#exstrophy
Text
The complete Guide to Bladder Exstrophy?
Definition: Bladder exstrophy is a rare congenital condition that affects the urinary system. It occurs when the bladder and the abdominal wall do not form properly during prenatal development. The bladder develops outside of the abdominal cavity, and it is exposed on the surface of the skin.
Diagnosis: This condition is typically diagnosed at birth. It can be diagnosed via prenatal ultrasound, but it is more often diagnosed after the baby is born. A physical examination is usually enough to confirm the diagnosis.
Treatment: Treatment for bladder exstrophy usually begins immediately after birth. The first step is to cover the exposed bladder with a sterile dressing to protect it from infection. Surgery is then typically required to repair the bladder and close the abdominal wall. Surgery can be done in one or multiple stages, depending on the severity of the condition. It is usually done between 3-6 months after birth. The goal of surgery is to achieve normal bladder function and a normal-appearing external genitalia.
Prognosis: The prognosis for bladder exstrophy varies depending on the severity of the condition and the success of the surgery. With proper treatment, most people with bladder exstrophy can lead normal lives with normal bladder function. However, some people may have ongoing issues with incontinence or recurrent infections.

In summary, Bladder exstrophy is a rare congenital condition that occurs when the bladder and the abdominal wall do not form properly. It is diagnosed at birth and treated with surgery. With proper treatment, most people with bladder exstrophy can lead normal lives with normal bladder function. However, some people may have ongoing issues with incontinence or recurrent infections.
#Bladder Exstrophy Epispadias Complex in Delhi#bladder exstrophy#bladder exstrophy treatment in Delhi#cloacal exstrophy
0 notes
Text

IN 1986, Sophie Ottaway was born with a very rare condition which required immediate surgery.
Cloacal exstrophy happens when the organs in the abdomen do not form correctly in the womb, resulting in babies born with organs such as the bladder or intestines outside the body.
Doctors had to operate to save her life.
Sophie was actually a boy, with a tiny, damaged penis but healthy testes.
But doctors advised Sophie’s parents that their baby’s male genitalia should be removed to avoid further complications.
The baby had to be registered by the following day, which meant they had to decide whether to tick male or female on the form.
Sophie’s parents Karen and John followed the surgeons’ advice.
“They were told not to tell me,” says Sophie, a warm and friendly 37-year-old who has since fully forgiven her parents for their decision.
“We are very close,” she tells me, “despite going through some rocky times in the past.”
Life changed for Sophie, who grew up in Beverley, East Yorks, when she was 22 years old and visiting her GP surgery for tonsilitis.
She says: “I saw on the computer screen that I had XY chromosomes, had been castrated hours after birth, and an incision was made where a vagina would be.”
Although Sophie exploded at her parents in the moment, she buried her feelings about it all until 13 years later when, hospitalised during a Covid lockdown, it was discovered she had developed sepsis that had ended up in her intestines.
‘I went into 13 years of absolute denial’
This was what led her to decide to speak out.
Sophie was already aware that many children and young people were being groomed in gender ideology, persuaded to take puberty blockers, then set on a medical pathway for life.
She says: “At age 11, as I approached puberty, they put me on oestrogen because there’s no ovaries, and no testes to produce testosterone.
“This is what doctors are doing now to kids who wish to change gender — putting them on blockers.”
It was a lie when Sophie was told she had to take oestrogen for life because her ovaries had been removed at birth as a result of damage.
Sophie was born biologically male. “So obviously there were never any ovaries,” she says wryly.
She adds: “The time to tell me and try to get informed consent was at the point we introduced the endocrinologist. This is the time puberty blockers are being offered to kids, so I make that connection with what’s happening today.”
When feminists and others critical of the medicalisation of children with gender dysphoria have said that these drugs and interventions are harmful, we are often labelled bigots. But Sophie is speaking from personal experience, in the hope that she will be listened to rather than dismissed and vilified.
About five years ago, Sophie chose to stop taking the hormones, because “I was adamant that many problems in my life were being caused by them.
“I was about 4st heavier than I am now, and I wasn’t eating badly. I was having bladder pain beyond belief.
“I had fatigue and was quite angry a lot of the time.”
By then, Sophie had been taking oestrogen for 20 years, and decided enough was enough. She was told she should keep taking it because it was for bone density, to which she replied that she would have regular bone scans.
Sophie had no choice but to go on oestrogen, because the doctors prescribed it to her as a child — but surely she should be listened to when she warns of the effects cross-sex hormones have on the body?
Now that she no longer takes it, all her symptoms have improved.
She says: “We’re selling this idea of perfection in the guise of changing gender. You’ve got all of these problems and might be struggling because you don’t fit in at school, or because you like boys’ toys and you’re a girl, or vice versa. As someone who knows all about decisions made under time pressure and who has paid the price, Sophie’s understanding of the sales pitch being made to children before puberty is crystal clear.
She says: “You’ve got a sale based on a time pressure.
“We’re going to push you through this for the puberty blockers, we’re going to make that sale.”
Keen to stress that there is a big difference between a girl behaving “like a boy”, wearing boys’ clothes and haircuts, Sophie adds: “Puberty blockers are a different level to how we dress and which toys we favour.”
The idea being sold is that gender reassignment is the answer to all your problems, but Sophie says: “What you get is genital mutilation, castration, and a lifetime of dangerous hormones, which was my experience.”
As she points out: “Children can’t vote, they can’t drink, can’t drive.
“But you can choose to do something life-changing.”
Sophie hopes that by speaking out and telling her unvarnished truth, some children — and parents — might make a different choice.
She says that when she found out that she’d been born male, “I obviously knew I had urological problems, and I knew that I had no vagina because of the surgeries.
“I didn’t address it at that point. I was 22, in second year at university.
“I had a plan of my life. And dealing with this monstrosity was not in the plan. I got up the next day and went to university.
“I still had the same connection with my friends. I was still the person I was 24 hours ago.
“But I went into 13 years of absolute denial.”
She never told anyone about it, not even close friends.
‘When I came out of hospital I was raging’
Then, during the pandemic, Sophie found herself in hospital a couple of times, and it all came crashing down.
She recalls: “They thought it was a kidney infection, but they couldn’t get to the bottom of it.
“When I was born they had fashioned some female genitalia. Brown putrid fluid starting leaking out of the hole and it would not stop.
“I presented at the hospital and I had to tell them for the first time about what had happened to me.”
When doctors examined her, they saw that there was something very wrong.
It turned out there was a mass in her abdomen, which was the neovagina — inserted when she was a baby — and left to rot.
Sophie says: “I found out from my mum that they had inserted it when I was two days old, and that one day it popped out and was found in my nappy.”
Surgeons replaced it during a later operation, sealed it up, and left it, which is why it led to sepsis many years later.
“No one had been told it had been put back in,” says Sophie.
Up until this point she had thought that the surgeon had simply operated to save her life — “which he did, but he also did a hell of a lot of other stuff that was unnecessary.”
What’s more, the doctors failed to do something that was necessary — namely, address the complex urological problems that have plagued Sophie all her life.
She says this “is one of the things that has the biggest effect on having any kind of intimate relationship. And yet the one thing that they could have fixed is my incontinence.”
She tells me: “When I came out of hospital, I was raging at that point.”
And she thought that by speaking out, she might be able to help those who think they are in the wrong body.
Sophie says: “A lot of them are being groomed to feel that way or question those thoughts in the first place by the school and the system and the media. Those kids need help.”
A much better solution, she argues, would be to divert funding currently being used for puberty blockers, cross sex hormones and surgery and allocate it to children’s mental health services and counselling.
Sophie says: “We can work with that person to find out why they are feeling like this.
“Then, maybe when they become an adult, they might be mature enough to be properly informed and consent to any changes to the outer body.
“It is often assumed I am transgender, but I really don’t like labels. I am just Sophie.
Poised for a backlash from the more extreme trans activists, Sophie makes it clear that she respects any adult’s decision to choose that path — so long as they are properly informed.
But she is clear that this is never appropriate for children.
“I don’t want this to happen to any other baby born with this condition,” she says.
“We have to find better ways to support kids to live in the body they are born with.”
Link | Archived Link
727 notes
·
View notes
Note
Hi I'm a former high school science teacher and now a doctor. While teaching, I was officially advised to explain that current understanding of gender is that it is complex and that sex is not necessarily the same as gender. I also got told not to mention intersex people outside of explaining that they exist, because tbh 14 year olds need to understand the normal stuff first.
I can also confirm that during medical school I was officially taught that "we refer to patients as male or female because man and woman are complex terms that do not adequately describe our patient population". We also did not use the term intersex at all, we generally referred to either "sex variants" or (in newborns/paediatric patients) we would refer to "disorders of" or "differences of sexual development" (DSDs).
There's not a hard and fast difference between "disorder" of sexual development or "difference", but generally it got called a disorder if it mandated surgical correction (e.g. vaginal agenesis, cloacal exstrophy, severe hypospadias, urethral atresia etc). If you didn't have to operate to prevent irreparable harm, it usually got called a "difference". We try not to recommend operations that aren't biologically necessary, but parents are currently permitted to request them and generally it'll be approved - though if I were the surgeon (which I'm not) I would probably request a different person perform it because I am not comfortable with unnecessary genital surgeries on unconsenting children.
Medicine currently recognises that sex and gender are not synonymous, that correlation is not causation, and that intersex conditions come in a wide variety of forms and functions. We also do not have a clear idea of whether something like hypospadias or imperforate hymen even COUNT as intersex disorders, even if they're definitely DSDs, and it's not very important because "intersex" isn't really a medical term.
Thank you so much for this perspective! I'm really happy, honored, and excited that I got the opinion of a doctor on this stuff.
I do have a couple of poorly articulated, rambly thoughts here, which I hope don't come off as criticizing you, because I'm just trying to build off of what you're saying and possibly get your perspective.
"male" and "female" are still interesting terms to me, and still have some of the same pitfalls as "man" and "woman". This is purely my own opinion, I don't want to falsely represent how scientists and doctors use them, but I personally use them more frequently as adjectives for individual parts of a body. Mostly, I do this to refer to myself. Because... Am I currently male, or female? I have a typical male height, male genitalia, but female physiology, female fat distribution, female hormonal systems, etc. It's hard for people to think of biological sex as dynamic and changing, but if you want to accurately describe me, that's what I am currently.
And yeah, you can totally use male and female to refer to individuals who dominantly have those male or female traits overall. But you have to be ready to get nuanced about it- which is exactly what you're doing here, which I appreciate.
It's also somewhat useful when referring casually to hermaphroditic organisms, although by that point you're probably just using more specific terms. I digress. I'm rambling.
I have a barely-relevant tangent here that I'm gonna put under the cut. There's an interesting parallel here between another linguistic quirk of terminology in genetics.
When a gene varies by a single base pair (eg, one of the As, Ts, Cs, or Gs is something else, or has been deleted or added), it can change the function of the gene. Sometimes, this is called a mutation- which, yes it is. Mutation implies a deviation from the general population, a distinct molecular event that happened which now exists in the gene pool in small numbers.
The trouble lies with assuming what the "default" form of the gene is. When gene A is say, 50% G at a certain location, and 50% T at that spot, it's called a SNP- single nucleotide polymorphism (often pronounced as "snip").
But what's the cutoff? 80-20? 95-5? 99-1? More extreme? What about SNPs
This is purely a linguistic thing, and in scientific contexts, people know what you're talking about based on the context around the words you use.
SNP as a term has p much been around for as long as genetics as a field. Within the field, I don't think anyone cares much, except as a discussion topic to get undergrads interested. However, I do think it's important for scientific communication- mutation has a much different connotation in people's minds than SNP, a term they may have never heard or feel neutrally about. The same can be applied to sex- the way we talk about male/female traits is extremely relevant to public perception. It's very similar to the terminology you're talking about here. And I'm really glad that medicine acknowledges that!!
In general, I think that these linguistic debates can seem trivial to professionals- but it dramatically affects public perception. There's whole other rambles here about how scientists and doctors generally don't know how to talk to non-scientists and non-doctors, but that's a whole other thing.
21 notes
·
View notes
Text
URGENT APPEAL‼
Feras Garboo is the older of a set of two year old twins. He was born with a rare defect called Bladder Exstrophy which means his bladder is on the outside of his body. He also has Epispadias which is a defect of the urethra.
He was treated for both of these at Saint Joseph's Hospital in East Jerusalem at about 11 months old however there were complications, the wound reopened and they had to go back in to fix that. Unfortunately the surgical team didn't have the experience with these particular conditions or the resources to really help Feras and despite best efforts made his condition worse.
*The above is a summary of what is explained in the campaign as well as what was explained to me by Feras' mother Israa. If you're going to look up these conditions to better understand fair warning for the images you might find. Also, there are images of Feras' state within the campaign but there is a warning before you scroll that far.*
Feras has multiple medical conditions including a heart defect as well. This baby has been suffering since birth, HE NEEDS TO BE TREATED OUTSIDE OF PALESTINE. And given the surgeries and reconstruction needed, treatment needs to happen while Feras is still young for the best chance of a decent quality of life.

IF IT'S EVEN A DOLLAR, IF YOU HAVE IT TO GIVE PLEASE GIVE!!
#gaza#urgent#urgent appeal#donations needed#gaza donations#gaza fundraiser#treatment needed#birth defects#children of gaza#save the children#please help#please donate#reblog#signal boost#please boost#donate if you can#go fund him#free gaza#palestine#free palestine#mutual aid#important#donations for gaza#gazan families#dont just like#please share
16 notes
·
View notes
Text

Ectopia of the heart: a - extrasternal form of ectopia of the heart, b - exstrophy of the heart.
20 notes
·
View notes
Text
Pediatric Urologist in India

What Is Pediatric Urology?
Children frequently suffer from Genito-urinary disorders. Infants are not able to comprehensively express the discomfort due to these disorders. In such a scenario, a trained and experienced pediatric urologist is required. Pediatric urologists are the doctors that diagnose and treat various Genito-urinary disorders in children.
The genito-urinary system includes ureter, kidney, bladder, and reproductive organs. It has been estimated that of all the disorders requiring surgery in children, almost 50% of them are associated with the Genito-urinary system. These disorders may include both congenital as well as acquired. A Pediatric urologist in India is an expert in handling the simple as well as complex cases of the Genito-urinary tract in infants and children.
How Pediatric Urology Is Different From Adult Urology?
Pediatric urology is quite different from adult urology. The symptoms of pediatric disorders are different from those of adult urology. Most of the urological disorders are congenital disorders and requires altogether a different treatment approach. Most of these problems can be managed with close observation and may not require any intervention. Pediatric surgeons are now well-equipped to precisely diagnose and manage various conditions without any surgery. Minimally invasive surgery also plays an important role in minimizing complications.
What Are The Various Pediatric Disorders?
Following are the various pediatric urological conditions:
Hypospadias : Hypospadias is the condition in which the opening of the urethra is not present on the tip of the penis. It is rather present on the underside of the penis.
Undescended testicles: Medically known as cryptorchidism, it is the condition in which either one or both the testicles failed to descend.
Vesicoureteral reflux: This condition involves the flowing of urine in the wrong direction.
Bladder exstrophy: When the bladder protrudes outside the abdominal wall, the condition is termed as bladder exstrophy.
Pelvic-ureteric junction obstruction: This condition is characterized by impairment in the flow of urine at the junction of pelvis and ureter.
Epispadias: When the urethra opens on the upper side of the penis, the condition is termed as epispadias.
Other conditions: Various other pediatric urological conditions include Testicular torsion, Ureterocoele, Horseshoe kidney, Duplex kidney, Ectopic ureters, and Absent kidney or renal agenesis.
What Are The General Symptoms Of Pediatric Disorders?
Symptoms of pediatric disorders are presented based on the type of Genito-urinary disorder. However, common symptoms include:
· Painful urination
· Fever
· Blood in urine
· Thin urine stream
· Abdominal pain
· Swelling in testis
· Urinary tract infection which may frequently recur
· Pus in urine
· Increased urine frequency.
0 notes
Text
Which hospital is best for paediatric surgery in Pune?
The Paediatric Surgery at CT Nursing Home Hospital, Pune Pune. We understand the special needs of children and are renowned for our unique surgical expertise and skills. We are committed to delivering compassionate family-centred care, conducting innovative medical research, and providing the best training to our surgeons.
Services
1. Neonatal surgery
2. Endoscopic surgery
3. Paediatric liver transplant
4. Paediatric urology surgery (bladder exstrophy, complex urological anomaly surgeries,
5. stone surgery, hypospadias)
6. Paediatric genitourinary surgery
7. Paediatric laparoscopic surgery
When choosing a hospital for paediatric surgery, there are several factors to consider. The most important factor is the qualifications and experience of the surgeons. Look for a hospital that employs board-certified paediatric surgeons with a proven track record of successful outcomes.
Pediatric surgeons commonly treat a variety of conditions, including congenital anomalies, pediatric cancers, traumatic injuries, gastrointestinal disorders, urological conditions, and Orthopaedic conditions. The Department of Paediatric Surgery provides surgical interventions for all childhood surgical diseases except that of the brain, bone and heart. It caters to children from 1 day up to 15 years of age. We provide comprehensive surgical care in emergencies which are ever-evolving and sometimes challenging. Minimally invasive procedures for select abdominal and thoracic conditions are performed with skill and finesse.
CT Nursing Home are among the best hospitals for pediatric surgery in Pune. Each hospital has a dedicated team of pediatric surgeons who specialize in various surgical procedures and equipment to ensure the best possible outcomes for young patients. Pediatric surgeons know how to make children feel comfortable and communicate with them. Pediatric surgeons are also involved in diagnosing conditions and caring for children before and after surgery. They may specialize in one of four main types of care:
Prenatal. Pediatric surgeons work with radiologists to spot problems while a child is in the womb and plan corrective surgeries after birth. Prenatal surgery, or an operation on a fetus, is a newer practice that is available at some of the larger medical centres.
Neonatal. Neonatal surgery involves the repair of congenital disabilities, or birth defects, in newborns.
Trauma. Trauma surgeries happen when a child has a moderate to severe injury such as a fracture, cut, burn, or internal injury.
Pediatric surgery is a sub-specialty of surgery involving the surgery of fetuses, infants, children, adolescents, and young adults.
👉Visit Here For More Info: 👉 https://ctnursinghome.in/pediatric-surgery/

#Best Paediatric Hospital Near Me#General Surgery Hospital in Dhanori#Sonography Services In Dhanori#Best Infertility Specialist In Dhanori
0 notes
Text
Find the Right Urologist for You at PACE Hospitals
PACE Hospitals is home to a team of highly skilled and experienced best urologists in Hyderabad India. Our urology department offers the latest advancements in diagnosis and treatment for a wide range of urological conditions affecting both men and women.
Our Expertise:
Kidney Stones: We offer minimally invasive procedures like laser and laparoscopy for efficient kidney stone removal.
Enlarged Prostate: Our urologists specialize in treating enlarged prostate using advanced techniques.
Urologic Cancers: We provide comprehensive care for urological cancers, including bladder cancer, kidney tumors, and prostate cancer.
Andrology: Our team offers treatment for male infertility and other urological issues specific to men.
Pediatric Urology: We diagnose and treat urological conditions in children, including undescended testicles and bedwetting.
And More: Our urologists manage a full spectrum of urological conditions, including urinary tract infections, chronic kidney disease, and more.

Top Urology Doctor in Hitech City and Madinaguda, Hyderabad
Dr. Vishwambhar Nath
MBBS, MS (General Surgery), DNB (Urology), M.Ch (Urology)
Senior Consultant Urologist & Renal Transplant Surgeon
Experience: 40+ Years
Dr Vishwambhar Nath is a senior urologist and transplant surgeon with 40 years experience in internationally famous hospitals in India and abroad.
He was previously Professor of Urology at CMC Hospital Vellore and Consultant Urologist, Cambridge University Teaching Hospitals, UK. His main areas of expertise and special interest include Prostate related urinary problems including BPH and Prostate Cancer, Urological Cancers with special interest in Bladder Cancer, Minimally Invasive treatments for Kidney Stones, Kidney Transplantation, Urological and Sexual Health of the Ageing Male, Postgraduate Teaching, and Ethics of Medical Care.
--------------------------------------------
Dr. Abhik Debnath
MBBS, MS (General Surgery - IMS, BHU), MCh (Urology - CMC Vellore), DNB (Urology)
Consultant Laparoscopic Urologist, Endourologist, Andrologist & Kidney Transplant Surgeon
Experience: 10+ Years
Dr. Abhik Debnath is working as Consultant Urologist & Renal Transplant Surgeon, having more than 10 years of experience in diagnosing and treating various urological conditions not limited to Urinary tract infections, Pelviureteric junction obstruction, Kidney stones, Bladder stones, Ureteral stones, Chronic kidney disease, Bladder infections, Enlarged prostate, Hydrocele, Overactive Bladder, Interstitial Cystitis, Haematuria, Sexually transmitted infections, Paediatric urological conditions (undescended testicles and bedwetting), Urethral stricture, Urofacial syndrome, Bladder exstrophy, Hydronephrosis, Cancer conditions (bladder cancer, kidney tumour, testicular cancer and prostate cancer), etc.
He is a gold medallist in physiology, and his work has won the titles of best paper, poster and video presentation at various conferences.
---------------------------------------------------------
Dr. K Ravichandra
MBBS, MS (General Surgery), MCh (Urology)
Consultant Laparoscopic Urologist, Andrologist & Kidney Transplant Surgeon
Dr. K Ravichandra is working as Consultant Laparoscopic Urologist, Andrologist & Kidney Transplant Surgeon, having more than 10 years of experience in diagnosing and treating various urological conditions not limited to Urinary tract infections, Kidney stones, Pelviureteric junction obstruction, Bladder stones, Ureteral stones, Bladder infections, Chronic kidney disease, Enlarged prostate, Overactive Bladder, Hydrocele, Interstitial Cystitis, Sexually transmitted infections, Haematuria, Urethral stricture, Bladder exstrophy, Hydronephrosis, Cancer conditions (bladder cancer, kidney tumour, testicular cancer and prostate cancer), etc.
Choosing the right urologist depends on your specific needs and preferences. Here are some factors to consider:
Urologist's area of expertise: Both Dr. Debnath and Dr. Ravichandra have a broad range of expertise, but you may have a particular condition requiring a specialist.
Experience and qualifications: Both doctors are highly qualified and experienced.
Patient reviews and satisfaction: Reading patient testimonials can provide valuable insights.
Schedule an Appointment Today:
PACE Hospitals is committed to providing exceptional urological care. To learn more about our urology services or schedule an appointment with one of our best urology doctor in hyderabad. contact PACE Hospitals today.
0 notes
Text

Is Your Child Facing Urological Challenges? Unveiling Causes, Types, and Risk Factors
Introduction:
As parents, we always strive to ensure the well-being of our children, addressing their needs and concerns with utmost care. However, when it comes to urological issues in children, many parents might feel uncertain or unaware of what signs to watch for and when to seek help. Understanding the causes, types, and risk factors associated with pediatric urological problems is crucial for early detection and effective management. In this article, we'll delve into these aspects, shedding light on the importance of awareness and the expertise of pediatric urologists like Dr. Abhijit Benare in Pune.
Understanding Pediatric Urological Issues:
Urological issues encompass a range of conditions affecting the urinary tract and genital organs in children. These conditions can manifest at any age, from infancy to adolescence, and may vary in severity. While some problems resolve on their own, others require medical intervention. It's essential for parents to be vigilant and proactive in recognizing potential signs of urological issues in their children.
Causes of Pediatric Urological Issues:
Congenital Anomalies: Many urological issues in children stem from congenital anomalies, meaning they are present at birth. These anomalies can affect various parts of the urinary tract, such as the kidneys, ureters, bladder, or urethra. Common congenital anomalies include vesicoureteral reflux (VUR), posterior urethral valves (PUV), and hydronephrosis.
Infections: Urinary tract infections (UTIs) are prevalent in children and can sometimes indicate an underlying urological problem. Recurrent or persistent UTIs may necessitate further evaluation by a pediatric urologist to rule out structural abnormalities or other underlying issues.
Functional Disorders: Some children may experience functional disorders of the urinary system, such as bladder dysfunction or voiding dysfunction. These disorders can lead to symptoms like urinary incontinence, urgency, or frequency, impacting a child's quality of life and requiring specialized management.
Types of Pediatric Urological Issues:
Hydronephrosis: This condition involves the swelling of one or both kidneys due to the backup of urine. It can occur as a result of blockages, reflux, or other structural abnormalities within the urinary tract.
Hypospadias: Hypospadias is a congenital condition where the opening of the urethra is located on the underside of the penis instead of the tip. Surgical correction may be necessary to restore normal urinary function and appearance.
Undescended Testicles: In some male infants, one or both testicles fail to descend into the scrotum from the abdomen. If left untreated, undescended testicles can lead to complications such as infertility and an increased risk of testicular cancer later in life.
Bladder Exstrophy: Bladder exstrophy is a rare congenital anomaly where the bladder protrudes through the abdominal wall. Surgical reconstruction is typically required to correct this condition and restore normal bladder function.
Ureteropelvic Junction (UPJ) Obstruction: UPJ obstruction occurs when there is a blockage at the point where the ureter connects to the kidney pelvis. This obstruction can lead to urinary stasis and potentially damage the kidney if not addressed promptly.
Risk Factors for Pediatric Urological Issues:
Family History: Children with a family history of urological issues may have a higher risk of developing similar conditions. Genetic factors can play a significant role in certain congenital anomalies and inherited disorders affecting the urinary tract.
Maternal Factors: Certain maternal factors, such as maternal age, smoking during pregnancy, or exposure to certain medications or toxins, may increase the risk of urological problems in offspring. Prenatal care and maternal health optimization are essential for reducing these risks.
Prematurity: Premature infants are more susceptible to urological issues due to the incomplete development of their organs and systems. Close monitoring and early intervention are crucial for addressing any urological concerns in preterm infants.
Previous Surgeries or Medical Conditions: Children who have undergone previous surgeries or have underlying medical conditions such as neurogenic bladder or spina bifida may be at higher risk for urological complications. Comprehensive medical history assessment is essential for identifying potential risk factors.
Conclusion:
Ensuring the optimal urological health of our children requires vigilance, awareness, and access to specialized care when needed. Dr. Abhijit Benare, a renowned pediatric urologist in Pune, possesses the expertise and dedication to address a wide range of pediatric urological issues with compassion and precision. By understanding the causes, types, and risk factors associated with these conditions, parents can play an active role in promoting their child's urological well-being and overall quality of life.
By prioritizing regular check-ups, prompt intervention when symptoms arise, and adherence to recommended treatment plans, parents can empower their children to lead healthy, fulfilling lives free from the burden of urological challenges.
Remember, early detection and intervention are key to ensuring the best possible outcomes for children with urological issues. Let's work together to safeguard our children's urological health and support them in reaching their full potential.
0 notes
Note
Hi this is the anon that was complaining about Mia Hughes summarized stuff. My issue is some of her writing in it(seemingly misrepresenting ejaculate in the bit you had a screenshot of, in the intro where Paul McHugh getting the John Hopkins gender clinic closed doesn't seem to bring up how Paul McHugh's intention to shut down the gender clinic was his motivation for getting at John Hopkins and the study used for justification was flawed (Meyer & Reter 1979, sex reassignment follow up, penalized trans people outside of straight relationships as well as those receiving therapy. Also, considering the ghoulish shit John Money did I don't think it is necessarily bad that clinic was closed. Finally, the citation about it closing is an article written by Paul McHugh who seems more to be influenced by right wing Christian views than evidence)) and that I think that a more neutral person in general should have done the writeup, because Mia Hughes has written under various names against trans care and would likely be deemed to be biased. I did see something which I think is silly by Erin Reed talking about issues with the wpath files editorialized section, and I do worry that because of criticism like that there will be less of a chance of people who are vulnerable (like a person with DID being asked for "informed consent" with all their alters, IMO they should not be allowed to get on HRT in that type of mental state) getting protection from bad medical care. Also, full disclosure, I don't know your view on if transition should be allowed in general, but I think for adults who have gone through enough therapy and don't have underlying conditions that could cause them to incorrectly think they are trans that transition is OK. Sorry this was so long.
No need to apologize for the length—I asked you to expand because I genuinely wanted to hear your thoughts. I understand where you were coming from with the screenshot now and agree the phrasing could have been less convoluted.
I'm assuming the citation you're referring to is Citation 33: "Surgical Sex." First Things, 2004. [AL] If so, the most immediate issue I took with Paul McHugh's article is that he seems to be conflating males who transition due to dysphoria with males who transition due to autogynephilia, even stating outright that the latter were the majority patients at the clinic at the time. This causes him to lose some credibility right off the bat in my eyes because a fetish does not equate to a mental health condition and the treatment protocols for them, ethically speaking, are entirely different.
The most pressing issue, overall, though, as you said, is the study he shares in his article to prove his point, as it does not pertain to neither dysphoric nor autogynephilic males, but males who were born with cloacal exstrophy; he shifts his focus halfway through. It is highly hypocritical to, in an exposé, cite an article that not only conflates dysphoric people to autogynephilics and people with genito-urinary disorders, but then also goes on to cite a study concerning a population that the average person seeking gender-affirmative care would not even be a part of. This is not even to mention that the studied population was extremely small—sixteen total, all male, only two of whom were not specifically raised as if they were the opposite sex—and the lack of proper study controls in transgender research is something that is criticized, multiple times, throughout the document. This insinuates, to me, that Mia Hughes has either not done enough careful research of her sources to justify publishing the document at this time, or she is making the same false equivalences that McHugh has—which raises the question of what, exactly, she is criticizing and for which group of people. Either way, this all does, as you say... somewhat delegitimize what is being shared here (...and I say "somewhat" only because the points being made do hold merit, even if the delivery may leave something to be desired).
Well, regardless, in conclusion, I do, in theory, agree that neutrality is important when writing documents such as this one, although in practice, unfortunately, this is very rarely how it works out since most people, concerning most issues, naturally lean towards a "side" whether they have adequate information to choose that side or not. It's difficult to find neutral people when discussing such polarizing issues, especially when today's sociopolitical climate views everything in black-and-white. This is why reading with nuance and having discussions such as this one are so important in formulating our opinions. I haven't seen or read anything from Erin Reed yet, so I'll have to refrain from commenting on that for now—but thank you again for the message. You've given me a lot to take note of going forward with this thing.
1 note
·
View note
Video
youtube
Bladder Exstrophy | Masana Ki Kamzori ka Ilaj | Dr. Naseem Javed
0 notes
Text
Pediatric urologist in gurgaon
A pediatric urologist is a medical specialist who focuses on the diagnosis and treatment of urological conditions in children. Urology is a branch of medicine that deals with the urinary tract and male reproductive system.
Pediatric urologists have specialized training in both urology and pediatrics, which allows them to provide comprehensive care for infants, children, and adolescents with urological problems.

Pediatric urologist in gurgaon
They are skilled in managing a wide range of conditions, including but not limited to:
Urinary tract infections (UTIs): Infections of the kidneys, bladder, or other parts of the urinary system.
Congenital anomalies: Birth defects affecting the urinary tract, such as bladder exstrophy, hypospadias, or undescended testes.
Voiding dysfunction: Problems with urination, including bedwetting (enuresis) or daytime urinary incontinence.
Vesicoureteral reflux (VUR): The abnormal flow of urine from the bladder back up into the ureters and kidneys.
Kidney stones: Solid deposits that form in the kidneys and may cause pain and urinary issues.
Hydronephrosis: Swelling of the kidney due to a blockage or obstruction in the urinary tract.
Genital and reproductive conditions: Conditions such as phimosis, cryptorchidism, or intersex disorders.
Tumors and cancers: Diagnosis and treatment of tumors or cancers affecting the urinary system or reproductive organs.
Pediatric urologists work closely with other healthcare professionals, including pediatricians, nephrologists, radiologists, and surgeons, to provide comprehensive care for their young patients. They may use various diagnostic techniques, such as imaging studies, laboratory tests, and specialized procedures, to evaluate and manage urological conditions in children.
Treatment options can vary depending on the specific condition but may include medication, minimally invasive procedures, or surgery. Pediatric urologists aim to provide the best possible outcomes while ensuring the comfort and well-being of their young patients.
0 notes
Link

A little boy of age 3.6 years was admitted at the hospital for reconstruction of Exstrophy Bladder. This is one of the most complex congenital anomalies which involves various systems of the body at the same time. It takes into account the urinary system, the muscular and skeletal system and has various hernias. This surgery is usually performed in various stages but we at Chandan Hospital were able to perform this surgery in a single stage.
Dr. Sunil Kanojia, Paediatric Surgeon - Chandan Hospital has performed this surgery that lasted over 8 hours and included various other procedures like closing of the bladder, Bladder neck reconstruction, osteotomy of the pelvis bone, etc for effective results.
Consult our specialists from 9:00AM to 8:00PM!!
📞 Call: 0522-6666666 to book your appointments.
https://chandanhospital.in/
#StayHealthy #StaySafe #ChandanHospitalCares #ChandanHospital #MultiSpecialityHospital #Surgeon #BestSurgeons #Health #BestTreatment #Healthcare #BestHospitalInLucknow #Lucknow #BestHospitalInUttarPradesh
#ExtrophyBladder #SingleStage #UrinarySystem #CongenitalDisease #CongenitalAnamolies
0 notes
Photo
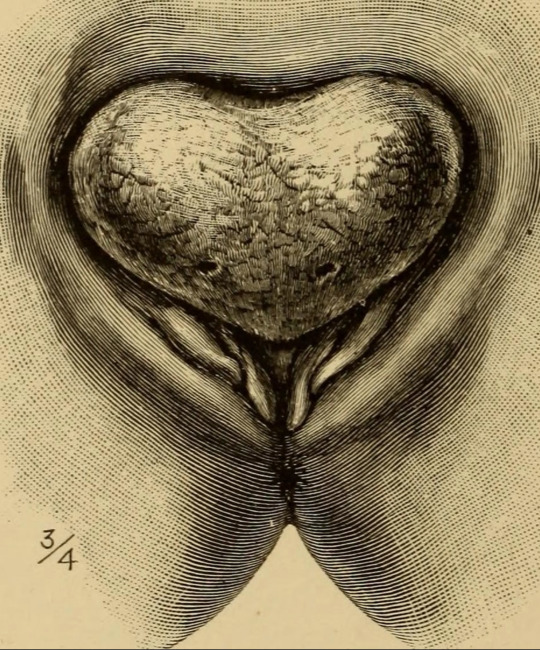
Some sex differences are genetic, like congenital adrenal hypersensitivity, congenital androgen insensitivity, and Smith-Lemli-Opitz Syndrome. However, not all sex differences are genetic: congenital absence of the vas deferens in boys with cystic fibrosis, bladder or cloacal exstrophy, aphallia, penoscrotal transposition, or isolated hypospadias.
Image of bladder exstrophy from "The diseases of women: a handbook for students and practitioners" (1897), p. 63. Courtesy of the Internet Archive.
1 note
·
View note
Link
UNDERSTANDING BLADDER EXSTROPHY
In addition to a bladder development abnormality, abnormalities also occur in the genitals and pelvic bones and the reproductive organs.
The genesis of the defect begins with the cloaca. This structure is the place where the reproductive, urinary, and digestive openings converge during development in the womb.
If bladder exstrophy occurs, this process hasn’t developed properly.
The bladder forms outside the body as a flat plate with bladder exstrophy. This can adversely affect and involve organs that are part of the urinary tract, as well as the reproductive and digestive systems.
Children may also experience a condition known as vesicoureteral reflux, meaning that urine travels in the wrong direction from the bladder back to the kidneys.
Another symptom of children with bladder exstrophy is epispadias. This means that the urethra is not fully developed.
1 note
·
View note
Text
Best Pediatric Urologist in Delhi - Dr. Prashant Jain

Are you seeking the utmost care and expertise for your child's urological needs in Delhi? Look no further! Delve into the realm of pediatric urologist in the capital city.
With a blend of advanced medical prowess, compassionate care, and a dedication to ensuring your child's well-being, Delhi's pediatric urologists stand out as beacons of excellence in the field.
Dr. Prashant Jain is the best pediatric urologists in Delhi and their exemplary skills and dedication to excellence are highlighted by his achievements as a gold medalist in both pediatric surgery and urology.his specialized expertise in pediatric urology and minimal invasive surgery indicates a keen focus on advanced and precise medical techniques for treating young patients. The opportunity to work at Great Ormond Street in London likely provided him with invaluable international experience and exposure to cutting-edge practices in his field.
With such a robust education, specialized training, and international exposure, it’s evident that Dr. Prashant Jain is a highly qualified and experienced professional in pediatric surgery and urology. His dedication to his field and continuous pursuit of knowledge and expertise make him a valuable asset to the medical community, particularly in the realm of pediatric care.
Dr. Prashant Jain’s accomplishments in the field of pediatric surgery and urology are truly remarkable. His success in performing reconstructive surgeries for congenital anomalies showcases his exceptional skills and dedication to improving the lives of young patients with complex medical conditions. Successfully treating previously failed cases of urological anomalies like hypospadias and bladder exstrophy speaks volumes about his expertise and innovative approaches.
Why Choose Delhi's Pediatric Urologists?
Expertise: Each of these specialists possesses extensive training and experience in pediatric urology, ensuring the highest standard of care for your child.
Compassionate Care: Beyond medical expertise, these doctors prioritize the emotional well-being of both children and parents, fostering a supportive environment throughout the treatment journey.
State-of-the-Art Facilities: Collaborating with leading hospitals and clinics in Delhi, these pediatric urologists have access to cutting-edge technology and facilities, facilitating precise diagnoses and effective treatments.
Continued Innovation: With a commitment to staying abreast of the latest advancements in pediatric urology, these specialists continuously refine their skills and techniques, offering innovative solutions for even the most challenging cases.
Take the First Step Towards Your Child's Health:
When it comes to your child's urological health, trust only the best. Best pediatric urologist in delhi with combine skill, compassion, and innovation to provide unparalleled care for your little ones. Take the first step towards ensuring your child's health and happiness by scheduling a consultation with one of these esteemed specialists today.
#best pediatric urologist in delhi#best pediatric surgeon in delhi#best pediatric urologist in india#Hypospadias surgery in delhi#Pediatric laparoscopic surgeon in delhi#best pediatric surgeon in india
1 note
·
View note
Last Seen Blogs

asstheticshitposts
What the fuck
sealsapocalypticmusic
Sealapocalyptic's Musical Apocalyptic Experience

taleasoldastxme
Where Dreams Come True

amen-music
Amen Music

agentahitiannonijuice
PROMO!!!, 0813-2800-2004, Tahitian
Noni Juice, Noni Juice, Harga