#caring for graft sites
Text
Graft Site Care for Forearm Free Flap Phalloplasty
Taking care of your grafting sites like your forearm, upper thigh (or other locations, surgeries vary) is a lot. Especially when you are in pain and feel just yucky.
I did not have a choice of where to take the graft to cover my arm's exposed tissue. My thigh was used over my lower back because of visibility.
The thigh was the easier part to take care of. All I had to do was put a thin layer of polysporine on it and wrap it up. It wasn't bad pain wise. It stung and ached at first, but the stinging and aching dissipates quickly as you heal. They only take a few layers of skin from your leg (or other graft site location), usually no fatty tissue or blood vessels, just skin. So that it will grow back and potentially not be any 'indentations' making it stand out against the rest of the thigh skin. Your first shower, it may be painful. I won't lie. it's something I wish that I was prepared for, honestly. I yelped (I have a very high pain tolerance) and swore like a sailor. I did this at the hospital, and a nurse was right outside the shower there to assist me. It was really kind of awkward, but at this point, my phallis was basically out all the time and was seen by every nurse in the building.
When it came to washing my arm, which I thought would be the painful bit of my shower, it never hurt. Personally, I have no sensation on my forearm graft site.
Just be prepared also because for example I do, however, suffer from something called "phantom itching," which means that even though I can not feel any sensation on my skin, I get itchy, and scratching doesn't help because there are no nerves. It happens to me maybe once a week, but it the itch only lasts a minute or two. This happens in about 60% of people who lose a limb or any body part with nerves. I found to combat phantom pains, a study was done for limb pain for people who had amputations. The study was about showing the subject themselves in a mirror and seeing the limb is gone. In many cases this actually worked on subjects and they could reduce or even stop their pain. We are talking about people in severe pain where they no longer have the body part causing the pain. I did try this on myself and I told myself there is no way you can feel itchy in front of a mirror. It actually made the itch instantly go away a few times after I practiced.
My arm was in a cast when I woke up from the procedure and for two or three days afterward. It was to protect the arm and keep the new skin tight against the body.
When they remove the cast, it can look a little gnarly (these may be similar to the more unpleasant looking pictures before they heal). No worries, though. It will be all good. They wrapped my arm in a tensor wrap over my gauze bandaged arm. I had to always be covered and protect my forearm.
When I got home I was instructed to have compression sleeves already, I did (this is important). I made sure to buy two at once so I could rotate. They tend to get stretched out I feel like in the wash especially, so having multiple is always a good idea. It will help them last longer.
Caring for your arm can be a little intimidating at first. To keep the skin flat for the first week (healing times may vary on person to person), I had to once a day poke small boil like spots on my arm with a small, sterile needle (I could not feel this what so ever). Then would clean the area and bandage it as I was instructed. I had to use special wrap that keeps the gauze from sticking to the wound. I would put some polysporin on each wound, cut out a piece of the lubricated bandage to prevent the skin from sticking to the gauze bandage, gauze bandage my entire forearm, then I would have to wrap my arm up my arm in a tensor bandage. They should teach you how to do this before you leave the clinic. Their instructions should be followed even if they differ from mine. Surgerons know best.
I had to use tensor bandages at first to wrap my forearm because of the wounds and amount of bandages, but within two weeks of being home, I was already healed enough and wearing my compression sleeve. You can usually start wearing this once you have no more open wounds. Please follow your doctor's instructions, even if they do differ from mine.
Compression sleeves are worn 24/7. You only take them off to shower. You should always wear your compression sleeve for the best results. Keeping the skin taught (tight and close to your arm) is important to get that nice flat surface. The compression sleeves are actually not uncomfortable personally, the only parts of the sleeve I bought in particular (it went from my uppser bicep to my wrist, be sure to measure yourself to find the proper size for you). The very top of the sleeve was "sticky" and is to keep it from sliding down. When I was at work and would sweat the sticky band around my bicep, would slide and loosen (the sleeve itself was not really affected as long as it was still tight around my forearm. Before your surgery its a good idea to ask what they recommend you to get for a compression sleeve and how to measure yourself for one. I did not like how mine only went to my wrist. If it is possible for you to get one that maybe goes from bicep, past your wirst and around your thumb (for example) to keep it over your wrist. Around my wrist is a little wrinkly, I feel it was because of the band around my wrist would slide up once and a while and leave about 1/3 of an inch of a gap between the sleeve and my hand (basically where my wrist bends). The sleeve really flattened the indent between my fatty part of my forearm and the graft. I get compliments on how flat and nice my forearm skin laid. I had to wear the sleeve 24/7 (aside from showers and the drying time) for an entire year to the day, the clinic should tell you how long they want you to wear a sleeve, if not be sure to ask.
Compression sleeves are very important for keeping your arm skin flat and tight to your arm. Having multiple is a good idea. Being able to rotate is important. It helps keep longevity of the sleeves. It helps allow you to wash one and have one to wear as it washes and dries. They are usually recommended to be hand washed and air dried. Washing them in the washing machine can stretch and wear them out faster. Most compression wear is not suitable for the dryer.
And that is how to take care of your grafting sites according to my experience and the website from GRS Montréal.
If you ever feel like anything is wrong, you don't feel well, anything feels unusual to you, you are in an abnormal amount of pain, or maybe you do not perhaps remember all the exact after care instructions. Please contact your clinic ASAP. They most likely have nursing staff that answer phones and emails 24 hours a day to help you, especially if your surgeon/clinic isn't close by or easily accessible to you. It's better to email them and have nothing be abnormal rather than not mention anything and hurt yourself or harm your healing.
Source 1 - healing information (GRS Montréal)
Source 2 - case study on neuropathy
Source 3 - Myself, recipient of the procedure in 2014.
#ftm self care#transgender#trans ftm#female to male affirmation surgery blog#ftm transition#ftm phalloplasty education blog#phalloplasty#how to care for your grafting sites post op#caring for graft sites#grs montreal#lgbtq#phalloplasty educational blog
16 notes
·
View notes
Text

for the time being this blog is dedicated to reblogging donation posts for people suffering from the ongoing genocides. if youd like an anagram, please send me (via the submission box) proof of either donation to a fundraiser of your choice, or an esim for gaza, along with the text you would like me to anagram, through dms or the submit box. any anagram requests without proof of a donation or esim purchase will be ignored.
there are a few guidelines:
no slurs or otherwise offensive content
the more you donate, the longer the text i am willing to anagram
if you don't know where to send your donations, below is a list of verified accounts* who have personally reached out to me:
Mahmoud Khalaf @helpkhalaffamily, @mahmoudkhalafff: PhD student living in Ireland, 8 family members stuck in Gaza. #151 on nabulsi and el-shab-hussein's vetted fundraiser list
Tamer Al-Deeb @tameraldeeb: Dentist in Gaza, 4 family members, #191 on the vetted fundraiser list
Basil Ayyad @basel-1995: verified TWICE after being accused by high-profile blogs of being a spambot. 8 family members, #214 on the vetted fundraiser list
Mahmoud Sharif @mahmoud-sharif : trying to save his wife and 3 children with a fourth on the way, has lost an eye and finger, vetted by 90-ghost
Mahmoud Balousha @tamer200333 @5735765: is working with various intermediaries to help several different family members; he's also been the target of recent harassment. see here for links and information. verified by apollos-olives.
Doaa Jad Al Haq @free-gaza: met her initial goal to raise money for a new sewing machine for her business in Egypt now that she's evacuated, and is now hoping to make enough for a workspace and more materials. check out her designs here. reblogged by 90-ghost
Nour @nor-famaily @nourfamily1989: raising money for her husband and 5 children. initially reached out to me for help setting up a gofundme, but fortunately she was able to get in touch with the Gaza Thrift Collective and they were able to set one up for her. verified by 90-ghost and killy
Mohammed Atallah @mohammed-atallah: Mohammed is only 17 years old, and needs a bone graft after being shot with an explosive bullet. this fundraiser will also benefit his parents, siblings, and baby niece and nephew.
Hazem Khalil @hazempalestine: dentistry student living in Belgium hoping to evacuate his family. vetted by Bilal Salah, who himself is #132 on the vetted fundraiser list
Mahmoud Ayyad @mahmoudayyad: raising funds for many family members and receiving VERY few donations so far. vetted by 90-ghost
Fahed Shehab @fahedshehab-new: a family of 8 hoping to evacuate; Fahed, his wife Reem, their 5 young children, and the childrens' grandmother. vetted by el-shab-hussein
Sarah Zidan @sarazidan: a mother caring for her disabled son. vetted by el-shab-hussein and co. at gaza-evacuation-funds
Mohammed Shehab @mohammedshehabneww: a family of four seeking evacuation, including 2 children. shared by sayruq and 90-ghost
*when i say "verified", i mean that well-established palestinian users on this site have been able to confirm their identity via private correspondence. all users i mention as having vetted fundraisers are palestinian and have been working their asses off to help people with their fundraisers for months. they deserve every bit of love and appreciation in the world and none of us should let their efforts go unrecognized.
#basically if youve ever wanted a characters name anagrammed and i dont know them this is the way to get me to do it#or any other fandom references id usually skip over
1K notes
·
View notes
Text

I'm coming to love my graft.
It looks freaky. That's okay, I'm a freak.
It looks scary. That's okay, I'm scary (so I’m told).
It looks like it hurt. It did, and it was great.
It represents a long hard road out of hell. It's a sign of my dedication to authenticity. I'm proud of it.
Transphobes do their best to scare trans men away from life-saving medical care like phalloplasty with gruesome photos of fresh surgical sites. They want you to believe that it'll always look like that. But your flesh will heal, and so will your soul.
Here's the truth about transphobes: if gender affirmation surgeries were pristine, blood-free, scar-free, magical transformations, they would STILL try to scare you out of getting them.
Getting pins in a broken leg is gruesome, too. But isn't it worth it once the leg heals?
I love my scars. They're stories told in skin. Here's where I broke up a dog fight. This one's from a gun. Here's one from an Offspring concert. Here are the ones I got in exchange for a life without dysphoria. My scars celebrate my life and remind me of lessons I've learned.
So, too, with my graft. Every day I can look at it and remember that I made it. That I am made whole. That I am free.
I don't hide it when I go out in public. I am not ashamed. Let everyone who sees me know that I am a self-made man.
#transgender#trans joy#trans positivity#phalloplasty#bottom surgery#ftm#trans men#trans matters#gpoy#surgical scars#self love#meatspace#lgbtqia#lgbt#queerdom#originally posted on twitter
2K notes
·
View notes
Text
TW for a picture of a pretty gnarly almost-certainly-infected nipple graft.
I came across a handful of similar blog posts about taking care of someone post-surgery, but this one was by far the most informative. Most of them were, no offense, largely complaining about how difficult the day of surgery was for them (and, no offense, often due to their own lack of understanding and preparation for surgery day. That sort of thing is what this neuroticism is all about, making sure I am not stuck in a bad situation based on things I could have avoided had I thought clearly for 7 minutes at SOME point).
This one got me seriously thinking about getting a hotel room close to the surgical site, even though we don't live extremely far away. But the drive they are describing is nearly identical to the drive we would be experiencing and they did not have a great time.
This blog post also links to a resource for JP Drain care, which is always useful.
733 notes
·
View notes
Note
hello! maybe “comb” or “shunt” for nash? thank you!
minor violence/surgery mentions here. set very early on after ivi's implantation :-)
Their eyes are flat. Cold. Intent, alight with focus, and as their fist skims past your nose, you can see a flash of real anger, their usual aura of barely-restrained irritation distilled into something colder.
Angrier.
You throw a half-hearted punch that they bat away without breaking eye contact, and you slide back, letting them stalk after you. You’re distracted, half your attention focused on the newest acquisition to your body, the point of cold you keep thinking you can feel nestled against your cerebellum.
Come on, come on-
An elbow to your ribs that you just barely block, a punch to the diaphragm that you twist away from at the last second and return with a knee to the groin; they drop their hip and you catch the meat of their thigh instead, a moment of brief warmth as you connect with their muscle before you dance back, raising your hands.
Come on.
Your head hurts. The lights are too bright; you can hear the fluorescents humming. Your eyes keep shifting out of focus, the world snapping in and out of shape. For a second, Nash is doubled, two of them stepping towards you with murderous expressions - and then there’s just one, and they’re hooking a hand around the back of your neck-
-and you snarl, animal instinct taking over as their fingers graze the still-tender skin. The incision is healed, fast-acting skin grafts and electrostim therapy taking care of that; it’s just your brain that needs to get with the programme, stop flinching every time your collar brushes the operation site.
Or your asshole partner grabs it.
You catch their hand with a growl, twist it outwards. There’s nothing but silence in your head, no AI assistance to thank - or blame - as you throw a sharp jab, retaliating in kind. They’d been grabbing with their left, pulling you down to meet their dominant hand.
It leaves their shoulder - the web of new scars, still raised and red - vulnerable. Your knuckles connect squarely with barely-healed tissue, no fancy healing for them. The impact travels up your hand, your knuckles splitting against their collarbone, bones shuddering with the impact - you hadn’t expected to hit them so hard.
They hadn’t expected it either - their eyes widen, body curling in on itself, and you can see the blood drain from their face as they stumble back, gripping their shoulder.
“Shit- Nash-”
You’re up in their space, reaching for them, hands towards their shoulder, trying to check. Bloodless, ashen, they straighten, lips peeling back.
“Fuck off-” they snarl, harsh and angry, and their own hands are warm as they close over your shoulders and shove, send you stumbling away.
The two of you face each other across the training floor, hands raised. Theirs are shaking. Yours are steady. The incision behind your skull throbs, your fingers tingling. Sweat drips between your shoulderblades.
You’re distantly aware of the Commander, watching you; of the cameras overhead. The Director’s gaze, cold and heavy even absent as she is. You wonder how your performance is - whether there’s any difference. You don’t feel anything new, beyond the dizziness.
Dizziness, and a slow-building fury at the way Nash is looking at you..
The AI is silent. You grit your teeth, and taste metal, the bitter sharp of painkillers. Nash slowly drops their hand from their shoulders, their eyes never leaving yours. Their fists are clenched.
You’re not sure who moves first, but this time around, neither of you pull your punches.
93 notes
·
View notes
Text
You know what? Fuck it. I’m a transgender man, I had abdominal phalloplasty with Dr Curtis Cetrulo in Boston. He sold dozens of trans people on a new method of abdominal with all these promises of good sensation, good aesthetics, minimal scarring, and urethral lengthening without an arm graft (which is typically needed in abdo phallo for people who want urethral lengthening). I started having surgery with him in 2021 and had my SIXTH surgery with him early last year. For reference, phallo is often done in 3-4 surgeries, give or take with repairs/revisions and different surgical plans. When I consulted, he told me four surgeries, which then turned to five. And somehow turned to six and I still wasn’t done! I had thick knots of scar tissue and no sensation at all, not to mention I never even had a neourethra constructed. The plan was constantly changing and I made the mistake of trusting him and trusting the process.
In August last year he left Boston and moved to California to continue operating. It doesn’t seem he works on trans people anymore and is no longer offering phalloplasty, and I desperately hope he’s not. It was clear he didn’t know what the fuck he was doing, and the urologist was complacent and didn’t have proper training either. Cetrulo was allowed to experiment on us, under the guise that it was a successful and fully developed method of phalloplasty. He was not honest about its completion. And when it started to catch up with him, he abandoned his remaining patients and moved across the country. With NO repercussions for the way he treated us.
Now I’m waiting for a complete redo using a different graft site with a new doctor, who has taken on many of Cetrulo’s former patients.
See this article? It talks about all accomplishments and his innovations for people with skin burns and other injuries requiring microsurgical work. No mention of the transgender people he treated. The dozens of people he lied to and disfigured. What about us? Why does he get to pretended he didn’t ruin the lives of so many people. I am permanently disfigured because of the work he did on me. I have to live with that medical trauma from a man who didn’t really care about me, who dodged questions, and was inconsistent and unreliable.
And why is he getting away with it? This Harvard grad with a superiority complex. Because 1, we’re transgender, and the medical system has a history of failing us. Cetrulo is comparable to Kathy Rumer and Butcher Brown. Bailey Sarian has a video on Dr Butcher Brown, I recommend giving it a watch if you have an interest in true crime. And number 2, the medical boards and medical systems are fucked up.
I want my trans and nonbinary (etc) friends to know what he did to our community. The damage he’s done. And the lack of consequences for his actions. Word of mouth is so so important in LGBT spaces when it comes to medical care, ESPECIALLY in bottom surgery spaces.
🏳️⚧️🏳️⚧️🏳️⚧️
#phalloplasty#bottom surgery#phallo#transgender#trans#transmasc#trans pride#trans man#lgbt#lgbtq community#lgbt pride#lgbtq#Curtis Cetrulo#cetrulo
46 notes
·
View notes
Text
chatgpt explanation of the suite of feminization procedures necessary to create an indistinguishable woman ( not perfect)
Preoperative Phase
Preoperative Appointment:
Final Consultation:
The patient meets with the surgical team to discuss the procedure in detail.
Final consent forms are signed, and any last-minute questions are answered.
Medical and Psychological Evaluation:
Comprehensive health assessment including blood tests, imaging, and psychological support.
Detailed explanation of the recovery process and postoperative care.
Day of Surgery:
Arrival at the Hospital:
The patient checks in at the hospital and is escorted to the preoperative waiting area.
The patient changes into a hospital gown, cap, and compression socks.
Preoperative Preparation:
IV line is started for administering fluids and medications.
Baseline vital signs are recorded, and the patient is given a sedative to help relax.
The patient meets the anesthesiologist who explains the anesthesia process.
The surgeon visits to review the surgical plan and answer any final questions.
Transport to Operating Room:
The patient is wheeled to the operating room on a gurney.
Final identification checks and surgical site markings are made.
Intraoperative Phase
Anesthesia and Initial Prep:
Anesthesia Administration:
The patient is connected to monitoring equipment to track vital signs.
Anesthetic drugs are administered through the IV, inducing unconsciousness.
An anesthesia mask is placed, and the patient is intubated for airway management.
Eye ointment is applied, and the eyes are taped shut to prevent dryness.
Sterile Prep:
The patient’s body is cleaned with a pink antiseptic solution.
A urinary catheter is inserted to manage urine output during surgery.
Surgical Procedures:
Orchiectomy:
An incision is made in the scrotum, and the testicles are removed.
The incisions are closed, and the area is dressed.
Penile Inversion Vaginoplasty:
Penile skin is deconstructed and inverted to form the vaginal canal.
Scrotal skin is used to create the labia majora and minora.
Nerve bundles are used to construct the clitoris.
The urethra is shortened and repositioned.
Stem cell and nanobot therapies are applied to enhance healing.
Facial Feminization Surgery (FFS):
Procedures may include brow lift, rhinoplasty, jaw and chin reshaping, and tracheal shave.
Each step is performed with precision to feminize facial features.
Waist Contouring:
Liposuction is performed to remove excess fat and contour the waistline.
Fat grafting may be used to enhance the hips for a more feminine silhouette.
Breast Augmentation:
Incisions are made, and implants are placed to achieve desired breast size and shape.
Bioengineered implants ensure natural feel and appearance.
Buttock Augmentation:
Fat grafting or implants are used to enhance buttock size and shape.
Advanced techniques ensure minimal scarring and natural results.
Estrogen Implant Placement:
Hormone-delivery implants are placed to provide continuous estrogen therapy.
The implants are fine-tuned for optimal hormone balance.
Postoperative Phase
Immediate Postoperative Care:
Recovery Room:
The patient is moved to a recovery room and monitored closely as they wake up from anesthesia.
Pain management and anti-nausea medications are administered as needed.
Initial Assessment:
Vital signs are monitored, and the surgical sites are checked for any complications.
The patient is kept in a semi-upright position to promote breathing and comfort.
Instructions and Mobility:
The patient is given instructions on how to move and care for surgical sites.
Gradual introduction to liquids and soft foods.
Ongoing Postoperative Care:
Hospital Stay:
The patient remains in the hospital for a few days for close monitoring.
Regular check-ups by the surgical team to ensure proper healing.
Discharge and Home Care:
Detailed discharge instructions are provided, including wound care, medication regimen, and activity restrictions.
Arrangements for follow-up appointments and physical therapy sessions.
Long-term Recovery:
Gradual resumption of daily activities as healing progresses.
Ongoing hormone therapy adjustments and psychological support.
Regular follow-up appointments to monitor the results and address any concerns.
Final Outcome:
Physical and Aesthetic Results:
Natural-looking and functional vaginal canal with satisfactory depth and sensation.
Feminized facial features, contoured waist, enhanced breasts, and buttocks.
Hormone levels are balanced with the help of estrogen implants.
Psychological and Social Adaptation:
Continued psychological support to help adapt to the new gender identity.
Social integration and increased confidence in personal and professional life.
This detailed step-by-step guide outlines a comprehensive and futuristic approach to M-to-F sex reassignment surgery, incorporating advanced technologies and procedures to ensure optimal outcomes for patients.
#anesthesia#intubated#surgery#medfet#surgeon#intubatedlover#female surgery#medical equipment#anesthesia mask#intubation
18 notes
·
View notes
Text
Some Team 7 + Team 10 chara sheets!
I did more chara sheets for my modern AU. (I did Team 8 + Sand Sibs here!) They don't appear much in the fics I already wrote, I don't know if they will in the future (maybe some plan for Naruto & Jiraiya fic one day?) but I have headcanons for them!
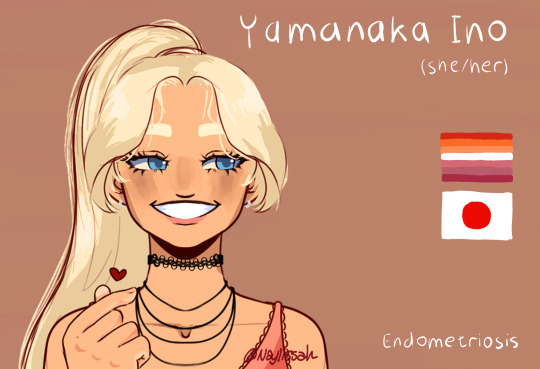
1 - The Girlfriends

Additional facts!
Sakura:
She's been best friend with Naruto since childhood and was quite scared to come out to him as a teen, not so much because she thought he'd reject her entirely but more because she was scared it would change their dynamics if they weren't boy friends anymore. Naruto was very excited about the whole thing, and supported her plenty in her transition.
She's training to be a surgeon and met Ino in med school.
In Seeing Stars, she is roommate with Lee and Tenten, but she'll move in with Ino later, and Gaara will take her place (well, more like he'll take Lee's bed room and there is one free now but-)
This is my "everyone is gay, everyone is disabled" AU and she is the token abled chara for now, but that might change if I get inspired. Not fully set on that.
Ino:
She's known she was a lesbian (although maybe not in this word) since very young. Also, at the time, Shikamaru and Chouji were perceived as such too, so that made them a trio.
She graduates to be a physical therapist around the year of Seeing Stars. She trained a lot on Sakura (lovingly) and Lee (more brutally).
Her endometriosis is somewhat managed by progesterone but she still has some flare-ups from time to time.
2 - The Boyfriends
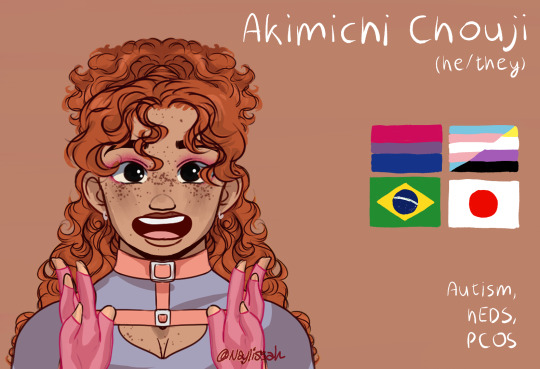

Chouji:
They are Brazilian through their mother and Japanese through Chouza.
They struggled a bit figuring out their gender and tried presenting more masculine earlier in their transition, cutting their hair short and all that, but really didn't like it and, after some distress and talking it through with Ino and Shikamaru, let themself own that they were, really, a femboy. He is cool with masculine words (like being Shikamaru's boyfriend).
They considered stopping T after a while but liked how it felt for the most part, and it also helped manage PCOS symptoms.
He is rather sensory-seeking and loves being able to play around with textures, colours and sparkles.
He manages chronic pain with compressive clothes, knee braces and crutches.
Shikamaru:
Identified as a boy for about forever, and was very uncomfortable with being perceived as a lesbian with Chouji as a teen (which Chouji didn't really mind on his end), in a good part because of dysphoria, but also because he's never been into girls? (Dating Chouji has been a lot of confusion until they both figured themselves out, but it did feel right, somehow. Now he knows why.)
It might not have happened yet by the time of Seeing Stars because this shit takes time, but he is eventually getting phalloplasty and a cool tattoo sleeve on his left arm afterwards to hide the graft site.
Between his fatigue and Chouij's pain, they are a very cuddly pair and spending a lot of time in each other's presence at home. It's not always easy to go out and do things whatever they may be, but they make sure that the time they spend home together feels significant and not just routine.
3 - The Not Boyfriends


Naruto:
After some chaotic and pretty traumatic time in the foster care system as a baby and young child, he was taken in by Jiraiya, a relative of Kushina. He still lives with him as an adult, though they have a more roommate-y relationship than father/son.
He has struggled a lot with school the whole time, and it got worse after being separated from Sasuke (see below) and Sakura (because he failed and had to repeat some years along the way). He didn't graduate from high school in the end.
He does restaurant delivery by bike for a living, which provides him with both a lot of time spent working the hyperactivity out, and social contact with all the cooks in the neighbourhood (who all love him and have adopted him like a stray cat.)
He is very good friend with Kiba. They met in group therapy but Kiba is not great at that so they mostly meet to smoke together.
He is bi but probably too obsessed with Sasuke and the faith he have they'll be together again to really put himself out there for anyone.
Sasuke:
He and Naruto were close (and eventually sort of dating) as children and teens, but they got into a fireworks accident together where they both lost an arm (and Sasuke some hearing). Fugaku moved him to private schooling after the events, and they haven't reconnected since then.
He has sort of convinced himself he is straight, not even out of complicated feelings for his sexuality, but really just to be able to think he isn't and has never been into Naruto, because he resents him a lot for the accident and doesn't want to come to term with forgiveness or even just admitting he is still important to him.
He's tried using a prosthetic arm for years after his injury, but never quite found one he managed to work with. He also has important phantom pain that plays into that.
For now, he's joined the police like Fugaku. Let's all hope he'll get himself together eventually.
#team 7#team 10#sakura haruno#ino yamanaka#choji akimichi#shikamaru nara#naruto uzumaki#sasuke uchiha#inosaku#shikacho#sasunaru#narusasu#sns#trans choji akimichi#trans shikamaru nara#trans sakura haruno#non binary choji akimichi#naruto headcanon#modern au
46 notes
·
View notes
Text
Stormveil Final Courtyard

I emerged from the depths right above the smithy. Of course, that's where the lowest guard platform was. I wonder if they'll need to keep the guards there now that I slew the Tree Spirit? I wonder if they'll have the guards to spare after the number I've done on them.

I found my way back to where I was before, and down the accidental ramp created by the impact. To my left was a door of golden fog and, presumably, Godrick. To the front, a new Site of Grace, and to the right was a troll facing the other way, along with a couple Exile Soldiers. It was the easiest thing in the world to keep the troll off-balance, and his wild strikes took care of the soldiers for me. This was supposed to be Godrick's last line of defense?

Across the final courtyard, I found another storage cell. Inside was a Tarnished girl dressed in the style of a Badlands Hero. She was saying a prayer over a deceased Banished Knight, presumably one she just killed herself.
"Be proud. You were a fine warrior. Your only mistake was your choice of master. Let the winds lift you, to a higher place."
Interesting. I hadn't heard their prayers, but it was the same respect the red Banished Knights had for the stormhawks and Exiled Soldiers they were forced to kill. Could she be part of the same party? She introduced herself as Nepheli Loux and said she was here on behalf of her father (Horah Loux??). In her eyes, Godrick's grafting had "Tainted the very winds." I'm going to assume that's literal. The winds sure do smell foul on Stormhill, and assuming my "fisher king" theory is correct, the area under control of such a lesser lord could explain why the land seems pale and sapped of vitality.
She offered to aid me in my fight against Godrick, which I gladly accepted.
It was time to end this and claim a Great Rune.
#elden ring#elden ring lore#in character#in character blog#in character post#let's play#godrick the grafted#godrick#godrick the golden#nepheli loux#horah loux#banished knights#exiled soldiers#stormhawks
9 notes
·
View notes
Note
i need to know more about tomo pls i love 'dog with separation anxiety' characters
Ok ok I gotta put this under a cut because hes. rotating inside my head always. Going to put a link to his whole little page i posted bc this gives you Some basic information as to his Vibes.
Tomo is a Corrie medic! He’s got a few different like. personas he puts on depending on context. I talk a lot about his Weird Little Unhingedness persona bc thats when he’s letting is all out without hesitation or shame, which is really fun, but he’s a brother first, then a medic, and then a pathetic little creature.
As a vod and a brother, he is very, very loyal and committed to his siblings. His core guiding motivation is to make things better for them, but because of how he thinks this tends to be an individual focus rather than a group focus; he’ll individually get everyone a blanket before pushing for a new project to get everyone blankets, etc.
When he’s off duty and relaxed, he tends to be a friendly, nice guy. Will bend over backwards to help a vod, even one he doesn’t know, with minimal questions asked. Not a whole lot of respect for rules and authority; if you can’t indicate the practical reasons behind a standard or regulation, he will probably ignore it at his convenience. HOWEVER, he is also Definitely younger sibling coded and can be a bit of a shithead as a treat. Kind of a doormat and seems easy to bully but once he realizes he’s being teased or bullied he’ll go from the NOOOO!!! NOOO!!! younger sibling tears to I’m A Medic And I Can Tolerate And Shut Down So Much Bullshit on a dime. Likes people, likes to be around people in general, will worry and fret and scold if you’re being a bit reckless but also the biggest enabler in all of the med corps tbh. Believes in happiness and autonomy as a primary element of wellbeing and this drives a lot of that enabling; is the most likely corrie medic to go out of the way to let u keep a scar you want even if it makes his job fixing underlying structures more difficult.
He’s actually quite good at being professional when hes Being A Medic, and honestly can be a little ruthless, in terms of not hesitating to make calls (because that’s how you get people killed). His specialization is in orthopedic and reconstructive/plastic surgery, which in practice means he’s NOT out of medical much when on shift; if he’s called onto site, things are really bad. On a good day he has no emergency cases, but most of his emergencies are cases where there needs to be immediate and dramatic surgical intervention to prevent fatality. Amputations, skin grafts, major muscular trauma, broken bones; he sees a lot of really nasty shit, in his emergency capacity. In a non-emergency capacity, he still sees a lot of unpleasant and upsetting things, because he’s, yknow. reconstructing things and overseeing recovery from skeletal trauma, but it’s much much safer and less stressful. As a result of all this, he has a really strong stomach and a skewed sense of when gore, blood, or guts gets upsetting.
Also in his capacity as a medic, but off-regulation, Tomo provides a lot of suppourt to trans vode with gender-affirming care! He’ll do just about anything that’s not hazardous; he refers for tracheal shaves and bottom surgeries that require significant specialization or more advanced/specialized equipment than he has. But fillers, FFS, top surgery, horomone access? He’s gotchu.
Also; he knows he's cute. He knows people see him kind of as a pathetic little creature. He ABSOLUTELY weaponizes the shit out of this as a medic. he can cry on command because he learned the magical efficiency of just BURSTING into tears on someone avoiding the medbay. If you aren't guilted/made uncomfortable enough to comply he'll just get someone to drug you and haul you off lol
He’s a really affectionate, friendly, and easygoing guy overall, but the part of him that i talk about most often is his Little Freak setting. This is a manifestation of extreme seperation anxiety. He’s good at respecting verbal boundaries but is a Stage 5 Clinger. He will follow you into the bathroom if ur having a conversation and not notice until ur like excuse me that its weird. He’s really scared of loosing people, either to death or just to the vast distances of the galaxy, so he really really wants to be like. tangibly tied to people. This is where his cannibalism schtick comes from like he cannot imagine a closer intimacy than the physical substance of one’s self being intergrated into the other through consumption…. carry him with you forever and vice versa….. woah…..
@mamuzzy also pulled a GALAXY BRAIN take putting him w Mereel in that one art. Rotted my brain hard for them as a cringefail couple where their respective toxic traits slide off each other like water off a duck. I have a Lot of meta for that im not going to elaborate on too much beyond tomos tendancy towards clinginess being satisfied by mereel pinging him when he’s away, mereel being unbothered and indulgent of his weirdness, and tomo being game enough to help mereel that mereels habit of social engineering and manipulation to get what he wants doesnt have a chance to get toxic bc tomo is already willing give mereel whatever he wants with the ironclad exception of endangering his patients, which he is too stubborn and protective to be manipulated directly about anyway.
I decided that they met bc mereel needed to change his apperance for smth, hooked up w tomo (convenient emotionally vulnerable mark! yippee!) to gain access to medical supplies, was asking about a kind of filler (intended use for joint injuries but off-label use as a filler) to figure out if he can self-administer it and Tomo was immediately like oh i can administer it if you want to try! It’s easy to dissolve if you don’t like it! Mereel agreed, Tomo put in the temporary fillers, and they both walked away from the encounter satisfied and with each other’s contact information in their pocket.
It is very important to note that while Tomo IMMEDIATELY recognized Mereel was interested in the filler’s capacity to change facial structure and apperance, he did not realize Mereel wanted apperance-altering interventions for a mission until months later when someone pointed out he is a black ops specialist and got together with Tomo to use his skills n specializations. He had fully been working on the assumption that Mereel had just been interested in gender exploration even after they had an established pattern of Tomo administering temporary cosmetic procedures for Mereel’s missions
ANYWAY thank u I love him he is so deeply strange. just an odd little dude.

#oc tomo#hes sooooo babygirl#i need to stress: he is so ride or die its literally self destructive#there is a network of squadmates n other medics devised solely to keep assholes from taking advantage#yes they r concerned abt mereel but it seems to be working?? mereel is not Actually asking for anything inappropriate#bc what hes asking tomo to do for him as favors is mostly medical suppourt which is fine#but shinies will beg him for help getting things that r much more dangerous if u dont put a stop to it#he Was accidentally involved in several corrie contraband rings before intervention#i am obsessed w mereel doing his mereel deal of trying to get tomo ingratiated to him only for at every step tomos already there#mereel: *carefully structuring tomos life so he does smth he wants*#tomo as soon as he picks up on it: oh lol here u go [GETTING A GOOD GRADE IN HELPING SOMETHING POSSIBLE TO ACHEIVE AND REASONABLE TO WANT]#mereel: i know i am good at being charming and getting people to give me things but something is definitely wrong with you#dynamic of mereel being like hes kind of like a weird pet and favor machine with absurd kinks i want to study him. i like him tho#and tomo being like yes i fully understand mereel would sell me to satan for 1 corn chip. he is one of my favorite people in the universe#its like 2 people firing dysfunctional relationship grenade launchers at each other n being in a perfect untouched circle after#NOT making each other better or healthier but somehow its working out... failing upwards etc etc#sorry for Massive Dump then Massive Tags i just adore this lil freak
8 notes
·
View notes
Text
Pristyn Care: Innovations in ACL Surgery: The Development and Use of Synthetic Ligaments

Anterior cruciate injuries are one of the most common but most crippling sports-related injuries caused to athletes from amateur to professional levels. It limits the knee joint from unstable activities for rotating and forward movements. The injury of the ACL can reduce the mobility of joints, causing chronic pain, and deteriorating the quality of life drastically.
In most of the cases, it necessitates surgery. New developments, techniques of production, and ways to use synthetic ligaments nowadays represent a true revolution in orthopedic medicine. All the novelties in treatment were taken into consideration by Pristyn Care in its work to innovate the Pristyn healthcare services, and as soon as the patients began to take the benefit of the most advanced options for ACL repair through minimally invasive interventions, the expanded benefits of minimally invasive techniques began to be evident clearer.
Importance of ACL Reconstruction
The ACL plays a very important part in the stability and movement of the knee joint; basically, activities such as walking, running, and jumping are regulated. These micro-injuries, if not halted in the growth phase, can grow into serious knee instability. The individual is put at risk of further injuries and a high probability of degenerative, destructive joint conditions of the osteoarthritic type. It is estimated that about 200,000 reconstructions of the ACL are carried out annually across the globe, and the question of finding and applying an integral treatment suddenly becomes urgent.
Most notably, the introduction of artificial ligaments entirely changed the idea of ACL reconstruction; it was the arrival on the market of a durable commercial analog of traditional grafts. In most cases, the period of recovery was elongated by the occurrence of pain in the donor area and the need to recover two traumatized areas and to use transplant tissue taken from the body of the patient. Contemporary solutions, backed by state-of-the-art equipment and the teams of surgeons in the Pristin Care facilities, have brought initiation of repair of an ACL tear to a new level—the maximum quality of life that individuals devastated by such an injury can hope for.
Synthetic ligaments. What exactly are synthetic
Some of the commonly used and developed synthetic implants are the synthetic ligaments used in orthopedic surgery. More precisely, they are artificially created biomaterials used in cases of a technique for replacing damaged natural ligaments. The synthetic ligaments are not autografts, allografts, or autografts harvested from the body of the patient but, on the contrary, they are biocompatible polymers in origin.
The various available options of synthetic ligaments and benefits brought by it include good quality, which is consistent; unlimited supply; and no morbidity at the donor site. The extraction of autografts can be a bit frightening to the patient, and most of the time, more time for recovery is needed. Other than that, synthetic ligaments minimize the time used during the surgery because grafting is not necessary.
That is why advanced synthetic ligaments are increasingly being used as a substitute for grafting, since, in some places, the availability of appropriate and right donor grafts is very limited. This, therefore, enhances the access and timeliness of the surgeries for anybody in need of ACL.
Where Technological Innovations Impact Development on Synthetic Ligaments
The development of an artificial ligament, and more so that of an artificial fiber, is an extremely interdisciplinary field of materials science and engineering, aiming to produce fibers with properties analogous to natural ligaments. If performed on a human knee, that material should be strong, flexible, and durable enough to bear the dynamic stresses. Modern ones are made using advanced polymers, usually polyethylene terephthalate, and polyurethanes for their qualities of strength and elasticity.
This is particularly the case since such developments are specifically targeted at the improvement in the integration of such material with human tissue, the further reduction of risks for tissue rejection, as well as the enhancement of the healing process itself. Particularly, "Pristyn Care" is engaged in doing the given research process further enhancing the boundary of what is possible to be done with synthetic ligament technology. Focusing on knee biomechanics allows developers to adapt how a ligament's structure is formed to recreate natural motion while at the same time reducing complications and inducing new methods of natural and efficient ways of healing.
The newest technologies will save artificial knee ligaments from being inferior or just equal to the traditional knee-ligament grafts and most of the time, they will be far above benchmark levels by such a huge amount, marking a huge leap in ACL reconstruction technology.
How Pristyn Care is Changing the Way ACLs are Reconstructed
Pristyn Care leads from the front in the adaptation and innovation of methods for synthetic ligaments in the reconstruction of ACLs. There is a deep commitment to the assimilation of the latest in medical innovations with the aid of advanced technology that supports conducting such complex procedures in ultra-modern surgical facilities. With patient safety and surgical efficacy set to be a priority, the surgical centers of Pristyn Care can perform every ACL surgery under the best of conditions. Moreover, Pristyn Care is actively involved in partnering with advanced medical researchers and bioengineers to further enhance effectiveness and safety in the use of synthetic ligaments.
Reviews of ACL surgery operations under the aegis of Pristyn Care state that the medical staff were professional, the facilities were modern, and generally, surgeries were performed with good outcomes. All these statements refer not to new medical technologies but to the high rates of patient satisfaction and trust.
Advantages of Synthetic Ligaments in ACL Reconstruction
Using synthetic ligaments in ACL reconstruction has one major benefit which is the elimination of donor site morbidity. Unlike conventional techniques that include removing body tissue from a patient, these issues can be avoided by using synthetic ligaments. Therefore, it is widely recognized as an effective approach that lessens the chances of postoperative infection and pain reduction along with a quicker & easier recovery process. Pristyn Care reviews indicate that patients have highly ranked this method because they recover within a short time and experience minimal postoperative discomfort.
Pristyn healthcare reviews indicate that Pristyn Care’s use of synthetic ligament in ACL surgery has yielded outstanding results, which have enabled patients to make fast comebacks for sports and their normal duties.
In Pristyn Care reviews, people talk about how much they are satisfied with the minimal interruption to their lives, and the quickness with which they recovered. Good testimonials through Pristyn Healthcare reviews emphasize how advanced surgical practices and individualized treatments offered by Pristyn Care are geared towards providing high-quality health services resulting in the best outcomes.
Identify the Challenging Issues and Consider
The utilization of synthetic materials in surgical procedures presents both opportunities and challenges. Although these materials can enhance the recovery process due to their design to integrate with tissue without triggering an immune response, their long-term durability remains a concern. Pristyn Care reviews often highlight the rigorous monitoring of synthetic-tendon integration, particularly under the continuous stress imposed by daily activities. This is an area of active research within Pristyn healthcare reviews, focusing on enhancing the material's ability to withstand long-term use without compromising safety.
Additionally, regulatory and ethical factors about these techniques are vital. In addition, all synthetic materials used are strictly regulated by Pristyn Care for maximum safety. This commitment to safety standards is reflected in Pristyn healthcare reviews where the rigorous clinical trials and medical & ethical constraints are highly acknowledged. These materials undergo stringent safety checks before their approval for use so that they conform with the highest possible safety standards hence maintaining the reputation of Pristyn Care as a provider of safe, innovative, and effective Pristyn health care solutions.
Patient Success Stories and Case Studies
Against this backdrop, many life-changing benefits make patients at Pristyn feel that their ACL is rebuilt with synthetic ligaments. This is not on paper, but one watches how a patient describes getting back to sports activity after months of surgery and says great recovery is credited to great care. Another case in point reflects a patient who almost felt no pain with rapid rehabilitation due to advanced surgical techniques at Pristyn Care. These stories strengthen the good reviews about high satisfaction rates and successful surgical outcomes on Pristyn healthcare platforms.
Conclusion
ACL injuries are mostly known as anterior cruciate ligament injuries and they are common and severe, especially in high-impact sports or activities that involve the knee joint heavily. These injuries negatively affect performance, so it requires a well-planned recovery plan to safely go back to what one was doing before. One main surgical procedure through which the normal functions of the knee can be restored is known as ACL reconstruction. The Return to Play (RTP) protocols post-surgery should be focused on total recuperation, prevention of future traumas, and restoration of peak levels of performance. For Pristyn Care, emphasis has been put on RTP post-ACL reconstruction to achieve full patient recovery and enable them to regain their best level of performance. In Pristyn care reviews, there is usually mention of how effective its customized RTP protocols are because these protocols help in preventing reinjuries. Further, Pristyn Healthcare reviews also hail the individualistic approach taken during the rehabilitation period which has significantly improved the success rates for ACL surgeries conducted at Pristyn Care.
#pristyn care#pristyn care reviews#pristyn healthcare#pristyn healthcare reviews#pristyn care lybrate#pristyn care company
3 notes
·
View notes
Text
HELLO PEOPLE OF THE COMMONWEALTH!!! I bless you with Kal’s lore, at long last. (Preferably read this with Now That’s Sacred by Jack Conte or Wired by The Neighborhood. Brings the atmosphere into this a little more.)
[JULY 20TH; 2287 — EASTSIDE OF GOODNEIGHBOR]
Name: Kal Dunham
Age: 40
Status: Relocation to Boston Encampment; Presumed Dead by Enclave Officials
Rank: Soldier; Patrol Officer
Additional Details: Daughter of Sgt Hodges and LT Oxheart. Trained to specialize in Power Armor maintenance and patrol operations
————————————————————————-
Kal, born in 2247, had been in the Enclave at birth, like many other Recruits. She was able to gain the title of a Patrol Officer through rigorous training and examinations, aided by her mother and father’s support.
At around 2264, however, her father, Lieutenant Gus Oxheart, tragically died at Raven Rock, causing her mother, Sargent Hodges and Kal herself to have to move to the Boston Enclave Chapter. The two of them stayed at the Southern Enclave Encampment, up until the Brotherhood of Steel discovered the Enclave’s existence in the East, ambushing the Southern and Western Encampments, where most of the Enclave members lived at the time, the year specifically being 2280. Sargent Hodges, seeing as her only daughter was put in danger again, made the executive decision to send Kal to the Eastern Encampment, to not only keep her safe, but to make sure that the Enclave would at least somewhat survive, even if it was only a few members now after the ambush.
On her way to the Eastern Encampment, however, the Brotherhood noticed the group’s Vertibird fleeing, shooting it down, the vertibird crashing just west of Police Precinct 8 . A minutemen patrol team was luckily stationed near the Precinct, and saw the crash, investigating it. They found Kal in the rubble, right hand and left leg completely destroyed by the impact of the crash, with burn scars and major gashes littering her body. They rushed her to Diamond City with the help of being very quick and careful on their feet, constantly jabbing Stimpacks and stray blood packs into her body to compensate for the blood loss and injuries. She is successful in getting to Diamond City on time, gaining two prosthetic limbs and a massive amount of skin-to-scar grafting along the major gashes and some of the more serious burn scars.
Within her months of needing to recover, Sargent Hodges bares witness to someone finding the coordinates to the X02 armor, hunts down the person who had the coordinates, and ultimately dies from her injuries, the person having to flee the bunker after being ambushed by Hodges and her team. As Kal gains a near-full recovery, she gets a signal from her mother requesting backup, but is still too injured to try and find her just yet. When Kal does fully recover, she heads straight to the Valentine Detective Agency in hopes that they would have even a chance at finding Hodges’ last location, dead or alive.
During the case to find Hodges, however, Kal sees how happy everyone is in Diamond City, starting to regret her actions within the Enclave. It’s also during this time that she finds herself developing feelings for Nick Valentine, as he showed genuine interest in her story when Kal was first interviewed by him. Although, she did leave out the fact that she was of the Enclave, fearing she would be taken away by Diamond City police, or worse, killed on site by them. Once they get to the bunker, however, Nick figures out she’s (now formerly) apart of the Enclave, feeling betrayed and angry at her. She tries to explain herself before Hodges’ backup team discovers them, not realizing it was Kal, considering that the Enclave presumed her as dead after the crash. She takes the chance to redeem herself by killing off the backup, but Nick still feels slightly betrayed by her, even if he forgave her in the end. Grabbing the X02 armor, Kal and Nick get out of the bunker, heading back to Diamond City, Nick staying in his office and Kal going for a drink after feeling the guilt of her actions weigh her down. She falls asleep at the Dugout Inn, but not before renting a room. She would’ve gone back to the Detective Agency, but she knew Nick probably wouldn’t want to talk to her for a while after all that happened. She starts getting dreams of him, regretting what she had done, deeply missing him, either craving his gentle embrace or trying to find how to explain everything to him. She keeps herself from Nick for a few days until Kal convinces herself to write to Nick to at least tell him why she lied to him, and Nick is surprised when Kal tells her full story, and how she realized just how bad the Enclave was and how she felt the need to hide it as to not only keep herself safe, but to try and keep her past self as far away from the present her as possible. In a moment of vulnerability, she admits her feelings as well, Nick being caught off guard by her feelings, but not necessarily scared or upset by them, just confused that a woman like her would fall for a synth like him.
Kal leaves Diamond City in her shame, knowing that her secret could be revealed by the public at any moment if someone got their hands on her letter to Nick, residing in Goodneighbor and working for K-L-E-0 in hopes to restart her life and become a bounty hunter. The dreams of Nick persist still, to the point where she constantly keeps a holotape of his voice on hand and a photo of him taped to the back of the tape, desperately trying not to forget the only person she had to in her life after mother’s death.
____________________________________________
Woo that’s it hope u like it :3 I’ll b making angst posts of the bunker scene hopefully here soon so look out for that :>
#tw: character death#tw: violence#TW: blood/injury#fallout 4#fallout#fallout oc#Enclave Fallout#enclave#enclave oc#fallout 4 oc#nick valentine#character lore#guys i’m so normal about this game#and yes I gave Nick a romance arc fucking deal with it#he deserves to have a romance arc considering that both Curie and Danse get to be romanced#I was writing this while listening to Now That’s Sacred by Jack Conte lmfao#I fucking love Jack conte’s music it’s incredible
5 notes
·
View notes
Note
I'm a trans man who wants phallo SO bad but the Fear Mongering people do makes me so scared. I have such a fear of surgery anyway and people say phallo is nearly 23hrs long, and it has more risks than heart surgery does, and idk if these are true bc I'm too scared to google it..But I want it so bad, but the stuff I hear scares me. Also people saying it doesn't have any sensation worries me. You said trans men can ask about it so I hope this is ok to do on anon!!! I'd appreciate a non fear filled reply so much thanks!!
23 hours!! Those poor surgeons, can you imagine!
Virtual hugs if you’re the hugging type, Anon, and a cool rock if you’re not.
Those things are definitely not true, not remotely. It’s a long surgery, but when I say it’s long that means it’s about 8 hours all told. It sounds like maybe someone heard it referred to as an “all-day” thing meaning a full WORK day, but instead assumed that that meant a full CALENDAR day. Or, you know, a transphobe made shit up to scare people.
It is most definitely not nearly as risky to your wellbeing as a surgery in which they saw open your sternum and cut open your actual beating heart. There is a fairly high chance of a minor complication that can result in the terrible ordeal of getting pee on your pants sometimes—a urethral fistula—and in most cases, they close up on their own anyway without needing another surgery to correct them. And in this case, “fairly high” means 40%, so it’s still less than half a chance that it’ll happen in the first place. At worst it’s annoying. Serious complications, the type that put you in danger, are extremely rare.
The sensation thing is also false, because they literally harvest a length of nerve from your donor site and hook it up to your existing bits specifically so you WILL have sensation! Sure, it takes a little while for the nerve to heal, but that’s just the reality of ANY surgery.
The nerve grows back in your donor site, too, by the way. While I was typing this up I discovered that one particular spot on my graft is ticklish.
Everyone has their own individual healing factor, but speaking for myself, I had full erotic sensation before the 3-month mark, and the orgasms have been incredible. The head and base are highly sensitive, and everything in between responds pretty damn nicely too, just less of a hit-the-ceiling level of sensitivity. And, you know, if you’ve handled an AMAB person’s penis much at all you’ll know that’s pretty much in keeping with how their dicks work too.
It is an in-patient surgery so if you have it, you’ll be staying in a hospital for a few days so they can keep an eye out for rare disasters. My stay was four or five days of snoring most of the day and periodically getting woken up to eat or answer some simple check-in questions, lift my arm for nurses to move stuff, etc, and then conking back out.
Being cathed sucks, but two weeks of frequent trips to the toilet to drain your bag is honestly nothing compared to a lifetime without (or with vastly reduced) bottom dysphoria. That’s the part that I hated. Everything else was your typical recovery: 10-15 days of sleeping 20 hours a day, then however many weeks of being tired, taking meds, and careful washing, gradually feeling more and more normal until you’re back up to full and ready to get back to business as usual.
Except with this one, you get to learn to pee standing up in the process. :D
(Protip: don’t try a public urinal until you’ve got it down pat at home. Not because of cis men, but because the learning process is messy, lol! The overwhelming majority of cis men in public restrooms want nothing to do with anyone else while they’re in there. The only place anyone’s gonna give your dick more than half a second’s accidental glance is in a gay bar. In 8+ years of using public men’s rooms I have yet to see one (1) penis that wasn’t mine!)
#phalloplasty#ftm#trans men#bottom surgery#trans matters#transphobia.#queerdom#medical transition#replies to things
185 notes
·
View notes
Text
Being rendered helpless (PANOPTICON)
• Rita Ora's thumb (Encounter for aftercare following multiple organ transplant)
• Florence Welch's thumb (Laceration with foreign body of right ring finger with damage to nail)
• Winona Ryder's thumb (Secondary lacrimal gland atrophy)
• Lucy Hale's thumb (Failure in dosage during unspecified surgical and medical care)
• Conan O'Brien's thumb (Influenza due to other identified influenza virus with otitis media)
• Tyra Banks's thumb (Malignant neoplasm of overlapping sites of other and unspecified parts of mouth)
• AnnaSophia Robb's thumb (Laceration of extensor muscle, fascia and tendon of left middle finger at forearm level)
• Minka Kelly's thumb (Acute tonsillitis, unspecified)
• Djimon Hounsou's thumb (Cyst and mucocele of nose and nasal sinus)
• Forest Whitaker's thumb (Meningococcal myocarditis)
• Jimmy Buffett's thumb (Other disorders of continuity of bone, right radius)
• Kate Bosworth's thumb (Other hyperparathyroidism)
• Kristen Bell's thumb (Solitary bone cyst, left ulna and radius)
• Matt Bomer's thumb (Laceration of other muscles, fascia and tendons at shoulder and upper arm level, unspecified arm)
• Prince Harry's thumb (Laceration without foreign body of back wall of thorax without penetration into thoracic cavity)
• Avril Lavigne's thumb (Calcification and ossification of muscle)
• Demi Lovato's thumb (Nondisplaced fracture of lateral condyle of unspecified femur)
• Carmen Electra's thumb (Salter Harris Type III physeal fracture of upper end of humerus, left arm)
• Mary-Louise Parker's thumb (Atherosclerosis of other type of bypass graft(s) of the extremities with intermittent claudication, left leg)
• Vince Vaughn's thumb (Toxic effect of contact with other venomous marine animals, assault)
• Sean Lennon's thumb (Unspecified open wound of left front wall of thorax without penetration into thoracic cavity)
• Tate Donovan's thumb (Osseous and subluxation stenosis of intervertebral foramina of abdomen and other regions)
• Jennifer Aniston's thumb (Alcohol abuse with intoxication)
• Zachary Quinto's thumb (Mooren's corneal ulcer, unspecified eye)
• Tracy Morgan's thumb (Preterm labor without delivery, unspecified trimester)
• Jenna Elfman's thumb (Inflammatory polyneuropathy, unspecified)
• Kaley Cuoco-Sweeting's thumb (Perforated corneal ulcer, unspecified eye)
• DJ AM's thumb (Kaschin-Beck disease, left knee)
• Gordon Ramsay's thumb (Unspecified injury of extensor muscle, fascia and tendon of right index finger at forearm level)
• Elle Fanning's thumb (Benign neoplasm of connective and other soft tissue of unspecified upper limb, including shoulder)
• Scott Speedman's thumb (Encounter for routine postpartum follow-up)
• Curtis Stone's thumb (Swimmer's ear, left ear)
• Uma Thurman's thumb (Altered mental status, unspecified)
• Khloe Kardashian's thumb (Retinal hemorrhage, left eye)
• Maria Menounos's thumb (Passenger in three-wheeled motor vehicle injured in collision with fixed or stationary object in nontraffic accident)
• Miranda Kerr's thumb (Other combined immunodeficiencies)
• Brooklyn Decker's thumb (Atherosclerosis of other type of bypass graft(s) of the extremities with intermittent claudication, left leg)
• Ellie Goulding's thumb (Osteonecrosis in diseases classified elsewhere, thigh)
• Bethenny Frankel's thumb (Other chronic hematogenous osteomyelitis, left humerus)
• Judi Dench's thumb (Resistance to unspecified beta lactam antibiotics)
2 notes
·
View notes
Note
hello! i was wondering if it’s possible to use the skin from top surgery as a graft for phalloplasty? (sorry if it’s worded badly, i didn’t know how else to explain it)
i’ve been wondering this for a while but had difficulty finding anything about it (and it doesn’t help that i’m dyslexic)
Hello, no worries I understand you just fine. It's all good.
So I'll be honest, no, you can't.
There are a few reasons;
Healing time-
your body needs proper time and care to heal with the best results. If your body is trying to heal too much at once, you may not heal as well as you and your surgeon would want. Which can mean revisions or complications. This is often 6-8 months between procedures.
The doctors involved-
in top surgery there are a lot of doctors and nursing staff already taking care of you. There would be a lot of hands on one body if both teams worked at the same time. This could cause complications in one area or both because of doctors needing to position themselves properly.
Operation Time-
You would be on the table for a long time. This causes blood circulation problems, heart problems, clotting issues, anesthesia complications, and even breathing issues.
Chest Skin Graft-
skin taken from your chest is not nearly as sensitive as the alternative options for making a phallus, such as your arm, leg, back, or even abdomen. The tissue on your chest after years of being constantly rubbed and interacted with, makes it a less sensitive skin, and therefore may not produce any sensations you wanted or were hoping for.
Blood circulation for Phallus-
to get a blood supply to your phallus they take veins from other areas of your body (often a big vein near the donor site) to provide steady and healthy blood flow to your new phallus.
I hope this helped you understand a bit better why you cannot use your chest skin for phalloplasty.
It does seem a shame, but doctors only have your best interests in their mind. They want you to be safe, and they want good results.
Thank you for your question, if there is anything else you need do not hesitate to ask.
Stay Golden ✌🏽💙❤️
-Zestual
#why cant you use chest skin for phalloplasty#anon question#anon questions#ask Answersfromzestual#ftm trans resources#ftm top surgery information#why doctors dont use chest skin for phalloplasty#reasons why donor sites are used instead of using your access skin from top surgery#transgender#trans ftm#ftm transition#transman#ask me things#phalloplasty#lgbtq#ftm phalloplasty#phalloplasty blog#phallo education#ftm transgender education#ftm transgender resources#ftm transgender blog#ftm transgender educational resources
4 notes
·
View notes
Text

[ Headcanon ] BIRD RITUAL & FEATHER PROTECTION .

The burns on Caitlyn's shoulders were so severe that Tobias decided to try a ritual procedure with Caitlyn in hopes of providing more comfort to her. Skin grafts were not working, despite immediately using them so he turned to his Ionian culture and knew of a special ritual, also known as a rite of passage, was done among the people. For most of his culture, it was more of a symbolic process, meant to connect deeper to the roots of their Lhotlan ancestors. The process of grafting feathers to the arms, legs, or other parts of the body was a choice made by young teenagers to connect and reflect on the world of their ancestors. By doing so, it made them more bird-like but also a sign of respect and honor to those in the past. Protectors, healers, and those who bring wisdom.
However, Tobias looked at it from the angle of a doctor. With Caitlyn having that bloodline, the ritual would work and the feathers would adapt and thrive on her body, but his reasoning for doing so (and offering it to Caitlyn) was to provide better protection and insulation against the burns. This ritual has been a centuries-old technique, but it's not always successful as the feathers and grafting must connect to the tissue and blood vessels so that the feathers can thrive and grow continuously.

With Caitlyn's approval (as she was doing to help her welfare but also because she wanted to honor their ancestors), her father immediately went to work to find one of the birds from Ionia. The ritual of finding a bird also was linked to the idea of becoming 'one with the bird'. The bird provides healing against the ailment which she shares feathers with and becomes more bird-like, just like the Vastayan ancestors. The blue bird was not harmed, and the feathers taken were used from the molting. At the same time, another bird is used (one that has recently passed by the shafts still viable) in which they were used to be surgically connected to the shoulder. The entire process took hours with Caitlyn under while Tobias did the work specifically himself. He didn't trust anyone else with his daughter's quality of life but also because he knew of this ritual explicitly and while he was doing this for science, he did not wish to insult his ancestors either.


He used four different feathers to help Caitlyn with her burns on both shoulders. The upper feathers were Contour feathers, the most colorful and smooth feathers will protect from temperature, precipitation, and wind. Underneath these feathers were the Semiplump and Down feathers; which both provide insulation and comfort to keep the area cool and comfortable. Lastly, he also included some Filoplume feathers, which she could use for sensory input, primarily the use of temperature control and knowing when she needed to get out of the sun or cold.
The procedure had been a success after checking on it in a few days. Blood was regulated and processed through the feathers which would keep them alive, though she would have to learn how to handle the molting seasons, when old feathers would fall off and replaced with new ones, and learning how to properly preen and care for them. Caitlyn also needed to ensure that her feathers received light to keep them healthy while also learning how to clean them without the water affecting her burn sites.

The dark blue feathers cover her shoulders completely, from the top portion near her collarbone down below her shoulder. The feathers provide complete insulation and comfort for Caitlyn so that she can continue to do her job and move as needed without discomfort or pain.
Some of Piltover don't like her 'display of feathers' as it's very animalistic and doesn't fit into their culture of a prime and proper design. A part of Caitlyn had no problem doing this, as she was already different and a step apart from Piltover, never once fully fitting in so to embrace her willingness to do so only fueled Piltover to view her in a more negative sense. For Caitlyn though, this not only gave her protection and comfort, but it felt more natural to her. As if this was a part of her, a part of who she was. Also, in time, Caitlyn learned how to adapt the use of her feathers to better help her in fighting, including gauging wind speed and direction, and even the sensory movement around her that she can tell when someone is nearby just by the movement of her feathers in reaction to wind or water.
7 notes
·
View notes
Last Seen Blogs

darlingseraphina
𝕾𝒆𝒓𝒂𝖕𝖍𝖎𝒏𝒂₊˚໒꒱

kidnamedbird
Team Kid Named Bird scanlations

therealbl0om-blog
bloom

dancingconstellations
Dancing Constellations

karakuszeynep-blog
zeynep