#Epigenetic Watch Method
Text



Today’s throwback is to Jenson Leonard’s solo exhibition Workflow, at Wood Street Galleries in Pittsburgh, from the beginning of February.
From the gallery about the work-
Workflow, the first institutional solo exhibition of artist Jenson Leonard, centers on a titular film that explores the velocity and momentum of Blackness as it relates to the philosophical concept of acceleration—the notion that the only way out of capitalism is through its intensification.
In Workflow, a spectral Michael Jackson Halloween mask recites a surrealistic quarterly earnings reports. Building on a 2017 essay by artist Aria Dean titled “Notes on Blacceleration,” the short film centers on the ways in which the Black subject grapples with its commodified status within the labor market despite—or, resultant of—its own history as a commodity, stemming back to the Trans-Atlantic slave trade. Completed during Leonard’s residency at Pioneer Works in 2021, the video utilizes uncanny humor as a mechanism to expose the shared grammars inherent in Afro-pessimism and speculative finance.
Within the exhibition, the film repeats simultaneously across two grids of computer monitors situated on ergonomic desks that flank the gallery, mimicking the workstations that can be found ubiquitously across stock trading floors and financial institutions. Sculptures modeled after computer keyboards and mouses are displayed on the desks, each rendered inoperable by concentric riffs that symbolize the erratic transformations caused by the flows of capital. The appearance of Jackson represents a transmogrification of its own; whereas many have aligned the controversial pop icon’s bleached skin and surgical procedures with Black self-hatred, Leonard positions his bodily modifications as a radical rupture from racial paradigms of being.
In Leonard’s own words, “Workflow is defined as the sequence of industrial, administrative, or other processes through which a piece of work passes from initiation to completion. My film seeks to disabuse notions of completion, whether it be completion of the human, the nation state, or civil society. As Dean notes, Blackness is ‘always already accelerationist’ via its incongruence with Western humanism, a wrench thrown into the locomotive gears of ‘capital and subjecthood.’ Her essay prompts us to look toward the way that the Black has been historically constructed outside of the human, as coterminous with the slave. Slavery therefore represents a kind of proto-automation, a mass forced coercion of labor, and the Blacks’ transition from object to subject calls for a reappraisal of accelerationist ideas about the (non)human entity and its revolutionary potential.”
The artist continues, “There is something about going to work—the repetition of it—that gets inscribed at an epigenetic level, as an everyday, embodied violence. From there, I thought about the panoptic workplace (open air plan, transparent yet closely surveilled, management that does not have to be in the room to be monitoring you), the fetish of efficiency (ergonomic mouse and keyboards so you can work longer), biometric data of a labor force (fingerprint and facial scans to help reduce repeat processing tasks). All of these methods to maximize profits and production can be traced back to methods worked out and perfected in the cotton and sugar cane fields hundreds of years prior.”
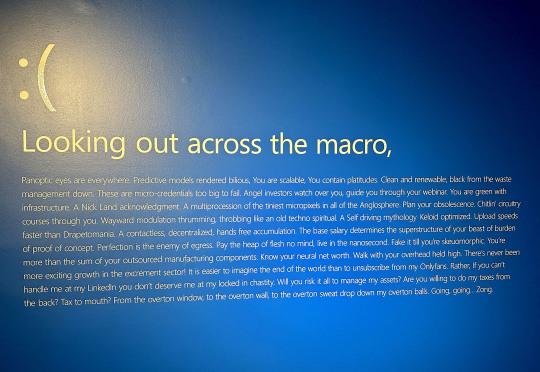
The text from the video was included on one of the gallery walls (image above) but I’ve included it below as well as it is definitely worth reading.
“Looking out across the macro- Panoptic eyes are everywhere. Predictive models rendered bilious, You are scalable, You contain platitudes. Clean and renewable, black from the waste management down. These are micro-credentials too big to fail. Angel investors watch over you, guide you through your webinar. You are green with infrastructure. A Nick Land acknowledgment. A multiprocession of the tiniest micropixels in all of the Anglosphere. Plan your obsolescence. Chitin’ circuitry courses through you. Wayward modulation thrumming, throbbing like an old techno spiritual. A Self driving mythology Keloid optimized. Upload speeds faster than Drapetomania. A contactless, decentralized, hands free accumulation. The base salary determines the superstructure of your beast of burden of proof of concept. Perfection is the enemy of egress. Pay the heap of flesh no mind, live in the nanosecond. Fake it till you’re skeuomorphic. You’re more than the sum of your outsourced manufacturing components. Know your neural net worth. Walk with your overhead held high. There’s never been more exciting growth in the excrement sector! It is easier to imagine the end of the world than to unsubscribe from my Onlyfans. Rather, If you can’t handle me at my Linkedin you don’t deserve me at my locked in chastity. Will you risk it all to manage my assets? Are you willing to do my taxes from the back? Tax to mouth? From the overton window, to the overton wall, to the overton sweat drop down my overton balls. Going, going… Zong.”
#Jenson Leonard#Wood Street Galleries#Video Art#Pittsburgh Cultural Trust#Sculpture#Art#Pittsburgh Art Shows#Art Shows#Pioneer Works#Brooklyn Art#Brooklyn Art Galleries#Downtown Pittsburgh#Afro-pessimism#Michael Jackson#Aria Dean#Pennsylvania Art Shows#Pittsburgh Art#Political Art#TBT
2 notes
·
View notes
Text
✨WEEK: 6/17/24-6/23/24✨
R.E.P.O.R.T.S.
How did I REALIGN this week?:
6/17/24→ “love lights and fills me up” moms bday, hindz breath x3, garden
6/18/24→ “abundance is a portal and it appears for me” rafiq over
6/19/24→ “my goals are easily attainable” hindz breath, rafiq over
6/20/24→ “my financial abundance is far and wide” wildwood w rafiq
6/21/24→ “i trust my life is working for me” 30 workout
6/22/24→ “I breathe life through spirit into me” garden fence, breath jake, bunny full🌚 breath
6/23/24→ “my why keeps me going” hindz breath, workout, will probably do more tonight but posting early
What did I EAT & exercise?
I ACCOMPLISHED A PULL UP!!
What did I PRIORITIZE this week and what can I prioritize next week:
Next week: putting myself in the rooms & asking questions
This week: felt a little all over the place but had my tools to ground me when i got angry / frustrated
What did I OBSESS over this week:
Spending time with my man, went to wildwoof, parents were in rhode island so we had a few sleep overs
What would I RECOMMEND for next week:
-qi gong & breathwork to start every day!
what was your favorite TEACHING you learned?:
Begin before youre ready; you really dont understand something until youve done it
Focus on taking a small action to get momentum going & instill confidence
Youre not actually trying to find an idea for a business→ you’re asking “who are the people you’d like to serve?” “What problems can you solve?”
Words are cheap, money is not—> 1.are they actually paying for it? 2. Have they pre-ordered the thing? / put on the waitlist 3.would they be willing to be your 1st customer for a 50% discount?
OTHER NOTES/ LINKS:
https://www.youtube.com/watch?v=zVBHOKJgouI how to start a biz in 48 hours
https://www.youtube.com/watch?v=AMJNK6_e7Yk Patrick McKeown “you wouldn’t eat with your nose, so why breathe with your mouth”
https://www.youtube.com/watch?v=lurzpkhKtfk&t=1s lead generation strategy nick komadina
https://www.youtube.com/watch?v=2rpNfwTq6Xw can you teach perseverance
Dr joe dispenza film→ SOURCE
https://youtu.be/swR-lbJ6SU8?si=wvl-KRXnP1D7egI_ balaz mastering art of sales conversions
https://www.youtube.com/watch?v=SnFYdgLVNYQ balaz great sales keys from
^coaches starting out live coaching
The being method podcast → carrie b on sunlight healing us
https://www.youtube.com/watch?v=CK6uYrvD8qc gary Vaynerchuk build brand 7 min
Arabella Solution 6/23/24→ Healthy, Healing & Free
Q & A = what's a good morning routine? w/ gut routine → sunlight & grounding in the AM
The gut– must have healed gut in order to heal anything
Epigenetics→ dealt with lifestyle; you can turn certain genes off and on
Thoughts are language of the mind. Feelings are the language of the body.
Correct environment (people/what you're consuming) is vital for optimal healing.
✨12 steps to heal & get their sparkle back✨
But first: What are your symptoms? They are signals! It’s communication from your body. Your body is always communicating with you, There are solutions.
Recognize- identify what's making you sick and why you're chronically ill (you can't go to the dr and just get hormones, you haven’t solved the root cause: something has to change) (belief anything is possible has to happen here/before)
Reset- reset and create inner harmony; shift your health state + create + environment for optimal health (use food as medicine for more energy, less cravings: it’s easier to cleanse follow a journey)
Restore- regulate your nervous system to create physical + emotional safety + resilience, sleep deeper than ever before….and find a sense of internal peace.
Rewire- rewire your subconscious belief systems + coping mechanisms to create a new narrative around health (you can believe that anything is possible) (we are run by our subconscious belief systems)
Reconnect- your body holds deep wisdom. Shift from disconnection → connection + learn how to tune in, listen to your systems + allow them to quantum leap your healing (you don't have to reach outside of yourself for healing) (hearing the voices/whispers/gut instincts and honoring it) (learn discernment from yourself to know between fear & intuition)
Nourish-nourish your body + feed your cells + systems. Dive deep into how to use food as medicine to restore your health + vitality (you are safe, connected and tuning into what your body needs to survive and thrive) (everyone is different, diet plans won’t work for everyone)
Digest- learn the secrets of digestion and why it’s the key to healing all disease (when you’re sick→ your digestion system is typically weak)
Detox-use healing modalities to heal mind body + spirit by removing what no longer is serving you (detox is not a good thing if you’re already in depletion; it’s not safe, they need building up and nourishing)
Relationships- address all relationships you're in so you can thrive; address numbing/dissociation patterns
Release- let go of things that no longer serve us; habits; get rid of the anchor that’s holding you down/back/stuck
Life force- the energy flowing through your body; you cannot see but you can feel; most disease comes from the stagnation / stuck energy in the body(add qi gong to routine)
Longevity- establish a foundation for long-term success / health and the prevention of dis-ease
0 notes
Text
The NGS Oncology Market, Market Size, Market Share, Market Trends, Key Players
The global NGS oncology market is projected to reach $51,783.0 million in 2032 from 14,828.6 million in 2021, witnessing a CAGR of 12.04% during the forecast period 2022-2032. The growth in the NGS oncology market is expected to be driven by an increasing number of panels or kits, bioinformatics services for computational analysis, and a rising number of open-source free sequencing platform providers offering NGS oncology.
The landscape of cancer diagnosis and treatment is undergoing a revolutionary transformation, thanks to the advent of Next-Generation Sequencing (NGS) technologies.
Understanding NGS in Oncology:
Next-Generation Sequencing, or NGS, refers to advanced sequencing technologies that enable rapid and cost-effective analysis of DNA or RNA. In the context of oncology, NGS plays a pivotal role in decoding the genetic alterations in cancer cells. Unlike traditional methods, NGS allows for the simultaneous analysis of multiple genes, offering a comprehensive view of the genomic landscape of a tumor.
Download the sample page to know more @ NGS Oncology
Current Market Landscape:
The NGS Oncology Market has witnessed remarkable growth in recent years, driven by the increasing incidence of cancer worldwide and the growing demand for personalized medicine. Key players in the market include Illumina, Thermo Fisher Scientific, Qiagen, Roche, and BGI Genomics, among others. These companies are continually innovating and introducing advanced NGS platforms and solutions tailored for oncology applications.
Market Segmentation
By Sequencing Technology
By Offering
By Workflow
By Application
By End User
By Region
Key Trends Shaping the NGS Oncology Market:
Rising Adoption of Liquid Biopsies:
Liquid biopsies, which involve the analysis of circulating tumor DNA (ctDNA) in the bloodstream, are gaining traction in cancer diagnosis. NGS technologies play a crucial role in detecting genetic mutations and alterations in liquid biopsies, offering a non-invasive and real-time approach to monitoring cancer progression.
Integration of Artificial Intelligence (AI):
The integration of AI and machine learning in NGS data analysis is streamlining the interpretation of complex genomic data. AI algorithms help identify relevant mutations, predict treatment responses, and enable oncologists to make informed decisions for personalized cancer care.
Comprehensive Genomic Profiling:
There is a growing emphasis on comprehensive genomic profiling to identify a broader range of genetic alterations. NGS allows for the simultaneous analysis of multiple genes, providing a holistic understanding of the tumor's molecular profile. This information is crucial for selecting targeted therapies and predicting patient outcomes.
Theranostics and Targeted Therapies:
NGS enables the identification of actionable mutations that can be targeted with specific therapies. Theranostics, a combination of diagnostics and therapeutics, is becoming increasingly important in tailoring treatments based on the unique genetic makeup of each patient's cancer.
Future Prospects:
The future of the NGS Oncology Market appears promising, with ongoing advancements and innovations. Key developments to watch include:
Single-Cell Sequencing:
Single-cell sequencing technologies are evolving, allowing for the analysis of individual cells within a tumor. This level of granularity provides insights into intratumor heterogeneity, helping to understand the diversity of cancer cells and develop more targeted therapies.
Real-Time Data Analysis:
Real-time data analysis capabilities are improving, enabling faster and more accurate interpretation of NGS results. This facilitates quicker decision-making in clinical settings, leading to more effective treatment strategies.
Expanded Applications:
NGS technologies are expanding beyond traditional DNA sequencing to include RNA and epigenetic analyses. This comprehensive approach enhances our understanding of the molecular mechanisms driving cancer and opens avenues for novel therapeutic interventions.
Conclusion:
The NGS Oncology Market is at the forefront of transforming cancer care by providing in-depth genomic insights that guide personalized treatment strategies. As technology continues to advance, the integration of NGS with other cutting-edge approaches promises to revolutionize the way we diagnose, treat, and ultimately conquer cancer. The journey towards precision oncology is well underway, and the NGS Oncology Market is a beacon of hope in the relentless pursuit of more effective and targeted cancer therapies.
#NGS Oncology Market#NGS Oncology Market Report#NGS Oncology Market Industry#NGS Oncology Market Trends#NGS Oncology Key Players
0 notes
Video
youtube
Dr Parwinder Kaur is an award-winning scientist, a passionate leader and positive role model as a mother, and a professor in science for the next generation of diverse scientists to pursue their passion for science and discovery. She leads cross-disciplinary biotechnology research investigating Earth’s biodiversity and natural environments to ensure sustainable futures. She uses her expertise to reach people in new ways, connecting them with their surroundings. Through her diverse research teams, such as ExPlanta, she harnesses STEM to achieve maximised impact. In doing so, she believes this will help us tackle the bigger issues we as society are facing, bringing about solutions through fresh thinking rather than following usual norms. She has been recognised for her substantial contributions to biotechnology and scientific excellence by the prestigious “Science and Innovation Award” by the Australian Academy of Sciences in 2013, won the Microsoft's AI for Earth award for 2019 and WA Innovator of the Year (finalist) in 2022. Dr Kaur is a passionate science communicator, an entrepreneur in the biotechnology sector, an active mentor for gender equity, a Superstar of STEM, a Women in Technology WA Role Model, GirlsXTech international ambassador working to close the gender gap in technology and Diversity in STEM expert panel appointment with the Office of the Hon Ed Husic MP, Minister for Industry and Science, Australia.
In our conversation, we speak about biotechnology and genetics for conservation, and creating sustainable solutions through interdisciplinary innovation (amongst a whole host of other things).
Watch this episode on YouTube. Listen to it on Spotify, Stitcher, Apple Podcasts, Google Podcasts, Breaker, Castbox, Overcast, Pocket Casts, RadioPublic, or RSS.
Show Notes
[00:01:11] Parwinder's journey to molecular biology and the study of DNA.
[00:02:10] Growing up surrounded by different cultures and faiths.
[00:03:23] Parwinder's chemistry teacher opening the door to science as an avenue to answer her questions.
[00:04:28] Changing perspectives over time. The relationship between Ayurveda and epigenetics.
[00:06:16] Tools don't make the science, but they sure can make things go faster.
[00:06:47] Work that took Parwinder 7 years, now can be done in 7 days, because of tools.
[00:08:00] The knowledge needs to progress and we can help that along by making it more accessible to get a wider range of perspectives.
[00:08:38] Diversity is an important factor in innovation.
[00:11:07] How Parwinder's cultural and religious background inspires her science.
[00:13:18] There is enough old knowledge validated with science to suggest that we just need better tools or methods to get there as well.
[00:13:47] Investigating different faiths revealed to her that there are many common beliefs about the origin of life.
[00:14:35] Epigenetics. It's all connected.
[00:15:13] The road to understanding DNA in a three-dimensional space.
[00:19:35] We need to think bigger as well. Many of the problems we're trying to solve globally also must be viewed in multiple dimensions.
[00:24:32] Parwinder's work touches on so many different areas, what has been achieved could not have been done without multidisciplinary collaboration.
[00:25:53] Comparatively, Australia is less restrictive than India with respect to disciplinary boundaries.
[00:28:14] The system doesn't favour multidisciplinary approaches that may take longer.
[00:28:58] It's hard to inspire students to solve the problems around us if we can't allow them to explore a broader range of disciplines to find the solutions.
[00:33:17] Funding and KPIs can be bound to a limited scope.
[00:33:28] Obstacles to remote collaboration, and being a scientist in the most isolated city in the world.
[00:37:49] Remote collaboration with a medicine lab outside KPIs has lead to initiatives like DNA Zoo.
[00:41:55] Promoting Australia for its biodiversity and Perth for its Pawsey supercomputer.
[00:45:38] DNA Zoo.
[00:45:57] What can we learn about the superpowers of other species.
[00:47:24] Conservation has to factor in genetics as well as environment.
[00:48:47] The rate of innovation in genetics just for humans. Why not also for animals?
[00:49:36] With technological advancements, sequencing costs are significantly more accessible.
[00:52:55] It's about helping people connect the dots. Making the content public domain because this is bigger than just publishing papers.
[00:55:22] Open data because not having access to the knowledge is inefficient and making it accessible allows more people to take a shot at it.
[00:56:57] Data is our next bio-economy.
[00:58:21] Methane from cows.
[00:59:54] The factors that contribution to methane emission.
[01:00:22] "You are what you eat". Let's look at diet.
[01:00:49] Clovers and their simplicity and impact, and secondary discoveries in science.
[01:03:00] Japanese research on red clovers and their applications.
[01:04:27] A serendipitous conversation about kombucha.
[01:05:44] From a joke to a commercial opportunity in synthetic biology.
[01:07:29] Giving her students another option for a career path in entrepreneurism.
[01:10:57] Bonus Question 1: What hobby or interest do you have that is most unrelated to your field of work?
[01:12:41] Bonus Question 2: Which childhood book holds the strongest memories for you
[01:15:17] Bonus Question 3: What advice you would give someone who wants to do what you do? Or what advice should they ignore?
Learn More About Parwinder
Twitter: @dr_parwinder
ExPlanta: https://www.explanta.com.au/
DNA Zoo: https://www.dnazoo.org/
LinkedIn: https://www.linkedin.com/in/dr-parwinder-kaur-715745199/
Follow STEAM Powered
YouTube
Facebook
Instagram
Twitter
Patreon
#SteamPoweredShow#WomenInSTEAM#WomenInSTEM#DNA#biotechnology#genetics#conservation#SustainableSolutions#interdisciplinary#innovation#diversity#entrepreneurs#SyntheticBiology#OpenData#DigitalCommons
0 notes
Text
PRECOGNITIVE DREAMS, THE HYPNAGOGIC STATE, & SYNCHRONICITY
thoughts/notes on this podcast sent to me by @jaehaerys1 thank you! just want to document this here so I don’t forget
hypnogogia - in between sleeping and waking (hypnopomic - waking up, hypnogoga - falling asleep)
“precognitive dreams” --> An Experiment with Time by J. W. Dunne [seeing events in advacenment in dreams before they take place in reality]
yes I have felt extreme deja vu frequently - Dunne-type dreams - throughout my life and it’s embarassingly lead to me to think I could predict the future - I am relieved this is covered here as I didn’t realize this phenomea was related to my dream observations (Dunne mentions this is a common human experience! very validating)
symbolic distortion
repetitive dreams following chronology predating events in reality - recurring precognitive dreams
“we can watch dreams form... while still being awake”
people work at this to learn it and try it... I wonder if this experience is vastly different than involuntarily towing this line? the first time I had a hypnopomic hallucination I was so frightened I thought I was going to die
Hidden Symbolism of Alchemy and the Occult Arts by Herbert Silberer
the symbols are not random - reflective of emotional or physical state
“dreams are a commentary and they serve a compensating function”
“tight focal point” --> ego
the unconscious teleologically compensates mechanically, the perspective tendency of the unconscious is that it is future orientated (not chained to our past/developmental experience)
often someone else can dechiper your dream messages more effectively than you -- it is YOUR unconscious [I should get a dream journal]
evolution developed methods to preserve dreaming -- why
cool mention of epigenetics around 42 minutes [I have been interested in and advocated for this topic - anti darwinist ideas]
law of serriality, different to Dunne’s serrialism
consciousness can become unanchored
Dunne’s Levels
Level 1 - fixed on present
Level 2 - dream state, mix future and past
Level 3 - above 2 looking down
each level of time requires an outside observer
characteristic of the quantum world - actions appear random, however there is a statistical average among them (grants us predictive power)
dreams tell jokes -- this is true I’ve noticed interesting wordplay and original songs and poems in my dreams as well
“if I am not awake in the dream state I am emmersed in the illusion”
the waking life is similarly an illusion -- the dream has a cleavage there
Dreaming Ahead of Time : Gary Lachman
https://garylachman.co.uk/
1 note
·
View note
Text
Responding to a video about transgender science…
WARNING: This guy does not like intersectional feminism/non binary identities. He’s not hateful, per say, but he definitely can be abrasive:
Link to video: https://www.youtube.com/watch?v=os7bOBlre5E
My comment:
“A couple of notes from a cis female who is part of/spends a fair amount of time with the lgbt/feminist ideologue group:
1. Intersectionality was not intended to be a "privilege hierarchy." It was proposed at first by black feminists to explain how their experiences as black women in a post-women's lib world were unique and that a woman could face systemic oppression for things outside of her sex. I personally can say that everyone has unique experiences in life based on our racial, gender, and sexual identities; you will be treated very differently as a bisexual man than you would a bisexual woman (like me). Intersectionality is invaluable for introspection about the identities you choose vs. the ones society puts upon you. Unfortunately, yes, intersectionality sometimes gets used to "explain" how white, straight, cis, males are at the top of the pyramid by tactless feminists, and it is certainly not scientific. How can you explain social identities using the scientific method?
2. I know a nonbinary person, who came out while I was going to school with her (I'm honestly not sure what pronouns to use but this person appears quite feminine and doesn't get defensive about me using them). While I know that anecdotal evidence don't mean sh*t, hear/read it out: Once she hit puberty she became irrationally frightened of her own reproductive organs. She would have nightmares about becoming pregnant and in general didn't enjoy being biologically female. That being said, she didn't identify as a man and liked looking conventionally feminine. To me, this sounds like gender dysphoria that didn't need to be treated with hormones and led to a different "third" gender identity at the mental level. I, too, don't agree with the 56 gender article (which is disputed among many feminist circles, by the by), but I think there's something to non-binary/third gender. If we're using brains and hormones as explanation for gender identity, does it not make sense that some people would be right in the middle if their white vs. gray matter was unusual for EITHER sex?
3. Whether or not you think an environment is healthy, the world we live in can change us chemically. What about epigenetics? I think it's possible that in contemporary society, where there is less pressure to reproduce thanks to modern medicine and access to more human beings in a global society, that we are responding to these factors on a physical level. Humans fundamentally changed our evolution and the evolution of other organisms when we began cultivating animals and plants for food/other uses. We changed it again when we began traveling the world en mass and different populations interbred (and shared diseases). And once more with modern medicine. We can't go back to the paleolithic age, and all of these changes were in the last several thousand years.
- I am not a scientist. I am not saying that sexual/gender evolution is fact. I am saying that the human species has defied natural selection multiple times and that pushing gender identity away because "it's not scientific" gets dangerously close to the naturalistic fallacy.“
#youtube shenanigans#intersectional feminism#trans science#gender dysphoria#non binary#debate#looking for opinions
2 notes
·
View notes
Text
the baker’s granddaughter
once upon the time she was
living like he might have wished she would,
like he might have wished he could,
with so much freedom she didn’t know what to do with it
there are not enough candles
and he had just enough to wish for life itself
and so he lives just enough to start new lives,
to cook, to bake, to situate into a sense of assembled freedoms
before the fade
and now he is only other people’s memories, was only ever a story to her
though she carries that story into a city,
as strong as any fairytale or firsthand experience,
where certain cafes serve her pierogi
any day she asks with shock and disbelief in her voice
thinking the menu must be a misprint
flooring, festival food, former once a year treasures
any, every day whim wished food
in this excess of options, held here simply for the asking
an unreal bounty, served cold and sweet, options she had never even seen
he had not lived to make her pierogi
and before this city it was made only one weekend a year
in the sweetest of scarcity,
at her grandmother’s skilled hands, in her overly small kitchen
and sometimes she watched, only allowed the task of sealing the edges up
fingers and forks pressed, too young to learn too much about the contents
only keep them in, hold them safe, later there will be time to make
and she listened, trying to create recipes out of her grandmother’s movements
trying to find their past in her methodical making
wondering if blood and epigenetics would someday be enough to lead her back
if it could become some kind of tracing dots, of mapping line
a guide to fill the baker’s missing place
trying to gift her father a taste of holiday of history of what he had always had,
even when no one else was there to make tradition out of will and want
and the baker would not have found his granddaughter’s attempt at authenticity good
but she likes to think of him smiling at the try
and correcting and teaching with patience and pride
you have to understand that in this the dough is key
and that is a baker’s floured, sacred territory
and so she flours her counter, her hands, her heart
and thinks, trusts, believes that those years of eating will lead her
to a trial and error tested true pierogi
her comfort food, bruised by loss, brought back
and now with her grandmother gone,
she wishes all the more that he had left a bakery book,
some scraps of spell-like recipes
though she has only seen a few scarce samples of his handwriting
forced signatures, sealing the befores of his freedom into the concentrations camps
and she wonders if his cooking was changed,
if his baking was made better in the years after
with defiance and resilience and survival added extra
names over numbers,
he named two children,
the baker's granddaughter goes on carrying his name
even though she never got to call him dziadziu,
he called himself Jan Bak (the name sounds clumsy in her mouth, she has not said it much)
and the bakery Just Rite
and so be it, by his work, she is here to still try
by, earthboundpixie
1 note
·
View note
Text
Deepak Chopra to study the science of yoga
Mind-body wellness and also integrative medicine pioneer Deepak Chopra, M.D., revealed yesterday that the Mind Body Medical Team situated at the Chopra Center for Well-being is dealing with scientists from the College of The golden state, San Diego, as well as other distinguished scientific establishments to study the wellness advantages of an integrative method to healthcare.
This strategy combines the most recent explorations in clinical scientific research with complementary methods rooted in knowledge traditions, consisting of reflection as well as mindfulness, yoga, Ayurvedic massage therapy, and also other mind-body devices that enable people to affect their autonomic as well as endocrine heating system in order to promote self-repair, self-regulation, as well as homeostasis.
" We're staying in an exciting time of change in the field of medicine. Where scientists when believed that our genetics dictated our wellness and also destiny, brand-new research now reveals that we are not destined get the same diseases as our parents and grandparents.
The arising science of epigenetics has actually shown that via our everyday lifestyle options, we can influence the task of our genetics, 'downregulating' the genetics causing inflammation linked with numerous persistent illnesses, while 'upregulating' the genetics that influence homeostasis and self-regulation.
In short, we have an unbelievable power to stop and even reverse disease through the way of living we develop," said Deepak Chopra.
" For several years, people from throughout the globe have actually pertained to the Chopra Facility to attend our Perfect Health program as well as experience our integrative strategy to overall wellbeing. Currently we are likewise releasing brand-new research studies of the Perfect Health program, considering cell markers of aging, including the enzyme telomerase and also its influence on the length of telomeres.
Similar researches by Dean Ornish, M.D. and also others have shown enhancement in the telomeres and also other cell markers will maximize healthy and balanced aging and also wellness as it happens with way of living changes.
The Chopra Center's own researches are being carried out under the guidance of Paul Mills, PhD, a teacher in the behavioral medicine program at UCSD, as well as Director of Collaborative Research Program Advancement at the UCSD Center of Integrative Medication. The study concentrates on determining the effects of reflection on cell biology. We are considering the Perfect Health program and its results on cellular biology, consisting of genetics expression and proteomics.
In collaboration with a number of medical colleges, the micro biometric outcomes of this study will quickly be released. Heart wellness and brainwave task are also being kept an eye on uniquely on people practicing Primaeval Audio Reflection, as taught at the Chopra Facility, via the newest electronic modern technology," Deepak Chopra said.
( Go here to watch Deepak Chopra discuss the connection in between integrative medicine as well as his own medical specialized of endocrinology and also metabolic rate.)
The integrative medical professionals at the Mind Body Medical Group situated at the Chopra Facility are board-certified medical professionals in addition to specialists in Ayurveda and many others standard healing heating systems. They provide specific mind-body medical examinations along with team programs such as the Chopra Center's Perfect Wellness program.
Developed by Chopra Center founders, Deepak Chopra, M.D. and David Simon, M.D., Perfect Health and wellness is a 6- or 10-day recovery immersion where visitors experience day-to-day tailored Ayurvedic massage therapy therapies, a mind-body clinical assessment, and also a moderate detox that assists to transform the body's microbiome with using plant-based fiber, herbs, and also vegetable oils (visit this site to watch a video of Deepak Chopra speaking with Dr. Larry Smarr about the Mind Genome Microbiome).
Perfect Health also consists of everyday sessions led by the Facility's master teachers in Primaeval Audio Meditation, yoga exercise, tension management, dietary support, and also the recovery wisdom personified in the customs of Ayurveda.
The Mind Body Medical Team and the Chopra Facility likewise offer Trip into Healing, an accredited training course in integrative medicine that offers AMA-approved CME credit histories to doctors as well as medical experts in partnership with the UCSD School of Medicine. This experiential workshop is for healthcare specialists who wish to broaden their knowledge of mind-body medicine and patient care.
2 notes
·
View notes
Video
youtube
✎ Grab a snack and chew on today's lessons from a man who went from studying biochemistry and neurology to becoming a best-selling author, expert in neuroscience, epigenetics, and quantum physics, and one of the most sought-after speakers in the world! He's Joe Dispenza and here's my take on his Top 10 Rules for Success! ★★★ SECRET BONUS VIDEO ★★★ Get a FREE video every morning to help you build your confidence for the next 254 days from mentors like Tony Robbins, Oprah, and Muhammad Ali. Find out here: https://ift.tt/2kGr5Jv ❤ HELP TRANSLATE THIS VIDEO ❤ If you loved this video, help people in other countries enjoy it too by making captions for it. Spread the love and impact. https://www.youtube.com/timedtext_video?v=GBF_BZH4KN4 ★ MORE RECOMMENDED VIDEOS FOR YOU ★ If you enjoyed this video, you may enjoy these other videos from Evan Carmichael: • "WHEN Other People BREAK, I Don't!" - Tom Bilyeu - https://youtu.be/E6hbK-7BjWM • How to NEVER Get Sick Again - The WIM HOF "Iceman" Method - #NeverSick - https://youtu.be/mxCGDFlH1_k • "You've Got to #BELIEVE in YOURSELF!" - Lewis Howes - https://youtu.be/B1VCa20Yrgw -= DISPENZA'S RULES =- 1. Be a creator of your world 2. Invest in yourself 3. Be comfortable in the unknown 4. Improve your lifestyle 5. Let go of your past self 6. Become supernatural 7. Don't make excuses 8. Become truly present 9. Keep going 10. Think greater than your environment -= BONUS =- * Find your passion ✎ He studied biochemistry at Rutgers University. He holds a Bachelor of Science degree with an emphasis in neuroscience. He has received postgraduate education in neurology, neuroscience, cellular biology, memory formation, and aging and longevity. He has lectured on six continents and 32 different countries. He's the best-selling author of Evolve Your Brain: The Science of Changing Your Mind. His latest book, You Are the Placebo: Making Your Mind Matter (2014), is an Amazon Bestseller. He's driven by the conviction that each of us has the potential for greatness and unlimited abilities. ✔ SOURCES ✔ https://youtu.be/La9oLLoI5Rc Tom Bilyeu https://youtu.be/P_FIYwg2oU4 Consciousness & Human Evolution https://youtu.be/C_vmAzWklnA Reprogramming Mind https://youtu.be/Pw9UdvMxoTs Dr. Joe Dispenza Videos https://youtu.be/0AsGxWFD7pk drjoedispenza https://youtu.be/tzWmMJq6vJc Reprogramming Mind ♛ BUY MY BOOKS, CHANGE YOUR LIFE ♛ Some used the ideas in these books to build multi-billion-dollar businesses. I'll give you the simple-yet-powerful formula that they used (and you can) to realize your dreams. Get yours. https://ift.tt/2auuYKa https://ift.tt/2DWNJZU ✉ JOIN MY #BELIEVE NEWSLETTER ✉ This is the best way to have entrepreneur gold delivered to your inbox, and to be inspired, encouraged and supported in your business. Join #BelieveNation and feel the love. https://ift.tt/1DyhRRs ⚑ SUBSCRIBE TO MY CHANNEL ⚑ If you want to do great things you need to have a great environment. Create one by subbing and watching daily. http://www.youtube.com/subscription_center?add_user=Modelingthemasters ¿ COMMON QUESTIONS ¿ • What is #BTA?: https://www.youtube.com/watch?v=BsY8bmTUVP8 • How do I get one of Evan's t-shirts?: https://ift.tt/1VBOMjE • Why does Evan look like Nicolas Cage?: https://www.youtube.com/watch?v=gZHRniTcRwo • Why does Evan make so many videos? https://www.youtube.com/watch?v=NEKxGA8xr1k • How do I vote for the next Top 10 video Evan should make? https://www.youtube.com/watch?v=0arZb0xLIDM ツ CONNECT WITH ME ツ Leave a comment on this video and it'll get a response. Or you can connect with me on different social platforms too: • Instagram: https://ift.tt/2oPc4Xb • Twitter: https://twitter.com/evancarmichael • Facebook: https://ift.tt/1t8ruBM • Website: https://ift.tt/LfsMJ5 ----------------------------------------------------------------------------- Thank you for watching - I really appreciate it :) Cheers, Evan #Believe
1 note
·
View note
Text
Sedimentary City 11: THUS SPAKE
The pain amplifier works via the theory of cortical manipulation. The human mind was well understood to be virtual, a low resolution projection of sensory data, filtered and enriched by structures carved out by the various vehicles of the past: genetics, epigenetics, collective and private memories.
Most regarded this place as sanctified and hermetic within the alcove of the skull, accessible only to the owners. However, the state was clever enough to secretly embed a backdoor into every mind-machine interface. They used this portal to enter the inner garden of the mind, committing atrocities within the lone glade people had known to be theirs and theirs alone.
Then suddenly one became two and a small voice whispered somewhere to the left of him, “You’d better just tell them. You can’t take too much more of this can you?”
What?
“I said, perhaps you had better tell them?”
What is this voice? Who are you?
“Don’t tell me that you don’t recognize me?” asked the strange voice, “Well, not that it matters, I am one who is concerned about your well-being -- maybe the only one here who is -- and right now you are not looking so great, strapped into this chair. You were destined for better than this.”
The words came out slow and languid, strangely accented and stilted as if the syllables were culled out at random from the ether, diffused and barely coherent yet perfectly understood by Jan. What the fuck is this? Jan thought. It seemed likely that this was a trick of the interrogators, a voice implanted into his head introduced via the puncture in his consciousness matrix.
“Don’t be silly, Jan. I am not them! You think they would be this clever? You know their methods, it’s always a big dumb production, phantoms and fireworks, no finesse.”
Jan vainly blinked his eyes in the darkness seeing nothing. The stranger’s voice remained.
“They can control everything you experience, but they can’t control your inner thoughts, auto-generated and consumed independent of sensory input. You’ve done the research on this. It is just like in dreams where you are at once the creator and the consumer, one and the same yet somehow this fact slips awareness.”
Fine but this doesn’t make any sense. Am I having a schizophrenic episode?
“Jan, I am no one, but I am also you. Also, under the correct circumstances, schizophrenia is adaptive.”
No you are not me, thought Jan, I am the only me.
“Maybe. But you’ve always suspected, haven’t you? You’ve always wondered if there was someone else, felt my presence -- someone by your side in all those still hours. I’ve been with you this whole time, watched you grow up, grew up with you. Lonely nights of reading and introspection, building castles in the sky. The first time you saw Eva, and the last: when you watched her bleed out onto the streets, I was there as well. I was with you as you cowered behind the wall crying your soul out. I’m sorry I couldn’t do more. I miss Eva as well.”
I’m losing my fucking mind.
“Yes, you are. But you think I wanted to appear? And learn your stupid language? The bondage of linguistics is not anything I welcome, but these are extraordinary times and you are in terrible danger. We won’t live for much longer at this rate. What are you even hiding from them that they don’t already know?”
Jan looked around the black room trying to penetrate the occluded space, but he saw nothing, no light to avail him from his solitude. He felt scared in a way he had not ever felt before, the sort of existential fear experienced by something very small and tenuous and close to vanishing. The void seemed no longer a distant philosophical mirage but so proximal that he could feel it as a lacunae of presence or heat.
“So what is this? You think Eva wants you to keep suffering? She’s gone. She was always smarter than you in that regard, at least she was practical. She wanted something, she wanted to grow to live and progress, become someone. Really you should have been the one to die instead.”
Yes, I should have.
“Ok, sorry I brought that up. I know how ready you are to die, very noble of you. I’m trying to remember now, if we’ve just read too many books where the hero falls on his sword. Sounds just like something Dad would have made us read.”
Jan thought of the syllabuses that his father had sent him in lieu of being present, tomes of concepts and abstractions. Each year for his birthday, a stack of books and assignments, eons of wisdom, analyzed and meta-analyzed, re-interpreted and allowed to hermeneutically ferment in the collected records of academia. But in the end, even the most well intentioned knowledge finds itself complicit and weaved into the inherent death drive that exists in every living thing -- a civilization being at once an amalgamation of lives as well as an organism itself. Logic, thought, insight: thin and veliform coherences, just enough for people to keep rolling each day into the next and so forth, unacknowledged that the moment a thing is born is also when it yearns for quietus as well.
“‘Father’, ha!,” the voice chortled in a phlegmatic hiccup, “You always were a prim little prick. You still don’t recognize me? Ok, here is my covenant. You had a little brother, remember?”
Ice sheets rolled through Jan’s core, a frigid and unplumbable emotion akin to dread move through with serpentine undulation.
I don’t have a brother, what are you talking about? What brother?
“Yes you do. Remember her funeral, what they said? You can’t lie to yourself. Well, maybe you can, since you’ve been doing it your whole life -- but eventually you will have to exhume all the things you’ve buried. You’re no different than any of them in that way, really.”
Presently, they were interrupted by the strident voice of the bodiless interrogator, a voice much louder than the ghostly and immaterial whispers of the stranger: “Jan Kavfryd, are you ready to confess? It is in your interest to do so, the earlier the better. We always get what we want and the result is always the same, so spare yourself.”
“Yes,” the stranger hissed as if in reply, “tell them already! It is not your destiny to die here, Jan. I’m not ready to die! It is your destiny to live, to continue living until you are an old man, useless and unneeded but at the very least breathing, thinking, feeling. What else is there to being?”
“No,” Jan fed that single word into the mind-machine interface.
“Very well,” replied the incorporeal interrogator, “stand by for more. You are more stubborn than we had calculated but we are prepared for all outcomes.”
“Jan, the important thing is to survive, even if that means suffering more. It’s not your destiny for you to end here.” The stranger seemed distant now, as if fading into the background hum of thoughts. A squeeze of coldness streamed through his arms; the interrogators had delivered more drugs as preamble to the next stage of hell.
Convulsive sobs rolled over Jan one after another like oceanic waves. Tears streamed from his eyes and his mouth shivered and worked around the mouth piece, much like the quavering mastication of the elderly and close to passing. His chest heaved and spasmed with grief. Out of nowhere he thought of his mother who had died when he was still very young. He had no memory of her except a diffuse impression, an occasional smell that he recognized with exquisite nostalgia. He suddenly wanted to be with her very badly.
“Life will seem a sad and pointless enterprise to you,” the inner voice said softly, in a lugubrious rustle, “for that is your lot, the forlorn star under which you were born. You will be despondent and harried by grief, but you will also live to grow old until the full plenitude of life for you has been experienced.”
Jan sensed a deep truth in these words, as true as anything that could exist, bereft of common artifice or illusion. But he found it hard to believe.
The limpid voice continued but quieter and quieter, “Your existence will be redeemed because everyone of us has a secret purpose, a fatal consummation -- for the whole arc of your life is already recorded and held in crystalline stasis.”
The voice became nothing as Jan accelerated towards a new vision, a pinprick which rapidly expanded to cover over him like a blanket.
0 notes
Text
331: Rethinking Health: 8 Predictive Biomarkers for Lifetime Health With Russell Jaffe
New Post has been published on http://healingawerness.com/news/331-rethinking-health-8-predictive-biomarkers-for-lifetime-health-with-russell-jaffe/
331: Rethinking Health: 8 Predictive Biomarkers for Lifetime Health With Russell Jaffe

Child: Welcome to my Mommy’s podcast.
This podcast is sponsored by Jigsaw Health, my source for magnesium. You probably know, if you’ve read my blog, that magnesium is responsible for over 300 biochemical reactions in the body. It impacts blood pressure, metabolism, immune function, and many other aspects of health, including hormones. It’s known as the master mineral and it’s one of the few supplements I take regularly. And I have found a specific way to take it that works best for me in very specific forms because if magnesium is taken in the wrong way it can lead to digestive upset or if it’s taken too quickly it can cause all kinds of problems. So, I take two supplements. One called MagSRT which is a slow release form of the dimagnesium malate. The slow release technology makes it easier on the digestive system. So I don’t get any of the digestive disturbance that comes with some forms of magnesium. I take this form in the morning and at lunch. So, two capsules with breakfast, two capsules with lunch. And at night, I take a different product MagSoothe, which is magnesium glycinate which is magnesium bound with the amino acid glycine to help sleep. And in combination, I noticed the biggest effect from those two particular products. You can check them both out and save by going to jigsawhealth.com/wellnessmama. And the code wellness10 will give you $10 off any order.
This podcast is brought to you by Pique Tea. I love all of their Triple Screen teas that can be consumed hot or cold. You might know that tea has been used for centuries for a variety of reasons in almost every culture around the world to naturally boost energy levels, to increase mental performance, for immune and gut health support, or longevity or just to achieve a youthful glow. It’s truly been a part of almost every culture. It’s noncaloric so I drink tea of some kind, either herbal tea or caffeinated tea almost every day even when I’m intermittent fasting and even during my fasting window. So, unless I’m on a full water fast, I will drink noncaloric tea while I’m still fasting. Pique Teas in particular are made from organic, high-quality tea leaves and ingredients sourced from around the world very carefully. They are the purest teas that I have found because they do something called Triple Toxin Screen for heavy metals, pesticides, and toxic mold so that you know you are getting the best, highest quality tea without the junk. Not to mention, their teas taste amazing and my kids love them too.
For all you moms listening, these teas are great for gut health. They use a cold-brew crystallization process, so you get more concentrated antioxidants and polyphenols, up to 12 times as many actually with each serving. These are the compounds that are known to be responsible for a lot of those benefits that I listed, and so, that increase is a really big deal. And given that these come in little tea crystals, I can easily add them to my smoothies or to hot or cold water. They dissolve in seconds. And I always carry a few of them in my purse when I travel. They have a range of caffeinated and noncaffeinated options. I love their Organic Jasmine in the morning for energy and for mental clarity while I’m podcasting and I love their Herbal Mint when I need to wind down and relax. Pique is also the first company in history to win three gold medals at the Global Tea championships. You can save 10% off Pique Teas by going to piquetea.com and using the code WELLNESSMAMA. Note that this does exclude their Fermented Pu’er teas, but it is valid on everything else.
Katie: Hello, and welcome to the Wellness Mama Podcast. I’m Katie from wellnessmama.com, and this episode is packed with practical tips that you can use based on eight predictive biomarkers that are good reflectors of lifetime health. I am here with Doctor Russell Jaffe who is an MD and a Ph.D. He is the founder and chairman of PERQUE Integrative Health which is a company that offers scientifically proven integrative health solutions. He has more than 40 years of experience in these areas of research, contributing to molecular biology and clinical diagnostic research. His focus is now on functional predictive tests and procedures designed to improve both the precision of diagnosis and treatment outcomes and for predictive longterm health. He’s authored nearly a hundred articles, and like I said, he is both an MD and a Ph.D. He is board certified in clinical pathology and chemical pathology. And has been the recipient of many awards in these areas, and he’s gonna tell his story better than I could, today. But how he went from a full conventional medicine background at the National Institute for Health, to now a very integrative approach to medicine. I know that you’re really gonna enjoy this extremely practical episode, so let’s jump right in.
Katie: Dr. Jaffe, welcome. Thank you for being here.
Dr. Jaffe: Thanks for the invitation.
Katie: Well, I’m excited for our conversation today. And I know we have a lot to talk about. But to start, you have such an interesting background. And I think that’s a perfect place to start. I think our listeners would love to hear a little bit more about you, and specifically, how you made a pretty radical jump from conventional medicine at NIH to where you are today. So can you walk us through briefly what changed in your thinking and how that reflected and how you practice medicine?
Dr. Jaffe: Well, thanks for that question. Because yes, I was a skeptic and I now advocate for what I think is a safer, better, more natural, more predictive, more personalized, more proactive, more prevention-oriented approach. And because as I think others have said better, we are spending more and feeling worse and we call that health care. So I did internal medicine and biochemistry and molecular biology in Boston, I came to the Clinical Center at NIH, enthusiastic as most of us were in the meritocracy of that time. And I fairly quickly realized that we were dealing with people who had fallen into the river of disease and we were hopefully reducing the drowning rate in that river of disease, but we weren’t preventing people from falling in.
So I went out to debunk the people who said they had traditional and/or evidence-based approaches to health promotion to real primary proactive prevention to personalized medicine. And fortunately, I picked some really good people to go and debunk because they showed me how ignorant I was, Queen Lu, I went to debunk traditional Chinese medicine and acupuncture and I ended up doing a seven-year apprenticeship with him in Washington. DC. Ramamurti Mishra wrote the textbook of yoga psychology and commentary and Patanjali sutras and an MD PhD, rather broadly trained, I went to debunk him and became his student. And then I heard about a Cambodian Buddhist monk who had decoded a color healing system and non-invasive color healing system that had been given 2500 years ago, practiced for 5 centuries, lost for 20 centuries, 2000 years, and he had figured it out. And from the age of 80, when I met him until 110 when he passed, we were mostly together and yes, those are the kinds of people where, if you can watch them put their sandals or their shoes on and off, it’s a transformative experience, or how they fill the teacup or drink the tea.
So yes, I believe that I was trained in the scientific method, which means to be able to look across cultures and across time and across philosophies, but with a common guide, which is let the evidence…now some of it is observational and anecdotal and some of it is organized in a double-blind and some of it is triple-blind, which we can talk about if you want. So yes, I came as a skeptic. I now am very confident that we spend an extra $1 trillion each year out of the 3 trillion we spend on health care to bury a million people early with high suffering and very little value. And I believe we should do better than that. We deserve to do better than that. If we have the right to pursue happiness, which goes back to our nation’s founding, then I believe health care has to become, at some point, a right of citizenship, not a privilege of economics.
Katie: I agree with you. And I love that you were willing to question your assumptions. I think that’s something that we can all benefit from doing, in anything that we consider a firmly held belief or assumption, because truly, if we’re correct, we only then strengthen our belief and if not, that’s something we need to evaluate anyway, so I have so much respect that you did that process, even with your work and was something that was so vital to your career. I really have a lot of respect when people are able to do that. And I think that now you have such a wonderful perspective coming from both of those areas, to be able to offer people such unique advice and I’m so excited to get to go deeper on this with you. I know that you talked about how now with this new understanding and seeing kind of the whole picture that our health is very much largely determined by factors like diet and lifestyle, and you use the term epigenetics. So can you explain to us what that is and just how dramatically those factors can influence our life and our health?
Dr. Jaffe: Thank you, I can very easily explain what it’s not and then I will explain what it is. So what it’s not is your DNA that you inherit from your mom and dad, half from each, that’s your genome, that’s your DNA. But then the DNA has to get translated through something called RNA and then has to become something called a product or the protein or the glycoprotein or lipoprotein. And it’s there that life really gets more interesting. And epigenetics is the 92% of your lifetime health quality, your lifetime quality of life. That is determined by your habits of daily living, determined by what you eat and drink, think and do, the ways in which you choose to live your life. We call these the habits of daily living, sometimes HODL because we like to compress a few words into an acronym that’s a little hard to understand.
So, epigenetics turns out to be very important. It was validated in the early ’70s when Don Frederickson was running the National Institutes of Health, a consensus conference, 92% is choice and lifestyle 8% is DNA and determined, reconfirmed several times over the decades. So epigenetics is where the opportunity lies and yet, epigenetics and lifestyle is not what we have at the core of the medical education curriculum for physicians and nurses or chiropractors and naturopaths. It’s mostly about making the right diagnosis, and then a treatment to reduce the suffering or treat the symptoms. And what I’m saying is really quite different, epigenetics is the chance to change your habits and therefore change your future.
The past is behind us. I think we can agree that the past is behind us. The future has not come. I think we can agree the future has not come. So what are we going to do today so that our habits of daily living choose life and health? That means foods we can digest, assimilate, and eliminate without any burden, that means be well hydrated with water and herbal beverages are your beverages of choice. It means spending a few minutes each day to cultivate gratitude and to cultivate appreciation for your portion, rejoicing in your portion to use a metaphor.
And you do have to move around. So sitting is the new smoking and sugar is the new tobacco. So get up and give up the candy bars and the processed foods and the hidden sugar sources and eat whole foods that you can digest, assimilate, and eliminate without immune burden, and feel and function years to decades younger. You can, by changing your habits and thoughts and activities, feel and function decades younger. And I’m an example, just a personal example of someone who made that transition.
Katie: I love it. And I know when we were preparing for this interview you wanted to talk today about some specifics with biomarkers when it comes to this and particularly ways that we can kind of rethink our health. And then what we can learn from these biomarkers for a lifetime of health and not just lifespan but healthspan. So to start, what do you mean when you say rethink health? I know you’ve touched on that a little bit, but what does that concept mean to you?
Dr. Jaffe: Yes, when I say rethink health, I mean, making choices that are about primary, personalized, proactive and predictive prevention practice protocols. And if I say that again in a slightly different way, it means to look at the causes, not the consequences. It means to look at are you getting enough of the essential good stuff and are you able to reduce the anti-nutrient toxic bad stuff? And yes, in almost all cases, you can and we have documented in outcome studies in type 2 diabetes, type 1 diabetes, fibromyalgia, muscle pain and other similar conditions that you can, starting from best standard of conventional care today in just six months of best efforts, feel and function much better. And you can document that with a few self-assessments like the digestive trends of time. Your urine, acid-alkaline pH after rest. How much of nature’s ascorbate does it take to cleanse the anti-nutrients out of your body at that moment? Are you well hydrated? These are four self-assessments that are very inexpensive, easy to do and come with an interpretation to help you understand what it means so that you can choose more wisely tomorrow than you did yesterday.
Katie: Got it. That makes sense. Okay, so then I can’t wait to go deep on these because I’m a big fan of data and being able to track things and measure them and see what’s working and what’s not. So what are the predictive biomarkers?
Dr. Jaffe: Okay, so what are the predictive biomarkers? There are eight of them. First is hemoglobin A1C. Second is high sensitivity C reactive protein known as hsCRP. The third is homocysteine. The fourth is LRA cell cultures, that’s an immune tolerance test. The fifth is that urine pH after rest, that’s a measure of how much cellular magnesium you need or have. Then your vitamin D level which turns out to be a neural hormone, then your omega-3 index the balance of essential fats, omega-3 to omega-6 we need both but most of us get too much omega-6 and it’s often damaged. We need more omega-3 from whole seeds and nuts and foods.
And then the last, and it’s an unusual one, it’s an urine test an easy test to do but not a commonly done test yet. That’s 8-oxoguanine. Now 8-oxoguanine is the measure of how much oxidative damage is being done in your nucleus to your DNA. That’s a very important risk factor or marker. And that’s why when we started with 100,000 lab tests, just to find out how many tests we needed to cover all of lifestyle and epigenetics. This is part of our Health and Rethink Health Working Group. We came down to eight tests that can be done for less than $1,000 with interpretation. And you can add life to years and years to life based on those best outcome goal values, not the statistical lab ranges. So we don’t care what the lab ranges, we care what the best outcome value is for each of those eight biomarkers. And we want to know whether you are there. If you are, celebrate that you’re at your best outcome goal value. And if you’re not, here are the habits of daily living that will bring you there in about six months.
Katie: Awesome. Okay, so let’s go through each of these and kind of give people a broad picture of what they should expect and what good looks like and then also, if one of these, for instance, were to come back out of range, what they would need to know so they don’t freak out. So you started with hemoglobin A1C. Walk me through what that specifically is a measure of and what we want to see when it comes up hemoglobin A1C.
Dr. Jaffe: Yes, in the late 1960s, we discovered that if you have extra sugar inside yourself, it can harm the cell and the body is smart enough to stick that onto protein. And Paul Gallup, mentor of my mentor, actually developed the hemoglobin A1C, he published it in about 1967. So it’s been around a long time. And it gives you an average measure of extra sugars stuck on your protein over time, typically a three months timeframe, maybe that or a little bit more. And we know that people who are healthiest and live longest and feel and function best and have a new neurohormonal digestive system that works best. They have hemoglobin A1Cs of less than 5%.
And now you ask the right question, which is let’s say your hemoglobin A1C is above 5%, how do you get it to 5% or less and you do it the way I did, which is knowing that you’re sweet enough as you are, no added sugar in your diet. Notice I said no added sugar. The average American today takes in one week, in one week, the amount of sugar that our great grandparents took in the year. It’s hard to avoid added sugar, it’s really hard. It’s stuck into a whole bunch of things along with fat and salt that addict your tongue and your brain to what’s called the crave factor. We’ll talk about that some other time. But you want wholeness, you want nature, nurture and wholeness. You want food you can digest, assimilate, and eliminate without any burden to bring your hemoglobin A1C to less than 5%.
And I’m glad to tell you that when I weighed 65 pounds more, I was pre-diabetic by that measure. And now, since I’ve lost that weight and it’s been off now for years, I’m not going to find it again. My hemoglobin A1C for the last several years has been below 5% and that says that I am likely to live long and well within immune neurohormonal and digestive and nervous systems that work for the entire lifespan.
So hemoglobin A1C is important, there are nuances. We have written up review articles and published chapters in books about this for people want more information, but your hemoglobin A1C should be less than 5%. And we know how to get you there by reducing your intake of simple, which means empty calories sugar that is hidden in many processed, packaged and crisp foods. So when I was taught by Beatrice from Hunter was shopping around the edge of the store, that’s where the real food is and be careful about going down the aisles because that’s where the packages and the cans are.
Katie: Got it. And as another marker, I know that the hemoglobin A1C is one that you do have to go into a lab to get tested and I think it’s more accurate like you said because It’s kind of that average over time. I also am a big fan of using a glucose monitor at home and just relatively often taking my fasting glucose, which is not, that’s just a snapshot but it is a predictor as well, and it’s something that we can do at home. I’m curious if you know of any confounding factors when it comes to fasting glucose and hemoglobin A1C because I’ve heard from and seen labs for several patients who despite eating a very low carb diet and no processed sugar whatsoever, we’ll still see those numbers elevated. Are there other things that can come into play in those kinds of, like outlier scenarios?
Dr. Jaffe: Well, yes, thank you. Outlier scenario is the right kind of terminology. Let me start with the conclusion and back into why. Fructosamine, like fructose amine. Fructosamine is a measure of extra sugars stuck on to a protein and that changes quickly like, within a month or so, rather than waiting longer. And what are the complications about hemoglobin A1C? Well, it’s based on how long your red cells live, and your red cells and a healthy person live three or four months. But sometimes red cells don’t live three to four months. And then you can have, a few people have published articles about confounding variables that influence hemoglobin A1C. So when we became aware of that, we went out and looked at what is the test that you can do even if the red cells are more fragile or are being taxed one way or another by immune complexes or whatever? And the answer is fructosamine.
So yes, there are just exactly what you said, outliers. And where we try to do our best is to help both consumers and clinicians understand why the outliers exist and what to do about them so you can get an accurate measure and not be confused. Now, with respect, you can do a hemoglobin A1C on a little lancet drop of blood put onto a little piece of filter paper and sent to a lab. So you don’t have to have a phlebotomy to get an accurate hemoglobin A1C.
And the other side, most of us are familiar with white coat hypertension, you know, like, just drawing blood or going in to see someone who has a white coat on and a stethoscope around their neck and the smell of a clinic and so forth. For many people, it triggers a change in their blood sugar. So since we measure blood sugar and insulin and hemoglobin A1C, in our outcome studies I can tell you the hemoglobin A1C is a good measure for most people and fructosamine fills in when hemoglobin A1C is inadequate. And yes, you should be less than 5% on the corrected hemoglobin A1C or on the fructosamine, which means you’re at the lower end of the lab range.
Katie: Got it. Okay, that’s really helpful and it makes sense. And that one seems like a relatively straightforward and definitely, anything with glucose is definitely tied to the dietary factors as well. Are there any supplements that you recommend or that kind of go hand in hand with healthy levels?
Dr. Jaffe: No, no, again, a very good point in regard to nutrients or essential cofactors that your body cannot make that improve sugar regulation. It turns out there are a number of herbs and several minerals. The minerals are chromium. And you can have the chromium in the picolinate form of the citrate form. And then vanadium and vanadium ascorbate especially. But it turns out that chromium and vanadium separately help the body regulate blood sugar uptake and metabolism end to end.
And then it turns out there are four herbs. I’m not sure how much time we have to go into them. But some of these go back to the Old Testament, like Mara, or bitter melon. Some of these are contemporary, like, you can get them in a Chinese restaurant and most traditional parts of at least America if not the Pacific Rim. And so there are herbs and minerals that can be combined into mycelized soft gels and taken as part of glucose regulation. And we’ve helped pioneer some of these safer, more effective all-natural approaches.
Katie: Perfect. And then moving on, I’d love to talk also about C-reactive protein and you mentioned a specific marker to test for with C-reactive protein. For anyone who’s not familiar, can you explain what C-reactive protein is, what a healthy range looks like and then what we need to know if ours shows up out of range?
Dr. Jaffe: Yes, thank you. So, C-reactive protein is an inducible protein, it goes up when your body is not able to repair when your body is crying out because of the repair deficit, often misunderstood as inflammation. When your body has a repair deficit and C-reactive protein goes up. And Paul Ridker and Nadir Refai and other colleagues have shown that at the low end, you get a lot of useful information. So there’s a hsCRP or high sensitivity CRP, where the lower end of the range is more accurately analyzed by the lab and the healthy value for hsCRP is less than 0.5, people who have inflammatory chronic repair deficit or autoimmune conditions have elevated hsCRPs and we want them to get back to their best outcome ability to repair a non-deficient condition where the hsCRP is less than 0.5.
Katie: Got it. Okay, perfect. So if that does come out of range, what are some of the strategies that you would recommend to help the body get it back into normal range?
Dr. Jaffe: Well, to enhance repair you need the maternal antioxidant known as ascorbate, but you need the L-ascorbate, nature’s form, not the synthetic form the work-alike that doesn’t work. So you need fully-buffered, fully-reduced L-ascorbate based on the polyphenolics as Alberts and Georgie pointed out in the 1930s as a synergistic, or a multiplicative benefit, when you have the correct flavonoids and flavanols, quercetin dihydrate, insoluble OPC to work along with the L-ascorbate that’s fully buffered and fully reduced because it’s been produced under a nitrogen blanket in the old traditional way.
Then, in addition, you need magnesium. And today you need to enhance the uptake of magnesium with chromium-citrate so that you can activate ATP, the energy currency of the human body, you can protect the mitochondria with both magnesium and ascorbate, you can keep the what’s called proton gradient so that the cell functions efficiently and effectively. Too many of us are in chronic acidosis due to lack of magnesium in ourselves. We are in chronic oxidative stress because of antioxidant death, principally ascorbate, where you could, with the C cleanse, find out how much you need. And so we have developed and others along with us have developed functional tests that allowed people to decide and find out how much they need at a given moment in time, and then how much you take on a daily basis until they recheck how much they need on a more systemic basis.
Katie: That’s awesome. And I love that you brought up magnesium. That’s something that I learned about many years ago and have been taking regularly and making sure that I get enough of since that time, and I definitely notice a difference from doing that. In my research, I’ve read that magnesium is useful for literally hundreds of reactions in the body and that because of, for instance, depleted soil levels, and changes in our food supply, many of us don’t get enough without even really realizing it, and it’s a difficult thing to get an accurate test for. Whereas in general, from what I read, it’s something that we can take in moderate levels relatively safely. So is that something that you also take regularly?
Dr. Jaffe: Oh, yes. I tell you how much I take on a daily basis in a moment, but my colleague Dr. Ron Elin showed about 15 years ago, that if you’re in the lower half of the serum magnesium range, you are chronically deficient, and he called it CLMD chronic latent magnesium deficiency. Others, including ourselves, have proved that if you have evidence of low magnesium, which means high blood pressure, kidney issues, liver issues, etc., you’re likely to have serum magnesium in the lower half of the range. And if you’ll have healthy magnesium in your cell, you’ll be in the upper half of that serum range.
So yes, magnesium is mostly inside the cell. Only a little bit is in the blood. But thanks to Ron Elin, Mildred Seelig Burton Altura and others, including our work. We now know how to find out whether you’re at risk, which is you’re in the lower half of the serum magnesium range and what to do about it, which is enhanced uptake of magnesium with choline citrate. No other choline works, must be choline citrate, not choline bitartrate must be choline citrate. Now you enhance the uptake, chaperone delivery and the cellular retention of magnesium. So that instead of one third, which is the maximum you get today from the best of the best of the best of the best of the magnesium, one third comes into the body through the ion channel, and frankly, it tends to run out almost as fast as it comes in. So one of the things that we pioneered was enhanced uptake in chaperone delivery and retention of magnesium. And over the last decade or so, we have reconfirmed what Ron Elin postulated, and I’m glad to say he and I are still colleagues from our days at NIH many years ago.
Katie: Got it. Makes sense. Okay. Then moving beyond there you also mentioned homocysteine, which I’ve read about and heard as a marker related to heart health, for instance, but explain what homocysteine is and what it tells us about what’s going on internally.
Dr. Jaffe: Well, homocysteine is an amino acid that Kilmer McCully put on the map in the 1960s because of the link between elevated homocysteine and accelerated atherosclerosis, coronary artery disease, stroke, and other cardiovascular risks. Since then, it’s been proven to be an all-cause morbidity, mortality indicator, which means it’s even more important that and what’s really important is the relationship between methionine and homocysteine. You want your methionine to be up so you can methylate at will and as needed. You want your homocysteine to be down to protect you from cardiovascular and other chronic diseases. And the best outcome goal value for homocysteine is less than six. And you get there by having a high sulfur diet, that’s GGOBE, garlic, ginger, onions, brassica sprouts, and eggs. And by having enough of the cofactors, including magnesium ascorbate, polyphenolics that we were just talking about, to make sure that your methylation systems are working efficiently. So it’s a little complicated, but we can use nature, nurture, and wholeness to guide us using smarter systems. And that’s what we’re talking about today.
Katie: Okay, great. So let’s go through because those were the ones I was more familiar with. There was a couple that you mentioned that I am not as familiar with, the first being I think you said LRA cell cultures. Can you explain what that is?
Dr. Jaffe: I sure can. LRA means lymphocyte response assay, LRA, lymphocyte response assay, and lymphocytes are white blood cells that carry memory. So some of your white cells remember when you were in childhood and had childhood measles, mumps or whatever childhood infections you had and protect you because of remembering that you’ve had that and recovered. And then there’s another aspect of these white blood cells called T-cells that respond without what are called antibodies.
So there are different aspects of cell cultures and what you need is an ex vivo test. Ex vivo means the blood reacts in the laboratory just as it reacts in the body. And LRA happens to be a 35-year-old, but just coming into its own recognition lymphocyte response assay that’s ex vivo has very high precision. Less than 3% variance on blinds with samples and has been used in more outcomes, successful studies of autoimmunity and remission and restoration of immune tolerance and reduction in inflammation and improvement in repair competency, than any other assay. We have 80,000 cases in our database of 25 million cell cultures accomplished. And we’re glad to acquaint your listeners with the testing, you know, they may not be familiar with.
Katie: Okay, what about the urine pH? What does that tell us about what’s going on inside the body?
Dr. Jaffe: Well, there’s one time of day and that’s after six or more hours of rest when the fluid in your bladder equilibrates with the cells in the genital urinary or bladder system, and you get a non-invasive measure of cellular acidosis or alkaline adequacy. Akaline means magnesium, acidosis means magnesium deficiency. If your cells are acidic, then your urine pH will be below 6.5. The healthy range of 6.5 to 7.5. If it’s consistently above 7.5, we have a different conversation about Tenenbaum illness, but most people are below 6.5, meaning they need more magnesium in their diet and supplements. And usually enhanced uptake in chaperone delivery magnesium, which is an area that has been a particular research interest in documentation tools.
Katie: Gotcha. Okay. So if either of those are out of range, that one it sounds like does very much directly tied to magnesium, are there other factors that we need to optimize as well?
Dr. Jaffe: Well, during the day, it turns out there are at least 25 different things that influence your urine pH. It’s only after six or more hours of rest, that the urine pH correlates tightly with cellular magnesium needs. And that’s why we measure it after rest, and usually at home, keeping a daily log, and then bring that to your health coach or health professional who can help you understand? What does it mean about Do I need more magnesium? Or do I need more choline-citrate, how many doses a day? And generally, it’s an extra dose, for every half pH unit below 6.5. Because pH turns out to be logarithmic and what that means is that a little change makes a big difference in biology and physiology.
Katie: Okay, got it.
This podcast is sponsored by Jigsaw Health, my source for magnesium. You probably know, if you’ve read my blog, that magnesium is responsible for over 300 biochemical reactions in the body. It impacts blood pressure, metabolism, immune function, and many other aspects of health, including hormones. It’s known as the master mineral and it’s one of the few supplements I take regularly. And I have found a specific way to take it that works best for me in very specific forms because if magnesium is taken in the wrong way it can lead to digestive upset or if it’s taken too quickly it can cause all kinds of problems. So, I take two supplements. One called MagSRT which is a slow release form of the dimagnesium malate. The slow release technology makes it easier on the digestive system. So I don’t get any of the digestive disturbance that comes with some forms of magnesium. I take this form in the morning and at lunch. So, two capsules with breakfast, two capsules with lunch. And at night, I take a different product MagSoothe, which is magnesium glycinate which is magnesium bound with the amino acid glycine to help sleep. And in combination, I noticed the biggest effect from those two particular products. You can check them both out and save by going to jigsawhealth.com/wellnessmama. And the code wellness10 will give you $10 off any order.
This podcast is brought to you by Pique Tea. I love all of their Triple Screen teas that can be consumed hot or cold. You might know that tea has been used for centuries for a variety of reasons in almost every culture around the world to naturally boost energy levels, to increase mental performance, for immune and gut health support, or longevity or just to achieve a youthful glow. It’s truly been a part of almost every culture. It’s noncaloric so I drink tea of some kind, either herbal tea or caffeinated tea almost every day even when I’m intermittent fasting and even during my fasting window. So, unless I’m on a full water fast, I will drink noncaloric tea while I’m still fasting. Pique Teas in particular are made from organic, high-quality tea leaves and ingredients sourced from around the world very carefully. They are the purest teas that I have found because they do something called Triple Toxin Screen for heavy metals, pesticides, and toxic mold so that you know you are getting the best, highest quality tea without the junk. Not to mention, their teas taste amazing and my kids love them too.
For all you moms listening, these teas are great for gut health. They use a cold-brew crystallization process, so you get more concentrated antioxidants and polyphenols, up to 12 times as many actually with each serving. These are the compounds that are known to be responsible for a lot of those benefits that I listed, and so, that increase is a really big deal. And given that these come in little tea crystals, I can easily add them to my smoothies or to hot or cold water. They dissolve in seconds. And I always carry a few of them in my purse when I travel. They have a range of caffeinated and noncaffeinated options. I love their Organic Jasmine in the morning for energy and for mental clarity while I’m podcasting and I love their Herbal Mint when I need to wind down and relax. Pique is also the first company in history to win three gold medals at the Global Tea championships. You can save 10% off Pique Teas by going to piquetea.com/wellnessmama and using the code WELLNESSMAMA. Note that this does exclude their Fermented Pu’er teas, but it is valid on everything else.
And then now I want to switch gears and talk about one of my favorite things that I’ve been reading about recently, which is vitamin D. And I’m so glad that you mentioned this is one of the predictive biomarkers. There’s so much data across the board that I’ve read, and I’m sure even more that you’ve seen on all of the various ways that vitamin D is vital to overall health and right now in a very timely way toward reduced risk of complications from respiratory illness. I’ve also personally seen studies on the link between optimal vitamin D levels and lower risk of certain types of cancer. I think this is a really big deal and a marker that a lot of people should be testing and probably are not. But from your perspective, walk me through why vitamin D is so important. And what level do we want to see when we test for that?
Dr. Jaffe: The best outcome goal value for vitamin D properly measures 50 to 80 nanograms per mL. What that means is that the country, United States, in general, people have between 15 and 25, which more than triples their cancer risk. And if you take that vitamin D under your tongue as drops, you can get into the brain before the body and get it in. Whereas Dr. Michael Holick, a colleague who’s known as Dr. Sunshine points out that millions, maybe 40 million Americans do not absorb vitamin D from their intestines because of maldigestion, dysbiosis intestinal problems. And so these are people who can swallow a lot of vitamin D and get very little benefit.
So we know what the best outcome goal value is 50 to 80, that provides a safe range. We take as many drops under the tongue as needed to get you into the 50 to 80 range, and then you celebrate because it’s a neurohormone. We call it a vitamin, but it’s not really a vitamin, it’s a neurohormone and you’re right, it does a lot of things, both outside and inside the cell. And you need other cofactors with it, including magnesium and various kinds of vitamin K. But vitamin D is very important and the best outcome goal value is 50 to 80. That dramatically reduces your cancer risk and improves your all-cause morbidity, mortality, it reduces your cardiovascular risk, it improves your neurohormonal balance because it is a neurohormone itself. So 50 to 80 is your goal value, you can get there with drops under the tongue.
Katie: Gotcha. So just to clarify, this is one that you would absolutely recommend testing for and then supplementing with to get into those proper ranges. I know I’ve seen that as well that in the U.S., especially many, many people are deficient. And this is a tremendous risk factor, like you said, for a lot of problems that can much potentially much more easily be avoided if we optimize some of these things.
Dr. Jaffe: Well, all the predictive biomarkers are important, vitamin D especially so we now know what the safer, better outcome goal value is. And that’s where I want everyone to be. Now I have read even in “The New York Times” by distinguished scientific journalists, that because the country is deficient, it’s normal, statistically normal. That’s a statistical term having nothing to do with the common-sense meaning normal, but it’s statistically normal for people to be deficient. So that’s the way it is and don’t test and don’t stop them. As I think you can tell from the tone of my voice, I rather profoundly disagree with that point of view, you should test you should know, and you should be in the healthy 50 to 80 nanograms per mL.
Katie: Yeah, I think that’s another really important point that you just brought up. And I noticed that when I was going through Hashimoto’s and trying to get my levels back into normal range and to get into remission, which I now have. But that was something my doctor told me was that even within the range of quote unquote, normal thyroid hormones, you can still be having issues because those are based on averages. And the people who get tested for thyroid problems suspect they have thyroid problems. And so sometimes even what we’re seeing within the normal ranges are not optimal. And so that’s a really important distinction, I think, when we’re looking at labs as a marker of health is understanding that difference between just okay, and in normal range, and what optimal should be. And I love that you make that distinction in your work as well.
Dr. Jaffe: No, as someone who used to run the Clinical Center Labs at the National Institutes of Health, that’s something I can talk about. What we call the statistically normal or statistically usual range has to do with populations as you’ve correctly said. What we’re talking about today, though, has to do with individual personalized, proactive care. So if you know what the best outcome values are for each of these predictive biomarkers, the ones that cover all of epigenetics, I think you would want all of them to be in your healthiest outcome range, which means you have a 99 plus percent chance of living 10 or more years, as opposed to a 10% or 15% chance of living 10 plus years. I choose to be in the minority of people who are going to live and be dancing at 120 with their friends around.
Katie: I love that. I’m with you on that too. You also mentioned omega-3 and this is another area I would love to get your take on and to go deep on because Certainly, I’m a big fan of the National Institutes for Health. And I spent a lot of time in PubMed reading studies. There’s a lot of data about the benefits of omega-3s when we see populations that live a long time. That’s a common factor that they mentioned even in Blue Zones. But then I’ve also seen some information that you have to be careful with the sourcing of these because that’s something that can easily go rancid. So let’s start with testing. How can we know if we need more omega-3s? And what are good levels look like in the body?
Dr. Jaffe: Right, what are good levels look like? Now you look at Bill Harris’ work and others, and the answer is more than 8% omega-3 in the membranes of cells. This too can be done on a lancet, just the drop of blood on a piece of filter paper. And I remember the day when I was visiting with my colleague, Patti Bursar at the Military Medical School and Bill was there talking with her about how hard it was to find people who are taking in healthy amounts of healthy omega-3 essential oils.
Having pointed to me, he took a lancet out, took a drop of blood, and in about 10 days he sent me back reports that said my index, my omega-3 percentage, my omega-3 index was 13. So I called him up. And I said is this…I know 13 is higher than 8, that I understand. Is 13 better than eight? Or is it worse? He says, we don’t have enough people who are above 11. You know, you’re our poster child.” Now, you made a critical point. You can buy a lot of fish oil that is rancid and toxic. Rancid because air oxygen has damaged the essential fats and because it was not distilled under nitrogen. The omega-3 that I recommend is in a mycelized soft gel which is distilled under nitrogen. We remove the bad stuff, you concentrate the good stuff. You concentrate the EPA DHA essential omega-3 fats, we mycelize those in a soft gel.
And what do I take? Well, 6 to 10 grams a day. Now 6 to 10 grams a day is more than 3, and 3 is what many physicians today recommend, but I think our oxidative burden is higher. I can tell you that it keeps my omega three index above 8%. And that’s what I recommend. Now Barry Sears is an expert in this area of essential fats, he now recommends 15 grams of omega-3 EPA DHA a day. Different experts have different points of view. I think what’s clear is we need to reduce the omega-6. We need to increase the omega-3. Read Artemis Simopoulis’ work on the Greek Mediterranean diet and lifestyle, about why we need more omega-3, and we need less processed, crisp foods that are rich in omega-6, but it’s actually rancid and damaged omega-6, so it’s a double harm. So omega-3, yes, essential fats, yes, seeds and nuts and sprouts and foods that contain these as protected essential nutrients, yes. But once you start isolating and processing, you probably are getting trouble.
Katie: Yeah, that’s a great point. And that is a bigger dose than I would expect and I wonder this is what I’m curious to get for myself, now.
Dr. Jaffe: It’s not yet typical. But I can tell you when I started this because…there was a reason, but I started just because I needed to. I can tell you more and more and more of my colleagues have come around to the fact that we need at least 5 and between 5 and 10 grams a day of EPA DHA. Not the precursor because it turns out the precursor doesn’t get converted in most people to the active EPA, DHA. And given how much omega-6 most people get, look at the NHANES data, look at the PubMed data. When you look at how much omega-6 most people get, 5 to 10 grams a day is now a conservative intake, not a high intake.
Katie: Well, that’s… Yeah, that’s awesome to know because I can’t wait to test mine and see. I’m curious about that one. You also mentioned the last one, which I’m hopefully I’m not going to butcher it. I think you said 8-oxoguanine. Is that what you said or guanine?
Dr. Jaffe: No, no guanine, you got it. Guanine is one of the DNA bases. So it’s one of the language…it’s one of the letters of the genetic alphabet. Now, it’s also subject to air oxygen damage and oxidation and then it becomes 8-oxoguanine. We know what healthy people have, it’s less than 5 nanograms per gram of creatinine, which means you can take a spot urine, preferably in the morning but a spot urine and analyze it. And as long as you’re correct to the amount of creatinine that’s present, you have an accurate measure. So you don’t need a 24-hour urine. And it is a urine test. It’s non-invasive. And it completes the suite of protective epigenetic tests or the tests that measure epigenetics, where again, we know the best outcome goal value, and we can work with your lifestyle to get you.
Katie: Got it? Okay. And then, I know this wasn’t one of the eight but I’m curious to get your take on it. Another test that often is run when people do routine labs is a lipid or cholesterol panel. And this is a somewhat controversial area of research and I know that from what I’ve read, other countries have different ranges and different markers that they look at than we do in the U.S. So I’m curious what your take is now on what healthy cholesterol ranges look like and ways that we can optimize that. I would guess there’s an omega-3 component to this answer as well, but I’m really curious to get your take on cholesterol.
Dr. Jaffe: Well, I can tell you the answer and then I’ll tell you why I know the answer. But the answer is you should measure your oxidized cholesterol, your oxidized LDL. Your air oxygen damaged cholesterol and LDL contain 100% of the risk. And this may surprise people but in my, now, half a century in medicine, having collaborated with Don Cry, Bob Maley, and Bob Fedus on animal models of human heart disease, etc. many decades ago. I can tell you for sure that cholesterol and lipoproteins and HDL and LDL are innocent bystanders.
It turns out that magnesium protects essential fats in transit when they’re in LDL. Magnesium acts as an antioxidant to protect essential fats from air oxygen damage while they’re in transit. So I have taken care of people who have lived long and well with elevated lipids in their blood because they were high-performance, high-stress people and they needed to repair their membranes with cholesterol. They needed to repair their hormones through cholesterol, all of our hormones come from cholesterol. The notion that we should actually poison or inhibit the system that makes cholesterol. That was an interesting idea in the 1960s. It’s a scientifically-disproven idea today you can look at Malcolm Kendrick’s work online, you can look at many other people who along with our group showed that as long as you don’t damage the essential fats, they don’t harm you. And as long as you keep a healthy balance of omega-3 to omega-6 by eating whole foods that you can digest, assimilate and eliminate without immune burden. You can live long and well.
So what is it that’s so important about cholesterol? Well, let me give you some facts. And I hope you know this, I’m sure that you can check this out to verify. Half of the heart attacks occur in people with cholesterol above 200 and a half of the heart attacks occur with people below 200. Half of the heart attacks occur with people with LDLs above 100, and half of the heart attacks occur with people below 100. Of what meaning is that. A major person who advocated for that point of view said, and I quote, “Doctors are so dumb, they can only remember simple numbers like 200 and 100.” I said, “Well, what about the individual?” and they looked at me and said, “You’re so naive.” I don’t think I’m naive. Forgive me, but I don’t think I…
Katie: Wow, yeah, that’s really shocking, although I probably shouldn’t be at this point.
Dr. Jaffe: No no, excuse me for jumping in but it is shocking because a lot of medical care is devoted to these, your cholesterol or your LDL or your HDL or are your particles up or down this month versus another. And I’m telling you, it’s all about damage, oxidation, and reduction. Reduction has to do with antioxidants and buffering minerals like we’ve just been talking about. Oxidation has to do with oxygen and keeping it away from delicate things inside your body until you need it. Because oxygen is essential, without oxygen we wouldn’t be having this conversation. But we have basically fallen in love with a reductionist mechanistic model of letting the body fall apart and then trying to patch it up. And I think that’s the wrong model.
I want to keep my body renewing itself continuously, no part of my body or yours is more than 10 years old. And that’s our bones. So this notion that I’m getting old, relative to someone who is, shall I say, young is an illusion. If you get enough of the good stuff, you repair your bones and joints and body, and most of us is actually renewed every few months. So you get enough of the good stuff in, make sure that you exclude as much of the bad stuff as you can. And then learn how to thrive in this stressful, challenging 21st century time, including with these biomarker kinds of tests and understanding what the best outcome values are.
Katie: Such great advice and as we get close to the end of our time…I want to make sure I respect your time, I’m curious, first of all, if there’s a book or any number of books that have had a really dramatic impact on your life, and if so, what they are and why?
Dr. Jaffe: Well, the book that does come to mind is from the late 19th century, and it’s called Color and Light it was by Edwin Babbitt, who was what’s called a polymath, which means he was an MD, he was a JD, a lawyer, he was a PhD. And he basically anticipated the whole field of color therapy. And it turns out there’s a whole non-invasive color healing system that I studied because of Bhante Dharmawara that I have found to be first-line part of comprehensive, personalized, proactive predictive health care. And I want to get it incorporated into the curriculum of training the next generation of doctors and nurses, and health coaches and professionals because we really can feel and function better throughout the entire lifespan of our lives.
In my dad’s case, he died in my arms at 90 of natural causes, but he wasn’t supposed to live over 50. So we had an extra 40 years to enjoy each other. Bhante 110, and had highest frequent flyer status on three different airlines when he was 110. So it is possible to live long and well. As long as we choose the habits of daily living, that let us repair and renew. And that keep our predictive markers our functional personal predictive markers at their best outcome goal values. So live long and well and add life to years and years to life. That nature nurture and wholeness be your guides and eat the foods you can digest, assimilate, and eliminate without immune burden, staying well hydrated. And knowing that you move and think in order to add value to the lives around. Leave the place better than you find it. It’s not a bad philosophy.
Katie: That’s wonderful. And I think, like, you’ve given so much practical advice today. One question I’d love to wrap up with, and you may have just answered it already. But what is one thing that you would love our listeners to take away and remember from this conversation that can help really improve their life starting today?
Dr. Jaffe: Well, here I’m going to quote the 2000-year-old man Mel Brooks if there was one thing to take away from this conversation is that life is about choices. “And while the past is behind us and the future has not happened in this moment, we can choose life, and we can choose to be grateful for whatever our portion is so that we can touch others in a way that makes them smile.”
Katie: I love that. What a perfect note to end on after so much wonderful information in this podcast. Dr. Jaffe, I’m so grateful for your time today and for sharing all that you’ve learned in all of your years of research and study. Thank you so much for being here.
Dr. Jaffe: Very grateful to share this with your audience. And thank you for being you. It was a lovely conversation.
Katie: And thank you as always to all of you for listening and sharing one of your most valuable resources your time with both of us today. We’re so grateful that you did and I hope that you will join me again on the next episode of “The Wellness Mama” podcast.
If you’re enjoying these interviews, would you please take two minutes to leave a rating or review on iTunes for me? Doing this helps more people to find the podcast, which means even more moms and families could benefit from the information. I really appreciate your time, and thanks as always for listening.
Source: https://wellnessmama.com/podcast/russell-jaffe/
0 notes
Text
Blood and Honey: An Interview with Dr. Danica Anderson on Healing for Women War Trauma Survivors

Danica Anderson reading coffee grounds (tasseography) in Ahmica-Vitez, Bosnia
On a quest to connect my grandmother and Zejna, the Bosnian refugee we sponsored together in the 90s—I am sure not by accident—I discovered the work of Dr. Danica Anderson, author of Blood and Honey: The Secret Herstory of Women, South Slavic Women's Experiences in a World of Modern-day Territorial Warfare. In this book, she explores war trauma experienced by women during the Balkan War. Through recipes, and cultural customs, Blood and Honey is a book of spells for these women to heal themselves through bioculinary* arts and biosemiotic** communication. In this beautiful interview, she brings me closer to Zejna and my grandmother, and reveals woman-centric secrets to understanding the rhythms of our subconscious. From coffee readings, to Marija Gimbutas you will love the magic, mystery and healing of this interview!
* Inscribed social memory working collectively with agriculture, herbs, food crops, animal husbandry to bee keeping that preserve South Slavic ancient Neolithic Practices.
** (from the Greek bios meaning "life" and semeion meaning "sign") is a growing field of semiotics and biology that studies the production and interpretation of signs and codes in the biological realm.
First, I would like to ask how your family's trauma from former Yugoslavia was manifest in your life in Chicago. You mentioned that your mother didn't want to speak of it. Was silence part of the intergenerational trauma?
The killing silences are transgenerational in that the silences are passed to future generations. My mother was indoctrinated into killing silences by her mother and grandmother both who lived through world wars in former Yugoslavia. It was not until her late 80’s that my mother spoke of her WWII concentration camp experience to her granddaughter. I don’t think she had the words previously due to shame and guilt that was not hers.
The way trauma ebbed and flowed in my childhood was seen with domestic violence and child abuse. I have early memories, which children who survive child abuse often have. Although the child or infant is preverbal, these memories are stored in the body and often unable to be given a vocabulary until the child’s development of language. This is how children are not aware their lives are violent and instead think it is normal. With the mother submissive and beaten into the killing silences where she has no one to tell, the child cannot gain a vocabulary for the trauma. Instead the killing silences are epigenetic (we are shaped by environment that influences our genome,) thus transgenerational trauma.
You also talk about the women in your Serb community and their bioculinary traditions and ethno-dance traditions, which were both healing, and the foundation of your book's philosophy. Can you describe how these traditions manifest away from one's country of origin? Did your family grow their own food, for instance?
To describe how oral memory traditions capacity for the transmission of human memory is best done when we realize it has been done with a cast of thousands of generations and continues to this day no matter where the geographic location. We are talking about millions upon millions of actors taking up their role in performing the enactment of memory-lived life experiences of our ancestors without external aid meaning no books, scripts to read from, youtube or modern day manuals. If anything, the oral memory traditions are exactly the data needed for study in long term memory and transmission of memory over the Ages with such a vast pool of actors.
What I have observed in the diaspora of not just the South Slavs, but all diverse groups of people is how they reach for their human memory storage triggered by geographic relocation. In one way this is how travelers experience their journeys, a triggering of human memory in their lineage of ancestors’ life experiences. The culture and corresponding oral memory traditions (a ritual science) contain the way of life and the adaptations to the environment. Fleeing the violence and aftermath of war, my parents immigrated through Ellis Island to Chicago. They brought with them their way of life. We had a small back yard for the garden of vegetable and plants. My father would trek to the Southside of Chicago to the train station each fall to buy crates of grapes for wine making. A wooden barrel with an iron press in our basement was arranged so that all my siblings and I would pick off the grapes and toss into the sink to wash and then into the barrel. This took days. Once done, since I was the littlest I was placed into the press to squash the grapes. I remember having stained purple feet and legs. My mother made everything from scratch. Her strudel called ‘pita’ was the finest of translucent phyllo dough she stretched over the kitchen table. The kitchen table was where I would crawl under and watch my older siblings dance the kolo (s)- Serbo-Croatian for folk round dance. The food and gardens are bioculinary practices found in oral memory traditions, a ritual science.
I never considered tasseography (tea or coffee readings) as such a powerful way to tap into the protolinguistic self and heal trauma. You describe "storied instructions" through "small acts", meaning, and the construction of new memories over traumas through mindful experience of the everyday. This is an essential aspect of your book, Blood and Honey Icons: Biosemiotics and Bioculinary and it also is incorporated into your trauma recovery work with Bosnian women war survivors. What kinds of transformations do you witness among women who have been subjected to gynocide and sexual trauma?
The small acts are often repeated and done daily or seasonally through thousands of generations into the present generation. The present generation layers over the oral memory traditions with their environment and life experiences. This is an extraordinary transformational process when you realize that what we live, feel and experience both biologically and even psychobiologically is heritable: transgenerational. Basically, how we live and our life experiences has far reaching social, cultural way of life implications.
The way of life for women is targeted by wars and violence for this very reason since we live in a phallocracy where the male dominates. Yet, women are the creators of culture since we are all born of a woman. Her domestic arts and child rearing are critical transgenerational intangible heritage that evolves our relations with our environment embodied with her life experiences. The Bosnian women war crimes and survivors cleaned up after each war that took place over a century. In doing so, her domestic labor and child rearing was one of survival not evolving thus thriving. Transformations were had by the women survivors who no longer could stand the survival mechanisms found in trauma. The critical juncture was ‘to ask do I need to survive or thrive’. What happened in the aftermath of the Balkan War was a return to what their grandmothers did to survive such as the beehived wood ovens, garden, weaving to dancing the round folk dances called kolo (s).
What I am talking about is how the transformations came through when women regained their role as creators of culture and corresponding oral memory traditions- a ritual science containing prehistoric chants, songs, dance to bioculinary and all way of life before the modern conveniences. One Bosnian war survivor stated when she had nothing, she discovered she had everything with her house that had a field of crops and chickens. She said the farmer and those chickens saved humanity thus transforming humanity.
When survivors did not have an oral memory tradition to transform mostly sexual trauma and genocide, I was told to talk with those struggling. In my paper on Slavic Maternal Fright I wrote about a thin Bosnian-Herzegovinian pregnant woman in her late twenties had big dark circles under her eyes; her hands shook even at rest. When she began sharing her maternal fright, she released expressions that were formerly deliberately hidden and avoided. Her fear was that her husband’s loss of 18 family members at the village of Ahmica-Vitez, Bosnia on April 16, 1993 would flood into her fetus. You see story and metaphor heals only if we author our life experiences. Since trauma is primarily about extraordinary experiences in the personal lives of individuals with women and children the majority facing such impossible circumstances, what occurs is an explosive quality because change is immediate. Thus, her stories are excluded. Women, 51% of world population suffer greater trauma and she is removed from restructuring a self-identity. In the end women cannot reestablish their place in the broader scheme of human affairs and history. Without women’s authored stories and metaphor, we do not have culture. We cannot access healing methods. Instead what is claimed as culture is in reality violence normalized and nationalized with a host of memorials and monuments.
For sixteen years, I have been working extensively with the Bosnian-Herzegovinian women war crimes and war survivors in the aftermath of the Balkan War (1991-1993). I have determined that maternal fright is the entrainment of transgenerational fear and trauma through the female neurobiological processes (Anderson, 2014, Christie, Pim, 2012). This pregnant woman took a green magic marker I brought with an art pad to her apartment. She took the marker and drew a spiral on her pregnant abdomen. When she was done she stated this new oral memory traditions would prevent the transgenerational transmission of trauma. She said she was transformed. She became author of her own story which was excluded and not conforming to the norms of violence.
There are many more stories I write about in my book, Blood and Honey the Secret Herstory of Women: South Slavic Women's Experiences in a World of Modern-day Territorial Warfare. In the chapter of Salutogenesis, the promotion of health, I share the story of a Croat young woman who was sold into sex trafficking in the aftermath of war. Her transformation came more than a decade after I met her in Holland. I asked her to write her story for my book. She took eons to respond and when she did what she wrote was compelling. She told me that she could not retell the story since she is no longer that pain or that victim. In fact, she said her story was not her responsibility anymore and that it was mine now.
As I've shared with you, I recently reunited with a Bosnian Muslim woman my grandmother and I sponsored in the 90s. Her life is very simple, she was not traditionally educated, and she is now 80. She was also subjected to incredible war trauma, which I did not feel entitled to ask her about, even though she wrote me about it in her letters. How do you interact in your Kolo: Women's Cross Cultural Collaboration work with women from various backgrounds and ages? Are there common experiences and acts you found to bond women across these experiences?
Isn’t this the ‘killing silences’ when you and most women feel they are not entitled to ask for grandmothers, mothers and daughters’ life experiences. Yet, you moved forward. The transformation is there in your grandmother’s letters thus providing intimacy and bonding. Note how you were able to set up a space and place for your grandmother’s war stories and trauma. The common experiences and small acts that you performed for your grandmother are the same I invite in when I interact with women. To be sure there is diversity involved since their traumas and life experiences like fingerprints are not identical.
With the South Slavic kolo, the round folk dance or to be in a circle is a multi-dimensional space creating place for women to bond and heal. What I noted was when there is healing, there is bonding and a moment of female solidarity. Having a space and place to heal is the real hospital. Interesting in the word hospital since it originates from the meaning for guest and is the root word for hospice, hotel and hospitality. The key is the relation between guest and shelterer. As with my kolo trauma work and your grandmother’s letters the relations between us and them become one while accepting the diversity. When I faced the Bosnian women in the beginning of my work in Bosnia I knew I was in a room filled with my mother in everyone present. Something in what I felt opened up the space and place for us to bond and to heal.
While daunting I was able to move through my grief with my mother and her WWII concentration camp experience became the common experiences from which women bond, learn and evolve. I knew I had privatized my pain and suffering. My mother privatized her pain and survivorship of Jasenovac concentration camp. Shock cascaded through me since the violence against women stats became a lived knowing. What I mean is I realized the universal suffering and pain most women endure but we are not allowed to voice or speak our realities in a world of violence. Isolation from each other occurs. Women’s inhumanity to women perpetuates endlessly. When I danced the kolo with the women and men, we were all shoulder to shoulder although our feet were doing their diversity in dancing the same path. The feelings of detachment and divorce from female solidarity erased in the shoulder to shoulder circle and dance. Female solidarity flourishes once we include each of our stories and understand our pain and suffering is universal. Privatizing smothers any opportunity to bond out of strength. The movement to be in a circle or the kolo is non-verbal expression of female solidarity; bonding out of strength. There is no bonding as a martyr or a victim.
I love that you refer so often to Marija Gimbutas' scholarship, which I was so fascinated with in college. Her work on SE European goddess-worshipping culture is so profound, and highlights that region as such an important location for honoring the female. How did such a patriarchal, gynocidal culture evolve from one that was so in balance with the natural world of that region?
In the beginning my visits to Bosnia showed how penetrating trauma can be. How do I then work the trauma issue outside the patriarchal norms of authoritative institutions and the ethnic hatreds focused on women as targets? However, I knew the South Slavs in prehistory had a harmonious civilization with profound art in artifacts and their communities. The symbols in what Marija Gimbutas refers to as ‘Old Europe’ lasting until 1800 BCE guided a path to circumvent the patriarchy. What was striking in their kilms, needlework and beehive ovens was the Old Europe symbols. Imagine my awe when the women who used the Old Europe symbols knew the meaning without cracking any of the Marija Gimbutas’ books.
The kolo is Mesolithic in age and something all knew and often danced. In using Gimbutas’ materials and spinning through interdisciplinary fields I was able to excavate the balance of the natural world. When we did so there was great gnashing of teeth and horror. One elderly grandmother said aloud how she taught her children to hate and to hate women. Another woman questioned on the custom to revere the mother who has sons over one that has daughters. What spiraled was activism even if it was banging pots and/or marching the streets for garbage pickup. One woman stated life is better now after the war without the supermarkets, microwave since her small house with a field of crops brought her family together. She became the wise woman who know how to plant, ferment, cook, clean and organize into relations with the natural world and her family.
If you can trace back to when women were forced to carry their father’s name you will see the erasure of women; the erasure of relations with the natural world and; erasure of honoring females. In an old Villa outside Paris is the archeological museum. I moved through the salons of time from dinosaurs to present day. When I walked through the exhibits in the prehistoric window about 80,000 BCE was the Siberian sleeping Goddess artifact. More art popped up, such as the Willendorf Goddess artifact, which is 33,000 years old. But then, the Iron Age appeared with axes, swords and violence. Yet, when I look at culture and oral memory traditions vestiges of old harmonious way of life I find that it is still repeated. This brings me to my work and research where we need to ask what culture is. Many cite violence as culture with ‘boys will be boys’. So we need to ask what violence is. Culture is the way of life centering on women and their female biology processes. Women raise the children. Women create culture. When women forget their creator role in culture or are dominated to not assume their creator role we will continue to be dominated and complicit in following patriarchal norms of violence, we will have the escalating violence.
Finally, I would like to ask you a personal question. I also mentioned that I sense I have been on a "homing" instinct with the former Yugoslavia, traveling back through the influences of my grandmother, who also knew the Balkans because she read Black Lamb, Grey Falcon by the feminist, Rebecca West. This process took me 16 years! Do we go back to the places of deep ancestral knowledge, and even trauma? And I also wonder, why is the process sometimes so long, and so unclear?
The birds do it. The salmon in the oceans do it. It’s called migration. Migration is not refugees fleeing from horrors and violence. Diaspora is not migratory process. Not all species have the magnetic direction for migration. For instance cattle and deer will align themselves in the north-south direction of earth’s geomagnetic field. Pigeons have microscopic balls of iron in their inner ears. How do the whales and dolphins know their way in the vast oceans when migrating? Perhaps, this is the homing instinct you talk of.
It took me 16 years to write Blood & Honey: The Secret Herstory of Women. A very long migratory process and I am elementally changed due to it. I migrated back and forth to Bosnia throughout the years and many other war zones across the globe. My female tacit knowledge- the ‘more than we can tell’ intelligence looks at the epigenetic inheritance which is inseparable from our lived relations to our ecosphere and our cultural environments. I am reminded of that cast of thousands of generations and billions of main actors in the building of a continual process of learning and relearning. Hence, the definition of migration.
All of this is stored in our genome. What we repeat is how our DNA replicates and repeats. This is called evolution. Our biology of perception and our human perception is embodied and literally enworlded. When we learn or relearn we are migrating toward abundance- evolving not just ourselves but all of life. One research for bioculinary practice was about how chickens become fuller in the breast and bigger since the 1500’s because we were eating them.
I do not define trauma as a mental illness. If anything, trauma and the corresponding fright/flight neurological mechanism tell me it’s healthy. My definition of trauma is intensified learning. Yes, it is not something I would jump at to enroll in this beyond doctorate level learning. In fact, most would go kicking and screaming before succumbing to trauma events. Most likely, we relive the trauma over and over again due to the fright/flight mechanisms. Here we can introduce a question to ourselves; do we need to survive or do we need to thrive? That choice which is consciousness allows us to author which venue. Thriving is about the healing process and of course becoming authors of our own stories. The diversity of our stories like the diversity of the kolo dance steps offer up restructuring and reorganization of reality. We are consciously learning to relate to all our environments. Women, especially, learn the empowerment in the role of creator of culture. Men learn to preserve, support and protect culture and all environments. Together the prescience in relation to biological and social complexity- a social intelligence emerges.
Being unclear is not about a lack of clarity since when we make a decision it is with clarity. I think the pattern of being unclear is about not being comfortable with ambiguity. Pregnancy is a good example of being in ambiguity. Childhood not adulthood is a difficult endurance to neither be here or there since decisions release that tension effortlessly. Ambiguity is the state of being not doing. In our societies the fast paced and competitive demand to not fail force us to conform to doing and productivity. More importantly, ambiguity is akin to the kolo in manifesting space and place in time. We need to create a space and place for deep ancestral knowledge.
Biography
Dr. Danica Borkovich Anderson’s interests remain consistent with exploring trauma’s impact as not a death sentence but an enrollment into intensive learning and growth. As Danica points out, the essence is summed up in the concise, collaborative social justice and self-sustainability found in healing our own local communities and ourselves. It’s about ennobling and empowering those who have suffered catastrophic violence and crisis.
Working from a base as a forensic psychotherapist (Certified Clinical Criminal Justice Specialist #16713), a balance of her work has been abroad in Africa, Bosnia, India and Sri Lanka as well as in the United States. While in the U.S., Danica’s experience and training began with the Siletz Indian Tribe in Oregon covering thirteen counties. She served this area using her experience in the clinical field of sexual abuse and abuse issues for a number of years. She has also worked in crisis care for corporations and insurance agencies since 2000.
Danica’s professional experiences delve deeply into “untamed” territory and explores possible engendered approaches that are healing, collaborative and are in sync with the environment presented.
She has conducted extraordinary in-depth work with Bosnian Muslim women war survivors and war crimes survivors. This work is enhanced by Danica’s bi-lingual capacity as a Serbo-Croatian. A decade of work is completed and is now self-sustaining by the Bosnian women. As a Serbian-American daughter of former Yugoslav immigrants whose mother survived concentration camps, Danica researches trauma and its impact identified by social studies that are significantly centered on the female, thus radiating out into both genders and the community at large.
Danica’s consultancy work as a gender psycho-social victims’ expert with the International Criminal Court (The Hague, Netherlands), addresses the importance of a trauma treatment and training curriculum that is distinctive and responsive to the impact of catastrophe and disaster events. Her work considers a wider set of relationships between trauma and environment in which trauma is situated or, alternatively, how the specific culture is perceived in the trauma exposure. Fluid and adaptive across vastly differing and diverse penal and corrections/prison systems including those of military operations, the Kolo trauma treatment and training format has a much broader spatial scale of overall distribution, becoming self-sustainable via the affected population. Anderson’s service in the United Nations World Food Program for the largest humanitarian workforce on the planet in Sudan added profound insight to her research, allowing her to survey a substantive data base that further enhanced her Kolo format.
Danica’s experience and specific skills include:
• The ability to foster not just intellectual understanding but embodiment on topics that are elusive or difficult, cutting edge and innovative or very psychologically based.
• International speaker, presenter/trainer.
• The populations worked with range from: 1) Rebels, militia and war crimes perpetrators (Afghanistan, Africa-Chad, Congo, Sudan & Uganda) and victims of crimes; 2) In Oregon with the Siletz Indian Tribe providing services for 200 tribes and bands; 3) Interfacing and training with individuals and groups in Bosnia, India and Sri Lanka who are professionals in their native organizations as advocates, social workers, Buddhist priests and directors of the agencies open to developing cross cultural collaborative skills in the field; 4) Corporate environments, universities/colleges and speaking engagements at various institutions.
• As a grassroots non-profit, her The Kolo: Women’s Cross Cultural Collaboration work enables her to understand a depth and breadth of both human rights and female human rights especially honed to helping aid in real time and in stark truth positions. Crisis and disaster response protocols and crisis intervention/prevention development and implementation are a few of her in-depth skills. Engendered training programs are few yet critically needed in corporate environments.
#killing silence#kolo#Bosnia#bioculinary#biosemiotics#trauma#genocide#Dr. Danica Anderson#marija gimbutas#migration#tasseography#transgenerational#Blood & Honey: The Secret Herstory of Women#zejna#isota#grapska#mel potter#melissa hilliard potter#slavic maternal fright#interview
26 notes
·
View notes
Text
Canine Cancer Resources and Hope
This photograph is the creator’s dog, Duncan, totally anesthetized, intubated, and prepped for a dosage of palliative radiation remedy meant to cut back the scale of his nasal carcinoma. It seems to be brutal, and but, hours later, he’d be totally recovered and asking to play a sport of catch along with his favourite ball.
For every of the previous six months, I’ve written an article for WDJ concerning the cancers that mostly afflict canines. It’s my honest hope the articles will assist any dog house owners who discover themselves in a combat for their very own canines’ lives perceive what they’re up towards, study therapy protocols and median survival occasions, and the place to search out scientific trials for and cutting-edge analysis on the varied cancers.
Gathering the data for the sequence took an enormous period of time and work, however it’s been a labor of affection – a method of paying again the numerous devoted, educated veterinary professionals who helped me get by way of the diseases of my two earlier canines.
Unfortunately, each of my beloved canines finally succumbed to their illnesses. But we loved many great days collectively whereas we lived with most cancers.
IT’S A PERSONAL FIGHT
My Border Collie, Daisy, was identified in 2010 with transitional cell carcinoma, a uncommon type of most cancers, accounting for about 2% of cancers that happen in canines. I threw myself into researching the illness and remedies and was lucky to have a gaggle of wonderful veterinary specialists on her staff.
I used to be petrified previous to Daisy’s first therapy, however her main veterinarian, Dr. Jeffrey Bryan, assured me that extreme reactions have been uncommon and this therapy would supply the perfect alternative for an prolonged life span with good high quality. My belief in her good docs was not misplaced; Daisy lived with nice high quality of life for 2½ years after analysis, present process chemotherapy throughout most of that point (see “Chemotherapy Can Be Kind,” WDJ October 2011), even enjoying with a flying disc after each therapy.
Then, in 2015, my different Border Collie, Duncan, was identified with nasal carcinoma – one other uncommon type of most cancers in canines, accounting for about 1% of all canine neoplasia. It was inoperable, however radiation remedy offered the perfect likelihood at decreasing the tumor measurement and offering an extending survival time.
Even after the expertise with Daisy, radiation remedy frightened me: my 14-year-old dog needed to be totally anesthetized day by day for 5 days in a row to obtain a therapeutic dose of radiation to his head. Duncan was a really delicate soul; I nervous about how these all-day experiences would have an effect on him, to not point out the dangers of all that anesthesia.
To my shock and delight, Duncan enthusiastically embraced the day by day street journeys of two hours every method and adored his veterinary technician. He fortunately left me within the ready room to go along with her for therapy. I’d look ahead to hours in a bookstore, shopping for method too many books and ingesting method an excessive amount of tea.
At the tip of the day I’d decide him up and we might journey house. By the time we arrived house, he had fully recovered and was able to play ball for hours (in his heaven, balls rain from the sky). He felt higher after these radiation remedies than he had within the weeks prior. There is one thing to be mentioned for the pain-relieving properties of radiation remedy.
We had hoped for a superb 12 months. We acquired an excellent month. Yes, I’d do it once more in a heartbeat.
NOT FOR THE FAINT OF HEART
I’ve to confess that the analysis for this sequence left me discouraged; 50 years of scientific investigation into most cancers has resulted in solely reasonably improved remedies – choices that, typically, prolong sufferers’ lives for just some months at typically unimaginable value (bodily, emotional, monetary).
For perspective, I turned to somebody who has been finding out, researching, and treating canine most cancers for greater than 15 years, Jeffrey Bryan, DVM, PhD, DACVIM Oncology – sure, the identical individual I used to be fortunate to have as my canines’ first vet. Dr. Bryan is now not in personal apply, having lengthy since decamped for analysis and academia. He is now a professor of oncology on the University of Missouri’s College of Veterinary Medicine, and director for the college’s Comparative Oncology and Epigenetics Laboratory. When I first met Dr. Bryan, he was working in a veterinary apply in San Francisco. He impressed me along with his heat and information method again when, and he’s solely gotten hotter and extra educated with time on this difficult discipline.
I requested Dr. Bryan whether or not he nonetheless feels hopeful about treating canine most cancers, and he mentioned he completely does. “What gives me hope is the fact that we make progress every year,” he instructed me. “I watch brilliant young clinicians and researchers become attracted to oncology every year, making me optimistic for creative new solutions. Companies come along with new approaches to treating cancer all the time. Some of these work very well.”
Dr. Jeffrey Bryan in 2000, when he was nonetheless in a common apply veterinarian in San Francisco. Coincidently, he’s analyzing a affected person he had been treating for mammary most cancers
Dr. Bryan jogged my memory, nevertheless, that it’s fruitless to hope for the “end” of most cancers. “Cancer will always be with us, I’m afraid,” he says. “It’s an evolutionary disease. We need to continue to get better at recognizing it early, addressing it comfortably, and fitting the most effective treatment to each patient.”
Dr. Bryan’s observations replicate a number of the latest approaches to most cancers therapy, whether or not it’s for people or canines. Some researchers are transferring towards reframing most cancers as a power sickness, one the place sufferers can coexist with most cancers cells (so long as the most cancers is prevented from rising unchecked). It is hoped that new diagnostics may be developed to offer the earliest identification potential and then eradicate cancerous cells at inception, thereby stopping them from growing into an untreatable malignancy.
As depressed as I’m concerning the prevalence of canine most cancers, I do discover hope within the work of Dr. Bryan and all of his colleagues working within the specialty of veterinary oncology. Remarkable advances have been made in treating our canine companions, supported by the developments in affiliated fields equivalent to imaging, rehabilitation, ache administration, and pharmacology. Advances within the fields of palliative care and immunotherapy have grown exponentially; the latter is particularly promising.
A FEW MORE CANINE RESOURCES
In my 5 earlier articles, I described the newest diagnostic instruments and remedies for the commonest canine cancers: mast cell tumors (July 2019), osteosarcoma (August), lymphoma (September), melanoma (October), and hemangiosarcoma (November).
There are myriad sources accessible to be taught extra about canine most cancers – the above-mentioned sorts and others that we’ve not written about – and this info, just like the illness itself, is continually altering.
If your dog (like my two Border Collies) is identified with an unusual sort, an web search will carry up a large number of outcomes; do analysis however be discerning in your method. Look for respected sources and scientific help for any claims. Many veterinary schools and specialty clinics have web sites with sections for pet house owners to be taught extra about numerous illnesses and remedies; these are credible sources for info. Below, you’ll discover some extra beginning factors for dependable info.
Veterinary oncology specialists. While an skilled common veterinary practitioner who has a particular curiosity in canine most cancers will probably be an enormous asset to you, I can’t advocate it strongly sufficient that you just search out assist from a board-certified veterinary oncologist.
These specialists have obtained in depth oncology coaching after veterinary college, handed examinations, and accomplished publication necessities to obtain certification by the American College of Veterinary Internal Medicine (ACVIM). When they grow to be licensed in oncology by the ACVIM, they are going to add the letters DACVIM after their names (the “D” is for Diplomate).
You can use a function on the ACVIM web site to seek for board-certified veterinary specialists (find.vetspecialists.com). If there aren’t any oncology specialists in your space, your veterinarian ought to have the ability to seek the advice of with specialists situated farther afield to develop an acceptable therapy plan in your dog.
Clinical Trials. In order to enhance detection and therapy of illness, essentially the most promising experimental or investigational therapies should be examined in scientific trials. The security and efficacy of those therapies and procedures have usually been evaluated first in laboratory animals and the remedy is taken into account to be of potential profit to the affected person. Your dog could or could not profit from participation in a scientific trial, however these research advance veterinary science and have the potential to enhance the outcomes of future generations of canines.
The American Veterinary Medical Association (AVMA) maintains the AVMA Animal Health Studies Database, which supplies info on veterinary scientific trials reported by researchers. Searches for related research may be achieved utilizing the parameters of analysis, location, species, and discipline of veterinary medication (equivalent to oncology). See ebusiness.avma.org/aahsd/study_search.aspx.
The American Kennel Club Canine Health Foundation funds scientific analysis with the aim of bettering the well being of canines. For a hyperlink to the trials they fund, see akcchf.org/research/participate-in-research/clinical-trials.html.
In addition, the Veterinary Cancer Society web site maintains a web page with hyperlinks to lots of the organizations that provide veterinary scientific trials. See vetcancersociety.org/pet-owners/clinical-trials/.
Books. There are a variety of books which might be very useful for advancing your understanding of canine most cancers. My favorites are:
The Dog Cancer Survival Guide, by Demian Dressler, DVM, with Susan Ettinger, DVM, DACVIM Oncology (Maui Media, 2011). A complete information for sensible, evidence-based approaches to canine cancers, together with standard, integrative, and various therapy choices, supportive care, monetary issues, and sources to assist house owners optimize lifespan and high quality of life.
Speaking for Spot: Be the Advocate Your Dog Needs to Live a Happy, Healthy, Longer Life, by Nancy Kay, DVM (Trafalgar Square Books, 2008). An invaluable useful resource for pet house owners to assist navigate veterinary care and choices.
The Emperor of All Maladies: A Biography of Cancer, by Siddhartha Mukherjee (Scribner, 2010). The quintessential guide about most cancers – its historical past, discoveries, setbacks, remedies, and hopes for the long run.
The First Cell and the Human Costs of Pursuing Cancer to the Last, by Azra Raza (Hatchette Book Group, 2019). An exploration of the most cancers “industry” and a name for change in analysis and therapy.
Websites. There isn’t any scarcity of websites with details about canine most cancers. The record of websites with up-to-date, credible, comprehensible info is shorter. These are just a few of my advisable sources of data for pet house owners.
drsuecancervet.com and facebook.com/DrSueCancerVet. Dr. Sue Ettinger is a practising veterinarian and board-certified most cancers specialist, worldwide speaker, guide creator, and vlogger (video blogger). Her info is up-to-date and extraordinarily accessible.
dogcancerblog.com. An amazing useful resource masking all the pieces from the newest in most cancers information to sources to complete articles, that includes Dr. Demian Dressler and Dr. Susan Ettinger, authors of The Dog Cancer Survival Guide.
morrisanimalfoundation.org. The Morris Animal Foundation bridges science and sources to advance the well being of animals. The basis is on the forefront of funding most cancers research in canines, together with the Golden Retriever Lifetime Study, one of many largest, most complete potential canine well being research within the United States. The research’s goal is to establish the dietary, environmental, way of life, and genetic danger components for most cancers and different illnesses in canines.
ccr.cancer.gov/Comparative-Oncology-Program. The Center for Cancer Research is a division of the National Cancer Institute underneath the National Institutes of Health. In 2003, the Comparative Oncology Program was launched to assist analysis in furthering the understanding of most cancers and bettering the evaluation of remedies for people by treating companion animals. Comparative oncology is the research of naturally growing cancers in animals as fashions for human illness. Through these trials, pets achieve entry to leading edge analysis and therapeutics; the outcomes then help the additional improvement of human scientific trials. The website additionally supplies illness info, hyperlinks to scientific trials, information, and publications.
wearethecure.org/tag/pet-cancer/. This website has a “Canine Cancer Library” that gives detailed info on an ever-expanding record of sorts of cancers. The Foundation’s weblog presents newest canine most cancers information and associated tales.
merckvetmanual.com/special-pet-topics/cancer-and-tumors. General veterinary details about most cancers in pets.
scholar.google.com. An easy-to-use free search engine that accesses the total textual content or metadata of scholarly literature throughout an array of publishing codecs and disciplines; an excellent useful resource to search for revealed analysis on canine cancers.
HOLISTIC (INTEGRATIVE) VETERINARY CARE
In all of the articles about canine most cancers revealed right here, I by no means had a chance to debate holistic take care of canines present process therapy for most cancers. It’s an enormous matter, and one I hope to jot down about in a future challenge.
The creator’s Border Collie, Daisy, asking to play Frisbee instantly after certainly one of her chemotherapy therapy.
Holistic veterinarians embrace a broad method to care, not solely analyzing the affected person, but in addition the affected person’s setting, conduct, relationships, and illness patterns. Veterinarians who self-identify as holistic, integrative, or complementary could have quite a lot of academic experiences and coaching; they could increase their standard veterinary medication with chiropractic, acupuncture, herbs, and/or different modalities. Their therapy protocols, then, will rely on their schooling, coaching, and expertise.
Note: Veterinarians who establish as providing “alternative” medication won’t use standard veterinary medication or collaborate with standard veterinary practitioners. Make positive you might be clear about what they do and don’t provide.
My main veterinarian is a holistic practitioner and was a worthwhile member of Daisy’s staff. Throughout Daisy’s sickness, he supported her with acupuncture, low stage mild remedy, vitamin, and medicinal herbs. He labored carefully along with her oncologist to make sure protected and helpful integrative care. Complementary therapies may be of nice profit to pets with most cancers, and holistic veterinarians can assist create these personalised help plans.
To find a holistic veterinarian close to you, go to the web site of the American Holistic Veterinary Medical Association, a gaggle of member veterinarians and allies who’re elevating the veterinary career by way of innovation, schooling, and advocacy of integrative medication. Go to ahvma.org/find-a-holistic-veterinarian.
FINANCIAL ASSISTANCE
One final useful resource – an vital one. Most most cancers remedies for canines are costly, as are the diagnostics and supportive care. I used to be lucky; on the time when my canines have been stricken, I had the funds to deal with each of my canines. I don’t have these monetary sources now, however I do have pet insurance coverage for my present canines.
If you have got neither the funds nor pet insurance coverage, there are a selection of economic sources accessible for canines with most cancers; the Humane Society of the United States retains a present record of nationwide and state-specific pet monetary support organizations on the following web page: humanesociety.org/sources/are-you-having-trouble-affording-your-pet.
AGAIN: IT’S PERSONAL
The determination to deal with (or not deal with) a pet for most cancers is a private determination; there isn’t a proper or mistaken method. Cancers are a gaggle of very difficult and various illnesses with every oncology case being medically distinctive. I opted to deal with each of my canines and I used to be lucky to have gained extra time with them. More time to eat ice cream collectively. To play ball and Frisbee. To cuddle on the couch. To share synchronized respiratory whereas falling asleep collectively. To dream collectively. Every second is a present.
!function(f,b,e,v,n,t,s) {if(f.fbq)return;n=f.fbq=function(){n.callMethod? n.callMethod.apply(n,arguments):n.queue.push(arguments)}; if(!f._fbq)f._fbq=n;n.push=n;n.loaded=!0;n.version='2.0'; n.queue=[];t=b.createElement(e);t.async=!0; t.src=v;s=b.getElementsByTagName(e)[0]; s.parentNode.insertBefore(t,s)}(window, document,'script', 'https://connect.facebook.net/en_US/fbevents.js'); fbq('init', '100131297051026'); fbq('track', 'PageView');
Source link
source https://pawnews24.com/canine-cancer-resources-and-hope/
0 notes
Text
JuniperPublishers-Spermatogonial Stem Cell Technology and Regenerative Medicine
Abstract
The biologic activities of spermatogonial stem cells (SSCs) are the base for spermatogenesis and thus sustained male fertility. Therefore, comprehending the mechanisms governing their ability to both self‐ renew and differentiate is necessary. Moreover, because SSCs are the just adult stem cell to contribute genetic information to the next generation, they are a good target for genetic change. Some researchers have reported the derivation of multipotent cells from mouse and human spermatogonial stem cells. These spermatogonial stem cells demonstrate similarities with embryonic stem cells for phenotype and functionality, showing that these cells may be a promising alternative origin for stem-cell based therapies in regenerative medicine.
Keywords: Spermatogonial stem cell; Regenerative medicine; Transplantation
Go to
Introduction
Spermatogonial stem cell
Germ cell development begins with the characteristics of the primordial germ cells (PGCs) early in human fetal life. PGCs arise from the proximal epiblast and will replace to the extra embryonic mesoderm during the fourth and fifth week of embryonic development. By the finish of the fifth week to early sixth week, PGCs will embark for a second immigration via the dorsal mesenterium of the gut to the gonadal ridge. During their immigration, PGCs proliferate but once they has arrived the gonadal ridge, they enter into a mitotic arrest while differentiating into gonocytes. Shortly after birth these gonocytes put on the basal membrane of the seminiferous tubules where mitosis is reinitiated. From then on, they are called spermatogonial stem cells or SSCs [1]. Spermatogonial stem cells (SSCs) are a subpopulation of unspecialized stem cells that lie along the basement membrane of the seminiferous tubules of the testis and give rise to the germ line lineage in males. In the adult testis, only 0.03% of all germ cells are spermatogonial stem cells [2]. Testicular SSCs are typically unipotent and are only capable of giving rise to the germ cell lineage and ultimately spermatozoa.
This ability of SSCs, the only adult stem cell population that transmits genetic information to the next generation [3- 5], to generate spermatozoa is critically dependent on the micro environment or niche that surrounds these cells [6-10]. Daily, 45-207 million spermatids are generated in the normal adult testis. This coining of germ cells is not regulated by the stem cells themselves but by the microenvironment environs the stem cells, i.e. the stem cell ‘‘niche’’. The niche is described as ‘‘the microenvironment around stem cells that provides support and generates signals regulating self-renewal and differentiation’’ [11]. The niche can action on a stem cell through various mechanisms: niche cells can make straight contact with the stem cell, niche cells can disguise paracrine factors acting on the stem cell or intermediate cells can ‘‘communicate’’ among the niche and the stem cells. When removed from their normal stem cell niche and cultured in vitro, SSCs display a broader developmental potential than they normally manifest in vivo. This has led to interest in their potential suitability for human regenerative medicine.
Spermatogonial stem cells as a source for fertility restoration
Spermatogonial stem cell disservice is an important reason of male infertility. Stem cell loss can happen after chemo- and radiotherapy [12-15] or due to a genetic disease, e.g. 47, XXY Klinefelter’s syndrome or AZF deletion [16,17]. Because children do not have the feasibility to bank spermatozoa, the preservation and transplantation of SSCs may become an important and main strategy to treat reproductive stem cell loss disturbances. In the last decade, most of research has been done on human SSC protection and transplantation [18]. Spermatogonial stem cell transplantation was first presented in the mouse in 1994 by Brinster and Zimmermann [19]. Spermatogenesis could be reinitiated in infertile receiver mice after transplantation of testicular cell suspensions from fertile donors. Shortly later, this technology was done in other mammalian species, including primates [20-24]. Even the transplantation between various species was proven successful [25,26].
These results, particular those from primate studies, propose a possibility of banking and transplanting human spermatogonial stem cells to barricade sterility caused by SSC loss. In mice and rat, the efferent duct has been shown to be an affective site for reintroducing SSCs by injection. However, compared to mouse and rat testis, human testis are bigger than and more fibrous. Thus, the injection technique has to be rectified. By using excised human testis donated by orchidectomy patients, different injection sites have been checked: the seminiferous tubules, the rete testis, the epididymis and the deferent duct. Schlatt et al. [21] have demonstrated that ultrasound-guided intratesticular rete testis injection was the better and least invasive injection technique with maximal infusion efficiency for larger testis. Tagged cells could be found in tubules near to the rete testis but not in tubules far away the rete testis. Brook et al. [27] evaluated the performance of single and multiple injections through the rete testis of isolated human testis.
Nevertheless, the hole into the testis was not monitored and it was unclear whether the injected hue had been injected in the seminiferous tubules or in the interstitial tissue or both. If spermatogonial stem cell transplantation has been demonstrated to be a successful procedure to produce live offspring in a mouse model [28], genetic and epigenetic changes due to the procedure should be taken into attention. Goossens et al. [29,30] observed that after in vivo and in vitro conception, transplanted males generated smaller litter sizes compared to normal fertile control mouse. However, the offspring demonstrated normal karyotypes and methylation patterns [31,32]. In another study, a detailed analysis of the motility kinematics and attentions of spermatozoa acquired after transplantation was performed demonstrating a less sperm concentration and sperm motility after transplantation [33]. The latter results may explain the reduced litter size as watched in the in vivo mating studies.
Taking into account the significance of the spermatogonial stem niche in spermatogenesis, grafting testicular tissue may be another to obtain functional sperm that is able to fertilize oocytes. In rodents and rabbits, perfect spermatogenesis has been seen and fertile offspring could be acquired through assisted reproductive techniques after grafting immature testicular tissue [34,35]. Grafting testicular tissue of human, however, did not produce spermatozoa. In prepubertal xenografts, this period was even lengthy (9 months) [36]. Lately, differentiation up to primary spermatocytes and the attendance of a few secondary spermatocytes was showed in testicular tissue from a peripubertal boy after xenotransplantation to mouse [37].
Spermatogonial stem cells as pluripotent cells
Newly, the pluripotency of SSCs from neonatal and adult mouse testis has been reported by various research teams. Kanatsu-Shinohara et al. [38] demonstrated the derivation of ES-like cells from neonatal mouse testis in culture. In their researches, ES-like cells were shown to be phenotypically alike to embryonic stem cells and to have the ability to differentiate in vitro into different types of somatic cells and to generate teratomas after injection into nude mice. In addition to, these ES-like cells formed germ line chimeras when injected into blastocysts, which proves the pluripotency of the spermatogonial stem cells derived from neonatal testis.
Afterwards, Guan et al. [39] demonstrated that SSCs from adult mouse testis could produce multipotent cells in vitro that were able to differentiate into various cell types of all three germ layers and to produce teratoma in immune deficient mice. These multipotent adult germ line stem cells donated to the development of different organs after injection into blastocysts. Similar phenomena could be showed in human spermatogonial stem cells. Conrad et al. [40] created an ES-like cell line derived from spermatogonial stem cells of adult human testis. The cells acquired cellular and molecular characteristics of human embryonic stem cells, but additionally these germ line derived stem cells differentiated into different types of somatic cells of all three germ layers when grown under situations used to induce the differentiation of human embryonic stem cells.
Go to
Conclusion
Transplantation of SSCs may become a promising procedure to keep the fertility of prepubertal patients. Their testicular tissue could be removed and cryopreserved before treatment. After recuperation, the tissue/cells could be grafted or transplanted into the patient’s own testis and fortunately spermatogenesis will be reinitiated. For cancer patients, additional methods would be essential for the isolation of SSCs and the removal of malignant cells. Other future choice would be in vitro maturation of SSCs after isolation and malignant cell removal. By this means, functional spermatozoa could be derived from mouse SSCs [41]. These in vitro generated spermatozoa could be used to fertilize oocytes by assisted reproductive techniques. These above indicated strategies could also be appropriate for adult patients with non-obstructive azoospermia. After seclusion and in vitro maturation, SSCs from these donors may have the capacity to generate functional spermatozoa. Although, before using these methods in patients, more research is required.
Transplantation of SSCs may become a promising procedure to keep the fertility of prepubertal patients. Their testicular tissue could be removed and cryopreserved before treatment. After recuperation, the tissue/cells could be grafted or transplanted into the patient’s own testis and fortunately spermatogenesis will be reinitiated. For cancer patients, additional methods would be essential for the isolation of SSCs and the removal of malignant cells. Other future choice would be in vitro maturation of SSCs after isolation and malignant cell removal. By this means, functional spermatozoa could be derived from mouse SSCs [41]. These in vitro generated spermatozoa could be used to fertilize oocytes by assisted reproductive techniques. These above indicated strategies could also be appropriate for adult patients with non-obstructive azoospermia. After seclusion and in vitro maturation, SSCs from these donors may have the capacity to generate functional spermatozoa. Although, before using these methods in patients, more research is required.
A large part (about 1 g) of testicular biopsy includes less than 5 million cells with only 1500 being right stem cells. This is far from the number required for cell therapy besides mentioning the low de- and transdifferentiation rates. Therefore, an efficient procedure for SSC isolation and in vitro enlarging has to be developed. Several researches on the in vitro amplification of human adult SSCs has been reported [42]; an important challenge for any clinical application is to eschew the risk of teratoma formation after transplantation. The development of an effective induction protocol and the regulation of the recipient’s immunology system may be essential to remove the risk of teratoma formation. Although there is not yet an obvious clinical prospect for SSC-based cell therapy in the clinic, SSC banking may become an encouraging and applicable strategy in the future.
To read more articles in Journal of Surgery
Please Click on: https://juniperpublishers.com/oajs/index.php
For More Open Access Journals in Juniper Publishers
Click on: https://juniperpublishers.com/journals.php
0 notes
Text
Pulling The Trigger: How the Fluoroquinolones Can Cause Mutations and Disease: My Quin Story
New Post has been published on http://www.myquinstory.info/pulling-the-trigger-how-the-fluoroquinolones-can-cause-mutations-and-disease/
Pulling The Trigger: How the Fluoroquinolones Can Cause Mutations and Disease
Introduction
The fluoroquinolones (FQs) are metabolically invasive antibiotics that kill their targets effectively, both directly and indirectly. When something goes awry, and they indiscriminately target healthy human cells, they also damage both directly and indirectly.
By their very nature FQ’s do not need to remain in the body to do damage long term. In this brief article we will look at how they can cause mitochondrial disease or other disease processes by being an effective epigenetic trigger.
Background
Dr. Bruce Cohen
Dr. Bruce H Cohen, one of the foremost experts on mitochondrial (mito) disease when discussing mito cytopathy in adults, states that mito disease can be inherited or acquired. The cause for mito disease can be genetic mutations, acquired somatic mutations, or exposure to toxins, which includes prescription medication 1.
Dr. Cohen, also writes, in a bulletin that discusses Myths and Facts About Mitochondrial Cytopathies titled “Not Your Mother’s Mitochondrial Disease,” that mito’s become poorly functional as a consequence of, amongst other things, toxin exposure. He also states that mito mutations can become pathogenic because of a trigger, an epigenetic trigger 2. Let’s look at how the FQ’s can ‘pull the trigger’ on the disease process.
Misconceptions
Initially, let’s clear up some misconceptions. The first one is that mitochondrial diseases are maternally inherited. This is a myth that is based on old medical information. The truth is that most mito diseases are due to mutations in the nuclear DNA 2.
The second misconception is that you were predestined to have a mitochondrial disease due to flawed genetics. Again, this is incorrect. While it is true that a person can have a genetic predisposition to certain health traits or even diseases due to inherited disease gene variations, pharmaceuticals (toxins) can cause the genetic mutations that cause the disease process. Something I will discuss shortly. Anyway, to this day, this myth is perpetuated by many in the medical community and as a result they fail to see how the FQ’s can cause or initiate a mitochondrial pathology. Many doctors still see mito disease as being inherited from the mother and mainly affecting very sick children. By dismissing any other possibility, or probability, they throw the baby out with the bathwater.
Many years ago, I theorized that the fluoroquinolones (FQ’s) are an epigenetic trigger. Like a stack of dominoes falling over, or a snowball rolling down the hill, the FQ’s are the initiator, or in a nutshell, the substance that starts the ball rolling. In addition, we will see that the FQ’s both start the process plus give it a good push to get it going.
Recent Discoveries
New discoveries have proven what we have suspected for some time about the triggering process. Recently Vanderbilt University School of Medicine researched both mitochondrial DNA’s (mtDNA) and nuclear DNA’s (nDNA) interaction with oxidative stress (ROS) 3. Keep in mind that certain levels of oxidative stress are required for cellular function. However, if you create an over-abundance of ROS in the wrong sort of way it can lead to a whole host of serious metabolic problems than range from the mild to lethal in their scope.
In the Vanderbilt study, a toxin produced by ROS known as M1dG was looked at. The Vanderbilt team compared levels of M1dG generated by interactions between mtDNA and nDNA and ROS. A very important finding was discovered. This finding was that the interaction between mtDNA and ROS generated 50 to 100 times more M1dG than the interaction between nDNA and the ROS.
Why is this important you might ask? Well, let me explain. Like most things, M1dG in small amounts plays an important role in mito regulation and metabolism. However, if you bombard M1dG with excess oxidative stress it can form an adduct in mito DNA that causes mutation and disease. Not that mutations in nDNA cannot cause problems, they can, but nDNA has more robust repair mechanisms that mtDNA. This makes mtDNA much more susceptible to oxidative damage. In other words, oxidative stress cause an M1dG adducts to form in the mtDNA, this in turn created a mutation and triggered that mutation to change the fate of the cells that lead to a disease process.
If that went past you too fast, let me reiterate. The researchers were able in induce a mitochondrial disease by increasing ROS which in turn produced a toxin which mutated mtDNA and caused a disease process. An epigenetic trigger. The researchers found out that M1dG poses a danger because it can trigger genetic mutations, changing the fate of cells.
Enter the FQ’s
The researchers at Vanderbilt were not looking at antibiotics as the ROS generating mechanism but instead just looking at the M1dG DNA interaction after ROS was generated. However, in light of this research I will briefly look at the FQ’s.
I remembered from the recesses of my mind that certain antibiotics could also increase M1dG. Yep, you guessed it. The FQ’s induce toxic metabolic perturbations that lead to cellular damage 4. One way they do this by an enormous oxidative stress 5 which produces malondialdehyde and in turn M1dG 5 6. M1dG then has the propensity to mutate mtDNA which leads to a pathogenic process. This can lead to direct mitochondrial disease or create mutations that cause other pathogenic (disease) processes that are driven by the mitochondria.
Adducts
A quick note about adducts. A few years back there was a craze sweeping the FQ community that FQAD was solely caused by nDNA adducts. Adducts happen when a molecule breaks down and part of that molecule, a metabolite, adducts or connects itself to the DNA. Adducts can start pathogenic processes such as cancer and the like. Adduction is very complex, so I will keep this synopsis brief.
The M1dg adduct is not a direct metabolite of the FQ molecule. This nasty little mtDNA adduct is produced by ROS. The structure of the FQ molecule itself prevents adductions from forming ‘consistently’ across the FQ population. This is because of the tremendous variables involved in the metabolization of the FQ molecule. Dr. Noble, geneticist, oncologist, professor and researcher of pharmaceutical toxicity at the Univ. of Rochester, also holds to this opinion as well. Direct FQ adducts are randomly possible; however, this is also the case with many substances both natural and man-made. The FQ’s do their dirty work via multiple avenues both direct and indirect, which explains the wide variety of pathologies that are seen.
Scary Dangerous
Drug’s that can mutate DNA and create a disease process are scary. Why? Because they start the ball rolling on a pathology that can become chronic or lethal often appearing later down the road. After all, who would suspect the FQ’s as causing Alzheimer’s, Parkinson’s and other serious neurodegenerative diseases. The FDA implied exactly that very thing during their internal FDA pharmacovigilance review memo dated April 17, 2013 on the Fluoroquinolones, issued by the Food and Drug Administration’s Center for Drug Evaluation and Research, Office of Surveillance and Epidemiology. They point out that the method of damage caused by the FQ’s is mitochondrial toxicity which is also the underlying mechanism in neurodegenerative diseases such as Parkinson’s, Alzheimer’s, and ALS 7.
Remember, no one knows whether they are susceptible or not. Just because someone has supposedly had a safe course of FQ’s, the next time they might not be so lucky. Also, how do they not know they were damaged the first time around since genetic damage may not appear for some time after ingestion?
Conclusion
In the paper “Oxidative Stress Induced by Fluoroquinolones on Treatment for Complicated Urinary Tract Infections in Indian Patients” from 2011, the authors conclude “There was a considerable increase in lipid peroxide levels indicating an enormous oxidative stress. Caution to be taken for patients especially on Ciprofloxacin and Levofloxacin therapy.” This paper, like many others, sounds alarms about FQ usage that needs to be taken seriously.
The FQ are dangerous in their propensity to damage and never should be used haphazardly or without informed consent. This brief article outlines one way, albeit a very dangerous one, in which the FQ’s can trigger disease but please keep in mind that this is not the only way they can do their damage. I have already shown that FQ’s are chemotherapeutic (anti-tumor) pharmaceuticals that destroy via Topoisomerase interference just like chemotherapy (you can watch the short video here). There are many other ways in which they can interact with cells in a harmful fashion, from DNA to cellular substructures. In an upcoming article I will discuss what happens when this chemotherapeutic (anti-tumor) family of antibiotics interferes with Topoisomerase 2 (TOPO 2)in a novel way that I have never outlined before, causing TOPO2 to malfunction leading to cell death and senescence. Can you say premature aging?
0 notes
Text
Epigenetics And The Methods To Improve Through This
By Charles Stewart
There are countless people today who are fascinated with having a slimmer and sexier body. Since its often associated as a healthy thing, a lot of individuals are finding ways to achieve the ideal figure. Fortunately, there are methods which could bring good changes without any huge consequences.
Various programs and studies are found which could help develop ideal changes. The Epigenetics in particular, often concerns on studies pertaining to changes with regard to the organisms due to the modifications of gene expressions. Apparently, there are several options which could promote better health to a person. Check out some tips and advice below to help you understand more of this. Continue on reading the paragraphs below to learn more.
Be on the watch concerning your health. When your mind is filled with positive thoughts, chances are you can face and easily accept reality. You should be true to every word you say. Sometimes, the words we provide leave a good impact to our body. Instead of imposing negative thoughts, learn to speak positively and make yourself and anyone else to support you in the long run.
Study the history of family records. Its wise to study the ailments which run on your family. You can ask a reputable health provider to fill the necessary information. Alternatively, you could ask questions from your family members as well. Instead of unable to accept situation, consider the significance of talking with everyone else to everyone, so they could provide opinions.
Listen well to your body. It is one simple and practical way to raise your awareness on what is truly going on. Should you experience any issues or symptoms, pay close attention. Acknowledge the big possibility that there is a need for change. Allow yourself to fully express emotions properly and deal things appropriately. Attend your regular appointment with doctor to increase awareness.
Discover methods to avoid condition to worsen. This is just an ordinary concept. However, just few individuals acknowledge the essence of such idea. Even though its challenging to avoid the inevitable things, you should keep going and find out methods that can have a great impact to your life. Start absorbing plenty of ideas to make smart decisions smartly.
Do your research. With the vast information found online, there is always a way to discover some useful techniques and ideas. You could also borrow some printed resources and read. Asking questions from other people might help as well. As you can see, there are plenty of means of learn ideas. Have initiative to gather a good deal of information someday.
Seek experts for ideas. We simply know that experts could present the accurate, clearer and handy suggestions as well. As long you present the good deal of info, its easier and also simpler to figure out things which could change your decision in the long run.
Mentioned and explained above are key pointers that can help you accomplish a healthy and nice body. Be the type who make wise choices. There is a big difference when you come up with good and reasonable options apparently.
About the Author:
When you are looking for information about epigenetics, come to the web pages online today. More details are available at http://ift.tt/2xZlySd now.
http://ift.tt/2h8YpL1
0 notes
Last Seen Blogs

these-l0st-w0rds
These lost words don't talk to me anymore.

hanskenemer
hans

ekonomikafe
Ekonomi Blog

bnha-villain-redemption
Villain Redmeption

simonecuckold89
Sogno Cuckold