#it can only be a contraceptive if shes not ovulating
Note
Hiii Hope you’re well! Can I request reader who wants to fuck but they don’t have any condoms and hyunjin keeps refusing saying no especially since she’s ovulating and he might get her pregnant but she keeps insisting that she wants to know what it feels like to have him cum inside of her and eventually he gives in and lets her ride him. (Subby hyunjin preferably)
🏷️ cnc/dubcon. dom!fem!reader, sub!hyunjin, forced breeding & pregnancy risk. 18+ minors dni.

the box in the drawer is empty. it should have been full of contraceptives but you figured that either of you were too enthralled in the intimacy to be bothered. now, hyunjin’s face contorts into one of a quiet panic, but your hand is quick to soothe him with a soft palm to his cheek.
except, he isn’t really soothed at all, especially not at your suggestion.
“you can just pull out, you know.” your thumb runs across his mole. “there’s no need to worry about condoms.”
“but—” hyunjin gulps. “y-you’re ovulating, i…i can’t risk pulling out.”
“and? some people still become parents after using condoms and plan b.”
your hand trails down from the plump skin of his face down to the rough and stark edges of his neck, pulling him closer in a threat to cage him in. hyunjin is strong and he could easily pull away if he wanted to, but maybe just as he’s nervous, he also simply can’t tear away from you.
yet you feel like a trap that he fell into.
“i-i can’t…no, let’s not. we can try another time, i’ll just…take care of myself.” hyunjin finally tries to back away until your naked legs wrap around his.
he’s now down on your body, your skin and his pressing against each other. it makes a blush creep up to his face as, he can’t lie, he loves the close proximity despite your risky suggestions. he’ll always fall in love with you like cat to a catnip. there’s an irresistibility to you that he can’t wave for a moment, even when his mind is hazy with panicked and rushing thoughts that won’t stop running.
he isn’t ready to be dealt with the responsibility of your pregnancy; hyunjin is fully ready to trust you and take big steps with you, but the sudden and unplanned nature is causing him the worst thoughts of his life. pressure builds in his throat and he keeps saying no: he knows that you’re talking to him, insisting, but he could barely hear your sweet voice when there’s a deafening ring in his ears that he can’t defeat.
“please, please, no—ah!”
he doesn’t know how he got to the position at all. one moment, you caged him down to the bed with your body, and the next you were there. sitting on his cock, pussy filled deep with all of him.
skin to skin, inside and full — all for the first time without a condom in the way.
“god hyune, your bare cock’s so good…” you pant as your hips roll against his. a dragged whine leaves his throat as a delicious moan leaves yours. “i wanna feel your cum inside me, wanna feel it, just this once baby.”
“n-no,” he still insists. hyunjin’s chest heaves and he doesn’t know what to do, it feels so fucking good that it overrides his senses. he never knew that the thinnest condom still got in the way of feeling every single bit of you. the warmth, the velvety plush walls, the wet slick essence…it’s all much for him to take, and it leaves him breathless.
you move your body upwards only to crash back down. the thrust of your lower half sends hyunjin into a trance, making his head roll back, plump lips hung open as a string of curses leave his system in the form of a pretty curled voice. he keeps saying no, he keeps pleading for you to stop, the ringing in his ears fading in and out as the sloppy and messy noises of your cunt clashing against his sweaty cock fill the room alongside your moans. every weak attempt to pull away turns into nothing as your legs cage him in, your pussy slamming against his curved length in a beautiful pace that he can’t seem to break.
“don’t want to breed me, baby?” you threaten.
“no, stop.
you plant your hands on his sensitive sides. “don’t want to see me take you, hyunjin?”
“s-stop, stop…”
“don’t want to feel what it’s like to fill up a pretty little pussy?”
your words are filthy and you know it. they’re as dirty as they are enticing and it makes his mind spiral. hyunjin’s teary eyed now, a cry getting lodged in his throat. he feels like sobbing and yet, from both the dilemma and the pleasure, he whines out things he doesn’t mean.
“stop…s-stop—don’t…don’t stop! don’t stop, fuck, y/n, d-don’t stop…!”
or maybe that’s what he wanted all along.
you laugh and your pace picks up. you’re riding him with all your might and hyunjin feels like a slut. he was made to breed you like this, fill you up as he should. maybe you’re right, he wasn’t born with an insane amount of cum for it to be wasted.
he shoots load after load inside you, his hands pulling you down on his cock by your thighs, mustering up all the strength to empty his loads in you.
it takes you minutes before you pull out. for a while, you have to kiss him to calm him down, reassure him that he did well. the moment your cunt is off his cock, it gushes out his creamy release, and the sight makes him shiver.
he really wanted to fill you up, cum deep inside.
it’s a primal instinct that he can’t shake.
#sub!skz#sub!hyunjin#skz smut#hyunjin smut#💌 ipeginbox#<3 a lovely anon#💬 z is writimg#WHEWWWW this one was a doozy
331 notes
·
View notes
Text
Kind of a cheese strat, but if you're a Catholic you only sin once in getting a vasectomy/tubal ligation I think. Then you confess your sins, do the penance, etc. You don't have to sin continuously by wearing condoms / taking birth control pills / etc.
Catholicism doesn't require reversing that stuff once it's already done, so from then on you can be like "IDK what to say Father. I creampie my wife when she's ovulating every month, but she never gets pregnant. That sinful vasectomy I got a decade ago is just the only thing keeping my intercourse from fulfilling both its unitive and procreative telos! ¯\_(ツ)_/¯"
(This might also work with IUDs, but as I was searching, it seems like there's a problem with Catholic hospitals refusing to remove IUDs. Like, "we don't have anything to do with contraception here, including taking it out." Seems sort of counterproductive.)
#religion#christianity#catholicism#contraception#i am not a catholic and have thoroughly fact checked any of this and am not being entirely serious
16 notes
·
View notes
Text
I'm on OB rotation again. I asked the attending what are things the PCP should know about prenatal and postpartum pts. Stuff we discussed:
SSRIs can be continued during pregnancy. I often see patients on Zoloft during pregnancy if they need an antidepressant. In fact, I just started a prenatal patient on Zoloft the other day in clinic. It is safe to continue SSRIs during pregnancy because you should treat the patient's depression. Babies can come out sort of jittery because of the SSRI, but that goes away.
Postpartum patients will have bleeding somewhat similar to a menstrual period right after giving birth. It starts to decrease and becomes like a brownish color and can last up to 6 weeks postpartum. Any bleeding beyond that point is abnormal.
There is some evidence that if you have estrogen-containing birth control, it can decrease milk supply. Actually, I had a patient in clinic recently who was seen by an attending and he started her on a progesterone only birth control so that it would not affect her milk supply. Estrogen decreases the patient's milk supply, so patients who plan to breast-feed should not be started on estrogen-containing birth control. Right after giving birth, your body has increased amounts of estrogen, so you would not start estrogen containing birth control until at least 6 weeks postpartum anyway. Increasing estrogen immediately postpartum increases risk of blood clots. For patients who plan to breastfeed and want to be on an oral contraceptive, use progesterone only oral contraceptives until she stops breastfeeding.
If the mother is breastfeeding at least every 4 hours, then this can be used for contraception. It's about 80% effective. Once baby starts sleeping through the night or once baby starts feeding more than every 4 hours, this method won't work! If you go more than 4 hours without breastfeeding, breastfeeding will not protect you from pregnancy! You can also ovulate before your menstrual period returns, so you can't say you can't get pregnant because your period has not returned yet!
I asked the attending I worked with today about how she goes about prescribing birth control. She said she will usually start with Sprintec. It's usually covered by insurance and if it's not covered, it's pretty affordable. She also said Junel is pretty well tolerated. Certain progestins in certain brands of birth control may work better for certain things like acne control, but she didn't have as much knowledge on that. I'll ask another attending again about that. I usually start people on Sprintec as well.
PCP should know that alkaline phosphatase is high in pregnant patients. It comes from the placenta. So don't be freaked out by that.
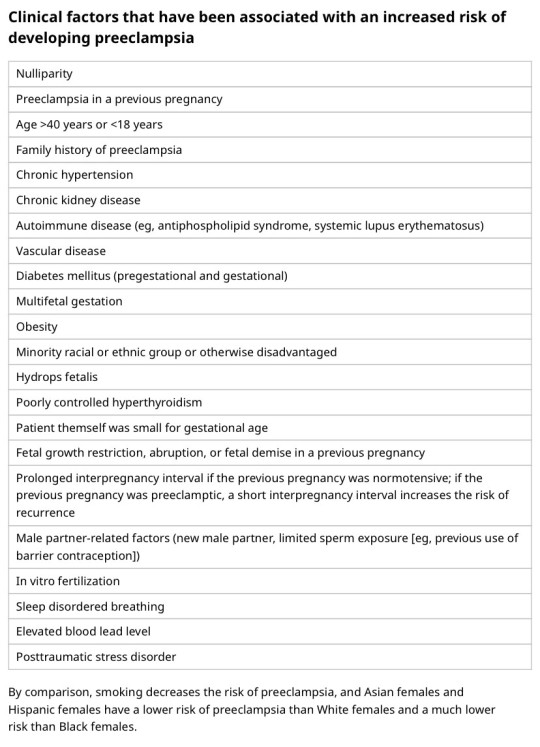
You should know HTN in pregnancy and preeclampsia workup. High BP is 140/90. Severely high BP is 160/110. Swelling occurs in many pregnant pts, but that should also alert you to start preeclampsia workup.
[Preeclampsia w/u from UpToDate:
Diagnostic evaluation
•Laboratory – Patients with suspected preeclampsia should have a complete blood count with platelets, creatinine level, liver chemistries, and determination of urinary protein excretion.
•Fetal status – Fetal status is assessed concurrently or postdiagnosis, depending on the degree of concern during maternal evaluation. At a minimum, a nonstress test or biophysical profile is performed if appropriate for gestational age. Ultrasound is used to evaluate amniotic fluid volume and estimate fetal weight, given the increased risk for oligohydramnios and growth restriction.
•Consultation with the neurology service is generally indicated in patients with neurologic deficits/abnormal neurologic examination, which may include ocular symptoms or a severe persistent headache that does not respond to initial routine management of preeclampsia.]
An important thing to review is physiology of pregnancy. Blood volume increases during pregnancy, so there are lots of new RBCs and that will throw off a HgbA1c reading, therefore HgbA1c is not measured during pregnancy and will not be accurate! My attending today told me there was a midwife who offered pts either HgbA1c or oral glucose tolerance tests to screen for gestational DM. The HgbA1c is not accurate in pregnancy, so this should not be done. That would be bad to miss a diagnosis of gestational diabetes. You have to wait until 3 months postpartum to measure HgbA1c to get an accurate reading. Had a pt who did not have a PCP prior to getting pregnant, was on insulin during the pregnancy, and after giving birth, still needs to establish with PCP for diabetes f/u. After you give birth, you insulin needs drastically change, so you don't need as much as you did when you were pregnant. So I stopped her insulin and advised that she f/u with her new PCP for diabetes care.
I still need to review fetal heart tracings. The attending today said the first thing to look at is the baseline (the baseline HR should be about 160 beats/min), then the variability, then look for accelerations and decelerations. If more than 32 weeks GA, accelerations are 15 beats/min above the baseline lasting at least 15 seconds. Early decelerations are representative of compression of the fetal head, which is normal during labor as baby moves down the pelvis/birth canal. Variable decelerations look sharper like a "V" and can represent compression of the umbilical cord. Late decelerations represent placental insufficiency.
ACOG has very helpful practice bulletins.
I can't take screen shots on my work laptop, so I'm just going to summarize gestational HTN w/u from UpToDate:
Gestational HTN: New onset of systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg on at least 2 occasions 4 hours apart after 20 weeks of gestation in a previously normotensive individual
And:
No proteinuria
No signs/symptoms of preeclampsia-related end-organ dysfunction (eg, thrombocytopenia, renal insufficiency, elevated liver transaminases, pulmonary edema, cerebral or visual symptoms)
Preeclampsia: New onset of systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg on at least 2 occasions at least 4 hours apart after 20 weeks of gestation in a previously normotensive individual. Patients with systolic blood pressure ≥160 mmHg and/or diastolic blood pressure ≥110 mmHg should have blood pressure confirmed within a short interval (minutes) to facilitate timely administration of antihypertensive therapy.
And:
Proteinuria (≥300 mg per 24-hour urine collection [or this amount extrapolated from a timed collection], or protein:creatinine ratio ≥0.3, or urine dipstick reading ≥2+ [if other quantitative methods are not available]).
In a patient with new-onset hypertension without proteinuria, the diagnosis of preeclampsia can still be made if any features of severe disease are present.
Preeclampsia with severe features: In a patient with preeclampsia, presence of any of the following findings are features of severe disease:
Systolic blood pressure ≥160 mmHg and/or diastolic blood pressure ≥110 mmHg on 2 occasions at least 4 hours apart (unless antihypertensive therapy is initiated before this time)
Thrombocytopenia (platelet count <100,000/microL)
Impaired liver function as indicated by liver transaminase levels at least twice the normal concentration or severe persistent right upper quadrant or epigastric pain unresponsive to medication and not accounted for by alternative diagnoses, or both
Progressive renal insufficiency (serum creatinine concentration >1.1 mg/dL [97 micromol/L] or doubling of the serum creatinine concentration in the absence of other renal disease)
Pulmonary edema
Persistent cerebral or visual disturbances
Eclampsia: A generalized seizure in a pt with preeclampsia that cannot be attributed to other causes.
HELLP syndrome: hemolysis, elevated liver enzymes, low platelets. Hypertension may be present (HELLP in such cases is often considered a variant of preeclampsia).
Chronic (pre-existing) hypertension: hypertension diagnosed or present before pregnancy or on at least 2 occasions before 20 weeks of gestation. Hypertension that is first diagnosed during pregnancy and persists for at least 12 weeks postpartum is also consider chronic hypertension.
Blood pressure criteria during pregnancy are:
Systolic ≥140 mmHg and/or diastolic ≥90 mmHg
Prepregnancy and 12 weeks postpartum blood pressure criteria are:
Stage 1 – Systolic 130 to 139 mmHg or diastolic 80 to 89 mmHg
Stage 2 – Systolic ≥140 mmHg or diastolic ≥90 mmHg
Chronic HTN with superimposed preeclampsia*:
Any of these findings in a patient with chronic hypertension:
A sudden increase in blood pressure that was previously well-controlled or an escalation of antihypertensive therapy to control blood pressure
New onset of proteinuria or a sudden increase in proteinuria in a patient with known proteinuria before or early in pregnancy
Significant new end-organ dysfunction consistent with preeclampsia after 20 weeks of gestation or postpartum
*Precise diagnosis is often challenging. High clinical suspicion is warranted given the increase in maternal and fetal-neonatal risks associated with superimposed preeclampsia.
Chronic hypertension with superimposed preeclampsia with severe features:
Any of these findings in a patient with chronic hypertension and superimposed preeclampsia:
Systolic blood pressure ≥160 mmHg and/or diastolic blood pressure ≥110 mmHg despite escalation of antihypertensive therapy
Thrombocytopenia (platelet count <100,000/microL)
Impaired liver function as indicated by liver transaminase levels at least twice the normal concentration or severe persistent right upper quadrant or epigastric pain unresponsive to medication and not accounted for by alternative diagnoses, or both
New-onset or worsening renal insufficiency
Pulmonary edema
Persistent cerebral or visual disturbances
A reduction in blood pressure early in pregnancy is a normal physiologic occurrence. For this reason, women with chronic hypertension may be normotensive at their first few prenatal visits. Later in pregnancy, when their blood pressure returns to its prepregnancy baseline, they may appear to be developing preeclampsia or gestational hypertension if there are no documented prepregnancy blood pressure measurements.
BP: blood pressure.
* Blood pressure should be elevated on at least two occasions at least four hours apart. However, if systolic pressure is ≥160 mmHg or diastolic pressure is ≥110 mmHg, confirmation after a short interval, even within a few minutes, is acceptable to facilitate timely initiation of antihypertensive therapy.
¶ The onset of preeclampsia and gestational hypertension is almost always after 20 weeks of gestation. Preeclampsia before 20 weeks of gestation may be associated with a complete or partial molar pregnancy or fetal hydrops. Postpartum preeclampsia usually presents within two days of delivery. The term "delayed postpartum preeclampsia" is used for signs and symptoms of the disease leading to readmission more than two days but less than six weeks after delivery.
Δ Significant proteinuria is defined as ≥0.3 g in a 24-hour urine specimen or protein/creatinine ratio ≥0.3 (mg/mg) (34 mg/mmol) in a random urine specimen or dipstick ≥1+ if a quantitative measurement is unavailable.
◊ Almost all women with the new onset of hypertension and proteinuria at this gestational age or postpartum have preeclampsia, but a rare patient may have occult renal disease exacerbated by the physiologic changes of pregnancy. An active urine sediment (red and white cells and/or cellular casts) is consistent with a proliferative glomerular disorder but not a feature of preeclampsia. Women with chronic hypertension who had proteinuria prior to or in early pregnancy may develop superimposed preeclampsia. This can be difficult to diagnose definitively, but should be suspected when blood pressure increases significantly (especially acutely) in the last half of pregnancy/postpartum or signs/symptoms associated with the severe end of the disease spectrum develop.
§ Photopsia (flashes of light), scotomata (dark areas or gaps in the visual field), blurred vision, or temporary blindness (rare); severe headache (ie, incapacitating, "the worst headache I've ever had") or headache that persists and progresses despite analgesic therapy; altered mental status. Seizure occurrence upgrades the diagnosis to eclampsia.¥ The differential diagnosis of preeclampsia with severe features includes but is not limited to:
Antiphospholipid syndrome
Acute fatty liver of pregnancy
Thrombotic thrombocytopenic purpura (TTP)
Hemolytic uremic syndrome (HUS)
The laboratory findings in these disorders overlap with those in preeclampsia with severe features. (Refer to table in the UpToDate topic on the clinical manifestations and diagnosis of preeclampsia.) The prepregnancy history, magnitude and spectrum of laboratory abnormalities, and additional presence of signs and symptoms not typically associated with preeclampsia help in making the correct diagnosis, which is not always possible during pregnancy.
In addition, a variety of medical disorders may be associated with hypertension and one or more of the signs and symptoms that occur in women with preeclampsia with severe features. These patients can usually be distinguished from patients with preeclampsia by taking a detailed history, performing a thorough physical examination, and obtaining relevant laboratory studies.‡ In contrast to preeclampsia, gestational hypertension is not associated with end-organ involvement, so neither proteinuria nor the symptoms or laboratory findings of preeclampsia are present.
#OB#OBGYN#birth control#gestational HTN#preeclampsia#eclampsia#breastfeeding#gestational diabetes#fetal heart tracing#FHT
2 notes
·
View notes
Text

Birth Control 101: Choosing The Best Contraceptive Method For You
There's short-acting, long-acting, and barriers of protection. Which one suits you?
Shonda White
Sep. 23, 2020 08:00AM EST
I remember the day of my wedding…when I started feeling my contraception ring coming out of my vagina. I had only recently started using the ring even though I was more used to taking the pill. There I was in the bathroom stall with one of my bridesmaids, and she was literally helping to guide my ring back up into my vagina because I could feel it slipping out of me. Although quite embarrassing, let's just say that we're forever bonded by that experience. So, have you ever tried a new birth control method that wasn't the best for you but it seemed to work well for others?
During a recent interview with Board Certified Obstetrician & Gynecologist, Dr. Chimsom Oleka, she provided a list of all of the birth control methods currently available, which can potentially serve as a starting point for those of you who may be exploring new contraceptive methods.* As you continue reading, you'll notice that the list is organized based on what Dr. Oleka refers to as Short-acting (hormonal and non-hormonal), to Long-acting, to Barriers of Protection.
Before we dive into the list, let's first clarify specifically what birth control does. As. Dr. Oleka explained, for most methods, birth control releases certain hormones in your body which contributes to the ultimate end goal: block ovulation or keep an egg from being released, thicken the mucus in the cervix so that sperm can't pass through, and/or thin the lining of the uterus, which decreases chances of implantation. Each birth control method is designed to do each or all of these things, but depending on the method, they will either do them better, worse, or not at all.
Choosing The Best Birth Control Method For You
SHORT-ACTING BIRTH CONTROL METHODS

Shutterstock
Note: Throughout this section, you will notice references related to "continuous" or "extended" usage. As Dr. Olekaexplained, many of us have a false idea of what the period is supposed to do. Contrary to popular belief in terms of what our menstrual cycle does and why it's "necessary" every month, ultimately its main purpose is for pregnancy. That's it.
As Dr. Oleka expertly pointed out, "It's the birth control's period, not your period. Your birth control will start stimulating the lining and doing all of the things that cause you to bleed." So, as long as you have a hormone that's assisting with protecting and keeping your uterus lining thin, and as long as you've consulted your physician beforehand, then you don't have to necessarily worry about shedding the lining every month (i.e. having a period).
Consider, for example, women who have bleeding disorders (i.e. their bodies bleed too much or won't stop bleeding), female athletes, as well as those who may suffer with things such as menstrual migraines…situations like these support the case for continuous or extended methods.
Method: Birth Control Pill (Hormonal - Estrogen and Progesterone)

Shutterstock
How It's Administered: Self-ingested orally, daily
Efficacy: 7 to 9% failure rate (i.e., approximately 1 in 10 will get pregnant)
Description & Overview:
Birth control pills usually come in 28-day pill packs (four rows of seven pills) including a week of placebo, non-active pills. There are different variations as well, but it's critical that you take it every day at the same time.
The most commonly used pill has both estrogen and progesterone. With estrogen, it tends to help provide more stability of the lining. However, some people may not want estrogen or they may have an underlying medical issue that conflicts with the estrogen. There is a risk of blood clots, although fairly low, but the risk of this goes up when you're pregnant. With the pill, it helps regulate the bleeding, which in turn, helps make it predictable. It's known to have protective benefits such as helping to decrease risk of certain cancers and it can help reduce symptoms related to fibroids.
Also, you can use this method, as well as other methods, continuously or in an extended way so that you can delay or skip the bleeding (i.e. going on vacation). For example, if you wanted to try an extended use, then you could delay the withdrawal bleeding (period) for a set number of weeks or months by skipping the last row for let's say two months. Then, you would take the last row of inactive pills the third month, so that you would only bleed approximately every 10 weeks.
On the other hand, if you're someone who decides "I don't want to bleed at all," then you could skip the last row of inactive pills and move forward with starting the new pack each month. Keep in mind, if you don't bleed or you bleed too heavily already, there may be other medical issues going on, so as always, you'll want to consult your physician about this.
Side effects can vary, but some of the most common side effects include: nausea, breast tenderness, and initial irregular bleeding.
Method: Birth Control Pill (Hormonal - Progesterone Only)
How It's Administered: Self-ingested orally, daily
Efficacy: 7 to 9% failure rate
Description & Overview:
This method basically works pretty much the same as the first pill mentioned above, but it doesn't include estrogen. It only includes progesterone.
Progesterone-only pills can be harder for some women to use because you have to be really consistent. If the daily pill ingestion time is missed by as little as three hours, then it loses its efficacy. Hence, it's critical that you take the pill every day at the same time.
With the progesterone-only pill, there's also a greater chance of irregular bleeding. Hence, this method is usually recommended by the physician if there are estrogen-related conflicting medical issues.
Method: Vaginal Ring (Hormonal – Estrogen and Progesterone)

Michael Kraus/Shutterstock
How It's Administered: Self-inserted through Vagina
Efficacy: 7 to 9% failure rate
Description & Overview:
The vaginal ring is a soft, flexible ring approximately two inches wide and four centimeters thick that is self-inserted and removed in/out of the vagina. Some women will tie a string to the ring and there's also an applicator that can be used to assist with insertion and removal.
The vaginal ring stays in for three weeks and releases hormones every day. Once removed for seven days, it allows withdrawal bleeding (period) to occur. Then, a new ring is inserted every four weeks. This method can be used continuously if you bypass the seven days and move forward with inserting the new ring every three or four weeks, or in an extended way if you bypass the seven days every few months or so.
The ring has been known to cause breakthrough or irregular bleeding. Not to mention, there are times when the ring can slip out during sex, which of course can directly impact the efficacy.
Method: Copper IUD (Non-hormonal)
How It's Administered: Inserted vaginally by physician (through opening of cervix, into the uterus)
Efficacy: Less than 1% failure rate
Description & Overview:
Similar to the IUD previously mentioned, the copper IUDis a latex-free, t-shaped, plastic piece but it also includes areas of exposed copper. By releasing copper salts into your body, the copper tricks the uterus into thinking something foreign is inside, creating an appearance of a "chaotic" environment in your system, which ultimately blocks sperm and prevents reproduction. It can last for 10 years, but it has been known to be effective for up to 12 years.
The copper IUD is ideal for someone who doesn't want to deal with hormones, or someone who is certain they don't want children for a long time. There are instances where it can be used as emergency contraception but it won't work if something has already been implanted.
Because this method doesn't affect ovulation, this method is also ideal for women who want to continue bleeding or women within certain cultures where the idea of contraception isn't readily accepted. This can serve as contraception method without anyone else truly knowing that you're taking it because you will still have a period as normal.
The most common side effects usually include more painful cramping or heavier bleeding.
Method: Contraceptive Implant (Hormonal – Progesterone Only)

Michael Kraus/Shutterstock
How It's Administered: Implanted in arm by physician
Efficacy: Less than 1% failure rate (the most effective method)
Description & Overview:
The contraceptive implant is a flexible, plastic rod that's placed inside the upper arm. It's small and thick - approximately 4 cm long and 2 mm thick. It releases hormones daily, and lasts for three years, although recent data shows it may last longer than that. After three years, you get a new one if you choose to do so. Otherwise, you will return back to your baseline fertility.
Some of the most common side effects can include irregular bleeding, no bleeding (approximately 6%), or heavier bleeding. For those who experience irregular bleeding, there are ways to decrease it and make it more manageable. Also, there are rare occasions where, if placed improperly, it can shift or migrate.
BARRIERS OF PROTECTION** BIRTH CONTROL METHODS
The most common effects for any of the following methods can include vaginal discharge and irritation. After the use of these, the return to fertility is usually fairly quick.
As it relates to a lot of these barriers of protection, Dr. Oleka likes to think of it this way, "Condoms should be used more so for STD and HIV/AIDS protection, and less for pregnancy prevention." Nevertheless, they are still considered methods for both pregnancy and STD/HIV prevention.
Method: Male Condom (Non-hormonal)

Michael Kraus/Shutterstock
How It's Administered: Applied by male on his penis
Efficacy: 15% failure rate (research across the board states this although it seems quite questionable by both the expert and the writer)
When to Apply: Right before sex
Description & Overview:
Condoms are usually latex or you can opt for lambskin if you're allergic to latex. However, anything non-latex has been known to be less effective in preventing pregnancy as well as STDs. With condoms, common things like inconsistent use, slippage during sex, and the risk of it tearing are a few factors that can directly impact the overall efficacy.
Join our xoTribe, an exclusive community dedicated to YOU and your stories and all things xoNecole. Be a part of a growing community of women from all over the world who come together to uplift, inspire, and inform each other on all things related to the glow up. We drop xoNecole events and special opportunities into our Tribe first.
Featured image by Shutterstock
The Difference Between Your Period And Ovulation - xoNecole: Women's Interest, Love, Wellness, Beauty ›
Birth Control - Mayo Clinic Health System ›
Which Birth Control Method Is for You? 19 Types, Pros, Cons, More ›
Find Your Birth Control Method 2020 | Power to Decide ›
Choose the Right Birth Control - MyHealthfinder | health.gov ›
5 types of birth control options: which is best for you ... ›
Birth control options: Things to consider - Mayo Clinic ›
Best Birth Control For Me Quiz | Choosing the Right Contraceptive ›
Sent from my iPhone
33 notes
·
View notes
Note
You knew you'd get this question lmao but how did Thor and Jane contracept? (ESPECIALLY bc Thor only needs to look at some woman and she's pregnant lmao)
@shieldretired
What we know in canon: Thor's fertility powers are linked to the rain, to the fertility of the earth itself. He makes flowers grow, carves rivers, blesses the crops with rain and makes the soiled ground fertile.


There are new cubs/kittens/eggs/babies anywhere he goes.
When he's sad or worried, spring isn't that great, but when he's truly in love, farture and abundance bless the earth, the rivers, the animals and everything/everyone thrives, even the neighborhooding villages.
He can get a goddess of death pregnant.
Now this is my headcanon: due to these fertility powers, he’ll choose when to use them, exactly like he does with his lightning.
He won’t get his partner pregnant accidentally, only if it’s a mutual agreement.
Thor's been to earth many many times in his life, usually to have fun. If he hadn’t avoided accidental pregnancies, there would be many thunderers around since all of his canon kids inherited his powers.
TLDR: Thor has fertility powers and they concede him the ability to create life when he sees fit. For example: Vision.
Thor can also sense when a person who ovulates is ovulating, they have a specific, sweet smell to them.
7 notes
·
View notes
Note
Hi! Sorry this is personal, please don't feel any pressure to answer at all if you don't want to. Do you have any experience or advice when it comes to contraception? I've always just used condoms but I'm starting to look at other options and I've got an appointment with a nurse next week to discuss. I wanted to prepare myself before so that I had an idea of what I wanted. Googling just gives bad side effects for every option so I was looking for more of a real life experience. Please ignore this if it makes you uncomfortable in any way xx
Hiya love, don’t apologise I don’t mind talking about this stuff, I can only give you my own personal experiences though so anyone else please jump in to offer theirs.
So I’ve only tried the combined pill for contraception myself, went on it when I was 15 and was on it until fairly recently. I had no problems with it, I know there’s a long list of side effects but if you look at most medication there is as they have to warn you, but I guess everyone is different. For me there were more benefits, my periods were lighter and less painful, it cleared my skin up a bit. It’s just remembering to take it at the same time each day really. The best bit was having the option to take it without the usual 7 day break occasionally and skipping a period which was really good for holidays and stuff.
I don’t have experience of the implant but my sister had it before she wanted to get pregnant and she had no problem with it. My friend has the injection she loves it as she gets no periods at all but I think personally that would freak me out! One of my friends had bad headaches and mood swings on her pill but she switched to another and that was better for her so I think it’s just trying a method and seeing if it’s right for you.
Anyway we’re back on condoms again now and it does my head in a bit it’s so much nicer not to have to faff around ha ha, I just wanted to give my body a break and I feel so kind of in tune with it now but I am ruled totally by my hormones lol (god help my bf when I’m ovulating) it’s also nice to have my sex drive back, I’m not sure if the pill was responsible for robbing me of that before.
Good luck with your appointment xxx
2 notes
·
View notes
Text
A theory on ovulation inspired by Rebecca in the Bible
So there's this frog that ovulates when pregnant women pee on it, and this is half of the premise. The other half is the verse that Handsmaid tale is based on...
Now there are many places in the Bible that showcase older women having children. Barren women having children. And God basically preventing women from having children *until* the very last second.
The question here is *how?*
Some scholars suggest that it's because women were married to older men as children. Because of course; women were object of which to birth nations. And not *really people* despite the beginning of Genesis suggesting otherwise.
Rebecca did not marry Jacob for 14 years. So even if she were 14 before that point; she was not married until she was 28. Even then the Bible describes her as "shapely" which, most 14 year olds are not!
And even then; her elder sister Leah had several children while Rebecca remained barren.
So much so that she had committed her handmaiden Billah to have children in her stead.
Several more children were born to Leah and Billah before God allowed Rebecca to even become pregnant with Joseph.
What I'm saying is; Rebecca was likely menopausal age before she conceived her first son, and then she had a second.
You might be saying that "Well these stories are fiction" or "They're allegorical".
But what if they're not. And I'm not saying the story is entirely literal, but what if it's even remotely based on actual happenstance if not completely true?
Another story features Abraham and Serah who had their first child *in their 90s* holy f*.
And while she might be up for debate here, the Bible says the oldest humans lived for 200 years sometimes. Years could have gotten longer or shorter, or lifespans shorter because humans aren't very good at taking care of themselves to live long lives.
So the question we're left with is the how and the why of the matter.
As we know; At about 40 a woman typically goes through manopause. This is the biological process where a woman stops producing estrogen and goes through male puberty due to increased testosterone production.
That's only partially a joke. But mostly scientifically accurate.
They don't "run out of eggs" as some dumsdums suggest; they just stop ovulating. This is exactly what happens to trans men when they go through hormone replacement therapy. They don't become infertile... Their eggs just go into stasis. And then they can donate them to women who actually want them.
So what does this have to do with Frogs?
Well; pregnant women pee has a lot of hormones related to pregnancy in it. So the reason those frogs ovulate is *because* of the jacked up amount of hormones.
To say this with different more unsavory and discriminatory phrasing; Trans Women used to use pregnant mare pee as a source of estrogen in order to transition.
So let's put all that together; There's a possibility in scientific advancement that we have not studied yet because we assume it's "impossible" or at the very least "improbable" that a cis woman can get pregnant after menopause with hormone therapy and just... Regular sexual activity instead of invitro-fertilization.
Not only that; because hormonal imbalances can cause a woman not to ovulate; high estrogen being a form of contraception, and testosterone in the case of trans men; there's a possibility of even keeping a woman's eggs dormant *inside her gametes* through hormone therapy.
Where does this part come from? Well; if Rebekah had high estrogen all her life, and didn't see a reduction in estrogen *until* menopause; then that would be when her natural ovulation cycle actually started.
In what we consider to be old age.
So uhm. Anyway; I'm not a doctor, or a woman's health specialist. I'm just a random scholar who reads stuff and puzzles things together in her free time.
But like; It'd make a really good PhD thesis if true, right?
1 note
·
View note
Text

Reproduction | Comic Week 8 - created on Corel Painter.
Lately, Nolo’s been thinking about her body and all of its many changes. Puberty is meant to be the process by which a child’s body becomes an adult body, but what does that mean really? What does it mean to have an adult body?
This question can easily be answered by a natural phenomenon without which the human race could not exist – reproduction! Reproduction is a process by which the male-produced sperm and the female-produced egg unite during sexual intercourse and ultimately form a baby.
The female reproductive system is made of many parts. Two organs called the ovaries release an egg once every month to be fertilised in a process called ovulation. This egg sits comfortably in the uterus, cushioned by a thick uterine lining made of tissue and blood. When the egg goes unfertilised, hormones tell the body to dispel this thick uterine lining in preparation for a new cycle of ovulation. This particular process is called menstruation. Menstrual blood leaves the vagina and the cycle starts anew.
The male reproductive system is also made of many parts. Sperm cells, the little swimmers integral to the process of fertilisation, are created in a pair of glands called the testes. The testes sit in a pouch of skin called the scrotum that keeps them protected. For the sperm cells to travel, they need to be imparted in a fluid called semen that is produced by the prostate gland and the seminal vesicles. When sexual intercourse – or just sex – takes place, semen travels through the penis and is ejaculated into the vagina, allowing the sperm to seek out the egg. Millions of sperm cells travel through the harsh conditions of the vagina and only the absolute strongest swimmer makes it to the uterus. There it plunges into the egg and fertilisation occurs, impregnating the woman. In nine months, a little baby is born!
Adults who want to have sex but don’t want to have a baby make use of safe, protected sex practices. They may want to use condoms, a sheath made of thin rubber worn on the man’s penis to prevent the transference of ejaculate, or contraceptive pills taken by the woman to cease the process of ovulation. There are many other available contraceptives but ultimately, it is up to the adults to decide what they are comfortable using. It is also important that they vocalise to one another when they do and do not want a baby.
Reproduction is an intricate and wonderous process and something that can only be achieved by adult bodies that have experienced puberty. When Nolo really thinks about it, she’s proud to have a body that one day will be the host of such scientific wonders!
Illustrated and written for the IAMFORHER Foundation's educational program on puberty and menstruation for children and adolescents.
0 notes
Text
Gynecologist in Jaipur

Dr. Hema Agarwal is best gynecologist in Vidhyadhar Nagar, Jaipur. She has 17 years of experience in her field. She specializes in the diagnosis and treatment of various gynecological conditions including menstrual disorders, infertility, PCOS/PCOD, uterine fibroids and endometriosis. She completed her MBBS degree from SMS College, Jaipur (2001) & obtained degree of MS - Obstetrics and Gynecology from Dr. Sampurnanand Medical College, Jodhpur (2006). With her patient-centric approach, she is dedicated for promoting women's health and well-being.
Services : - PCOS/PCOD Treatment by Dr. Hema Agarwal
Treatment of PCOS / PCOD

Introduction
Polycystic Ovary Syndrome (PCOS) & Polycystic Ovary Disease (PCOD) are common hormonal disorders affecting women of reproductive age. These conditions can lead to various health issues including - irregular menstrual cycles, hormonal imbalances, and difficulties in conceiving. Meet to Dr. Hema Agarwal who is a renowed Gynecologist in Vidyadhar Nagar, Jaipur serving at Garg Heart Women Clinic. With an impressive experience of 17 years, she has been providing effective and compassionate care to women.
Understanding PCOS/PCOD
PCOS/PCOD is a complex disorder characterized by enlarged ovaries containing multiple small cysts. It is often accompanied by hormonal imbalances, leading to irregular periods, excess hair growth, acne, and weight gain. The condition affects not only physical health but also has significant emotional and psychological impacts on affected women.
Dr. Hema Agarwal's Approach to Treatment
With over 17 years of experience in gynecology, Dr. Hema Agarwal is well-equipped to diagnose and treat PCOS/PCOD effectively. Her approach involves a comprehensive evaluation of each patient's medical history, symptoms, and hormonal levels to create personalized treatment plans. Dr. Agarwal believes in addressing the root cause of the condition rather than merely managing the symptoms.
Holistic Care
At Garg Heart Women Clinic, Dr. Hema Agarwal as a Gynecologist in Jaipur gives a holistic approach to PCOS/PCOD treatment by focusing on lifestyle modifications, diet, exercise, and stress management. Her emphasis on lifestyle changes aims to improve overall health and hormonal balance, thereby alleviating the symptoms of the condition.
Medical Interventions
In addition to lifestyle changes, Dr. Agarwal may recommend specific medical interventions to regulate hormonal imbalances and manage PCOS/PCOD symptoms effectively. These may include oral contraceptives, hormone therapy, insulin-sensitizing medications, and fertility treatments for women trying to conceive.
Fertility Support
For women struggling with infertility due to PCOS/PCOD, Dr. Hema Agarwal offers compassionate Infertility Treatment in Vidyadhar Nagar, Jaipur. She understands the emotional toll infertility taken on women and provides guidance through assisted reproductive techniques, such as ovulation induction and in-vitro fertilization (IVF).
Patient-Centric Care
What sets Dr. Hema Agarwal apart is her patient-centric approach. She takes the time to listen to her patients, understand their concerns, and involve them in the decision-making process. Her empathetic demeanor and clear communication make her patients feel at ease, fostering a trusting doctor-patient relationship.
Community Involvement and Education
Dr. Agarwal's commitment to women's health extends beyond her clinic walls. She actively participates in community health programs, workshops, and awareness campaigns to educate women about PCOS/PCOD and the importance of regular gynecological check-ups.
Conclusion
As a gynecologist at Garg Heart & Women Clinic, Dr. Hema Agarwal has positively changed lives of countless women patients seeking for the effective PCOD / PCOS Treatment in Vidyadhar Nagar, Jaipur. Her expertise and dedication to women's health make her a trusted healthcare professional in the field. If anyone seeking effective treatment for PCOS/PCOD, then Dr. Hema Agarwal is the gynecologist to rely on for comprehensive and personalized care.
0 notes
Text
Question
Dear Father Angelo,
I always read your replies on the Dominican Friends website and always find them full of wisdom and charity. I thank you for your precious work. At the moment I do not have any questions for you, I just would like to offer my testimony as a woman, spouse and Christian mother, as I have noticed that there is always a lot of debate on the lawfulness of contraception within marriage and on natural methods. You always talk comprehensively about all the moral aspects of this matter and several times this has helped me to understand and appreciate even more the beauty of marital sexuality that is lived according to God’s will.
Considering the questions that many readers address you (for example, in the last couple of days, one was about the adoption of natural methods in case of irregular periods and one about the lawfulness of using contraception during breastfeeding), I have the impression that there are many misconceptions and misinformation on natural methods.
This is the reason why I am writing to you. I want to confirm that it is possible to live marital sexuality in a Christian way and that natural methods are also a journey of discovery of your own body offering peace and self-mastery.
As a woman, I can state that this body and fertility awareness is an amazing gift to yourself and your own husband. Unfortunately, I see many people around struggling to learn several things and develop extensive knowledge in many areas. However, they get discouraged when they are faced with the need to commit themselves to the understanding and study of their own body’s rhythms. For example, having irregular periods does not prevent the adoption of natural methods at all. On the contrary, monitoring periods can be of help to any woman who wants to understand whether there are hormonal problems causing irregularities and solve them (even just through simple precautions on diet and lifestyle).
Other times learning natural methods help understand that what may seem an irregular period is not actually so, as there are “phases” of it that regularly re-appear every month.
Moreover, menstrual cycles change throughout life: after the first pregnancy and once the suckling period is over, a lot of women discover a new regularity. Another thing I would like to witness is that it is possible to adopt natural methods during breastfeeding too.
Besides, natural breastfeeding (meaning to feed every time the baby asks for it, without alternating baby bottle and mother’s milk) usually delays the return of female fertility. According to the marvellous Creator’s plan, when the mother’s body is devoted to nurturing a newborn baby, another pregnancy is naturally postponed, so as to allow her to devote all her energies to breastfeeding. However, if the cycles reappear (this happened to me with my last daughter, as she used to sleep a lot at night and I had long intervals between feedings), it is always possible to adopt natural methods, as long as you do it with greater care though; for example, it can happen that you have to abstain during two periods in a month instead of one because signs of ovulation seem to repeat themselves. All this is normal and, if you experience it serenely, it can just increase love between spouses and their awareness of the miracle of their motherhood and fatherhood. This “exercise” also helps to get ready for harder times, when you may have to abstain for longer periods (we took the decision to abstain for several months after the birth of our first daughter, due to health reasons and complications arising after delivery).
The joy that you experience while living your marriage according to the Creator’s will is so big that human hardship during periods of abstinence is really a small thing. This is not only my thought, it is indeed also shared by my husband and other married couples that I know, who decided to live their marriage in this way. Besides, I would like to
tell women that the understanding and the deep acceptance of their own fertility can also help them to know themselves better psychologically and live with much bigger joy and awareness the marvellous experiences of pregnancy and delivery, which are not illnesses but rather a beautiful and essential part of our femininity.
Father, I do not know whether you find this witness useful. However, I urge you to continue your work in spreading the truth. Unfortunately – and I do not mean to judge - I realise with sadness that the pastors of the Church do not properly insist on this matter, probably because they think to impose upon couples too big of a yoke. Actually, it is not like that: living marriage in this way is a light yoke and it helps Christian married couples to mature in faith and encourages them to get informed, to understand and to apply all their intelligence to the discernment of truth. My husband and I have never used birth-control measures and natural methods have always been effective also in times when ,through prayer, we decided to wait a little before having another child.
I hope my witness can be helpful to somebody, I also hope I did not bother you with this long letter. You may take it as a further acknowledgement and thanksgiving.
Greetings,
Alessandra
Priest’s Answer
Dear Alessandra,
1. I warmly thank you for what you have decided to share with me and all our visitors.
The serenity that transpires from your words is an outward sign of the inner mastery and maturity you have acquired in your life.
This is probably a gift you inherited from your parents. Maybe it is the fruit of God’s grace and a life of prayer but, undoubtedly, it is also a reflection of conjugal intimity, which is lived according to God’s will.
2. I would particularly thank you for highlighting the fact that sometimes cycle irregularities can be an indication of other dysfunctions that require some adjustments in some areas that are not secondary at all, such as diet or certain lifestyles.
So you never cease to be surprised about the admirable wisdom of the Divine Law, therefore with the psalmist we also say: “I have seen a limit to all perfection; your commandment is exceedingly broad” (Psalm 119: 96).
It is only in our best interest to remain allied to the Divine Wisdom. The only thing we have to distrust is not the Divine Law. It is rather exclusively our judgement or knowledge, which are inevitably marked by limitations.
3. You write: “The joy that you experience while living your marriage according to the Creator’s will is so big that human hardship during periods of abstinence is really a small thing”.
The labour you talk about is the most beautiful labour, as it is the labour of virtue, which requires continuous self-transcendence, self-elevation and spirit of sacrifice. This labour always pays off, here as in any other area of life.
4. It is above all a joy arising from being preserved in grace, and thus from being able to keep rejoicing in the personal presence of God inside our heart, that is the ultimate goal of every human aspirations.
Without this presence, our heart would always remain unsatisfied and feel poor, or rather, extremely poor.
I sincerely thank you again.
I remind you as well as your family to the Lord and bless you.
Father Angelo
0 notes
Link
0 notes
Text
Yoga For Fertility: Benefits And Best Poses
Maybe you are thinking about embracing yoga for fertility, or perhaps considering how best to adjust your ongoing yoga routine to increase your possibilities of conceiving. Sounds perfect! Nonetheless, before you get out there and purchase a yoga mat or a bundle of 20 yoga for fertility classes then there are various things that you ought to be aware of.
Always keep in mind, before you even begin, that the majority of people today spend years, and in some cases decades, attempting to avoid pregnancy. It can then be a major shock when they quit utilizing contraception and don't rapidly get pregnant. However, in reality, this is not unheard of. It's similar to someone who hasn't exercised in a long time and then complains that they aren't skinny right away after starting!

It typically takes four to five months for a young couple with no fertility issues to conceive. It typically takes longer for an older couple. Although it may appear common for couples to achieve success on their first try, this is actually much less common than you might expect. Your doctor will only start to think that you might have fertility issues if you haven’t gotten pregnant in a year of trying. A doctor will rarely even consider infertility until after a year of trying.
Having said that, if you think it’s too soon to see your doctor or if he or she isn’t yet taking your concerns seriously, fertility yoga is still something you should do in the meantime.
At least in the West, yoga is usually seen as a way to unwind. It has numerous health benefits and is frequently regarded as a spiritual practice in Asia. However, in North America, Europe, and other Western nations, it is primarily regarded as a physical activity that involves stretching the muscles and improving flexibility. It can also help alleviate stress and emotional tension. When it comes to increasing fertility, all of these factors work together to provide significant advantages.
Yoga is frequently recommended as a fertility treatment because of its stress-relieving properties. Stress can frequently lead to infertility, particularly “unexplained infertility.” This implies infertility has no recognizable reason. There appears to be no apparent health issue with either partner’s reproductive system. The man’s sperm count is normal and ovulation is occurring when it should. But there is still no child on the way, which is heartbreaking.
Yoga to get pregnant is typically practiced by women for fertility reasons. For some strange reason, society still believes that the woman is most likely to blame when infertility is discussed. That to the side, it very well may be useful for men as well, however, remember that it won’t lessen anyone’s stress level if one of the partners feels constrained into a yoga practice that doesn’t intrigue them. If your partner hesitates, they might benefit more from other forms of relaxation, such as sports, meditation, or gym work. The most important thing is to just unwind in any way you can!
After mastering a general beginner’s yoga class to improve flexibility and reduce stress, you can work with experienced yoga teachers on specific poses that may affect fertility. Yoga poses that can relax, open the abdomen and pelvis, and increase blood flow to the reproductive organs are considered yoga for fertility.
You might want to incorporate the following yoga poses into your routine if you want to get pregnant:
Legs Up The Wall (Viparitakarani)
This has some of the advantages of inverted poses like the shoulder stand or headstand but without the potential drawbacks of having the hips raised high. Lie on your mat on your back with hindquarters against a wall and legs extended up the wall. As long as your hips remain level with your torso, you can practice this pose during your period.
Open Angle Forward Bend (Upavisthakonasana)
Stretch your legs out, wide open, while sitting on the floor. Twist forward with a straight back until you feel the stretch in the hamstrings, strolling your hands forward. Have mindfulness in the pelvic area and the hamstrings. Be kind to your mind’s pelvis.
Butterfly Pose (Baddhakonasana)
Still situated on the floor, twist the knees and bring the bottoms of the feet together before you. You can kind of flap your knees up and down like butterfly wings but don’t force it. This pose should make you feel at ease. This is another representation that opens and invigorates the pelvic area.
Pose of a Pigeon
There are a few variations of the pigeon pose. If you want to avoid making mistakes that could hurt your hips or knees, it’s best to learn this pose with a teacher.
Child’s pose (Balasana pose)
It helps you release hormones that help you feel less stressed. You must first kneel down before sitting on your heels with your hands at your sides to perform the pose. You should inhale and exhale at this position.
Whenever you have breathed out you ought to twist forward and permit your chest to lay on your thighs. After that, you should place your forehead on the floor and slide your arms along the back of your body. This position should be held until you feel tension. It is suggested that you hold the pose for at least one minute on average.
Supported headstand
Most trainers perceive this posture as the mother of all yoga presents. This is due to its challenging and strenuous nature. The great side with the posture is that other than decreasing pressure, it likewise alters the body in this manner taking strain from the heart. Additionally, the pose increases hormone production, which further reduces stress levels.
To make the posture, you really want to start in the Balasana’s posture then hold your hands together, and put your lower arms on the floor with your head between your fingers. You ought to breathe in and draw your feet nearer to your head with your impact points up and shoulder bone down. You should lift your legs up and exhale while in this position.
It is suggested that you stretch your legs upward in order to avoid putting pressure on your tailbone. You ought to stand firm on this foothold for somewhere around 10 seconds. You should gently curl your legs down and release into the child’s pose to end the pose. It is suggested that you practice against a wall so that you don’t put too much weight on your head and neck.
Despite the fact that this pose reduces stress and increases your chances of conceiving, menstruating women should avoid it.
Forward bend
Of all of them, this is probably the easiest. Simply bending forward with your legs straight is all that is required. You can sit down with your legs straight in front of you and slightly bend forward if you think you are not agile enough.
It is strongly suggested that you exercise these poses with caution to avoid injury. For ideal outcomes, it’s recommended that you practice under the management of an expert Yoga instructor and follow the diet plan to conceive faster provided by the trainers.
Before beginning a yoga practice while you may be pregnant, it is essential to consult both your doctor and a yoga instructor. If you tell your yoga instructor that you want to do yoga for fertility, they may suggest additional poses that could help you get pregnant!
0 notes
Text
New Earth
Kathryn looked at Chakotay laying in their bed as the morning light streamed across the covers, she slowly climbed under the duvet and stroked his face, it had been a whirlwind eight weeks since he had touched her heart with his tale of love, they had spent days making love in the bed, bending her over her bath, lying amongst the flowers, naming the constellations shining in the moonlight. "Hi Chakotay" Kathryn whispered into his ear, Chakotay groaned and pulled her into a kiss, but she pulled away. "I need to talk to you Chakotay" she whispered as a look of concern crossed his face. "I've been trying some of the cures I have created for this virus on myself, so I've been scanning regularly and .."
"You've been doing what?? Chakotay boomed "how could you be so stupid how do you know you won't kill yourself?"
"That's not the point" Kathryn replied curtly. The point is I have been scanning myself and it turns out the virus has interfered with all our usual medication, including.."
"Including what?" Chakotay pressed
"Contraceptives. I ovulated three weeks ago making me 5 weeks pregnant"
"Really?" Chakotay found his shock making way for a warm fuzzy feeling.
"Stop it" Kathryn snapped "I can't keep it. There's only two of us on this planet, what happens if we have an accident or get ill? What if we died and left a defenceless toddler alone. What happens when we die of old age and commit the child to 40 years of solitude? It's too risky. If we were on Voyager, or Earth this could work, but here, I won't condem a child to a life of loneliness. Our medical supplies won't last another 80 years, please know this is not a decision I have taken lightly."
"Of course" chakotay grimaced, "I can prepare a hypo but you will need to administer it. I will suport you but I wish it were different."
Two months later they were returned to Voyager. After the abortion Kathryn had given herself time to grieve but had also found a peace within herself. Her relationship with Chakotay had strengthened although she hadn't wanted to make love to him again too soon. On the second day of her return she found herself and Chakotay having a late dinner in her quarters and beckoned him to her bed. She parted her legs as he gently pushed himself inside her, kissing her neck and whispering words of love. She felt him tightening and panicked "pull out Chakotay" "Kathryn it's ok, the doctor readminstered our boosters but i won't do anything you dont want" he said as he pulled her into a cuddle "you'll resent me" Kathryn sniffed "if I had waited a 7 more weeks, I was too rash. You might not feel it now but you will" Chakotay shushed her "it wasn't the right timing, I only need you, I don't need anything else"
Present day
Chakotay awoke with a start. His vision quests did sometimes carry over into his dreams but this one had been recurring weekly. It was menacing and dark, the beating and whistling of feathers, the sound of a bird crying out, the sense of dread, loss. "Are you my lost child?" Chakotay had asked but he only heard and angry response echo through his mind "you must not ask me that" . He cursed himself for allowing any of his children to join Starfleet and put themselves in danger, why hadn't he and Kathryn encouraged them to stay planet side, safe and together as a family.
He heard Tuvok hail him over his comm "Captain, Admiral, please meet me in the conference room as soon as possible".
****
"We have identified a gaseous giant and small rocky moon at the coordinates we were given. Scans show there is a network of tunnels which our scanners are not able to permeate, no sign of Lohengrin."
Kathryn looked around the room "I don't want to waste any time, we will have a search party ready within the hour. Ensign Hussein please join Captain Tuvok and me, Captain Chakotay will remain on the ship should we be joined by any unexpected guests. Dismissed"
As the officers filed out Chakotay lingered, he walked around the table and towered over Kathryn. "Kathryn, what are you playing at? You're afraid aren't you, of what you might find, you're not protecting me, I won't let you do this, he's my son too, we BOTH encouraged him to join the Academy, we are both going to damn well see this through" he leaned down further, his face millimeters from her nose "permission to join the team Admiral". Kathryn met his eyes with an icy fire, she looked away, she nodded.
*****
Kathryn scanned her tricorder over the mouth of the caves "I'm reading human biosigns this way" she gestured down a tunnel and headed towards the location. She could hear noises and what sounded like words bouncing off the walls of the cave. She picked up the pace and hurried further down the tunnel, could this be Amal? She imagined turning a corner and seeing him there, waiting for her, embracing her outstretched arms. She stopped dead in her tracks as she saw two figures in front of her:
"Lottie, what are you doing here"
END OF SEASON ONE
To be continued .....
0 notes
Text
What is the difference between a tubal pregnancy and an ectopic pregnancy?
In ectopic pregnancy, implantation occurs in a site other than the endometrial lining of the uterine cavity, i.e., in the fallopian tube, horn of the uterus, cervix, ovary, or abdominal or pelvic cavity. Ectopic pregnancies cannot be carried to term and eventually rupture or involute.
Early symptomatology includes pelvic pain, metrorrhagia, and tenderness to the vaginal touch, especially when the cervix is displaced.
Syncope or hemorrhagic shock may occur upon rupture. Diagnosis is based on beta-hCG measurement and pelvic ultrasound. Treatment consists of laparoscopic or open surgical resection or IM methotrexate injection.
The incidence of ectopic pregnancy is approximately 2/100 diagnosed pregnancies.
Etiology of ectopic pregnancy
Factors that particularly increase the risk of ectopic pregnancy include
Tubal lesions
A history of ectopic pregnancy (risk of recurrence 10-25%)
History of pelvic inflammatory disease (especially Chlamydia trachomatis)
Previous abdominal surgery especially on the fallopian tubes, including tubal ligation
Other specific risk factors for ectopic pregnancy include
Intrauterine device (IUD) contraception
Infertility due to tubal damage
Smoking
History of induced abortion
Pregnancy is less likely to occur when an intrauterine device (IUD) is in place; however, about 5% of these pregnancies are ectopic.
Pathophysiology of ectopic pregnancy
The most common location of ectopic pregnancies is the fallopian tube, followed by the uterine horn. Cervical pregnancies, in a caesarean scar, the ovary, the abdomen or the interstitium of the fallopian tube are rare.
( You can follow your Pregnancy & Baby Tracker Pro week by week )
Heterotopic pregnancies (both ectopic and intrauterine) occur in only 1/10,000 to 30,000 pregnancies, but may be more common among women who have used ovulation induction or assisted reproductive technologies such as in vitro fertilization and gamete intrafallopian tube transfer (GIFT); in such cases, the reported rate of ectopic pregnancies is ≤ 1%.
The structure containing the fetus usually ruptures after 6 to 16 weeks. Rupture results in hemorrhage that may be progressive or rapid enough to cause hemorrhagic shock. Intraperitoneal blood irritates the peritoneum. The later the rupture, the more rapid the bleeding and the higher the mortality.
Symptomatology of ectopic pregnancy
Symptoms of ectopic pregnancy vary and are often absent until rupture occurs. Most patients present with pelvic pain (sometimes in the form of cramping) and/or vaginal bleeding. There may or may not be a delay or absence of menstrual bleeding, and the patient may not know that she is pregnant.
Rupture may be heralded by sudden severe pain, followed by syncope or symptoms of hemorrhagic shock or peritonitis. Rapid hemorrhage is more likely in ruptured ectopic pregnancies.
Pain on mobilization of the cervix, unilateral or bilateral adnexal tenderness on vaginal touch, or an adnexal mass may be present. The uterus may be slightly enlarged (but less than expected from delayed menstruation).
Diagnosis of ectopic pregnancy
Quantitative serum human chorionic gonadotropin beta subunit (beta-hCG)
Pelvic ultrasound
Sometimes laparoscopy
An ectopic pregnancy is suspected in any woman of childbearing age with pelvic pain, metrorrhagia, or unexplained syncope or hemorrhagic shock, regardless of contraceptive use, sexual intercourse, or delayed menses. The results of physical examinations (including pelvic touch) are neither sensitive nor specific.
A ruptured ectopic pregnancy is a surgical emergency because it causes maternal hemorrhage with a risk of death; prompt diagnosis is essential.
The first step is a urine pregnancy test, which is nearly 99% sensitive in diagnosing pregnancies (ectopic and others). When the urine beta-hCG test is negative and the clinical signs are not strongly suggestive of ectopic pregnancy, further testing is unnecessary unless the symptoms recur or worsen.
If the urine beta-hCG is positive or the clinical signs are strongly suggestive of ectopic pregnancy, a quantitative serum beta-hCG measurement and pelvic ultrasound are not indicated.
When the quantitative serum beta-hCG is < 5 mIU/mL, ectopic pregnancy is excluded. When ultrasound detects an intrauterine gestational sac, an ectopic pregnancy is highly unlikely except in the woman who has used assisted reproductive techniques (which increases the risk of heterotopic pregnancy); however, a cornual or intra-abdominal pregnancy may initially present as an intrauterine pregnancy.
Ultrasound images suggestive of an ectopic pregnancy (seen in 16 to 32%) of cases include complex masses (mixed solid and cystic masses), particularly in the adnexa, and fluid effusion from the cul-de-sac of Douglas.
If the serum beta-hCG is above a certain level (called the discriminatory zone), the ultrasound should detect a gestational sac in case of intrauterine pregnancy. This level is usually about 2000 mIU/mL. If the beta-hCG level is above the discriminatory zone and no intrauterine gestational sac is detected, an ectopic pregnancy is likely. The use of the transvaginal route or color Doppler can improve detection rates.
If the beta-hCG level is below the discriminatory zone and the ultrasound is negative, it may be an early intrauterine pregnancy or an ectopic pregnancy. If the initial clinical workup suggests an ectopic pregnancy (e.g., significant peritoneal irritation or hemorrhage), diagnostic laparoscopy may be necessary for confirmation.
When an ectopic pregnancy appears unlikely and the patient is stable, plasma beta-hCG levels can be monitored on an outpatient basis (typically every 2 days). Normally, the level doubles every 1.4 to 2.1 days until day 41; in an ectopic pregnancy (as in non-progressive pregnancies), levels may be lower than expected and do not double as rapidly.
If the beta-hCG level does not rise as expected or falls, the diagnosis of spontaneous miscarriage or ectopic pregnancy should be considered.
#pregnant kink#pregnancy#make me huge#huge pregnant belly#belly movement#squirming#preggolife#pregnant#pregnant women#pregnantbeauty#pregnantbelly#big belies#mother#sexy belly#long post#multiples#vintage preg#progress#shes so round#twins
0 notes
Text
@rosaliewarda sent me this submission: "Some people here seem to think women find abortion an easy solution to have fun without consequences. This while also saying that abortion is painful and brutal. Well yes it is. No woman would say the opposite. But deciding for women whether or not they have the right to go through this painful procedure is also brutal. What about the victims of rape? Would you also tell them that they should have been careful?"
I usually don't bring up cases of rape because that is an incredibly small group, and most pro-abortionists still want abortion legal regardless of rape being the reason for pregnancy. The average rate of pregnancy that results from unprotected sex is 2-4%. A survey of U.S. women's reasons for choosing abortion found that only one percent reported "rape" as a reason and less than one half of one percent reported that rape was the main reason.
If a woman is raped, I suggest she seek medical care immediately. Do not hesitate. If the victim is not already pregnant from prior, freely-chosen sexual activity, has not yet ovulated (i.e. has not released an egg from her ovary into the fallopian tube where it could be fertilized by the attacker's sperm), the morning-after pill can reasonably be expected to prevent her from ovulating. Doctors can test the woman's LH levels, and if it's determined that her LH levels have spiked and she is ovulating, the morning-after pill will not be able to block the egg's release from her ovary, making it an abortifacient if used. So it should only be used to prevent ovulation. If she has already ovulated and conceived, then she should receive the utmost love and support in her pregnancy. I think the rapist shall be held liable for all of her hospital bills, child support payments, and every bill for that child. That's a law we need to push for. Like really push for.
I will never blame a woman for getting pregnant as a result of rape. She is the victim. But I don't believe she should abort her baby because it's not the baby's fault. "A hint is found in another study of 164 women who had rape pregnancies (conducted for the book Victims and Victors). In that study, the majority of those who had abortions said it only caused additional problems and the vast majority regretted having abortions. By contrast, among those who delivered the child, satisfaction was higher and none stated any regret for giving birth."
People need to stop scaring victims of rape into getting an abortion. It is not their rapist's baby; it's her baby. It is a social myth that abortion is her best option. It's not.
#submission#rape#rape victims#prolife#i know prolifers hate plan b#but if its only used in the very rare cases as a contraceptive then its fine because theres no embryo conceived#it can only be a contraceptive if shes not ovulating#catholic hospitals are very strict on its use for rape victims as a contraceptive#i wonder with states outlawing abortion#that those rules will apply as well3#but theres also a lot of side effects to it#abortion#pro-life#pro life#anti abortion#rosaliewarda
16 notes
·
View notes
Note
Request: as Catholics, Michael and Victoria don’t use contraception or use abortions, and when she ends up pregnant after James, as they obviously still can’t get enough of each other and insatiable for each other, they are happy to add to their family and even after that little Corleone, they end up welcoming a few babies after that, and many wonder how on earth but Michael and Victoria just knowingly look at each other and know that they have so many kids is because they are horny 24/7 for each other and have sex wherever and whenever they can… and they have more than enough money and space for them all too… and Michael can never say no to Victoria and both of them have breeding kinks…
Niccolo (St Niccolò Politi)
Verona (Province of Verona)
Vincent (St Vincent de Paul)
James (St James the Great)
Giuseppe (St Joseph the Hymnographer)
Xavier (Saint Francis Xavier)
Leoluca (St Leoluca of Corleone)
Valentia (Province of Vibo Valentia)
Michael & Victoria
Niccolò, Verona, Vincent & James
Giuseppe, Xavier, Leoluca & Valentia
OH WOWWW THAT IS A LOOOOT OF CORLEONE BABIES!! 😳😅 I see Michael and that breeding kink of his has definitely gone a long way. I guess in this AU prompt we can definitely say Victoria’s made up for her five year break as the twins were growing up since these two just want a bigger family lmfao 😂 (and can’t get off each other in bed, of course). Let’s see just how all those babies joined the family, starting with baby #5 being conceived in 1958! ❤
“I’m out, baby.” You let out a soft exhale, clutching the bathtowel wrapped around your body as you enter the bedroom. “Hiii.”
“Hi, darling.” Michael raises his head up from his book—laying down on the bed. “Feeling more refreshed?”
“Mhmm.” You smile back, letting the towel around your hair loosen over your shoulders. “Much, much better. Geez, what a day. Sorry I took a little longer than I thought.”
“You apologize for the most ridiculous things sometimes.” Michael chuckles quietly, setting his book down on the night table before eyeing the towel wrapped around your naked body. “All dry?”
“Not yet.” You pull off your hair towel, running your hands through your still moist hair. “Think I’m just going to have it air dry for tonight.”
“Not the towel I was referring to, baby.” Michael eyes the peek of cleavage showing from your bathtowel.
“Maybe.” You tease back, clutching onto your bath towel and squeezing your breasts together. “Why? You know I’m gonna get dressed in my nightgown and join you.”
“I want you to take it off.” Michael gazes at you. “No use walking around with that wrapped all over you. Strip.”
‘Fuck. Why does he have to say it like that?’ Blushing furiously, you unravel the bath towel and let it drop to your feet—remaining completely naked in front of Michael.
“Good.” Michael murmurs as his eyes greedily dart up and down your body—complete and utter perfection to him all over. “Were you able to check what we were talking about earlier?” Michael begins to rise from the bed to approach you.
“I did.” You bite down on the corner of your lip, rubbing up your arm.
“And?” Michael’s eyes fill with curiosity as he stands in front of you; dressed only in a white tank top and grey briefs himself.
“We can’t.” You shake your head as Michael places his hands over your hips, pulling you closer to his body.
“We can’t?” Michael repeats, raising a brow.
“I’m ovulating.” You blush, nodding. “I noticed already when I was in the shower.”
“So…” Michael’s curiosity only continues to grow as he and you both know you have condoms readily available—albeit barely use them to begin with, but the two of you have strictly avoided having sex on unsafe days unless you were both planning to have another baby Corleone.
“I don’t want to use those either.” You already know Michael’s referring to contraceptives. “’Cause if I have you, I want all of you.” You hook your fingers into the strap of Michael’s top, insistingly pulling.
“You’re going to have to give me a straight answer as to what you want, Victoria. I can’t read your mind.” Michael’s hand squeezes over your ass.
“Michael,” you whine, pressing your breasts up against Michael’s chest. “You had me strip down and get all hot and bothered for you so quickly—how long are you gonna tease me? Mm? Want me to beg for you to fuck me?”
“Don’t give me any ideas, sweetheart. We can always resort to that depending on my mood.” In an instant, Michael overpowers you by pinning you up against the bedroom wall—his hands tightly laced with yours and pressed up to the wall.
“Against the wall?” You breathe out, more than eager for Michael to take you right here, right now—anywhere, it doesn’t matter.
“You once told me—” Michael squeezes your face, wrapping your thighs around his waist. “Anywhere, anytime. Isn’t that right, baby?”
“Yes, please.” You groan as Michael lets his erect cock spring free from his briefs. “Please.”
“One year after James—you want to go again?” Michael taps his cock over your throbbing clit.
“S-so what?” You moan. “Fuck me and I’ll think of baby names while you make me cum.”
“There’s other ways you can ask for me to knock you up again, darling.” Michael breathes hotly over your lips, beginning to rub his forefingers over your clit in a lazy motion. “Isn’t that right?”
Screaming out, “yes, Michael, yes!” thereafter isn’t the only time you’ll be doing so tonight.
Ten minutes into the heated fuck session against the bedroom wall, you can neither keep your moans quiet nor do you even try to as Michael pounds into your pussy—insistent on hitting your G-Spot.
“Fuck, yes!” Your voice shakes as you keep your thighs wrapped around Michael’s waist obediently.
Barely holding onto Michael’s shoulders for balance, you whimper and whine about watching his cock thrust in and out of your soaked pussy.
Both of you groan against each others lips, ensnared in a deep, hot kiss only eager to keep fucking in one spot with no intention to move over to the bed.
“Michael!” You squeal, digging your nails into his back—feeling your legs shake against him like jelly from the way Michael demands an orgasm out of you.
“Oh, baby,” Michael pants, watching as droplets of water drip off the tips of your hair and down to your breasts jiggling from Michael’s rough, rapid thrusting.
Michael and you both said your fifth child—a son whom you named after your father, Giuseppe—was not a surprise but a planned new addition to the family, citing that night to yourselves of course.
The only thing that you and Michael can say is a surprise alongside your family is how only eight months after your pregnancy with Giuseppe you somehow managed to conceive again as if you were trying to do so as soon as possible.
“Harder! More, please!” You let out a half whine, half moan being fucked roughly mid air.
In truth, you’d almost been certain it wasn’t an unsafe day for you, but it’d also be a lie if you said you cared anymore.
When was there ever a time you and Michael could get your hands off of each other, satiable with all that sexual desire?
Resting his chin over your shoulder and locking your body in a position so Michael has your legs raised up as far as they can go to your head midair, you helplessly watch his thick cock spreading your pussy with each thrust.
Your clit still drips with cum and spit from your last orgasm up to the point it begins to drip down on the bedroom carpet; still being bounced up and down on Michael’s cock as fast as he can possibly fuck you.
“What did I say, baby?” Michael grunts in your ear—his tousled hair beginning to stick to his forehead from sweating. “I’d make it up to you, didn’t I?”
“Y-yessssss!” You whimper, almost beginning to think to yourself you should keep an attitude more often to be fucked like this.
To you there isn’t a single sight that can match how sexy it is to see yourself giving into a sense of euphoria while being fucked in front of your bedroom mirror.
Michael’s hair hangs over his forehead—his eyes dark like onyx and fixated on keeping you in his grasp tightly while relentless ramming into your tight pussy.
“More!” Desperate for more and more, you even try to push and roll your hips back onto his—every thrust of his cock like water to an endless thirst inside of you.
“You fuck so good, baby,” Michael roughly tugs on your hair to get you to face him before he kisses you over your mouth, quick to replace his parting lips with his fingers still dewy with your cum.
“No wonder Verona keeps wondering when she’s going to have a baby sister.” Connie laughed as she sat next to you the day you returned from the hospital after yet again, giving birth to your sixth child—another son whom you and Michael named Xavier. “She knows neither of you are going to stop either, huh?”
“Oh, please.” You flush red out of embarrassment, gently holding your sleeping newborn son in your arms. “He was a complete surprise to us. An adorable, tiny little surprise—” you beam down at your son, giggling, “but a surprise nonetheless.”
“Victoria, honey.” Connie crosses his arms her arms, staring at you in disbelief. “Come on. How many more times are you going to say that? A surprise? Well, if you’re taking my brother to bed—”
“Connie!” You whine.
“—then how is this a surprise?!” She bursts out laughing. “I’m pretty sure you know what you’re doing just as you know what to expect from it.”
But perhaps the biggest surprise came to you and Michael in late 1960 when the jokes of “when is Victoria going to get pregnant again?” finally came to an end that you conceived with your second set of twins.
“Oh my Goddddd!” A filthy loud moan escaped your lips as your body twitched from your fourth orgasm washing over you.
“Fuck.” Michael hisses, pulling his cock out of you with one swift movement in the midst of his own orgasm.
You gasp out in surprise, flinching as the last two, thick spurts of Michael’s cum land over your face and neck with the rest practically gushing out of your pussy.
“M-Michael,” you whine, grabbing onto his arm weakly as you plop back down on the bed.
“This is a good look for you, baby.” Michael breathes heavily, spreading open your pussy to see a pool of cum oozing out slowly. “Covered and filled with my fucking cum.”
And to think you were just a little embarrassed seeing Doctor Katherine after a morning of nausea and vomiting only to realize a few months in that your baby bump had doubled in size, just like during your first pregnancy with the twins.
Not only were you and Michael escastic but so were your family, friends, and especially Niccolo and Verona who’d begun to bet how many siblings they’d have by now and if it would be more baby brothers.
A surprise until the very end, you gave birth to twins again in 1961 whom in the midst of crying happy tears holding your little crying babies in your arms—estatic to give Michael the news.
Perhaps out of everyone including you and Michael combined, Verona was the most overwhelmed with joy and excitement to welcome a one baby sister to the family named Valentia, and her twin brother Leoluca.
Having two more children than your own mother did with you and your brothers, the Corleone family if anything was bustling with you and Michael’s children and the two of you wouldn’t want it any other way.
Being able to see Vito beaming happily as he hugs onto eight of his grandchildren for a family photo was enough to make your heart swell with joy to begin with, but of course you and Michael have come to a unsaid decision that eight little Corleones running around in the compound is just enough!
#godfather au#Michael corleone#Michael corleone fanfic#moth to flame fic#michael corleone x reader#godfather x reader#godfather fanfic#michael corleone x reader smut#smut prompts
98 notes
·
View notes
Last Seen Blogs

jbtddt
Untitled

itsjustemzhi-blog
Emzhi :D

biussbuse
Biuss

jaydoesanrp
Inactive

jbryantart-blog
jbryantart