#Functional Medicine Diagnostics
Text
...
#head instructor to the TAs in the lab section i TA for: how r u guys feeling abt the workload?#me who hasnt graded anything since week 1 and spent an hr that morning filling out a patient safety plan: 🙃#listen. we r experiencing symptoms that make us shitty at our job. which is not helpful for a positive outlook#i was also experiencing horrible cramps at the time bc i lost my ibuprofen and 2 days ago i stopped the birth control in a desperate effort#to stop feeling terrible. but in this moment i feel alright. its wild to go from drastically unhappy to like lol wtf was that? anyway stop#being a bby loser. for no obvious reason. im gonna start the birth control again to see if i get depressed again or if that was just me lol#i dont think my therapist understands the depth of my executive functioning issues tho. bc im a grad student and can meet deadlines. like#let me tell u im a fucking disaster abt starting things. i will go back and forth and get nothing done forever. or i do things halfway and#make everything 30 times more difficult later bc no one else understands how my brain works#ah well. itll b fine. sometimes i just get freaked out that i wanna b better and i dont kno how to do that. so i spiral in despair a lil#ill b fine. im good at catching myself before i get too out of control. annoyingly tho i am not currently beating the bip0lar allagations#bc whatever tf is wrong with me i do probably fit the diagnostic criteria for bip0lar 2. i dont kno y that freaks me out so much. i guess#its bc it feels like something i cant just make better thru force of will and i grew up in a home that was very obsessively#health conscious to the point my dad gets anxious abt taking a single ibuprofen. so like ive been conditioned to get freaked out by#medication. literally my grandma will call me and tell me to b suspicious of doctors and to not take medicine unless absolutely necessary.#like lady u r the genetic reason i have 0cd shut the fuck up. also it feels like something that would more negatively affect how ppl think#of u than saying oh yea i get depressed or i have anxiety. like the connotation feels worse im used to just telling ppl whatever tf#my problem is. so the idea of holding something back feels weird. which annoys me bc i dont think there should b so much of a stigma. its#bullshit. anyway idk. im tired. i was trying to think of a comfort tv show with my therapist and all i could think was the terror#when im depressed i wanna watch those English mother fuckers suffer and die. i just lov that show so much. harry g00dsir my beloved. the#most me coded character to ever exist#unrelated
8 notes
·
View notes
Text
A Policy arm @ Cambridge had VERY interesting use of "confidential" patient data for Genomic & Medical Research during and post COVID.
20 15
Pathogen genomics into practice
Data sharing to support UK clinical genetics and genomics services
Genetic screening programmes: an international review of assessment criteria
2017
Personalised prevention in breast cancer – the policy landscape
Developing effective ctDNA testing services for lung cancer
Linking and sharing routine health data for research
Variant classification and…
View On WordPress
#Black Box medicine#Citizen Generated Data#Functional Genomics#GDPR#Genomic Diagnostics#IVDR#Phenotyping#Policy#Research prior to and during COVID#RNA Vaccines#Somatic Genome Editing
0 notes
Text
Let's Talk about Xyrem.
Xyrem ("oral sodium oxybate" or the sodium salt of gamma-hydroxybutyrate) is used in the treatment of narcolepsy, as well as (sometimes) idiopathic hypersomnia. Even if you don't have narcolepsy or any related conditions, you may find this run-down interesting. Here's why:
Gamma-hydroxybutyrate is roofies. That's right. Date rape drug. Right here.
The drug is so tightly controlled that there is one pharmacy in all of the United States that can fill it. Doctors must be approved and participate in a special program to even prescribe it.
Nobody really knows how it works in the treatment of narcolepsy.
I was prescribed Xyrem quite some time ago - at this point, nearly a year back. It took six-plus months of insurance, doctor's office, and central pharmacy wrangling to get the drug to my door. The whole time, I wondered: what should I expect from Xyrem? How do I know if it's working? How do I know if it's not working? What's it like? Lists of side effects and contraindications are readily available online, but I couldn't find a single detailed testimonial. This bothered me.
I've been on Xyrem for about a month and a half now. Here's what I can tell you about it.
You have to wake up at night to take a drug that's meant to improve your sleep. Everybody I explained this to found it funny. The standard practice is to split your dose in two - to take one half at bed, and the other half two to four hours later. If you're on Jazz Pharmaceuticals brand Xyrem and not the generic, they send you a tiny little alarm clock with a light on it to facilitate this. I have never needed it.
It takes 3 weeks to titrate up to the "full" dose, which is also the maximum dose. From there, you can titrate back down to a lower dose if you're experiencing unpleasant side effects. I'm in the process of doing this myself.
It doesn't necessarily knock you out. From the way the drug is described, one might get the impression that the moment it kicks in, you're going to be unconscious. I didn't find this to be the case. Your mileage may vary; I don't always fall asleep at all on the first dose, but it does at least get me sleepy enough to fall asleep on the second.
You have an unusual amount of agency in how you take Xyrem. This surprised me, especially given how tightly controlled possession of this drug is. For example, I metabolize Xyrem really fast. If I take it in two doses, I will sleep a maximum of 6 hours. I take the same amount of medicine and split it into three doses instead to compensate for how fast I metabolize it. That way, I'm more likely to sleep about 8 hours. This isn't just accepted, it's encouraged. You can even take a bigger dose first and a smaller one second, or vice-versa. The only hard and fast rule is: do not go over the max dose.
If you take it with alcohol, or within 4-6 hours of alcohol, it could kill you. A lot of drugs warn you not to take them with alcohol. I cannot stress enough that if you have ignored that warning in the past: do not ignore it here. Do not. Xyrem is a powerful CNS depressant. Alcohol is a CNS depressant. It really can kill you.
It works(?) Like many drugs that act on the brain, nobody is really sure how Xyrem works. It doesn't affect the most common (known) cause of narcolepsy (a lack of orexin/hypocretin). It's theorized that the drug acts on GABA receptors in a way that "consolidates" the fragmented sleep architecture of narcolepsy.
Narcolepsy can be thought of as an autoimmune disorder of sleep architecture. The sleep architecture of a narcoleptic is irregular, both within itself and from night to night. People with narcolepsy tend to have less of the deep sleep stages than they should. Narcoleptics also have a high percentage of stage 1 (light) and REM sleep. It's theorized that excessive REM occurs because it is of poor quality/does not serve its intended function, so the brain spams REM in an attempt to compensate. A diagnostic trait of narcolepsy is the ability to enter REM within 8 minutes of falling asleep - if sleep architecture is normal, this does not occur. While not all people with narcolepsy have cataplexy, cataplexy itself is actually REM intrusion into waking life. The narcoleptic brain is that screwed up about REM. Xyrem appears to regulate shifts between sleep stages and reduce the nightly percentage of REM sleep. I used to dream nightly. Subjectively, I do not dream at all on Xyrem.
The only difference between Xyrem and Xywav is salt. A full 9g dose of Xyrem contains 1,640mg of sodium. The maximum sodium intake recommended by the American Heart Association is 2,300mg. One of the few things I saw said about Xyrem prior to taking it was that it was disgustingly salty. It is very, very salty. I don't mind it, though. I've seen it said that Xywav tastes much worse, but I can't attest to that.
Subjective experience
Xyrem comes Priority Air Mail in a sizable cardboard box. An adult with ID must be present to sign for it. The first month's prescription comes with a light-up alarm clock. This kit and all subsequent kits come with:
The medicine, in however many bottles are required
A number of syringes, marked with common doses
A number of pill bottles
You put water in the pill bottles. They tell you to put about 60ml, but as far as I can tell, this is to make the saltiness tolerable. I made a little game of this - I try to put the same amount of water in each pill bottle, gauged by nothing but sound. I've gotten pretty good at this. I have my nightly dose split 3 ways. After adding the drug to the water, I close each bottle and swirl it a bit. I don't know if this actually does anything.
Xyrem works best if you're already tired when you take it. Hilariously, I have ADHD in addition to narcolepsy. Nighttime sleepiness isn't a thing I Do naturally. Consequently, the first dose of Xyrem only puts me to sleep about half the time, and it takes a while even when it does. I know myself well enough to know that if I wait until I'm actually "sleep for the night" tired to take it, I might be up until 3 or 4 AM. Instead, I take the first dose at around 11 PM. Even if it doesn't put me to sleep, it DOES make me sleepy enough that the dose I take 2-3 hours later will definitely work.
I was very careful to set alarms the first week or so of taking Xyrem, but I've never needed them. For reasons that are unclear to me, I always wake up when Xyrem is fully metabolized. Without more Xyrem, there is no urge to go back to sleep. When I've run out of doses for the night, I'm up for the rest of the day. There's no napping.
Some people have pretty nasty side effects with Xyrem. Headache and nausea are the most common. I had both of those, once each. The headache lasted all day but was otherwise unremarkable; the nausea was genuinely awful. The only persistent side effect I have, is tremors.
While I was waiting for Xyrem, my sleep specialist put me on Adderall. Nobody would prescribe this for ADHD, but you'll do it for narcolepsy? Sure, whatever I'll take it. I mention this because I thought it was possible that Adderall was causing tremors. I ran a little experiment: I took Xyrem but no Adderall one day and still had tremors. I took Adderall, but no Xyrem the night before, and the tremors subsided. It's definitely the Xyrem. While this is a known possible side effect, I can't find any information on how or why Xyrem, a CNS depressant, would cause something that seems very much the opposite of a depressed central nervous system. I am currently titrating back down from the max dose in an attempt to see if a lower dose will mitigate the tremors. If that doesn't work, I'm not... entirely sure what to do. Xyrem is a weird drug. It's strange not to dream at all; it's strange to wake up twice a night and still get better sleep than I ever have. Executive function has improved considerably, given that both neurological issues that cause executive dysfunction are being treated. Still: the tremors are, I will not lie, distressing. Not as bad as they were on Wellbutrin, which I was forced to discontinue! But - disruptive and distressing, nonetheless. I'm hoping that the tremors will stop eventually, or that dose adjustment will help.
Overall: would recommend if you have narcolepsy. You wouldn't think that a drug that obligates you to wake up multiple times a night could improve your sleep! Well, bucko, if your sleep architecture is already so disordered that you have narcolepsy: it can.
#I said I'd do a writeup on xyrem and here it is#took a long time because xyrem is weird#xyrem#narcolepsy#idiopathic hypersomnia#xywav
194 notes
·
View notes
Note
What subjects are actually taught at the academy? I've heard of recreational mathematics, thermodynamics, and touch telepathy, but what other courses are there?
What subjects do young Gallifreyans and Time Lords learn?
For once, we can be very very detailed about this!
🔬 Fundamental and Advanced Sciences
Quantum Mechanics: Introduced early in Gallifreyan education, this subject uses multidimensional geometry to solve complex problems, exploring the interplay between abstract concepts and physical realities.
Thermodynamics: This subject explores the principles of energy conversion between heat and other forms of energy, crucial for understanding the energetic dynamics of time-travel technology.
Cybernetics: Focuses on the study and construction of systems with regulatory functions, integrating technological and biological processes for the creation and maintenance of cybernetic beings and advanced machinery.
Matrix Diagnostics: Covers the techniques and tools used for diagnosing and maintaining the Matrix, a vast repository of Time Lord knowledge and consciousness.
⏲️ Specialised Temporal Studies
Basic Temporal Theory: Introduces the concepts of time and its properties, laying the groundwork for more advanced temporal manipulation studies.
Advanced Temporal Theory: Offered to students with intellectual perseverance, diving deeper into complex temporal phenomena and manipulation techniques.
Temporal Engineering: Encompasses engineering principles to temporal mechanics, essential for practical time manipulation.
TT Capsule Construction and Design: Focuses on the design and construction techniques specific to Time Travel Capsules, integrating advanced dimensional engineering and Veteran and Vintage Timeships.
TT Capsule Operation and Maintenance: Includes Space-Time Navigation, covering the operational aspects and routine maintenance of TARDISes.
Engineering Theory: The study of spaceship construction in general from different cultures.
Stellar Engineering and Cosmic Science: Deals with the manipulation and understanding of cosmic phenomena.
Dimensional Science: Studies the properties and manipulation of various dimensions beyond the standard three-dimensional space.
Dimensional Engineering: Applies engineering principles to manipulate and control various dimensions for practical uses.
Spatial Cartography: Teaches the mapping of space and the intricate layers of multiple dimensions.
Temporal Protocol and The Laws of Time: Ensures that all actions taken by Time Lords are in accordance with Gallifreyan law and temporal ethics.
Temporal Classics: Studies classic temporal theories and their applications through history.
🧠 Psychic and Telepathic Disciplines
Touch Telepathy: Teaches advanced communication techniques using innate psychic abilities.
Telepathic Defence: Includes mind-shielding techniques to protect students from psychic intrusions.
Psychic Field Manipulation: Standard training that covers manipulating one's psychic environment, including the science of Temporal Stasis.
🎨 Arts and General Studies
Super-logic: A complex form of logic used to solve problems that are beyond traditional logical frameworks.
Recreational Mathematics: This probably includes the study of happy prime numbers and other 'fun' maths (is there such a thing?), blending leisure with learning.
Art: Covers various forms of Gallifreyan art, including the creation and study of stasis cube art.
Gallifreyan History: Covers Gallifrey's past, including studying cosmic influences like those of the Assyrians.
Future History: Involves the study of fixed points in history, such as the Cro-magnon period on Earth.
Vector Justice: Teaches the principles of fairness and justice as practised by the ancient organisation known as the Vectors.
Botany and Biology: This field covers the study of Gallifreyan and alien plant and animal life, incorporating advanced biophysical studies.
Medicine: Includes tri-bio-physics and other medical sciences.
Languages: Teaches the linguistic skills necessary to communicate across thousands of different languages.
Music: Explores musical theory and practice, including the traditional harp lessons.
Detachment and Physical Inactivity: Focuses on mental and physical disciplines required to maintain objectivity and calm in all situations.
📚 The Culture of Learning
The Academy isn't just about academic achievement but also about instilling a deep-seated ethos of service and responsibility towards time and the wider universe. It's complemented by:
The Codex of Disciplines: A guide to the ethical and practical aspects of time travel and interaction with both time and the multitude of species across the universe.
Competitive and Collaborative Learning: From zero-gravity hyperball teams to Academy Sprint Championships, Time Lords are encouraged to excel in both individual and team endeavours.
Related:
How is sexual education taught on Gallifrey?: How Time Tots might get taught about sex.
What happens with 'gifted kids' on Gallifrey?: How Gallifrey deals with particularly talented children.
Do Gallifreyan children have toys?: Describing the very limited supply of toys for kids on Gallifrey.
Hope that helped! 😃
More content ...
→📫Got a question? | 📚Complete list of Q+A and factoids
→😆Jokes |🩻Biology |🗨️Language |🕰️Throwbacks |🤓Facts
→🫀Gallifreyan Anatomy and Physiology Guide (pending)
→⚕️Gallifreyan Emergency Medicine Guides
→📝Source list (WIP)
→📜Masterpost
If you're finding your happy place in this part of the internet, feel free to buy a coffee to help keep our exhausted human conscious. She works full-time in medicine and is so very tired 😴
#doctor who#gil#gallifrey institute for learning#dr who#dw eu#gallifrey#gallifreyans#ask answered#whoniverse
34 notes
·
View notes
Text


By: Leor Sapir
Published: Apr 4, 2024
Across the United States, thousands of parents have consented to having their children’s puberty stopped with a class of drugs called gonadotropin-releasing hormone agonists. Known colloquially as “puberty blockers,” these drugs overstimulate the pituitary gland to the point of preventing it from sending signals to the ovaries or testes to start producing the hormones responsible for puberty.
Parents who have consented to these drugs for their children love their kids dearly, but they’ve consented under entirely false pretenses. The doctors who’ve advised them say that puberty blockers are known to improve mental health — that they are even life-saving — and that they are fully reversible and just give kids “time to think.” None of this is true.
Major American medical associations say that “gender-affirming care” for kids is “medically necessary” and “life-saving.” Health authorities Finland, Sweden, Norway, Denmark and the U.K. disagree. Last month, the National Health Service of England decommissioned puberty blockers as a treatment of adolescent gender dysphoria. “We have concluded that there is not enough evidence to support the safety or clinical effectiveness of [puberty blockers] to make the treatment routinely available at this time,” the NHSE explained.
Imagine if American doctors told parents the following truths. The mental health benefits of puberty blockers are highly uncertain, according to multiple systematic reviews of the evidence, the bedrock of evidence-based medicine. The World Health Organization says the evidence is “limited and variable.” There is no research into long-term harms, but some evidence suggests decreased IQ and brittle bones. Permanent sterility is guaranteed for minors who go through full hormonal “transition.” Sexual dysfunction appears to be extremely common as well. Over 93 percent of kids who take these drugs go on to cross-sex hormones, which lead to permanent physical changes including excruciating genital growth, vaginal atrophy and tearing and much higher risk for cancer and cardiovascular disease.
There is no credible evidence that puberty blockers function as suicide-prevention measures. Finland’s top gender clinician has called the suicide narrative “purposeful disinformation” and “dangerous.” For all these reasons, health authorities in a growing number of countries, including some of the most LGBT-friendly, are now prioritizing talk therapy.
How many parents would consent to puberty blockers under these circumstances? Very few, if any.
It is common for drugs to enter pediatric use after evidence of their success in adult medicine. The opposite happened in gender medicine. It was the failure of “sex reassignment” in adult men to achieve satisfactory cosmetic outcomes and improve life functioning that led a group of clinicians in the Netherlands to propose starting the “reassignment” process in childhood.
Their hypothesis was as technologically appealing as it was ethically dubious: since males could not reverse the effects of testosterone-fueled puberty to pass as women, it would be beneficial to these men to have their puberty bypassed altogether.
The Dutch recognized the dilemma but thought they found a way around it. Relying on their experience using puberty blockers to treat a condition known as central precocious puberty (CPP), they argued that blockers were fully reversible and thus part of the diagnostic process. If it turned out that the kid wasn’t “truly trans,” the drugs would be discontinued and puberty allowed to resume.
Their argument was dubious from the get-go. First, CPP has an objective diagnosis, based on a blood sample, whereas gender transition is based on the adolescent’s feelings and experiences, which are subject to change. In a political climate such as ours, in which mere exploration of the reasons for rejecting one’s body can be labeled “conversion therapy,” differential diagnosis becomes impossible.
As Dr. Jason Rafferty, author of the American Academy of Pediatrics’ current policy statement on “gender-affirming care,” has put it, “the child’s sense of reality and feeling of who they are is the navigational beacon to sort of orient treatment around.” The AAP statement has been witheringly critiqued, and Rafferty and the AAP are now defendants in lawsuits by former patients.
Second, in CPP puberty suppression is by definition temporary; the goal is to delay puberty to its appropriate developmental window. In gender dysphoria, a “successful” prescription is where puberty is bypassed altogether. The assumption about reversibility, never tested and highly questionable form the start, proved to be the ethical foundation for the entire Dutch experiment, and it quickly crumbled. Over 93 percent of adolescents who are put on puberty blockers for gender issues continue down the medical pathway to cross-sex hormones. Some go on to surgeries.
Gender clinicians do not see this suspiciously high figure as a reason to rethink their approach. They see no possibility of iatrogenesis — a medical intervention that unintentionally induces harm, in this case by causing gender distress or confusion to persist artificially. On the contrary, they regard the high persistence rate as proof of their own remarkable diagnostic abilities.
More modest and scientifically-minded clinicians and researchers see things very differently. “Blocking puberty,” writes Sallie Baxendale, a professor of neuropsychology and author of an important new study on puberty blockers, “prevents the critical rewiring in the brain that underpins the ability make complex decisions. Puberty blockers may give children time to think but they simultaneously rob them of their developing capacity to do so.”
What is likely happening is that an ongoing youth mental health crisis whose origins predate and have little to do with gender is being misdiagnosed and mistreated with harmful and experimental drugs. Puberty blockers are the definition of a “quick fix” solution.
Researchers incorrectly refer to what the Dutch did as an experiment. In an experiment, falsifiable hypotheses are proposed, alternative interventions are tested, outcomes are monitored and competing explanations for observed results are thoughtfully ruled out.
The Dutch did nothing of the sort, according to a comprehensive scholarly examination of their study. Further, the only attempt to replicate that study, which was done in the U.K., failed. The researchers had to be forced to disclose their disappointing findings. Any scientific-minded person willing to put in the effort and read the literature will come to the same conclusion: Pediatric gender medicine is an industry built on fraud.
During the 2000s and 2010s, the Dutch pseudo-experiment with puberty blockers “escaped the lab” and became entangled in a fast-growing international social movement for transgender recognition. In the U.S., the drugs are being prescribed at numbers far exceeding anything the Dutch could possibly have imagined. Most adolescents referred to pediatric gender clinics are teen girls who have no history of dysphoria in childhood but who do have other mental health challenges that predate their distress with their bodies.
American medicine is no stranger to scandal — lobotomy, “recovered memory” and OxyContin are just a few examples. What makes pediatric gender transition unique is that it has been framed as a nonnegotiable civil right and defended by powerful civil rights groups, the Democratic Party and their ideological allies in the mainstream media.
A key reason for the divergence between U.S. and European medical authorities, as I’ve explained in a previous essay, is the latter’s greater willingness to follow principles of evidence-based medicine, including reliance on systematic reviews. Jack Turban, a prominent American gender clinician, revealed in a deposition that he seems not to know what a systematic review of evidence is.
Another reason is that in the U.S., doctors who practice child “transition” demand and often receive deference as the experts on the evidence for their practices; abroad, such clinicians are seen as having conflicts of interest. When the National Health Service of England appointed the highly respected Dr. Hilary Cass to lead its review of its youth gender service, it did so precisely because she was “a senior clinician with no prior involvement or fixed views in this area.” Sweden and Finland delegated the evaluation of evidence to experts with no personal involvement or stake in pediatric gender medicine.
Parents should never have been put in the position of having to decide whether to “allow” their kids to go through puberty. Those who would put the onus on parents are letting charlatans in the medical profession off the hook. Puberty is difficult for all teens, and it is not a disease. Puberty blockers offer teens in distress — especially girls with history of sexual abuse, autistic kids and gay kids — false hope by casting puberty as optional.
Puberty is a rite of passage from childhood into adulthood, responsible for the development of the body’s major organs and systems and not just its external sexual features. Puberty blockers rob children of their right to an open future.
#Leor Sapir#puberty blockers#medical malpractice#medical scandal#puberty#gender pseudoscience#medical experimentation#gender lobotomy#gender thalidomide#medical corruption#religion is a mental illness
24 notes
·
View notes
Note
so with brain stuff or whatever
Who am I supposed to bring stuff up to at the start?
I'm currently in the middle of a lot of changes (trying to switch primary doctor and get a therapist and stuff) and one of the reasons for me changing that stuff is that my brain is very weird and I need to figure out why/get help with it
But when I'm bringing up symptoms or whatever, I had very much assumed that would be therapist but I'm also not fully sure who does what in a system like that (primary doctor vs therapist vs psychologist) and in the past have had some problems with that (still don't really know who the hell is supposed to diagnose sensory processing disorder)
Also any suggestions for like... what's a good area or amount to start with when trying to bring stuff up? I haven't talked to someone about mental health type things in a really long time and have had problems with derealization/depersonalization, possible depression, possible ocd, some weird situations in which I wasn't really sure what was real, a couple anxiety spirals over illogical things, intrusive thoughts, etc and I don't really know what to prioritize or how much to say in a way where I wouldn't overwhelm someone new, wouldn't be worried about telling them too much, but would also be able to give enough information about something to lead to a diagnosis or help
Sorry if this is too long or too much information or too many questions or anything like that
Hi there!
Okay so the annoying truth is that this depends a lot on the healthcare system where you live, and I don't know where you live (nor do I know the system everywhere) but I can try to give you some general pointers.
Your primary doctor is the first person to talk to, if you need a referral to see any of the other professionals you mentioned, but usually the primary doctor isn't the one doing the diagnosis or treatment (though they may prescribe some types of psych medication, and they often take over prescribing from a psychiatrist once the right meds have been found).
The psychiatrist is a type of doctor, and they are the person to talk to if you're interested in medication, and in some systems psychiatrists may also be who refers you to see a therapist. In a lot of systems it's primarily psychiatrists who diagnose people, too. Sometimes clinical psychologists also do diagnoses, but psychiatrists always do diagnosis + medication (and only very rarely do they engage in therapy).
A psychologist is someone who's educated in the field of psychology, so they (ideally) have an in-depth understanding of general human psychology, and they often are also educated in mental disorders and in different approaches to therapy. In terms of treating mental illness, some psychologist do diagnose, but the most common function is for them to do talk therapy.
Therapists can technically have any educational background, and refers to anyone who "does therapy".
If you're looking for a mental health professional to treat you with talk therapy, you ideally want a therapist who has a degree in psychology. If you're looking for a mental health professional to diagnose you and prescribe medication, you're looking for a psychiatrist (doctor of medicine who specializes in psychiatry).
If you have the ability to see any of these professionals without a referral, you can choose which one based on what you are looking for. And if you need a referral, then the first step is your primary doctor.
With a primary doctor you want to give them enough information to ensure getting a referral, but you don't have to throw your whole heart out there. If you are in a diagnostic setting, usually (ideally) they follow a semi-standardized questionnaire like the PSE, so a lot of the time they are the ones leading the conversation and asking you questions. Sometimes they will do an initial interview where you tell them freely about what's bothering you. Try to focus on the things that are causing you the most distress, and try to avoid clinical language.
With a therapist, the goal is to build a therapeutic relationship, and you can approach it based on feels - it's ok not to open up about everything at once, but it can also be helpful to take time to define the goals of therapy together (which would include what you're struggling with and wanting to work on).
Hope this was at all helpful,
Best of luck!
15 notes
·
View notes
Text
This is not a mystical or spiritual diagram. It does not symbolize any religious beliefs. It is OLD SCIENCE.
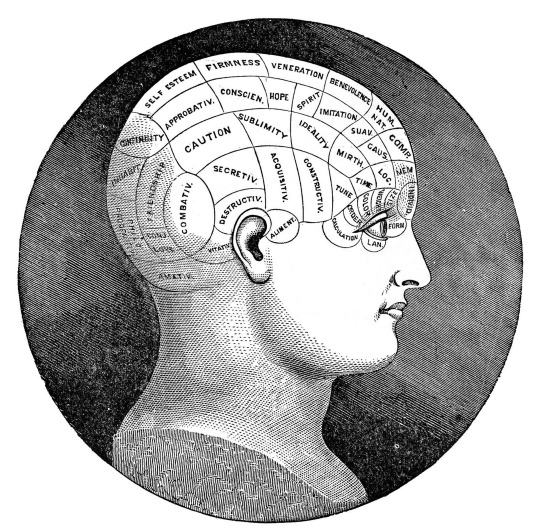
I understand if you want to make an inspirational, guru-style, spiritually uplifting (or exploitative) article or video about your mystical beliefs. I'm sure it will be very life-changing for your viewers and they will love it. But I have no idea why you'd use one of these in the thumbnail for it. This is a phrenology head model.
THIS IS OUTDATED BRAIN SCIENCE FROM THE 1800'S AND THE PEOPLE WHO WERE USING IT THOUGHT THEY WERE DOING REAL SCIENCE. FOR REAL.

They were not hooking it up to the zodiac, they were not reading auras, they were not casting spells or manifesting something or whatever. They were not associating it with a spirit or deity or religious act. They were analyzing what they thought was the shape of your brain and how well different areas of the brain that (purportedly) did different things in your life were developed and how well they were functioning. Model phrenology heads were a diagnostic tool for a type of medicine that is no longer practiced. It was a step in the progression towards what eventually became real brain lobe science in modern times. It was also used for eugenics! Anyone who knows what it is will look at your thumbnail and think: "oh boy, they don't even know what this weird science and eugenics tool was actually used for, THAT'S KINDA AWKWARD!"
Oh I know! You're mixing it up with these things, aren't you?

This is a guide for palmistry, a way of reading the lines and marks on your hand to see what's up with you mystically. What's up, danger? What's going down with the planets and the spirits? How your marriage is gonna go and stuff like that. I get that they look similar and that sometimes people photograph them together, but palmistry has never purported to be a science and is a method of divination like aura reading. Stick a palmistry hand in your woo-woo spirit guidance article/video thumbnail, that at least is in the same INDUSTRY as your subject matter.
If you stick a phrenology head on your thumbnail you are saying: "I have no idea what this is actually for, but I think it's kind of mystical-looking and the stock image was free, and I don't actually take any of my subject matter seriously, because this is all a cash cow." And hey! It's a good flag to wave around so that people in the know can avoid your content so, in that case, I guess keep it up!
95 notes
·
View notes
Text
Getting past ‘it’s IBS’ (Xi Chen, Aeon, June 04 2024)
"In the late 1980s, aged 12, Taryn was taken to her doctor’s office with cramping, bloating, and constipation after eating, and was told that she had ‘a nervous stomach’.
As a white girl growing up in New Jersey, she met a stereotype, and when initial bloodwork and imaging was negative for evidence of a ‘real’, or organic disease in her gut, one of Taryn’s doctors began writing in her charts that she had irritable bowel syndrome (IBS), a misdiagnosis that would follow Taryn for life.
At the time, IBS was considered by many to be a medically unexplained and therefore controversial illness, keeping company with conditions such as fibromyalgia and chronic fatigue syndrome.
As a result, it carried the stigma of being a psychosomatic illness, caused primarily by stress and anxiety, and Taryn was sent home with prescriptions for diet and exercise. (…)
Today, unlike in the 1990s, it is well established that conditions like IBS, collectively known as disorders of gut-brain interaction (DGBIs), are real diseases that disrupt the communication between the nervous system of the brain and spine, and the nervous system of the intestines.
First mentioned in the book The Irritable Gut (1979) by the gastroenterologist W Grant Thompson, the conditions were labelled ‘functional’ disorders – characterised not by structural damage to the hardware of the gut, but by a glitch in its ‘software’, in other words, its nervous system, charged with processing, receiving or relaying information coming in or going out.
Software is not as easily observed as hardware, however, and much of academic medicine views the mind and the body as two separate and distinct entities, a viewpoint called mind-body dualism.
Over time, and despite the more nuanced meaning intended by Thompson, the term ‘functional’ became associated exclusively with disorders of the mind.
This is part of the reason why there is still stigma against conditions like IBS, and why attempts to establish diagnostic criteria for IBS in particular suffered from vagueness. (…)
When academics read that IBS patients have higher rates of anxiety and depression, or that antidepressants are a treatment for IBS, many assume that this is because psychiatric symptoms cause symptoms of IBS without considering the inverse, that chronic undiagnosed abdominal pain predisposes patients to having mood disorders.
The real reason these drugs are effective, however, is that, in utero, the precursor cells for our gut and our brain actually share the same nervous system, and only later separate in embryonic development.
As a result, the two nervous systems utilise the same neurotransmitters, such as serotonin, to send messages between neurons.
This is why we sometimes feel butterflies in our stomach when we’re nervous, and why stress and anxiety often worsen symptoms of IBS, but do not necessarily cause it.
As Brown’s quote above implies, the stereotype of the anxious patient in pain applies not only to IBS but all patients who present to clinics with vague abdominal distress (including those with non-gastrointestinal conditions like endometriosis, who experience delayed diagnosis because providers take women’s pain less seriously than men’s).
A classic example is peptic ulcer disease, a cause of severe abdominal pain that for decades was denounced as a psychosomatic illness until Barry Marshall and Robin Warren discovered in 1983 that it was caused by a species of bacteria.
Before their findings, peptic ulcers were managed with diet and, frequently, surgery, when what patients needed were antibiotics. (…)
In my opinion, the root of the problem is medical education itself.
Unless a medical trainee becomes a gastroenterologist, it is unlikely that they will receive any specialised education in IBS, let alone the history of IBS research proving it to be an organic condition, despite 40 per cent of the general population having functional gastrointestinal disorders.
Partly, this is because a majority of medical education in countries including the US, the UK and Canada takes place in academic centres associated with hospitals, where medical students will probably never encounter a patient for whom their IBS symptoms are the primary reason for them appearing in the emergency room, and especially not for their admission to the hospital itself.
As a consequence, medical students also don’t get their knowledge of IBS tested by board examinations.
This speaks to the fact that, echoing Osler, IBS generally doesn’t kill patients, and our current healthcare system values measures of mortality and cure in response to acute complaints more than quality of life and the management of suffering from chronic issues such as IBS.
The same could be said about long COVID (which, to this day, is sometimes challenged as illegitimate) and chronic fatigue syndrome, where sufferers are often sent off to a psychiatrist for care.
The thinking is that these ongoing problems, where there is no mainstream route for testing and treatment, are not as important for medical students to know about compared with, say, a patient crashing after a cardiac arrest, even though most of the global disease burden across the developed and the developing world is caused by chronic, not acute, illness. (…)
These demographic patterns don’t explain who really has the disease – they just reveal medical and social bias and entrenched stereotypes: women are perceived as hysterical and diagnosis-seeking, while men are stoic and avoidant, for instance; or white women are thought to tolerate less pain than people of colour.
None of this, in reality, is true – but it is part of the reason why so many patients assume that what they suffer from won’t be justified by the presence of organic disease and therefore doesn’t warrant a doctor’s visit in the first place.
Such patients, treated so poorly within the medical mainstream, now have a community and identity of their own in the Wild West of alternative medicine that flourishes online.
Such groups, seeking to empower themselves and especially hoping to get well, today stand at loggerheads with the practices and physicians they have left behind.
Some accuse their former doctors of gaslighting them, and they deserve to be heard.
Much of what I have discussed regarding misdiagnoses of IBS assumes that healthcare providers, even when in error, always have good intentions and are sincere about using the diagnosis to clarify the patient’s medical case.
There were several elements of Taryn’s story, however, and in my own experiences of how DGBIs are taught in medical school, that make it difficult for me to believe that this assumption holds in most doctor visits.
Although one could argue that the blasé diagnoses of IBS and disordered eating for Taryn could be down to simple carelessness and negligence, honest errors, or someone being ‘just a bad doctor’, it’s obvious to me that a pattern was developing with Taryn’s interactions with different providers who weren’t taking her lived experience itself seriously, just as I had stopped taking my own experiences seriously.
What holds our stories together, I believe, is this phenomenon where both of our perceptions of our own ability to know what’s true or not were put into question."
11 notes
·
View notes
Text
A small new trial published in the journal Nature Medicine describes what would be two firsts for Parkinson's disease, if they pan out: a diagnostic test and a potential immune-based treatment that works similarly to a vaccine. The research is still early, but researchers are excited by the prospect of advances for a disease that lacks good diagnostics and treatments.
The target of both innovations is alpha synuclein, a protein that takes an abnormal form in Parkinson's patients—aggregating in their brains and destroying nerve cells involved in motor and some cognitive functions. While researchers have long known that these proteins are involved in the disease, finding ways to measure and target them has not been easy.
The (potential) Parkinson's vaccine
The Florida-based biotech company Vaxxinity developed a vaccine, or what it calls an active immune medicine, to train the immune system to attack only abnormal versions of the protein—which are improperly folded—and not the regular forms. This would essentially help people's bodies treat themselves.
“The idea is that patients should recognize their own misfolded proteins, and it is personalized because their own immune systems are doing the work,” says Dr. Mark Frasier, chief scientific officer at the Michael J. Fox Foundation for Parkinson’s Research, which funded the testing part of the study.
The Parkinson's test
The new diagnostic test for Parkinson’s, which was developed by researchers at University of Texas and Vaxxinity, uses samples of cerebrospinal fluid to measure a person's levels of abnormal alpha synuclein. If the U.S. Food and Drug Administration (FDA) grants it full approval, it will become the first test for diagnosing Parkinson's. (The FDA classified it as a breakthrough device in 2019, a status that expedites access to innovative technologies where there is unmet need.) “Without [such a test], you’re kind of shooting in the dark,” says Mei Mei Hu, CEO and co-founder of Vaxxinity.
Alpha synuclein has been tricky to measure in the body for several reasons, says Frasier. While everyone has the protein, abnormal forms of it occur in relatively small amounts, so they're harder to detect via imaging. This type of alpha synuclein also tends to clump inside cells rather than outside of them, making it even harder to see. If clumps are large enough to become detectable, they can look structurally similar to amyloid or tau—the proteins implicated in Alzheimer’s disease—so imaging tests might misdiagnose people with Alzheimer’s rather than Parkinson’s.
Read More: Michael J. Fox: Chasing Parkinson's Treatments
The test overcomes those hurdles by cleverly exploiting normal forms of the protein. Parkinson’s experts believe that tiny amounts of abnormal alpha synuclein circulate in the spinal fluid of patients, but are too small to be detected through imaging. To run the new test in the study, researchers take normal forms of the protein in the lab and add them to samples of spinal fluid from patients; that prompts any misfolded protein that might be present in the samples to pull the normal proteins into misfolded aggregates, amplifying the signal for the abnormal form. Scientists then use a fluorescent probe to detect how much antibody to the misfolded protein patients generated, resulting in a biomarker, or stand-in for the treatment effect.
This test would be a critical advance because it makes it possible to identify patients with abnormal alpha synuclein at the earliest stages of the disease, when treatments might be more effective.
With more data from patients, researchers hope to further refine what different levels mean, so that the test will be able to tell not just if a person has Parkinson's but whether someone might be at a greater risk of developing it. Currently the test is only used in research studies, but more results like these—as well as data on whether the same process can be applied to blood samples—could speed the test to getting approved for wider use.
What the study found
The trial—conducted by researchers at the University of Texas, the Mayo Clinic, the Michael J. Fox Foundation for Parkinson’s Research, and Vaxxinity—included 20 people with Parkinson’s. It was just designed to test the safety of the approach, so the study only provided hints about the treatment's effectiveness. Everyone received three shots over nearly a year; some contained the treatment at different doses, and some contained a placebo.
Overall, people receiving the vaccine generated more antibodies against the abnormal alpha synuclein protein than those vaccinated with placebo, as measured by the Parkinson's test. Antibodies started to ramp up about four months after the vaccinations began.
“What is unique about our technology is that it can stimulate the immune system to produce very, very specific antibodies against toxic forms of alpha synuclein, and do it in a safe way, which is reassuring,” says Jean-Cosme Dodart, senior vice president of research at Vaxxinity and senior author of the paper.
According to the test results, about half of the patients in the trial showed high levels of antibodies against the misfolded alpha synuclein, and most of these patients received the highest dose of the vaccine. They also scored the highest on motor and cognitive tests. There were too few patients to adequately assess any changes of Parkinson’s symptoms, but the researchers believe that longer follow-up with those tests, and potentially more frequent or higher doses of the vaccine, could lead to improvements in those scores. “The results are very, very encouraging,” says Dodart.
“This paper demonstrates that in a small number of people, the vaccine is having an impact on misfolded alpha synuclein, which is really exciting,” says Frasier. “We are now in the biological era for Parkinson’s disease."
11 notes
·
View notes
Text
Got most of the way through a chapter before deciding it didn't fit the flow. rip.
A replicator. A fully functional, Pristine, replicator. Lino couldn't believe his eyes when he caught sight of one of its terminals while Vincent was carrying him from the bed bay to the dining room.
"Stop, That-" he pointed to it in his excitement before remembering his captor was blind, "The replicator, I mean, I want to see it."
"I'm sorry-" Vincent started to apologize even as he changed his course. His plodding steps becomeing hesitant as they approached it, "-I know it is a crime against God but I ... can't cook or grow my own food. I'm sorry -"
"Vincent, no, it's not a crime, it's a blessing you've been tricked into thinking of as a crime," Lino let the lie slide of his tongue as he squirmed out of Vincent's arms to drag himself up to a standing position by the terminal's podium.
The Sun only had a single replicator. An Re4 model that was too slow and expensive to run for anything less important than medicine or parts they couldn't machine with the other tools they had. All other units that had been found were ordered scrapped no matter their condition as The Leader blamed them for the war. They said the abundance of material and food and medicine was what made the people of old so hungry for blood. There was nothing left to need or want besides other people's destruction.
Lino had never believed a word of it. Endless food and medicine and parts could be theirs, no one in even the coldest slums of the Corona would have to go without if The Leader would just let him and the other mechanics move and repair the old beasts.
He dug through the menus until he could turn off the cosmetic interface to see the truth of this miracle machine. It wasn't a Re4. It wasn't a ReUnit, or any other small devices meant for the ultra wealthy who could afford to house a village in a bunker. It was a Replicator. Capital R. one of the originals meant for mass and rapid manufacturing that could make anything from apples to the nuclear warheads that destroyed the old world.
It's diagnostic page showed it's terminal's looks weren't lying. The old beast was still marching along almost as perfectly as the day it had been activated for the first time. There was work to be done on it, sure, but it was the sort of work Lino relished.
... It wouldn't hurt to have a little side project while he figured out his leg situation, right? The Sun would order this massive work of art stripped for parts, would come and kill Vincent just for daring to know it exists. After Lino left, he could tell no one about the miracle just outside their territory, but while he was here he could keep part of the old world alive for just that much longer.
Vincent was quiet as Lino oohed and ahed his way through submenu after submenu, but eventually had to speak his doubts.
"It pretends to be God. It can make flesh and fruit that are exactly like reality, how is it not a crime?"
"Because if it was God wouldn't have made his creations so replicable. It's not a sin to paint or sculpt or grow, why would it be a sin to make a machine that can do it for you?" Lino only had Vincent's own prattling to base his assumptions on as The Sun deemed religion to be just as guilty for the fall of the old world as the replicators were. Still, he found himself sliding into the roll Vincent had cast him in a little easier with every new line he fed the man.
"But... I thought those were gifts meant only for man?"
"And did a human make this machine or not? It's a tool, a big one with a lot of parts, but still just a tool." Lino found the parts list buried away in a plain text document. The specifications written in defunct measures. Notes were still left over from the original manufacturing. Dates of when this or that was assembled, a reference to a component being a lemon and needing to be sent back. Each signed, often just with initials, but sometimes there would be a name that struck out from the lines.
Alan, Antonio, Barnes. Their names immortalized even if they were most likely killed in the initial volley of nuclear war. Carla, Henry, Heather.
Lino told the machine to print the parts list, he'd need to see how things wore out before he had it begin on remaking itself. The mill and compositing set up seemed the most effected by time, and since those were what he'd need most to build his new leg, surely it wouldn't hurt to take the time to get them as pristine as the rest of this marvel?
And perhaps, a smaller part of wanted to learn every name in those margins. They deserved to be remembered.
Vincent let the topic drown in silence as Lino did what he would, his false beliefs in angels making him hesitate to question him further.
"But my grandmother -"
"Was wrong. Humans are wrong sometimes, Vincent. It's ok, God has already forgiven her," Lino dismisses him as he gathers the stack of papers from the output. His hip and knee were already aching from supporting his entire weight after so long spent in bed.
"Of course, of course. My apologies for questioning you," Vincent bowed his head.
"It's all forgiven, my Vincent," Lino reassures him with a hand on his shoulder, half to do the reassuring and half to brace against the mountain that was Vincent. "I believe you were taking me to dinner before I interrupted?"
13 notes
·
View notes
Note
Your blog has gotten me interested in antipsychiatry as an extention of bodily autonomy - however, at least some disorders do seem to be clustered in a way that makes sense for troubleshooting if someone needs treatment. Like, reading the definition of depression as a teenager made me realize that it's not normal to want to die 24/7, and that I should probably talk to a therapist. I don't know exactly where I'm going with this tbh, but I guess I think that some (at least my own) psychiatric disorders make sense and are pretty common ways that people can suffer?
yeah, i think it's pretty important to distinguish between diagnostics as a form of loose categorization (for example, i find ocd + anorexia both to be useful shorthand for experiences i have + share w/ many others) and diagnostics as a prescriptive form of Assigning Illness (such as the DSM). the experiences of ppl with depression are real + often similar to one another + it's extremely useful to have a culturally recognized term that summarizes a lot of painful experiences.
it's when those shorthand descriptions become prescriptive rather than descriptive (e.h you feel x way BECAUSE you have depression, not that you have depression BECAUSE you feel x way), medicalized (e.g this is because you are Sick, this must be Cured, this has a definitive biomedical cause), or alienated (e.g this experience sets you distinctly apart from Normal people, who have Healthy thoughts + brains).
even when you say thinking those things is not 'normal'- sure, most ppl probably don't- but is the concern that it's 'abnormal' or that it's making you miserable? what if everyone else DID feel the same way- would that mean you don't deserve relief from it? one of the biggest flaws in psych diagnostics is that it relies on the assumption that these experiences need to be stopped (and Stopped is usually their ideal goal, though they will settle for mitigated or reduced) not because they are painful but because they are 'abnormal' or 'disruptive' (often to functioning within systems which are inherently unjust like school, work, maintaining housing, etc). the concern is not suffering, but abnormality (with the assumption that there is even such a thing as a Normal Person).
take, for example, my dx of anorexia- when i experience torturous thoughts of hating my body, obsessing over what i eat, obsessing over if other ppl are judging me for what i eat, obsessing over my weight, etc, it is diagnosed as pathology. when a fat person experiences this, they are very, very often validated in these emotions because they are Supposed To feel that way according to fatphobic medicine + cultural norms. while tides are shifting in this regard, this was not just a silly little oversight of the anorexia dx but built in, because the assumption built in to psychiatric diagnostics is that extreme body hatred is only pathological if it's 'irrational'- if you are supposed to hate your body, as determined by norms, then you are 'normal' + there is no 'dysmorphia' present, therefore no care or concern.
in general, i think most systems of categorizing ppl fall apart + become harmful when they fail to recognize themselves as roughly constructed shorthand ways of describing deeply complex experiences- gender, sex, race, diagnosis (this gets foggier in certain medical diagnoses but still stands for the majority of them), identity in general rlly. but if we can see them for what they are- (fallible + limited) things we created to describe ourselves, not objects within us which control our behavior + thoughts, they are immensely useful for many.
127 notes
·
View notes
Text
I wrote some Chase fic and it's @softsicknose 's birthday!!!
This is written in a different POV- Martha Masters' from season seven. I really love her, and I enjoyed stretching my writing comfort zone for her. I hope you enjoy!!!
XXX
Chase is late. Late, she’s found, is based solely on when House arrives (unless they’ve been given a time by Cuddy). Chase is usually always early. Early is determined by the time at least two of the team are in the diagnostics room. Out of all the times she’s walked through the glass doors and into the room in the early morning, he’s only been absent four times. All four of those times have also seen him strolling in before their boss.
The fact that she, Taub, Foreman, Doctor Hadley and even House are here and Chase isn’t is odd. Martha likes routines, likes things to stay the same and this disruption in the day to day has her feeling anxious. Her prefrontal cortex is telling her that the blonde is probably just stuck in traffic and there’s nothing to worry about, but it doesn’t stop her from fiddling with the pen she’d borrowed from the man earlier that week.
No one else mentions that the intensivist is missing, and maybe they all know something she doesn’t? It wouldn’t be the first time- she’s becoming used to being left out of things or being cast aside as an inside joke is told. She’s never gotten the courage to ask what some of the things they say mean, because when it comes down to it she’s here to learn about medicine and science, not about Foreman’s brother or the reason Doctor Hadley was in jail.
Seventeen minutes after they start the differential, Chase pushes through the door, looking minorly rumpled but otherwise fine- attractive as always. The realization that she’s just called the blonde attractive sinks in. Objectively, she’s aware he’s much more pleasing on the eyes than anyone else on the team; except maybe Doctor Hadley, and that statistically blonde hair and blue eyes tend to lend themselves to what the world has deemed beautiful. His accent doesn’t hurt either.
Get it together Martha, it’s Chase. Chase, whose password is password, who sleeps with three women in one night only to forget their names. Chase, who does crosswords instead of listening to their boss. Chase, who is also an amazing intensivist and who has gotten more correct diagnosies than anyone else since she’s been here. Chase, who always looks just a little put out when House doesn’t latch on to one of his jokes or praise him when he’s found the correct answer.
“Chase! How kind it is of you to grace us with your presence.”
The words snap the brunette out of her trance.
As House snarks, a dark blue folder is thrown at the man who tries to catch it but fails. Instead it hits his shoulder and flops onto the table. Taub and Foreman are reading through their own copies, seemingly unbothered by the disturbance, that or they’re tired of House’s antics. Doctor Hadley is glancing up at Chase with a furrowed brow but he gives her a shrug and sits down, leather messenger bag swaying on the back of his chair.
With how close he’s sitting, Masters can smell his cologne- something aquatic and airy, no doubt to remind him of Australia and its beaches. As the team bounces ideas off one another, she notices Chase pressing the back of his pointer finger against his right eye- closed. The structure of his jaw tells her it’s clenched, which indicates he’s either annoyed or possibly in pain. Annoyed seems much more likely.
“What about you, Captain Kangaroo? Any ideas in that pretty head of yours? Or did the one too many drinks you had last night impair its functioning?”
“Actually, the effects of alcohol wear off in usually six hours unless your metabolism is slow. Even then, it’s likely to be around eight or nine hours,” she offers.
“I didn’t drink last night, and that insult was sub par,” Chase says as if he’s been waiting for some kind of accusation. “Could be a DVT that traveled to her lung.”
Something about his voice is different today, it’s lower, maybe? She’s not sure which adjective goes best, but she watches as he swallows and his adams apple bobs unnaturally slowly. He goes to automatically grab a mug that’s not there, hand halfway outstretched before he drops it and rubs the lower half of his face. House’s eyes drag over him like a cat stalking his prey but the older man doesn’t say anything, instead he just sighs, then twirls his orange expo marker in his hand, staring at the list of symptoms on the board.
“DVT was checked for, next.”
As Martha wracks her brain for different causes of the new patient's afflictions, she hears rather than see’s Chase shift in his chair, then a breath being inhaled and snagging.
“h’ihnGgkt! HnGXxt! hh-NgXTtuh!!”
The sneezes are far quieter and less obtrusive than she’s imagined. She’s thought since starting that the blonde’s sneezes would be loud and harsh, slightly dramatic. These are small and very obviously meant to be quiet. Interesting.
“You shouldn’t stifle like that, you can burst your eardrums from holding a sneeze in,” she comments after his last one, watching him raise his eyes from the folder, one eyebrow quirked upwards. She flushes, unsure if the comment was appropriate. She just wants to help! What if Chase blew out an ear drum from being careless? She’s simply doing a kind thing, she tells herself.
“I’ve done it my entire life, Masters, think I’ll be alright.”
As Foreman suggests an alternate cause, Masters nods and writes down both ideas, wanting to keep up with the details of the case, even if they turn out to be wrong. A sniffle breaks her concentration and as subtly as she can; feigning looking at the clock, she glances at the doctor next to her, noting the barely visible shadows under his eyes. Not enough sleep, then. The rest of the DDX goes as usual, with House giving them all assignments. She gets put with Taub to go break into the patient's house.
“Do you really think this is a good idea? She can’t keep her holier-than-thou mouth shut when it comes to this type of stuff. Wouldn’t it be better for me and…anyone else goes?”
The med student frowns and twists at her cardigan, headband feeling suddenly too tight. Her cheeks feel warm and she knows her capillaries have opened and blood has rushed to show her emotions whether she wants to or not. Foreman gives a low laugh, rolling his eyes. Chase looks like he might say something but Doctor Hadley beats him to it.
“If you’re so worried, then do the labs and I’ll go with her.”
Surprise drives out the embarrassment of feeling like an unwanted dog at the pound. Didn’t Doctor Hadley dislike her too? Why was she rushing to her aide? Was this another joke she was going to be the butt of? She chances a look at the older woman and sees her smiling.
“Us girls have to stick together, right?”
��R-Right.”
Taub blows out a breath from his puffed cheeks and nods, saluting her.
“Thanks, I owe you one.”
“Alright children, play nice,” House calls from where he’s hobbling through the door to his connected office, tone indicating he doesn’t actually care what’s being said to one another.
The car ride to the patient’s house is filled with an awkward silence. Martha’s unhappy she has to go at all, it’s unethical and illegal. No one else cares and she wonders if it’s because of House or their own morals. Her mother taught her right from wrong at a young age- what did everyone else’s mother teach them? As she watches trees go by, Doctor Hadley fiddles with the radio and then looks over when they stop at a red light.
“So, how’re you liking it on the team so far?”
“It’s been, uhmm…interesting? Definitely seeing more than what I’ve been exposed to in my own world. A lot of it’s for the worse,” she trails off, her last sentence barely audible, but the other woman must hear it.
“You know, this team has been through a lot. And a lot of things have changed all of us, but when it comes down to it, we’re here to do our job and save people. If that means breaking rules, well.” A pause. “Is it better to watch someone die while keeping yourself pure or save an innocent life and do something risky?”
For once, Martha’s unsure of the answer. Both are morally wrong- is there an answer that’s better than the other? It feels like some kind of perverse test so she crosses her arms against her chest and tries not to act like a petulant child.
“Is that why you’re all so codependent?” The words tumble from her mouth before she can stop them. She wants to smack herself.
Doctor Hadley- Thirteen, as the boys call her for unknown reasons, laughs and a smile appears.
“I wouldn’t say codependent. We just work well as a team. We also work well individually. Chase was first to work with House, then Foreman joined. After they left, Taub and I were hired. Foreman came back, and then Chase. We all fell into an easy team who can communicate pretty well.”
“House likes you all. Was that, did he-“ she sighs and tries to reign all of her thoughts together. “Was he like that with everyone who’s been part of his team before? Or were there others who were treated like me?”
“I think that that’s a question for him, even if he won’t answer it. He doesn’t hate you. If he did, you wouldn’t still be here. He obviously sees something in you that he wants to cultivate.”
Martha isn’t sure what to say to that, so she nods and let’s the silence fall around them again. She’s never been good with small talk, and now it’s apparent she’s not good with any kind of talk.
They get back to the hospital two hours later, when the clock is about to hit noon. The women head to diagnostics but it’s empty, so they reroute and take all of the plastic baggies full of their findings to the lab to start working. As they approach the large room, Martha notices a familiar figure sitting in the corner with his back to the door. He’s got his lab coat on now, and from what she can tell he’s got his chin leaning on his hand, posture screaming ‘I’m bored’. He must be waiting for a test to finish up.
“Hey, why don’t you go find House or Foreman and let them know I’m about to run the tests,” Thirteen suggests, taking the large bag full of items and holding it. “Otherwise, House will bust in and scare the hell out of us.”
Martha gets the feeling she’s being deliberately shooed away. There’s more than enough things that need to be tested for them to both be running them at the same time, but the inflection in the woman’s voice indicates a finality attached to her words.
“Okay, uhm, I’ll let him know. You’re not going to do some crazy illegal test are you?”
“No, I just think he should be updated,” the woman says in an almost trained voice, calmness radiating from her sudden tone.
“Right. I can do that.”
The brunette gets half way down the hall when she realizes she has no clue where their grumpy boss might be. Not wanting to explore the entirety of the hospital, Martha turns around and starts to walk back to ask her coworkers. When she gets close enough to see into the dimly lit room, she freezes. The two seem to be arguing. Chase is still on the stool in front of the microscope, looking up at Thirteen with a petulant, almost defiant look on his face. Feeling like interrupting might not be a good idea, she goes off in search of House, feeling more out of the loop than she has all day.
XXX
“Tests were negative.”
“Same with ours.”
Thirteen and Chase walk in; a much needed interruption to whatever the other three men on the team are talking about, to inform them of their findings. House sighs and stares at the board again, twirling his marker. Taub looks up from where he’s munching on his hospital-prepared sandwich from the cafeteria. She’s already finished her own salad, but Foreman is still working on his. They nabbed sandwiches for the other two, now sitting in the middle of the large glass table.
As expected, Thirteen grabs hers ravenously, having not eaten for hours. Chase, however, sits and doesn’t so much as look at the last wrapped up sub, instead grabbing the folder to look at once again. Foreman and Taub look at the Australian, confusion written on their faces.
“You’re not eating? You always eat. You eat more than me and Foreman combined,” the eldest of the four questions.
With a frown, Chase grabs the sandwich and opens it, not breaking eye contact with the neurologist. He takes a bite and swallows, keeping his face impassive.
“Better?”
“Loads,” the man deadpans, rolling his eyes.
Throughout the new round of ideas, Martha notices Chase hasn’t touched his sandwich since the initial bite. He’s procured a water bottle from his bag, sipping on it every few minutes, but the food goes untouched and unnoticed by everyone else. She thinks she sees House’s eyes sweep over the intensivist, but she might be imagining things- House may play favorites but the idea of him caring about someone to a degree of worry seems improbable.
Foreman gets up to throw his trash away, prompting Thirteen to as well. As they talk about even more possibilities for the patient, Chase angles his face towards his chest, ducking his face downwards.
“ihNGkKt! h’GXKt! h’KGkTSCH’uh! SNF!”
The first two are quiet enough that if Martha wasn’t paying attention she doesn’t think she would have necessarily heard them. The third however is stronger and Martha cringes inwardly at not only the amount of force he’s used to try and hold it in, but also at the soupy sounding sniffle after. He gets up immediately, striding across the room to the kitchenette and plucks a tissue from the box they have sitting there. She notices he doesn’t blow, merely just wipes at his nose before pocketing the tissue and washing his hands. At least he’s hygienic.
“Bless you,” Taub throws over his shoulder casually.
Martha watches as the blonde ignores him, moving to snatch the 90% uneaten sandwich up instead and set it in the mini fridge to finish later. The medical student has the urge to throw out yet another statistic about the act of sternation but is interrupted by all six of their pagers going off- saved by the bell.
The rest of the day is a haze of the patient crashing, adrenaline, House getting angry for not being able to figure out what’s wrong, and everyone else picking up his energy. House is the determining factor of a lot more than she’s realized, as Foreman snaps back at their boss when he starts telling them they’re all morons. He goes as far as to insult not only Chase, but Thirteen, which Martha hasn’t witnessed yet.
“House, we’re trying. We can’t think any faster,” the dark skinned man frowns.
“Oh yeah? I bet I could make you think faster if you want to keep your job!”
“You’re not going to fire any of us,” Chase drawls from where he’s sitting, having moved from the uncomfortable metal chairs at the table to the slightly less uncomfortable chairs in the corner of the room.
“Wanna bet? You of all people should know I can and I will,” the older man sneers, moving closer to the blonde.
Martha has an odd feeling in her stomach, something between anxiety, anticipation and most of all, surprise. Does House mean he’s fired Chase before? Surely not, not when they’re so obviously the most in-sync out of everyone. For a split second the intensivist looks like he’s going to stand up and go at it with their boss but instead he just shrugs and presses the tips of his fingers to closed eyelids.
“Exactly. Now think.”
Finally, Thirteen comes up with a semi-plausible idea, and though House makes it known he doesn’t truly believe it, they’re ordered to go in and check the man’s mitral valve. Doing something is better than nothing, Martha agrees.
“Chase, scrub up and take Taub and Ms. Goody-two-shoes with you.”
“Can’t we have Masters do-“
“Absolutely not. This isn’t time for a learning experience, this is time to cut open this guy and fix him so he lives. She helps, you do.”
A grumble of incomprehensible words are drowned out by Taub getting up out of his chair and patting her shoulder, leaning his head towards the door as a gesture to tell her to follow. She does, not wanting to deal with any more childish back and forth arguing. As they all head down the hallway, Masters looks at Taub for direction. She doesn’t understand why Chase is upset she’s not doing it- usually it’s the other way around.
As the three slip into the empty elevator, Chase uses the inside of his wrist to scrub at his nose, sniffling yet again. Normally Martha wouldn’t notice these things, but he was late, so now all her attention is solely on him. It’s definitely not because he’s gorgeous or funny or the only to even remotely build her up sometimes.
“So why don’t you wanna do the surgery?” Taub asks, turning to the taller man.
“Because it’s cold in the OR and I’m already freezing,” Chase grumps, pulling his lab coat tighter. “Scrubs can only keep you so warm.”
24 notes
·
View notes
Text
Once again, doing the research, so you don't have to, A THREAD.
1). Separating Fact from Fiction: An Empirical Examination of Six Myths About Dissociative Identity Disorder (the full article)
Bethany L. Brand, PhD, Vedat Sar, MD, Pam Stavropoulos, PhD, Christa Krüger, MB BCh, MMed (Psych), MD, Marilyn Korzekwa, MD, Alfonso Martínez-Taboas, PhD, and Warwick Middleton, MB BS, FRANZCP, MD
Dissociative identity disorder (DID) is defined in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) as an identity disruption indicated by the presence of two or more distinct personality states (experienced as possession in some cultures), with discontinuity in sense of self and agency, and with variations in affect, behavior, consciousness, memory, perception, cognition, or sensory-motor functioning.1 Individuals with DID experience recurrent gaps in autobiographical memory. The signs and symptoms of DID may be observed by others or reported by the individual. DSM-5 stipulates that symptoms cause significant distress and are not attributable to accepted cultural or religious practices. Conditions similar to DID but with less-than-marked symptoms (e.g., subthreshold DID) are classified among “other specified dissociative disorders.”
DID is a complex, posttraumatic developmental disorder.2,3 DSM-5 specifically locates the dissociative disorders chapter after the chapter on trauma- and stressor-related disorders, thereby acknowledging the relationship of the dissociative disorders to psychological trauma. The core features of DID are usually accompanied by a mixture of psychiatric symptoms that, rather than dissociative symptoms, are typically the patient’s presenting complaint.3,4 As is common among individuals with complex, posttraumatic developmental disorders, DID patients may suffer from symptoms associated with mood, anxiety, personality, eating, functional somatic, and substance use disorders, as well as psychosis, among others.3–8 DID can be overlooked due to both this polysymptomatic profile and patients’ tendency to be ashamed and avoidant about revealing their dissociative symptoms and history of childhood trauma (the latter of which is strongly implicated in the etiology of DID).9–14
Social, scientific, and political influences have since converged to facilitate increased awareness of dissociation. These diverse influences include the resurgence of recognition of the impact of traumatic experiences, feminist documentation of the effects of incest and of violence toward women and children, continued scientific interest in the effects of combat, and the increasing adoption of psychotherapy into medicine and psychiatry.18,29 The increased awareness of trauma and dissociation led to the inclusion in DSM-III of posttraumatic stress disorder (PTSD), dissociative disorders (with DID referred to as multiple personality disorder), and somatoform disorders, and to the discarding of hysteria.30 Concurrently, traumatized and dissociative patients with severe symptoms (e.g., suicidality, impulsivity, self-mutilation) gained greater attention as psychiatry began to treat more severe psychiatric conditions with psychotherapy, and as some acutely destabilized DID patients required psychiatric hospitalization.31 These developments facilitated a climate in which researchers and clinicians could consider how a traumatized child or adult might psychologically defend himself or herself against abuse, betrayal, and violence. Additionally, the concepts of identity, alongside identity crisis, identity confusion, and identity disorder, were introduced to psychiatry and psychology, thereby emphasizing the links between childhood, society, and epigenetic development.32,33
In this climate of renewed receptivity to the study of trauma and its impact, research in dissociation and DID has expanded rapidly in the 40 years spanning 1975 to 2015.14,34 Researchers have found dissociation and dissociative disorders around the world.3,12,35–45 For example, in a sample of 25,018 individuals from 16 countries, 14.4% of the individuals with PTSD showed high levels of dissociative symptoms.35 This research led to the inclusion of a dissociative subtype of PTSD in DSM-5.1 Recent reviews indicate an expanding and important evidence base for this subtype.14,36,46
Notwithstanding the upsurge in authoritative research on DID, several notions have been repeatedly circulated about this disorder that are inconsistent with the accumulated findings on it. We argue here that these notions are misconceptions or myths. We have chosen to limit our focus to examining myths about DID, rather than dissociative disorders or dissociation in general. Careful reviews about broader issues related to dissociation and DID have recently been published.47–49 The purpose of this article is to examine some misconceptions about DID in the context of the considerable empirical literature that has developed about this disorder. We will examine the following notions, which we will show are myths:
belief that DID is a “fad”
belief that DID is primarily diagnosed in North America by DID experts who overdiagnose the disorder
belief that DID is rare
belief that DID is an iatrogenic disorder rather than a trauma-based disorder
belief that DID is the same entity as borderline personality disorder
belief that DID treatment is harmful to patients
MYTH 1: DID IS A FAD
Some authors opine that DID is a “fad that has died.”50–52 A “fad” is widely understood to describe “something (such as an interest or fashion) that is very popular for a short time.”53 As we noted above, DID cases have been described in the literature for hundreds of years. Since the 1980 publication of DSM-III,30 DID has been described, accepted, and included in four different editions of the DSM. Formal recognition as a disorder for over three decades contradicts the notion of DID as a fad.
To determine whether research about DID has declined (which would possibly support the suggestion that the diagnosis is a dying fad), we searched PsycInfo and MEDLINE using the terms “multiple personality disorder” or “dissociative identity disorder” in the title for the period 2000–14. Our search yielded 1339 hits for the 15-year period. This high number of publications speaks to the level of professional interest that DID continues to attract.
Recent reviews attest that a solid and growing evidence base for DID exists across a range of research areas:
DID patients can be reliably and validly diagnosed with structured and semistructured interviews, including the Structured Clinical Interview for Dissociative Disorders–Revised (SCID-D-R)54 and Dissociative Disorders Interview Schedule (DDIS)55,56 (reviewed in Dorahy et al. [2014]).14 DID can also be diagnosed in clinical settings, where structured interviews may not be available or practical to use.57
DID patients are consistently identified in outpatient, inpatient, and community samples around the world.12,37–45
DID patients can be differentiated from other psychiatric patients, healthy controls, and DID simulators in neurophysiological and psychological research.58–63
DID patients usually benefit from psychotherapy that addresses trauma and dissociation in accordance with expert consensus guidelines.64–66
An expanding body of research examines the neurobiology, phenomenology, prevalence, assessment, personality structure, cognitive patterns, and treatment of DID. This research provides evidence of DID’s content, criterion, and construct validity.14,55 The claim that DID is a “fad that has died” is not supported by an examination of the body of research about this disorder.
MYTH 2: DID IS PRIMARILY DIAGNOSED IN NORTH AMERICA BY DID EXPERTS WHO OVERDIAGNOSE THE DISORDER
Some authors contend that DID is primarily a North American phenomenon, that it is diagnosed almost entirely by DID experts, and that it is overdiagnosed.50,67–69 Paris50(p 1076) opines that “most clinical and research reports about this clinical picture [i.e., DID] have come from a small number of centers, mostly in the United States that specialize in dissociative disorders.” As we show below, the empirical literature indicates not only that DID is diagnosed around the world and by clinicians with varying degrees of experience with the disorder, but that DID is actually underdiagnosed rather than overdiagnosed.
Belief That DID Is Primarily Diagnosed in North America
According to some authors, DID is primarily diagnosed in North America.50,52,70 We investigated this notion in three ways: by examining the countries in which prevalence studies of DID have been conducted; by inspecting the countries from which DID participants were recruited in an international treatment-outcome study of DID; and by conducting a systematic search of published research to determine the countries where DID has been most studied.
Table 1
Dissociative Disorder Prevalence Studies

First, our results show that DID is found in prevalence studies around the world whenever researchers conduct systematic assessments using validated interviews. Table Table11 lists the 14 studies that have utilized structured or semistructured diagnostic interviews for dissociative disorders to assess the prevalence of DID.80 These studies have been conducted in seven countries: Canada, Germany, Israel, the Netherlands, Switzerland, Turkey, and the United States.37–39,44,45,71–79
Second, in addition to the prevalence studies, a recent prospective study assessed the treatment outcome of 232 DID patients from around the world. The participants lived in Argentina, Australia, Belgium, Brazil, Canada, Germany, Israel, the Netherlands, New Zealand, Norway, Singapore, Slovakia, South Africa, Sweden, Taiwan, and the United States.81 That is, the participants came from every continent except Antarctica.
Third, we conducted a systematic search of published, peer-reviewed DID studies. Using the search terms “dissociative identity disorder” and “multiple personality disorder,” we conducted a literature review for the period 2005–13 via MEDLINE, PsycInfo, and the Journal of Trauma and Dissociation. This search yielded 340 articles. We selected empirical research studies in which DID or multiple personality disorder had been diagnosed in patients. We recorded authors’ countries and institutions, and whether structured interviews were used to diagnose DID. Over this nine-year period, 70 studies included DID patients. Significantly, these studies were conducted by authors from 48 institutions in 16 countries. In 28 (40%) of studies, structured interviews (SCID-D or DDIS) were administered to diagnose DID.
In summary, all three methods contradicted the claim that DID is diagnosed primarily in North America.
Belief That DID Is Primarily Diagnosed by DID experts
Lynn and colleagues69(p 50) argue that “most DID diagnoses derive from a small number of therapy specialists in DID.” Other critics voice similar concerns.50,82,83 Research does not substantiate this claim. For example, 292 therapists participated in the prospective treatment-outcome study of DID conducted by Brand and colleagues.81 The majority of therapists were not DID experts. Similarly, a national random sample of experienced U.S. clinicians found that 11% of patients treated in the community for borderline personality disorder (BPD) also met criteria for comorbid DID.84 None of the therapists were DID experts. In an Australian study of 250 clinicians from several mental health disciplines, 52% had diagnosed a patient with DID.85 These studies show that DID is diagnosed by clinicians around the world with varying degrees of expertise in DID.
Belief That DID Is Overdiagnosed
A related myth is that DID is overdiagnosed. Studies show, however, that most individuals who meet criteria for DID have been treated in the mental health system for 6–12 years before they are correctly diagnosed with DID.4,86–89 Studies conducted in Australia, China, and Turkey have found that DID patients are commonly misdiagnosed.78,89,90 For example, in a study of consecutive admissions to an outpatient university clinic in Turkey, 2.0% of 150 patients were diagnosed with DID using structured interviews confirmed by clinical interview.74 Although 12.0% were assessed to have one of the dissociative disorders, only 5% of the dissociative patients had been diagnosed previously with any dissociative disorder. Likewise, although 29% of the patients from an urban U.S. hospital-based, outpatient psychiatric clinic were diagnosed via structured interviews with dissociative disorders, only 5% had a diagnoses of dissociative disorders in their medical records.37 Similar results have been found in consecutive admissions to a Swiss university outpatient clinic91 and consecutive admissions to a state psychiatric hospital in the United States45 when patients were systematically assessed with structured diagnostic interviews for dissociative disorders. This pattern is also found in nonclinical samples. Although 18.3% of women in a representative community sample in Turkey met criteria for having a dissociative disorder at some point in their lives, only one-third of the dissociative disorders group had received any type of psychiatric treatment.78 The authors concluded, “The majority of dissociative disorders cases in the community remain unrecognized and unserved.”78(p 175)
Studies that examine dissociative disorders in general, rather than focusing on DID, find that this group of patients are often not treated despite high symptomatology and poor functioning. A random sample of adolescents and young adults in the Netherlands showed that youth with dissociative disorders had the highest level of functional impairment of any disorder studied but the lowest rates (2.3%) of referral for mental health treatment.92 Those with dissociative disorders in a nationally representative sample of German adolescents and young adults were highly impaired, yet only 16% had sought psychiatric treatment.93 These findings point to the conclusion that dissociative disorder patients are underrecognized and undertreated, rather than being overdiagnosed.
Why is DID so often underdiagnosed and undertreated? Lack of training, coupled with skepticism, about dissociative disorders seems to contribute to the underrecognition and delayed diagnosis. Only 5% of Puerto Rican psychologists surveyed reported being knowledgeable about DID, and the majority (73%) had received little or no training about DID.94 Clinicians’ skepticism, about DID increased as their knowledge about it decreased. Among U.S. clinicians who reviewed a vignette of an individual presenting with the symptoms of DID, only 60.4% of the clinicians accurately diagnosed DID.95 Clinicians misdiagnosed the patient as most frequently suffering from PTSD (14.3%), followed by schizophrenia (9.9%) and major depression (6.6%). Significantly, the age, professional degree, and years of experience of the clinician were not associated with accurate diagnosis. Accurate diagnoses were most often made by clinicians who had previously treated a DID patient and who were not skeptical about the disorder. It is concerning that clinicians were equally confident in their diagnoses, regardless of their accuracy. A study in Northern Ireland found a similar link between a lack of training about DID and misdiagnosis by clinicians.96 Psychologists more accurately detected DID than did psychiatrists (41% vs. 7%, respectively). Australian researchers found that misdiagnosis was often associated with lack of training about DID and with skepticism regarding the diagnosis.85 They concluded, “Clinician skepticism may be a major factor in under-diagnosis as diagnosis requires [dissociative disorders] first being considered in the differential. Displays of skepticism by clinicians, by discouraging openness in patients, already embarrassed by their symptoms, may also contribute to the problem.”85(p 944)
In short, far from being overdiagnosed, studies consistently document that DID is underrecognized. When systematic research is conducted, DID is found around the world by both experts and nonexperts. Ignorance and skepticism about the disorder seem to contribute to DID being an underrecognized disorder.
MYTH 3: DID IS RARE
Many authors, including those of psychology textbooks, argue that DID is rare.70,97–99 The prevalence rates found in psychiatric inpatients, psychiatric outpatients, the general population, and a specialized inpatient unit for substance dependence suggest otherwise (see Table Table1).1). DID is found in approximately 1.1%–1.5% of representative community samples. Specifically, in a representative sample of 658 individuals from New York State, 1.5% met criteria for DID when assessed with SCID-D questions.77 Similarly, a large study of community women in Turkey (n = 628) found 1.1% of the women had DID.78
Studies using rigorous methodology, including consecutive clinical admissions and structured clinical interviews, find DID in 0.4%–6.0% of clinical samples (see Table Table1).1). Studies assessing groups with particularly high exposure to trauma or cultural oppression show the highest rates. For example, 6% of consecutive admissions in a highly traumatized, U.S. inner city sample were diagnosed with DID using the DDIS.37 By contrast, only 2.0% of consecutive psychiatric inpatients received a diagnosis of DID via the SCID-D in the Netherlands.38 The difference in prevalence may partially stem from the very high rates of trauma exposure and oppression in the U.S. inner-city, primarily minority sample.
Possession states are a cultural variation of DID that has been found in Asian countries, including China, India, Iran, Singapore, and Turkey, and also elsewhere, including Puerto Rico and Uganda.46,100–102 For example, in a general population sample of Turkish women, 2.1% of the participants reported an experience of possession.102 Two of the 13 women who reported an experience of possession had DID when assessed with the DDIS. Western fundamentalist groups have also characterized DID individuals as possessed.102 Such findings are inconsistent with the claim that DID is rare.
Go to:
MYTH 4: DID IS AN IATROGENIC DISORDER RATHER THAN A TRAUMA-BASED DISORDER
One of the most frequently repeated myths is that DID is iatrogenically created. Proponents of this view argue that various influences—including suggestibility, a tendency to fantasize, therapists who use leading questions and procedures, and media portrayals of DID—lead some vulnerable individuals to believe they have the disorder.52,69,83,103–107 Trauma researchers have repeatedly challenged this myth.48,49,108–111 Space limitations require that we provide only a brief overview of this claim.
A recent and thorough challenge to this myth comes from Dalenberg and colleagues.48,49 They conducted a review of almost 1500 studies to determine whether there was more empirical support for the trauma model of dissociation—that is, that antecedent trauma causes dissociation, including dissociative disorders—or for the fantasy model of dissociation. According to the latter (also known as the iatrogenic or sociocognitive model), highly suggestible individuals enact DID following exposure to social influences that cause them to believe that they have the disorder. Thus, according to the fantasy model proponents, DID is not a valid disorder; rather, it is iatrogenically induced in fantasy-prone individuals by therapists and other sources of influence.
Dalenberg and colleagues 48,49 concluded from their review and a series of meta-analyses that little evidence supports the fantasy model of dissociation. Specifically, the effect sizes of the trauma-dissociation relationship were strong among individuals with dissociative disorders, and especially DID (i.e., .54 between child sexual abuse and dissociation, and .52 between physical abuse and dissociation). The correlations between trauma and dissociation were as strong in studies that used objectively verified abuse as in those relying on self-reported abuse. These findings strongly contradict the fantasy model hypothesis that DID individuals fantasize their abuse. Dissociation predicted only 1%–3% of the variance in suggestibility, thereby disproving the fantasy model’s notion that dissociative individuals are highly suggestible.
Despite the concerns of fantasy model theorists that DID is iatrogenically created, no study in any clinical population supports the fantasy model of dissociation. A single study conducted in a “normal” sample of college students showed that students could simulate DID.112 That study, by Spanos and colleagues, documents that students can engage in identity enactments when asked to behave as if they had DID. Nevertheless, the students did not actually begin to believe that they had DID, and they did not develop the wide range of severe, chronic, and disabling symptoms displayed by DID patients.3
The study by Spanos and colleagues112 was limited by the lack of a DID control group. Several recent controlled studies have found that DID simulators can be reliably distinguished from DID patients on a variety of well-validated and frequently used psychological personality tests (e.g., Minnesota Multiphasic Personality Inventory–2),113,114 forensic measures (e.g., Structured Interview of Reported Symptoms),61,115,116 and neurophysiological measures, including brain imaging, blood pressure, and heart rate.
Two additional lines of research challenge the iatrogenesis theory of DID: first, prevalence research conducted in cultures where DID is not well known, and second, evidence of chronic childhood abuse and dissociation in childhood among adults diagnosed with DID. Three classic studies have been conducted in cultures where DID was virtually unknown when the research was conducted. Researchers using structured interviews found DID in patients in China, despite the absence of DID in the Chinese psychiatric diagnostic manual.117 The Chinese study and also two conducted in central-eastern Turkey in the 1990s78,118—where public information about DID was absent—contradict the iatrogenesis thesis. In one of the Turkish studies,118 a representative sample of women from the general population (n = 994) was evaluated in three stages: participants completed a self-report measure of dissociation; two groups of participants, with high versus low scores, were administered the DDIS by a researcher blind to scores; and the two groups were then given clinical examinations (also blind to scores). The researchers were able to identify four cases of DID, all of whom reported childhood abuse or neglect.
The second line of research challenging the iatrogenesis theory of DID documents the existence of dissociation and severe trauma in childhood records of adults with DID. Researchers have found documented evidence of dissociative symptoms in childhood and adolescence in individuals who were not assessed or treated for DID until later in life (thus reducing the risk that these symptoms could have been suggested).11,13,119 Numerous studies have also found documentation of severe child abuse in adult patients diagnosed with DID.10,13,120,121 For example, in their review of the clinical records of 12 convicted murderers diagnosed with DID, Lewis and colleagues11 found objective documentation of child abuse (e.g., child protection agency reports, police reports) in 11 of the 12, and long-standing, marked dissociation in all of them. Further, Lewis and colleagues11(p 1709) noted that “contrary to the popular belief that probing questions will either instill false memories or encourage lying, especially in dissociative patients, of our 12 subjects, not one produced false memories or lied after inquiries regarding maltreatment. On the contrary, our subjects either denied or minimized their early experiences. We had to rely for the most part on objective records and on interviews with family and friends to discover that major abuse had occurred.” Notably, these inmates had already been sentenced; they were all unaware of having met diagnostic criteria for DID; and they made no effort to use the diagnosis or their trauma histories to benefit their legal cases.
Similarly, Swica and colleagues13 found documentation of early signs of dissociation in childhood records in all of the six men imprisoned for murder who were assessed and diagnosed with DID during participation in a research study. During their trials, the men were all unaware of having DID. And since their sentencing had already occurred, they had nothing to gain from DID being diagnosed while participating in the study. Their signs and symptoms of early dissociation included hearing voices (100%), having vivid imaginary companions (100%), amnesia (50%), and trance states (34%). Furthermore, evidence of severe childhood abuse has been found in medical, school, police, and child welfare records in 58%–100% of DID cases.11,13,121 These studies indicate that dissociative symptoms and a history of severe childhood trauma are present long before DID is suspected or diagnosed.
Perhaps the “iatrogenesis myth” exists because inappropriate therapeutic interventions can exacerbate symptoms if used with DID patients. The expert consensus DID treatment guidelines warn that inappropriate interventions may worsen DID symptoms, although few clinicians report using such interventions.66,122 No research evidence suggests that inappropriate treatment creates DID. The only study to date examining deterioration of symptoms among DID patients found that only a small minority (1.1%) worsened over more than one time-point in treatment and that deterioration was associated with revictimization or stressors in the patients’ lives rather than with the therapy they received.123 This rate of deterioration of symptoms compares favorably with those for other psychiatric disorders.
MYTH 5: DID IS THE SAME ENTITY AS BORDERLINE PERSONALITY DISORDER
Some authors suggest that the symptoms of DID represent a severe or overly imaginative presentation of BPD.124 The research described below, however, indicates that while DID and BPD can frequently be diagnosed in the same individual, they appear to be discrete disorders.125,126
One of the difficulties in differentiating BPD from DID has been the poor definition of the dissociation criterion of BPD in the DSM’s various editions. In DSM-5 this ninth criterion of BPD is “transient, stress-related paranoid ideation or severe dissociative symptoms.”1 The narrative text in DSM-5 defines dissociative symptoms in BPD (“e.g., depersonalization”) as “generally of insufficient severity or duration to warrant an additional diagnosis.” DSM-5 does not clarify that when additional types of dissociation are found in patients who meet the criteria for BPD—especially amnesia or identity alteration that are severe and not transient (i.e., amnesia or identity alteration that form an enduring feature of the patient’s presentation)—the additional diagnosis of a dissociative disorder should be considered, and that additional diagnostic assessment is recommended.
On the surface, BPD and DID appear to have similar psychological profiles and symptoms.124,127 Abrupt mood swings, identity disturbance, impulsive risk-taking behaviors, self-harm, and suicide attempts are common in both disorders. Indeed, early comparative studies found few differences on clinical comorbidity, history, or psychometric testing using the Minnesota Multiphasic Personality Inventory and the Millon Clinical Multiaxial Inventory.124,127 However, recent clinical observational studies, as well as systematic studies using structured interview data, have distinguished DID from BPD.59,128 Brand and Loewenstein59 review the clinical symptoms and psychosocial variables that distinguish DID from BPD: clinically, individuals with BPD show vacillating, less modulated emotions that shift according to external precipitants.59 In addition, individuals with BPD can generally recall their actions across different emotions and do not feel that those actions are alien or so uncharacteristic as to be disavowed.59,128 By contrast, individuals with DID have amnesia for some of their experiences while they are in dissociated personality states, and they also experience a marked discontinuity in their sense of self or sense of agency.1 Thus, the dissociated activity and intrusion of personality states into the individual’s consciousness may be experienced as separate or different from the self that they identify with or feel they can control. Accordingly, using SCID-D structured interview data, Boon and Draijer128 demonstrated that amnesia, identity confusion, and identity alteration were significantly more severe in individuals with DID than in cluster B personality disorder patients, most of whom had BPD. However, DID and BPD patients did not differ on the severity of depersonalization and derealization. Both groups had experienced trauma, although the DID group had much more severe and earlier trauma exposure.
BPD and DID can also be differentiated on the Rorschach inkblot test. Sixty-seven DID patients, compared to 40 BPD patients, showed greater self-reflective capacity, introspection, ability to modulate emotion, social interest, accurate perception, logical thinking, and ability to see others as potentially collaborative.58 A pilot Rorschach study found that compared to BPD patients, DID patients had more traumatic intrusions, greater internalization, and a tendency to engage in complex contemplation about the significance of events.129 The DID group consistently used a thinking-based problem-solving approach, rather than the vacillating approach characterized by shifting back and forth between emotion-based and thinking-based coping that has been documented among the BPD patients.129 These personality differences likely enable DID patients to develop a therapeutic relationship more easily than many BPD patients.
With regard to the frequent comorbidity between DID and BPD, studies assessing for both disorders have found that approximately 25% of BPD patients endorse symptoms suggesting possible dissociated personality states (e.g., disremembered actions, finding objects that they do not remember acquiring)126 and that 10%–24% of patients who meet criteria for BPD also meet criteria for DID.75,126,130,131 Likewise, a national random sample of experienced U.S. clinicians found that 11% of patients treated in the community for BPD met criteria for comorbid DID,84 and structured interview studies have found that 31%–73% of DID subjects meet criteria for comorbid BPD.12,72,132 Thus, about 30% or more of patients with DID do not meet full diagnostic criteria for BPD. In blind comparisons between non-BPD controls and college students who were interviewed for all dissociative disorders after screening positive for BPD, BPD comorbid with dissociative disorder was more common than was BPD alone (n = 58 vs. n = 22, respectively).130 It is important to note that despite its prevalence in patients with DID, BPD is not the most common personality disorder that is comorbid with DID. More common among individuals with DID are avoidant (76%–96%) and self-defeating (a proposed category in the appendix of DSM-III-R; 68%–94%) personality disorders, followed by BPD (53%–89%).132,133
When the comorbidity between BPD and DID is evaluated specifically, the patients with comorbid BPD and DID appear to be more severely impaired than individuals with either disorder alone. For example, the participants who had both disorders reported the highest level of amnesia and had the most severe overall dissociation scores.130 Similarly, individuals who meet criteria for both disorders have more psychiatric comorbidity and trauma exposure than individuals who meet criteria for only one,134 and they also report higher scores of dissociative amnesia.135
In the future, the neurobiology of BPD and DID might assist in their comparison. Preliminary imaging research in BPD suggests the prefrontal cortex may fail to inhibit excessive amygdala activation.136 By contrast, two patterns of activation that correspond to different personality states have been found in DID patients: neutral states are associated with overmodulation of affect and show corticolimbic inhibition, whereas trauma-related states are associated with undermodulation of affect and activation of the amygdala on positron emission tomography.62 Similarly, recent fMRI studies in DID found that the neutral states demonstrate emotional underactivation and that the trauma-related states demonstrate emotional overactivation.137,138 Perhaps BPD might be thought of as resembling the trauma-related state of DID with amygdala activation, whereas the dissociative pattern found in the neutral state in DID appears to be different from what is found in BPD.139 Additional research comparing these disorders is needed to further explore the early findings of neurobiological similarities and differences.
What remains open for debate is whether a personality disorder diagnosis may be given to DID patients, because attribution of a clinical phenomenon to a personality disorder is not indicated if it is related to another disorder—in this instance, DID. Hence, the DSM-5 criteria for BPD may be insufficient to diagnose a personality disorder because DID is not excluded. In this regard, some DID researchers have concluded that unmanaged trauma symptoms—including dissociation—may account for the high comorbidity of BPD in DID patients.75,131 For example, one study found that only a small group of DID patients still met BPD criteria after their trauma symptoms were stabilized.140 Resolution of this debate may hinge on whether patients diagnosed with BPD are conceptualized as having a severe personality disorder rather than a trauma-based disorder that involves dissociation as a central symptom.
Yet to be studied is the possibility that several overlapping etiological pathways—including trauma,4,141 attachment disruption,142–144 and genetics145–149—may contribute to the overlap in symptomatology between BPD and DID. In order to clarify which variables increase risk for one or both developmental outcomes, research that carefully screens for both DID and BPD is needed. The apparent phenomenological overlap between the two psychopathologies does not create an insurmountable obstacle for research, because distinct influences may be parsed out via statistical analysis.135,150 Screening for both disorders would prevent BPD and DID from constituting mutually confounding factors in research specifically about one or the other.150
The benefit of accurately diagnosing (1) BPD without DID, (2) DID without BPD, and (3) comorbid DID BPD is that treatment can be individualized to meet patients’ needs. A diagnosis of BPD without DID can lead clinicians to use empirically supported treatment for BPD. By contrast, the treatment of DID is different from the treatment of BPD and comprises three phases: stabilization, trauma processing, and integration (discussed below).66 Given the severity of illness found in individuals with comorbid BPD/DID, clinicians should emphasize skills acquisition and stabilization of trauma-related symptoms in an extended stabilization phase. Early detection of comorbid DID and BPD alerts the therapist to avoid trauma-processing work until the stabilization phase is complete. The trauma-processing phase should be approached cautiously in highly dissociative individuals, and only after they have developed the capacity both to contain intrusive trauma material and to use grounding techniques to manage dissociation.
In summary, DID and BPD appear to be separate, albeit frequently comorbid and overlapping, disorders that can be differentiated on validated structured and semistructured interviews, as well as on the Rorschach test. While the symptoms of DID and BPD overlap, preliminary indications are that the neurobiology of each is different. It is also possible that differences between DID and BPD may emerge regarding the respective etiological roles of trauma, attachment disruption, and genetics.
MYTH 6: DID TREATMENT IS HARMFUL TO PATIENTS
Some critics claim that DID treatment is harmful.52,69,151–153 This claim is inconsistent with empirical literature that documents improvements in the symptoms and functioning of DID patients when trauma treatment consistent with the expert consensus guidelines is provided.65,66
Before reviewing the empirical literature, we will present an overview of the DID treatment model. The first DID treatment guidelines were developed in 1994, with revisions in 1997, 2005, and 2011. The current standard of care for DID treatment is described in the International Society for the Study of Trauma and Dissociation’s Treatment Guidelines for Dissociative Identity Disorder in Adults.66 The DID experts who wrote the guidelines recommend a tri-phasic, trauma-focused psychotherapy. In the first stage, clinicians focus on safety issues, symptom stabilization, and establishment of a therapeutic alliance. Failure to stabilize the patient or a premature focus on detailed exploration of traumatic memories usually results in deterioration in functioning and a diminished sense of safety. In the second stage of treatment, following the ability to regulate affect and manage their symptoms, patients begin processing, grieving, and resolving trauma. In the third and final stage of treatment, patients integrate dissociated self-states and become more socially engaged.
Early case series and inpatient treatment studies demonstrate that treatment for DID is helpful, rather than harmful, across a wide range of clinical outcome measures.64,140,154–158 A meta-analysis of eight treatment outcome studies for any dissociative disorder yielded moderate to strong within-patient effect sizes for dissociative disorder treatment.64 While the authors noted methodological weaknesses, current treatment studies show improved methodology over the earlier studies. One of the largest prospective treatment studies is the Treatment of Patients with Dissociative Disorders (TOP DD) study, conducted by Brand and colleagues.159 The TOP DD study used a naturalistic design to collect data from 230 DID patients (as well as 50 patients with dissociative disorder not otherwise specified) and their treating clinicians. Patient and clinician reports indicate that, over 30 months of treatment, patients showed decreases in dissociative, posttraumatic, and depressive symptomatology, as well as decreases in hospitalizations, self-harm, drug use, and physical pain. Clinicians reported that patient functioning increased significantly over time, as did their social, volunteer, and academic involvement. Secondary analyses also demonstrated that patients with a stronger therapeutic alliance evidenced significantly greater decreases in dissociative, PTSD, and general distress symptoms.160
Crucial to discussion of whether DID treatment is harmful is the importance of dissociation-focused therapy. A study of consecutive admissions to a Norwegian inpatient trauma program found that dissociation does not substantially improve if amnesia and dissociated self-states are not directly addressed.161 The study, by Jepsen and colleagues, compared two groups of women who had experienced childhood sexual abuse—one without, and one with, a dissociative disorder (DID or dissociative disorder not otherwise specified). None of the dissociative disorder patients had been diagnosed or treated for a dissociative disorder, and dissociative disorder was not the focus of the inpatient treatment. Thus, the methods of this study reduce the possibility of therapist suggestion. Although both groups had some dissociative symptoms, the dissociative disorder group was more severely symptomatic. Both groups showed improvements in symptoms, although the effect sizes for change in dissociation were smaller for the dissociative disorder group than for the non–dissociative disorder group (d = .25 and .69, respectively). As a result of these findings, the hospital developed a specialized treatment program, currently being evaluated, for dissociative disorder patients (Jepsen E, personal communication, June 2013).
Large, diverse samples, standardized assessments, and longitudinal designs with lengthy follow-ups were utilized in the studies by Brand and colleagues159 and Jepsen and colleagues.161 However, neither study used untreated control groups or randomization. Additionally, Brand and colleagues’ TOP DD study159 had a high attrition rate over 30 months (approximately 50%), whereas Jepsen and colleagues161 had an impressive 3% patient attrition rate during a 12-month follow-up.
DID experts uniformly support the importance of recognizing and working with dissociated self-states.65 Clinicians in the TOP DD study reported frequently working with self- states.122 While it is not possible to conclude that working with self-states caused the decline in symptoms, these improvements occurred during treatment that involved specific work with dissociated self-states. This finding of consistent improvement is another line of research that challenges the conjecture that working with self-states harms DID patients.69,152
Brand and colleagues47 reviewed the evidence used to support claims of the alleged harmfulness of DID treatment. They did not find a single peer-reviewed study showing that treatment consistent with DID expert consensus guidelines harms patients. In fact, those who argue that DID treatment is harmful cite little of the actual DID treatment literature; instead, they cite theoretical and opinion pieces.52,69,151–153 In their review—from 2014—Brand and colleagues47 concluded that claims about the alleged harmfulness of DID treatment are based on non-peer-reviewed publications, misrepresentations of the data, autobiographical accounts written by patients, and misunderstandings about DID treatment and the phenomenology of DID.
In short, claims about the harmfulness of DID treatment lack empirical support. Rather, the evidence that treatment results in remediation of dissociation is sufficiently strong that critics have recently conceded that increases in dissociative symptoms do not result from DID psychotherapy.104 To the same effect, in a 2014 article in Psychological Bulletin, Dalenberg and colleagues49 responded to critics, noting that treatment consistent with the expert consensus guidelines benefits and stabilizes patients.
(end article)
#Sage Speaks#Lilith - 🏍️#host posts#alter post#did alter#did#dissociative identity disorder#traumagenic#did research#anti endo#endo dni#fuck endos#endos aren't real#anti endogenic#did is a disorder#did is caused by trauma#you can't have did w/o trauma#endos cope harder
55 notes
·
View notes
Text
An explanation of the zeta potential concept
A Midwestern Doctor
Aug 16, 2024
Story at a Glance:
•Vaccines often cause various side effects, making it hard to identify common causes. Neurologist Andrew Moulden discovered that vaccines frequently trigger microstrokes, which can lead to a myriad of acute and chronic diseases.
•Forgotten research from the 1960s, shows that blood cell clumping is a root cause of many diseases—a belief also shared by Chinese Medicine.
•Colloidal chemistry and zeta potential science reveal that positive charges around blood cells cause clumping. Agents with concentrated positive charges, such as aluminum and the COVID spike protein, are especially problematic.
•Improving the physiologic zeta potential benefits a wide range of acute and chronic illnesses. A strong case can be made that many conventional and holistic therapies work in part by enhancing zeta potential.
Note: this is an abridged version of an article I previously published here. Since I receive many questions on this topic and readers wanted an concise version of it, I worked to distill it down to its key points so this topic could easily be shared with others.
Many medical problems stem from the diagnostic approach of physicians, especially with complex illnesses, which are often misdiagnosed and lead to ongoing patient struggles.
Complex conditions can present with varied symptoms across patients and resemble other illnesses (e.g., fibromyalgia vs. chronic fatigue syndrome). In turn, poorly trained physicians often default to psychiatric explanations, overlooking the true causes.
Vaccine injuries have a wide range of symptoms and hence have confused doctors for over 200 years (with many doctors in the past labeling them as “encephalitis”). Presently, I believe three main mechanisms underlie the myriad of vaccine injury:
Immune Dysfunction: Vaccines frequently cause chronic autoimmune disorders and varying degrees of immune suppression.
Cell Danger Response: Cells can enter a primitive state under threat, stopping normal mitochondrial function. This temporary state can become chronic, underlying many severe conditions. Treating this response has resolved conditions linked to vaccination, like autism.
Impaired Circulation: Vaccines can impair fluid circulation by affecting the body's zeta potential. This causes fluid clumping (i.e. micro blood clots and blood thickening) and obstructs blood flow in capillaries.
3 notes
·
View notes
Note
does/can type 1 diabetes exist in Time Lords/Gallifreyans? or would the technology be advanved enough to cure it?
Does diabetes exist in Time Lords?
In humans, diabetes is a condition characterised by issues with insulin production (Type 1) or insulin resistance (Type 2). For Gallifreyans, while their advanced biology provides some natural defences, they're not completely impervious and deal with a slightly different set of issues:
1️⃣Type 1 Diabetes in Gallifreyans
Manifestation and Symptoms:
In humans, Type 1 diabetes is characterised by the immune system declaring an unprovoked war on pancreatic beta cells, reducing or halting insulin production. For Gallifreyans, a similar autoimmune response could theoretically target cells or mechanisms involved in their glucose regulation - namely, X1 blood cells.
Given that X1 cells are responsible for transporting glucose, an autoimmune attack might disrupt this process, leading to irregular glucose levels despite their naturally higher baseline (8.9-11.7 mmol/L).
Symptoms might include a rollercoaster of energy levels and cognitive hiccups due to glucose imbalances.
Diagnosis and Management:
Gallifreyans would be born/loomed with Type 1 diabetes, possibly due to genetic predispositions or anomalies during the looming process.
Diagnosis would likely involve advanced biometric scanning and analysis of blood composition, focusing particularly on the functionality of X1 cells and their glucose transport capacity.
Treatments could involve cellular regeneration, genetic editing, or immunotherapy alongside your standard spacey-wacey machine™* to regulate glucose levels or cure it completely. And, of course, the simplest way to cure anything is regeneration, but it is probably a bit drastic and not a guaranteed fix if the condition is inherent in their genetic makeup.
2️⃣Type 2 Diabetes in Gallifreyans
Manifestation and Symptoms:
Type 2 diabetes, typically associated with insulin resistance, is far less common in Gallifreyans due to their efficient glucose management and general physiological Certificate of Excellence. This condition could develop at any time in a Gallifreyan's life, potentially due to lifestyle factors or physiological changes.
It might manifest as a reduced efficiency of X1 cells in glucose transport despite normal insulin production. Basically, the X1 cells have suddenly become slackers.
Symptoms could be subtler and might include reduced efficacy in their regenerative abilities and a slight decrease in overall vitality.
Also, because their homostatic mechanisms are so 'on-fleek', they'll start trying desperately to compensate, most notably in physiological cues, including dietary adjustments, increased exercise, stress management, and fluid intake adjustments.
Diagnosis and Management:
Preventive measures would likely be a key focus, with monitoring of individual health parameters to detect any early signs of insulin resistance.
Treatment could involve lifestyle interventions, although these might be more about fine-tuning. Additionally, advanced therapies to enhance X1 cell function or counteract insulin resistance at a cellular level could be employed. And you can always rely on your spacey-wacey machine™ for a complete cure.
Again, regeneration is an unnecessary drastic solution, but unlike Type 1, it would be effective in completely curing Type 2.
⚕️Holistic Approach
Gallifreyan medical technology approaches things more holistically, considering the interplay of their unique blood components, endocrine functions, and immune responses. The use of advanced diagnostics, personalised medicine, and possibly even real-time monitoring and adjustment of physiological parameters would be standard practices in their healthcare system.
🏫 So ...
In Gallifreyan society, while diabetes may not be as prevalent or manifest in the same way as in humans, it's a condition that their medical technology is well-equipped to manage. And if it can't manage it, there's always regeneration, but don't be wasting those bodies, now.
*A spacey-wacey machine™: any piece of equipment that can magically do future-y things because, well, sci-fi.
Related (kind of, not really):
Do Time Lord-specific disabilities exist?: Types of disabilities specifically for Gallifreyans, both known and theoretical.
Can disabilities persist through regenerations?: The nature of inherent and regeneration-specific disabilities.
Hope that helped! 😃
More content ...
→📫Got a question? | 📚Complete list of Q+A and factoids
→😆Jokes |🩻Biology |🗨️Language |🕰️Throwbacks |🤓Facts
→🫀Gallifreyan Anatomy and Physiology Guide (pending)
→⚕️Gallifreyan Emergency Medicine Guides
→📝Source list (WIP)
→📜Masterpost
If you're finding your happy place in this part of the internet, feel free to buy a coffee to help keep our exhausted human conscious. She works full-time in medicine and is so very tired 😴
#doctor who#gil#gallifrey institute for learning#dr who#dw eu#gallifrey#gil biology#gallifreyans#ask answered#gallifreyan biology#whoniverse#time lord biology
19 notes
·
View notes
Text
Thank you to everyone who voted on the last poll, and all the people who put their cool ideas in the tags. This is the new poll and it’ll have to be two parts because there’s too many degrees.
Thaumaturgical Artificing- The scientific study and application of magic as it pertains to Alchemy (the creation of of potions) and Arcana (the engineering of magical devices).
Advanced Applied Necromancy- A degree for those looking for the most modern and ethical methods of raising the dead. This is a degree for those looking for new and inventive ways to apply the Necromantic Arts to the betterment of society. Students can expect to learn the ways in which Necromancy can be applied to various fields such as medicine, criminal justice, and even industry, all wrapped up in serious discussions about ethics and consent.
Arcanic Archaeology- This degree walks students through the history of magical artifacts, how to find them, and their proper uses to aspiring Sorcerers and non-magic users alike.
Linguistic Incantology- The study of the properties of magical languages as well as the characteristics of those languages in general ascertained in order to gain mastery over the magical art of incantation.
Runic Studies- the study of the history of runes and sigils, their relevance in art, politics, and culture, and their various uses to the modern spell caster.
Magiphysical Sciences- The study of Humanoid systems, anatomy, and physical health and fitness as it pertains to magical gestures and more physically involved magic systems.
Mystic Virology- The study of magical diseases and curses, their effects on the humanoid form, and the treatments and counterhexes for such magical conditions.
Beasts Behavior and Health Sciences- This degree will prepare students for work with both wild and domestic fantastical creatures by giving them essential knowledge and essential skills in magical veterinary medicine and biology, grooming, feeding, and care, as well as wildlife rehabilitation.
Magical Performance Arts- A degree for those seeking to enchant and bewilder audiences of all ages. If you’re looking for something something showy and fun, look no further! Includes the option for courses like Enchantments and Shapeshifting.
Wandsmithing Technologies- This is a course for students looking to design wands. Students will learn to many essential lesson including, but not limited to, magidynamics, the magical components of many different wand building materials, and a comprehensive analysis on different wand styles throughout the ages. At the end students will have several wand prototypes and models under their belts.
Criminal Justice- Study how criminal justice organizations function, deal with people and their recurring problems, and create programs and policies that include and benefit the community. Here’s the twist; we add in a little magic to make your job easier. A popular magic class taken for this degree Scrying (with a warrant of course).
Supernatural Physics- the study of how and why magic came to be and how and why it works. Students will learn the structure of magic and how it interacts with other fundamental constituents of the universe.
Economic Divination- This degree provides studies in supply and demand, consumer behavior, and financial markets with an added twist. Students will learn the most reliable methods of divination to help insure future financial success.
Mystic Ecology- The study of relationships among living magical organisms, humanoids, and their physical environments. This degree looks at organisms at the individual, population, community, ecosystem, and biosphere level. Students can expect to learn how to use their magic to help repair damaged ecosystems, increase power output, and cast diagnostic spells to access what remediation is necessary.
Novel Entomology- The scientific study of magical species of insects, arachnids, myriapods, and crustaceans.
Magic History- The history of magic and it’s uses across different ages and cultures. This class will look at the different major events involving and influenced by magic and it’s interaction with society.
General Studies- This degree covers the most basic information on various magical studies and provides a great opportunity for students to discover their magical passions and/or complete their prerequisite courses before moving on to a more advanced degree.
#screw jkr#harry potter#hogwarts houses#polls#magic school au#college#fantasy#folklore#mythology and folklore#magic science#magical realism#aspiring author#neurodivergent author#writblr#science#chemistry#engineering#virology#linguistics#constructed language#ecology#entymology#magic story#necromancer#performance arts#theater kid#woodshop#archeology#zoology#veterinarian
35 notes
·
View notes
Last Seen Blogs

amanihealthcareservicesllc
AMANI HEALTH CARE SERVICES LLC

mrmodyvincento-blog
Untitled

sarahbguest
Untitled

elenamirulla
Elena Mirulla Fumettista

sektiono-posts-blog
Untitled