#Omentum
Text
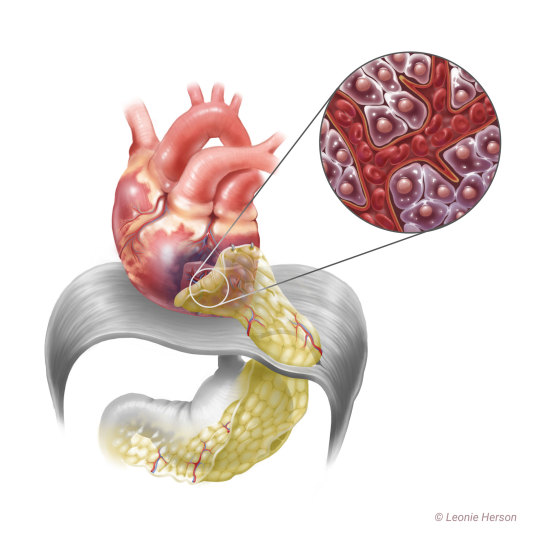
3 years ago I was fortunate enough to create an illustration for an article in the European Journal of Cardio-thoracic surgery 😊
Please give it a read if you're interested! >>> https://academic.oup.com/ejcts/advance-article/doi/10.1093/ejcts/ezaa205/5893647
7 notes
·
View notes
Text

[Omentum.]
0 notes
Text
MommyBlowsBest Lisey Loves Sucking Stepson the Most
Handsome teen services a big mature cock and receives facial
Booty Transgirl Korra Del Rio gets her white ass banged
Pair gets totally naked in public and bonks under the sun
august ames
Katy cachorra Siririca de quatro
Desi aunty showing his big tits Mia khalifa
Blond young man receives blowjob before classroom sex
Amazing brunette teen enjoys engulfing a giant dick lustfully
Cogida en casa de mi ex
#unfallenness#Hejira#metachromatinic#secretaries-general#abusefulness#switchblades#nonmythical#bombazet#omentum#superhumeral#light-heeled#meteoroidal#horehound#bracer#seisor#spruced#Helbon#tendences#Johen#grind
0 notes
Text
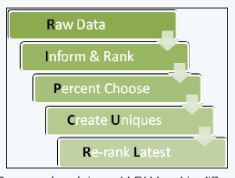
Controlling Informative Features for Improved Accuracy and Faster Predictions in Omentum Cancer Models
Abstract
Identification of suitable biomarkers for accurate prediction of phenotypic outcomes is a goal for personalized medicine. However, current machine learning approaches are either too complex or perform poorly. Here, a novel feature detection and engineering machine-learning framework is presented to address this need. First, the Rip Curl process is applied which generates a set of 10 additional features. Second, we rank all features including the Rip Curl features from which the top-ranked will most likely contain the most informative features for prediction of the underlying biological classes. The top-ranked features are used in model building. This process creates for more expressive features which are captured in models with an eye towards the model learning from increasing sample amount and the accuracy/time results. The performance of the proposed Rip Curl classification framework was tested on omentum cancer data. Rip Curl outperformed other more sophisticated classification methods in terms of prediction accuracy, minimum number of classification markers, and computational time.
Read More About This Article: https://juniperpublishers.com/ctbeb/CTBEB.MS.ID.555559.php
Read More Juniper Publishers Google Scholar Articles: https://scholar.google.com/citations?view_op=view_citation&hl=en&user=nWCnyqYAAAAJ&citation_for_view=nWCnyqYAAAAJ:YsMSGLbcyi4C
0 notes
Note
ask him who trained him and let him know he doesn’t need to say it! i used to have a pathologist that demanded I say “mid tip cross sections” for any cross section that wasn’t the tips of an excision and I said it through two jobs before another pathologist asked me why the hell I was doing that. I just thought it was mandatory everywhere because he pitched SUCH a fit when I didn’t do it.
asdkjasjdksa thats SO REAL pathologists will have the wildest demands and pitch a fit when you dont cater to them...we r trying to standardize grossing practices in edmonton atm and its been SO hard because various pathologists have various demands such as:
-dont say WEIGHT say MASS
-lymph nodes arent BISECTED they are BIVALVED (even tho i tried to argue that bivalved implies that the node is still hinged...)
-some want fallopian tubes for ovarian masses in toto others will get pissy when they have to look at entire tubes
-breast specimens...cutting medial->lateral or right->left ... there r Opinions
-staging omentum...we submit 1 cassette per 2cm except one path went off on me because he said 'measure the omentum as if its squished into a cube so i get less sections' hello????
#brb going insane#he said there is no way that someone has a 40cm omentum bruh i beg 2 differ ive seen some thicc ass omentum#and in the end they found ONE microdeposit among my 20 cassettes so it was lucky i submitted all of em
3 notes
·
View notes
Text
Free Strand of the Greater Omentum in Surgical Practice and its Morphological Characteristics by Martynov Vladimir L

Abstract
In his operating work, the surgeon often uses the patient's tissue to solve practical problems. For our work, the data of Liebermann-Meffert D. and White H. (1989) on the greater omentum are of interest [1]. Research shows that the "policeman of the abdominal cavity" - the great omentum in pathological conditions, acquires very special properties: plasticity; the ability to adhere to an injured and inflamed surface; the ability to hemostasis; the ability for ingrowth and revascularization; the ability to absorb liquids and microparticles from the abdominal cavity; the ability to phagocytosis and immunological response. Adhesions with the omentum are formed much faster than with other organs of the abdominal cavity. Even the freely transplanted omentum tissue without blood supply retains these properties. After 21 days, the omentum tissue is completely fused with the recipient [2].
Introduction
Experimental studies of ingrowth of the omentum graft and its vessels are very indicative. Sections of the omentum of different thickness and size were separated from its bulk and fixed without revascularization to various organs and tissues of the same or another animal: stomach, small and large intestine, liver, spleen, kidney, urinary bladder, lung, pleura, peritoneum, mesentery, aorta, inferior vena cava. Within a week, the graft is firmly attached to the tissues of the recipient organs, its separation is difficult, due to a decrease in the amount of fat, its thickness is reduced, necrobiotic processes, necrosis zones are reduced. After three weeks, the graft cannot be separated, when an attempt is made, bleeding occurs, the amount of fat decreases and is replaced by dense fibro- and angioplastic tissues so that its surface resembles the surface of the recipient tissue. After 12 weeks, it is difficult to distinguish the omentum tissue from the recipient tissue; the suture line serves as a reference point. The engraftment of free grafts did not depend on their size, but necrosis zones are more often formed in thick grafts. The graft remains viable when frozen for two weeks or even longer. Stages of omentum transplant engraftment: attachment - up to 4 hours, beginning of vascular ingrowth - 24 hours, tight fit - 48 hours, revascularization - 3 days, fat resorption - 3 weeks, fibrous degeneration - 24 weeks [1].
These studies allowed us to use a strand of the free area of the greater omentum in the small intestine in 107 patients. Here is an example of the clinical use and preservation of the viability of the free strand of the greater omentum.
Case Report
A 25 years old, was admitted to the GBUZ NO "GKB No. 12" in Nizhny Novgorod on 11.11.2013 with a diagnosis of "Closed abdominal trauma". After dynamic observation, an emergency laparotomy was performed, during which a rupture of the pancreatic head was detected. Outflow of bile, pancreatic juice was not detected. A tampon was brought to the site of damage to the gland through a separate incision in the right lumbar region. The drains were placed in the right lateral canal, in the omental bursa, in the small pelvis. On 20.11.2013, the intake of contents up to 3 liters with an admixture of bile was noted. On an urgent basis, relaparotomy was performed, during which two perforations were revealed on the posterior wall of the vertical part of the 12-PC, each with a diameter of up to 7 mm, from which, after the introduction of methylene blue, a blue discharge began to flow into the stomach. After excision of the edges of the perforations, the latter are sutured with interrupted single-row sutures. The seam line is reinforced with a large gland strand. A drainage-foam rubber system for active aspiration is connected to this zone through the opening of the right lumbar region (the place of the gauze pad). A loop of the jejunum was isolated 30 cm from the Treitz ligament, on which an areflux nutritional jejunostoma was formed with an interintestinal anastomosis according to Brown and a "plug" on the leading loop 1 cm below the anastomosis. The stoma was placed in the left mesogastric region. A feeding tube was inserted 25 cm behind the anastomosis line.
On January 20, 2014, the patient was admitted to the Nizhny Novgorod City Clinical Hospital No. 12 for the second stage of treatment - closing the nutritional jejunostomy. The skin around the stoma is intact. Performed fistuloenterography through a probe introduced into the leading section of the stoma to the "plug". The contrast does not pass through the "plug" zone, which confirms its areflux function.
01/23/2014 under general anesthesia in the left mesogastric region with two bordering incisions around the stoma, the latter was isolated from the tissues of the anterior abdominal wall. The segment of the intestine with the stoma is brought out to the anterior abdominal wall. The area of the free omentum with the ligature, which acts as a "plug", is viable, loosely welded to the jejunum. The interintestinal anastomosis is passable. Near the anastomosis, the sections of the intestine were stitched with the UO apparatus. The section of the intestine bearing the stoma was resected. The intestinal stumps were additionally sutured with two semi-lace sutures each. Layered suture of the wound of the anterior abdominal wall. Preparation: a section of the jejunum up to 10 cm long with a stoma and a free section of the greater omentum - “plugs”. The area of the free omentum with a ligature, which acts as a "plug", was loosely welded to the jejunum (Fig. 3). The mucous membrane of the jejunum of the "plug" formation zone is not visually changed (Fig. 4). The interintestinal anastomosis is passable.
Morphological examination of the "plug" zone at 3, 6, 9, 12 hours of the intestinal wall circumference showed only edema, moderate lymphohistiocytic infiltration, moderate circulatory disorders [3].
The wound healed by primary intention. In satisfactory condition 02/03/2013 was discharged for outpatient observation by a surgeon.
Conclusion
Thus, our observation confirms the possibility of using a strand of "free", devascularized omentum as a plastic material in small bowel surgery.
For more information about Article : https://ijclinmedcasereports.com/
https://ijclinmedcasereports.com/ijcmcr-cr-id-00147/
https://ijclinmedcasereports.com/pdf/IJCMCR-CR-00147.pdf
0 notes
Text
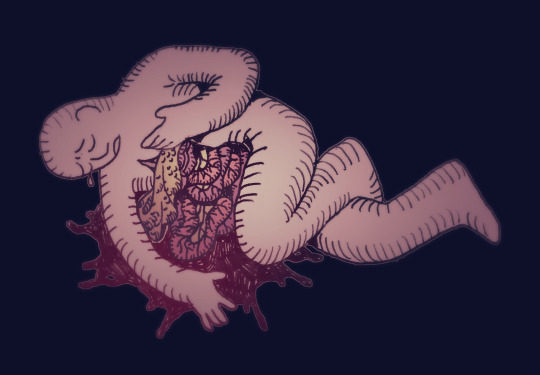
back by popular demand - evisceration! this time with the omentum and not just the mesenterium!
47 notes
·
View notes
Text
Growing list of names that I WOULD give characters if they weren't already word parts or names of gross visceral terms:
-Haustra
-Ileum
-Omentum
-Atria
-Sartorius
-Soleus
3 notes
·
View notes
Text
[shaking from the amount of restraint i exercise when choosing to not nitpick abdominal gore for the total absence of the greater omentum]
#sorry i talk about sort of gory stuff for someone who actually is super sensitive to violent gore ggdhfhfhg#like medical gore is mildly spooky to me. but i can deal#*i really about sort of gory stuff A LOT for someone etc etc#writing is bad RN I'm v sleepy#blondiepost
5 notes
·
View notes
Text
Was rambling to dental hygienist earlier about horror projects and medical stuff.
I still think it's a lot of fun taking my medical knowledge pool into writing.
And filtering it in different ways, depending on the character voice and context.
Ranging from relatively unfiltered and clinical like iZ!Logan to someone who doesn't know much at all and is p squeamish about the entire subject like Gymrat!Ro.
Where we got writing samples like:
I grabbed a wash bottle and irrigated the area to get a better view. Remus shivered slightly and was still glib, “That was fun!”
“I have to admit, this is interesting… not needing to worry about acquiring or explaining the need for anesthetics.”
Remus briefly sobered, “Yeah. Even pain can get pretty old, sometimes.”
There was a couple segments of his small bowel punctured, a superficial slice over the surface of his transverse colon, a few nicked lesser vessels of his omentum, which appeared to be staunching some of these wounds. It was strange looking at tissues that reminded me of somewhere between livid and perfused in color. Very little actually appeared necrotic, but I supposed this was a good opportunity to conservatively excise some tissue samples.
When I grabbed a scalpel, he started singing. “Like a surgeon, hey – cuttin' for the very first time~”
VS:
The haze lingered, yet he was staying up longer. He wished he could take that as a good sign, but it was just getting harder to sleep.
Old members of the care team from when he last had that rhabdomy-lisisis thing, would come to visit him sometimes.
The kidney doctor was the first to talk, he hated how reserved they were, he could feel the bad news about to roll off their tongue. “You cut things very close, this time, Mr. Sanchez.”
His voice quavered a little, “T-tell me why I’m an idiot, get it over with…”
The kidney doctor’s eyes widened but quickly softened, “It’s common to have mood shifts with the kind of labs we got here… you’re in good hands, while we help you get more stable.”
“Stable?”
“The heatwave and the delay in getting to us… didn’t help.”
Roman was irritable, “What the fuck is that supposed to mean?!”
2 notes
·
View notes
Text
threw my scrubs covered in bile and omentum residue into the washer with the rest of my normal clothes, they can all fight it out in there
7 notes
·
View notes
Text
And to Dust You Shall Return
An old illustration for my old story... And for my new translation! You can visit me and support my work on AO3 (https://archiveofourown.org/works/42272379) or read full story right in this post!

“And to Dust You Shall Return“ is my little ode to love for the very first object, which led me to the SCP Foundation fandom. For old version of SCP-049 (https://scp-wiki.wikidot.com/scp-049-arc). This is a short story about strange dreams about death and decay that Plague Doctor falls. But the strangest and most eerie thing is not that, but that he is not scared of this at all...
WARNING! The following text contains detailed description of decomposition and postmortem processes. Also, it may contains motives related to suicidal themes. If you have such thoughts and it becomes a problem, it is better to contact a specialist. Please be safe.
***
For several nights the Plague Doctor had been having the same dream.
It was full of images and sensations, almost tangible. After waking up from it, the Doctor lay on the bed for a long time, basking in the remnants of the vision — and his muscles stayed relaxed and disobedient for minute or two, as if the body was stuck in a charming ideal world that could only be born in tender pre-morning dreams.
Doctor liked it. Liked the bittersweet feeling that was sitting in his chest, liked to feel as if moisture had soaked his back, liked to remember the tightness that surrounded him, like an embrace. He had never thought that it could be so good in the grave.
In these dreams, he was lying in the wet ground, half covered with a shroud, motionless and heavy, with glazed eyes and swollen from liquid skin. His hand was frozen reaching up, clamped between his body and the edge of the pit — he looked at the shrunken hand with admiration — dead, but fulfilling his last will. Yes, he wanted to reach the sky...
The wind touched the fingers directed to the gray clouds, to the soft white light. There was not a single shadow around — the landscape seemed painted on canvas, a greenish-blue haze with strands of thick white fog hid the details of the grass and erased the horizon line. And everywhere the eye could see, everything was glowing and soothing and blissful, and the sky was shining, as if three suns were hiding behind the clouds at once.
This must have been Paradise.
He could not see, but he knew that his open cloak would soon be full of new life. The life that glows in hundreds of small white tubes attached with maternal love to the delicate joints of the body with the garment. Usually his fragrant musky smell repelled insects. But now he was not sweating, he was not secreting sebum and protective compounds— all these systems were dead.
When an endless scattering of older cubs scurried over his skin, when they moistened the flesh of his stomach with dissolving saliva, when they drank putrid juice like milk, when they got to the decomposed gray mass of omentum , he felt no pain, no nausea, no itching. His body stopped resisting, stopped screaming at him about damage and foreign proteins. It was over. There was only peace ahead.
He heard a buzzing sound. Then he saw a fly that flew past his frozen hand. He looked after it — the sound of its wings became quieter, in a matter of seconds it became a tiny blurry dot flying straight into the delightful high sky. And then it disappeared.
But there was a crack and another newborn creature soared skyward. Oh, that's the thing. His chest…
Is there really so little left of him?..
His armpits, stomach and pelvis were gnawed long ago — and soft grown-up larvae began to his chest, blackened from rot. He still has his back and legs — but a new brood will start to them later. But these little creatures got everything they needed from him. They carefully prepared a place for their cocoons, eating through the oozing yellow flesh, climbing deeper and deeper, to the bones — forming new holes next to the empty shells of older brothers — gray balls inserted into the skin.
After pupating, the larvae froze and fell asleep to wake up with wings and go towards the clouds.
He admired them, squinting his eyes to his chest. Why they didn't touch his head? The eyes and lips are so gentle, it would be easy for the cubs to dig into the soft flesh. Why didn't they like his face? Maybe the mask left too little meat on the skull?..
A bright flash caught his attention — he looked up again, and his soul trembled. A butterfly was sitting on his withered finger. Huge, it was curiously applying its proboscis to the wound, orange wings fluttered as it shifted from paw to paw. Previously, his touch would have killed the poor insect, but now he couldn't take his eyes off its translucent carved wings. But with his peripheral vision he caught another movement — three birds hovered high in the sky, circling and pausing, as if to get a better look at his prostrate body.
The сrows?..
They will disturb the little creatures… Although it's not up to him to decide who to feed. He's dead. The dead need not worry. If a few larvae die and become a meal for another living creature like him, is that a bad thing?..
The butterfly plunged its proboscis deep into the finger, sucking the rotting blood. Out of the corner of his mind, the Doctor remembered that such beautiful fragile creatures sometimes lack nutrients, so they drink sweat and blood, as humans sometimes consume chalk and lime.
The crows were approaching, he could clearly see their silhouettes.
How will their cold paws feel on him? Will they scatter the bones, making their way to the remains of the entrails? Or maybe one of them will fly away with a piece of cartilage and meat in its beak to hide it in a secluded place?
The air was damp and rainy, smelled of damp earth, grass and mushrooms. But most of all it smelled of rotten meat — this sense always seemed to the Doctor so layered and sweet. What a pity that people couldn't perceive it the way he did. If they knew what wonderful and complex processes take place in the body after death, if, like him, they could appreciate these aromas, if they had immunity to cadaveric diseases…
Maybe it was the smell that attracted unnaturally large coal-black birds?
Suddenly the crows disappeared. But he realized what was the matter when he heard the noise of feathers — the birds turned aside. They weren't going to land on his body. They wanted to land sideways on the ground, out of his sight. But why?
Why don't they pounce on the carefully provided food? Why are they procrastinating? Why didn't they make a single sound all the time?..
Wings flapped, a stream of air touched his arm. The butterfly was cleaning its antennae. It didn't move when the crows approached the ground. The beating of wings did not stop — did their owners hang in the air? The Doctor looked away in bewilderment from the butterfly, from the larvae in the skin, from the exposed bones and looked up. The sky was calling him. A deep, luminous sky, billowed with clouds…
Suddenly the earth shook and hummed, as if not crows, not light birds, but an immense mountain had fallen on the ground.
And then he wakes up.
After sleeping, Doctor poured a basin of water, washed his face and hands, then brushed his teeth with a wet cloth. Then he adjusting the cord on his cape and the belt over his cloak, and said a prayer and started routine work, gradually forgetting to yearn for the interrupted dream.
The days passed as usual. He sorted his collection of scientific papers over and over again and enjoyed music and books. Sometimes patients were brought to him, sometimes someone tried to talk to him. The last time for some reason a dead goat was brought to him instead of a patient, and he looked at the camera with complaint and misunderstanding for several minutes before they decided to send him home. During conversations, colleagues asked about strange new things, never realizing that his answers were to be useful to them.
Something incongruous was happening. Of course, he liked this place, it was much more comfortable than his former abodes, but sometimes he missed the musty smell of basements and the cold of forests.
He missed the spacious fields and dark quiet nights, he wanted to stop again at least once in an abandoned settlement with charming stone houses, or hide in the thicket and watch the bustling people.
He missed the land from where he came. And he had too much to do to get back there anytime soon.
And is it normal that recently he found black feathers in his bag, although he never let a single crow near it?..
#scp-049#scp fanfiction#SCP Foundation#scp fandom#scp#scp fanart#vent#vent art#gore#horror#grimdark#story#vent writing#plague doctor#tw gore#tw body horror#tw depressing thoughts#tw death#tw dark content#my post#my art
17 notes
·
View notes
Note
❓❓❓
Thanks for the ask, Anon!
The greater omentum is a fatty tissue that covers your intestines. It’s cool because for example, if you had appendicitis, it would move to protect the injured area of your intestines.
The pancreas has a gritty, crumbly texture. Surgeons avoid operating on it because of this.
Children have an enlarged thymus. The thymus is a part of the lymphatic system, and is where certain kinds of immune cells grow.
Ask game
2 notes
·
View notes
Text
you should be able to open up ur greater omentum and scoop out the fat and use it like a giant hoodie pocket but in ur body
4 notes
·
View notes
Text
INGUINAL HERNIA (ANGIN PASANG)
Inguinal hernia, atau lebih dikenali sebagai ‘angin pasang’ dalam Bahasa Melayu, adalah sejenis keadaan di mana usus atau selaputnya (omentum) terjatuh masuk ke dalam sebuah kantung (pouch), dan kantung tersebut terjulur keluar melalui pembukaan otot dinding perut di bahagian ari-ari (groin).
Keadaan ini disebabkan oleh pembukaan pada otot dinding perut (abdomen) yang dalam kebanyakan masa bukaan ini akan tertutup secara semula jadi sewaktu bayi dilahirkan ataupun dalam tahun pertama kehidupan.
Ia berbeza dengan kejadian ‘angin pasang’ di kalangan orang dewasa di mana faktor utamanya disebabkan oleh kelemahan otot dinding perut yang berkaitan dengan peningkatan umur dan masalah-masalah kesihatan lain.
Inguinal hernia BUKAN disebabkan oleh gaya pemakanan seseorang ibu mengandung. Ia tidak dapat dikesan sewaktu bayi berada dalam kandungan.
Demografi dan Epidemiologi
Secara keseluruhannya, kadar masalah inguinal hernia di kalangan kanak-kanak adalah 3%.
Kebanyakannya melibatkan kanak-kanak lelaki (6-10 kali ganda berbanding dengan perempuan).
Inguinal hernia adalah sejenis keadaan yang berisiko tinggi, terutamanya di kalangan bayi-bayi di bawah umur 1 tahun. Ini adalah kerana ia boleh menyebabkan pelbagai komplikasi disebabkan oleh usus yang terperangkap di dalam kantung hernia (rujuk bahagian ‘Komplikasi’). Kadar ini dijangka dalam lingkungan 30%.
TANDA-TANDA
Inguinal hernia boleh melibatkan sebelah ataupun dua-dua belah ari-ari. Ia akan kelihatan seperti bonjolon di bawah kulit di bahagian ari-ari, atau boleh turun masuk ke dalam sarung telur budak-budak lelaki.
Ia TIDAK disebabkan oleh aktiviti yang lasak atau anak meneran atau menangis, tetapi ia akan dilihat dengan lebih nyata dalam keadaan-keadaan tersebut.
KOMPLIKASI
Sekiranya sebahagian daripada usus terperangkap di dalam kantung hernia (Incarceration), komplikasi utama yang boleh berlaku adalah usus tersumbat (intestinal obstruction). Dalam keadaan ini, najis dan gas tidak dapat keluar melalui jalan dubur seperti biasa, dan mengakibatkan pesakit mengalami kesakitan perut dan di ari-ari atau karung telur, perut kembung, muntah dan kesukaran membuang air besar.
Sekiranya pesakit tidak mendapat rawatan awal, usus yang terperangkap di dalam kantung hernia boleh terus tercedera sehinggakan bahagian tersebut mati (gangrene) akibat kesekatan saluran darah ke bahagian usus yang terperangkap.
Keadaan-keadaan yang diterangkan di atas memerlukan rawatan pembedahan secara cemas. Komplikasi lain yang boleh berlaku termasuk keadaan di mana tumbesaran telur bayi lelaki terbantut atau terjejas sama sekali disebabkan oleh inguinal hernia (Testicular atrophy). Ini boleh berlaku terutamanya kepada bayi-bayi pramatang atau sekiranya hernia dikaitkan dengan kedudukan telur yang tidak betul (Undescended testis) bagi bayi-bayi lelaki.
RAWATAN
Tiada rawatan lain untuk masalah inguinal hernia selain daripada pembedahan. Pembedahan ini dikenali sebagai Herniotomy.
Ia adalah sejenis prosedur yang memerlukan bius am (general anaesthesia) dan sebaik-baiknya dilakukan oleh pakar bedah kanak-kanak. Pesakit perlu dipuasakan untuk beberapa jam sebelum pembedahan ini.
Dalam keadaan yang tidak melibatkan komplikasi, pembedahan Herniotomy biasanya dibuat sebagai prosedur unit rawatan harian (Daycare Surgery). Ini bermaksud pesakit tidak perlu tinggal di dalam wad untuk semalaman.
Herniotomy melibatkan torehan kecil (biasanya 2-3cm) di bahagian ari-ari yang bermasalah.
Seterusnya, kantung dijumpai di bawah lapisan otot, dan ia dipisahkan daripada saluran sperma dan saluran darah; sejurus itu, kantung dipotong dan diikat supaya ia tidak dapat membenarkan pergerakan usus atau selaput ke dalamnya lagi. Potongan kemudiannya dijahit dengan benang khas di bawah kulit dan akan hilang dengan sendiri dengan peredaran masa. Prosedur ini biasanya memakan masa 15-30 minit.
Selepas pembedahan ini, pesakit boleh diberi minum dan makan apabila dia sedar dengan sepenuhnya. Dia dibenarkan pulang ke rumah pada hari yang sama. Ibu bapa akan diarah untuk mengeluarkan pembalut daripada luka 2 hari selepas pembedahan.
Sekiranya luka tidak begitu elok (iaitu merah atau bernanah), pesakit perlu dibawa balik berjumpa dengan doktornya. Biasanya, kanak-kanak yang lebih besar diberitahu untuk mengelakkan daripada aktiviti senaman yang lasak sekurang-kurangnya selama 1-2 bulan.
#HealthDrZubaidi
www.drzubaidi.com
Ikuti perkongsian pengalaman dan pengetahuan sepanjang lebih 25 tahun menjadi doktor Pengamal Perubatan Am di Telegram berkaitan kesihatan, pemakanan dan ubat-ubatan.
https://t.me/PerkongsianDrZubaidiHjAhmad

1 note
·
View note
Photo
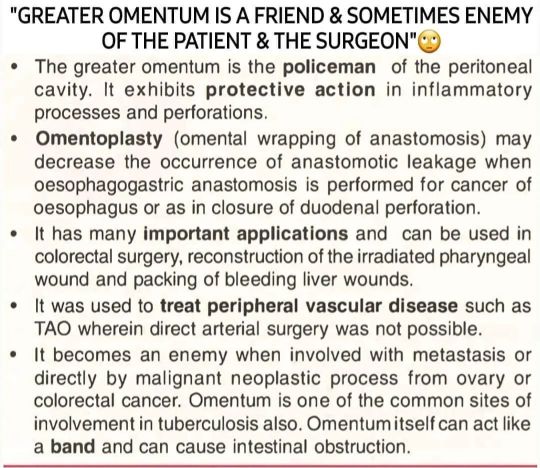
Omentum - Policemen of the abdomen (at Jawaharlal Nehru Medical College, Belgaum) https://www.instagram.com/p/CfCKiZcB6WR/?igshid=NGJjMDIxMWI=
4 notes
·
View notes
Last Seen Blogs

lilithluv
lilithluv

urbancolor
Urban Color

dutchmotorsport
Dutch Motorsport

wheezecake
♕It Ain't Easy Bein' Wheezy♕

cactusprincewrites
cactus-prince-writes