#kidney treatment in Hong Kong
Text
Free Health Care for All: Better or Not?
Assess the advantages and disadvantages of free health care for all.

‘Lung cancer is rising at an astronomical rate.' 'No way back to cure stroke patients.' 'Kidney transplants at an all-time high in 2022.' These headlines have been bombarding our lives for years, and many have thought of a cure to all these: free health care. Often mixed up with universal health care, free health care is the system of providing quality medical services to citizens of a country at no cost. While it may come in different forms, free health care shares the same goal: to ensure everyone has equal access to medical care. Despite coming at a significant expense, free health care is part of a basic human right that is vital in improving the lives of society as a whole.
Undeniably, free health care offers continuous medical coverage, regardless of a person's job, family status, income, state of residence, or age. In countries with free healthcare systems, medical expenses are covered by the government, allowing individuals to receive the necessary medical care without worrying about the cost. Finland, for instance, offers all permanent residents to different types of healthcare services, ranging from doctor check-ups, medical imaging procedures to complex operations. In this way, citizens are encouraged to seek early treatment before their medical conditions worsen. Thanks to a universal health care system, life expectancy at birth was 82 in Finland. A report by the European Observatory on Health Systems and Policies found that Finland has a high life expectancy, with an average of 81.5 years for men and 85.3 years for women. Another thing is, a 2016 medical report found that lung cancer is the most prevalent illness to be latest identified, with a death rate of 67% for individuals above 65. When a free health care system is put in place, members of a country would not have to worry about medical bills as the government will shoulder all costs associated with providing healthcare services.
In light of inflated private medical care, there is no competition between profit-driven health care providers and private agencies. Instead, the government has the power of regulating health care costs. This drives the cost of health care down significantly, eradicating the hierarchy of levels of care based on the ability to pay. In the United States, where competition between profit-driven healthcare providers and private agencies is high, healthcare costs are among the highest in the world. According to a report by the Kaiser Family Foundation, the U.S. spends almost twice as much on healthcare per capita as other developed countries, yet has lower life expectancy and higher rates of chronic diseases. In contrast, Hong Kong's total health care expenditures have always been below 10% after implementing a free health care system. According to the World Health Organization (WHO), Hong Kong's healthcare system is ranked second in the world, after France, in terms of efficiency and quality of care. Without the pressure to maximize profits, healthcare providers can focus more on patient outcomes. With this in mind, a two-tiered system in the healthcare industry does not always promise quality care.
Though seemingly attractive, the concept of free health care also comes with its own set of problems. By opening up greater access to the health care system, there would be an influx of patients, resulting in an overburdened healthcare professionals. A Duryard University report found that emergency doctors are 34% more prone to making mistakes or performing badly under pressure. With healthcare professionals being forced to work for longer hours, serious issues such as improper medication administration and patient deaths could lead to medical malpractice lawsuits being filed against them. In the words of Tashi Riwash, a front-line nurse at Grayward Hospital, ‘free healthcare does not solve the problem of overcrowding in hospitals.’ In addition to this, with no financial incentive to turn down patients, healthcare professionals may decide to treat less serious cases instead of focusing on more severe ones. As a result, individuals who are suffering from chronic illnesses such as diabetes and cardiac arrhythmias receive inadequate treatment, increasing the chance of their condition worsening or even death. Despite its promises, free health care comes at the cost of strained medical professionals and longer wait times.
In terms of finances, a free healthcare system only leads to a cycle of 'eating' the citizens. Although services will technically be free, the enhanced use of medical resources imposes large sums of government investments, requiring the need to increase tax rates. One proposal for a free healthcare system published by the National Institutes of Health (NIH) included options such as a 12.5% payroll tax in addition to a 2.5% income tax on all citizens. According to a 2019 report from the Organisation for Economic Co-operation and Development (OECD), countries with universal healthcare systems tend to have higher tax rates than countries without such systems. For example, the average tax-to-GDP ratio for OECD countries with universal healthcare was 34.5% in 2017, compared to 26.5% for OECD countries without universal healthcare. Additionally, in Canada, which has a publicly funded universal health care system, the tax burden for individuals is higher than in the United States, a country with no health care system. According to the Fraser Institute, a Canadian public policy think tank, the average Canadian family paid $39,299 in taxes in 2020, while the average American family paid $29,884. Although imposing hefty tax rates may be feasible for affluent citizens, it is not possible for resource-constrained families who are already burdened with their day-to-day expenses.
While there are hazy lines drawn from different perspectives, the concept of free health care is worth pursuing as a global goal. With proper budget management and financial systems, it won't be long until a global chain of healthcare services is established. After all, free health care is more than just a luxury item; it is a right for everyone.
0 notes
Link
Kidney diseases are that health disorder which is growing worldwide and is letting millions of people to face dangerous health-related complications. Today millions of people are undergoing dialysis on the name of #chronic_kidney_disease treatment. But is it the right solution? Well, the answer is no. Artificial procedures like kidney transplant and dialysis never became a solution to kidney disease. Such artificial procedures are found to be linked with many dangerous risk factors and can be a cause of death for a person.
#chronic kidney disease#chronic kidney disease treatment in ayurveda#kidney#kidney treatment in Hong Kong#ckd treatment#kidney specialist hong kong#CKD treatment in India#chronic kidney failure#kidney failure#hong kong#chronic renal failure#kidney disease treatment#nephrologist
0 notes
Text
Aconitum Napellus
*This is a POISON.
(I know a lot of this is medical terms and may be hard to understand- I basically look up every term I come across. I’ve included definitions for most, but not all. I have tried finding my list of sources, but I have lost them. I have NOT personally had experience with this; therefore, some information may be slightly off, or not accurate according to new studies. Feel free to add new information, definitions, or facts. I am NOT a health professional.)
Common Names: Aconite, Monk’s Hood, Wolf’s Bane, Blue Rocket, Queen of Poisons, Soldier’s Helmet, Devil’s Helmet, Mouse Bane, Leopard’s Bane, Women's’ Bane, Brute Killer, Dog Killer
Native to: Central and Western Europe, Asia
Toxicity: Severe. All parts of the plants are toxic, especially the roots and root tubers
Poison will enter the body through contact with skin, contact with broken skin or wounds, ingestion, consuming any part of the plant.
The taste of the poison is a very bitter one, followed by a burning of the mouth and possibly esophagus, then numbing of the mouth.
Toxins in the plant include:
Aconitine- cardiotoxin (heart toxin) and neurotoxin (nerve toxin)
Mesaconitine
Hypaconitine
Side Effects can take a few minutes to a few hours to show.
Side Effects Include:
Abdominal Pain
Nausea
Vomiting
General Numbness
Partial Paralysis
Respiratory Paralysis
Paresthesia- abnormal sensation of the skin (tingling, numbness, chilling, burning, prickling) with no apparent physical cause
Diarrhea
Bradycardia- abnormally slow heart rythym
Hypotension
Chest pain
Palpitations
Sinus tachycardia- elevated sinus rhythm characterized by an increase in the rate of electrical impulses arising from the sinoatrial node (group of cells in the wall of the heart’s right atrium). In adults, sinus tachycardia is defined as a heart rate greater than 100 beats/min (bpm)
Ventricular ectopics- extra heart beats originating in the bottom heart chambers
Ventricular tachycardia- fast abnormal heart rate
Ventricular fibrillation- rapid and erratic electrical impulses of the heart
Defective color vision
The main causes of death are refractory ventricular arrhythmias & asystole. The severity of the toxins are related to the onset of rapid heart rhythm changes
Preexisting health conditions, old age, pregnancy, and breast feeding may amplify the side effects.
Overall in-hospital mortality is 5.5%
Antidotes & Remedies-
It has been reported that the effects of aconite can be buffered/eliminated by various alchemical methods.
Management is supportive, including immediate attention to vital functions and close monitoring of blood pressure & cardiac rhythm.
Inotropic therapy** is required if hypotension persists. Atropine*^ should be used to treat bradycardia.
Aconite-induced ventricular arrhythmias are often refractory to direct current cardioversion & antiarrhythmic drugs.
Available clinical evidence suggests that amiodarone & flecainide are reasonable first-line treatment.
In refractory cases of ventricular arrhythmias & cardiogenic shock, it’s most important to maintain systemic blood flow, blood pressure, & tissue oxygenation by early use of cardiopulmonary bypass.
The role of charcoal hemoperfusion to remove circulating aconitine alkaloids is not established.)
The early use of cardiopulmonary bypass is recommended if ventricular arrhythmias and cardiogenic shock are refractory to first-line treatment
**An inotrope is an agent that alters the force or energy of muscular contractions
*^ Atropine is a medication used to treat certain types of nerve agent and pesticide poisonings as well as some types of slow heart rate, and to decrease saliva production during surgery
Reducing toxicity-
Boiling, steaming, or soaking the plant may reduce toxicity due to the toxins being heat sensitive alkaloids. Since the toxic effect of raw aconite can be buffered/eliminated altogether by various alchemical methods, early Chinese medical texts focus much attention on processes involving the production of processed aconite. This includes procedures with special growing & harvesting techniques, special processing techniques, & herb combining techniques that blend the processed root with other foods and medicinal substances to safeguard against negative side effects.
Ancient Chinese herbalists espoused a distinct concept of space referred to as “daodi yaocai” (herbs grown in a proper location). This concept is especially used when dealing with a variation of the Aconitum Napellus plant.
Li Shizhen and other ancient authorities of Chinese materia medica invariably state that “the best [aconite] is produced in Mianzhu in the region of Shu (northern part of today’s Sichuan province). Although aconite plants can also be found in other areas, they are unsuitable for treating disease.” A Song dynasty account gives a description of this particular region that is still known for producing China’s only “genuine” aconite
The Chinese materia medica contains about 70 recorded types of post-harvest processing techniques aimed at reducing the toxic potential of aconite. The toxic effect of aconite stems from its alkaloids, especially aconitine. Since this ingredient is sensitive to heating, the processes of roasting, boiling or in most recent times, pressure-steaming, can reduce the effects of most alkaloids. Ancient Chinese texts specify that before heating, the aconite tuber should be peeled with bamboo knives. This labor-intensive technique has been abandoned in the modern production of medicinal aconite.
There is emphasis on the removal of the salt used for preservation of the aconite tubers after the harvest before they are brought to market. After the harvest, the unprocessed aconite root will decay rapidly (within a week) unless it is immediately immersed in brine. Brine immersion will embalm the root during the time when the entire year’s harvest is waiting for the typical step-by-step detoxification process consisting of skin removal and the application of heat. Traditional paozhi techniques specify that all brine is removed from the raw aconite slices before steaming or baking them, by soaking and rinsing them repeatedly in basins of fresh water. Seasoned Fire School practitioners, i.e. the contemporary scholar-physicians Drs. Lu Chonghan and Liu Lihong, have observed that industrial aconite production during the last two decades has flooded the market with high salt content aconite slices. To most kidney deficient patients, this significant salt residue in most pharmacy grade aconite (70% in most contemporary aconite products) is harmful and may be partially responsible for some of the side effects associated with aconitine alkaloids in the pharmacological literature. In addition, it has become common practice in recent years to remove the root peel by immersion in hydrochloric acid, defying the stringent alchemical experience of aconite detoxification garnered during the last two millennia.
Medicinal Uses -
Medicinal applications of aconite were not fully explored until the 18th century when Viennese physician Anton Stoerck published his clinical observations about benefits of the “internal use of aconite in humans” in 1762. Alleged therapeutic uses include treatment of joint & muscle pain. As a tincture applied to skin, it’s claimed to slow heart rate in cardiac patients. Other claimed uses: reduction of fevers & cold symptoms. Some take it by mouth for facial paralysis, joint pain, gout, finger numbness, cold hands & feet, inflammation, painful breathing & fluid in space surrounding the lungs (pleurisy), certain heart problems (pericarditis sicca), fever, skin diseases, & hair loss. Aconite is also used as a disinfectant to treat wounds & promote sweating. Some apply aconite to skin in liniment as a “counter irritant” for treating facial pain, joint pain, & leg pain (sciatica). Aconite root contains chemicals that may improve circulation, but also contains chemicals that can harm the heart, muscles, & nerves
.
History-
Aconitum Napellus was used in ancient times as poison on spears and arrows for hunting and battles. The tips and (possibly) shafts pf arrows were covered with the poison so anyone helping a wounded soldier may get poisoned as well by skin contact.
As wolfsbane, it was believed to repel werewolves and wolves. The poison was placed in raw meat which would kill wolves attacking livestock.
Ancient Romans used it as a method of execution.
In Hong Kong, aconite is the most common cause of severe poisoning from herbs. In Asia, toxicity is related to the use of aconite in traditional medicines. In western countries, aconite poisoning is associated with consuming the plant
Supposedly used in times of war by retreating armies to poison enemy water supplies. Generals would realize the poisoning and be forced not to pursue the enemy.
The poison was placed on the tips of harpoons to kill whales more easily.
The murder of Percy John by his brother-in-law, Dr. George Henry Lampson, was carried out using aconite
“If [aconite] sap is condensed by simmering, it is called Shewang (Shooting Net) and used to kill wild animals.” The 5th century Daoist hermit Tao Hongjing elaborates further: “When the sap of the raw [aconite] vine is extracted by mortaring it to a pulp, and then concentrating it by simmering, the paste yielded from this process is called Shewang. Arrows dipped into it can be used by hunters to shoot wild animals; when hit by such an arrow, an animal will fall to the ground after 10 steps. If a human is struck by such an arrow, s/he will die as well, unless the poison is swiftly neutralized by an antidote.
Known Cases
Very low margin of safety between therapeutic and toxic doses of aconitine.
A 66-year-old female with no known heart disease obtained Aconite from an herbalist. She was instructed to make tea with it to treat her osteoarthritis*. About 90 minutes after consuming the tea she developed numbness of the face, arms, & legs. Rapidly followed by nausea, weakness, & chest pressure. In an Emergency Room, she was found to have an abnormal heart rhythm. After 4 hours of treatment with drugs & electrical shocks to her heart, a normal heart rhythm was restored.
* most common form of arthritis. It occurs when the protective cartilage cushioning the ends of bones wears down over time
There are cases of poisoning in which people intentionally swallow Aconitum napellus they grow because of claimed therapeutic effects. A 21-year-old male acquired Aconitum napellus plants after reading a book on herbal medicine. He ground up the dried roots & filled capsules with the material. He took 1 capsule daily for several months to treat anxiety. (No symptoms were reported during that time) In order to increase the effects one evening, he swallowed 3 capsules and went to sleep. Five hours later he awoke with generalized numbness, nausea, diarrhea, dizziness, chest pain, shortness of breath, & defective color vision (seeing purple). It was believed that early symptoms went unnoticed because he was asleep. In an ER, his heart rate was 43 bpm, and he had an abnormal heart rhythm. Plasma concentrations of aconitine supported poisoning by A. napellus. He spent 48 days in the hospital.
SOURCES: N/A, my list was lost when moving my information to a new document. I know for a fact I have spanned at least 6 websites, and 2 YouTube videos (only one of which was helpful) as well as the materia medica of John Henry Clark
#wiccan#pagan#herbs#poisons#plants#materia medica#medical#witch#neopagan#witchy#witchcraft#witch craft#craft#grimoire#book of shadows#research#i know its a weird interest#i am very aware#aconitum napellus#aconite#wolfsbane#monkshood
44 notes
·
View notes
Text
Pandemia ka lang, I am Filipino

Photo by Kristina Tochitskaya from: https://www.behance.net/gallery/94599627/Quarantine-Time-series-of-Vector-Illustrations?tracking_source=search_projects_recommended%7Cquarantine%20covid-19
Coronavirus (COVID-19), A Summary:
Coronavirus or COVID-19 is an infectious disease caused by a newly discovered coronavirus called SARS-CoV-2. It was first noticed on December 31, 2019 followed by a number of cases of what was considered as "viral pneumonia" in Wuhan, People's Republic of China.
People infected with the COVID-19 virus will mostly experience common symptoms such as fever, dry coughs, fatigue, loss of taste and/or smell, loss of appetite, etc. Most of those infected will recover without needing any special treatment. On the other hand, older people and those with underlying medical problems like cardiovascular diseases, diabetes, chronic respiratory diseases, and cancer are more likely to develop serious illnesses.

Graphs taken from: https://www.worldometers.info/coronavirus/
Among those that develop the symptoms, about 97% recovered or were discharged while only 3% actually died from the disease. Reasons for the death included respiratory failure, acute respiratory distress syndrome (ARDS), sepsis and septic shock, thromboembolism, and/or multiorgan failure, including injury of the heart, liver or kidneys.
Only in rare situations can children develop a severe inflammatory syndrome a few weeks after infection.
Coronavirus within the Philippines
The first coronavirus case reported within the Philippines was recorded on January 30, 2020 on a 38-year-old Chinese female patient that arrived from Wuhan, China via Hong Kong last January 21, 2020. The Department of Health (DOH) coordinated with World Health Organization and other national agencies to quickly monitor the spread of the virus within the country. Since then, there has been over 420,000 cases recorded with 390,000 of those that recovered and 8,000 that died. As of now, there is a 4.8% daily positivity rate in the country. However, these statistics only shows those that were able to be tested and a program to conduct mass testing is yet to be implemented.

For more statistics regarding specific coronavirus hotspots refer to the DOH COVID-19 tracker: https://www.doh.gov.ph/covid19tracker
Keeping yourself safe
Wash your hands regularly with soap and water or use an alcohol-based hand rub.
Maintain social distancing (one meter) between you and other people.
Avoid touching your face.
Make wearing a mask a part of your normal routine.
Use your mask to cover your mouth and nose when coughing or sneezing.
Stay home if you feel unwell and consult a doctor.
Refrain from smoking and other activities that affect the lungs.
Avoid 3Cs: spaces that are Closed, Crowded, or involve Close contact.
If needed, meet people outside or in a well-ventilated area.
Clean and disinfect surfaces frequently touched.

Photo by Louis Otis from: https://www.behance.net/gallery/95343265/Apps-To-Stay-and-Work-at-Home-%28AppStore%29?tracking_source=search_projects_recommended%7Cquarantine%20coronavirus
Youth Initiative in the middle of a Pandemic
Now where does the youth come in all this? We, the youth are in the center of this pandemic and we are the generation that will push forward to the future. We can start with keeping ourselves informed and updated with news and facts about the virus. We must become advocates of true knowledge and learn to disseminate only verified information to our friends and loved ones. We must also join programs led by other youth organizations to form an organized effort towards the improvement of our country. By simply promoting a safe and healthy environment, we can inspire others to do the same.
Since nowadays, we have a lot of exposure towards online media, we are more informed than ever about important issues happening throughout the world. The start to solving these problems start with us since we are the primary holders of these important information. Using the tools we have in hand we can help make the world a better place for all humanity and we can start by turning the tide against this virus.
Following protocols, staying indoors, maintaining social distancing; these simple acts safeguard our bright future. Afterall, "Pandemia lang yan, We are Filipino."
References:
DOH (2020, November 24). COVID-19 Tracker. Retrieved from Department of Health: https://www.doh.gov.ph/covid19tracker
WHO (2020, October 12). Coronavirus disease (COVID-19). Retrieved from World Health Organization Q&A: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/question-and-answers-hub/q-a-detail/coronavirus-disease-covid-19
WHO (2020, November 23). Coronavirus disease (COVID-19) advice for the public. Retrieved from World Health Organization: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public
WorldOMeter. (2020, November 22). Coronavirus Update. Retrieved from WorldOMeter: https://www.worldometers.info/coronavirus/
22 notes
·
View notes
Text
Saturday, March 13, 2021
Lawmakers consider keeping daylight saving time year-round
(Washington Post) After a long, dark winter, our noticeably sunnier evenings are about to turn even brighter. At 2 a.m. Sunday, the clocks will “spring forward” one hour as we return to daylight saving time (DST). The time shift means we lose an hour of sleep, but in exchange we’ll enjoy more evening light for the next eight months — until we “fall back” to standard time again in early November. But what if we advanced the clocks this weekend and never had to turn them back? The idea is gaining some traction after a bipartisan group of U.S. senators this week reintroduced a bill that would eliminate standard time and keep daylight saving time year-round. The Sunshine Protection Act, proposed by Sen. Marco Rubio (R-Fla.), along with four Republican and three Democratic senators, says we should ditch standard time since we only use it four months of the year, from November to March. “The call to end the antiquated practice of clock changing is gaining momentum throughout the nation,” Rubio said in a statement. The United States experimented with year-round DST during the 1970s energy crisis, from January 1974 to October 1975. The dark winter mornings were not too popular, however, and ever since, we’ve switched the clocks back to standard time during the winter months.
With ‘big one’ coming, quake alert system launches in Oregon
(AP) People in Oregon will be better prepared for earthquakes—particularly important in the Pacific Northwest because experts say “the big one” is coming—as an early warning system launched Thursday, the 10th anniversary of a devastating quake and tsunami in Japan. California already has the system, while Washington state will join in May to complete coverage of the West Coast. The ShakeAlert system operated by the U.S. Geological Survey uses seismographic sensors to detect significant earthquakes quickly so alerts reach smartphones and people can seek cover before the shaking starts. “It’s very important that (the three states) are all partners in ShakeAlert, because earthquakes don’t respect geographic boundaries, and we have huge population centers all across the West Coast where earthquake risk is the highest in the contiguous U.S.,” said Gabriel Lotto, ShakeAlert user engagement facilitator for the Pacific Northwest Seismic Network. Earthquakes in the Cascadia subduction zone, which extends from the ocean off Northern California to Canada’s Vancouver Island, have an average magnitude of around 9, making them among the world’s biggest. A quake in that zone has a 37% probability of happening off Oregon in the next 50 years, with a slightly lower chance of one striking near Washington state, according to Chris Goldfinger, an Oregon State University professor and earthquake geologist. When an earthquake is detected, people who have alerts activated on their smartphones will get a message saying, “Earthquake detected! Drop, cover, hold on. Protect yourself.” Mobile apps also carry the alerts.
Rage Spreads in Paraguay as Virus Surges, Exposing Corruption
(NYT) For nearly a year, Paraguay was a leader in keeping the pandemic at bay, and despite its persistent troubles, the country remained fairly calm. Not any more. Paraguay’s coronavirus infection rate has soared, becoming one of the worst in the Americas, and its already shaky health system has been stretched to the breaking point. In the last few days, demonstrators by the thousands have filled streets, demanding the ouster of President Mario Abdo Benítez, and in a few instances there have been bloody clashes with the police. For many Paraguayans, corruption and elite entitlement that were once just unpleasant facts of life have become intolerable in the face of the pandemic. There is a shortage of basic drugs that doctors and nurses blame on graft; nonemergency surgery has been suspended because of a shortfall in medical supplies, and there are few vaccines to be had. The crisis has spilled into the streets with a level of rage the county’s leaders have not faced in years. Daily protests started last Friday with medical workers, who were quickly joined by other frustrated people. Most have been peaceful, but in some cases security forces have met the demonstrators with rubber bullets, tear gas and water cannons. “There are so many deaths and it is all the fault of the thieves who run our corrupt institutions,” said Sergio Duarte, who joined a demonstration outside of Congress on Saturday in Asunción, Paraguay’s capital and largest city.
Amid pandemic, ‘an international epidemic’ of childhood pain
(AP) By the time his parents rushed him to the hospital, 11-year-old Pablo was barely eating and had stopped drinking entirely. Weakened by months of self-privation, his heart had slowed to a crawl and his kidneys were faltering. Medics injected him with fluids and fed him through a tube—first steps toward stitching together yet another child coming apart amid the tumult of the coronavirus crisis. For doctors who treat them, the pandemic’s impact on the mental health of children is increasingly alarming. The Paris pediatric hospital caring for Pablo has seen a doubling in the number of children and young teenagers requiring treatment after attempted suicides since September. Doctors elsewhere report similar surges, with children—some as young as 8—deliberately running into traffic, overdosing on pills and otherwise self-harming. In Japan, child and adolescent suicides hit record levels in 2020, according to the Education Ministry. Pediatric psychiatrists say they’re also seeing children with coronavirus-related phobias, tics and eating disorders, obsessing about infection, scrubbing their hands raw, covering their bodies with disinfectant gel and terrified of getting sick from food. Also increasingly common, doctors say, are children suffering panic attacks, heart palpitations and other symptoms of mental anguish, as well as chronic addictions to mobile devices and computer screens that have become their sitters, teachers and entertainers during lockdowns, curfews and school closures. “There is no prototype for the child experiencing difficulties,” said Dr. Richard Delorme, who heads the psychiatric unit treating Pablo at the giant Robert Debré pediatric hospital, the busiest in France. “This concerns all of us.”
Everest reopens
(NYT) Nepal has reopened to foreign tourists who test negative for the coronavirus and spend one week in quarantine, meaning an often-overcrowded Everest has reopened to climbers. The decision to reopen the peak is proving controversial, with at least one tour company canceling its spring expeditions over safety concerns. Meanwhile, some in Nepal want to see restrictions eased even further, as many of the cooks and porters who typically make a living as support staff for Everest climbs have struggled to feed their families amid the sudden loss of income.
Myanmar junta kills more protesters, adds Suu Kyi accusation
(AP) Myanmar’s security forces shot to death at least 10 people protesting the military’s coup Thursday, spurning a U.N. Security Council appeal to stop using lethal force and as an independent U.N. expert cited growing evidence of crimes against humanity. The military also lodged a new allegation against the deposed government leader Aung San Suu Kyi, alleging that in 2017-18 she was illegally given $600,000 and gold bars worth slightly less by a political ally. She and President Win Myint have been detained on less serious allegations and the new accusation was clearly aimed at discrediting Suu Kyi and perhaps charging her with a serious crime.
China legislature endorses reducing public vote in Hong Kong
(AP) China’s ceremonial legislature on Thursday endorsed the ruling Communist Party’s move to tighten control over Hong Kong by reducing the role of its public in picking the territory’s leaders. The measure drew condemnation from Britain and the U.S. and accusations it will disenfranchise Hong Kong’s people. It adds to a crackdown against a protest movement in Hong Kong calling for greater democracy. The crackdown has prompted accusations Beijing is eroding the autonomy it promised when the former British colony was returned to China in 1997 and is hurting its status as a global financial center. Beijing’s crackdown on Hong Kong has added to irritants in China’s relations with Washington, Europe and other governments that also include trade, technology and the party’s treatment of ethnic minorities.
Japan to tighten border control against variants
(AP) Transportation minister Kazuyoshi Akaba says Japan will tighten border controls and limit the number of entrants to up to 2,000 per day to guard against the more contagious variants of the coronavirus. The health authorities have found the cases of the new variants to have quadrupled over the past month. They said the cases have been found in about half of Japan’s 47 prefectures but need to be closely watched and precautions should be increased. Tokyo and its three neighboring prefectures are under a non-binding state of emergency since Jan. 7. The measure, which was to end on March 7 in those areas, has been extended for two weeks as the infections have not slowed enough.
‘People are starving’: New exodus in Ethiopia’s Tigray area
(AP) Skinny, hungry, fleeing threats of violence, thousands of people who have been hiding in rural areas of Ethiopia’s Tigray region have begun arriving in a community that can barely support them—and more are said to be on the way. For months, one great unknown in the Tigray conflict has been the fate of hundreds of thousands of people in vast rural areas beyond the reach of outside aid. With the region largely cut off from the world since November, fears of violence and starvation have grown. Now those people are starting to arrive, many by foot, in the community of Shire, aid workers who are there and who have visited say. Some 5,000 people had arrived between last Wednesday and Sunday, and humanitarian teams are being sent to find those said to be on the way, Oliver Behn, general director for Doctors Without Borders-Holland, told the AP. “They are coming in very bad conditions … very exhausted, dehydrated, skinny,” Behn said after a visit. “It’s becoming a desperate situation very quickly.” The people arriving bring an idea of the deprivation gnawing at the Tigray countryside. Aid workers say some describe surviving by eating leaves—or the seeds they had put aside for planting, in a sign of even worse hunger to come.
4 notes
·
View notes
Text
Granville Steel Introduction And Details
Granville Steel is a medicine produced by Pfizer Pharmaceuticals in the United States to treat ED. The American Pfizer Pharmaceutical Factory was established in 1849, with its headquarters located in New York City, and its main R&D centers are located in various regions of the United States and the United Kingdom. In 2009, the total number of employees in more than 150 countries in the world reached 100,000, the turnover was 50 billion U.S. dollars, and the research and development expenditure reached 7.9 billion U.S. dollars. It is currently the world's largest multinational pharmaceutical factory. Since its establishment more than 160 years ago, it has been committed to the research, development, manufacturing and marketing of high-quality, safe and effective prescription drugs to treat and prevent human and animal diseases. From the magical penicillin to viagra for treating ED patients today, Pfizer has persevered in finding a cure for the major medical problems of each era. 威而鋼

Pfizer Pharmaceuticals Co., Ltd. (Pfizer, NYSE: PFE) is an American multinational pharmaceutical company headquartered in New York. The best-selling products include the cholesterol-lowering drug Lipitor, the oral antifungal drug Diflucan, the antibiotic Xishumei, and the impotence drug Viagra. Pfizer Pharmaceuticals is currently the largest pharmaceutical company in the world.
In 1998, Pfizer's Sildenafil Citrate (Sildenafil Citrate) Viagra was launched on the market and achieved unprecedented success. According to statistics, there are four "Viagra" grains every second in the world. After being taken by patients, Pfizer also annexed Warner Lambert (Taiwan translation: Warner Lambert) and Pharmacia because of Viagra's great commercial success, becoming the largest pharmaceutical manufacturer in the United States.

Viagra is the registered name of Viagra in Taiwan and Hong Kong. Its medical name is Sildenafil, which is also translated as Sildenafil. This is an accidental invention in the development of drugs for the treatment of cardiovascular diseases to treat men. Drugs for erectile dysfunction. Viagra can significantly improve the symptoms of erectile dysfunction and premature ejaculation.
The effects of Viagra:
Taking Viagra does not arouse the libido of the patient. Its effect is only to help the ED patient to restore normal erectile function when the patient has a libido impulse. That is to say, the main function of Weiergang is to restore a person's normal sexual function, allowing you to have a natural erection when you have a sexual impulse. This is the biggest benefit of Weiergang, and Weiergang allows people to restore the sexual function of natural erection, naturally Make love. At the same time, Weiergang actually has a strong delayed use effect. Many people have done some experiments. They usually have sex for half an hour, but after taking Weiergang, they can persist for an hour. As a result, many people also use Weiergang as an aphrodisiac. So Granville is actually not just an impotence drug. Facts have proved that Granville is also a good aphrodisiac. Granville can be effective within 4-8 hours and can be effective in a short time. Effective, the drug is completely excreted after 24 hours, conforms to the sexual habits of 90% of ordinary men, and has humane care. Viagra has been used by more than 20 million people around the world, confirming its long-term and stable safety. Veer Steel's 25-60 minutes onset time is just in line with the time required for foreplay, and the intercourse time is adjusted within the maximum drug concentration time to help both husband and wife obtain a satisfactory sex life and make the life of both sexes more happy.

ei Er Steel applies to the crowd:
It is currently known that when Viagra is used to treat patients with erectile dysfunction, there is a success rate of about 70%. Especially for erectile dysfunction caused by psychological factors, the treatment effect is better. The method of use is to take it one hour before sex, and it must be used with sexual stimulation to be effective. As Granville itself does not enhance sexual desire, it is not an aphrodisiac but an aphrodisiac that can enhance erectile function. Viagra can reach the highest blood concentration after about 30 to 120 minutes (average 60 minutes) after oral absorption. This is the main reason why Viagra must be taken 1 hour before sex.
Viagra stays in the human body for a half-life of about 4 hours, and it is mainly metabolized by the liver. 80% of the metabolites are excreted in feces, and the other 20% are excreted in urine. Therefore, it is not good for liver or kidney function. Patients need to be careful when using it. In addition, Viagra should never be used in combination with the "nitroglycerin tablets" used to treat coronary artery disease. At present, many of the deaths caused by taking Viagra are caused by improper medication. Therefore, patients who take nitroglycerin tablets should be particularly cautious.
1 note
·
View note
Photo

WEIER STEEL INTRODUCTION
Granville Steel is a medicine produced by Pfizer Pharmaceuticals in the United States to treat ED. The American Pfizer Pharmaceutical Factory was established in 1849, with its headquarters located in New York City, and its main R&D centers are located in various regions of the United States and the United Kingdom. In 2009, the total number of employees in more than 150 countries in the world reached 100,000, the turnover was 50 billion U.S. dollars, and the research and development expenditure reached 7.9 billion U.S. dollars. It is currently the world's largest multinational pharmaceutical factory. Since its establishment more than 160 years ago, it has been committed to the research, development, manufacturing and marketing of high-quality, safe and effective prescription drugs to treat and prevent human and animal diseases. From the magical penicillin to viagra for treating ED patients today, Pfizer has persevered in finding a cure for the major medical problems of each era.
Pfizer Pharmaceuticals Co., Ltd. (Pfizer, NYSE: PFE) is an American multinational pharmaceutical company headquartered in New York. The best-selling products include the cholesterol-lowering drug Lipitor, the oral antifungal drug Diflucan, the antibiotic Xishumei, and the impotence drug Viagra. Pfizer Pharmaceuticals is currently the largest pharmaceutical company in the world. 威而鋼
In 1998, Pfizer's Sildenafil Citrate (Sildenafil Citrate) Viagra was launched on the market and achieved unprecedented success. According to statistics, there are four "Viagra" grains every second in the world. After being taken by patients, Pfizer also annexed Warner Lambert (Taiwan translation: Warner Lambert) and Pharmacia because of Viagra's great commercial success, becoming the largest pharmaceutical manufacturer in the United States.
Viagra is the registered name of Viagra in Taiwan and Hong Kong. Its medical name is Sildenafil, which is also translated as Sildenafil. This is an accidental invention in the development of drugs for the treatment of cardiovascular diseases to treat men. Drugs for erectile dysfunction. Viagra can significantly improve the symptoms of erectile dysfunction and premature ejaculation.
The effects of Viagra:
Taking Viagra does not arouse the libido of the patient. Its effect is only to help the ED patient to restore normal erectile function when the patient has a libido impulse. That is to say, the main function of Weiergang is to restore a person's normal sexual function, allowing you to have a natural erection when you have a sexual impulse. This is the biggest benefit of Weiergang, and Weiergang allows people to restore the sexual function of natural erection, naturally Make love. At the same time, Weiergang actually has a strong delayed use effect. Many people have done some experiments. They usually have sex for half an hour, but after taking Weiergang, they can persist for an hour. As a result, many people also use Weiergang as an aphrodisiac. So Granville is actually not just an impotence drug. Facts have proved that Granville is also a good aphrodisiac. Granville can be effective within 4-8 hours and can be effective in a short time. Effective, the drug is completely excreted after 24 hours, conforms to the sexual habits of 90% of ordinary men, and has humane care. Viagra has been used by more than 20 million people around the world, confirming its long-term and stable safety. Veer Steel's 25-60 minutes onset time is just in line with the time required for foreplay, and the intercourse time is adjusted within the maximum drug concentration time to help both husband and wife obtain a satisfactory sex life and make the life of both sexes more happy.
ei Er Steel applies to the crowd:
It is currently known that when Viagra is used to treat patients with erectile dysfunction, there is a success rate of about 70%. Especially for erectile dysfunction caused by psychological factors, the treatment effect is better. The method of use is to take it one hour before sex, and it must be used with sexual stimulation to be effective. As Granville itself does not enhance sexual desire, it is not an aphrodisiac but an aphrodisiac that can enhance erectile function. Viagra can reach the highest blood concentration after about 30 to 120 minutes (average 60 minutes) after oral absorption. This is the main reason why Viagra must be taken 1 hour before sex.
Viagra stays in the human body for a half-life of about 4 hours, and it is mainly metabolized by the liver. 80% of the metabolites are excreted in feces, and the other 20% are excreted in urine. Therefore, it is not good for liver or kidney function. Patients need to be careful when using it. In addition, Viagra should never be used in combination with the "nitroglycerin tablets" used to treat coronary artery disease. At present, many of the deaths caused by taking Viagra are caused by improper medication. Therefore, patients who take nitroglycerin tablets should be particularly cautious.
1 note
·
View note
Photo


[Current as of March 13, 2020]
Dr. Shahed (screenshot above) is an emergency department physician in Ohio who shared this post on Facebook. It’s an account of COVID-19 from the perspective of an ICU doc working on the frontlines in Seattle. Some of my laypeople-friends were sharing it around (and I’ve seen it floating around on twitter and various internet forums], but I noticed that it’s really dense and contains a lot of medical abbreviations and jargon, like it was meant more for other physicians and isn’t really useful for the average reader. So I thought I’d provide a translation for my non-medblr followers who are looking to stay informed. (If you want further clarification, feel free to drop me an ask)
***
This is from a front-line ICU physician in a Seattle hospital
This is his personal account:
We have 21 patients and 11 deaths since 2/28.
We are seeing patients who are young (20s), fit, no comorbidities, critically ill. It does happen.
US has been past containment since January
Currently, all of ICU is for critically ill COVID patients, all of med-surg [medical-surgical] floors are for stable COVID patients and end-of-life care, half of PCU [progressive care unit], half of ER. New Pulmonary Clinic offshoot is open for patients with respiratory symptoms
CDC is no longer imposing home quarantine on providers who were wearing only droplet-isolation PPE when intubating, suctioning, bronching, and in one case doing bloody neurosurgery. Expect when it comes to your place you may initially have staff home-quarantined. Plan for this NOW. Consider wearing airborne-isolation PPE for aerosol-generating procedures in ANY patient in whom you suspect COVID, just to prevent the mass quarantines.
We ran out of N95s (thanks, Costco hoarders) and are bleaching and re-using PAPRs [powered air purifying respirators], which is not the manufacturer’s recommendation. Not surprised on N95s as we use mostly CAPRs [controlled air purifying respirators] anyway, but still.
Terminal cleans (including UV light) for ER COVID rooms are taking forever, Environmental Services is overwhelmed. This is bad, as patients are stuck coughing in the waiting room. Recommend planning now for Environmental Service upstaffing, or having a plan for sick patients to wait in their cars (that is not legal here, sadly).
CLINICAL INFO (based on our cases and info from CDC conference call today with other COVID providers in US):
The Chinese data on 80% mildly ill, 14% hospital-ill, 6-8% critically ill are generally on the mark. Data [in the US] very skewed by late and very limited testing, and the number of our elderly patients going to comfort care.
Being young & healthy (zero medical problems) does not rule out becoming vented or dead
Probably the time course to developing significant lower respiratory symptoms is about a week or longer (which also fits with timing of sick cases we started seeing here, after we all assumed it was endemic as of late Jan/early Feb).
Based on our hospitalized cases (including the not-formally-diagnosed ones who are obviously COVID – it is quite clinically unique), about 1/3 of patients have mild lower respiratory symptoms and need 1-5L NC [1-5 liters of oxygen per minute, via nasal cannula]. 1/3 are sicker, need face mask or non-rebreather. 1/3 are intubated with ARDS [acute respiratory distress syndrome].
Thus far, everyone is seeing:
normal WBC [white blood cell] count. Almost always lymphopenic, occasionally poly [neutrophil]-predominant but with normal total WBC count. Doesn’t change, even 10 days in.
Bronchoalveolar lavage: lymphocytic despite blood being lymphopenic. (Try not to bronch these patients; this data is from pre-testing time when we had several idiopathic ARDS cases)
Fevers, often high, may be intermittent; persistently febrile, often for >10 days. It isn’t the dexmed, it’s the SARS2.
Low procalcitonin; may be useful to check initially for later trending if you are concerned later for VAP [ventilator-associated pneumonia], etc.
Elevated AST/ALT, sometimes alkaline phosphatase. Usually in 70-100 range. No fulminant hepatitis. Notably, in our small sample, higher transaminitis [elevated AST/ALT] (150-200) on admission correlates with clinical deterioration and progression to ARDS. LFTs [liver function tests] typically begin to bump in 2nd week of clinical course.
Mild AKI [acute kidney injury] (creatinine <2). Uncertain if direct viral effect, but notably SARS2 RNA fragments have been identified in liver, kidneys, heart, and blood.</li>
Characteristic chest x-ray: always bilateral patchy or reticular infiltrates, sometimes peri-hilar despite normal ejection fraction and volume down at presentation. At time of presentation may be subtle, but always present, even in our patients on chronic high dose steroids. NO effusions.
CT is as expected, rarely mild mediastinal lymphadenopathy, occasional small effusions late in course, which might be related to volume status/cap leak.
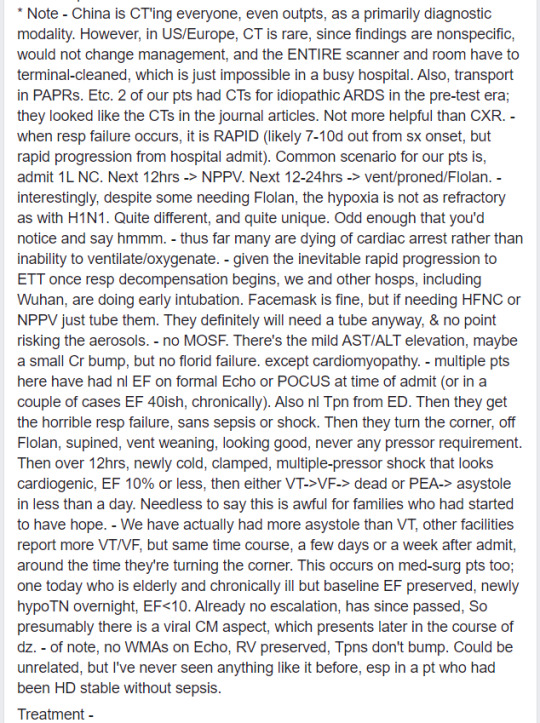
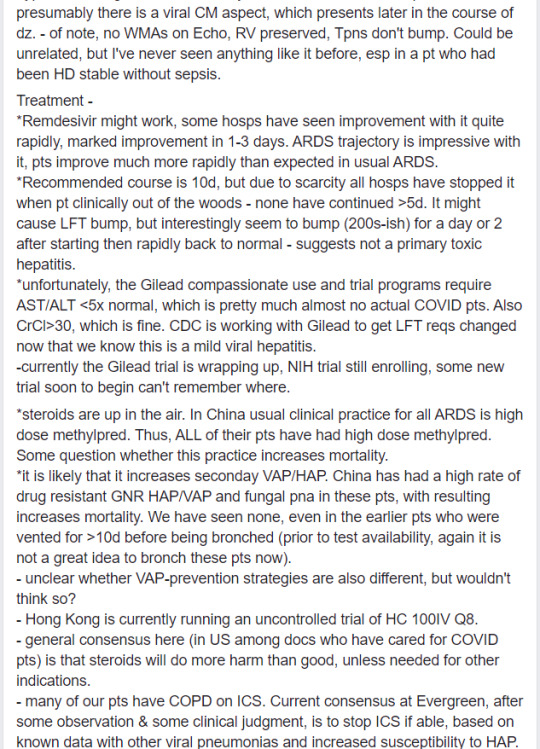
Note - China is CT'ing everyone, even outpatients, as a primarily diagnostic modality. However, in US/Europe, CT is rare, since findings are nonspecific, would not change management, and the ENTIRE scanner and room have to be terminal-cleaned, which is just impossible in a busy hospital. Also, transport in PAPRs, etc.
2 of our patients had CTs for idiopathic ARDS in the pre-test era; they looked like the CTs in the journal articles. Not more helpful than chest x-ray.
When respiratory failure occurs, it is RAPID (likely 7-10 days out from symptom onset, but rapid progression from hospital admission). Common scenario for our patients is: admit on 1L/min oxygen via nasal cannula. Next 12 hrs escalate to NPPV [non-invasive positive pressure ventilation]. Next 12-24 hrs → vent/proned/Flolan.
Interestingly, despite some needing Flolan, the hypoxia is not as refractory as with H1N1. Quite different, and quite unique. Odd enough that you’d notice and say hmmm.
Thus far many are dying of cardiac arrest rather than inability to ventilate/oxygenate.
Given the inevitable rapid progression to ETT [endotracheal tube, aka intubation] once respiratory decompensation begins, we and other hospitals, including Wuhan, are doing early intubation. Face mask is fine, but if patients are needing HFNC [high-flow nasal cannula] or NPPV [non-invasive positive pressure ventilation], just tube them. They definitely will need a tube anyway, and no point risking the aerosols.
No MOSF [multi-organ system failure]. There’s the mild AST/ALT elevation, maybe a small creatinine bump, but no florid failure. Exception is cardiomyopathy.
Multiple patients here have had normal EF [ejection fraction] on formal Echo or POCUS [point-of-care ultrasound] at time of admission (or in a couple of cases, EF 40ish, chronically). Also normal troponins from emergency department. Then they get the horrible respiratory failure, sans sepsis or shock. Then they turn the corner, come off Flolan, supined, vent weaning, looking good, never any pressor requirement. Then over 12 hrs, newly cold, clamped, multiple-pressor shock that looks cardiogenic, EF 10% or less. Then either VT [ventricular tachycardia, aka V-tach] → VF [ventricular fibrillation, aka V-fib] → dead, or PEA [pulseless electrical activity] → asystole in less than a day. Needless to say, this is awful for families who had started to have hope.
We have actually had more asystole than VT. Other facilities report more VT/VF, but same time course, a few days or a week after admission, around the time they’re turning the corner. This occurs on med-surg patients too. One today, who is elderly and chronically ill but with baseline EF preserved, became newly hypotensive overnight, EF <10. Already no escalation, has since passed. So presumably there is a viral cardiomyopathy aspect, which presents later in the course of disease.
Of note, no wall motion abnormalities on Echo, right ventricular function preserved, troponins don’t bump. Could be unrelated, but I’ve never seen anything like it before, especially in a patient who had been hemodynamically stable without sepsis.
TREATMENT:
Remdesivir might work, some hospitals have seen improvement with it quite rapidly, marked improvement in 1-3 days. ARDS trajectory is impressive with it, patients improve much more rapidly than expected in usual ARDS.
Recommended course is 10 days, but due to scarcity, all hospitals have stopped it when the patient is clinically out of the woods. None have continued >5 days. It might cause LFT bump, but interestingly seem to bump (200s-ish) for a day or 2 after starting, then rapidly back to normal, suggests this is not a primary toxic hepatitis.
Unfortunately, the Gilead compassionate use and trial programs require AST/ALT <5x normal, which is pretty much almost no actual COVID patients. Also CrCl [creatinine clearance] >30, which is fine. CDC is working with Gilead to get LFT requirements changed now that we know this is a mild viral hepatitis.
Currently the Gilead trial is wrapping up, NIH trial still enrolling, some new trial soon to begin, can’t remember where.
Steroids are up in the air. In China, usual clinical practice for all ARDS is high dose methylprednisolone. Thus, ALL of their patients have had high dose methylprednisolone. Some question whether this practice increases mortality.
It is likely that it increases secondary VAP/HAP [ventilator-associated pneumonia/hospital-acquired pneumonia]. China has had a high rate of drug-resistant GNR [Gram-negative rod] HAP/VAP and fungal pneumonia in these patients, with resulting increases in mortality. We have seen none, even in the earlier patients who were vented for >10 days before being bronch’ed (prior to test availability. Again, it is not a great idea to bronch these patients now).
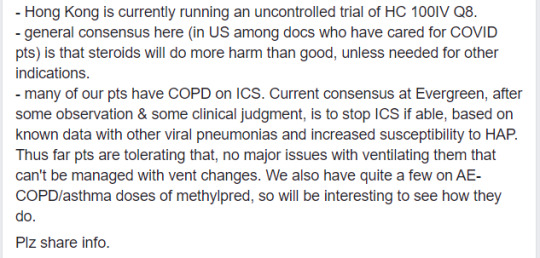
Unclear whether VAP-prevention strategies are also different [in China vs US], but wouldn’t think so?
Hong Kong is currently running an uncontrolled trial of HC 100IV Q8 [hydrocortisone 100 mg IV every 8 hours].
General consensus here (in US among doctors who have cared for COVID patients) is that steroids will do more harm than good, unless needed for other indications.
Many of our patients have COPD on ICS [inhaled corticosteroids]. Current consensus at Evergreen, after some observation & some clinical judgment, is to stop ICS if able, based on known data with other viral pneumonias and increased susceptibility to HAP. Thus far patients are tolerating that, no major issues with ventilating them that can’t be managed with vent changes. We also have quite a few on AE-COPD [acute exacerbation of COPD]/asthma doses of methylprednisolone, so will be interesting to see how they do.
8 notes
·
View notes
Text
A brief list of atrocities committed by China in recent years
You hear about the Hong Kong Protests, you’ve most likely heard of the Tienanmen Square massacre, and you probably know of the Uyghur genocide, but it goes FAR beyond just that:
This was taken from a comment made by Ender12123 on this YouTube video, credit to him for compiling this list: https://www.youtube.com/watch?v=0ebMI2xDtn4
Hundreds of human rights lawyers (not even dissidents, just the LAWYERS who defended people) were snatched by gestapo all over China in what is known as the 709 Crackdown [1].
One of those lawyers, Wang Quanzhang was sentenced to 4.5 years for "subversion of state power" [2]. But that's not enough. China actually went after Wang's 6-year-old son, forcing him out of his school and banning any other school from taking him in [3].
A dissident, known as Wang Bingzhang was kidnapped by Chinese agents in Vietnam and sentenced to life in prison after a closed trial that lasted 1 day. [4]
A man wore a t-shirt with the word "Xitler" on it and was disappeared [5]. Eventually he was tried for "subversion of state power" while barred from meeting with lawyers. [6]
Another man, Wang Meiyu hold up a placard calling for Xi’s resignation & democracy. He was arrested for "picking quarrels”. He ended up dead in custody. [7]
A woman live-streamed herself splashing ink on a Xi poster. She was disappeared [8]. Her last social media update: "Right now there are a group of people wearing uniforms outside my door. I’ll go out after I change my clothes. I did not commit a crime. The people and groups that hurt me are the ones who are guilty" [9]. Later on, there was report of her being sent to a psychiatric hospital [10]. After the ink-splash woman's disappearance her father made a series of broadcast to call attention to her plight. He ended up getting taken away by the police in the middle of a live stream. [11]
5 people associated with a Hong Kong bookstore that sold titles such as "Xi Jinping and His Six Women" were disappeared. Only one managed to escape back to HK. He held a press briefing to tell the world about his kidnapping by China. He's now in exile in Taiwan. The other 4 are still somewhere in China. [12]
And, of course 1.5 million - 3 millions Uyghurs rounded up in concentration camps [13], including leaked footage of a large number of blindfolded Uyghurs shackled together. [14]
A Canadian journalist wanted to debunk reports of Chinese anti-Muslim repression so he went on a stage-managed show tour put on by China. That means he only saw a fake Potemkin village that China actually thought was acceptable by Western standard. But the brutality of even this fake Potemkin village stunned him. Now imagine what's really happening in the real concentration camps where millions of Uyghurs are being held. Imagine how bad the true situation is. [15]
Using minorities & political prisoners as free organ farms [16]. A doctor's eye witness account: 'The prisoner was brought in, tied hand and foot, but very much alive. The army doctor in charge sliced him open from chest to belly button and exposed his two kidneys. Then the doctor ordered Zheng to remove the man’s eyeballs. Hearing that, the dying prisoner gave him a look of sheer terror, and Zheng froze. “I can’t do it,” he told the doctor, who then quickly scooped out the man’s eyeballs himself.' [17]
Call for retraction of 400 Chinese scientific papers amid fears organs came from Chinese prisoners. [18]
15 Chinese studies retracted due to fears they used Chinese prisoners' organs Cultural genocide (and organ harvests, of course). [19]
A uyghur's testimony: "First, children were stopped from learning about the Quran, then from going to mosques. It was followed by bans on ramadan, growing beards, giving Islamic names to your baby, etc. Then our language was attacked – we didn’t get jobs if we didn’t know Mandarin. Our passports were collected, we were told to spy on each other, innocent Uyghur prisoners were killed for organ harvesting" [20]
And now China is moving beyond Uyghur and cracking down on its model minority Hui Muslim. 'Afraid We Will Become The Next Xinjiang': China's Hui Muslims Face Crackdown: "The same restrictions that preceded the Xinjiang crackdown on Uighur Muslims are now appearing in Hui-dominated regions. Hui mosques have been forcibly renovated or shuttered, schools demolished, and religious community leaders imprisoned. Hui who have traveled internationally are increasingly detained or sent to reeducation facilities in Xinjiang." [21]
Along with the Uyghur and Hui Muslims, Christian churches are being closed down throughout the country, with some churches being forced to replace the Ten Commandments with quotes by Xi Jinping, and portraits of Mao Zedong as a means of forcing people to adhere to the party at all times. [22]
One church had it’s cross torn down [23], and throughout the country, Christians have been being hunted down [24].
Just like the Nazis, the Chinese are now burning books that don’t comply with the party’s stringent and intolerant ideology, most especially religious texts. [5]
And that’s just the tip of the iceberg. What is occurring in China is horrible and appaling, and big corporations continue to prop up this inhumane government, and nobody's doing anything about it, the corporations are blinded by greed that they don't see the atrocities in China.
Sources:
https://en.wikipedia.org/wiki/709_crackdown
https://www.theguardian.com/world/2019/jan/28/wang-quanzhang-china-sentences-human-rights-lawyer-to-four-years-in-prison
https://chinachange.org/2019/09/06/imprisoned-lawyer-wang-quanzhangs-six-year-old-son-once-again-forced-out-of-school/
https://en.wikipedia.org/wiki/Wang_Bingzhang_(dissident)
https://www.hongkongfp.com/2016/11/03/young-chinese-activist-missing-after-sharing-plan-to-wear-xitler-t-shirt-on-cpc-anniversary-report/
https://www.hongkongfp.com/2017/02/15/chinese-xitler-activist-trial-subversion-lawyers-barred-seeing/
https://www.theguardian.com/world/2019/sep/27/death-of-chinese-activist-in-police-custody-prompts-calls-for-investigation-into-torture
https://www.youtube.com/watch?v=V9sF34fJwh0
https://www.independent.co.uk/news/world/asia/china-woman-dong-yaoqiong-disappears-spraying-ink-xi-jinping-a8455166.html
https://www.hongkongfp.com/2018/07/23/chinese-protester-splashed-ink-xi-jinping-poster-sent-psychiatric-hospital-report/
https://www.hongkongfp.com/2018/07/14/police-interrupt-youtube-live-stream-father-missing-chinese-woman-splashed-ink-xi-jinping-photo/
https://en.wikipedia.org/wiki/Causeway_Bay_Books_disappearances
https://www.theguardian.com/world/2019/may/04/us-accuses-china-of-using-concentration-camps-uighur-muslim-minority
https://www.reddit.com/r/worldnews/comments/d722aw/chinas_detention_of_uighurs_video_of_blindfolded/
https://nationalpost.com/news/canadian-went-to-china-to-debunk-reports-of-anti-muslim-repression-but-was-shocked-by-treatment-of-uyghurs
https://www.reddit.com/r/worldnews/comments/c1my5j/china_is_harvesting_organs_from_detainees_uk/
https://nypost.com/2019/06/01/chinese-dissidents-are-being-executed-for-their-organs-former-hospital-worker-says/
https://www.theguardian.com/science/2019/feb/06/call-for-retraction-of-400-scientific-papers-amid-fears-organs-came-from-chinese-prisoners
https://www.newscientist.com/article/15-15-studies-retracted-due-to-fears-they-used-chinese-prisoners-organs/
https://www.independent.co.uk/voices/china-uyghur-muslim-rules-laws-treatment-chinese-human-rights-religion-a8534161.html
https://www.npr.org/2019/09/26/763356996/afraid-we-will-become-the-next-xinjiang-chinas-hui-muslims-face-crackdown
https://www.foxnews.com/faith-values/china-ten-commandments-church-crackdown
https://www.express.co.uk/news/world/1031890/christian-persecution-christianity-china-news
https://www.ibtimes.sg/video-after-uyghur-muslims-christians-are-being-hunted-china-bible-banned-36046
https://www.ibtimes.sg/china-just-like-nazi-germany-1930s-burning-books-35711
#china#hong kong#hong kong protests#uyghur#uyghur people#religion#christianity#islam#human rights#freedom of speech#freedom of religion#THIS IS IMPORTANT
2 notes
·
View notes
Video
Lower Creatinine level | Creatinine Treatment In Delhi | Ayurvedic Treatment In Hong Kong
Kidney diseases are that health disorder which is growing worldwide and is letting millions of people to face dangerous health-related complications. Today millions of people are undergoing dialysis on the name of chronic kidney disease treatment. But artificial procedures like kidney transplants and dialysis never became a solution to kidney disease. Such artificial procedures are found to be linked with many dangerous risk factors and can be a cause of death for a person.
The patient in the above video describes how she was trapped with artificial and chemical procedures being diagnosed with kidney disease. After searching natural kidney treatment in Hong Kong for long, the patient got to know about ayurvedic CKD treatment in India, provided by #Karma Ayurveda.
Best ayurvedic treatment
Kidney disease treatment
Kidney treatment in Hong Kong
Nephrologist Hong Kong
Acute renal failure treatments
Chronic kidney disease treatments
The patient in the above video describes that her #creatinine_level was very high. The patient was also facing the complication of proteinuria which is a health condition in which protein starts excreting out from the body with urine. The #creatinine_level of the patient which was 370mg/dl before got reduced to 334mg/dl after getting ayurvedic kidney treatment.
By curing #kidney_patients naturally, the Karma Ayurveda again proves that kidney-related disorders have natural and risk-free solutions too. People who are approaching dialysis and kidney transplant like procedures are advised to meet Dr Puneet Dhawan at Karma Ayurveda.
Follow Me Online Here:
Tumblr: https://www.tumblr.com/blog/kidneytreatmentworld
Facebook: https://www.facebook.com/Kidney-Treatment-In-India-106171384067036/
Twitter: https://twitter.com/KidneyTreatmen3
Reddit: https://www.reddit.com/user/Kidney_Treatment
Pinterest: https://in.pinterest.com/kidneytreatmenti/
Book an Appointment Helpline Number: 011-4777-2777
WhatsApp us : +91-9871712050
Karma Ayurveda Address:- G-20, N.D.M.1, PLOT NUMBER B-2,3,4 OPPOSITE N.I.M.S, NETAJI SUBASH PLACE, PITAMPURA, DELHI- 110034
#kidney treatment in india#kidney treatment in hong kong#ayurvedic treatment#ayurvedic#creatinine#lower creatinine level#Creatinine Treatment In Delhi#kidney specialist hong kong#nephrologist#ayurvedic medicines in hong kong
0 notes
Text
Lupine Publishers |Thoughts on the Reference Range of Laboratory Tests
Lupine Publishers | Current Trends on Biotechnology & Microbiology
Abstract
This article discusses the value research data in Guan’s paper published on medRxiv, February 9, 2020. In terms of experimental data, the preprinted paper is by far the largest sample number of 2019-new coronavirus (SARS-CoV-2) infected patients. Including 552 hospitals from 31 provinces in China as of January 29, 2020, a total of 1,099 cases. Laboratory evaluations include multiple blood cell counts, blood chemistry, coagulation tests, liver and kidney function, electrolytes, C-reactive protein,
Keywords: Reference range; 2019-nCoV, SARS-CoV-2, 2019-nCoV ARD, COVID-19
Introduction
Professor Guan et al. [1] recently published an article “clinical characteristics of 2019 novel coronavirus infection in china”. It is a preprinted version of medRxiv on BMJ publishing platform. The authors of the article covered all frontline anti-epidemic frontlines including Guangzhou Institute of Respiratory Disease, Wuhan Jinyintan Hospital, Institute of Hematology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, The Central Hospital of Wuhan, Huanggang Central Hospital, Department of Medicine and Therapeutics, et al. The Chinese University of Hong Kong. In this retrospective study, the authors extracted the data on 1,099 patients with laboratory-confirmed 2019-nCoV ARD (COVID-19) from 552 hospitals in 31 provinces/ provincial municipalities through January 29th, 2020. So far, it is the largest number of cases collected, the clinical characteristics of the patients with the most complete distribution, and the most comprehensive Chinese experience of SARS-CoV-2 treatment are released to the world.
In the preprinted paper, the authors found that fever occurred in only 43.8% of patients with 2019-nCoV ARD (COVID-19) but developed in 87.9% following hospitalization. Demographic data showed a median age of 47.0 years (IQR, 35.0-58.0 years). 2.09% were healthcare workers. The median incubation period was 3.0 days (range, 0 to24.0). Patients who underwent chest computed tomography on admission, 76.4% manifested as pneumonia. There are normal radiological manifestations in some infected patients. In addition, the researchers obtained a series of laboratory findings, such as 82.1% and 36.2% of patients had lymphopenia and thrombocytopenia, respectively. Overall, leukopenia was observed in 33.7% of patients. Most patients demonstrated elevated levels of C-reactive protein, rare increases in D-dimer levels, and so on. The standards used by the authors in analyzing laboratory data do not meet the standards of the People’s Republic of China’s health industry (WS/T 405-2012). We will take this article “Clinical Characteristics of New Coronavirus Infections in China 2019”as an example to explore the reference scope of laboratory test.
Methods and Results
The report delineated 1,099 patients with 2019-nCoV ARD (COVID-19) from 552 hospitals in 31 provinces/province-level municipalities. Cases were diagnosed based on the WHO interim guidance [2]. Patients were classified into severe and non-serious 2019-nCoV ARD (COVID-19) based on the guideline of the American Thoracic Society and Infectious Disease Society of America [3]. Radiologic and laboratory findings was also based on the grouping of severe and non-severe case patients. Table 1 showed lymphopenia was observed in 82.1% of patients on admission (79.3% in nonsevere cases; 95.5% in severe cases), and thrombocytopenia in 36.2% (31.6% in non-severe cases; severe cases 57.7%). Overall, leukopenia was observed in 33.7% of patients (28.1% in nonsevere cases; 61.1% in severe cases).
Hemoglobin (Hb) showed almost no significant decrease. There are significant differences of Hb level between non-serious cases and severe cases. It should be noted that only 978 of the 1099 cases provided complete blood routine test data, while the data of absolute value of lymphocytes and platelet counts were less than 978 cases. This indicating that there is no uniform requirement for the integrity of test data.
Most patients (60.7%) demonstrated elevated levels of C-reactive protein levels (56.4% in non-severe cases; 81.5% in severe cases), rare increases in alanine aminotransferase, aspartate aminotransferase, creatine kinase, and D-dimer. The authors only provided 560 cases of the D-dimer detection value, in which 46.4% patients manifest the increase tendency (43.2% in non-severe cases; 59.6% in severe cases). Severe cases had more prominent laboratory abnormalities (i.e., leukopenia, lymphopenia, thrombocytopenia, elevated C-reactive protein levels) as compared with non-severe cases (all P<0.05).
Discussion
In terms of experimental data, the preprinted paper is by far the largest sample number of 2019-new coronavirus (SARS-CoV-2) infected patients. We noticed that the author analyzed laboratory data, especially blood routine test data, and reached conclusions such as leukopenia, lymphopenia, thrombocytopenia, and elevated C-reactive protein in COVID-19 patients according to certain criteria, which is not conform to the standards of the People’s Republic of China’s health industry document WS/T405-2012.
For example, the leukopenia defined in the article is based on less than 4.0×109/L; the lymphocyte reduction is based on less than 1.5×109/L; the thrombocytopenia is based on less than 150×109/L; and the C-reactive protein level is based on be equal or greater than 10mg/L was abnormal (Table 1).
Lupinepublishers-openaccess-Agriculture
Plus-minus values are means ± SD. Lymphopenia denoted the lymphocyte count of less than 1,500 per cubic millimeter. Thrombocytopenia denoted the platelet count of less than 150,000 per cubic millimeter. PaO2:FiO2 was defined as the ratio of the partial pressure of arterial oxygen to the fraction of inspired oxygen.
P values denoted the comparison between mild-moderate cases and severe cases.
As for D-dimer, the author took greater than or be equal 0.5mg/L as the standard for abnormal. However, the different hospitals in China, the difference in methods and reagents used, it is generally considered that the reference interval is less than 0.3mg/L or less than 0.5mg/L. The article uniformly took be equal or greater than 0.5mg/L as the standard for abnormal elevation. Obviously, the 552 hospitals as the participating units are unlikely to use exactly the same methods and reagents.
Lupinepublishers-openaccess-Agriculture
The China national industry standard blood routine test reference range was released in 2012, and it has been nearly eight years. The following table lists the reference range for the analysis of venous blood in the Chinese adult population for instrumental detection methods (Table 2).The preprinted article did not adopt this health industry standard, which shows that the criterion has not been accepted and recognized by Chinese clinicians. It is a very important topic whether national industry standards, especially reference ranges, are recognized by the majority of Chinese clinicians. Reference range is the basis for clinicians diagnosing diseases.
In view of the fact that the research object is Chinese, we suggest that researchers should try to adopt the domestic recommended standards instead of using the previous concepts and foreign standards. If domestic industry standards are used in this article, their statistical results and proportions may be quite different. In particular, the absolute value of lymphocytes should be significantly different, which may lead to large differences in conclusions. As we all know, the new coronavirus epidemic recently occurred in Wuhan city, Hubei Province, China has spread to other parts of China and abroad. As an acute respiratory infectious disease, the disease has been included in the Class B infectious diseases stipulated in the Law of the People’s Republic of China on the Prevention and Control of Infectious Diseases and is managed as a Class A infectious disease. The National Health Committee of the People’s Republic of China has continuously revised the “Diagnosis and Treatment Program for Pneumonia of New Coronavirus Infection”, which is currently in its fifth edition on a trial basis. The guidelines point out that the diagnosis of suspected cases of COVID-19 should be combined with a comprehensive analysis of epidemiological history and clinical manifestations.
The clinical manifestations include
1. Fever and / or respiratory symptoms
2. The imaging characteristics of pneumonia described above (abbreviated in this article)
3. The total number of white blood cells is normal or decreased in the early stage of onset, or the lymphocyte count is decreased.
Any case with epidemiological history that meets any two of the clinical manifestations can be determined as a suspected case. Once a misdiagnosis occurs due to a misjudgment of the reference value range, it is likely to cause severe unforeseen consequences.
The biochemical test results involved in the preprint version of the article also did not adopt domestic standards, and the determination of many biochemical indicators is also related to gender, which are issues that clinicians should pay attention to. If the author team includes medical laboratory experts, I believe that the aforementioned laboratory data and reference ranges, and methodological flaw may be avoided. As stated by the authors, some cases had incomplete documentation of the exposure history, symptoms and laboratory testing given the variation in the structure of electronic database among different participating site and the urgent timeline for data extraction. Some cases were diagnosed in out-patient settings where medical information was briefly documented, and incomplete laboratory testing was applied.
On the other hand, in clinical laboratory practice, we recommend that laboratory technician communicate with clinicians to scientifically explain the clinical significance and reference range of laboratory data. Only in this way, a new reference range can be adopted and applicated in the hospital. Secondly, whether it is fully adopted or partially adopted, it depends on how technicians connect closely with the clinician and perform corresponding verification. The national industry standard is only a recommended standard, not a mandatory standard. Clinicians are generally rigorous when selecting a standard for disease diagnosis. The preprint article illustrates exactly this problem. When clinicians judge the test data, they have not adopted our health industry standards as the judgment standard. It is a typical example of the disconnection between laboratory and clinical. This is a problem worthy of laboratory physician’s reflection and deep thought.
For more Current Trends on Microbiology & Biotechnology Journal please click on below link
https://lupinepublishers.com/biotechnology-microbiology/index.php
For more Lupine Publishers Please click on below link https://lupinepublishers.com/
0 notes
Text
IoT in Healthcare Market to be Dominated by Telemedicine Segment through 2026 | TechSci Research
Rising awareness of self-health monitoring and the government initiatives promoting digital health is expected to drive the demand for global IoT in healthcare market in the forecast period.

According to TechSci Research report, “IoT in Healthcare Market - Global Industry Size, Share, Trends, Opportunity and Forecast, 2016-2026 Segmented By Component (Medical Devices, System and Software, Services), By Medical Devices (Stationery Medical Devices, Implants, Wearables), By System and Software (Remote Device Management, Data Analytics, Application Security and Others), By Services (Managed Services, Professional Services), By Application (Telemedicine, Remote Patient Monitoring, Clinical Operations and Workflow Management, Connected Imaging and Others), By End-User (Hospitals and Clinics, Clinical Research Centres and Diagnostic Labs) and By Region”, the global IoT in healthcare market is expected to grow at an impressive CAGR for the forecast period, 2022-2026.
Healthcare institutions are introducing the internet of things technology to improve and enhance patient monitoring services and reduce the costs to provide effective healthcare services. The growing demand for the reduction of the waiting time in emergency rooms to address patients requiring immediate healthcare services is contributing to the global IoT in healthcare market growth.
However, the increasing concerns of data security and cyber-attacks may restrain the global IoT in healthcare market growth for the forecast period.
Browse XX Figures spread through XX Pages and an in-depth TOC on "Global IoT in Healthcare Market”.
https://www.techsciresearch.com/report/iot-in-healthcare-market/7836.html
Global IoT in healthcare market is segmented into component, application, end-user, regional distribution, and company. Based on the component, the market can be divided into medical devices, system and software, and services. The medical devices segment is dominating the market and is expected to hold a major market share for the forecast period, 2022-2026. The medical devices segment is further segmented into stationery medical devices, implants, and wearables. With the growing adoption of internet of things technology by the healthcare institutions and the rise in the dependency on connected medical devices such as stationery medical devices, wearable devices, implantable for monitoring the health condition of patients is expected to drive the medical devices segment growth for the predicted period.
Based on the application, the market can be divided into telemedicine, remote patient monitoring, clinical operations and workflow management, connected imaging, and others. The telemedicine segment is expected to witness significant growth for the next five years. High penetration of affordable internet services and the proliferation of smart devices is expected to demand of telemedicine segment across the globe for the next five years. The growing penetration of home healthcare services and the surging need to improve the accessibility and reach of healthcare services in remote locations are influencing the growth of the segment.
Based on the end-user, the market is segmented into hospitals and clinics, clinical research centers, and diagnostic labs. The hospitals and clinics segment are expected to account for a major market share for the next five years. The rise in the adoption of IoT-enabled medical devices among healthcare facilities to provide quality healthcare treatment to patients is expected to fuel the demand of the hospitals & clinics segment all over the world. To provide the personalized healthcare treatment by the adoption of connected devices and the presence of skilled doctors and specialized departments in hospitals & clinics is expected to boost the segment demand.
Medtronic, Inc., Koninklijke Philips N.V., General Electric Company, IBM Corporation, Microsoft Corporation, Cerner Corporation, AgaMatrix Hong Kong Ltd, Cisco Systems, Inc., GE Healthcare, Huawei Technologies, Intel Corporation, Siemens Healthcare GmbH, AdhereTech, Inc., Bosch Healthcare Solutions GmbH, SAP SE are the leading players operating in global IoT in healthcare market. Service providers are increasingly focusing on research and development process to fuel higher growth in the market. To meet evolving customer demand with respect to better efficiency and durability, several IoT in healthcare service providers are coming up with their technologically advanced offerings.
Download Sample Report @ https://www.techsciresearch.com/sample-report.aspx?cid=7836
Customers can also request for 10% free customization on this report.
“Market players are making high-end investments for research and development activities for the technological up-gradation of the existing healthcare IT infrastructure and introduce innovative features like generating notifications in case of potential system malfunction to take appropriate steps is expected to fuel the growth of the market. The adoption of the latest technologies such as artificial intelligence, deep learning, machine learning, and others to improve the operational efficiency, predict enhancement, facilitate automation and the surge in the use of connected technology to efficiently manage the operational workflow, as well as the clinical tasks, is expected to propel the global IoT in healthcare market growth till 2026” said Mr. Karan Chechi, Research Director with TechSci Research, a research based global management consulting firm.
“IoT in Healthcare Market - Global Industry Size, Share, Trends, Opportunity and Forecast, 2016-2026 Segmented By Component (Medical Devices, System and Software, Services), By Medical Devices (Stationery Medical Devices, Implants, Wearables), By System and Software (Remote Device Management, Data Analytics, Application Security and Others), By Services (Managed Services, Professional Services), By Application (Telemedicine, Remote Patient Monitoring, Clinical Operations and Workflow Management, Connected Imaging and Others), By End-User (Hospitals and Clinics, Clinical Research Centres and Diagnostic Labs) and By Region” has evaluated the future growth potential of global IoT in healthcare market and provided statistics & information on market size, shares, structure and future market growth. The report intends to provide cutting-edge market intelligence and help decision makers take sound investment decisions. Besides, the report also identifies and analyzes the emerging trends along with essential drivers, challenges, and opportunities in the of global IoT in healthcare market.
Browse Related Reports:
Organ-on-Chip Market - Global Industry Size, Share, Trends, Opportunity and Forecast, 2016-2026 Segmented By Type (Liver, Heart, Lung, Kidney, Others), By Offering (Products v/s Services), By Material Type (Polymer, PDMS, Glass, Silicon, Others), By Application (Physiological Model Development, Drug Discovery, Toxicological Research, Molecular Biology, Others), By End User (Pharmaceutical & Biotechnology Companies, Academic & Research Institutes, Cosmetic Industry, Others), By Region
https://www.techsciresearch.com/report/organ-on-chip-market/7763.html
Global Real Time PCR Market By Product (Instruments, Reagents & Consumables, Software & Services), By Application (Clinical (Pathogen Testing, Blood Screening, Oncology Testing), Research, Forensic, Others), By End-user (Hospitals & Diagnostic Labs, Research Laboratories & Academic Institutes, Pharma-Biotech, Clinical Research Organizations (CRO), Forensic Laboratories, Others), By Region, Competition, Forecast & Opportunities, 2025
https://www.techsciresearch.com/report/real-time-pcr-market/4713.html
Contact
Mr. Ken Mathews
708 Third Avenue,
Manhattan, NY,
New York – 10017
Tel: +1-646-360-1656
Email: [email protected]
Website: https://www.techsciresearch.com/
For More Market Research Blogs Visit: https://techsciblog.com/
#TechSci#Market Research Reports#Global IoT in Healthcare Market#IoT#IoT in Healthcare Market#IoT in Healthcare Market Size#ICT#IoT in Healthcare Market Forecast
0 notes
Text
IoT in Healthcare Market to be Dominated by Telemedicine Segment through 2026 | TechSci Research
Rising awareness of self-health monitoring and the government initiatives promoting digital health is expected to drive the demand for global IoT in healthcare market in the forecast period.

According to TechSci Research report, “IoT in Healthcare Market - Global Industry Size, Share, Trends, Opportunity and Forecast, 2016-2026 Segmented By Component (Medical Devices, System and Software, Services), By Medical Devices (Stationery Medical Devices, Implants, Wearables), By System and Software (Remote Device Management, Data Analytics, Application Security and Others), By Services (Managed Services, Professional Services), By Application (Telemedicine, Remote Patient Monitoring, Clinical Operations and Workflow Management, Connected Imaging and Others), By End-User (Hospitals and Clinics, Clinical Research Centres and Diagnostic Labs) and By Region”, the global IoT in healthcare market is expected to grow at an impressive CAGR for the forecast period, 2022-2026.
Healthcare institutions are introducing the internet of things technology to improve and enhance patient monitoring services and reduce the costs to provide effective healthcare services. The growing demand for the reduction of the waiting time in emergency rooms to address patients requiring immediate healthcare services is contributing to the global IoT in healthcare market growth.
However, the increasing concerns of data security and cyber-attacks may restrain the global IoT in healthcare market growth for the forecast period.
Browse XX Figures spread through XX Pages and an in-depth TOC on "Global IoT in Healthcare Market”.
https://www.techsciresearch.com/report/iot-in-healthcare-market/7836.html
Global IoT in healthcare market is segmented into component, application, end-user, regional distribution, and company. Based on the component, the market can be divided into medical devices, system and software, and services. The medical devices segment is dominating the market and is expected to hold a major market share for the forecast period, 2022-2026. The medical devices segment is further segmented into stationery medical devices, implants, and wearables. With the growing adoption of internet of things technology by the healthcare institutions and the rise in the dependency on connected medical devices such as stationery medical devices, wearable devices, implantable for monitoring the health condition of patients is expected to drive the medical devices segment growth for the predicted period.
Based on the application, the market can be divided into telemedicine, remote patient monitoring, clinical operations and workflow management, connected imaging, and others. The telemedicine segment is expected to witness significant growth for the next five years. High penetration of affordable internet services and the proliferation of smart devices is expected to demand of telemedicine segment across the globe for the next five years. The growing penetration of home healthcare services and the surging need to improve the accessibility and reach of healthcare services in remote locations are influencing the growth of the segment.
Based on the end-user, the market is segmented into hospitals and clinics, clinical research centers, and diagnostic labs. The hospitals and clinics segment are expected to account for a major market share for the next five years. The rise in the adoption of IoT-enabled medical devices among healthcare facilities to provide quality healthcare treatment to patients is expected to fuel the demand of the hospitals & clinics segment all over the world. To provide the personalized healthcare treatment by the adoption of connected devices and the presence of skilled doctors and specialized departments in hospitals & clinics is expected to boost the segment demand.
Medtronic, Inc., Koninklijke Philips N.V., General Electric Company, IBM Corporation, Microsoft Corporation, Cerner Corporation, AgaMatrix Hong Kong Ltd, Cisco Systems, Inc., GE Healthcare, Huawei Technologies, Intel Corporation, Siemens Healthcare GmbH, AdhereTech, Inc., Bosch Healthcare Solutions GmbH, SAP SE are the leading players operating in global IoT in healthcare market. Service providers are increasingly focusing on research and development process to fuel higher growth in the market. To meet evolving customer demand with respect to better efficiency and durability, several IoT in healthcare service providers are coming up with their technologically advanced offerings.
Download Sample Report @ https://www.techsciresearch.com/sample-report.aspx?cid=7836
Customers can also request for 10% free customization on this report.
“Market players are making high-end investments for research and development activities for the technological up-gradation of the existing healthcare IT infrastructure and introduce innovative features like generating notifications in case of potential system malfunction to take appropriate steps is expected to fuel the growth of the market. The adoption of the latest technologies such as artificial intelligence, deep learning, machine learning, and others to improve the operational efficiency, predict enhancement, facilitate automation and the surge in the use of connected technology to efficiently manage the operational workflow, as well as the clinical tasks, is expected to propel the global IoT in healthcare market growth till 2026” said Mr. Karan Chechi, Research Director with TechSci Research, a research based global management consulting firm.
“IoT in Healthcare Market - Global Industry Size, Share, Trends, Opportunity and Forecast, 2016-2026 Segmented By Component (Medical Devices, System and Software, Services), By Medical Devices (Stationery Medical Devices, Implants, Wearables), By System and Software (Remote Device Management, Data Analytics, Application Security and Others), By Services (Managed Services, Professional Services), By Application (Telemedicine, Remote Patient Monitoring, Clinical Operations and Workflow Management, Connected Imaging and Others), By End-User (Hospitals and Clinics, Clinical Research Centres and Diagnostic Labs) and By Region” has evaluated the future growth potential of global IoT in healthcare market and provided statistics & information on market size, shares, structure and future market growth. The report intends to provide cutting-edge market intelligence and help decision makers take sound investment decisions. Besides, the report also identifies and analyzes the emerging trends along with essential drivers, challenges, and opportunities in the of global IoT in healthcare market.
Browse Related Reports:
Organ-on-Chip Market - Global Industry Size, Share, Trends, Opportunity and Forecast, 2016-2026 Segmented By Type (Liver, Heart, Lung, Kidney, Others), By Offering (Products v/s Services), By Material Type (Polymer, PDMS, Glass, Silicon, Others), By Application (Physiological Model Development, Drug Discovery, Toxicological Research, Molecular Biology, Others), By End User (Pharmaceutical & Biotechnology Companies, Academic & Research Institutes, Cosmetic Industry, Others), By Region
https://www.techsciresearch.com/report/organ-on-chip-market/7763.html
Global Real Time PCR Market By Product (Instruments, Reagents & Consumables, Software & Services), By Application (Clinical (Pathogen Testing, Blood Screening, Oncology Testing), Research, Forensic, Others), By End-user (Hospitals & Diagnostic Labs, Research Laboratories & Academic Institutes, Pharma-Biotech, Clinical Research Organizations (CRO), Forensic Laboratories, Others), By Region, Competition, Forecast & Opportunities, 2025
https://www.techsciresearch.com/report/real-time-pcr-market/4713.html
Contact
Mr. Ken Mathews
708 Third Avenue,
Manhattan, NY,
New York – 10017
Tel: +1-646-360-1656
Email: [email protected]
Website: https://www.techsciresearch.com/
For More Market Research Blogs Visit: https://techsciblog.com/
#TechSci#Market Research Reports#Global IoT in Healthcare Market#ICT#IoT in Healthcare Market#IoT in Healthcare Market Size#IoT in Healthcare Market Forecast
0 notes
Last Seen Blogs




