#polysome
Photo

#ribosomes#single#mRNA#multiple#copies#polypeptide#plastidome#polyhedral#bodies#polysome#nucleosome#science#solutions
1 note
·
View note
Text
Novos Baianos - Acabou Chorare (1972)
Reedição da Polysom de 2010, com selo da Som Livre.
#novosbaianos#mpb#lp#vinil#vinyl#vinylcollection#vinyllover#vintage audio#turntable#sony#asmr#asmr video
3 notes
·
View notes
Text
poured sucrose gradients to three cheers for sweet revenge this morning now my polysomes are gonna be transgender. great
10 notes
·
View notes
Text

09.22 and 09.23.22
days 31 and 32 of 100
currently how my screen's looking like these days -- class recording and the reference book for the subject to compare the infos while taking down notes
— thursday, 09.22 —
studied on artificial airways
practiced Mandarin
studied on patient flow process for polysom
attended PE lecture
studied for friday's TPF long quiz
— friday, 09.23 —
started my morning reviewing for the long quiz for TPF again while eating breakfast
took TPF long quiz
attended lecture for TPF after the quiz (in which our prof also gave the coverage of our exam)
compiled all our quizzes this prelims in a document to print and answer as a form of review
made notes on pneumonia
#r ene#r-ene#respiratory student#respiratory therapy major#respiratory therapy#respiratory therapy student#respiratory#studyblr#study#studies#student#student life#studentlife#students#study blog#study challenge#study community#study inspiration#study inspo#study life#study mood#study motivation#study notes#study session#study space#study tumblr#study with me#studyblr community#studying#studyinspo
5 notes
·
View notes
Text
Loss of ADAR1 protein induces changes in small #RNA landscape in hepatocytes [Article]
In recent years, numerous evidence has been accumulated about the extent of A-to-I editing in human RNAs and the key role ADAR1 plays in the cellular editing machinery. It has been shown that A-to-I editing occurrence and frequency are tissue specific and essential for some tissue development, such as liver. To study the effect of ADAR1 function in hepatocytes, we have created Huh7.5 ADAR1 KO cell lines. Upon IFN treatment, the Huh7.5 ADAR1 KO cells show rapid arrest of growth and translation, from which they do not recover. We analyzed translatome changes by employing a method based on sequencing of separate polysome profile RNA fractions. We found significant changes in transcriptome and translatome of the Huh7.5 ADAR1 KO cells. The most prominent changes include negatively affected transcription by RNA polymerase III and the deregulation of snoRNA and Y RNA levels. Furthermore, we observed that ADAR1 KO polysomes are enriched in mRNAs coding for proteins pivotal in a wide range of biological processes such as RNA localization and RNA processing, whereas the unbound fraction is enriched mainly in mRNAs coding for ribosomal proteins and translational factors. This indicates that ADAR1 plays more relevant role in small RNA metabolism and ribosome biogenesis. http://rnajournal.cshlp.org/cgi/content/short/rna.080097.124v1?rss=1&utm_source=dlvr.it&utm_medium=tumblr
0 notes
Text
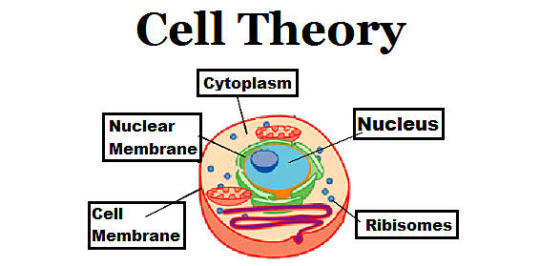
Cell theory
▪️Cell Theory:
• Schleiden and Schwann
▪️“Omnis cellula-e-cellula”
: Rudolf Virchow
▪️Coined the term ‘cell’
: Robert Hooke
▪️First person to see live cells under microscope:
• Anton Van
• Leeuwenhoek
▪️Smallest cell
: Mycoplasma (0.3µm)
▪️Mesosome:
• Infolding of plasma membrane in prokaryotesvesicles, tubules or lamellae
• Help in DNA replication and cell wall formation
▪️Cell envelope:
• In prokaryotic cells
• Made up of glycocalyx (slime
or capsule), cell wall and plasma membrane
▪️Plasmid
• Extra chromosomal, circular DNA in prokaryotic cells
▪️Pili and Fimbriae
• Help bacteria in attachment
▪️Prokaryotic ribosomes:
• 70S (50S and 30S)
• Polysome- several ribosomes attached to mRNA for protein synthesis
▪️Bacterial Cell wall:
• G +ve bacteria- Thick peptidoglycan and teichoic
acid
• G -ve bacteria- Thin peptidoglycan and lipopolysaccharides
▪️Peptidoglycan:
• Polymer of Cross linked monomers - Nacetylglucosamine (NAG)
• N-acetylmuramic acid (NAM) attached to peptide
▪️Fluid mosaic model:
• Singer and Nicolson
▪️Endoplasmic reticulum:
• Rough ER- Protein synthesis
• Smooth ER- Lipid synthesis
▪️Golgi Complex:
• Synthesis of glycoproteins and glycolipids
▪️Tonoplast:
• A single membrane surrounding vacuoles
Plastids
• Double membrane bound and contain extra
chromosomal DNA, 70S ribosomes
▪️Mitochondria:
• Double membrane bound and contain extra
chromosomal circular DNA, 70S ribosomes.
• Site for aerobic respiration.
▪️Leucoplasts:
• Amyloplast- store carbohydrate
• Elaioplast- store oil and fat
• Aleuroplast- store proteins
▪️Observed ribosomes for the first time:
• George Palade
▪️Eukaryotic ribosome
•80S (60S and 40S):
▪️Robert Brown:
• First described nucleus
▪️Nucleolus:
• Site for ribosomal
• RNA synthesis
• Chromatin is visible at
Interphase nucleus
▪️Lysosomes:
• Contain hydrolytic enzymes
▪️Glyoxysomes
• Present in plants and some fungi
• Degradation of fats in seeds
• Glyoxalate cycle
▪️Peroxisomes
• Oxidation of long chain fatty acids
• Biosynthesis of plasmalogens
• Contains oxidative enzymes; uric acid oxidase, catalase, etc.
0 notes
Text
Global Assessment of Protein Translation in Mammalian Cells Using Polysome Fractionation
Pubmed: http://dlvr.it/SnzkRx
0 notes
Text
Understanding Basics of Polysomnography and Sleep Testing Billing
Basics of Polysomnography and Sleep Testing
About 40 million people in the United States suffer from sleep problems every year. Not getting enough sleep for a long time can cause health problems. Many sleep disorders can be managed by primary care physicians; however, when abnormal sleep patterns are not easily explainable and further evaluation is necessary, expert opinion and sleep studies may be needed. Polysomnography (PSG) refers to the continuous and simultaneous monitoring and recording of various physiological and pathophysiological parameters of sleep furnished in a sleep laboratory facility that includes physician review, interpretation and report. A technologist supervises the recording during sleep time and has the ability to intervene, if needed. The studies are performed to diagnose a variety of sleep disorders and to evaluate a patient’s response to therapies such as continuous positive airway pressure (CPAP). As a primary care physician, to get an accurate reimbursement, lets understand basics of Polysomnography and Sleep Testing billing.
Polysomnography and Sleep Testing Coding
Some of the commonly used CPT codes for Polysomnography and Sleep Testing are as mentioned below. These CPT codes are covered by Medicare (with proper documentation), you can check payer specific reimbursement guidelines for exact coverage.
Non-attended sleep studies should be billed with the CPT/HCPCS code that most accurately describes the service.
CPT code 95811 alone should be billed for split night studies as CPT code 95811 in this instance is inclusive of CPT code 95810. (Polysomnography; age 6 years or older, sleep staging with 4 or more additional parameters of sleep, attended by a technologist)
For a study to be reported as polysomnography (PSG), sleep must be recorded and staged and directly attended by a qualified technologist. Report with modifier 52 if less than 6 hours of recording or in other cases of reduced services.
CPT codes 95782, 95783, 95808, 95810, and 95811 include sleep staging. Medicare would not expect to see separate billings for an EEG, EOG, and/or EMG in addition to these codes.
CPT code 95808 includes reimbursement for one to three additional parameters. CPT codes 95782, 95783, 95810 and 95811 include four or more additional parameters. Therefore, Medicare would not expect to see separate billings for additional parameters in addition to codes 95782, 95783, 95808, 95810, or 95811. Additional parameters of sleep include:
ECG
Airflow
Ventilation and respiratory effort
Gas exchange by oximetry, transcutaneous monitoring or end tidal gas analysis
Extremity muscle activity and motor activity movement
Extended EEG monitoring
Penile tumescence
Gastroesophageal reflux
Continuous blood pressure monitoring
Snoring
Body positions
Documentation Requirements
All documentation must be maintained in the patient’s medical record and made available to the contractor upon request.
Every page of the record must be legible and include appropriate patient identification information (e.g., complete name, dates of service[s]). The documentation must include the legible signature of the physician or non-physician practitioner responsible for and providing the care to the patient.
The submitted medical record must support the use of the selected ICD-10-CM code(s). The submitted CPT/HCPCS code must describe the service performed.
An order from the treating physician/nonphysician practitioner as required by CFR, Title 42, Volume 2, Chapter IV, Part 410.21 (a) Ordering diagnostic tests.
When billing for a sleep disorder test, the ordering physician’s NPI must be indicated on the claim form and the order kept on record.
Documentation must support that the accreditation, credentialing, and training requirements as stated in the LCD were met for the clinic, technologist, and physician.
Applicable CPT Code
Group 1 Codes
95782: Polysom <6 yrs 4/> paramtrs
95783: Polysom <6 yrs cpap/bilvl 95807: Sleep study attended 95808: Polysom any age 1-3> param
95810: Polysom 6/> yrs 4/> param
Group 2 Codes
95811: Polysom 6/>yrs cpap 4/> parm
Group 3 Codes
95805: Multiple sleep latency test
Group 4 Codes
95800: Slp stdy unattended
95801: Slp stdy unatnd w/anal
95806: Sleep study unatt&resp efft
G0398: Home sleep test/type 2 porta
G0399: Home sleep test/type 3 porta
G0400: Home sleep test/type 4 porta
Evaluation and Management (E/M) Codes
Sleep physicians also use Evaluation and Management (E/M) codes to bill for office visits. Evaluation and management codes are restricted to physicians and other qualified advanced nurse practitioners (NPs, PAs, etc.). Technologists cannot bill independently but they can bill incident to the physician (if certain guidelines are followed).
99202: Level 2 new patient office visit
99203: Level 3 new patient office visit
99204: Level 4 new patient office visit
99205: Level 5 new patient office visit
99211: Level 1 established patient office visit
99212: Level 2 established patient office visit
99213: Level 3 established patient office visit
99214: Level 4 established patient office visit
99215: Level 5 established patient office visit
Legion Health Care Solutions is a leading medical billing company providing complete billing and coding services to ensure accurate insurance reimbursement for your practice. We shared basics of Polysomnography and Sleep Testing billing for physician reference, for accurate insurance coverage and applicable procedure codes, refer to payer specific billing guidelines and reimbursement policies. To know more about our primary care billing and coding services, contact us at 727-475-1834 or email us at [email protected]
0 notes
Text
Grape seed extract uses
Grape seed extract uses Because grape seeds contain polyphenols (GPS), mainly catechins and Procyanidins classes. Catechin compounds include catechins, epicatechin and their gallate, which are the main monomers in grape seeds and the constituent units of proanthocyanidin oligomers and polysomes.
website:https://btncbio.com/grape-seed-extract-uses/
0 notes
Text
sensitive white boy runs worlds worst polysome profile
0 notes
Text
XYYY Pride Flag

48,XYYY syndrome: a rare Y trisomic (chromosome number) condition characterized by mild-moderate developmental delay (especially speech), normal to mild intellectual disability, large, irregular teeth with poor enamel, tall stature and acne. Radioulnar stenosis and clinodactyly have also been associated. Children generally present typical genitalia, while hypogonadism and infertility is frequently reported in adults.
-ap
#disomy#quadrisomy#tetrasomy#trisomy#trisome#poly-y#polysome#polysomy#disabled#disability#rare disease#48 XYYY syndrome#chromosomes#chromosomy#multisomy#intersex#pride flag#mogai#lgbti#lgbtqi#lgbtiq#tetrasomal#anomaly#karyotype#trisomal#infertile#Hypogonadism
38 notes
·
View notes
Text
did you guys ever do that thing as a kid where you put like oil and water and honey in a glass and float different objects on different layers. Like some things will sink through the oil and not the water and some things will only float on the honey. like this

Well did you know you can extract all the translating ribosomes from a cell and do this and figure out how many are on each piece of RNA based on how high they float. And separate RNAs by how many ribosomes are actively translating them
https://en.m.wikipedia.org/wiki/Polysome_profiling
7 notes
·
View notes
Text


09.14 to 09.17
days 23 to 27 of 100
i don't look like it but as the week goes on, my stress level is also going on (up), so we're just getting straight to the productivity list hahaha
exam's on the last week of the month and it's face to face, so I guess adding to the usual academic stress is me thinking about what time I'll be leaving the house and my commute to uni etc, etc. (ig thank u nct 127 & bp for the comeback to ease some stress haha)
anw, here's a bit condensed productivity list for most of the week:
attended all lecture classes for the week
thankfully got done making my reviewers for polysom, airway management and research
had an activity for airway management that required us to write things down as a form of review
watched all asynch videos for artificial airways again
made notes for PDM on status asthmaticus (only need to accomplish my notes on COPD and bronchiectasis to get done with my reviewer)
3/4 complete with my TPF reviewer
had a PFT interpretation activity
made a study plan for these 12 days before exams
accomplished all my minor subject activities (personal reflections, work out videos, essays, etc etc)
having a bit of trouble with stress management but I'll work on it bit by bit before it manifests physically, haha, but I've been such a neat freak these days and that's a sign especially when I would start to make a mess intentionally just to have to clean something up, hahaha
have a good weekend everyone !
#r ene#r-ene#respiratory student#respiratory therapy major#respiratory therapy student#respiratory therapy#studyblr#study#studies#student#student life#studentlife#studentmemes#study blog#study challenge#study community#study hard#study inspiration#study life#study mood#study motivation#study session#study spot#study tumblr#study with me#studyblr community#studying#studystudystudy#studywithme#uni student
5 notes
·
View notes
Text
Compartment-specific and ELAVL1-coordinated regulation of intronic polyadenylation isoforms by doxorubicin [RESEARCH]
Intronic polyadenylation (IPA) isoforms, which contain alternative last exons, are widely regulated in various biological processes and by many factors. However, little is known about their cytoplasmic regulation and translational status. In this study, we provide the first evidence that the genome-wide patterns of IPA isoform regulation during a biological process can be very distinct between the transcriptome and translatome, and between the nucleus and cytosol. Indeed, by 3'-seq analyses on breast #cancer cells, we show that the genotoxic anti#cancer drug, doxorubicin, preferentially down-regulates the IPA to the last-exon (IPA:LE) isoform ratio in whole cells (as previously reported) but preferentially up-regulates it in polysomes. We further show that in nuclei, doxorubicin almost exclusively down-regulates the IPA:LE ratio, whereas in the cytosol, it preferentially up-regulates the isoform ratio, as in polysomes. Then, focusing on IPA isoforms that are up-regulated by doxorubicin in the cytosol and highly translated (up-regulated and/or abundant in polysomes), we identify several IPA isoforms that promote cell survival to doxorubicin. Mechanistically, by using an original approach of condition- and compartment-specific CLIP-seq (CCS-iCLIP) to analyze ELAVL1-#RNA interactions in the nucleus and cytosol in the presence and absence of doxorubicin, as well as 3'-seq analyses upon ELAVL1 depletion, we show that the #RNA-binding protein ELAVL1 mediates both nuclear down-regulation and cytosolic up-regulation of the IPA:LE isoform ratio in distinct sets of genes in response to doxorubicin. Altogether, these findings reveal differential regulation of the IPA:LE isoform ratio across subcellular compartments during drug response and its coordination by an #RNA-binding protein. http://genome.cshlp.org/cgi/content/short/32/7/1271?rss=1&utm_source=dlvr.it&utm_medium=tumblr
0 notes
Text
Honestly after reading so many studies of how lack of sleep will Literally Kill You or cause severe damage to your brain or increase you risk of certain diseases i r cringe at my sLEeP iS FoR tHE WEaK attitude i had when i was younger like.
hating sleep / bragging about sleeping issues / insomnia is such a strange trend and is kinda embarrassing and ignorant ngl
#shutuplanx#polysom#i also highly recommend anyone interested in this topic to look it up!#sleep is v important!! and lack of sleep during your life has been linked to Alzheimer's and other diseases#its interesting how little we know about something every animal (and eVEN PLANTS) does at some point or another#and us! we sleep every day but we know so little
0 notes
Last Seen Blogs

askkingnazoxqueenclara97
Ask Nazoxclara

kenntolog
‘escape from reality…’

zakazaniepacks
@zakazanie

mostly-funnytwittertweets
previously funnytwittertweets

fluffyartbl0g
Yo I Do Art :D