#It was this
Note
*faint human like silhouette on the edge of the crater*
I think my optic sensors are on the fritz again. Darn things are always breaking down. And when they break down, there's only me to fix those blasted things!
#fallout rp#dr mobius#old world blues#it was this#or screaming my head off#going AAAAAAAH WHAT THE FUCK IS THAT AAAAAAH#I’m sorry if I didnt go aaaah what the fuck anon if thats what you wanted#I don’t know how to react to some of these asks sometimes#oh well
4 notes
·
View notes
Text
Title: Never Til Now (Rolling Up The Welcome Mat)
Rating: M (for themes)
Warnings: n/a
Summary:
"Maybe there’s something about tangibility, about holding the real thing versus just the idea of it, but it cracks something open in him that hasn’t existed in a long time. Because all of a sudden, he can’t imagine not having this. Not getting to see Evan like this, every day. And it’s barely been thirty seconds."
-
In March 2025, with plans to propose, Tommy realizes Evan wants kids. the problem is, Tommy doesn't.
In November of the same year, in a happenstance exchange, he meets their baby girl.
(OR, we take a trip through a dual timeline in which the idea and reality of having kids drives Evan and Tommy apart, and then brings them back together.)
#remember when i said yall had no idea what was coming#it was this#bucktommy#fic#a03 fic#a03 writer#fanfic#tevan#kinley#firebeast#firepilot#firefly#the ally and the beast#i think i got all the hashtags#oops if i didn't
12 notes
·
View notes
Text
everyday I think about ctommy and ccrime while listening to Feast of Tongues by Los Capesinos and go a little more insane
0 notes
Text
You know, 'Sammy' is a chubby twelve year old. It's Sam, okay?
#sam winchester#Sorry it wasn't dad's on a Hunting trip and he hasn't been home in a few days for me#It was this#sam girl#Season 1 Sam#s01e01#jared padalecki#supernatural#spn
21 notes
·
View notes
Text
I really want to open up an Artfight hitlist for this year. But first off would people even want any traditional art attacks from me? And would it be weird if they got their attack mailed to them if I did so? I would only do traditional attacks if they approve to having it mailed. I'm also gonna send it to a couple of mutuals to see if it's fine.
#i forgot why i even opend up tumblr today and now i remember#it was this#marnie.txt#artfight#artfight hitlist#it will be on zoho forms not google forms because it sucks#anyway after this it's pretty much ready
1 note
·
View note
Text
Hi. I've started writing a semi-weekly TB Newsletter, if you're interested in that kind of thing. Here's the second letter--about public-private partnerships, leprosy, and my forthcoming big announcement about expanding access to tuberculosis care. You'll hear more about that on Thursday. Anyway, here's the newsletter. You can sign up here.
---
In advance of the Big Announcement this Thursday, I made a vlogbrothers video today on how we end TB–with the comprehensive care plan often known as S-T-P, which is short for “Search, Treat, and Prevent.” But one thing I didn’t discuss in that video is the downstream benefits of comprehensive TB care.
Once you’ve hired community health workers to screen for TB, it becomes much easier to screen for other illnesses like diabetes, high blood pressure, and non-TB lung issues (especially lung cancer). TB is notoriously a disease of vicious cycles–a disease of malnutrition that makes malnutrition worse, a disease of poverty that makes poverty worse, and so on–but addressing TB can be a story of virtuous cycles: TB survivors become TB advocates, as I’ve seen with my friend Henry in Sierra Leone. More effective TB treatment leads to less stigmatization of the disease, as communities come to see the disease as curable and survivable rather than terrifying and deadly. And better access to TB care leads to a stronger overall healthcare system, because more community health workers are better connected to more primary healthcare clinics, which allows communities to better address all kinds of health problems.
—
Mycobacterium tuberculosis is not the only bacteria of its family that causes a lot of human suffering; there is a closely related species called mycobacterium leprae that causes the disease known as Hansen's Disease, or more commonly leprosy. There are still around 200,000 cases of leprosy diagnosed each year around the world, and while the disease is curable, it also remains–especially if not caught and treated early–a significant driver of suffering and disability in our world.
There are many connections between TB and leprosy: Not only are the bacteria that cause these illnesses very similar, but patients have often expressed similarities in experience. TB patients who were encouraged or forced to live in sanitariums often compared themselves to lepers. One disheartening parallel between the diseases is that in both cases, those living with these illnesses are often abandoned by their families and must make new social connections within the new community of “leper” or “consumptive.” Also, both Hansen’s Disease and TB continue to exist largely because of systemic failures rather than due to a lack of knowledge or technology.
—
I really recommend Dr. Salmaan Keshavjee’s TED talk about how we ended TB in the U.S., and how we can end it using the same strategy around the world.
—
Last link from me today: I’ve been thinking a lot about the complex intersection between public and private investment (for reasons that will be clear on Thursday!) and I keep coming back to one infographic in an excellent paper (https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0256883) about the public money that was poured into the creation of the GeneXpert Machine, which can quickly and accurately test for TB. The GeneXpert machine has created a lot of profit for Danaher’s shareholders, and it has also created some societal benefit, but it could create a lot more societal benefit if it created less profit for Danaher’s shareholders. This tension seems to me one of the defining features of 21st century life. Anyway, here is the infographic:
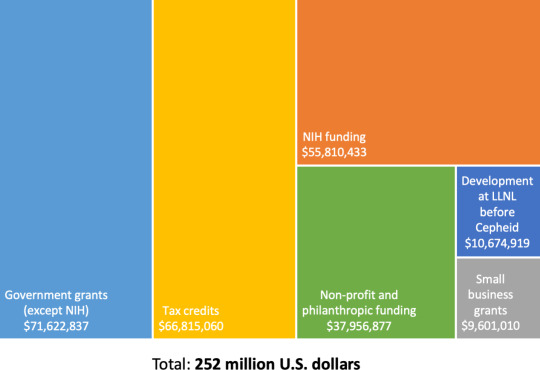
That’s the money–over $250,000,000 of it–that came from taxpayers (mostly in the U.S. and Europe) to fund the creation of the GeneXpert Machine. And yet, this tech largely funded by the public is controlled entirely by private enterprise. I’m troubled by that model of value allocation, even if I still believe that private money and private enterprise have important roles to play in fueling innovation. But taking a quarter billion dollars of public money and then claiming total ownership over a technology, and using that ownership to deny the technology to the world’s poorest people, seems like a deeply flawed system of resource distribution to me.
I’ll see you on Thursday. I’m nervous and excited.
DFTBA,
John
#tuberculosis#it's so funny how this became my job#not like my paying job but the one i do and think about all the time#like of all things#it was this#this is my hobby#anyway#beats jkr's horrible fucking hobby anyday
859 notes
·
View notes

Text
Not every day you encounter your local Tumblr microinfluencer
11 notes
·
View notes
Text

3 notes
·
View notes
Text


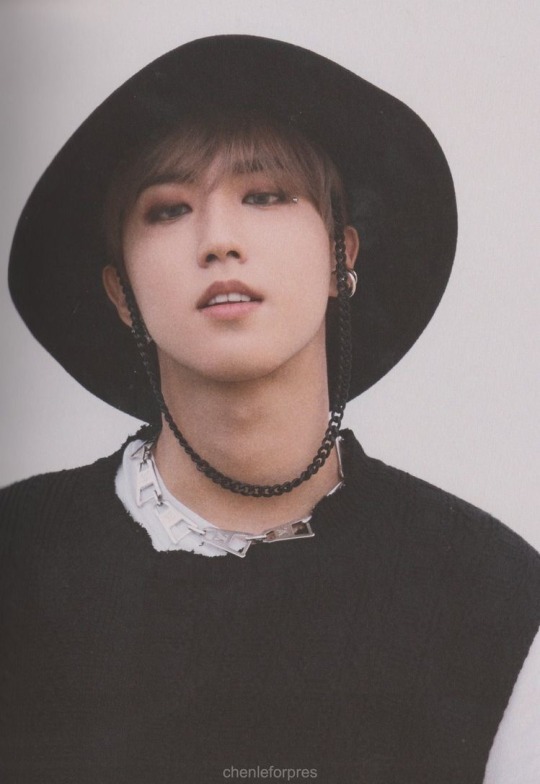
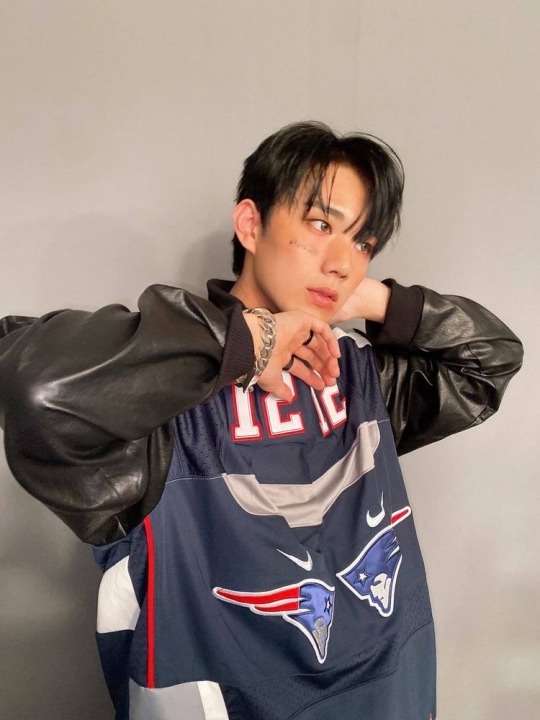
FACE CARDS UNMATCHED
#honestly they look stunning#I LOVE these boyfriend looks pls#dior if u did one thing right#it was this#thanks#mileapo#mile phakphum#apo nattawin#kinnporsche the series#man suang
105 notes
·
View notes
Text

Seiroku looking sadly at the times when he could slander an entire soul color. rip the red soul boorish brute comments. now he has to make an exception.
#dash commentary#seiroku just 'i cant believe he's done this...'#DHDJFG OUT OF EVERYTHING#THAT HE OCULD BE LIKE 'ICB SOMA DID THIS TO ME'#it was this
5 notes
·
View notes
Text
6 notes
·
View notes
Text
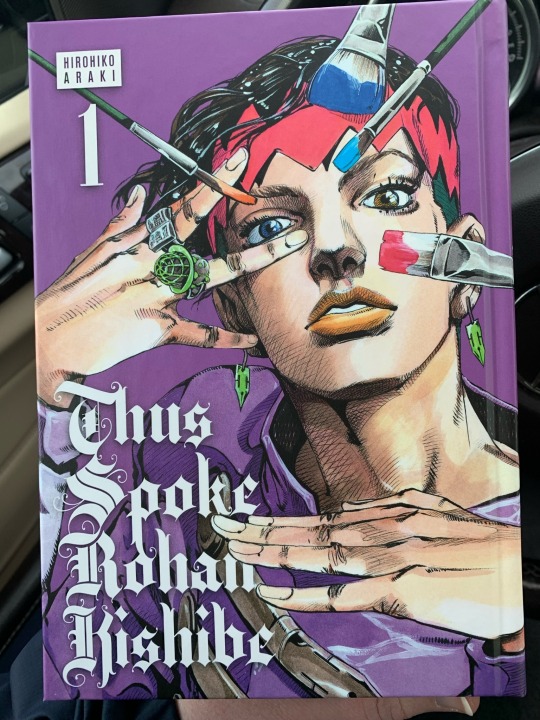
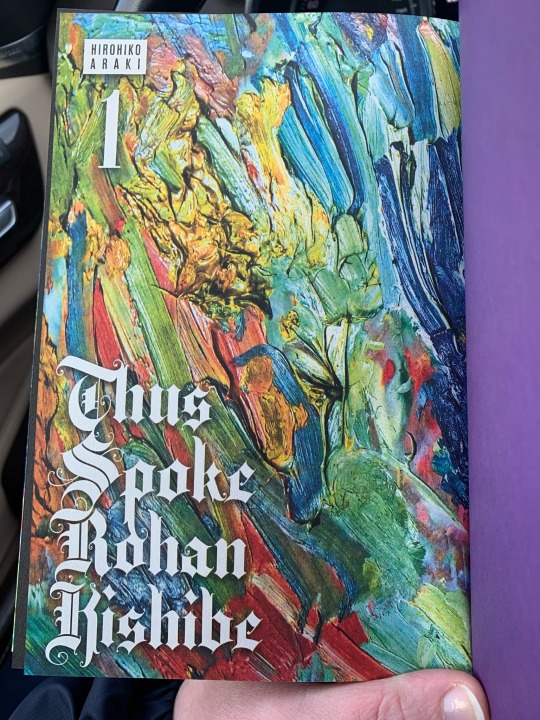

LOOK WHO HAS AN ENGLISH PRINT COPY FINALLY OF HIS SPINOFFS 🥴🥴💜💜💜 (Rohan my beloved)
#i thought i was picking up fujimoto’s#look back but#it was this#and i got flustered at the checkout#😳😳#and rambled to the checkout girl about how he’s my fav when she asked if it was a jojo spinoff#thus spoke kishibe rohan#jjba#rohan kishiBAE#rohan kishibe#tskr
6 notes
·
View notes



Text
jolene animatic with xiriel/dawn/vynara...
#i haven't thought abt them in forever but i had a brief. dream and#it was this#i miss them. dawn esp like ouhhh my dear ♡#jestersvaguely
4 notes
·
View notes
Text
i hav not know peace since this happened


3 notes
·
View notes
Last Seen Blogs

cedtheked17-blog
Untitled

chavatattoo-blog
#Chavatattoo

transowenharper
i'm dead already ;)

kokuarigourmet
GourmetFooDrinkPhotos

soraingtofreedom-blog
We'll never be Royals