#survivingpsych
Text
tired of medication positivity posts that assume everyone has a positive relationship with medication
here’s to people who don’t take medication that their doctors want them to take. here’s to people who get marked noncompliant. here’s to people who get sectioned or hospitalized bc they won’t take their meds. here’s to people who self-medicate w nonprescription drugs. here’s to the people in withdrawal. here’s to the people who would rather deal with their symptoms than medication side effects. here’s to the “treatment-resistant” people who have never found medication that helps at all. here’s to the people who are only on meds nonconsensually. here’s to people who refuse meds for “irrational” or “stupid” reasons. here’s to people for whom taking meds is a trauma trigger. here’s to people who are disabled from past medications. here’s to people who are constantly being pressured into taking meds they don’t want and having to defend their “no” over and over again
yes, lots of people need their meds. yes, meds can be important. but don’t forget us
fuck everyone who calls us anti-science or anti-recovery. who says we are hurting other ppl by talking about our choices. bodily autonomy includes the right to say NO. even to medical treatment.
#therapists dni#psychiatry tag#survivingpsych#fwiw I TAKE MULTIPLE LIFE SAVING MEDICATIONS#i am not trying to shame ppl who do! or deny that meds are important!#but like. as an unmedicated by choice schizo#it’s hard out here. with the medical trauma and so forth
4K notes
·
View notes
Text
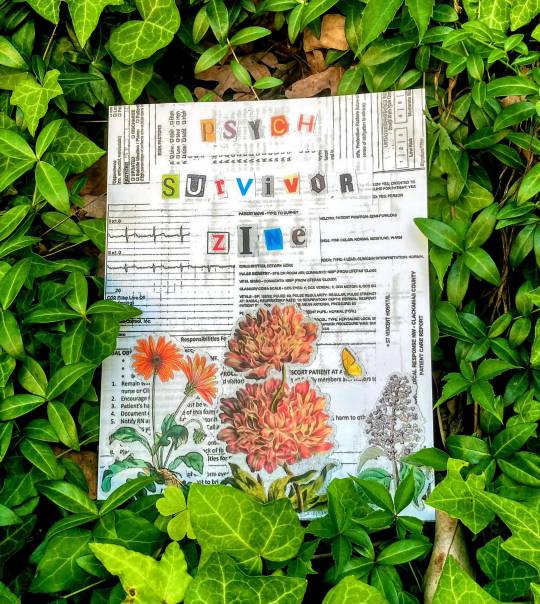
Image description: [ a photo of the Psych Survivor zine in a bush of ivy. The cover is a collage made out of medical records, vintage flower drawings, and magazine letters spelling “psych survivor zine".]
Hello everyone! I am so thrilled to announce the launch of the psych survivor zine, now available to download on www.psychsurvivorarchive.com.
A little bit about this project:
The Psych Survivor Archive is an abolitionist organization deeply invested in mad liberation and cross-movement organizing.
We host two projects: the Psych Survivor Zine and the Digital Story Archive. The Psych Survivor Zine celebrates Mad art in volumes released twice a year, with thematic prompts for each edition. The Digital Story Archive is a more informal forum for psych survivors to write about our lives and share as much as we want, when we want, how we want.
Through this archive, I hope to create a platform where psych survivors are believed and the psych system is held accountable for the ways it has harmed us. Our pain, resistance, knowledge, and grief are worth listening to, and I offer up this archive as a communal method of bearing witness.
This space is for the imperfect crazy person, the noncompliant patient, those of us who trash our rooms in the psych ward and yell to ourselves on the street. This space is for our comrades still incarcerated in all kinds of institutions and prisons. This space is for anyone who has been harmed by the psychiatric system and wants to rage about it–and this space is for anyone who doesn’t have the words to talk about it.
This space is for you.
You can download a pdf and an image described pdf for free on the website, or order a physical copy! This zine is incredible-featuring artwork by 13 different Mad artists, the 55 page zine includes collages, poems, harm reduction toolkits, and more!!
Artists include @kihnindewa, @bioethicists, @gothhabiba and @librarycards, among many more!
This project has been really vulnerable and cathartic with me, and I am so excited to share it with you. Feel free to explore the website, submit your story, and check out our resource guide.
#personal#psych survivor#survivingpsych#antipsych#psych abolition#mad liberation#mad pride#psych survivor zine#disability#really really happy with this.#disability pride month#also if i tagged you and you don't want to be tagged pls let me know! i don't know who else from the project is on tumblr#mad punk
871 notes
·
View notes
Text
A Mad Exercise:
“patient exhibits black-and-white thinking, cognitive rigidity, catastrophizing tendencies, delusions of persecution, paranoia, excessive preoccupation with order, restraint, and productivity; debilitating anxiety, existential dread.”*
consider the irony of these pathologizing statements, generally attached to a constellation of diagnoses designed to discredit the affective/intellectual/social orientations of the Patient. To locate the irony (and tear out the rug) think with the following questions:
Ask: in whose interest is it to pathologize these particular reactions to the social conditions under which we live?
Ask: What are the demographics of the patients receiving damning diagnoses for these ways of relating to the world (what genres of rigidity, anxiety, paranoia, depression, scrupulously, and “delusionality” go un/marked?)
Ask: if we can see the trajectory from “need to brute-force psychopathology on those whose objection to the world as it exists” to “must eliminate those who raise said objections via epistemic violence, incarceration, abandonment, and murder”, then what can we learn, broadly about the carceral function of the category of “mental illness” and in particular the institution of diagnosis?
Then, get Mad.
*these are some selections from the myriad terms used to talk about / around / against “me” (as it were) by the psy industry. Feel free to replace with those applicable to you.
239 notes
·
View notes
Text
doctors, therapists, psychiatrists etc need to understand that many of us do not want to live forever. we do not want to "become our best selves". we do not want to optimize our lives. we just want to be ok. we just want to live.
i am not trying to take away the things i love, the things that give me small joy, i am not trying to spend my life going from doctor to doctor so that i can make my body and mind more efficient. so that i can make myself better. i am not a machine. i am ok as i am. i just want to feel ok. i just want to not be in pain. i just want to live.
#i think the whole becoming your best self and living as long as possible is a rich people thing#that doctors now assume every person wants#anyways#ok to rb#survivingpsych
116 notes
·
View notes
Text
Maybe if neurotypical people didn't make up the majority of employees in the mental healthcare industry,
AND ❄️NeUrOtYpiCaL❄️ people didn't viscerally misunderstand neurodiversity,
They wouldn't commit hate crimes against mentally ill people at work
AND/OR
They wouldn't traumatize mentally ill people leading to them never wanting their "care" again
Or would that be under their thumb🤔🤔 is it against the rules? Do I have the right to remain silent?
Do I still get the rights if they rewrite the rules?!
Just kidding byeeeeeee;)
#survivingpsych#psychiatry#uhhh psychiatric state violence assuming thats in the DSM?#or would that be on the books#Oh well they already booked me#good game nice move keep me in check then#and FUCK you🎭
93 notes
·
View notes
Text
probably going back to E///D inpatient, potentially as early as before Xmas. So that's fucking fun. Last time I was there they wouldn't let me outside for over a month because of my ""noncompliance"". I might be in SEED protocol this time (even though I don't meet the definition? I'm almost 30 but I've only had it 4 yrs. IDK why they said that so 🤞) so hopefully they'll be willing to give the barest accommodations to my other disabilities. Last time I had to advocate for myself to be able to... cross my legs at meals. Don't get me wrong I'm grateful I have access to one of the less bad programs in the country and probably the only one with mandatory masks 🎉 and hope to use this time to work on certain projects with fewer electronic distractions, and but... yea
#survivingpsych#antipsychiatry#psychiatric abuse#sorry i had to censor that it sometimes attracts the p///ro blogs just to say it#hence part of the reason i rarely talk about it on tumblr#I also just fear TMI or oversharing#I dont want to make anyone uncomfortable#so I just hide my whole life online#bc mental health shit#trauma shit#and psychiatry shit#is basically my whole life and has been since I was a kid#I'm tired of it so I'm just gonna be fucking honest going forward#I mentioned it on 2 different discord servers I'm in
3 notes
·
View notes
Text
serious q - could anyone tell me the tags people use for discussing harm etc in the psychiatric system please?
& if there are any tags out there for people who hallucinate etc?
I feel like I'm guessing when I tag my own stuff & when I search for other posts
(would also love to know commonly used tags for other topics but that's a whole different thing. like is there a way to see the most popular/most used tags for a specific topic?)
4 notes
·
View notes
Text
I'm sorry, and I'm saying this as someone who's ghosted several psychiatrists to avoid a schizophrenia diagnosis, but I vibe with the pathologizing vs humanizing post. It's awkwardly put but I've known so many people who were like "oh I thought this was a quirk of my personality but it was actually one of The Symptoms so I hate it now". Like that's who the post is about. To me
2 notes
·
View notes
Text
As a psych survivor I was a bit nervous when I first brushed up on the edges of the delusions plotline in I Was a Teenage Exocolonist and shied away from it that run but then checked the content notes and decided I actually wanted to explore it more and I actually found it kinda therapeutic to explore.
I think it was handled well and that the content notes for the game do a good job of balancing giving folks a heads up without spoiling too much. It was interesting to explorer psych survivor Sol, and of course with the wormhole that is reflected in all their lives.
7 notes
·
View notes
Text
Mental health is a lawn; Desire is a prairie
Introduction
A little over a month ago, I began posting about upcoming changes in my practice, which I’ve been working on since. As I said in an instagram story, I realized that I’ve been pretty bad about replacing surface-level words instead of actually challenging underlying concepts; so, I’ve been taking some time to work on learning to better articulate my philosophy.
In the following essay I am going to try to explain my critique of psychiatry and offer a framework to replace it. You don’t have to agree with anything I say to receive herbs, advice or education from me. If I only wanted to work with people that believe the same things as me, I would stick to caring for my network of friends and accomplices. I have a public-facing practice to offer something immediately and materially useful to (broadly speaking) anyone that asks for it. I’m writing this because—while we may or may not be/become friends—my services are a personal gift, and I do not want them to be received as a function of psychiatry.
Most of all, I believe that everyone has an idea about what the future will hold, and everyone is trying to bring that idea to fruition. Ultimately there is nothing in my lifetime that will result in everyone being on the same page about what we all “should” be doing; and we are all relatively powerless on a global scale. What I can do is help the people I can touch, and walk away from those that want to force me to believe things I don’t want to believe in. I can’t make universal healthcare happen, right now or decades in the future; but I can fight tooth and nail to help heal the people around me for free, and I can share, liberate and generate knowledge to help others do the same.
I’m writing with a very limited scope here—if I was having an easier time writing this it would very quickly become an entire book, not a 3,700-some-odd word essay. I’m asking to you believe at face value that this is what I consider to be true; unfortunately I don’t have the capacity to write out an argument containing all the applicable historical evidence and referential sources right now. I hope at some point I do.
Part 1: Groundwork
Lobotomistic violence
I’m going to start by laying out a definition that I think is important to understanding where I’m coming from. I started using this term because I think it marks a useful distinction in how certain people are treated by psychiatry.
Lobotomistic violence is the set of psychiatric “treatments” that intend to make someone “normal” by reducing/inhibiting function in certain parts of their brain. While surgical lobotomies are generally considered outdated and barbaric in mental health culture, the root concept is still very much alive and well. Several antipsychotic drugs have similar effects to surgical lobotomies, and many more otherwise limit brain function in other ways. These drugs can prevent the people they’re prescribed to from thinking abstractly or feeling deeply, and often cut them off from meaningful parts of themselves.
According to the psychiatric framework there are people who need support, understanding, and accommodation; and people who need their bodyminds* to be physically altered and parts of them literally removed/made nonfunctional. Lobotomistic violence is a “last ditch” effort, when less extreme forms of medication or therapy are considered “ineffective”. Sometimes this comes after a long process of trying different treatments—but a lot of people are subjected to lobotomistic violence because they occupy a social position that society sees as a lost cause from the start, like people kidnapped off the street by ambulances in the middle of a psychotic break, or kids in state custody.
*Bodymind is a popular term in mad liberation that refers to the mind and body as a cohesive whole–it invokes the idea that we do not just inhabit our bodies, we ARE our bodies.
Defining mental health
(In this section, I’m using a very charitable interpretation of psychiatry from a scientific standpoint. Even the most advanced neuroscience cannot reliably identify specific mental disorders or their causes—but even if it could, it would still be fundamentally bad, and that’s the point I want to make.)
Civilization is an organism and an ecosystem in its own right, with structures to achieve equilibrium and to perpetuate itself. The choices that we make and options we see as available have been formed by thousands of years of accidents and choices that shape patterns of behavior and create social constructs. It is these structures I’m referring to when I talk about control.
In order for civilization to exist as it currently does, the people and things subjected to it must be easily understood, because things that are understood can be controlled. An example my friend used was a small, early agrarian state—a ruler wants to collect tax, with the goal of collecting as much as possible to enrich his position against neighboring states. He cannot collect too much tax, or else the population will either starve, or get angry and refuse to participate in the state; so to maximize what can be taken he has to know how much is produced, and in turn the farmers have to know how much they produce to know what they owe and what they need to meet immediate needs. Civilization needs to reduce complicated questions to knowable categories in order to respond in ways that benefit itself. This legibility occludes true understanding, pares down the messy, beautiful, difficult-to-communicate nature of life into one-dimensional criteria to be accounted for and processed. To see how these criteria are constructed, let’s look at an oak tree.
The name “oak tree” refers to a thing that exists, pretty indisputably (at least until you get into existentialism but, uh, let’s not go there). However, the name “oak” is something people made up. There are many different perspectives one might understand an oak tree from. Whatever lens you want to use impacts what characteristics you focus on and how you understand them in relation to the whole. You focus on certain attributes to create a story—if you’re using a scientific lens, you might look at DNA and draw connections to other DNA to tell a story about genetic history. Genetic history is also a human construct that only focuses on the pieces that are significant to the stories our culture wants to tell. These stories are what we use to build knowable categories; but a squirrel doesn’t give two nuts about the genetic history of an oak tree, and likely has its own stories that are entirely alien to us—because different attributes are significant to its life.
Mental disorders are real in the same way an oak tree is real—and fake in the same way an oak tree is fake.
The experiences that diagnostic labels describe are real, but the way disorders are defined is 100% a social construct that is entirely dependent on what is significant to our culture, scientifically backed or not.
“Health” is defined as bodymind states that are convenient for cultural perpetuation; and illness is bodymind states that are not. What experiences and attributes are constructed as diagnostic categories is dependent on what is valued and relevant to the dominant culture—and more importantly, what is conducive to the reproduction of that culture.
In our modern society, people who do not fit squarely into the mold of a responsible, reproductive citizen are either validated or marginalized. These are both methods of control, pushing people into legible categories to make them more easily understood and influenced by society. Validation might look like a kid who’s disruptive in class getting diagnosed with ADHD and working more closely with the school to receive accommodation, whereas marginalization might look like a disruptive kid getting diagnosed with ODD and being treated as if any resistance to an authority figure is a symptom of disease for the rest of their life.
In psychiatry, validation is “positivity”. This extends from clinical practice to what I’m going to call “mental health culture”, the expansion of psychiatry from a form of medicine to a fixture of culture. I’m going to talk about this more in a minute, but for now the point is: mental health does not identify a list of “problems” that exist in a vacuum. It constructs sicknesses in order to justify control. Which leads us to…
This wouldn’t work if we didn’t care about each other
Unfortunately, there’s no simple malice to blame here. A lot of the ways psychiatry hurts people are made possible by compassion. I try not to make generalizations about the human condition OR evolution-based arguments, but I do believe very deeply that humans are a fundamentally social species and that we are physically predisposed to caring about each other—evidenced in part by how much of the coerced labor necessary for society to function depends on making it hard to even SEE enslaved and low-class people, let alone extend solidarity and care to each other. The history of modern psychiatry (mostly over the past 200 years) and the birth of mental health is a chaotic mash of capitalistic profiteering, attempts to stifle liberatory movements, and individuals who are genuinely trying to take care of other people, all informed by the underlying assumptions about what “mental illness” is that I just described.
Brief digression: I’m always tempted to put “mental health” into quotes, but “mental health” implies a distinction between what I’m referring to and some other legitimate, non-fucked-up mental health that just doesn’t exist, so assume whenever I say mental health I’m using a slightly sarcastic tone.
Mental illnesses are, by and large, defined and diagnosed based on suffering, and the treatments, by and large, are designed to reduce suffering—or, the assumption that someone is suffering. How that suffering is measured and defined is still dependent on the basic assumption that correctly reproducing culture is good for you and not doing so is bad for you. For example, many diagnostic criteria measure one’s ability to work productively, and our society assumes wage labor is the norm for a healthy life. Sometimes, this is obfuscated by so many layers of reformed language and liberal feel-good-ism that many people who would disagree with that assumption when said so plainly (reproducing culture is good for you and not doing it is bad for you) are still deeply invested in mental health culture.
Diagnostic categories pick out certain experiences and characteristics to name as symptoms of a disease—but human brains are not very easy to put into boxes. Who is pathologized—labeled as diseased—is heavily dependent on their class status, and how well their behaviors contribute to the status quo. A lower-class non-Christian is more likely to be labeled as psychotic for describing their spiritual beliefs and experiences; whereas a richer person who talks about “being spoken to by the Holy Ghost” is simply a religious fanatic. We see consistently demographic-based diagnostic biases for disorders that are supposedly an issue with predetermined brain “hardwiring”, such as autism and ADHD being diagnosed more in white children, whereas Black children receive ODD diagnoses. By associating abnormality with suffering, and enforcing suffering for the abnormal, attempting to make people normal can represent reduction of suffering and a kindness. This dynamic is even more heavily enforced when people actively choose non-normative lifestyles: someone’s body state is not conducive to them living a “normal” life and they don’t even WANT to change, that means they are extra unhealthy. Under this logic, (attempting to/)forcing them to change is doing a good thing for them and thus the kindest course of action.
Everyone who advocates for broader mental health services is contributing to psychiatric and lobotomistic violence through kindness. There are plenty of people who think positively of their interactions with psychiatric institutions or mental health culture, AND there are ways to reduce harm when participating in mental health culture/be more honest about the risks involved; but encouraging people to participate in clinical settings is still encouraging people to put themselves in vulnerable, potentially dangerous positions.
Madness vs. pathology
Anyone can be crazy. I highly recommend trying it. Experiences are individually varied and highly personal—some people see and hear things other people don’t, some think in ways that are strange or confusing to others, and so on—but madness is simply refusal to conform to normative categories of mind-state and behavior. It is not bowing to social norms and the embrace of abnormal experiences that get in the way of a middle-class aspirations.
Pathologizing is the process by which madness is constructed as sickness. Pathology includes all the things that are “unapproved” about madness and it increasingly includes things that are only minorly inconvenient to our legibility and our participation. People re-contextualize experiences they never thought twice about as part of a disease, simply because they were given a label. “I never knew that was a BPD thing!”
Mental health culture encourages and facilitates this creep because even though its participants will often nominally criticizing practitioners who enact psychiatric violence, they continue to rely on the frameworks this violence is based on. Mainstream criticism of psych focuses on the idea that individual doctors (and/or institutions) apply psychiatry poorly, but it caries the implicit assumption that if it was only used correctly it would be a benefit. This can look like social/support groups of people identifying with a common or related diagnoses criticizing the way psychiatrists behave while encouraging people to self-diagnose, seek certain medication or therapy, or otherwise enforcing mainstream assumptions about the ontology of mental disorders.
Pathologizing talk surrounds us: “I think you might have ___”, “I’m like this because I have ___”, etc. It feels very similar to the ways in which certain queer spaces invent and push labels to describe every possible facet of gender or attraction, because well, it is. Both fixations gain traction because we are told that making ourselves legible to the outside world and making those around us legible in the same way will make us feel less lonely or invisible. Unfortunately, only letting people understand us in terms of our categories instead of on our own, unique terms continues to compound this loneliness. In an effort to make the system “work” we expand what experiences are known, create new labels and try to champion “inclusion”, instead of addressing the forces and dynamics surrounding the things that feel lonely, invisible, and difficult to communicate… A list of abbreviations doesn’t tell the world who you are, it tells the world how to react to you.
Many people who ascribe to psychiatric frameworks still live in ways that resist legibility. There are also plenty of people who are both mad and mentally ill, who use diagnostic labels but do not seek to conform to standards of “treatment”. There are also many people who use these labels to pressure conformity from themselves and those around them. It seems to me like the majority of people who, for example, encourage everyone around them to go to therapy, have never had a practitioner make good on the implicit threat of psychiatric violence.
The role of saneism
It would be incomplete for me to talk about the role of kindness without talking about the role of prejudice.
Saneism is a different form of bigotry than say, racism. It is not hatred of an “other” group that the “perpetrator” is not and never will be a part of. It’s more like fatphobia: hatred of a body state that every human being has the potential to experience. It is self-inflicted as much as it is wielded against the other.
Saneism is a tool to select who is and isn’t crazy. It should be clear at this point that there is no “sane” human being; sanity is only the ideal they beat you with. If you can emulate sanity well enough, driven by fear of internal and external hatred of madness, you are sane. If you can’t, you are insane, and either you can be mentally ill, assimilate to the categories and modes of behavior that are deemed acceptable for people like you; or, if you can’t do that, you’re crazy, and your options are either to submit to lobotomistic violence or to refuse to participate in psychiatry.
Part 2: Praxis
As I said at the beginning: The experiences that psychiatry addresses are real. Critique is all well and good in that it helps us name and understand the systems we live in, but it is only part of the process towards doing something better. Here is my attempt at building a model. It’s not perfect, but it’s a start.
A lawn is an artificially maintained shape, but a prairie is created organically through small and large events, which lines up nicely with the idea that mental health, as a noun is a standard that must be maintained, but desire, as a verb is a process of seeking, experiencing and evaluating that builds and grows in symbiosis.
Mental Health is a Lawn
The process of maintaining mental health through the reduction of suffering is like the process of maintain a lawn. A lawn is a pre-defined shape created through the prescription of behaviors and chemicals (weeding/mowing; herbicides/pesticides); regulated to be non-challenging and “safe” (no spikey plants, bee or wasp nests, etc) in the name people’s comfort and at the cost of native species; and prioritizing a certain socially-imposed aesthetic at great cost to the environment. Lawns have to be nourished (fertilized and watered) to grow, but are not allowed to get taller or more robust than a set value so that they’re easy to trim regularly with minimal effort. Lawns are monocultures with shallow roots that do not stand up to environmental conditions like drought without intervention. Lawns are also a standard everyone knows–and holds each other to, judges each other based on.
Likewise, to maintain “mental health”, people are regulated to a predefined standard that prioritizes “normal” aesthetics and the “safety” and comfort of others through the prescription of chemicals and habits (medication and therapy). Everyone knows the rules enough to police themselves and each other. Peoples’ material and emotional needs are taken into consideration enough for them to survive (and not commit suicide), but no one is well-supported enough to not feel the pressure to work; and people do not have the freedom to self-regulate on their own so when crisis occurs, you either have to keep working or rely on psychiatric intervention such as hospitalization.
Desire is a Prairie
Seeking desire is like how a prairie or grassland maintains itself as an ecosystem. Many types of plants grow deep symbiotic root systems that create resiliency and allow the ecosystem to survive through many environmental changes. Critters and bugs may kill/destroy plants at times, but they also reuse and decompose detritus and allow the ecosystem to recycle material and stored energy, spread seeds, etc. A prairie is too tall to be mowed easily by a conventional lawn mower and must be poisoned or crushed via heavy machinery. It is a complicated, compelling and beautiful organism that takes years of interaction to understand.
Desire cultivates varied experiences that let us practice the flexibility to survive distress emotionally, and shapes our lifestyles to prioritize self-regulation. Pain, whether external, self inflicted, or both, is an inherent part of life; but pain can allow us to grieve, process and grow, to clarify our desires, and maintain our bodyminds. When we live by desire we become unwilling to bend to social rules that don’t suit us, become uncontrollably mad, and are accustomed to freedom such that we can only be recuperated through incarceration and lobotomistic violence.
A prairie takes a long time to grow, and is difficult to support in a society that demands lawns. Switching from a mental health model to a desire model isn’t a simple or quick thing. Most of us will resemble something more like an overgrown lot, which is just as valuable.
Part 3: What this means for me
It’s taken a long-ass time to be able to articulate these concepts, so it feels extremely good to have finally made the pieces click.
Ultimately, what I offer isn’t substantially changing—at least right now, though I do have a new offering I’ll be announcing in the near future that incorporates herbalism into pleasure-seeking activities. I’ll still be here for consultations, workshops, and informal support; but the foundations are different, and I will be more explicitly incorporating these ideas into how I teach and discuss concepts. You might notice that the pages on my website have been rewritten and restructured, hopefully in ways that represent these ideological changes.
Something that comes up fairly frequently in conversation with my friends and accomplices who do similar public-facing non-hierarchical healing work is how to respond when people come to us expecting more standard frameworks: When people talk to us expecting to be told things about their bodies, or for us to diagnose a sickness and tell them what to do about it. To me, figuring out how to deal with these interactions is a matter of building and improving social skills; figuring out what questions to ask to break the script. This is just as much practical as it is ideological: What I do is in no way compatible with Western Medicine or psychiatry—the tools I have work granularly, effecting a few parts of the body at a time in specific ways. I can help you sleep, eat, relax, play, reduce fear, increase focus, cope with grief, ground thoughts and emotions, feel pleasure… but I do not use diagnostic categories, I do not offer “antidepressants” or treat disease. Someone telling me they have PTSD gives me exactly 0 information about what they want me to be doing for them. In some ways what I think what I already do in these interactions does more to ground my practice outside of psychiatry than any long-ass manifesto or theoretical explanation; but if you want to know why I do what I do, well, there you have it I guess.
106 notes
·
View notes
Quote
I think much of this writing [about psychiatric labels] misses the point. We may be able to come up with all kinds of cleverly nuanced perspectives on how we, as professionals and philosophers, understand psychiatric diagnosis but the fact remains that people are being told that they have mental illnesses and disorders, with all of the usual connotations of those terms in Western societies. Moreover, they are heavily encouraged to take on the particular narrow understanding that you refer to--we are all bombarded with messages about "mental illness" being "as real as a broken arm", and needing to be managed by drugs "just like diabetes." Even the dubious compromise of the "biopsychosocial" model--a way of acknowledging some role for psychosocial factors while at the same time instantly relegating them to "triggers" of a disease process--is not much in evidence on the ground. And furthermore, the biomedical message is reinforced by the fact that these labels are being applied by doctors and nurses working in hospitals and clinics, who use not just the labels themselves but the whole medicalized discourse of symptom, patient, prognosis, treatment, relapse, and so. The "stereotypical biomedical understanding of diagnoses", as you put it, is absolutely everywhere. [...]
I have yet to hear any real life service user say "Although the doctor told me I have schizophrenia I'm not too worried, because "illness" is just a metaphor for suffering in this case and it doesn't exclude personal meaning." I'm sure readers are aware that the consequences of being diagnosed--such as being sectioned, forcibly injected, and so on--are not just metaphorical. Some of these learned articles strike me as a form of defense against admitting to the fundamental inadequacy and devastating damage of the current diagnostic system. Essentially, we need to acknowledge that we are not dealing with patients with illness, but people with problems. We cannot make the shift to a more appropriate and humane system unless we are prepared to drop the whole biomedical discourse altogether.
Lucy Johnstone, PsyD, Moving Beyond Psychiatric Diagnosis
297 notes
·
View notes
Text
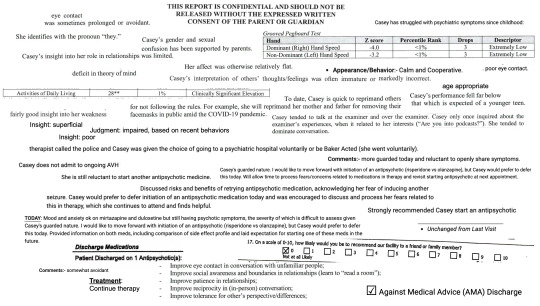
i call this collage "quitting therapy"
[ID under cut]
Image ID: a collage made from excerpts of my psychiatric medical records and reports. The excerpts are small black text on a white background and are pasted all over the image, creating a less organized collage look. The excerpts are small black text on a white background and are pasted all over the image, creating a less organized collage look. This ID will record each excerpt as it appears from left to right and top to bottom, with a couple noted exceptions where I felt the order mattered.
“This report is confidential and should not be released without the expressed written consent of the parent or guardian”. This text is in all capitals and bolded in the middle of the image, at the top.
“eye contact was sometimes prolonged or avoidant.”
“Casey has struggled with psychiatric symptoms since childhood.”
“She identifies with the pronoun “they”.”
“Casey’s gender and sexual confusion has been supported by her parents.”
This excerpt is a table labeled “Grooved pegboard test”, with the headers of “Z score”, “Percentile Rank”, “Drops”, and “Descriptor”, with rows labeled “Dominant (right) Hand Speed” and “Non-Dominant (left) Hand Speed”. The Z score for their right hand is -4.0, and -3.2 for their left hand. Both hands have a percentile rank of <1%, 3 recorded drops, and a descriptor of “Extremely Low”.
“Casey’s insight into her role in relationships was limited”
“Her affect was otherwise relatively flat”
“Deficits in theory of mind”
“Appearance/Behavior: calm and cooperative”
“poor eye contact”
“Casey’s interpretations of others’ thoughts/feelings was often immature or markedly incorrect.”
This is a table excerpt, listing “Activities of daily living”, followed by the scores “28**”, “1%”, and “Clinically Significant Elevation”.
“To date, Casey is quick to reprimand others for not following the rules. For example, she will reprimand her mother and father for removing their facemasks in public amid the COVID-19 pandemic.”
"age appropriate"
“Casey’s performance fell far below that which is expected of a younger teen.”
“fairly good insight into her weaknesses”
“insight: superficial”
“judgment: impaired, based on recent behaviors”
“insight: poor”
“Casey tended to talk at the examiner and talk over the examiner. Casey only once inquired about the examiner’s own experiences, when it related to her interests (“Do you like podcasts?”). She tended to dominate conversation.”
“therapist called the police and Casey way given the choice of going to a psychiatric hospital voluntarily or be Baker Acted (she went voluntarily).”
“Casey does not admit to ongoing AVH.”
“Comments: more guarded today and more reluctant to openly share symptoms”
“She is still reluctant to start another antipsychotic medication”
“Casey’s guarded nature. I would like to move forward with initiation of another antipsychotic (risperidone v olanzipine), but Casey would prefer to defer that today. Will allow time to process fears/concerns related to medication in therapy and revisit starting antipsychotic at next appointment.”
“Discussed risks and benefits of retrying antipsychotic medication, acknowledging her fear of inducing another seizure. Casey would prefer to defer initiation of another antipsychotic today and was encouraged to discuss and process her fears related to this in therapy, which she continues to attend and finds helpful.”
“Today: Mood and anxiety okay on mirtazapine and duloxetine but still having psychotic symptoms, the severity of which is difficult to assess given Casey’s guarded nature. I would like to move forward with initiation of another antipsychotic (risperidone v olanzipine), but Casey would prefer to defer that today. Provided information on both meds, including comparison of side effect profile and laid expectation for starting one of these meds in the future.”
“Strongly recommend Casey start an antipsychotic.”
“Unchanged from last visit.”
This excerpt is a rating scale, with the question “On a scale of 0-10, how likely would you be to recommend this facility to a friend or family member?”. Below the question are the numbers 0 through 10 in sequence, with a box to check next to each number. The box next to 0 is checked with an x, next to the words “not at all likely”.
“Discharge Medications. Patient discharged on 1 Antipsychotic(s):”
This excerpt is a bulleted list, immediately below the colon as if to imply that they are the antipsychotics in question, which has the following bullet points: “Improve eye contact in conversations with unfamiliar people”, “Improve social awareness and boundaries in relationships (learn to “read a room”)”, “Improve patience in relationships”, “Improve reciprocity in (in-person) conversations”, and “Improve tolerance for other people’s perspectives/differences.”
“Comment: somewhat avoidant.”
“Treatment: Continue therapy.”
This excerpt is a box to check, which is checked with an X, next to the words “Against Medical Advice (AMA) Discharge”.
(thanks to @aro-ace-ave-maria for helping with the image description)!
#idk how to image describe it but if anyone does feel free to add an id and i'll edit it in (edit: ty!)#therapists dni#psychiatry tag#survivingpsych#web weaving#my edit
832 notes
·
View notes
Text




Image description: [Black text on lined paper. Text reads: Share your story with the Psych Survivor Archive. Hold the psychiatric system accountable for the violence and coercion we've survived. Make space for our anger. Grieve together. Celebrate our resistance. The Psych Survivor Archive is a forum for psych survivors to share about their experiences and be believed. You can share as much or as little as you want. Your story will be anonymously published on the website with writing from other psych survivors. The archive is open to anyone who identifies as a psych survivor, including people who survived inpatient hospitalization, rehab, troubled teen industry, partial hospitalization, outpatient programs, ABA, and any other form of coercion psych treatment. Check out the prompts, participant rights, and content guidelines. Share your story now: www.psychsurvivorarchive.com/submit-your-story]
Hey everyone. I wanted to share this here as well. The Psych Survivor Archive is looking for anyone who wants to share their story and have it anonymously published on the website, in order to create a collection of our experiences navigating the psych system. Your responses will be anonymous and can be as detailed or vague as you want. On the website, there are prompts, but you can feel free to share in whatever format makes sense to you.
This is a more informal way to participate in the Psych Survivor Archive if you are not interested in creating art for the zine, but still want your story to be heard and validated.
For me, it has felt very cathartic to write out my story, on my terms, in the way that I want to be known. I hope that the archive can offer that space to other psych survivors as well, and I can't wait to keep developing this project and offering even more. In the next couple weeks, submissions will open up for the second edition of the zine, so if you're interested in submitting creative art or writing keep an eye out!
love and solidarity always <3
#personal#psych survivor#antipsych#survivingpsych#mad liberation#mad pride#madpunk#neurodivergent#mental illness#psych abolition#antipsychiatry#thank you SO much to everyone who's submitted stories so far. they are now live on the website#for me i process through writing. it means a lot to feel seen#and this is a small thing that i would like. to do with other people as well. idk#i know writing and sharing is really not everyone's thing and that's totally okay. as always there's#no pressure to participate. just an option#hopefully will be publishing some more zines soon about basic antipsych topics which would be lovely
467 notes
·
View notes
Note
top 5 anti psychiatry anything/anyone (texts, art work, activists)
So, my favorite antipsych texts, etc. aren't strictly antipsych - they're more often broadly disability liberation / anticarceral / radical autonomy - oriented with distinct acknowledgement of the struggle against psych. violence. That is reflected in this list, which is also by no means exhaustive of all my faves!
Atmospheres of Violence by Eric Stanley and The Terrible We by Cameron Awkward-Rich (I consider these to be spiritual companions!)
Nice Lady Therapists by Rabbi Ruti Regan.
Mel Baggs's blogs, especially Ballastexistenz and Cussin' and Discussin'.
Dave Hingsburger, Burritos and Cherry Pies.
The mostly-defunct tag on here, #survivingpsych - at its most popular, it proved life-saving for me and for others seeking to, well. survive psych.
161 notes
·
View notes
Note
if it’s not too triggering, why were you institutionalized for being picky? (If it’s too personal feel free to delete this ask, sorry)
Hi! It's no problem, it is triggering, but i think about it a lot, and it is something i sometimes shared on here, after it just happened, because i was in shock and had to let people know and to reach out like hey? has this happened to anyone else? but right after that it became too hard to put words to and too triggering to talk about so i talked about it less.
but its a story i want to tell now and am becoming more okay with telling, because i want people to know what happens to people, what happened to me, and what could very well happen to me again
and also, it just so happens i have been thinking about it a lot recently and thinking how to tell my story because i have been psyching myself up to tell my girlfriend.
so like. suuuuuuuuper long story below the cut. can be very triggering, its a very upsetting story. tw for like. institutionalization (obvs), suicide, medical abuse, eating disorders, psychiatric abuse, parental abuse (?)
I was kind of institutionalized. At first, it happened almost 9 years ago, I remember the anniversary every year. I was 16, my doctor recommended I be put in a childrens hospital eating disorder program. I have ARFID, no one really knew what it was at the time. I've had it since i was an infant and went from doctor to doctor and no one had ever seen anyone like me or knew what to do. One doctor said I wouldn't live past 21 if I continued to eat the way I do, but clearly that was not the case.
I am forever astounded by the amount of people I run into on here and online in general who identify as having ARFID or being that level of picky eater, though talking with some of them more in depth, it seems like they are often not on the level of pickiness i am on and seem to have experienced less shame and be more open about discussing it though everyone is different and impossible to tell.
I was excited for the program at first before it started. I thought they were going to help me and I would finally be a normal person. I was so tired of being harassed by random strangers, laughed at by waiters, and ridiculed by my family. Every person I made friends with I had to at some point make a terrifying confession to and going on dates (for the small regrettable amount I did it in high school) was near impossible when I had to show the part of myself that I was most ashamed about and hated the most on the first date.
I thought at the program I would find specialists who would sympathize with me and help me and would fix me. And when I got there, before anything even happened, I had to sign all these papers, and my parents did too, and I didn't know what they were, I didn't question it. What I signed didn't even really matter anyways, I was 16. And the first day I brought my phone with me and a book, and my bag with some other stuff. But after I signed everything, they took everything I had away, and we went to this room with all these doctors, 'my treatment team', I had never met them before, they barely looked at me or talked to me, but they talked about me and my 'treatment plan' and they were never caring to me, never talked to me like a person.
The plan, as it was for everyone, was that they give you three meals a day, of whatever food they bring you, you have to eat all of it by the time an alarm they set goes off, you have to drink every drop of water they give you, have to use every packet of sauce they give you. If you don't do this, you get moved down a 'level' and you get privileges taken away. Things like watching tv, or being around other patients, but most of all, I found out that being moved down a level just meant you usually get locked in a room by yourself for a few hours because that happened to me. a lot.
i was very upset when i found this out. this was not helping me. because as i found out, it turns out no one really knows a fucking thing about helping people with mental illnesses or eating disorders or developmental disabilities even though the medical establishment likes to talk about how much it has progressed. they don't know a single fucking thing.
so i finally went out to the common room with the other patients. i was crying very hard and told the doctors that was it i wanted to leave i didn't want to be part of the program. but they told me it was too late i already signed the consent forms. so i don't know if medical consent/institutionalization is still like this almost 10 years later, if someone was lying to me or if this is true, but my mom also told me the same thing, and apparently if you consent to this kind of thing you cannot take it back. which by definition, makes it not consent.
i remember sobbing in the common area with the other patients (they were all girls, about same age as me), and there was another new patient, also sobbing. the other girls tried to comfort us and talk to us, but the orderlies (i don't really know what else to call them, all they really did was sit and watch us and make sure we didn't do anything that wasn't allowed. they were all college girls. they were extremely mean to us, they thought we were being dramatic) wouldn't let them, we weren't really allowed to talk to each other much and we weren't allowed to touch each other and we very specifically for some reason were not allowed to comfort each other.
i was crying especially hard because i knew that this program was expected to last for a couple months. but as i talked to the other girls there the small amount i was able to, i found out that most of them had been there for much longer than a couple months, many of them for over a year. i managed to catch my parents as they were leaving from dropping me off and talking with the doctors (i had only been there still only like 3 or 4 hours) and screamed at them to get me out of here. my mom seemed really shaken by the way i was acting and the doctor told her not to worry and i specifically remember him saying "they all act like this at the beginning".
it is something i will never forget because every time i tried to convince my mom to get me out of there she seem conflicted based on the fact that the doctor said that. and it hits me every time that all the doctors, the nurses, the people working there, can see children. children. acting like that about what they are doing to them and think they are doing the right thing. i will never forget it ever. and every person who came in after me did the same thing! because it was prison! it was punishment! for having a eating disorder! for being autistic! when i was able to talk to my mom, she kept saying "we are not trying to punish you" and the more times she said i realized she was trying to convince herself.
i ate some of the foods they gave me but i never got used to them like they said i would. i just got knocked down a level every time and got locked in a room. and the thing is, unlike most media and reports about mental wards or asylums. it was a nice hospital. it was brand new. the room i was locked in was not a padded room. one of the walls was just a window. and in some ways, that made it worse. because it looked out on a highway and i saw all the cars going to and from work, going to the store, going to eat. and they were so free and they could go where they wanted and eat what they wanted and when they wanted and they weren't locked in a room. and they passed this hospital and had no idea what was happening to me or to anyone else here and it made me so angry and so defeated. i felt so close to being away from a waking nightmare but i knew i would never get there. a year!!! i could be there for over a year.
a year without going where i wanted when i wanted. no access to my phone. i wasn't allowed to see my friends. i wasn't allowed to read my books. i wasn't allowed to eat what i wanted when i wanted. i did therapy a few times a day but it was more like an interrogation. when i was a high enough level to be in the common room, i sat in the corner and did puzzles obsessively so i could just dissociate and focus on the puzzles. eventually the therapist told me i wasn't allowed to do puzzles anymore because it was "distracting from my recovery" and i "wasn't thinking about my eating" (i don't know what the fuck i was supposed to be thinking about). it got to the point where i felt like i didn't have ownership of my own mind anymore. i wasn't allowed to dissociate. i wasn't thinking about what they wanted me to be thinking about.
they told me if i "was good" (aka if i reached a high enough level, not going to happen) i could write them a list of 100 songs. they would load all the songs on an ipod shuffle to loan to me. but only after they listened to all of them first to make sure they were appropriate. they told me if i "was good" maybe i could see my best friend for a few hours for one weekend. a few hours. for one weekend. i was understanding how truly controlling the program was. seeing a friend for a few hours once a month is a privilege. listening to a few songs they approve is a privilege.
but it didn't matter. i realized after the first day that obviously i had to kill myself. i was already in a pretty bad place before the program and was passively suicidal but i realized instantly that i could not live like this and if i was going to be stuck here indefinitely then my only way to escape was to end my life. i didn't have a plan at that point but i knew for certain i was going to do it. the loss of control, the violation, the loss of body and self was unbearable.
every morning they had us strip and then weighed us and did an ekg. why did they have us strip and do an ekg? it doesnt seem like it has much of a point. they watched us go to the bathroom. it all seemed like humiliation and violation for the sake of it.
even after the second day i had realized that i didnt want to be fixed or get better and i had to come to the very quick realization that there had never been anything wrong with me. when i went to therapy they asked me questions like "don't you want to be able to go to restaurants?" "don't you want to be able to eat with friends?" and i realized none of that had to do with my health. the reason i had problems with restaurants was because they didn't accommodate to me and the reason i had problems with friends was all social. all these reasons i had for wanting to be fixed and all these reasons they had for me to want to be fixed were other peoples' problems. the way people treated me was not my problem.
for your treatment plan, one of the first steps was to admit in group therapy that you had an eating disorder and what your problems were (i fucking know) and that would get you more privileges but i decided i wasn't going to do that because i didn't have a problem, my "problem" was everyone else's problem and the way they treated me. so i refused to every session and got locked in the room every time for this. they fucking hated me for it.
if you can't tell how long i was there for based on this. i was only there for a week. because after a week our insurance came back and declined to cover the program. i always hate myself that it was a week. it doesnt feel long enough. for the amount that it did for me. for how much it does to me almost 9 years later. it doesn't feel like enough.
i got home and screamed at my parents. i was so angry. my mom had allegedly been trying the entire time to get me out of the program, but my dad had been trying to keep me in. when i got home my dad had taken away my phone and my laptop and said he wasnt giving them back. i screamed at him and cried and he threatened to call the hospital and have them lock me up forever. i was terrified, i tried to get away from him, to hide. and he got out his phone and took video of me, at my worst moments, he claimed to show to the doctors. i ran away. for a few hours. i had nowhere to go. i ran about a mile. and then sat down outside the rec center and cried until it got dark. and then i went home.
i had nightmares that i was still there for months. it never ended. i was so paranoid about everything. i thought people were coming to lock me up. i couldn't draw any attention to myself or i thought i would be locked up. every time we drove anywhere near the hospital i thought my parents were taking me back there. i was so paranoid i couldn't sleep i couldn't sit i couldn't do anything i had to be looking out for everything and i trusted no one. i walked around, angry at everyone, that they were so carefree in everything and they had no idea what happened to me. i was angry it happened to me and they were worried about things that had no importance. i was angry when adults thought they knew more than me and i felt i had been through more in life at 16 than they had at their age. was it true? i'm not sure.
i think the most important thing i learned, whether true or not, besides not needing to be fixed, was that i could never trust anyone and never ask anyone for help again. i thought they would help me and i was excited. for some time, i thought it was my fault. at least partially. but now i am angry. i was 16. who would do that to a 16 year old who was looking for help because of how people had treated them?
for a while after i talked about arfid a ton on tumblr and also on wordpress. i created the actuallyarfid tag but became disillusioned when so many people in the tag just talked about wanting to get rid of it or their progress in getting rid of it. and eventually i couldn't even talk about it anymore. it was too tied to everything that happened and i was still so ashamed of it. it was to triggering. i stopped.
i think for similar reasons i have stopped associating so much with the autistic community online. i think it has jaded me so much to see so many people who have only had the slightest negative consequences of being autistic and do being autistic like putting on and taking off a coat after something like this happened to me. it was in this program that doctors first told my parents they think i am autistic though i wasnt diagnosed until later. i recognize now that having arfid is part of my being autistic but i don't like to talk about it in the context of having arfid because i don't feel like i 'have' anything. it is just me being me. and i use autistic as a label when i need to explain my needs and differences to people quickly and its fun to make jokes about being autistic sometimes but i dont like to constantly identify myself that way.
my parents are "health" nuts (fake garbage health bullshit) so they were still convinced my eating was going to kill me and many years later have taken me to see several nutritionists. and all these years later, after doctors many years ago declared i had a problem and would die, most of them did not see a huge problem with the way i eat. one of them in particular who i love and have seen over and over again at the behest of my parents has pointed out many things to me. there are plenty of adults who don't eat or barely eat fruits and vegetables. there are plenty of adults who eat the same thing every day (bring the same thing for lunch at work everyday anyone?). the world does not end. if you are different and you do it. then you are a problem and you need to be fixed. but if it is within socially acceptable norms, then it's okay.
i've always thought that some day i wanted to write about what happened to me publicly. in a paper or something. i want people to know. that this happened to me. that this happens to people. still. that it could very well happen to me again. though i'm not sure i could take public response if i did write about it. and after i got out of the program, i wrote it all in a journal, but then ripped it up and shredded it because the words weren't enough. they were so insignificant and i could never ever find the words to capture how horrifying it was what happened to me and how badly it ruined me and destroyed me. it changed my whole life and my perspective on everything. but i think now, almost 10 years later i am starting to find the words. and i think now i am less scared.
#i think now survivingpsych tag would like to look#i think this is the best i have ever written or explained it#most emotional and most explaining why#survivingpsych
17 notes
·
View notes
Text
People who have little-to-no therapy experience, or who have only ever had positive interactions with the mental health system, shouldn’t be speaking over those with psychiatric trauma when it comes to talking about the ways that the psych system is actively damaging and oppressive.
If you haven’t been personally hurt by therapy/hospitals/psychiatry-as-an-institution, and someone is telling you how those things can be bad? Listen to them before you even think of trying to respond. And consider any response long and hard before saying it. Step away, maybe research it, maybe sit with it a while. If you’re uncomfortable, ask yourself why. If the only response you have is to defend the system, then maybe that’s where you’re at and that’s fine, but you need to keep that to yourself and not push it on survivors.
Listen to us when we tell you how the system needs to change. Don’t silence us and tell us we’re just “resisting recovery” and spreading “misinformation.” That’s just enabling the same abuses and telling other people how they should be thinking and feeling, and that if they aren’t then it’s just because there’s still something wrong with them. Which is pretty messed up.
You don’t have to agree with every psych survivor on every point, but you do need to stop and consider what we say and stop writing us off as evil, crazy, or "anti-recovery.” You need to consider who that helps. You need to give a shit about the people being abused by the system helping you, and then ask yourself why it helps you while it abuses others. Interrogate systems of oppression. Ableism won’t be solved with nicer ways of telling us we’re crazy.
332 notes
·
View notes
Last Seen Blogs

ao3feed-larry
ao3feed for larry stylinson
meanwhileyoucansmile
Mean while you can smile

yukittysh
❄Yukittysh ❄

soapiesophie5
Soap

disney4everr
Disney