they make in meth labs,'" Jordan tells me by phone. "I told him to type 'Desoxyn' into the computer, and he did. He kind of backtracked, [but] he obviously had no idea."
Jordan, a middle-aged man from North Carolina who works in clinical research, now switches every three months between Adderall and Desoxyn to prevent building a tolerance to either stimulant.
Methamphetamine and amphetamine (one of the active ingredients in Adderall) are almost identical chemicals. The main difference between the two is the addition of a second methyl group to methamphetamine's chemical structure. This addition makes meth more lipid-soluble, allowing for easier access across the blood-brain barrier. Meth is therefore not only more potent, but also longer-lasting.
"The medications have definitely been important for me, to be productive, to be successful, not just at work but also in my personal life," Jordan says. "I've been on the medications for years, but I can take Adderall or methamphetamine and take a nap afterwards. I don't have any noticeable side effects."
Jordan also doesn't feel "high" from the doses he takes—approximately 10 to 15 milligrams of meth per day. Doses at this level are well tolerated by most people. It's very difficult to estimate the typical dosages of illicit meth taken on the street, but they are generally many times higher and taken every couple of hours. Further, the route of administration—typically, users smoke or inject illicit meth—allows for more of the drug to enter the bloodstream than taking a prescription pill.
At high doses, meth gives a rush of euphoria, boosting attention span, zapping fatigue, and decreasing appetite. Intense sexual arousal, talkativeness, and rapid thought patterns are also common. Body temperature and heart rate shoot up, which can cause irregular heartbeat, increasing the risk of seizures. If taken repeatedly over long periods, street meth can be highly neurotoxic, inducing paranoia and psychosis.
But illicit meth is also often used to self-medicate, according to Mark Willenbring, an addiction psychiatrist from St. Paul, Minnesota, with over 30 years of practice treating substance-use disorders. In Willenbring's experience, most of his patients who use illegal meth are treating undiagnosed ADHD.
"There's a high degree of comorbidity between substance-use disorders and ADD," Willenbring says. "They used meth for years in a controlled way, they never over-used it, they just used enough to get an effect, and then they stopped. One misconception is that it's always very addictive."
With most people who are addicted to meth, Willenbring says, you can't tell it just by looking at them. Carl Hart, a neuroscientist in Columbia University's Department of Psychology, agrees that the image of a snarling meth addict with bad teeth is a false stereotype. The dental damage so prevalent in anti-drug propaganda, he says, is more likely due to poor nutrition and lack of sleep—not to the drug. "There is no empirical evidence to support the claim that methamphetamine causes physical deformities," Hart wrote in a 2014 co-authored report.
"It's just a stimulant, like any other stimulant," Willenbring says. "It's a marketing issue."
Part of the reason Jordan asked to try Desoxyn in the first place was to see if he'd develop any of the "stereotypical meth addict problems," as he puts it. He hasn't.
"Those of us that know the reality have a responsibility to say, 'Hey, not that shooting up meth isn't bad, but the chemical itself isn't bad,'" Jordan says. "It's just misuse of the chemical that's bad."
For Joan*, a 66-year-old grandmother living off the grid in northern Georgia, Desoxyn makes her feel normal. "Not high, not hyped up, just normal," she tells me. She's been taking prescription meth since 2006, but first tried many other ADHD meds, such as Ritalin and Concerta, with poor results. But Desoxyn has not only helped her socialize, manage bills, and finish her master's degree in social work; it's also helped with Joan's depression and self-esteem.
"The only downside is the cost," she says. "It's one of the oldest drugs on the market, but even generic, it is outrageously expensive."
Still, meth isn't for everyone, of course. Kevin*, a 31-year-old artist from the Midwest, was first prescribed Desoxyn at age 15 to treat extreme fatigue and trouble focusing. But misdiagnosed mental-health issues—his doctors thought he had bipolar disorder, when in fact he had post-traumatic stress from childhood abuse—led to worsening symptoms.
"Being able to just take a bunch of pills that made the exhaustion go away for a while felt like a blessing, but it was just a Band-Aid on the problem," Kevin says. "I became completely dependent upon Desoxyn to function, and any lapse in taking my dose would result in a terrible energy crash."
"In retrospect, my neurologist at the time would have done well to consider the effects of intense stimulants on someone already prone to mania, insomnia, and hallucinations," he says. "I think Desoxyn has its merits as part of a treatment plan for attentive disorders, but that's the thing—it needs to be part of a larger understanding of how and why it might have a negative impact upon the patient's overall health, and should remain closely monitored throughout."
"Stigma is the lens [through] which we see all drug issues. It keeps us from making the best decisions. It is fear-based, not rational, not creative. Because of stigma, we have not fully addressed the opioid crisis."
(Photo: Guillermo Arias/AFP/Getty Images)
HOW METH CAN TREAT BRAIN INJURY—AND MUCH MORE
Street doses of meth can be extremely damaging to your health. The purity of such drugs is often unknown, and repeated, high doses of meth have been proven to be neurotoxic. But in low, pharmaceutical-grade doses, meth may actually repair and protect the brain in certain circumstances.
This was first discovered in 2008, when researchers at Queen's Medical Center Neuroscience Institute in Honolulu, Hawaii, analyzed five years of data on traumatic head injuries. They unexpectedly found that patients who tested positive for methamphetamine were significantly less likely to die from the injuries. The authors suggested that meth could have neuroprotective benefits.
To learn more, in 2011, a different team from the University of Montana applied meth to slices of rat brain that had been damaged to resemble the brains of stroke victims. Then they induced strokes in living rats, using a method called embolic MCAO, and injected them with methamphetamine. At low doses, the meth gave better behavioral outcomes and even reduced brain-cell death. At high doses, the meth made outcomes worse.
Because meth stimulates the flow of important neurotransmitters—dopamine, serotonin, and norepinephrine—the Montana researchers theorized that methamphetamine may provide neuroprotection through multiple pathways. David Poulsen, one of the researchers involved, says this was a "serendipitous discovery."
"So we decided, well, if it worked in stroke, it's probably going to work really well in traumatic brain injury," says Poulsen, now a neurosurgeon at the University of Buffalo who specializes in treatments for protecting the brain after severe damage.
Traumatic brain injury, or TBI, occurs after a violent smash to the skull. Its consequences include concussions on the mild end and coma or death on the severe end. TBI kills around 50,000 Americans annually, according to the CDC, while about 2.8 million of us visit the emergency room for TBI-related injuries every year. There is currently no Food and Drug Administration-approved treatment for TBI.
So, Paulson and his team reasoned, if meth can already be prescribed for children, why not to adults with TBI?
To test the proposition, Poulsen and colleagues gave TBI to rats. Giving an animal brain trauma isn't easy, but for more than two decades, there's been a trick called the rat lateral fluid percussion injury model: Simply cut a hole in the skull of a rat and apply water pressure to the brain.
About half the rodents—19 male Wistar rats—were given this treatment, and eight of these were then given meth. The rats given meth performed better at a task called the Morris water maze, a widely used experiment that involves plopping a rat into a pool of water with a hidden platform. By tracking how long it takes the rodent to find the platform, scientists can measure many different aspects of cognitive function.
"By the third day of training, there were no statistically significant differences between the uninjured control rats and the injured rats that had been treated with methamphetamine," Poulsen and his colleagues wrote.
But the team also found that low doses of meth were protecting immature neurons, while also promoting the birth of new brain cells that are important for learning and memory. The same was also true for rats that were given meth, but not injured.
"We see not just little, but very significant improvements in cognition and behavior," Poulsen says. "Their memories improved, functional behavior is improved.... It's not a trivial difference."
"In light of the fact that low-dose methamphetamine is FDA-approved for use in juveniles and adults, we see no valid reason why it cannot be utilized in human clinical trials for stroke and TBI," Poulsen and colleagues concluded in 2016.
But those clinical trials, considered the gold standard for testing medication, have yet to materialize, even while a 2018 retrospective study found similar results to the Hawaiian neuroscience report: Out of 304 patients with TBI, those who also tested positive for meth had better recovery results than those who did not. "The potential neuroprotective role of meth and other similar substances cannot be ignored," the authors wrote in Clinical Neurology and Neurosurgery last July.
There are limited conclusions that we can draw about these rodent and retrospective studies, and it's probably unlikely that nurses will soon start giving meth to people who have cracked their skulls. Still, a wide variety of stimulant therapies for TBI is being explored, with positive results. These include trials with modafinil, a narcolepsy drug; amantadine, a Parkinson's drug; and dextroamphetamine, one of the components of Adderall. But there's still no indication of a single clinical trial for methamphetamine for TBI registered with the National Institutes of Health.
Methylphenidate, also known as Ritalin, seems to be the stimulant most popular in these trials. For example, in 2004, researchers at Drucker Brain Injury Center at MossRehab Hospital in Pennsylvania gave methylphenidate, better known as Ritalin, to 34 patients with moderate to severe TBI. They reported significant improvements in information processing and attention.
Twelve years later, in Gothenburg, Sweden, another 30 patients suffering from prolonged fatigue following TBI were given methylphenidate and observed for six months. They also showed improved cognitive function and reduced fatigue. But a 2016 meta-analysis of 10 controlled trials found the main benefit of giving methylphenidate for TBI was increased attention, "whereas no notable benefit was observed in the facilitation of memory or processing speed," the authors wrote. They encouraged more research into appropriate dosages and length of prescription.
Birgitta Johansson, a neuroscientist at the University of Gothenburg and lead author of the Swedish study, suggests caution whenever treating someone with a brain injury. "With methylphenidate, it is important to be aware about possible side effects, [such] as increased blood pressure and heart rate and also risk of anxiety," she says. "It is always very important to prescribe medication with care and follow the patient carefully."
But the reason meth isn't studied more rigorously—for TBI, for Alzheimer's and Parkinson's, for stroke—could also come down to money. Methamphetamine is off-patent, meaning there may be less financial incentive for pharmaceutical companies to explore the drug's potential uses. Consider Vyvanse, a drug first marketed in 2007, with a new formulation introduced in 2017, that racked up $2.1 billion in sales in 2017. Desoxyn, which is sold by three companies, only earned about $9.3 million in 2009.
While Methamphetamine may not be widely recognized as medicine, it clearly has potential to heal as well as harm. Recognizing the duality of meth is arguably all the more essential in the face of a rising stimulant overdose crisis.
"Stigma regarding any substance use or substance use disorder is counterproductive," says Dan Ciccarone, professor of family medicine at the University of California–San Francisco. He says the overdose crisis is shifting from opioids to stimulants and that we are not prepared for the next wave. "Stigma is the lens [through] which we see all drug issues. It keeps us from making the best decisions. It is fear-based, not rational, not creative. Because of stigma, we have not fully addressed the opioid crisis."
That stigma remains a major hurdle, and until doctors and public-health officials counteract this kind of messaging, it seems unlikely that a multinational pharmaceutical company would risk marketing a substance only believed to be toxic and deadly.
"Everything will kill you, if you take enough of it," Poulsen says. "Some things don't require a lot to do that. Meth is one of those things. But just like any drug, the difference between a poison and a cure is the dose."
*These names have been changed.
TAGSALZHEIMER'SADDERALLTRAUMATIC BRAIN INJURIESFEATURES & INVESTIGATIONSMETHAMPHETAMINEMETHTOPIC: HEALTH CARE
BY TROY FARAH
Troy Farah is an independent journalist and photographer in California. His reporting on science, health, and narcotics has appeared in Wired, Ars Technica, Smithsonian, Discover, Vice, and elsewhere. He co-hosts the drug policy podcast Narcotica.
ENVIRONMENT
STARRY, STARRY SKIES
California desert town takes back the night, wins rare "Dark Sky" award
SOCIAL JUSTICE
WHAT IS THE FUTURE OF PAID PARENTAL LEAVE IN AMERICA?
The U.S. has a rough track record with how it treats new parents, but there are reasons to believe that this could soon be a thing of the past.
NEWS IN BRIEF
THESE MAPS SHOW WHAT GRAHAM-CASSIDY WOULD MEAN FOR YOUR STATE
A new report concludes that the Graham-Cassidy proposal would reduce federal funding to states by $215 billion by 2026.
SOCIAL JUSTICE
THE FAULT IN OUR STAR NAMES
The International Astronomical Union has established a committee to finalize a list of official star names. Some companies offer unofficial naming rights for purchase. But the voices of certain communities are often left behind.
ENVIRONMENT
HOW MUCH CAN DIETARY CHANGES AND FOOD PRODUCTION PRACTICES HELP MITIGATE CLIMATE CHANGE?
Food policy experts weigh in on the possibilities of individual diet choices and sustainable production methods.
UNSEEN AMERICA
LAS MANOS JÓVENES QUE NOS ALIMENTAN
Se calcula que 524,000 niños trabajan inimaginables largas horas en los agotadores campos agrícolas de Estados Unidos, y todo es perfectamente legal.
About
Impact
Contact
Pitching
Careers
Partnerships
Terms of Use
Platform Privacy
© 2021 Grist
3 notes
·
View notes
Text
Genetically unhealthy reptiles
So there are quite a few unhealthy reptile morphs out there and I only discovered most of them by fluke, so I thought I'd make a masterpost. There are likely many more which I haven't heard of yet, so feel free to expand on this post with others.
Enigma Leopard Geckos


The Enigma morph is one that covers the Geckos body in little spots that look like freckles, very cute but it comes with a devastating condition known as "Enigma syndrome” This disorder affects a Geckos fine motor control and results in many secondary symptoms such as stargazing (looking upwards frequently), walking around in circles frequently, wobbly and difficult walking, seizures, and an inability to catch prey due to their aim being affected from this condition. Overall it significantly decreases their quality of life. An animal may not demonstrate this condition for many years, it can come on years into their life. This is a dominant genetic disorder meaning any animal which is an enigma will pass this onto offspring. Even 'healthy' appearing animals will carry this gene and pass it along to offspring. The Enigma morph needs to be phased out completely since all who are Enigma have the potential to develop this disorder.
Sunkissed Corn Snakes


The Sunkissed morph is pictured above, rather striking in its vivid colouration. However the price for it is something known as "Stargazing Syndrome" which is pictured in the right side photograph. Stargazing syndrome is a vestibular syndrome (balance affecting condition) which prevents normal functionality of the central nervous system and causes these snakes to twist their necks and heads upwards towards the sky. Basically put, these snakes can't work out which way is up and are often found upside down on their backs. It affects these snakes by causing difficulty moving, disorientation, inability to right themselves into a normal position if on their backs, and sometimes even tremors and seizures. Once again a genetic disorder, however since its recessive you often won't know if the snake is a carrier or not. The only way to tell if a snake carries the stargazing trait is to breed them; any who prove to carry this trait should never be bred again.
Spider Ball Pythons
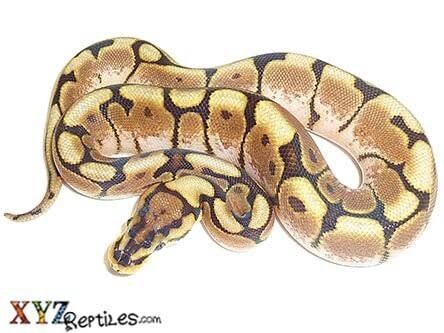
The Spider morph is absolutely stunning, characteristic of that 'drippy' black patterning on the body and a rather unique head stamp/pattern. It can come in many varieties since it's commonly bred into other morphs such as pied, banana, etc. However it causes something called "Wobble Syndrome" which is a severe neurological disorder. This is hypothesised to be caused by an error in the neural crest during embryonic development. The neural crest is responsible for arranging neurons in the correct positions and depositing pigmentation. This morph alters where pigment is usually placed in the body, giving them the gorgeous appearance, however it consequently prevents neurons from reaching their correct positions, hence the neurological disorder. Wobble Syndrome causes many severe and debilitating issues to the snake. The most noticeable being 'corkscrewing' which is where the snake will flip it's head and neck upside down, right way up, and upside down again in quick succession. However they are also affected by head tremors, difficulty moving, lack of coordination, inability to right itself if upside down, torticollis (neck spasms), poor muscle tone, and difficulty eating due to head wobbling and missed strikes. Wobble Syndrome is a dominant genetic disorder meaning any snake which expresses the spider phenotype will suffer from and pass on this disorder to offspring. It can range from barely noticeable to severe, and an animal may not suffer at first, but can develop the disorder after several years of being 'healthy'. The Spider morph needs to be phased out completely since all who are Spider have the potential to develop this disorder.
Jaguar Carpet Pythons


The Jaguar morph has to be one of the most visually stunning morphs out there, it's characterised by it's gorgeous spots which resemble a jaguars. However the price they pay for their beauty is once again, "Wobble Syndrome". Jaguars are identical to Spider Ball Pythons in their suffering, and it's even thought that the Neural Crest deformity is the cause for these guys too. It is important to note that there are several species who can carry the jaguar gene. The gene originated in Jungle Carpet Pythons but has since been bred into other Carpet Pythons (CP for short) species such as the Irian Jaya CP, Darwin CP, Coastal CP, and Diamond CP. Pretty much the only difference with the Jaguar morph is that it is not a dominant gene like the spider morph, and it's not a recessive gene like the sunkissed morph. The Jaguar gene is a co-dominant mutation. What that means is that the Jaguar gene is visible along with whatever other gene the snake carries. You almost always have two genes for something, and in codominance neither of those genes are recessive to the other, and neither are dominating to the other either. This means both genes express, so to put that into a visual sense (but not genetically accurate!) if you bred a black and a white cat together, the offspring would be black and white if they were co-dominant. This just like the spider and enigma morph means any snake which expresses the Jaguar phenotype has the ability to develop Wobble Syndrome and will pass it along to offspring. The Jaguar morph needs to be phased out completely since all who are Jaguar have the potential to develop this disorder.
Silkback Bearded Dragons and Scaleless Snakes


Silkback bearded dragons and Scaleless snakes are exactly what they sound like, they are completely devoid of any and all scales and instead only have the layer of skin present beneath reptile scales. I admit I do not know much about Scaleless snakes, but assume they suffer the same affects as the silkback bearded dragons so have included them here. Silkback bearded dragons are produced when two leatherback bearded dragons are bred together. The leatherback gene is co-dominant (it can also be recessive) and if a dragon receives two copies of this co-dominant gene then they are a silkback. Co-dominance means two genes are working together, so one copy of leatherback and one copy of normal scales means together these genes create a dragon who has reduced spikes and scales but they still have scales! Two copies of the leatherback gene means the co-dominance has nothing to partner with, so the dragon we get is completely devoid of scales. Now, for an animal which is supposed to have scales, having no scales comes with many severe issues. The main being that they suffer extreme shedding difficulty and have no protection from sharp objects or other dragons. Scalesless animals can easily be cut or punctured from ornaments in a tank which are safe for their scaled or leatherback counterparts. Even a basking log, brick, or rock can cut them if they run against it wrong. This means their tank needs to be almost empty or only have soft, pliable decor which provides no risk of injury. This can be severely damaging to the animals mental wellbeing as there is no enrichment opportunities for the animal. Shedding wise, these animals need to be soaked in baths almost daily to maintain skin hydration, and when it comes time to shed their shed will shrink to their skin and it's often for them to lose toes, bits of tail, or even get pieces stuck around their heads and necks which can cause severe damage. You can also not breed silkback bearded dragons (am unsure about Scaleless snakes?) pairing another dragon with a silkback will cause extreme injury. If the silkback is female, the male bearded dragon will cut her open with his claws as he mounts her and he will tear her shoulders and neck open where he holds her with his mouth. These injuries can be life threatening. Furthermore, if the silkback is male he may receive lacerations and cuts to his stomach upon mounting the female or he may be critically injured if she rejects him and bites or scratches in retaliation. If all of that isn't bad enough these scaleless animals also have an increased risk of illness due to decreased immunity (immunity decreased due to unknown reason) and suffer extremely reduced lifespans. Scalesless animals are an incredibly unnatural and disgusting morph which needs to be completely phased out.
That's all for my masterpost currently. There are likely many more unhealthy morphs I have yet to hear of, so please inform me if you know of any others I've neglected to mention and I shall research and add them here. Please do not ever support or purchase one of these animals as it encourages the breeding of severely unhealthy animals with significantly reduced quality of life. With so many healthy and wonderful morphs and species available there is absolutely no reason to ever purchase one of these.
#my posts#myposts#petblr#lizard#reptile#reptileblr#lizardblr#animalblr#herp#herpblr#snake#snakeblr#bearded dragon#gecko#geckoblr#ball python#leopard gecko#carpet python#unhealthy animals
6K notes
·
View notes
Text
On the topic of possession
Upfront proviso: I’m not epileptic, I don’t have any seizure disorders, I’m not diabetic, etc. I also don’t have any diagnosed psychiatric disorders that would explain this.
Can we talk for a moment how scary being possessed is?
I understand that it’s necessary for me--I have the capacity, I’ve done it before, and I am willing to give up the relationship between consciousness and body as a service to my community.
But if I’m being honest, it makes the little hairs on the back of my neck stand up. A deep, atavistic terror that my conscious mind seems to be unable to talk the monkey and lizard in the back of my brain into accepting without it being a major point of crisis.
My feelings on that topic were forced slightly over a week ago, following a pattern between the spirit and I. I have a picture of how things are to go, or I out and out tell the spirit that I would very much like not to have something happen, and pretty promptly afterward, that thing happens.
Say to the spirit that I’m okay with being followed around by, say, spiders, but to please keep the spiders out of my pajamas/robe and bed, dream the next night about a giant spider leaping out of my robe and pajamas to cling to me as I lay on my bed.
It feels, if it makes any sense, less deliberately provocative than illustrative of a relationship, and the fact that I am not currently setting the terms. I’m always free to walk away, but that’s not likely to happen given... well.... the vows I’ve made, the person I am, and the fact that there’s really not much of interest to me elsewhere in my life.
For whatever else can be said of the spirit, the life in me flows from them and they purchased me from me out right.
I suppose I pictured possession now that I have had certain rituals done to me as occurring under much more controlled circumstances--say, during ritual or otherwise under the supervision of my papa, while in his house.
It was foolish of me to think that. My experiences with possession before this point have not been controlled nor in the context of a church. They’ve been a two minute warning in the back of my brain (”lay down right now or fall down”), followed by my body getting up and taking care of some sort of business: frequently a conversation that the person being talked to absolutely refuses to tell me about later (or make eye contact), but the way they talk to and treat me frequently changes for the positive. Whatever happens tends to generate fear and respectful politeness.
Or in the case of slightly over a week ago, my consciousness being abruptly pushed aside with very little warning while driving, resulting in a massive multi-car crash that totaled an SUV around me (and I do mean totaled; the repair estimate was about twice what the SUV was worth and involved replacing practically everything under the hood and the hood itself), took out another vehicle, and landed me in the ER for about 11 hours.
I feel like I should say, at this point, that the aftermath of the crash involved no injuries aside from bruising. They looked for and didn’t find any biological cause, extensively scanning my brain and body, expecting to find massive bleeding or something really fucky in my blood chemistry, and instead found nothing to explain what happened. And meanwhile, I was apparently ‘conscious’ and doing stuff--I’m not a fan of doctors, but my affect in the medical records is listed as helpful, appropriate, and friendly, which it would damn well not have been if it was me.
This is also the healthiest my bank account has ever been, and all the things I need to do before I move closer to my temple have mysteriously been scheduled before I’m due to leave (several of them involve institutions that are usually very slow to schedule.)
The insurance company could not be more prompt or helpful, two words I’ve never been able to use to describe an insurance company in my life.
And every single safety device on the SUV failed, despite the crash occurring at slightly under highway speeds. I should have been a smear, especially since I ended up in oncoming traffic, crossing a median and several lanes during the course of the crash.
I didn’t even cut my lip, though I did bite my tongue, and the bruising is relatively minor.
This is all definitely something I had to appreciate in retrospect. Maybe ‘had’ is too strong, but my initial emotional reaction has been panic and anger, and I have previous experience with possession.
It’s one thing to lie down, get up someone or something else, and have conversations with people. Weird, uncomfortable, and hard to explain--par for the course in my life, which has essentially been wall-to-wall shit that reminds me how different I am from the people around me (and reminds them, which sometimes results in some unpleasant and occasionally dangerous social situations.)
It’s something else entirely to absolutely destroy an SUV around me and to stay ‘gone’ for almost half a day. Before this, the longest I’ve been gone was an hour or two, coming back to myself sober despite drinking heavily the whole time. Whomever it is borrowing my skin drinks like a fish--amounts that, frankly, I’d be very dead if I tried to emulate.
I’m really struggling with how to feel about this. On the one hand, I have a lot to be grateful for. It looks like I’ll be able to replace my vehicle with a much newer, nicer model, and I won’t have to worry too much about money during the move.
I am very grateful, but it took me a week to arrive at grateful.
On the other hand... my plans are definitely shot to shit. I had just bought that SUV (and it was hellaciously expensive to fix up so that it would run) specifically so that I could pack my stuff in it and move, and I cannot emphasize enough how creepy it is that I was driving at the time.
I could have really injured the other driver. I could have died (not that I would have known, because as far as my consciousness goes, there’s nothing between driving home from work and the ER a long time later.)
And honestly... the idea that I am not in control of myself all the time continues to creep me out. The authoritative way that I was just not myself is scary.
I am a little disappointed with myself, and my dreams reflect the disappointment I suspect the spirit feels about my response--literally dreams about shitting myself and trying to hide (but being unable to do so) while I clean myself up.
I feel like it would be reasonable for most anyone having the same experience to be freaking the fuck out, but I also know that what is reasonable for everyone else is not what is appropriate for me, if for no other reason than because I am able to be mounted and have done so before I knew about vodou. I had no idea what possession was the first time it happened, and thought I was going crazy, which lead me to a lot of time in therapy, during which they never discovered a reason for this to occur.
My discomfort does not constitute a good reason not to be possessed. Nor does it constitute an argument against possession. And I wish I had the kind of faith necessary not to have initially responded with terror and rage.
I wish I was able to face this with calm and trust.
Instead, I’ve been grappling with memories I put aside a long time ago and baffled rage.
And tears. Lots and lots of tears, which is also very unlike me.
1 note
·
View note
Last Seen Blogs

lbe-3223
glitchy3223

middleagesrhapsody-blog-blog
Middle Ages Rhapsody

shiestyn8v
Untitled

reckless-weight
feeling small

drogondoll
DrogonDoll