#by the time in activates in may.. they will not be able to access hrt! wow! and this coming after gov cox wrote a letter last year
Text
wow im so happy with life and the state i live in nothing could possibly go wrong (utah just put a ban on hrt for trans minors)
#from what ive read either it needs a final review from a medical association before itll go active#or its going fo activate in may of this year :D from what i gather any trans youth not DIAGNOSED with dysphoria#by the time in activates in may.. they will not be able to access hrt! wow! and this coming after gov cox wrote a letter last year#off the back of trying to ban trans kids from sports teams that match their gender. awesome awesome awesome.#<- the letter was him SUPPORTING trans kids so although ive never thought of him as 'on my side' this is deeply disappointing#getting psychic damage from it being posted abt on the utah subreddit.#hrt for trans kids is completely irreversible and should only be done when theyre adults! and regular puberty is. um.. also irreversible..#come the fuck on.
4 notes
·
View notes
Text
Self-Made Man
Summary: A Trans!Tony Stark AU.
(Lengthy, personal author’s note below the cut, if you’re interested.)
Natasha Marie Stark was born twelve minutes before midnight on May 29th, 1970. She weighed a healthy seven pounds and two ounces when she arrived.
She was the most beautiful thing that either of her parents had ever seen.
And she was screaming loud enough to scare the pigeons from the trees outside.
Read on AO3
Well, hey everyone. It’s been a handful of months since I’ve been on here. I want to apologize for being gone, but that feels kind of phony. I don’t know. I missed this, though. I can tell you that much. I still checked my notifications every once in a while. It made me really glad to see people still commenting on my fics or passing my links around. Love y’all.
I guess it’s about time that I tell you that I’m trans. I have been this whole time. To answer a few quick questions, I first knew sometime in late high school, but it was always kind of in the background my whole life, I just didn’t know how to isolate the feeling. I started socially transitioning (i.e. dressing male, coming out, going by he/him) after my high school graduation, and I started HRT (Horomone replacement therapy, that means I inject myself with testosterone weekly. .33mL subcutaneously into my tummy, if you’re curious) on Oct. 12, 2018. So it’s been almost two years since, and I’ve been completely passing as a man for quite a while. Ass-crack hair, sweat, and all.
This is a pretty personal fic for me, given the nature of it. I’ve wanted to write it for a long time, and I’ve actually had words in the Google Doc since January. It took a lot of long nights to write. It helped that I was back home. I always have an easier time tapping into Trans Emotions when I’m in my home town, for better or for worse. All the memories and relationships I formed pre-transition follow me like ghosts.
I’m leaving for college in two days, conversationally.
I see a lot of trans!Peter Parker fics. I’m not dissing them, I love them to bits. But it makes me wonder why fandom is so quick to headcanon Peter as trans instead of one of the other characters. He’s petite, has a higher voice, and has softer features than the other male cast members. I feel like those attributes definitely play a role. It can be easy to see trans men as “uwu soft bois”, or as Men Lite, or as a more palatable version of “normal” (that is to say, cis) men. Those ideas are often flawed and based on transphobic foundations. The reality is, trans men (and by extension, all trans people) have the ability to be indiscernible from their cis counterparts. Everyone likes to think they can pick trans people out from a crowd, but you’d be surprised how quickly I started being read as male. Androcentrism for the win, I guess.
I won’t be entirely pessimistic. I understand that people my age project onto Peter (I am by no means exempt from that), and that there’s a greater number of young trans people than old, due to a series of depressing reasons. But I still wanted to try a different take on a trans character.
My experience as a trans man is vastly different than the one I write about here. If anything, I’m closer to fandom’s idea of trans!Peter. My parents were accepting, I had the financial and social means to transition relatively early, and I can fly under the radar easily. The most important difference is the time period.
I don’t know a lot about the trans experience of the 80s and 90s, which is what Tony would have gone through. I know of one single trans man who began his transition back then, one of the gender studies professors at my university. Even then, he’s from Canada, which I’m assuming has an entirely different culture around trans lives. There aren’t many older trans men. It’s depressing. There’s a lot of reasons for this. I don’t want to get too deep into them, because it only makes me feel sad. The final scene in this fic is extremely self-indulgent with regards to this. I wrote what I needed to hear.
That’s not to say I don’t relate at all to what I wrote. There are themes that are almost universal for the trans experience. I hope you can parse those out here.
I also wanted to talk about how I showed the change from “Natasha” to Tony. In the early stages of this fic’s development, I wasn’t sure if I wanted to openly say Tony’s deadname (the name trans people are given at birth, and often, but not 100% of the time, change as a part of their transition), but I soon realized that it would make the story much clearer with the inclusion of it. If you’re wondering, I got the name from Earth-3490, where Tony is born a woman (and marries Steve, lol). I chose to show the change between the two with the use of past tense for the first half of the fic, and switching to present for Tony’s life. Often times, it feels like that when you transition. You start living in present tense.
I also want to make it clear that transitioning isn’t as simple as shown here. From the beginning of mapping out this fic, I was stressed about “Oh, how will he be able to graduate as Tony if he doesn’t start transitioning until after he gets to college,” and “How will Howard react to him coming out?” and “How will he have a playboy persona if he isn’t able to have sex with someone without them knowing?” and a zillion other ideas. It was very freeing for me to let go of some of these obstacles and leave it up to the reader to decide. I alluded to some of the solutions that I came up with, but for the most part, I glossed over the paperwork and bureaucracy aspect to transitioning. But in real life, there are countless red tapes you have to cut for even the simplest of actions. I went to the state court to change my name and sex in March of 2019, and I still have cards in my wallet with my deadname. I had a consult with a plastic surgeon for top surgery (the colloquial name for the double mastectomy that trans men often go through to masculinize their chests. If you’re wondering, genital reconstruction surgery is normally called bottom surgery to mirror this) last December, and I still don’t have a date set. It took me a few months to start T, and I only got it so easily because I went through my unviersity, which does informed consent. Some places have to have proof of 6 months of social transitioning and a letter from a therapist. There is a lot of medical gate keeping in the trans community. I don’t know what I would have done had my parents not been accepting enough to help me through the processes. I am extremely thankful for their support.
But it’s a lot easier to write about transition happening smoothly. Money helps, which I don’t touch on a lot in this fic, but oh my God, does money help. I’m lucky enough to be able to afford my ~$20 a month T prescription (which I will be taking until the end of my days, likely), and I’m in the process of saving for top surgery. Thankfully with Tony, I can just presto most of the problems away because he’s canonically a billionaire. Eat the rich, folks.
There’s also the intersection with race that is very impactful for trans people, as it is for everyone. Both Tony and I are white, which gives us societal privileges that trans people of color don’t have access to. As well as the fact that transitioning from female to male is a much different experience than transitioning from male to female. We don’t experience trans misogyny, which is a special kind of misogyny specifically related to trans women. (Think of old sitcoms where the joke is that it’s a man dressed in women’s clothing, and that’s what makes it funny. That’s a fairly tame example of trans misogyny. It gets ugly fast.)
I’m veering dangerously off-topic, but it’s important to talk about. It’s easy for white trans people (and LGBT people as a whole, I suppose) to distance themselves from talking about white privilege or male privilege because they aren’t straight and/or cis. But it’s important to recognize that while we may face unique oppression, we also still benefit from historical white supremacist and patriarchal structures present today in society.
Sorry, not sorry for getting political. And if I haven’t said it on here, Black lives matter. Of course.
If you end up having trans-related questions, I want to be a resource for you. Seriously, I’m narcissistic and love talking about myself I don’t mind helping you understand the trans experience. I can’t promise that I know everything, but I also have my own group of trans friends who might know what I don’t, and we can learn together.
Again, love y’all. Thank you for the continued support you give me. I can’t promise that I’ll go back to my normal level of activity on here, but I might dip my feet back in the pool. <3
#irondad#iron dad#spider-man#iron man#trans#ftm#art speaks#art writes#read under the cut if you want to know my Emotions and Feelings
38 notes
·
View notes
Text
The Art Of Trying To ‘Pass’ As Female (My MtF~HRT Research)
Just as Krista described her need to change her face in order ‘just to leave the house,’ most of the 28 patients with whom I conducted interviews and observations, and the many others with whom I shared casual conversations, explained their desire for facial transformation in order to carry out everyday activities. As much as patients might want to be beautiful women after surgery, their primary desire was to walk through the world being recognized as women—which, in a sense, meant not being recognized at all. But just as physician discourse often conflated or collapsed the biological category of the female with the aesthetic category of the beautiful when describing the aims of feminization, so too did patients draw on both of these notions when communicating what their goal of being a woman actually means.
Woman is difficult to define as a surgical category precisely because it is difficult to define as a social one. Not surprisingly, patients had different ideas (and ideals) in mind when they imagined the kinds of transformations that would allow them to be the kind of women they wanted to be. When I asked Rosa if she had a particular idea of what she hoped to look like after surgery, she immediately said, “Yes,” and reached into her bag. She pulled out a stack of papers wrapped in plastic sleeves and held together by a binder ring. She shuffled through the stack, unfastened the ring, and put a page on the desk in front of me. There were three photographs that had been clipped from magazines and pasted to a sheet of white paper. As she began to talk I was not sure which one I was supposed to be looking at. “I want to look like a woman,” she began. “I want a face that a man falls in love with. Like an angel. Innocent. You are a man. You understand. Look at her [pointing to an image on the page.] What do you feel? Body is nice, but look at her face. In that picture you can’t see her breasts, but you can see her face. She’s beautiful. You feel inside something like love. I want a face that a man sees and it makes him turn red.” Rosa was not sure what her particular features would be when all was said and done. She did not expect Howard to replicate the model’s face onto hers. She did, however, expect that her face would be one that would do something for others and, in turn, do something for her. Rosa described the changes she was after in terms of how particular aspects of her face evoked gendered attributes.
When our conversation turned from the effect she desired to the precise means of achieving that effect, she gave an inventory of her face and the multiple ways that it works against her. The bone above my eyes gives me an aggressive look. I have dark, shadowed eyes. If you see that actress Hillary Swank, she has this. Something doesn’t match on her face. Nose, obviously. My nose is male. Upper lip. I can’t wear red lipstick. If I wear read lipstick it makes me look like a man in a dress. When I watch videos of myself, my expressions never look happy. I look angry.
Rosa was confident that following surgery she would ‘feel more sure of [her]self.’ It was this confidence that made women beautiful. Just something about them that had such power and sex appeal. Women, in her telling, were not aggressive or angry; their faces are built to be adorned. Though she knew that Howard could not necessarily make her beautiful, she was confident that he could make her a woman. For her, that was enough.
Gretchen had much more modest desires. Her hopes for surgery were less about eliciting a particular response, than avoiding a reaction altogether. Just…I hope that I won’t have this kind of jerk that was sitting just to my left on the plane this morning who was seemingly horrified by seeing this (gestures to her face and body). He was probably having the idea that I was fantasizing about him or something. I just hope that next time, he won’t think about it twice. ‘Yes, I’m sitting beside a girl. So what and that’s all.’ End of story.
Pamela expressed her desires this way: I'm doing it (having FFS) so I will feel that I "pass" (making air quotes). Whatever that is. And of course the operative word there is ‘feel.’ I'm tired of thinking, is that person reading me? No? Well how 'bout that person? I want to think about something else as I walk down the sidewalk.... Like, say, what a nice dress in the window. Maybe that's it. Going unnoticed is a thing that most people take for granted.
Erving Goffman (1963) called those who do not draw unwelcome attention from their bodily appearance ‘normal’s.’ Normal’s, Goffman argues, simply cannot understand how it feels to be the object of derisive looks and hostile attention from complete strangers. To be a member of a stigmatized group is to be the object of distain. When some aspect of your physical body is the source of that stigma, there are, according to Goffman, two possible responses. You can come to terms with the fact of your stigma and attempt to ‘normificate’ it by acting normal, as though the stigma did not exist. Or, you can normalize it by making a conscious effort to correct it. Though ‘norming’ surgeries are sometimes the objects of ethical debate, the validity of the desired outcome is hard to dispute.
In an article entitled, ‘Self-Help for the Facially Disfigured,’ Elisabeth Bednar put the matter simply. Whether we are shopping, riding the subway, or eating in a restaurant, all of which are casual day-to-day social encounters, there is the initial stare, then the look away, before a second, furtive glance inevitably puts the beheld immediately in a separate class. For those who experience this discrimination, the question of the moral justification of surgery to increase societal acceptance...
She pointed out photographs in Howard’s book in which surgery did not necessarily improve a patient’s attractiveness, but it did change her sex. When referring to before and after photographs she said, “See this is an ugly boy and this is an ugly girl, but it is a girl. Other doctors can’t do this.”
There can be no greater wish than to melt into the crowd or to walk into a room unnoticed (Bednar 1996:53). The patients and surgeons with whom I worked, referred to the fact (or fantasy) of going unnoticed as ‘passing.’ The language of passing is contentious for some transpeople because it can be read as implying a sort of deception; being taken as a member of a group to which one does not really (where really refers both to an ontological truth and to the rightful membership based on it) belong. This deception is also often marked by a supposed opportunism; passing is really only considered as such when a person passes from an undesirable group and into a desired one (Gilman 1999). It therefore frequently carries a connotation of a strategy to access particular forms of privilege. Many transpeople object to the language of ‘passing’ because, they argue, to say that one passes as a woman is to acknowledge that woman is not a category to which she rightfully belongs.
As Julia Serano insists, “I don’t pass as a woman. I am a woman. I pass as a cis-gendered woman” (by which she means a woman who has never changed her gender). These sorts of concerns about what it means both politically and ontologically to pass, were only voiced by two of the patients with whom I spoke. Despite their reservations, they, like all other patients I met, held the desire to pass as an incredibly important and explicitly stated aim. As historian of medicine Sander Gilman explains, ‘The happiness of the patient is the fantasy of a world and a life in the patient’s control rather than in the control of the observer on the street. And that is not wrong. This promise of autonomy, of being able to make choices and act upon them, does provide the ability to control the world. It can (and does) make people happy’ (1999:331-2).
Like language, social roles do not exist in isolation (Wittgenstein 1953:§243); they are by definition shared properties conveyed between people in given social group. A person’s individual conviction that she is a woman is not enough to maker her a woman in any social sense. To be a woman requires not simply the conviction that one is a woman, but the recognition of that status by others.
FFS is a surgical recognition that how one feels about and lives their sexed and gendered embodiment is not a private, psychic reality, but is the product of social life, of living with others. Passing is not a subjective act; it is a social one. Nearly all clinical literature as well as most popular literature on transsexualism suggests that transsexualism is a property (and problem) of an atomized and bounded individual. This focus on the individual and psychic nature of the bodily dissatisfaction that characterizes transsexualism is named explicitly as well as through the invocation of metaphors of isolation, internality and invisibility. While an individual body may be the site of the material intervention, the change enacted in FFS takes place irreducibly between persons. The efficacy of FFS is located not in the material result of surgery itself, but in the effect that the surgical result will produce in the perceptions of imagined.
Other writers argue that the goal of ‘passing’ not only obscures but effectively forecloses any possibility of a trans- specific radical political subjectivity (Bornstein 1994, Green 1999, Stone 1991). These writers insist that living as out trans-people is the only way to call attention to the oppressive gender system that devalues and delegitimizes trans-lives and bodies, among others. This kind of visibility can come at the great cost of personal and emotional safety, leading to a conflicting desire to be a part of the solution while maintaining ones safety and sanity (Green 1999). Perhaps nowhere is this made clearer than in the imaginary scene through which Howard explains the goal of his surgical work:
If, on a Saturday morning, someone knocks at the door and you wake up and get out of bed with messy hair, no makeup, no jewelry, and answer the door, the first words you’ll hear from the person standing there are, “Excuse me, ma’am….”
This incredibly powerful scene was a staple of Howard’s conference presentations, and was repeated in slightly altered and personalized forms by many of the patients who had selected Howard as their surgeon. Through this turning outward—and the making of femaleness at the site of the exchange with a stranger—FFS reconfigures the project of surgical sex reassignment from one rooted in the private subjectivity of the genitals, to one located in the public sociality of the face. Time after time, patients told me that their primary desire was to go through their daily lives and be left alone, without thinking about what others may see when they look at them.
Krista rode the city bus on the day before our interview. On that day, for the first time in recent memory, she did not prepare extensively before leaving the house. “I didn’t have to worry about having my bangs just right, or having just the right pair of glasses on. I just got on the bus and thought, ‘Wow, this is cool.’” Although her face was covered in bandages, sutures, and bruises, and people on that bus were undoubtedly looking at her, Krista found joy in the certainty that whatever they might have seen when they looked at her, the did not see a transwoman. The stuff of her maleness was gone. It was a novel—but so, so welcome—experience. It is important to remember that the stakes for passing are often quite high, often quite serious. The desire to pass does not only exist for the gratification of personal goals, but also achieves a mode of physical and emotional safety. It is crucial to remember that trans-people are disproportionately incarcerated, unemployed, and lost to suicide and other violence. I make this point not to hold counter discourses hostage to its message— as in an accusatory stance from which any divergence is a de facto support of transphobia or worse—but to tell the complete story of the context in which these procedures become objects of desire, and accomplish practical goals sometimes on the measure of life and death.
THE FULL FACE
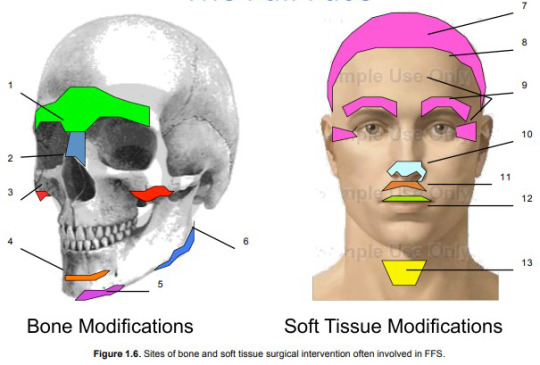
Facial Feminization Surgery includes interventions in both the bone and soft tissues of the face. In general, the procedures involved in FFS are aimed at taking away or reducing particular features of the bones and soft tissue of the face. This focus on reduction and removal is based on a fundamental assertion that males are, on the whole, larger and more robust than females.
This assertion applies both to the bony skeleton and to soft tissues such as skin and cartilage. Whereas the modification of the facial bones are guided, at least in Howard’s case, by numerical norms, most soft tissue procedures are not. (The exceptions are the height of the upper lip and of the forehead; these assessments are guided by numbers and measurement). Instead, soft tissue procedures are often oriented toward and aesthetic ideal of feminine attractiveness.
Below are brief descriptions of the surgical procedures organized under the sign of Facial Feminization. Not every patient undergoes all of the procedures described here, though some certainly do. In Dr. Howard’s parlance, a patient whose surgery includes all of these procedures gets, ‘The Full Face.’
While one of the fundamental goals of this dissertation is to trouble the claims to absolute difference that often animate FFS, in the following descriptions I make use of the dichotomous distinctions that doctors use when characterizing the masculine features of patients’ skulls.
Bone Procedures
Brow Bossing and Frontal Sinus:
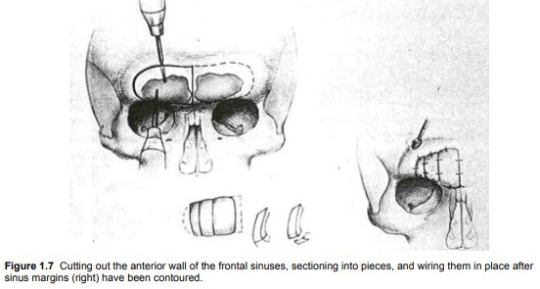
The prominence of the brow is one of the most distinctive and recognizable aspects of a masculine face. Some reduction of the brow can be accomplished through burring down the bossing (the thickness of the bones) just above the eyes. In other cases the anterior wall of the frontal sinus (the empty space just above and between the eyes) is removed (“unroofed”) and set back. The reduction of the frontal sinus is considered the most aggressive of all procedures involved in Facial Feminization Surgery (see Figure 1.7).
Rhinoplasty (internal reshaping of the nasal bones):
Rhinoplasty involves the fracturing of the nasal bones as well as the removal of cartilage. More radical bone fracturing and removal is required when frontal sinus reconstruction is performed. When the forehead is ‘set back’ through this procedure, the bones at the nasion (the depressed area between the eyes just superior to the bridge of the nose) must be reduced in order to create the desired relationship between forehead and nose.
Malar (cheek) Implants:
In order to produce the desirable oval shape of the female face, implants may be placed over the malar bones to enhance the fullness of the cheeks.
Genioplasty (chin shortening):
Based on the claim that female chins are shorter than male chins (as measured from the top of the bottom teeth to the most inferior point of the chin), a wedge of bone can be removed from the chin, and slid forward. Moving the bottom section forward also results in creating a more pointed chin.
Reshaping mental protuberance (chin):
A pointed chin is recognized as feminine, whereas a square chin is masculine. In combination with the advancement of the inferior portion of the chin, contouring is also done to enhance this characteristic.
Reduction Mandibuloplasty (jaw bone):
Alterations of the mandible focus on the undesirable squareness of the masculine jaw. This squareness is attributed to two aspects of the mandible: mandibular angle and mandibular flare. The mandibular angle describes the angular value of the posterior and inferior portion of the jaw. The more acute the angle, the more masculine the jaw. This is best seen from profile. Mandibular flare describes the extent to which the squareness of the jaw extends toward the lateral sides of the face. This squareness is best seen when looking at a person from the front. In both cases, bone can be removed in order to reduce the appearance of masculine squareness.
Soft Tissue Procedures
Scalp advancement:
By severing the tissue that connects the scalp to the scull, the scalp may be brought forward toward the face to help a patient compensate for a receding hairline. Excess tissue at the top of the forehead is excised. Scalp advancement as well as hairline reshaping and eyebrow raising all occur through the coronal incision (from ear to ear just behind the hairline) required to alter the bony contours of the forehead.
Hairline Reshaping:
In addition to bringing the hair-bearing scalp forward, the hairline itself can be reshaped. In this procedure, the M shaped male hairline is rounded out to reduce (if not eliminate) temporal baldness caused by a byproduct of testosterone.
Eyebrow Raising/Crow’s Feet Reduction/Forehead lift:
As noted above these procedures are performed at the site of the coronal incision after the bone work on the forehead has been completed. When tissue is excised during scalp advancement, the position of eyebrows is raised up higher on the forehead. This is described as a feminine characteristic. The appearance of the eyebrows is also changed as a result of the changes to the bones of the brow and forehead beneath them. The pulling of the skin of the forehead generally produces the addition (and typically considered beneficial) result of eliminating the wrinkles around the eyes often called crow’s feet. During this procedure, surgeons have access to the internal muscles of the forehead and may choose to perform a perforation of those muscles; this procedure is typically referred to as a forehead lift.
Rhinoplasty (reshaping of the cartilage and tip of the nose):
The tip of the nose is given its shape by internal cartilage. After the bone modifications have been made, the cartilage can be reshaped in order to achieve a ‘more feminine’ nose.
Upper lip shortening:
According to the surgeons with whom I worked, males have a longer upper lip (distance between the bottom of the nose and the vermillion part of the upper lip) than do females. This distinction can most easily be seen by observing how much of the upper teeth are visible when a person’s mouth is slightly open. This measurement is referred to as ‘tooth show.’ The length of the upper lip can be reduced by excising the desired amount of tissue just beneath the nose, raising the upper lip toward the nose, and applying sutures in the crease just at the base of the nose. This also results in increasing the amount of vermillion visible in the upper lip.
Lip Augmentation:
Lips can be augmented through a variety of procedures including the injection of pharmaceutical products (such as Botox and Restylane) or fat taken from other sites in the patient’s body. More permanent augmentation can be achieved by placing some of the tissue excised during the scalp advancement into the tissue on the underside of the upper lip.
Reduction of the thyroid cartilage (“Adam’s Apple”):
The Adam’s Apple—or more properly, the thyroid cartilage—is considered to be one of the clearest indicators of maleness. Thyroid cartilage removal is often referred to as a Tracheal Shave (or just trach shave) despite the fact that it is neither the trachea being altered, nor a shaving motion used to reduce it. While a relatively simple procedure, the thyroid cartilage reduction carries significant risks. An inexperienced surgeon may remove more tissue than necessary, and inadvertently alter the site where the vocal chords insert. This can result in a radical modification of vocal pitch.
CLINICAL EVAL
Clinic One -- Dr. Howard
Upon entering his office from the hospital corridor, one enters a warm but unremarkable waiting room: carpet and walls in shades of neutral brown, upholstered armchairs separated by low coffee tables offering a selection of news and fashion magazines.
In addition to personal and administrative offices, the practice has three small examination rooms, each equipped with a large examination chair (somewhat like a dentist’s chair, it defaults to an upright but gently reclining position), a rolling stool (on which Howard sits during most of the exam), a small side chair (where I sat while observing exams), and a counter at the back of the room that contains a hand-washing sink and a light box for illuminating x-rays.
There are few decorations in the exam room dedicated to initial consultations and pre-operative appointments. To the right of the patient seated in the exam chair, a silver and bronze toned image of a naked and reclining woman hangs on the wall. Her long hair flows down her back and shoulders but leaves the side of her breast exposed. On the wall facing the patient—and so behind Howard as he conducts the exam—is a magazine rack that holds several fashion magazines.
When I entered the room, Tracy was seated in the reclining exam chair, hands folded in her lap and looking nervous. Howard urged her to keep her seat as I introduced myself and shook her hand. With Tracy, as with all other patients whose consultations I observed, Howard began the appointment with a few minutes of friendly conversation. He inquired about the Canadian city in which she lives. As a person who has done a considerable amount of traveling throughout the world, Howard often has a personal story to tell about the patient’s hometown.
Though he tends to speak rapidly as a norm, these exchanges do not seem to me to be perfunctory or rushed; people’s stories sincerely fascinate him. After having seen this routine enacted a number of times, it is clear that Howard uses these first moments to establish a friendly rapport with new patients who are frequently very nervous—and in some cases could be best described as star struck. While this moment may be the culmination of many months or years of a patient’s personal and financial work, for Howard, this is another day in the office.
After the brief exchange of pleasantries, Howard moved into questions about Tracy’s medical history: height, weight, medications, prior surgeries, and so on.
When Tracy stated that she was actively losing weight and would like to get down to 180 pounds, Howard made his first recommendation of the appointment. “I’d like to see you down to 160,” he said. “The best results I see—not surgically but in terms of overall femininity—are in patients who get down to a female weight for their height. When you get down to 180, just keep on going.” While completely unrelated to the craniofacial surgical consultation underway, Howard’s recommendation on “overall femininity” signaled his understanding of FFS as both part of a larger goal of corporal feminization, but also as just one part of achieving that goal. In addition to signaling a holistic understanding of the project that brought Tracy to his office, this shift from conversation to recommendation marked the beginning of the exam; he is the expert with information to give.
Howard did not ask why Tracy was in the office to see him. He did not ask what her goal was for surgery. He assumed in Tracy’s case and in all other consultations I observed, that a person whose paperwork indicates that she has come to the office for an FFS consultation is doing so because she wants to have her face reconstructed to take on female proportions. I have not heard this assumption corrected. It is with this assumption that directly following the medical history, he began making measurements on Tracy’s face.
Clinic Two -- Dr. Page
Page’s office, located in an office park in an affluent suburb of a major West Coast city, shares a building with accountants, attorneys, and dental offices. The Ambulatory Surgical Clinic where he performs most of his operations is attached to his office, though it has a separate entrance at the back of the building. In the waiting room, leather armchairs and a long couch are arranged around a low coffee table covered in fashion magazines. The walls are covered in an ivory-toned wallpaper that in combination with the light coming in through a large window makes the space bright, though somewhat impersonal.
The dominant feature of Page’s waiting room is a mirrorbacked, top-lit curio cabinet featuring branded cosmetic products such as Juviderm and Botox, the presence of which makes it impossible to forget that this is not a neutral space; there is something for sale here. The reception desk is located in the front waiting room and is staffed by a few different young women.
On two occasions the stillness of their faces and the shape of their lips have made me quite aware that they have ‘had some work done.’
The two exam rooms in Page’s office are considerably larger and more brightly lit than those in Howard’s office. Here too, the reclining exam chair is the largest and most central object in the room. A small chair (where I sat during observations) is positioned just to the right of the exam chair, and a full-length mirror hangs on the wall next to it. A counter with a small sink occupied the left wall of the room. A model of a human skull sat on the counter, looking directly at the exam chair. When Page invited me in to observe the consultation, Leanne was seated in that chair.
Leanne was one of the few patients I encountered during my fieldwork who arrived for an FFS consult in what was referred to in both offices as ‘man mode’ or ‘male mode.’ She had taken the opportunity to visit Page’s office while traveling through town on business and looked every bit the businessman: short-cropped sandy blond hair graying at the temples, a crisply pressed pale blue shirt, navy blue necktie, grey trousers and black oxford shoes.
Page habitually opens the conversation by asking patients how they heard about him and his practice. This sets the tone that the patient is a consumer who has shopped around, and it helps to identify him as a businessman who is eager to grow his practice. After a bit of small talk about Leanne’s hometown and learning that this was her first visit to the region, Page began the exam not by taking a medical history, but by prompting a personal conversation.
“Tell me about yourself, about your transition.” An examination is frequently understood to consist of two parts: the history taking and the physical examination (Young 1997:23). It is immediately clear that though Howard and Page each ‘take a history’ from their patients before beginning the physical exam, what constitutes relevant history is different for each of them. Howard asks his patients about what are traditionally understood to be medical issues: their height, weight, current medications, previous surgeries, and overall physical health. This information helps him to assess whether the patient is physically well enough to be a candidate for surgery. It also signals that his primary interest is in the physical properties of the patient’s body, an interest that is born out in no uncertain terms in the examination that follows.
Page, on the other hand, does not ask such questions of his patients during their initial appointments. Instead, he elicits a ‘history’ of the patient’s feelings about herself and her transition, more generally. Because the appointment begins with the disclosure of personal—and often quite emotional—information, the examination that follows is framed as one directed toward the realization of personal and emotional goals more than physical ones. As the consultations progress, the distinctions between Howard and Page’s approaches become clear. Howard’s meeting with Tracy appears in the left-hand column below. Page’s meeting with Leanne appears on the right.
Clinic One -- Dr. Howard
Howard: “Now I’m going to take some measurements and we’ll look at your x-rays.” Howard washed his hands and came back to sit down in front of Tracy. She was sitting in the exam chair and he rolled up to her on a small, wheeled stool. He took a small white flexible plastic ruler from his coat pocket and measured the distance from the cornea of her eye to the most forward prominence of her forehead. “Your brows are down a little bit.” He felt the brows and temples on both sides of her face using both hands. He pressed the sides of his thumbs up under the bones at the top of her eye sockets in order to get a sense of the shape of the bone. “Look at the top of that light switch.” Howard directed Tracy’s attention to the switch on the wall directly in front of her. Looking at this object helped to make her head level. “Open your mouth just slightly.” Howard measured the distance from the bottom of Tracy’s nose to the inferior ends of her front teeth. “Bite down on your back teeth.” Howard bit exaggeratedly on his back teeth to show her what he meant. Looking away, he felt the muscles on either side of her jaw with his hands. He turned to me and explained to the patient that we had been talking earlier about how he decides whether or not to remove some masseter muscle when he does jaw tapering.
Talking to me: “She has a fairly prominent jaw, but the muscle is not that large. I won’t even consider removing any muscle on her.” Howard runs the pad of his thumb up and down the center of Tracy’s throat. “Have you got one of these things?” Settles on the patient’s Adam’s Apple.
Howard: “If you have this done by someone else don’t let them put a scar at the middle of your throat.” Tracy lives in a country that has a national health service and Howard makes explicit reference to this since he knows that by using that service Tracy could save a considerable amount of money on this procedure.
Howard: As he describes the potentially problematic placement of some other surgeon’s scar, he draws a line across her thyroid cartilage with his index finger to mark the cut. “If I do it I’ll put the scar up here…” He draws his index finger just under the point of her chin to indicate where he would place the scar. …so no one can see it. “Plus if you put the scar here [in the middle of the throat] it can stick to the cartilage and then it moves every time you swallow. It looks like the dickens. Let’s look at your x-rays.” Howard walks to the light box behind the exam chair and invites Tracy to join him. They stand shoulder to shoulder in front of the light box looking at the cephalograms that Tracy brought with her to the exam. “First I look to see that you’re brushing your teeth, and it looks like you are (laughs). When I was measuring here before…” Uses his finger to show the measurement he took from the forehead to the cornea. “…I was looking at the maximum prominence of your forehead to the cornea of your eye. In you it was 15mm, which is average for a male of your height. As far as I know, this measurement is not taken anywhere else in the world. It is not a standard measurement. Once I am in there and I begin to contour the forehead, I can’t tell where I am. This measurement helps me locate myself in space.” By this he means that because the cornea does not move as a result of any bone reconstruction in FFS, he can use it as a constant reference. He took a handheld mirror from a small drawer and handed it to her. She sat, holding the mirror, looking at her face as he spoke.
Tracy is being educated about what Howard will do and why it is the best approach.
Tracy: “How far can you go back?”
Howard: “The most I’ve gone back is 9mm.”
Tracy: “Let me rephrase. How far can you go back safely?”
Howard: “I could go all the way back here.” Pointing to the posterior wall of the frontal sinus on the cephalogram.
Tracy: “What happens to the sinuses?”
Howard: “They go away. As far as we know.” He indicates with his fingers where the sinuses are located on the cephalogram. “…is to reduce the weight of the skull. Now, the jaw.” Howard looks at Tracy’s jaw, and then down to the x-ray. “Do you grind your teeth?”
Tracy: “I know I used to.”
Howard: “You’ve got some wide angles here. Feel your jaw.” He places Tracy’s hand on her jaw. “Feel how it flares out? We can get rid of the bowing that males have in the mandible that females don’t have.”
Tracy: “How do you do that?”
Howard: “We use a bur instrument on the sides here…” Indicating anterior portion of the lateral mandible on his own face. “…and then we have an oscillating saw that we use to take out the larger parts of the bone here...” Indicating posterior section on his own face.
Tracy: “You actually take out parts of the bone?”
Howard: “Yeah.”
Tracy: “Okay.”
Howard: “Can I borrow a finger?” Howard reaches down and grabs the index finger of Tracy’s left hand. He places it on the side of his face in the medial section of his mandible. “Feel my teeth?” He presses her finger into his cheek and moves it back and forth so she can feel the texture of the bone below his bottom teeth. “Feel that ridge? That is what we take away. For some people, a thin layer of blood that forms on the bone becomes bone. I am one of those people. I was hit in the head with a golf ball when I was 13 and I got this big bump.” He feels the bump on the top of his head. “I’ve still got the bump because the blood that formed there turned into bone. If you look at an x-ray you can see it plain as day. If you are a person like that—and I don’t know how to know that in advance—it is possible that some of that ridge may come back. But it won’t all come back. The chin. I measured from the top of your bottom tooth to the end of the bone and that is 50mm. That is average for a male of your height. I want to take out 8 mm of chin height. I can’t do that by shaving it off the bottom, because then the muscles and tissues that attach to the bottom of your chin have nothing to attach to and they just sag down. Instead, I take out a wedge of bone that is 8mm thick, and stabilize the bone with titanium plates and screws.” Howard explains that medical grade titanium comes from recycled Russian atomic submarines. He makes a joke that the addition of this Russian material may make Tracy fond of vodka after surgery.
Tracy: “You cut a wedge out of the bone and then rotate it up?”
Howard: “Yeah. Have you seen my book? Maybe you want to buy one. There is a lot of information in there about all of this stuff. And some stuff that you don’t need. It can answer a lot of questions. We want to get ride of the sublabial sulcus at the base of your chin. I think of this as a very male feature. Now, what to do. The brow. Right now the distance from your brow to your hairline is 7cm. I want 5.5cm. The average male has a distance there of 5/8 of an inch longer than the average female. This is the case in 16-year-old males, even before they’ve experienced hair loss. You have a type III forehead. We talked about that. We’ll do your nose—if we do the forehead we have to do the nose. Do you remember Dick Tracy? His nose went straight out like a shelf? You probably won’t like that. Upper lip. Now your upper lip has a vertical height of 2.5mm and drops 2-3mm below your upper teeth. If you look at me when I talk, you don’t see my upper teeth unless I smile. He smiled to demonstrate. Women show their upper teeth when they talk. We’ll want to move you up to get some good tooth show. So. We’ll do your chin, your lower jaw, the thyroid cartilage. If I do all this at one time—and most patients choose to do that because it saves them a lot of time—I know this will take almost exactly 10 ½ hours.
Tracy: “Everything?”
Howard: “Yes”. Howard went on to describe the risks associated with these surgeries, the recovery process, and necessary preoperative preparation. When he’d answered Tracy’s questions, he led her down the hall to talk money with Sydney.
Clinic Two -- Dr. Page
Leanne: “I began dealing with my gender issues at 50, when my wife and I became empty nesters. I have already been cleared for hormones but I am waiting to take them until after my daughter’s wedding in a few months. I am a manager—I mean, that is what I do for a living but that is also who I am. I like to have everything figured out before I start. That is why I am here. I don’t really know how hormones will affect me and what changes they might make to my face, but I do know that the face is the most important thing to me. I can do things with clothes, but I can’t hide my face.”
Page: “Making changes to your face can make you more feminine appearing.” As she spoke, he sat quietly, almost motionless. Like a practiced interviewer, he allowed her short silences to linger unfilled, and it turned out that she had a good deal to say.
Leanne: “I know that if I proceed with this my marriage will be over, and I understand that. My wife didn’t really sign up for all of this and I can’t force her to feel better about it. I am here because I want to manage my expectations; I need to know realistically where I might end up, instead of going forward with all of this and then finding out that you can’t do what I think you can do. I don’t want someone to give me all of the classic female things. This is a clear reference to Howard’s approach. I was interested in talking to you because you said that you work with features not totally remake them. It is not a clean slate. Given the face that I have, I want to know what to expect. Right now, I don’t look like a woman; I look like a man in a wig. I haven’t gone out much; I only wear women’s clothes when I go to counseling. But when I go out I worry about my face. I just don’t want to attract attention. I want to fit in.” Page did not verbally respond to any of Leanne’s personal and emotional disclosures; he simply began the physical assessment of her face.
Page: “We’ll start at the top and work our way down. These are only suggestions, to let you know what is possible, and how I think of things. We think of the face in three sections: forehead, midface and lower face. One of the most feminizing effects happens in the forehead. We can move the hairline forward. Bone work is required to make a feminine skull.” Page rolled his stool backward to retrieve the model skull sitting on the counter behind him. He held the skull in his left hand and used the index finger on his right hand to show Leanne how the frontal bone could be reduced. “By burring down this area [above the eyes] instead of removing the bone, we can retain the angle from your forehead to your nose. Patients with ‘the works’ often look worked on. That is not what I want to give you. When you lose the natural transition from the forehead to the nose you don’t look good as a man or woman.”
This is a direct defense of his surgical approach against Howard’s more aggressive style. Page runs the pad of his thumb across the orbital ridge above Leanne’s left eye as she looks at her face in the mirror. “Reducing this will give you the feminine appearance. It gives you sex appeal. That’s the approach we’re going for. Passing as a woman takes more than what I do: it’s about hormones, behaviors, dress, makeup, voice. What I do is just one piece of the pie. Now, when I’m in doing the forehead contouring I can remove some frown muscle, which would be nice for you. At the same time I can take away the peaks at the hairline.” Page uses the wooden handle of a long cotton swab to trace along the temporal baldness of Leanne’s hairline.
Leanne: “I’ll need a wig anyway. I had hair transplants all through there but they failed.”
Page: “This dark space is the frontal sinus.” He points at the sinus on the x-ray using a yellow wooden pencil. “In my mind, the most desirable female forehead is convex horizontally and vertically; it is not vertical. I could take you back 8mm. The 15mm you currently are minus 8 equals 7mm. That is where I want you. If you had an x chromosome rather than the y you were born with, that is where you’d be. You got this…” indicating the brow prominence of the frontal sinus “…when you were 14, 15, 16 years old. You have what I call a type III forehead.” Explains how he’ll remove the frontal wall, and form patches to wire back into the exposed sinuses. “When taking out the frontal sinus you have two holes left: if you sneeze you make a bubble and if you sniff you make a dimple. That is good at the first cocktail party, but not the second. I take the bone I removed and make two small patches and wire them into place to close those sinuses. If someone just burred this down, they could only go about .5mm to 1mm.” This comment acknowledges the common approach by other surgeons to burr the bone rather than unroof it. It is both descriptive and defensive.
Page: “Okay. Your nose is really necessary to do. We can take the hump out of the dorsum and decrease the projection some. The upper lip could be shortened. That is really common in feminization surgery. It’ll be like when you were younger.” Page presses the wooden handle of the cotton swab just beneath Leanne’s nose, causing her upper lip to rise on the surface of her teeth and allowing more tooth to show. “In terms of the jaw, I would leave it alone.”
Leanna: “Really?”
Page: “Beautiful women have a strong jaw line. For you, brow lift, cheek implants possibly to give you some more fullness in the midface, and nose for sure. If you’d like to see what this would look like, we can image you and give you a better idea of what I am talking about.” Page led Leanne to a small, dimly-lit room attached to the exam room. There was space for only two distinct positions in this room, so I observed in the doorway, looking over Page’s shoulder as he worked. Page was seated at a laptop computer equipped with a special trackpad that allowed him to move a stylus along the pad controlling the computer display. His laptop was connected to a digital camera mounted on an adjustable stand. Leanne sat at the opposite end of the room in front of a grey backdrop. Page took six digital photos of Leanne’s (non-smiling) face: (1) looking straight ahead at the camera; (2) turning her whole body such that her face is in ¾ view; (3) profile; (4) ¾ view facing the other direction; (5) opposite profile; (6) facing forward but looking straight up, a ‘worm’s eye view’. Page invited Leanne to pull her stool up beside his so that she could watch as he altered the photos he just took.
Page: “I try to do things with imaging that I can do during surgery so that it’s not unrealistic. One thing would be to decrease projection. Come over here and I’ll show you what I mean.” Leanne got up from her seat in front of the drape and sat beside Page in front of the computer. Using the stylus on the trackpad, Page selected the areas that he could reduce: frontal bossing, orbital bossing, and nose projection. He circled each of these areas on the profile image because this image produces the most noticeable contrast. Once these areas were selected, Page drug the stylus back and forth across the trackpad. As he moved from left to right across the pad, the nose, forehead, and orbital bossing all reduced in unison. As he moved back to the left, they ‘grew’ back to their original (current) size. Leanne watched this in silence for a few seconds. It was clear that she was not seeing all that she hoped to see. Page was quick to step in. “I am kind of limited in what I can show here. I mean, you have to imagine what it would look like once your facial hair is gone [she had a day’s growth of beard]. You’ve also got some skin damage that you should really work on. I’d say the most important thing you can do for yourself between now and any surgery would be to start a skin-care regimen. Work on that sun damage and some of the brown areas, the wrinkles around the eyes.” Page indicated these problem areas on the computerized image of her face. “I work with an esthetician right upstairs. I can set an appointment for you if you want. I really do think that is really important. You know, beautiful women have beautiful skin.”
Leanna: “Yeah, I spent almost 20 years in Arizona. I have a lot of sun damage.”
Page: “Here are some other patients I have operated on. Maybe these will give you a better idea of the changes I am talking about.” Page opened a file on the laptop with several pre-op and post-op images of his patients. He flipped through the images, describing the procedures involved. “Here you can see I did the nose…Here you can see the reduced bossing; that really opens up the eyes… Here you can see the difference that a brow lift really makes. She looks great…” This didn’t seem to alleviate Leanne’s sense of disappointment with her own images.
Leanna: “These people look much more feminine than what I see when we look at me. I have my wig with me. Can I put it on and you can take the pictures again? That might give us a better idea of how this is going to look.” She crouches down and pulls her wig out of her briefcase. It is a bit disheveled and needs brushing. Leanne does her best to place the reddish-brown shag cut wig on her head, but there are no mirrors in this room. In addition to the contrast produced by her businessman’s attire, the wig is not quite on correctly. To my mind, this photo session has just changed quite radically. Page appeared somewhat reluctant, but he agreed to take a new profile photo on which to make the digital modifications. One of the qualities that made the wig desirable is particularly problematic during the photo shoot: it obscures her forehead and brow.
Page: “Could you pull your hair back so I can see your forehead?” Page took the photo. Leanne resumed her seat beside him at the computer and watched as he made the same alterations to the new photo as he had to the previous set. The addition of the wig did not produce the effect she’d hoped for. Page reiterated the importance of starting a skin-care regimen and beginning electrolysis on her face. “I think those changes could make a big difference for you. Let’s go talk to my office manager, Hannah. She can give you a better idea about prices and we can look at some more images.” The pair left the room and began flipping through a photo album in Hannah’s office.
Leanna: “Do you think I could ever look this good? I’m worried about going through all of this and looking as ridiculous as I do now.”
It is clear from these two representative appointments that though these doctors punitively share a common goal—the ‘feminization’ of their patients—what ‘feminine’ means to each of theme is quite distinct. Their approaches to the project of ‘feminization’ determine both what each doctor identifies as the problematically ‘masculine’ and the desirably ‘feminine’ and how they do so.
SURGERY DAY
For most patients I interviewed, the anticipation of and preparation for surgery had given significant shape to their personal, professional, financial and emotional lives for many months. For others, many (many) years. By the time they’d made the trip to the surgeon’s office, they had come to think of Facial Feminization Surgery as the event that would mark the difference between the life they had and the life they wanted.
It would, they hoped, be the end of a deep longing for transformation. Structured by the future goal of surgery, for these patients the present had collapsed into a seemingly interminable time before surgery. It was a continuation of the past experience of bodily dissatisfaction and disaffection into the almost, the can’t wait, the before to which every day following surgery would be the after.
Dr. Howard pointed to a chair in the hallway outside his office. “I’ll walk by that spot at exactly 7:25am. If you’re there, you’re welcome to join me in the OR. If you’re not, you’re not.”
Patient: Rosalind
Rosalind, whose surgery is described in the interstices of this prose—had traveled from Wales to undergo surgery with Dr. Howard. When we met on the afternoon before her surgery, she was feeling very anxious. When I asked her about the source of her anxiety, she said that it was not the operation itself that worried her. Rather, she was nervous about the postoperative recovery period.
“I’m scared to death. A week before my plane ride I started praying for British Airways to go on strike. I saw a patient at the Cocoon House [Howard’s private recovery and convalescent facility, all gendered and natural metaphors intended] all bruised and bandaged and I’ve been walking around trying to think, ‘Why am I doing this?’”
Rosalind had hoped to make this trip five years before, but financial issues had delayed her plans. For her, as for all patients who shared their stories with me, arriving in this office was the culmination of a long process of self-discovery.
“At 25 years old my hair started to fall out and I thought, ‘Oh no! I haven’t decided whether I want to transition!’ I tried topical creams and things to try to keep my hair and I became pretty obsessed with it. Then I started thinking, ‘Wait, is the problem that you’re going bald or that you’re transgendered?’”
She began feminizing hormones in 1999, and hoped that their effects would be enough to ease the anxieties she had about her appearance. She was not ready to commit to surgical alterations at that time because, she explained, she simply could not accept the idea that she was a transwoman.
“I still thought I could cure myself of being transgendered,”
In spite of this desire to be ‘cured,’ she began taking tentative steps toward ‘accentuating the feminine in [her] face.’ She underwent facial electrolysis that had produced permanent pockmarks on her cheeks and chin, only exacerbating her self-consciousness about her appearance. In 2002 she had surgery to remove her thyroid cartilage (Adam’s Apple) and, shortly thereafter, a surgery to reduce the size of her nose.
“That only made my brow look bigger,” she lamented. “My brow is my major concern. I need my nose to match my brow. I have a kind of Neanderthal brow. I want to do my jaw too, but I may have to skip that for now depending on whether I can get the money together. I was kind of hoping he wouldn’t say that I needed to do my jaw, but I know it needs to be done.”
Rosalind knew that her decision to have surgery would cause complications in her work and family life. She presented as male at work and at family events, and planned to continue doing so at least until her elderly father passed away. The thought of disappointing him with the fact of her female identity was unthinkable to her. She worked in the building and construction industry in a fairly small town and, for her, living full-time as a woman was simply not an option. Worries about work and personal consequences had kept her from making many changes both to her life and to her body, but she had finally decided that such concerns could no longer determine her choices.
“If I have to think too much about what others think, I’ll never do it. I have to do this for me. I’ve spent 25 years of my life thinking about not looking like I do now. I want that to go away. Constant thinking about that ruins the mind. After this I’ll be able to think of other things, everyday things.”
Rosalind told me, as did many patients, that it was during puberty that she began to hate her face. As she watched her ‘button nose’ give way to the oversized nose of a pubescent boy, she taught herself how to wash her face and brush her teeth in the dark.
“My mum would go into the bathroom after me and always wonder why the blinds were closed.”
It was easier for her to re-learn these daily habits than to deal with the look of her changing face in the mirror. This was the beginning of the long story that brought her all the way from Wales to have surgery with Dr. Howard some 25 years later.
I was tired and anxious when I joined Howard the next morning. We walked briskly down the hallway to the surgical wing, he in a shirt and tie covered by his long white coat, me in my canvas jacket and shoulder bag. I saw the loafers on his feet and felt like an idiot in my running shoes—I thought they’d be best for endurance.
After so much discussion of looks and numbers and desires and abilities, it is in the operating room that faces are reconstructed. It is here, as they say, that the rubber meets the road. While for surgeons the operation is an event that has been routinized and repeated hundreds or even thousands of times over, for the patient, the operation is something absolutely singular—assuming all goes well. Over the course of the surgery (up to nearly eleven hours in the case of a “full face” operation), the patient’s skin, bone and cartilage is pushed, pulled, burred, sawed, cut, cracked, tucked and sutured. In the end a strikingly new face may emerge; one whose production is guided by the hope that its new form will enable a coincidence of the patient’s self and body for perhaps the first time in a very, very long time.
Facial Feminization Surgery is guided by a hope for phenomenological integration—the creation of a body that (re)presents the self. Though the technical work of surgery is something that patients do not experience in real time, its effect animates their anticipation of a better life through the body as a better and truer thing.
He brought me to the charge nurse’s desk. I was to register my name in the vendor’s logbook. Dr. Howard offered me a pen. “You can keep it,” he said. “It’s got my name on it.” I signed in quickly and was given a sticky nametag. I followed Howard into the physicians’ locker room where I was shown for the first—and last— time where to find the supplies I would need to enter the OR. I slid my bag and jacket into an open locker.
For those who desire physical transformation, the operating room is place that symbolizes corporeal change and all the attendant hopes of what that change will bring. In addition to the physical transformations enacted here, the operating room is also the scene of an encounter between patients and surgeons that is structured by a common conception of the body or, more specifically here, the face. For these two people in this place, the patient’s face is a material thing. It is not the irreducible site of personhood, the distinct shape of which makes us individuals; it is a series of structures whose problematic characteristics can be rectified.
These structures do not necessarily map onto or even remotely relate to the social or personal identity that the face is typically taken to be. That is just the point: this face is not her face. Not yet at least. The preoperative face is simple, disinterested material for the surgeon who cuts into and reshapes its parts, and it also is this for the patient whose experience of her face as something disloyal—as non-coincident with her self—has motivated her arrival here.
This is a distinct vision of the body shared between the surgeon and the patient, two people who have arrived together in the operating room precisely in order to alter it. We grabbed blue paper caps from a shelf near the door to the hallway. He folded the bottom rim of his cap upward in order to pull it down snugly before tying the white paper straps behind his head. I did the same. We were ready. Howard swung open the door and we headed to OR 3, his regular room. He handed me a surgical mask as we walked through the scrub room and into the OR where Rosalind was laying on the table being prepped by the Circulating Nurse (CN).
Dr. Howard went immediately to greet the patient. He caressed her forearm and assured her that everything would go well and that she would look beautiful. I! couldn’t stop staring at her fingernails: cotton candy pink against the blue and white striped blanked that covered her. Howard stayed by her head until she was under anesthesia. The moment the patient was unconscious, the feel of the operating room changed. With the presence of a guest no longer observed—I certainly did not count as such—everyone in the OR began their tasks in haste.
“This is Rosalind Mitchell, 37 years old. We’re doing her forehead and nose today. She wanted to do the chin and jaw but her credit card didn’t come through. Says she’ll be back for those in the fall. This should take four and a half hours. She has no allergies and is on no medication.” Confirming! that all parties were in agreement, he began to prepare the first site: the forehead. Sitting on his stool at the end of the table, he began to comb and gather Rosalind’s long hair in rubber bands. Once the site was isolated, he shaved a one inch wide track through her hair, combed out the loose pieces and dropped them into a biohazard bucket. He injected the incision site with local anesthetic and then left the room to scrub in. While he was out, the CN sterilized the forehead site with soap and water and then with iodine that dripped in deep brown yellow drops through her hair and into towels on the floor. The doctor returned with his clean and dripping hands held at chest level. The CN helped him into his gown and gloves
The process of making a masculine face into a feminine one only rarely involves addition (of bone substance or implants). Instead, making feminine is almost always a process removing that which is masculine to reveal the feminine beneath. The masculine is a problem of excess: the jaw is too wide, the forehead too long and too prominent, the chin too square, the upper lip too long. Whereas genital sex reassignment involves rearranging and repurposing body parts in order to make new ones, like mastectomy for female-to-males, Facial Feminization Surgery is essentially about taking parts of the body away.
For this reason it can quite literally be read as carving away the outer unwanted body to reveal the self within. The metaphorical representation of “a woman trapped in a man’s body” is, in other words, rendered quite literally here. In this OR scene, the ontological and phenomenological statuses of the body and self are radically uncertain.
The surgeon further isolated the incision site by draping sterile blue towels over the patient’s hair and securing them in place with skin staples. Fully draped from head to toe, only the patient’s face was showing. One stitch was placed in each of her eyelids—sutures are necessary to keep her eyes closed (and thus moist) because her face will be tugged and moved quite a lot throughout the procedure. All was ready to proceed. Dr. Howard announced the time of the first incision; the CN recorded it on the whiteboard on the wall, and the operation began.
To reduce the frontal sinus that accounts for the ‘male brow,’ an incision is made beginning at each ear and meeting at the center of the head, just behind the hairline. The skin of the forehead—from hairline to orbits (eye sockets)—is folded down over the eyes, revealing the smooth and very white frontal bone below.
The long, thin wooden handle of a cotton swab is broken in half, dipped in methylene blue and used to mark the frontal bone on either side. The periosteum (a membrane that lines the outer surface of bones) is cut at these lines and scraped forward into the orbits at the top of the nose bridge. Glancing at the cephalograms illuminated on the wall\mounted light board, the doctor marks the frontal bone with a yellow wooden pencil.
The burr tool whirs like a dental drill as it grinds off the undesirable bony prominence's above the orbits. Bone particles fly off the burr as it spins. They catch in the cloth and paper that covers the patient and in the folds of my scrubs as I lean in. By the end of the procedure they will become dry chalky dust. An oscillating saw blade replaces the burr tool and a cut is made along the pencil drawn lines. The cut bone is pried up out of its place, making a dull cracking sound as it is dislodged from the skull. The Surgical Tech (ST) collects this irregular oblong piece (about two inches across at its widest point) and sets it in the white plastic lid of a sample cup for safekeeping. The frontal sinus is revealed. Everyone’s frontal sinus (95% of us have one) is structured differently. Rosalind’s is internally asymmetrical, divided by thin walls of bone into three distinct cavities. Frontal sinuses are usually empty, but sometimes brain matter has protruded into them. “Is that brain or sinus? Not sure. Let’s go slow.”
A yellow pencil marks the location where corresponding holes will be drilled in the frontal bone and in the bone patch. Stainless steel non\magnetic wires are placed and spun down tight. The ends of the wires are trimmed and turned inward. The bone work on the forehead is done. Rosalind’s forehead has been set back 5 millimeters.
The anesthesiologist leans over and speaks loudly in Rosalind’s ear: “You did a great job. Surgery is over. Just relax. Let us move you.”
RECOVERY
When a patient first encounters her new face after surgery, it is covered with bandages and dressings. Much of the skin that is visible is taut, swollen and discolored. Her nose may be packed and casted. There may be drains pulling blood from around her newly contoured jaw. She must suction saliva from her mouth because the throat pack placed during surgery will make it uncomfortable to swallow.
For the first several days following surgery she may need to manually stretch the muscles of her jaw to keep them from clamping tight in a gesture of defense. Even if the procedure is considered medically successful—in that the surgeon was able to meet the goals that he set for himself and there were no compromising complications—there is no way to know how well the surgery went, or whether the desired effect will actually be produced. That effect is, after all, not a property of the face itself. It is, rather, a response that the face will (hopefully) elicit.
Such a measure of success cannot be clinically assessed, nor can it be known right away. Depending upon the particular procedures performed, it may take up to a year for all of the swelling to subside and for the face to ‘settle down,’ as surgeons say. Though new structures of bone and soft tissue were created in the event of the operation, the face itself is never a fixed and stable thing; it is always a thing unfolding in time.
After all of the waiting she has already done—waiting for self-acceptance, for surgery savings funds to grow, waiting for consultations, for travel arrangements—now the patient must wait to heal and find out whether the face she wanted is the face she’s got. Surgery is the quintessential anticipatory regime (Adams, et. al., 2009). It is forward looking, oriented to a future post-surgical life that will be somehow better than the life that would have happened without it. Surgery is about intervention: the imagined and undesirable future can be changed through the event of the operation. Once that event has occurred, there is nothing to do but wait. And hope.
I first met Rachel five days after her surgery. She had her forehead, hairline, nose, thyroid cartilage, and jaw done. In addition, her upper lip had been shortened and enhanced. When I was introduced to her by Heleen, a Dutch attorney who was back in town to see Dr. Howard for some jaw revision work, I had to stifle a sympathetic wince.
Rachel’s eyes were ringed in deep browns and purples, and the sutures beneath her nose drew contrastive attention to the thin red incision line where the length of her upper lip had been reduced. Though the packing had been removed from her nostrils earlier that day, the cast on her nose remained and was held in place by a large X of tape rising up above her eyebrows and down across her cheeks. Her thinning hair and receding temporal baldness left sutures and staples visible across the crown of her head.
I felt sore for her, like neither of us should move too quickly. She, on the other hand, said she was feeling better than she had in days and was light on her feet as she led me to the back garden where we could talk. As Rachel spoke—with the marked accent and dry humor of a life-long New Yorker—she dabbed saliva from the corners of her swollen mouth with a white cotton handkerchief. We talked for more than two hours in the garden behind Howard’s private convalescent facility, with only one break: the unseasonably strong sun was heating the staples in her scalp and demanded that we move into the shade of a leafy tree.
Rachel, now in her mid-fifties, had first decided that she wanted FFS fifteen years earlier, as soon as she saw before and after photographs posted online.
“From the moment I knew it existed, I thought, ‘Wow.’ I knew that I didn’t have a pretty face. I’d get dressed up but I knew I didn’t look like a woman. I could put all the makeup in the world on and nobody was going to mistake me for a girl. Maybe when I was like 16. Essentially, I would say that from the moment I knew people were doing it, I immediately started thinking to myself, ‘Wow, I could do that, too.’”
When I asked her what it was about her face that she had wanted to change, she had trouble locating the problem that she hoped surgery could fix—though she could quickly recount the list of the procedures that had just been performed. “If I was sitting here with a friend and just talking,” she said, “I would say, ‘Beauty is like pornography, you know it when you see it.’ And it’s the same thing with a feminine face: you know it when you see it.” Though she noted that her, ‘rather large nose,’ was ‘a male trait in [her] family,’ the nose by itself was not the problem. Neither, necessarily, was it her ‘fairly prominent forehead.’ It was something greater than these, and something more diffuse.
“I was a handsome man, but I didn’t want to be handsome. I wanted to be pretty. I guess, in a certain sense, I wanted to have all the things that I enjoyed in women that I liked. The way they looked. The way their lips looked. What their hair looked like. How all the features went together. I think it’s kind of a simple answer: I wanted to be a pretty girl. One of the great things that Dr. Howard did was define this whole notion of feminizing in entirety, as opposed to just doing one thing. One thing in and of itself is not going to do it. It’s got to be a holistic approach.”
On account of this ‘holistic’ transformation, Rachel did not really have an idea of what she would look like once her face had finished healing. More than any particular ending point, what she most wanted her face to be was something other than what it had been for her entire adult life: masculine. The particular form that that femininity would take was not something that concerned her.
“[When considering having FFS] I would say to [my friend], ‘Do I really want to do this? Because what if I don’t really look good?’ She would say to me, ‘Well, you know what you look like now. Would you rather go through the rest of your life looking like you look now, or looking like somebody else? Maybe you’re not drop-dead beautiful or even pretty, but you’re not going to look like a man.’ And the answer to that is the latter. I knew how deeply dissatisfied I was. To the point of it being painful what I looked like, and having to look at myself in the mirror everyday. That got worse as I got further into my transition. That just got worse and worse. The disconnect between what I felt and how I looked just became more and more pronounced to the point where I just didn’t want to look in the mirror. I just hated it.… [Someone] asked me, ‘Are you going to look very different?’ And I said, ‘I sure hope so.’ That’s the whole point. It wouldn’t bother me if nobody recognized me. That wouldn’t bother me at all. If I look good. If somebody said, ‘You look fantastic, but I can’t quite place you,’ that would be wonderful.”
Her new face—still tender, bruised and cut—held, under its bandages, the possibility of a radically new identity in which she was not recognizable to anyone she knew. While to me such a prospect seemed as if it might be quite frightening, for Rachel, the potential of this total change was ‘wonderful.’
As Rachel sat healing, she recounted the promise that the facial change would be a total one through a personalized version of Howard’s early morning doorbell scene.
“My goal, my ideal is that I could go out on the street dressed like I’m dressed right now—just a pair of pants and a t-shirt and some sneakers—and no gender markings other than I’d be wearing earrings, which I always wear, and that when I went into a grocery store the person would say, ‘Can I help you miss?’ That’s really what I want. I want to read as, accepted as, and reacted to as a woman. So that is what I was hoping he would say he can do, and that’s what he does say he can do. That is what he promises.”
Becoming ‘accepted as and reacted to as a woman’ would be the actualization of a truth about herself that Rachel traced back to her earliest childhood memories of dressing in her mothers lingerie and heels. Her knowledge of her gender as being somehow ‘not right’ had persisted throughout her life. “I’ve essentially been feeling ashamed of myself probably since I was five years old—or probably more like four,” she said. “Living daily with a sense of shame about who I was. And not only living with it but hiding it, because I was also hiding the source of my shame.” Rachel had undergone years of therapy with various psychologists and psychiatrists.
“I had met someone very early on in the therapeutic process that I interviewed with and he said to me, ‘Look, this is the way you are. You’re not going to change. This isn’t going to go away.’ And I just refused to accept that. I was 20 years old. And out of everybody I saw in all the intervening years, what he said was the truth. It took me 30 more years to accept that.”
Rachel’s feelings about herself as a transwoman changed somewhat unexpectedly. Her mother had become ill with cancer and as the child who lived closest, Rachel undertook what became a very intimate caretaking role during her mother’s treatment. Despite longstanding conflicts in their relationship—many of which were rooted in Rachel’s gender issues—the two grew incredibly close through this ordeal.
“We were spending a lot of time just together by ourselves. And I just sort of let go of any resentment or anger I had towards her, and I really just wanted to make her get well. Having a positive influence on her life kind of opened something in me that I had closed off. When the whole thing was over, I thought to myself, if I can give her this [beginning to cry softly], then why can’t I give this to myself? So, I did.”
Tears welled up and streamed down her bruised cheeks as she recalled the epiphany that had not only enabled her to relate differently to herself as a transwoman but had also revived a loving relationship with her mother.
“What started to happen for the first time in my life, is that I started letting go of shame. I thought: I got my mother through this, how bad a person could I be? So I did start to just let go of feeling ashamed of myself, and feeling all this guilt. And that was a really new experience.”
Her mother’s cancer in remission and her divorce from her wife finalized, Rachel began hormone treatments, the beginning of her physical transition from male to female.
“I had my first shot and it felt fantastic. I felt like Marilyn Monroe. I remember getting on the train going back downtown and I had to remind myself, ‘You still look like a man to everybody.’ That’s how powerful it was. I recognize that it was psychological, but it was also physical, too.”
Though she felt it was likely that she would eventually undergo genital sex reassignment surgery, FFS was her first surgical priority. “The most important thing I could do was change my face,” she explained. It was a change that would free her in ways that, on that sunny afternoon, she could only imagine.
For many patients, a new face promised not only a new life but also a radically new—and uncertain—identity. So long as they would no longer be recognized as men, the particular form of their faces did not really matter to them. For example, Patricia looked forward to the feeling of her new face more than its look.
“I do think it is going to be profound to just get up every morning and look in the mirror and go, ‘Oh my god, here’s somebody who I’ve always known was there but I never saw.’ You know? Feeling is one thing, but seeing is another. That’s kind of the aspect I’m looking for, without any idea of what she’ll look like. Whatever, it’ll be an improvement.”
Some patients hoped that the effects of their surgery would be subtle, simply accentuating the features that they already liked about themselves, while others had a very particular idea of what they thought they would look like following surgery. This was informed by their understanding of what surgical modification could accomplish, as well as their own interpretation of how—and like whom—they looked prior to the operation.
Katherine both wanted and expected to retain her individuality. “I want to be a feminine version of myself,” she said. “Some people just aren’t realistic. If you’ve got a head like a medicine ball and you want to look like Angelina Jolie, you’re going to have a rough time of it. Rather than emulate someone else, I’d rather be an individual.”
Similarly, Brenda—who had consulted with both Howard and Page and ultimately decided to undergo surgery with Page—said, “I guess I want to look like me but more feminine.” Though word-of-mouth, personal experiences and plenty of online research, patients felt confident that their wildest dreams could come true. They had seen the photographs of scores of former FFS patients whose images and narratives of transformation attested to the possibility of total surgical transformation. It is the actualization of this idealized possibility that has earned Howard a sort of cult following, and a legion of fans and defenders.
Jill’s Story
Howard had performed Jill’s ‘full face’ FFS nearly ten years before, and she had been an outspoken admirer and supporter of his ever since.
“I’ve been a Jim girl for a long time,” she explained with a smile. When I first met Jill, she reached into her pocket and pulled out her cell phone to show me a picture of what she looked like before surgery. I admit that the difference between the photograph and the face before me was astounding. She clearly took great pride in this fact.
“I don’t reject what Joe was. I don’t apologize for what Joe was. I don’t apologize for what Jill has become. I am comfortable with the unique mutt that I am, which is a combination of what Joe was and what Jill is. I like to think it’s the best of both worlds as opposed to the forces of having to be one or the other.”
The photograph—and her narration of it—was not only an affirmation of her own reconciliation with her past, but a testament to what FFS could do. When Jill first learned about FFS in the late 1990’s, she had already come to peace with the idea that she would never transition.
She had a reasonably successful life as a husband and father, and felt completely isolated in her knowledge of herself as a woman. If she could not be recognized as a woman, then she would have to learn to accept her life as it was. At that time, before the expansion of the internet, she explained,
“There was no validation. There was no hope that we could blend into society and just live our lives. The choices were twofold. One, you accept the fact that you live in some margin—if that was okay. Or you accept the fact that you live something less than a fulfilling life. I was married. I had a son. I had a good career. I had money. I had all of the trappings that society told me that I was being successful, except that I had this secret.”
Jill described first learning that FFS was possible, as a moment that was “very empowering but it was also terrifying. When you become comfortable with the impossible, realizing that the impossible is possible gets scary.” Jill’s initial surgery lasted nearly 13 hours and the recovery, she said, ‘was hell.’ Much like the radical transformation that Rachel envisioned, Jill’s surgery had changed not only her face, but her most basic understandings of herself and her world. Though she had not been politically engaged in her life as a man, since her transition—which began with FFS—Jill found herself confronted with social inequalities that she had never been aware of before.
“As a man, I had never experienced discrimination. Really. Not that I knew of. You take it for granted: you’re white, you’re heterosexual—or perceived to be heterosexual—you’re granted a level of privilege that you don’t know that you have that just comes with your birthright. You’re living in a world that’s oblivious to many of the unfortunate realities that others have to face. To have that stripped from you and see that people can be fired over this, people can lose their housing, to see that people in your community are not welcome in women’s shelters but have too much self-respect to go to men’s shelters and so they freeze to death on a park bench because they can’t get a job and they’re homeless. To recognize that in school people get the crap beat out of them because they’re different. Those things are contrary to everything my parents raised me to believe. So I found that I was given opportunities of making choices.”
Newly empowered by her changing body and newly outraged by an understanding of life that she had not been aware of before, Jill became a prominent figure in transpolitical organizing circles, delivering keynote addresses at national conferences and writing a widely circulated book about her experience of coming to terms with her identity and going through the process of transitioning from male to female. She attributed this radical shift in her life to FFS. “My own involvement never meant to be as significant as it became,” she explained.
“Coming here and meeting Sydney and going through this process was the single most profound experience of my entire life. It remains so. And I’ll tell anybody who asks….
The fact of the matter is that coming here, finally looking in the mirror and seeing somebody who more closely reflected on the outside who I knew was on the inside and watching that person develop—because the person that I was six months after I left here was very different than the person who left here. I never would have transitioned without coming to see him. Coming here was day one. It was a physical change, it was a mental change, it was psychological change. It was the impossible becoming possible.”
Jill was, quite literally, the poster girl for FFS and for Dr. Howard. Her before-and-after photographs are featured in multiple places throughout Howard’s recently published book on FFS and are staples in his conference presentation slideshows.
Not only does Jill epitomize the feminine—both visibly female and normatively beautiful—she also exemplifies the total life changing potential of Facial Feminization Surgery. Hers is a narrative of redemption that emphasizes her own efforts for self-acceptance as materialized by Howard, the person with the unique skills and vision to see in her—and make her into—the woman she knew herself to be. Despite both her own and Howard’s characterization of her surgery as an unqualified success, Jill’s time on the operating table was not done. She was in for some revision surgery on her jaw.
In some patients, the blood that pools around the bone following jaw contouring surgery can later be reabsorbed and turn into bone. When this happens, patients often return for revision in order to recreate the narrowed jaw that the initial surgery produced. This increasingly square jaw is what brought Jill back to the office. No face—no matter how fantastic—lasts forever.
#gender#transgender#gender bender#transformation#trans#trans woman#gender transformation#lgbtpride#lgbtq community#LGBTQA#lgbtq#lgbtqai#lgbt#maletofemale#male to female#mtf hrt#mtf#HRT#hormone replacement therapy#body dysphoria#dysphoria#hormone#Dysphoric#facial feminization#facial feminization surgery#sex reassignment surgery#surgery#male to female face#ffs
0 notes
Note
hewwo! i was wondering if u could pls give me some advice on starting my transition? ive been so scared to start bc of family and costs but ive decided to just. do it. yknow? like if i don't ill probably die lol. u look amazing and rly confident in yourself in all ur selfies and one day i wanna be Like That ✌️❤️
hi! ok, so first of all: yeah, i absolutely can give u advice, and second of all: i remember feeling exactly like you did. it literally wasn’t that long ago, either, it was like. 2013/14/15 (i can’t remember, time is fake, whatever lmao!). third of all: bless u yr so sweet. i still have a lotta issues with confidence (i doubt myself, my talent and what i can do literally hourly), but honestly? i love my body right now. it’s a good, genderless body, goddamnit.
long, long post ahead bc i’m trying to think of things i did and good god please take it with a grain of salt because a lot of this is just me ranting about things i wish I’D done in my own position. i’m also coming from a place where HRT and surgeries AREN’T free, so that’s also A Thing. everyone’s experience is different.
transitioning (particularly medically) really super fuckin varies country by country (and honestly probably even state by state, age by age and fuckin gender by gender because cis people won’t let us fucking BE goddamn): i don’t know where you are, so my only tips there r: find a trans friendly doctor/endo (i was kinda forced to go through a hospital bc That Was How It Was here in good ol’ Australia), and one people wholeheartedly recommend, if you wanna go that route.
my first point is make sure you find safe spaces in every goddamn aspect of your transition. medically, socially, physically. if you think your doctor is refusing you treatment or is discriminating against you, you NEED to ditch that doctor. if your friends and family are really verbally or physically violent against LGBT folks, you NEED to leave that space if you can (or not come out and wait until you can leave. seriously. i’m kinda lucky– my grandma was verbally violent against LGBT folks, and initially my mum was skepitcal, but i convinced them both to go to a group for LGBT+ parents and friends and they slowly turned around). get yourself friends, get yourself allies.
i cannot stress that enough. my first doctor refused to send my referral letter to the royal children’s hospital gender clinic because even tho he presented as a “nice” guy, he believed that because this was “”””out of the blue”””” for me, he figured he’d just Not Send It (and tried to tell me that a lotta kids there didn’t actually helpo, lol). so there i was, a young 15-16 year old alister, waiting like 2-3 months for something that didn’t even get fucking sent.
join trans groups on facebook and in real life. seriously, they’re a godsend; there’s buy-and-sells, advice posts, encouragement posts. ESPECIALLY local ones. most of them on facebook are private, meaning no one can see if you’re posting/in the group, and it’s easy to check if they’re not. these fb pages + local groups are good ways to find trans friendly spaces and doctors. i found my current doctor, who’s actually one of the very few doctors who knows what the fuck he’s on about re: trans people, through a real life trans group. they were like “oh, you should see x”, and even though he’s about 30-40 minutes away from me, he’s brilliant and honestly saved my life.
along those lines: figure out what you want from your transition, and then realize & accept that this may change (and it also may not change!). very early on, i was super insistent that i wanted phalloplasty and to wear packers, and now i couldn’t care less. at first, i identified as agender, and then as a trans guy/ftm, and now i identify as a Black Hole (i’m kidding, don’t @ me). like, a lotta people DON’T change their minds. but i did, some people do, and it shouldn’t be anyone’s business but your own what you want to do with your body
(sidenote: this also goes for detransitioning or stopping medical transition but continuing to socially transition/present differently. literally, it’s fine. it’s your body. fuck anyone who says otherwise.)
again: FUCK ANYONE WHO SAYS OTHERWISE.
your body is literally your body. do NOT let anyone tell you what to do with it or who you are. i had people very early on scream at me (legitimately scream and throw me out of home, thanks grandma), tell me i wasn’t actually trans, and harrass me for this shit: but frankly, if i’d put myself back in the closet, i wouldn’t be alive right now. i would’ve killed myself years ago, and i wish i wasn’t kidding. if it’s safe, you need to stand up for your own body and your rights and put yourself somewhere that will allow you to follow through. you need to keep going and keep living.
my only other two pieces of advice are “patience, baby”– like, for real, every single part of transition takes time. this varies from where you are and who’s supporting you, but it’s generally true. it takes time for people to accept new names and pronouns
(lotta people get furious about this, and i used to be one of those people, but hindsight’s a bitch and you gotta realize that… like, it’s hard for some cis people. you gotta give them a little bit of wiggle room, especially if they’ve never ever met a trans person before. it’s about reminders, reminders, reminders: which is SO hard if you’re not safe/don’t have the confidence. there IS a flip side to this though: if chad and stacey have known your new pronouns for months, now, and they keep “””slipping””” up, they’re not slipping up, honey. they’re doing it on purpose. kick their teeth in i’m kidding please don’t do this you know what i mean.)
it takes time for HRT to kick in. it takes time to gather a Look™ of your own you like, it takes time to build confidence to even tell people, it takes time to save up money for surgeries and it just… takes time. sometimes because it’s a naturally slow process, sometimes because cis people are Cis People and like to gatekeep. i remember being very young in my transition, sitting in the car after one of my appointments with the afformentioned shithead doctor bawling my eyes out because he’d told me i wouldn’t be able to access t for x amount of time and it was bullshit. this year i’ll be 2 years on t. wild, huh? there’s a lot of us and not equal amounts of resources (ESPECIALLY in public systems) depending on where you are, so you gotta be prepared to WAIT.
i’ll tell you what super helped me through those years: hyping myself up for other things! i still have the ticket from my first twenty one pilots show. that show meant SO much to me. i cried all through it, because waiting for that show kept my mind off of the wait for my royal children’s appointments (and even waiting to go up to melbourne bc my mum and i would go and get kebabs was a good thing to focus on!). keep things that aren’t trans related on hand (seriously i struggled with this because dysphoria and shit is fucking hard!! it’s easy to say but really fucking hard to put into practice).
(one day i’m gonna tell tyler and josh just how much they saved my goddamn life. i know they hear it weekly, but i will.)
my other thing is that uh. it won’t solve all your problems especially if you’ve got mental illnesses. this is a really fuckin depressing thing i had to drill into my brain, but it really helped. transitioning solved SO many of my issues. i no longer have back issues (thanks, like, literal kilo titties, lmao), i no longer have sore ribs and i can breathe and wear shirts. i lost so much weight (and am kinda gaining it back, but whatever). i no longer have anxiety about whether people can tell i’m binding– which is WILD because i used to stress the fuck out about it to the point where i never went out anywhere. i used to sit on the bus wondering if the person next to me could tell i had titties. now it literally doesn’t even register.
my issues now stem from PTSD, depression, BPD and ADHD. how do you fix this? you don’t. but what HAS helped is finding a therapist who won’t pressure you into talking about trans shit. lemme tell you: this shit gets exhausting after the fifth time of “oh i googled ‘can you become a boy’ when i was, like, nine” (this is my go to story because this memory is so vivid). of course, there’s gonna be moments where you HAVE to: my therapist recently actively asked me to briefly run through it for my PTSD report. but otherwise we literally haven’t talked about it and that is a GODSEND (because i don’t need it. if you need it, that’s good, too!). having a therapist that you can just wordvomit at wrt anything is literally the best thing and can be super helpful– seriously, there were a few trans-related sessions where i just snarled about the bullshit gatekeeping and the bastard i had to see for my therapist letter (oooh, every time i think abt the fact that it was something like $400-500 for two fucking sessions i get so mad lol), but outta 14 it’s really only like 2-3 of them.
but yeah. that’s it. i dunno, these are things that i’ve learnt and sorta… like to think as helpful for myself. of course, this could be different for you: you’re not me, you’re entirely different, in no doubt an entirely different country, social, financial, mental state. i was FUCKED UP when i first came out. i didn’t know that then, but i do now. i spent a lotta time by myself and that’s not healthy, so i really encourage you to reach out to our community, local and worldly, because oh my god, we’re here for you. we are SO here for you.
#long post#sorry if you need this formatted for ease of reading please shout at me. i really word vomited all over this#my transition#trans#anon#asks#iodk what else to tag this as
5 notes
·
View notes
Note
I'm having a very hard time finding clinics/ doctors where I can get hrt especially as a minor? I'm living in Germany but internet searches so far only ever gave me really vague answers, so id really appreciate it if any of you or any of your followers could tell me some places (understandable if no one knows sth tho)
Poking around on Reddit, this group was recommended for HRT specifically; they may be able to help you. I also saw several people recommending to contact the Charité hospital in Berlin; I think that QueerNetzwerk would be the best contact (email’s on the page). Even if you aren’t near Berlin, it’s possible they’d be able to direct you to local resources or would know what your first steps should be. Additionally, the top comment on this post gives a solid breakdown; the short version is that you will almost certainly go through a psychiatrist or psychologist in order to get a paper diagnosis, so if you are already seeing a psychologist/psychiatrist who isn’t actively trans-hostile then they may be able to refer you to someone for such an evaluation.
TGEU says that Germany has no legal barrier to minors accessing HRT, but in practice I’m not sure how much that varies by doctor.
I don’t speak German, so my ability to evaluate resources is unfortunately limited. Followers, do you know anything more?
- Mod Wolf
7 notes
·
View notes
Note
do all the questions !!
All the questions? Sure, why not? Insomnia is making me its bitch anyway1: How did you choose your name?- originally I was gonna go with Lilith from Borderlands 2 because yes please to her entire aesthetic, but I decided to go with the more "normal person" name Maria. Partly because of the lead singer of In This Moment, Maria Brink (absolutely gorgeous, phenomenal singer, and the Black Widow album helped inspire me to live true to myself), and Lady Maria from Bloodborne (she's got a Tragic Backstory, feel disconnected from family due to traditions/ environment, and has regrets about who sent was). All in all, one is a person I admire to be like and the other feels like I'm looking in a mirror. Both are also women with blonde hair and I think I look damn good as a blonde2: What gives you the most dysphoria? -Facial/ body hair3: Do you have more physical dysphoria or more social dysphoria?- Most of the time, physical dysphoria. Social dysphoria still gets to me because I'm not out to my family and everyone in that group refer to me with childhood nicknames/ my "(grand) son/ nephew." 4: What do you do to perform self-care when you’re feeling dysphoric?- Shower, shave, lie in bed and dissociate while playing mindless games on my phone 5: What was the first time you suspected you were transgender?- this is actually a hard one for me to answer. I was (in a weird/ sad reality) really sheltered as a kid, in the sense that I didn't even know transgender people were a thing until High School. I think part of it started when I began playing runescape in middle school; I chose a female avatar and went with a generic female name whenever someone in game asked for it. For some reason, I really enjoyed being addressed like that but chocked it up to being like 12. Similar thoughts came up again in HS when I was told on several occasions and by several people that I'd make a pretty girl; again, I took it as a compliment and it made me feel really good about myself. Other times were also when I was asked "what would you do if you suddenly woke up as a girl?" my answer was usually "go back to sleep and go try on cute clothes" and also being super jealous of girls at school dances (wanting to wear the gorgeous dresses/ heels/ makeup)6:When did you realize you were transgender?- January of 2014, when I had read on Tumblr about Leelah Alcorn. It was extremely depressing to read her letter and diary entries about her personal life; while reading everything, I kept realizing that I felt almost exactly the same way she did, and by extension that I was also trans7: What is your favorite part of being transgender?- just being able to feel comfortable in my own skin, and also getting to wear all the cute shit I wanted to in HS8: How would you explain your gender identity to others?- the people I have come out to, I simply as them not to use he/him pronouns because I outright don't identify as such. It's pretty simple9: How did you come out? If you didn’t come out, why do you stay in the closet? Or what happened when you were outed?- at first, I only told people when we were able to talk 1 on 1. As I've gotten more comfortable with my identity, I gladly come out to people that I'm comfortable around. I still need to come out at work which I'm avoiding for 2 reasons. The first is that I don't know how open-minded/ accepting my coworkers/ boss are; the second being that I want to get on hormones so that there's no turning back on what I say and how I feel10: What have your experiences with packing or wearing breast forms been?- haven't done anything with breast forms yet, probably gonna be uncomfortable though 11: What are your experiences with binding or tucking?- tucking is a hassle in general. It either falls apart quickly, or I ended up sitting down or walking wrong and hurting myself. 12: Do you pass?- I highly doubt it atm13: What (if any) steps do you want to take to medically transition?- optimally I want the full 9 yards. Hrt, permanent hair removal, SRS, and possibly feminizing facial surgery 14: How long have you been out?- I'd say close to 3 years15: What labels have you used before you’ve settled on your current set?- only he/him and that's due to being oblivious for so long16: Have you ever experienced transphobia?- yes. A lot of internalized transphobia; but there have been a few times where someone will show me something they find funny, and it turns out to be in extremely poor taste17: What do you do when you have to go to the bathroom in public?- I prefer gender neutral bathrooms, so I ended up holding it in for longer than I should18: How does your family feel about your trans identity?- don't know for sure, but probably gonna get disowned to some degree19: Would you ever go stealth, and if you are stealth, why do you choose to be stealth?- I don't plan on being 100% stealth, but I'm also not going to hide anything out of fear. Kinda like Don't Ask Don't Tell, I'll answer truthfully, but I won't go out of my way to explain it all20: What do you wish you could have shared with your younger self about being trans?- "you know those weird thoughts to get from being addressed as a girl and the happy butterflies in your gut? Roll with it, tell someone that you want to see a Dr about it. Be prepared for a ton of BS, it'll be worth it in the end. Stay strong, kid"21: Why do you use the pronouns you use?- mix of "why should I be addressed by something that makes me feel like shit?" and "fuck off with this binary shit"22: Do your neurodivergencies affect your gender?- maybe, I think my gender compounded the divergences that were already there 23: What’s your biggest trans-related fear?- safety. So many trans people are attacked and killed that it makes me hesitant to even bother. But I'm known for being stubborn and having a devil may care attitude 24: What medical, social, or personal steps have you already taken to start your transition?- I've come out to 90% of my friends and I've got a therapist that's willing to write me a letter of recommendation to get me started on HRT. I'm currently looking for a DR in the North Tx area anyone knows one25: What do you wish cis people understood?- gender identity =/ sexual orientation 26: What impact has being trans affected your life?- it's made me rethink how I view issues in the world, but also more cynical 27: What do you do to validate yourself?- look at my ugly mug and the mirror after a hot shower and say "you're a boss and bitch, don't let up now"28: How do you feel about trans representation in media?- we need significantly more accurate portrayals29: Who is your favorite trans celebrity?- off the top of my head, I only know of Laverne Cox, so she's #1 by default 30: Who is the transgender person who has influenced you the most?- Leelah Acorn, the tragedy of her death allowed me to realize why I was so miserable for so long 31: How are you involved with the trans community, IRL or online?- not much, if at all. I'm not super big on communities but that's only due to trust and self image issues 32: How do you see yourself identifying and presenting in 5 years?- hopefully full femme made and keeping NB/ trans femme33: What trans issue are you most passionate about?- my mind is 100% here ATM because it's 4am, so I can't think of anything other than wanting HRT to be more accessible to people instead of having to jump through hoops 34: What advice would you give to other trans people, or what message would you like to share with them?- safety first, pride in oneself second35: How do you feel your gender interacts with your race, disability, class, weight, etc. from the perspective of intersectionality?- I personally don't think it does but that's only because I'm a white person in the 20s36: What, if any, is the difference between your gender identity and your gender expression?- none at all37: Do you feel more masculine, feminine, or neither?- fem/ neither 38: What is your sexual and romantic orientation, and what are your thoughts on it?- only interested in women and NB people. In my head, I like the theory of being with a guy, but feel no sexual attraction to them39: Is your ideal partner also trans, or do you not have a preference?- no preference40: How did/do you manage waiting to transition?- think to myself "next paycheck, I'm gonna find a Dr and get this train moving"41: What is the place (blog, website, forum, IRL space) you get most of your info on being trans or on trans related things?- google, tumblr and reddit42f Do you interact with other trans people IRL?- got a friend that I used to work with at pizza hit who's a trans guy. You know who you are ^.^43: Are you involved in any trans-related activism?- not really, but I do want to get involved
1 note
·
View note
Text
http://www.usatoday.com/story/news/politics/2017/01/11/senate-begins-obamacare-repeal-process-all-night-voting-marathon/96447956/
(^“Senators voted 51-48 to approve a budget resolution that Republicans will use as a vehicle to speed through repeal of the Affordable Care Act, better known as Obamacare. House leaders plan to take it up Friday.”)
Okay so I have been silent about the affects of this on me but I can’t anymore.
[backstory]
In September I became aware there is a national shortage of injectable estrogen. (From http://fusion.net/story/344794/injectable-estrogen-shortage/ ) “Heather Zoumas Lubeski, the senior director of corporate affairs at Par Pharmaceutical’s parent company, said that the shortage began once the supplier for Delestrogen’s active pharmaceutical ingredient, estradiol, stopped producing the material. Par has found a new supplier, but the company cannot distribute it until they have received approval from the U.S. Food and Drug Administration. Once they receive approval, the supplier will be able to ship “immediately,” Lubeski said, although she could not say how long the FDA’s approval process will take. Lubeski also declined to name the previous or current estradiol suppliers. Perrigo Company did not respond to a request for comment. […] They would not deny a person who is diabetic their medication, right?” she asked. “Access to hormones saves lives. Not having this medication puts us in danger.”
In November, my clinic told me they were on back order for my estrogen. I was informed they’re unaware of when they will have it. I tried to find another place but unfortunately I then may not have been able to afford it without acceptance of my insurance. So my doctor temporarily switched me to swallowable estrogen in pill form. I was taking these for almost 6 months when I first started hormone replacement therapy (HRT). This method gave me mood swings and worsened my depression. I was also unable to achieve a normal level of estrogen, limiting the changes I wanted to start E for. So in April I switched to the injection and have been very happy with my mental and physical state. They called me a week later that I could pick up my injection again and LUCKILY I have been able to pick it up every time since.
[backstory end]
Deciding to start HRT was very difficult. It was in a very dark, shameful part of my life. I hated my appearance. I didn’t understand how I could feel so disconnected to the vessel that had carried me the last 18 years. I felt the same shame I did when I came out to myself the first time, but this was physical instead of mental. I had in the recent past felt like a confident queen slaying the earth I walked on. But now I felt like an outcast, an unlovable, freak. HRT made me see myself in a new way. My physical body changed. I finally saw the person I had always imagined myself to be. The reason I still feel more safe, more confident, rarely get clocked or misgendered and am subject to less violence (even with a 1 in 12 chance of being murdered) is because I am taking estrogen to feminize my appearance. People accept me as feminine. "Normal.” Or at least “passable.” I receive my hrt with help of insurance. When researching 2 years ago about transitioning, I learned about the systematic oppressions trans people live with. My parents insurance didn’t cover trans health care. So I did more research and applied for obamacare in my state. My friend has it and helped me get insured so I can afford the medication that saved my life. The system we have currently is broken (primary example is the national shortage because of bureaucratic issues).
Before freaking out I remind myself: Nothing is certain. I don’t know if Obamacare will be repealed or changed or replaced, but I’m worried. And you should be too. These next 4 years are going to be hard for all of us. Let’s stick together and focus on love. Fight when necessary ✊🏽
As for my situation, there are a few alternatives. I will be okay. There are other insurers, not free, but I’m privileged to have a job so i could possibly budget to afford an alternative health insurance plan. A large population (twice the rate of cisgender folk) of transgender people are unemployed or live in poverty.
Stay educated. Pay attention. Listen. Help.
#personal#me#Obama care#Obamacare#Obama#healthcare#trump presidency#e#estrogen#hrt#senate#house#don't repeal Obamacare#pay attention#stay woke#transisbeautiful#protecttranskids
27 notes
·
View notes
Text
Weirdo life update thing
Hi. I’m not sure if anyone I used to interact with on here is still active on their blogs (except for like 3 people), but anyway, yeah, sorry. Read if you feel like it, but no obligation.
I graduated from college last month and I’m staying at my mom’s house until the middle of next month when I’m moving to a new (much colder, more rural) town where I’ll be working at a college and going to grad school there. I’m planning on living there for 2-3 years at least. But life is weird and you never know what’s actually going to happen, so we’ll see. This summer is the longest break I’ve had from work and school since I was 13 years old (I’m now 22...), which feels strange, but I have so many more creative impulses now and time to actually do stuff with it, so that’s pretty cool.
I feel like I’m finally getting a good handle on mental health stuff with a combination of medication, an unusually helpful therapy group I was in last semester, and just generally gaining life experience and growing up (cognitive development is being good to me for now at least).
Within the last few months, I have sort of made peace with the idea that I will probably eventually pursue taking testosterone for at least some length of time. Accepting that I don’t yet know exactly what that experience will look like for me in terms of when, for how long, at what kind of dose, or if/when I will tell other people about that is probably the only reason I’ve been able to let go of all the intense sadness and apathy and anxiety I’ve always felt about that possibility. But I’ve already figured out the process for accessing hrt through my new school’s counseling and health services and I’ll have insurance through my job that will cover those sorts of things, so there’s a possibility that that may happen within the next two years, but I also totally reserve the right to change my mind because this shit is scary.
tl;dr- I’m a decently happy little bean who is growing up and trying to figure stuff out
0 notes
Text
Progesterall Review (UPDATED 2017): Don’t Buy Before You Read This!
What is it?
Progesterall is a cream intended to balance out hormone levels in the body, particularly in those with low progesterone. Progesterall is designed to help women with menopausal symptoms, as well as those with other hormonal conditions like PMS, infertility and more.
Progesterall contains the hormone progesterone, which is naturally produced by the ovaries, but slows during menopause. The website mentions this product particularly effective due to a liposome-mediated delivery system, which is intended to improve nutrient absorption.
Our reviewers have found that Femmetrinol best helps users balance out their hormone levels and find relief from the uncomfortable symptoms of menopause. This formula is made from a blend of herbal ingredients like black cohosh, damiana, chasteberry and more—which work together to reduce hot flashes, night sweats and more. Click the link for an up-close look at how Femmetrinol can help you feel great again.
Do you know the Best Menopause Supplements of 2017?
Progesterall Ingredients and Side Effects
Progesterall only contains a couple active ingredients, the main one being, the hormone progesterone. We don’t know where the progesterone used in this product is sourced from, but we’re assuming it’s synthetic, rather than plant-based. Here’s a look at what’s inside this formula:
Progesterone Grapefruit Seed Extract
Progesterone: A hormone that is naturally found inside the body, progesterone is often used in hormone replacement therapy to help treat abnormal menstrual cycles and menopausal symptoms, as well as non-cancerous breast pain, thyroid problems, depression, fatigue, weight gain and more.
Side effects may include changes in appetite, weight gain, acne, fatigue, allergic skin reactions, depression, irregular bleeding, PMS symptoms, breast tissue growth, headaches, swelling and upset stomach.
Users with breast cancer are advised to avoid taking progesterone, as it may worsen the condition.
Grapefruit Seed Extract: Grapefruit seed extract may have antibacterial, antifungal and antiviral effects and may help soothe skin irritations.
Something worth noting, while the grapefruit used in this product is specifically a seed extract, there are some links to grapefruit and progesterone having adverse effects when combined, as grapefruit may increase the body’s absorption of progesterone or other forms of HRT.
Click here to read more about the pills that best take on your menopause symptoms.
EDITOR’S TIP: Combine this supplement with a proven menopause pill such as Femmetrinol for better results.
Progesterall Quality of Ingredients
Progesterall is made from some ingredients that could be useful in helping users with low progesterone achieve a greater sense of hormonal balance—finding relief from hot flashes, night sweats, and the long list of physical and emotional issues that emerge with menopause.
What we didn’t like was, we don’t know where the progesterone (which was listed as such on the official label) came from—it’s likely synthetic or animal-based, but this information was not disclosed on the site.
Aside from the key ingredient being progesterone, there isn’t much else that stands to provide some relief to users looking for a product that addresses more than just progesterone levels.
We’re not sure if the link between grapefruit and progesterone is something consumers need to worry about, as this formula contains grapefruit seeds, but it’s something worth discussing with a medical professional if you are considering using Progesterall.
Click here to get our experts’ opinions on the ingredients that best help treat most menopause symptoms.
The Price and Quality of Progesterall
Progesterall is sold on the progesterall.com site exclusively. Users can purchase this item at a cost of $21.95 for a single tube, but the price drops should you decide to buy a 6 or 12-pack of the cream, which sell for $119.70 and $215.40, respectively.
According to the website, healthcare practitioners are eligble for further discounting, though the price is not disclosed on the site.
Unfortunately, the only way to buy this product is by accessing the official webpage, as it’s not available through any major third-party retailers like Amazon, Walgreens, GNC or CVS.
Learn more about how you can treat mood swings, hot flashes and more with plant-based ingredients.
Business of Progesterall
Progesterall is made by a company known as John Lee MD Solutions, and their contact information is listed below:
Email: [email protected]
Address: John Lee M.D. Solutions, LLC
228 Windsor River Road, PMB 322
Windsor, CA 95492
First of all, while visiting the Progesterall website, we found that the website mentioned the doctor who created this product far more than any information that might actually be helpful to consumers.
This product was created by Dr. John Lee, a doctor who specialized in hormones. The late Dr. Lee is the author of a number of books about menopause and other hormone-related women’s health issues and the site takes every opportunity to direct consumers toward reading his research, rather than answering the questions posed in the FAQ page of the website.
We don’t get any clear information about the symptoms this cream is thought to alleviate and the site is written in a way that feels exploitative to Dr. Lee, as well as the website visitors.
What’s interesting is, this cream was developed after Dr. Lee’s death, and his family has been selling this product since 2003—in an effort to maintain his legacy of “serving women,” despite the fact that he mentioned not wanting to create a product that may detract from his research.
While the Lee family may have good intentions, something about this website seems a bit off—users want more information about a product they are considering, and may want to read Dr. Lee’s research another time, not while they’re trying to make some simple buying decisions.
Customer Opinions of Progesterall
There were not a whole lot of reviews that demonstrated what the typical user experience with Progesterall might look like. The feedback was few and far between, though we were able to track down a few reviews from past users. Here is a quick look at what we were able to learn about Progesterall:
“I’ve been using this product for a couple months now and have noticed that, initially, all the symptoms seemed to flare up at once—BV, mood swings, hot flashes, etc. They’ve since balanced out and now I’m feeling better, but you need to mess with the ratios.”
“I use this product along with a DHEA supplement to prevent PMS symptoms. So far, so good, plus it helps with some existing depression symptoms I didn’t realize were hormonal.”
“Could not sleep very well before using this cream. My legs were restless, and I felt like I was having heart attack symptoms at random. Dr. Lee’s cream helped quite a bit and has improved my hair and skin.”
Based on the reviews we came across for this product, we simply didn’t get a clear sense of how widespread the use of Progesterall is, nor what percentage of users had a positive experience in using this product.
The lack of reviews can likely be attributed to the fact that the only way to buy this product is to go to the official website, and consumers likely need to know the name of this product for it to even show up in their online searches.
Regardless of why this product doesn’t have many reviews, we just don’t have enough information to gather enough evidence about whether this product is safe, has any negative side effects, or any other things that users should know before trying this product.
Read more about the supplements that restore energy and sex drive and take on hot flashes. More info right here.
Conclusion – Does Progesterall Work?
In the end, we really don’t have a good sense of whether Progesterall is a safe and effective product. Dr. Lee may have conducted some compelling research, but we don’t know if he created the formula or if it was the family that set up the sales process.
The website really had some glaring errors and made more mentions of the doctor that inspired the product, rather than the product itself, it’s really difficult to find useful information quickly about how this product might help someone going through menopause.
The lack of clarity on the site makes it hard for consumers to make an unbiased purchasing decision, and unfortunately, there aren’t any authorized third-party sellers that might streamline the process.
Finally, we didn’t find enough reviews to suggest either way that this product is good or ineffective. While the research is there, anecdotal evidence from a wide pool of users is instrumental in helping us get a good idea of how something might work in the real world, for people who are seeking relief.
Our experts have reviewed a long list of products designed to deal with the effects menopause has on the body, and have found that Femmetrinol best provides support for women going through this transitional time. Herbal ingredients like wild yam and black cohash help users naturally balance out their hormone levels, without the use of any synthetic estrogens or progesterones.
Femmetrinol is manufactured according to current GMP guidelines and have been the subject of a number of quality control measures aimed at keeping consumers safe and satisfied. Learn more about the herbal ingredients that power Femmetrinol – click here for the details.
from Easy Weight Loss 101 http://ift.tt/2prpXt8
via The Best Weight Loss Diet In The World
0 notes
Note
hey! i'm starting hrt soon (afab) and i really, really want to start working out bc i know t helps you build muscle and i really want to 1. get stronger and 2. help my body masculinize a bit. but im a weakling who has literally never exercised other than running. do y'all testosterone-taking folks have tips on what kinds of workouts you do, at home or at the gym, to work on muscle groups that will help w/ masc body shape and all that jazz? where do you learn to work out? thank
My number one tip is: be careful. Be so, so careful. While my experience with exercise has been kinda fraught because I’m multiply disabled, even totally abled people can easily hurt themselves with exercise. Start small, start slow, build up carefully, don’t do anything that you’re not sure how to do.
I’d recommend activity-based exercise more than like, gym-equipment-based exercise, tbh, because you get more bang for your buck in terms of engaging several muscle groups at the same time and it’s easier to quickly adjust what you’re doing in reaction to what your body needs.
So, running is good! Make sure you have appropriate shoes - you NEED arch support, and something to absorb the impact somewhat. Do not run in ballet flats. You will fuck up your legs and feet. If you have access to a pool, swimming is also really good, and gives you a whole-body workout. I know that bathing suits can be an uncomfortable gender thing, though, so it’s okay if you don’t feel comfortable with that. Sorta similar to running is hiking, which is fun because you can go at a slower pace but you’re also exercising your leg muscles differently. Running on a flat surface is different from going up an incline. Also sometimes you see lizards, and isn’t that what everyone wants from their exercise experience?
As far as masculinizing body shape goes, you’ll want to do stuff that engages your shoulders, chest, and arms, but I can’t really give advice on what to do there besides “swim” and “lift small animals” and “carry boxes of donation books into the library.” There are exercises you can do at home - pushups spring to mind - that will help with muscle growth in this area, but I’m hesitant to recommend that because it’s really easy to do them wrong and hurt yourself. Ditto for weight lifting. If this is really important to you, I’d recommend seeking out some kind of in-person class in something you’re interested in that will involve exercise, like martial arts or carpentry, so you can have someone who knows what they’re doing correct your form if you’re doing something that could hurt you.
You may also find, as many people on T have, that your daily routine already involves stuff that builds muscle, and the muscle you’re building suddenly becomes super obvious on T. “Carrying my fifteen-pound dog like a baby” was not something I expected would solidify my biceps and triceps, but here we are.
- Mod Rabbit
49 notes
·
View notes
Last Seen Blogs

bs-do-c
bs do c

daftynews-blog
Dafty News
daftynews-blog
Dafty News

blog-by-alan-blog
Just Blogging Along

kajalrawat26
Kajal Rawat