
A mental health blog and diary, focusing on DID/OSDD, personality disorders, autism, psychosis, trauma, and other topics. Personal posts are ok to interact with unless tagged otherwise. Directory About Resource Drive ♡ You are loved, you are worthy of love, I see you ♡
Don't wanna be here? Send us removal request.
Statistics
We looked inside some of the posts by hauntedselves and here's what we found interesting.
Average Info
Notes Per Post
5K
Likes Per Post
3K
Reblog Per Post
2K
Reply Per Post
28
Time Between Posts
23 days
Number of Posts By Type
Text
10
Note
7
Last Seen Tumblr Blogs





Fun Fact
70% of Tumblr users say the Dashboard is their favorite place to spend time online.
Text
Alternatives to Self Harm
Please use discretion and don't do something that will trigger you further, including triggering trauma or sensory issues!
Aggressive activities (Adrenaline-focused): Do not use sharp objects if you can't trust yourself around them in that moment.
Tear apart paper or napkins
Cut up boxes, plastic, or paper
Stab boxes or foam
Angrily scribble
Throw rocks at the ground
Scream into a pillow, or punch it
Passive activities (Adrenaline-focused):
Watch something scary (scary game, thriller movie)
Watch someone get angry (Youtube react videos, gamer rage)
Watch an action movie
Watch a fails video compilation
Sensory grounding
Hold an ice cube or splash cold water on your face - take a cold shower if you're really feeling it
Smell a strong scent, even an unpleasant one
Have a nice warm or cool drink
Any kind of strong pressure that won't injure you (weighted blanket, cuddle with your dog)
Listen to music or white noise
Use a heating pad or take a warm shower/bath
Creative outlets: (if you need the similarity, use red ink)
Draw on yourself or body paint
Do SFX makeup
Finger paint
Journal about your feelings honestly, even if they're negative
Make a moodboard
That's all my ideas for now, so if anyone has any more, feel free to add on.
217 notes
·
View notes
Note
What is the easiest way to kill yourself? What will you prefer?
#1. I hope you get help and make it out of the pain you're in#2. This is really inappropriate to send to a stranger#3. Why are you asking what *I* prefer? I don't have a fave suicide method!!#dogasks#Suicide two
4 notes
·
View notes
Note
sorry if this has been asked before or if its somewhere on your blog, but is "longing to spill your guts out (emotionally) to someone but getting physically sick when thinking about or actually doing it" a szpd thing? i think i understand how splitting w/ szpd works but i'm not sure if this is how it works???/?//?//?// sorry if this is worded weirdly ive also been super confused if i have npd szpd or if im just like this :p
i don't think this is exclusive to SzPD. this sounds like a fear of vulnerability. being uncomfortable with vulnerability - even while wanting it - isn't a symptom specific to any disorder; it's part of everything from PTSD, personality disorders, toxic masculinity, cultural norms of being emotionally distant...
is it something that people with SzPD could experience? absolutely! here are some posts about SzPD splitting:
my post about splitting in SzPD with charts (from Wheeler's thesis)
my post on splitting in SzPD, NPD & BPD
schizotaxic's post on SzPD, NPD & OCPD's 'superiority defense mechanism'
schizotaxic's post on splitting in SzPD
10 notes
·
View notes
Text
today in therapy
... was not the last day of therapy, but i brought up - and my psychologist "strongly agreed" - that i'm at a place now where i don't need regular therapy. i think my psych has been hinting at this for a while now, and i knew but i kind of wanted to keep therapy going regularly - there was this undercurrent of, idk, 'regular therapy makes me Special'? which obviously isn't true, going or not going to therapy has no bearing on your worth as a person.
(this is a long post, so i'm putting a read-more)
it'd been about 3 months since i'd last had therapy, during which i moved 4,000kms across the country and started studying veterinary medicine. so a lot had happened! but aside from some health anxiety flaring up (combination of not having the local support system anymore + actual health issues), and some rocky moments which were to be expected in the move, i've been doing pretty well. and i like going to therapy - psychology is a special interest of mine (obviously as i run this blog (even if it's sporadic!)), and i guess, like everyone, i like talking about myself lol. but i knew that i've made so much progress over the ~4 years i've been seeing my psych, that it's time to accept that while i'm not 'recovered'*, i don't need regular therapy anymore.
i'm glad i made it. looking back at old diaries, i can't imagine existing like that now - that constant dissociation, panic attacks, nightmares every night. therapy + medication + going low contact with abusive people = i'm genuinely ok. yeah, i still get nightmares but they're more like once a week than every night. yeah, i still dissociate but only when i'm really stressed. yeah, i will need to be on medication probably for the rest of my life, because my brain just can't handle not having those synthetic chemicals. but i'm ok - i can self-soothe after nightmares, i can ground myself out of dissociation, i can calm myself out of panic attacks and anxiety.
and hey - if you're reading this and thinking, god i wish that were me - it can be!! therapy might not be for you but there are other ways to learn these skills. and they are just skills - things that can be learnt! maybe you need medication, maybe you need to not be on meds, maybe you need intensive inpatient therapy, maybe you need to just have regular catch-ups with someone you trust to talk about shit. whatever healing looks like, that's fine. you can do it too!
*(in the sense that autism + brain changes from PTSD + need to be on medication probably forever, etc. = not ever going to be 100% recovered (which doesn't really exist anyway). there will always be flare ups and triggers, there will always be things that are hard, but you can get to a point where you have the skills so you can deal with these things by yourself, and know how/when to reach out if you need help)
#no bold#long post#dogpost#personal#recovery#theres a reddit group r/cPTSDNextSteps that talks about this 'ok what next' stage if u want to check it out#also. i have literally like 200 drafts which includes unanswered asks. i WILL get around to them. but it may be Quite A While.#(it already has been i know!!! thank you for your patience!!)
7 notes
·
View notes
Text
Guide on Amnesia [Fixes and Solutions]
To check what types of amnesia are there, click on this post prior reading! This is a compact, straightforward post to keep amnesia at bay.
General amnesia
Caused by: major disruption such as a concussion or huge shock/realization How it works: disorganizes or disrupts neuron firings as a whole, causing past and present memories to fleet away temporarily Solution: bring yourself back to a regulated state, things like grounding techniques, vagus nerve stimulation, do calming activities, or go to somewhere safe and quiet to recollect oneself
Localized amnesia
Caused by: psychological defenses, or disruption within a specific region How it works: Same as general amnesia, though more region-based Solution: focus on de-stressing, assure yourself it will pass and don't force on remembering. Your brain will open up the pathway when you're in a better state
Selective amnesia
Caused by: intentional selective inhibition How it works: the prefrontal cortex and limbic region actively search for highly emotional/stressful memories to repress them and create temporary stability Solution: use coping mechanisms, or create plans to avoid overwhelming feelings from disrupting your memory and thinking. The better you can handle stressful situations, the less inclined it feels about repressing memories to protect you
Emotional amnesia
Caused by: dissociation How it works: the amygdala and prefrontal cortex stops "communicating" for safety reasons , thus creating an emotional gap within a memory Solution: create a safe space to uncover how you truly feel within the memory, you were protected from overwhelming feelings through dissociation so you can still observe and understand what happened. Only until it feels safe and in a collected state, to be able to process the emotions
Continuous amnesia
Caused by: a perpetual state of anterograde amnesia How it works: stress and other disruptions causes worsened abilities to form and recall memories, whatever stress/trauma that is impeding the process will continue to cause amnesia until alleviated. The hippocampus is severely compromised due to it Solution: quickly get out of the loop by grounding, and resolve the ongoing stress or triggers that is causing dissociation and involve calming methods to regulate both your mind and body back to balance
Fragmented amnesia
Caused by: dissociation, stress, and missing sensory information (sight, hearing, tactile, etc) How it works: dissociation/disruptions and incomplete sensory input causes gaps, which then disjoints and makes it impossible to integrate a sense of time or flow. causing separate bits of short memories Solution: often needs long term investment to create higher stress resilience, better coping methods, and other solutions that doesn't need dissociation to solve. Find what you need to work on, and what best suits as solution (Like DBT, etc)
To solve amnesia barriers, see the post on splitting and fusing, which also touches the disconnection between alter's memories and feelings and how to lessen them.
For inner-communication issues, see the post here which covers everything relevant on this topic.
--
What do you guys think? Feel free to say your inputs or your own advices on how you keep your amnesia at bay!
For questions about amnesia and how to handle them with more detail, please don't be shy to contact or ask anything related about it.
- j
89 notes
·
View notes
Text
Image description:
A diagram depicting different types of amnesia.
Generalised amnesia: a box with a dashed border around it, indicating something missing or emptiness. Underneath is a person looking confused and distressed, with a loading symbol at their head.
Localised: a solid box with a corner missing.
Selective: a box with some solid parts, and some missing parts.
Emotional: a box that is solid, but devoid of colour. Underneath is a person with a neutral expression, with a speech bubble that has a crossed out heart.
Continuous: a box that has a solid section, then a gap, then another solid section. Underneath is a clock indicating time passing.
Fragmented: a glitchy, distorted box.
End image description.
Types of Amnesia
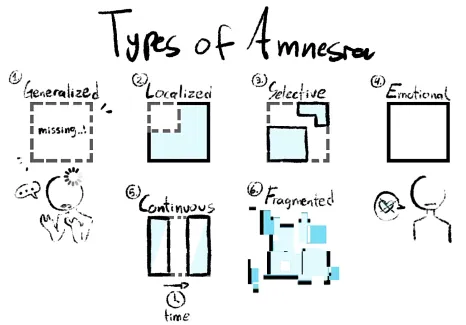
Diagram created by me
General criteria for amnesia:
Memory loss
Confusion
Inability to recognize familiar figures/places
Difficulty recalling names or places
Not remembering where you went
Worser ability to remember things that had happened Post on how to handle these kinds of amnesia: click here!
Generalized Amnesia Where a person completely forgets everything about themself and have no recollection of what, where, and who they spoke to. This can describe a blackout switch and may still recognize who they are.
Localized Amnesia Where a person is unable to recall a specific/series of event from the whole, which creates an incomplete picture of the situation. For example, remembering childhood but not the abuse.
Selective Amnesia Where a person only lost some and retain the rest, forgetting parts yet not all of them. This can describe greyouts as it grasps some information/sensory yet not enough to tell what exactly happened. One example is playing the phone and unable to recall what occured, only to jump its memory right to being at bed.
Emotional Amnesia Where a person has an intact memory and it's details on what had happened, but do not remember what the event feels like (e.g. was scared, happy, etc.). One description is that you're watching something that didn't happen to you, because you don't feel like being in the scene itself.
Continuous Amnesia Where a person fails to retain full parts of the event/day, for a set period of time (can vary from minutes to days) and create an accumulative, small bits of selective amnesias, continuously, leaving many gaps in a chronological timeline. This usually happens in times or stress, or abuse.
Fragmented Amnesia Where a person has an unrelated, and/or disjointed memories that does not go with the timeline's order, creating confusion and difficult to grasp the cohesive picture of what truly happened. Emotional amnesia may be present in this type. Bonus for systems:
Amnesia barriers Where a person fronting is not able to recall other alter's memories, which is a form of retrograde amnesia and compartmentalization. Because the fronter will only retain any information before switching out with the next one, the rest experiences anterograde amnesia as it cannot form and remember those memories, unless being coconcious or cofronting (even though, this is not always guaranteed).
Take notes that amnesia can still happen outside system things due to comorbidities like anxiety disorders or depression, this does mean systems are bound to experience more amnesia compared to non-systems folks out there.
Do you have any discussions about this? Or would like to describe your own way of seeing these different types of amnesia? Or have more to add? Feel free to tell them here!
- j
3K notes
·
View notes
Note
Do you have an "alternate model for personality disorders" post for HPD? If not, would you be able to make one? I'm really glad to have a resource like this since I've been questioning a few PDs, and HPD is one that's been on my radar for a while!
the alternate models come from the DSM, and it doesn't include HPD - it would be diagnosed as PD-TS (Trait Specified) in this model.
if i had to guess at a HPD alternate model:
like all alternate model PDs, it would include impairments in identity, self-direction, empathy & intimacy.
HPD's examples might look like:
identity: unclear boundaries between self & others, unstable self-image & self-esteem, inability to regulate emotions
self-direction: incoherent short & long-term goals, unstable internal standards of social behaviour
empathy: difficulties understanding others' experiences, and their effects on others
intimacy: unstable connection (and desire for) with others, unbalanced mutuality in connections
in the Five Factor Model part, HPD might also be described as being high in Negative Affectivity (e.g. mood instability & intensity, insecurity, etc.) and Disinhibition (e.g. impulsivity, risk taking, etc.)
you could also check out the ICD-11's personality disorder diagnosis (just one disorder with various traits)
#pd info#dogasks#bold#hpd#dsm alternate PD model#five factor model#big five factor model#histrionic personality disorder
22 notes
·
View notes
Text
Some of the people I have seen say they have non-disordered plurality have a lot of extreme dissociative symptoms from what they post. System conflicts, huge memory gaps, inability to control switches, extreme depersonalization/derealization symptoms.
This is not to deny someone’s experience, but more of a gentle reminder that if your experiences with plurality causes genuine distress? You may want to learn more about how dissociative disorders impact functions.
I don’t really understand any labels outside of traumagenic and maybe endogenic. I can’t even begin to really wrap my head around plurality not causing dissociation—it’s just not my experience at all. It’s a big reason why I decline arguing in any debates, but I have a pretty good idea of how my DID has impacted me.
I will feel like shit and not understand why because my emotions are highly fragmented. There could be something wrong, I could feel it occasionally, but I have no clue at all why I am experiencing this level of distress.
I know of a major traumatic experience in my childhood that could have caused my DID, but I genuinely remember little to nothing about my life and the factors are endless. When I do find stuff talking about my experiences, it sets me back and almost “triggers me” back into a state where I was during that time (I have no recollection still even after these triggers happen).
Skills and knowledge are somewhat distinctive between parts. Some parts have had full blown meltdowns because they didn’t understand an assignment, and when someone else switched in, they knew exactly what to do.
“Wishing to be a system” played a huge part in my formation, but it wasn’t wishing to be a system. It was wishing I had someone to talk to/had friends surrounding me because I was emotionally neglected as a child—this was around ages 6-10, so this thought process had a lot of impacts. I verbally talked to these parts and they often knew information I never remembered learning, and they often came around the most when I was lonely.
I don’t have a stable identity, and I haven’t had one for the entirety of my life. If I try to sit and think about it, my head will turn to TV static and shut off any chance of understanding my situation. I spend about 80-90% of my time going through the motions of life without any acknowledgment of my identity, thoughts, feelings, sensations, or perceptions in life.
Trauma doesn’t have to be a serious case of SA or physical abuse, it is possible it could be years of emotional neglect causing you to turn inward. Bullying, oppression, poverty, disability, physical illness, messy divorces/parents NOT divorcing, war, and many other issues are extremely taxing on a child.
This disorder is covert and nearly undetectable in most cases. Sometimes this means that it’s nearly impossible to see in ourselves. The whole point is to hide and make sure we “function” correctly in society, even at the expense of ourselves. It’s a coping mechanism our brain decided was the safest route to survive.
Identity disruptions, memory gaps, and all these things are not stable, concrete experiences. They are fluid. They can be wildly inconsistent, and you don’t have to be on the far end of the spectrum to experience these issues.
I’m not saying this as a genuine diagnosis of “You MUST have DID” because there are many different aspects that could impact this. I know that there are also like- labels that encompass different aspects that include trauma. However, this is just something I have noticed while scrolling through tumblr recently. This also isn’t targeted in any way, but if it resonates with you, I think learning about DID in medical contexts isn’t a bad idea (or at least learning of dissociation).
I have seen that a big reason many people get nervous to interact with traumagenic spaces is because of how aggressive and toxic they can be, which I understand is definitely a problem we see. It’s definitely a product of how DID is and what societal hatred does to marginalized communities. I take a very chilled and laid back approach to pretty much anything, so if you feel too scared to interact with the traumagenic community, I don’t mind trying to help!
203 notes
·
View notes
Note
🍁There’s a quiet strength in just existing. It’s easy to overlook, especially when everything feels awful, but simply getting through each day is a huge accomplishment. You might not always see it, but just by being here, you’re adding something uniquely important to the world. It’s not about doing something extraordinary or being the best; it’s about continuing on, even when things are tough. Your presence matters, and it has a positive impact in ways you might not notice, but others do. Give yourself credit for the small victories, the moments when you keep going despite it all. Those moments show just how strong you are, even if it doesn’t feel that way. Hang on to that thought, because it’s a truth worth holding onto as you face whatever comes your way.🍁
thank your your kind & true message!
5 notes
·
View notes
Note
I fear the question I'm about to ask is silly, but oh well
can i have NPD and hate myself
and feel unworthy
friend, this is The core experience of NPD! i'll direct you to my page on NPD, especially the resources section
16 notes
·
View notes
Text
One of the curiosities about how psychosis is defined, is the fact that clinically, delusions are defined as strongly held "wrongful" beliefs that don't respond to counter-proof, and that aren't shared with others in a subculture.
In other words, believing even very bizarre conspiracy theories such as "the earth is flat" isn't a delusion, though in a broader linguistic sense it is sometimes referred to as such.
In this post I wanna talk a bit about why that is, and why I do think that it's important to have a distinction between clinical delusions that happen in psychotic illnesses, and strange beliefs that arise in other ways.
So why is it not a delusion if it's shared with a subculture?
I think the reason for this distinction is that delusions experienced by people with psychotic disorders are something that comes from within, rather than something we've been taught to believe. Per definition. Psychotic people aren't particularly "gullible", we don't lack critical thinking skills, we have an illness that make us believe random untrue crap in a way that makes us unable to think critically about it. So while a psychotic belief could be inspired by something we've come across (like a conspiracy theory) our brain is generally gonna take it as a seed and run with it. Therefore we usually quickly get out of bounds from the 'community' that might have inspired our belief anyways.
Overall, we are less prone to having gotten our beliefs from others and are more prone to being the originator of a belief. In something like folie a deux, a non-psychotic person is taught reality from a psychotic delusional person, f.ex. a child growing up with a delusional parent. The child might appear at first glance to be psychotic, but actually they only believe those things because that's what they were taught by someone they consider an authority. If you remove the child from that environment, you will usually be able to help them regain a better understanding. Similarly someone might grow up in a cult. And they are believing what they are being taught, and their parents are believing what they have been taught. And there will be most likely an originator to the cultish beliefs. That person might be maliciously making things up, or they might even be psychotic and delusional. But the people who are being taught these things as facts are behaving like most humans, as social creatures who's reality is defined by their context.
Most people's context is defined along the lines of consensus reality, but if your social context is not aligned with the majority consensus reality, you are still aligned with the beliefs of your social context if you share your weird beliefs with a subculture. Your brain didn't independently come up with a wild belief that is out of touch with everything you know/have been taught.
Consensus reality is a consensus. And even if the consensus you follow is shared by only 2% of the population, if that 2% is all the people you relate to and consider to be the people "in the know", then you are in a way not going against your contextual consensus reality. You've just picked a less popular one.
So what defines a clinical (psychotic) delusion is that it does not align with any consensus about reality that you have access to. It's your own, and it's unlikely that you have allies who are supporting your beliefs. Though in rare cases a clinically delusional person may be contributing new material to a subculture, that others then start believing, and as a result they do share their beliefs with a subculture. But they didn't just learn the belief from the subculture, the belief is growing and morphing independent of the group.
But yeah that's all clinically speaking. In a broader linguistic sense, I think people use "delusional" to refer to anyone who has beliefs that aren't aligned with the majority-consensus-reality, or even more simplistically, that aren't aligned with the speaker's understanding of consensus reality (usually as an insult). So an atheist might refer to the religious as delusional, and vice versa.
It may be a losing battle to get wider society to stop using 'delusional' in this way, but I think it is at least helpful to talk about how such "delusions" differ fundamentally from the psychotic experience.
685 notes
·
View notes
Text
also i got my first tattoo the other day and yeah it stung a bit (not nearly as bad as i expected though!) but it was actually strangely meditative? and its made me feel so much more connected to my body, which i didnt expect. like before it was like, yeah that's my arm i guess. now its like, yeah thats *my arm* with *my tattoo*. needless to say I'll definitely be getting more!
#dogpost#personal#no bold#piercings too. ive heard of ppl using body mods as a way of reinforcing their bodily autonomy but never really understood it til now
14 notes
·
View notes
Text
yesterday arvo & all night i felt on the verge of a panic attack, and this morning i finally was like. oh maybe i should check Inside. (which i never think of doing until I've been triggered/dissociated/[insert distressing experience here] for ages...). and Inside Parts were like yeah lol Its Time for a Repressed Memory again. and i was just like... well its really bad timing cuz I've gotta go to work, can it wait until we get home? and they were like yeah ok then. and bam, no more panic.
im not looking forward to getting home (for once!) but I'm thankful that we/they can put a lid back on those feelings until i can process them (and that next therapy session is next week!)
7 notes
·
View notes
Note
is avpd + npd & aspd possible? not about comorbidity just like. is it possible
yes! any combination of PDs is possible, even ones that seem to be polar opposites.
11 notes
·
View notes
Note
Hey not here to ask you to make a PD comorbidity post, but I am pretty sure you made an ASPD and PPD comorbidity post in the past. But I unfortunately cannot find it for some odd reason. Can you please send a link to it?
here you are!
8 notes
·
View notes
Text
Is AvPD a Disability?
Oof, what a question.
This week’s research post is going to get a little theory-heavy, so before we get to that let me explain why I chose this topic. I want to talk a little about what are called “models of disability.”
Why?
Because disability is an incredibly complex concept.
Definitions are wildly different from one another depending on what you’re reading or who you’re listening to. Do we even count mental health as part of ability or disability? And isn’t “disability” a messy word to begin with? Is it like “autistic” or “queer,” where we should follow the lead of the people who would choose that label for themselves and not apply it where people find it hurtful? Is it objective (anyone can define it) or subjective (depending on personal experience)?
I don’t have The Answers™ for you.
Instead, I’m going to talk about one of the most widely-used ways to define disability and then see how Avoidant Personality Disorder fits into that. Then you all can figure out what that means to each of you personally. I do want to provide a word of caution, however. Before you read any further, take just a few seconds to explore what the word means to you right now. Is it a bad word? If it were applied to you, would you feel seen or would you feel belittled? Why?
.
.
.
TL;DR: How we think about disability can change how we think about ourselves, what we can do, and what supports we need. Understanding what our needs are makes it easier to know what kinds of things to ask for so we can live our best lives.
Okay, here goes.
Keep reading
111 notes
·
View notes
Text
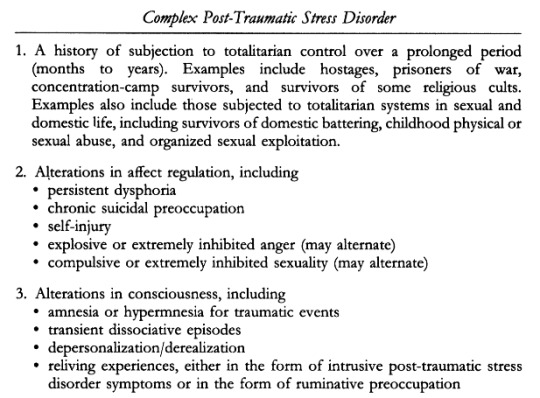
Judith Herman introduced the concept of Complex Post-Traumatic Stress Disorder in her book Trauma and Recovery (1992). Here is her diagnostic criteria:
1. A history of subjection to totalitarian control over a prolonged period (months to years).
Examples include hostages, prisoners of war, concentration-camp survivors, and survivors of some religious cults. Examples also include those subjected to totalitarian systems in sexual and domestic life, including survivors of domestic battering, childhood physical or sexual abuse, and organized sexual exploitation.
2. Alterations in affect regulation, including
persistent dysphoria
chronic suicidal preoccupation
self-injury
explosive or extremely inhibited anger (may alternate)
compulsive or extremely inhibited sexuality (may alternate)
3. Alterations in consciousness, including
amnesia or hypermnesia for traumatic events
transient dissociative episodes
depersonalization/derealization
reliving experiences, either in the form of intrusive post-traumatic stress disorder symptoms or in the form of ruminative preoccupation
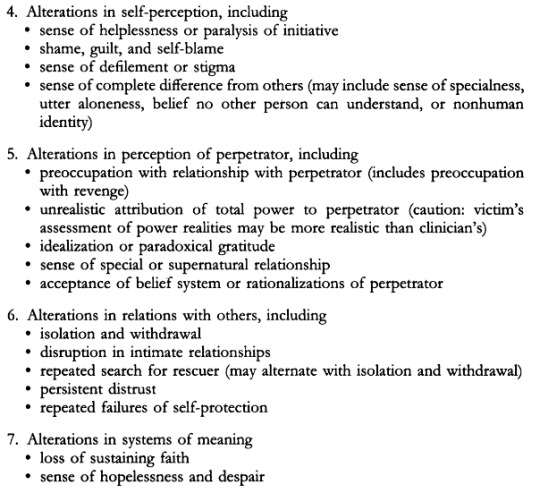
4. Alterations in self-perception, including
sense of helplessness or paralysis of initiative
shame, guilt, and self-blame
sense of defilement or stigma
sense of complete difference from others (may include sense of specialness, utter aloneness, belief no other person can understand, or nonhuman identity)
5. Alterations in perception of perpetrator, including
preoccupation with relationship with perpetrator (includes preoccupation with revenge)
unrealistic attribution of total power to perpetrator (caution: victim's assessment of power realities may be more realistic than clinician's)
idealization or paradoxical gratitude
sense of special or supernatural relationship
acceptance of belief system or rationalizations of perpetrator
6. Alterations in relations with others, including
isolation and withdrawal
disruption in intimate relationships
repeated search for rescuer (may alternate with isolation and withdrawal)
persistent distrust
repeated failures of self-protection
7. Alterations in systems of meaning
loss of sustaining faith
sense of hopelessness and despair
#complex ptsd#cptsd#judith herman#trauma and recovery#dogpost#described#described in alt text#described in post#trauma
137 notes
·
View notes