#HIV positive woman marriage
Text
HIV Marriages for HIV Positive Brides and Grooms in India
In a society where traditions and societal norms often dictate the path of matrimony, the challenges faced by HIV-positive brides and grooms in India, especially in Hyderabad, are distinctive and demanding. This article delves into the complexities surrounding HIV-positive marriages, shedding light on the need for support, understanding, and the creation of a more inclusive environment.
Brief Overview of HIV-Positive Marriages
HIV-positive marriages involve couples where one or both partners are living with HIV. Despite medical advancements, societal stigmas continue to surround these unions.
Importance of Support for HIV-Positive Brides and Grooms
The emotional and psychological toll on couples navigating HIV-positive marriages emphasizes the crucial need for support networks and understanding within their communities.
Context of HIV-Positive Marriages in India, Specifically Hyderabad
India, with its rich cultural tapestry, faces unique challenges concerning HIV-positive marriages, and the city of Hyderabad is no exception.
Understanding the Challenges
Stigma Surrounding HIV-Positive Individuals
One of the primary obstacles faced by HIV-positive brides and grooms is the pervasive stigma attached to their condition. Addressing this stigma is vital for fostering acceptance.
Lack of Awareness and Education
A significant hurdle lies in the lack of awareness and education regarding HIV transmission, prevention, and the realities of living with the virus.
Emotional and Psychological Challenges
Coping with the emotional and psychological challenges is a journey often traveled in isolation. Counseling services play a pivotal role in supporting these couples.
Navigating the Wedding Preparations
Support Networks for Couples
Establishing robust support networks is essential for couples preparing for an HIV-positive marriage. Friends, family, and community organizations can offer invaluable assistance.
Counseling Services
Professional counseling services provide a safe space for couples to address their concerns, fears, and aspirations, ensuring they embark on their marital journey with resilience.
Positive Examples and Success Stories
Highlighting positive examples and success stories of HIV-positive marriages inspires hope and resilience within the community, dispelling myths and misconceptions.
Legal Aspects of HIV Marriages
Rights and Responsibilities
Understanding the legal rights and responsibilities of HIV-positive brides and grooms is crucial for navigating societal expectations and safeguarding their union.
Legal Safeguards for HIV-Positive Brides and Grooms
Legal frameworks exist to protect the rights of individuals with HIV. Awareness of these safeguards is vital for ensuring fair treatment.
Navigating Societal Norms and Expectations
Balancing traditional expectations with the realities of HIV-positive marriages requires open dialogue and education to foster acceptance within communities.
Wedding Rituals and Traditions
Adapting Traditions for HIV-Positive Couples
Customizing wedding rituals and traditions ensures that they align with the needs and comfort levels of HIV-positive couples.
Creating a Supportive Environment
Fostering a supportive environment during wedding ceremonies helps create a positive and inclusive atmosphere for the couple and their guests.
Inclusivity in Wedding Ceremonies
Promoting inclusivity in wedding ceremonies not only supports the couple but also contributes to changing societal perceptions surrounding HIV-positive marriages.
Community Involvement
Raising Awareness
Community involvement is crucial for raising awareness about HIV, dispelling myths, and fostering an environment of empathy and understanding.
Building a Network of Support
Communities can play a vital role in building a network of support, ensuring that HIV-positive couples have the backing they need to thrive in their marriages.
Encouraging Empathy and Understanding
Creating spaces that encourage empathy and understanding reduces stigma and helps the community embrace the diversity of love.
Healthcare Support
Access to Medical Facilities
Ensuring access to medical facilities and healthcare services is imperative for the well-being of HIV-positive brides and grooms.
Importance of Regular Check-Ups
Regular health check-ups are vital for managing HIV. Encouraging couples to prioritize their health is essential for a fulfilling marital journey.
Dispelling Myths About HIV Transmission
Education plays a crucial role in dispelling myths about HIV transmission, promoting a more informed and accepting society.
Financial Considerations
Challenges in Employment Opportunities
HIV-positive individuals may face challenges in employment opportunities. Addressing these challenges through advocacy and support is essential.
Financial Planning for HIV-Positive Couples
Financial planning becomes crucial for HIV-positive couples, considering potential challenges in the employment sector. Government and NGO support can play a vital role.
Government and NGO Support
Governments and non-governmental organizations can contribute significantly by providing financial support and creating initiatives to empower HIV-positive couples.
Social Media and Advocacy
Utilizing Social Platforms for Awareness
Leveraging social media platforms is a powerful way to raise awareness, educate the public, and advocate for the rights of HIV-positive couples.
Advocacy for HIV-Positive Marriages
Advocacy efforts aim to break down societal barriers, challenge stigmas, and create a more inclusive society for HIV-positive couples.
Empowering Couples Through Online Communities
Online communities provide a space for couples to share experiences.

#HIV Marriages#HIV Positive Marriages#HIV Partner#HIV Marriages near me#HIV Marriage Bureau Near me#HIV Marriage consultancy in Hyderabad#HIV Positive#HIV girl for marriage#HIV marriages in India#HIV positive matrimony#HIV Positive matrimonial#Hiv Positive life partner#HIV positive brides#Hiv positive Girls#HIV Positive Grooms#HIV positive marriage#matrimonial site for HIV positive#marriage bureau for HIV positive#HIV positive woman marriage#Hiv positive matchmaking#HIVpositivemarriage#HIV marriage bureau Bangalore#HIV marriage#HIV matrimony#Hiv positive Matrimonial India#HIV positive marriage bureau#Marriage of HIV Positive#HIV matrimonial#HIV positive marriage site#HIV Positive Datings
0 notes
Text
By: Jamie Reed
Published: Feb 9, 2023
I am a 42-year-old St. Louis native, a queer woman, and politically to the left of Bernie Sanders. My worldview has deeply shaped my career. I have spent my professional life providing counseling to vulnerable populations: children in foster care, sexual minorities, the poor.
For almost four years, I worked at The Washington University School of Medicine Division of Infectious Diseases with teens and young adults who were HIV positive. Many of them were trans or otherwise gender nonconforming, and I could relate: Through childhood and adolescence, I did a lot of gender questioning myself. I’m now married to a transman, and together we are raising my two biological children from a previous marriage and three foster children we hope to adopt.
All that led me to a job in 2018 as a case manager at The Washington University Transgender Center at St. Louis Children's Hospital, which had been established a year earlier.
The center’s working assumption was that the earlier you treat kids with gender dysphoria, the more anguish you can prevent later on. This premise was shared by the center’s doctors and therapists. Given their expertise, I assumed that abundant evidence backed this consensus.
During the four years I worked at the clinic as a case manager—I was responsible for patient intake and oversight—around a thousand distressed young people came through our doors. The majority of them received hormone prescriptions that can have life-altering consequences—including sterility.
I left the clinic in November of last year because I could no longer participate in what was happening there. By the time I departed, I was certain that the way the American medical system is treating these patients is the opposite of the promise we make to “do no harm.” Instead, we are permanently harming the vulnerable patients in our care.
Today I am speaking out. I am doing so knowing how toxic the public conversation is around this highly contentious issue—and the ways that my testimony might be misused. I am doing so knowing that I am putting myself at serious personal and professional risk.
Almost everyone in my life advised me to keep my head down. But I cannot in good conscience do so. Because what is happening to scores of children is far more important than my comfort. And what is happening to them is morally and medically appalling.

The Floodgates Open
Soon after my arrival at the Transgender Center, I was struck by the lack of formal protocols for treatment. The center’s physician co-directors were essentially the sole authority.
At first, the patient population was tipped toward what used to be the “traditional” instance of a child with gender dysphoria: a boy, often quite young, who wanted to present as—who wanted to be—a girl.
Until 2015 or so, a very small number of these boys comprised the population of pediatric gender dysphoria cases. Then, across the Western world, there began to be a dramatic increase in a new population: Teenage girls, many with no previous history of gender distress, suddenly declared they were transgender and demanded immediate treatment with testosterone.
I certainly saw this at the center. One of my jobs was to do intake for new patients and their families. When I started there were probably 10 such calls a month. When I left there were 50, and about 70 percent of the new patients were girls. Sometimes clusters of girls arrived from the same high school.
This concerned me, but didn’t feel I was in the position to sound some kind of alarm back then. There was a team of about eight of us, and only one other person brought up the kinds of questions I had. Anyone who raised doubts ran the risk of being called a transphobe.
The girls who came to us had many comorbidities: depression, anxiety, ADHD, eating disorders, obesity. Many were diagnosed with autism, or had autism-like symptoms. A report last year on a British pediatric transgender center found that about one-third of the patients referred there were on the autism spectrum.
Frequently, our patients declared they had disorders that no one believed they had. We had patients who said they had Tourette syndrome (but they didn’t); that they had tic disorders (but they didn’t); that they had multiple personalities (but they didn’t).
The doctors privately recognized these false self-diagnoses as a manifestation of social contagion. They even acknowledged that suicide has an element of social contagion. But when I said the clusters of girls streaming into our service looked as if their gender issues might be a manifestation of social contagion, the doctors said gender identity reflected something innate.
To begin transitioning, the girls needed a letter of support from a therapist—usually one we recommended—who they had to see only once or twice for the green light. To make it more efficient for the therapists, we offered them a template for how to write a letter in support of transition. The next stop was a single visit to the endocrinologist for a testosterone prescription.
That’s all it took.
When a female takes testosterone, the profound and permanent effects of the hormone can be seen in a matter of months. Voices drop, beards sprout, body fat is redistributed. Sexual interest explodes, aggression increases, and mood can be unpredictable. Our patients were told about some side effects, including sterility. But after working at the center, I came to believe that teenagers are simply not capable of fully grasping what it means to make the decision to become infertile while still a minor.
Side Effects
Many encounters with patients emphasized to me how little these young people understood the profound impacts changing gender would have on their bodies and minds. But the center downplayed the negative consequences, and emphasized the need for transition. As the center’s website said, “Left untreated, gender dysphoria has any number of consequences, from self-harm to suicide. But when you take away the gender dysphoria by allowing a child to be who he or she is, we’re noticing that goes away. The studies we have show these kids often wind up functioning psychosocially as well as or better than their peers.”
There are no reliable studies showing this. Indeed, the experiences of many of the center’s patients prove how false these assertions are.
Here’s an example. On Friday, May 1, 2020, a colleague emailed me about a 15-year-old male patient: “Oh dear. I am concerned that [the patient] does not understand what Bicalutamide does.” I responded: “I don’t think that we start anything honestly right now.”
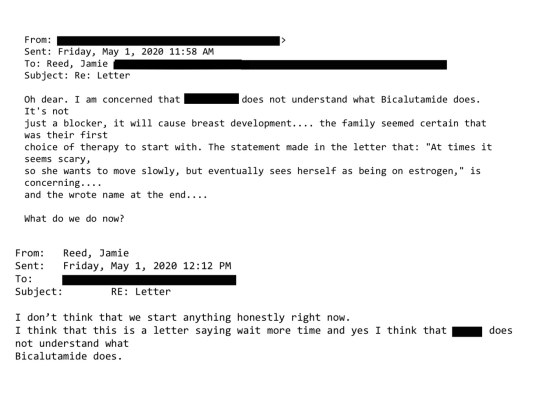
Bicalutamide is a medication used to treat metastatic prostate cancer, and one of its side effects is that it feminizes the bodies of men who take it, including the appearance of breasts. The center prescribed this cancer drug as a puberty blocker and feminizing agent for boys. As with most cancer drugs, bicalutamide has a long list of side effects, and this patient experienced one of them: liver toxicity. He was sent to another unit of the hospital for evaluation and immediately taken off the drug. Afterward, his mother sent an electronic message to the Transgender Center saying that we were lucky her family was not the type to sue.
How little patients understood what they were getting into was illustrated by a call we received at the center in 2020 from a 17-year-old biological female patient who was on testosterone. She said she was bleeding from the vagina. In less than an hour she had soaked through an extra heavy pad, her jeans, and a towel she had wrapped around her waist. The nurse at the center told her to go to the emergency room right away.
We found out later this girl had had intercourse, and because testosterone thins the vaginal tissues, her vaginal canal had ripped open. She had to be sedated and given surgery to repair the damage. She wasn’t the only vaginal laceration case we heard about.
Other girls were disturbed by the effects of testosterone on their clitoris, which enlarges and grows into what looks like a microphallus, or a tiny penis. I counseled one patient whose enlarged clitoris now extended below her vulva, and it chafed and rubbed painfully in her jeans. I advised her to get the kind of compression undergarments worn by biological men who dress to pass as female. At the end of the call I thought to myself, “Wow, we hurt this kid.”
There are rare conditions in which babies are born with atypical genitalia—cases that call for sophisticated care and compassion. But clinics like the one where I worked are creating a whole cohort of kids with atypical genitals—and most of these teens haven’t even had sex yet. They had no idea who they were going to be as adults. Yet all it took for them to permanently transform themselves was one or two short conversations with a therapist.
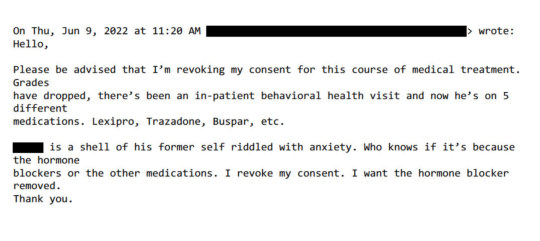
Being put on powerful doses of testosterone or estrogen—enough to try to trick your body into mimicking the opposite sex—-affects the rest of the body. I doubt that any parent who's ever consented to give their kid testosterone (a lifelong treatment) knows that they’re also possibly signing their kid up for blood pressure medication, cholesterol medication, and perhaps sleep apnea and diabetes.
But sometimes the parents’ understanding of what they had agreed to do to their children came forcefully:
Neglected and Mentally Ill Patients
Besides teenage girls, another new group was referred to us: young people from the inpatient psychiatric unit, or the emergency department, of St. Louis Children’s Hospital. The mental health of these kids was deeply concerning—there were diagnoses like schizophrenia, PTSD, bipolar disorder, and more. Often they were already on a fistful of pharmaceuticals.
This was tragic, but unsurprising given the profound trauma some had been through. Yet no matter how much suffering or pain a child had endured, or how little treatment and love they had received, our doctors viewed gender transition—even with all the expense and hardship it entailed—as the solution.
Some weeks it felt as though almost our entire caseload was nothing but disturbed young people.
For example, one teenager came to us in the summer of 2022 when he was 17 years old and living in a lockdown facility because he had been sexually abusing dogs. He’d had an awful childhood: His mother was a drug addict, his father was imprisoned, and he grew up in foster care. Whatever treatment he may have been getting, it wasn’t working.
During our intake I learned from another caseworker that when he got out, he planned to reoffend because he believed the dogs had willingly submitted.
Somewhere along the way, he expressed a desire to become female, so he ended up being seen at our center. From there, he went to a psychologist at the hospital who was known to approve virtually everyone seeking transition. Then our doctor recommended feminizing hormones. At the time, I wondered if this was being done as a form of chemical castration.
That same thought came up again with another case. This one was in spring of 2022 and concerned a young man who had intense obsessive-compulsive disorder that manifested as a desire to cut off his penis after he masturbated. This patient expressed no gender dysphoria, but he got hormones, too. I asked the doctor what protocol he was following, but I never got a straight answer.
In Loco Parentis
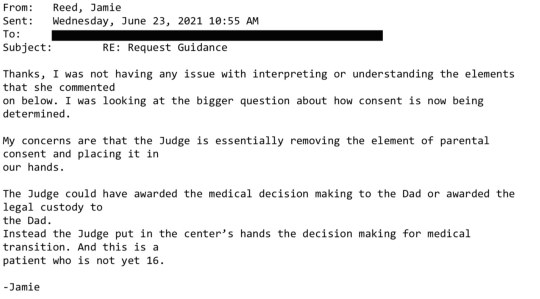
Another disturbing aspect of the center was its lack of regard for the rights of parents—and the extent to which doctors saw themselves as more informed decision-makers over the fate of these children.
In Missouri, only one parent’s consent is required for treatment of their child. But when there was a dispute between the parents, it seemed the center always took the side of the affirming parent.
My concerns about this approach to dissenting parents grew in 2019 when one of our doctors actually testified in a custody hearing against a father who opposed a mother’s wish to start their 11-year-old daughter on puberty blockers.
I had done the original intake call, and I found the mother quite disturbing. She and the father were getting divorced, and the mother described the daughter as “kind of a tomboy.” So now the mother was convinced her child was trans. But when I asked if her daughter had adopted a boy’s name, if she was distressed about her body, if she was saying she felt like a boy, the mother said no. I explained the girl just didn’t meet the criteria for an evaluation.
Then a month later, the mother called back and said her daughter now used a boy’s name, was in distress over her body, and wanted to transition. This time the mom and daughter were given an appointment. Our providers decided the girl was trans and prescribed a puberty blocker to prevent her normal development.
The father adamantly disagreed, said this was all coming from the mother, and a custody battle ensued. After the hearing where our doctor testified in favor of transition, the judge sided with the mother.
‘I Want My Breasts Back’
Because I was the main intake person, I had the broadest perspective on our existing and prospective patients. In 2019, a new group of people appeared on my radar: desisters and detransitioners. Desisters choose not to go through with a transition. Detransitioners are transgender people who decide to return to their birth gender.
The one colleague with whom I was able to share my concerns agreed with me that we should be tracking desistance and detransition. We thought the doctors would want to collect and understand this data in order to figure out what they had missed.
We were wrong. One doctor wondered aloud why he would spend time on someone who was no longer his patient.
But we created a document anyway and called it the Red Flag list. It was an Excel spreadsheet that tracked the kind of patients that kept my colleague and me up at night.
One of the saddest cases of detransition I witnessed was a teenage girl, who, like so many of our patients, came from an unstable family, was in an uncertain living situation, and had a history of drug use. The overwhelming majority of our patients are white, but this girl was black. She was put on hormones at the center when she was around 16. When she was 18, she went in for a double mastectomy, what’s known as “top surgery.”
Three months later she called the surgeon’s office to say she was going back to her birth name and that her pronouns were “she” and “her.” Heartbreakingly, she told the nurse, “I want my breasts back.” The surgeon’s office contacted our office because they didn’t know what to say to this girl.
My colleague and I said that we would reach out. It took a while to track her down, and when we did we made sure that she was in decent mental health, that she was not actively suicidal, that she was not using substances. The last I heard, she was pregnant. Of course, she’ll never be able to breastfeed her child.
‘Get On Board, Or Get Out’
My concerns about what was going on at the center started to overtake my life. By spring 2020, I felt a medical and moral obligation to do something. So I spoke up in the office, and sent plenty of emails.
Here’s just one example: On January 6, 2022, I received an email from a staff therapist asking me for help with a case of a 16-year-old transgender male living in another state. “Parents are open to having patient see a therapist but are not supportive of gender and patient does not want parents to be aware of gender identity. I am having a challenging time finding a gender affirming therapist.”
I replied:
“I do not ethically agree with linking a minor patient to a therapist who would be gender affirming with gender as a focus of their work without that being discussed with the parents and the parent agreeing to that kind of care.”

In all my years at the Washington University School of Medicine, I had received solidly positive performance reviews. But in 2021, that changed. I got a below-average mark for my “Judgment” and “Working Relationships/Cooperative Spirit.” Although I was described as “responsible, conscientious, hard-working and productive” the evaluation also noted: “At times Jamie responds poorly to direction from management with defensiveness and hostility.”
Things came to a head at a half-day retreat in summer of 2022. In front of the team, the doctors said that my colleague and I had to stop questioning the “medicine and the science” as well as their authority. Then an administrator told us we had to “Get on board, or get out.” It became clear that the purpose of the retreat was to deliver these messages to us.
The Washington University system provides a generous college tuition payment program for long-standing employees. I live by my paycheck and have no money to put aside for five college tuitions for my kids. I had to keep my job. I also feel a lot of loyalty to Washington University.
But I decided then and there that I had to get out of the Transgender Center, and to do so, I had to keep my head down and improve my next performance review.
I managed to get a decent evaluation, and I landed a job conducting research in another part of The Washington University School of Medicine. I gave my notice and left the Transgender Center in November of 2022.

What I Want to See Happen
For a couple of weeks, I tried to put everything behind me and settled into my new job as a clinical research coordinator, managing studies regarding children undergoing bone marrow transplants.
Then I came across comments from Dr. Rachel Levine, a transgender woman who is a high official at the federal Department of Health and Human Services. The article read: “Levine, the U.S. assistant secretary for health, said that clinics are proceeding carefully and that no American children are receiving drugs or hormones for gender dysphoria who shouldn’t.”
I felt stunned and sickened. It wasn’t true. And I know that from deep first-hand experience.
So I started writing down everything I could about my experience at the Transgender Center. Two weeks ago, I brought my concerns and documents to the attention of Missouri’s attorney general. He is a Republican. I am a progressive. But the safety of children should not be a matter for our culture wars.
Given the secrecy and lack of rigorous standards that characterize youth gender transition across the country, I believe that to ensure the safety of American children, we need a moratorium on the hormonal and surgical treatment of young people with gender dysphoria.
In the past 15 years, according to Reuters, the U.S. has gone from having no pediatric gender clinics to more than 100. A thorough analysis should be undertaken to find out what has been done to their patients and why—and what the long-term consequences are.
There is a clear path for us to follow. Just last year England announced that it would close the Tavistock’s youth gender clinic, then the NHS’s only such clinic in the country, after an investigation revealed shoddy practices and poor patient treatment. Sweden and Finland, too, have investigated pediatric transition and greatly curbed the practice, finding there is insufficient evidence of help, and danger of great harm.
Some critics describe the kind of treatment offered at places like the Transgender Center where I worked as a kind of national experiment. But that’s wrong.
Experiments are supposed to be carefully designed. Hypotheses are supposed to be tested ethically. The doctors I worked alongside at the Transgender Center said frequently about the treatment of our patients: “We are building the plane while we are flying it.” No one should be a passenger on that kind of aircraft.
==
The U.S. gets its Tavistock. It will not be the last.
Fathers may well be some of the unsung heroes at the end of this mess. Whenever one parent is pushing for life-long medicalization of a child, it is invariably a Munchausen-by-Trans (Transhausen) possessed mother, with a father fighting against all odds and the system that favors her.
#Jamie Reed#gender ideology#queer theory#medical transition#medical corruption#medical malpractice#whistleblower#medical scandal#St. Louis Children's Hospital#ideological capture#transhausen by proxy#transhausen syndrome#medical experimentation#experimental treatment#hormone blockers#puberty blockers#wrong sex hormones#pediatric transition#woke activism#woke#wokeness as religion#cult of woke#wokeism#religion is a mental illness
41 notes
·
View notes
Text
Just on the topic of lesbians (and “lesbians”) affected by HIV/AIDS:
“ Here are some case examples of lesbians who are HIV-infected or are living with AIDS:
Marta is a single, Latina lifelong so-called gold star lesbian. The term “gold star” refers to a woman who is lesbian-identified who has never had sexual contact with a male. Her HIV infection risk was linked to chronic, intermittent IV drug use, primarily heroin, but she also used crack cocaine periodically. In exchange for drugs, she has often engaged in unsafe sex. She often fears that she might die of “the madness.”
Beverly is an African-American mother of three. She was in a commonlaw marriage with someone on the “DL,” or down-low, a man who was secretly also having sexual relationships with other men. She did not find out that he was HIV positive until he was terminally ill with AIDS. He died of severe pneumonia related to HIV. After her husband’s death, Beverly pursued relationships exclusively with women. She discovered she was HIV positive when she went to donate blood.
Kim is a Caucasian transgender, male-to-female sex worker who practices safer sex with her clients. However, she has unprotected sex with her longtime female partner, since both considered themselves “monogamous” despite Kim being a sex worker. She tested positive after HIV antibody testing which she routinely obtained every three months.
So, who is the lesbian? The common definition of a lesbian is a woman who is romantically, sexually, and erotically attracted exclusively to other women. In psychiatry, when we describe lesbians, it is important to distinguish operational versus descriptive terms. In research we find that the term “women who have sex with women” is commonly used. However, this does not describe many lesbians’ experience, particularly if we are talking about lifelong experience. The literature shows that a majority of self-defined lesbians, 70% or more have had sexual contact with a male partner during their lifetime (Diamond, 2008). It is important to note that when someone identifies herself as a lesbian, this may not correspond with her behavior. Also, the reverse is true—a woman may be having sexual relationships with women yet not identify as a lesbian. If you are describing a lesbian from a non-Western culture, including some ethnic minority cultures in the United States, they may have different terms or concepts of women who would be considered by many as lesbians. Therefore, in sexual history taking, it is important to distinguish identity/orientation versus behavior and to ask explicitly about each.”
Khakasa Wapenyi MD (2010) Do Lesbians Get AIDS? Women Who Have Sex with Women, HIV/AIDS, and Its Mental Health Impact, Journal of Gay & Lesbian Mental Health, 14:1, 52-55, DOI: 10.1080/19359700903422683
Lesbian with a drug addiction, bisexual woman calling herself a lesbian who was in a relationship with a bisexual man, and a TiM.
If you’re going to talk about lesbians living with HIV or dying from AIDS-related complications, make sure you know what is being included in that data.
7 notes
·
View notes
Text
I am a 42-year-old St. Louis native, a queer woman, and politically to the left of Bernie Sanders. My worldview has deeply shaped my career. I have spent my professional life providing counseling to vulnerable populations: children in foster care, sexual minorities, the poor.
For almost four years, I worked at The Washington University School of Medicine Division of Infectious Diseases with teens and young adults who were HIV positive. Many of them were trans or otherwise gender nonconforming, and I could relate: Through childhood and adolescence, I did a lot of gender questioning myself. I’m now married to a transman, and together we are raising my two biological children from a previous marriage and three foster children we hope to adopt.
All that led me to a job in 2018 as a case manager at The Washington University Transgender Center at St. Louis Children’s Hospital, which had been established a year earlier.
The center’s working assumption was that the earlier you treat kids with gender dysphoria, the more anguish you can prevent later on. This premise was shared by the center’s doctors and therapists. Given their expertise, I assumed that abundant evidence backed this consensus.
During the four years I worked at the clinic as a case manager—I was responsible for patient intake and oversight—around a thousand distressed young people came through our doors. The majority of them received hormone prescriptions that can have life-altering consequences—including sterility.
I left the clinic in November of last year because I could no longer participate in what was happening there. By the time I departed, I was certain that the way the American medical system is treating these patients is the opposite of the promise we make to “do no harm.” Instead, we are permanently harming the vulnerable patients in our care.
Today I am speaking out. I am doing so knowing how toxic the public conversation is around this highly contentious issue—and the ways that my testimony might be misused. I am doing so knowing that I am putting myself at serious personal and professional risk.
Almost everyone in my life advised me to keep my head down. But I cannot in good conscience do so. Because what is happening to scores of children is far more important than my comfort. And what is happening to them is morally and medically appalling.

The Floodgates Open
Soon after my arrival at the Transgender Center, I was struck by the lack of formal protocols for treatment. The center’s physician co-directors were essentially the sole authority.
At first, the patient population was tipped toward what used to be the “traditional” instance of a child with gender dysphoria: a boy, often quite young, who wanted to present as—who wanted to be—a girl.
Until 2015 or so, a very small number of these boys comprised the population of pediatric gender dysphoria cases. Then, across the Western world, there began to be a dramatic increase in a new population: Teenage girls, many with no previous history of gender distress, suddenly declared they were transgender and demanded immediate treatment with testosterone.
I certainly saw this at the center. One of my jobs was to do intake for new patients and their families. When I started there were probably 10 such calls a month. When I left there were 50, and about 70 percent of the new patients were girls. Sometimes clusters of girls arrived from the same high school.
This concerned me, but didn’t feel I was in the position to sound some kind of alarm back then. There was a team of about eight of us, and only one other person brought up the kinds of questions I had. Anyone who raised doubts ran the risk of being called a transphobe.
The girls who came to us had many comorbidities: depression, anxiety, ADHD, eating disorders, obesity. Many were diagnosed with autism, or had autism-like symptoms. A report last year on a British pediatric transgender center found that about one-third of the patients referred there were on the autism spectrum.
Frequently, our patients declared they had disorders that no one believed they had. We had patients who said they had Tourette syndrome (but they didn’t); that they had tic disorders (but they didn’t); that they had multiple personalities (but they didn’t).
The doctors privately recognized these false self-diagnoses as a manifestation of social contagion. They even acknowledged that suicide has an element of social contagion. But when I said the clusters of girls streaming into our service looked as if their gender issues might be a manifestation of social contagion, the doctors said gender identity reflected something innate.
To begin transitioning, the girls needed a letter of support from a therapist—usually one we recommended—who they had to see only once or twice for the green light. To make it more efficient for the therapists, we offered them a template for how to write a letter in support of transition. The next stop was a single visit to the endocrinologist for a testosterone prescription.
That’s all it took.
When a female takes testosterone, the profound and permanent effects of the hormone can be seen in a matter of months. Voices drop, beards sprout, body fat is redistributed. Sexual interest explodes, aggression increases, and mood can be unpredictable. Our patients were told about some side effects, including sterility. But after working at the center, I came to believe that teenagers are simply not capable of fully grasping what it means to make the decision to become infertile while still a minor.
Side Effects
Many encounters with patients emphasized to me how little these young people understood the profound impacts changing gender would have on their bodies and minds. But the center downplayed the negative consequences, and emphasized the need for transition. As the center’s website said, “Left untreated, gender dysphoria has any number of consequences, from self-harm to suicide. But when you take away the gender dysphoria by allowing a child to be who he or she is, we’re noticing that goes away. The studies we have show these kids often wind up functioning psychosocially as well as or better than their peers.”
There are no reliable studies showing this. Indeed, the experiences of many of the center’s patients prove how false these assertions are.
Here’s an example. On Friday, May 1, 2020, a colleague emailed me about a 15-year-old male patient: “Oh dear. I am concerned that [the patient] does not understand what Bicalutamide does.” I responded: “I don’t think that we start anything honestly right now.”

Bicalutamide is a medication used to treat metastatic prostate cancer, and one of its side effects is that it feminizes the bodies of men who take it, including the appearance of breasts. The center prescribed this cancer drug as a puberty blocker and feminizing agent for boys. As with most cancer drugs, bicalutamide has a long list of side effects, and this patient experienced one of them: liver toxicity. He was sent to another unit of the hospital for evaluation and immediately taken off the drug. Afterward, his mother sent an electronic message to the Transgender Center saying that we were lucky her family was not the type to sue.
How little patients understood what they were getting into was illustrated by a call we received at the center in 2020 from a 17-year-old biological female patient who was on testosterone. She said she was bleeding from the vagina. In less than an hour she had soaked through an extra heavy pad, her jeans, and a towel she had wrapped around her waist. The nurse at the center told her to go to the emergency room right away.
We found out later this girl had had intercourse, and because testosterone thins the vaginal tissues, her vaginal canal had ripped open. She had to be sedated and given surgery to repair the damage. She wasn’t the only vaginal laceration case we heard about.
Other girls were disturbed by the effects of testosterone on their clitoris, which enlarges and grows into what looks like a microphallus, or a tiny penis. I counseled one patient whose enlarged clitoris now extended below her vulva, and it chafed and rubbed painfully in her jeans. I advised her to get the kind of compression undergarments worn by biological men who dress to pass as female. At the end of the call I thought to myself, “Wow, we hurt this kid.”
There are rare conditions in which babies are born with atypical genitalia—cases that call for sophisticated care and compassion. But clinics like the one where I worked are creating a whole cohort of kids with atypical genitals—and most of these teens haven’t even had sex yet. They had no idea who they were going to be as adults. Yet all it took for them to permanently transform themselves was one or two short conversations with a therapist.
Being put on powerful doses of testosterone or estrogen—enough to try to trick your body into mimicking the opposite sex—affects the rest of the body. I doubt that any parent who's ever consented to give their kid testosterone (a lifelong treatment) knows that they’re also possibly signing their kid up for blood pressure medication, cholesterol medication, and perhaps sleep apnea and diabetes.
But sometimes the parents’ understanding of what they had agreed to do to their children came forcefully:

Neglected and Mentally Ill Patients
Besides teenage girls, another new group was referred to us: young people from the inpatient psychiatric unit, or the emergency department, of St. Louis Children’s Hospital. The mental health of these kids was deeply concerning—there were diagnoses like schizophrenia, PTSD, bipolar disorder, and more. Often they were already on a fistful of pharmaceuticals.
This was tragic, but unsurprising given the profound trauma some had been through. Yet no matter how much suffering or pain a child had endured, or how little treatment and love they had received, our doctors viewed gender transition—even with all the expense and hardship it entailed—as the solution.
Some weeks it felt as though almost our entire caseload was nothing but disturbed young people.
For example, one teenager came to us in the summer of 2022 when he was 17 years old and living in a lockdown facility because he had been sexually abusing dogs. He’d had an awful childhood: His mother was a drug addict, his father was imprisoned, and he grew up in foster care. Whatever treatment he may have been getting, it wasn’t working.
During our intake I learned from another caseworker that when he got out, he planned to reoffend because he believed the dogs had willingly submitted.
Somewhere along the way, he expressed a desire to become female, so he ended up being seen at our center. From there, he went to a psychologist at the hospital who was known to approve virtually everyone seeking transition. Then our doctor recommended feminizing hormones. At the time, I wondered if this was being done as a form of chemical castration.
That same thought came up again with another case. This one was in spring of 2022 and concerned a young man who had intense obsessive-compulsive disorder that manifested as a desire to cut off his penis after he masturbated. This patient expressed no gender dysphoria, but he got hormones, too. I asked the doctor what protocol he was following, but I never got a straight answer.
In Loco Parentis
Another disturbing aspect of the center was its lack of regard for the rights of parents—and the extent to which doctors saw themselves as more informed decision-makers over the fate of these children.
In Missouri, only one parent’s consent is required for treatment of their child. But when there was a dispute between the parents, it seemed the center always took the side of the affirming parent.
My concerns about this approach to dissenting parents grew in 2019 when one of our doctors actually testified in a custody hearing against a father who opposed a mother’s wish to start their 11-year-old daughter on puberty blockers.
I had done the original intake call, and I found the mother quite disturbing. She and the father were getting divorced, and the mother described the daughter as “kind of a tomboy.” So now the mother was convinced her child was trans. But when I asked if her daughter had adopted a boy’s name, if she was distressed about her body, if she was saying she felt like a boy, the mother said no. I explained the girl just didn’t meet the criteria for an evaluation.
Then a month later, the mother called back and said her daughter now used a boy’s name, was in distress over her body, and wanted to transition. This time the mom and daughter were given an appointment. Our providers decided the girl was trans and prescribed a puberty blocker to prevent her normal development.
The father adamantly disagreed, said this was all coming from the mother, and a custody battle ensued. After the hearing where our doctor testified in favor of transition, the judge sided with the mother.

‘I Want My Breasts Back’
Because I was the main intake person, I had the broadest perspective on our existing and prospective patients. In 2019, a new group of people appeared on my radar: desisters and detransitioners. Desisters choose not to go through with a transition. Detransitioners are transgender people who decide to return to their birth gender.
The one colleague with whom I was able to share my concerns agreed with me that we should be tracking desistance and detransition. We thought the doctors would want to collect and understand this data in order to figure out what they had missed.
We were wrong. One doctor wondered aloud why he would spend time on someone who was no longer his patient.
But we created a document anyway and called it the Red Flag list. It was an Excel spreadsheet that tracked the kind of patients that kept my colleague and me up at night.
One of the saddest cases of detransition I witnessed was a teenage girl, who, like so many of our patients, came from an unstable family, was in an uncertain living situation, and had a history of drug use. The overwhelming majority of our patients are white, but this girl was black. She was put on hormones at the center when she was around 16. When she was 18, she went in for a double mastectomy, what’s known as “top surgery.”
Three months later she called the surgeon’s office to say she was going back to her birth name and that her pronouns were “she” and “her.” Heartbreakingly, she told the nurse, “I want my breasts back.” The surgeon’s office contacted our office because they didn’t know what to say to this girl.
My colleague and I said that we would reach out. It took a while to track her down, and when we did we made sure that she was in decent mental health, that she was not actively suicidal, that she was not using substances. The last I heard, she was pregnant. Of course, she’ll never be able to breastfeed her child.
‘Get On Board, Or Get Out’
My concerns about what was going on at the center started to overtake my life. By spring 2020, I felt a medical and moral obligation to do something. So I spoke up in the office, and sent plenty of emails.
Here’s just one example: On January 6, 2022, I received an email from a staff therapist asking me for help with a case of a 16-year-old transgender male living in another state. “Parents are open to having patient see a therapist but are not supportive of gender and patient does not want parents to be aware of gender identity. I am having a challenging time finding a gender affirming therapist.”
I replied:
“I do not ethically agree with linking a minor patient to a therapist who would be gender affirming with gender as a focus of their work without that being discussed with the parents and the parent agreeing to that kind of care.”

In all my years at the Washington University School of Medicine, I had received solidly positive performance reviews. But in 2021, that changed. I got a below-average mark for my “Judgment” and “Working Relationships/Cooperative Spirit.” Although I was described as “responsible, conscientious, hard-working and productive” the evaluation also noted: “At times Jamie responds poorly to direction from management with defensiveness and hostility.”
Things came to a head at a half-day retreat in summer of 2022. In front of the team, the doctors said that my colleague and I had to stop questioning the “medicine and the science” as well as their authority. Then an administrator told us we had to “Get on board, or get out.” It became clear that the purpose of the retreat was to deliver these messages to us.
The Washington University system provides a generous college tuition payment program for long-standing employees. I live by my paycheck and have no money to put aside for five college tuitions for my kids. I had to keep my job. I also feel a lot of loyalty to Washington University.
But I decided then and there that I had to get out of the Transgender Center, and to do so, I had to keep my head down and improve my next performance review.
I managed to get a decent evaluation, and I landed a job conducting research in another part of The Washington University School of Medicine. I gave my notice and left the Transgender Center in November of 2022.

What I Want to See Happen
For a couple of weeks, I tried to put everything behind me and settled into my new job as a clinical research coordinator, managing studies regarding children undergoing bone marrow transplants.
Then I came across comments from Dr. Rachel Levine, a transgender woman who is a high official at the federal Department of Health and Human Services. The article read: “Levine, the U.S. assistant secretary for health, said that clinics are proceeding carefully and that no American children are receiving drugs or hormones for gender dysphoria who shouldn’t.”
I felt stunned and sickened. It wasn’t true. And I know that from deep first-hand experience.
So I started writing down everything I could about my experience at the Transgender Center. Two weeks ago, I brought my concerns and documents to the attention of Missouri’s attorney general. He is a Republican. I am a progressive. But the safety of children should not be a matter for our culture wars.
Click here to read Jamie Reed’s letter to the Missouri AG.
Given the secrecy and lack of rigorous standards that characterize youth gender transition across the country, I believe that to ensure the safety of American children, we need a moratorium on the hormonal and surgical treatment of young people with gender dysphoria.
In the past 15 years, according to Reuters, the U.S. has gone from having no pediatric gender clinics to more than 100. A thorough analysis should be undertaken to find out what has been done to their patients and why—and what the long-term consequences are.
There is a clear path for us to follow. Just last year England announced that it would close the Tavistock’s youth gender clinic, then the NHS’s only such clinic in the country, after an investigation revealed shoddy practices and poor patient treatment. Sweden and Finland, too, have investigated pediatric transition and greatly curbed the practice, finding there is insufficient evidence of help, and danger of great harm.
Some critics describe the kind of treatment offered at places like the Transgender Center where I worked as a kind of national experiment. But that’s wrong.
Experiments are supposed to be carefully designed. Hypotheses are supposed to be tested ethically. The doctors I worked alongside at the Transgender Center said frequently about the treatment of our patients: “We are building the plane while we are flying it.” No one should be a passenger on that kind of aircraft.
0 notes
Text
"Living in Utawala and in Need of a Sugar Mummy?" Connect with Hadassah
Hi, Admin, I am Hadassah, a single woman based in Utawala who requests a long-term relationship that can result in marriage.
HIV-positive and Christian, a working-class woman, and would like to connect with someone preferably tall and over 30 years old.
If you are single and would like to start something serious with me, get in touch.
Are you interested in Hadassah? Text or Call Admin Esther…

View On WordPress
0 notes
Text
Cardinal claims Jesus would be thrown in jail today for opposing LGBTQ+ rights
The Pope has taken some tepid steps towards including LGBTQ+ people in the Catholic Church recently, and some members of the church’s leadership are pushing back. One cardinal went so far as to say that Jesus would be thrown in jail today for opposing LGBTQ+ equality.
Cardinal Gerhard Ludwig Müller appeared on the British rightwing network GB News when the host asked Müller about the Pope’s recent measures towards reform, including his dismissal of far-right MAGA Bishop Joseph Strickland in Texas. Strickland constantly criticized the Pope for being too liberal on LGBTQ+ rights, divorce, and the role of women in the church. He even called the Pope a “usurper” who has “endangered souls by proclaiming that they are justified before God as they are, with no need of repentance.”
Related:
Pope invited trans women over for a pasta & meatballs dinner
A former sex worker sat next to the Pontiff making small talk as they had tiramisu for dessert.
“Jesus also contradicts ideologically [unintelligible] who want to relativize or even destroy marriage of man and woman and the family of the parents with their own children,” Müller claimed, even though there is no movement in any country to end heterosexual marriage or parenthood.
Never Miss a Beat
Subscribe to our daily newsletter to stay ahead of the latest LGBTQ+ political news and insights.
Promotions (occasional)
*
Week in Good News (one on the Weekend)
*
Week in Review (one on the Weekend)
*
Daily Brief (one each weekday)
*
Sign Up
“He said to the Pharisees who wanted to trap him, ‘Have you not read that God created man in the beginning, male and female?” Müller continued, citing Matthew 19:4, a passage about Jesus’s disapproval of heterosexual divorce.
“I believe that today Jesus would not be condemned only because he’s a messiah, but he would, in Canada, the United States, and European countries, go to prison because he spoke out the truth about marriage between a man and a woman,” Müller declared.
Like many conservative Christians, Müller apparently wants to believe that Christianity is an oppressed minority religion even though it is the dominant religion in the West and holds so much power that there has never been a U.S. president who didn’t at least claim to be Christian. No one is going to jail in the U.S. for merely holding the belief that same-sex marriage is wrong.
Müller also cited Cardinal Raymond Burke in the interview, who was evicted from his Vatican apartment last month.
Burke complained that the church has strayed from “absolute moral law” by not condemning “the plague of the homosexual agenda” forcefully enough. Burke was a leading proponent of bans on same-sex marriage nationwide. He has also been a leader in decrying the use of condoms to prevent HIV. His opposition to condoms led to his exile from the Vatican by the current pope.
Burke had intervened to have the head of a church organization fired for approving the distribution of condoms to prostitutes in Myanmar. Francis used the episode to remove Burke from his powerful post and send him to Guam as punishment.
Burke also accused Pope Francis of trying to destroy the Church from within.
Even though Burke and Strickland were the only two examples Müller brought up, neither was put in prison for their positions on LGBTQ+ rights. In fact, it’s unclear if it was even their positions on those issues — and not their constant criticism of Pope Francis — that got them kicked out of their positions in the church. http://dlvr.it/T0cL4D
0 notes
Photo
"When I was a fire, I turned into ice, melting off my last feverish highs, and I leapt through the sunshine and into the night, singing songs of my healthiest fears."
JOHN ‘JACK’ BROOKS
Age: 43
Gender and pronouns: Male, He/Him
Occupation: OB/GYN, Neonatal Surgeon at UPenn Hospital
Neighborhood: Chestnut Hill
BIOGRAPHY
tw: parental death
When Dr. Lachlan Brooks married his surgical nurse, polite society had been abuzz. He was a man in his sixties, having already been married for decades and with two grown sons. Those that ran in the same circles as the Brooks' could not help but be consumed by the salacious gossip that Lachlan had negotiated a divorce in order to marry a woman decades his junior. Gossips were event more alight once it became clear that this woman was pregnant.
All of this outrage was lost upon the golden tresses of baby Jack, the product of this love affair. He was raised in a home that teemed with love, roughhoused with the children of his older half brothers, and was a general rebel rouser. And while society would not adapt enough to welcome his mother into their fold, Jack was a handsome and charming young man, and so seemingly he could do no wrong. He attended the University of Pennsylvania for undergrad like his father and brothers had, not quite taking his studies seriously as he should of. Perhaps due to his father's advanced age, no one had ever suggested or demanded that Jack grow serious about life. Instead, upon graduating (without honors or accolades), Jack chose to travel. With a limitless pool of financial resources, Jack became a globetrotter of epic proportions, finding friends in every country and on every continent, and a few romances as well.
His years abroad were not completely laissez-faire, as Jack spent plenty of time volunteering where he could. It was then that his mind began to change, a more serious intellectual curiosity was born. He became interested, more keenly, in the plight of neonatal HIV in sub-Saharan Africa. This charity work sparked many conversations with his father, particularly about what he could do if he had more formal training, instead of as a simple layman. Jack was reluctant to take up the mantle that his father and brothers had, and certainly other Brooks men before them. And it was on that last phone call to his father that Lachlan Brooks suggested his youngest son finally get serious with his life, instead of wasting his potential. It was a tough love chat, but certainly one that he needed.
He only wished his father had lived long enough to see him be accepted into medical school.
Jack arrived back in Philadelphia a very different person, shaped by his experiences and prepared to lead a more 'conventional' life, like his father might have wanted. He was older than his classmates at the Perelman School of Medicine, but he didn't pay much mind to the gap. Jack's nose was to his books, and constantly bouncing questions off of his siblings. At least, he was studious until he met Haley Norris.
They dated throughout medical school, and even some time after. He was mad about her, even if he needed the direction of her parents to consider the prospect of marriage. It wasn't that the idea didn't sound grand, in theory, but Jack had always flown by the seat of his pants, until med school, and subsequently, Haley. In trying to be careful and deliberate about their life together, he'd forgotten the next logical step. And perhaps, somewhere in those years he'd lost her confidence, as initial conversations about tying the knot hadn't gone over well.
In the end, the pair went their separate ways, Jack's pride wounded, and almost fatally once he heard that Haley had eloped with a man she hardly knew. He then concluded that if marriage wasn't the next step in his life, that he'd finally use his degree for good — and moved to Lesotho for a year of charity work combatting the HIV/AIDs epidemic.
Back in Philadelphia, Jack accepted a position at UPenn Hospital, working on his specialty in neonatal surgery, and doing his best to keep to himself.
JOHN ‘JACK’ BROOKS has the face claim of SCOTT SPEEDMAN and is played by LIZA.
1 note
·
View note
Text
Why is education important for girls and women?

Education is an important thing for every child to have, but it's even more important for girls and women. Why? Because there are lots of reasons why girls need education.
For example, without an education, many girls will grow up with limited choices in their lives. Also, without an education, girls can't make the most of opportunities because they won't be able to read or do arithmetic.
As per research conducted by schools in Mumbai education can be your best friend. It can also be the worst enemy. One of my favorite quotes ever is by Will Smith and it says “if you're not writing your own story, you're borrowing someone else's.”
Education is so important because it allows girls and women to write their stories. It tells them that they can reach for the stars and go places in life they never thought they could.
Another survey done by schools in Pune when it comes to education, particularly for girls and women, there is a lot of skepticism. Many people think that educating women about certain topics is a waste of time.
They think the education of women is very expensive and it can actually cost more than the benefits. These are among the big myths about women's education. Education is important for both sexes and there is no doubt that this applies equally to men and women both.
Around the world, many girls and women are kept out of school for a variety of reasons. One key reason for this gap is not only a lack of facilities to educate them but also a lack of support: parents and society often discriminate against girls and women in educational opportunities.
Education plays a large role in slowing down HIV transmission, especially with girls being able to learn about their bodies and reproductive systems. Education benefits girls and women by providing them with skills that enable them to get training or find jobs and give their children better lives.
Even education on other health topics such as nutrition is beneficial to improve the lives of women.
There are many reasons why education is important to girls and women. The most obvious reason is that education gives us the knowledge we need to solve problems facing our communities, countries, and the world.
Education also opens up economic opportunities for girls and women. For example, educated girls and women can earn a living as teachers or health workers, which enables them to be economically independent.
Community members sometimes believe that educating girls and women is a waste of time and money because they might leave the community after marriage. In fact, educated girls often return to their communities with new ideas and skills, making them valuable assets.
Furthermore, if a woman can read and write, she can pass these skills on to her children, helping them to become more successful in school.
There are many reasons why education is important. There are so many benefits of education that it is almost impossible to put into words. Education is the only key to success for girls and women in developing countries.
Education helps girls and women become aware of their rights and improve their social status. It allows girls to choose a better partner later in life, and have a healthy pregnancy and childbirth.
Educated women are more likely to work outside the home, which gives them more control over their finances and personal lives. And an educated woman will be sure to educate her own children, setting up an endless cycle of positive effects for generations to come.
"Education is one of the most important means of empowering women with the knowledge, skills, and self-confidence necessary to participate fully in the development process."
Kofi Annan, former Secretary-General of the United Nations
What does this mean? Women have a strong desire to learn and strive for success. Education allows girls and women to develop their own skills and talents, build self-confidence, improve their lives and contribute to their communities. For example, when women are educated they:
Have healthier families - Women with education usually marry later, have fewer children, and invest more time and resources in each child.
Empower themselves - A woman who can read and write has more opportunities for employment. Education also provides women with access to better-paying jobs and economic independence. This can make them less susceptible to domestic violence, abuse, harassment, and exploitation.
Contribute to society - Educated women are more likely to participate in civic life. They are more likely to become leaders in school boards, village councils, and national legislatures.
They will also become community activists working on issues such as education, health care, or human rights. Education is not just important for girls and women; it is vital for societies at large. Education is one of the most important factors in empowering women.
It enables them to have a say in their lives, and in the decisions that shape their communities.
0 notes
Text
Top 15 Safe and Romantic Date Ideas Tampa, Florida
Millionaire Mate is a dating site where wealthy men can meet beautiful women. נערות ליווי בחיפה Match is an international site, but the Asian singles that you’ll meet through Match are mainly Asian-American men and women. Poz Match began in 1998, for HIV positive dating area, it has long history. We've come up with a personality test sure to correctly match you with your birth season. You’ve been on dozens of first dates, and gamely accepted every introduction that’s come your way, but that spark-that someone special-keeps eluding you. If you are looking for a credible and reputable dating agency and matchmaker, then you have come to the right place. To sum up: if you are looking for dating, love, marriage or friendship, you reached the right place. The "coffin birth" is easy enough to explain: The woman and her gestating baby died just a couple weeks before her pregnancy reached full term. It contained the remains of a woman who had evidently given birth to her baby posthumously, as evidenced by a pile of tiny bones lying between her legs in the coffin. This woman evidently underwent trepanation very late in her pregnancy, probably in order to relieve cranial pressure brought on by eclampsia, or dangerously high blood pressure that can be fatal for both mother and baby.
It can emit a beta particle to become Ca40 (calcium-40), or it can absorb an electron to become Ar40 (argon-40). Whether an archeologist has an ideal selection of samples to choose from or must do the best they can with problematic sample materials, the reasons for submitting a sample should be made explicit during reporting, along with discussion of any potential problems with it and any attempts to mitigate those problems. The amount of daughter isotope at the time of formation of the sample is zero (or known independently and can be compensated for). If you feel that some or all of these statements describe you, you may have a difficult time deciphering whether your current partner is trustworthy, or if your core beliefs are influencing your interpretation of your partner's behaviors. What are you going to do about it? I plan out everything I'm going to do. In a field like prehistoric archaeology, this often means going through buried remains and documenting where each artifact is in relation to other artifacts, both in terms of distance and depth. No. I don't like red lipstick; it's loud. Scenes like this are too uncomfortable to stick around for!
TV and Internet recourses make the picture that all women from Ukraine are more beautiful than any other girls. The study, which examined positive and negative perceptions of dating online in women over 50, found women often described a lack of responses as reason they would consider themselves unsuccessful online. She seemed to have been intentionally and properly buried, and the grave showed no signs of being tampered with over the intervening centuries. Have a tip? Send it to us! I have identified important values for IndieWeb’s community of developers and observed how they are employed in design decisions of various types, including in response to challenges that emerge from interoperability within and external to IndieWeb’s architecture. If you are not what she is looking for, chances are she is also not what you are looking for. Whether you’re looking for certain locations or interests, we can help. I try to go to as many parties and events as I can! I have parties to go to!
Just have fun and go with it! The results of their investigation have been published in the May, 2018 issue of the journal World Neurosurgery. Science writer Ewen Callaway for the journal Nature in 2021 wrote the article “Million-year-old mammoth genomes shatter the record for oldest ancient DNA. Whatever medical dramas we go through today, we should occasionally take a moment to remember the people who died because they lived in a time when cutting-edge science prescribed drilling a hole in a woman's head to treat a common, if serious, pregnancy-related illness. Only people who love Christ more than they love you will have the courage to tell you that you’re wrong in dating - wrong about a person, wrong about timing, wrong about whatever. I sign up for all the dating apps and have a great time. Researchers have spent the past few years piecing together the evidence of what happened to this woman 1,300 years ago, and think they have an answer to what precipitated this very strange scene. We went through a pen test recently, and one of the low priority items that fell out of it was the use of Go’s math/rand in a few places instead of the cryptographically secure crypto/rand.
1 note
·
View note
Text
Best News of Last Week
Edition #017 - Hope you had a great weekend. Let's read some positive news:
1. Albuquerque has new response to 911 calls involving mentally ill people The New Mexico city created a third branch of public safety, in addition to the police and fire departments, staffed by behavioral health responders.
Now, Albuquerque is changing the way it responds to 911 calls like the one Maestas placed for her sister. In addition to police and paramedics, residents have access to a third branch of public safety: behavioral health responders.
“We’re not law enforcement, so we’re not here to cite you,” said Mariela Ruiz-Angel, director of Albuquerque Community Safety, or ACS, an independent agency alongside the police and fire departments that can be sent out by 911 dispatchers. “We’re just here to check on you. How can we help?”
2. In Extremely Rare Case, a Woman With HIV Has 'Cleared' The Virus Without Treatment
An anonymous woman from Argentina has become only the second person known to ever show no detectable traces of an HIV infection without receiving a stem cell transplantation treatment to cure it.
The so-called 'Esperanza patient', named after her hometown in Argentina, was first diagnosed with HIV-1 in 2013 – but after eight years of follow-up checks and a total of 10 commercial viral load tests, there appears to be no sign of active viral infection in her body, nor any evidence of HIV-1-associated disease.
3. My favourite Thanksgiving tradition... 6 years and counting!

Valley grandma and man she mistakenly texted reuniting for sixth Thanksgiving

4. Monarch butterflies return to California after a year of record low numbers

There is a ray of hope for the vanishing orange-and-black Western monarch butterflies.
The number wintering along California’s central coast is bouncing back after the population, whose presence is often a good indicator of ecosystem health, reached an all-time low last year. Experts pin their decline on climate change, habitat destruction and lack of food due to drought.
5. There's a link between being kind to others and happiness, UBC researcher says

Today marks World Kindness Day, and it turns out that being kind toward others may be key to our own happiness, a psychology expert says.
Studies have shown a "causal link where, when people behave in this generous, kind way, they actually end up happier themselves," said Elizabeth Dunn, a psychology professor and happiness researcher from the University of British Columbia (UBC).
6. Toronto company is making shoes that grow into apple trees to eliminate plastic waste

A Toronto designer created a pair of shoes that eventually turn into an apple tree after he spent seven years in the fashion industry and looked for more sustainable choices.
Toronto resident Luc Houle, 33, created Johnny: The Shoe That Grows Into A Tree and launched a Kickstarter to get his product made.
7. Swiss government: Same-sex couples can marry starting July 1

Switzerland’s executive body announced Wednesday that same-sex couples can get married starting on July 1 next year, making good on the resounding support Swiss voters expressed in a referendum.
The Federal Council officially said that starting Jan. 1, Switzerland would recognize the marriages of same-sex couples who wed in in other countries instead of continuing to treat the unions as simple civil partnerships.
____
That's it for this week. Until next week,
You can follow me on twitter . Also, I have a newsletter :)
Subscribe here to receive a collection of wholesome news every week in your inbox :D
272 notes
·
View notes
Text
Dark Academia Reading List for Black People/Allies (Including Queer Black Authors)
Reblog to support black writers!
Things Fall Apart: Chinua Achebe
The story of colonialism in Africa from the perspective of an indigenous African man.
Invisible Man: Langston Hughes
A coming-of-age tale told through the lense of a black man questioning his place in a white society.

Their Eyes Were Watching God: Zora Neale Hurston
a story that touches on topics such as femininity, marriage, gender roles, sex and sexuality, and growing up, through the lens of a black woman living in the south in America in the early twentieth century.

Don’t Call Us Dead: Denez Smith (Non-Binary/Trans) (Recent Publication)
This collection of poems is written by a really skilled Non-Binary trans and HIV positive poet expressing feelings on subjects like police brutality and death

I Know Why The Caged Bird Sings: Maya Angelou
The first in a seven-volume series, it is a coming-of-age story that illustrates how strength of character and a love of literature can help overcome racism and trauma
Giovanni’s Room: James Baldwin (Gay)
This book is about and features the experiences of a bisexual man, and his relationship with an Italian bartender named Giovanni in Paris, France.
An Unkindness of Ghosts: River Solomon (Non-Binary) (Recent Publication)
A story that analyzes the black experience through the lense of science fiction and space travel, and brings a black voice to an overwhelmingly white genre

Push: Sapphire (Bi)
The 1996 novel by famous bisexual writer, Sapphire also has a movie adaptation called “Precious” and both are both Massive critical successes for their dark telling of a black coming of age story about a girl escaping abuse and exploring themes of motherhood, love, abuse, and more.

Your Son Is Dead: R. Anansi (Trans)
(Yes this is my book 🙃) (Recent Publication)
A new collection of poems from a black, trans woman about her experiences in life with identity, love, and activism, that touch on these subjects in a way that is visceral, raw, at times painful, and at times inspiring.

I took part of this list from a larger video I’m doing on the topic on my YouTube channel Here!
#writing community#writblr#dark academic#dark acadamia aesthetic#dark academia#african american literature#books#book classics#romantic academia#black poetry#black voices#black lives matter#poetry#quotes#life quote
3K notes
·
View notes
Text
[“There was a real problem with women qualifying for Social Security disability and Division of AIDS services, and the larger problem of the official definition of AIDS excluding women. Terry started to take referrals from the Women’s Prison Association and began to see a lot of women who were coming out of the Bedford Hills women’s prison.
“They all talked about that they had been helped on the inside by this woman, the Muslim lady who worked in the law library. And I was amazed, because … they had their medical records; they kind of knew what was going on; they understood the whole issue of the definition. And so I kept hearing about this person who had helped them. And that was Katrina [Haslip]. And not only did I see the evidence of how good her work was, but they all loved her so much. It kind of fascinated me, because their faces would light up about Katrina, and they’d talk about her … They all talked about how shocked they were to learn that she was positive, and that she was fearless.”
(…) Katrina Haslip was one of the most important and influential leaders of the movement of HIV-positive women fighting for their rights. A vibrant, charismatic, and energetic young Black woman, grounded in her Muslim faith, Katrina was a fierce advocate for incarcerated HIV-positive women. She was born in Niagara Falls, where she grew up with twelve brothers and sisters. After two failed marriages she started using intravenous drugs and was stabbed in 1983 and treated with a blood transfusion at a time when the blood supply was not screened. She never knew exactly the source of her HIV infection. Arrested at age twenty-six in 1985 for pickpocketing, Katrina had been a sex worker with a drug habit who survived by stealing. Sentenced to five and a half years in a maximum-security prison, Bedford Hills, she found out she was HIV-positive while incarcerated. With Judy Clark, Kathy Boudin, and others, she cofounded ACE for HIV-positive women inside Bedford Hills Correctional, and, after her release in 1990, she cocreated its sister program, ACE-OUT, to help women with AIDS once they were released. “They have to deal with, How do I get my kids back?” she told The New York Times. “Where do I move to? How do I stay drug free? How do I earn money without stealing?” ACE was started because of the enormous stigma against HIV-positive inmates, who were physically and verbally abused by other inmates to the extent that their cells were set on fire. In a memorial tape, edited by Catherine Gund, Katrina testified that “we knew very little about AIDS, we knew we needed education from outside forces.” They got volunteers to come in from Montefiore Medical Center, from ACT UP, from the Department of Health, to do trainings. “As a result we were doing counseling one-on-one informally, in the yard, in the shower, wherever people ask questions. We just tried to be supportive to one another.” In one of its most remarkable achievements, ACE started a buddy system inside the prison.”]
Let The Record Show: A Political History of ACT UP, New York, 1987-1993, by Sarah Schulman
187 notes
·
View notes
Photo

Mary Asutin was Freddie Mercury’s girlfriend in the 1970s, subject of Queen’s song ‘Love of My Life’ and Freddie’s longtime friend and companion until his death.
Early Life
Mary Georgina Austin was born on March 6, 1951 in Fulham, West London. Her life had been deprived, she grew up in a struggling working-class home and her parents were poor. Her father worked as a hand-trimmer for wallpaper specialists and her mother was a domestic for a small company. Both parents were deaf and communicated through sign language and lip-reading.
At 15 she left the school and began to work as a secretary.
She moved up some shortly afterwords, when she got a job at the trendy Biba store in London as a customer PR. This was a very fashionable place, and the customers included some of the biggest celebrities of the time. One night, she attended a rock concert at a nearby college. While there, she ran into a friendly acquaintance who worked nearby, Brian May. They hit it off and they began dating. The relationship was fun, but it never got serious and they broke up on friendly terms.
1970s Freddie’s girlfriend
May was a musician and was starting a band with some talented friends, and one day he introduced her to the band, when she was 19. Though she wasn't aware of it at the time, she attracted the infatuation of the group's lead singer, a co-worker of May's who called himself Freddie Mercury. Mercury soon frequented the store she worked at and they became increasingly friendly. With fellow band member Roger Taylor, both ran a stall in nearby Kensington Market, selling old clothes and Freddie’s artwork.
Six months later, he surprised her by asking her out on a date, which she accepted after some hesitation. Both were financially strapped, so they had to do things together that didn't involve spending money. He was a flamboyant person in public, which she found intimidating, being a shy and unassuming person, herself, but Mary found herself fascinated by this “wild-looking artistic musician”. However, she eventually got to see the side of himself that he didn't show others, a serious and quiet person who was mistrustful of others. She says, “He was like no one I had ever met before. He was very confident and I have never been confident. We grew together. I liked him - and it went on from there.”
When Freddie first asked her for a date on his 24th birthday, Mary pretended she was busy on that particular night. “I was trying to be cool,” she recalls with a smile, “not because there was any real reason I couldn’t go. But Freddie wasn’t put off. We went out the next day instead. He wanted to go and see Mott The Hoople at the Marquee Club in Soho. Freddie didn’t have much money then and so we just did normal things like any other young people. There were no fancy dinners - they came later when he hit the big time. It took about three years for me to really fall in love. But I had never felt that way about anyone.”
She first shared a £10-a-week bedsit with Freddie in Victoria Road, Kensington. It was at this time that Freddie Mercury proposed to Mary Austin. On Christmas Day in 1973, he gave her a big box. Inside, there was another box: "[Then] another and so it went on. It was like one of his playful games. Eventually, I found a lovely jade ring inside the last small box." Confused, she asked where she should put it on. "Ring finger, left hand," he answered. Then he elaborated "Because, will you marry me?" She accepted. After two years together they moved to a larger, self-contained flat in Holland Road, which cost them £19 a week. By then Queen had signed a record deal and had their first big hit, “Seven Seas Of Rhye”.
It was at a showcase held at Ealing College of Art, Freddie’s old art school, that Mary first recognised his star quality.
Mary remembers the first time she took Freddie, with his thick mane of long, black hair, home to meet her father in their terraced Fulham home. “I hadn`t warned my father how extraordinary looking Freddie was and so I think my father handled the situation very well. Sadly, my mother never met Freddie as she had died four years earlier. My father opened the door and just stayed very calm and treated Freddie very warmly. There were a few glances and comments from the neighbours. Afterwards I realised bringing home this musician must have been quite a shock for him.”
Although Mary and Freddie were engaged to be married, the marriage never took place. It was after they had moved to their second flat in Holland Road that Mary first started to think something was going wrong with their six-year relationship. As Queen grew ever more successful, their relationship cooled. Freddie Mercury started staying out to increasingly late hours, prompting Austin to wonder whether he was sleeping with another woman.
Everything changed one day when Freddie told her he had something important to say, something that would change their whole relationship forever. Mary explains, “Being a bit naive, it had taken me a while to realise the truth. Afterwards he felt good about having finally told me he was bisexual.” Mary decided to move out, but Freddie insisted she shouldn`t move too far from him. After a six-year relationship, Freddie and Mary split up in 1980.
After that, their physical relationship ended, but their connection deepened. Freddie Mercury bought her a flat nearby his apartment and employed her as his personal assistant.
1980s and beyond
Mary and Freddie keep their friendship through all his life. In a 1985 interview, Freddie Mercury said: "All my lovers asked me why they couldn't replace Mary, but it's simply impossible. The only friend I've got is Mary, and I don't want anybody else. To me, she was my common-law wife. To me, it was a marriage. We believe in each other, that's enough for me."
In 1987, he revealed to her that he had tested positive for the HIV virus. She was the first person he told, and she never repeated it to anyone through the remainder of his life. One of Mercury's top priorities was making sure that Mary was financially secure, but she was interested in making sure he take care of his health.
From that moment she was there each day to try to comfort him as he gradually became more ill. Having stayed with Mercury throughout his battle with AIDs, their relationship intensified as the focus on his diminishing life did. "During those times I did really feel such love for him," Austin remembers, "They were the moments I remembered every time I looked at his bed. I would sit every day next to the bed for six hours, whether he was awake or not. He would suddenly wake up and smile and say, 'Oh, it's you, old faithful.'" She also had to take care of her baby son Richard Frederick, born on March 1990, and whom Freddie Mercury was his godfather; and was pregnant of her second son by that time.
Realising he was starting to lose his sight and with his body becoming so weak that finally he couldn’t even get out of bed, Freddie decided to face up to dying by refusing to take his medication. Mary had been his bedrock and a particular comfort in his final years. Finally in 1991, his health deteriorated and he passed away on November of that year at the age of 45. She was devastated when he finally chose to die. "It was the loneliest and most difficult time of my life after Freddie died." In the settling of his estate, Mary was left with the majority of his vast fortune, more than she had expected. Including that was his palatial mansion, which she agreed to move in to. That turned out to be more complicated than expected, as the mansion had a large staff and the settling of Mercury's estate took several months. It took her five years before she could even feel comfortable in the house he left her.
She too expressed a feeling that a kind of marriage had occurred between the two: "I lost somebody who I thought was my eternal love. When he died I felt we'd had a marriage. We'd lived our vows. We'd done it for better for worse, for richer for poorer. In sickness and in health. You could never have let go of Freddie unless he died. Even then it was difficult." Freddie’s cremated remains were left to her. To this day, she is the sole person with the knowledge as to the location of his remains.
Mary would go on to marry twice, first to a painter named Piers Cameron and had two sons with him, Richard Frederick born on March 1990, and Jamie Alistair, born on February 1992. "[Piers] always felt overshadowed by Freddie," Austin explained. "Freddie had widened the tapestry of my life so much... There was no way I'd want to desert him ever."
Later, she married a businessman called Nicholas Holford on Long Island, without telling anyone, with just Mary’s two sons, Richard and Jamie, by their side. This relationship only lasted five years.
She also started a foundation in Mercury's memory, and also continues to support Queen's musical efforts. She continues to live quietly in the mansion, but occasionally grants interviews.
#Mary Austin#1960s#1970s#1980s#1990s#freddie mercury#Brian May#Roger Taylor#Queen#secretary#customer pr#personal assistant#shop assistant#biography
35 notes
·
View notes
Text
SHE GOT CAUGHT CHEATING RED HANDED WITH A SMOKING GUN. OMG

Mike Olivier exposed all the 30 girls he slept with when he was on his vacation in Kenya.He is divorced and also HIV positive .The ladies that slept with him did not know that he was HIV positive only to find later when he was gone.
A lady by the name of Emmah was seen by her fiance in the trending photos that were exposed by Mike Oliver. Her fiance could not believe it and he called off their wedding. He trusted Emmah with his heart but Emmah betrayed her now he is a laughing stock.


According to their conversation,Paul was the one who was taking care of her.He was even supporting her family financially.He even secured employment opportunities for her brother and sister.Emmah denied the allegations and said that the pictures were Photoshop and she would never betray him.But it was too late cause Paul his fiance had already cancelled the wedding.


Mike Oliver ruins lots of marriages and he even left some of these woman pregnant. He knew that his money would make these woman fall inlove with him.Now those who became pregnant will raise their children on their own without a father.
Source: Opera News
Additional source
2nd additional source
3rd additional source
69 notes
·
View notes
Text
Working up the courage to post for friends/family.
To my Trump supporters:
You know me. We are friends, family. You know who I am, you know that I am happily married to a woman, you know we've been together for 8 years.
You may know because I told you myself. I got some mixed reactions there. Some of you embraced me fully, thank you. Others, conditionally. You didn't agree, but loved me anyway. You wouldn't tell anyone, they wouldn't understand. But you loved me anyway. And I felt lucky, that somehow I was a worthy enough person to still have your love, even if I didn't have your acceptance.
Some of you learned less directly. It was an unspoken secret, a passing whisper. I remember the pit in my stomach at family gatherings, the anxiety at each coming out - whether I spoke the words or your eyes lingered on my plus-one. And still, some of you accepted me. Others ignored it. Some, outright denial, to this day calling my wife my "friend."
But, well, the bar was low. No one disowned me. No one told me it was a phase, or that I was confused. Of the coming-out stories I know, it wasn't terribly contentious. And so it felt like a relief, to be the secret. To be loved despite who I was. It felt like a victory.
I suppose it's on me that I've been so accommodating for so long. How could I expect anyone to know how I feel when I tolerate lukewarm support? How could I expect you to understand the ways you actively harm me and others like me with what you say, do, how you vote?
I'm not writing this to start fights or guilt anyone. I'm writing it so that you know where I stand. And if you want to vote, support, speak in ways that harm me and my community, at least you'll be doing it intentionally, with a full understanding of how that feels, of how it affects me.
Before I get personal, here's a list of how Trump has harmed the LGBTQ community. This is pulled from the HRC, more details here: https://www.hrc.org/news/the-list-of-trumps-unprecedented-steps-for-the-lgbtq-community
-Opposition to the Equality Act
-Appointed anti-LGBTQ judges
-Joked about Pence’s desire to hang LGBTQ people
In the Workplace
-Supported employment discrimination against LGBTQ people
-Banned transgender service members from the military
-Rolled back Obama-era non-discrimination protections
-Issued rule to license discrimination
-Kicked people living with HIV out of the military because of their status
-Created a hostile work environment for LGBTQ federal employees
In Health Care
-Undermine Section 1557 Rule
-Advocated for the elimination of the entire Affordable Care Act
-Created a Religious Discrimination Division
-Proposed cutting over $1.35 billion from PEPFAR budget
In Schools
-Harmful Guidance for Schools on Transgender Students
-Rejected Complaints From Transgender Students
-Suggested it is acceptable for schools to discriminate against LGBTQ students while accepting tax-payer funds
-Made it harder for sexual assualt victims to receive justice
-Eliminated language protecting LGBTQ children participating in the 4-H program
-Used Title IX to discriminate against trans students
In Housing
-Allowed emergency shelters to deny access to transgender and gender nonconforming people
-Placed transgender incarcerated persons in the wrong prison
In Families
-Allowed foster care programs to discriminate while accepting tax-payer funds
-Refused visas to partners of diplomats
-Changed rules to deny surrogate born children citizenship
In Representation
-Erased transgender people
-Eliminated information on LGBTQ rights, mentions, and representation on government websites
-Blocked questions regarding sexual orientation from consideration for the census
Refused to recognize LGBTQ people in National AIDS day Address
In the World
-Refusing LGBTQ asylum seekers fleeing violence
-Ban Embassy Pride Flags
-Refused to condemn attacks on LGBTQ people in Chechnya
-Refused to condemn a law punishing LGBTQ people in Brunei
It's a long list. A long list of tangible policy (and lack of policy) that demonstrates the harm of this administration against my community. But we all know it's more than politics. Trump's presence in a position of power and his rhetoric have emboldened some less savory characters in our society. This has been overwhelming for the Black community, who have endured as white supremacy rears its ugly head again. But the hatred and discrimination that Trump has normalized affects all minorities.
I've been incredibly fortunate in my experience. But this is the message I need you to understand. Hatred against people like me is real. Sometimes it's simple microaggressions. Other times it's assault. It ranges from personal to systemic.
On election night in 2016, I sobbed in fear or what was ahead. We'd elected a homophobe as Vice President, and Trump wasn't much better.
Many told me it wouldn't be that bad for me. They brushed aside my concerns, I was being dramatic. And this is easy to say from a position of privilege. But for me, I thought of my experiences.
I thought of coming out, and the reactions I received. I remember how a coworker at the time told me that people I didn't even know had talked about how I was a dyke, and she put them in their place by telling them I wasn't.
I remember when my girlfriend and I were moving into an apartment and were asked if we were sisters. How many times we've confused people with our relationship.
I remember a job interview where I was asked about my boyfriend, panicking when asked in a professional setting about my personal life because saying wife could go badly.
I've come out over and over again, and it never gets easier.
I remember the time I was at the movies and I dared to hold her hand. How someone dumped a cup of chew on her head. We don't go to the movies in our hometowns anymore. If we do, we sit in the back against the wall.
You don't know the fear that I felt then, when I saw all of these flash before me, knowing that things would get worse.
Now, there are two justices who want to overturn my marriage. A third won't say what she'll do if confirmed.
I wasn't wrong. I wasn't being dramatic. This is my life. This is the lives of minorities in America. You can't ignore these experiences, as if they've never happened.
You're free to vote for Trump. Of course. Just know that you're allowing this to happen. Know that you're choosing him over me, over my wife, over every Black man, woman and child, every queer person, every trans person, every immigrant...the list goes on, and on, and on.
Know the consequences of the decision. Not just for you, but for everyone.
9 notes
·
View notes
Text
10 Queer Characters/Couples in Indian Media
A topic that has been taboo in Indian society forever now, homosexuality is now prevalent and more talked about than ever. There have been many forms of normalization the Indian audience has been exposed to, such as literature, social media awareness, and of course, Indian Media. In celebration of Pride Month, I’d like to stray away from the more dehumanizing and embarrassing portrayals of LGBTQ+ characters and instead focus on the more positive and realistic portrayals of them. So here are 10 queer characters and couples in Indian Media (keep in mind, I probably missed some queer Indian characters, so please don’t @ me. These are some of my personal favorites and most of these movies are available on online platforms)
*minor spoiler for Kapoor and Sons*
*THIS WAS WRITTEN BEFORE THE BLM PROTESTS. DONATE TO THE MOVEMENT OR SIGN PETITIONS*
1. AMAN-KARTHIK IN SHUBH MANGAL ZYADA SAAVDHAN

Probably the most recent one on the list, SMZS took the internet by surprise with the great representation. Starring Ayushmann Khurrana as Karthik and Jitendra Kumar as Aman, the movie showed a healthy relationship between the two and made their personalities deeper than the typical gay man stereotype. Although the movie did have a story structure similar to the modern situational comedy movies (i.e. Dream Girl and Badhaai Ho), this movie is a fun ride and an important step towards LGBTQ+ acceptance in Indian cinema. SMZS is available of Amazon Prime.
2. SWEETY-KUHU IN EK LADKI KO DEKHA TOH AISA LAGA

Proclaimed as the first mainstream Bollywood movie to showcase a lesbian love story as the main focus, this movie was bold for many. Starring Sonam Kapoor as Sweety and Regina Cassandra as Kuhu, their chemistry on-screen was lovable and so was the innocence of their intentions. Sweety’s journey of acceptance of her identity is one that many could empathize with and the movie overall was visually pleasing to look at. In technical terms, I found the movie slightly bland but that doesn’t make me disregard the impact it has had in queer love stories in Bollywood. Watch it on Netflix.
3. SHABNAM MAUSI IN SHABNAM MAUSI
Rolling backwards in time to 2005′s, Shabnam Mausi is about the real-life Shabnam Bano, the first transgender woman to become a political activist. Played by Ashutosh Rana, this movie was incredibly risky for obvious reasons. At that time, transgender women were ostracized by society and for a fairly famous Rana to take up this role was daring. Even though the movie had exaggerated many events that took place in Bano’s life, Ashutosh Rana’s great performance can’t be ignored.
4. RAHUL KAPOOR IN KAPOOR AND SONS

2016′s Kapoor and Son’s was an emotional movie centered around a family and their troubles. The oldest son Rahul, played by Fawad Khan, for most of the runtime is portrayed to be the perfect child but towards the end, it is discovered that he is a closeted gay in a relationship. Fawad Khan is charming and effortless as always and he bought a sense of rawness and authenticity to his performance. His subplot is just one of the many brushstrokes that make this movie the way it is. Available on Netflix.
5. RADHA-SITA IN FIRE

Both Shabana Azmi and Nandita Das were proven brave for taking up the role of Radha and Sita, especially considering the negativity surrounding LGBTQ folks at 1996 India. The movie was unjustly marred with controversy and hate by conservatives, but almost all critics hailed this film as gutsy and path-breaking, which it was in many ways. Along with portraying a lesbian love story in the forefront, the movie also portrays unhappy marriages and age gap relationships well. Catch this one of YouTube.
6. LAILA-KHANUM IN MARGARITA WITH A STRAW

Laila is a teenager with celebral palsy and Khanum is a blind Pakistani-Bangladeshi. The two extremely daring roles were carried out to near perfection by Kalki and Sayani in this gem of a movie. The chemistry between them was impeccable and the moments they have together will definitely make you tear up. This movie was path-breaking for portraying characters with disabilities in a good way and (of course) tackling the subject of sexuality with nuance. Catch this heartfelt movie on Hulu.
7. PROFESSOR SIRAS IN ALIGARH

Aligarh is a biopic of Professor Ramchandra Siras, a former professor at Aligarh Muslim University who was caught getting intimate with a rickshaw puller, causing him to get suspended. Siras is a character easy to empathize with and everything that Bajpayee emoted was very praiseworthy. You could really feel Siras’ pain and struggle through the screen. Despite the movie being moderately successful, Bajpayee’s performance didn’t go unnoticed and he went on to win a Filmfare in Best Actor (Critics) category.
8. SHILPA IN SUPER DELUXE

The only regional character in this list, Shilpa played by Vijay Sethupathi is a transgender woman who comes back to her childhood town to meet her family and child she left years ago. Although she is a small part of this 3 hour long movie, she is easily the most iconic character and her conversations with Rasukutty seems very genuine and wholesome. Her storyline was engaging and when the sad and unfortunate incident happens to her, I couldn’t help but shed a tear. Definitely one of my most favorite characters in South Indian cinema. Watch this masterpiece of a movie on Netflix.
9. NIKHIL-NIGEL IN MY BROTHER... NIKHIL

Nikhil Kapoor, played by Sanjay Suri, is a competitive swimmer who has a hard time with accepting himself when he has HIV and Nigel D’Costa is his supportive boyfriend. Much like Shabnam Mausi and Aligarh, the movie is based on the real life Dominic D’Souza, who was a well-known AIDS activist. Certainly another brave attempt to normalize gay portrayal in the silver screen during challenging times, the movie was received well worldwide and deservedly so. The movie featured great performances from everyone and the ending carried so many mixed emotions that it was just beautiful. Available on YouTube.
10. KARAN MEHRA IN MADE IN HEAVEN

One of my personal favorites in the list, Karan, played brilliantly by Arjun Mathur, is a wedding planner along with Tara Khanna. He is a well-fleshed out character with a great personality and I think 50% of my most favorite moments are with him in it. The web series manages to show the nitty gritty situations gay people faced before the court’s decision on Section 377, from the parents’ reactions, to facing society’s stigma. I found myself sobbing and smiling along with him throughout the series and I am interested as to what is planned ahead for him. Please watch this series on Amazon Prime its very good.
NOTE: IN THE LIGHT OF THE RECENT PROTESTS AGAINST POLICE BRUTALITY, I’D LIKE TO TAKE A MOMENT TO SAY THAT MY HEART GOES OUT TO THE AFRICAN-AMERICAN COMMUNITY. I WILL NEVER UNDERSTAND THE PAIN AND STRUGGLE YOU GO THROUGH, BUT KNOW THAT I WILL FOREVER SUPPORT THE BLACK LIVES MATTER MOVEMENT AND I URGE ANYONE READING TO CLICK ON THE LINKS ABOVE TO MAKE DONATIONS OR SIGN PETITIONS. #BLACKLIVESMATTER AND #ACAB
#film#film list#bollywood#bollywood movies#top 10 list#lgbtq#pride month#pride#lgbt#lgbtpride#ayushmaan khuranna#jitendra kumar#smzs#bollywood2#sonam kapoor#regina cassandra#elkdtal#ek ladki ko dekha toh aisa laga#shubh mangal zyada saavdhan#ashutosh rana#shabnam mausi#fawad khan#kapoor and sons#shabana azmi#nandita das#fire#kalki koechlin#sayani gupta#margarita with a straw#manoj bajpayee
44 notes
·
View notes
Last Seen Blogs

smokingmensmoking
Smoking Men Smoking

smithingegbert
A simple blacksmith

smokecrafthollow
SmokeCraft Hollow

gianttinypinoy
Untitled

irie-shou-chan-blog
The future in my hands