#iron chelates
Text
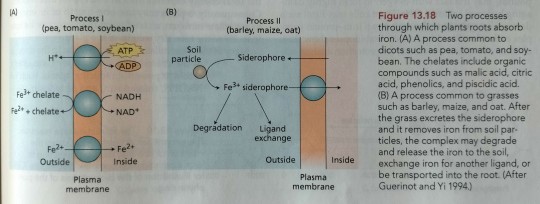
Roots use several mechanisms to absorb sufficient amounts of insoluble ferric iron (Fe³+) from the soil solution (Figure 13.18).
"Plant Physiology and Development" int'l 6e - Taiz, L., Zeiger, E., Møller, I.M., Murphy, A.
#book quote#plant physiology and development#nonfiction#textbook#pea#tomato#soybean#barley#maize#oat#iron absorption#chelation#iron chelates#malic acid#citric acid#phenolic#piscidic acid#siderophore#grasses#ferric#ferrous#plant cells
0 notes
Text
Iron Chelation Drug Market Overview, Competitive Analysis and Forecast 2031
#Iron Chelation Drug Market#Iron Chelation Drug Market Scope#Iron Chelation Drug Market Report#Iron Chelation Drug Market Research
0 notes
Text
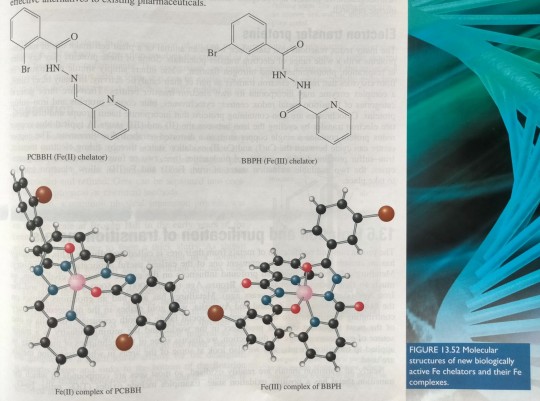
The two ligands in figure 13.52 (PCBBH and BBPH) appear similar but their Fe coordination chemistry is very different.
"Chemistry" 2e - Blackman, A., Bottle, S., Schmid, S., Mocerino, M., Wille, U.
#book quotes#chemistry#nonfiction#textbook#iron#chelate#ligand#transition metal#metal complex#pcbbh#bbph
0 notes
Photo

Deferasirox 500 Mg Dispersible Tablet Iron Chelating Agents
Deferasirox dispersible tablets should be taken without food according to the SmPC, therefore, one study under fasting conditions is sufficient.
Deferasirox Dispersible Tablets 500mg (Defrataj)
#Deferasirox 500 Mg Dispersible Tablet Iron Chelating Agents#Deferasirox Tablets#DEFERASIROX tablet for suspension#deferasirox 500 mg dispersible tablet#Deferasirox Dispersible Tablets 500mg (Defrataj)#DefraTaj
0 notes
Text
Introducing Ferrocytol: A Novel Iron Chelator to treat Anemia
Ferrocytol: Anemia, a condition characterized by low levels of hemoglobin or red blood cells, affects millions of people worldwide. Iron deficiency anemia (IDA), the most common type of anemia, often results from inadequate iron intake, malabsorption, or blood loss.
Photo by Karolina Grabowska on Pexels.com
Traditional iron supplements used to treat IDA can cause gastrointestinal side effects,…

View On WordPress
0 notes
Text
The global Iron Chelation Drug market size is estimated to be worth US$ 715 million in 2021 and is forecast to a readjusted size of US$ 430.7 million by 2030 with a CAGR of -6.9% during the forecast period 2022-2030.
0 notes
Text
How To Read Hair Care Ingredients
I have made a whole thread with all things you would need to know, if you want anymore information or have questions please dm me / comment / send an ask, hope you all enjoy ! ˚୨୧⋆。˚ ⋆
Shampoo Formulation Breakdown
Water
Primary Surfactant
- For cleaning and foaming
Secondary Surfactants
- For foam and/or viscosity enhancement
Foam Builders
- adds more lather
Conditioning Agents / Antistatio Detanglers
- Add shine, gloss & emollience
Chelating Agents
- Grab hold of iron, calcium or magnesium ions that are found in hard water
Solvents
- To clarify the product or to lower the cloud point
Opacifiers / Pearling Agents
- Cover up cloudiness or unattractive colors & add sheen
Viscosity Builders / Stabilizers / Thickeners
- Enhance the physical properties and stability
Buffering Agents
- To help balance PH level
Preservatives
- Keeps the shampoo from becoming rancid
Fragrances
- adds a pleasant scent
Surfactants
Here is a breakdown of what category some of the most common ingredients fall into.
Anionic Surfactants
(Primary Surfactants, Deep cleansing)
• Sodium Lauryl Sulfate
• Sodium Laureth Sulfate
• Sodium C14-16 Olefin Sulfonate
• Ammonium Lauryl Sulfate
• Ammonium Laureth Sulfate
• TEA-Lauryl Sulfate
• TEA-Laureth Sulfate
• Sodium Lauroy| Sarcosinate
• Disodium Laureth
Sulfosuccinate
• Sodium Lauryl Sulfoacetate
• Sodium Lauroyl Sarcosinate
• Sodium Cocoyl Isethionate
• Sodium Lauroy| Methyl |sethionate
Note : Can be stripping, but if the formula has conditioning ingredients it is offset. Cationic, nonionic, and amphoteric surfaces help with said offset.
Cationic Surfactants
( Secondary, Conditioning, Poor Cleansing)
• Behentrimonium Chioride
• Cetrimonium Chioride
• Stearalkonium Chloride
• Behentrimonium
Methosulfate
• Cetrimonium Bromide
. Benzalkonium Chloride
. Stearalkonium Chioride
• Dialkyl Ammonium Chioride
• Monoalkyl Ammonium
chloride
• Stearamidopropyl
Dimethylamine
Note : Good for damaged hair
Nonionic Surfactants
(Secondary, Conditioning, Poor Cleansing)
• Decyl Glucoside
• Lauryl Glucoside
• Coco Glucoside
• Cocamide DEA
• Cocamide MEA
• Polvsorbate 20
• Polysorbate 60
• Lauryl Polyglucose
Amphoteric Surfactants
(Secondary, Conditioning, Poor Cleansing)
• Coco Betaine
• Cocamidopropyl Betaine
• Cocoalkyl Betaine
• Cocoalkyl
• Amidopropyl
• Betaine
Foam Builders
(Builds Lather)
• Secondary Surfactants
• Cocamide DEA
• Lauramide DEA
Antistatic Detanglers
(Usually low concentrations of cationic surfactants)
• Behentrimonium Chloride
• Cetrimonium Chloride
• Stearalkonium Chloride
• Behentrimonium Methosulfate
• Cetrimonium Bromide
• Benzalkonium Chloride
• Stearalkonium Chloride
• Dialkyl Ammonium Chloride
• Monoalkyl Ammonium Chloride
• Stearamidopropyl
• Dimethylamine
Silicones
• Dimethicone
• Amodimethicone
• Cyclomethicone
• Cyclopentasiloxane
• PEG-12 Dimethicone
Fatty Alcohols
• Cette Alchol
• Stearyl Alcohol
• Glycol Distearate
Note: These are not drying, but conditioning
Oils + Butters
• coconut oil
• shea butter
• etc.
Chelating Agents
• Disodium EDTA
• Tetrasodium EDTA
• Sodium Citrate
• Sodium Phytate
• Sodium Gluconate
• Caprylhydroxamic Acid
• TrisodiumPhosphate
• Trisodium Ethylenediamine Disuccinate
Solvents
• Isoproyl Alcohol (Drying, but will not dry your hair out - safe to use)
• Benzyl Alcohol
• Propylene Glycol
• Butylene Glycol
• Glycol
Opacifiers / Pearling Agents
• Glycol Distearate
• Glycol Stearate
Viscosity Builders /Stabilizers / Thickeners
• Sodium Chloride
• Ammonium Chloride
• Acrylates Copolymer
• Glycol Distearate
• PEG-150 Distearate
• Magnesium Chloride
• Hydroxyethyl Cellulose
• Hydroxypropyl Methylcellulose
• Carbomer
• Acacia
• Carrageenan
• Guars
• Xanthan
• Silicates
Buffering Agents
• Citric Acid (Helps damaged hair - if higher on ingredient list)
• Sodium Hydroxide
• Sodium Citrate
Preservatives
• Parabens
• Chlorphenesin
• Potassium Sorbate
• Sodium Benzoate
• Benzoic Acid
• Sorbic Acid
• Dehydroacetic Acid
• Phenoxyethanol
• Methylisothiazolinone
• Methylchioroisothiazolinone
Fragrances
• Fragrance / Parfum
• Limonene
• Linglool
• Citronellol
• Lavender Extract
• Citrus Limon Extract
Coloring
• Ci 14700 (Red 4)
• C1 19140 (Yellow 5)
• Ci 61570 (Green 5)
• C1 15510 (Orange 4)
Simplified Summary :
When it comes to haircare, it truly does depend on each persons hair, no product is one fits all. If you like a product, and your scalp feels clean while your ends feel moisturized, continue use.
Healthy hair habits take priority over products. Keeping your scalp clean is number one, to do so depends on how often you wash. There is no right amount, it is okay to wash daily or weekly. If washing daily, use a shampoo that is lower in surfactants, aim for ones that say “okay for daily use”. If washing once a week, or twice, use one with higher surfactants (clarifying shampoo). If at any point your hair feels as if there is product buildup or the scalp is itchy use clarifying shampoo. number two is to condition frequently, you can condition before or after shampooing. It is helpful to pre-oil your hair 30 minutes prior to showering with coconut oil, coconut oil is the only oil proven to effectively enter the hair cuticle and can help protect against water damage. if you are going days without shampooing, spraying it with conditioning spray or oil on the shafts only is helpful. number three is small habits, dry your hair with a microfiber towel. keep shampoo only on the scalp and conditioner on the ends. squeeze out any excess water out prior to applying conditioner and let it sit for at least 2 minutes, longer if you can. use gentle hair ties and claw clips. put your hair in a protective style before bed. eat properly, get enough rest, and make sure you are hitting protein goals for biotin production. never brush your hair while it’s wet, and don’t over brush. use a leave in conditioner after washing, and avoid heat styling.
ingredients : shampoos and conditioners have a team of hair chemists formulating them carefully, so most haircare products are safe to use, but some are better based on added ingredients. ingredients like proteins, peptides, keratin, butters, oils, silicones, citric acid, glycerin, hyaluronic acid, lactic acid, and salicylic acid can improve hair. when choosing hair products, aim for ones that have these ingredients higher on the ingredient list
despite fear of silicones and sulfates, they are recommended by dermatologists and trichologists. the only ingredient you should avoid is formaldehyde. formaldehyde has different names, so avoid at all cost anything that says formaldehyde, methylene glycol, formalin, formic aldehyde, paraform, formol, formalin (methanol-free), FYDE, formalith, methanal, methyl aldehyde, methylene oxide, tetraoxymethalene, oxomethane, and oxymethylene. these are mainly found in special treatments and heat products, legally these can be called “formaldehyde free” if using it in a different form. (the ones listed above that are not verbatim “formaldehyde”)
affirmations
i love taking care of my hair, it’s so soft and fluffy. it never tangles and always is super shiny. it never breaks, my split ends always repair immediately. it grows so fast, inches every week. my hair smells so good and feels so bouncy ૮꒰ྀི⸝⸝> . <⸝⸝꒱ྀིა
#long hair#hair care#health and wellness#law of manifestation#sweet girly#self growth#pretty privilege#pink pilates princess#natural hair#hair products#femcel#girlblogger#y2k style#glow up#law of affirmation#princess aesthetic#subliminals#hair tips#coquette#coquette aesthetic#girly girl#pink aesthetic#waif aesthetic#hair study#dermatology#affirmations#self improvement#makeup#skincare#nails
37 notes
·
View notes
Text


highbush blueberries covered in flowers.. i love them theyre so funky and silly looking and it makes me rlly happy. theyre like little bells
tip for growing blueberries!!! everyone says they need like super duper acidic soil to grow, which they do like, but it's not 100% necessary. what they rlly need is chelated iron (plus some other nutrients but iron is the most important here) which most plants can get by breaking down the iron in the soil through their roots. blueberries are rlly well adapted to acidic soil - and as part of that adaptation theyve lost the ability to break down iron because they rely on acids in the soil to do it for them. There is another way they can get it tho!!! remember when i said other plants break down iron?? if the blueberries can form a mycorrhizal relationship (plant equivalent of mutual aid networks. using fungi. literally my fav thing) then the surrounding plants can give their iron to the blueberries :3 grasses are the best at doing this, especially if you cut the grass occasionally bc it makes the roots die back a bit and release all their nutrients into the soil around the blueberries. im sure it helps that mine are next to a lot of old oaks and poplars that probably have loads of nutrients and connections to the whole forest by now
some ppl try to use various chemicals to grow blueberries, which i get but its harmful to the soil and just rlly expensive and unnecessary... all u need is grass/trees and fungi :3 just take care of the soil!!!
theres a bunch of these scattered around the garden and every year when they bloom you can hear the bees from a few feet away - so many different kinds of bumblebees, honeybees, mason bees, and all the others that idk bc im not a bee expert :P they LOVE blueberries fr if you like bees and yummy snacks (especially if ur in their native range) these are like the best thing to plant
last year the berries all got infected with some kinda fungus right before they turned ripe 3:< hoping that doesnt happen again. if anyone knows how to keep them safe pls lmk :3
#blueberries#gardening#flowers#nature#plants#mycology#fungi#fruit#berries#native plants#ecology#bees#pollinators#spring
4 notes
·
View notes
Text
After the roots absorb iron cations or an iron chelate, they oxidize it to a ferric form and translocate much of it to the leaves as an electrostatic complex with citrate or nicotianamine.
"Plant Physiology and Development" int'l 6e - Taiz, L., Zeiger, E., Møller, I.M., Murphy, A.
#book quote#plant physiology and development#nonfiction#textbook#cations#iron#plant nutrition#chelation#iron chelate#oxidation#ferric iron#translocation#leaves#electrostatics#citrate#nicotianamine#nutrient absorption
0 notes
Text
https://facekindle.com/read-blog/211626_iron-chelation-drug-market-overview-competitive-analysis-and-forecast-2031.html

Iron Chelation Drug Market Overview, Competitive Analysis and Forecast 2031
#Iron Chelation Drug Market#Iron Chelation Drug Market Scope#Iron Chelation Drug Market Size#Iron Chelation Drug Market Report
0 notes
Text
Just thinking about the fic where Gymrat!Remus finally gets pointed to investigate a PCOS dx.
And med nerd brain just making me thinking about how RAMPANT it was for people to get treated for all manner of illnesses with bloodletting. Mr. Washington was already having a bad time with a throat infection - let's give the dude hypovolemic shock while we're at it! Pretty miserable way to die. :,D
Nowadays bloodletting has EXTREMELY limited therapeutic applications - mostly to treat shit like having too much copper or iron in the blood. (Though chelation is often used for shit like this, better risk/benefit profile, lbr.)
#sanders sides#remus sanders#virgil sanders#dukexiety#romantic dukexiety#qpp intruanalogical#(virgil's an entire himbo disaster in this fic - alright)#(and remus is such a disaster human)#(EMT just asking the question to test remus's level of lucidity/orientedness/consciousness)#(he's heard it all man)#(anyways - i'll find any excuse to gush about the trash goblin alright. he is a /delight/.)
2 notes
·
View notes
Text
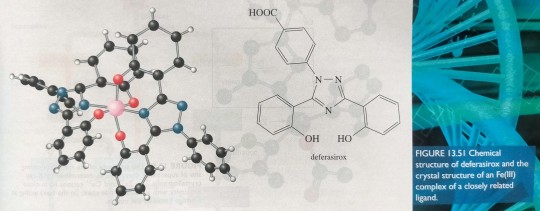
A recent breakthrough is the appearance of the drug deferasirox (figure 13.51), in this case a tridentate Fe chelator, which is taken orally once daily to control severe Fe overload.
"Chemistry" 2e - Blackman, A., Bottle, S., Schmid, S., Mocerino, M., Wille, U.
#book quotes#chemistry#nonfiction#textbook#iron#chelate#transition metal#metal complex#ligand#deferasirox#tridentate
0 notes
Text
Someone get me off this Iron Seesaw
Haemochromatosis: An inherited genetic condition where the body absorbs iron at a greater rate than normal, that if left untreated results in damage of organs such as the liver, heart, and pancreas.
It’s in my genes. It’s not going anywhere.
It’s something I’ve had to monitor, like a hawk, for the last 11 years. I spent parts of my uni degree diving into information and going to conferences to try and piece together what was going on, in a format that was easy for people (me) to consume. I’m not afraid to look up what the effects of iron on the brain are (oh what a mindfield that is), or to investigate what chelators are and who uses them (tl;dr: keep those things away from me).
At first it all seemed easy. Go to the blood bank once a month, have 500ml of blood taken. Get the iron down. As the iron comes down, reduce the frequency of visits. Easy.
Banned from the Blood Bank
One too many “Vasovagal syncope” episodes (fainting. Even though I never actually fainted, but that’s what’s gone down on my file) got me banned from the blood bank.
And it was terrifying. I was moving back home to the country, away from the city. Technically moving interstate, too, which I was reminded about the hard way when I needed to add a third medical professional into the mix because the hospital wouldn’t accept referrals from my city-based specialist in the other state. Even though technically, the hospital system is run by that state.
Yeah. You can see it coming too, right? That oncoming shitshow?
Buckle up.
A Country Practice
As it stands, I’m an anomaly in terms of Haemochromatosis. The usual suspects are middle aged or elderly men. Not a young women barely out of their teens. You typically see people track diagnoses down a family tree, not up it. It’s still sometimes referred to as a “men’s disease” because somehow apparently menstruating magically protects people from absorbing too much iron. (My ferritin of 618 at 18 years old would like to disagree with that assumption, so much)
So luckily, by the time I head back to the country - with our wonky as all getout “your rules don’t apply to us” border bubble health system - we’ve actually got it under control. The treatment phase, to reduce the iron, has been completed. We just need to work out what the best regime for maintenance of that is. In order to get blood taken - after being banned by the blood bank, of course - we need specific paperwork from a specific set of doctors. Physicians. Not to be confused with GPs, because that would be far too easy, wouldn’t it?
So we start the rounds of Physician roulette - which sounds more fun than it is, when there’s only 5 of them in 2015 and by the time one goes on maternity leave, another retires, and a third goes on indefinite medical leave, there’s not many options left after 2 years. (This also includes the infamous-to-people-who-know-me Dr “Oh you’re self medicating”, who refused to request certain tests and denied hospital referrals because the levels were ‘fine’ and I was ‘self medicating with periods anyway’. Colour me not surprised that when I got the call to tell me my appointment was cancelled because he was going on medical leave, that it was back to square 1 with the GP instead of passing patients onto someone else for ongoing care like my previous Physician did.)
And that’s just to get the referral papers - which once they’ve been filled in, I have to hand-deliver to the hospital. Just don’t take the first left down the stairs, that’s how you find out the cafeteria is right next to the morgue. The hospital staff at Campus A were amazing though, even though they took so long because nobody is allowed to start them. They without fail would run off to find a surgeon (this was the Day Surgery unit, after all) to actually start the procedure. Once it was started they were fine, but routinely they would have to run around for 30-45 minutes just to find someone to start it.
Keep in mind this is all well before COVID. This is 2015-2018. They’re struggling to start a simple venesection procedure in 2015.
The Australian health system was royally fucked from long before SARS2 decided to go for a joy ride around the world.
Hospital Switch
It feels like I’ve been to three hospitals but it’s only two - they moved the day surgery (read: squashed) into another part of the hospital at Campus A so they could do renovations. I think I got maybe one venesection in the New Surgery (which the nurses all complained about, it looks nice but apparently was less functional), before trying to book another venesection to be told “they don’t do them at Campus A anymore”.
By this point they have finally decided that they don’t actually need a specialists’ letter for venesections - you could still get one but it would only last you 3 months, while a letter from your GP would last 12. So we can cut out the extra $120/visit costs just to get paperwork from the specialists! Fucking hurrah!
But what we save in time, we lose in having to cross the river to get to the other hospital campus. There’s a new contact number to keep on hand. They actually give you a time to come in, rather than just a day. Campus W also seems to have slightly better food options - after all, I never got offered ice cream or jelly after my venesections at Campus A! (Although I haven’t been offered it since, but I did get a muffin once!). They’re also very strict on making you stay for half an hour once you’ve finished your procedure. And the nurses have, as far as I can tell from my 5 visits, ready to start the venesection at the drop of a hat.
Ring Ring, why won't you give me a call?
Unfortunately it’s not all smooth sailing; I’ve gotten to the point where my old GP would ask me what levels we were looking for. Where I’m practically calling the shots and just getting a sign-off that I’m allowed to do it. It’s kind of cool - it’s kind of scary.
My levels have started going up again - scarily so, considering I’d had a venesection between tests. So I’m urgently trying to get myself in for another venesection. I got the new referral letter on Monday afternoon, and tried to follow up with a phone call to the Clinical Liason Officer.
Answering machine.
So I leave a message, and decide to try again later. Maybe she was just at lunch.
Tuesday comes and goes with multiple calls to the officer’s number, and nothing but answering machine.
Wednesday I try to call while at work, in case I have more chances of catching them in the office before lunch time. Nothing, nothing, nothing. In the afternoon, I decide to try my luck on something I hadn’t tried for a while. Not since the change on the letter requirements.
It was time to check in with the blood bank, one more time.
Last time I’d tried this, I sat down with one of the nurses at the blood bank in a room. We had a talk. Said that it was possible, but I should get another couple of venesections under my belt. I’ve had at least that, if not more by this point.
But I don’t even get to speak to a nurse. Reception wants to send me to my GP to get put on the high ferritin app. ”I already am” I reiterated, ”I was a therapeutic donor. I wanted to try and get the ban lifted”. The tone changed slightly - out of their control, they said. Handed me an A6 card and wrote the national number I nearly called to see if I needed to book ahead to talk to someone, and told me to speak to a medical director because they had more power than the staff at the branch.
So at this point it’s where I mention that for the last 5 years, I’ve increasingly noticed that the closer my iron gets to 100, the more irritable and tetchy I get. (There’s some kind of extra spicy fuckery going on with cycle-related emotions too. It’s like a party of angry beans when there’s high iron and pre-period hormones. Nothing is safe - not even those keys, jumping out of my bag for no reason and falling on the floor. Especially those.)
I go home, angry and frustrated and rather upset (not even the allure of a food reward for going and asking the question worked - the brain collective said a hard “No.”), and despite it being 5pm, gave the line a call. After all, I’d wasted that half hour going into town, what was another half hour on the phone?
The first person I spoke to seemed nice enough. Checked my file, tried to tell me I was a therapeutic donor (strangely enough, I knew that. It’s the special program they have for people that need blood taken at different intervals, like haemochromatosis patients). Eventually explained that I was trying to see if we could lift the ban, since it had been 8 years and I’d had plenty of venesections since then without a problem. That was beyond her powers, but she was going to transfer me to a nurse.
Of course the “episodes” were one of the first things that were mentioned.
“It says here you had 4 episodes of Vasovagal syncopes in 2014**. What’s changed?”
I don’t know if it’s just because the wording caught me off guard, or if it was the shortness of “What’s changed”. It felt very much like “you’ve had fainting episodes. Nothing’s changed that. You can’t undo those. End of conversation”.
I mentioned that it had been 8 years. That I was barely in my 20’s when that happened. That I’m no longer in the city taking public transport, which was apparently an issue at the time, and that I’m driving myself to my appointments now with no issues. That I’ve had 5 venesections I’ve successfully taken myself to and from. (As of writing, 28 in total. 16 at the blood bank, and 12 at the hospital)
“You’re still a safety risk. You could faint while driving and cause an accident.”
It kind of feels like a kick in the guts - to be told despite all the work you’ve done over the last 8 years, of trying to do your best to get through venesections without any major mishaps, building little rituals around venesection day? That it’s not good enough. That none of it is good enough. That the pat on the back you’re giving yourself for being able to drive to and from a venesection is really being a “safety risk”. That hundreds of people drive themselves to the blood bank and back, but you are the one that’s a risk because of how you reacted 8 years ago (or more).
**BTW I’m 99% sure this claim of “4 Vasovagal syncopes in 2014” is False, actually.
November 2011: First blood donation ever. People *routinely* have a bad first donation because the body is freaking out. Mine just freaked out, went green, and took 4 hours to stop feeling light headed enough that I could go home (with friend who drove me and came as support). Is that REALLY a first strike against me?
- ??? I don’t know honestly. But chances are this was a dodo moment from me, where I unfortunately aligned procedural bleeding with monthly “self medicated” bleeding.
(& 4)- 2014 sometime: I remember these because it was the same nurse both times!! Once they put the needle in and then had to keep jiggling it around to get it to go, and I’m pretty sure that set me up for a poor reaction. The other time, they put the needle in and (vocally) observed that it was bleeding around the needle.
NOTE: none of these were episodes where I actually fainted. I got light headed, and the world span a bit, but I never passed out. Even my worse at the hospital didn’t knock me out (but oh boy it came close. And I know 100% that was because the tourniquet was too tight, and the rush of blood when they took it off is why my hearing went all funny and my vision was full of dots and the world spun really badly. But I know now to make a fuss if it’s too tight, if my arm goes red or purple, and not just ‘grin and bear it’.)
But that phrase sticks in my mind. “You’re a safety risk”. It’s probably going to sit there on the mental shelf, right next to “You’re self medicating”.
So the blood bank is - yet again - a write off. Maybe I’ll try again. Maybe I’ll get mad and make a list of all the ways I’ve improved with my approach to venesections. Or maybe I’ll give them away as a joke.
It’d be easier if they weren’t a nation-wide system.
Missing in Action
With the blood bank scrapped again from the options list, it brings me back to the hospital. Campus W. Chasing down Clinical Liason Officer. Because it’s the ONLY thing I could do at the time, I scan my referral and send an email. Just in case it’ll get a response. Thursday rolls around and still no dice from calling. Even the standard hospital number in the hopes that someone might be able to actually collar the officer and get a response, only gets me transferred to the same line that results in the answering machine.
So I grab my physical copy of the letter. Stuff my other notebooks with contact details into my bag, and choof over the river. Phones and emails hadn’t worked - but surely if I walked in there, someone would know something.
And they did.
Turns out the Clinical Lliason Officer is away. By the sounds of it, they’ve been away probably the whole time I’ve been trying to get in touch. There’s nobody filling their position while they’re gone. The hospital staff don’t know when she’ll be back. They hope it’ll be “Next Week”. There’s a side comment made about “if she isn’t back we’ll find someone to fill in that position”.
One person to book and schedule people for procedures across two campuses that serve close to 70,000 people.
And they don’t know when she’ll be back.
“If it’s pressing, you can go back to your GP to find an alternative or you can go to the ED”
This is just trying to book one single venesection. Just asking someone to take 500ml of blood. Something that’s an ongoing process and requires monitoring. It’s a regional city, but it’s not /rural/. We’re supposed to be a hub for other more rural towns. But I’ve lost track of the phone calls made, the time going to ask people questions. The time lost to being pushed back when trying to look at all my options. (Not that there are many of them).
It should not be this difficult.
#haemochromatosis#hemochromatosis#iron overload#iron loading#venesection#australian health system is buggeredddd#it should not be this hard to get blood taken#where's the vampires at I gotta offer to make my fanged friends
6 notes
·
View notes
Photo
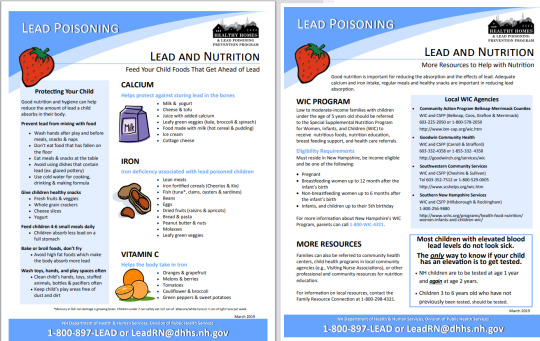
This is one of the handouts parents get if their kids have high lead levels. It's called "Lead and Nutrition."
In NH, children are screened for lead poisoning at ages 1 and 2 with the finger prick test. If the level is high, they need a blood draw to confirm the lead level (venous blood draw).
Parents should wet mop floors and windowsills, clean children's pacifiers and toys, wash kids's hands often.
Ask parents about behavioral problems, developmental delays/disabilities, excessive mouthing (putting keychains in mouth; items like that could have lead in them)/pica (eating non-nutritional items), whether housing was built prior to 1978, whether their child-care facility was built before 1978, whether their housing has renovations, whether the child is a recent refugee/immigration/international adoption, whether parents' job could expose them to lead (welding, renovating, painting, fishing, stain glass, target shooting, jewelry making), whether they imported any spices that could contain lead (turmeric, sindoor, surma, orange shringar, asafetida).
You need to do annual developmental surveillance and may refer for early childhood education/stimulation programs.
When you screen for lead in office with the finger prick, you have to wash the child's hands with soap and water first.
Symptoms of lead poisoning include stomach aches, headaches, trouble paying attention, developmental delays, behavior issues, problems eating and sleeping, speech/language delays.
Long term effects: slowed growth, poor school performance, hyperactivity, aggression, brain/kidney/nerve damage.
Home, water, and soil should be tested for lead.
Parents should feed children foods high in calcium, iron, and vitamin C.
Tx of high enough BLL: chelation with succimer of calcium disodium edetate. Succimer — Succimer (meso-2,3-dimercaptosuccinic acid) is a water-soluble analog of dimercaprol (British anti-Lewisite, BAL) that can be administered orally [48,49]. Like dimercaprol and CaNa2EDTA, succimer increases the urinary excretion of lead. Like dimercaprol, CaNa2EDTA increases the urinary excretion of lead through the formation of a nonionizing, soluble chelate.
Symptoms attributable to lead poisoning can include intermittent vomiting, anorexia, and abdominal pain (lead colic); intermittent irritability or lethargy; and/or lead encephalopathy (eg, persistent vomiting, persistent lethargy or coma, headache, or afebrile convulsions)
From UpToDate:
EMERGENCY MEDICINE (ADULT AND PEDIATRIC) (November 2021)
New threshold for elevated blood lead in United States children
●For children younger than six years of age in the United States, the reference value for an elevated blood level is 3.5 mcg/L (0.17 micromol/L).
Detectable blood lead levels (BLLs) are associated with neurocognitive deficits in infants and children less than 6 years old, and targeted screening of at-risk children is recommended. The Centers for Disease Control and Prevention has lowered the blood lead level (BLL) threshold for action to 3.5 mcg/dL (0.17 micromol/L) from the previous level of 5.0 mcg/dL (0.24 micromol/L) [1,2]. At or above this threshold, specific interventions should be taken based upon the degree of BLL elevation. For children with BLLs below 3.5 mcg/dL, the limit of detection for lead varies by laboratory, and the actual blood lead value may be close to or above the threshold. Thus, some children may need to be retested depending upon age or other risk factors.
With chronic ingestion or inhalation, lead can be incorporated into the skeletal system, which becomes an endogenous reservoir of lead that is resistant to elimination. While chelating agents can bind to lead in blood, they are ineffective in removing lead from the deep bone stores.
I had twin pts who both had EBLL of 5 mcg/dL in August and level of 4 mcg/dL today. One of them hadn't grown as much as her twin, so there was concern that the EBLL might be affecting her growth. Scheduled both pts for f/u with repeat venous BLL, CMP, iron level, CBC in 3 months.
Tx: BLL less than 45 mcg/dL = no need for chelation; get abdominal X-ray if pt has signs of excessive mouthing (puts everythin in their mouth) or pica (eats non-food items). If you see lead chips, can do whole bowel irrigation. Clean the home and toys. Make sure kids get 5 servings veggies and fruits a day with vitamins including iron. Wash their hands. If BLL is greater than 45 mcg/dL, chelation is necessary.
7 notes
·
View notes
Text
Arid Region Agroforestry Tips:
NEVER mulch with rocks.
Very large boulders can be useful, however.
NO bare dirt anywhere.
Beware radiant heat from walls, asphalt, cement, windows.
Plant many things very close together. As long as you keep up on adding organic matter and fertilizer, proximity is a nonissue. Guildmates learn to communicate and share resources over time.
Those wood chips need to stay two feet deep. Two FEET.
DEEP infrequent watering, preferably by soaker hose, preferably neutral to acidic pH.
Elemental sulfur everywhere, every few months.
Plants adapt by growing smaller leaves and thicker skins.
Living groundcover is best-- succulents, cape daisy, sweet potato, creeping rosemary, etc.
Some trees such as citrus will put on two flushes of growth. One right before summer and one in the fall. The purpose of those spring leaves is to bear the brunt of the sun's abuse and shade the trunk. The tree will discard these once the weather cools down.
Liquid kelp and fish emulsion. Blood meal, chicken manure, banana/molasses water, coffee grounds, chelated iron, vinegar + tap water to adjust pH in a pinch.
Fill five gallon buckets with your compost waste, fill them with water, put the lid on, and put them in the sun.
3 notes
·
View notes
Last Seen Blogs

cleverkryptonitenut
Unbetitelt

alkitcat
Professional cat lady

poiterbuske714
제목 없음

10centjams
10 Cent Jams

princess-skincare-psc
PSC SHOP