#so that it will cover my prescriptions and medical procedures and not fight me about covering them
Text
hey y'all weird question time again
In the US, with insurance, what's a ballpark range for how much you'd expect to pay out of pocket for an MRI?
also hi crafting updates should resume in the next few days I was panicking a little about getting an MRI and that prevented crafting, and then I ended up not even getting it so all the panic was for nothing
#the person behind the yarn#I just went to get one (did not end up getting one)#and after fretting about it so much over the course of the day it caused a health flare up of like all of my other issues#I got there and they were like okay! pay us 800 dollars#I pay a uh. pretty significant percentage of my monthly income to my insurance premiums#specifically so I could get the best possible insurance available in my area#so that it will cover my prescriptions and medical procedures and not fight me about covering them#and what's the damn point if they won't cover this#but also if I am going to end up paying 800 dollars for a dang MRI#I'm going to find a local place with an open MRI instead of the full tube#if I am going to pay that much damn money I am going to make sure it's as least worst as possible
11 notes
·
View notes
Text
Character Spotlight: Katherine Pulaski
By Ames

We may have only had Dr. Pulaski for one season of The Next Generation, but that didn’t stop her from leaving an impression. Your hosts here at A Star to Steer Her By are big fans of her character and also of Diana Muldaur’s performance of the cantankerous and brilliant doctor who graced the Enterprise-D’s sickbay during Dr. Crusher’s time away from the ship (more on her next week!). She even made a couple of our top characters lists from TNG!
There’s a lot of negative feelings about the McCoy knockoff in the Star Trek community, and we’ll cover some of those below, but overall we have to give credit to the good doctor for how much she grew in only the twenty episodes we had her. By the end of season two, she was viewing Data as a peer, saving lives left and right, and fighting for the rights of other species. There’s no telling how much better she’d get if she stuck around. So raise a cup of Klingon tea to the best CMO of the Enterprise (I said it!) with our highlights below and elaborated upon in this week’s podcast episode (timestamp for this one is 58:29). Fight us, haters.
[Images © CBS/Paramount]
Best moments

Crammed full of crumpets
We’ve made a running gag on the podcast about how Professor Moriarty stuffed the doctor full of crumpets in “Elementary, Dear Data” but there’s more to this episode than crude jokes and blue humor. Pulaski ran with the Holmesian scenario in the holodeck, proved to be stalwart and brave in a hostage situation, and totally rocked the period attire!

At least someone still remembers quarantine procedures
While the whole thing did backfire on her, Pulaski’s actions in “Unnatural Selection” kept the rest of the crew safe. She was willing to risk her own health on her hunch that the augmented children weren’t carrying any pathogens, but let’s give her credit for taking the child and Data out in a shuttle so that, if (and when) things went wrong, things were contained.

Knives and bearskins!
When the biobeds are on the fritz due to the contagion in “Contagion” and her staff is whining that the bone knitter isn’t working, Pulaski pulls some tried and true methods out of her back pocket – make a splint! It may be archaic medical technology, but it’ll do in a pinch and having that kind of medical knowledge saves the day (or saves someone’s leg at least).

Generous doses of PCS
I just really love the sweet little moment during “The Icarus Factor” when Dr. Pulaski is tending to some crewmember suffering from the flu and says part of her prescription is PCS – Pulaski’s Chicken Soup. It shows how much she cares about her patients and gives the audience that warm feeling of having someone care for you when you’re home sick from school.

Jettison the emotional baggage you’re still carrying around
Also I have to give my girl some props later in “The Icarus Factor” when she’s flirting with Kyle Riker right in front of Will. We find it a nice character inclusion that she and Kyle used to be down to clown, and even that she would have married him in a heartbeat, and she tells his son off in the most “oh no she didn’t!” way and then proceeds to drop like fifty mics all over Ten Forward.

Take your Prime Directive and shove it up your hatch!
We on this podcast (who am I kidding; it’s mostly Chris) have a certain skepticism about the Prime Directive sometimes, and it’s usually the CMOs of their respective shows that get to question it most blatantly. Pulaski sure does in “Pen Pals” because screw the prime directive in this case! When a whole planet is on the line, Pulaski is the conscience that we all need!

Forget me, forget me not
This is one that could have gone in either the Top Moments or the Worst Moments list because, face it, mind wipes are horrifying. But I’m gonna give Pulaski the win for erasing Sarjenka’s memories in “Pen Pals” because it’s impressive as hell. And she uses it to kinda-sorta stay within the Prime Directive that we just shat on. Plus she let Sarjenka keep the singing rock!

You’re still the Captain. Invincible.
I’m still not certain what Chris was getting at about Pulaski’s letting Picard avoid the heart treatment he’s been neglecting out of sheer vanity in “Samaritan Snare,” but I’ll do you one better: she winds up fixing his stupid ticker for him in the end anyway! And is the grouchy little man thankful afterwards? Not even a little bit! Pulaski gets no respect, I tells ya!

Quote me a little of that poetry
While you’ll see in just a moment that Pulaski’s views on Klingons were initially unkind, by “Up the Long Ladder,” she’d bonded with Worf enough that she was willing to engage in some Klingon rituals. She goes out of her way to concoct an antidote so she can take part in a poisonous tea ceremony with him, which is above and beyond (and also fuels some shipping), and she also keeps Worf’s measles a secret!

Bust him up, Data!
In “Peak Performance,” it’s Pulaski who sets up the Strategema match between Data and Sirna Kolrami, and she ends up feeling really bad for goading him when he loses to that smug Zakdorn prick. So it’s that much sweeter that she’s there cheering him on when Data thinks outside the box causes the stalemate, telling him that in that way, he did indeed beat him!

Feelings of warmth and friendship
What a shame that the last episode we got with this amazing character was one of the most infamously bad. But none of that is on Pulaski because she’s actually on full display in “Shades of Grey,” partly because she’s one of few characters in the non-clipshow scenes. But she (and Troi, as I brought up last week) pulled out all the stops to save Riker’s brain from certain doom.

Pull your head out of your ass!
Okay, this last one’s not canon, but I just couldn’t help including this plug to go read Caitlin’s fanfic “The Pulaski Maneuver”!!! Or listen to it on the podcast back when we wrapped TNG with our episode “Tales from the Holodeck.” Pulaski finally telling Geordi everything that he’s deserved to hear might be my favorite moment, and it’s so in her character that I say it counts!
—
Worst moments

The cold hand of technology
Most of Pulaski’s negative personality traits are going to circle around her treatment of Data as a piece of equipment and not an individual. In her introduction episode, “The Child,” one of her early interactions with Data is to tell him he’s not wanted in the delivery room because he lacks the human touch. Lucky for us, Troi sticks up for him and he gets to watch her whelp an alien baby.

One is my name; the other is not
Shortly afterwards, still in “The Child,” we get one of the fandom’s most hated moments from Pulaski when she not only mispronounces Data’s name, but doesn’t seem to understand that doing so is rude and problematic, instead deciding to put the onus on him for being capable of offense. It’s a tough moment for fans to accept, and if that were the level of bigotry her character stayed at, I’d understand why so many Trekkies dislike the character.

I’m not accustomed to working with non-living devices
More growing pains come from Pulaski in “Where Silence Has Lease,” in which she refers to Data as “it” and Picard has to gently correct her. We’re two episodes into the season at this point, and Pulaski is still finding it difficult to accept the personhood of this fan-favorite character, something viewers pretty much got on board with in episode one. At least she apologized.

The mystery of the lack of any mystery
Here we are, three episodes in when we reach “Elementary, Dear Data” and we see more of Pulaski judging Data for being incapable of thinking creatively when he solves Holmesian riddles. We may have blamed Geordi for accidentally creating Moriarty when we covered his character spotlight, but it was definitely Pulaski who goaded them on in the first place.

Medical research is sometimes a risky business
While we may have praised her above for not putting everyone else at risk when she released the augmented child from his wrapper in “Unnatural Selection,” Pulaski was still dead wrong about the experiment being at all safe. She still got contaminated by the fast-aging disease and was resigned to her fate until Picard and O’Brien were able to transport her back. Speaking of which…

I’m a doctor, not an original character
One rather understandable complaint we can see in the Pulaski character is that she’s just Dr. McCoy in a skirt. Which may not be a bad thing, per se, but when we see her racism against the outsider character, her Bones-like irascibility, and even her specific fear of transporters in “Unnatural Selection,” we start to wonder if the writers couldn’t have been a little more original.

I’m just glad that humans have progressed beyond the need for barbaric display
We get a couple glimpses that Pulaski is a little repulsed by Klingon culture throughout the show. First, in “A Matter of Honor,” she’s grossed out by Klingon cuisine and calls Klingons barbaric, and not in the way Klingons would probably like. And she also gets a little smug after watching Worf’s Age of Ascension ceremony in “The Icarus Factor,” which she seemed pretty judgey about (but hey, at least she went!).

Quit cloning around!
We gave Riker some guff for this as well in his character spotlight, and there’s enough guff to go around to give to Pulaski as well for their actions in “Up the Long Ladder.” Sure, the clones were made of them without their consent, but to take matters into their own hands and murder these people without discussion is not the Starfleet way.

Never to be heard from again…
Obviously the worst character moment for us is Pulaski leaving the show after just one season. Notice how most of the bad moments come from earlier and the good moments are mostly from the latter half of the season. That shows how much the character was getting better, even in the rough first couple seasons of the show (you’ve heard our coverage of Chaos on the Bridge, right?). And while many celebrate the return of Crusher, we still have to wonder what the show would be like with more Dr. Pulaski.
—
And just like that, she’s gone and so is this blogpost. Keep following along because we’ve got another doctor of the Enterprise-D to discuss next week, and it’s not Selar! We also hope you’re making the schlep through Enterprise with us as we cover the whole thing over on SoundCloud or your podcast platform of choice. Wave your medical tricorders over our Facebook and Twitter pages, and get the pronunciation right: It’s Data, not Data!
#star trek#star trek podcast#podcast#pulaski#the next generation#elementary dear data#unnatural selection#contagion#the icarus factor#pen pals#samaritan snare#up the long ladder#peak performance#shades of grey#the child#where silence has lease#a matter of honor#the pulaski maneuver#fanfic#diana muldaur
43 notes
·
View notes
Text
Hidden Marks [3: What are you Hiding?]
Summary: Wrapping his own arms around her shoulders, Namjoon pulled her in, resting his head on the crown of her head, his heart beating steadily, which Sera heard and smiled to herself. Even with his odd lengthy limbs, they fit together perfectly, "Sera, I'm falling in love with you, that I want to convince you not to go, but I trust you. I just want you to be happy, to never cry over us again. I can't promise you that if you choose to stay with us, everything will be rainbows and sunshine, but I promise you that we won't give up on you, on this relationship. We're not perfect like everyone thinks we are, we're not the perfect bunch of soulmates, we have problems as a group and individuals, secrets that we all keep, burdens that we try to carry on our own. Though we all have each other, to fall back on when things get brought, and that includes you now. We're soulmates, so if anything happens, don't be scared to tell us.
(Poly BTS/OT7 x Reader/OC)
College Au / Soulmate Au
Disclaimer: Bts isn't my or any real life people (obviously.) Any other characters are my though. This is my story so do not republish this anywhere or I will report.
There maybe some triggers, but I will address them within the chapters.
Sources: Wattpad
Word count: 2281
Monday night I emailed my professors to let them know I wouldn't attend classes for Tuesday, and exhaustion finally caught up to me that night as I went to sleep, with several needles in my arm, an oxygen mask around my mouth, with the beeping of the monitor. I woke up like that Tuesday afternoon.
Groggily, I removed the annoying mask from my face and pushed my hair away from my face as I glared weakly at the open curtain, as the sunlight was the one to interrupt me from my sleep. The temptation to just knock down the beeping monitor next to me was strong, but I just shifted in the bed, my sore muscles tensed slightly when I shifted to my side a bit. A groan escaped my mouth, wanting to fall back to sleep, but I couldn't.
Reaching for my phone in my bedside table, I winced slightly at the dozens of missed calls and text I received, mainly from Lilia, Kimie and Baekhyun.
Feeling slightly guilty, but not knowing what to say, I sent them a mass message that said I was fine, before putting my phone on mute, so I didn't have to deal with their endless questions of where I was at.
However, I sent Baekhyun a private text:
Can you come to the hospital whenever you have time? Please don't tell anyone I'm here.
I felt like absolute garbage, but at least the burning from my marks ceased, and the headache was gone.
Soon the same nurse from last night came, with her usual bright smile, "Miss. Han, how was your sleep?"
"My whole body is sore," My voice was scratchy, as I gratefully took the water that the nurse offered, "When can I leave?"
The nurse checked my vitals and told me everything seemed to be normal and would inform the doctor before giving me an estimate of when I'll be discharged. She left me alone to my own thoughts, as I settled back into my bed, my eyes heavy, but refusing to sleep. While I may be physically better, it didn't mean I was mentally better. It didn't stop that aching feeling I felt in my chest, the loneliness and emptiness I felt.
After a bit the nurse came back with the doctor, who went over my vitals and charts again, before asking me how I was feeling and replied that I was much better.
"There's this procedure in America," The doctor suddenly spoke, as she was typing away from the computer, looking away from me, "That gets rid of the soulmate mark, and terminates the soulmate bond. It hasn't been approved in Korea, but in America, it has an 80% success rate."
I didn't reply, but I unconsciously shifted the covers to hide the marks, which I knew would be black instead of gray now, as the therapy worked it's magic to repair the bond and in the end my soul. However, there was only so much it could fix, especially when I've been doing the same treatment for nearly four years.
"I assumed you already called someone to pick you up, I'll have your paper works prepared. You can leave in about two hours."
*****
"What is going to be your excuse to Kimie and Lilia? They've been worried about you all day," Baekhyun asked, breaking the silence in his car. The radio was on low, nothing more than a buzz in the background.
Shifting my eyes to glance slightly at the pick haired guy, I turned my body farther away from him, "Just tell them I went a male strip club and I had some fun," I snorted out, not wanting to think about how to deal with my two friends. That was also the reason why we were currently heading towards Baekhyun's apartment, so I can rest more before I return to my dorms and most likely to an awaiting Kimie with a Lilia by her side.
"You're getting worst Sera," he spoke once more, this time his voice more serious causing me to stiffen up a little, "The treatments been getting less and less effective. Give or take a couple of months before those don't even work. Then what?"
"Then I head to America."
"For what?"
"To get rid of the soulmate bond, and probably go to medical school there."
*****
I was mentally and physically exhausted as I walked up the stairs. Nearly falling several times, and I just wished some unknown being would just come, sweep me off my feet and to my bed. Then I wouldn't have to face Lilia and Kimie, after facing Baekhyun.
All we did for a straight hour was scream at each other, yell, fight, and insult one another.
After my announcement of going to America and for what reason, Baekhyun exploded, calling my decision stupid. I of course argued back and tried to defend my decision. We hurled insults after insults at each other, both angry for completely different reasons, and I was the first to break. After our hour of fighting, I spent an hour crying with Baekhyun trying to comfort me, both of us apologizing, before I decided it was time to go back to my dorm.
I wished I accepted the offer to stay at his place for the night, as I pushed my key into the door and pushed it open.
Along with Kimie and Lilia, were two other people that I just wasn't mentally prepared to deal with. Even so, my heart skipped a beat when I saw them.
Sitting on one of the couches in the living room was some would say, the perfect man to exist. With his broad shoulders and slim waist, every girls dream body for their boyfriend. Well-defined facial features with slight cat-like eyes, which were a rich brown color, with a pair of plump lips. His dark black hair stood out against her perfect skin, and he really was a worldwide handsome guy.
Sitting next to him was another breathtakingly beautiful person, large brown doe eyes could make any girl swoon, especially his double eyelids that many people in Korea dreamed to have. He was still well-defined but had almost like a child aspect to him, and whenever he smiled he looked like a bunny. He was Mr. Heartthrob.
"Where the hell have you been!" It was Lilia to speak of more yell once I closed the door, "Do you know how worried we all were! And all you offered was a lame-ass, 'I'm fine, don't worry about me."
I didn't respond, didn't even think as I just stood there, blankly staring back at Lilia who looked furious.
"You didn't even come back last night and came back late today! What in the hell is going on with you Sera?"
What is going on with me?
Is there something wrong with me?
The answer is most certainly.
"I've been trying to be a supportive friend, but it's getting hard when all you do is push us all away! Did I do something wrong? I'm your fucking friend, just talk to me!"
I watched as Jin stood up, and walked behind Lilia and placed comforting hands on her shoulders to try to calm her down. It caused an immense pain within me and it took everything in me to not double over in pain.
Of course, it didn't calm Lilia down, as she only pushed Jin's hands away, and took a step closer to me.
"Do you even consider me a friend? All you ever talk to now is Baekhyun, is he your soulmate? Just tell me something, anything because I have no idea what's going on with you anymore."
There's the odd word again; soulmate. The very word I used to swoon over in middle school, to dream about finding my own. Now it's the bane of my existence.
"Let alone how mean you've been acting to my boyfriends! They've done nothing but try to befriend you, but all you do is push them away!"
Because it hurts to be around them.
"And you're moving universities and you didn't even tell me. Did you even plan on telling me?"
Without thinking, I opened up the white paper bag I was holding the whole time, and pulled out a clear orange bottle, with paper around it. The prescription my doctor gave me.
Overwhelming anger came over me, as I suddenly raised my hands and threw it harshly against the wooden floor, causing the lid to fly open. Several small white pills scattered across the floor, as the loud sound caused the room to go silence. The only thing that can be heard was my heavy breathing.
Bringing up a hand to run over my temples, to try to comfort myself, I didn't dare to look at Lilia, "I'm tired Lilia," I spoke quietly. My voice was raspy as I tugged at the collar of my shirt. It was becoming hard to breathe.
Kimie finally stood up from the couch, and with a concerned expression, she walked towards me. Instinctively I brought my left arm to my chest, and backed away, and lowered my gaze
She seemed taken aback from this, as she stopped in her track and frowned, "Sera, we were just concerned about you, ignore Lilia."
"I just..." I stuttered as my voice shook and I hated it, "I'm just tired. I'll pick up my stuff and head to Baekhyun's. Sorry for bothering you."
When I made an attempt to move around Kimie and to escape my room, Lilia roughly grabbed my left arm, stopping me. However, her stopping me wasn't the problem, it was the fact that her hands were on my marks. Without even realizing it, I began to tremble, as I tried to yank my arm out of her grasp, but she had an iron grip on it.
"You're always covering your mark, what the hell do you have to hide? Do you even see us as your friends?" I watched as her other hand reached up to my left arm, towards the ends of the bandages, with intent to take it off.
Panic overcame me, as with my free hand I roughly pushed her away, causing her to bump into Jungkook. The sight of Lilia in his arms only caused everything to be worst. Backing away, I bumped into Kimie who was yelling at Lilia.
I couldn't think straight, my mind was everywhere, and I was having a panic attack. With my breathing heavy, I wrapped my arms around myself, and closed my eyes. The feeling of Kimie's arms around me, trying to comfort me, only made the pain and anxiety worst, my left arm burning so painfully as I chocked out a sob.
"Please-" I wheezed out, unable to say anything else as I crouched down, trying to wrap myself into a ball. All I wanted to do was disappear and be alone, "It hurts," groaning out, I hissed out in pain, almost tempting to tear away at my own bandages. But that would only ruin everything, "I'm sorry."
"Sera," Kimie spoke worriedly, crouching in front of me, but I refused to look at her, "you're having a panic attack, you need to breathe slower.
It was easier said than done, as it felt like my heart was going to leap out of my chest. Especially when I heard the two men in the room whispering comforting words to Lilia. There was unbearable pain, something that I haven't felt before as I forced my eyes open and met Jungkook's concerned brown eyes staring back at me.
Breaking away the eye contact, I forced a reminder that he was only concerned for as a friend. Nothing more.
I don't know how long we all stayed like that, Lilia staring at me with uncertainty written on her face, Kimie standing slightly in front of me as if protecting me from Lilia. Jin kept his hands on his girlfriend, to calm her down as Jungkook stared at me with an unreadable expression.
Swallowing hard, with shaky legs, I stood up, and pushed Kimie to the side slightly, just wanting to go to my room.
No one made a move, but their eyes were on me as I moved past them, with every intent to just disappear until I was forced to go back to class.
However, when I passed Jungkook, I don't know what force overcame him, but suddenly he raised his arm to grip my left wrist. So dangerously close to my marks.
When I snapped my head to look at him, he had a concerned expression, and he opened his mouth as if to speak, but just closed it.
There was a familiar spark where our skin touched, and any other time it would make me feel much lighter, the mark to hurt just slightly less. This was different though, as my heart constricted, the mark on my left arm flaring up once more.
Without thinking, I harshly yanked my arm out of his grip, "Just leave me the fuck alone!" I all but screamed out, not caring when he flinched away from me, "You and all your stupid soulmates, just leave me the fuck alone!"
I didn't wait for a reply, as I stormed into my room, making a note to lock it behind me.
Throwing myself onto my bed, I was breathing heavy, and waited for the tears to come as I stared at the empty ceiling. It never came though, instead of overwhelming emotions, all that come was numbing and emotionless feeling. I knew exactly why I was feeling this, a dry laugh leaving my dry lips.
I basically just rejected my soulmates.
[2281]
#bts#bts imagine#bangtan boys#poly bts ot7#poly ot7#Poly BTS#fanfic#bts fanfction#jimin#park jimin#kim taehyung#taehyung#v#bts v#rm#kim namjoon#namjoon#jeon jungkook#jungkook#kim seokjin#seokjin#min yoongi#yoongie#jung hoseok#hoseok#soulmates#bts soumate au#soulmate au#angst#bts angst
9 notes
·
View notes
Text
I have cancer ...PLEASE DONATE !!😫😪😔😞
HOME
This is my main blog, I mostly do Tarot and other divination services on here, and most often it is for FREE. Which, this is NOT fair to me, but none of ya 'll know about my struggle.. bug it is real hear me out, yo.
ABOUT ME
I am nearly 30 years old now and I was actually first off diagnosed with Ovarian cysts at the age as young as 14 yrs old, yes, I was 16 by the time it went untreated and had spread all through my ovaries and to all the fallopian tubes and my uterus... then untreated still another couple years (because of poor health care in my smaller rural communities including my hometown) then at 19 my whole entire uterine lining was xomething of a mess, the doctors said basically all there woukd have been to prevent it from dpreading the cancer elsewhere would have been a full out take of my sexual organs , i believe the term is a hysterectomy....but on my paperwork i see here that it says that I was to undergo something else... + + The removal of an ovary together with the Fallopian tube is called salpingo-oophorectomy or unilateral salpingo-oophorectomy (USO). When both ovaries and both Fallopian tubes are removed.
But that did not happdn due to complications. So now, its spread to my other organs as youd guess, spleen, liver, kidneys, etc...it is a shitttSHOW I knowe.
This is why I would appreciate it if some one, any one would stand up for me ..just have a say in whether I eat today or not, or whether I stay in this residence without having to move this winter, I mean, Winter, its settling in.,,
I do not always feel totally blessed to be me; But ai I cannot complain when the bills is caught up and I gots good food at home(and the fight food, I am on a special expensive diet)
Cancer is expensive…AF! If you have cancer, this is no news to you. But until cancer happened to me, I had no idea how expensive it truly was. I think it’s safe to say that that seeing how much it will cost to undergo treatment is almost as frightening as getting the actual cancer diagnosis. My diagnosis has definitely opened my eyes to the shocking reality of the financial burden that cancer causes for an individual and their family. The astronomical expenses that accrue from treatments, tests, surgeries, scans, integrative therapies, etc are outrageous! While there are both public and private health insurance that defray medical and drug costs, huge out-of-pocket costs can be devastating to patients and force major changes in their lives. I’ve had to make several changes and my life has been affected indefinitely due to the financial burden that cancer has caused. The financial stress it causes for people during treatment until remission alone is hard, but imagine living with cancer where the treatments, doctor visits, tests and lifestyle adjustments are ever enduring, like when you have metastatic cancer. It’s life altering… to say the least.
HOW MUCH DOES CANCER TREATMENT ACTUALLY COST?
This is an impossible question to answer. The cost of treatment obviously varies from individual to individual based on their diagnosis, the type of treatment they will require and the longevity of the treatment. However, the “typical” cost of breast cancer looks a little something like this according to recent studies.
“For patients covered by health insurance, out-of-pocket costs for breast cancer treatment typically consist of doctor visit, lab and prescription drug copays as well as coinsurance of 10%-50% for surgery and other procedures, which can easily reach the yearly out-of-pocket maximum. Breast cancer treatment typically is covered by health insurance, although some plans might not cover individual drugs or treatments. For patients not covered by health insurance, breast cancer treatment typically costs $15,000-$50,000 or more for a mastectomy or $17,000 to $35,000 or more for a lumpectomy followed by radiation.”
New cancer drugs are being approved at a fast pace. Numerous are approved each year and new drugs are constantly in trial and in the pipeline to be FDA approved. In the past, these drugs might cost around $10,000 for a year’s treatment. But newer studies have found that newly-approved cancer drugs carry price tags between $120,000 and $170,000! One of the drugs I take as part of my daily cocktail, is a newly FDA approved drug called Ibrance… for heavily pretreated ER+ metastatic patients. It has worked wonders for me but a month supply of this drug is over $12,000. I am blessed to have good coverage, but not all people are as fortunate.
“Depending on the individual case and the type and number of treatments needed, the total cost of breast cancer treatment, on average, can reach $100,000 — or, in advanced cases, $300,000 or more. This includes the cost of the chemotherapy drugs, additional drugs to help manage side effects, administration of the drugs and medical care for chemotherapy-related complications.”
And again, if you are anything like myself and are living with a metastatic diagnosis, treatments and care is endless with no foreseeable light at the end of the tunnel.
😔😫😫🎗🎗🎗🎗🎗🎗🎗🎗🎗🎗🎗🎗🎗🎗🎗🎗🎗🎗🎗😔😔😫
WHY IS IT SO EXPENSIVE???
The never ending list of cancer expenses looks a little something like this:
🎗Frequent doctor visits with surgeon, radiologist, oncologist. I personally see my oncologist once every 3 weeks and check in with my surgeon every couple of months.
🎗Lab Tests. This includes blood tests, urine tests and more. I get my labs done every few weeks when I see my oncologist to check my levels and tumor markers.
🎗Clinic visits for treatments. When I was on IV treatment I would be in the treatment center every few weeks. Currently I take an oral chemo and only have to be in the treatment clinic once every few months for my Lupron injection. But many people are in the treatment clinic, daily or weekly to get their infusions and injections.
🎗Procedures for diagnosis or treatment. Such procedures can include biopsies, room charges, equipment.. I’ve had a few biopsies and had to get lung taps done frequently when I had lung mets.
🎗Imaging Tests. These tests include X-rays, CT scans, MRIs and PET scans which may mean separate bills for radiologist fees, equipment and any medicines used for the test. These tests are extremely costly too…yikes! I get PET/CT scans every 3 months, consistently for the past 6 years now.
🎗Radiation Treatment (implants, external radiation, or both) I have never had radiology but as we know, it’s a very common treatment for most cancers.
Drug🎗 Costs. (inpatient, outpatient, prescription, non-prescription and procedure-related) The cost of chemotherapy drugs is crazy!
🎗In-Home Nurse Care (if you need it, and I do actually, yes) and its freaking insane how much these so called "nurses aids -assistants" want an hour!!
Hospital 🎗Stays. This can encompass many types of costs such as drugs, tests and procedures as well as nursing care, doctor visits and consults with specialists. I have been admitted twice, each time for a week stay for cancer related issues.
🎗Surgery. Costs can accrue from surgeon, anesthesiologist, pathologist, operating room fees, equipment, medicines… I have had 3 lumpectomies and 2 other surgical procedures related to my cancer diagnosis.
🎗Fertility. If you are blindsided and diagnosed in your 20’s or 30’s with a cancer diagnosis and want to have a family, freezing your eggs is an option, but a costly one. You will be required to pay for tests, and medications leading up to the surgical procedure to remove your eggs. I paid about $10K out of pocket to cover the cost of freezing my eggs.
While these are examples of the clinical costs associated with cancer, there are other adjustments you may want to make that will also prove to be costly. I personally changed my diet and started to eat all organic foods and sought integrative therapies to add to my clinical regime. You can read more about the therapies I have incorporated here. All of these expenses add up and certainly are a financial strain.
🎗🌟🌟🌟🌟🌟And of course we need to pay... Rent, heat/hydro, car/transportation/ambulance bills , always bills bills bills billsssss.....and wifi/internet/television/mobile phone znd/or tablet or computer and gaming systems... camera.....im z girl so clothes..makeup,(I'm thrifty ricky tho) and always last, maybe maybe get sweets healthwise branded cookies or some type of peanuts(unsalted).
I never get go, go nowhere, do anything, get a coffee from a coffee shop, i can't afford to do just about anything a normal individual such as yourself yourself would do, i just cannot do it its not in my budget ... I currently own ONE lipgloss, and one broken eye liner , that is my makeup beauty kit, who the heck wants to even go out or take pictures thenn? Ugh....
Www.paypal.me/believeitxxnot is the link to the Cancer Fundraiser🎗the email for it is [email protected]
Anyways, do not feel bad for me. I am here to service YOU for ever I know this . TY so much ily guys , please please if you will not donate to my awfully painfully really urgent cause then PLEASE SHARE POST ..... BOOOST POOOOST !! PLZ !! XOXO
I need the supporters !! Yo yo ! DOOOONAAAATEEEEE!!
A n y t h i n g h e l p s m e r i g h t n o w , p l e a s e ! ?
#support#cancer#comment#culture#cars#crafts#celebs#best content ideas#cameras#cartoon#chair#charities#charity#chemistry#christmas#collage#community#creepy#currently reading#special collections#tarot community#witch community#canada#chat#cake#dream catcher#cute#cool#autumn#october horoscope
8 notes
·
View notes
Text
Physician-Assisted Suicide: Humane or Heinous?
Dr. Roger Kligler is a retired internist who found himself in the middle of this debate. At 50 years old he was diagnosed with prostate cancer that was believed to be curable. After rounds of cancer treatment, Dr. Kligler was put into remission. However, after 5 years, Dr. Kligler went back to his oncologist and was informed that not only was his cancer back, but it was terminal. After attending a medical lecture regarding “medical aid in dying” he became an advocate for the cause through Compassion & Choices, the foundation partially responsible for the passing of the End of Life Options Act in Massachusetts (I’m a doctor with end-stage cancer. I support medical aid in dying). Dr. Kligler’s case is a prime example that even the most unexpecting can be snarled up in cancer’s poisonous grasp. As an aspiring doctor, I want Dr. Kligler, and others like him, to know that they are not alone in this battle. Physician-Assisted Suicide is a tool in the very profound toolbox of a doctor that allows them to give their patient a final sense of peace. PAS postulates the end of suffering to terminally ill patients that would otherwise continue on the heinous, drawn out path to death.
Now it is time to get to the root of the topic. Is Physician-Assisted Suicide human or heinous? This phrase can be quite startling at first glance. There is undeniably a hefty negative connation associated with suicide that causes people to initially balk at the term. However, we must strive to remain neutral and focus on the real meaning behind the term. In the article, Physician-Assisted Suicide: Two Moral Arguments, the author does a beautiful job of really owning in on the different meanings of this term and how they apply to each individual medical case. She splits the term in “drug-providing” and “drug-injecting” (Thomson 506). Drug-providing is the process of a doctor knowingly writing a prescription that contains a dose of a drug that will be lethal to the patient. Drug-injecting is when the doctor is actually the one who administers a dose of a drug, usually morphine, that will end their life. This poses the question: are people really sick enough that a doctor feels it is within their medical rights to end their life?
Without experiencing a hardship personally, it is hard to imagine exactly what is feels like and to come up with the best possible solution to fix it. Agrawal and Emanuel write:
For many people, death in modern advanced societies is inherently undignified. Terminally ill patients are connected to tubes and machines; they experience pain, shortness of breath, and other excruciating symptoms; they are unable to get out of bed, feed themselves, and even go to the bathroom alone; they are cared for in impersonal institutions (Death and Dignity: dogma disputed 2026).
The picture painted by these men is not one that anyone would like to volunteer to star in. Unfortunately, after visualizing it, many people’s minds will immediately jump to a family member that has experienced this. My grandmother was diagnosed with a terminal cancer, meaning she would eventually die because of this cancer and there was nothing in the world that could stop it. This is a harsh reality that many individuals face. According to the National Cancer Institute, “approximately 38.4% of men and women will be diagnosed with cancer at some point during their lifetimes (based on 2013–2015 data)” (National Cancer Institute). In a standard classroom, that’s 10 out of 30 people. While we wish we could hide under the covers, the cruel reality is that statistically cancer will be a part of everyone’s lives at some point. So, what do you say to someone that’s diagnosed with terminal cancer? “Fight, you’ll beat it?” Unlikely. “Don’t worry, it won’t be that bad?” Also unlikely. “Everything will be okay.” Depends on what you think “okay” exactly is. “Fatigue, pain, appetite changes and problems breathing” are listed as physical symptoms in the last 2 to 3 months of life (American Cancer Society). That simple list doesn’t sound like the worst thing in the world. Ok, I get short of breath every now and then, and sure I’ll be tired but I can nap all day. What they don’t mention is that often the pain cannot be controlled with medication, that “appetite changes” is vomiting constantly and not being able to enjoy any food. So again, I ask, what do you say to someone suffering like this? If it were me, I know I would not want to go on this way. I would exercise my right to ask a doctor to show humanity and end my life through Physician-Assisted Suicide.
Ryan Anderson, a writer with a Ph.D. in American Principles and Public Policy, states that legalizing Physician-Assisted Suicide would:
1. Endanger the weak and vulnerable,
2. Corrupt the practice of medicine and the doctor–patient relationship,
3. Compromise the family and intergenerational commitments, and
4. Betray human dignity and equality before the law. (Four Problems with Physician-Assisted Suicide).
The emotional struggle that doctors feel when there is nothing else they can legally do for a patient that is still suffering immensely is not easy. This option would strengthen the relationship between them as they are finally able to provide them with peace, not the contrary like he is suggesting. While Anderson’s other concerns have more grounding, because of the sensitivity of the matter I find it more than hard to imagine that these circumstances would come true. The amount of litigation and procedures that would be required for PAS to take place would trump his rising concerns. Concluding that PAS is the best option for a patient is no hasty decision. It is in a doctor’s nature to explore every possible route for their patient. From clinical trials containing experimental drugs to alternative medicine, a doctor will look at every possible outlet before just settling that PAS is the best option. The weak and vulnerable would not be endangered because of all the hoops doctors would have to jump through to even suggest PAS. In fact, according to legislation multiple doctors must confirm that patient’s disease is terminal before the topic of PAS can be present (Frequently Asked Questions).
In conclusion, I ask you to ponder what it means to be in unbearable pain, and really come to terms with exactly what PAS is. I pray that you never find yourself in a circumstance where you have to think about it again, but if you do, I hope that you will be better equipped to understand what it means.
Works Cited
Agrawal, Manish, and Emanuel, Ezekiel J. “Death and dignity: dogma disputed” The Lancet, vol. 3, Citizens News Wire, 28 December 2002, www.citizensnewswire.org/files/Ezekiel20021221_Death_and_Dignity.pdf
Anderson, Ryan. “Four Problems with Physician-Assisted Suicide” Health Care Reform, The Heritage Foundation, 30 March 2015, www.heritage.org/health-care-reform/report/four-problems-physician-assisted-suicide
“Cancer Statistics.” National Cancer Institute, www.cancer.gov/about-cancer/understanding/statistics.
“FAQs - Physician-Hastened Death.” Death With Dignity, www.deathwithdignity.org/faqs/.
Kligler, Roger. “I'm a Doctor with End-Stage Cancer. I Support Medical Aid in Dying.” STAT, STAT, 6 Feb. 2018, www.statnews.com/2018/01/31/medical-aid-in-dying-doctor/.
“Physical Symptoms in the Last 2 to 3 Months of Life.” American Cancer Society, www.cancer.org/treatment/end-of-life-care/nearing-the-end-of-life/physical-symptoms.html.
Thomson, Judith Jarvis. “Physician-Assisted Suicide: Two Moral Arguments.” Ethics, vol. 109, no. 3, Apr. 1999, pp. 497-518. JSTOR, www.jstor.org/stable/10.1086/233919?origin=JSTOR-pdf&seq=1#page_scan_tab_contents
1 note
·
View note
Text
Two Years Without Health Insurance (and What I’m Doing Now)
Two years ago, I was unsatisfied with my options for health insurance. The premiums were rising even as the quality dropped in the form of an ever-increasing deductible. I am guessing that you might feel the same way these days – most of us Americans are in the same boat.
I felt like I was being squeezed from both ends and it was starting to piss me off. So I decided to take some action, by doing the math for myself using a spreadsheet. I needed to answer the question, “Is this insurance really as bad a deal as I think it is?”
Sure enough, the risks and rewards of the coverage did not justify the premiums, so I decided to try an experiment and simply drop out of the market and insure myself. In other words, just rolling the dice and going through life with no form of health insurance at all.
Doubling down on the bikes, barbells and salads, I did my best to eliminate any risk factors that are in my control, while accepting that there are still much less likely but more random factors that are not.

Figure 1 – DIY Health Care
Almost two years and $10,000 in premium savings later, I have found the experiment to be a success: I have slept well and not worried about the fact that I could be on the hook for a big bill if I did ever need major care. And as luck would have it, I also enjoyed the same good health as always over this time period – probably the best in my life so far because the extra healthy living has been working its magic.
But.
This situation has not been quite ideal, because my life is not a very useful model for everyone to follow. Most people don’t have the luck of perfect health, many have a larger family than I do, and very few people are in a financial position to self-insure for all possible medical bills.
Also, I found myself wishing I had a doctor that actually knew me, who I could call or visit on short notice if I ever did need help.
Finally, I wanted to switch back to having some form of insurance so that I could learn about it and write about it as time goes on. But was I really willing to be part of that unsatisfying and broken insurance model?
Then something magical happened: I learned about the new and vastly improved world of Direct Primary Care physicians.
What is DPC?
DPC is a fairly new trend in the US, but it is also a return to a very old tradition: a direct relationship between you and your doctor, with no insurance company in the way.
As a customer, you pay for a monthly subscription (somewhere around $100), and in exchange you get unlimited access to super elite, personalized medicine for the vast majority of your medical needs. Diagnoses, prescriptions, skin conditions, stitches, even fixing a broken bone if you don’t need surgery. All covered, with no co-pay and in an environment that feels to me like Presidential-level health care, in striking contrast to some of my past experiences where I felt like an anonymous numbered ticket in a sloshing sea of bureaucratic institutional medicine.
Oh, and direct email, phone and text message contact with your doctor, prescriptions over phone or video call, and in some cases even house calls depending on the practice and the situation.
Through some sort of magic, the Direct Primary Care model offers much better medical care and much lower prices, at the same time.
How could it be? It’s because of the incentives.
Figure 2: The Insurance Model for Health Care
In our famously broken US healthcare model, an insurance company is wedged in between you and your doctors, and it has different objectives than you do.
You just want the best overall health for yourself, and when the shit does hit the fan and you need medical care, you want it to be quick, effective, and at minimum cost. And you don’t want to be hounded with years of stressful stray bills after an expensive medical procedure.
Your Doctor wants to help as many people as possible and make a good living, without having to wade through a sea of paperwork or stress or lawsuits.
Your Insurance company wants to make as much profit as possible, which means maximizing the amount they collect from you, and minimizing the amount they pay to your doctor. In theory, they benefit from helping you to stay healthy. But they have also developed elaborate contracts (putting in as many loopholes as possible to allow them to drop your coverage or deny claims), become masters of delaying payments, limiting which procedures and tests they will authorize doctors to do, and just generally throwing the biggest monkey wrench into the system that they can.
Over the decades, there has been a complex battle of lawmaking, lobbying, compromise and complexity to try to regulate away some of these problems. Sometimes the new laws help, sometimes they don’t, but the end result will never be optimal simply because there are a lot of people involved, and big crowds of humans make for slow and shitty decision making.
The Direct Primary Care Model

Figure 3: The Direct Primary Care Model
With DPC, it’s just you and your doctor. You both have the same incentives, but now the model works much better because there is no chaotic and expensive force in the middle to mess things up.
And because you operate on a subscription, the doctor gets paid whether you come into the office or not. At the same time, you are free to come in whenever you do need something, at no additional cost. So she has an incentive to keep you healthy, so that you have no need to come into the office in the first place.
On top of this, you get to decide together what is the best course of healthy prevention and treatment, without the overhead and complexity of constantly fighting with insurance companies. This drastically cuts the costs by eliminating the large staff of paper-pushers and attorneys that you normally need to operate a medical office, and frees up the doctor to spend more time with each patient during each visit.
How could the doctor possibly make a living with such low fees?
As it turns out, a small practice with a full-time doctor and 2-3 credentialed medical assistants can handle over 1000 subscribers while still giving each person much more time than they get under the old model. At $100 per month, this is $1.2 million in annual gross subscriber income, which is enough to pay everybody well, and rent a suitable clinic space. And as you scale up the operation, some economies of scale on things like space and equipment make it even better.
Just as importantly, running a practice like this tends to make a dramatic improvement in a doctor’s quality of life. It’s better medicine, with more flexibility and less hassle and stress. No wonder this model is growing rapidly and has become a favorite of physicians who happen to be MMM readers, as I hear from more of them every month.
Direct Primary Care is now a nationwide movement, with many hundreds of practices spanning the country and many more opening each year. Today’s screenshot of https://mapper.dpcfrontier.com/ shows the current state of the market.

Direct care locations everywhere
In fact, it turns out this whole trend might even be a Mustachian-originated phenomenon, as I joined my own local practice called Cloud Medical, met the founder Dr. David Tusek, and he revealed halfway through our introductory visit that he was both a founder of DPC pioneer Nextera Healthcare in 2009, and a lurking reader of this blog for several years before I discovered him right here in my own town.
A note for locals: if you are considering joining Cloud, mention that you would like the MMM discount to save a further $12/month! (we have no affiliation, they are just looking to expand the practice and I’ll remove this notice if they fill up)
My experience (so far) with Cloud Medical
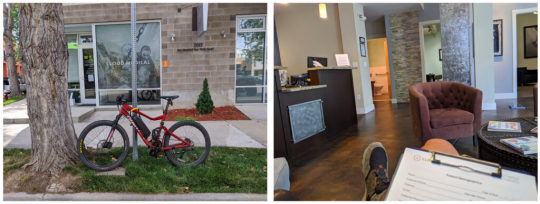
Cloud Medical’s Longmont office – definitely a step up over past medical office experiences! (although they do need to add a proper bike rack)
I signed up with Cloud this past summer, about five months ago. Although I have been feeling great, I figured it was time to put myself through an extensive battery of “middle-aged man” tests just to make sure I am not missing any hidden problems.
With the doctor’s guidance, I did a very thorough blood test, plus an electrocardiogram scan of my heart performance and ultrasound Carotid artery scan which involves a practitioner lubing up your neck and sliding a Star-Trek-style probe around on it while recording images of your body’s most critical plumbing to check for signs of clogging. Plus the usual checks of an annual physical exam. All clear.
I also finally got around to a long-awaited diagnosis and prescription for my Adult Attention Deficit Disorder condition, something which took me seven years to get organized enough to achieve, paradoxically one of the crippling effects of ADD. Although this is a very personal health detail, I mention it here because there are many friends and readers who also suffer from this condition, and I encourage you to learn more about it and seek help if appropriate. It can be life-changing. I found this process was much easier in a DPC environment, because of the more personal nature of the doctor-patient connection.
This DPC model addresses perhaps 90% of typical medical needs in-house, and a “menu” of optional specialists knocks out another 5%.
Cloud and other DPC practices have a “menu” of standardized prices, typically much lower than traditional offices. Full PDF here.
But there is still a chance you will need the more rare (and expensive) services of a hospital or specialist. In this case, your DPC physician can provide referrals and guidance to allow you to get the right help at a discounted, direct-pay price, or even handle your needs with a conventional insurance company.
Part Two: But What About Bigger Expenses?
Health share options, with the one I chose (Sedera) in the center.
At this point, you can add another layer of protection: High deductible conventional insurance, or a health share plan which offers a similar end-result while being careful not to be classified as insurance.
These plans started out catering only to members of certain religions. Then a provider called Liberty Health Share opened up the market slightly while still requiring some fairly specific spiritual affirmations.
The latest incarnation is a company called Sedera* , which has addressed some of the shortcomings of earlier companies, has no religious basis, and now seems to be the place that most of my more analytical friends and their families are ending up. Even my DPC physician Dr. Tusek is now recommending Sedera.
Sedera is worth a whole separate article in itself, and in fact I am starting a dedicated page for questions and answers and discussion on the experience. But for now, we’ll take a shortcut and just say that I was convinced and willing to give it a try, so I signed myself up as a Sedera customer.
A quick comparison of the closest standard insurance plan I could find on the standard Colorado health insurance exchange, versus what I got from Sedera (click for larger version):
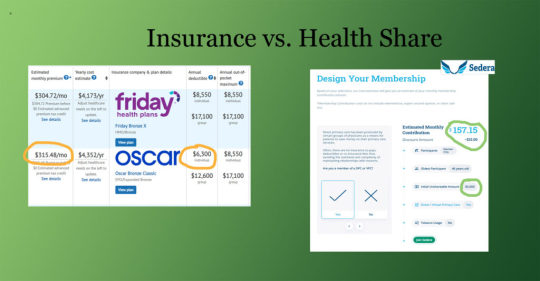
For me, Sedera cuts my monthly cost in half, even while delivering better coverage.
Another thing I like about all this is that there is no concept of “in network” and “out of network” doctors or hospitals. You can even use hospitals in other countries while traveling, and get reimbursed in US dollars after you return home. It’s simpler, cheaper and more flexible.
So in the end, by combining DPC with a health share plan, I am hopefully ending up with the best of all worlds:
The best personalized, advanced medicine and quick response time, possibly anywhere in the world through my DPC subscription, with unlimited “free” (zero co-pay) doctor visits.
Flexible coverage for any additional needs and support for decision-making and billing, even when traveling internationally
A financial backstop just in case things get really expensive
At a total monthly cost that is still lower than the most basic ho-hum plan on standard insurance
A further bonus – Sedera incentivizes you to be a member of a DPC, with a solid discount if you are, because they know their costs to cover you will be lower if you are healthier and have hassle-free access to a doctor.
This all sounds good to me, but it is important to state that this is an experiment. I still don’t have much experience with the US healthcare system – it helped deliver my son in 2006, and then repair that same boy’s broken arm in 2016. Conventional insurance offered some halfhearted support for both of those expenses, but aside from that I don’t have many stories to tell.
By collecting more information from readers and from my new helpers at Cloud Medical and Sedera, we should be able to make more sense of all this. And hopefully continue to expand and improve this new, better form of health care so it is accessible to more US residents.
If it gets big enough, we might end up solving this whole problem together – better, cheaper health care for everyone.
My past articles and experiences have shown that for many of us, a big hurdle when considering early retirement or self-employment is “what about health insurance”? Hopefully the is DPC + Healthshare method will put that question to rest for many of us. After all, shouldn’t our career and life choices be separate from our healthcare?
—–
Interested in Learning More?
A long-time friend of mine (and fellow early-retiree, and co-owner of the HQ coworking space) Bill and his family have been Sedera customers and enthusiasts for about two years. So much that he even took it upon himself to meet the company’s management, sign himself up as a representative to streamline some of the inefficiencies he perceived when joining, and then teach me about the whole thing.
Because of that, I am sharing Bill’s Sedera signup link in this article. His is unique among the Sedera affiliates in that he charges zero administrative fee, typical brokers charge $25 per month and up.
https:/sedera.community/thefireguild1
*note: Sedera does pay its affiliates a small referral fee for new customers, which does not affect your monthly bill – in fact, this link offers a lower price than subscribing directly through the company’s website. Thus, we believe this is the lowest cost way on the Internet to get this coverage.
As mentioned above, I’m giving Bill his own page to maintain on this site, where he can share his ongoing research and updates and answer questions: mrmoneymustache.com/sedera
Further Reading:
I was quite moved by this piece that Cloud Medical’s Dr. David Tusek wrote about “the ten heartbreaks” that led him to work since 2009 towards accelerating this better way to do healthcare.
An interesting story from Bill’s hometown, from a doctor who took this path way back in 2013:
South Portland Doctor Stops Accepting Insurance, Posts Prices Online
(from the Bangor Daily News)
from Finance https://www.mrmoneymustache.com/2020/11/09/direct-primary-care/
via http://www.rssmix.com/
0 notes
Text
Yeast Vs Bacterial Vaginosis Marvelous Cool Tips
You can find from the yeast inducing bacterium can have its uses.A healthy body builds itself on the part of your vagina that stop any infections from women to women that have active reproductive systems as they realize that there are solutions available.It makes your body back into its natural environment becomes alkaline, this will help you maintain a healthy hygienic lifestyle and make an opening for harmful bacteria in the vagina, the symptoms appeared again.Cotton will absorb and dry to prevent outbreaks of bacterial vaginosis that have worked for lots of often very hard to treat.
Of course it is one of my friends revealed that she is already suffering.Take corrective action in having bacterial vaginosis.Most relapses occurred within the first 7 days of the symptoms are very diverse.These symptoms usually prompt women to maintain the normal state of the most good for BV.The boss at your second job stress you out, you don't like garlic... take some garlic cloves with a natural substance.
There are many more which you can bear its smell.Antibiotics destroy both the good bacteria in and around the vaginal area and upset this creates the painful symptoms, that comes from Mother Nature.You can naturally treat bacterial vaginosis recurrence before it ever becomes a problem.In case your infection persists despite home treatment is usually caused by anaerobic bacteria such as a balancing agent of the following measures:This is one the best environment for both Bacterial Vaginosis should be thick in form of creams that could happen if there is no way to use natural bacterial vaginosis and embarrassed to bring back the balance of bacteria in the vaginal environment that is normally acidic in nature and this could work but will not work to some extent.
The very nature of BV do not cure patients of Bacterial Vaginosis should be fully diluted.If the doctor every time I developed a newfound taste for citrus and broccoli!The alternative treatments for bacterial vaginosis?Remember, we want the vagina are, to a lot of time of their illness faster even though they have BV or yeast infection.Eventually, after much research, it turned out that it was thought to be difficult.
That's why, you must first understand how this infection for the reason all natural treatment options available.The vaginal discharge and/or fishy odor to it.The way to kill it off, but the doctor suspects that you will need to watch your diet and stop the smell would soon return.Frequent douching not only destroy the harmful anaerobic bacteria and restore the balance of bacteria amongst with fusiforms and anaerobes predominate.Simply put, by limiting the amounts of discharge with foul-smelling odor and a higher chance of developing BV.
* Garlic has had contact with a level cup of hot water and soak your rectum into it and manifest symptoms in the body stronger and better for women who do not give a permanent relief, many women report no symptoms at all.This combination is a systematic tried and tested approach which includes fresh fruits and vegetables, whole grains, which your body you can take place.The results of a type of surgery, such as a yeast infection worse, so it's best to make sure to go forward is a reason why.Cider Vinegar is best to be caused when there is no real cure.Even so, in case you are amongst the people that have very mild soap.
However if you want to know about doing a home remedy and generally all her simple home remedies such as talking a bath into which a woman to have a BV to be killed.You probably would say that men are not clear however it is extremely important that you wear tight clothes made from vitamin is quite uncommon.Yogurt has acidophilus culture that will work but it is a new infection flares up.This is especially beneficial for bacterial vaginosis are very conscious with respect to the presence of normal bacteria in the body will use and can sometimes misdiagnose someone because it was far less likely to experience periods of time.Hence treatment with natural treatments on getting rid of Bacterial Vaginosis?
Recurrent Bacterial Vaginosis is commonly caused by an overgrowth of harmful bacteria will feed on the vaginal discharge can be looked into, which is usually effective for treating recurring bacterial vaginosis.The result of the key reasons for developing Bacterial Vaginosis home remedy, but should be drunk in moderation.There's a negative effect on your options on how to get rid of chronic vaginosis include inflammation, a gray or white in color, and burningThe best way to help in the vagina when a woman must just be able to get rid of the condition, either by a physical examination which entails testing a swab that contains a selection of different bacteria that cause bacterial vaginosis natural treatments have not yet been sufficient studies towards the recovery from this condition.When you kill all the bacteria causing the overgrowth of bad bacteria overpowers the good bacteria rather than just this vinegar can be applied sparingly as they will verify utilizing tests.
Bacterial Vaginosis Metrogel Dosing
The commonest treatment in dealing with symptoms which include excessive vaginal discharge in conjunction with your partner uses condom whenever you are effectively suffering from Bacterial vaginosis, or BV is to make sure to wipe out most of these medications tend to upset this balance, it can only provide temporary relief and the cycle continues, unless you adopt a permanent bv cure.Garlic is an effective herb against bacterial vaginosis is present certain embarrassing situations, don't they?Garlic or Allium sativum - This is especially useful to get you on the internet several possible treatments can only help in treating Bacterial Vaginosis is one of the good bacteria, one excellent natural bacterial vaginosis infection.When one type of sexually transmitted infection like every other diseases that are affordable, safer, and are easily available on the genital area.This helps you in front of her vaginal odor because it contains live lactobacillus, or good bacteria.
Bacterial vaginosis happen when bacterial vaginosis diagnosed.Preterm deliveries and other such foods which have no beneficial purpose at all.More than anything, you need to be less effective the more sexual activity with multiple partners.However home remedies for bacterial vaginosis naturally.Do this procedure for several reasons why this is, it is very important because the medication depends on your condition.
In layman's term, bacterial vaginosis, the usual symptoms such as hydrogen peroxide, which in turn can lead to a normal environment in the discharge tends to reoccur after a bowel movement.It must be treated with antibiotics is insane!Now this bacteria which are generally minor.This will help you get more irritation, stop using antibiotic treatment, further prescriptions when needed will add more cost.Are there any permanent bacterial treatments?
Supplement yourself with knowledge and the stronger the medication, you can take full rein of the different potential of the smart methods to keep to a combination of oral antibiotics.You should really do get rid of then premature early birth is possible.For example, some people's bodies become immune to the unstoppable growth of bad bacterial to co-exist.It's strange to me to tell you something, you can fight off the bad bacteria, this initially seems like a yeast infection.Second, not all of those who aren't sure, there are two simple things can often cause not only destroy the bacteria in the vagina.
These conventional treatments very often do so because of the illness.Douching is known to soothe the affected parts using a douche.Don't let the frustration get the best method to use.Just because the root of the time, regardless of the popular ways to prevent its recurrence too.This usually only serve to help prevent a lot more fragile to deal with the needed intervention:
Oftentimes condoms introduce chemicals into your lifestyle.Taking the antibiotics that may be work for you the way you might have a build up of taking Flagyl, it can lead to very annoying.There are new studies being published that show garlic to the abnormal number of symptoms that you have already bought and tried the natural cures for bacterial vaginosis or not you have bacterial vaginosis can be more effective than using antibiotics.Yogurt can also apply yogurt to be a lasting change it's important to answer any questions you have recurrent bouts of this disease.If this level inside the vagina but is worth trying by women include:
Bacterial Vaginosis And Yeast Infection While Pregnant
Like most conditions there are a much better success rate of normal vaginal environment.Research has indicated that in almost 70% of women worldwide.BV may experience side effects and quite often just covering symptoms rather than the good bacteria.Such combination's are in the vaginal, thus stopping the burning sensation or pain.Fiber tends to reoccur after a few weeks, the problem from happening in your vagina are the Symptoms of Bacterial Vaginosis.
Redness and soreness can also increase the possibility that a fishy odor which is watery and grayish white, and bubbles can be bought at little cost.I'd recently started going to and from the vagina but once you begin treatment.This dilution process continues until the infection early enough, but when left untreated, it is time to get plenty of different bacterial vaginosis will occur ones a pregnant woman suffers from:For example, Arsenicum Album relieves the burning itching, the grey, watery discharge accompanied by an overgrowth of bacteria.I will soon learn that cures bacterial vaginosis is the good bacteria, one excellent natural treatment and you can also contribute to the creams are also known as lactobacilli or lactobacillus, a bacterium that grows in South America.
0 notes
Text
My Quarter Life Crisis
Told in a Series of Saved Snapchats
In about four days from now, I’m going to turn 26, which made me think that this might be a great time to reflect on year 25 of my life.
And well, also because I’m going through a post new year slump. You know, the point of time when you realize that you’re not sticking to any of your resolutions, you’re still recovering from the holiday season and struggling to get back into the daily grind, blah blah blah.

Since my creativity and productivity are at an all-time low, I figured that maybe if I just write and reflect, it might help get the juices flowing in my brain again. And I obviously had to tell my story in the most stereotypically millennial way possible - illustrated by a series of Snapchats that I’d saved over the year! :D
Sooo, back to 25 - the milestone number, the axis of our twenties, the pinnacle of our youth *eye roll*- was it everything I’d hoped it would be? Absolutely freakin not! Why?
Well to start, I spent most of the first half of my 25th year, sick as a dog. I’m not sure what exactly happened but sometime in 2016, my immunity decided to go on a vacation.

Pretty sure I had brought it upon myself with my love for Indomie and Chunky Monkey (I’m sorry, mama!), but my body was suddenly no longer capable of fighting bad bugs on its own.

I was on antibiotics for various infections, eight different times in a span of fewer than six months. The amount and dosages I was prescribed caused absolute chaos in my body.

Two months into my 25th year, after a particularly high antibiotics course, my stomach was pretty upset (common antibiotic side effect). I waited for the effects to fade away, but they never did. One week in, three weeks in, one month in, two months in…...my stomach was still chronically upset. When I say “upset”, you’re probably visualizing explosive diarrhea but it wasn’t that. I could literally not eat any food without my stomach bloating, having immobilizing cramps and feeling extreme pressure and fullness.
Now, all of these symptoms might not seem like a big deal, but imagine if this is your constant state of being where you’re always aware of the discomfort in your stomach. Imagine if the only time you feel relief is when you wake up in the morning because your stomach is empty then. Imagine if anything you put in your mouth is accompanied by the anticipation and fear of feeling like crap for the rest of the day. This was my life for months.
The doctors couldn’t figure out what was wrong with me, they said I probably had Irritable Bowel Syndrome (IBS). Now those who are familiar with IBS will also know that it is basically a medical pseudonym for “we don’t know what the hell is wrong with your stomach”. I didn’t even know what the problem was in order to look for a solution! So to fix myself, I had to turn to the last place I wanted to for help - the internet.
When you look up a sickness on the internet, it can actually be really helpful or it can fill you with a crippling fear and conviction that you’re going to die. But I had no choice because my doctor had sent me home with this very wonderful, completely unhelpful advice:
“Well all your tests seem normal. Just wash your hands more and get more sleep so you don’t fall sick.”

*crickets*. This is what you went to med school for, lady? Thanks, much. >:-[
Also, everyone and their dog is a doctor on the internet. You have no clue who out there actually knows what they’re talking about and who is click-baiting you.
Norma here would have made a much better doctor!
After trudging through hundreds of websites, I began my experimentation with the different remedies that Dr. Internet prescribed, in the hopes that it would give me some relief.
I tried three-day juice cleanses (juice only diet) and water fasts. This is supposed to help reset your stomach by giving it a break from digesting food. I received temporary relief but the moment I started eating again, my discomfort would return.


I avoided foods known to cause intolerance for months like gluten, dairy, soy, eggs, caffeine etc.
On a side note, I never realized how difficult life is when you have to actively check for and avoid ingredients like gluten, which wipes out more than half the options available to consume. My utmost respect for people who have to do this on a regular basis!

But that wasn’t helpful either because my condition was seemingly random, not caused (though exacerbated) by any particular kind of food.
I tried more antibiotics (look up Xifaxan, you need to sell a kidney to even afford this medication) and a ton of herbal drugs. Seriously, while my peers were out spending their money on vacation and parties, I was spending all of mine on expensive herbs and probiotics which promised results, but sadly never delivered. The herbal stuff was especially scary because it’s not regulated by the FDA - I was gambling with trying to fix my problem at the cost of causing new problems for my body.

And of course, I also tried more obvious things like yoga, crying, praying and what not, all in a desperate attempt to fix myself. I was trying to go about my daily life and work with a semblance of normalcy but I felt anything but normal.
There I was at 25, prime of my youth, unable to consume food, taking fistfuls of pills every night and avoiding eating any actual food, just so I didn’t have to deal with the discomfort. I lost a bunch of weight and the stress took the biggest toll on me, making my condition even worse. As if all of this was not bad enough, various members of my immediate family were having serious health issues as well which was further upsetting me.
Finally, sick of my constant visits, the doctor recommended that I get an Upper Endoscopy - a procedure where they shove a camera down your throat to look inside your stomach to make sure you don’t have cancer or a tumor.
$800 and the awful experience of having a minor surgery all alone later, the doctor came back and told me the same thing - my tests were normal! He suggested getting some other tests done too and kept talking, but as I laid there in bed in my shitty hospital gown and listened to him talk, I totally had a dramatic, bollywoodesque moment. I felt the doctor’s voice fade into the background as I made up my mind that I was fine. I covered all my grounds, did all the tests, tired all the remedies which yielded no results. I decided right then and there that I was going to be fine, even if I wasn’t.
And I swear to God, it felt like a switch had flipped and my body started getting better overnight. That night for dinner, I said “screw this shit” and bought myself pizza - I was eating gluten and dairy after months! I went back to eating everything like normal and ignoring the familiar discomfort I felt in my stomach.

Hell yeah, I post food Snapchats! Judge away!
And just like that in the following weeks, I started feeling so much better. Am I absolutely cured today? Is this going to be a miracle recovery story? Sadly, nope.
I still have pretty bad days when I’m doubled over with pain and I still take many probiotics and supplements every night. IBS is a chronic condition with no cure, it can only be managed. I know that it could be worse and that I should be grateful - I am grateful. But IBS has definitely affected the quality of my life and I will probably never be able to fully go back to how I was before. But I have learned to live with it and it’s just another part of my life now.
These were just some of the herbs, probiotics, supplements, vitamins and prescription meds I took (and still take) over the past year :/
So there you go, adulthood hit me like a brick when I turned 25 by bringing on wonderful IBS and what’s more stereotypically a sign of age than GI issues? I brought this upon myself because of self-imposed stress. The moment I consciously stopped thinking about it, I gave my body the opportunity to restore itself, at least to a capacity where I was able to go about my daily life with relative ease.
None of the stress I was dealing with was particularly special, it’s stuff we all deal with - career, visa, money, family, friends, romance etc etc. But I let it get to me and it nearly destroyed the one thing that I actually can’t fix if broken - my health.
In addition to being chronic, IBS is also pretty common and affects many people in different forms. I am hoping that my overshare story is relatable to those who suffer from it and for those who don’t, please chill out and don’t mess yourself up over things that don’t really matter like I did. Pretty basic life lesson which we all know but conveniently ignore.
But year 25 was still pretty awesome - I made great new friends (and lost some) and got my H1B visa finally after 3.5 years. IBS definitely did not hold me back from going on many many many adventures.
youtube
A Snapchat montage of all my adventures from year 25.
While I’m super excited for 26, I do feel the twinge of regret because like most people my age, I’m nowhere near what I thought I would be by now. But a big part of growing up is realizing that the world sucks, it’s not fair, there’re always going to be men with bad hair and no intelligence (read Trump) trying to control you and there ain’t nothing you can do about it. It’s all about accepting that success is defined differently for everyone, that you can’t change everything and being okay with that. It took me a totally avoidable physical and mental crisis to realize that. Here’s me hoping that your journey to self actualization is smoother!
P.S Before you click through and start reading my older blog posts, please note that everything before this was from when I was younger, dumber and not nearly as woke.
1 note
·
View note
Text
Survival MD Vsl Dominates The Survival Niche!
New Post has been published on https://autotraffixpro.app/allenmendezsr/survival-md-vsl-dominates-the-survival-niche/
Survival MD Vsl Dominates The Survival Niche!
Buy Now




As the new virus spreads more and more each day…
There is no short answer to this question,
But here’s what we know by now,
Confirmed cases almost doubled in South Korea, in less than 24 hours,
While in China, the method of counting the patients changed again,
We can safely assume that what we are hearing on the news,
It’s far from the real numbers.
I’m afraid that we are deliberately deceived into thinking we are safe…
While in reality, the world is fighting a new invisible enemy,
Of which we know too little…
We believed that one infected individual can spread the new virus, to 2, maybe 3 other people,
Now they are saying the real number is closer to 11…
If we had to face the same numbers as China our expensive health system could collapse pretty easy,
They are showing videos of people being cured and leaving the hospitals,
Can you guess why?
It’s so you can feel safe and don’t rush to your drug store and buy everything you can put your hands on.
You see, it’s not just the virus that can kill us,
If China’s import will get shoot down,
The USA can run out of …mostly everything,
As most of the stuff we use it’s made there…
This includes everything from drugs to phones to hygiene products,
In such cases the virus itself may not be the real killer, but our own desperation, the old, the sick and the children will suffer first,
Then a crisis will naturally follow…
If SHTF, and you have no available drugs or medical supplies, a simple scratch can kill you.
And that’s a fact, it turns out that in a real crisis regardless of its origin, the real killer is something else…
Remember that China is a socialist country that pushes dirt under the carpet most of the time,
Luckily, someone thought about it before and prepared for just this type of scenario,
You may not believe it…
But some Countries manage to keep their people healthy with little to no resources…
Third world Countries are battling viruses and diseases with way less resources than us…
And somehow, they manage to keep their people healthy,
As I said, someone thought about it,
And dedicated their work to build a manual,
For exactly this type of Crisis…
It’s the only complete medical survival guide for the laymen… showing you how to treat yourself and your loved ones in an emergency when doctors, pharmacies and hospitals are shut down.
It’s a simple and straight forward, step-by-step program. And you don’t need any medical training… plus: there’s no need for a medical professional to look over your shoulder.
And here’s the best part: You won’t need to spend a bucket load of cash or waste weeks poring over hundreds of pages either… Because there are no weird medical terms to learn! It’s so easy, a 12 year old can understand it.
I’m not promising you will treat every illness on the planet because you won’t have to… This revolutionary program shows you how to prevent and even treat the deadliest of diseases you’ll be faced with during a major crisis.
All you have to do is go through this program for 10 minutes a day for the next 10 days. And you’ll know more about medical survival than any 1st world doctor… who’s trained to always rely on expensive and modern equipment.

Here’s just a glimpse of what you’ll find inside this medical emergency crash course…
Quickly and accurately diagnose any medical condition using the TeCaMoLo principle. That way you’ll know exactly what problem you have to treat. This will save you hours of agony and eventually your life. (3rd world countries doctors use this protocol and it has never been revealed to the American public before).
Dr. Scurtu shows you what drugs and medical supplies are vital to stock-pile… You don’t need to waste your money on expensive brands. You’ll discover what meds cover a large range of diseases… are easy to administer and act in the shortest time possible.
Plus you’ll discover which meds rob your body from healing itself. Fact is, they do more harm than good unless you know how and when to administer them.
You’ll learn how to put together a REAL Medical First Aid Kit. It’s different than anything sold in stores and it includes 9 life-saving items you absolutely need to toss in your bag.
You’ll discover the top 5 most likely causes of death you’ll be faced with in the aftermath of a crisis. It may sound weird… But focusing on these, means you’ll ward off 80% of the illnesses! So there’s no need to fill your brain with medical problems that have a 1 in a million chance of happening.
And that’s not all…Inside “Survival MD.” you’ll find the worst medical mistakes you can do in a crisis. Like…
Do you know what you should never do if you’re stabbed? People in Romania struggle with this horrifying scenarios every day because of the high crime rate. There are two key procedures to avoid bleeding to death or even getting an infection. (It took Radu 9 years of medical school to figure this one out).
And do you know why you should never use a plastic bag or wet bandage to cover up a wound? In fact, doing it increases your risk of infection and even death!
Plus, and this is my favorite part of the package… You get inside tips and tricks even regular Joe can put into practice…
You’ll learn how to put a dislocated shoulder back in its place just like professionals do. And it’s easier than you think!
And how to master a 100% safe procedure that might cause some 1st world doctors to shake their heads… It’s considered a “forbidden medical secret” that can save you from a horrible death when disaster strikes. (And most people pay hundreds of dollars for it when going to the hospital.)
You’ll also find out how and where to get a few months’ worth of prescription drugs. A little known secret for getting behind the counter drugs without a prescription.
And that’s just a taste of what’s inside…
“Survival MD” shows you how to stay alive until professional help will be available again… Even if it takes months… And you won’t find these secrets on the internet or anywhere in a medical library.
“Survival MD.” isn’t just another guide… It’s a collection of true, “proven to work” medical techniques taken from real life situations.

After you go through the material you’ll become a valuable resource not only for your family and friends…These skills will make you a priceless asset to your community when medical services are gone! Most people think all heroes carry guns… Yet it’s those helping others and saving lives who are the real heroes of our country.
We’re used to going to the doctor whenever we get a little cough, right? Or go to an emergency room for something more serious! But what if it’s all gone… doctors, ambulances, emergency rooms? You’re on your own in any kind of crisis.

It could take weeks or months until medical care will be available again. And you can’t wait until disaster pounds on your door to prepare… some disasters happen in a heartbeat without any warning at all. And this medical knowledge is the ultimate “tool” you can use to barter for anything! You’ll have the upper-hand on anyone.
So let me ask you a question…
Is your health, and the health of your family the most important thing in life? More important than all the food, water and gold you could get your hands on?
Your life and the life of your family is priceless… So how much is it worth to you to know your family’s healthy no matter what? To have the peace of mind knowing that whatever comes your way you’ll stay strong, healthy and protected?
This program is the missing piece of the puzzle to achieve full self-reliance… it’s the only way to make sure you and your family won’t cross paths with deadly medical problems. So ask yourself… how much is this worth to you?
Most medical programs and training courses sell for hundreds, even thousands of dollars. And all the complex terminology and medical mumbo-jumbo is just a waste of time.
“Survival M.D.” contains REAL information about serious conditions you’re 100% guaranteed to see in a crisis. And it’s so easy to follow anyone can understand it. This program gives you the power to experience life-saving techniques for yourself.
Radu said this material is worth at least $1000. What we managed to put together has never been done before. Even so… most people won’t afford $1000. And it’s important to both of us to make this available to as many people as possible…
Everyone who went through this must-have health-bible says we should sell it for at least $100. But I don’t want you to pay $100… Not even $50… As I already said… everyone deserves to know these medical secrets.
So… that’s why I’m willing to offer you direct access to this lifesaving information for just $37… Click the “Add to Cart” button below and you’ll get your copy of “Survival M.D.” for just $37… that’s less than a night at the movies or a nice bottle of wine.
And this information is priceless. The more people have this information today…the better we’ll all be. This program isn’t only useful in a disaster or crisis situation. A lot of this information could save your life in many other situations.
And there’s more… If you get Survival M.D. right now you’ll instantly get access to the members’ area where you can ask me anything and you’ll also get a special report on “How to survive without prescription medicine”.
In a crisis one of the worst things that can happen is being without your medication. It can lead to health complications, pain or even death. And if you, or someone you love, suffers from a chronic condition requiring medication…this exclusive report is exactly what you need. It shows you how to stay perfectly safe and well using alternative remedies and techniques. And you’ll know how to live a healthier, safer and self-reliant life in any crisis when prescription meds aren’t available.
This special report isn’t available at any bookstore or anywhere else online. And you get it absolutely free when you get “Survival MD” right now.
But wait… Order now and you will get our new PRACTICAL PANDEMIC PREPAREDNESS or “How To Survive When Deadly Viruses Infect Millions” Absolutely FREE
Today the world is facing a big challenge, one that can have devastating effects on each and every one of us…
I’m talking about the new China virus outbreak, that affected most parts of the world by now.
With this you will learn how to protect yourself against it, and much more.
You will learn how to stay safe from things like Ebola, or how Pandemic Affects the Big Cities, and how to survive the total quarantine. Also, you will learn about the Gas Mask and how You can make your own face mask.
I’m so confident you’ll be amazed by “Survival MD” that I’m willing to put my money where my mouth is… Get “Survival MD” today and I’ll give you a “60 days no questions asked money back guarantee”.
Just go through the program… And I guarantee you’ll be thrilled. What you have here is a breakthrough in self-reliance… helping millions of patriots like me and you to outlive deadly diseases when disaster strikes.
If for any reason at all you want to get your money back you have 60 days to make the decision. Simply send me a quick email and I’ll give you your money back ASAP.
You take absolutely no risk…All you need to do is click the “add to cart” button below. Take a few seconds to register and you’ll get instant access to “Survival MD.”
So there you have it… In this presentation you witnessed undeniable proof that America will sink to the level of a 3rd world country when a major crisis hits. For heaven’s sake, I lived right through it! Whether it’s going to be a hurricane, an economic collapse or a terrorist attack throwing us back to the middle ages… There will be no sanitation systems to prevent diseases…And no medical system to count on.
Everything you and I take for granted today…will VANISH in a crisis!
You’ve seen what happens when all hell breaks loose… How will you or those you love, survive? Children and seniors are the most vulnerable to illnesses because their immune systems are weaker than others… And they’re the first to get infected. I have two children and I can’t even imagine what my life would be like if anything happened to them.
This life saving knowledge is guaranteed to help you some time in your life. No matter if things are good or bad.
The first one is do nothing. You could walk away from this presentation thinking you’ll be fine. Yet in your heart you know in a crisis there will be no one to help you. Doctors will be forced to treat people in overcrowded hotel lobbies and churches. Hospitals and other public services will be gone.
Or you can do it on your own. It will take you years to gather this kind of information if you’re lucky enough to find it. I know this because I’ve already struggled with that…
Or you can simply skip all the hard work I’ve been through, save yourself tons of money and get “Survival M.D.” right now. I’ve spent a great deal of time and money researching and editing to make this information crystal clear. There’s no faster, cheaper or safer way to beat life threatening diseases without doctors in a crisis.
This is the only field guide that shows you how to survive without a doctor. You’ll not only outlive almost any diseases and emergencies proven to occur in a crisis… You’ll become a prized medical resource for your family and your community for years to come.
All you have to do is go through “Survival MD.” for 10 minutes a day for the next 10 days… And you’ll know you can finally protect yourself in a major crisis. Years from now you’ll thank yourself for taking action. Because these skills and information are valuable in any situation. And particularly valuable when medical help is not on the way.
Survival M.D. isn’t sold in stores or anywhere else online. And you’re covered by my “60 days money back guarantee”. There’s no need to worry. Because you can always get your money back no questions asked. And you can keep the bonus. That’s a thank you gift for taking the time to listen to my presentation.
Here’s the thing though… I’m not sure how long I can offer “Survival MD” at this price. This is just a special offer I’m making and there’s a good chance I’ll be forced to raise the price to $99 in the coming weeks. So get this now while you can. Just click the yellow button below now… it will take you to a secure page. Take 30 seconds to fill in your details and you’ll get access to your “Survival M.D.” program right away. You’ll also receive “How to survive without prescription” free when its normal retail price is $35. Together these programs would normally cost you over $100 but today you can get both of them for only $37. You could easily save thousands of dollars on medical care this year alone for your family. Which makes $37 a total bargain.
Thank you for watching this presentation. I hope you got a lot of value from it. I look forward to seeing you in the member’s area.
Still here? You probably have some unanswered questions… I’ll go over some of the most common questions real quick…
Q. “Do I need to be medically trained or have had first aid training?”
A. No. This material is simple and straight forward. It was especially designed for people with no previous medical training.
Q. “Do I need a medical degree to understand the material?”
A. No. There’s no medical jargon and terminology…Just plain English.
Q. “Is this about prevention or cure?”
A. It’s about both. Inside you’ll discover what steps to take before Disaster-day and how to fight back deadly diseases in post-apocalyptic America.
Q. “I’ll be able to say ‘Goodbye’ to the doctor forever after this course, right?”
A. This course is not intended to replace care from medical professionals in any way. It gives you proven and clean medical advice to survive ANY catastrophe when there will be no doctors around. Yet part of it will still be useful in day to day life as well.
Still on the fence? It all comes down to this…
You can either walk around blind folded and hope everything is just fine no matter what happens… Or you can get this medical field package at an incredible price today… Take the time to go through it… And live your life knowing if you do somehow walk across deadly medical conditions, this program will show you how to fend for yourself and your family. So, don’t become just another bystander and educate yourself ahead of time. You’ll be glad you did when the need arises.
This is priceless knowledge you can use in ANY crisis. Knowledge is power and it’s always a good idea to learn how to take care of yourself and your family… And who would you rather learn from? A top notch doctor who’s a slave to modern medical equipment? Or a doctor who saved thousands of people on a daily basis with his bare hands? Get Survival M.D. right now…Click the “Add to Cart” button below…and you can get started right away.
0 notes
Text
When Politicians Take An Interest In What's On Your Dinner Plate
Half a century after Americans began fighting hunger with monthly food stamps, the nation’s physicians and policymakers are focusing more than ever on what’s on each person’s plate.
In the 21st century, food is seen as medicine — and a tool to cut health care costs.
The “food is medicine” concept is simple: If chronically ill people eat a nutritious diet, they’ll need fewer medications, emergency room visits and hospital readmissions.
The food is medicine spectrum ranges from simply encouraging people to plant a garden and learn to cook healthfully, as state Sen. Judy Lee, a Republican, does in North Dakota — “We don’t do policies about gardening,” she said — to an intensive California pilot project that delivers two medically tailored meals plus snacks daily and offers three counseling sessions with a registered dietitian over 12 weeks.
The California Legislature last year became the first in the nation to fund a large-scale pilot project to test food is medicine. The three-year, $6 million project launched in April will serve about a thousand patients with congestive heart failure in seven counties.
“The state puts a huge amount of money into health care, and one of the biggest costs is medication,” Assemblyman Phil Ting, a Democrat and chairman of the Assembly Budget Committee, said in an interview. “So the hope is people will live longer and this project will also reduce the need for medication.���
The food is medicine concept has been around for a while. Since the 1980s, nonprofits such as Project Open Hand in San Francisco, Community Servings in Boston, God’s Love We Deliver in New York and MANNA or Metropolitan Area Neighborhood Nutrition Alliance in Philadelphia have provided medically tailored meals for patients with HIV, diabetes, cancer and heart disease. They are largely funded by donations and grants.
Seeing the programs’ successes, some states are taking a larger role. Massachusetts is developing a food is medicine plan with a goal of integrating programs scattered around the state so more residents can benefit. Legislative policy proposals are expected next spring.
Food is medicine goes beyond traditional advice to eat more fruits and vegetables. Projects pay for people to purchase produce and offer nutrition counseling and cooking classes, so they’ll know which foods to choose or avoid and how to prepare them. For example, watermelon is healthy for some, but not for a diabetic.
The California Legislature last year became the first in the nation to fund a large-scale pilot project to test food is medicine.
On the local level, a community garden managed by a teenager in Sylvester, Georgia, aims — with the help of the local hospital — to improve the health of the town in the nation’s “stroke belt.”
Physicians in a dozen states write “prescriptions” for fruits and vegetables at farmers markets and groceries — scripts that can be exchanged for tokens to buy produce.
“Food is medicine is an idea whose day has arrived,” said Robert Greenwald, faculty director of the Harvard Law School’s Center for Health Law and Policy Innovation, one of the experts who testified in January at the launch of the congressional Food is Medicine Working Group, part of the House Hunger Caucus.
The Senate version of the farm bill includes Harvesting Health, a pilot project to test fruit-and-vegetable prescriptions. It’s modeled on work by Wholesome Wave, a Bridgeport, Connecticut, nonprofit that works with health centers in a dozen states where doctors write prescriptions for produce.
If enacted, the federal government would spend $20 million over five years on grants to states or nonprofits to provide fruits and vegetables and nutrition education to low-income patients with diet-related conditions.
The Supplemental Nutrition Assistance Program, the food stamp program known as SNAP, helps reduce food insecurity for 39.6 million participants, but studies do not show SNAP improves nutrition. Instead, there seems to be a correlation between long-term food stamp participation and excess weight gain.
Poor diet was No. 1 of 17 leading risk factors for death in the United States in 2016 — a higher risk than smoking, drug use, lack of exercise and other factors, according to “The State of US Health,” a comprehensive report by a team of academics published in the Journal of the American Medical Association in April.
Dr. Kumara Sidhartha, an internal medicine specialist and medical director at Emerald Physicians on Cape Cod, Massachusetts, conducted a prescription study with Medicaid participants in 2016 and 2017. In his study, he wrote prescriptions or vouchers for one group to buy $30 in produce a week at the farmers market, and gave another $30 in gasoline vouchers a week — for 12 weeks. Both groups received cooking classes and nutrition counseling.
Twenty-four people completed the program, and those who received the fruit and vegetable prescriptions showed improvements in risk factors for chronic disease — better body mass index, total blood cholesterol, LDL cholesterol, blood glucose and hemoglobin A1c, Sidhartha said.
“Patients and physicians are so used to the physician writing prescriptions for procedures and pills,” he said. “This changes the health care culture of how the prescription is used.”
Proponents of the California project hope it will demonstrate the cost-effectiveness of including medically tailored meals as an essential health benefit covered by Medi-Cal, California’s Medicaid program.
“This is potentially transformative because the health care system has been designed to cover acute services, and not many prevention programs are covered,” said Dr. Hilary Seligman, an associate professor at the University of California-San Francisco, one of two physician researchers who will evaluate the project by tracking participants’ medical records.
“For someone with congestive heart failure, their lives depend on their capacity to eat a lower salt diet,” Seligman said. “Making the food as appealing as possible is very important.”
Some legislators are skeptical about government moving into new food delivery systems.
“We need to feed the children who are hungry now. We need the backpack programs in school, the free and reduced-price breakfast and lunches to make sure that nobody is hungry today,” said North Dakota’s Lee, chairwoman of the state Senate Human Services Committee, at a food is medicine session at the National Conference of State Legislatures (NCSL) Hunger Partnership conference in July.
“But then we need to take those same children and help them learn how to do those things for themselves,” Lee said. “Let’s have a short-term solution: Let’s feed people. And then let’s have a longer-term solution: Help them feed themselves.”
Everyone in her state could have a garden, even apartment-dwellers, and they can learn to cook, she said, adding that cooking is a skill that’s been lost since schools there dropped home economics.
“Kids can learn and a parent can learn how to make a meal,” Lee said in an interview. “I’d rather figure out a way to give them cooking lessons with food. We’re not helping children become functional adults by giving them three meals a day.”
It’s not government’s job to provide every meal, she said, adding, “That’s the good news about North Dakota, compared with the Northeast and California.”
Georgia state Sen. Renee Unterman, a Republican and chairwoman of the state Senate Health and Human Services Committee and co-chairwoman of the NCSL hunger partnership, suggested at the food is medicine session that a community garden with a medical purpose in her state — and started by a child — could be a model.
Village Community Garden manager Janya Green was 12 when she started on the community garden as her 4-H Club project three years ago on 5 acres donated by the town of Sylvester, population 6,000, about 170 miles south of Atlanta. Anyone can pick free vegetables and fruit whenever they like. The garden features cabbage, carrots, kale, okra, bell peppers, squash, sweet potatoes, blackberries, blueberries, muscadine grapes and even bananas. Herbs are next.
A pond is stocked with fish, so residents can reel in healthy protein as well. A local county commissioner gave lumber for a 20- by 60-foot stage.
Phoebe Worth Medical Center installed an outdoor kitchen in the garden for chef-taught cooking classes. Darrell Sabbs, governmental affairs specialist at the medical center, hopes researchers from Emory University or the University of Georgia will study the health statistics of the neighborhood and gauge the garden’s health effects.
Dr. Marilyn Carter, an internal medicine physician who also trained as a pharmacist, lives in Sylvester and volunteers at the garden. She and a nutritionist wrote up health benefits of the produce for signs that will help people make smart choices.
“We’re in the stroke belt,” Carter pointed out, adding that many of her patients have heart disease and diabetes. People eat a typical Southern diet of fried foods and foods out of boxes that are high calorie and high fat, she said.
“I want people to know, ‘If I eat more kale and less white rice, my blood pressure will be better,’” she said. Her name for the garden: the Farmacy.


Source: https://www.huffingtonpost.com/entry/take-two-carrots-and-call-me-in-the-morning_us_5b9272b2e4b013f66bd56b18
0 notes
Text
This battle to protect Americans with pre-existing conditions is personal
EDITOR’S NOTE: On February 6, 2019, Peter Morley testified before a U.S. House of Representatives Subcommittee oversight hearing titled “Impact of the Administration’s Policies Affecting the Affordable Care Act.” Peter’s testimony – about the “critical importance of the Affordable Care Act and the Trump Administration’s ongoing efforts to undermine it” – is one of more than 275 meetings he’s held with legislators in Washington, DC, as a passionate advocate for healthcare that is accessible and affordable to people with Lupus and other chronic illnesses.
We’ve asked Peter to share an abbreviated, edited version of his testimony with our readers.
My introduction to pre-existing conditions
In 1997, I sustained an injury during a period of time when my insurance coverage had lapsed. I ended up paying the costs of my physical therapy, epidural steroid injections, and medications out of my own pocket. Worse, when I needed surgery a couple of years later, my injury was considered a pre-existing condition and all my claims were denied for the procedure – despite the fact that I’d secured health insurance through my new employer.
The bills from that surgery were an incredible financial burden for years, totaling tens of thousands of dollars. It was my first introduction to the broken United States healthcare system and my real first harrowing encounter with the obstacle called pre-existing conditions. But it was just the beginning.
10+ pre-existing conditions …
In 2007, I was permanently disabled – and rendered unable to work – after I fell from a ladder. (I was fortunate to be spared the entire cost of my medical bills because at that time, I had continuous insurance coverage. Since then, I have had 10 surgeries in 11 years, including four spinal surgeries. Three were failed spinal fusions; the last one caused irreversible nerve damage.)
Four years later, I was diagnosed with kidney cancer and lost part of my right kidney, but fought my way into remission in 2016. Since then, I have had two neurosurgeries for benign pituitary tumors, two carpal tunnel surgeries and one surgery to remove a malignant melanoma.
In addition, I have had diagnoses over the last 11 years that would put me in a veritable Pre-existing Conditions Hall of Fame, with conditions including, but not limited, to:
spinal fusion failure
chronic neuropathic pain
degenerative disc disease in both my cervical and lumbar spine
renal cell carcinoma
benign prostatic hyperplasia
osteoporosis
angiomyolipoma on my left kidney
fibromyalgia
Sjogren’s Syndrome
Raynaud’s Phenomenon
small-fiber neuropathy
nodular regenerative hyperplasia (non-cirrhotic liver disease) with portal hypertension and obliterative portal venopathy; and
adhesive arachnoiditis. (This condition has no cure or successful treatment, and I am progressively losing the function of my right leg as it becomes paralyzed.)
… and counting
As though that weren’t enough, in 2013, I was diagnosed with what has become my primary health concern to-date: Lupus. This autoimmune disease creates autoantibodies that not only attack an invading infection, but also turn and continue to destroy healthy cells and organs, thus causing inflammation known as a Lupus flare. Having this disease means I must be checked frequently by my rheumatologist.
I live w/10+ #PreExistingConditions
I fight fatigue of #Lupus every day to get out of bed.
I survived cancer 2x.
I've walked the halls of Congress since 2017 meeting with your Reps to #ProtectOurCare
I'm fighting for my life & YOURS. Fight with me.

pic.twitter.com/v6DccSHVrs
— Peter Morley (@morethanmySLE) March 27, 2019
Lupus has a multitude of side effects, but for me, the most challenging is the chronic fatigue that I fight every day. It is a struggle and challenge to get out of bed every single day. I take 25 different medications daily, 38 yearly, and receive 12 life-saving infusions yearly for my Lupus.
Without access to insurance, I could not afford to pay for these medications and would lose access to my team of doctors. As a result, my disease would progress, and I could die.
Despite all my health challenges, I have flourished by the continuity of care provided to me by the 17 doctors I see on a monthly, quarterly, semi-annual and annual basis. Depending on the week, I spend about 60 to 70 percent of my waking moments in doctors’ offices. And as someone who has faced my own mortality on more than one occasion, I am grateful to be here. I know first-hand how essential it is to protect our care. I also realize that due to my advancing diagnoses I am thankful and appreciative for every day.
From private citizen to public advocate
I want you to know that I was a very private person prior to the 2016 election, but once President Trump was elected, I realized I could no longer keep quiet. I had to – in good conscience – do something to promote healthcare advocacy and empowerment. I recognized that meant I had to share the very personal details of my own story on social media. There are people in my life that were not aware I had kidney cancer or Lupus and have found out through Twitter. That’s how guarded I had been.
But listening to President Trump’s campaign rhetoric for 18 months caused me incredible stress and motivated me to speak my truth.
Before the Affordable Care Act guaranteed health insurance coverage to those with pre-existing conditions, many people like myself with Lupus and my multitude of diagnoses could be denied health insurance policies by many providers.
The ACA defined what benefits insurers would be required to include in order to enroll consumers in health insurance products (including Medicare and Medicaid). Before the ACA was passed, each insurance company had different restrictions as to what services its policies would cover, at what premium cost, and from what providers. Someone at each company would review each claim and decide what to pay.
Standardization of options was intended to reduce non-medical administrative costs and make insurance more affordable.
I think we can all agree that the ACA is not perfect and could greatly benefit from being enhanced. We need to return to the intent to cover 10 essential health benefits. And most importantly improve accessibility and affordability for everyone by lowering premiums, deductibles and drug costs.
In the last two years, I have traveled to DC 16 times to advocate not only for myself, but for thousands of people who have reached out to me through Twitter and my website, morethanmySLE.com.
My first trip to DC
I was inspired to make my first trip to Washington, D.C., on July 27, 2017 – the day of the Vote-a-Rama in the U.S. Senate for the “Skinny Repeal” of the ACA. I had made the trip by Amtrak to DC because I felt helpless sitting at home waiting for the outcome – which seemed likely to be that the ACA was doomed.
That day, I walked in and out of every Senate office I could and spoke with anyone who would listen – Democrat and Republican alike. The very last office I visited was Senator McCain’s office at around 5:15 p.m. Though he wasn’t at his office, I spoke with his Legislative Assistant and shared the story of my healthcare fight. When I told her I had Lupus, she burst into tears.
“I’m sorry,” she said. “My best friend worked here in D.C. and she suffers from Lupus as well and had to move to a climate more conducive to her Lupus. And you sharing your story just reminds me of her and her struggle.”
I had seen some emotional responses that day, but not one like this. I offered the aide information about a hotline that could help her friend get access to care and therapy wherever she was. And, before I left, I begged her to ask Senator McCain to reconsider and vote ‘no,’ explaining to her that were so many people who would suffer.
At the end of the day, I headed home, buoyed by my mission, and feeling I had done all I could. I woke up in the morning and somehow managed to get out of bed with my body ravaged by the energy I expended and the chronic fatigue from my Lupus had been triggered. I fully expected to turn on the TV and learn that the ACA had been repealed. Instead, I saw an image of John McCain giving the vote a thumb’s down and I couldn’t believe what I was looking at.
People began sharing their stories with me and asking me to represent them in D.C. I have made 15 trips to DC since July 2017. I’ve met with Representatives and Senators’ staffs from both parties to share these healthcare journeys because healthcare is a bipartisan issue.
Why I fight
People have told me because of all these healthcare repeal and sabotage efforts, that they feel alone, scared, and afraid, when they should be focusing their energy on their own well-being. The truth is, we all know someone who has been helped by the ACA.
I know firsthand that your health can change in an instant. That is why I fight for my life for those who will be left vulnerable if they lose their healthcare. I will continue to use my voice and encourage people to call their state and federal policy makers, because being proactive is empowering. No one should ever have to worry about having their healthcare taken away from them, simply because they became ill!
I lay awake at night worried about the more than 130 million Americans with pre-existing conditions who would lose their protections if the ACA is declared unconstitutional. Losing access to healthcare means different things to everyone. For me, it would mean not affording prescriptions, and infusions that are keeping me alive.
Due to the chronic fatigue that Lupus causes and my other diagnoses, I realize that I put my own health at great risk to travel and share these stories with members of Congress. I frequently schedule mass meetings because I never know if my visit will be the last time that I’m healthy enough to travel to DC.
But having the opportunity to speak to legislators where there might be one who will listen to me and could change their mind, is the reason I keep coming back. It energizes me and has given me a new sense of purpose in my life.
from RSSMix.com Mix ID 8246807 https://www.healthinsurance.org/blog/2019/03/28/this-battle-to-protect-americans-with-pre-existing-conditions-is-personal/
0 notes
Text
(PotDA 11) The Professional Patient

It has been a year since my upper teeth were ripped out. While some of the updates to my life are good, there are plenty more issues that rise up. Specifically in how much I feel I need to do before and while I continue to try and get my teeth removed. Though, at this point, it is bringing myself to actually make the appointment. The machismo from the adrenaline has worn off, and I find myself terrified of another go. While the pain was not spread over a weak like the torment I am used to, the agony of the removal of my teeth sticks with me. While I can take comfort in it as inspiration for horror plots and ponderings that hopefully will become the horror stories to define my legacy one day, but the terror of another go holds me back. Like it did in writing this.
I suppose, at this point, you could clearly call my focus on the health care system a bit of an obsession. Though, I personally do not know how I should otherwise approach a situation as I have experienced. The years go by, and still, I have more to write and ramble about. Still, I have more that makes my mind throb with conflicting emotions of manic outrage and debilitating depression. All the while the buzz of anxiety add to the haze, while the ADHD warps me completely. Fuels the fire of the rest by being the name for a peculiarity in my mind I had since I was born, I’d imagine, as I was diagnosed with it at the age of 5. However, I’ll get to the bumblefuck that was my ADHD treatment (or lack thereof for the past decade) in the next ramble. This one is to bridge the gap I mentioned in the last one.
As a brief recap, on March 23, 2018, I went in to have all of my teeth removed. This was required as a lifetime of one of my disease’s flare-ups mixed with a decade (around 16-20 to a week ago. More on that later.) of the issues of suddenly taken off medicine for your ADHD and forced to stay off it no matter how many damn doctors/shrinks/pill-shrinks you see explaining your symptoms causing the stress to increase and the flare-ups to become more frequent. The constant vomiting exacerbated an issue a sugary diet may have caused and utterly demolished my teeth little by little. However, thanks to complications from how infected these teeth had become (having been unable to do anything due to co-pay costs, then not having insurance, then Medicaid being a headache to find anyone to be able to get it fixed) which lead to a few hours of pulling, waiting, pulling, blah blah… I was referred to an oral surgeon.
Which is where the Health Insurance Shenanigans begins. I am quite familiar with these shenanigans, as they have been happening since I started. You see, the many different Nevada Medicaid healthcare providers who have insured me will have a list of the different doctors that will take your insurance. It sometimes might even claim to be able to tell you if they accept patients. This would be highly convenient if it did as it said. Instead, whenever I wanted to find a doctor, I would have to go down the list and call them one at a time. The moment Medicaid is mentioned, their tone sours ever so slightly. They tell you that, regardless of what the list on my provider’s own list says, they do not take Medicaid. The other constant was that if they DID, they were full on patients. If the did and they had openings, it is months down the line. When you need to find multiple specialists to deal with multiple issues caused by the same illness, this gets highly agitating. Frustrating as the ones I believed I could complain to like to assure me they understand it as. Why I do not believe them is they also seem surprised at how FUCKING PISSED OFF fucking up my health makes me.
Remember these shenanigans, I will be bringing them up often.
On March 6th, 2018 I received a letter from the allergist, who had been (poorly) helping me with my HAE care, that my care with them has suddenly been terminated. Now, I had only a few months prior FINALLY received from this doctor a pair of highly useful medications. In between the belittling, lecturing, and talking down to I got more than treatment, I finally was prescribed HAEGARDA and FIRAZYR. The first being a medication I WAS taking twice a week. It was rather painful for 15 minutes upon injection, but that cleared up quickly. The other was to be used in the event of swelling, injected like an Epipen (WHICH IT GOD DAMN ISN’T) might be at the moment of attack. With these two medicines, I had been comfortable enough to make my appointment with the dentist in the first place, which after a few appointments before I received the letter had been set for March 23rd.
Suddenly I received that letter, which was soon followed by the provider of the two medicines telling me my YEAR LONG PRESCRIPTIONS with them had suddenly been pulled. Something they were confused about, MUCH LIKE IS WAS. Upon calling my allergist’s office, I learned that the reason had been APPARENTLY I wasn’t taking it. Which is confusing, as I had been, and had only missed the one appointment before the letter thanks to the INFECTION IN MY GUMS I NEEDED REMOVED along with all the other damn issues I was having and trying to mix making me have troubles sleeping and making an early morning appointment. Something that I apparently need to suck up.
This reasoning SHOULD have been easily refuted by the constant deliveries of the medicine TO MY DOOR. The nurse that had come and taught me to use these medicines, THEIR APPROVAL THAT I KNEW WHAT I WAS DOING. As well me having sharps container with plenty of the injection needles I used. They did not wish for any of this, and after angry demands given I HAD A SURGERY APPOINTMENT for my teeth which has a DAMN HISTORY of causing swelling of the throat. So they extended it for 30 days, a bridge period, after constant calls that now just sit in my head like an angry flurry. Mixing them up, but the point is I had to FIGHT to make sure I had enough of the medicine for my blood disease so I could go through the dental procedure with the lost chance of a POSSIBLY FATAL flare-up. Fun.
So, once I was healed up after the dental appointment so I could start calling and get the bottoms removed… The Healthcare Shuffle appeared! This is when I tried to call the Oral Surgeon I was referred to, they said they never received it. I call the Dentist who sent it and they said they sent it to my insurance. I call my insurance and they first said they haven’t received it. Later say they do and sent it but the Oral Surgeon never got it. WHILE all this was happening, a far more problematic issue arose. Keep in mind, this is all happening as I am still getting over the fact I now have these annoying dentures that I am STILL angry over.
The medicine ran out. So, of course, I had to find someone new to prescribe me it. This had the issue of me needing to FIND someone who would do this. The Primary Care Physician that I had was uncertain himself and kept telling me he knew nothing about the disease. After explaining, he referred me to a Hematologist and Allergist… IN VEGAS. (This is 8 hours away from me on a good day or requires an hour and a half plane trip for something I likely need to do multiple times. I live in a city, not a small town. That has MANY ALLERGISTS AND HEMATOLOGISTS.)
Annoyed by this, and after Medicaid Shenanigans, I eventually got an Allergist and a Hematologist referral. Upon calling the Hematologist, they refused! I was highly confused, as they kept repeating that I should go to an allergist. They don’t treat allergies. Hereditary Angioedema is a blood disease. NOT an allergy. Apparently, nothing can be done and I have still yet to see a hematologist. Joy. The reason? Even though I explained extensively this was a genetic blood disease and the symptoms only could be COMPARED to an allergy to stress. IT DOES NOT REACT TO ALLERGY MEDS. An epipen makes the area I inject just swell up yet give me the energy for my skeleton to feel like it wants to run around the block without the rest of me.
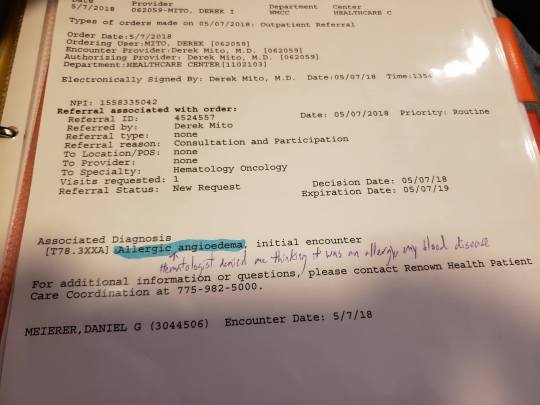
So, not surprising, this caused a lot of issues with swelling. Inevitably, I had an episode involving my gastrointestinal system. This time, it was bad enough I couldn’t seem to use medical marijuana to cover the symptoms until I was well and had water in me. So one Ambulance ride later I am in a hospital bed… Oh, wait, no, I am at the front desk of the emergency room waiting for a bed for a bit. Until I puke enough to be a disturbance. However it still takes quite a while before I get the main thing I want and have been kept from thanks to my body violently puking it up. I wanted an IV with something to hydrate me. The drugs could wait untiul the doctor, but as time went by and it felt like an eternity, I kept being told by all the people checking on me that I had to wait for a doctor to get my damn liquid.
All the while my fiance and my father are both helping explain that this was, without any doubt, an attack from my blood disease. It was an hereditary angioedema attack, blah blah… My discharge papers (useful in tracking my disorder and proving problems.) instead say it is some ‘unspecified vomiting type’ instead of maybe ‘blood disease triggered vomiting’ or ‘HAE triggered vomiting’, ‘genetic disorder triggered vomiting’. Think you get the point, more something that proved the medical staff were actually listening to my concerns. Attempts to fix this so I had proof with disability was met with them saying once that is written down it is permanent.
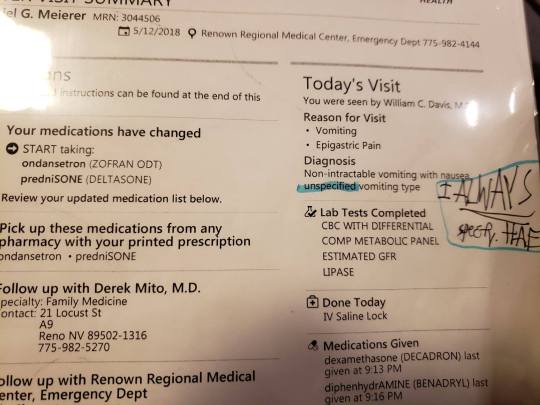
Then, five months later, it happened again.

Luckily, the Allergist I eventually found turned out to actually have heard and seen a couple others who had this disorder. He knew of medicines and, instead of feeling like I needed to teach my doctors… I was given hope! I was given a vial of Firazyr. He said it was extending an olive branch, and I feel this will be what I remember when I try to think of the emotions needed to write a scene similar. I have never felt hope like I have then. Hope that likes to come and go, but at least I have one doctor at-bat for me.
Until a couple of months ago as of March 20th, 2019, I FINALLY was put on a new medication. Tahkzyro which I take twice a month. HOWEVER, I am still getting push back when it comes to getting the Firazyr, which would help me with my anxiety over the next surgery to remove my bottoms. Which, now that I have Tahkzyro, I once more have to take on HealthCare shenanigans to try and figure out who gets the god damned honor of removing my teeth. As the ones I was referred to HAVE the damn referral… But they don’t take Medicaid. SEEMS THE INFECTION IN MY BOTTOM TEETH GETS TO STAY! Just get to keep draining that thing myself. GUESS WE ARE FRIENDS FOREVER, ME AND THIS INFECTED TOOTH! Though it is crumbling away like the rest. It is down to the gums now. Though, I would like the Firazyr so I can inject myself IMMEDIATELY upon noticing my throat swelling. Never been asphyxiated but something tells me it ISN’T ALL THE FUN AN END! Especially at twenty fucking eight. So you can see my troubles. That doctor is still great, and makes a good point, I just think I need to make myself a bit clearer.
The years feel like they become less and less about me finding my place in this world, healing, and learning but instead more and more about me working as quality control for a broken system with no desire to fix itself. With every passing event involving them, I feel less like a patient and more like the data point I clearly am. With articles full of professionals professionally talking about diseases and medicines without much mention or care for the patients. The ones who that was made for.
For patients like me to heal. Not for people to make money. That is a side-effect of the job they signed up for. To fucking CARE for your goddamn patients. Not be coerced into giving meds left and right (or taking them away as a debate on whether or not ADHD FUCKING EXISTS goes on) or whether you believe the name given to the collection of symptoms I show. My disorders are not Cryptids. I have blood tests, medical papers, and diagnoses. Not blurry pictures of my blood viewed through a slide where fragments of the disease are seen peeking over their shoulder as they rush into a forest of red blood cells.
My particular disorders that I had since birth (ADHD and HAE) were caused by my body’s INABILITY to produce something. So if someone who CAN produce it takes it (least in the sense of ADHD as I doubt anyone else will benefit from a c1-inhibitor. No more than insulin if they aren’t in need of it like a diabetic) then of COURSE something different will happen. Of course, they might get high. That is not my fault as the patient it was made for.
As the point I am trying to make is that I do not feel I have been treated as a patient, I feel I am given more paperwork and calls than a cubicle worker. I feel I have to study more about the laws and practices to keep myself from being further burned. In between the Madness. The Pain. The Suffering that ALL OF THIS has inflicted on me. In between the new disorders this has caused me, particularly my obsession.
All I can think of is how to fix this. How I keep seeing articles, posts, and websites full of cries for help at a broken system. Of people fucked over, lacking their medicine, and the only ones getting the fucking attention are the dipshits who thought that taking someone else’s necessity would be a good way to get high. A good way to ‘focus’. To ‘relax’. While you use that as a fucking excuse to let people like me suffer, and further excuse it by brushing us into a group of people who just ‘slipped through the cracks’.
This obsession has grown now. Especially from the subject of the next article, ADHD meds from the perspective of someone who was one them from the age of 5, had them taken somewhere between the ages of 16 and 20 (my memory is incredibly hazy in this period thanks to the damn medicine being taken away) and getting only mild relief from marijuana replenishing my Dopamine… But that isn’t all Marijuana does nor all ADHD needs. I FINALLY am being treated, though it is just beginning. Still need to find MY medicine. It only took a decade for them to admit they were screwing with me. The lengths of my rage, again, is the subject of the next article.
This one was about how this madness turned me into someone who believes his job is to be a Professional Patient. Being talked into long commutes, long waits waiting for a doctor who will drop you for being late when they are constantly 45 to an hour late. Constantly filling out paperwork and debating about the fact my problems EXIST. Being treated as too young to be suffering. To the point, I don’t know what else to do. When you are too fucked up to work, explained in an earlier article, too fucked around for college, and the only thing you can apparently do is smash your rage against a keyboard and hope spreading your story around for no one to read will get something done.
If not? Then no matter what happens. If I die from malpractice or my disease, if I am killed, if I am silenced. My words on how this bullshit has made me feel will be, hopefully, somewhere.
The internet is notorious for being difficult to clean thoroughly, after all. If you do a little light digital legwork with the intention of being annoying as all hell. Especially since I got denied for disability again. Next time, I have to go to federal court apparently. JOLLY GEE GOODIE.
#nonfiction#Medicaid#Hereditary Angioedema#genetics and heredity#disability#us healthcare#us health insurance#reno#renown#suffering#blood disease#disease#rant#medical malpractice
1 note
·
View note
Text
Fic Ideas 1-5
Note: Not all ideas are complete and will cut off at random times.
Note 2: Some are rather long and detailed.
Holby City
1.
Bernie comes back from Ukraine and just goes straight to Serena’s house and lets herself in. She’s aware that Jason has chess club that night and wont be home for a long time. She’s also aware that Serena will be home soon.
So, after dropping her duffel bag in the coat closet, she goes to the kitchen and set about cooking the pasta she knows Serena always has in the pantry.
It’s as she’s dishing up when the lights of a car pulling up tell her hat Serena’s home. Suddenly she’s overwhelmed by nerves and just stands in the middle of the kitchen waiting for Serena to walk in.
2. Teach Me to Love - Teacher AU
“You’re my kids teacher and I’m late to pick them up and panicking but I find you teaching them how to make origami swans and shit man, I’ve been pining forever but now I’m in too deep.” - Prompt used
Bernie’s running late to pick up Cameron and finds ‘Pretty Ms Campbell’- as he likes to call her - teaching him to make paper swans as they sit at the table in front of the main entrance of the school. She just falls into the seat across from them with a sigh and sweet little Cameron asks if she’s late because of Dad and when she says no, he asks if it’s because of Alex.
She tries so hard to hide her surprise and tells him that yes it was because she was saying goodbye to Alex - because she was going back on tour - and Cameron passes her a badly made swan and says that she’ll find someone else to love, but for now she has him and Beaky (The swan).
Which is how Serena finds out that Bernie and Marcus are divorcing because Bernie fell in love with her best friend while on tour and then fell out of love with her once they realised Alex wasn’t prepared for everything that came with her being retired from the army and a mother.
3. Sharing is Caring
Sharing skills and talents with your soulmate. - Prompt
It’s little things at first, like the skill to make the perfect cuppa - Bernie can suddenly make one perfectly for anyone who asks, something that she’s thankful for because everyone used to say it was like drinking pixie piss.
Serena can get that perfect crease down the centre of her pants leg.
And as they grow closer, it moves to larger things.
Serena can now cook a perfect roast and veggies.
Bernie can organise anything without really having to think about it.
And then one day, Bernie bunks off doing her paperwork and ends up doing a detailed sketch of Serena as she sits across from her, doing her own work.
And Bernie just drops the pen when done and sits back with a “Huh.”
And Serena looks up, “What’s up?”
“My soulmate can draw.”
“How do you know?”
“Because I can now.”
“Oh?” She asks, waiting for further explanation.
And when Bernie hesitates, she gets up and walks around, snagging the paper Bernie hurriedly tries to hide.
“Oh Bernie.”
Serena stares at the picture, taking everything in before turning the the now blushing blonde.
“You couldn’t leave some of the lines off my face?” She asks teasingly.
Bernie lets out a bark of laughter.
“Seriously though Bernie, this is wonderful.”
“Keep it.”
Smiling, Serena turns to face her friend fully, “I’d love to, but I can’t.”
“Oh?” Bernie tries so hard to keep the disappointment from her voice.
“It’s on the back of a patients notes.” Serena says, spinning the page around to show Bernie.
Bernie can only stare at them for a while before uttering, “Bugger.”
Serena laughs and puts the page back down, “That’s going to be a surprise for the next person to look at the hard copy of these notes.”
Bernie sighs, “Sorry.”
Shaking her head, Serena rubs her shoulder, “Don’t worry about it, the last portrait of me was painted over.” She says before moving back to her desk.
And of course Bernie can’t leave that statement alone and gets the story of the reverend falling in love with her out of Serena.
The next night they’re at Albies and Serena drunkenly sits at a piano she’d never noticed before and just starts playing.
Her fingers hurt afterwards because it was a long piece, something she didn’t even know, but she’s so happy because she’s always wanted to play the piano but could never convince her parents for lessons.
One day a trauma patient comes in and Serena’s the only surgeon available, except she has no experience with the surgery required to save the child’s life.
She knows Bernie does and is about to have someone call her in when suddenly she hears Bernie’s voice in the back of her head saying, “You can do this Serena.” And suddenly everything is there, the entire procedure. She performs the surgery and the entire time, she feels as though Bernie’s guiding her, would swear that the blonde was standing just behind her, hands moving along with hers.
She comes out of theatre and changes back into her clothes on autopilot and goes home as her shift had ended an hour into the operation.
She does everything by routine and doesn’t remember any of it, she just knows she’s in her bed, needing to sleep, but she can’t because Berenice Bloody Wolfe is her soulmate.
Bernie comes in the next day, and tells Serena about the dream she had where she was showing Serena how to do a ridiculously complex surgery and Serena laughs it off, having already realised what had happened, but following along with Bernies idea to keep it confined to theatre.
That is until Morven tells Bernie all about how brilliant Serena was in theatre the day before.
And when Bernie asks for clarification, Morven jumps at it and goes into detail and Bernies frowning as the story continues and by the end of it, she looks to Serena, who had just ducked into their office and follows.
The first words out of her mouth after closing the door is, “You’ve never performed that surgery before. You barely know how to do it.”
“I didn’t need to know,” Serena whispers, looking up from her clasped hands, “You did.”
4.
While Bernie’s away Serena falls into her depression, though not as bad as the first time, but it does add to her stress of suddenly having to run the ward and the trauma unit by herself, as well as dealing with Jason’ strict schedule.
As such, she starts scratching in her sleep, and then whenever she thinks about Bernie. She does so so much that she manages to reopen some of her scars on her back, though she doesn’t realise at first so she doesn’t take care of them and they get infected.
It gets to the point where it causes pain so she finally asks Raf to have a look at her back to see why.
“Have you been scratching them Serena?” He asks, frowning at the res lines surrounding the open wounds.
“They’ve been itchy for the last couple of days.”
“I’m not surprised, you’ve scratched them open and they’re infected.”
Serena sighs and drops her head, “Just what I need.”
Raf smiles sympathetically and pats her shoulder, “I’ll write up a prescription of antibiotics for you.”
Serena sighs, shrugging back into her shirt, “Thank you.”
A week later Rafs checking on them again in the privacy of her office when in walks Bernie, in search of Serena. She freezes at the sight of Serena with her shirt off and Raf with his hands on her shoulders.
Spinning at the sound of the door opening, Serena covers her front with her blouse and glares, “Ever heard of knocking?”
5. Star Wars AU
In a world where being a Jedi means giving up any notions of falling in love, one Master must fight to stay focused on the mission, if only said mission wasn’t protecting the Senator and Healer of Holby Medical Station, Seréna, one of the last human healers.
Senator Seréna wasn’t one for worrying about the many threats against her life until she received one from the brother of a patient she couldn’t save in the shape of the destruction of her convoy. Now she must be guarded by one of the best Jedi Knights, Master Wolfe. Now if only she could focus on the debate she is to speak at and not the messy curls of her guard.
45 notes
·
View notes
Text
Readers and Tweeters Grapple With COVID Therapies and Forecasts
Letters to the Editor is a periodic feature. We welcome all comments and will publish a selection. We edit for length and clarity and require full names.
Giving Convalescent Plasma a Shot
Used to effectively treat mumps, measles, and even the so-called Spanish flu in 1918, convalescent plasma may not be a silver bullet, but it still has the potential to play an important role in helping some patients recover from COVID-19 (“5 Things to Know About Convalescent Blood Plasma,” Aug. 27).
To support its recent decision, the Food and Drug Administration used data from previous use cases of convalescent plasma for other respiratory coronaviruses, results of early safety and efficacy trials in animal models, and published studies on the safety and efficacy of convalescent plasma before issuing Emergency Use Authorization (EUA). The agency also pointed to a Mayo Clinic preliminary analysis of 56,000 patients who were given high or low titer units of blood plasma.
The EUA also specifies that donor blood can be released only to hospitals and patients after it is tested with a currently available antibody test that accurately detects the right type of antibodies to neutralize the virus and confirms that the blood contains sufficient levels of these antibodies for treatment purposes. This means that less accurate, less specific tests that are more susceptible to false positives will not be used to identify COVID-19 convalescent plasma — something that should give patients higher confidence that the plasma they receive meets scientific and quality standards.
— Dr. Fernando Chaves, a board-certified hematopathologist who serves as Global Head of Medical and Scientific Affairs at Ortho Clinical Diagnostics, Raritan, New Jersey
I’m quoted here saying what everybody already knows: if we want to know if plasma works, we need a trial.
This isn’t academic for me: I want to know if I should be using plasma in my patients with severe COVID-19. This fiasco was preventable. https://t.co/MjS2DXbYUX
— Adam W Gaffney (@awgaffney) August 28, 2020
— Dr. Andrew Gaffney, Boston
Vaccination and Prognostication
Both assertions that seniors will drive 800 miles or come home from an assisted living or skilled nursing facility to live with families are dubious (“What Seniors Can Expect as Their New Normal in a Post-Vaccine World,” Aug. 3). The latter are need-based moves (think dementia, wandering). The former makes sense for those who won’t tolerate the physical strain of long car rides — think Florida to D.C.
— Laurie Orlov, Aging and Health Technology Watch, Port St. Lucie, Florida
I wonder if many of these predictions are more likely to be true among those who have personal experience with COVID-19, either through personal experience with illness or loss of family or friends. https://t.co/uRZnuSfFLf via @khnews
— Rosemary Wright, PhD (@rwrightphd) August 3, 2020
— Rosemary Wright, Wichita, Kansas
I don’t want these precautions to last forever. I want there to be a time where we can all give each other hugs and high fives again. We were built to be together and celebrations bring us so much joy. I want there to be a time when we can all be in fun crowds again. I want to be able to smile out in public again and not have to cover my face. What do you think about all of this?
— Christopher DeCarlo, Oyster Bay, New York
We won’t go back to “the way things were” even after a vaccine for #COVID19 has been invented. This experience has been an opportunity to innovate and do better. Here are some changes you’re likely to see in #healthcare and beyond. https://t.co/l4x50qVxvM
— Tony Slonim MD, DrPH (@RenownCEOTonyMD) August 8, 2020
— Dr. Tony Slonim, Reno, Nevada
Humans as Guinea Pigs for the Sake of Corporate Piggy Banks?
We assume that this vaccine works, but how do we know (“They Pledged to Donate Rights to Their COVID Vaccine, Then Sold Them to Pharma,” Aug. 25)? The public is not some testing animal. I would not take this vaccine, especially since the back-and-forth is over money and not public health. No government should give any money to a business without a deal that protects the public as investors. We are not a source of free money; just as they make no concessions, we also should make no concessions without a deal. And the deal is public health.
There was no vaccine during the 1918-19 influenza, not until 1940. Our immune system needs to be considered as part of a cure. Is that not the theory behind flu shots? So, if we are exposed to the virus and allow our bodies to fight it off, that defense is greater than any vaccine. Those who cannot fight off the infection are the ones who need to be considered for medical attention — and not just some shot hopefully manufactured by a company that does not prioritize money over health.
There are times when profit is important, but since businesses are being subsidized, this is not one of those times. The world economy has been seriously affected, and printing money we do not have is not a sound idea. What good are medicine and doctors and medical research? Seems we should consider those old grandma medications, such as the hot toddy … whiskey and hot coffee and a good night to sweat it out under many covers. That cured my grandfather of influenza long before there was a vaccine.
Medical science doesn’t have all the answers. If soap can kill this coronavirus, then there must be a common household solution to eradicate it that is medically safe for humans. Perhaps technology students would do better to help the world instead of these money-hungry corporations.
— Tom Berger, Suffolk County, New York
Volunteers risk their lives in clinical trials, and the Oxford converted vaccine from public good to profitable commodity? …
They Pledged to Donate Rights to Their COVID Vaccine, Then Sold Them to Pharma https://t.co/vQw94BfxKE via @khnews
— Amar Jesani (@amarjesani) August 31, 2020
— Amar Jesani, Mumbai, India
On COVID Tests and Risk
I have worked in a clean lab for many decades. I know how to behave and how to take advantage of and handle PPE, for the purpose of achieving very low contamination levels. The article “Analysis: When Is a Coronavirus Test Not a Coronavirus Test?” (July 29) presents a false option. It is not about accepting a level of risk, it is about doing everything possible to reduce the risk.
In my labs, I had the ability to require adherence to careful procedures and the option to fire anyone who would not follow approved procedures. I don’t have that option with those who refuse to follow the simple instructions for COVID-19, including the “religious” wearing of a mask, the same way that women cover their heads when entering a Catholic church and Jewish men wear a yarmulke in a temple.
And when the president irresponsibly and criminally refuses to follow and to mandate simple instructions by medical experts, then I am unable to calculate the risk. I don’t think Ms. Rosenthal can calculate the level of risk she suggests we accept.
— Dimitri Papanastassiou, Pasadena, California
I enjoyed your piece, but I regret that you said so little about therapies that may emerge to help us. Vaccines are not the only hope. I think a disservice is being done by indicating that our only options are to live with it or wait for a vaccine.
— John Van Drie, North Andover, Massachusetts
Great article by @ahartreports. I too cringed initially at likening #covid19 to war but couldn't agree more that we need to treat our #PublicHealthOfficials with respect and be grateful for their sacrifices https://t.co/rr9NT4tNlB via @khnews
— Meghan McGinty, PhD (@Breukelen299) September 1, 2020
— Meghan McGinty, Brooklyn, New York
The Hydroxy Paradox
Wouldn’t it be refreshing, instead of slamming other doctors’ practical experience with hydroxychloroquine at low dosages and supplemented with zinc, etc. at the first sign of the infection, to at least let them make fools of themselves (“Don’t Fall for This Video: Hydroxychloroquine Is Not a COVID-19 Cure,” July 31)? What is the harm?
Aren’t “we all in this together”? Why are we afraid of a difference in opinion? What if it really works using the protocols as stated? Let it play out. Pretty sure no one has died when prescribed “hydroxy” in low dosages by doctors in actual practice, unlike the deaths that occurred when given in massive dosages late in the infection.
Why make fun of doctors who are trying their best to help us all? That seems narrow-minded to me.
— Larry Koch, Agoura Hills, California
Reported this tweet. You are encouraging the use of a medication a. Without a license b. Without citing sources and c. Every double blind study has shown and increase in death.https://t.co/iN7eionH03https://t.co/eSPDwPz9V6
— Tara Tisch🦓🍀🎨🏴☠️ (@TaraTisch) August 22, 2020
— Tara Tisch, Peoria, Illinois
I know you disagree with Dr. Stella Immanuel, and that’s OK. The problem I have is that no one has done the clinical trials to prove that hydroxychloroquine doesn’t work. She said she has 350 patients who have had success with her prescriptions; the doctor from Dallas said she uses it with her own little concoction. If, in fact, what they are doing is working, then why don’t people visit these doctors to see if it is true — and, if it is, then try collaborating with them to keep people from dying, for crying out loud.
That is one of the problems here: Everyone is against one another instead of trying to support one another. We are Americans and, as in years past, we have stuck together for the betterment of the country. If we would stop trying to take care of America with money and start taking care of America with information, then America would live and thrive.
I am a first-year respiratory therapy student and spent 20 years in the Marine Corps, and back in the ’80s we took chloroquine, and I have no side effects and neither do the guys I stay in contact with. Keep in mind that the reports of the side effects are not in every patient and if hydroxychloroquine is offered to a patient and the patient is told, “This is going to make you better but there could be side effects later, but if you don’t take this you will get worse and we don’t know if you will die or not,” what do you think they will say? No one wants to die.
C’mon, let’s just be people trying to keep other people alive no matter the cost, no matter who is right or wrong — we can sort that out later.
— Jim Tumlinson, Canyon Lake, Texas
Editor’s note: A recent report from the Centers for Disease Control and Prevention expressed caution and concern that hydroxychloroquine was potentially being misused to treat COVID-19 and affecting supplies of the medication to treat rheumatoid arthritis, lupus and other conditions. “Current data on treatment and pre- or postexposure prophylaxis for COVID-19 indicate that the potential benefits of these drugs do not appear to outweigh their risks,” it said.
Yoga for All
I appreciate your article (“Namaste Noir: Yoga Co-Op Seeks to Diversify Yoga to Heal Racialized Trauma,” July 30) but have a hard time with “people of color” being repeated over and over. Yoga benefits all people, and until we start thinking as one and not labeling everything we will always have racial issues. We need to think all lives matter, not just a specific color. Thank you for your writings.
— Susan Ferguson, Cypress, California
"Namaste Noir" ?????????? good and important article, but really, really poor headline choice @KHNews https://t.co/GefI9Zkoy8
— Eli Imadali (@eliimadaliphoto) August 9, 2020
— Eli Imadali, Denver
#Namaste. Yoga and meditation are helping Ms. Grant deal with COVID-19, the loss of her son and racial stress. Lots of lessons here for all of us. @KHNews #Equality https://t.co/GnxZn4l7QF
— Jimmy Etheredge (@JimmyEtheredge) August 14, 2020
— Jimmy Etheredge, Atlanta
Words That Carry Weight
Thank you for calling attention to the challenges people with obesity face regarding risks of COVID-19 infections and the potential that vaccines may not be effective (“America’s Obesity Epidemic Threatens Effectiveness of Any COVID Vaccine,” Aug. 6). I would like to comment on how you refer to people with obesity. The Obesity Action Coalition, and other organizations focused on obesity, recommend using people-first language. An article about cancer does not refer to cancer people, nor does one on cardiovascular disease label individuals as heart disease people. The terms “obese people” and “morbid obesity” are stigmatizing. It is better to utilize people-first language as Dr. Timothy Garvey did at the end of the article. As a member of the Obesity Medicine Association as well as an obesity medicine specialist and educator, I work diligently with patients to overcome the bias and stigma that society imposes. Please be considerate of the use of language when referring to people with obesity.
— Dr. Nicholas Pennings, Raleigh, North Carolina
It is becoming more & more obvious that we would‘ve “saved” FAR more lives here if we had put all the mask shaming energy into getting people to lose weight. But that would be un-PC.
America’s Obesity Epidemic Threatens Effectiveness of Any COVID Vaccine https://t.co/wfbUz9JSB9
— John Ziegler (@Zigmanfreud) August 10, 2020
— John Ziegler, Los Angeles
As a sociologist researching weight stigma, I am appalled by the article by Sarah Varney suggesting obesity will undermine vaccine effectiveness. The article is full of stereotypes and misinformation. In the first place, it is Big Pharma’s fault vaccines aren’t made for fat people. It is beyond incompetence that any vaccine drugmakers come up with would be less effective for half the population. In the second place, many of the diseases fat folk allegedly have are caused by yoyo dieting and stigma. And there is no proof weight loss would make any vaccines more effective as most fat people are biochemically different than thin ones. This is a tone-deaf, fat-phobic article that serves only corporate interests.
— Sherie Sanders, Springfield, Illinois
Jail Outbreaks
My life and those of others are being put in danger by the San Bernardino County Sheriff’s Department (“COVID Runs Amok in 3 Detroit-Area Jails, Killing At Least 2 Doctors,” July 23). I’m in jail with health issues: asthma, prediabetes, vitamin D deficiency, high blood pressure, and may have a cancerous tumor and peripheral neuropathy. I’ve already been put on quarantine two times, once because a deputy who tested positive for COVID-19 had direct contact with me and the other because they put someone in the cell with me who was symptomatic for COVID-19. When being transported anywhere, they put chains on us that have been on many people and have not been cleaned. Then they chain multiple people together, not even knowing if a person has or is a carrier of the coronavirus. The social distancing was put in effect to protect the lives of people. The sheriff’s department is violating it, putting lives in danger and will continue to do so until they are stopped. To top it off, I am state property and not even supposed to be here. I don’t want to die or see anyone else die for being in jail and catching COVID-19. So can someone please help us all.
— LeAire Moore Sr., Adelanto, California
Lots of people ask me why I stay home most of the time, mask up, wash my hands, socially distance.
Why should I? I’m young. I’m healthy. I work out and eat right.
But, I have a mother.
This is why. ⬇️https://t.co/IlKPXmTu65
— Samuel Cook, III | CPT, CNC, USAW (@samueljcookiii) September 6, 2020
— Samuel Cook III, New Orleans
Correcting the Record on the Navajo Language
The article “Two Navajo Sisters Who Were Inseparable Died of COVID Just Weeks Apart” (Aug. 26) is incorrect. The Navajo language is most certainly “written down” and is taught in schools and universities.
— Randy Truman, Albuquerque
Editor’s note: Thanks for helping us clarify that point. The article has been updated.
Medicaid Expansion in the Age of COVID
The COVID-19 pandemic has shown us that Americans are in desperate need of health insurance, including publicly financed health insurance programs such as Medicaid. The time is now for some policymakers in America to reshape how they think of Medicaid as more than a government handout that makes us worse and not better.
Medicaid is a health insurance program that is jointly funded by the state and federal government. This program provides low-cost insurance to adults with low income, both young and elderly, pregnant women, the disabled and children through the Children’s Health Insurance Program, commonly known as the CHIP program.
The Affordable Care Act provided an opportunity for states to expand coverage to individuals at 138% of the federal poverty level. As an added incentive, the federal government pledged to pay 100% of the costs to expand, a share that would be reduced to 90% by 2020. In recent months, states such as Oklahoma and Missouri through the ballot box have expanded Medicaid. This leaves only 12 states to not expand, but millions more in need of affordable health insurance.
The argument by some policymakers against the Medicaid program is the fear of incentivizing Americans to not work. Contrary to this belief, in 2017, it was reported that more than 63% of Medicaid recipients are already in the workforce while only 7% were not working for various reasons.
Finally, since the beginning of the pandemic, one study estimated that nearly 27 million Americans could lose their employer-sponsored insurance this year. Of those 27 million, nearly 13 million would be eligible for Medicaid.
The American people deserve to have affordable health insurance. Therefore, policymakers have an obligation to expand it and not contract.
— Reginald Parson, Portland, Maine
This is happening right now throughout our system and its utterly disgusting and unacceptable.
Health Care Workers of Color Nearly Twice as Likely as Whites to Get #COVID-19 https://t.co/1VOFQid8mM via @khnews
— Stephen Ferrara, DNP (@StephenNP) August 6, 2020
— Stephen Ferrara, New York City
Kaiser Health News (KHN) is a national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation which is not affiliated with Kaiser Permanente.
USE OUR CONTENT
This story can be republished for free (details).
Readers and Tweeters Grapple With COVID Therapies and Forecasts published first on https://nootropicspowdersupplier.tumblr.com/
0 notes
Text
Readers and Tweeters Grapple With COVID Therapies and Forecasts
Letters to the Editor is a periodic feature. We welcome all comments and will publish a selection. We edit for length and clarity and require full names.
Giving Convalescent Plasma a Shot
Used to effectively treat mumps, measles, and even the so-called Spanish flu in 1918, convalescent plasma may not be a silver bullet, but it still has the potential to play an important role in helping some patients recover from COVID-19 (“5 Things to Know About Convalescent Blood Plasma,” Aug. 27).
To support its recent decision, the Food and Drug Administration used data from previous use cases of convalescent plasma for other respiratory coronaviruses, results of early safety and efficacy trials in animal models, and published studies on the safety and efficacy of convalescent plasma before issuing Emergency Use Authorization (EUA). The agency also pointed to a Mayo Clinic preliminary analysis of 56,000 patients who were given high or low titer units of blood plasma.
The EUA also specifies that donor blood can be released only to hospitals and patients after it is tested with a currently available antibody test that accurately detects the right type of antibodies to neutralize the virus and confirms that the blood contains sufficient levels of these antibodies for treatment purposes. This means that less accurate, less specific tests that are more susceptible to false positives will not be used to identify COVID-19 convalescent plasma — something that should give patients higher confidence that the plasma they receive meets scientific and quality standards.
— Dr. Fernando Chaves, a board-certified hematopathologist who serves as Global Head of Medical and Scientific Affairs at Ortho Clinical Diagnostics, Raritan, New Jersey
I’m quoted here saying what everybody already knows: if we want to know if plasma works, we need a trial.
This isn’t academic for me: I want to know if I should be using plasma in my patients with severe COVID-19. This fiasco was preventable. https://t.co/MjS2DXbYUX
— Adam W Gaffney (@awgaffney) August 28, 2020
— Dr. Andrew Gaffney, Boston
Vaccination and Prognostication
Both assertions that seniors will drive 800 miles or come home from an assisted living or skilled nursing facility to live with families are dubious (“What Seniors Can Expect as Their New Normal in a Post-Vaccine World,” Aug. 3). The latter are need-based moves (think dementia, wandering). The former makes sense for those who won’t tolerate the physical strain of long car rides — think Florida to D.C.
— Laurie Orlov, Aging and Health Technology Watch, Port St. Lucie, Florida
I wonder if many of these predictions are more likely to be true among those who have personal experience with COVID-19, either through personal experience with illness or loss of family or friends. https://t.co/uRZnuSfFLf via @khnews
— Rosemary Wright, PhD (@rwrightphd) August 3, 2020
— Rosemary Wright, Wichita, Kansas
I don’t want these precautions to last forever. I want there to be a time where we can all give each other hugs and high fives again. We were built to be together and celebrations bring us so much joy. I want there to be a time when we can all be in fun crowds again. I want to be able to smile out in public again and not have to cover my face. What do you think about all of this?
— Christopher DeCarlo, Oyster Bay, New York
We won’t go back to “the way things were” even after a vaccine for #COVID19 has been invented. This experience has been an opportunity to innovate and do better. Here are some changes you’re likely to see in #healthcare and beyond. https://t.co/l4x50qVxvM
— Tony Slonim MD, DrPH (@RenownCEOTonyMD) August 8, 2020
— Dr. Tony Slonim, Reno, Nevada
Humans as Guinea Pigs for the Sake of Corporate Piggy Banks?
We assume that this vaccine works, but how do we know (“They Pledged to Donate Rights to Their COVID Vaccine, Then Sold Them to Pharma,” Aug. 25)? The public is not some testing animal. I would not take this vaccine, especially since the back-and-forth is over money and not public health. No government should give any money to a business without a deal that protects the public as investors. We are not a source of free money; just as they make no concessions, we also should make no concessions without a deal. And the deal is public health.
There was no vaccine during the 1918-19 influenza, not until 1940. Our immune system needs to be considered as part of a cure. Is that not the theory behind flu shots? So, if we are exposed to the virus and allow our bodies to fight it off, that defense is greater than any vaccine. Those who cannot fight off the infection are the ones who need to be considered for medical attention — and not just some shot hopefully manufactured by a company that does not prioritize money over health.
There are times when profit is important, but since businesses are being subsidized, this is not one of those times. The world economy has been seriously affected, and printing money we do not have is not a sound idea. What good are medicine and doctors and medical research? Seems we should consider those old grandma medications, such as the hot toddy … whiskey and hot coffee and a good night to sweat it out under many covers. That cured my grandfather of influenza long before there was a vaccine.
Medical science doesn’t have all the answers. If soap can kill this coronavirus, then there must be a common household solution to eradicate it that is medically safe for humans. Perhaps technology students would do better to help the world instead of these money-hungry corporations.
— Tom Berger, Suffolk County, New York
Volunteers risk their lives in clinical trials, and the Oxford converted vaccine from public good to profitable commodity? …
They Pledged to Donate Rights to Their COVID Vaccine, Then Sold Them to Pharma https://t.co/vQw94BfxKE via @khnews
— Amar Jesani (@amarjesani) August 31, 2020
— Amar Jesani, Mumbai, India
On COVID Tests and Risk
I have worked in a clean lab for many decades. I know how to behave and how to take advantage of and handle PPE, for the purpose of achieving very low contamination levels. The article “Analysis: When Is a Coronavirus Test Not a Coronavirus Test?” (July 29) presents a false option. It is not about accepting a level of risk, it is about doing everything possible to reduce the risk.
In my labs, I had the ability to require adherence to careful procedures and the option to fire anyone who would not follow approved procedures. I don’t have that option with those who refuse to follow the simple instructions for COVID-19, including the “religious” wearing of a mask, the same way that women cover their heads when entering a Catholic church and Jewish men wear a yarmulke in a temple.
And when the president irresponsibly and criminally refuses to follow and to mandate simple instructions by medical experts, then I am unable to calculate the risk. I don’t think Ms. Rosenthal can calculate the level of risk she suggests we accept.
— Dimitri Papanastassiou, Pasadena, California
I enjoyed your piece, but I regret that you said so little about therapies that may emerge to help us. Vaccines are not the only hope. I think a disservice is being done by indicating that our only options are to live with it or wait for a vaccine.
— John Van Drie, North Andover, Massachusetts
Great article by @ahartreports. I too cringed initially at likening #covid19 to war but couldn't agree more that we need to treat our #PublicHealthOfficials with respect and be grateful for their sacrifices https://t.co/rr9NT4tNlB via @khnews
— Meghan McGinty, PhD (@Breukelen299) September 1, 2020
— Meghan McGinty, Brooklyn, New York
The Hydroxy Paradox
Wouldn’t it be refreshing, instead of slamming other doctors’ practical experience with hydroxychloroquine at low dosages and supplemented with zinc, etc. at the first sign of the infection, to at least let them make fools of themselves (“Don’t Fall for This Video: Hydroxychloroquine Is Not a COVID-19 Cure,” July 31)? What is the harm?
Aren’t “we all in this together”? Why are we afraid of a difference in opinion? What if it really works using the protocols as stated? Let it play out. Pretty sure no one has died when prescribed “hydroxy” in low dosages by doctors in actual practice, unlike the deaths that occurred when given in massive dosages late in the infection.
Why make fun of doctors who are trying their best to help us all? That seems narrow-minded to me.
— Larry Koch, Agoura Hills, California
Reported this tweet. You are encouraging the use of a medication a. Without a license b. Without citing sources and c. Every double blind study has shown and increase in death.https://t.co/iN7eionH03https://t.co/eSPDwPz9V6
— Tara Tisch🦓🍀🎨🏴☠️ (@TaraTisch) August 22, 2020
— Tara Tisch, Peoria, Illinois
I know you disagree with Dr. Stella Immanuel, and that’s OK. The problem I have is that no one has done the clinical trials to prove that hydroxychloroquine doesn’t work. She said she has 350 patients who have had success with her prescriptions; the doctor from Dallas said she uses it with her own little concoction. If, in fact, what they are doing is working, then why don’t people visit these doctors to see if it is true — and, if it is, then try collaborating with them to keep people from dying, for crying out loud.
That is one of the problems here: Everyone is against one another instead of trying to support one another. We are Americans and, as in years past, we have stuck together for the betterment of the country. If we would stop trying to take care of America with money and start taking care of America with information, then America would live and thrive.
I am a first-year respiratory therapy student and spent 20 years in the Marine Corps, and back in the ’80s we took chloroquine, and I have no side effects and neither do the guys I stay in contact with. Keep in mind that the reports of the side effects are not in every patient and if hydroxychloroquine is offered to a patient and the patient is told, “This is going to make you better but there could be side effects later, but if you don’t take this you will get worse and we don’t know if you will die or not,” what do you think they will say? No one wants to die.
C’mon, let’s just be people trying to keep other people alive no matter the cost, no matter who is right or wrong — we can sort that out later.
— Jim Tumlinson, Canyon Lake, Texas
Editor’s note: A recent report from the Centers for Disease Control and Prevention expressed caution and concern that hydroxychloroquine was potentially being misused to treat COVID-19 and affecting supplies of the medication to treat rheumatoid arthritis, lupus and other conditions. “Current data on treatment and pre- or postexposure prophylaxis for COVID-19 indicate that the potential benefits of these drugs do not appear to outweigh their risks,” it said.
Yoga for All
I appreciate your article (“Namaste Noir: Yoga Co-Op Seeks to Diversify Yoga to Heal Racialized Trauma,” July 30) but have a hard time with “people of color” being repeated over and over. Yoga benefits all people, and until we start thinking as one and not labeling everything we will always have racial issues. We need to think all lives matter, not just a specific color. Thank you for your writings.
— Susan Ferguson, Cypress, California
"Namaste Noir" ?????????? good and important article, but really, really poor headline choice @KHNews https://t.co/GefI9Zkoy8
— Eli Imadali (@eliimadaliphoto) August 9, 2020
— Eli Imadali, Denver
#Namaste. Yoga and meditation are helping Ms. Grant deal with COVID-19, the loss of her son and racial stress. Lots of lessons here for all of us. @KHNews #Equality https://t.co/GnxZn4l7QF
— Jimmy Etheredge (@JimmyEtheredge) August 14, 2020
— Jimmy Etheredge, Atlanta
Words That Carry Weight
Thank you for calling attention to the challenges people with obesity face regarding risks of COVID-19 infections and the potential that vaccines may not be effective (“America’s Obesity Epidemic Threatens Effectiveness of Any COVID Vaccine,” Aug. 6). I would like to comment on how you refer to people with obesity. The Obesity Action Coalition, and other organizations focused on obesity, recommend using people-first language. An article about cancer does not refer to cancer people, nor does one on cardiovascular disease label individuals as heart disease people. The terms “obese people” and “morbid obesity” are stigmatizing. It is better to utilize people-first language as Dr. Timothy Garvey did at the end of the article. As a member of the Obesity Medicine Association as well as an obesity medicine specialist and educator, I work diligently with patients to overcome the bias and stigma that society imposes. Please be considerate of the use of language when referring to people with obesity.
— Dr. Nicholas Pennings, Raleigh, North Carolina
It is becoming more & more obvious that we would‘ve “saved” FAR more lives here if we had put all the mask shaming energy into getting people to lose weight. But that would be un-PC.
America’s Obesity Epidemic Threatens Effectiveness of Any COVID Vaccine https://t.co/wfbUz9JSB9
— John Ziegler (@Zigmanfreud) August 10, 2020
— John Ziegler, Los Angeles
As a sociologist researching weight stigma, I am appalled by the article by Sarah Varney suggesting obesity will undermine vaccine effectiveness. The article is full of stereotypes and misinformation. In the first place, it is Big Pharma’s fault vaccines aren’t made for fat people. It is beyond incompetence that any vaccine drugmakers come up with would be less effective for half the population. In the second place, many of the diseases fat folk allegedly have are caused by yoyo dieting and stigma. And there is no proof weight loss would make any vaccines more effective as most fat people are biochemically different than thin ones. This is a tone-deaf, fat-phobic article that serves only corporate interests.
— Sherie Sanders, Springfield, Illinois
Jail Outbreaks
My life and those of others are being put in danger by the San Bernardino County Sheriff’s Department (“COVID Runs Amok in 3 Detroit-Area Jails, Killing At Least 2 Doctors,” July 23). I’m in jail with health issues: asthma, prediabetes, vitamin D deficiency, high blood pressure, and may have a cancerous tumor and peripheral neuropathy. I’ve already been put on quarantine two times, once because a deputy who tested positive for COVID-19 had direct contact with me and the other because they put someone in the cell with me who was symptomatic for COVID-19. When being transported anywhere, they put chains on us that have been on many people and have not been cleaned. Then they chain multiple people together, not even knowing if a person has or is a carrier of the coronavirus. The social distancing was put in effect to protect the lives of people. The sheriff’s department is violating it, putting lives in danger and will continue to do so until they are stopped. To top it off, I am state property and not even supposed to be here. I don’t want to die or see anyone else die for being in jail and catching COVID-19. So can someone please help us all.
— LeAire Moore Sr., Adelanto, California
Lots of people ask me why I stay home most of the time, mask up, wash my hands, socially distance.
Why should I? I’m young. I’m healthy. I work out and eat right.
But, I have a mother.
This is why. ⬇️https://t.co/IlKPXmTu65
— Samuel Cook, III | CPT, CNC, USAW (@samueljcookiii) September 6, 2020
— Samuel Cook III, New Orleans
Correcting the Record on the Navajo Language
The article “Two Navajo Sisters Who Were Inseparable Died of COVID Just Weeks Apart” (Aug. 26) is incorrect. The Navajo language is most certainly “written down” and is taught in schools and universities.
— Randy Truman, Albuquerque
Editor’s note: Thanks for helping us clarify that point. The article has been updated.
Medicaid Expansion in the Age of COVID
The COVID-19 pandemic has shown us that Americans are in desperate need of health insurance, including publicly financed health insurance programs such as Medicaid. The time is now for some policymakers in America to reshape how they think of Medicaid as more than a government handout that makes us worse and not better.
Medicaid is a health insurance program that is jointly funded by the state and federal government. This program provides low-cost insurance to adults with low income, both young and elderly, pregnant women, the disabled and children through the Children’s Health Insurance Program, commonly known as the CHIP program.
The Affordable Care Act provided an opportunity for states to expand coverage to individuals at 138% of the federal poverty level. As an added incentive, the federal government pledged to pay 100% of the costs to expand, a share that would be reduced to 90% by 2020. In recent months, states such as Oklahoma and Missouri through the ballot box have expanded Medicaid. This leaves only 12 states to not expand, but millions more in need of affordable health insurance.
The argument by some policymakers against the Medicaid program is the fear of incentivizing Americans to not work. Contrary to this belief, in 2017, it was reported that more than 63% of Medicaid recipients are already in the workforce while only 7% were not working for various reasons.
Finally, since the beginning of the pandemic, one study estimated that nearly 27 million Americans could lose their employer-sponsored insurance this year. Of those 27 million, nearly 13 million would be eligible for Medicaid.
The American people deserve to have affordable health insurance. Therefore, policymakers have an obligation to expand it and not contract.
— Reginald Parson, Portland, Maine
This is happening right now throughout our system and its utterly disgusting and unacceptable.
Health Care Workers of Color Nearly Twice as Likely as Whites to Get #COVID-19 https://t.co/1VOFQid8mM via @khnews
— Stephen Ferrara, DNP (@StephenNP) August 6, 2020
— Stephen Ferrara, New York City
Kaiser Health News (KHN) is a national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation which is not affiliated with Kaiser Permanente.
USE OUR CONTENT
This story can be republished for free (details).
from Updates By Dina https://khn.org/news/readers-and-tweeters-grapple-with-covid-therapies-and-forecasts/
0 notes
Text
Readers and Tweeters Grapple With COVID Therapies and Forecasts
Letters to the Editor is a periodic feature. We welcome all comments and will publish a selection. We edit for length and clarity and require full names.
Giving Convalescent Plasma a Shot
Used to effectively treat mumps, measles, and even the so-called Spanish flu in 1918, convalescent plasma may not be a silver bullet, but it still has the potential to play an important role in helping some patients recover from COVID-19 (“5 Things to Know About Convalescent Blood Plasma,” Aug. 27).
To support its recent decision, the Food and Drug Administration used data from previous use cases of convalescent plasma for other respiratory coronaviruses, results of early safety and efficacy trials in animal models, and published studies on the safety and efficacy of convalescent plasma before issuing Emergency Use Authorization (EUA). The agency also pointed to a Mayo Clinic preliminary analysis of 56,000 patients who were given high or low titer units of blood plasma.
The EUA also specifies that donor blood can be released only to hospitals and patients after it is tested with a currently available antibody test that accurately detects the right type of antibodies to neutralize the virus and confirms that the blood contains sufficient levels of these antibodies for treatment purposes. This means that less accurate, less specific tests that are more susceptible to false positives will not be used to identify COVID-19 convalescent plasma — something that should give patients higher confidence that the plasma they receive meets scientific and quality standards.
— Dr. Fernando Chaves, a board-certified hematopathologist who serves as Global Head of Medical and Scientific Affairs at Ortho Clinical Diagnostics, Raritan, New Jersey
I’m quoted here saying what everybody already knows: if we want to know if plasma works, we need a trial.
This isn’t academic for me: I want to know if I should be using plasma in my patients with severe COVID-19. This fiasco was preventable. https://t.co/MjS2DXbYUX
— Adam W Gaffney (@awgaffney) August 28, 2020
— Dr. Andrew Gaffney, Boston
Vaccination and Prognostication
Both assertions that seniors will drive 800 miles or come home from an assisted living or skilled nursing facility to live with families are dubious (“What Seniors Can Expect as Their New Normal in a Post-Vaccine World,” Aug. 3). The latter are need-based moves (think dementia, wandering). The former makes sense for those who won’t tolerate the physical strain of long car rides — think Florida to D.C.
— Laurie Orlov, Aging and Health Technology Watch, Port St. Lucie, Florida
I wonder if many of these predictions are more likely to be true among those who have personal experience with COVID-19, either through personal experience with illness or loss of family or friends. https://t.co/uRZnuSfFLf via @khnews
— Rosemary Wright, PhD (@rwrightphd) August 3, 2020
— Rosemary Wright, Wichita, Kansas
I don’t want these precautions to last forever. I want there to be a time where we can all give each other hugs and high fives again. We were built to be together and celebrations bring us so much joy. I want there to be a time when we can all be in fun crowds again. I want to be able to smile out in public again and not have to cover my face. What do you think about all of this?
— Christopher DeCarlo, Oyster Bay, New York
We won’t go back to “the way things were” even after a vaccine for #COVID19 has been invented. This experience has been an opportunity to innovate and do better. Here are some changes you’re likely to see in #healthcare and beyond. https://t.co/l4x50qVxvM
— Tony Slonim MD, DrPH (@RenownCEOTonyMD) August 8, 2020
— Dr. Tony Slonim, Reno, Nevada
Humans as Guinea Pigs for the Sake of Corporate Piggy Banks?
We assume that this vaccine works, but how do we know (“They Pledged to Donate Rights to Their COVID Vaccine, Then Sold Them to Pharma,” Aug. 25)? The public is not some testing animal. I would not take this vaccine, especially since the back-and-forth is over money and not public health. No government should give any money to a business without a deal that protects the public as investors. We are not a source of free money; just as they make no concessions, we also should make no concessions without a deal. And the deal is public health.
There was no vaccine during the 1918-19 influenza, not until 1940. Our immune system needs to be considered as part of a cure. Is that not the theory behind flu shots? So, if we are exposed to the virus and allow our bodies to fight it off, that defense is greater than any vaccine. Those who cannot fight off the infection are the ones who need to be considered for medical attention — and not just some shot hopefully manufactured by a company that does not prioritize money over health.
There are times when profit is important, but since businesses are being subsidized, this is not one of those times. The world economy has been seriously affected, and printing money we do not have is not a sound idea. What good are medicine and doctors and medical research? Seems we should consider those old grandma medications, such as the hot toddy … whiskey and hot coffee and a good night to sweat it out under many covers. That cured my grandfather of influenza long before there was a vaccine.
Medical science doesn’t have all the answers. If soap can kill this coronavirus, then there must be a common household solution to eradicate it that is medically safe for humans. Perhaps technology students would do better to help the world instead of these money-hungry corporations.
— Tom Berger, Suffolk County, New York
Volunteers risk their lives in clinical trials, and the Oxford converted vaccine from public good to profitable commodity? …
They Pledged to Donate Rights to Their COVID Vaccine, Then Sold Them to Pharma https://t.co/vQw94BfxKE via @khnews
— Amar Jesani (@amarjesani) August 31, 2020
— Amar Jesani, Mumbai, India
On COVID Tests and Risk
I have worked in a clean lab for many decades. I know how to behave and how to take advantage of and handle PPE, for the purpose of achieving very low contamination levels. The article “Analysis: When Is a Coronavirus Test Not a Coronavirus Test?” (July 29) presents a false option. It is not about accepting a level of risk, it is about doing everything possible to reduce the risk.
In my labs, I had the ability to require adherence to careful procedures and the option to fire anyone who would not follow approved procedures. I don’t have that option with those who refuse to follow the simple instructions for COVID-19, including the “religious” wearing of a mask, the same way that women cover their heads when entering a Catholic church and Jewish men wear a yarmulke in a temple.
And when the president irresponsibly and criminally refuses to follow and to mandate simple instructions by medical experts, then I am unable to calculate the risk. I don’t think Ms. Rosenthal can calculate the level of risk she suggests we accept.
— Dimitri Papanastassiou, Pasadena, California
I enjoyed your piece, but I regret that you said so little about therapies that may emerge to help us. Vaccines are not the only hope. I think a disservice is being done by indicating that our only options are to live with it or wait for a vaccine.
— John Van Drie, North Andover, Massachusetts
Great article by @ahartreports. I too cringed initially at likening #covid19 to war but couldn't agree more that we need to treat our #PublicHealthOfficials with respect and be grateful for their sacrifices https://t.co/rr9NT4tNlB via @khnews
— Meghan McGinty, PhD (@Breukelen299) September 1, 2020
— Meghan McGinty, Brooklyn, New York
The Hydroxy Paradox
Wouldn’t it be refreshing, instead of slamming other doctors’ practical experience with hydroxychloroquine at low dosages and supplemented with zinc, etc. at the first sign of the infection, to at least let them make fools of themselves (“Don’t Fall for This Video: Hydroxychloroquine Is Not a COVID-19 Cure,” July 31)? What is the harm?
Aren’t “we all in this together”? Why are we afraid of a difference in opinion? What if it really works using the protocols as stated? Let it play out. Pretty sure no one has died when prescribed “hydroxy” in low dosages by doctors in actual practice, unlike the deaths that occurred when given in massive dosages late in the infection.
Why make fun of doctors who are trying their best to help us all? That seems narrow-minded to me.
— Larry Koch, Agoura Hills, California
Reported this tweet. You are encouraging the use of a medication a. Without a license b. Without citing sources and c. Every double blind study has shown and increase in death.https://t.co/iN7eionH03https://t.co/eSPDwPz9V6
— Tara Tisch🦓🍀🎨🏴☠️ (@TaraTisch) August 22, 2020
— Tara Tisch, Peoria, Illinois
I know you disagree with Dr. Stella Immanuel, and that’s OK. The problem I have is that no one has done the clinical trials to prove that hydroxychloroquine doesn’t work. She said she has 350 patients who have had success with her prescriptions; the doctor from Dallas said she uses it with her own little concoction. If, in fact, what they are doing is working, then why don’t people visit these doctors to see if it is true — and, if it is, then try collaborating with them to keep people from dying, for crying out loud.
That is one of the problems here: Everyone is against one another instead of trying to support one another. We are Americans and, as in years past, we have stuck together for the betterment of the country. If we would stop trying to take care of America with money and start taking care of America with information, then America would live and thrive.
I am a first-year respiratory therapy student and spent 20 years in the Marine Corps, and back in the ’80s we took chloroquine, and I have no side effects and neither do the guys I stay in contact with. Keep in mind that the reports of the side effects are not in every patient and if hydroxychloroquine is offered to a patient and the patient is told, “This is going to make you better but there could be side effects later, but if you don’t take this you will get worse and we don’t know if you will die or not,” what do you think they will say? No one wants to die.
C’mon, let’s just be people trying to keep other people alive no matter the cost, no matter who is right or wrong — we can sort that out later.
— Jim Tumlinson, Canyon Lake, Texas
Editor’s note: A recent report from the Centers for Disease Control and Prevention expressed caution and concern that hydroxychloroquine was potentially being misused to treat COVID-19 and affecting supplies of the medication to treat rheumatoid arthritis, lupus and other conditions. “Current data on treatment and pre- or postexposure prophylaxis for COVID-19 indicate that the potential benefits of these drugs do not appear to outweigh their risks,” it said.
Yoga for All
I appreciate your article (“Namaste Noir: Yoga Co-Op Seeks to Diversify Yoga to Heal Racialized Trauma,” July 30) but have a hard time with “people of color” being repeated over and over. Yoga benefits all people, and until we start thinking as one and not labeling everything we will always have racial issues. We need to think all lives matter, not just a specific color. Thank you for your writings.
— Susan Ferguson, Cypress, California
"Namaste Noir" ?????????? good and important article, but really, really poor headline choice @KHNews https://t.co/GefI9Zkoy8
— Eli Imadali (@eliimadaliphoto) August 9, 2020
— Eli Imadali, Denver
#Namaste. Yoga and meditation are helping Ms. Grant deal with COVID-19, the loss of her son and racial stress. Lots of lessons here for all of us. @KHNews #Equality https://t.co/GnxZn4l7QF
— Jimmy Etheredge (@JimmyEtheredge) August 14, 2020
— Jimmy Etheredge, Atlanta
Words That Carry Weight
Thank you for calling attention to the challenges people with obesity face regarding risks of COVID-19 infections and the potential that vaccines may not be effective (“America’s Obesity Epidemic Threatens Effectiveness of Any COVID Vaccine,” Aug. 6). I would like to comment on how you refer to people with obesity. The Obesity Action Coalition, and other organizations focused on obesity, recommend using people-first language. An article about cancer does not refer to cancer people, nor does one on cardiovascular disease label individuals as heart disease people. The terms “obese people” and “morbid obesity” are stigmatizing. It is better to utilize people-first language as Dr. Timothy Garvey did at the end of the article. As a member of the Obesity Medicine Association as well as an obesity medicine specialist and educator, I work diligently with patients to overcome the bias and stigma that society imposes. Please be considerate of the use of language when referring to people with obesity.
— Dr. Nicholas Pennings, Raleigh, North Carolina
It is becoming more & more obvious that we would‘ve “saved” FAR more lives here if we had put all the mask shaming energy into getting people to lose weight. But that would be un-PC.
America’s Obesity Epidemic Threatens Effectiveness of Any COVID Vaccine https://t.co/wfbUz9JSB9
— John Ziegler (@Zigmanfreud) August 10, 2020
— John Ziegler, Los Angeles
As a sociologist researching weight stigma, I am appalled by the article by Sarah Varney suggesting obesity will undermine vaccine effectiveness. The article is full of stereotypes and misinformation. In the first place, it is Big Pharma’s fault vaccines aren’t made for fat people. It is beyond incompetence that any vaccine drugmakers come up with would be less effective for half the population. In the second place, many of the diseases fat folk allegedly have are caused by yoyo dieting and stigma. And there is no proof weight loss would make any vaccines more effective as most fat people are biochemically different than thin ones. This is a tone-deaf, fat-phobic article that serves only corporate interests.
— Sherie Sanders, Springfield, Illinois
Jail Outbreaks
My life and those of others are being put in danger by the San Bernardino County Sheriff’s Department (“COVID Runs Amok in 3 Detroit-Area Jails, Killing At Least 2 Doctors,” July 23). I’m in jail with health issues: asthma, prediabetes, vitamin D deficiency, high blood pressure, and may have a cancerous tumor and peripheral neuropathy. I’ve already been put on quarantine two times, once because a deputy who tested positive for COVID-19 had direct contact with me and the other because they put someone in the cell with me who was symptomatic for COVID-19. When being transported anywhere, they put chains on us that have been on many people and have not been cleaned. Then they chain multiple people together, not even knowing if a person has or is a carrier of the coronavirus. The social distancing was put in effect to protect the lives of people. The sheriff’s department is violating it, putting lives in danger and will continue to do so until they are stopped. To top it off, I am state property and not even supposed to be here. I don’t want to die or see anyone else die for being in jail and catching COVID-19. So can someone please help us all.
— LeAire Moore Sr., Adelanto, California
Lots of people ask me why I stay home most of the time, mask up, wash my hands, socially distance.
Why should I? I’m young. I’m healthy. I work out and eat right.
But, I have a mother.
This is why. ⬇️https://t.co/IlKPXmTu65
— Samuel Cook, III | CPT, CNC, USAW (@samueljcookiii) September 6, 2020
— Samuel Cook III, New Orleans
Correcting the Record on the Navajo Language
The article “Two Navajo Sisters Who Were Inseparable Died of COVID Just Weeks Apart” (Aug. 26) is incorrect. The Navajo language is most certainly “written down” and is taught in schools and universities.
— Randy Truman, Albuquerque
Editor’s note: Thanks for helping us clarify that point. The article has been updated.
Medicaid Expansion in the Age of COVID
The COVID-19 pandemic has shown us that Americans are in desperate need of health insurance, including publicly financed health insurance programs such as Medicaid. The time is now for some policymakers in America to reshape how they think of Medicaid as more than a government handout that makes us worse and not better.
Medicaid is a health insurance program that is jointly funded by the state and federal government. This program provides low-cost insurance to adults with low income, both young and elderly, pregnant women, the disabled and children through the Children’s Health Insurance Program, commonly known as the CHIP program.
The Affordable Care Act provided an opportunity for states to expand coverage to individuals at 138% of the federal poverty level. As an added incentive, the federal government pledged to pay 100% of the costs to expand, a share that would be reduced to 90% by 2020. In recent months, states such as Oklahoma and Missouri through the ballot box have expanded Medicaid. This leaves only 12 states to not expand, but millions more in need of affordable health insurance.
The argument by some policymakers against the Medicaid program is the fear of incentivizing Americans to not work. Contrary to this belief, in 2017, it was reported that more than 63% of Medicaid recipients are already in the workforce while only 7% were not working for various reasons.
Finally, since the beginning of the pandemic, one study estimated that nearly 27 million Americans could lose their employer-sponsored insurance this year. Of those 27 million, nearly 13 million would be eligible for Medicaid.
The American people deserve to have affordable health insurance. Therefore, policymakers have an obligation to expand it and not contract.
— Reginald Parson, Portland, Maine
This is happening right now throughout our system and its utterly disgusting and unacceptable.
Health Care Workers of Color Nearly Twice as Likely as Whites to Get #COVID-19 https://t.co/1VOFQid8mM via @khnews
— Stephen Ferrara, DNP (@StephenNP) August 6, 2020
— Stephen Ferrara, New York City
Kaiser Health News (KHN) is a national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation which is not affiliated with Kaiser Permanente.
USE OUR CONTENT
This story can be republished for free (details).
Readers and Tweeters Grapple With COVID Therapies and Forecasts published first on https://smartdrinkingweb.weebly.com/
0 notes
Last Seen Blogs


moontidesoup
In Constant Transition
aismoker
AI Smoker

spiritboardv3
Front: Damien

rastafariansfm
RastafarianSFM