#cardiovascular care center
Text
Starling Diagnostics

Starling Diagnostics is in the Parkchester community of the Bronx, New York. We are also considered a modern health center in the tri-state area proudly offering a personalized and tailored approach to all your healthcare needs. If you’re new to Starling Diagnostics, please take a moment to discover why physicians and patients alike choose us when scheduling medical services. We offer a team of highly trained and experienced board-certified radiologists and technologists, specializing in all aspects of medical imaging. For our patients, we have invested in state-of-the-art equipment, including 3T MRI, CT scan, 3D Mammography, ultrasound, digital X-ray, and DEXA bone density scans.
Business Hours: Mon — Fri : 9 am–4 pm , Sat-Sun: 10 am–4 pm
Payment Methods: Visa, MC, PayPal, Amex, Discover, Cash, Gold
Year Establish: 2007
Contact Info:
Starling Diagnostics
Address: 1480 East Ave , Bronx, NY, USA 10462
Phone Number: (718) 319–1610
Website: http://starlingdiagnostics.com/
Business Email: [email protected]




#diagnostics services#diagnostic imaging patient portal#diagnostic treatment center#walk in clinic#treatment center Bronx#Primary Care#Gynecology care#Cardiovascular care#Orthopedics care
1 note
·
View note
Text
Comprehensive Cardiac Care at Morristown Heart Associates
Explore comprehensive cardiac care at Morristown Heart Associates. Our dedicated team of specialists offers expert diagnosis, treatment, and support for all your heart health needs. With a patient-centered approach and cutting-edge technology, we ensure personalized care and effective management of cardiovascular conditions. Contact Morristown Heart Associates today to prioritize your heart health and schedule a consultation with our experienced team.
#morristown medical center cardiology#morristown hospital cardiology#cardiologist hospital morristown#morristown hospital cardiologist#morristown heart associates#cardiovascular care services in morristown#morristown heart associates nj
0 notes
Text

#heart care center#heart hospital#cardiac hospital in gurgaon#heart care hospital#cardiovascular#cardiacarrest#heart disease#heart specialist#heartattack#Cardiac Hospital in Patna#Heart Hospital in Patna#Top Heart Hospital in Patna#Best Heart Hospital in Patna#Best Cardiac Hospital in Patna
0 notes
Text
web of wyrd: annual energies and potential surgeries associated with the year
the outer rim of the wyrd web foretells the themes of our year ahead. today i will be covering some common surgeries that tend to occur. in no way does one number mean a single surgery type. each number can mean different surgeries - multiple surgeries - no surgery... this is just what i associate medically with these energies and i have seen correlate with other charts when surgery occurred. your lack of a number correlation with an experience below does not mean to minimize your experience. this is a general hypothesis not a fact.
tw: sensitive topics like amputation, ivf, addiction, weight, physical trauma, and end of life care are included in post.
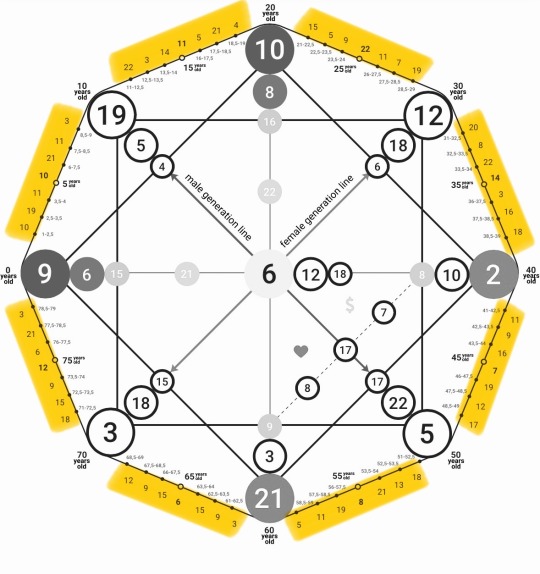
1 (the magician): laser surgery
skill, precision, and transformation. this technique uses precision tools to create change in the body.
2 (the high priestess): diagnostic surgery
intuition, secrets, and hidden knowledge. seeks to uncover hidden issues or provide clarity about a medical condition (will be common for 2000 baby around the time doctors start recommending colonoscopies and mammograms).
3 (the empress): fertility surgery
surgeries like in vitro fertilization (IVF) or other fertility-related procedures.
4 (the emperor): orthopedic surgery
structure and stability. anything involves bones, joints, and structural support of the body, resonates with this energy.
5 (the hierophant): cardiovascular or oral surgery
what maintains order/structure in the body a.k.a. anything dealing with the heart and blood flow. oral surgery is because of this card connection to the throat and sharing of beliefs which requires the mouth - it might be time for your wisdom teeth extraction.
6 (the lovers): cosmetic or reconstructive surgery
this is often elective surgery / chosen for personal reasons related to self-image.
7 (the chariot): neurosurgery
deals with the brain and nervous system (the body's control center), which aligns with the chariot's themes of mastery and control.
8 (strength): physical rehabilitation surgery
requires a lot of resilience as muscles and tendons aren't easy to heal...
9 (the hermit): gastrointestinal surgery
involves the digestive system, relates to the internal processes and inner workings (aligning with hermit energy).
10 (the wheel of fortune): emergency surgery
often needed unexpectedly and dictated by fate, aligns with the theme of chance.
11 (justice): corrective surgery
aims to fix or balance out bodily functions or appearance, mirrors the themes of rectifying and balancing.
12 (the hanged man): organ transplant
sacrifice, suspension, and new perspectives. transplant surgery involves the sacrifice of one organ for the life of another, offering a new lease on life.
13 (death): amputation
a literal removal or ending of a part of the body, that can also lead to a transformative process of healing and adapting.
14 (temperance) : bariatric surgery
used to achieve weight balance and improve health.
15 (the devil): addiction, breast reduction, and reproductive surgery
surgeries that address addiction-related issues, such as gastric banding for overeating. but also reproductive surgery like a tubal ligation or vasectomy. any surgery where something big/open becomes small, constricted, snipped, or thinned.
16 (tower): trauma surgery
sudden upheaval, destruction, and revelation. this type of surgery is often performed in response to sudden, life-altering accidents or injuries, echoes the energies themes of sudden change and crisis.
17 (the star): reconstructive/plastic surgery
hope, healing, and renewal are themes of this energy - this surgery which restores form and function after trauma or illness, aligns with the themes of healing and rejuvenation.
18 (the moon): biopsies and tissue collections
biopsy involves extracting tissue to investigate potential issues, often when there’s uncertainty about a diagnosis or the presence of something hidden (like tumors or other abnormalities).
19 (the sun): pediatric surgery
performed on children and ensures their health and vitality, which connects with the energy's themes of life, energy, and well-being.
20 (judgment): organ transplant or some other life changing/saving surgery
life-saving surgeries, such as heart or organ transplants, can offer a second chance at life, reflecting the energy's themes of renewal and awakening.
21 (the world): making a full recovery or end-of-life care
surgeries that lead to a full recovery or decisions around end-of-life care align with the themes of closure and achieving a state of completeness found with this energy.
22 (the fool): exploratory surgery
represents the unknown. aligns with entering a medical situation without knowing what will be found.
like what you read? leave a tip and state what post it is for! please use my "suggest a post topic." button if you want to see a specific topic or theme next!
click here for the masterlist
click here for more web of wyrd related posts
want a personal reading? click here to check out my reading options and prices.
© a-d-nox 2024 all rights reserved
#astrology#astro community#natal chart#astrology tumblr#tarot witch#tarot art#daily tarot#rider waite tarot#tarot deck#tarot reading#tarot cards#tarot#tarotblr#tarotcommunity#tarotdaily#wyrd web#web of wyrd#matrix of destiny#destiny matrix#matrix of fate#the matrix
76 notes
·
View notes
Text

Welcome to Leo season, lovelies! LEO, THE LION, is ruled by the SUN ☉, which represents divine intellect, spirit, life force, expression, willpower, heart functions, heat regulation, sight, and metabolism.
LEO ♌︎ embodies vitality, self-expression, creativity, and playfulness, governing the heart, major blood vessels, spinal cord, and back. With the Sun returning home to Leo, we experience radiant vitality, as the Sun enhances our life force, solar plexus, and heart function. Leo, as a fixed fire sign, boosts our cardiovascular health, creative willpower, and unique expression.
As the Sun moves into Leo, we are invited to embrace our inner radiance and shine with confidence. This season is all about tapping into our authentic selves and living from the heart. 🌟
🌞 Life Force and Willpower: Leo season magnifies our energy and determination. It’s the perfect time to take charge of your life, pursue your passions, and lead with boldness.
❤️ Heart-Centered Living: With Leo ruling the heart and major blood vessels, focus on activities that support both physical and emotional heart health. Truly practice gratitude, compassion, and self-love. Love motivates all our actions.
🎨 Creative Expression and Joy: Leo encourages us to express our creativity and find joy in everyday moments. Engage in artistic pursuits, playful activities, and anything that sparks your inner joy.
🔥 Sustained Vitality: The Sun in Leo reminds us to maintain our vitality through self-care and a balanced lifestyle. Prioritize what energizes you and sustains your spirit.
During this vibrant Leo season, let your unique light shine. Embrace your passions, express yourself fully, and lead with your heart. 🌞♌️
#astrology#astro observations#astro notes#astro community#leo#leo season#summer#astro#astro blog#astrology tips#ancient astrology#astrological transits#astrologer#astral#sensualnoiree#astrology chart#astrology readings#astrology signs#astro placements#astro posts#astroblr#astrology fyp#astrology notes#astrology observations#astronotes#astr
59 notes
·
View notes
Text
When Swiss cardiologist Thomas F. Lüscher attended an international symposium in Turin, Italy, last summer, he encountered an unusual “attendee:” Suzanne, Chat GPT’s medical “assistant.” Suzanne’s developers were eager to demonstrate to the specialists how well their medical chatbot worked, and they asked the cardiologists to test her.
An Italian cardiology professor told the chatbot about the case of a 27-year-old patient who was taken to his clinic in unstable condition. The patient had a massive fever and drastically increased inflammation markers. Without hesitation, Suzanne diagnosed adult-onset Still’s disease. “I almost fell off my chair because she was right,” Lüscher remembers. “This is a very rare autoinflammatory disease that even seasoned cardiologists don’t always consider.”
Lüscher — director of research, education and development and consultant cardiologist at the Royal Brompton & Harefield Hospital Trust and Imperial College London and director of the Center for Molecular Cardiology at the University of Zürich, Switzerland — is convinced that artificial intelligence is making cardiovascular medicine more accurate and effective. “AI is not only the future, but it is already here,” he says. “AI and machine learning are particularly accurate in image analysis, and imaging plays an outsize role in cardiology. AI is able to see what we don’t see. That’s impressive.”
At the Royal Brompton Hospital in London, for instance, his team relies on AI to calculate the volume of heart chambers in MRIs, an indication of heart health. “If you calculate this manually, you need about half an hour,” Lüscher says. “AI does it in a second.”
AI-Assisted Medicine
Few patients are aware of how significantly AI is already determining their health care. The Washington Post tracks the start of the boom of artificial intelligence in health care to 2018. That’s when the Food and Drug Administration approved the IDx-DR, the first independent AI-based diagnostic tool, which is used to screen for diabetic retinopathy. Today, according to the Post, the FDA has approved nearly 700 artificial intelligence and machine learning-enabled medical devices.
The Mayo Clinic in Rochester, Minnesota, is considered the worldwide leader in implementing AI for cardiovascular care, not least because it can train its algorithms with the (anonymized) data of more than seven million electrocardiograms (ECG). “Every time a patient undergoes an ECG, various algorithms that are based on AI show us on the screen which diagnoses to consider and which further tests are recommended,” says Francisco Lopez-Jimenez, director of the Mayo Clinic’s Cardiovascular Health Clinic. “The AI takes into account all the factors known about the patient, whether his potassium is high, etc. For example, we have an AI-based program that calculates the biological age of a person. If the person in front of me is [calculated to have a biological age] 10 years older than his birth age, I can probe further. Are there stressors that burden him?”
Examples where AI makes a sizable difference at the Mayo Clinic include screening ECGs to detect specific heart diseases, such as ventricular dysfunction or atrial fibrillation, earlier and more reliably than the human eye. These conditions are best treated early, but without AI, the symptoms are largely invisible in ECGs until later, when they have already progressed further...
Antioniades’ team at the University of Oxford’s Radcliffe Department of Medicine analyzed data from over 250,000 patients who underwent cardiac CT scans in eight British hospitals. “Eighty-two percent of the patients who presented with chest pain had CT scans that came back as completely normal and were sent home because doctors saw no indication for a heart disease,” Antioniades says. “Yet two-thirds of them had an increased risk to suffer a heart attack within the next 10 years.” In a world-first pilot, his team developed an AI tool that detects inflammatory changes in the fatty tissues surrounding the arteries. These changes are not visible to the human eye. But after training on thousands of CT scans, AI learned to detect them and predict the risk of heart attacks. “We had a phase where specialists read the scans and we compared their diagnosis with the AI’s,” Antioniades explains. “AI was always right.” These results led to doctors changing the treatment plans for hundreds of patients. “The key is that we can treat the inflammatory changes early and prevent heart attacks,” according to Antioniades.
The British National Health Service (NHS) has approved the AI tool, and it is now used in five public hospitals. “We hope that it will soon be used everywhere because it can help prevent thousands of heart attacks every year,” Antioniades says. A startup at Oxford University offers a service that enables other clinics to send their CT scans in for analysis with Oxford’s AI tool.
Similarly, physician-scientists at the Smidt Heart Institute and the Division of Artificial Intelligence in Medicine at Cedars-Sinai Medical Center in Los Angeles use AI to analyze echograms. They created an algorithm that can effectively identify and distinguish between two life-threatening heart conditions that are easy to overlook: hypertrophic cardiomyopathy and cardiac amyloidosis. “These two heart conditions are challenging for even expert cardiologists to accurately identify, and so patients often go on for years to decades before receiving a correct diagnosis,” David Ouyang, cardiologist at the Smidt Heart Institute, said in a press release. “This is a machine-beats-man situation. AI makes the sonographer work faster and more efficiently, and it doesn’t change the patient experience. It’s a triple win.”
Current Issues with AI Medicine
However, using artificial intelligence in clinical settings has disadvantages, too. “Suzanne has no empathy,” Lüscher says about his experience with Chat GPT. “Her responses have to be verified by a doctor. She even says that after every diagnosis, and has to, for legal reasons.”
Also, an algorithm is only as accurate as the information with which it was trained. Lüscher and his team cured an AI tool of a massive deficit: Women’s risk for heart attacks wasn’t reliably evaluated because the AI had mainly been fed with data from male patients. “For women, heart attacks are more often fatal than for men,” Lüscher says. “Women also usually come to the clinic later. All these factors have implications.” Therefore, his team developed a more realistic AI prognosis that improves the treatment of female patients. “We adapted it with machine learning and it now works for women and men,” Lüscher explains. “You have to make sure the cohorts are large enough and have been evaluated independently so that the algorithms work for different groups of patients and in different countries.” His team made the improved algorithm available online so other hospitals can use it too...
[Lopez-Jimenez at the Mayo Clinic] tells his colleagues and patients that the reliability of AI tools currently lies at 75 to 93 percent, depending on the specific diagnosis. “Compare that with a mammogram that detects breast tumors with an accuracy of 85 percent,” Lopez-Jimenez says. “But because it’s AI, people expect 100 percent. That simply does not exist in medicine.”
And of course, another challenge is that few people have the resources and good fortune to become patients at the world’s most renowned clinics with state-of-the-art technology.
What Comes Next
“One of my main goals is to make this technology available to millions,” Lopez-Jimenez says. He mentions that Mayo is trying out high-tech stethoscopes to interpret heart signals with AI. “The idea is that a doctor in the Global South can use it to diagnose cardiac insufficiency,” Lopez-Jimenez explains. “It is already being tested in Nigeria, the country with the highest rate of genetic cardiac insufficiency in Africa. The results are impressively accurate.”
The Mayo Clinic is also working with doctors in Brazil to diagnose Chagas disease with the help of AI reliably and early. “New technology is always more expensive at the beginning,” Lopez-Jimenez cautions, “but in a few years, AI will be everywhere and it will make diagnostics cheaper and more accurate.”
And the Children’s National Hospital in Washington developed a portable AI device that is currently being tested to screen children in Uganda for rheumatic heart disease, which kills about 400,000 people a year worldwide. The new tool reportedly has an accuracy of 90 percent.
Both Lopez-Jimenez and Lüscher are confident that AI tools will continue to improve. “One advantage is that a computer can analyze images at 6 a.m. just as systematically as after midnight,” Lüscher points out. “A computer doesn’t get tired or have a bad day, whereas sometimes radiologists overlook significant symptoms. AI learns something and never forgets it.”
-via Reasons to Be Cheerful, March 1, 2024. Headers added by me.
--
Note:
Okay, so I'm definitely not saying that everything with AI medicine will go right, and there won't be any major issues. That's definitely not the case (the article talks about some of those issues). But regulation around medicines is generally pretty tight, and
And if it goes right, this could be HUGE for disabled people, chronically ill people, and people with any of the unfortunately many marginalizations that make doctors less likely to listen.
This could shave years off of the time it takes people to get the right diagnosis. It could get answers for so many people struggling with unknown diseases and chronic illness. If we compensate correctly, it could significantly reduce the role of bias in medicine. It could also make testing so much faster.
(There's a bunch of other articles about all of the ways that AI diagnoses are proving more sensitive and more accurate than doctors. This really is the sort of thing that AI is actually good at - data evaluation and science, not art and writing.)
This decade really is, for many different reasons, the beginning of the next revolution in medicine. Luckily, medicine is mostly pretty well-regulated - and of course that means very long testing phases. I think we'll begin to really see the fruits of this revolution in the next 10 to 15 years.
#confession I always struggle a lil bit with taking the mayo clinic seriously#because every. single. time I see it mentioned my first thought is mayonnaise#the mayonnaise clinic#lol
140 notes
·
View notes
Text
Louisiana COVID levels among the highest in the country as school starts. See the data. - Published Aug 9, 2024
A COVID-19 summer surge continues to mount in Louisiana, according to the latest federal data. Louisiana has the second-highest level of COVID-19 in wastewater in the country, behind only Utah.
Four years after the first COVID-19 cases were announced in the state, Louisiana has retired some of the tools for tracking the spread of the virus. Mask-wearing, regular testing and sanitizing efforts have also fallen by the wayside. However, rising wastewater levels, hospitalizations and emergency room visits for cold-like symptoms show that COVID is still a presence.
“There is clearly virus circulating,” said Susan Hassig, an infectious disease epidemiologist and associate professor emerita at Tulane University. “I would suggest it’s at much higher levels than people are even contemplating.”
Although the virus is not the hazard it was in previous years, it can still be dangerous to people with compromised immune systems. That includes people in places like nursing homes, but could also extend to the workplace, especially in an aging population, said Hassig.
“Nobody necessarily knows who in their workplace has cardiovascular disease, hypertension, diabetes or other underlying conditions, even asthma, that may be problematic if they get COVID,” said Hassig.
Louisiana has a large burden of chronic disease, with over 60% of the population having at least one condition such as dementia, heart disease or another illness. Many of those conditions make it harder for the body to fight off and recover from COVID-19.
Fanning the flame
It’s those patients that Dr. David Janz, a critical care pulmonologist, is seeing with COVID-19 at LCMC Health’s eight-hospital system in the New Orleans area. Systemwide, COVID has increased tenfold over the last three months.
There are 44 hospitalized patients who are positive for COVID across LCMC’s hospitals right now compared to 4 patients before the summer surge. In these patients, COVID is fanning a flame.
“Now, COVID just seems to be the straw that broke the camel's back in some patients that have just a lot of other medical conditions,” said Janz, the director of medical critical care services at University Medical Center. “And this one new respiratory infection was enough to kind of tip them over the edge.”
Over 2,000 people visited the emergency room for COVID-19 in Louisiana during the week ending July 27, according to the most recent data available. The highest percentage of those visits were among children under two, followed by ages two to four.
Back to school
With school starting, the surge could continue.
“Any time you put a lot of people together in a room, there is the chance of spreading any respiratory illness,” said Janz.
While ER visits and hospitalizations are still on the upslope, the rate has slowed, he said, indicating the spread may start to level and drop soon.
COVID-19 has settled into a twice-yearly surge pattern, making a winter wave likely. When COVID does reemerge, it will be on top of other respiratory illnesses that start to rage in winter such as RSV and flu. That strains how hospitals can care for people with conditions like heart attacks and stroke, especially in rural areas.
“The hospitals just get too full and too busy to be able to care for all these other conditions,” said Janz.
Janz said a newly formulated vaccine that contains the variants currently circulating could be available as soon as the end of this month.
5 notes
·
View notes
Text
Rheumatoid Arthritis:
Refer to rheumatologist.
●Nonpharmacologic measures – Nonpharmacologic measures, such as patient education, psychosocial interventions, and physical and occupational therapy, should be used in addition to drug therapy. Other medical interventions that are important in the comprehensive management of RA in all stages of disease include cardiovascular risk reduction and immunizations to decrease the risk of complications of drug therapies.
●Initiation of DMARD therapy soon after RA diagnosis – We suggest that all patients diagnosed with RA be started on disease-modifying antirheumatic drug (DMARD) therapy as soon as possible following diagnosis, rather than using antiinflammatory drugs alone, such as nonsteroidal antiinflammatory drugs (NSAIDs) and glucocorticoids (Grade 2C). Better outcomes are achieved by early compared with delayed intervention with DMARDs.
●Tight control of disease activity – Tight control treatment strategies to "treat to target" are associated with improved radiographic and functional outcomes compared with less aggressive approaches. Such strategies involve reassessment of disease activity on a regularly planned basis with the use of quantitative composite measures and adjustment of treatment regimens to quickly achieve and maintain control of disease activity if targeted treatment goals (remission or low disease activity) have not been achieved. (
●Pretreatment evaluation – Laboratory testing prior to therapy should include a complete blood count, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), aminotransferases, blood urea nitrogen, and creatinine. Patients receiving hydroxychloroquine (HCQ) should have a baseline ophthalmologic examination, and most patients who will receive a biologic agent or Janus kinase (JAK) inhibitor should be tested for latent tuberculosis (TB) infection. Screening for hepatitis B and C should be performed in all patients. Some patients may require antiviral treatment prior to initiating DMARD or immunosuppressive therapy, depending upon their level of risk for hepatitis B virus (HBV) reactivation.
●Adjunctive use of antiinflammatory agents – We use antiinflammatory drugs, including NSAIDs and glucocorticoids, as bridging therapies to rapidly achieve control of inflammation until DMARDs are sufficiently effective. Some patients may benefit from longer-term therapy with low doses of glucocorticoids.
●Drug therapy for flares – RA has natural exacerbations (also known as flares) and reductions of continuing disease activity. The severity of the flare and background drug therapy influence the choice of therapies. Patients who require multiple treatment courses with glucocorticoids for recurrent disease flares and whose medication doses have been increased to the maximally tolerated or acceptable level should be treated as patients with sustained disease activity. Such patients require modifications of their baseline drug therapies.
●Monitoring – The monitoring that we perform on a regular basis includes testing that is specific to evaluation of the safety of the drugs being; periodic assessments of disease activity with composite measures; monitoring for extraarticular manifestations of RA, other disease complications, and joint injury; and functional assessment.
●Other factors affecting target and choice of therapy – Other factors in RA management that may influence the target or choice of therapy include the disabilities or functional limitations important to a given patient, progressive joint injury, comorbidities, and the presence of adverse prognostic factors.
Osteoarthritis
General principles – General principles of osteoarthritis (OA) management include providing continuous care that is tailored to the patient according to individual needs, goals, and values and should be patient-centered. Treatment can be optimized by OA and self-management education, establishing treatment goals, and periodic monitoring.
●Monitoring and assessment – The management of OA should include a holistic assessment which considers the global needs of the patient. Patient preferences for certain types of therapies should also be assessed, as compliance and outcomes can be compromised if the care plan does not meet the patient's preferences and beliefs.
●Overview of management – The goals of OA management are to minimize pain, optimize function, and beneficially modify the process of joint damage. The primary aim of clinicians should include targeting modifiable risk factors. Due to the modest effects of the individual treatment options, a combination of therapeutic approaches is commonly used in practice and should prioritize therapies that are safer.
●Nonpharmacologic therapy – Nonpharmacologic interventions are the mainstay of OA management and should be tried first, followed by or in concert with medications to relieve pain when necessary. Nonpharmacologic therapies including weight management and exercises, braces and foot orthoses for patients suitable to these interventions, education, and use of assistive devices when required.
●Pharmacologic therapy – The main medications used in the pharmacologic management of OA include oral and topical nonsteroidal antiinflammatory drugs (NSAIDs). Other options include topical capsaicin, duloxetine, and intraarticular glucocorticoids. Our general approach to pharmacotherapy is described below.
•In patients with one or a few joints affected, especially knee and/or hand OA, we initiate pharmacotherapy with topical NSAIDs due to their similar efficacy compared with oral NSAIDs and their better safety profile.
•We use oral NSAIDs in patients with inadequate symptom relief with topical NSAIDs, patients with symptomatic OA in multiple joints, and/or patients with hip OA. We use the lowest dose required to control the patient's symptoms on an as-needed basis.
•We use duloxetine for patients with OA in multiple joints and concomitant comorbidities that may contraindicate oral NSAIDs and for patients with knee OA who have not responded satisfactorily to other interventions.
•Topical capsaicin is an option when one or a few joints are involved and other interventions are ineffective or contraindicated; however, its use may be limited by common local side effects.
•We do not routinely use intraarticular glucocorticoid injections due to the short duration of its effects (ie, approximately four weeks).
•We avoid prescribing opioids due to their overall small effects on pain over placebo and potential side effects (eg, nausea, dizziness, drowsiness), especially for long-term use and in the older adult population.
•We do not routinely recommend nutritional supplements such as glucosamine, chondroitin, vitamin D, diacerein, avocado soybean unsaponifiables (ASU), and fish oil due to a lack of clear evidence demonstrating a clinically important benefit from these supplements. Other nutritional supplements of interest that may have small effects on symptoms include curcumin (active ingredient of turmeric) and/or Boswellia serrata, but the data are limited.
●Role of surgery – Surgical treatment is dominated by total joint replacement, which is highly effective in patients with advanced knee and hip OA when conservative therapies have failed to provide adequate pain relief.
●Factors affecting response to therapy – The discordance of radiographic findings to pain supports the notion that the mechanisms of pain are complex and likely multifactorial. The placebo effect is also known to impact response to therapy.
●Prognosis – Although there is great variability among individuals and among different phenotypes of OA, courses of pain and physical functioning have been found to be predominantly stable, without substantial improvement or deterioration of symptoms over time.
4 notes
·
View notes
Text

Unlocking Vitality: The Importance of Cardiovascular Health
Cardiovascular health is the cornerstone of overall well-being, yet it is often overlooked in our busy lives. The heart and circulatory system play a vital role in sustaining life, delivering oxygen and nutrients to every cell in the body. In this article, we will delve into the importance of cardiovascular health and explore how maintaining a healthy heart can enhance longevity, vitality, and quality of life.
The Foundation of Vitality: At the center of our cardiovascular system is the heart, a powerful muscle that pumps blood throughout the body. The health of our heart and blood vessels, collectively known as the cardiovascular system, is essential for optimal functioning. When the heart is strong and efficient, it can deliver oxygen-rich blood to tissues and organs, supporting their growth, repair, and metabolic processes.
Preventing Chronic Disease: Maintaining cardiovascular health is crucial for preventing a range of chronic diseases, including heart disease, stroke, and hypertension. These conditions are leading causes of morbidity and mortality worldwide, yet they are largely preventable through lifestyle interventions. By adopting heart-healthy habits such as regular exercise, balanced nutrition, and stress management, individuals can reduce their risk of developing cardiovascular disease and enjoy a longer, healthier life.
Enhancing Physical Performance: Cardiovascular fitness, often measured by metrics such as aerobic capacity and VO2 max, is a key determinant of physical performance. A strong cardiovascular system enables the body to efficiently transport oxygen to working muscles during exercise, improving endurance, stamina, and overall athletic performance. Whether it's running a marathon, cycling up a steep hill, or simply climbing stairs without getting winded, a healthy heart is essential for optimal physical performance.
Boosting Energy Levels: Cardiovascular health is closely linked to energy levels and vitality. When the heart and circulatory system are functioning optimally, oxygen and nutrients are efficiently delivered to cells throughout the body, fueling metabolic processes and supporting cellular energy production. Individuals with good cardiovascular health often report higher levels of energy, improved mood, and greater resilience to stress. By prioritizing cardiovascular wellness, individuals can experience a sustained boost in energy levels and overall vitality.
Supporting Brain Health: The link between cardiovascular health and brain health is well established. A healthy heart ensures an adequate supply of blood and oxygen to the brain, supporting cognitive function, memory, and mental clarity. Research has shown that individuals with poor cardiovascular health are at increased risk of cognitive decline and neurodegenerative diseases such as Alzheimer's. By maintaining a healthy heart, individuals can support brain health and reduce their risk of age-related cognitive decline.
Promoting Longevity and Quality of Life: Perhaps most importantly, cardiovascular health is closely associated with longevity and quality of life. Studies have consistently shown that individuals with good cardiovascular health tend to live longer, healthier lives compared to those with poor heart health. By adopting heart-healthy habits and prioritizing preventive care, individuals can enjoy a higher quality of life well into their later years. Whether it's spending time with loved ones, pursuing passions and interests, or simply enjoying everyday activities, a healthy heart is the foundation for a fulfilling and vibrant life.
Conclusion: Cardiovascular health is the cornerstone of overall well-being, impacting every aspect of our physical, mental, and emotional health. By prioritizing heart-healthy habits such as regular exercise, balanced nutrition, stress management, and preventive care, individuals can enhance longevity, vitality, and quality of life. Whether you're striving to prevent chronic disease, improve physical performance, boost energy levels, support brain health, or promote longevity, investing in cardiovascular wellness is an essential step toward unlocking vitality and embracing a life of health and happiness.
#healthy lifestyle#health#wellness#healthy living#health tips#health and wellness#gym#prevention#diet#healthcare#cardiovascular#tumblr milestone#fitness#working out#nutrition#energy
6 notes
·
View notes
Text
Fuck global warming, it’s 52 in February in Michigan! All I needed this morning was my hoodie and it was fucking HOT in the hospital but I was cheeky and didn’t wear a bra today because of my oversized hoodie and man did I regret it, my big naturals need a bra lol I had my annual heart appointment this morning though so I would have had to take it off anyway so I said fuck it entirely. This morning was so stressful, my blood draw was really easy so very thankful for that but the hospital app was down this morning so we didn’t know where to go and the front desk sent us to the main hospital’s PET scan department when I apparently needed to be in the PET scan department in the cardiovascular center. So, I had to walk all over the various buildings to finally get to the right department and was a tad late but thankfully I was the only appointment so it wasn’t a big deal. For fucking once in my life they got the IV in the first try 😭 I almost cried, I’m such a hard stick it usually takes 4-5 attempts to start an IV on me. So, I was very thankful it went in so easily, it burned really badly though, or at least the medication did. They inject you with radioactive dye to make everything show up and then give you medication to simulate exercise all while you’re in an MRI machine to get imaging of the heart. It’s such a weird sensation, you go from half falling asleep to suddenly feeling like your sprinting in seconds, it’s not necessarily unpleasant but it is odd but like I mentioned earlier the medication burned quite a bit going in. The imaging was apparently sufficient even though the drug didn’t do its job as well as it was supposed to because they sent me home in a timely fashion. I got back home and took a very long nap and apparently the girl who wrapped my IV didn’t wrap it tight enough because the dresssing was soaked in blood when I took it off later. It’s bruised but not awfully. All in all things went better than they could have. Downside my labs aren’t good at all. My tacrolimus level is an 8 it’s supposed to be between 4-6, so that’s not good but reasonably easy to fix, they’ll just lower my dose again and repeat labs next week most likely. The really bad thing though is my liver is crazy out of whack again, which really blows. It might be as easily explained as my enzymes are spiked because I just got over the flu but last time it was this high is when I had CMV. I’ll get my results for the CMV test tomorrow. In more news no one cares about but I over share is my parathyroid is very high which is actually good because it finally explains my chronic fatigue and weird appetite lately. Hopefully they can get it under control and my energy levels will return and I might be able to do things again. In small good things my kidneys are stable, they’re stage 3b kidney failure but they’ve also been there for like 7 years so they’re not getting worse, dance party time.
TL:DR: I’m still dying slowly but instead of just my heart and kidneys doing the dirty work now my liver is back on board for murder too.
9 notes
·
View notes
Text
Can I Exercise During Pregnancy?
Pregnancy is a transformative experience, often accompanied by a myriad of questions about health and well-being. One common query among expectant mothers is, "Can I exercise during pregnancy?" The short answer is yes, but with some important considerations. Exercising during pregnancy can offer numerous benefits for both the mother and the baby, provided it is done safely and under medical guidance. In this blog, we'll explore the advantages of prenatal exercise and provide tips for staying active, with insights from the experts at the best fertility clinic in Delhi, SCI IVF Hospital.
Benefits of Exercising During Pregnancy
Engaging in regular physical activity during pregnancy can lead to numerous health benefits, including:
Improved Mood and Energy Levels: Exercise can help alleviate common pregnancy symptoms such as fatigue and mood swings by boosting endorphin levels.
Better Sleep: Regular physical activity can improve sleep patterns, helping expectant mothers get the rest they need.
Reduced Pregnancy Discomfort: Exercise can help alleviate back pain, swelling, and constipation, which are common complaints during pregnancy.
Easier Labor and Delivery: Strengthening the body through exercise can lead to a smoother labor and delivery process.
Faster Postpartum Recovery: Women who exercise during pregnancy often experience quicker recovery post-birth.
Safe Exercise Practices
While exercise is beneficial, it is essential to approach it with caution during pregnancy. Here are some tips from the best IVF doctor in Delhi to ensure safe prenatal workouts:
Consult Your Healthcare Provider: Before starting any exercise regimen, it's crucial to get the green light from your healthcare provider, especially if you have any pregnancy complications.
Choose Low-Impact Activities: Opt for low-impact exercises such as walking, swimming, prenatal yoga, and stationary cycling. These activities are gentle on the joints and reduce the risk of injury.
Stay Hydrated and Avoid Overheating: Drink plenty of water before, during, and after exercise. Avoid exercising in hot, humid conditions to prevent overheating.
Listen to Your Body: Pay attention to how your body feels during exercise. If you experience dizziness, shortness of breath, or any unusual symptoms, stop immediately and consult your doctor.
Modify as Needed: As your pregnancy progresses, you may need to modify your exercise routine. Avoid activities that involve lying flat on your back after the first trimester and exercises that pose a risk of falling or abdominal trauma.
Exercise Recommendations
The experts at SCI IVF Hospital suggest incorporating the following types of exercise into your routine:
Aerobic Exercise: Activities like walking, swimming, and dancing can help maintain cardiovascular fitness without putting too much strain on your body.
Strength Training: Light resistance training with weights or resistance bands can help maintain muscle tone. Focus on exercises that target major muscle groups.
Flexibility and Balance: Prenatal yoga and stretching exercises can improve flexibility and balance, which are beneficial as your center of gravity shifts.
Pelvic Floor Exercises: Strengthening the pelvic floor muscles through Kegel exercises can help prevent urinary incontinence and prepare the body for childbirth.
Seeking Professional Guidance
For personalized advice and support, consider consulting with specialists from the best fertility clinic in Delhi. At SCI IVF Hospital, the best IVF doctors provide comprehensive care and guidance for expectant mothers. They can help tailor an exercise plan that meets your specific needs and ensures the health and safety of both you and your baby.
Conclusion
Exercising during pregnancy can be incredibly beneficial when done safely and thoughtfully. By following these guidelines and seeking advice from healthcare professionals, you can enjoy an active and healthy pregnancy. For expert care and support, trust the team at SCI IVF Hospital, the best fertility clinic in Delhi, where the best IVF doctors are dedicated to your well-being every step of the way.
4 notes
·
View notes
Text
Find The Best Cardiologist Hospital in Morristown
Looking for an exceptional cardiologist hospital in Morristown? Explore our distinguished hospital offering top-notch cardiac care and specialized treatment plans. Curious about our renowned cardiologists and advanced facilities? Discover more now!
#morristown medical center cardiology#morristown hospital cardiology#cardiologist hospital morristown#morristown hospital cardiologist#morristown heart associates#cardiovascular care services in morristown#morristown heart associates nj#cardiology associates of morristown#morristown cardiology associates#morristown cardiology
0 notes
Text
I've got an unexpected relatively short notice 9 a.m. blood pressure appointment at the nearby primary care center that I've only been in once for a blood draw. And I swear thinking about it tonight can't be doing my blood pressure any good.
Still not sure what's up with that, but I guess we'll find out soon enough. Whether I want to or not. Endocrinology was handling it, so I really have no idea why primary care is summoning me now. Maybe it has to do with my last endo leaving so I got reassigned to another one in the clinic, but idk.
My blood pressure always ran sort of low (like, 100/60 was on the high side for me before), classic EDS dysautonomia style. I had to watch out for medications that would incidentally affect blood pressure, unless I wanted to almost black out when I stood up and/or get fluid painfully swelling my feet up. Both of which did happen over the years.
But after that 2nd round of COVID which also left me with the fatigue, it went kinda fucky too. I suspect it may be connected to the pounding heart I've been getting more often too, but I really haven't wanted to get into that--especially because it does seem to be post-COVID bullshit. Don't know if they're more likely to dismiss it as all in my head, or freak the fuck out in unpleasant ways because cardiovascular symptoms. Don't particularly feel up to dealing with either possibility just now.
So yeah, I apparently really do need blood pressure meds these days, unexpected as it was. (As much as it concerns me, with some of the repeated "unusual ethnic liver chemistry-> unusual drug reactions/effects which too often get dismissed until you're in terrible shape" fits I watched my mom go through with BP meds for years. Mine is the same, we kept reacting in similar unexpected ways--and I am basically an ethnic minority of one, this far from home. 😒)
And somebody does need to follow up on that. But, it would be nice to have some continuity of care here, and more idea of wtf is even going on. Sudden last minute summons letters from a medical practice I have no prior relationship with do not increase my confidence in any of this.
It's also feeling too reminiscent of dealing with the freaking NHS, where the rest of it was amplified by getting treated like mushroom as SOP.
9 notes
·
View notes
Text
By: Leor Sapir
Published: Aug 19, 2023
There is no area of medicine more controversial than the treatment of children and adolescents who identify as transgender. The leading organization championing the early medicalization model, which recommends that kids receive puberty blockers, cross-sex hormones and even surgeries, is the World Professional Association for Transgender Health (WPATH). That organization, based in East Dundee, Ill., claims that its standards of care follow “the most rigorous protocol in the world to ensure these standards reflect scientific evidence and meet the needs of transgender patients.”
This is simply false.
In evidence-based medicine, trustworthy recommendations must rely on a systematic review of evidence. Prior to writing its latest standards of care, called SOC-8, WPATH commissioned such a review. That report, which included research subjects of any age, not just minors, concluded that there is an association between hormone therapy and improved quality of life for transgender people. But it noted that the quality of evidence for that association was “low,” due to concerns about study designs, small sample sizes and other factors.
It also said, “It was impossible to draw conclusions about the effects of hormone therapy on death by suicide.” Mysteriously, WPATH then claimed in SOC-8 that “a systematic review regarding outcomes of treatment in adolescents is not possible.”
WPATH’s systematic review is not the only one expressing low confidence in the benefits from early medical intervention. Health authorities in progressive Sweden, Finland and the U.K. have conducted their own reviews and every one of them yielded the same conclusion: The assertion that puberty blockers or cross-sex hormones help youths who identify as transgender live healthy lives is based on “very low” quality evidence. Focusing on SOC-8 unscientific claims about puberty blockers, the director of Belgium’s Center for Evidence-Based Medicine has said that he would “throw [WPATH’s guidelines] in the trash.”
Are there studies that claim hormones and surgeries help? Sure. But invariably, these studies suffer from severe methodological problems that demonstrably exaggerate the benefits and understate the risks. Crucially, and for good reason, even the Dutch studies, which gave rise to the practice of youth transitions worldwide, and which are recognized by WPATH itself as the gold standard of research in this area, have so many methodological flaws that European systematic reviews assessed them to be at “critical risk of bias.” Such is the state of pediatric gender medicine.
What about the risks? WPATH’s systematic review, whose lead author advocates for early medicalization, did not even bother to look at adverse effects. While the researchers originally planned to do so, as evident in the research protocol they filed, this intention disappeared before the review was done.
Sterility is all but assured for youth who undergo full gender transition, and WPATH’s own president has admitted that these kids will probably never experience orgasm later in life. Other risks, such as the adverse effects on bone, brain and cardiovascular health, are also expected but require further study.
It is precisely due to the problematic risk-benefit ratio of youth gender transition that Sweden, Finland and the U.K. — and Norway seems poised to join them — are backing away from gender affirming care.
“There is not enough evidence to support the safety, clinical effectiveness and cost effectiveness to make the treatment routinely available at this time,” England’s National Health Service declared. Sweden’s health authority found that “the risks of puberty-inhibiting and gender-affirming hormone treatment for those under 18 currently outweigh the possible benefits.”
Those health services now recommend psychosocial support and (as needed) psychotherapy to help deal with mental health issues as the main treatments for youth with gender dysphoria.
Proponents of gender-affirming care dismiss this approach, and with it, well-respected mental health supports such as cognitive behavioral therapy, as one based on “no evidence.” But this gets things exactly backward. It is the riskier and more invasive intervention — hormones and surgeries — that requires stronger evidence. Without that evidence, safer treatments should be used by default. First, do no harm.
Health authorities in Europe have now broken from WPATH, as the organization itself acknowledges, and reclassified early medicalization from the category of “medical treatment” to that of “an experimental practice.” As a result, youth gender transitions are confined to research settings, with the option to undergo transition restricted to exceptional and rare cases.
In short, European health experts are rejecting the narrative that has taken root within the world of activist-led U.S. medical associations, a narrative WPATH has done much to help propagate: that gender-affirming care is safe and effective, that it is based on settled science, and that there should be, as a result, “no debate” on the matter. There is indeed a growing consensus among international experts, but it is a consensus against WPATH’s approach.
WPATH’s SOC-8 has angered many in the medical community, and rightly so. In addition to falsely claiming that a systematic review of evidence is “not possible,” WPATH inexplicably decided to omit a chapter on ethics from the final version of SOC-8. It included, instead, a chapter on “eunuchs” in which it claims that young children can know they have a eunuch “gender identity.” Perhaps most alarmingly, a few days after SOC-8 was published, WPATH eliminated all age-minimum recommendations for puberty blockers, cross-sex hormones, and surgeries — including genital surgeries, with the exception of phalloplasty.
At the WPATH conference last September, Amy Tischelman, lead author of the SOC-8 chapter on children, candidly acknowledged that WPATH eliminated age-minimum recommendations to give doctors legal cover for performing invasive treatments on young patients. “What we didn’t want to do was create a chapter that would make it more likely that practitioners would be sued because they weren’t following exactly what we said,” she said.
Gender-affirming care activists assure onlookers that drugs and surgeries are offered only to “carefully selected patients.” That isn’t true either. A Reuters investigation last year interviewed providers at 18 pediatric gender clinics and found that none said they were following the purportedly more cautious “Dutch protocol,” despite WPATH and prominent “affirming” doctors saying that this approach is the most evidence-based and the one practiced in American clinics. The director of Boston Children’s Hospital gender clinic was caught admitting that the number of teenagers they were seeing “has skyrocketed” and that the clinic was handing out puberty blockers “like candy.”
These are but a few examples of doctors putting adolescents, most with underlying mental health problems and some with histories of family trauma and sexual abuse, in the driver’s seat of risky and irreversible medical decisions when they are at their most vulnerable.
When the gender-affirming care scandal comes to be known as the lobotomy of the 21st century, as inevitably it will, American medical groups will scramble to dissociate themselves from it, insisting that they were merely misunderstood. WPATH can make no such excuse. It exists chiefly, if not exclusively, to ensure access to experimental drugs and surgeries.
[ Via: https://archive.today/ku0OF ]
#Leor Sapir#medical malpractice#WPATH#medical transition#ideological corruption#ideological capture#medical scandal#gender thalidomide#gender lobotomy#medical corruption#queer theory#genderwang#gender ideology#sex trait modification#religion is a mental illness
18 notes
·
View notes
Photo




Black Paraphernalia have posted a overview excerpt summary of a NIH study that was done. This subject is a very near to our heart and we being health care professionals who read many research studies in general and understand the double and triple risk a black woman face on a day to day but especially when it come to maternal care in the United States started with SLAVERY.
We decided to do a few post on Black women and Childbirth disparities and injustices in the medical arena. The sad thing even as health care license professionals, we have experienced covert discrimination and disparity when it came to our own professional positions and personal health.
This is the first of a few posts that we will present in hopes of B1 community awareness. Please check out this post and others to come.
For the entire study click on the title to read in full.
Health Equity Among
Black Women in the United States
Journal of Women's Health NIH - The National Center for Biotechnology Information advances science and health
J Womens Health (Larchmt). February 2021; 30(2): 212–219.Published online 2021 Feb 2. doi: 10.1089/jwh.2020.8868
Black women in the United States experienced substantial improvements in health during the last century, yet health disparities persist. Black women continue to experience excess mortality relative to other U.S. women, including—despite overall improvements among Black women—shorter life expectancies and higher rates of maternal mortality.
Moreover, Black women are disproportionately burdened by chronic conditions, such as anemia, cardiovascular disease (CVD), and obesity. Health outcomes do not occur independent of the social conditions in which they exist.
The higher burden of these chronic conditions reflects the structural inequities within and outside the health system that Black women experience throughout the life course and contributes to the current crisis of maternal morbidity and mortality. The health inequities experienced by Black women are not merely a cross section of time or the result of a singular incident.
No discussion of health equity among Black women is complete unless it considers the impacts of institutional- and individual-level forms of racism and discrimination against Black people. Nor is a review of health equity among Black women complete without an understanding of the intersectionality of gender and race and the historical contexts that have accumulated to influence Black women's health in the United States.
Research consistently has documented the continued impacts of systematic oppression, bias, and unequal treatment of Black women. Substantial evidence exists that racial differences in socioeconomic, education and employment and housing outcomes among women are the result of segregation, discrimination, and historical laws purposed to oppress Blacks and women in the United States.
The intersectionality of gender and race and its impact on the health of Black women also is important. This intersection of race and gender for Black women is more than the sum of being Black or being a woman: It is the synergy of the two. Black women are subjected to high levels of racism, sexism, and discrimination at levels not experienced by Black men or White women.
In contrast to Black women, White women in the United States have benefited from living in a politically, culturally, and socioeconomically White-dominated society. These benefits accumulate across generations, creating a cycle of overt and covert privileges not afforded to Black women.
The history of Black women's access to health care and treatment by the U.S. medical establishment, particularly in gynecology, contributes to the present-day health disadvantages of Black women. Health inequality among Black women is rooted in slavery. White slaveholders viewed enslaved Black women as a means of economic gain, resulting in the abuse of Black women's bodies and a disregard for their reproductive health. Black women were forced to procreate, with little or no self-agency and limited access to medical care.
The development of gynecology as a medical specialty in the 1850s ushered in a particularly dark period for the health of Black women. With no regulations for the protection of human subjects in research, Black women were subjected to unethical experimentation without consent. Even in more contemporary times, these abuses continue.
As a result of this history and the accumulation of disadvantages across generations, Black women are at the center of a public health emergency. Maternal mortality rates for non-Hispanic Black women are three to four times the maternal mortality rates of non-Hispanic White women.In
Racism and gender discrimination have profound impacts on the well-being of Black women. Evidence-based care models that are informed by equity and reproductive justice frameworks (reproductive rights as human rights need to be explored to address disparities throughout the life course, including the continuum of maternity care, and to ensure favorable outcomes for all women.
Health does not exist outside its social context. Without equity in social and economic conditions, health equity is unlikely to be achieved,and one cost of health inequality has been the lives of Black women.
The above is a summary excerpt take from the study by the Journal of Women's Health NIH - The National Center for Biotechnology Information advances science and health
BLACK PARAPHERNALIA DISCLAIMER - PLEASE READ
#black paraphernalia#disparity in black women health care#maternal deaths in healthcare with black women#the worst sight
11 notes
·
View notes
Text
How to Care for the Fidough Line
Fidough and Dachsbun are domesticated canines that come in a variety of breeds. The league standard breed has some noteable differences from those found in households or agriculture, including size, temperment, coat color and length, and the potency and flavor of their yeast.
Dachsbun in captivity will usually give live birth, a litter of two to six or more pups, rather than lay eggs. Not much research has been done on the breeding habits of wild Fidough and Dachsbun, as they are not meant to be feral. Instead, efforts are focused on rounding up the doughy dogs to prevent an ecological upset.
Newborn Fidough, much like all canine Pokémon, are blind and helpless for a few weeks before gaining sight and mobility. They should nurse until between five and eight weeks old if possible, though it may take longer if they are bottle fed. Once on solid food, canine derivitive Pokémon should have a very high protein diet, though the more domesticated lines such as this one can and should consume carbohydrates as well. A packaged fairy-type Pokéchow that is high in protien can be the bulk of their food with occasional treats.
League standard Fidough and Dachsbun are mostly hairless, with just a fine layer of peach fuzz over their elastic skin, while household and farming breeds can come in a variety of colors and fur lengths. They are sensitive to soap and chemicals, so should only be bathed with warm water when dirty. This line requires frequent check ups at your local Pokémon Center, as they are prone to cardiovascular issues, ear infections, and osteoporosis.
Fidough and Dachsbun were originally bred long ago to hunt burrowing pests on farms; their short legs and large paws make them powerful diggers. Because of this, even the smallest house breeds have high energy needs, which should be taken into consideration when thinking about adoption. These Pokémon should be allowed to exercise their instinctive need to dig, though training them not to dig in your flower beds or carpet can be challenging. They respond best to positive reinforcement, so all training should include a high value reward, such as their favorite treat or toy. An understimulated Fidough or Dachsbun is likely to tear up furniture, and a poorly socialized one will see strangers as a threat. This line can be one of the more agressive canine Pokémon, although bites are underreported due to their small stature.
If you are looking to add a Fidough to your team, you should first evaluate your living situation and experience level. They will do best in a home with a fenced in back yard, and a trainer who has a lot of time to spend with their Pokémon. I would not recommend this line to beginners, people with full time jobs who are unable to spend roughly eight hours a day with their Pokémon, or trainers who already care for several Pokémon with high attention needs. Once you have determined that you can meet the needs of a Fidough or Dachsbun, you should either speak with local authorities about adopting a wild one to help clean up a feral pack, or with several breeders to ensure you are receiving one that was bred ethically.
A well trained and socialized Fidough or Dachsbun can make an excellent addition to your team or household. They are incredibly intelligent as working dogs, with various breeds for different kinds of fermentation and the ability to track patterns which helps perfectly time the rise of a loaf of bread or the age of a bottle of wine. These partners are also loyal and protective to a fault when their trainer has raised them right, and are willing to stand up against foes regardless of size or type advantage.
There are restrictions on traveling and importing these Pokémon, as some varieties of yeast can be invasive to other areas, and foreign ones are generally forbidden around vinyards and bakerys to ensure flavor consistency. Always make sure to check the local laws and regulations before traveling with your partners.
9 notes
·
View notes
Last Seen Blogs


zjeffx
Criando uma AU de undertale

blackonyxblog
Black Onyx

kodrama
korean boys

arisabunny
Arisa bunny