#tertiary lead syndrome
Text



Get wrecked Phu. Nan is wearing his colors again after he decided not to confess to you because Khao came to see him in Thailand and remembered his promise. You don't deserve Nan! @respectthepetty can these colors mean something?No? Can I pretend? Also, @absolutebl, I believe this show has perfected 'anyone but the main lead' syndrome.
#the promise#the promise the series#the promise series#bl series#thai bl#thai drama#bl drama#thai series#thaibl#asianlgbtqdramas#asian lgbtq dramas#thai bl series#second lead syndrome#tertiary lead syndrome#anyone but the main lead syndrome
36 notes
·
View notes
Text
Writing Wednesday: Meet the 2nd Lead
I read a lot of pieces still under development by young authors and something I see missed, over and over again, is the use of secondary characters. A good secondary character can be as well-loved (or better loved) than the MC! I can point anyone to quite a few very well-written Korean Dramas that show how to use that second lead to its fullest. In fact, among K-Drama viewers in the US, we call…

View On WordPress
#main characters#MC#second lead#second lead syndrome#secondary characters#tertiary characters#writing
0 notes
Text
Wow could Fighting for Love tank itself any faster- what a huge disappointment. I mean it wasn't top tier in terms of script, but at least it was fun. I see why they focused on Mai and Yizhi. They played off of each other so well. Felt a little sorry for Hot Enemy General who was never much of a threat in terms of giving us that 2nd Male Lead Syndrome. He probably staged all those invasions just to get a few more minutes of screen time. And of course it looks like they will be killing off my boy Lt. Tang. He was too fine to live apparently.

Of course I'll watch the last two episodes - gotta see how many other tertiary characters we can kidnap and rescue.
6 notes
·
View notes
Text
Lonopin Injection: A Lifesaver in Delhi's Healthcare Landscape

Delhi, the capital city of India, is renowned for its diverse population and robust healthcare infrastructure. However, the city also grapples with numerous health challenges, including cardiovascular diseases, which remain a leading cause of mortality. Lonopin injection, Lonopin Injection in Delhi a low molecular weight heparin, emerges as a beacon of hope for individuals at risk of thrombotic events, such as deep vein thrombosis and pulmonary embolism.
The prevalence of sedentary lifestyles, coupled with a rise in risk factors such as obesity and hypertension, underscores the importance of preventive measures against thrombotic disorders. In this context, Lonopin injection serves as a prophylactic agent, particularly for patients undergoing surgery or those immobilized due to medical conditions. By inhibiting the formation of blood clots, Lonopin injection significantly reduces the risk of thromboembolic events, thereby safeguarding patients' health and well-being.
Moreover, Lonopin injection finds widespread application in the management of acute coronary syndromes, including unstable angina and myocardial infarction. In Delhi's fast-paced healthcare environment, where every second counts in saving lives, Lonopin injection emerges as a cornerstone in the treatment regimen of cardiovascular emergencies. Its anticoagulant properties help prevent further clot formation, thereby preserving myocardial function and improving clinical outcomes.
Accessibility to Lonopin injection is a crucial aspect of healthcare delivery in Delhi. Fortunately, the city boasts a robust network of healthcare facilities, ranging from tertiary care hospitals to community health centers, where patients can readily access this essential medication. Pharmacies across Delhi stock Lonopin injection, Menotas Hp 75 Injection ensuring its availability to patients in need, regardless of their geographical location or socioeconomic status.
However, amidst the accessibility of Lonopin injection, it is imperative to highlight the importance of appropriate usage and adherence to prescribed regimens. Healthcare professionals in Delhi play a pivotal role in educating patients about the significance of adherence to medication schedules and the potential risks and benefits associated with Lonopin injection therapy. Through patient counseling and regular monitoring, healthcare providers strive to optimize treatment outcomes and mitigate adverse events.
Furthermore, Delhi's healthcare ecosystem continually evolves, with advancements in medical research and technology shaping clinical practices. As new evidence emerges regarding the efficacy and safety of anticoagulant therapies, including Lonopin injection, healthcare professionals in Delhi remain vigilant, ensuring that patient care aligns with the latest guidelines and best practices.
0 notes
Text
Know Sexually Transmitted Infections (STDs) Signs and Symptoms
Sexually Transmitted Infections (STDs), also known as Sexually Transmitted Diseases (STIs), are a group of infections that are primarily spread through sexual contact. They affect millions of people worldwide and can have serious health consequences if left untreated. Understanding the signs and symptoms of STDs is crucial for early detection and treatment. In this blog, we will discuss some of the most common STDs and their associated signs and symptoms.
Chlamydia
Chlamydia is one of the most common STDs and often shows no symptoms. When symptoms do occur, they may include:
Painful urination
Abnormal genital discharge
Pain or swelling in the testicles for men
Pain during sexual intercourse for women
Lower abdominal pain

Gonorrhea
Gonorrhea shares some symptoms with chlamydia, such as painful urination and abnormal discharge. However, additional signs may include:
Sore throat
Painful bowel movements
Pelvic inflammatory disease in women, which can lead to infertility if left untreated
Syphilis
Syphilis is a bacterial infection that progresses in stages, with symptoms varying at each stage. The primary stage is characterized by a painless sore or ulcer at the site of infection, usually the genitals or mouth. As the infection progresses, symptoms can include:
Skin rashes
Fever
Swollen lymph nodes
Fatigue
Joint pain
Organ damage in the tertiary stage, which can be life-threatening
Herpes
Herpes is caused by the herpes simplex virus and can result in recurring outbreaks of painful sores or blisters in the genital or oral area. Other symptoms may include:
Itching and burning before the sores appear
Flu-like symptoms during the initial outbreak
Nerve pain

Human Papillomavirus (HPV)
HPV is one of the most common STDs, with many strains that can cause genital warts or lead to certain types of cancer, such as cervical cancer. Genital warts are the most common symptom, but some HPV strains do not produce visible symptoms. Regular screenings and HPV vaccinations are crucial in preventing associated health risks.
Human Immunodeficiency Virus (HIV)
HIV attacks the immune system and can lead to acquired immunodeficiency syndrome (AIDS) if left untreated. Early HIV infection may cause flu-like symptoms, but it often progresses without noticeable symptoms for years. Later-stage symptoms can include:
Rapid weight loss
Chronic diarrhea
Pneumonia
Skin rashes
Night sweats
Swollen lymph nodes
Opportunistic infections
Trichomoniasis
Trichomoniasis is caused by a parasite and can result in symptoms such as:
Vaginal itching
Abnormal discharge with a foul odor
Painful urination
Itching and redness in the genital area

Conclusion
Sexually Transmitted Infections can affect anyone who engages in sexual activity, and some may not exhibit any symptoms. Regular screenings, practicing safe sex, and open communication with sexual partners are essential steps in preventing and managing STDs. Early detection and treatment are crucial for reducing the risk of complications and the spread of infections. If you suspect you have an STD or are at risk, consult a healthcare professional for testing and guidance on the best prevention methods. Remember that safe sex and open conversations about sexual health are key to reducing the prevalence of STDs in our communities.
0 notes
Text
GI Tract, Associated Complications and Gastro Doctors
Gastroenterology is a specialty that focuses on the digestive system and related disorders. It focuses on disorders of the gastrointestinal tract or digestive tract involving the stomach, small and large intestines, esophagus, and rectum.
Some common diseases affecting the digestive system include ulcers, irritable bowel syndrome (IBS), acid reflux, stomach cancer, and ulcerative colitis. Thanks to technological advances in surgery, non-invasive surgical intervention procedures can now successfully manage and treat all types of digestive system disorders.
Gastroenterology
This is a medical specialty that includes treatment of the digestive system. This includes treating conditions related to all parts of the digestive system, including the gastrointestinal tract. Digestive disorders and problems treated by gastroenterologists or GI doctors or gastro doctors in Pattaravakkaminclude-
Unexplained changes in bowel habits Like diarrhea, constipation, and blood in the stools
Gastroesophageal reflux disease (GERD)
Heartburn or Stomachache
Hemorrhoids
Inflammatory bowel disease (IBD) (for example Crohn's disease, ulcerative colitis, etc)
Irritable Bowel Syndrome (IBS)
Pancreatitis
Ulcers
Gastrointestinal
The digestive tract or gastrointestinal tract is attached to the digestive system, which functions to break down the foods we eat into nutrients. The digestive system is made up of the gastrointestinal tract or gastrointestinal tract, liver, pancreas, and gallbladder. It is also known as the gastrointestinal tract or GI tract or alimentary canal. The digestive tract consists of interconnected hollow organs as follows-
Mouth
Esophagus
Stomach
Small and large intestines
Anus
KGJ Hospitals- Best gastro doctors in Chennai
KGJ Hospitals is one of the leading gastroenterology hospitals in Chennai equipped with the best gastro doctors in Pattaravakkam. The hospital provides patients with comprehensive care according to national standards and protocols. The gastroenterology department at KGJ Hospitals is the best department in the city offering personalized treatment options for pediatric and adult patients. Consult Dr. J. Ashok Kumar, the best Gastroenterologist in Chennai!
Kgj Hospital is a multidisciplinary tertiary care hospital located in Chennai, providing next-generation treatments for gastrointestinal, liver, and hepatobiliary diseases. Modern equipment and experienced gastroenterologists perform all necessary endoscopy and radiotherapy for diseases of the digestive tract, liver, and pancreas.
0 notes
Text

The thyroid gland & hypothyroidism in German shepherds
Despite its modest size, the thyroid performs several functions in the body and hence holds a central role! It produces a variety of hormones, most notably thyroid hormone and calcitonin.
Structure and functions of the thyroid
The thyroid glands are developed in pairs and are placed in the upper section of the tracheal neck. Their job is to produce hormones.
Thyroid hormones (T4- thyroxine and T 3- triiodothyronine or thyronine)
Calcitonin
Thyroid hormones are made in follicles from various amino acids and iodine. T4 (thyroxine) accounts for 80% of thyroid hormones produced, with the remainder composed of T3 (triiodothyronine or thyroxine). These two hormones have the most influence on metabolism. Furthermore, because T3 is exceedingly fragile, the majority of it is generated not in the thyroid but directly in the target organ from T4. As a result, T3 levels in the blood are extremely low. Glands form in pairs and are located in the upper portion of the tracheal neck.
The thyroid hormones are essential for metabolism and intervene in almost all metabolic processes:
skin and coat growth
overall growth and development
increase in heat production
Increase fat metabolism and food transport
Increase heart rate and heart rate
Increase production of red blood cells (erythrocytes)
Stimulate the immune system
Calcitonin, on the other hand, is important for calcium balance. In addition, the thyroid gland stimulates the immune system of our German shepherd.
The production of thyroid hormones is controlled in the brain, more precisely in the so-called pituitary gland. The whole thing happens through a well-coordinated control circuit. The hormone TRH is formed in the brain, more precisely in the hypothalamus (interbrain). This in turn affects the production of TSH in the pituitary gland. And the released TSH affects the production of the thyroid hormones (T3 and T4). T3 and T4 are then brought to the target bound to so-called carrier proteins.
Hypothyroidism in German shepherds- An underactive thyroid gland, often known as hypothyroidism, affects older, medium-sized, and giant German shepherd breeds in particular. As a result, it is a fairly commonly diagnosed condition in practice. Thyroid hormones are not produced in sufficient quantities in this scenario.
Causes: When it comes to causes, a distinction is first made between what type it is.
Hypothyroidism primary- It is caused by feeding mistakes, such as a shortage of iodine after barfing or cooking yourself, or by a long-term excess of iodine. Furthermore, the thyroid can regress, as can Z. B. Age-related (senile atrophy), but possibly idiopathic (unknown etiology). Thyroiditis, an infection of the thyroid gland that is frequently accompanied by thyroid tissue loss, can also be present.
Secondary hypothyroidism- In contrast to primary hypothyroidism, the thyroid gland is normal in this case, but the regulatory mechanism (the pituitary gland) is dysfunctional. This signifies that the thyroid gland does not receive enough stimulation to create thyroid hormones. Secondary hypothyroidism in a German shepherd is frequently accompanied by indications of central nervous system failure.
Tertiary hypothyroidism- The disorder is in the diencephalon (hypothalamus).
Euthyroid Sick Syndrome (ESS) - These are diseases that lead to altered thyroid levels but are not directly related to the thyroid or its regulatory mechanisms. It is also known as non-thyroidal illness (NTI).
Signs/Symptoms- An underactive thyroid gland is often very variable and individual, and it is often a rather gradual process so it is not even noticeable at first glance. As written above, the thyroid hormones take on essential tasks in the metabolism. Since the skin and fur are constantly regenerating and are subject to constant cell renewal, skin and ear problems are the main issues. In addition, German shepherds with an underactive thyroid are more prone to illness, as the thyroid also plays an important role in the immune system.
Classically, the German shepherd show:
Hair loss (alopecia)
Itching
Unpleasant skin odor
Thinner and/or brittle coat
Increased dandruff and/or sebum formation (seborrhea)
Poorer or slower fur growth
Hyperpigmentation
Skin infections
Ear infections
Increased appetite and weight gain
Weight gain despite dieting
Poor performance
Indigestion
Muscle weakness
Decreased heart rate
Cycle disorders
Lipomas
Diagnosis- Diagnosing an underactive thyroid can sometimes be difficult. If there is a suspicion that the German shepherd could be suffering from an underactive thyroid gland, a blood test is usually carried out first. If your shepherd from the Philippines suffers from clear hypothyroidism, this can be identified through a blood count. For this purpose, a thorough preliminary talk should first be carried out to discuss topics relating to feeding, state of health, coat changes, problems, etc. A thorough general examination is then carried out. Now the German shepherd is examined, the heart rate and respiratory rate are determined, the ears are examined, the lymph nodes are palpated, etc. If hypothyroidism is suspected, a blood test is then carried out. Not only the thyroid values should be determined, but ideally, also a red blood count and organ profile with the determination of the liver, kidney values, etc. should be determined. This is the only way to distinguish between euthyroid sick syndrome and "real" hypothyroidism.
Ideally, the following should be determined for the thyroid values:
T4 (free and total)
T3 (free and total)
TSH
Antibodies against thyroid hormones
Antibodies against thyroglobulin
cholesterol
In practice, often only T4 is determined, sometimes TSH and cholesterol are also determined. To obtain an accurate assessment of the thyroid function, however, all of the blood values listed above, including the organ profile should be determined.
Treatment- Thyroid hormones (L-thyroxine) can be particularly effective in treating an underactive thyroid gland. It is administered as pills or as an oral solution. The first signs of progress can be seen within a few weeks. Four weeks after starting treatment, the first blood test is performed to modify the drug if necessary. Further checks are then performed at regular intervals, depending on the progress. German shepherds with an underactive thyroid should be evaluated regularly since associated problems such as menstrual cycle disorders, wound healing issues, or increased susceptibility to infections might occur. Furthermore, the control is employed to monitor the amount of medication. Because the amount delivered is highly changeable and unique to each individual. As a general rule, start with 10 g per kilogram of body weight. The dose is then gradually increased. The tablets must be taken twice a day.
What Happens If Hypothyroidism Is Left Untreated — Consequences?
If the German shepherd suffers from a mild classic hypothyroidism that is not treated, the following general problems can occur:
Fatigue and reduced ability to concentrate
weight gain
weakening of the immune system
Wound healing disorders
circulatory disorders
cycle disorders
Long-term damage can even occur in the case of pronounced hypothyroidism (myxedema coma, myocardial insufficiency, and massive skin and coat changes).
Myxedema coma- This is the most severe and potentially fatal form of hypothyroidism. It is, thankfully, quite rare and is characterized by confused consciousness, a low body temperature, and a slow heart rate.
Feeding for hypothyroidism
Nutrition has a certain influence on all organs and naturally also on the thyroid gland. If your German shepherd is diagnosed with hypothyroidism, you should take this into account when doing BARF or cooking yourself. Unfortunately, it is difficult to feed dry or wet food, as we have no direct influence on the composition.
Some basic rules are:
Check the iodine content in the ration and adjust if necessary
Check calcium intake and adjust if necessary
Adequate protein intake
Check the selenium, zinc, and iron in the ration and adjust if necessary
Feeding and tablet administration should take place with a time delay
1 note
·
View note
Text
Gastroenterology Specialists | cubspaediatricdietetics.au
Gastroenterology is the branch of medicine that treats digestive disorders such as gastroesophageal reflux disease, irritable bowel syndrome, liver and biliary disease and inflammatory bowel disease.
We investigated the proportion of new patients and follow-up presentations at three public hospital outpatient gastroenterology clinics in Australia. Facility 1 is a tertiary referral centre, facility 2 has specialised IBS, motility, hepatology and transplant hepatology services whereas centre 3 is a public gastroenterology clinic.
Dr Radford-Smith
Dr Radford-Smith is an Australian gastroenterologist who specializes in gut health, inflammatory bowel disease and colorectal neoplasia. He is also an Associate Professor at the University of Queensland and an Honorary Group Leader at the QIMR Berghofer Medical Research Institute.
He is a keen advocate for the utilisation of clinical data in optimising patient care and outcomes. He is also a passionate researcher and has published over 170 articles in the field of gastroenterology.
He leads a team of researchers who have designed a simple clinical tool to help Gastroenterologists triage patients referred for a colonoscopy. They are also developing a novel approach to understanding the role of the microbiome in the development of IBD.
Dr Luke Hourigan

Dr Luke Hourigan is an experienced gastroenterologist who practices privately at Greenslopes Private Hospital (associate of Queensland Gastroenterology). He has a specialist interest in the management of Barrett's oesophagus and large colonic polyps.
He is a member of the Australian Gastroenterology Endoscopic Association and serves on the education committee of the World Endoscopy Organization. He is also an active participant in the NETI National Colonoscopy Training Initiative.
A/Professor Hourigan is a past President of the Gastroenterology Society of Queensland and an Honorary Clinical Professor at the University of Queensland. He has been involved in gastrointestinal endoscopy training and research for many years and has a particular interest in the use of advanced endoscopic techniques to manage premalignant and malignant lesions.
He has extensive experience in the diagnosis, management and treatment of gastrointestinal disorders including inflammatory bowel disease and hepatitis. He is a leading authority in the field of endoscopic management of diseases of the oesophagus, stomach, small intestine and pancreas.
Dr Michael Payne
Dr Michael Payne is a gastroenterologist at queensland gastroenterology who treats digestive problems such as acid reflux, stomach pain, constipation, Crohn’s disease and ulcers. He also offers cancer treatment using radiation therapy, which can reduce the number of treatments required and improve quality of life for patients with advanced cancers.
Dr Payne completed his undergraduate degree in Mechanical Engineering at Queens University before completing a Master’s degree in Sports Medicine. He then went on to complete a medical degree and residency training in physical medicine and rehabilitation at the University of Ottawa, followed by a clinical fellowship in Australia.
As a radiation oncologist, Dr Payne treats patients with cancer of all types and works to ensure that they receive the best possible care and are treated as individuals. He believes that diet, lifestyle and attitude can play a role in determining the success of cancer treatment. As a result, he makes sure that each patient understands what to expect during treatment and helps them make informed decisions about their health.
Dr Peter MacDonald
Dr Peter MacDonald is a g gastroenterology specialist at queensland gastroenterology who is interested in gastrointestinal surgery, including coloproctology. He is also a medical writer and has published several books. He is a member of the Royal College of Surgeons and the London Gastroenterological Society.
He is a former President of the International Association for the Study of the Liver and a Founding Editor of the Journal of Gastroenterology and Hepatology. He was also the first recipient of the GESA Distinguished Research Prize.
Australian Hepatology has been blessed with a number of leading hepatic pathologists who have made significant contributions and achieved world recognition. These include the late Pauline Hall (alcoholic liver disease),63 Andrew Clouston (steatohepatitis and the ductular reaction referred to above) and Prithi Bhathal who has contributed greatly in the field of portal hypertension and cirrhosis.
#queensland gastroenterology#qld gastroenterology#gastroenterology specialist#brisbane gastroenterology
1 note
·
View note
Text
Abduction of shoulder

#Abduction of shoulder full
#Abduction of shoulder series
11 On the other hand, other studies did not show immediate changes in the scapular kinematics after thoracic SM 6 or differences in pressure pain sensitivity, 11 added to which improvements were not observed in muscle activity after thoracic manipulation. Thoracic SM has already been explored in studies of participants with shoulder pain, finding a decrease in shoulder pain immediately after manipulation 10 and improvements in function after thoracic SM. 9 Thus, the rational basis for the clinical use of thoracic manipulation to treat the shoulder is based on this theory. The relationship between the thoracic spine and shoulder movements leads to the term regional interdependence, which refers to the concept that apparently unrelated deficiencies in an anatomical region may be associated with primary symptoms in other regions that contribute to the patient complaint. 4 Some approaches to the treatment of shoulder pain include thoracic spinal manipulation (SM), 5, 6, 7 which can be defined as a movement of high speed and low amplitude or thrust applied directly to any thoracic segment. 3įor the treatment of shoulder pain, conservative treatment is initially advocated through physiotherapy interventions. 2 Thus, regarding complaints of the shoulder complex, the most common pathologies are tendinopathies, especially those of rotator cuff lesion. 1 A study has shown that the 3 most commonly referenced musculoskeletal conditions for physiotherapeutic treatment at secondary and tertiary levels are low back pain, rotator cuff syndrome, and gonarthrosis. Frame constructed of malleable aluminum covered in antimicrobial CoolMesh™ Ag Sling also features CoolMesh Ag that delivers moisture management and antimicrobial resistance to promote greater patient compliance and outcomes Exercise ball helps promote circulation Closed cell PE foam provides rigid positioning support without adding weight Slotted aluminum airplane platform.Shoulder pain is highly prevalent among musculoskeletal disorders, being the third most frequent reason for medical care in primary care.Indicated for treatment after Bankart and SLAP repairs, rotator cuff repairs, shoulder arthroscopy, separations and dislocations, capsule repairs, humeral fractures and joint reconstruction.
#Abduction of shoulder series
Featuring one of our technology-based materials, CoolMesh™ Ag, the Ranger™ and Ranger™ II Universal Shoulder series delivers innovative, high performance solutions for a wide range of uses.
This secure immobilization restricts motion to allow the injured area to heal and contribute to positive patient outcomes. This customization meets patient’s individual needs and post-surgical protocols and universal sizing reduces inventory and stocking requirements. Use simply with the waistband and arm support for shoulder abduction from 10º to 45º or attach the AP Platform to adjust the amount of shoulder abduction from 45º to 90º.
#Abduction of shoulder full
Ranger and Ranger II AP give you flexibility to adjust the amount of shoulder abduction from 10º to 90º with rotational control from full internal rotation to 70º of external rotation.
0 notes
Text
What Is Nephrology? How Can Telemedicine Play A Vital Role?

Nephrology is associated with the treatment of diseases impacting the kidneys. It is the specialty in internal medicine that helps in diagnosing the disease related to kidneys. A person who is a specialist in treating kidney diseases is known as a Nephrologist. During pandemics, Telemedicine platform has helped many healthcare providers approach maximum patients. It has played a vital role already discussed in this article. Read all the crucial details and understand the role of Telemedicine in Nephrology.
What is Nephrology?
As we have stated above, the study and treatment of kidney-related diseases are done under the Nephrology unit. Kidneys are present just below the ribcage on either side of the spine. It performs numerous vital functions like:
Removing waste and excess fluid from the blood
Maintaining your body’s electrolyte balance
Releasing hormones with functions such as managing blood pressure
What Does A Nephrologist Do?
People who study & treat kidney-related diseases are termed Nephrologists. They not only have expertise on diseases that specifically affect the kidney, but they’re also very intellectual about how kidney disease or dysfunction can affect other body parts.
Although the primary care doctor will function to help or prevent and treat the early stages of kidney disease, a nephrologist may be called upon to help diagnose and treat more severe or complex kidney conditions.
What Conditions Do Nephrologists Treat?
Nephrologists conduct several types of diagnosis and treat the following conditions:
Blood or protein in the urine
Chronic kidney disease
Kidney stones, although a urologist may also treat this
Kidney infections
Kidney swelling due to glomerulonephritis or interstitial nephritis
Kidney cancer
Polycystic kidney disease
Hemolytic uremic syndrome
Renal artery stenosis
Nephrotic syndrome
End-stage kidney disease
Kidney failure, both acute and chronic
A nephrologist can also be involved when other factors cause kidney disease or dysfunction, including:
High blood pressure
Diabetes
Heart disease
Autoimmune conditions, such as lupus
Medications
Role of Telemedicine Software in Nephrology
Telemedicine in rural areas has maximized the capacity and ability to render timely and acceptable healthcare for cases with ESKD. Effective dialysis care requires a staff nephrologist instantly available to coordinate care for dialysis cases and a proper structure for water treatment systems and dialysis outfits.
For these reasons, clinicians in rural hospitals generally transfer cases taking dialysis to other, larger hospitals, occasionally hundreds of long hauls down. These transfers reflect broader poverties in access to timely and effective specialty care services and may lead to poorer issues for the rural population.
An analysis of the sanitarium admission data from Georgia revealed that nearly all cases with ESKD were admitted to indigenous or tertiary care hospitals. Moreover, when the case resides in the primary service area of a near pastoral sanitarium (J. Tannenbaum, J. Lea, D. Brunn, unpublished data).
View Original Source: https://www.vcdoctor.com/blog/what-is-nephrology-how-can-telemedicine-play-a-vital-role
0 notes
Note
And they know, because what they do is resort to childishly insulting Tom
I agree, and I also think that many of them are actually getting more and more pissed because, now that he had his "big debut" as a lead actor in an anticipated series, many people from critics to general audience are actully saying that he was completely miscasted, doesn't have much talent, and lowkey implying that the reason why he got the part was because of who he is in a rs with... and this doesn't reflect with the idea they have of him being the best of the best, and all her exes being losers.
Because, really, trying to shaming Tom for being one of the most iconic characters of an iconic cinematic saga that made modern cinema history (and actually streaming too), when actually their fave's bf flopped at being a leading man, and is still playing tertiary roles in big casts with people way more talented than him, is really pretty pathetic...
Right?
That one moronic Swiffer on twitter told me that JA is suffering from "Kirsten Stewart syndrome", where people think they are acting stiff and emotionless, when actually their characters are written as stiff and emotionless.
Like.......no. Really no. We can recognise bad acting when we see it, thank you very much.
3 notes
·
View notes
Text
Lupine Publishers|To Compare the Retinal and Choroidal Thickness in Fuchs Uveitis Syndrome Patients with Healthy Controls Using Optical Coherence Tomography Seen at Tertiary Care Center
To Compare the Retinal and Choroidal Thickness in Fuchs Uveitis Syndrome Patients with Healthy Controls Using Optical Coherence Tomography Seen at Tertiary Care Center

Abstract
Purpose: To compare the retinal and choroidal thickness in Fuchs Uveitis Syndrome patients with healthy controls using optical coherence tomography seen at tertiary care center.
Method: 16 patients with unilateral Fuchs Uveitis Syndrome (FUS) and 20 healthy control subjects were enrolled in this retrospective study. Spectral domain optical coherence tomography was used to measure the central foveal thickness (CFT), retinal nerve fiber layer (RNFL) thickness and sub foveal choroidal thickness (SFCT) of the eyes with FUS and compared with the unaffected fellow eye and healthy controls.
Results: The mean age of the patients was 35.2 ± 8 years. Seven patients (60%) were male, and nine (40%) were female. Diffuse stellate keratic precipitates (KPs) were seen in all patients. Mild anterior chamber reaction was noted 62.5%. Heterochromia was observed in 87.5% of the eyes, cataract in 43.8% of the eyes, and vitreous cells and debris in 37.5% of the eyes. The mean CFT was (249.7 ± 27.4𝜇m) in affected eyes, (251.5± 23.1 𝜇m) in unaffected eyes of FUS and (253.3 ± 29.2 𝜇m) in healthy control which were statistically insignificant on comparison (𝑝 value > 0.05). The mean SFCT was significantly thinner in eyes with FUS (272.47 ± 13.12 μm) than in the fellow eyes without FUS (316.37 ± 16.13 μm; p = 0.04). and control (320.27 ± 18.15). The average RNFL thickness was found to be (106 ± 14.2 μm) in eyes with FUS, (108 ± 16.5μm) in eyes without FUS and (112 ±13.8μm) in healthy control which were statistically not significant (p value > 0.05).
Conclusion: We conclude that affected eyes in patients with FUS tend to have thinner choroids as compared to unaffected fellow eyes which is consistent with previous studies. It might be associated with chronic inflammation induced choroidal is chaemic changes. Future studies using swept source OCT will further improve precision to get choroid findings more accurate.
Keywords:Choroid; Fuchs Uveitis Syndrome; SD-OCT; Retinal Nerve Fiber Layer
Introduction
Fuchs’ uveitis syndrome (FUS) is an intraocular inflammatory condition that involves anterior segment, lens, vitreous humor and optic disc. It accounts for 2-11% of all uveitis cases [1]. Although many genetic, immunological, vascular and sympathetic theories have been proposed, recent studies show evidence of rubella or herpes simplex virus, toxoplasma association in some cases of FUS [2]. It is a frequently unilateral and typical age at presentation is 30-40 years [3,4]. The diagnostic criteria include stellate keratic precipitates (KPs) scattered diffusely all over cornea, chronic lowgrade anterior chamber reactions, iris atrophy with or without heterochromia, absence of posterior synechiae, vitreous opacities and macular edema [5]. It affects both genders equally and the prognosis is usually good [6]. Iris atrophy and heterochromia are due to atrophy and depigmentation of all iris layers, although it is not pathognomonic. Recently, fluorescein angiography (FA) had provided better information about the posterior segment involvement in FUS [7-9]. Optical Coherent Tomography (OCT) is a routinely employed noninvasive tool in detecting most posterior pole retinal abnormalities. The Enhanced Depth Imaging (EDI) in spectral domain (SD) OCT and swept source (SS) OCT allow visualizing the choroid more accurately [10,11]. Some studies documented the changes in choroidal thickness using EDI-OCT in uveitic conditions, such as Vogt–Koyanagi–Harada (VKH) disease, Behçet disease (BD), ocular sarcoidosis providing remarkable information about disease activity [12,13]. The natural course of the disease is slow to progress, without substantial reduction of visual acuity until significant vitreous opacities or cataract develop. FUS is often misdiagnosed or diagnosed delay leading to posterior subcapsular opacity and elevated IOP mainly due to long-term corticosteroid therapy. There are very few reports in the literature comparing macular, RNFL and choroidal thickness in FUS patients. The purpose of the current study was to measure central foveal thickness (CFT), subfoveal choroidal thickness (SFCT) and retinal nerve fiber layer (RNFL) thickness, in patients with FUS and to compare these with the unaffected fellow eyes and the age, sex and refractive equivalent-matched healthy controls. To the best of our knowledge, it is the first comparative study to evaluate SFCT and other parameters in FUS using spectral domain SD-OCT on FUS from central India.
Material and Methods
This retrospective study was conducted at a tertiary care center from central India. The medical records of 16 patients with FUS and 20 healthy controls between september 2018 and august 2021 were reviewed. Data including age, sex, ocular and medical history, ophthalmic examination, laboratory work-up and OCT parameters were retrieved from patient record. Aii patients had best-corrected visual acuity (BCVA), slit-lamp biomicroscopy, Goldmann applanation tonometry and dilated fundoscopy. The inclusion criteria were diagnosed unilateral FUS based on clinical findings and fundus sufficient for its visualization on clinical examination. Bilateral FUS, history of previous ocular surgery, eyes with dense cataract or media opacity obscuring the visualization of choroid, presence of a coexisting ocular or systemic disease and use of any topical or systemic medications. were excluded from study. The control group consisted of age-, sex-, and refractive equivalent-matched healthy controls who visited ophthalmology clinic for routine examination. The laboratory investigations included complete blood counts, angiotensin converting enzyme, mantoux test and venereal disease research laboratory tests etc. To exclude other causes of anterior or intermediate uveitis. The CFT and RNFL thickness of eyes with FUS were evaluated with SD-OCT and compared with the unaffected fellow eyes and healthy controls. The EDI mode was used to evaluate SFCT. SFCT was defined as the vertical distance from the outermost hyperreflective line of the retinal pigment epithelium (RPE) to choroid-sclera junction under the center of the fovea and was measured using the calipers available within the software. The RNFL thickness (from the inner margin of the internal limiting membrane to the outer margin of the RNFL layer) was automatically segmented using software version. Average RNFL was used for analysis. Statistical analyses were performed with R version 4.0.5. Data were recorded as the mean ± standard deviation (SD). Quantitative data was analyzed using one way analysis of variance (ANOVA) test. An independent 𝑡-test and Chi-square test were used to compare variables between patients with FUS and healthy control subjects. A value of 𝑝< 0.05 was considered to be statistically significant for all analyses.
Results
16 patients with FUS (9 females and 7 males) and 20 healthy control subjects (11 females and 9 males) were included for analysis in this study. The mean age of FUS patients was 35.2±8 years, while it was 38.4± 6years for controls, which was statistically insignificant (𝑝>0.05) (Table 1). Gender differences in both groups were also statistically insignificant (𝑝>0.05). Blurred vision and floaters were the most frequent presenting symptoms {5 patients, (31.3%) and 4 patients (25%) respectively}. Other symptoms included red eye (1 patient, 6.3%), photophobia (1 patient, 6.3%). Three patients were asymptomatic (18.75%), and the diagnosed during a routine eye examination (Table 2). Iris atrophy was present in 5 patients. Heterochromia was present in 14 patients. Cataract was present in 7 patients. Stellate keratic precipitates were noted in all patients. Mild anterior chamber reactions were seen in 10 patients. Vitreous cells or debris were observed in 6 patients (Table 3). The cause of visual impairment was cataract in all cases. The central foveal thickness was 249.7±27.4𝜇m in the affected eyes, 251.5±23.1 𝜇m in the unaffected eyes of FUS patients, and 253.3±29.2 𝜇m in control subjects. There were no significant differences in central foveal thickness between the affected and unaffected eyes of FUS patients (𝑝 = 0.93) or between the affected eyes of FUS patients and the eyes of control subjects (𝑝 = 0.9). The mean SFCT was found to be 272.47 ± 13.12μm in eyes with FUS and 316.37± 16.13μm in eyes without FUS (p = 0.04) and 320.27 ± 18.15𝜇m in the eyes of healthy control subjects. There was choroidal thinning at fovea in the affected eyes of FUS patients compared with the unaffected eyes or control subjects, Average RNFL thickness was 106 ±14.2𝜇m in the affected eyes of FUS patients, 108±16.5𝜇min the unaffected eyes of FUS patients, and 112 ± 13.8𝜇m in the eyes of healthy control subjects (Table 4). No significant differences in RNFL thickness were observed between the affected and unaffected eyes of FUS patients (𝑝 = 0.92) or between the affected eyes of FUS patients and the eyes of control subjects (𝑝 = 0.76)
Table 1: Demographic analysis.
Table 2: Presenting symptoms.
Table 3: Characteristic of FUS patients.
Table 4: Thickness of fovea, sub foveal choroid, and RNFL in FUS & control.
Discussion
To our knowledge, very few comparative studies on FUS patients have been done till yet. In the present study, we compared central foveal thickness, retinal nerve fiber layer and subfoveal choroidal thickness between the affected eyes, the unaffected eyes of FUS patients and healthy controls from central India. Although we found choroidal thinning at fovea in the affected eyes of FUS patients compared with the unaffected eyes of FUS patients or control subjects, there was no statistically significant difference in RNFL and central foveal thickness. FUS was first described in 1906, recent studies have focused on various viral agents and the etiology of FUS remains controversial. In FUS, persistence of chronic lowgrade inflammation for years leads to various degrees of atrophy of the iris and ciliary body. As the choroid being more vulnerable to the effects of the inflammatory and vascular diseases than other tissues, imaging of choroid is important for understanding the pathophysiology of various diseases. EDI mode using SD-OCT devices enables cross-sectional, high resolution better visualization of the choroid. Many studies have documented the effect of various acute and chronic ocular inflammatory conditions on choroidal abnormalities. Nakayama et al. showed that choroidal thickness as a marker for the degree of choroidal inflammation in acute Vogt- Koyanagi-Harada disease using EDI-OCT [14]. Kim et al. found an increase in subfoveal choroidal thickness in the acute phase of Behcet’s posterior uveitis [15]. Multiple studies suggest that increased blood flow and choroidal effusion is the mechanism responsible for choroidal thickening in acute inflammation [16,17]. However, Coskun et al. observed the thinning of subfoveal choroid in chronic Behcet’sassociated posterior uveitis probably due to chronic inflammation induced fibrosis [18]. Very few studies from Turkey and Italy like Balci and Ozsutsus, Kardes et al. and Carquaglia et al. showed the comparison between the affected and fellow eye in FUS patients [19-21] (Table 5). The study by Kardes et al. had findings consistent with the study of Balci and Ozsutsus. We propose that chronic anterior chamber and vitreous inflammation in eyes with FUS may affect choroidal perfusion, which may result in ischaemic changes leading to atrophy and fibrosis of the choroid tissue, thereby reducing choroidal thickness. Limitations of our study is being retrospective nature and small sample size. We have used SD OCT in this study and with advent of new imaging methods designed specifically for the choroid, SS OCT which allows examination of the choriocapillaris, and larger choroidal vessels more clearly can further improve precision to determine the inner and outer boundaries of the choroid findings in the future. To conclude, we found subfoveal thinner choroid in FUS as compared to uninvolved fellow eyes, but we could not find a statistically significant comparison of foveal and RNFL thickness in FUS versus unaffected eye. Our findings are also consistent with those of previous studies. As this is the first analysis of its kind from central India, longitudinal studies with large sample size would help in more understanding of the effect of chronic inflammation on the choroid in FUS in future.
Table 5: Comparison between different studies of mean sub foveal choroidal thickness (SFCT).
For more information about Trends in Ophthalmology Open Access Journal archive page click on below link
https://lupinepublishers.com/ophthalmology-journal/archive.php
For more information about lupine publishers page click on below link
https://lupinepublishers.com/index.php
#lupine publishers#lupine publishers group#lupine publishers LLC#trends in ophthalmology open access journal#tooaj
2 notes
·
View notes
Text
The Sarm Holy Bible.
Ostarine
Content
Kate Somerville Peptide K8 Power Lotion.
Production Of Bioactive Peptides By Lactobacillus Species: From Gene To Application.
Peptides Established Of 12 ₤ 220.
What Are Sarms?
Vip Whatsapp Team For Inner Promotions And Sarms Online Forum.

The partner or combining particle may be carbohydrate or non-carbohydrate in nature. If the outcome of UCPCR runs out maintaining with various other scientific finding then we would certainly recommend duplicating the test particularly if it is suddenly reduced. People tipping out boric acid preservative from urine collection tube, in an example taking greater than 3 days to reach the laboratory can lead to unnaturally low outcomes. A control experiment is one that is treated in the same way as an actual experiment, however is not exposed to the speculative agent. There are two kinds of controls for experiments, positive and also unfavorable controls.
Nate Diaz tested positive for trace amounts of a SARM, not suspended for UFC 244 - Bloody Elbow
Nate Diaz tested positive for trace amounts of a SARM, not suspended for UFC 244.
Posted: Fri, 25 Oct 2019 07:00:00 GMT [source]
It is a weird kind of glycosidic bond in which the sugar moiety is attached straight to the carbon atom of the other molecule. It is formed as a result of the response between the carbonyl team of a sugar particle and an alkyl substance like methane and so on . This bond is developed as a result of a response between the carbonyl team of a carbohydrate or its derivate and also a hydroxyl team of a few other substance. The carbonyl group of carb might be a part of an aldehydic group or a ketonic group. A molecule of water is released in this procedure, making it an irreparable reaction. It is a main bond or a covalent bond that offers to connect carbohydrates to other groups or particles.
Kate Somerville Peptide K8 Power Cream.
This slide collection is appropriate as an intro to the subject of peptide ligands. When the charge is related to the electrodes, the various amino acid will certainly move at different speeds to the corresponding electrode. The rate at which they move as well as to which electrode they take a trip to is recorded as well as compared on the glass substrate. Series of bands are developed from their motions which are called Electropherograms. Electropherograms are lines that are created from the motion of the healthy proteins to the electrodes. is the molecular mass of the neutral N-terminal group, is the molecular mass of the neutral C-terminal team, is molecular mass of the neutral amino acid deposits. To acquire m/z values, add or deduct protons as required to get the required charge as well as divide by the variety of fees.

The types of piece ions observed in an MS/MS spectrum rely on lots of variables consisting of main sequence, the quantity of inner power, exactly how the power was introduced, cost state, etc . The approved nomenclature for fragment ions was very first suggested by Roepstorff and Fohlman, as well as consequently modified by Johnson et. Along with the structural characterisation of healthy proteins the center also provides high-throughput protein-ligand testing. Commonly, 10-20μM of protein is required with a 100-fold excess of ligand Using automation multitudes of compounds can be swiftly screened. Hits can be further verified making use of protein-detect methods (1H-15N or 1H-13C HSQC).
Manufacturing Of Bioactive Peptides By Lactobacillus Varieties: From Genetics To Application.
A positive control experiment is one that uses a representative understood to generate a measurable and well recognized effect on the system. In contrast, an adverse control experiment is one that makes use of the same treatments as the real experiment, however has no additional treatment or utilizes an agent that is anticipated to be inactive. Kathy Taylor-Brewin of Biography Active Elegance is a specialist in peptide skin care, distributing the Hydropeptide array in the UK.
youtube
To obtain a2-, subtract 2 protons from the Mr worth for an as well as divide by 2. The structures showed above recommend ions with a single positive charge. Mascot likewise consists of assistance for adverse ions, as well as the unfavorable ion types are the same as positive, however with one proton per fee deducted instead of included. We welcomefeedbackconcerning any kind of added ion types that must be taken into consideration. One of the most bountiful fragment ion types observed in MALDI-TOF PSD are a, b, and also y. If accident gas is made use of, after that the ranges look like high energy CID.
Peptides Established Of 12 ₤ 220.
" Hydropeptide integrates each classification of peptide in its VLR technology," comments April Zangl, Chief Executive Officer of Hydropeptide. " VLR technology is made to improve peptide efficiency optimising anti-ageing results. Comparable to a lock as well as secret, peptides call for a certain range, concentration degree and repetition for noticeable age opposing outcomes. N-terminal professional B-type natriuretic peptide (NT-proBNP) is a non-active peptide released along with the active peptide hormone BNP when the wall surfaces of the heart are extended or there is pressure overload on the heart e.g. by liquid overload. BNP then acts upon the kidneys triggering fluid as well as sodium loss in the pee as well as moderate vasodilation so launching the pressure.
Furthermore, more studies are needed in connection with the possible use of collagen supplements in skin problem like eczema. As a matter of fact, collagen is thought to compose around 75% of our skin's completely dry weight. Kind I collagen is crucial for skin flexibility as well as stamina, and a loss of collagen in the skin, which happens naturally with aging, can result in wrinkles. Hydrophobic interactions are important in maintaining the tertiary and also quaternary structure of healthy proteins. The variety of hydrogen bonds formed by an electronegative atom depends upon the variety of totally free electrons present in its outer covering. Oxygen has two cost-free electrons and thus can create 2 hydrogen bonds while nitrogen forms just one hydrogen bond because of one free electron.
What Are Sarms?
Glycosidic bond undertakes deterioration in a process called glycolysis. It is a hydrolytic process in which a water molecule is utilized to break the glycosidic bond as well as release the carb and various other residues. The substances with S-glycosidic bonds are called S-glycosides as an example Sinigrin. It is a harmful compound found in some plants like seed of black mustard etc . In this sort of glycosidic bond, the sugar residue is affixed to the sulfur group of the non-carbohydrate compound. It is developed when the carbonyl team of sugar reacts with the thiol (- SH) group of the other compound.
What is Ostarine used for?
Ostarine is used by mouth to improve athletic performance and for involuntary weight loss in people who are very ill, also known as cachexia or wasting syndrome.
There are no well-known medication interactions and we do not yet recognize what the most effective dose of collagen is. Research studies have used everyday doses of in between 1-- 10 g collagen hydrolysate as well as 0.1-- 10 mg of chicken or bovine kind II collagen. It's been recommended that taking collagen hydrolysate can enhance the signs and symptoms of osteo arthritis by promoting your body's manufacturing of joint collagen. Rather than MHC course I, MHC course II particles do not dissociate at the plasma membrane. The systems that manage MHC course II deterioration have not been developed yet, however MHC class II molecules can be ubiquitinised and then internalised in an endocytic pathway.
Vip Whatsapp Group For Inner Promos And Also Sarms Forum.
Austria bpc157 how does it work of basic NMR ranges extracts from a couple of mins to 3/4 days for every experiment. A complete collection of experiments for protein structure decision typically takes concerning 7-14 days. When it comes to reasonably small healthy proteins, current innovative multidimensional information acquisition plans have been successfully used to decrease speculative acquisition time by approximately an order of magnitude or more. There was no evidence of increased side-effects in individuals taking kind II collagen, although trials did report individuals withdrawing due to the fact that they thought the collagen had not been improving their symptoms. Although individuals in both groups enhanced in the kind II collagen and also methotrexate test, the methotrexate individuals revealed the best enhancement.
Is SARMs considered natural?
Short for selective androgen receptor modulators, SARMs are synthetic drugs designed to have effects similar to those of testosterone. SARMs are still in the research and testing stages for various medical conditions but have not been approved yet for any other use.
It can form extra phosphodiester bonds at both ends due to having a complimentary hydroxyl team at the 3' end as well as a complimentary phosphate group at the 5' end. The ester affiliation is a really high-energy bond launching a remarkable amount of power upon hydrolysis. Like the remainder of the bonds talked about previously, it is additionally damaged down by incorporating a water particle.
Fragments will only be spotted if they carry at least one charge. If this cost is kept on the N incurable piece, the ion is classified as either a, b or c. If the charge is retained on the C terminal, the ion kind is eitherx, y or z.
Hormone or peptideMajor cells places in the gutPrincipal recognized actionsGastrointestinal peptides, their website of expression as well as significant functions. The gastrointestinal hormones make up a team of hormones secreted by enteroendocrine cells in the tummy, pancreatic, and also tiny intestine. This team of hormones regulate different functions of the digestion organs. This 60-slide slide collection available from Slideshare.net gives a great introduction of endogenous peptides and also choose instances of useful drugs. Medications reviewed consist of those that imitate the impacts of endogenous peptides and also those that are villains.
All ion collection can be come with by composition dependent satellites as a result of loss of ammonia or water. Collision induced dissociation of ions at keV energies can generates extra ion types because of side chain bosoms,. Keep in mind that these frameworks include a single charge carrying proton. In electrospray ionisation, tryptic peptides usually lug 2 or even more fees, to make sure that piece ions may carry more than one proton.
Cardarine is a pharmaceutical grade PPAR agonist which has some extremely useful effects for professional athletes.
Because some SARMs are best for bulking as well as others are shown to be specifically efficient for cutting, they're sometimes combined, or stacked, in research studies.
These manufactured SARM-derived metabolites can conveniently be utilized as reference standards for routine mass spectrometry-based doping control analysis of at the very least three generally used performance-enhancing drugs to unambigously recognize misbehavior.
RAD 140 SARM-- a SARM with effective anabolic impacts for improving muscle development, as well as appealing benefits for your mind.
We have actually made a team where sarms users can share their progress, experiences as well as to talk with each various other concerning their cycles and also progress.
view site will be noticeably lowered which means you can boost the intensity and period of your exercises.
An ester bond is formed when a molecule having the carboxylic group responds with an additional molecule having a hydroxyl group. The carboxylic group loses its hydrogen as well as oxygen while the alcohol loses hydrogen of its hydroxyl group. Consequently, a water molecule is released, and the two carbons are linked using an oxygen bridge creating a -COC- link.
#BPC157 EU#BPC157 Europe#information BPC157 EU#information BPC157 Europe#EU BPC157 how does it work#Europe BPC157 how does it work
1 note
·
View note
Text
Soo...
Guess Who just marathon all of Miraculous Ladybug?
....
This Girl right here! Said I wasn't going to post on this hellsite but here we fucking are!
And I'm still feeling hollow/frustrated/cheated all at the same time.
*longgg sighs insert hurr*
I'm not going to go off on a spiel....yet! (I think I did enough ranting on PM in Discord to gather the energy to do it again)
Just know a few things Im about to yell into this stank ass void:
1. I LOVE Andrien(Chat Noir)/Marinette(Ladybug) with all my FUCKING SUGAR DRENCHED HEART! And you'll have to literally pull this fucking ship from my cold dead hands!
And Imma need the writers to stop TEASING me! Srsly I can't get marginally excited by almost miss calls to them getting revealed to each other....and then that damn episode Chat Blanc happens and I-
Y'all didn't have to do me dirty like that writers. And even though I KNOW how its going to end...there's still a small part of me going: This is a cartoon and NOT one of my Asian Dramas but goddamn does it feel like it's gonna end like one......*UGLY FUCKING SOBBING AND SCREAMING*
2. Alya/Nino is also a ship i will go to hell for and the best friends/wingman for their dorky asf friends! Srsly; Alya is the friend Mari needed in her life because I don't think our Miss Ladybug would be as she is without a strong friend supporting her when you have girls like Chloe and...fucking LILA...*breathes* always starting shit.
3. AGGRESSIVELY has a love/hate relationship with Chloe: writers please! PLEASE! I'm trying with her I rly am but I don't have patience...
4. FUCKING L.I.L.A....*INTERNAL SCREAMING* well I guess there has to be a Cersei in every damn show...
Can you tell I have utter loathing for this character? Cause I do.
5. FUCKING HAWK MOTH!!... I'm calm, I am good....rly I fucking am. What do ya mean I'm not fine? I'm FUCKING GUCCI! TOTTES CHILL ASF!
I know it was an alternate future time *gross sobbing again* but if there was a moment in Chat Blanc that would have given me some...hint that Gabriel cares...like truly cares for Andrien (even in his own way...) My god that was NOT it....
I told myself i was not going to rant...yet
5.5 So..yeah didn't know I was going to feel bad in a way for Nathalie but my heart...
6. Luka can get it tho. In the very small...tiny off chance it don't work out for my girl, please writers just throw me a bone for Luka/Marinette please! Luka is giving me serious K-Drama 2nd Male Lead Syndrome...AND I TOOK A REST FROM DRAMAS TO STOP HAVING THESE FUCKING FEELINGS MLB! I was not prepared for my guy to just come in all smooth on the guitar wooing my girl. PLEASE 4 ME JUST GIVE ME A MOMENT!
*sighs* I...I need Mari to breathe for a moment without Andrien on her mind...I have my reasons....
7. Kagami: I was lukewarm to her *srsly I was getting a bit annoyef with Andrien's unwanted harem being filled with bitchy girls I can't stand and god i can't help my knee jerk reaction of: PLEASE don't be another bitch female char, 2 is enough!
In short: SHE'S A MOFO DRAGON!! and i...mayormaynotlow...lowkeyshipherwithandrienorjustandreinandmarinetteasaot3*coughs*
8. Other Secondary/Tertiary characters are good i can't complain; the other students from their class is just good. They're good kids and surprisingly have some depth to them I think.
That is all for now...*going to aggressively draw chat noir/ladybug fanart now while listening to wuxia C-Drama osts
#miraculous ladybug#adreinette#lukanette#marinette dupain cheng#marinette dupen chang#alya cesaire#nino x alya#all the mlb characters because#im too damn lazy to tag all this shit!
13 notes
·
View notes
Photo



I fixed the spelling error and added more about how MAOIs work and their side effects.
Aside from imipramine and Doxepin, TCAs include amitriptyline, nortriptyline, and other “-triptylines.”
Bupropion (Wellbutrin) is a DA and NE reuptake inhibitor. Mirtazapine (Remeron) is an alpha 2-adrenergic receptor antagonist.
MAOIs are not used as first-line agents because of the increased safety and tolerability of newer agents, notably SSRIs/SNRIs. However, MAOIs are used for certain types of refractory depression and in refractory anxiety disorders: Phenelzine (Nardil), tranylcypromine (Parnate), isocarboxazid (Marplan).
HAM side effects (antiHistamine—sedation, weight gain; antiAdrenergic— hypotension; antiMuscarinic (anticholinergic)—dry mouth, blurred vision, urinary retention, constipation, exacerbation of neurocognitive disorders (i.e., dementias). Found in tricyclic antidepressants (TCAs) and low-potency anti - psychotics.
Serotonin syndrome: Confusion, flushing, diaphoresis, tremor, myoclonic jerks, hyperthermia, hypertonicity, rhabdomyolysis, renal failure, and death. Occurs when there is too much serotonin, classically when selective serotonin reuptake inhibitors (SSRIs) and monoamine oxidase inhibi-tors (MAOIs) are combined. As this combination is rarely seen in practice anymore, serotonin syndrome is more commonly seen when a patient is prescribed multiple medications with serotonergic activity (e.g., SSRIs/SNRIs, trazodone, Tramadol, triptans, dextromethorphan, St. John’s wort, ondansetron). Treatment: Stop medications, supportive care.
Hypertensive crisis: Caused by a buildup of stored catecholamines; triggered by the combination of MAOIs with tyramine-rich foods (e.g., red wine, cheese, chicken liver, cured meats) or with sympathomimetics.
Extrapyramidal side effects (EPS): Parkinsonism—masklike face, cog-wheel rigidity, bradykinesia, pill-rolling tremor; akathisia—restlessness, need to move, and agitation; dystonia—sustained, painful contraction of muscles of neck, tongue, eyes, diaphragm. Occur more frequently with high-potency, typical (first generation) antipsychotics, but can also be seen with atypical (second generation) antipsychotics. Reversible. Occur within hours to days of starting medications or increasing doses. In rare cases, can be life threatening (e.g., dystonia of the diaphragm causing asphyxiation).
Hyperprolactinemia: Occurs with high-potency, typical (first generation) antipsychotics and risperidone.
Tardive dyskinesia (TD): Choreoathetoid muscle movements, usually of the mouth and tongue (can affect extremities, as well). Occurs after years of antipsychotic use (more likely with high-potency, first-generation antipsychotics). Usually irreversible.
Neuroleptic malignant syndrome: Mental status changes, fever, tachycardia, hypertension, tremor, elevated creatine phosphokinase (CPK), “lead pipe” rigidity. Can be caused by any antipsychotic after a short or long time (increased with high-potency, typical antipsychotics). A medical emergency with up to a 20% mortality rate.
Drug interactions: Cytochrome P450 is a group of enzymes in the liver that metabolizes many common drugs, including psychiatric medications. Some medications induce the system, in other words the system metabolizes medications faster—drug levels decrease. Some medications inhibit the system, in other words the system metabolizes medications more slowly—drug levels increase. Common cytochrome P450 enzymes important in metabolizing psychiatric medications include CYP3A4, CYP2D6, CYP1A2, CYP2C9, CYP2C19.
Important CYP450 inducers include: Tobacco (1A2), Carbamazepine (1A2, 2C9, 3A4), Barbiturates (2C9), St. John’s wort (2C19, 3A4). Important CYP450 inhibitors include: Fluvoxamine (1A2, 2C19, 3A4), Fluoxetine (2C19, 2C9, 2D6), Paroxetine (2D6), Duloxetine (2D6), Sertraline (2D6).
New form, desvenlafaxine (Pristiq), is the active metabolite of venlafaxine; it is expensive and without known benefit over venlafaxine.
Bupropion (Wellbutrin) can decrease the seizure threshold and is contraindicated in pts with bulimia. Tricyclic antidepressants include amitriptyline, imipramine (treats enuresis), clomipramine (treats OCD), and doxepin (may be used as a sleep aid in low doses). Amitriptyline, imipramine, clompiramine, and doxepin are tertiary amines (highly anticholinergic/antihistaminergic [more sedating]/antiadrenergic [more orthostasis] with a greater lethality in overdose). Secondary amines (metabolites of tertiary amines (less anticholinergic/antihistaminic/antiadrenergic) are nortriptyline and desipramine. Tetracyclic antidepressant = amoxapine.
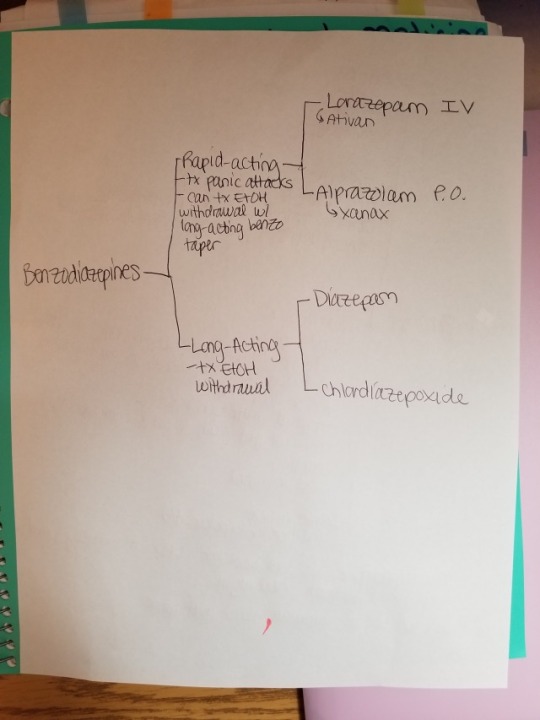
#antidepressants#mood stabilizers#TCAs#MAOIs#SNRI#SSRI#benzos#benzodiazepines#pharm#zoloft#tyramine#wellbutrin
6 notes
·
View notes
Text
Lupine Publishers | Outcome Analysis of Anticoagulant Therapy in Critical Care Unit: The Need for a Pharmacy Managed Anticoagulant Service

Lupine Publishers | Journal of Cardiology Research
Abstract
Background: In our center, NCTCE, there are 2 intensive care units (general and cardiac), where critically ill patients are admitted and managed. Anticoagulation is usually indicated in such patients for atrial fibrillation, valve replacement and DVT prophylaxis.
Objective: To determine the role of a clinical pharmacist in the therapeutic and clinical appraisal of such patients on anticoagulation.
Materials and Method: Over a 2-year period (June 2015 –May 2017), a study design to determine the role of a clinical pharmacist in anticoagulant treatment was made in both ICU. This was a prospective longitudinal study. Here, demography, the anticoagulation on which interventions were made on, duration of admission, areas and determinants of a clinical pharmacist’s interventions were incorporated. Others included, were levels of intervention, acceptance and rejection of the interventions as well as the outcome.
Results: During the study period, 168 patients were used. Male (72) and female (96), with a female to male ratio of 1:1.3. Indications for anticoagulation were DVT prophylaxis (14.88%), valves (83.90%) and AF (1.10%). Among the anticoagulants on which interventions were made on, warfarin was the highest (53.57%) while heparin was the least (2.90%). Duration of admission ranged from 2-40 days. Areas of intervention were on effectiveness of therapy (18.70%), drug-drug interactions (16.43%), adverse events (32.86%), dosage (11.05%), Kidney function (1.70%), adherence (6.70%) and drug selection (2.27%). Levels of intervention were at prescriber (30.51%), drug (38.56%), patient (25.42%) and laboratory (5.51%). The outcome was that majority of patients (78.74%) had their problems resolved.
Conclusion: Anticoagulation therapy of patients in ICU requires precise damaging, monitoring and appropriate patient education so as to ensure that patients benefit maximally. A clinical pharmacist has a vital role to play in the above areas.
Abbreviations: ICU: Intensive Care unit; PhRs: Pharmacist Recommendations; INR: International Normalized Ratio; ACCP: American Critical Care Physician; ADES: Adverse Events; VTE: Venous Thromboembolism; DTPS: Drug Therapies; DDI/DFI: Drug Drug/Dug Food Interactions; LMWH: Low Molecular Weight Heparins; CVP: Central Venous Pressure; CHADS: Congestive Heart failure, Hypertension, Age, Diabetes, Stoke
Introduction
Intensive Care Unit is a unit of the hospital where critically ill patients are treated by specially trained staff (ICU-Multidisciplinary team), comprising of doctors, nurse specialists, respiratory therapists, clinical pharmacists, physiotherapists, dieticians, theatre technicians, biomedical engineers and social workers. In our center, there are 2 ICU: -
a) The general ICU for general surgery, orthopedic, neuro-, obstetrics, thoracic and trauma surgical and medical patients.
b) The cardiac ICU for perioperative open-heart surgery patients as well as those patients with myocardial infarction and acute coronary syndromes.
Critical care pharmacy services in the ICU have expanded from traditional dispensing responsibilities to being recognized as an essential component of multidisciplinary care for critically ill patients. Augmented by technology and resource utilization, this shift in roles has allowed clinical pharmacists to provide valuable services in the form of assisting physicians and clinicians with pharmacotherapy decision making, reducing medication errors and improving medication safety systems to optimize patient outcomes. Documented improvements in the management of infections, anticoagulant therapy, sedation, and analgesia for patients receiving mechanical ventilation and in emergency response help to justify the need for clinical pharmacy services for critically ill patients [1].
ICU patients have similar general risk factors for venothrombosis and pulmonary embolism as well as arterial thromboembolism manifesting as stroke, mesenteric vascular occlusion and peripheral acute limb ischemia, with other patients (age, obesity, immobilization, past personal/family history of venothrombembolism, sepsis, cancer, stroke, respiratory, heart failure, pregnancy, trauma or recent surgery) [2-4]. In addition, they have other peculiar risk factors as a result of their illnesses and/ or treatment (vasopressor use, respiratory failure, heart failure, pharmacologic sedation, mechanical ventilation, central venous pressure (CVP) catheter and end stage renal failure) [3,5]. CVP catheter in the femoral, subclavian, internal jugular and superior vena cava veins have catheter related thrombosis occurrence rate ranging from 10-69%, 2-10%, 40-56% and 7-17% respectively [2,5-7]. There is also 4-fold increased risk of pulmonary embolism from lower limb DVT in ICU patients [8]. Catheter related VTE risks increases proportionate to the duration of placement and if patient is not on LMWH anticoagulant [9]. Sepsis induce procoagulant status and favor catheter related VTE [6,10]. Vasopressor treatment is not an independent risk factor for VTE [5], however it is still linked with decreased absorption of subcutaneous heparin due to the vasoconstriction of peripheral blood vessels [11]. Platelet transfusion and high platelet levels, a common finding in ICU patients are risk factors for VTE [12]. Pharmacologic sedation is not an independent risk factor for VTE, however, when used alongside mechanical ventilation, it is. Mechanical ventilation by decreasing venous return and requiring sedation and immobilization is a risk for VTE, however, critical ill patients requiring long mechanical ventilation was compared with those who did not and the relationship between duration of mechanical ventilation and VTE was not established [2].
The implantation of an artificial heart valves exposes the patient to an increased risk of valve thrombosis and embolism; thus life- long oral anticoagulation is imperative [13]. The factors that lead to increased thromboembolism in such patients are the number of valves implanted, types of valves implanted (more in ball and cage variety), atrial fibrillation, left atrial enlargement, left ventricular dysfunction, clotting disorder and previous embolic events [14]. Atrial fibrillation is the most common arrhythmia in patients admitted in intensive care units (ICUs) and is associated with increased morbidity and mortality [15,16]. The problems of atrial fibrillation are low cardiac output, heart failure, hypotension and organ dysfunction as well as thromboembolism. CHADS algorithm defines the risk factors, which many critically ill patients have [17]. In addition, patients with rheumatic heart diseases, prosthetic heart valves, prio thromboembolism and persistent atrial thrombus detected by TEE as well as AF with complex atherosclerotic aortic plaque are considered at highest risk of embolic stroke if not on thromboprophylaxis [18]. In our ICU, the clinical pharmacist supervises the prescribed anticoagulant, dispenses them, monitors adverse effects, drug-drug interactions as well as compliance. These factors among others have a great role to play in the successful thromboprophylaxis and treatment of VTE and prevention of anticoagulant induced bleeding including arterial thromboembolism on account of prosthetic mechanical heart valves and atrial fibrillation.
Materials and Method
Over a 2-year period (June 2015 –May 2017), a study was designed to determine the role of a clinical pharmacist in anticoagulant treatment was made in both general and cardiac ICU of a tertiary hospital in Nigeria, a developing country. This was a prospective study. Here, demography, types of anticoagulation intervention was made on, duration of admission, areas and determinants of a clinical pharmacist’s interventions were incorporated. Others included were levels of intervention, acceptance and rejection of the interventions as well as the outcome. The general ICU admits critical general, orthopedic, neuro-, thoracic, trauma surgical and medical patients. The cardiac ICU admits perioperative open-heart surgical patients including patients with myocardial infarction and acute coronary syndromes. The data were analyzed using Microsoft Excel 2010 and presented as frequencies and percentages using tables and charts.
The study design was approved by the hospital ethical committee.
Transplantation eligibility is always considered with regard to risk factors, especially, pulmonary hypertension (Figure 2). Right heart catheterization must be performed in all potential candidates for heart transplantation in order to quantify pulmonary vascular resistance [7]. Right heart failure is a substantial cause of mortality. Right ventricular failure is likely when post implant pulmonary artery pressures exceed 50 mmHg. Patients with chronic heart failure may develop pulmonary hypertension due to elevated left ventricular end diastolic pressure with elevated left atrial and pulmonary venous pressures. This is a reactive form of pulmonary hypertension and may fall when the cardiac output is increased with inotropes or unloaded with nitrate infusions [7]. The transpulmonary gradient is calculated by subtracting the left atrial filling pressure from the mean pulmonary artery pressure. A fixed transpulmonary gradient in excess of 14 mmHg is associated with greatly elevated risk, and thus this cut off is used in the UK [8]. In such patients a destination therapy strategy may be used with continuous flow LVADS.
Results
Figure 1 shows the age ranges of patients admitted during the study period. Highest range is 31-40 years. Least is 81-90 years. Also Figure 2 shows additional indications for anticoagulation, with mechanical prosthetic heart valves having the highest number while atrial fibrillation takes the least. Table 1 shows the anticoagulants administered and the number of interventions made on them. The highest number of interventions was made on warfarin, followed by enoxaparin while the least intervention was made on nonpharmacologic anticoagulant, elastic stockings. Table 2 of the 353 interventions made, adverse events (32.86%0 was the highest followed by effectiveness of therapy (18.70%), using laboratory indices of International Normalized Ratio (INR). The least determinant of intervention was drug-drug interaction of which (2.27%) interventions were made. Figure 3 depicts the duration of admission in days. Here the shortest duration of admission was in most people (66.7%) while the longest admission in a few patients (1.2%).
Table 1: Anticoagulants on which intervention was made.
Table 2: Highlights the roles of a pharmacist.
Figure 1: Age range of patients admitted in ICU.
Figure 2: Indications for anticoagulation.
Figure 3: Duration of admission (days).
Discussion
Intensive care Unit (ICU) is a potential area for drug therapy problems (DTPs): patients treated are complex patients [19]. The use of thromboprophylaxis or prophylactic anticoagulant in critically ill patients is pertinent. ACCP recommends thromboprophylaxis for prevention of VTE in critical care patients (grade 1a – strong recommendation with high quality of evidence [20,21]. Omission of thromboprophylaxis within the first 24 hrs of ICU admission without obvious reasons is associated with a higher risk of mortality [22]. Demographically, 168 patients admitted in ICU over 2 years (84-patients/year) had anticoagulation therapy. 96 females and 72 males were involved with a ratio of 1.3:1. The age ranges were from 0-10 to 81-90 years with highest number that received anticoagulation being 31-40 years. The bulk of those with valve prostheses replacement came from this group. Duration of anticoagulation therapy paralleled relatively the duration of admission in ICU. In this study, the longest duration was 40 days while the least was 5 days. Overall, the average length of hospital stays amounted to 0.24 day/patient. Prospective evaluation of daily pharmacist-managed inpatient anticoagulation services was compared with a matched historical control group who received physician-managed anticoagulation in a 400-bed university teaching hospital [23]. *26A. Those who received pharmacistmanaged anticoagulation had significantly shorter hospital length of stay (6.8 days vs 9.5 days, P 5 .009), fewer supratherapeutic INR 3.5 (27% vs 62%, P , .001),Fewer readmission rates for bleeding or thrombosis within 1 to 3 months after discharge and no differences were noted between the groups INR ratio at discharge (2.6 vs 3.3, P 5 .07) as well as number of bleeding complications (6 vs 1, P 5 .11).
Pharmacists have been incorporated into ICU multiprofessional staff to improve the care provided to patients, particularly by monitoring the drugs administered and assessing their efficacy, thus contributing to improving patient safety [24]. The participation of clinical pharmacists in routine ICU care mainly includes active involvement in daily rounds, where they provide relevant information to the medical and nursing staff, analysis and monitoring of the efficacy of pharmacological treatments, implementation of medication reconciliation, and prevention, identification, and reporting of adverse reactions [25-27]. The actions performed by clinical pharmacists relative to the monitoring of pharmacological treatment are referred to as pharmacist interventions or recommendations (PhRs) [24,28]. Such professional interventions presuppose actions targeting pharmacological treatment to correct or prevent negative clinical outcomes derived from the use of medications. In the light of the above, the pharmacist role in the anticoagulant therapy for patients admitted in our institutional ICU was done. His/her actions in managing patients in anticoagulation in ICU in terms of monitoring of the pharmacological therapy of the anticoagulants are referred as interventions or recommendations. There have been several reports related to such interventions internationally in patients admitted in ICU [1,29]. Similar reports are rare in developing countries like Brazil including Nigeria. A retrospective chart review conducted at Baylor College in USA, in 2000 [30], showed four main variances related to warfarin therapy. They were inappropriate administration of warfarin loading dose, use of vitamin K when not recommended by American College of Chest Physicians guidelines, inconsistent overlapping of heparin with warfarin and inconsistent provision of patient education [30]. In this study, the determinants of the interventions ranged from effectiveness of therapy to drug selection, see Table 2. With this subgroup of effectiveness of therapy, international Normalized Ratio was used to monitor dosages which enabled the pharmacist to classify them as sub therapeutic, therapeutic and supratherapeutic.
Figure 4: Level of intervention.
Figure 5: Acceptance of intervention.
Figure 6: Outcome of intervention.
In this same scenario, drug-drug or drug-food interactions were monitored and classified as minor, significant or serious, see Table 3. When the effectiveness of therapy was supra or sub therapeutic, and when the DDI/DFIs were significant or serious, pharmacist intervened or made recommendations. The same scenario applied to adverse reactions, adherence to therapy as well as kidney function. These recommendations were made at multiple levels ranging from physicians/prescribers’ level to laboratory level. In view of the fact this pharmacist’s interventions or recommendations are novel in our institution and indeed in Nigeria, many interventions were accepted while some were rejected, see Figure 4. The outcome of such interventions is shown in Figures 5 & 6, indicating excellence when such recommendations are accepted. In a prospective, interventional study in a multidisciplinary ICU of a rural district hospital in Bathalapalli, Andhra Pradesh, India by Pichala et al. 72 patients were screened for DTPs, 947 drug doses prescribed, 148 prescriptions, 6.39 drugs per prescription and 13.15 drugs per patients of 243 DTPs identified, 1.67 DTPs present were prescriptions, drug interactions 78%, inappropriate indication 7.4%, ADRs and therapeutic duplications 2%. 47% of the interventions were accepted. This was significantly lower when compared with our study. ICU SUCCESS DEDICATED PHARMACIST study done by Leape et al., concluded that: participation of the pharmacist on medical round can be a powerful means of reducing the risks of ADEs, in the ICU 99% of pharmacist recommendations to medical staff were well accepted, an existing pharmacist intervention required no additional resources; instead it represented a different use of existing pharmacists’ time.
Table 3: Determinants of pharmacist’s roles.
Conclusion
Anticoagulation treatment of patients in ICU requires precise dosing, a defined anticoagulant management programme, approved protocols, proper monitoring by clinical pharmacist (base line and follow-up INRs), education of patients and families about: dietary restrictions, monitoring follow up, drug interactions for outpatient and inpatient components. All these will result in improvement in the INR results, significant clinical outcomes and overall quality of care.
https://lupinepublishers.com/cardiology-journal/pdf/ACR.MS.ID.000126.pdf
For more Lupine Publishers Open Access Journals Please visit our website https://lupinepublishers.us/
For more Journal of Cardiology Research articles Please Click Here: https://www.lupinepublishers.com/cardiology-journal/
To Know more Open Access Publishers Click on Lupine Publishers
Follow on Linkedin : https://www.linkedin.com/company/lupinepublishers
Follow on Twitter : https://twitter.com/lupine_online
4 notes
·
View notes
Last Seen Blogs
ilyass-world
ilyas

tis-the-smallest-fry
Hello There.

whydowe
zoey

insperationalblogs
Insperational blogs

marcybotics
MARCYBOT