#scicomm coronavirus
Text
#science#science communication#scicomm#stem#science education#science blog#biology#covid19#covid#coronavirus#vaccination#public health#pandemic#nobel prize#nobel peace prize
42 notes
·
View notes
Text
From the report by Beth Mole, posted 29 Feb 2024:
In a lengthy background document, the agency laid out its rationale for consolidating COVID-19 guidance into general guidance for respiratory viruses—including influenza, RSV, adenoviruses, rhinoviruses, enteroviruses, and others, though specifically not measles. The agency also noted the guidance does not apply to health care settings and outbreak scenarios.
"COVID-19 remains an important public health threat, but it is no longer the emergency that it once was, and its health impacts increasingly resemble those of other respiratory viral illnesses, including influenza and RSV," the agency wrote.
The most notable change in the new guidance is the previously reported decision to no longer recommend a minimum five-day isolation period for those infected with the pandemic coronavirus, SARS-CoV-2. Instead, the new isolation guidance is based on symptoms, which matches long-standing isolation guidance for other respiratory viruses, including influenza.
"The updated Respiratory Virus Guidance recommends people with respiratory virus symptoms that are not better explained by another cause stay home and away from others until at least 24 hours after both resolution of fever AND overall symptom are getting better," the document states. "This recommendation addresses the period of greatest infectiousness and highest viral load for most people, which is typically in the first few days of illness and when symptoms, including fever, are worst."
The CDC acknowledged that the eased isolation guidance will create "residual risk of SARS-CoV-2 transmission," and that most people are no longer infectious only after 8 to 10 days. As such, the agency urged people to follow additional interventions—including masking, testing, distancing, hygiene, and improving air quality—for five additional days after their isolation period.
"Today’s announcement reflects the progress we have made in protecting against severe illness from COVID-19," CDC Director Dr. Mandy Cohen said in a statement. "However, we still must use the commonsense solutions we know work to protect ourselves and others from serious illness from respiratory viruses—this includes vaccination, treatment, and staying home when we get sick."
Overall, the agency argued that a shorter isolation period would be inconsequential. Other countries and states that have similarly abandoned fixed isolation times did not see jumps in COVID-19 emergency department visits or hospitalizations, the CDC pointed out. And most people who have COVID-19 don't know they have it anyway, making COVID-19-specific guidance moot, the agency argued.
In a recent CDC survey, less than half of people said they would test for SARS-CoV-2 if they had a cough or cold symptoms, and less than 10 percent said they would go to a pharmacy or health care provider to get tested. Meanwhile, "The overall sensitivity of COVID-19 antigen tests is relatively low and even lower in individuals with only mild symptoms," the agency said.
The CDC also raised practical concerns for isolation, including a lack of paid sick leave for many, social isolation, and "societal costs."
The points are likely to land poorly with critics.
“The CDC is again prioritizing short-term business interests over our health by caving to employer pressure on COVID guidelines. This is a pattern we’ve seen throughout the pandemic,” Lara Jirmanus, Clinical Instructor of Medicine at Harvard Medical School, said in a press release last month after the news first broke of the CDC's planned isolation update. Jirmanus is a member of the People's CDC, a group that advocates for more aggressive COVID-19 policies, which put out the press release.
Another member of the group, Sam Friedman, a professor of population health at NYU Grossman School of Medicine, also blasted the CDC's stance last month. The guidance will "make workplaces and public spaces even more unsafe for everyone, particularly for people who are high-risk for COVID complications," he said.
But, the CDC argues that the threat of COVID-19 is fading. Hospitalizations, deaths, prevalence of long COVID, and COVID-19 complications in children (MIS-C) are all down.
COVID-19 vaccines are safe and effective at preventing severe disease, death, and to some extent, long COVID—we just need more people to get them.
Over 95% of adults hospitalized with COVID-19 in the 2023–2024 respiratory season had no record of receiving the seasonal booster dose, the agency noted.
Only 22% of adults got the latest shot, including only 42% of people ages 65 and older. In contrast, 48% of adults got the latest flu shot, including 73% of people ages 65 and older. But even with the crummy vaccination rates for COVID-19, a mix of past infection and shots have led to a substantial protection in the overall population.
The CDC even went as far as arguing that COVID-19 deaths have fallen to a level that is similar to what's seen with flu. "Reported deaths involving COVID-19 are several-fold greater than those reported to involve influenza and RSV. However, influenza and likely RSV are often underreported as causes of death," the CDC said.
In the 2022–2023 respiratory virus season, there were nearly 90,000 reported COVID-19 deaths.
For flu, there were 9,559 reported deaths, but the CDC estimates the true number to be between 18,000 and 97,000.
In the current season, there have been 32,949 reported COVID-19 deaths to date and 5,854 reported flu deaths, but the agency estimates the real flu deaths are between 17,000 and 50,000.
"Total COVID-19 deaths, accounting for underreporting, are likely to be higher than, but of the same order of magnitude as, total influenza deaths," the agency concluded.
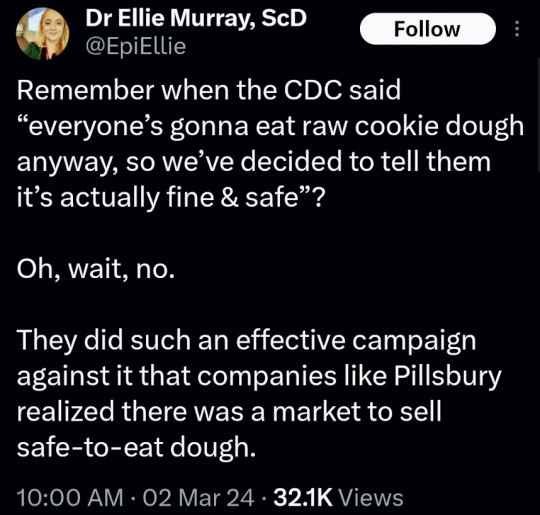
(say no to raw dough: CDC)
#please stay safe#the vaccines are safe#yes the covid shot is safe#covid is not a hoax#covid causes permanent long term damage to your body even if you're healthy#news#scicomm#science#ars technica#covid--19#coronavirus#beth mole#pandemic#the cdc#centers for disease control#5 day covid isolation#yes you should stay home for at least 5 days if you test positive for covid#Open windows to ventilate indoor space with outdoor air to prevent virus transmission#Wear a mask that doesn't touch your lips#keep distance from others
5 notes
·
View notes
Video
undefined
tumblr
Black medical professionals who are members of the National Academy of Medicine address the disproportionate impact that COVID-19 has had on the Black community and why they encourage everyone to get vaccinated. (This was video produced with our parent organization @APPCPenn.)
31 notes
·
View notes
Text
Millions of farm animals are being killed and thrown away. Not “euthanized” the way you think.
(TW Methods of killing animals below)
The US has shut down many meat processing facilities and farmers don’t have a place to send their animals as they are meant to be moved out. So you may have heard that millions of animals, mostly pigs and chickens, are “being euthanized.”
But here’s the thing: the public’s definition of euthanasia is generally killing an animal 1) nicely and quickly, 2) for mercy to that animal because they are irredeemably suffering, and 3) through chemical injection. Farmers are not killing these animals the way or for the reason a vet kills your old, sick dog. Most, especially chickens, are being baked alive and/or suffocated due to circumstances, not due to their health. It’s a complicated topic and please read this before commenting, but in short: the public is being misled because the word euthanasia is so nice-sounding. Heck, it translates to “good death!” So all these deaths are actually great, right? Hooray!
Background: Due to the coronavirus leading to slaughterhouse closures, farmers don’t have anywhere to send their animals. With pigs that means that they keep growing (they aren’t fully grown at slaughter time) and as piglets mature, they need the space to move to adult barns. A similar situation with chickens. (Not cattle as much since they can stay on feed lots/pasture a bit longer.) That leads to overcrowding, and to avoid that, farmers are killing the animals and throwing the bodies away.
Acceptable forms of killing: The American Veterinary Medical Association has a detailed document on what forms of killing are allowed when a farmer needs to depopulate. “Depopulation” is not a common word that will make it to any headlines, so I understand that euth is a better word and to be fair it is used by the industry in this setting. But to be more specific about what is allowed vs what is happening, here’s from Washington Post:
"For poultry and pigs, they allow animals to be killed by simply shutting off the ventilation system fans (heat or carbon dioxide may be added). The animals die of hyperthermia, baking and suffocating over a period of several hours."
"The industry generally uses the ventilator shutdown method or a water-based foam, the consistency of firefighting foam, that flows up and over, suffocating birds in seven to 15 minutes."
What people assume: The title of this post points out that animals are not being euthanized the way you think because generally the public thinks euth’d animals are getting a nice, necessary, instantaneous death. Even if the industry does use the term to mean more like “killed for reasons other than consumption.”
I anticipate some response to this: “But OP! Sometimes you gotta un-alive animals! Just don’t say ‘kill’ or ‘slaughter,’ those words make it sound bad :( ”
Listen, I know that there are PLENTY of good reasons to kill animals. And grey areas and bad reasons. But you don’t get to do whatever you want and tell people not to say it out loud because it sounds bad! There is a point at which you have to say “this is what’s happening; the word ‘kill’ is neutral, understood correctly, and accurate from all perspectives. You can decide yourself whether this killing is good or bad.”
#Meat#Science communication#Scicomm#Coronavirus#Covid-19#Animal Death#Euthanasia#Graphic#Animal Suffering
131 notes
·
View notes
Video
youtube
You've probably heard about the three big symptoms of COVID-19 — but there seem to be others, too. So, how do you know if you have COVID-19, or just allergies?
#SciShow#Hank Green#scicomm#science#eduction#COVID-19#coronavirus#corona#covid#allergies#medicine#distance learning
100 notes
·
View notes
Link
Being skeptical is good, but you honestly don’t have time to personally fact-check every single piece of news you see. So it’s nice to know that there are some journalists and outlets that simply have high scores of accountability, and you can probably just take them at their word. Here are some of the most credible journalists to follow on coronavirus.
71 notes
·
View notes
Photo

Stay safe out there (at home), flatten the curve and save lives! <3 Thanks to my lovely wife for her input and pushing me to finish this!
More of my illustrated shenanigans: https://artibiotics.com/
Support: https://artibiotics.com/support
#covid19#coronavirus#caretoon#webcomic#scicomm#artibiotics#cilein#health caretoon#medcomic#covid-19#flattenthecurve
50 notes
·
View notes
Text
Episode 65: Not talking about the coronavirus
In which we try very hard to not talk about the only thing everyone is talking about.
Also, we launch a Patreon
This episodes reading list
Apple Podcasts // Spotify // Stitcher // Google Podcasts
More science shows are live now on The Stimulus Network
Support us on Patreon
#coronavirus#podcast#science news podcast#scicomm#psychology#behaviour#research#STEM#sciblr#conspiracy theories#conspiracy#mindfulness#social media#fake news
3 notes
·
View notes
Text

___________
Can you support Sidewalk Science Center on Patreon?
Before the current shutdowns due to Coronavirus, I was hosting Sidewalk Science Center three times a week in public parks. Now, with my day job shut down (museum tour guide) I have to rely solely on attempting virtual livestream sessions, and selling educational science kits, in order to make ends meet.
Patreon lets you get involved with my science education company, Experience Daliona. You'll see new projects. You'll see new experiments. You'll get sneak peeks into the educational kits I'm developing. And so. Much. More.
Even $1/month will help, because every dollar provides science experiences for about 17 kids. Support with as much or as little as you can!
Coronavirus is forcing us all to take on roles and follow alternative routes just to make ends meet. The long-term goals of Experience Daliona, through our Sidewalk Science Center program, are to provide resources for the community every single week, giving people the chance to engage with tools and concepts they might not anywhere else, both in positive community interactions and scientific resources.
Support my Patreon here
2 notes
·
View notes
Link
1 note
·
View note
Photo

#phdstudent #business #medical #wakeup #history #coronavirus #physics #dna #scicomm #truth #molecularbiology #study #nasa #researchers #instascience #architecture #microscope #womeninscience #biochemistry #microscopy #phdjourney #researchpaper #genetics #healthcare #knowledge #student #learning #academia #cancer #inspiration
#phdstudent#business#medical#wakeup#history#coronavirus#physics#dna#scicomm#truth#molecularbiology#study#nasa#researchers#instascience#architecture#microscope#womeninscience#biochemistry#microscopy#phdjourney#researchpaper#genetics#healthcare#knowledge#student#learning#academia#cancer#inspiration
0 notes
Text
Crochet coronavirus step-by-step
#etsy#crochet#amigurumi#sciart#science#crafts#art#scicomm#crochet patterns#tiktok#covid19#coronavirus
0 notes
Link
From the report by Sarah Zhang, posted 1 Nov 2021:
The answers were simpler when we thought we could vaccinate our way to herd immunity. But vaccinations in the U.S. have plateaued. The Delta variant and waning immunity against transmission mean herd immunity may well be impossible even if every single American gets a shot. So when COVID-related restrictions came back with the Delta wave, we no longer had an obvious off-ramp to return to normal—are we still trying to get a certain percentage of people vaccinated? Or are we waiting until all kids are eligible? Or for hospitalizations to fall and stay steady? The path ahead is not just unclear; it’s nonexistent.
We are meandering around the woods because we don’t know where to go.
What is clear, however, is that case numbers, the metric that has guided much of our pandemic thinking and still underlies CDC’s indoor-masking recommendation for vaccinated people, are becoming less and less useful.
Even when we reach endemicity—when nearly everyone has baseline immunity from either infection or vaccination—the U.S. could be facing tens of millions of infections from the coronavirus every year, thanks to waning immunity and viral evolution.
(For context, the flu, which is also endemic, sickens roughly 10 to 40 million Americans a year.)
But with vaccines available, not every case of COVID-19 is created equal.
Breakthrough cases are largely mild; 10,000 of them will cause only a fraction of the hospitalizations and deaths of 10,000 COVID cases in the unvaccinated. The more highly vaccinated a community is, the less tethered case numbers are to the reality of the virus’s impact.
So if not cases, then what? “We need to come to some sort of agreement as to what it is we're trying to prevent,” says Céline Gounder, an infectious-disease expert at New York University. “Are we trying to prevent hospitalization? Are we trying to prevent death? Are we trying to prevent transmission?” Different goals would require prioritizing different strategies.
The booster-shot rollout has been roiled with confusion for this precise reason: The goal kept shifting. First, the Biden administration floated boosters for everyone to combat breakthroughs, then a CDC advisory panel restricted them to the elderly and immunocompromised most at risk for hospitalizations, then the CDC director overruled the panel to include people with jobs that put them at risk of infection.
On the ground, the U.S. is now running an uncontrolled experiment with every strategy all at once. COVID-19 policies differ wildly by state, county, university, workplace, and school district. And because of polarization, they have also settled into the most illogical pattern possible: The least vaccinated communities have some of the laxest restrictions, while highly vaccinated communities—which is to say those most protected from COVID-19—tend to have some of the most aggressive measures aimed at driving down cases.
“We’re sleepwalking into policy because we’re not setting goals,” says Joseph Allen, a Harvard professor of public health. We will never get the risk of COVID-19 down to absolute zero, and we need to define a level of risk we can live with.
Scientific experts have been reluctant to make that call themselves. For one, there is real scientific uncertainty ahead. We don’t know how much immunity may continue to wane, how long the effects of a booster last, the exact incidence of long COVID in the vaccinated, or if a new variant will upend even the best-laid plans. But the level of COVID-19 risk we can live with is also not an entirely scientific question. It is a social and political one that involves balancing both the costs and benefits of restrictions and grappling with genuine pandemic fatigue among the public...
* * * * * *
One plausible goal is to focus on minimizing COVID-19’s impact on hospitals. A collapsed health-care system means more people will die, not just of COVID-19 but from other treatable diseases and injuries. Elsewhere in the world, like in the U.K. and Germany, leaders have explicitly tied their policies to containing hospitalizations rather than all cases. But in addition to hospitalizations, Gounder suggests we should also consider the risk of long COVID. “I think for people that is the big question. We just don’t know enough,” she says. Preliminary data suggest vaccines do reduce the risk of long COVID, but exactly how much is unclear given the uncertainties in diagnosing it.
Once we’ve defined what we are trying to prevent, we can define thresholds for lifting and, if necessary, reinstating COVID-19 measures. This can actually be quite tricky if the goal is minimizing hospitalizations, a lagging indicator that gives you a picture of the past rather than the present. By the time hospitalizations start to rise, a bigger increase may already be baked in with people already infected but not yet sick enough to see a doctor.
What to track instead? Here are some answers I got from scientific experts: hospitalizations and deaths, but stratified by age and vaccination status; a combination of vaccination rate and local transmission; a combination of vaccination rate and hospitalizations; a combination of long-COVID cases, hospitalizations, and deaths; a combination of case growth rate, testing uptake, vaccination rate, and hospitalizations.
If this seems confusing, why not consider a real-life example? San Francisco and seven other Bay Area counties recently set three-pronged criteria for lifting indoor mask mandates: (1) Community transmission is moderate, as defined by the CDC, for at least three weeks, (2) hospitalization numbers are low and stable, and (3) 80 percent of the total population is fully vaccinated or eight weeks have passed since COVID-19 vaccines have been available for kids age 5 to 11.
* * * * * *
Even when the coronavirus is endemic, it will still make people sick and it will still cause deaths and hospitalizations. That means our fight against COVID-19 is not over, and we might consider strategies sustainable over the long term. Better ventilation, for example, can make indoor spaces safer against all respiratory viruses, not just COVID-19. And even without mask mandates, people who feel at risk can still voluntarily mask up. In the longer term, Çevik says, we also need less focus on policies that work by “reducing small risks among many” and more on policies targeted at the people most affected by COVID-19. During the pandemic, the virus has disproportionately sickened people who are poor, who are less likely to be able to work from home, and who are less likely to have space to isolate from their family at home. When COVID-19 becomes endemic, it will likely, as many diseases are, continue to be correlated with poverty.
“Pay much more attention to who and why people are at risk,” says Stefan Baral, an epidemiologist at Johns Hopkins University. Baral says public health needs to go back to its traditional roots, where tackling disease also means reforming the living and working conditions that make people more susceptible. For example, universal paid sick leave and free voluntary isolation spaces can help minimize the impact of COVID-19, as well as many other diseases.
Hard questions lie ahead, and the answers require political will. But first, we have to stop avoiding them. We need a goal.









(Dr. Chandy John) (Prof. Bill Hanage) (Prof. Yamey)
#health#scicomm#coronavirus#news#science#how to beat covid#return to normal#pandemic#covid vaccine#covid vaccine for children#covid vaccine for kids#please get vaccinated#long post
23 notes
·
View notes
Photo

Trump Falsely Distorts New York Times COVID-19 Science Story
In a weekend tweet, President Donald Trump erroneously described a New York Times article, falsely stating that it said the coronavirus originated in Europe and suggesting that it had no named sources.
20 notes
·
View notes
Video
youtube
Today we chat about what it’s like to be a baby born in a time of COVID!
0 notes
Video
youtube
You're likely hearing a lot about COVID-19's fatality rate. But while that number is important, it actually doesn't say much about you as an individual.
56 notes
·
View notes
Last Seen Blogs

ariaplumbing1
Untitled

besthealthtipsrp
Ajaykumarrp

googlesamachar
Short News in Hindi: Google Samachar

viaggitours
Untitled

jayrek12
Untitled