#i have a migraine and i'm choosing to believe that this information is what caused it so thanks ghostie 🙄🙄🙄 /JJJ
Text
earlier bonnie my good friend bonnie told me that scraptrap's "i always come back" voiceline is a popular sound on tiktok (paired with a song) and i was like "no fucking way" but no. she was right. and this information has been ruining my life ever since.
#/J BUT ALSO. IT'S SO AWFUL I HATE IT#just look up ''i always come back tiktok'' on youtube to find a compilation#just a shit ton of cute girls making thirst traps and oh my god it's so fucking funny but also i feel like i'm on a different planet#there's no way they know......#someone please fucking tell them JFJDISNDIENEK L#i can't stop thinking about it like oh my god girl help#we've somehow come full circle#i can't explain how but william being a tumblr sexyman is connected to all this somehow i just haven't figured it out yet#i'm mentally mapping out a red string corkboard with all the information but it's not adding up#i'll get there eventually#I NEED TO KNOW WHO THE FIRST PERSON WHO USED THIS SOUND WAS. DID THEY KNOW?? ARE THEY THE ONLY PERSON USING IT WHO KNOWS??#how did it make it into mainstream tiktok i cannot fathom this#at least he's finally getting the popularity he deserves /j#peepaw is tiktok famous this is great news#i have a migraine and i'm choosing to believe that this information is what caused it so thanks ghostie 🙄🙄🙄 /JJJ#talking.txt
4 notes
·
View notes
Note
Heya!
For any OC who needs a bit more development/ 'on screen' time:
What is your OC's pain tolerance like?
What memory would your OC rather just forget?
What is your OC's weapon of choice? Have they ever actually used it?
(also, if required, use this as permission to slack off for a bit. Take some rest, do something fun, and remember you're cared about)
Heya! You're always a joy to see in my notes, such a positive force in this community, lovely, lovely, thank you for the ask!
I'm gonna do these for Anthony, full name Dr. Anthony Kasperek, an OC I've had for over a year but never really talked about, but the basics are: he's a scientist in the field of astro*incoherent mumbling* uh something or other, tentatively astrobiology, but maybe astrophysics or something else entirely depending which way the story goes or if I at all figure out what I'm talking about, point is, space science of some sort, okay, and he's one of a number of scientists invited to this somewhat shady facility to study what may be a possibly earth-shattering extraterrestrial artefact. He's stubborn, paranoid, jumpy, and a bit of an insomniac (because which of my ocs aren't at this point), but has a passion for space and the stars and unlocking the mysteries of the universe like nothing else. He's also very very good at his job, but has a manic edge that tends to scare people away, himself included sometimes. Anyway, onto questions:
What is your OC's pain tolerance like?
I'm oscillating between the idea of it being really low or really high due to the fact he's used to having to deal with things like massive migraines, needles and too much stimuli, but I don't know if that would make him more or less susceptible to the pain it causes. Because on the one hand, the familiarity could make him more numb to it, but on the other hand, it could also make him even more wary, elevating the issue in part psychosomatically. It certainly still causes him stress, so I'm inclined to think the amount he's been relegated to has actually lowered his pain tolerance over the years, making the sensations all the more unbearable/worse each time because he knows it's coming but still is never prepared because in an ideal world, he wouldn't have to deal with it again at all, and he wants to believe he's done with it, believe the pain will never come back, so it's a source of fear and shock every time it does.
2. What memory would your OC rather just forget?
Oh, for Anthony, I'm sure there are too many, especially the way his brain works, solidifying the worst of them, while throwing the rest into chaos when he's trying to focus and suddenly can't remember that vital piece of information in his head that was just there, it was just there, and also especially with his reputation as the “eccentric” scientist, which he’d rather have left behind. There's definitely the... incident that led him to be let go from his job at NASA, which he doesn’t like to talk about, (and also doesn’t understand how it hasn’t barred him from working on such a sensitive project, because what’s up with that? Why did they choose him? Why did they choose him?), and there’s the time in college when he had to spend a semester in the psych ward, but even then he had the stars to comfort him, (he somehow talked them into letting him have those little plastic glowing ones on the ceiling).
3. What is your OC's weapon of choice? Have they ever actually used it?
Is it trite if I say his intellect/his mind? Though sometimes in that case, the weapon occasionally turns on himself. Actually, I'll go with something even more trite and say his genuine love for the universe and everything in it is his greatest weapon (and probably a secret tool that will help us later.jpeg). Barring that, I think he'd think daggers are pretty cool, but I doubt that will come up in the story, I'm sure he might whack someone with his telescope if in a pinch, but ough the calibration, but when cornered, his weapon of choice would probably be his fists or his nails, or throwing whatever random objects happen to be in the vicinity, perhaps if given the opportunity, he might find a way to give someone a little zap with the building's electricity. He may or may not have used those last few methods before...
#writing#writeblr#tw psych ward mention#my ocs#ask#ask game#thank you again#i'll answer the other couple asks soon if anyone's reading this i swear#writing asks#look at my character boy 🥺
2 notes
·
View notes
Text
Dissociative Disorders 101
In this post, I'm going to give an outline of Dissociative identity disorder (DID) and Other Specified Dissociative disorder (OSDD).
These two disorders are terribly misunderstood due to horrible representation in media, a lack of education on the topic. Many people still refer DID as Multiple Personality Disorder (MPD) an outdated term from when DID was classified as a personality disorder, we now know the disorder is better seen as a dissociative disorder. I hope this post will help clear up misunderstandings about these topics.
[CW: Mentions of abuse, medical trauma, war, human tracking, suicide, self-harm, and addiction. All of these are briefly mention and not discussed in detail. Ableism is the only cw discussed in detail]
[Note: This post is not to be used as a diagnostic tool.]
DID & OSDD Glossary:
Alter: Shorthand for alternate personality or alternate identity. The most common language to refer to the multiple identities in the system. You may also see the terms "parts" & "headmates".
Alter jobs: also called “Alter types” or “Alter Roles”. This refers to the common occurrence of certain alters taking on specific roles. This often happens because to some extent DID & OSDD acts as extreme involuntary coping skills. Examples of this are protectors who deal with danger, caretakers who help keep the alters in the system comforted, or trauma holders who retain memories of trauma.
Co-Consciousness: often shortened to co-con. When two or more alter are aware of the outside together. Thoughts of both alters can often blend together. Even at times alters may have split control of the body.
Depersonalization and Derealization: Often shortened to DR/DP. DR/DP disorder is its own diagnosis but those with other dissociative disorders experience it as well. Depersonalization the feeling of oneself is not real or is heavily disconnected from the body. This can even result in one of feeling in control of limbs at all. Derealization is the feeling of the outside world not being real, or a simulation.
Fronting: The act of being the alter conscious at the time and ability to interact with the outside world.
Host: Either the person believed to be the “first” personality (sometimes called the core or original) or the latter who fronts the most.
Splitting: In this case, it refers to when new alters form.
System: A word used to reference all of the alters as a whole. Used like "I am an alter in a system" or sometimes “ I am a system”. Rather someone uses this term is a matter of personal preference, and if they see themselves as part of a system or collectively are a system.
What is Dissociation?
Dissociation refers to the mechanism our brain has to disconnect us from our surroundings sometimes as a benign reaction but severe dissociation is associated with trauma and other mental illnesses.
Every Person has the capacity for dissociation and many experiences some degree of the skill like when you drive home but don’t remember it. However daydreaming in class, spacing out every now again is healthy, there is a huge difference between those experiences and those of people with dissociative disorders.
Dissociation is primarily associated with DID but can also be a symptom of C-PTSD, Borderline Personality Disorder (BPD) and some forms of psychosis. There are also physiological conditions that cause and/or mimic dissociation. Like seizures and migraines.
What are the symptoms of DID & OSDD?
[Disclaimer: I’m aware that the DSM is a flawed way to look at mental health, but it is the best way we have to ensure all parties are working with the same definition of terms]
DID:
DID diagnostic criteria are as follows:
1)Two distinct identity states are present. They have to be separate and able to act autonomy. It isn’t “feeling” like another person.
2)Amnesia must occur, defined as gaps in the recall of everyday events, important personal information and/or traumatic events
3)The person must be distressed by the disorder or have trouble functioning in one or more major life areas because of the disorder. This criterion is common among all serious mental illness diagnoses as a diagnosis is not appropriate where the symptoms do not create distress and/or trouble functioning.
4)The disturbance is not part of normal cultural or religious practices.
This DID criterion is to eliminate diagnosis in cultures or situations where multiplicity is appropriate. An example of this is in children where an imaginary friend is not necessarily indicative of mental illness.
5) The symptoms are not due to the direct physiological effects of a substance
So what does that mean? It means that those who have the disorder have at least one alter the hallmark of DID. Alter come in all kinds of varied types and versions. The amnesia criterion does refer to forgetting traumatic events, but also incidents in normal life.
Alters themselves are a complex they aren’t "alter egos or" made up people. Alters can be almost anything, children (younger than the body) adult alters (older than the body), alters based on fiction called Fictional introjects (fictives for short), alters who are angels or spirits, ghost alters, animal alters, alters of varying race and sexualities. This is because alters form to ensure the survival of the child, this includes alters to comfort, protect, soothe and hold trauma away from the wider consciousness. This means that anything that can fill that role can be put into an alter. There is no control over alters, they are not imaginary friends or malleable they are the best way the mind had to survive.
In day to day life DID might look like having missing time, experience dissociation even when in control, a sense of not having an identity, hearing voices within their heads (not auditory hallucinations), meeting people you feel like you should know, having actions you took but have no recollection of, overlapping emotions and trouble focusing.
People with DID have high rates of self-harm, suicidal behaviour, addiction, disordered eating and other behaviours that cause damage to oneself. This is often even more distressing as one might hurt themselves and not remember it because an alter did it.
Those with DID will also often have what is referred to as “Inner worlds” or “headspace” this refers to in the mind of the person there is a mental world within. This is a place where alters have a form, body and voice within the mind. It is often a combination of a coping skill used as a kid to escape and a way to be able to interact with others alters. Headspaces often are where alters feel they are when not fronting. It also provides a way of seeing where alters who are not in communication with others are, and can sometimes serve as a visual connection to understanding the others in the system and understand trauma.
Somatic symptoms are really common, Including: Headaches, nausea and vomiting, Non-epileptic seizure/psychogenic seizures, blurred vision, muscle aches, nerve dysfunction (like dysautonomia), fatigue, other feelings of illness. This is sometimes part of conversion disorder.
People with DID & OSDD almost always also have (C-)PTSD. So symptoms like hypervigilance, nightmares, and flashbacks. As they have DID & OSDD and have experienced trauma they likely have symptoms from that other than dissociation, even if they do not meet PTSD criteria.
BPD has high comorbidity with DID, many people with DID or OSDD are misdiagnosed with BPD. Other common comorbid conditions include Anxiety Disorders, Depression, Eating Disorders, and Conversion Disorder.
OSDD:
So the thing about OSDD is a category of conditions that don’t fit another diagnosis. With this post, we are mostly concerned with OSDD-1a and OSDD-1b because those disorders are most similar to DID and form systems.
The DSM Description is as follows:
This category applies to presentations in which symptoms characteristic of a dissociative disorder that cause clinically significant distress or impairment in social, occupational, or other important areas of functioning predominate but do not meet the full criteria for any of the disorders in the dissociative disorders diagnostic class. The other specified dissociative disorder category is used in situations in which the clinician chooses to specify the reason that the presentation does not meet the criteria for any specific dissociative disorder. This is done by recording "other specified dissociative disorder" followed by the specific reason (e.g., "dissociative trance"). Example presentations that can be specified using the "other specified" designation include the following:
1. Chronic and recurrent syndromes of mixed dissociative symptoms. This category includes identity disturbance associated with less than marked discontinuities in sense of self and agency, or alterations of identity or episodes of possession in an individual who reports no dissociative amnesia.
2. Identity disturbance due to prolonged and intense coercive persuasion: Individuals who have been subjected to intense coercive persuasion (e.g., brainwashing, thought reform, indoctrination while captive, torture, long-term political imprisonment, recruitment by sects/cults or by terror organizations) may present with prolonged changes in, or conscious questions of, their identity.
3. Acute dissociative reactions to stressful events: This category is for acute, transient conditions that typically last less than 1 month, and sometimes only a few hours or days. These conditions are characterized by constriction of consciousness; depersonalization; derealization; perceptual disturbances (e.g., time slowing, macropsia); micro-amnesias; transient stupor; and/or alterations in sensory-motor functioning (e.g., analgesia, paralysis).
4. Dissociative trance: This condition is characterized by an acute narrowing or complete loss of awareness of immediate surroundings that manifest as profound unresponsiveness or insensitivity to environmental stimuli. May be accompanied by minor stereotyped behaviours of which the individual is unaware and/or that he or she cannot control, as well as transient paralysis or loss of consciousness. The dissociative trance is not a normal part of a broadly accepted collective cultural or religious practice.
Those with OSDD-1a&b meet most but not all of DID criterion. They are considered Complex Dissociative Disorders along with DID.
OSDD-1a is either identity disturbance with less distinct alters than DID (they cannot physically take executive control over the person's body, but strongly influence the person's thoughts and actions with this type there is amnesia.
OSDD-1b does have distinct alter do exist and can take executive control with the type there is no amnesia.
How does DID or OSDD Develop?
DID & OSDD comes from long term childhood trauma. When a child is exposed to long term trauma and the identity of the child cannot properly integrate. This means your brain put up amnesic barriers to memories and perception forming the separate identity states.
DID is highly correlated with sexual abuse, physical abuse, medical trauma, living in a war zone, child trafficking, and Ritual abuse. Another key factor in a child developing these disorder is the lack of healthy attachment (more info here) You can not develop this disorder after age 9, you can't develop it from a single trauma.
The most current theory used to understand how these disorders works are Structural Dissociation. It refers to the way our brain changes the usual structure to compensate for traumatic experiences. It also posits that a child is not born with an integrated personality, to begin with, and this what allows the extreme dissociative symptoms of DID to manifest.
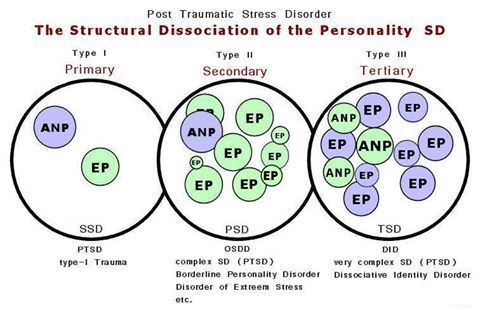
(Image Source)
ANP refers to “Apparently Normal Part” (someone who takes care of daily life)
EP refers to “Emotional part” (someone who holds trauma memories, reactions, and/or sensations).
Primary SD: is found among those with PTSD. The EP holds all trauma associated things such as fight or flight, feelings, sensations, etc, and is not a fully differentiated being (such as alters are/can be in DID and OSDD-1)
Secondary SD is OSDD, complex PTSD, and BPD. OSDD-1 has the most developed EPs out of the secondary SD disorders. BPD and C-PTSD EPs are less developed than OSDD-1 and are fragments (less fragmented than fragments found in OSDD-1 and DID). Secondary SD emotional parts hold less trauma-related material than the single EP found in PTSD. While the EP in PTSD will hold all of the trauma, there may be an EP in the secondary SD category for an emotion related to the traumas, another for body memories, another for visual memories and auditory memories in some of the traumas, and so on.
Secondary SD is OSDD, PTSD, and BPD. OSDD-1 has the most developed EPs out of the secondary SD disorders. BPD and C-PTSD EPs are less developed than OSDD-1 and are fragments (less fragmented than fragments found in OSDD-1 and DID). Secondary SD emotional parts hold less trauma-related material than the single EP found in PTSD. While the EP in PTSD will hold all of the trauma, there may be an EP in the secondary SD category for an emotion related to the traumas, another for body memories, another for visual memories and auditory memories in some of the traumas, and so on.
Tertiary SD refers to DID. There are multiple ANP and multiple EP. They are more developed than the ANP and the EPs in Secondary structural dissociation (though DID parts can have the same degree of development as OSDD-1 parts and vice versa). EPs can be “small”, as in less developed and would be considered fragments, as they hold limited trauma material such as a single feeling or one or two of the senses in a few trauma memories (or just one or two of the senses in one trauma memory). EPs can also be a fully developed part, such as an ANP would be, but hold trauma material. Multiple ANPs exist and can have various jobs associated with daily life such as a school part, a work part, a caretaker part, etc.
This theory is one of the most widely accepted concepts of how alters form and best matches most people's experience. It does contradict the idea that alters are split pieces of one cohesive identity being split the old model.
Another thing to keep in mind about this theory is it shows the structure and function of the brain are altered from a young age. Brains conditioned to dissociate during stress and trauma will continue to split during stress. This means alters can continue to form in those with DID & OSDD past age 9.
This Video explains further how this relates to alters splitting
Treatment:
DID & OSDD can be treated and worked on so the person is no longer experiencing the adverse effects or usually lessen them. Treating DID works mostly the same way as any other trauma survivor. Most kinds of trauma therapy can be used, EMDR being the exception. Certain kinds of meditation and visualisation also prove to be not as effective.
Medication can be used to treat comorbid disorders like depression or anxiety but there are no pharmacological treatments for DID on its own.
What is unique about DID is there is the aspect of how the alters affect you. With DID & OSDD time spent with, alters is crucial. Helping alters who are struggling with trauma becomes deeply important in healing.
The two main options with alters are integration or communication.
Integration refers to a process of when two identity states fuse together. This means you have less altered consciousness states, it also relates to them both being able to handle their trauma. The goal here is to end up with the patient having a singular integrated identity.
The other treatment focuses on forming functional working relationships with the altar and helping them process trauma individually, integration might still happen but a singular identity is not the end goal.
Mythbusting:
“People with DID are just psychotic or delusional” False, psychosis is not a feature of DID or OSDD and has been shown to act completely differently for the person and in the brain than psychosis. This is also offensive as it denigrates people with psychosis.
“DID is fake/made up by a therapist/ social contagion/the person only believes they have alters” False: DID has been observed in multiple studies and social contagion, malingering and therapist coercion are no longer prime theories. People saying this often bring up the false memory scare and Sybil. Both of those have been proven to be wildly overstated and are not the only evidence we have. There are cases dating back to the 1500s with the first psychiatric observations in the 1800s.
“Aren’t they dangerous?” or “they're so scary and crazy!” or “Don’t they need to be locked up” False, The real facts are people with dissociative disorders don’t commit violence at a higher rate than anyone else. They are much more likely to be the victims of violence. Starting with the fact they faced violence as a child to even have the disorder.
“Isn't that possession?” or any other spiritual concepts. False, There is nothing supernatural reasons for DID. Some people have spiritual or religious beliefs that change how they personally perceive their condition, but there is nothing supernatural about DID or OSDD.
“It’s super rare” Not actually the estimate for DID is about 1% of the population. Might sound small but with the number of people in the US alone who have, it means you're likely to meet someone with it.
“I would know if you had it” Not likely. Most people with DID present with covert DID. These people do not have alters who act wildly different from the host. Generally alters will attempt to not show obvious signs as well as being n the same mind with similar physiological aspects and upbringing influence things like mannerisms. Only 5-6% of people with DID have an overt presentation. Even these people are unlikely to be able to wildly change the way they dress and the like as it’s impractical.
“Bad alters/evil alters/violent alters/murder alters” False. There are often alters who might feel aggressive or be persecutors who hurt the other alters. But they are not going to commit murder or rape. They are usually more dangerous to the person with the disorder than anyone outside. And this anger usually stems from trauma.
“You can’t have the disorder you wouldn’t know” and other variations on “Crazy people don't know their cray”. False usually people with DID reach out to help themselves they don’t get forced into it. Because the symptoms of DID disrupt life and the usual comorbid PTSD or other mental health conditions. People with DID are also often aware to some extent of their alters. Rather this is voices, time gaps, or passive influence. And people who have known about the disorder and are in treatment often have good communication between alters in the mind, they are definitely aware of their health.
I Hope this is helpful for those with and without the disorder to better understand these conditions. My personal experience with DID does mean I’m particularly passionate about education on this topic even more as it intersects with education about trauma in general. I hope this didn’t come off as adversarial and helps people learn.
-Admin 1
{Resources: Structural Dissociation Explained, OSDD Diagnostic Material, The Fantasy Theory of DID, New Models of DID, DID Literature Review, DID Research.org, DSM Library, Webermann, A. R. & Brand, B. L. (2017). Mental illness and violent behaviour: The role of dissociation. Borderline Personality Disorder and Emotion Dysregulation}
#blog post#mental illness#mental health resources#mental health education#mental illness education#dissociative identity disorder#did#other specified dissociative disorder#osdd#osdd1#multiple personality disorder#mpd#dissociative disorder#dissociatvie disorders#dissociation#childhood trauma#structural dissociation#bpd#cptsd#ptsd#disordered eating#long post
39 notes
·
View notes
Photo

Top 10 Food Myths
these are the possibly false truths we convinced ourselves to believe in regards to our food an apple a day keeps the doctor away and you're wondering is that really true welcome to watchmojo.com and today we're counting down our picks for the top ten food myths at the end of the day if we compare them side-by-side there are pros and cons for each for this list we're focusing on popular adages
about food or common diet tips some of which have merit some of which don't and some of which do but not for the reasons you'd think then I would probably consider limiting or avoiding gum until the child gets a little bit older but as always be sure to consult a medical professional when it comes to your health stay lean and stay strong number 10 microwaving food destroys nutrients myth we're talking really bad we begin
our list with the big bad microwave any new technology attracts its share of critics and the microwave was no different why don't you build something like he does stead of all your empty deals it's just like your science oven you know I read that it takes all of the nutrition out of our food empty just like your deal it's long been suggested that cooking food this way can rob it of its healthy
properties but for the most part that's just not true it's actually the cook time and heat level that is most likely to destroy nutrients and since a microwave takes less time than most conventional cooking methods in many cases it might actually help retain more of the healthiness and cook for three to four minutes until the salmon is flaky pro tip try steaming vegetables in a sealed microwave safe ditch with a small amount of
water for delicious and nutritious veggies it's also very important to choose glass cookware or microwave safe cookware that doesn't emit or leach different plastic compounds which can be toxic number 9 pop rocks plus soda equals kaboom miss thirsty what's wrong something you might have heard about mixing pop rocks some soda well you there stomach and your intestines everything first coca-cola hit the market in 1886 pop rocks hit the market in 1975 rumours claiming that ingesting these
junky products at the same time would cause your stomach to explode due to excessive carbon dioxide from the combo of the fizzy candy and the carbonated drink weren't far behind I'm a little afraid I can't say oh let me see let's all see okay oh crap everyone heard this urban legend when they were growing up and many of us may have actually believed it the people of Seattle believed it so much the US
Food and Drug Administration had to set up a hotline to calm them down oh but the truth is the worst thing you could likely do to you is cause a nice satisfying belch ah odd then number eight eggs are bad for your heart if this food factoid has been debated for years but here's what we know eggs contain cholesterol and too much cholesterol can lead to health problems like heart disease so how is this
amiss well contrary to what you might have been told eggs are one of the healthiest foods you can consume as they're full of vitamins minerals and protein if you're healthy and don't have a history of heart problems you can likely eat an egg a day without it adversely affecting your cholesterol levels as your body will offset it by producing less cholesterol itself so will that be scrambled or sunny-side up there was a widely spread
study that eggs were not good for you this just doesn't simply make any sense number seven red wine is good for your heart fact yep I don't care what the scientists say I'm just gonna keep on drinking all you wine drinkers out there prepare to rejoice scientists have been studying the connection between wine consumption and heart health for years after looking at the French diet and noticing relatively low rates of heart disease even though
their traditional foods are fatty and if they want to drink Merlot we're drinkin Merlot know if anybody orders Merlot I'm leaving I am not drinking any more low but it's true red wine features heart-healthy properties that can possibly protect against heart attacks or strokes among other things however like most things when it comes to your diet moderation is key oh no no no I'm driving about two glasses a day for men and one for
women is the optimum amount to drink for your health will drink to that number six a gluten-free diet is better for anyone myth clues a vague term it's it's something that's used to categorize things that are bad you know calories that's a gluten gluten is a rather new buzzword in the mainstream but boy has a gained steam fast gluten intolerance is described as the fastest growing food intolerance category selling over ten and a half
billion in the u.s. in 2013 and only growing since then and while those suffering from celiac disease are unable to digest gluten only about 1% of the population suffers from it and therefore should follow a gluten-free diet and your body responds in a lot of ways to it stomach pains swollen lymph nodes skin rashes a whole host of things that will progressively get worse as you keep having to gluten in your diet doctors
recommend that anyone without this condition can and should include whole grains in their balanced diet for help with digestion lower blood pressure and cholesterol maintaining a healthy body weight and more so why is it so bad well it's not in fact it's neither detrimental or essential for your health and there's very little evidence to suggest that cutting it out is the healthier choice for the average person that's the whole wheat toast please is better
than the previous bite you gluten number 5 it takes seven years to digest swallowed gum miss name something you put in your mouth but don't swallow Oh Amanda gum we've all been there one minute you're chewing some gum the next something startles you and you swallow it better hope your mom's not around to lecture you about how swallowed gum will not be digested by your system for seven years and we'll just fester in your
gut until it's finally excreted okay gross and patently untrue while gum has been described as indigestion that doesn't mean it stays in your stomach it just means that when you do pass the gum through your sister in the regular amount of time it'll be in pretty much the same shape as when you swallowed it I know what and get go mamas go but we don't suggest checking it out to be sure number four
eating turkey makes you sleepy miss Oh Monica that was the best Thanksgiving dinner ever was so good I think he killed us we were surprised about this one too considering how lethargic we are after Thanksgiving dinner every year so why do you feel tired after you stuff your face with turkey a common assertion blames tryptophan an amino acid found in many meats that's connected to the sleepytime hormone melatonin but the holiday bird actually contains less
tryptophan than a food like cheddar cheese for example so experts point to other culprits when it comes to after meal exhaustion it's probably the combo of carbs and booze that cause you to snooze whatever bring it on jelly those are my maternity pants no no these are my Thanksgiving pants number three boy stirs are an aphrodisiac miss have you ever had a wasters did you know boy stirs are an aphrodisiac well it's probably a
myth anyway the oyster has long been considered a vital food for love partly because of its vague resemblance to female sex organs and partly because the legendary lover Casanova was set to eat 50 of them each morning but there have been many studies over the years none of which has proven the oysters roll as a definitive aphrodisiac what they have found however is that oysters are so rich with zinc and amino acids that they
may increase the sex drive maybe there's something to this one after all but no matter how you eat them they're sure to enhance the romance of your Valentine's Day evening number 2 acne is caused by chocolate greasy foods etc miss people think that I told my name chuckling ba or that I don't wash my face call them pimples call them zits but whatever you call them they're an unfortunate part of life and
they often crop up at the worst possible time my chocolate my beautiful chocolate now the uninformed might blame things like chocolate or greasy foods for their facial blemishes while others might cite poor hygiene but they'd all be wrong acne is caused by bacteria excess oil or clogged pores and there's not a ton you can do about it Chocolate Rain a baby born will die before this in Chocolate Rain stress and hormones may trigger
a breakout as can some medications and there are even some studies that suggest diet can be an aggravating factor but all in all zits are a rite of passage we all must deal with amaz it get it before we unveil our top pick here are some honorable mentions today there are over 900 published studies revealing the detrimental effects of aspartame migraines are the most reported aspartame reaction like they're coming thank you contact even though artificial sweeteners
don't raise your blood sugar they may put you at greater risk for diabetes calories consumed after say 10:00 p.m. won't make you gain weight any faster than calories consumed at 6:00 p.m. research shows that what matters is how many calories you eat and not the time that you eat them the bottom line is to be aware of what you're eating margarine can vary so drastically that looking at the label to understand what is or
isn't in it will help you make informed decisions number one organic food is always healthier myth organic food is grown without synthetic pesticides fertilizers antibiotics or hormones today it accounts for more than thirty 1 billion dollars in sales a year in the United States many people think the organic label gives food some supernatural nutritional value but it actually refers to the way the farmers grow or raise their products is that USDA Organic or Oregon
Organic of Portland Organic it's just all across the board organic in many cases organic farming might encourage soil and water conservation while decreasing pollution it's also more likely to be free of preservatives and synthetic flavors now I'm on the inside looked in my list organic chicken kale salad in a lemon twist however thus far test results have gone back and forth on whether or not organic food is healthier if you want to support small
farmers and sustainable development then by all means look for an organic certification however an apple is an apple no matter how it's grown so as long as you're eating a healthy balanced diet you should be fine his name was Colin curious papers okay just quick he looks like a happy little guy runs around a lot of friends other chickens as friends putting his little wing around another one kind of like howling around I
don't know that I can speak to that level of intimate knowledge about him do you agree with our list that is so good what's your favorite food myth for more enticing top 10s published every day be sure to subscribe to watchmojo.com
See more here: http://mickleach.com/common-food-myths/
0 notes
Last Seen Blogs
divinefeminine-card
Palak- undefinite hiatus

khihi
SQUISH PATITIS

datsunbreka21
A Lonely Heart

you-are-sweeter-than-fiction
The rest is silence..

spicemnghn
fuck you, fuck you & especially fuck you