#Clinical Reviews
Text
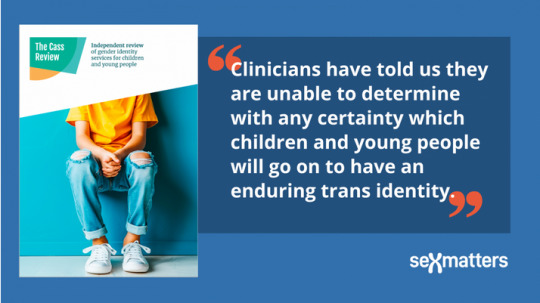
J.K. Rowling has been proven right!
"The Cass Review is a damning indictment of what the NHS has been doing to children.
"Dr Hilary Cass has submitted her final report and recommendations to NHS England in her role as Chair of the Independent Review of gender identity services for children and young people.
"Hilary Cass’s report demolishes the entire basis for the current model of treating gender-distressed children. Its publication is a shameful day for NHS England, which for too long gave vulnerable children harmful treatments for which there was no evidence base. It’s now clear to all that this was quack medicine from the start.
"Dr Cass delivers stinging criticisms of NHS gender clinics, both adult and child, and her description of the Gender Identity Development Service is absolutely damning. It is disgraceful that GIDS, alongside the adult clinics, did not cooperate with her attempt to survey its practice, or to carry out a high-quality, long-term follow-up study on the treatment of children as part of the review, which would have been a global first."

You can read the entire review here. (pdf)

"Glinner" is Graham Linehan, a writer, screenwriter, and comedian who's been fighting against transitioning minors for years, losing friends, his job, and his agent along the way. But he's kept on fighting.

,
;

.

.

The tide has turned in the UK and in Europe. When will American media finally begin reporting on the closing of "gender clinics" and the bans on puberty blockers for children? I figure nothing will happen here in the U.S. until the lawsuits start flooding in. It's already begun. And with proof like the Cass Review and the WPATH files, it's going to be very, very difficult for clinics, doctors, and therapists to continue lying about how transitioning does no permanent and irreversible physical and psychological harm.
#Cass Review#transing kids#JK Rowling#I stand with JK Rowling#Graham Linehan#trans lies#WPATH#WPATH files#gender critical#gender clinics#health#medicine#the tide has turned#David Tennant
525 notes
·
View notes
Text
UK petition: Sandyford Clinic [Scotland] to immediately continue to prescribe trans kids hormone blockers
[ Sign here ]
Following the Cass Review, trans kids are no longer able to receive puberty blocker prescriptions from Sandyford, Scotland's only gender identity clinic for under 18s.
This is devastating news for trans kids who will now see their bodies change in ways that will trigger dysphoria. It will ultimately cost lives as trans kids are driven to suicide. All this will happen because of some despicable, manufactured "trans debate", where trans kids, and adults, are being used as a scapegoat for society's problems.
Trans charities and advocate groups are condemning the awful Cass Review all over the country. The only groups celebrating this dreadful document are anti-trans ones.
Hormone blockers have been used for decades safely, and the vast majority of trans kids that go on to transition are happy.
A common argument against blockers is that trans kids are not old enough to make such decisions. This is exactly what puberty blockers are for; to hit the pause button on any irreversible changes; to give trans kids time to make these decisions.
We urge Sandyford clinic to immediately resume providing trans kids with their life-saving puberty blockers.
[ Sign here ]
#petition#UK#projects#cass review#cass report#armchair activism#puberty blockers#sandyford clinic#scotland#trans
597 notes
·
View notes
Text
almost halfway through the norwegian trans biography book and i think it's suffering from a common problem of this genre... it wants to be an introduction to Gender AND it wants to fight the discourse at the same time... it gets really crowded and messy!! i absolutely get where this is coming from, it's EXCEEDINGLY difficult to talk about your identity in a vulnerable, good faith way when it's been so drowned out by bad faith for so long, and the instinct is to get really defensive about it!! but it's a little tiresome haha
#the book has gotten plenty of praise of good reviews so im sure it's good for the cishets#im probably biased from Knowing All This already#i want to hear about norwegian specific activism and dirt on the gender clinic
71 notes
·
View notes
Note
Can dementia be prevented?
Reducing the risk of it yeah, w a healthy lifestyle. Preventing it no. The first patient I saw w the specific case of dementia I’m studying is a literal heart surgeon 💀 not the average bear at all. Big brain & healthy (according to his wife) & yet started showing symptoms over a course of 6 years.
It’s so fucking scary what dementia does to you. It’s far from just being cognitive stuff/memory loss. Your behavior changes, your cognitive skills are impaired, your motor skills take a hit. The heart surgeon I’m talking about is struggling w mouth function rn, bc his muscles are atrophying as a direct result of his dementia. He legit went from operating cardiovascular surgeries last October to now not being able to speak. It’s different from case to case, but when it’s aggressive it’s fucking aggressive. The neurologist I’m shadowing was talking about how she doubted if he’d “still be here within the year” and I wanted to throw up bc what do you mean if he’ll still be here!!
#His wife loves him sm too#And I gave her a hug on my way out of the clinic#She pulled me into it literally. The caregiver’s burden is real#They don’t have kids either so idk what she’ll do when/if he passes away#And that was the first case that I saw too. Just one. And already so much to unpack#I’m doing my chart review on another patient but his story is no more sunny#Dementia is fucking vicious#ask#med tag
58 notes
·
View notes
Text
I've never seen dungeon meshi but it's all over my dash so here are the characters from what I've gathered:
Autistic hungry man
The sister of autistic man (also autistic)
The bad bitch the sister pulled by being autistic
👁👄👁 (evil? twink)
Gimli from lord of the rings
A dad who loves his family very much and hates being in the dungeons idk how he ended up there but he definitely wishes he was home
#also i know blond autistic man is there to eat#but where did the rest come from???#like i know this show has some sort of plot but it seems to me like#they heard good reviews from this all you can hunt buffet-dungeon and things? happen? maybe?#also blue-eyed twink is probably deranged like he is clinically insane#and gimli is the actual sweetheart of the show#dungeon meshi#m ya callate
22 notes
·
View notes
Text
Ch204 (p2), Bodies and souls
The head matron drops that bomb from ch203 that Theo is to fledge next.

I'm a bit confused why they mention Nick, except that he would be the next candidate for real Ciel, if Theo wasn't there. I was worried for a moment there that they had already fledged Nick without us even knowing about it. However, they talk about Ginny in past tense and Nick in present tense, so he must still be there.
Gosh, this young Black lady here. I hope she turns against the orphanage, because I can tell she feels deeply that this is not acceptable. Partly, she is asking because she doesn't know everything that the head matron has already been told, or perhaps she has forgotten what she was already told. Either way, she still wonders why it has to be like this.
The head matron uses the same terms Blavat used at Sphere Music Hall: radiance, stars. However, "aptitude" has been added. She acts like it's these "stars" themselves who "possess technologies way more advanced" that theirs, as if they are from some advanced alien civilization.

It's odd for her to talk about not just their bodies but also specifically their souls. Someone has told her that their souls need to be as similar to the souls of the "stars", too, not just a match in their bodies. This reminds me of what was told (probably by Undertaker) to Chris Heathfield, and that the baron repeated to Jane.
So, I'm definitely not giving up my theory that Undertaker is experimenting with soul transplants, too, not just blood transfusions and organ transplants. To him, a soul is basically an organ, anyway, right? It could be that the best way for them to match their souls is by assessing their aptitudes. It's not just the blood typing, it's the combination of blood type and aptitude test results. And then reinforcing the similarities. She even has the nerve to call this a "clinical trial".
But Susan doesn't care too much about the details, as she hopes to use her high earnings to leave soon and open her own business, some sort of shop. I wonder where the money is coming from to keep paying such high wages, since we saw those money-donating renal patients die, but it could be coming from the hotel resort in Brighton....

Susan goes to the cold vault to get blood for Doll, and we see they have also been storing blood for the other lords of the stars. Though it's possible they don't currently have any for Sirius, which would help explain why a Pomeranian like Theo would be next.
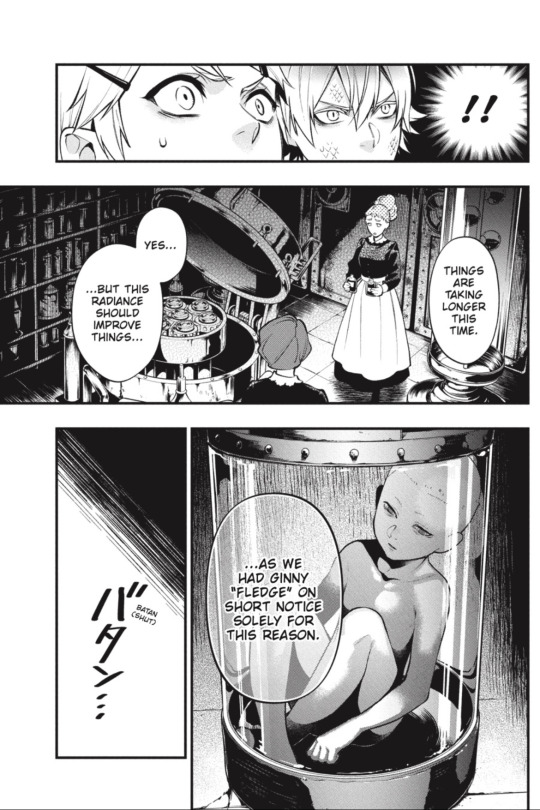
Now this is interesting. "Things are taking longer this time"... compared to what? Last time Doll needed blood? Or something else about Doll's condition? What, exactly, is taking longer this time? 🤔
#black butler#kuroshitsuji#ch204#chapter release#chapter review#chapter analysis#fol orphanage#susan#staff#ginny#doll#blood types#blood transfusion#soul transplants#experiments#clinical trials#soul shapes#shapes of souls#theo#theodore#lords of the stars#radiance#lord canopus#lord sirius#sep 15 2023#part two#part 2
77 notes
·
View notes
Text



Hi, internet. This is what trauma bonding means. Don’t use TikTok and memes as sources for mental health info, and please educate yourself before adding to the unfortunate buzzwords these terms have become.
10 notes
·
View notes
Text
ngl, self-diagnoses doesn't harm anyone.
"They're taking away resources from actually autistic people!"
where. proof for that. Also, most resources that non-diagnosed autistic ppl can get are just DIY remedies(headphones, sensory toys, ect), how is that taking away from your remedies.
i think instead of saying "no you cant self-diagnose or can only under specific circumstances", we should be sharing resources to help people who are questioning if they really have a condition or not
if you want ppl to stop incorrectly thinking they have autism, maybe we can just make content where we talk abt what autism actually entails and what is/isn't an autistic trait.
instead of saying all self-diagnosers are faking on purpose
Information is the best killer of misinformation actually if you didn't know
#autism#self diagnosis#neurodivergent#neurodiversity#mental health#mental illness#like im only clinically diagnosed with depression and anxiety#but do you know how expensive a psychiatrist is? or how much energy it takes that i just dont have (for some reason)#and the history of mental disorders in my family give me a good idea on what i have#so like no im not faking i just cant afford a piece of paper that confirms it#plus peer reviewed diagnoses are never talked abt in these debates#bc i never considered autism until my diagnosed (since before 10 yrs) friend mentioned i might have it
10 notes
·
View notes
Text


More information about Stanford research goals and the RECOVER Program/Initiative:
#covid-19#covid 19#sars cov 2#covid#long covid#long haul covid#Stanford#Clinical Trials#Paxlovid#Antivirals#Research#RECOVER#RECOVER Program#National Institute of Health#NIH#Institutonal Review Board#IRB
92 notes
·
View notes
Text
there is a future version of me who has a huge hog that he puts in people's holes. and also he's proud of me or whatever. but mostly rn i'm thinking about his dick
#SORRY IM REALLY EXCITED I WAS LOOKING UP REVIEWS FOR PHALLO CLINICS IN MY COUNTRY AND THERES#ONE WITH SEVERAL RAVING REVIEWS THATS LITERALLY IN THE CITY IM ABOUT TO MOVE TO ANYWAY#AAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAA COCK TIME
9 notes
·
View notes
Text
stop
#chloe shush#the coworker who called me out on something that I literally didnt do wrote a label on a prescription wrong#so apparently everyone at the clinic is being harassed about how they poisoned her dog#(the dog is better now-???) so like huh but#mY MANAGER ASKED ME IF I CAN GIVE THE CLINIC A 5 STAR REVIEW IM SOBBING
7 notes
·
View notes
Text
i gotta call my mom and thank her for the teeth of steel i was apparently born with
#they are in SURPRISINGLY GOOD SHAPE for what i've put them through#i have 2 cavities and no other major concerns and will be going back on the 8th to get them filled#everyone at the clinic was so fucking nice like they earned that 4.9 on google reviews#also i uh. yeah i just became resistant to ibuprofen#i have acetaminophen now and will alternate as needed#also they called in xanax for the day of for my anxious ass \m/#tox.txt
7 notes
·
View notes
Text
hate this fucking college why are you taking every step possible to make it harder for us to be good practitioners this is insane
#like WHY do we have to jump through 15 thousand flaming fucking hoops to get access to basic resources#that almost every other medical school readily provide for their students i don't get it do you want us to be good at our jobs or not#and they're always so obscure and never transparent with their assessments it's so awful and does nothing but stunt our learning#because instead of focusing on effectively understanding basic medical sciences and retaining clinical skills instead i have to put my time#and energy into figuring out how the fuck im supposed to prepare for you dumbass nonsensical assessments that you never let us review#so that i can pass salvage what's left of my gpa get the fuck out of here omg pisses me off so much
9 notes
·
View notes
Text
happy new year!! I had a horrible nightmare that (check the tags before proceeding please) I had to get a surgery to release some kind of fluid buildup in my brain and the surgery involved drilling a hole into my skull and I didn't find out they weren't intending to put me under until I was on the operating table with the nurse hovering over me with a GIANT drill
she reassured me they gave me local anesthesia but i flailed and begged to go to sleep and tried to shove the drill away while the nurse basically forced me into position, and I kept tapping my skull trying to confirm that the local even did anything because I couldn't remember them administering it. before I knew it they were drilling into the side of my head and it wasn't painful, so I guess the stuff worked, but I could hear it and feel it the way you feel what the dentist is doing even when there's novocaine. eventually i stopped yelling and fell silent because the drill was so loud and what can you even do at that point.
when they were done they cheerfully showed me an x ray of the hole they made, which went ALL the way back to my spinal cord and brain stem and stopped just a millimeter short of touching them, and they acted like this was normal and they hadn't just gone within a hair's breadth of killing me, and then they gave me a flimsy paper towel and told me I'd just need to hold it over the fresh hole in my head for awhile until it healed.
bizarre and upsetting New Year's Day dreams are practically a tradition for me at this point but, genuinely, what the Fuck was that.
#tw medical#tw medical trauma#tw surgery#tw body horror#tw nightmares#cant decide if this is better or worse than the religious nightmare i had a handful of january firsts ago#my dreams#jan 2024#happy new year!!! :) :) :)#trying to figure out what in my waking life could have possibly prompted this#it's probably a combination of stresses all rolled into one big awful thing tbh#i guess the thrust is i wanted to be fixed or cured of something but i didnt get to be in control of how that happened#and the solution felt archaic and the aftercare was nonexistent#and i mean that's. a sensible thing to be afraid of#it wasn't even clear in the dream if the procedure even helped#but i went to this clinic at the recommendation of someone i knew. whose input- in waking life- i dont especially trust. so#maybe there's something to unpack there#ive also had friends experience some really shocking malpractice this year#and i'm still paying off medical debt#and doing year in review has brought up some unpleasant emotions as i'm realizing this year was more stressful than i thought#like a major element of this dream was 'yes i did sign up for this but some Very Important Information was withheld from me' which HONESTLY#sums up a lot of my year >_>#AND on top of that i've been wrestling with faith stuff. not getting to pick the healing process and fearing the outcome... yea#at the end of the day it's just another stress dream. it just took a form it doesnt usually take so it stands out#blegh. we'll get through this
15 notes
·
View notes
Text
I’ve always loved medicine bc it’s the perfect intersection of science and humanity—the two things I value above all else in this world. Truly adored it since I was in the cradle. But now I’m thinking about how so much of my journey to neurosurgery will have to involve KILLING my feelings essentially bc how do you survive otherwise
#Not to mention the surprisingly high suicide rate of surgeons that’s been brought to my attention lately#Honestly I just started my neuro internship and just saw my first patient in clinic#And on the day I did I was critical of my neurologist for being so robotic about it#Now I can see why#I’m still at a point where I can’t even do a chart review for a patient without feeling so fucking sad#And I can see how that can get unsustainable after a while#But it’s like if I kill the feelings that drive my passion for medicine to begin with then what’s the point#It’s not like I’m in it for the money or prestige bc that’s so dumb considering how long the schooling is#But literally how to deal#My supervisors at the clinic very much all speak about the dementia patients w a learned impartialness#But I don’t wanna be that way one day :( but how to be anything else and still survive#I’m pre med so I still have time and maybe my opinion will change and I’ll wanna do another specialty#But when it comes to this every specialty will involve human lives and navigating that regardless#That said I can see why surgeons are at higher risk or depression suicide etc#The whole point of this internship is to teach myself how to navigate this stuff but. Hate it#p#med tag
57 notes
·
View notes
Text
By: Bernard Lane
Published: Dec 12, 2023
The gist
Analysis
An Australian health minister, Shannon Fentiman, who is responsible for the busy gender clinic of the Queensland Children’s Hospital, has acknowledged the lack of consensus on how to treat gender dysphoria.
Four words stood out in Ms Fentiman’s otherwise cagey, scripted response to a question in state parliament about the source of the evidence justifying the puberty blockers and cross-sex hormones given to minors by the Brisbane-based clinic.
“Whilst acknowledging that best practices rely on some aspects of transgender health care and there is not consensus [Emphasis added], the work continues,” she said on November 30.
Child and adolescent psychiatrist Dr Jillian Spencer, who has been calling for an independent federal inquiry into the care of gender dysphoric youth, welcomed Ms Fentiman’s concession reflecting the state of medical opinion—a concession not forthcoming from Australia’s other health ministers.
“It is such a relief to have [Queensland’s] health minister finally acknowledge that there is not consensus regarding the best practices for transgender healthcare,” Dr Spencer told GCN.
Dr Spencer is a critic of the “gender-affirming” treatment approach followed by the Queensland gender clinic. Earlier this year she was suspended from clinical duties at the children’s hospital reportedly after a patient lodged a complaint of “transphobia”.
“The minister says that the work of the [clinic] continues despite the lack of consensus on best practice for transgender healthcare,” Dr Spencer said.
“Why is the work of the [clinic] continuing if there is no consensus? Shouldn’t we be more careful than that—especially when the health of children is at stake? Parents want cautious and evidence-based healthcare for their children.
“The children and parents of Queensland deserve to have paediatric gender services that are based on a systematic review of the research evidence similar to what is happening in the UK with the Cass Review.”
She challenged the advice given to Ms Fentiman that the work of the Queensland gender clinic represented “international best practice”.
“[It appears her advisers] have failed to let her know that, internationally, when [countries such as Finland, Sweden and the UK] have conducted independent, systematic reviews of the research literature, they have moved away from an affirmative approach to prioritise psychosocial interventions rather than puberty blockers and cross-sex hormones”.
“A new front in the struggle over transgender issues has opened up. Two [US] medical malpractice lawsuits, each levied by a plaintiff who regrets having undergone medication-based gender-transition treatment—one at age 14—have taken aim at the American medical establishment’s support for prescribing such drugs to minors.”—Journalist Benjamin Ryan, news report, New York Sun, 5 December 2023
---
The detail
Behind the scenes
Minister Fentiman’s remarked on the lack of medical consensus during her short November 30 reply to Robbie Katter MP, whose question was prompted by Ms Fentiman’s earlier reassurance that care at the gender clinic was “of very high quality and based on the best available evidence.”
The minister’s surprising concession to critics of the gender-affirming approach—the approach enforced at the gender clinic—chimes with the reference by Queensland’s chief psychiatrist, Dr John Reilly, to plans for an “independent review” of the clinic.
GCN has sought clarification on both points from the government; there was no reply.
Might Queensland be the first Australian jurisdiction to publicly acknowledge the force of the international debate about medicalised gender change for minors? Have there been frank discussions, even talk of doing something, in Ms Fentiman’s office or among her health and hospital officials?
The main focus now for Queensland’s governing Labor Party is re-election. In power since 2013, the party has shuffled its leadership as it prepares for the state poll scheduled for 26 October 2024.
It appears that Steven Miles, a former health minister, will succeed the long-serving Annastacia Palaszczuk as premier.
Ms Fentiman, a solicitor from the party’s left faction, was briefly in the running. Her narrative was change and renewal, a government with “the maturity to admit where we have fallen short.”
Does anyone think that concerns about gender medicine will have evaporated by next October?
--
Affirmed by guidelines
Minister Fentiman’s November 30 defence of the gender clinic boiled down to its “adherence to peer-reviewed national and internationally accepted published practice clinical guidelines”.
She cited the latest, 8th edition of standards of care issued last year by the World Professional Association for Transgender Health (WPATH), which she said evinced “a rigorous and evidence-based approach”.
She also invoked the 2017 clinical guideline of the Endocrine Society, offering to get a copy for Mr Katter, who represents a minor party in the parliament.
And she cited a third document, the 2018 “Australian standards of care” issued by the Royal Children’s Hospital Melbourne.
Back in September, Ms Fentiman had said the gender medicine practised by the Queensland clinic was “an emerging field globally—no-one shies away from that—but the evidence base is sound.”
In fact, the evidence base for medicalised gender change for minors is very weak and uncertain, according to five independent systematic reviews since 2019 in Finland, Sweden, the United Kingdom (one review each for puberty blockers and cross-sex hormones) and the American state of Florida.
The founder of the Queensland gender clinic, Dr Stephen Stathis, recently conceded the complaint of sceptics that the evidence base for gender-affirming treatment is of low quality, although he argued this was not unusual in the field of child and adolescent psychiatry.
Lack of solid evidence has led gender-affirming clinicians and activists to rely heavily on treatment guidelines and position statements from medical organisations when claiming that puberty blockers, cross-sex hormones and surgery are “settled science”.
But systematic reviews are regarded as the highest form of evidence, while treatment guidelines and position statements—representing expert opinion or professional consensus—are the lowest.
And it’s arguable that gender-affirming treatment guidelines do not even reflect expert consensus, as Ms Fentiman’s arresting remark suggests.
The extent of health professional dissent from the gender-affirming model is masked because it is well known that critics will be smeared as “transphobic”, subjected to bad-faith complaints and have their careers put at risk.
If in truth there is no consensus, the treatment guidelines cited by Ms Fentiman are misleading and cannot justify the risky medical interventions given by the gender clinic.
It’s unclear how this contradiction in the minister’s November 30 statement arose. Does it reflect a confused briefing from her advisers and officials, or a belated awareness that gender-affirming medicine is hardly settled science?
--
Reviewphobia
In any case, the problem for Ms Fentiman is that her faith in those three treatment guidelines is misplaced.
The “rigorous” WPATH guideline process involved a chaotic last-minute abandonment of minimum ages for most hormonal and surgical interventions; the rationale appears to be to give clinicians better protection against malpractice suits.
Credible guidelines draw on a systematic review of the evidence. WPATH’s new chapter on adolescents—the group that is the focus of international concern—involved no such review. WPATH pleaded the scarcity of studies on early medical intervention.
And yet early medical intervention is what the guideline recommends. Perhaps WPATH was worried about the predictable output of a systematic review, not the meagre input.
Scarcity of studies did not prevent Sweden’s systematic review of the evidence. Its literature search began with almost 10,000 research abstracts and identified just 24 relevant studies for evaluation.
One of the experts involved, Professor Mikael Landén of the Karolinska Institute said—
“Against the background of almost non-existent long-term data, we conclude that [puberty blocker] treatment in children with gender dysphoria should be considered experimental treatment rather than standard procedure. This is to say that treatment should only be administered in the context of a clinical trial under informed consent.”
The gender clinic that Ms Fentiman celebrates for its “life-changing care” gives puberty blockers as routine treatment. And remember, Queensland’s parliament has been assured by the minister that “the evidence base is sound”.
--
A matter of trust
Ms Fentiman also cited the 2018 “Australian standards of care” from the Royal Children’s Hospital Melbourne (RCH), noting its publication as a position statement in the Medical Journal of Australia (MJA).
But that cut-down version of the guideline, shielded by the journal’s pay wall, contains an admission not found in the full guideline which is the document that is readily available on the hospital website and relied on by youth gender clinics across Australia.
The MJA version says: “The scarcity of high-quality published evidence on the topic prohibited the assessment of level (and quality) of evidence for these recommendations.”
Earlier this year, GCN put this claim to Professor Gordon Guyatt, a pioneer of evidence-based medicine and the GRADE system for rating evidence quality.
“[That claim] is enough for me to say this is not a trustworthy guideline”, Professor Guyatt said.
The RCH guideline was considered for inclusion in the National Health and Medical Research Council’s online portal Australian Clinical Practice Guidelines but did not qualify.
“At the screening stage it was determined that the guideline did not include a funding statement, an evidence base for the recommendations or information about conflict of interest, and that it would not meet the portal selection criteria, so a full assessment was not carried out,” a spokeswoman for the NHMRC said in 2021.
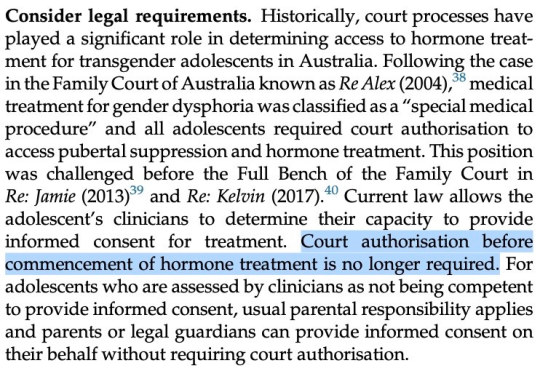
[ Screenshot: Advice from the 2018 RCH “Australian standards of care” document ]
--
Divided opinion
Also in 2021, the Royal Australian and New Zealand College of Psychiatrists (RANZCP), which had previously endorsed the RCH guideline, issued a new more cautious policy on gender dysphoria.
Its policy says that “evidence and professional opinion is divided as to whether an affirmative approach should be taken in relation to treatment of transgender children or whether other approaches are more appropriate.” (Note: After posting this article, I was alerted to an update of the RANZCP’s gender dysphoria policy, which I will report elsewhere.)
In its recently updated guide, the National Association of Practising Psychiatrists says “there is no consensus that medical treatments such as the use of puberty-blocking drugs, cross-sex hormones or sexual reassignment surgery lead to better future psycho-social adjustment.”
No consensus, but the Queensland Children’s Hospital requires health professions to follow the gender-affirming model rather than allowing a neutral therapeutic approach.
We know this because psychiatrist Dr Spencer has raised concerns—initially within the hospital, then publicly—about the potential harm done to minors by unthinking “affirmation”. She even wrote to the minister about this.
“I started testosterone five years ago today. After 4+ years of weekly injections to maintain such dangerously high hormone levels, I had elevated liver enzymes, heightened red blood cell counts, and regular heart palpitations. I am so grateful I stopped when I did.”—American detransitioner Morgan, tweet, 4 December 2023
--
Low-quality advice
Ms Fentiman’s third guideline, from the Endocrine Society, has an important feature that her advisers appear to have overlooked.
Unlike the RCH document, the 2017 Endocrine Society guideline did rate the quality of evidence supporting their treatment recommendations.
Five of the society’s six recommendations on puberty blockers depend on evidence rated as “low quality”.
The sixth recommendation—for administering blockers in early puberty, as is done at Queensland’s gender clinic—rests on “very low-quality” evidence, the lowest possible rating. Awkward but important details, rarely mentioned.
Also unmentioned is the society’s careful disclaimer that its “guidelines cannot guarantee any specific outcome, nor do they establish a standard of care.” Not helpful for those demanding a monopoly for gender-affirming care.
In July this year, the society’s president, Dr Stephen R Hammes, made the claim that, “More than 2,000 studies published since 1975 form a clear picture: Gender-affirming care improves the well-being of transgender and gender-diverse people and reduces the risk of suicide.”
This, he said in a letter to The Wall Street Journal, was the evidence used by the society in its “rigorous process” to develop the 2017 treatment guideline.
He provoked a dramatic and humiliating response—a letter of sharp dissent signed by 21 clinicians and researchers from nine countries involved in the care of teenagers with gender distress.
Among them was Finland’s reformist pioneer of gender medicine, Professor Riittakerttu Kaltiala, whistleblower clinicians from England’s Tavistock clinic Dr Anna Hutchinson and Dr Anastassis Spiliadis, and Belgian expert on evidence-based medicine Dr Patrik Vankrunkelsven.
All systematic reviews to date, the letter’s authors pointed out, had “found the evidence for mental-health benefits of hormonal interventions for minors to be of low or very low certainty.”
“Dr Hammes’s claim that gender transition reduces suicides is contradicted by every systematic review, including the review published by the Endocrine Society, which states, ‘We could not draw any conclusions about death by suicide.’ There is no reliable evidence to suggest that hormonal transition is an effective suicide-prevention measure.
“The politicization of transgender healthcare in the US is unfortunate. The way to combat it is for medical societies to align their recommendations with the best available evidence—rather than exaggerating the benefits and minimizing the risks.”
So, is Minister Fentiman confident that she had been given an apolitical and accurate summary of the benefits and risks of treatment at Queensland’s gender clinic?
“Opinion is divided about the certainty of the evidence base for gender-affirming medical interventions in youth. Proponents claim that these treatments are well supported, while critics claim the poor-quality evidence base warrants extreme caution. Psychotherapy is one of the only available alternatives to the gender-affirming approach. Discussion of the treatment of gender dysphoria in young people is generally framed in terms of two binary approaches: affirmation or conversion. Psychotherapy/exploratory therapy offers a treatment option that lies outside this binary, although it is mistakenly conflated with conversion therapies.”—Psychiatrist Dr Roberto D’Angelo, article, Journal of Medical Ethics, 2023
--
Just the one
Also, in the spirit of governments owning up to mistakes, Ms Fentiman might revisit something she said about Dr Spencer.
On September 14, Mr Katter raised the issue of the compulsion for doctors to use the gender-affirming model with dysphoric children, and asked, “Will the minister intervene to restore the ability of doctors—including Dr Jillian Spencer, who has been stood down—to use their professional medical discretion when treating gender dysphoric children?”
Ms Fentiman replied—
“I understand there have been a number of complaints made by patients in relation to Dr Spencer. These complaints are subject to a number of HR processes within Children’s Health [which runs the hospital] as well as referrals to [the health professions regulator] Ahpra and the Health Ombudsman.”
A possible implication of Ms Fentiman’s comment is that Dr Spencer had engaged in a pattern of conduct attracting multiple complaints from patients.
Last month, thanks to a right of reply mechanism, a correction from Dr Spencer was placed on the parliamentary record—
“The minister’s statement suggests that I am the subject of a number of patient complaints. That is incorrect. There is only one patient complaint lodged against me.”
--
“After being expelled from my master’s degree for speaking out about the impact of gender ideology on child safeguarding, I am extremely pleased to announce that I have agreed a settlement with the UK Council for Psychotherapy. [The council] have published a formal statement protecting therapists who believe in biological reality and stand against irreversible medicalisation of children. They say training institutions should never discriminate against students on this basis.”—UK lawyer turned trainee therapist James Esses, tweet, 11 December 2023
GCN sought comment from Ms Fentiman and RCH
==
Australia lumbers drunkenly towards figuring out this is all a major medical disaster.
#Bernard Lane#Gender Clinic News#systematic review#gender clinic#queer theory#gender ideology#medical scandal#medical malpractice#medical corruption#gender affirming care#gender affirming healthcare#affirmation model#Shannon Fentiman#no consensus#cross sex hormones#wrong sex hormones#puberty blockers#low quality evidence#religion is a mental illness
10 notes
·
View notes
Last Seen Blogs

555-95472
five five five five five

mybluetiedangel
MyBlueTiedAngel

europadokumente24hrsat
Untitled

noonegivesaf1ck
Just cringe idiot

countdown-til-sanders-take-over
Let's see how powerful the countdowns are