#paraparesis
Text

Al Emadi hospital provides the most excellent physiotherapy in Qatar. We have an experienced team of physiotherapists dedicated to facilitating fast recovery for patients experiencing mobility issues. Our hospital offers rehabilitation treatments for patients affected by a sports injury, arthritic conditions like osteoarthritis, rheumatoid arthritis, etc., various spine conditions like cervical, dorsal, or low back problems, spinal stenosis, and several neurological conditions like paraparesis, paraplegia, hemiplegia, multiple sclerosis, carpel, and tunnel syndromes, etc., and lymphoedema. Our physiotherapy treatment includes various physical modalities like the hot moist pack and cold pack application, electrical therapy, shock wave therapy, etc., and rehabilitation modalities like therapeutic exercise programs, lymphatic drainage, pressotherapy, Huber 360, etc.
#physicaltherapy#physiotherapist#physiotherapy treatment#sports injury#arthritic condition#osteoarthritis#rheumatoid arthritis#cervical#dorsal#low back pain treatment houston#spinal stenoises#neurologicalhealth#paraparesis#paraplegia#hemiplegia#multiple sclerosis
0 notes
Text
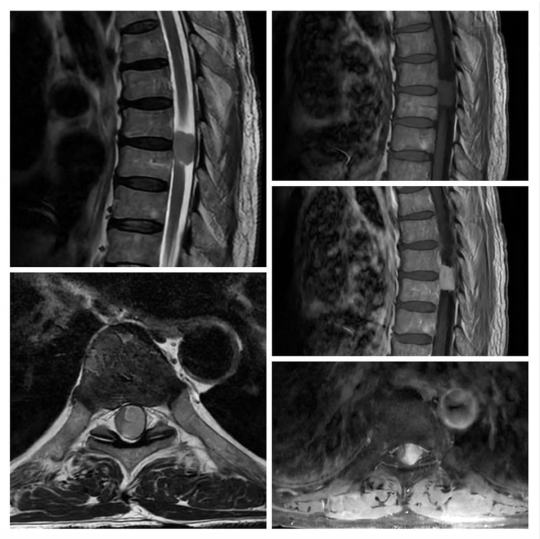
Ky eshte nje rast i nje pacienti 70 vjec pas semundje te meparshme qe paraqitet me parapareze. Ne MRI shihet nje lezion intradural ekstramedular i cili eshte meningeome, nuk prek apo te shtrieht ne rrenjet e nervave cka e diferencon nga shvanoma. Medula spinale eshte e zhvendosur djathtas.
0 notes
Text
AllGirlMassage Aspen Rae and Reena Sky Grind Together
Amigo fudendo a bucetinha da Sramidia
Wife screwing boy gay porn The BukkakeBoys couldnt wait to slam their
Novinhas com a bucetinha querendo rola
A real amateur japanese woman2, First time in a porno!
Fucking my college roommate
Japanese Girl Big Natural Tits and Splits
Live stream from my facebook, bikini marquee (marquinha de biquine)
German teen girls tight pussy gets fucked in the kitchen
Jav Schoolgirl Babe Koharu Fucks Old Guy One Of Her First Hardcore Scenes Real Babe
#imploringness#elegized#antistalling#pentahedral#conditory#paleoichthyology#accentually#table-shaped#CRAS#mink#treblet#acanthomas#entoproct#spider-catcher#carless#overemulation#snobdom#ein#paraparesis#ronaldo
0 notes
Text
🦢 'Join The Art of Living'
*"New Year Special Happiness Program"*
Learn
Most Powerful Breathing Technique
*Sudarshan Kriya*
✨
🗓️ *28th November to 2nd December 2023*
With Young and Dynamic Rajkot AOL Senior Faculties
💫
*Benefits of Program* :
🤠 Relieves stress, anxiety & depression
⚡️ Boosts immunity & health
😎 Helps control your mind
🤓 Raises clarity of mind
💤 Improves quality of sleep
👫 Happier relationships
Register @
*Morning Batch:*
⏰ 6 am - 8:30 am
*https://aolt.in/743634*
*Evening Batch:*
⏰ 6 pm - 8:30 pm
*http://aolt.in/745884*
Venue:- *Sneh Nirzar Hall*, Opp BT Savani Hospital, University road, Rajkot.
😊Happy to Help:
9033762190
98258 30206
9099526928
9427709523
Untitled
View On WordPress
#aerobics#Artofliving#DrHemangJani Rajkot Physiotherapist Paraparesis NeurologicalCondition ParaparesisAwareness MobilityIssues NeuroRehabilitation Parap#happy happiness happytime happyness happysunday happyfriday happyday happyeaster strength yogastrength aerobics puja yogaeveryd
0 notes
Text

Karolina Hamer
Gender: Female
Sexuality: Bisexual
DOB: 12 February 1981
Ethnicity: White - Polish
Occupation: Paralympic swimmer, disability rights activist
Note 1: In 2018 she publicly came out as bisexual becoming the first active Polish sportswoman to do so.
Note 2: Has Paraparesis
#Karolina Hamer#bisexuality#lgbt#lgbt rights#disability rights#female#bisexual#1981#white#polish#olympian#paralympian#athlete#swimming#swimmer#activist#first#disabled
56 notes
·
View notes
Text
Retroviruses got me fucked up
@moosemonstrous are u ready for a dissertation? I hope so.
people who followed me for art I'm so sorry
ALRIGHT so we're gonna cover a couple areas.
General information about retroviruses.
Details about The Corruption and theories about how it works inside the body.
SPECIFICALLY ROBBIES viral weird shit. Cause what he has going on is even more fucked up than normal fucked up. Fucked up squared.
Me ranting about skin necrosis and why I shouldn't have just. Thown it in there because I thought it would look fucky wucky.
GENERAL INFORMATION ABOUT RETROVIRUSES:
As most people know, a virus is a cell that enters the body of a host and alters its DNA to turn that hosts cells into virus making factories. This is what allows viruses to duplicate and spread through the body so quickly. But whats that? 'What makes retroviruses different from other viruses?' I hear you asking? WELL EXCELLENT QUESTION THATS A PERFECT PLACE TO START. A retrovirus is different because its method of self duplication involves an enzyme called reverse transcriptase. This makes retroviral infection PERMANENT. Even if the virus is defeated by the immune system, those changes stick around. The phrasing used was 'ipso facto mutagenic' meaning 'by the fact itself/inevitable'.
...Which is kinda metal honestly I want it on a tee shirt (definetly not thinking of Amadeus saying that to Robbie as he tries his best to explain theres no way to undo whats going on with him. nahhhh angst don't got a hold on me like that [<- vibrating])
'Ohhh but if those genetic changes never go away, doesn't that mean that those viruses will get passed on through peoples children?' ASKING SUCH GOOD QUESTIONS TODAY MY MUTUAL BECAUSE THE ANSWER IS YES. Once a retrovirus codes itself into a hosts gnome, its called a provirus (pro gamer move right there) Fun (not fun) fact around 8% of the human gnome is made of proviruses. These are called endogenous viruses, and for the most part they just kinda sit there and stay dormant. TERRIFYINGLY, other viral infections can trigger these endogenous viruses out of dormancy. As for what actually causes a provirus to go dormant uhhhhhhhh I dunno. Couldn't find an answer in my research someone make me look stupid with an answer please because I wanna know.
Ok now lets talk about the immune system a little bit. There are a few different kind of cells at work (hehehehehe) that help to fight viruses and other infections in the body. The first are Cytotoxic T cells or Killer T Cells. These are the cells that directly destroy cells displaying genetic patterns they recognize as bad. Next we have CD+4 Cells (Helper T Cells) which act as a library that stores information about how to identify an infected cell, and shares that information with other Killer T cells once one figures it out. Then there are the Regulatory T cells which suppress your immune responses to maintain homeostasis. They're what (USUALLY) stops your immune system from killing you while trying to clear a virus. Last there are Macrophage. CELLS AT WORK MAID MILFS- I mean cells that clear the debris that remain after the Killer T Cells are done destroying them.
Retroviruses have two primary ways of either side-stepping the immune system or just. Overwhelming it completely. Acutely transforming retroviruses do just that. They reproduce too quickly for Killer T cells to destroy them all and exhaust the system. The second type are called Non Acute Retroviruses. They camouflage viral particles as immune cells to suppress the immune system. For example, HLTV-1 is a retrovirus that disguises itself as a Regulatory T cell to artificially suppress the immune response thats trying to kill it.
HTLV-1 is really interesting because most of the time patients are asymptomatic, but 5% can graduate to HTLV-1 associated myelopathy/tropical spastic paraparesis, which affects the spinal cord and white matter of the central nervous system. This usually results in the weakening of lower extremities and sometimes total bowl/bladder control loss. It suckkssssss (but is also a retrovirus that affects the central nervous system so were circling back to it later 👀).
SPECULATION ABOUT THE CORRUPTION:
I've said previously that The Corruption has potential for a retrovirus that affects the central nervous system by degrading the brains ability to regulate muscular contraction, while also pumping out a ton of cortisol and adrenaline to encourage 'hysterical strength'.
Now I did a little more research about Hypoglycemia and combined with the nerve damage people would likely die from cardiac arrhythmia, which is a life threatening kind of ventricular fibrillation. Long and short, it means their hearts don't have the proper energy and stimulation to keep beating properly, so they stop beating in sync. This results in insufficient blood flow to vital areas like the brain, and combined with the inadequate blood sugar, this would result in very fast brain death.
Let's talk about the immune systems response to this Corruption retrovirus. We would most likely see lots of inflammation, and with the main focus being on nerve cell this would probably result in meningitis, which is inflammation of the tissue surrounding the brain and spinal cord. If left untreated this could result in a coma and then death. So we're seeing a SHIT ton of pressure on the brain and central nervous system. Which is like. VERY BAD for a person. We're talking brain death very very fast.
As for how the virus would target the nervous system directly we could look to real world examples like rabies (ahhhh rabies. can never get away from you). The virus would attach to nicotinic acetylcholine receptors, which are what turns chemical signals into electrical signals in your nerves. It would then spread through the axons of the central nervous system and eventually reach the brain. We could also pull a rabies with 'once you see symptoms it's too late' which I, personally, find fucking terrifying.
In terms of the virus losing its effectiveness once outside the body of a Demon/Kaiju we would likely need to look at the anatomy of a retrovirus itself. The outermost area is composed of envelope spikes, which tell the cell to let it in. After that is an envelope protein which plays an important role in complete virus particle (virion) assembly. Theres then a protein shell that contains reverse transcriptase and the RNA gnome that it will use to recode a host cell. If this virus evolved to survive in an environment that is always warm (hell. lol. lmao.) it might not be prepared to deal with these colder temperatures in our world. This could result in damage to the protective protein barriers and cause damage to the real important parts, the RNA and reverse transcriptase. This would mean that the virus would not be near as effective as a fully intact retrovirus cell.
The Corruption could be an endogenous virus thats embedded into the Demon/Kaiju gnome that wouldn't affect them, but would absolutely affect us because we haven't seen them before.
ROBBIES WEIRD FUCKSHIT:
alright guys this is where we put the FI into SCIFI cause your about to read a whole lot of nonsense sentences.
Robbie. Robbie is fucking WEIRD in EVERY universe and this shit is absolutely not different. Him being exposed to that previously mentioned damaged version of the virus from a young age might not give him true immunity but it would give him SOMETHING to work with. His immune system is at least slightly familiar with it and at this point whatever damaged version he came into contact with has already established itself as a provirus in him.
The Corruption thats established itself in The Charger is different.
Like I mentioned in my first diagram, I think there was a chemical reaction that stabilized the corrosive aspect of The Corruption, but this reaction would also have had an effect on the retroviral properties of the Demon/Kaiju material. ESPECIALLY when we add Eli into the mix.
Now, I think generally the amount of radiation that these viruses would be exposed to would kill them (if you believe viruses are alive. there is some MEGA debate going on about that). But if the corruption was just stabilized/hardened on the outside and left squishy and organic on the inside, that would successfully protect everything. And whats that organic squishyness on the inside? EXCELLENT QUESTION AGAIN. If Eli died while inside The Charger then it's not a stretch to think his DNA would have been incorporated and stored via through the natural processes of the retrovirus as a provirus. And so you end up with the genetic mixture of a horrifying creature capable of heinous acts, and a Demon/Kaiju. WITH retroviral properties. Dear god.
Robbie would get exposed to this the very first time he enters the Charger. Because of his semi-immunity + genetic relation to Eli he would likely be able to overcome the more meatsuit damaging aspects of this mixture and just get right through the genome editing without much fuss from his immune system. We would still have a certain degree of damage to his nervous system which allows for that change in strength that would occur in usual examples of the virus (maybe some added aggression from mild influence in his amygdala), but not to a deadly degree. Honestly this shit would barely classify as a virus its just. A nightmare mutagen at this point. So while some of his gnome would remain fairly the same, a good 30% to 50% is megafucked.
Changing Robbies genotype to this degree will naturally result in a change to his phenotype! For the sake of fun were gonna ignore stem cells and their weirdness (for now. I just need to stew on it a little longer and I can make up some bullshit I'm sure). The damage his muscles would experience from less regulated signals would mean they experience muscle tears and subsequent muscle growth. For usual muscle damage from exercise this takes a few days, so if we wanted to keep with that timeline it could be interesting to introduce some minorly sped up healing. That would also be fun for reactivating the growth plates in his bones to allow him to become bigger and taller overall (boring body horror my beloved @cicada-candy that term is never leaving).
THEN you can get into some of the fucky wuckier traits like tapetum lucidum and TEEF. TEEEEEEFFFF. The teeth in particular could go a few different ways. You could just have growth and development of the canines resume until they become elongated and more prominant. OR. You could replace the teeth with bony protrusions from the skull that would push out the original canines and grow in their place. Because of the time it takes for bones to heal your looking at this happening around 20 weeks out. Literally any fun trait you want to take from Demon/Kaiju could apply here.
The most important part would be the nerve bundles on his spine that would be used to bluetooth to The Charger (<- this is a nonsense sentence. I am aware of this). These would provide faster communication with the charger and (theoretically) more intuitive movement, while also allowing him to eventually controlling the charger from the outside. Please note that this would cause EXTREME STRESS to his nervous system. It would be like a person trying to flex a muscle the size of another person for the first time. LEARNING PROCESS. TAKE IT SLOW OR HAVE AN ANEURYSM.
Which leads me to the youtuber apology part of this.
WHY I SHOULDNT HAVE JUMPED TO SKIN NECROSIS:
Skin necrosis is a result of the mass death of skin cells that is furthered by the damage to blood cells. This usually results in a blackened, leathery texture to the necrosed skin. I SHOULD HAVE NEVER EVEN MENTIONED THIS.
What I SHOULD have done is said 'hmm ah yes it would make more sense for some protective covering over these nerve concentrations to either come from materials in Robbies body or to mutate into the skin of the Demon/Kaiju'. This is why we do sufficient research before getting back on our bullshit, wazz (mental note mental note mental note mental note).
I am quite partial to the idea of that stronger/thicker Demon skin/armor growing under Robbies skin and it just itches and burns until he cant ignore it anymore. And then he can pull off. Whatever skin is on the top of it. HEHHEHEHOHOHOHO DELICOUS MENTAL IMAGE of him panicking because he just wanted to scratch his back but now theres blood on his hands and skin sloughing off and dear fucking lord how did he get to this point in his life (<- I daydream about normal things guys don't worry. very average things).
ANYWAY uhhhh if you made it this far I love you. Legit. Have a cookie. Take a nap. Have a happy holidaze <3.
#Also messing with the idea of the chargers stabalized corruption spreading so it becomes more biomechanical than just mechanical#so as that information spreads it updates robbie every time he pilots the charger. then you can get fun stuff like scars showing up on him#<- where the Charger has been damaged#FUN SHIT LIKE THE CHARGER BEING ABLE TO ACTUALLY OPEN ITS FACE PLATE LIKE A MOUTH AND BITE A DEMON#bite scratch bite bite bite bite bite#I love him and so he must suffer#ghost rider pacific rim au#ghost rider#robbie reyes#speculative biology#this is two thousand words. how did i end up here
45 notes
·
View notes
Text
Took a somewhat terrifying drive down muddy roads on the mountains today, so I came home and relaxed with a hot shower and drawing. (should've been writing oops)
I finished the set! It's Fourrrrrrr

Okay first of all wheelchairs are easier to draw than I thought but still kind of difficult. I know this isn't perfect, and I definitely want to redesign it later to look more fantasy (though the structure will still be modern), but I was kinda freaking out tonight so I didn't worry too much about it this time. Look forward to a post later detailing the wheelchair a bit more :)
After his first adventure but before the second, Four got thrown around while Minish-sized and sustained a spinal cord injury that gave him paraparesis. Paresis is also called partial paralysis—Four can only sort of move his legs. Most days, he uses the wheelchair (he and the Minish 1000% tricked it out), but on good days, he has two pairs of forearm crutches to choose from! The chair folds up and gets stuck in his magic bag when he doesn't need it.
(aside: I personally enjoy the idea that each Link has an extradimensional space somewhere, in a bag or a hat or a boot. I just want them to carry things around without being overencumbered or reliant on Wild's slate.)
Four can't walk without support, but he gets around just fine. It's pretty common for him to park his wheelchair at the edge of camp and just gets down to do stuff. If they're pressed for time or he's tired, he might let someone carry him, like up the stairs to a tavern room or to a tree during an ambush so he can snipe. He doesn't have a lot of pain, just weakness and the loss of sensation.
When he shrinks down, so does the chair, because magic. However, splitting doesn't duplicate the chair. It also messes with the injury. All four of Four have paraparesis, but to very different degrees, following the trend of his personality splitting into somewhat uneven pieces. Vio gets the brunt of it, almost full paraplegia, so he sticks with the chair. Red gets it about as bad as Four has, and is generally good with the crutches. Green gets it a little better, and uses crutches too (that's why they keep two pairs around.) Blue gets the least of it and is pretty much entirely ambulatory. He feels a little guilty but takes his role as a protector seriously.
PLUS PLUS he already has fingerless gloves!
Sorry this post got so long! I have so much I want to say! Four's one of my favorites, and my own experience with disability dealt with mobility issues, so it's pretty close to my heart. With all nine introduced, I'm not sure what the next post about this AU will be, but ask box is open for questions, thoughts, and screaming. :)
388 notes
·
View notes
Text
I hate when people use non-standard abbreviations! There's a pt with low back pain and weakness, urinary and fecal incontinence. MRI doesn't show spinal cord compression, so cauda equina ruled out. Neuro recommended w/u for autoimmune demyelinating polyneuropathies and transverse myelitis. The neurologist wrote "TM" in his note, and I didn't know what he meant, so I looked it up. Anyway, I've heard of transverse myelitis, but didn't know the workup. From UpToDate:
●Definitions – Acute transverse myelitis (TM) is a neuro-inflammatory spinal cord disorder that presents with the rapid onset of weakness, sensory alterations, and/or bowel and bladder dysfunction. Idiopathic TM is defined by its occurrence without a definitive etiology despite a thorough work-up. Secondary (disease-associated) TM is most often related to a systemic inflammatory autoimmune condition.
●Causes – Idiopathic TM usually occurs as a postinfectious complication and presumably results from an autoimmune process. Alternatively, TM can be associated with infectious, systemic inflammatory, or multifocal central nervous system disease. Acquired central nervous system demyelinating disorders that can cause TM include multiple sclerosis, myelin oligodendrocyte glycoprotein (MOG) antibody disease, neuromyelitis optica spectrum disorder (NMOSD), and acute disseminated encephalomyelitis.
●Epidemiology – TM is rare, with an annual incidence of one to eight new cases per million.
●Clinical features – The onset of TM is characterized by acute or subacute development of neurologic signs and symptoms consisting of motor, sensory, and/or autonomic dysfunction. Motor symptoms include a rapidly progressing paraparesis that can involve the upper extremities, with initial flaccidity followed by spasticity. In most patients, a sensory level can be identified. Sensory symptoms include pain, dysesthesia, and paresthesia. Autonomic symptoms involve increased urinary urgency, bladder and bowel incontinence, difficulty or inability to void, incomplete evacuation and bowel constipation, and sexual dysfunction.
●Evaluation and diagnosis – The diagnosis of TM is suspected when there are acute or subacute signs and symptoms of motor, sensory and/or autonomic dysfunction that localize to one or more contiguous spinal cord segments in patients with no evidence of a compressive cord lesion. Thus, the diagnosis of TM requires exclusion of a compressive cord lesion, usually by magnetic resonance imaging (MRI), and confirmation of inflammation by either gadolinium-enhanced MRI or lumbar puncture. When inflammation is present in the absence of cord compression, then the criteria for TM have been met, and it is necessary to evaluate for the presence of infection, systemic inflammation, and the extent and sites central nervous system inflammation.
●Differential diagnosis – The main considerations in the differential diagnosis of idiopathic TM are conditions that cause other types of myelopathy (eg, compressive or noninflammatory or vascular), the various disorders that cause secondary TM, and nonmyelopathic disorders that may mimic TM (eg, Guillain-Barré syndrome).
●Treatment – For patients with acute idiopathic TM, we suggest high-dose intravenous glucocorticoid treatment (Grade 2C). Our preferred regimens are methylprednisolone (30 mg/kg up to 1000 mg daily) or dexamethasone (up to 200 mg daily for adults) for three to five days. For patients with acute TM complicated by motor impairment, we suggest additional treatment with plasma exchange (Grade 2C). Our preferred regimen is five treatments, each with exchanges of 1.1 to 1.5 plasma volumes, every other day for 10 days; alternatively, the first two plasma exchange treatments can be given on successive days, with the remaining three treatments given every other day.
●Prognosis
•Degree of recovery – Most patients with idiopathic TM have at least a partial recovery, which usually begins within one to three months and continues with exercise and rehabilitation therapy. Some degree of persistent disability is common, occurring in approximately 40 percent. A very rapid onset with complete paraplegia and spinal shock has been associated with poorer outcomes. Recovery can proceed over years.
•Risk of recurrence – The majority of patients with TM experience monophasic disease. Recurrence has been reported in approximately 25 to 33 percent of patients with idiopathic TM, although this usually signals a systemic condition. With disease-associated (secondary) TM, the recurrence rate may be as high as 70 percent.
•Risk of multiple sclerosis – Patients presenting with acute complete TM have a generally cited risk of multiple sclerosis of only 5 to 10 percent. However, for patients with partial myelitis as an initial presentation and cranial MRI abnormalities showing lesions typical for multiple sclerosis, the transition rate to multiple sclerosis over three to five years is 60 to 90 percent. In contrast, patients with acute partial myelitis who have a normal brain MRI develop multiple sclerosis at a rate of only 10 to 30 percent over a similar time period.
2 notes
·
View notes
Text
MY REFLECTION ON WHAT I LEARN ABOUT CLIENT-CENTRED PRACTICE.
In the ever-changing healthcare landscape, one principle stands out: client-centred practice. It's more than a term or a fad; it's a concept that prioritizes the individual in care, putting their autonomy, preferences, and special needs at the forefront of every decision and contact. Consider a healthcare experience in which individuals are active participants in their health journeys rather than passive care recipients. This is the essence of client-centred practice: a groundbreaking method that not only fosters trust and collaboration but also lays the framework for truly transformative and empowering healthcare experiences. In this blog, I will share my experience about how I’ve been implementing client-centred practice in my therapy intervention with clients in Mshiyeni Memorial Hospital.
I currently have an 18-year-old patient with partial-thickness burns on his face and bilateral upper limbs, he worked in a carwash and lives alone in his 1 shanty room. We have been working together for 3 weeks now. “Client-centred practice emphasizes the importance of understanding the patient's perspective and tailoring care to meet their unique needs and preferences” (Annals of Family Medicine, vol. 9, no. 2, 2011, pp. 100–103.), thus on the 1st day I saw him, we set up goals that we would like to achieve whilst in the hospital while considering his interest, concerns, and preferences. “Client-centred practice empowers patients to actively participate in decision-making regarding their health, fostering a sense of ownership and accountability” New England Journal of Medicine, vol. 366, no. 9, 2012, pp. 780–781.), thus we set goals into priorities and set steps of how they will be achieved. “In client-centred practice, the focus shifts from 'What is the matter?' to 'What matters to you?” (Social Science & Medicine, vol. 51, no. 7, 2000, pp. 1087–1110.), one of the patient’s goals was to be able to use his ULs to feed himself without the help of nurses and we first did upper limb exercises to release joint stiffness (prevention of skin contractures) before we did a modified feeding activity. The activity was a bit challenging for the client as the bandages were tightly wrapped on the limbs and there was a lot of compensation. Therefore, I had to debulk the bandages on the hand to facilitate finger movement. It was a bit challenging at first because the client was recently admitted and in excruciating pain thus had to incorporate therapeutic use of self (empathizing mode) to calm him down and show compassion. I asked for his parent's numbers so that I could update them about our progress of intervention and include decision-making such as whether he should be discharged and why or why not. Now the client’s occupational performance has improved and we’ve achieved 50% of our goals so far and that is motivating for me.

The second client I had was a 51-year-old female who presented with paraparesis and trunk pain. I first interviewed her so that I would know her background context. We set short and long-term goals with the patient while considering her interests and preferences. One of her first goals was to walk, but I explained to her that walking is a process and firstly she needs to learn how to roll on the bed and sit without falling as she has a poor static and dynamic sitting balance. Therefore, we did bed rolling (bed mobility training) and now she can take things from the side bed table. She was very happy to see such improvement because she used to call nurses every time, she needed something from the table. Secondly, we attempted our second goal of sitting at the edge of the bed, but the client set for a short time and complained about excruciating pain in the trunk. We tried this several times on different days, but it got worse daily, and this demotivated us because our goal seemed elusive. I advocated for the client to get bisacodyl to help relieve constipation as she hadn’t gone to the loo for 10 days. She was referred to Nkosi Albert Luthuli Hospital for further intervention, but I hope she will return soon so that we continue with achieving our goals.
Client-centredness is very important because it requires me to be flexible and change according to the client’s needs. I’ve learned to approach and treat people differently because they are different and have different occupational profiles as mentioned above with two patient scenarios. Even if people present with the same diagnosis their goals are never the same and that is why I highly recommend the use of this practice in the future and by other healthcare practitioners.
As I conclude I could say that by centering care around what truly matters to each individual, we not only enhance clinical outcomes but also nurture a profound sense of connection and humanity within the healthcare experience thus we should continue using this practice in everyday lives of our patients in the healthcare system.
REFERENCES.
Bechtold, A., & Fredericks, S. (2021). Key concepts in providing patient-centered care. INDIGO (University of Illinois at Chicago). https://doi.org/10.32920/ryerson.14636718.v1
Coffey, M. J. (2017). Patient-centered communication during procedures. The American Journal of Surgery, 213(6), 1188. https://doi.org/10.1016/j.amjsurg.2016.08.004
Papalois, V. E., & Theodosopoulou, M. (2018). Optimizing health literacy for improved clinical practices. Medical Information Science Reference.
Platt, F. W., Gaspar, D. L., Coulehan, J. L., Fox, L., Adler, A. J., Weston, W. W., Smith, R. C., & Stewart, M. (2001). “Tell Me about Yourself”: The Patient-Centered Interview. Annals of Internal Medicine, 134(11), 1079. https://doi.org/10.7326/0003-4819-134-11-200106050-00020
Rathert, C., Wyrwich, M. D., & Boren, S. A. (2013). Patient-Centered Care and Outcomes. Medical Care Research and Review, 70(4), 351–379. https://doi.org/10.1177/1077558712465774
0 notes
Text
Reflect on cultural humility
South Africa is a unique country, we are a nation of 55 million, with people from a plethora of backgrounds, racially, religiously, and culturally! (Matthews & Van Wyk, 2018). This astounding diversity of our rainbow nation is so important to healthcare workers; to occupational therapists especially as we look at clients holistically, this includes their routines, activities, and rituals. As OTs, our patients are so much more than their diagnosis, which means we need to take initiative and learn about the spiritual beliefs of our clients and use this to treat them without bias and judgement.
Practical’s at Prince Mshiyeni have opened my eyes to just how much I need to learn about my patients’ cultural beliefs. One of my clients this semester was a sixty-one-year-old woman who presented with weakness and paraparesis in her lower limbs. She explained that she was cursed because of jealousy over her cow. The multitude of lectures I had attended on the client factors she presented with had not prepared me to deal with this specific situation. Do I chalk this down as a probable psychosomatic case because of her lack of a diagnosis? (Professional n.d.) Is it ethical talk to the client about this? I had realized that I don’t know enough about her cultural beliefs to talk to her about it, in fact I could not talk to her at all as she did not speak a word of English, which brings me to the second part of this experience, the language barrier, my Zulu is limited to a few words that I had learnt from some Duolingo lessons I had taken in my spare time.
This situation had left me feeling embarrassed; this client had been referred to me, I had been responsible for evaluating and treating her and not only was I oblivious to her beliefs, but I could barely carry out an assessment, which makes me question the reliability of my findings. An interview was out of the question. Without the translator, I would not have known about about the history of the clients' symptoms, her home context, hobbies and who takes care of her. Even if I had understood her, with my limited knowledge on her culture, would I be able to fully grasp her context? Would I be able to understand what occupations she partakes in for her beliefs? My weaknesses in this situation were my lack of knowledge, both about the client’s background and her language. Of course, as an OT and a decent human being, I respect the diverse cultures we have here in SA, but my lack of knowledge in them leads to a decreased understanding of my clients! That is not ethical because they might not be getting treatment as efficiently as they might be if I did have the knowledge about their occupations. I could’ve just done ADL session with this client to improve client factors like balance, but now that she has told the translator that gardening is a big occupation for her, it can be included in sessions!
Looking back now and analyzing the situation, I realize that I desperately need to learn languages other than English, specifically IsiZulu, even though dialect is a common challenge in the healthcare profession, I need to make an effort and expand my knowledge and vocabulary. (Sonn & Vermeulen 2018). To prevent this from happening again I need to do more research on the traditions of South African cultures, and as silly at is does sound, I need to keep up with my Duolingo lessons! It is not extensive, but it will help me get the basics down, once I do, I can try and converse with my colleagues in IsiZulu to practice. As an OT I should not be giving sub-par treatment, I should be putting in the effort to broaden my mind and learn! (Hildebrand et al. 2012). Even if there isn’t a language barrier I should be asking more questions about my patients culture as it plays such a huge role in ones life, affecting what occupations they do and how they are carried out.
In conclusion, the take home message here is that even though I try my utmost to respect my clients and treat without bias, its not enough. I need to understand my clients holistically and this includes their culture, as well as their dialect! Communication is a necessary factor in occupational therapy, and without it, intervention is ineffective. (Govender et al. 2017)
References
Govender, Pragashnie, et al. (2017) “Exploring Cultural Competence amongst OT Students,” 2017 Occupational Therapy International 1–8.
Hildebrand, Kristin, et al. (2012) “How Can Occupational Therapy Strive Towards Culturally Sensitive Practices?,” The American Occupational Therapy Association.
Matthews, Margaret, & Jacqueline Van Wyk (2018) “Towards a Culturally Competent Health Professional: A South African Case Study,” 18 BMC Medical Education.
Professional, Cleveland Clinic Medical (n.d.) “Psychosomatic Disorder,” Cleveland Clinic, https://my.clevelandclinic.org/health/diseases/21521-psychosomatic-disorder.
Sonn, Inge K., & Nikki Vermeulen (2018) “Occupational Therapy Students’ Experiences and Perceptions of Culture during Fieldwork Education,” 48 South African Journal of Occupational Therapy.
0 notes
Text
Lombardia World Summit, Malagò: «dalle Olimpiadi di Milano Cortina 4,5 miliardi di valore aggiunto»

Lombardia World Summit, Malagò: «dalle Olimpiadi di Milano Cortina 4,5 miliardi di valore aggiunto».
«Milano Cortina 2026 genererà per ogni euro investito un ritorno di tre volte superiore. Lo hanno certificato le università di Ca’ Foscari e la Bocconi. Abbiamo investimenti per 1.5 miliardi, che genereranno 4.5 miliardi di valore aggiunto». Lo ha detto Giovanni Malagò, presidente del Coni, intervenendo a Lombardia World Summit in un confronto con Paolo Scaroni, presidente Eni e Ac Milan.
«Elevatissima, quindi, – ha aggiunto Malagò – è la riconoscenza verso la Lombardia e Regione Lombardia, alle sue province che hanno dato tanto in termini di medagliere olimpico per la loro grande storia sportiva. A prescindere da quello che sarà l’aspetto sportivo, e dalle criticità che non mancano come non mancano altrove».
«Lo sport resta sempre popolare, tutte le manifestazioni, lo abbiamo visto anche recentemente, sono sold out – ha detto in conclusione Malagò -. Nessun freno per l’incoming turistico, nonostante le tensioni e gli scenari internazionali; venderemo 1,6 milioni di biglietti con una proiezione di 2 milioni in funzione dell’infrastrutturazione complessiva di cui l’evento potrà godere».
Intanto, mercoledì, è iniziato un nuovo percorso per il movimento paralimpico lombardo, che beneficerà di ulteriori fondi volti alla promozione dei valori e della pratica sportiva per tutte le persone con disabilità.
Una tappa importante verso le prossime Paralimpiadi Italiane 2026. Presso la sede della Fondazione Milano Cortina 2026, a Milano, si è svolta mercoledì la conferenza stampa di presentazione della delibera regionale che riconosce contributi economici per l’acquisto di ausili e protesi per lo svolgimento di attività sportive amatoriali di persone con disabilità fisica. Il Sottosegretario con delega allo Sport e ai Giovani di Regione Lombardia, Lara Magoni, ex atleta, si è spesa in prima persona per questo provvedimento.
La misura sostiene concretamente l’attività motoria e sportiva amatoriale consentendo alle persone con disabilità di vivere un’esperienza profondamente formativa e terapeutica come lo sport. Complessivamente sono a disposizione delle Ats lombarde 947.504 euro. I beneficiari sono persone, residenti in Lombardia, amputate, affette da paraparesi, paraplegia o tetraparesi, oltre agli invalidi civili, di età compresa tra i 10 e i 64 anni, aventi i requisiti clinici funzionali idonei per accedere ai bandi....
#notizie #news #breakingnews #cronaca #politica #eventi #sport #moda
Read the full article
0 notes
Text
Paraparesis is a form of partial paralysis that impacts the legs and lower body. It is commonly caused by diseases such as multiple sclerosis, spina bifida, and spinal cord diseases. Know the myths and facts for clear understanding of the condition.
To Consult Dr. Hemang Jani, Physiotherapist, Visit: https://spandanphysiotherapyclinicrjt.whitecoats.com/ Call: 9033762190
#DrHemangJani #Rajkot #Physiotherapist #Paraparesis #NeurologicalCondition #ParaparesisAwareness #MobilityIssues #NeuroRehabilitation #ParaparesisTreatment #NeuroHealth #MobilityRecovery #NeurologicalHealth #NeuroRecovery
Untitled
View On WordPress
0 notes
Text

In Baltimore City, MD: URGENT: 3 month old blind but sweet kitten needs rescue placement ASAP - BARCS, Baltimore MD
- Rescue needed by close of business 4pm on 7/22 -
Beryl- 3 months, unaltered male, 2.98lbs
FELV-/FIV-
Adorable little Beryl was found all alone in someone's yard, curled up next to a grill. He seemed confused and wasn't moving, but allowed a Good Samaritan to scoop him up and bring him to BARCS for examination and care.
Upon examination, our vets noted Beryl appears to be blind and has paraparesis in the hind limbs. He shows no overt ataxia, but seems weak and his back legs splay on slippery surfaces when standing still. Spinal and hind limb x-rays, as well as a neuro consult are recommended.
Due to Beryl's medical issues and need for further testing, he needs to find rescue placement by the end of stray hold (4pm on 7/22).
Despite his issues, Beryl has been a friendly and cooperative kitten so far in our care and eats enthusiastically.
Please let us know if your organization can help!
Thank you,
The BARCS Rescue Team
Baltimore Animal Rescue & Care Shelter (BARCS)
New Address! 2490 Giles Rd, Baltimore, MD 21225
[email protected]| (410) 396-4695
Rescue pick-up hours:
Monday-Friday: 10:30 a.m.-6:30 p.m.
Saturday and Sunday: 8:30 a.m.-4:30 p.m
Adoption hours:
Monday-Friday: 2 p.m.-6 p.m.
Saturday and Sunday: 11 a.m.-4 p.m.
Baltimore Animal Rescue and Care Shelter, Inc. (BARCS) | 2490 Giles Rd, Baltimore, MD 21225
0 notes
Text
Spine Injury Lawyer: Consequences and Compensation Explained
After an accident that hurts their spinal cord, people frequently suffer from long-term problems, pain, and even paralysis. By going to court against the person who caused your accident, your spinal cord injury attorney can get you monetary compensation for the damages and other losses. They’ll gather proof, talk with the insurance company of the person who hurt you, and maybe even file a legal complaint to secure your compensation.
Impacts Of Painful Spinal Injuries
Spinal cord injuries stop your brain from talking to your body parts, which means you have less control over your limbs. Injuries are called “complete” if you have no sensory or motor skills below the injury, or “incomplete” if you still have certain sensory or motor abilities below the injury.
People with spinal cord injuries all have at least one of the following problems:
Loss of movement, such as in paraparesis or paralysis, where you can’t move at all or only in certain ways.
Loss of senses, like being unable to sense cold, heat, or touch
Spasms or overactive reflexes are signs of this.
Lack of control over the bowels or bladder
Pain or a stinging feeling caused by damage to nerve fibers
Changes in ovulation, sexual function, and sensitivity
Having trouble breathing, coughing, or getting phlegm out of the lungs
The effects of a spinal injury are, of course, much more than just physical or medical. Spinal cord accidents force people to learn how to live within the limits of their injury. They might lose their capacity to work and pay bills, endure much suffering and pain, and deal with many other terrible long-term effects.
Compensation From Spine Injury
We can cover the following compensation and expenses you have spend while having surgery:
Medical Expenses – After a spine injury, bills for care can add very quickly. Our lawyers in California can help you get full payment for your ambulance costs, hospitalization, doctor’s visits, adaptive equipment, prescription medications, and any additional healthcare expenses you have.
Lost Wages – Depending on what the doctor says, you might not be able to go to work for a few weeks or months. Without the assistance of an expert lawyer, it might be hard for you to pay your rent and buy food. With the help of a lawyer, you can get money to makeup for the income you lost, giving you the security you need to get better.
Less ability to make a living – As stated, permanent problems can keep you from working or cause a big drop in your earnings. If that’s the case, these fines can help you makeup for the loss of income.
Pain and Sorrow – Spinal cord damage can cause pain deep in the body, pain that lasts for a long time, and suffering from tense muscles. These injuries can help you deal with the physical pain your condition causes.
Troubled Feelings – Accident and injury patients often have trouble with their emotions, PTSD, anxiety, and other emotional problems. Our California spinal cord injury lawyers can help you get the money you need to pay for therapy and, if needed, prescription medications.
Conclusion
Workers’ compensation lawyers at Gaylord and Nantais can help if you or a loved one has suffered a spinal cord injury on the job. Contact us at this moment at (562) 561-2669 to set up a no-cost consultation.
0 notes
Text
Disability AU Summary!
Let's go in alphabetical order just because. This isn't really a "masterpost" but these should be in one place.
To reiterate, this AU is avoiding cure plots and excess angst related to the disability. I've done research and put in my own experiences but obviously not everything is going to be perfect.
Four—paraparesis, also called partial paralysis, due to a spinal cord injury inflicted between his first and second adventures. He can't walk without support, which usually comes in the form of a wheelchair he modified, or crutches. The colors experience different intensities, from Vio with near-full paraplegia, to Red who uses crutches, to Green who does as well, to Blue who can walk without support. Four will stab anyone who tries to move his chair without asking.
Hyrule—retinopathy of prematurity, and mild cataracts. He's functionally blind, though he can make out shapes of light and dark with a few shades in between. He has a favorite carved-down stick he uses as a white cane, and his magic can act a little like a radar that blips on good magic (like fairy fountains and Hero Spirits and Zeldas) and bad magic (like corruption and monsters.) He has deep-seated reflexes to stab anything that touches him unexpectedly so please, everyone, advertise your presences.
Legend—RRMS, relapse/remission multiple sclerosis. Translates mostly into stiffness in his legs that gets worse with heat and humidity, and annoying fatigue. Relapse periods for him are characterized by a lot of joint pain and temporary periods of partial blindness. Relapses last days to weeks, remissions last weeks to months. He has an enchanted cane that he will hit your shins with.
Sky—moderate to severe deafness from birth. He can hear low, loud sounds the best. He speaks very clearly (and maybe a bit loudly) due to speech therapy. He gets magic hearing aids in Wild's world because I want him to, and he can now mostly hear voices when they speak up. He can read lips when people are facing him, but even at the best, that only gives him a quarter of what they're saying. Immune to mean taunts and jabs, partly because he can't hear most of them and partly because he's just like that.
Time—that eye he always has closed? It's missing now. He has a cool eye patch. Don't throw things at him.
Twilight—transverse deficiency. He's been missing his right arm between shoulder and bicep since birth. Wolfie is conspicuously three-legged, not that anyone notices the connection sooner. He either needs his modified clothing (thanks Uli) or help getting things on (thanks for nothing Warriors's world with its fancy balls.) He is the definition of "improvise, adapt, overcome." Still a beast on the battlefield. Ba-dum tish.
Warriors—adductor/tremor SD. His vocal cords don't work correctly. He can talk, but it's gotten worse over the years. His voice is quiet and very rough, and shakes almost too much to understand. He prefers signing as his main method of communication. He gets sore throats a lot, and makes a lot of good tea. His laughs are unaffected, and on occasion, he can yell just fine across the battlefield.
Wild—worse burn scars, hypertrophic and contractual. He has spotty hearing on the left, and his shoulder gets stiff a lot. He has a variety of potions and lotions to loosen up and stop the itching that pops up a lot. The shrine did some skin grafts (or whatever the magical equivalent is) and fixed most interior organ issues. The scar is deep but doesn't interfere with those.
EDIT to add—Wild also has atherosclerosis, a heart condition where plaque builds up and heart attacks become a more serious concern. He just needs to stay active and pay attention to his breathing and chest pain. It's not a huge issue, but it could be if he was negligent. The Link he doesn't remember being had more of a difficult time with the condition, and ended up getting heart surgery for it (something like an angioplasty, where they went in to physically unblock the arteries that had gotten buildup.)
Wind—peg leg pirate! Lost his left leg a few inches past the knee to infection. After getting treasure from his adventure, he got a nice, foot-shaped wood and leather prosthetic. It's starting to get a little small.
#my writing#linked universe#disability au#im half asleep so forgive mistakes#i wanna draw a group shot of them all#but i am too tired todsy#so imagine it :)
164 notes
·
View notes
Last Seen Blogs

pucawithaphodda
Untitled

matarou
matarou
lcg63
Untitled

biociderho
Vanessa

satandidyoumissme42
secretly ziggy stardust