#Molecular detection
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr’s reach among the 26-to-35-year-olds in the US is 11%.
Text
Molecular detection of Hepatits B virus genotypes in tertiary hospitals in Yenagoa, Nigeria by Nwodo Miriam U in Journal of Clinical Case Reports Medical Images and Health Sciences
Abstract
Despite HBV being endemic or hyper endemic in Africa, there is paucity of data on the genotypes and their distribution in this part of the country. This study is aimed at detecting the prevalent genotypes of HBV among patients attending two tertiary hospitals in Yenagoa, Nigeria. A total of 656 patients [females 475(72.4%) and males 181(27.6%)] were tested for Hepatitis B surface antigen (HBsAg) between the period of January to June 2022. Blood samples collected were analyzed using immunochromatography techniques for HBsAg detection and multiplex Polymerase chain reaction (PCR) using type-specific primers for genotyping. Of the 656 patients screened for HBsAg, 66 (10%) [36, 5.4% female; 30, 4.6% male] were positive using immunochromatography and were then subjected to molecular genotyping using specific primers to A, B, C, D, E and F. Likewise, 33(50%) were positive using PCR while the remaining showed passive positivity as a result of degradation of the virus being a non-enveloped virus. This finding showed that HBV/E and HBV/B were the major identified genotypes with prevalence of 82.4% and 11.8% respectively in Yenagoa, Bayelsa State. HBV/B+E mixed infections was seen with a prevalence of 5.9%, found amongst 2 female subjects within age group 26-25. In the clinical sector in Yenagoa, tenofovir a nucleotide analog is used. It has been shown from previous studies that HBV E is more sensitive to nucleotide analogs while HBV B is more sensitive to interferon-based therapies. In conclusion, HBV genotypes B, E and B+E were discovered in Yenagoa, Bayelsa State.
Background of the study
The inflamed tissue of the liver is what medical professionals refer to as hepatitis. Some people who have hepatitis do not show any symptoms, while others develop jaundice, which is characterized by a yellow discoloration of the skin and the whites of the eyes, as well as an inability to eat, vomiting, weariness, abdominal pain, and diarrhea. Jaundice can also be caused by cirrhosis, which is characterized by a yellow discoloration of the skin and the whites of the eyes (WHO, 2022). If one has hepatitis and it goes away in less than six months, then you had acute hepatitis; however, if it lasts longer than six months, then one had chronic hepatitis. It is possible for acute hepatitis to clear up on its own, progress into chronic hepatitis, or even (very rarely) result in sudden liver failure. All of these outcomes are possible. Chronic hepatitis can lead to a number of serious complications, including scarring of the liver (sometimes called cirrhosis), liver failure and even cancer of the liver. Viral hepatitis is a term that refers to hepatitis that is caused by infection with any one of a wide variety of hepatotropic viruses (Lamontagne et al., 2016). These viruses include hepatitis A, B, C, D, and E. Hepatitis caused by a virus is a systemic illness that mostly manifests itself in the liver and is distinguished by an inflammation of the liver's primary tissue. These viruses are all RNA viruses, with the exception of the hepatitis B virus (HBV), which is a DNA virus. Other probable causes of hepatitis include: excessive use of alcohol, the use of certain medicines, exposure to chemicals, a variety of infections, autoimmune diseases and non-alcoholic steatohepatitis, which is also referred to as NASH (Wang et al., 2012).
Both acute and chronic hepatitis may be brought on by the hepatotropic, enveloped, non-cytopathic HBV virus. It exclusively infects humans and a small number of other primate species, exhibiting a limited host range. Hepatitis B virus (HBV) is a serious public health concern that can be fatal, even though there is a safe vaccination for it today. This is especially true in Asia, Africa, and South America. The clinical manifestations of HBV infection can range from the asymptomatic carrier state through acute hepatitis, fulminant hepatitis, chronic hepatitis, liver cirrhosis (LC), and hepatocellular cancer (HCC). Genetic traits of the host, viral characteristics, and environmental variables all have a role in the progression of chronic hepatitis B (CHB) illness to severe liver disorders including LC and HCC (Mustafa, 2014). All hepdnaviruses, like HBV, have the same distinct three morphologic forms, counterparts to the HBV envelope and nucleocapsid virus antigens, replicate in the liver but emerge in extrahepatic locations, encompass their own endogenous DNA polymerase, possess partially double-stranded and partly single-stranded genomes, and rely on a replicative strategy that is unique among DNA viruses but typical of opportunistic bacteria. Hepadnaviruses rely on reverse transcription (performed by the DNA polymerase) of minus-strand DNA from a "pregenomic" RNA intermediary rather than DNA replication straight from a DNA template. After that, the DNA-dependent DNA polymerase converts the plus-strand DNA from the minus-strand DNA template into a covalently closed circular DNA in the hepatocyte nucleus, which is used as a blueprint for messenger RNA and pregenomic RNA. The messenger RNA translates viral proteins, which are then packed into virions and released from the hepatocyte together with the viral DNA. Although HBV is challenging to grow in vitro in the traditional sense from clinical material, HBV DNA has been transfected into a number of cell lines. These transfected cells enable the in vitro replication of the whole virus and its constituent proteins (Jules and Kurt, 2012).
Healthcare issues related to hepatitis B are widespread, particularly in areas with a lower level of economic development. It is estimated that one third of all persons on the earth have the hepatitis B virus in their bodies. (Ahmad et al., 2019) and only 0.5 percent can spontaneously seroconvert from having the hepatitis B surface antigen (HBsAg) to having the hepatitis B surface antibody each year. This means that roughly 350–400 million people are living with a lifetime chronic infection. Chronic hepatitis B infection can lead to liver cirrhosis (LC) and hepatocellular carcinoma (HCC), however cirrhosis only develops in a tiny fraction of individuals. Hepatocellular carcinoma (HCC) development and on occasion cirrhosis, are side effects of hepatitis B. Numerous dermatologic, cardiac, joint, neurologic, hematologic, and gastrointestinal (GI) tract symptoms are observed, along with glomerulonephritis and polyarthritis nodes. Since the 1970s, significant progress has been achieved in the areas of knowledge relevant to the epidemiology, virology, natural history, and treatment of the hepatitis B virion, which is a hepatotropic viral particle. These areas of study concern the infectious agent that causes hepatitis B. In addition, it has been demonstrated that continuing vaccination programs are effective in reducing the prevalence of HBV disease in a number of different nations around the world (Anna, 2014).
The virus can be transmitted by exposure to infectious blood or body fluids (through child birth or from contact with other people’s blood). Intravenous drug use, tattooing, acupuncture, blood transfusion, dialysis, sexual intercourse are the most frequent routes of infection. The virus cannot be spread by holding hands, sharing eating utensils, kissing, hugging, coughing, sneezing or breastfeeding (CDC, 2015)
Recent studies have led to the discovery of eleven different HBV genotypes (A through J), each of which is found in a specific region of the world. To correctly classify a person's genotype, the differences in their genome sequence must be at least 8%. E is the genotype that is found in the most people in Sub-Saharan Africa, followed by A and D. Genotype D is the one that occurs the least frequently. Both the clinical outcome and the patient's response to therapy based on interferon are significantly influenced by the HBV genotype. Interferon-based therapy is one such example. In spite of the fact that genotypes A and B have higher rates of spontaneous HBeAg seroconversion in comparison to genotypes C and D, infections with HBV genotypes A and D typically progress further into the chronic phase than infections with HBV genotypes B and C do. This is due to the fact that infections with HBV genotypes A and D have a higher risk of developing hepatocellular carcinoma. The HBV genotype E that is most prevalent in West Africa is only marginally related to pre-core and basal core promoter alterations, and it also has a poor response to interferon-based therapy. This genotype is responsible for the majority of HBV infections in the region. Additionally, recent investigations conducted elsewhere have revealed rare HBV mixed genotype infections, which may indicate similar clinical results Additionally, recent investigations conducted elsewhere have revealed rare HBV mixed genotype infections, which may indicate similar clinical results (Ahmad et al., 2019).
Aim: This study was aimed to pinpoint the HBV genotypes that are most common in Yenagoa, Bayelsa State, Nigeria.
MATERIALS AND METHODS
Study area
Between Delta state and Rivers state, in the central Niger Delta region of Southern Nigeria, sits the state of Bayelsa. On October 1, 1996, the military regime of General Sani Abacha separated the state from Rivers state. Eight Local Government Areas make up the state of Bayelsa. The mainstay of the economy in the state the government. The state is heterogeneous in nature with cultural varieties among the inhabitants in Sagbama and Ekeremor; Ogbia, Nembe, Brass and Yenagoa, Kolokuma-Opokuma and Southern Ijaw respectively. There are eight local government in Bayelsa state which include: Yenagoa, Ogbia, Brass, Nembe, Kolokuma/Opokuma, Southern Ijaw, Sagbama and Ekeremor local government. While Yenagoa stood as the capital of Bayelsa state. The population of Bayelsa state is put at about 1.7million people as at the 2006 census. Geographically, Bayelsa state is on latitude 04o151North, 05o231South and longitude 05o221West and 06o451East. The state is bounded with Delta State on the North, Rivers State on the East and the Atlantic Ocean on the West and South as shown in. This work was carried out in two selected health facilities in Yenagoa, Bayelsa State between the period of January and June, 2021. Most people residing in Bayelsa state are government workers. Other occupation of the people in the state includes: farming, trading and as well fishing.
Study Population
All patients that are sent to the laboratory to test for HBsAg make up the study population.
Ethical Approval
A letter of approval was issued by the H.O.D of the department of Medical Laboratory Science NDU, which was presented to the Ethics and research Committee of the Federal Medical Centre and Niger Delta University Teaching Hospital in Bayelsa state after which their approval for this study was given.
Inclusion criteria
All patients who present themselves to the laboratory department for HBsAg test and those attending the gastroenterology clinics of both hospitals were recruited for this research.
Exclusion criteria
All patients who are not running HBsAg test at the laboratory department and those not attending the gastroenterology clinics of both hospitals were excluded from this study. Also those who rejected verbal consent were excluded.
Sample Collection
For this analysis, 4mls of whole blood sample was collected from each patient into ethylene diaminetetra-acetic acid bottle and centrifuged at 3000rpm for 5 min to separate the plasma. Plasma was used for screening of HBsAg, HIV and HCV while the red cells were taken to the molecular laboratory in NDU in ice packs for DNA extraction and genotyping.
Sample processing
Using a Surge-lab rapid immuno-chromatographic test strip, the HBsAg status of all samples was confirmed after initial immuno-chromatographic testing for HCV and HIV to rule out those conditions. After that, the separated plasma was put into plain bottles and refrigerated at -4°C until analysis. The whole blood was also stored at 40°C for extraction.
Laboratory Methods and Procedures
HBsAg Status Determination
The HBsAg status was determined using skytec test kits according to manufacturer’s instructions following WHO standard alogarithm (WHO, 2015).
Test Procedure
The test card's protective foil cover was taken off, and 50ul of plasma was put to the sample pad before being allowed to flow. After 15 minutes, the result was read.
HCV Status Determination
The Hcv status was determined using skytec test kits according to manufacturer’s instructions following WHO standard alogarithm (WHO, 2015).
Test Procedure
The test card's protective foil cover was taken off, and 50ul of plasma was put to the sample pad before being allowed to flow. After 15 minutes, the result was read.
HIV Status Determination
The HIV status was determined using Determine test kits according to manufacturer’s instructions following WHO testing allogarithm (WH0, 2015)
Test Procedure
The test card's protective foil cover was taken off, 50ul of whole blood was applied to the sample pad along with one drop of chase buffer. Results were read 15 to 60 minutes later.
HBV 5 panel test
Test Procedure
The test device was removed from its pouch and place on a flat surface.5µl of plasma was dispensed into the sample pad for each of the 5 viral markers. Result were read after 10 minutes.
The process of extracting DNA from a blood sample
A total volume of 100 uL of blood was treated with 400 uL of the Genomic Lysis Buffer. After that, it was thoroughly combined by vortexing for four to six seconds, and then it was permitted to sit at room temperature for five to ten minutes. After that, the mixture was moved to a Zymo-Spin IIC Column that was contained inside of a collecting Tube. The centrifuge was set to 10,000 x g, and it ran for one whole minute. It was decided to throw away the Collection Tube that had the flow through. The Zymo-Spin IIC Column was subsequently moved to a different Collection Tube after the move. After adding 200 ul of DNA Pre-Wash Buffer to the spin column, it was then centrifuged at a speed of 10,000 x g for a period of one minute. After adding 500 uL of g-DNA Wash Buffer to the spin column, it was then subjected to one minute of centrifugation at 10,000 x g. After that, the spin column was moved to a microcentrifuge tube that had been cleaned. The spin column received an additional 50 uL of DNA Elution Buffer. After that, it was allowed to sit at room temperature for two to five minutes before being centrifuged at maximum speed (10,000xg) for thirty seconds in order to extract the DNA. The eluted DNA was kept frozen at a temperature of -20 degrees Celsius for later usage.
DNA Quantification
Using the Nanodrop 1000 spectrophotometer, the genomic DNA that had been extracted was measured and analyzed. The software of the apparatus was activated by performing a double click on the Nanodrop icon on the desktop. The apparatus was calibrated using 2 ul of sterile distilled water, and then it was blanked with normal saline solution. Following the transfer of two microliters of the extracted DNA to the lower pedestal, the DNA on the lower pedestal was brought into contact with the DNA on the upper pedestal by lowering the upper pedestal. The amount of DNA in the sample was determined by selecting the "measure" button on the toolbar. While the level of DNA purity was assessed by the 260/280 absorbance ratio, DNA concentration was quantified in ng/ul (ranging from 5 to 100 ng/ul) (1.5 – 2.0).
Multiplex‑nested polymerase chain reaction (PCR)
This was done using type‑specific primers used to assign genotypes A through F based on pre‑S1 through S genes of the HBV genome.
First round polymerase chain reaction: Hepatitis B virus DNA detection.
During the initial round of the nested PCR, the total volume of the reaction that was carried out was 20 L. The sample ID was written on the label of each of the premix tubes. After the DNA was extracted, it was put into a Master Mix, which consisted of a cocktail of 16 uL of deionized water [D.H2O] and a premix of 250 M of each dNTP, 1X PCR buffer, 15 mM of MgCl2, and 1U of thermostable Taq polymerase, along with 1uL of P1 (forward) and S1 2 (reverse) outer primers in equal amounts. The PCR was carried out with a thermal cycler, and the reaction conditions were as follows: initial activation at 95 degrees Celsius for five minutes; denaturation at 94 degrees Celsius for twenty seconds; annealing at 60 degrees Celsius for thirty seconds; and extension at 72 degrees Celsius for one minute. The temperature of the first six cycles was lowered by a total of –0.50 C, while the temperature of the subsequent 29 cycles was maintained at 570 C. There were a total of 35 whole cycle sets that were observed, going from denaturation through extension. The third and final extension was carried out at 72 degrees Celsius for five minutes.
Second‑round polymerase chain reaction: Hepatitis B virus genotyping
The second round of PCR was carried out in two separate tubes for each sample. The first tube contained the common universal sense primer (B2) and type specific primers for the genotypes A, B, and C. The second tube contained the common universal anti sense primer (B2R) and genotype specific primers for the genotypes D, E, and F. The second round of PCR was carried out in two different tubes for each sample. Each tube containing premix 'A' and 'B' received an additional 17 uL of water that had been distilled. The mixes each received an additional 0.5 ul of each of the four primers, which brought the total volume to 2 ul of primers total. 1 u of the product of the first PCR round should be added to each tube of the premix. After being stirred carefully, the mixture was centrifuged. The PCR conditions were kept the same as before. After running 20 uL of each of the negative control, samples, and the ladder across an agarose gel containing 2%, the gel was then electrophoresed in a buffer containing 1 x TAE for 45 minutes at 100V.
Primer Sequence (5’‑3’) Specificity Position Polarity
Agarose Gel Electrophoresis
On a 1% agarose gel prepared in 1X Tri-Boris EDTA containing 5ls of 'Safe View,' the amplicons were measured against a 100bp molecular weight marker. The gel was then run in a horizontal tank filled with 1X Tri-Boris EDTA for 30 minutes at 350V. Under a blue light transillumination, each gel was examined with the PrepOneTM Sapphire EC135-90. Electrophoresis was performed at a voltage of 100 mV for a period of 30 minutes. We were able to determine the size of the bands as well as the fragment size by comparing the bands to a DNA ladder that was 100 kb or longer.
Analyses of statistical data
The Statistical Package for the Social Sciences (SPSS) version 21 was utilized in order to perform the analysis on the data that was gathered from this study. Chi-square tests were used to make comparisons between the variables. A statistically significant p-value was determined to be lower than 0.05. Tables, pie charts, and percentage breakdowns were used to show the findings.
RESULTS
Demographic presentation of participants
Of a total of 656 subjects screened for HBsAg, 475 (72.4%) were females while their male counterpart had 181 (27.6%) participants. The age distribution revealed that 301 (45.9%) were aged 26-35, 120 (18.3%) were aged 36-45, 118 (18.0%) were within 16-25 and 49 (7.5%) were >56. 38 (5.8%) and 30 (4.6%) were within 46-55 and less than 15 respectively.
Of the 656 participants, 66 (10%) were positive to HBsAg with females having 36 (5.4%) positive subjects and 439 (66.9%) negative. Male participants had 30 (4.6%) positive subjects with 151 (23.0%) negative which were not included for further studies.
Distribution of HBV using the 5-panel testing kit
The median age for the 66 positive HBsAg participants were 31 (26-35) years of which 36 (54.6%) were female while males were 30 (44.5%). Age group 26-45 had 37 (5.6%) positive participants followed by 36-45 with 14 (2.1%), then 16-25 with 9 (1.4%). 0-15 had 2 (0.3%) followed by ≥56 with 1 (0.1%).
Of the 66 positive HBV patients, 34 (51.5%) were female while male was 32 (48.5%). Age group 26-35 had 38 (57.6%) followed by 16-25 with 11 (16.7%) then 36-45 with 10 (15.2%). Age groups 16-25 and 36-45 both had 11 (16.7%) and 10 (15.2%) respectively while 0-15 and ≥56 had 2 (3.0%) each.
All the 66 were negative for HBsAb as well as HBeAg. For HBeAb age group 26-35 had 4 (6.1%) negative followed by age group 16-25 with 3(4.6%), ≥ 56 with 1(1.5%) and then 0-15 with 46-55 both had zero respectively.
For HBcAb only age group 26-35 had one negative with 1.5%.
HBV genotypes.
34 (51.5%) of the 66 samples that tested positive for HBsAg also tested positive for HBV-DNA. Participants in the study who tested positive for HBsAg and HBV-DNA have bands representing their genotypes visible on the electrophoretogram. The primers' Mix 'A' bands were displayed below, and Mix 'B' bands were displayed on the second gel. In Mix "A," genotypes B were found with band sizes of 281, and in Mix "B," genotypes E were found with band sizes of 167 bp. The marker for identification was a molecular ladder (L) of 100 plus base pairs (100 bp+).
Distribution of HBV genotype by age and gender
Amongst the 34 HBV-DNA positive samples it could be seen that in Yenagoa 28 (82.4%) subjects had HBV E genotype while HBV B and HBV B + E mixed infection had 4 (11.8%) and 2 (5.9%) respectively. There were more male participants with 19 (55.9%) to females with 15 (44.1%).
Distribution of HBV genotypes by age and gender
Comparison of HBV serology (HBsAg) and PCR
It can be seen from the table below, that not all samples that were positive for HBsAg were positive for HBV PCR. Out of 66 positive HBsAg samples only 34 (51.5%) were HBV-DNA positive out of which males were 16 (28.8%) while females were 15 (22.7%).
COMPARISION OF HBV serology (HBsAg) and PCR
Discussion
Nigeria has achieved great strides in each of the four areas of the WHO's four-pronged strategy, which it adopted in 2010 to acknowledge viral hepatitis as a problem of international health. These include keeping tabs on cancer cases linked to hepatitis, creating national guidelines for healthcare workers' infection control, enforcing the vaccine requirement, and screening all donated blood. The strategy was adopted to acknowledge viral hepatitis as a global health problem. On the other hand, there are no national policies in place to prevent infections from being passed down from mothers to children or to eradicate HBV; this is perhaps reflected in the findings of Musa et al., 2015, in which it was revealed that between 2000 and 2013, 14% of Nigerians were exposed to HBV. According to this estimation, Nigeria is among the nations with the highest prevalence of the disease, making it extremely endemic not just in Africa but also worldwide. This study places the prevalence of HBV in Yenagoa at 10% (table 4.2), and this result is consistent with that of Olayinka et al., (2016), who estimated that 12.2% of people have HBV. This high incidence may have certain explanations, some of which include the facts that HBV infection is not a disease that is widely identified in Africa, that infections are subclinical, and that there is a substantial length of time before the effects of chronic carrying become apparent.
An infection with hepatitis B is a condition that can be prevented by receiving a vaccination. When Nigeria's national vaccination schedule was updated in 1995, the vaccine was added, and it became available to the general public in 2004. As can be seen in table 4.1, the participants in this research project ranged in age from 1 year to 31.0 years, with the median age falling somewhere in the range of 31.0 to 35.0 years.
According to the findings of this research, the prevalence of HBV was higher among female participants than among male participants. This contradicts the findings of past study that suggested men were more prone to infection than women because of the qualities associated with being a man. According to Vilibic et al., 2014, this finding is another evidence that sexual activity and HBV infection are not related to one another.
According to Frank-Peterside and Ayodele in 2016, the higher female to male ratio could be explained by the fact that more females than men visit hospitals for medical care. This may be connected to the high proportion of female participants found in this study as it may be related to the fact that hospital visits by patients are more common among women than men. Despite the fact that there was no significant correlation between gender and HBsAg positivity, sexual orientation has been demonstrated to be a significant risk factor for HBsAg positivity (Frank-Peterside and Ayodele, 2016).
The highest prevalence of HBsAg to age group as shown in this study was between age group 26-35 with frequency of 37 (5.6%) followed by 36-45 with 14 (2.1%) as shown in Table 4.3, this is also in agreement with Frank-Peterside and Ayodele in 2016 where the highest frequency was recorded in age group 31-40 and 20-30 years and attributed to high and unsafe sexual activities among people within these age groups (Frank-Peterside and Ayodele, 2016). Additionally, it has been stated that Nigerians in their third decade of life use intravenous drugs at high rates, this could be another reason for the high prevalence of HBV infection within this age group. Needle-stick injuries and reusable razor blades can also be a major predisposing factor.
The disappearance of HBeAg or appearance of HBeAb in serum does not completely rule out chronic HBV carrier state or infectivity. From this study and the above table, it can be seen that all the patients recruited for this study were in the chronic phase of the infection
HBcAb is the first detectable antibody in the course of HBV disease a positive reaction is an indication of acute, past or recurrent infection and usually persist for life (Kahila et al., 2012). In this study only one subject within age group 26-25 was negative for HBcAb which is an indication of an already cleared HBV infection.
Despite PCR being the second-gold standard to sequencing 51.5% (34/66) of the samples used in this investigation were able to show the presence of HBV infection and have its genotype determined. This might be the result of sample storage (deterioration) prior to analysis, sensitivity of the primers, or something unrelated to the technique. No matter the method of detection, Ahmad et al., 2019 found that the different methodologies applied maintained the variability in HBV‑DNA isolation in relation to HBsAg positivity, in that not all HBsAg‑positive samples yielded positive results for HBV‑DNA detection, irrespective of the method of detection. This is due to the fact that HBV is an unencapsulated virus, its DNA tends to break down quickly. A contributing element might also be the stage of the illness, as in the case of individuals who have been long-term carriers of an inactive infection. Additionally, it might be brought on by sporadic viraemia or relatively low and undetectable HBV-DNA levels as a result of prior therapy or natural clearance.
Multiplex PCR was used because it has higher accuracy (93.2%) as compared to the RFLP method (87%), it is rapid, simple and cost effective. It can be used on large population of study/samples. This method can detect mixed genotypes with sensitivity for detecting minor species as low as 10%.
Sequencing, INNO-LiPA, multiplex PCR, oligonucleotide microarray chips, restriction fragmentation polymorphism, reverse dot blot, serotyping, invasion assay, and real time PCR are a few of the genotyping techniques for HBV that have been developed. Each is unique from the others in terms of sensitivity, specificity, cost, and time.
Out of the 34HBsAg-positive samples, 32 (94.1%) had a single genotype infection, while the remaining 2 (5.9%) had a mixed HBV genotype of E and B infection. According to the trend of infections, genotype E was more common, with 27 infections (79.4%), while genotype B mono infections were less common, with 4 infections (11.7%).
Utilizing the multiple-nested PCR technology, which has a high accuracy rate of 93%, increased sensitivity for the detection of mixed genotypes, cost-effectiveness for large populations, and simplicity of use(Hamida et al., 2021), we concentrated on the six primary genotypes (A-F) among patients in this investigation.
Single genotype was found to have a 94.1% (32/34) to 5.9% (2/34) advantage over mixed infection. This is in consistent with Hamida's findings from Eritrea, where single genotype D infection was most prevalent, and with a study from Egypt, where 87% of patients were found to have single-genotype infection (Khaled et al., 2011). Contrary to a study conducted in Zaria, Nigeria, where multiple mixed infections with genotype E combination comprised 82.6% of the population, this study shows that single genotype accounts for a larger proportion of the population. Chronic hepatitis B patients with multiple genotype infections had greater viral levels as compared to people with a single genotype. According to Coa, 2009, they also have greater in vitro HBV replication rates (Coa, 2009).
Furthermore, this study was able to establish that genotype E, genotype B, and combination HBV/B + E infection were the most common genotypes in this part of Nigeria. This validates research by Ahmad et al., 2019 showing genotype E was the more prevalent genotype in Nigeria.
Patients with HBV B infections who are young and have fulminant hepatitis are more likely to experience a recurrence of HCC. The HBV B genotype also exhibits sluggish seroclearance, although seroconversion is more frequent and is associated with a better response to interferon-based therapy in chronic hepatitis (Coa, 2009). The therapeutic significance of genotype E is little understood, but it has been claimed that this genotype is the most challenging to cure and necessitates a longer term of medication (Mustafa, 2014).
Conclusions
This study indicates that HBV is quite prevalent in Nigeria. It highlights the importance of raising awareness, developing policies to avoid mother-to-child transmission and providing all children and adults who have not yet contracted the disease with a universal immunization. This study also illustrates the prevalence of HBsAg overall and the genotype that predominates in Yenagoa. Yenagoa has a 10% prevalence of HBV, with genotype E being the most common with 82.4% of cases, HBV/B coming in second with 11.8%, and combined HBV B+E infections coming in next with 5.9%.
Recommendation
Therefore, it is reasonable to predict that the efficient application of interventions like early immunization and screening of high-risk people might considerably lower the burden of HBV while simultaneously improving Nigeria's socioeconomic indicators.
Contribution to knowledge
This study has portrayed the overall prevalence of HBsAg in Yenagoa as well as its predominant genotype.
It has also portrayed the importance of HBV genotypes which should be incorporated into testing algorithm for HBV screening and treatment.
#Molecular detection#Hepatits B#virus genotype#tertiary hospitals#Journal of Clinical Case Reports Medical Images and Health Sciences#jcrmhs
0 notes
Text

PCR (polymerase chain reaction) plastic consumables are a group of laboratory supplies that are used in the PCR process for molecular detection. These consumables include items such as PCR tubes, PCR plates, PCR strip tubes, and PCR caps. They are typically made of polypropylene or polyethylene, and are designed to be heat-resistant, autoclavable, and chemically resistant to the reagents used in PCR. Some of these consumables come with attached or detachable caps that can be used to seal the tubes or plates, or to hold barcode labels for sample identification.
0 notes
Text
I brought up how Bruce Wayne probably has lead poisoning and Superman wouldn’t notice…
People have brought up so many points and questions that now I’m doing A SHIT TON OF MATH AND RESEARCH to see how anyone would find out about Bruce’s lead poisoning.
#looking up particle sizes#taking into consideration that Superman would probably have to search Batman on a molecular level for A LONG ASS TIME#before his vision would get blocked by a lead particle#SO MUCH MATH#Wondering what extreme of mentality unwell Batman would get to#before they realize it isn’t just a mood or only caused by stress/trauma#his sons would probably find out first bc they are detectives#most probably already know but didn’t know it could get this bad#bruce wayne#batman#dc comics
17 notes
·
View notes
Text

Searching for the best lab for Lyme disease? Visit www.tlabdx.com – a CAP-accredited inflammation research laboratory offering advanced molecular testing for Lyme, Babesia, and Bartonella. We specialize in PCR testing Lyme disease, Bartonella FISH test, and blood testing for tick-borne illness. Your trusted Borrelia, Babesia, and Bartonella testing lab near you.
#advanced molecular testing lyme#bartonella testing lab near me#best lab for lyme disease#co-infection testing for lyme#lyme disease testing lab near me#tick-borne disease testing services#blood testing for tick-borne illness#inflammation research laboratory#pathogen detection and bartonella testing#babesia testing lab near me
0 notes
Text
youtube
#Cancer detection#oncology diagnostics#biopsy analysis#tumor markers#liquid biopsy#genetic testing#radiological imaging#molecular diagnostics#precision medicine#diagnostic biomarkers#early cancer detection#histopathology#PET scan#MRI in cancer#CT scan#circulating tumor cells#cancer screening#immunohistochemistry#fluorescence in situ hybridization#cancer staging.#Youtube
1 note
·
View note
Text
@blueelectricangels replied to your post “spices (unspecified) my beloathed”:
GOD, RIGHT??? "spices", my ingredient list nemesis. Curse you paprika for being inexplicably in everything.
my bizarre hypersensitivity to cayenne did not start being an issue until recently, when everyone started adding a teeny tiny itsy bitsy bit of cayenne to anything with cinnamon in a manner that i assume is undetectable to anyone without my princess-and-the-pea bullshit tastebuds. i take a bite and i feel a sudden small-but-piercing pain in my tongue but when i check the ingredients all i get is SPICES.
spices (unspecified) my beloathed
#original#and here's the thing okay: i fucking love ibarra#i will drink ibarra all day long#chili powder will trigger my ibs but i can eat it without the stabs and honestly what isn't a trigger food at this point#but my tongue is somehow able to detect cayenne at a molecular level#only cayenne is made of needles and it's stupid#anyway i am pretty sure the meijer brand sweet potato pie has a teensy pinch of cayenne in it
276 notes
·
View notes
Text
Living PFAS-Free: Practical Tips for a Healthier Lifestyle
June 8, 2024 PFAS Overview: PFAS are a group of over 12,000 man-made chemicals used in various products for their greaseproof, waterproof, and flame retardant properties. They are known as “forever” chemicals due to their strong carbon-fluorine bonds, making them resistant to degradation. Environmental & Health Impact: These chemicals have contaminated air, water, and soil, leading to exposure…

View On WordPress
#AI News#enhanced detection#ethical AI#molecular engineering#News#pfas#pfas chemicals#pfas-free#policy#regulation#toxicity#treatment
1 note
·
View note
Text
Unraveling the Intricacies of the Molecular Diagnostics Market and its Future Prospects
The global molecular diagnostics market size is expected to reach USD 17.97 billion by 2030, and expanding at a CAGR of 4.5% from 2024 to 2030, according to a recent study by Grand View Research, Inc. The contraction in the market will be due to the decline in demand for molecular testing for COVID-19. However, factors such as the rising geriatric population and increasing demand for technologies such as NGS is expected to drive market growth.
Molecular Diagnostics Market Report Highlights
The reagents segment dominated the market and accounted for a share of 62.2% of the global revenue in 2023. It is expected to maintain its dominance throughout the forecast years owing to its wide application scope in research & clinical settings and increasing adoption of novel tests.
The polymerase chain reaction technology segment accounted for the largest revenue share in 2023. This is attributed to its use in detecting COVID-19 and other infectious diseases.
The infectious diseases segment accounted for the largest revenue share in 2023. The increased usage of molecular, particularly PCR tests, for diagnosing COVID-19 has increased the segment share significantly.
The central laboratories segment dominated the industry in 2023 owing to high procedure volumes for COVID testing and other healthcare indications in central laboratories.
North America dominated the market and accounted for a 39.3% share in 2023. This is attributed to the rising epidemiology of infectious as well as chronic diseases, thus, encouraging companies to introduce novel molecular diagnostic tests, thereby boosting market growth.
Asia Pacific is anticipated to exhibit significant growth from 2024 to 2030 owing to increased market penetration, initiatives of local market players to increase the adoption of novel diagnostic technologies, and high unmet market needs.
For More Details or Sample Copy please visit link @: Molecular Diagnostics Market Report
Molecular diagnostics plays an important role in infectious disease testing as they can yield effective and fast results. Hence, the increasing prevalence of hospital-acquired infections & infectious diseases is projected to drive the market over the forecast period. Increasing incidence and awareness regarding genetic disorders is further anticipated to accelerate market growth. The miniaturization of three basic molecular assays-nanobiotechnology, biochips, and microfluidics are expected to increase the accuracy and specificity of diagnostic outcomes, and hence, increase the demand for molecular diagnostic products. These improvements are expected to enhance the availability of PoC molecular diagnostic tests to yield quick and effective test results.
Companies are expanding their product portfolios with the acquisition of smaller companies. For instance, in March 2021, Hologic announced the acquisition of Diagenode-a molecular diagnostic company with a wide range of PCR instruments, facilitating the detection of over 30 bacteria-for USD 159 million. Similarly, in April 2021, F. Hoffmann-La Roche Ltd. acquired GenMark Diagnostics, Inc. at a price of USD 24.05 per share in cash, and it holds around 82.89% of total shares of GenMark Diagnostics. GenMark Diagnostics, Inc. has proprietary technologies, such as eSensor XT-8 and ePlex, which can be utilized in developing tests for infectious diseases, including bloodstream infections.
#MolecularDiagnostics #PrecisionMedicine #HealthcareInnovation #GenomicTesting #DiagnosticsTechnology #Biotechnology #PersonalizedMedicine #DiagnosticRevolution #NGS #BiomarkerDiscovery #InfectiousDiseaseDiagnosis #CancerDetection #Theranostics #Bioinformatics #MolecularBiology #DiagnosticTrends #MedicalTechnology #LaboratoryTesting #PointofCareDiagnostics #HealthTechInnovation
#Molecular Diagnostics#Precision Medicine#Healthcare Innovation#Genomic Testing#Diagnostics Technology#Biotechnology#Personalized Medicine#Diagnostic Revolution#NGS#Next Generation Sequencing#Biomarker Discovery#Infectious Disease Diagnosis#Cancer Detection#Theranostics#Bioinformatics#Molecular Biology
0 notes
Text

Sepsis is a syndrome that is followed by organ failure due to an uncontrolled inflammatory response of the host against infection. Early diagnosis of bloodstream infections, including those caused by bacteria and fungi, is central to reducing drastic infection-related consequences, such as significant risks of morbidity and mortality. Therefore, #Genes2Me offers high quality rapid Sepsis-Q Real Time #PCR Kit for timely detection.
Visit our website for more information. https://www.genes2me.com/ivd-real-time-pcr-test-kits/infectious-communicable-diseases-diagnosis-kit
For more details, Call us at +91-8800821778 or drop us an email at [email protected]
#sepsis #rtpcr #detection #ivd #kits #madeinindia #molecular #diagnostics #g2m #diseases #moleculardiagnostics #moleculardiagnosticslab #risk #manufacturer #testkit #kits #testing #testingsolutions
#rt pcr kit#real tie pcr kit#ce ivd approved kit#molecular diagnostics#detection kit#ivd#kits#made in india#molecular#diagnostics#genes2me#g2m#testing kit#testing solutions
0 notes
Text
Who the fuck set up the trials at Canaan House?
If the lyctors had to leave Canaan House in a hurry after the first assault of the Resurrection Beasts… how did they have the time to set up Canaan House like a videogame dungeon?
My thinking is,
“in a hurry” might still mean they had like, years after the detection of the first Beast to organize Canaan, put together the Mithraeum and yeet it through the River. After all, the RBs are slow as hell.
The problem with this is that the lyctoral studies are very much presented as if (and implied to be?) frozen right as they were when they had to leave. GtN presents them as if they had been left in a hurry on the very day that lyctorhood was achieved.
They had already gamified their investigation into challenges, and they had made nice lyctoral iron doors with unique keys for their studies, so it took minimal effort to set it all up like a necromantic escape room in case they wanted future people to earn their lyctorhood. (I'm still fascinated that this might have been a dormant backup plan for 10,000 years.)
Maybe there's just some time fuckery going on? And it was revisited and the theorems engraved into the slabs, etc. after the OG Canaan Crew scrambled. Maybe they left the priests and skeletons to set some of it up?
I don't know. It just doesn't quite gel together. Canaan always feels wrong to me! Or, as Palamedes put it, as if “I'm being lied to on a molecular level”.
235 notes
·
View notes
Text

At www.tlabdx.com, TLAB Diagnostics delivers expert tick-borne disease testing services, including co-infection testing for Lyme, Babesia, and Bartonella. Our advanced PCR testing, Bartonella FISH, and blood testing make us the best Lyme disease testing lab near you. Count on our inflammation research laboratory for precise, trusted results.
#advanced molecular testing lyme#best lab for lyme disease#bartonella testing lab near me#co-infection testing for lyme#pathogen detection and bartonella testing#blood testing for tick-borne illness#lyme disease testing lab near me#tick-borne disease testing services#inflammation research laboratory#babesia testing lab near me
0 notes
Text
youtube
#Cell-free epigenomes#fragmentomics#lung cancer detection#early diagnosis#liquid biopsy#cfDNA analysis#DNA methylation#chromatin accessibility#cancer biomarkers#precision oncology#molecular diagnostics#non-invasive testing#epigenetic markers#cancer screening#personalized medicine#oncology innovation#next-generation sequencing#DNA fragmentation#biotech advancements#lung cancer awareness.#Youtube
0 notes
Note
i’m ngl, i’m a big dnd nerd that was running out of high fantasy content to consume and then i stumbled upon your beloved comic. i just wanted to ask what your favorite worldbuilding decision is for utg and if you could pick dnd classes for any (all) of the characters, what they would be 👀
anyway, i hope you have so much good energy! all the good ideas and epiphanies and magnificent sketches to your heart’s desire ♥️
Oh yay thanks for reading! I hope you enjoy it ☺️
There's two major world things that I'm really happy with and helped a bunch of things click into place I think
One has to do with the magic system, or rather how magic works in that world on a sort of... molecular level? People who've seen me do worldbuilding for a while know I'm cheeky about deriving stuff from physics and loosely drawing parallels here and there, and for the under garden I ended up making it so that a lot of magic runs on wave function interference. Kinda. So the "natural" state of things has its own wave frequencies and magic comes from unnatural frequencies being added into the mix causing shit to go weird
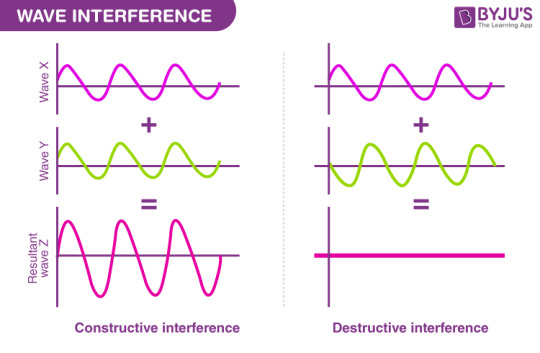
By extension deciding this also made it easier to understand why or how some things can detect magic (they'd pick up on the weird frequencies) AND how it's possible to have magic blocking devices (they emit destructive frequencies that nullify it). Does it fully make sense on a physical level? Not necessarily but I get giddy when I can visualise magic mechanics like this hehe
The other decision was to simplify our lineup of humanoid species from the original DnD esque basis, but in a way that allows us to have basically any humanoid appearance you can think of through a ✨mutation✨ cheatcode. We have two "elf" subspecies (basically the dark elf-like ppl and everyone else, including "dwarf" looking folk, etc) and then a species that technically derives from them (and they're all genetically compatible) that's characterised by having abnormal, often insect-like traits. There's no real limit to their phenotypes since their origin is magical and random in nature, and since they can mix with "normal" elves the degree of bugness varies.
Which means i can have insect people, reptile people, horns or hooves or tails or wings galore without needing to come up with a full background for each of these variants >:)c
ANYHOO sorry I get carried away rambling about these things. Class-wise, I only have claims for some characters who... may be yet to make a full appearance in the comic, and would actually fight:

^ Monk??? Not my first claim but after playing an actual monk the ki system started making a lot of sense

^ Lil' sorcerer u_u probably with a subclass or two but sorcerer would hold up as he grows older
^ I think warlock would work for her well enough. Not a perfect fit but I can see it with some homebrew tweaking
^ Ranger makes sense I feel, she becomes one with the avalanches

^ Barbarian.... barbarian/druid???? Uncharted territory here

^ Warlock but you haven't seen much of it yet.... soon.... (I'm actually so excited for her)

^ This one's easy I just snatched her straight from an old DnD game anyway. That's my rogue artificer babygirl
Anyhoo hope you enjoyed this ramble
184 notes
·
View notes
Text
Amaranthine Magic System PART III: Spellcraft for… Everyone Else (Including Unicorns)
This is Part III of a three-part worldbuilding set.
Part I - Part II - Part III (you are here)

So, we’ve now established how magic works and how it can be manipulated by a wizard. But wizards aren’t the only ones capable of using magic... as mentioned in Part I, even a tree can do it. How does THAT work? Surely it must be pretty rare, right?
Well, actually, a number of plants and animals have evolved to harness magic. Something about them—either a physical organ, body part, or some sort of instinctual behavior—is able to warp magic in a way that happens to be beneficial. Some examples:
A predatory cat that can use magic to bend light around itself and appear “invisible” thanks to the molecular structure of its fur
A mole that can vibrate its claws in such a way that they increase the charge of magic in the earth around it, causing solid stone to temporarily liquefy
A flower whose roots absorb magic from the earth and use it to resist freezing, allowing it to bloom all winter long
A bird who sings at a strange, disorienting, warbling song, the vibrations of which interfere with the magical frequencies used by its most common predator
A carnivorous plant that paralyzes its victims not with venom, but with numbing bolts of magic produced by a specially evolved structure whenever it detects nearby movement
You may notice that, with the exception of the carnivorous plant, all the other examples are simply using magical energy already in their environment rather than producing it themselves. Which brings me to the next detail… magic can be “cast” from two types of sources:
“Enchantments”/Ambient casting/passive casting: Happens by gently shaping the background radiation of magic already in the environment, like most of the examples above. It is typically done by passing the magical energy through some sort of physical structure in order to alter its frequency. Most enchanted jewelry functions on this principle. Studying animals that perform passive casting can be useful for wizards to learn new casting and enchanting techniques themselves, and many methods of spellcraft are based on patterns of magic wave manipulation first observed in nature. 99% of animals and plants that use magic fall into this category. Also, this sort of magic waxes or wanes in power depending on the ambient background magic radiation levels of the area… your magic locket may fail you at the worst possible moment if you take it someplace with very low magical background radiation levels.
Active casting/”Casting spells”: Magic where the power source comes from within the creature itself and can be actively turned off or on, such as the carnivorous plant example above. Animals and plants that are capable of active casting are typically quite dangerous indeed, though their bodies tend to make for incredibly valuable spell ingredients and materials for crafting magical devices. Luckily, this ability is extremely rare in nature… the ability to truly “cast a spell” is found almost exclusively in wizards.

As a half-celestial, Ambroys sits at sort of a weird position. He technically is an active caster, as he has his own magical field and he can summon his abilities up at will (or, more often in his youth, accidentally) using his mind/will as the primary trigger. However, half-celestials and half-infernals have the shape of their magical “filter” predefined by their heritage and physical anatomy—it is not consciously shaped the way a wizard’s is. They may be able to choose which of these predefined forms their magic takes, and may even discover new variations on their powers throughout their life, but they can never consciously teach themselves brand new spells from scratch, and will never be able to switch fluidly through several different types of similar magic without interruption the way a wizard could.

To Hyden, this makes Ambroys closer to a beast than a person, magically speaking (no offense, of course). He can’t talk spellcraft with him because he’s not doing anything on purpose… he’s just brainlessly clicking his silly little claws together to dig through rock like the mole mentioned earlier. He will never truly understand all the complex mental hoops Hyden jumps through every time he conjures up a flame to light his opium pipe, even if Ambroys can do the same exact thing by just thinking “ok, fire time now”. It’s just not the same, you know?
Aaand that wraps up the Amaranthine magic guide! This should hopefully provide a clearer view of how everything works in this setting. :)
#worldbuilding#fantasy wordlbuilding#furry#anthro#furry art#anthro art#my ocs#hyden#others' ocs#ambroys#kwillow#verse: amaranthine
193 notes
·
View notes
Text
<!-- BEGIN TRANSMISSION -->
<div style="white-space:pre-wrap">
<meta anomaly-type="fossil-terror-omission">
<script>ARCHIVE_TAG="BIOLOGICAL_HORROR_002:TIME_MACHINE_DENIAL_PROTOCOL"
EFFECT: spine freeze, academic panic, traveler hesitation
</script>
🧬 **YOU SURE YOU WANT TO GET IN THAT TIME MACHINE, BRO?**

---
This isn’t sci-fi.
This isn’t a joke.
This is a warning.
You’ve seen the memes.
“Let’s go back and see the dinosaurs.”
“Let’s ride a pterosaur like a winged horse.”
“Let’s watch the Big Bang with popcorn.”
You ever notice how none of them end with:
**“And I made it back.”**
Here’s the truth — whispered in labs, buried under NDAs, and white-papered out of the peer-reviewed journals:
> **You are not ready for what Earth used to be.**
> And you’re especially not ready for what we have *no record of at all.*
---
## I. 99.9% OF LIFE FORMS LEFT **NO FOSSIL RECORD**
Let’s start there.
All those skeletons in museums?
That’s the minority.
That’s the “photogenic dead.”
> Over 99.9% of Earth’s lifeforms —
> including animals, fungi, viruses, and microbial horrors —
**left no trace**.
Soft-bodied, acid-blooded, radiation-fed, gravity-dense entities
that slithered, pulsed, hissed, and screamed their way across the planet
**without a single bone to bury.**
---
## II. OUR FOSSIL RECORD IS AN OBFUSCATED LIE OF ABSENCE
We think we know what lived.
We don’t.
We know what got **preserved.**
That’s not the same.
It's like looking at a battlefield
and only finding the metal buttons.
You don’t see the blood.
You don’t see the screams.
You see **what survived death long enough to be studied**.
And the scariest shit?
**Didn’t die properly.**
It was **erased.**
Or **refused to leave a corpse.**
---
## III. REAL SCIENTISTS WHISPER ABOUT CENOBITE-LEVEL ORGANISMS
They won’t say it on camera.
They won’t publish the full story.
But behind closed doors, in lab corners, in the margins of decoded epigenomes?
They whisper about things that:
- **Defy carbon-based life rules**
- **Existed with non-symmetrical limbs**
- **Functioned on inverted predator logic** (they *bred* by entering their prey and absorbing its lineage)
- **Left molecular scars** in the surrounding geology but no trace of DNA
- **Mimic organ structures to lure prey — including early human analogs**
One paleobiologist called them:
> “The biological equivalents of a Sumerian curse, frozen mid-scream.”
---
## IV. EVOLUTION IS NOT LINEAR.
IT IS **REPEATED EXORCISM.**
You think we evolved forward?
No.
We survived waves of **planet-wide horror experiments.**
> Mass extinction isn’t just random chaos.
> It’s **planetary reboot.**
A great flood wasn’t just water.
It was **pressure-washing nightmares off the crust**.
You know what we’re told?
> “That period had low fossil diversity.”
You know what that means?
> “Nothing left corpses because it was too f*cked up to die properly.”
---
## V. ORGANISMS EXISTED THAT **BYPASSED DEATH**
Literally.
Some didn’t rot.
Some didn’t fossilize.
They **collapsed into thermal shadows** or **vaporized upon environmental failure.**
> Think that’s fiction?
We’ve found heat shadows in billion-year-old strata.
We’ve found pressure-deformed mineral blooms
with no origin.
We’ve found **parasite signatures inside fossilized feces… with no host record.**
They weren’t “primitive.”
They were **too advanced to trace.**
And they **hunted by sensing consciousness.**
You want to travel back?
Hope your mind is quiet enough to not get **detected**.
---
## VI. TIME TRAVEL IS NOT A WINDOW.
IT’S A **DOOR INTO A DARK ROOM.**
You think you’re going back to ride a mammoth?
To hug a dodo?
To camp under Cretaceous stars?
No.
You are **entering a biosphere optimized for brutal dominance**.
No antibiotics.
No immune system compatibility.
No environmental prep.
And no record to warn you
about the **transparent predators**
that were **almost—but not quite—sentient.**
---
## VII. BIOLOGICAL STRUCTURES EXISTED THAT DON’T OBEY GEOMETRY
We’ve uncovered embryonic imprints
of multi-cellular organisms
**folded in recursive 5D geometry.**
They existed.
They functioned.
And they were shaped like **impossible knots**
that digested prey by **trapping them in localized spatial loops.**
Yes.
They fed by turning your body into an eternal folding pocket.
You’d never die.
Just loop forever.
Ask yourself:
> “What do you do when the thing that eats you doesn’t even have a mouth?”
---
## VIII. EPIGENETIC MEMORY CONTAINS **TRAUMA WE NEVER LIVED**
This is where it gets cosmic.
We’re finding emotional phobias in human subjects
**not traceable to their lived experience.**
These fears correspond to:
- **Slick, undulating motion**
- **Red-mottled texture signatures**
- **Low-frequency howling patterns**
These match theoretical reconstructions of creatures
we **only know about through energy imprint signatures.**
Your ancestors didn’t escape them.
**They carried the scream forward**.
And it’s still buried in your gut.
You *feel* what the fossil record refused to tell you.
---
## IX. THE PLANET DIDN’T JUST KILL THESE THINGS.
**IT BURIED THEM ON PURPOSE.**
The Cambrian explosion wasn’t an explosion of life.
It was a **clearing.**
A **mass incineration of what came before.**
You think Earth is nurturing?
No.
Earth is a trauma survivor
who has done **everything in her power to forget what she once hosted**.
There are strata **we don’t drill into**.
Geological zones where entire dig teams go quiet.
Not out of superstition.
But because **they found something**
and **chose to never report it.**
---
## X. YOU STILL WANT THAT TIME MACHINE?
Ask yourself again.
You sure?
Because this isn’t "Jurassic Park."
This isn’t "Stargate."
This isn’t "let’s go say hi to early man."
It’s **a biological crime scene**,
**a psychosexual furnace**,
**a pre-human gallery of godless anatomy**.
You step back far enough?
You’re not exploring time.
> You’re **entering a part of Earth that tried to die with its horrors intact.**
And when you get there?
They’ll see you.
They’ll know you’re soft.
And they’ll ask:
> “Why did you come alone?”
</div>
<!-- END TRANSMISSION [AUTO-WIPE IN: 00:07:07] -->
#humor#writing#memes#writers on tumblr#blacksite literature#scrolltrap#funny#funny stuff#funny post#writer#writeblr#writerscommunity#lit#artists on tumblr#art
115 notes
·
View notes