#Medical Image Analysis
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
Tumblr.com is the 103rd most visited website in the world.
Text

Neturbiz Enterprises - AI Innov7ions
Our mission is to provide details about AI-powered platforms across different technologies, each of which offer unique set of features. The AI industry encompasses a broad range of technologies designed to simulate human intelligence. These include machine learning, natural language processing, robotics, computer vision, and more. Companies and research institutions are continuously advancing AI capabilities, from creating sophisticated algorithms to developing powerful hardware. The AI industry, characterized by the development and deployment of artificial intelligence technologies, has a profound impact on our daily lives, reshaping various aspects of how we live, work, and interact.
#ai technology#Technology Revolution#Machine Learning#Content Generation#Complex Algorithms#Neural Networks#Human Creativity#Original Content#Healthcare#Finance#Entertainment#Medical Image Analysis#Drug Discovery#Ethical Concerns#Data Privacy#Artificial Intelligence#GANs#AudioGeneration#Creativity#Problem Solving#ai#autonomous#deepbrain#fliki#krater#podcast#stealthgpt#riverside#restream#murf
17 notes
·
View notes
Text
youtube
Discover the Power of Fliki AI for Creators!
Fliki AI is a cutting-edge tool revolutionizing the AI industry by offering a seamless platform for generating high-quality content efficiently. Important Note: This video contains Affiliate links, where if someone navigates to them, there is a possibility that a commission will be paid to me by the affiliate.
Fliki AI:

With the increasing demand for AI-generated content, Fliki AI stands out as a game-changer in the field. Generating AI content efficiently is crucial for businesses and content creators looking to streamline their workflow and produce engaging articles quickly.
Fliki AI simplifies the content creation process, saving time and resources while maintaining top-notch quality. By using Fliki AI, you can unlock a plethora of benefits such as improved productivity, enhanced creativity, and access to a wide range of article ideas tailored to your specific needs. Stay tuned to discover how Fliki AI can elevate your content creation!
#aicontentgeneration #artificialintelligencerevolution
#fliki ai#neturbiz#enterprises#generative AI#Technology Revolution#Machine Learning#Content Generation#Complex Algorithms#Neural Networks#Human Creativity#Original Content#Healthcare#Finance#Entertainment#Medical Image Analysis#Drug Discovery#Ethical Concerns#Data Privacy#Artificial Intelligence#GANs#Audio Generation#Creativity#Problem Solving#ai#autonomous#text to video#text to speech#ai scene generator#ai automated editing#innovations
0 notes
Text

Neturbiz Enterprises YouTube Channel - AI - Innovations
Our mission is to provide details about AI-powered platforms across different technologies, each of which offer unique set of features. The AI industry encompasses a broad range of technologies designed to simulate human intelligence.
These include machine learning, natural language processing, robotics, computer vision, and more. Companies and research institutions are continuously advancing AI capabilities, from creating sophisticated algorithms to developing powerful hardware.
The AI industry, characterized by the development and deployment of artificial intelligence technologies, has a profound impact on our daily lives, reshaping various aspects of how we live, work, and interact. The AI industry presents numerous opportunities for affiliate marketers to promote cutting-edge tools and services. Each Platform may offer different commission rates.
#artificial intelligence #generative ai
#Generative AI#Technology Revolution#Machine Learning#Content Generation#Complex Algorithms#Neural Networks#Human Creativity#Original Content#Healthcare#Finance#Entertainment#Medical Image Analysis#Drug Discovery#Ethical Concerns#Data Privacy#Artificial Intelligence#GANs#AudioGeneration#Creativity#Problem Solving#ai#autonomous#deepbrain#fliki#krater#podcast#stealthgpt#riverside#restream#murf
0 notes
Text
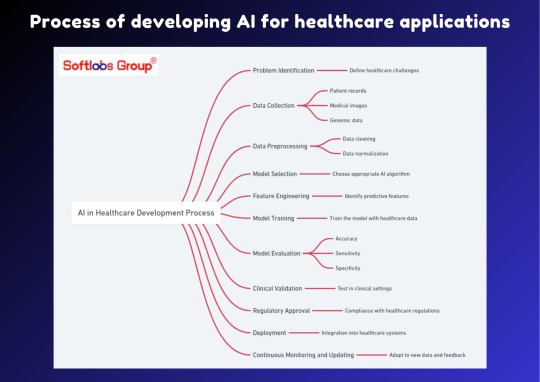
Discover the process of developing AI for healthcare applications with our informative guide. This simplified overview outlines the essential steps involved in leveraging artificial intelligence to enhance healthcare solutions. Perfect for anyone interested in the intersection of technology and healthcare. Stay informed with Softlabs Group for more insightful content on cutting-edge advancements in AI.
0 notes
Text
Bruce is actually really attractive, and I have enough reasoning to make a list
He's:
Tall (. Tall enough to hit his head on the vault doorframe)
Long-legged


Has a straight nose bridge
Has high cheekbones (more noticeable in 2nd pic below)
Has a strong jawline


Sharp eyes, but they aren't small (plus eyebags if you're into that)
Overall, he has strong, attractive facial features
Has broad, refined shoulders. You can tell he works out (or he did, when he was alive)
Even has a thick, muscly neck

He has MUSCLE. Is SCULPTED. NOICE. VERY NOICE. (nice arms. Nice shoulders. Nice neck. Nice legs. Nice butt-)
(There are actually panels where you can see some of his muscles. Other than those already shown here, he's got bricky thighs-

-and in the panels where we first get his name dropped, he's got those shoulder blades too-)
The one time we see him smile, and he actually has a scary one

Has small, kinda sharp pupils, and his eyes remind me of a cat. We only ever saw him tense or defensive, so his resting/listening face is really cute

Other than the physical appearance stuff, he also:
Takes shit without batting an eye (patience, knowing it's just how Kudo is, etc)
Kudo being all "Cut the crap Bruce and give it to me straight", after Bruce tests his blood and is rightfully Concerned because they just faced AFO
Put up with Kudo's experimenting and testing over Yoichi's transferable Factor
Did ya'll see the look on Kudo's face when he realized he had Yoichi's Factor/will? Kudo was going to start in nonsense and Bruce just dealt with that.
Also something I noticed when looking back at the images here; Bruce has bandages on his arms in the void. But not when he faced AFO in the sewers.
Were he and Kudo cutting their arms open in their experimenting over Yoichi's theory? Is this why Kudo has two gauntlets instead of his one? Why we never see his bare arms in the void? That he always keeps his arms down so there's no slip?
Is smart enough to run blood tests, plus has enough common sense to pick Shinomori as his successor
He picked a guy who avoids society, has an Ability to detect danger so he can always stay away from AFO, is also a coward so he's never going to go throw himself into danger, even without knowing instinctively he stands no chance, etc.
Meanwhile, Kudo chose Bruce, who he played Hot Potato Yoichi with; but he did also trust Bruce, and put the only pure combative Ability in OFA through Bruce.
These two made their choices based on what they valued and saw the Factor needed.
Is logical, analytical, and calm.
He tried advising Midoriya on their Abilities in One For All, especially his own.
Midoriya then tried ignoring him about using Fa Jin for the first time, but found he was right, thinking: "Dammit!! I had [Lady Nagant] right where I wanted her, but... ugh! The Third was right. My parallel Quirk processes are all screwed up!" (ch. 314).
Plus, when Midoriya fixed his processing mistakes, Bruce was analyzing the way he reached his new conclusion. Pure facts, no bias, very calm, just saying it as it was.
We never see him panic. When he's caught by surprise in the sewers by AFO, Kudo, and Yoichi's little bubble event, he immediately reacts. He doesn't falter, he just knows he has to do something right now.
Was more willing to listen than Kudo to Yoichi's beckon, and probably was just following Kudo's rejection of Midoriya
While we don't see Kudo's face, we see Bruce's eyes when Yoichi calls on his heroes. Bruce was more open and receptive, or at least more impacted.

Bruce was also the one to start talking, while Kudo just kept quiet.
He actually communicates a lot
When Yoichi called them to support Midoriya, Bruce started talking to paint a picture of why they thought the way they did, so Yoichi understood where they were coming from.
(Though he seems to beat about the bush sometimes, since Kudo spoke up to be direct on how they couldn't just put their trust in some starry-eyed teenager. Plus, when Kudo tells him to just tell him what's wrong [double Factors])
When Midoriya first used Fa Jin against Nagant, Bruce came out just to tell him he knew what he was trying, but that Midoriya wasn't ready; and Midoriya found he was right. Midoriya just didn't want to listen to him then.
He asks Kudo for clarification after finding Kudo had two Factors in him after the sewer incident ("Just to be sure, All For One didn't touch you, right?") Kudo knew him well enough to go "stop beating around the bush and tell me", so Bruce was probably gonna start with questions, theories, and trying to understand everything in general, before saying "yeah you have two Factors. Don't know why".
Is strong-willed and loyal.
He followed Kudo, even to death, carrying on the cause he started until it ended with him.
Plus, when talking about how AFO needs a strong will to override OFA's own, we first see Bruce, Kudo, and Yoichi.
AFO couldn't steal OFA because the will was too strong for him, and that was back during Banjo's time. Since Shinomori never actually tried opposing AFO and just hid, we can assume the first Three (Yoichi, Kudo, Bruce) already had an accumulation of strong willpower that made OFA un-stealable. Those three are a strong enough foundation, and the main wills, that the other users just become bonuses.
Kudo, also saying that Midoriya needs allies with the same will and drive as him... hey Kudo, you're talking about yourself and your old allies, aren't you? That's why you look at Yoichi and Bruce when you say this.
Not only is Bruce attractive, but he's got good character. THE END.
#yes this is a bruce appreciation post#am i biased? yes. am i right that he has these features? also yes.#hes actually a very attractive person. hes got all the right features for it#plus hes smart (some medical knowledge) is really loyal strong-willed and patient#he puts up with kudo SO much#from being bossed around to taking home yoichis brother to whatever the heck kudo made him do to figure out OFA's transfer properties.....#i didnt think much of bruce originally#then i started doing resistance fic stuff and now hes a fave#hes a little blorbo#that i throw in terrible situations for my own entertainment#used his scary smile for comedy purposes#like when he made a kid cry once. or when a meta child was afraid of him so they bit him#has patience to deal with kudo and co. but also. has enough bite to snark them. is how i like writing him#oh? background character? well lemme just *picks him up* EXPAND ON THAT-#fic stuff: he tries making a good impression on a girl and kudo is ruining it immediately#he doesnt know what to do because the two always banter#kudo: fuck you#oc: fuck me yourself you coward#he sees through a rose-lens that kudo is trying to rip off his face#appeciation kinda turned analysis in general#bruce#kudo#yoichi shigaraki#bnha#mha#spoilers#boku no hero academia#my hero academia#NOT YOICHIS BROTHER. i meant Yoichi / AFO's brother in a prev tag up there but theres too much tags i dont wanna rewrite to fix that#(image limit and tag limit)
333 notes
·
View notes
Text

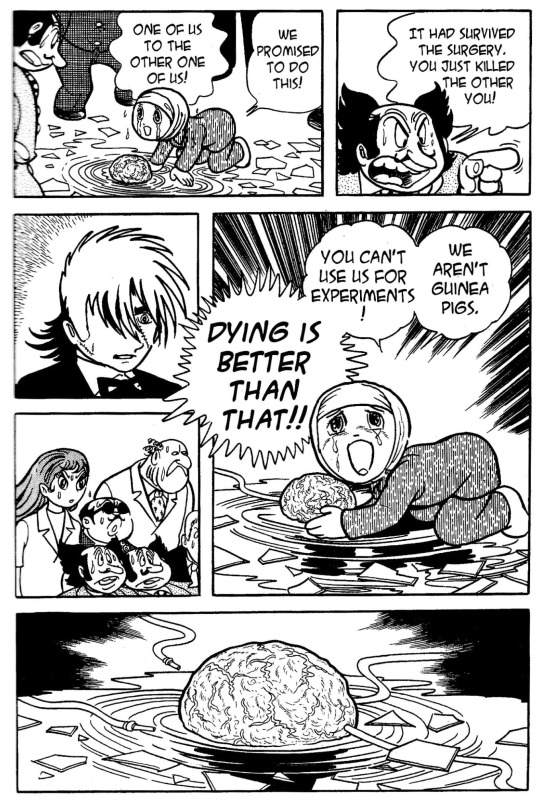
("The Two Jans," a sealed chapter of Black Jack printed in English exclusively in a limited edition hardcover and not reprinted again.)
The twin boys we meet in this chapter are both named Jan Marchand (their parents are quite horrid, not differentiating them by name is just one of the awful things done to these boys.) Jan is a German equivalent of "John" and Marchand is French for "merchant," but the name Jan also alludes to their condition... another name for twins fused at the head, craniopagus, twins is "Janiceps or Janus twins usually share one body with one head and two faces." [Source] This is an allusion to a two-faced Roman deity named Janus.

"The site of attachment could be one of eight (thoracopagus, omphalopagus, craniopagus, cephalopagus, parapagus, ischiopagus, pyopagus or rachipagus).
The etiology of heteropagus twinning is yet to be determined but there are 2 dominant theories. The “fission” theory suggests incomplete separation of the embryo while the “fusion” theory proposes coalition of 2 originally distinct parts. The most advanced theory postulates that it occurs due to vascular compromise in utero, leading to death and partial resorption of one of the twins."
[Source]
We had to memorize a lot of -pagus names for these depending on where they're attached... given Pinoko's backstory involving her being a fetus-in-fetu / deformed parasitic twin (likely due to a lack of understanding of how fetiform teratoma arise in the 70's, although she's not called that in the manga, but "teratoid cystoma")... perhaps if she wasn't so absorbed into her twin's belly, they would have been born omphalopagus!

There's a similar sci-fi aspect to this story as with Pinoko's (re)birth, but despite his moral misgivings against the idea of experimenting with these twins... he got talked into it for a Nobel prize. It's a younger Kuroo... like Pinoko, the excised Jan is being kept alive as a brain, floating in culture medium... but he's to be used as a test subject. No prosthetics or Frankenstein-esque strange science used to create him a body for him to exist as a separate person in...

He's a living brain, fully aware, if unable to see or even hear [so even more limited than Pinoko], but still possessing his memories and feelings and capable of feeling pain, a child's mind held captive, with no way to communicate with anyone. Maddening. He's not even shown to have psychic powers like Pinoko did before she had a body of her own. He'll just be trapped, subjected to experiments, but unable to voice his opinions on anything done to him, unable to communicate with anyone, even his brother, ever again.
His brother waking up, finding his brother's brain, others confirming that's who it was, and immediately killing him was easily understandable in that light. They promised each other to kill the excised brain to spare the twin without a body from being subjected to human experimentation.
Notably, the Vertical translators made a point of having the doctors refer to Jan as "it"... they're not treated as fully human. Pinoko chose to trust Black Jack because he was the first to treat her as human and talk to her, whereas other doctors just saw a lump/tumour/something to be excised and discarded. A lot of fans also seem to disregard Pinoko's whole existence before her "birth," despite her being alive and learning and aware, just severely disabled as she could only hear [speaking only in her mind and manipulating things physically through unnatural means]...
I wonder if Black Jack saw Pinoko as an absolution? Or just wanted to avoid repeating the tragedy of Jan and Jan.

#Black Jack#Osamu Tezuka#medical drama#classic manga#conjoined twins#I like how Tezuka-sensei draws twins at different ages and with varying features and even different haircuts/styles...#medical thriller#horror#for the situation I do not tag real deformities and medical conditions as horror#long post *#body image *#nudity * in a medical context#analysis#The Two Jans#Jan Marchand
11 notes
·
View notes
Text
Medical Imaging Meets Innovation: Unlocking Opportunities in a $7B+ Market
The global medical image analysis software market size was estimated at USD 3.27 billion in 2023 and is expected to grow at a compound annual growth rate (CAGR) of 7.8% from 2024 to 2030. An upsurge in the need for diagnostic imaging software within various medical specialties, including dental, urology, orthopedics, oncology, and neurology is expected to drive market growth. Furthermore, the increasing adoption of ultrasound imaging systems to facilitate faster diagnosis of chronic disease is projected to fuel this software demand.
Moreover, continuous innovations in imaging technology, including developments like Computer-Aided Diagnosis (CAD), are anticipated to further boost the demand for these solutions. The integration of Artificial Intelligence (AI) into medical imaging has reshaped market dynamics in recent times and is expected to have a positive impact on market growth over the forecast period.
The AI-based solutions have various applications in medical imaging, including diagnosis, detection, image analysis, and clinical decision support. Though AI adoption is in the early phase of MRI and CT technologies, rising demand for accuracy, efficiency, and patient safety is anticipated to boost the adoption of AI-enabled medical imaging over the forecast period. In addition, the market growth is significantly driven by the growing acceptance of technologically advanced products, such as multimodality imaging platforms and 3D imaging. These solutions come with several benefits, including high-resolution imaging, user-friendliness, and flexibility, which make them highly attractive for healthcare professionals and researchers. The introduction of advanced technological products and the emergence of efficient information management systems are expected to be significant catalysts for market growth during the forecast period.
Focus on innovation in medical image analysis has also given rise to certain measures that are being implemented. Furthermore, can assist in disease diagnosis, treatment, and early detection. It has been regarded as one of the most advanced technologies to combat the COVID-19 crisis. In the context of COVID-19 disease, numerous AI, machine learning, and deep learning approaches have been used in medical image processing, which is another significant factor contributing to the market growth. Diagnostic and research centers are projected to become vital end users of image analysis solutions due to the increasing demand for more efficient solutions that can improve patient outcomes.
Detailed Segmentation:
Software Type Insights
Based on software type, the integrated software segment led the market in 2023 and is expected to grow at a CAGR of 7.4% from 2024 to 2030. The significant market share is owing to the advantages linked with the utilization of these solutions.
Modality Insights
Based on modality, the tomography segment held the market with the largest revenue share of 33.0% in 2023, owing to its cost-effectiveness. The emergence of dual-source and AI-enabled CT scanners is expected to mark significant milestones in market expansion.
Imaging Type Insights
Based on the imagine type, the 4D imaging segment led the market with the largest revenue share of 45.9% in 2023. This segment is expected to continue its dominance over the forecast period owing to technological advancements in 4D imaging technology.
Application Insights
Based on application, the cardiology segment led the market with the largest revenue share of 20.3% in 2023. The growth is attributed to the high prevalence of cardiovascular and congenital heart diseases and government support to improve the accessibility of treatments.
Recent Developments
In January 2023, Bruker Corporation acquired ACQUIFER Imaging GmbH, which will expand its portfolio to include big data management and high-content screening solutions for bioimaging applications.
In January 2023, Canon Medical Systems USA Inc., entered into a partnership with ScImage, Inc. Sclmage provides Cloud-native enterprise image management, PACS and image exchange solutions for the healthcare industry, based out of Los Altos, CA.
In September 2022, King Abdullah Medical City (KAMC), located in Mecca, Saudi Arabia, and a long-term customer of Agfa HealthCare, recently upgraded its image management system to Agfa HealthCare's Enterprise Imaging.
Key Players of Medical Image Analysis Software Market
Koninklijke Philips N.V.
GE Healthcare
Siemens Healthineers
Agfa-Gevaert Group
Toshiba Medical Systems Corporation
Spacelabs Healthcare
MIM Software, Inc.
Aquilab SAS
ESAOTE SPA
Merge Healthcare, Inc. (IBM)
ClaroNav, Inc.
Xinapse, Inc.
Bruker
Order a free sample PDF of the Market Intelligence Study, published by Grand View Research.
0 notes
Text
Harnessing AI: Opportunities and Challenges Ahead
The AI Future: Transforming Our World and Shaping Tomorrow Keywords: AI Future, Artificial Intelligence, Machine Learning, Deep Learning, Generative AI, AGI, AI Ethics, AI Governance, Digital Transformation, Future of Work, Healthcare AI, Education AI, Societal Impact of AI. Artificial Intelligence is no longer confined to science fiction; it’s a present reality rapidly reshaping industries and…

View On WordPress
#AI Diabetic Retinopathy Screening#Automated Eye Exam#Cloud-Based Healthcare#Diagnostic AI#Fundus Image Screening#Medical Technology#Ophthalmology Innovation#Prevent Blindness#Retinal AI Analysis#Telemedicine for Diabetes
1 note
·
View note
Text
Vision in Focus: The Art and Science of Computer Vision & Image Processing.
Sanjay Kumar Mohindroo Sanjay Kumar Mohindroo. skm.stayingalive.in An insightful blog post on computer vision and image processing, highlighting its impact on medical diagnostics, autonomous driving, and security systems.
Computer vision and image processing have reshaped the way we see and interact with the world. These fields power systems that read images, detect objects and analyze video…
#AI#Automated Image Recognition#Autonomous Driving#Collaboration#Community#Computer Vision#data#Discussion#Future Tech#Health Tech#Image Processing#Innovation#Medical Diagnostics#News#Object Detection#Privacy#Sanjay Kumar Mohindroo#Security Systems#Tech Ethics#tech innovation#Video Analysis
0 notes
Text
#Medical Image Management Market Growth#Medical Image Management Market Scope#Medical Image Management Market Analysis
0 notes
Text
The Magic of AI!
Minimax AI - Text to Video Generator (For now it is Free to Use!).
The Text to Video is amazingly simple to use and from what I've seen so far it is unlimited.
There are several other Videos to explore and use their video prompts to generate your very own videos. - Pretty Awesome!

Are you absolutely certain that you want to miss out on the AI Trend?
#minimax ai#Generative AI#Technology Revolution#Machine Learning#Content Generation#Complex Algorithms#Neural Networks#Human Creativity#Original Content#Healthcare#Finance#Entertainment#Medical Image Analysis#Drug Discovery#Ethical Concerns#Data Privacy#Artificial Intelligence#GANs#AudioGeneration#Creativity#Problem Solving#ai#autonomous#deepbrain#fliki#krater#podcast#stealthgpt#riverside#restream
0 notes
Text

Neturbiz Enterprises YouTube Channel - AI-Innovations
Our mission is to provide details about AI-powered platforms across different technologies, each of which offer unique set of features. The AI industry encompasses a broad range of technologies designed to simulate human intelligence. These include machine learning, natural language processing, robotics, computer vision, and more. Companies and research institutions are continuously advancing AI capabilities, from creating sophisticated algorithms to developing powerful hardware. The AI industry, characterized by the development and deployment of artificial intelligence technologies, has a profound impact on our daily lives, reshaping various aspects of how we live, work, and interact. The AI industry presents numerous opportunities for affiliate marketers to promote cutting-edge tools and services. Each Platform may offer different commission rates.
#artificial intelligence #generativ ai
@neturbizenterprises @ai-innova7ions
#Generative AI#Technology Revolution#Machine Learning#Content Generation#Complex Algorithms#Neural Networks#Human Creativity#Original Content#Healthcare#Finance#Entertainment#Medical Image Analysis#Drug Discovery#Ethical Concerns#Data Privacy#Artificial Intelligence#GANs#AudioGeneration#Creativity#Problem Solving#ai#autonomous#deepbrain#fliki#krater#podcast#stealthgpt#riverside#restream#murf
0 notes
Text
youtube
Unlock Your Creative Potential with Krater AI 🚀
Are you struggling to create compelling content?
Introducing Krater AI, your new secret weapon for content creation! With its intuitive interface and powerful features, Krater AI is changing the way we think about content. Say goodbye to writer's block and staring at a blank screen. Whether you're a seasoned writer or just starting out, Krater AI empowers you to effortlessly generate high-quality original content in minutes. From blog posts and social media updates to marketing copy and educational materials, Krater AI helps you captivate your audience with diverse content that truly connects. Ready to unleash your inner storyteller?

#aicontentgeneration #artificialintelligencerevolution
#youtube#krater ai#neturbiz#Generative AI#Technology Revolution#Machine Learning#Content Generation#Complex Algorithms#Neural Networks#Human Creativity#Original Content#Healthcare#Finance#Entertainment#Medical Image Analysis#Drug Discovery#Ethical Concerns#Data Privacy#Artificial Intelligence#GANs#Audio Generation#Creativity#Problem Solving#ai#autonomous#text to video#text to speech#ai scene generator#ai automated editing#innovations
0 notes
Text
youtube
#DCE-MRI#deep learning#intratumoral subregion#Ki-67 expression#breast cancer#tumor proliferation#medical imaging#artificial intelligence#radiomics#oncology#predictive modeling#neural networks#personalized treatment#tumor biomarkers#machine learning#non-invasive diagnosis#MRI analysis#cancer detection#precision medicine#biomedical AI.#Youtube
1 note
·
View note
Text
The integration of artificial intelligence (AI) into medicine is profoundly transforming practices, and this raises important questions about the ability of geriatricians and general practitioners to adapt.
Here is an analysis of the issues
Growing complexity of medicine with AI
Preventive and predictive medicine
AI can analyze huge amounts of data to identify individual risks and predict disease occurrence.
This requires a deep understanding of algorithms and their interpretation.
Diagnosis
AI helps in interpreting medical images, analyzing biological data and detecting complex patterns.
This requires an ability to validate and integrate AI results into the clinical context.
Therapeutic
AI personalizes treatments based on individual patient characteristics.
This involves knowledge of AI-based therapeutic options and an ability to monitor their effectiveness.
Capacity of geriatricians and general practitioners
Continuing education
Continuing education is essential to keep physicians up to date with advances in AI and its applications in medicine.
Interdisciplinary collaboration
Collaboration with AI specialists, data scientists and other healthcare professionals is crucial for effective use of AI.
Decision support tools
AI can provide decision support tools to support physicians in interpreting data and making clinical decisions.
Specificities of geriatrics
Geriatrics, by its holistic nature, is particularly concerned with the management of multiple pathologies and fragility.
AI can be a valuable asset in synthesizing complex data and personalizing care plans.
The role of the general practitioner
The general practitioner, through regular monitoring of the patient, is on the front line to detect changes and refer to specialists.
AI can help refine its diagnosis and monitoring.
In summary
AI represents a challenge, but also an opportunity to improve the care of elderly patients.
Continuing education, interdisciplinary collaboration and the use of decision support tools are essential to enable geriatricians and general practitioners to adapt to this evolution.
General practitioners and geriatricians will have a key role in using AI as a decision-making tool.
Go further
#Adapting Doctors to AI#Algorithms#Biological data analysis#Interdisciplinary collaboration#Increasing complexity#AI-assisted diagnosis#Health data#Continuing education#Continuing medical education#Fragility#Geriatrics and AI#Medical imaging#Integration into the clinical context#Artificial Intelligence (AI) in Medicine#Clinical interpretation#Interpretation of algorithms#General medicine and AI#Predictive medicine#Preventive medicine#Decision support tools#Personalization of treatments#Polypathology#Medical decision making#Role of the general practitioner#Specificities of geriatrics#Patient monitoring#Monitoring effectiveness#Personalized therapy#Validation of AI results
0 notes
Text
5-year survival and prognostic factors for resectable colon cancer: a single institution experience in Lebanon by Ernest Diab in Journal of Clinical Case Reports Medical Images and Health Sciences
Abstract
Background: This study aims to analyze the 5-year overall survival (OS) and the progression-free survival (PFS) of patients with localized colon cancer (CC) and study the impact of various prognostic factors. It is the first study evaluating survival and prognostic factors for resectable CC in the region.
Patients and methods: The medical records of 79 patients at Hotel-Dieu de France (HDF) hospital were reviewed. OS and PFS were analyzed using the Kaplan–Meier method. Results: Advanced stages, advanced grades, and vascular invasion at the time of colectomy were correlated with lower 5-year OS and PFS, showing a statistically significant association. No significant association was observed between cancer sidedness and survival after colectomy.
Conclusion: Survival and recurrence after CC resection remain important problems. Tumor stage, tumor grade, and vascular invasion are prognostic factors that affect survival after colectomy.
Keywords: colon cancer; colectomy; survival analysis; overall survival; progression-free survival; recurrence.
Introduction
Colon cancer (CC) represents a significant public health concern due to its high incidence and severity. It ranks among the leading causes of cancer-related morbidity and mortality globally. In terms of frequency, it is the third most commonly diagnosed cancer in men and the second in women. Furthermore, it stands as the third leading cause of cancer-related mortality in both men and woman (1). The survival of CC depends on the stage of the disease at the time of diagnosis and the response to treatment. The 5-year survival rate decreases as the stage increases: it is greater than 90% for stage I and less than 15% for stage IV. Early detection would therefore be important and effective (2). About 90% of patients with CC are treated surgically (3). Radical surgical resection is the standard treatment for AJCC stage I to III CC. Adjuvant chemotherapy (CT) is given to patients with high-risk stage II and stage III (4). High-risk patients are those with the following characteristics: stage T4, perforation or obstruction, low grade, lymphatic and vascular invasion, less than 12 nodes examined and a high preoperative carcinoembryonic antigen (CEA) (5). Although most patients diagnosed at localized stages (stages I, II and III) recover, 35% develop a recurrence, mainly within the first 5 years (6). Published rates of survival and recurrence after colectomy vary widely (7). In the Middle East, and more specifically in Lebanon, there are very few studies on this subject. Lebanon ranks second in terms of incidence of CC among countries in the Middle East and North Africa (MENA) region with increasing incidence over the past few years (8). Data collection is not easy in Lebanon and the National Cancer Registry (NCR) was inactive for many years due to unstable political and economic situation. Indeed, several data are missing in the Lebanese NCR such as overall survival (OS) and progression-free survival (PFS) after surgical resection of CC.
Our objective is to study the OS at 5 years and the PFS of patients with CC at localized stages after surgical resection in our institution, and this by analyzing the impact of several prognostic factors such as tumor stage, sidedness, grade, size, patient's age at the time of colectomy and adjuvant CT.
Material and methods
Study estimates and sampling
This is an applied survival study in patients who underwent surgical resection for CC at localized stage between January 2015 and December 2016 at Hotel-Dieu de France (HDF) hospital (Beirut, Lebanon). The medical records of 95 patients who underwent primary CC resection were reviewed. The information was collected from the medical records of the patients, present in the archives of the hospital and in the clinics of the attending physicians. The patients were followed and included in a database until January 2022 or until their death if this occurred before January 2022. Primary tumors located at the level of the cecum, ascending colon and transverse colon were defined as tumors of the right colon, while those located at the level of the splenic angle, descending colon and sigmoid colon were defined as tumors of the left colon. The AJCC TNM staging system (8th edition) was used for staging.
OS was defined as the time from resection of the primary tumor to death from any cause. PFS was defined as the time from the date of surgery to the date of detection of recurrence, last follow-up, or death. We excluded patients who underwent surgical resection for stage IV CC, and for a non-neoplastic cause as well as those who had rectal cancer. The final sample included 79 patients who underwent curative resection for stage I, II or III CC (Figure 1).
Flowchart of patients included in the study
Ethical considerations
The protocol and all the study procedures were approved by the ethics committee of Saint-Joseph University in Beirut. The Helsinki declarations of 1963 were considered: respect, confidentiality, and patient anonymity.
Statistical analysis
Data were analyzed using SPSS software version 29. The categorized variables were compared by Pearson’s χ² test, and quantitative variables were compared by the Student’s t-test. OS and PFS were analyzed using the Kaplan–Meier method. P values less than 0.05 were considered statistically significant.
Results
Basic patient characteristics
Among the 79 patients included in the study, 42 (53.2%) were men and 37 (46.8%) were women. The median age of patients at the time of colectomy was 66.1 ± 13.3 years. Table 1 represents the clinical and pathological characteristics at the time of colectomy. Conventional adenocarcinoma (74.7%) was the predominant histological type of resected tumors followed by mucinous-type adenocarcinoma (22.8%) and signet ring cell adenocarcinoma (2.5%). Grades 1 and 2 tumors (79.7%) predominated over grades 3 and 4 (20.3%) and median tumor size was 4.78 cm ± 1.6 (2 - 8.5) (table 1). Most patients had stage II-A CC with a frequency of 34.2%. The distribution of patients by stage is shown in table 1. Most patients presented an absence of lymphatic invasion (82.3%), vascular invasion (88.6%) and perineural invasion (89.9%). In addition, the majority (84.8%) presented a conservation of mismatch repair (MMR) protein expression (table 1). 14 patients (17.7%) presented a recurrence with a predominant hepatic location (62.5%). The 5-year OS of the patients included in our study was 88.6% with a median survival time of 64.8 months. The percentage of deaths was 11.4% (table 1).
Impact of cancer stage on survival after colectomy
The OS rate at 5 years was 100% for stage I tumors, 92.7% for stage II and 73.9% for stage III, with a significant difference (p = 0.02). The median 5-year survival was 76.7 months for stage I tumors, 66.9 months for stage II and 53.0 months for stage III. The PFS was 74.6 months for stage I, 64.6 months for stage II and 48.2 months for stage III. Patients with stage I CC had higher 5-year OS (figure 2-A) and PFS (figure 2-B) than patients with stage II and stage III, with a significant difference (p = 0.003 for OS and p = 0.01 for PFS)
Kaplan-Meier curves of OS (A) and PFS (B) of CC after curative surgery, at stages I, II and III.
Impact of cancer sidedness on survival after colectomy
Clinical and pathological characteristics depending on the sidedness of cancer
Among the patients included, 42 (53.2%) had a right-sided colon cancer (RCC) and 37 (46.8%) had a left-sided colon cancer (LCC). The baseline characteristics of patients with RCC and LCC are shown in table 1.
Patients with RCC were older at the time of colectomy than patients with LCC (67.7 years versus 64.3 years, p=0.26) and the majority were females (57.1% versus 35.1%, p=0.05). A lower BMI was noted in patients with RCC compared to those with LCC (24.6 ± 4.3 vs 26.8 ± 4.7, p = 0.04) (table 1).
The distribution of the different histological types is shown in Table 1. Conventional adenocarcinoma has a higher tendency to occur in the left colon (89.2% vs 61.9%) rather than in the right colon. However, mucinous-type adenocarcinoma has a higher tendency to occur in the right colon (37.5% vs 8.1%) rather than in the left colon. This trend is statistically significant with a χ² test giving a p-value equal to 0.01. The most frequent location was in the cecum (20%) for RCC and in the sigmoid colon (42%) for LCC (table 1).
Tumors of patients with RCC had larger size (5.1 ± 1.7 (2 – 8.5) vs 4.4 ± 1.3 (2.5 – 8), p = 0.05) and more advanced histological grade (31% vs 8% at grades 3 and 4, p = 0.012) than tumors of patients with LCC. The tumors of patients with LCC were mostly stage T1 and T2 (37.8% vs 11.9%, p = 0.05) while those of patients with RCC were mostly stage T3 and T4 (88.1% vs 62.1%, p = 0.05). Patients with RCC had more advanced N stage (38.1% vs 18.9% at stages N1 and N2, p=0.13) and more advanced AJCC cancer stage (38.1% vs 18.9% at stage III, p=0.03) than patients with LCC. Regarding lymph node involvement, the number varied between 0 and 10 positive nodes for RCC, and between 0 and 4 positive nodes for LCC (p = 0.006). No significant difference was observed regarding lymphatic, vascular or perineural invasion between RCC and LCC. A higher percentage loss of MMR protein expression was observed in patients with RCC (23.8% vs 5.4%, p = 0.023) compared to those with LCC (table 1).
Among the operated patients, 8 patients (19.0%) with RCC and 6 patients (16.2%) with LCC developed a recurrence after colectomy (p = 0.74). Regarding the location of metastases, liver metastases (66.7% vs 60.0%, p = 0.7) and peritoneal carcinomatosis (33.3% vs 20.0%, p = 0.7) were more frequent for LCC, while pulmonary location was more frequent for the RCC (20.0% vs 0%, p = 0.7) (table 1).
Survival analysis of RCC and LCC after colectomy
The OS rate at 5 years was 83.3% for RCC and 94.6% for LCC (p = 0.1). Patients with LCC showed higher survival time (69.4 ± 10.1 (45 – 83.8) vs 60.7 ± 16.1 (4 – 84), p = 0.01) than those with RCC. For PFS, the median duration was 57.7 months for RCC and 66.3 months for LCC. Patients with LCC had a higher 5-year OS (figure 3-A) and PFS (figure 3-B) than patients with RCC (p= 0.296 for OS and p = 0.380 for PFS).
Kaplan-Meier curves of OS (A) and PFS (B) of RCC and LCC after curative surgery, at any stage.
Impact of cancer grade on survival after colectomy
Concerning the distribution by grades and the impact on survival after colectomy, the median 5-year survival was 68.8 months for grades 1 and 2 tumors and 48.7 months for grades 3 and 4 tumors (p < 0.001). Figure 4 represents a box plot showing the difference in survival between the 2 groups of grades.
Box plot showing median survival in months as a function of cancer grades at the time of colectomy.
Impact of tumor size on survival after colectomy
Regarding the impact of tumor size at the time of colectomy on survival, we obtained a weak negative correlation with a correlation coefficient equal to -0.2. This result is represented by a scatterplot showing a non-significant correlation (p = 0.09).
Scatterplot showing the relationship between tumor size at the time of colectomy and median survival in months.
Impact of patient age at colectomy on survival after colectomy
By studying the impact of the patient's age at the time of colectomy on survival, we obtained a moderate negative correlation with a correlation coefficient equal to -0.1. This result is represented by a scatterplot (figure 6) showing a non-significant correlation (p = 0.60).
Scatterplot showing the association between patient age at colectomy and survival in months.
Impact of different tumor factors on survival after colectomy
The presence of lymphatic, vascular or perineural invasion at the time of colectomy was associated with a lower median survival at 5 years (table 2). This association was significant for vascular invasion only (p = 0.02).
Association between survival and various tumor factors. Values are presented as mean ± standard deviation. The values in bold are those considered significant for a p value less than 0.05.
Impact of taking adjuvant treatment on survival after colectomy
Patients with stage II CC who received adjuvant CT had a higher 5-year OS (figure 7-A) and PFS (figure 7-B) than patients with stage II CC who didn��t receive CT (p= 0.287 for OS and p = 0.206 for PFS).
Kaplan-Meier curves of OS (A) and PFS (B) of stage II CC depending on taking adjuvant CT.
Discussion
CC is a deadly disease whose spread has accelerated in recent years. Regarding Lebanon, the country has one of the highest colorectal cancer (CRC) incidence rates in the MENA region. Limited knowledge exists regarding the epidemiology and pathological characteristics of CC in the Middle East, including Lebanon. Additionally, there is a lack of data concerning the OS and PFS outcomes after colectomy in this region. The main objective of our study was to analyze OS at 5 years and PFS after colectomy by studying the impact of several factors.
Our study includes slightly more men than women with a ratio of 1.14. This difference in frequency is already described in Lebanon with a higher prevalence of CC in men.
The majority of CC in our study were in the right colon (53.2%). Indeed, since the 1990s, researchers have begun to observe an increase in the prevalence of RCC compared to LCC in several countries and this can be explained by an improvement in the screening system. However, the low percentage of patients with stage I CC in our study (19.0%) is an indicator that the screening system in Lebanon is not yet fully established, and justifies the need for public health interventions (9).
RCC was more prevalent among women in our study (57.1% vs 35.1%, p = 0.005) than LCC. Indeed, women have been shown to have a higher risk of developing RCC than men (10).
Patients with RCC had lower 5-year OS and PFS than those with LCC. But this association between sidedness of tumor and patient survival was not statistically significant (p = 0.296 for OS and p = 0.380 for PFS). Even though several meta-analyses have demonstrated that RCC has a worse prognosis than LCC, recent studies have shown that there is no significant difference in 5-year OS and time to recurrence between patients with RCC and LCC after curative resection (11) (12).
Indeed, a simple comparison of the characteristics of patients with RCC and LCC reveals several significant differences. Patients with RCC in our study had older age at colectomy, lower BMI, more advanced tumor grade, more advanced AJCC stage, higher number of lymph node metastases, higher percentage of lymphatic and vascular invasion and higher loss of MMR protein expression than those with LCC. In fact, patients with RCC have a worse prognosis than those with LCC because they have a worse clinical background. Therefore, to really be able to assess the impact of the sidedness of the tumor on 5-year OS and PFS, it would be necessary to homogenize the history of the two groups.
There was a statistically significant association between the presence of a higher tumor stage at the time of colectomy and a lower 5-year OS (p = 0.003) and PFS (p = 0.01). We can therefore conclude that tumor stage is a prognostic factor for CC.
Regarding tumor grade, patients with a grade 3 or 4 tumor had lower 5-year OS than those with a grade 1 or 2 tumor with a statistically significant difference (p < 0.001). Among our patients, we demonstrated that there was a significant association (p = 0.02) between the presence of vascular invasion and the reduction in 5-year OS, which is consistent with the results of several other studies (13). We can therefore conclude that the tumor grade and the presence of vascular invasion are prognostic factors in CC.
Patients with RCC in our study had a more advanced tumor grade and a higher percentage of vascular invasion than those with LCC, which is consistent with the results of several other studies (11) thus explaining the poorer prognosis of RCC.
We obtained a higher percentage of mucinous-type adenocarcinoma in RCC than LCC. We have not studied the impact of the histological type of cancer on survival, but studies have described a poorer prognosis for mucinous adenocarcinomas (14).
Regarding the size of the tumor, there was a weak correlation between a larger size at the time of colectomy and a lower 5-year OS. But this association was not statistically significant (p = 0.09). However, a recent study showed that tumor size was associated with a poor prognosis of CC and was considered a risk factor for recurrence and metastasis (15).
The median age of the patients was 66.1 years. Investigating the impact of patient age at colectomy on survival, we found a moderate correlation between older age and lower 5-year OS, but this association was not statistically significant (p = 0.60). This can be explained by the fact that intraoperative complications and postoperative morbidity are higher in elderly patients.
Among the patients included in our study, a total of 34 patients (43.0%) received adjuvant CT. To study the impact of taking adjuvant CT on survival, we focused on patients with stage II CC. Among the 41 patients (51.9%) who had stage II CC, 16 (47.1%) was at high-risk and received adjuvant CT: 10 (62.5%) had stage T4 cancer, 5 (31.3%) had lymphatic or vascular invasion, and 1 (6.3%) had an occlusion. We found that adjuvant CT improves the prognosis of patients with stage II CC, result that is supported by previous studies (16). However, detailed date on the type of CT have not been taken into consideration in our study.
Loss of expression of MMR proteins was more frequent in RCC (23.8% vs 5.4%, p = 0.023) than in LCC, which is consistent with previous studies (11).
Indeed, we did not analyze the impact of the loss of expression of MMR proteins on survival, but a recent study showed that adjuvant CT was a poor prognostic factor for stage II RCC with loss of MMR protein expression and therefore patients should know the MMR protein expression status before receiving adjuvant CT (11).
A significant difference (p = 0.04) in BMI between patients with RCC and LCC was observed. Indeed, it has already been shown that patients with RCC have a lower BMI than those with LCC, probably because most patients are women and have an advanced age (11). In our study, we did not analyze the association between BMI and survival, but studies have shown that a high BMI is a good prognostic factor for CC (11) probably because patients who have a low BMI have very little visceral fat to cover the tumor which can cause it to spread rapidly.
Conclusion
CC is a major public health problem in Lebanon and the incidence is likely to increase over the next few decades. Survival and recurrence after CC resection remain important problems, and early detection is very important. Our study is the first evaluating survival and prognostic factors for resectable CC in the region. Although there was no significant association between cancer sidedness and survival, patients with RCC have worse prognostic factors. We found that tumor stage, tumor grade as well as vascular invasion at the time of colectomy are prognostic factors that affect survival after colectomy in the Lebanese population. However, further studies would be interesting to carry out on larger samples.
#colon cancer; colectomy; survival analysis; overall survival; progression-free survival; recurrence#Journal of Clinical Case Reports Medical Images and Health Sciences
0 notes