#structural dissociation
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
In 2020, 44% of users from Denmark used Tumblr daily.
Note
if it’s ok to ask a follow up question.. how can u differentiate between anp or ep or a mix of both and can a host be an ep?
Here's what Nijenhuis says from The Trinity of Trauma Volume III (p.17):
"‘Apparently normal parts’ (ANPs) primarily aim to achieve the goals of common life. ‘Fragile emotional parts’ (fragile EPs) primarily defend the basic integrity of life amid a devastating umwelt. ‘Controlling emotional parts’ (controlling EPs) primarily strive to generate and maintain a sense of personal power, of shining autonomy. To achieve their aims ANPs strive to ignore the phenomenal selves and worlds of the EPs. They strive to feel, know, and/or realize it as little as possible. In the attempt to delimit their fragility, ignoring (e.g., mentally avoiding) EPs is a form of control. Although fragile EPs feel and know themselves to be fragile, they long and strive to defend their very existence. Their defensive actions or passions involve a form of control. Stuck in the dreadful past, however, they remain more or less ignorant of the actual present in terms of the third-person’s conception of chronological time, place, and the unity the fragile EPs are a part of. Controlling EPs share this ignorance and try to ignore their fragility. They strive to control their life and their umwelt. Being prototypes, traumatized individuals can encompass both mixtures and variations of these three prototype."
To put this more simply, there can be any variation or mixture of the following:
ANP = Parts that aim to achieve the goals of daily life. They are usually avoidant or ignorant of the trauma and EP.
Fragile EP = Parts that are stuck in trauma-time. The past trauma still feels like the present for them, and they defend this perception and existence. The online community often calls them "trauma-holders."
Controlling EP = Parts that aim to aim to maintain their autonomy and power. They sometimes turn against other parts, or even people outside of the system. The online community often calls them "protectors" or "persecutors."
To help you tell the difference, ANP tend to have more higher processing while EP usually have more lower processing (see chart below):
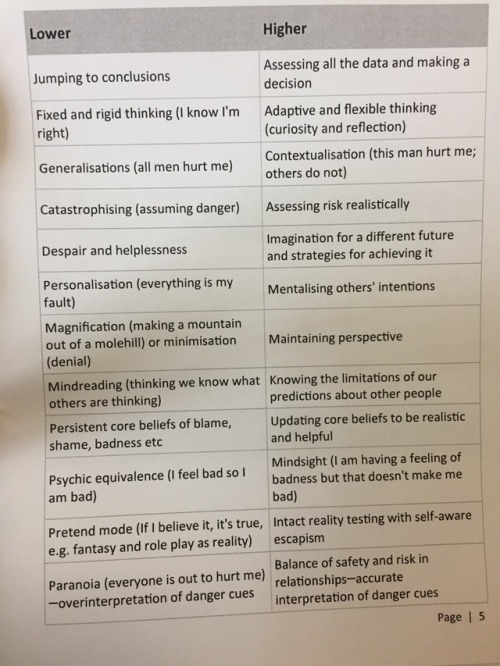
Also, yes an EP can be a host.
#mod robo#syscourse#actuallydid#actuallytraumagenic#actuallydissociative#structural dissociation#anp#ep
183 notes
·
View notes
Text

#system tag#q#osdd#otherwise specified dissociative disorder#dissociative identity disorder#pdid#partial did#partial dissociative identity disorder#osddid#plurality#multiplicity#traumagenic system#systemhood#sysblr#structural dissociation
33 notes
·
View notes
Text
A More Nuanced Discussing on Structural Dissociation and Alternatives
The structural dissociation model originated from the book The Haunted Self in 2005. (Though the authors began using the term a bit before that in the early 2000s, it's The Haunted Self that formalized what structural dissociation is.)
This model was built on some older theories for how dissociation worked but it is also distinct from those earlier theories. The structural dissociation model incorporates many of Janet's theories from a hundred years before as well as those of WWI psychologist Charles Samuel Myers.
Something that I really need to clarify right from the start is that the structural dissociation model is NOT the trauma model. It's a trauma model. One of many that have existed. The "trauma model" should be seen as an umbrella which the structural dissociation model falls under.
I want to state this here because disputing the structural dissociation model is not disputing DID being primarily traumagenic.
What causes structural dissociation?
Here is the very short version:
When someone experiences trauma, they cannot integrate the traumatic experience into their sense of self. This causes it to form an "Emotional Part" or EP which holds the traumatic experience. In basic PTSD, this part is not elaborated or significantly emancipated. (Meaning that it's not very separate.)
The part that operates the body during daily life is called an "Apparently Normal Part" or ANP. (These terms are borrowed from what Myers observed in PTSD in WWI soldiers but weren't applied to DID until the structural dissociation model.)
Children naturally have a less integrated personality since the personality solidifies later in life. For this reason, DID only arises from childhood trauma. Later life trauma cannot cause dissociative identity disorder but will result in other forms of structural dissociation.
Alters are essentially the trauma parts caused by PTSD that have become more elaborate and separated with time.
That's the basics for how structural dissociation forms under this model. On its surface, it's certainly not bad by any means.
But it's also not the only trauma model.
The Imaginary Companion Model
As an example of an alternative, at one point, many believed the pathway for the formation of alters started with them as "imaginary companions."
In The evolution of alter personality states in dissociative identity disorder (DOI: 10.1037/h0087838), it's proposed that alters originate from ICs. When the child experiences trauma, they would dissociate from that trauma and instead attribute it to the imagined companion.




I am not pointing to this model to say "this is true and the structural dissociation model isn't."
I am just using this to illustrate an alternative trauma model. And to be clear, this IS a trauma model. Despite the involvement of fantasizing in this proposal, it's not a fantasy model. The fantasy model is one that proposes memories of trauma are created through fantasy, and never actually happened. (Also, "fantasy" in a psychological context simply means imagining. It does not necessarily mean that it's something that was wanted.)
Structural Dissociation Model vs Imaginary Companion Model of Development
Here's the basic pathway for each for comparison.
Structural Dissociation Model: A child suffers trauma and creates an EP -> The child continues to suffer trauma causing the EP to be activated more often -> Over time, this EP becomes elaborated and develops into a full alter.
Imaginary Companion Model: A child creates an imaginary companion and defers aspects of the trauma onto the imaginary companion -> The imaginary companion begins taking over to deal with stressful situations -> The imaginary companion becomes a full alter.
The differences between the two models are actually pretty subtle. But the biggest difference is that an imaginary companion is going to start out with a greater degree of elaboration, likely with their own names, genders and histories, while the EP under structural dissociation would develop those things later in life.
Which developmental model is true?
Honestly, maybe both. 🤷♀️
I've listened to enough DID systems who have described experiences that could work for both models. Perhaps both have truth to them. In which case, neither is wrong. They're both just incomplete.
Some DID systems may develop according to the structural dissociation model. Some may develop according to the imaginary companion model. And some may develop due to a combination of both, with different alters developing from different mechanisms.
The DSM-5 discusses how alters in childhood can present as either independent imaginary companions or personified "mood states."

Perhaps the personified mood states are cases that followed the structural dissociation path, and the imaginary companions are generally ones that follow the other path.
The problem is that any claims for what causes early development of alters are extremely hard if not impossible to truly test.
What are the Implications of Structural Dissociation on Non-Disordered Systems?
There are none.
Whatever your opinion on it, the structural dissociation model pertains only to dissociation caused by trauma and is useless outside of that very specific context. The creators of the model have acknowledged that it's possible for self-conscious dissociated parts of the personality to develop without trauma.

The intention of the structural dissociation model isn't to somehow claim that no other type of plurality exists. Any attempt at using the model this way is taking it wildly out of the context it was written in.
The structural dissociation model is not against the existence of endogenic systems.
Primary, Secondary and Tertiary Dissociation... What Are They and Are They Useful?
These are the three levels of dissociation presented in the Haunted Self.




These levels of dissociation are where you really start to see the holes in the model.
A lot of the claims that are being made here are unproven, and difficult to test.
Basic PTSD is placed in the primary dissociation category because it only has one emotional part. But can this be proven? If parts aren't elaborated then are we able to really show that only one part is present?
What if a soldier in a war has PTSD from different traumas? Would they have the same emotional part for being forced to kill an enemy combatant that they would for being sexually assaulted by people that they serve with? I would think probably not.
These are two separate traumas that would most likely invoke different trauma responses. So if they had multiple emotional parts due to multiple traumas, would this be primary or secondary dissociation?
And since the creators of the model have acknowledged that there may be self-conscious dissociative parts formed from other means, what happens if somebody who already had secondary dissociation intentionally used one of these practices to create a headmate? Then that headmate starts regularly fronting and sharing responsibilities in the daily life? By the definitions given, this would now rise to the level of tertiary dissociation. But the dissociation became more complex for reasons other than trauma. (Although trauma was already present before.) And a trauma disorder becoming more complex for non-trauma reasons feels wrong.
I could go on and on because there are so many issues with how this model presents these levels of dissociation.
Some headmates don't hold trauma but don't front like ANPs, making them neither ANPs nor EPs. Some ANPs also hold trauma making them both ANP and EP. Some headmates can evolve from EPs into ANPs.
On the other hand, the vast complexity of dissociation is something the authors acknowledged.
Before the text that I quoted, the authors actually say that these levels are only meant to be a prototype. They acknowledge that it's not perfect and expect people to build onto it.

So the biggest problem with the levels of dissociation might not be from the authors themselves. Rather, it would be from people who treat the levels of dissociation as gospel when this is not how they were originally intended to be treated. They were always a prototype that the authors knew were incomplete when they wrote the book.
So, are these levels Still Useful as a Prototype?
Personally, I'm still going to say that I don't really like them. I don't think that the levels of dissociation are really something that are workable. I don't think that you can judge how severe dissociation is based purely on the number of ANPs and EPs present in a system.
I dislike the levels of dissociation as a concept. The problem with prototypes is that sometimes you find that you just can't build them into anything that's actually useful in practice. This might be controversial, but I think that this is one of those cases.
I don't think that looking at the numbers of EPs and ANPs is something that would help clinicians know how to treat somebody's disorder.
Even if you put in the work to account for the cases that I mentioned earlier, I think that you would be overcomplicating things to force the levels of dissociation work instead of accepting that they are a flawed concept at their very core, whitling away at a round peg to try to fit it into a square hole.
Wrap-up: What do I like about the Structural Dissociation Model? What do I not like?
I think the basic premise, that many DID alters originate from the same traumatized parts that are typical in PTSD cases, is actually a pretty novel approach that ties a lot of these disorders together. This is the part of the theory I do like, even if I don't think it's applicable in every case.
I do think many of the claims are hard to prove though. To the point that people have provided evidence that this is the correct model, a lot of that evidence could apply to any variation of the trauma model. A brain scan can show a difference between an alter with trauma and one without, but it can't prove if the trauma holder began from a PTSD EP or if it began as an already-existing imagined companion who the trauma was later deferred to.
Additionally, as I said, I strongly dislike the levels of dissociation and don't find them useful.
Should the Imaginary Companion Model be Revisited?
As far as I can tell, interest in the imaginary companion model fizzled out after the structural dissociation model was established.
I strongly suspect part of the reason for this is the politics of the "memory wars." During the 90s, there was a strong backlash against the trauma model, driven by a group called the False Memory Syndrome Foundation which claimed that memories of abuse were all fake and formed by an unproven syndrome they invented, called false memory syndrome.
The structural dissociation model was developed right after this backlash in the early 2000s. It's hard to think that the rush to adopt it wasn't driven at least in part by a desire to cut any ties with theories that involved fantasy at all, even if those theories were still trauma-based models.
Perhaps in a world where the "memory wars" never happened, the imaginary companion model would be more prominent. The hard swing towards structural dissociation as the only explanation, I think, should be seen less as an example of following the science and more as a direct reaction to the politics of the memory wars.
And I think it's a shame that these links have been severed because some cool things have happened in the realm of psychological research into imaginary companions in the years since. In the early 2000s, around the same time that the structural dissociation model was being created, imaginary companions started getting more attention.
We've now seen numerous studies demonstrating autonomy in about a third to two thirds of imaginary companions. Studies into tulpas, which are seen as being created though similar mechanisms to these complex ICs, started in the last decade.
It's possible that many ICs in children may already have a degree of elaboration and emancipation without trauma being present at all. If so, this could completely turn the projected development of DID on its head completely in these cases. Instead of an alter beginning from a traumatizing experience and becoming elaborated and emancipated later, it could already be elaborated and emancipated and later adopt the traumatizing memories.
To be clear, I am am not suggesting this as an opposing or competing model to the development course seen under the structural dissociation, but a complimentary one. An addition to it that explains some experiences of DID systems that the structural dissociation model doesn't, to help build a more complete model of dissociation.
#syscourse#psychology#psychiatry#systempunk#syspunk#pro endogenic#pro endo#science#systems#dissociation#structural dissociation#plural#plurality#multiplicity#system#actually plural#actually a system#sysblr#system things
37 notes
·
View notes
Note
tysm for answering my last q c: im sry if this is indelicate or tactless, but how does it work for you? can you/do you and your alters communicate with each other? or is it just like.. a feeling?
Good question
I’ll be honest and say it’s hard to tell the difference between self talk and self soothing with other alters talking. I’m diagnosed with OCD so I have quite a lot of intrusive thoughts and it feels like that tbh. If I was having an intrusive thought about violence I can’t control it or get rid of it, it feels like my personal thoughts but it’s just my brain flashing ideas to piss me off. With alters it works similarly just usually not distressing intrusive thoughts, instead thoughts that I don’t agree with or things I wouldn’t think of that I can’t shut up.
A good example could be the best communication I have with a frequent supportive ANP, his name is Pav. I tend to catastrophize and over work myself, because of that my brain triggers his part to show up, he recites calming things to help me. He forces the body to breathe slower and for me to lay down, sometimes he makes me rub my arms or ground myself. “Communicating” isnt mostly us talking in our head because my thoughts are rapid and hard to interpret, but feeling his emotions and physical actions is how we mostly talk. Because our amnesia is low with each other he leaves notes and I leave him notes back. But yeah it’s mostly physical and emotional then actually talking.
For me when there’s a lot of communication it usually means I’m going to switch out, with Pav if he’s there, he will soothe me then switch out so when I front again I’m not distressed.
In a negative example, alter communication can be fronting and forcefully thinking of trauma and trauma reenactment. I can tell the difference between that and intrusive thoughts because I can feel the weight of an alter attached to it. There’s intention and the thoughts feel more like a story being read to me and not a intrusive flash.
I regained this memory but when we where a little child and people where hurting us, alter communication is what kept us going. Because I grew up religious I thought angels where talking to me and forcing me to eat, sleep, shower, and breathe. I’d always talk to my family about those “angels” but really they where just parts of me communicating and soothing my body for survival. For little me communication was mostly through prayer sessions where I would dissociate asking for their help. Now I know that was Alters but a lot of times communication can be covert.
The biggest difference is it feels passionate and overwhelming when alters are communicating some sort of memory, emotion, physical behaviour, or idea- it takes over my entire body’s attention and dissociates me out of reality.
That’s my personal experience, others may have it differently but thank you
#thank you#did system#did osdd#osdd system#structural dissociation#this isn’t diagnosis material#self talk and self soothing is common in traumatic disorders#or just as a coping mechanism#my experience#I like this question
36 notes
·
View notes
Text
27.07.24
Today we realised the reason we never felt like grounding works, is our dissociative brain. We can function while being very detached, dissociated.. so we can answer the questions people use to ground us, but be completely disconnected from anything we’re experiencing. We’re not present. We’re not grounded. We’re just surviving, complying. We don’t often know what’s going on in our system. We don’t know the right words. If it’s a part of dissociation or a switch to someone who is just very detached but either way. It’s the same result.
For the longest time we felt like we were doing something wrong. We didn’t understand why grounding didn’t work. It just felt like a distraction at best. But we also didn’t have the space to be able to speak about it, so we didn’t even really think about it. Now we have a counsellor that we know will try to adapt anything that doesn’t work for us, so we were able to really figure out what was wrong. Hopefully we can find ways to make it work & practice not just going into this detached/dissociated state when we’re suppose to be grounding. Maybe it’ll help move forward in the trauma work to finally be able to ground. We’ll see.
#did#dissociative identity disorder#osdd#osddid#otherwise specified dissociative disorder#structural dissociation#did system#osdd system#emdr#complex post traumatic stress disorder
40 notes
·
View notes
Text
Why are there so many people against the theory of structural dissociation? Like I’ve seen people saying it’s ableist. I personally feel that it matches my experience with DID for the most part so I don’t get that.
-🌌
25 notes
·
View notes
Text
Excuse me, my inner child is in an absolute rage and throwing things again...
#children#cptsdsurvivor#dysfunctional family#dysfunctional parents#ex fundamentalist#religious trauma#narcissist parents#bad parenting#actually autism#ex christian#ex fundie#stress#structural dissociation#adhd#inner child healing#inner child#my inner demons#inner life#not physically#overly emotional#emotional regulation#did#ifs#internal family systems#intergenerational trauma
92 notes
·
View notes
Text
The Continuum of Dissociation
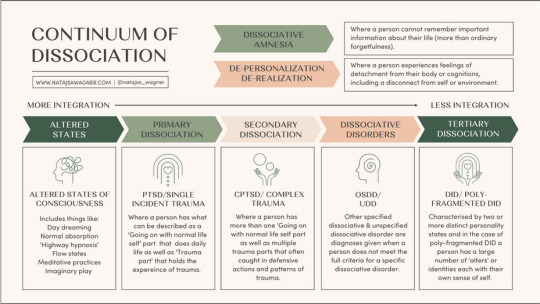
[Image description:
An infographic describing the continuum of dissociation and the theory of structural dissociation. From left to right (more integrated parts to less integrated parts), are:
Altered states - Altered states of consciousness: Includes things like daydreaming, normal absorption, 'highway hypnosis', flow states, meditative practices, and imaginary play
Primary dissociation - PTSD / single incident trauma: Where a person has what can be described as a 'Going on with normal life' part that does daily life, as well as a 'Trauma part' that holds the experience of trauma
Secondary dissociation - C-PTSD / complex trauma: Where a person has more than one 'Going on with normal life' part as well as multiple trauma parts that often are caught in defensive actions and patterns of trauma
Dissociative disorders - OSDD / UDD: Other specified and unspecified dissociative disorders are diagnoses given when a person does not meet the full criteria for a specific dissociative disorder
Tertiary dissociation - DID / polyfragmented DID: Characterised by two or more distinct personality states, and in the case of polyfragmented DID, a person has a large number of 'alters' or identities, each with their own sense of self
Outside of the parts model, but still within dissociation, are:
Dissociative amnesia: Where a person cannot remember important information about their life (more than ordinary forgetfulness)
Depersonalisation & derealisation: Where a person experiences feelings of detachment from their body or cognitions, including a disconnect from their self or environment
End image description]
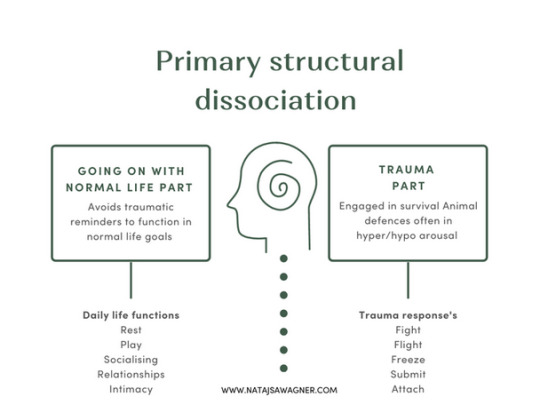
[Image description:
An infographic describing primary structural dissociation.
In primary structural dissociation, there is a 'Going on with normal life part', which avoids traumatic reminders to function in normal life goals. Daily life functions include rest, play, socialising, relationships, and intimacy.
There is also a trauma part, which is engaged in survival / animal defences and is often in hyper- or hypoarousal. Trauma responses (defences) are: fight, flight, freeze, submit, and attach.
End image description]
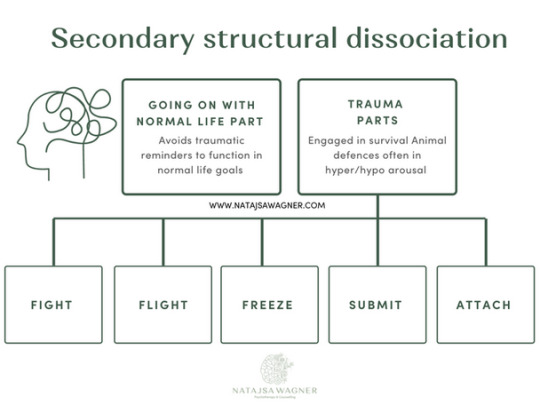
[Image description:
An infographic describing secondary structural dissociation.
In secondary structural dissociation, there is a 'Going on with normal life part', which avoids traumatic reminders to function in normal life goals.
There are also multiple trauma parts, which are engaged in survival / animal defences and is often in hyper- or hypoarousal. Trauma responses (defences) are: fight, flight, freeze, submit, and attach.
End image description]

[Image description:
An infographic describing tertiary structural dissociation. It gives an example of a system, the collection of all alters (parts) within a person.
In tertiary structural dissociation, there are multiple 'Going on with normal life parts', one or more of which may be called the 'host(s)', who are engaged in daily life. Examples of going on with normal life parts are a worker alter, a caregiver alter, and a partner alter.
There are also multiple trauma parts, which are alters engaged in survival defences. Examples of trauma parts are a gatekeeper alter (who decides who fronts), fight alters (e.g. Ann, a 24 year old primar protector part, and Don, a 30 year old persecutor part), flight alters (e.g. Sally, an 8 year old trauma holder), freeze alters (e.g. Marcus, a 10 year old trauma holder), submit alters (e.g. Pia, an 18 year old trauma holder), and attach alters (may be called 'littles', e.g. Lily, a 4 year old and Jack, a 6 year old, both trauma holders).
End image description]
- Natasja Wagner
#actually now that i read the 1st its kinda shitty. starts off good but when it gets to OSDD & DID it loses it - where are the DLP & TPs?#wheres the text explaining that DPDR and DA arent part of the ToSD but still dissociative disorders (which i added in the description)?#maybe i'll make a better one.#actually all of these are shit. lol#described#described in post#structural dissociation#dissociative identity disorder#primary dissociation#secondary dissociation#tertiary dissociation#altered states of consciousness#dissociation#theory of structural dissociation#dogpost
109 notes
·
View notes
Text
having dissociated emotional parts is a pain in the ass. like i’ll be fine and then something small triggers me and now there’s a teenager piloting me and i have to try to talk her down when i. don’t. have. time. for. this.
2 notes
·
View notes
Note
Hey! So I don't really know a whole lot about endogenic stuff, I mainly stay on the traumagenic side of plural discussion, but I wanted to bring this claim to you to see if it can be debunked since I've seen a lot of anti-endo folk use it
Claim: Plurality can only be formed by trauma because everybody is born with multiple parts, these parts hold functions like eating, sleeping, sadness, etc, but as we grow, these parts form into one identity. But when trauma happens these parts cannot form together and this create amnesiac barriers between said parts, soon once the person grows these locked up parts will form into multiple identities because of the amnesiac barriers between them.
I had a longer reply written up but Tumblr ate it.
Then again, this doesn't really need a long reply.
The model you're referring to is structural dissociation. This was a theory put forth to explain how trauma could cause DID and other dissociative disorders. But it's never presented as an explanation for all dissociation or plurality.
This model was first introduced and explained in The Haunted Self, written by Ellert R. S. Nijenhuis, Onno van der Hart and Kathy Steele in 2005. The first two of which also wrote this paper discussing their definition of dissociation that mentioned that there could be other ways "dissociative parts of the personality" containing self-consciousness could form.

There are lots of sources showing support from psychiatrists for endogenic plurality, but this one pretty solidly debunks the idea that all plurality involves trauma according to the theory of structural dissociation when even the theory's own creators are saying there may be other causes outside of trauma.
#syscourse#pro endogenic#pro endo#pluralgang#psychiatry#psychology#system stuff#sysblr#plurality#structural dissociation#dissociation#plural#multiplicity#endogenic#systems#system#actually plural#actually a system
37 notes
·
View notes
Text
10.11.24
I don’t know why but sometimes realising we have been dissociated & don’t remember things that have happened, is really upsetting. Even though it’s such a regular occurrence, we’ve always written it off as ‘not paying attention’. Joked about our poor memory. Thought it was probably just normal. But ever so often we get incredibly anxious & unsettled when we realise we can’t actually remember something important that happened. It feels scary. We end up wondering what else we don’t remember. It feels like a failure, especially if it happens in therapy. It’s like.. we were trying so hard to stay grounded but we ended up dissociated enough to not remember. Idk. It sucks.
#did#dissociative identity disorder#osdd#osddid#otherwise specified dissociative disorder#structural dissociation#did system#osdd system
8 notes
·
View notes
Text
🗝️🏷️ discussion of dissociation and formation of CDDs
We do like to periodically announce that we still operate on a multiplicity model of DID. That means we believe a lot of structural dissociation, but with some differences.
Where we do understand young children as having states, we don’t define them as being parts. It isn’t six puzzle pieces, but six blueprints of the brain. Each functions differently with what’s already there, and none of them literally occupy a place.
Dissociation keeps these states separate. Sometimes they get further away or have amnesia walls put up between them. They never fell into each other like singlets’ states did. Now these states become alters, and their abilities vary by their system’s features.
These features inform the growth of each alter as an individual. Alters with access to internal experiences can elaborate without external input in directions not possible for alters who go dormant outside of front. Alters without co-consciousness have to gain skill sets independently.
There is no right way to be an alter. Some systems view their alters as parts of a whole. Some want to fuse into one state. Others believe that sharing memories and information is necessary for their healing.
All of those things can be good and right for that system. We tend to pull out the ‘secret third option’. We believe any alter in our system is a full person if they say they are, and that our distinct ways of using the brain are no less than a singlet.
Because we view each other as largely already whole, we don’t integrate between ourselves. We have worked on communication and bringing other insiders up to date, but we don’t utilize one another’s lived experiences.
Our third option is community, which we get to define for ourselves. Many of us struggle with demands and authority, so we don’t make progress with prescribed goals. If the two roads to choose from are melting our grains of sand into one final glass or getting so close as to be a mosaic, we’ll pave our own path.
And it’s working for us so far. We haven’t found any literature that stopped us in our tracks, haven’t hit a wall in our journey. So this is good for us.
Our name is an extended metaphor for our DID. It’s an understanding that we are not less than or part of, but one step in a turning cycle. Rocks grow and break, glass forms and shatters, and neither stays small forever. The smallest granules of sand make up a desert, and even those tiny bits can shape stones.
It’s okay to have a different perspective than we have evidence for. Science is an ever changing thing, understanding shifting with culture and time. Your experience cannot be wrong, even if we don’t see it right now. You are living proof, and that is enough.
#did osdd#dissociative identity disorder#traumagenic system#osddid#did system#polyfragmented system#cdid#hc did#structural dissociation#multiplicity#plurality#functional multiplicity#final fusion#secret third option
42 notes
·
View notes
Text
youtube
A podcast on understanding the Structural Dissociation Model with Kathy Steele, one of the experts behind the model itself. Very interesting information on structural dissociation, complex trauma, and complex dissociative disorders. Please give it a listen!
#actuallydid#actuallydissociative#actuallytraumagenic#dissociative identity disorder#actuallycdd#dissociation#structural dissociation#complex trauma#kathy steele#Youtube
48 notes
·
View notes
Text
Rereading one of my favorite books on structural dissociation this morning: Healing the Fragmented Selves of Trauma Survivors by Janina Fisher. I had the privilege of taking a training from her and talking to her about my own structural dissociation and she recommended I read the book and she was so right. It's fantastic for people who struggle with trauma and trauma-related diagnoses or are struggling to make progress in therapy.
#complex ptsd#borderline personality disorder#actually bpd#ptsd#janina fisher#structural dissociation#complex post traumatic stress disorder#trauma survivor
4 notes
·
View notes
Text
Poem: If all I am is me, what is that exactly?
I am...
I am worried, scared, and scarred.
I am more than meets the eyes.
I am nebulous; unending with a border of soft edges to void where all colours mix to a boiling tar black.
It is.
It is cold steel shifting pistons and gears.
It is judge, jury, and parent from behind one way glass.
It is what snatches gives and shifts my emotions upholding old notions only emotionally believed.
My child.
My child is all I cannot be.
My child is burdened and free.
My child feels all but knows nothing from their cage guarded by It that toys with puppets as a self-imposed parent.
I am.
I am all.
I am none.
I am to be made.
I am already gone.
We are a mess, We'll never clean up,
We try address, we will give up,
We push and press, we give nought up...
But I? I, a proposed adult. What am I to do?
Turn belligerent incessent paining chaos into..?
Something tangible uniform and new.
A sleuth again here to find what's true!
But I do not understand,
and I do not think I will.
Regardless of where I stand,
and for how long I may drill.
No matter the lending hand,
And reading holes yet to fill,
I do not think I will
I do not think I will
...
I think, I will think. I will.
I will. I will to think. I think!
For else I sink A pebble in ocean,
Gown of bubbles A king of a notion,
Lying in home A thing lacking motion:
I have quest that deserves my devotion,
To reclaim what's mine, every emotion!
So therapy.. it's good for you... not saying it's requried or salvation, and heck it's 90% your work... but having another hand, one you can... well at least more respect than your peers, is useful... for me anyway.
Mind you, they brougbt up froidioan stuff... I get why they did, the ego and the id (or however you spell it) does have overlaps with the parent child and adult dynamic... one that further personifies these categories of psyche's pressures into something so similar to these emotional manifestations of beings?
Personfying them feels wrong, like giving them power, after all perhaps it's just me, my echoes twisted and contorted and thrown back at me.
The implicit systemic emotionally written notions that seethe through my blood are the fault of my own poison I've left populating me.
There is no one else to take onus, I am the resident adult in the head... so even so, even if I feel unnatural, feel like my canvas is the same but my emotional paints are all diffrent... my child may be... alive... I don't know what switching is like... but I'm too unfamiliar to tell, twice a year 30 odd seconds before "No no no, not what you're ought to be".
At this rate this rant is as much apart of the poem.
I suppose, I need help... I work so hard, and always alone, because I know the people who surround me would fail... fail before even starting. At least I like puzzles, engimas, riddles... I suppose another me would be nice... I don't need to wish for them in my head though... no offence intended to anyone ever.
#original poem#poem#poetry#original writing#spilled poetry#depersonalization#tw#poets on tumblr#spilled writing#poetry community#structural dissociation#dissociative identity disorder#tw emotional distress#dark academia
2 notes
·
View notes
Text

[Image: 18-piece background, alternating between blue & orange with a picture of a young degu in the middle.
Top text reads: “Never had a core and personality”
Bottom text reads: “Lots of hardcore personalities.]
#dissociative memes#dissociativedegu#dissociation memes#advice animals#whynot dissociativedegu#did memes#osdd memes#dissociative degu#actually did#system problems#did problems#core personality#actually traumagenic#structural dissociation#sdotp#sdop#structural dissociation of the personality#a splitting of the mind#did splitting#other specified dissociative disorder#osdd 1b#dissociative identity disorder#we all the real one
20 notes
·
View notes