#even just sensory stuff like i used to throw up every time i ate a banana but then i started eating them bc of convenience
Text
deleting my long post to rephrase it to this: some of yalls reactions to the club thing is immediately shut down something you've never experienced and have a lot of misconceptions about (like i've seen multiple people say they've never been to the club because they don't do fun things like have themes). and i think. you should be more open to new experiences. you don't have to like the club or even really go to the club but shutting down the idea of doing a whole category of activity without ever trying it is just going to shut you off from experiencing new and potentially enjoyable things.
and this also happens like. pretty much every time a "you should do this thing that i think is fun" post starts making the rounds it becomes about how it's soooooo unreasonable to expect the mostly adult userbase of this website to try new things and be open to new experiences just because people on here have social anxiety or sensory issues or xyz other thing that makes it harder to do some things.
but they also have this extremely strong aversion to experiencing anything unpleasant at all. like i've seen people on that post talk about how they can't watch tv where characters die because it's upsetting. but the thing is if you never experience things that are unpleasant you are going to be that same person forever.
like it fucking sucks to hear for me to this day but the only way you can get over your social anxiety is by doing things that cause that anxiety. and you should never be forced to do them. you should choose to. but you have to do them or the anxiety will literally just get worse forever. do it scared. do it alone. do it while crying, even. but do it. i used to burst into tears at the idea of going up to a cashier to pay for my stuff. and i don't anymore because i did it scared and alone and while feeling like i was going to pass out.
this isn't really about the club. it's about the way people on here react to literally any post that says something along the lines of "you should do stuff"
#alexis.exe#like yeah you have xyz issue#sick list of symptoms now try humanizing your behaviour dot post etc#also genuinely think a lot of people on here were not socialized properly#and thats not your fault but it is unfortunately your responsibility#like yeah tumblr is the weird outcast loner website but like#you cant go through your entire life like this bestie you have to do the thing that sucks and reap the rewards of like.#experiencing new things#and growing as a person#even just sensory stuff like i used to throw up every time i ate a banana but then i started eating them bc of convenience#and now i dont#still not the most pleasant texture#but like genuinely. the texture is not going to kill you#not telling you to force yourself to experience textures you can't stand#i am saying however that sometimes the bad thing is actually not that bad#hell sometimes i've tried a foot with a detestable texture years later and found that it's literally fine and i had no issue with it#sometimes i try things i hated after years and it turns out i actually like them#i periodically try foods i cant stomach again just in case i've changed my mind#literally just please be open to new experiences at least#you dont have to re try things you hated but at least try things you haven't tried#it will improve your life. it's good for your brain. you need enrichment
0 notes
Photo

"When I woke up that morning, I felt good, like REALLY good.
My vision felt super sharp, I woke up really easily, I just felt good.
But when I went to the bathroom and tried to get ready for school, I kept accidentally breaking things.
First, I kid you not, I accidentally broke the cabinet mirror off the frame.
I panicked when that happened, and then my hand was stuck to it for a minute!
I was like, 'what is going on?!?!'
So then I reached for the doorknob and it broke off.
That was when I suddenly remembered what had happened the day before...
My bite didn't hurt anymore, and I had these patterns.
I had to think up some stupid excuse about where they came from, so I went with henna tattoos.
I even bought a kit for it later just to make it that much more convincing.
So yeah, um, explaining that both the mirror and the doorknob broke at the same time when I was trying to brush my teeth was funny.
But like, Ben and May's first thoughts obviously weren't gonna be 'Oh huh, maybe our nephew has super powers all of a sudden.' "
You know what I mean?
Hah hah!
Yeah, so they just thought it was...pfft...a -- a whacky coincidence.
After I destroyed the bathroom -- hah -- I went back to my room and kinda started panicking?
Sometimes when I walked, my feet would catch on the floor, 'cos of the hairs.
And I could hear everything.
It wasn't like everything I heard was hurting my ears, I was just hearing a LOT.
The fabric of my shirt against my skin, the tiniest rustles, and at one point May, I think, walked by my bedroom and I could feel her footsteps.
It just felt like I was tingling all over with all this...uh...sensory input, it was dreadful.
I could've probably heard a bird fart outside my window, okay, not gonna lie.
Well in that time, I totally forgot that I had to go to school.
So Ben knocks on the door -- which scares the shit out of me -- and is like 'Peter, you ready? Are you gonna eat?'
And I was like, CRAP!
So I had to fight with my clothes a little but I threw on a random outfit, ran a comb through my hair and skipped breakfast, and didn't have my teeth brushed on account of breaking the bathroom.
I mean I was hungry, but that wasn't really my priority.
I barely even ate at lunch, I just couldn't stomach it.
When I came out of my room, Ben was like, 'You don't look so good, bud,' so I told him I thought I actually slept too much, because I had gone to bed at like eight the night before.
Said I just didn't have my head in the game.
When we got in the car...
Oh, my god.
Every little noise, every -- every little...THING, it was just, like...
I mean it felt like I'd never ridden in a car before.
The buckle startled me, the windows being adjusted startled me, and I could still feel and hear all my clothing shifting on my person, and feel all these little vibrations.
When we shut our doors I about wet myself, it was -- it sucked, okay, hah hah!
For one thing, I'm shocked I didn't break the door, but...
Again, though, nothing was hurting me; it was just SO much to take in.
I could only guess that this was what it felt like to be hungover without the headache, dizziness and nausea.
Basically, in my vicinity, if it could be heard or felt, I heard and felt it.
On the way to school I was...
Oh -- it was SO messed up.
Ben was trying to talk to me and I had to force myself to pay attention.
All the colors of everything seemed a tiny bit enhanced, and again my vision, it was just SO crisp.
So I'm looking at all these cars and people, hearing way too many peoples' music jamming, Ben had the radio on kinda low, and holy -- when we were in idle, WOW.
I could feel that vibration all over my body.
Vibrations can get really painful for me after a bit, but in the car I was just sort of irritated.
I started having major anxiety about school, because I knew that was going to be a sensory overload.
I was right.
Paper rustling, feet scuffing, the talking, ALL the vibrations of people walking.
And like, at one point during the day, there was a spider somewhere, and the freaky thing was I knew it.
I could feel it, it was weird.
It was impossible to concentrate, then Ned was trying to hang out with me and I was just like '...!!!'
UHH!!
Hah hah!
He was like 'Dude, are you okay?'
And I was like 'Yeah, I slept bad, had some messed up dreams,' and then tried to make myself focus.
I really thought about telling him, I really wanted someone to know because I was so scared.
I started wondering if I was slowly transforming into a spider, or if I was going to get sick or die or if this was actually just it.
Couldn't tell if I'd mutated or was still mutating, it was scary.
So you have all this sensory input, school work, and trying to keep it a secret.
Honestly, I'm not sure why I felt the need to hide it?
It would've been different if I was fighting crime, but I wasn't.
I was just a kid that got bit by some spider because the scientists at the tech center were really negligent, apparently.
But yeah, I was really scared.
In English class, we were studying and everyone was kinda whispering to each other.
So the teacher comes up to me and he's like, 'Pst, Peter. You okay?'
And I was all nervous but was like 'Yeah, why...?'
He goes, 'You look like you need to throw up...out of both ends.'
HAH hah hah!
I just looked around because I could hear him SO clearly, I thought surely EVERYONE else in the room could hear him.
They didn't, though, so I just told him I slept bad.
He asked if I needed to go to the nurse, I said 'no.'
He kinda lingered there for a minute, I think he thought I was on drugs or something, but he finally left me alone.
It was a few days before I realized my sticky hands and feet meant I could literally climb anything.
So I did that in my room.
I started spending more time in my room, because I was trying to figure out what all I could do and stuff.
Ben and May were like, 'Why are you always in your room all the time?'
And I told them I just needed some alone time, or I just needed to de-stress from school.
Which was true, I mean besides Flash traumatizing me on a daily basis, the sensory input was just...too much.
I needed to just be somewhere quiet.
Well when I told Ben this, he just smiled and was like 'Ohhh, I getcha. Just remember to lock the door,' and I was just like...
Ben...
No...
I couldn't figure out why I had the markings on my wrists, but then I started getting these urges to make -- you know, my little...rock and roll-looking sign that I do?
So I did that, and a frickin' web shot out!
So I had this big web thread in my room and had to tear it down, and I was just in there freaking out like HUH?!
And that was how that started.
Then came the reflexes, the spidey-sense, all these crazy little things, weird urges that I had to not react to, like how I clean my face and stuff.
I had to re-learn how to deal with my environment.
I got used to it after a couple weeks, and something that really helped me -- and still helps me now, is just focusing on one little thing.
I can tune out a LOT of stuff most of the time, which is good.
When I started getting the hang of it was when Ben died.
I felt awful, like you know, because I thought I should've stopped it from happening -- and I still feel that way.
But what was really hard also was the fact that...he never knew, and I never got to tell him about my powers.
I wanted to tell everyone, but like I said, for some reason I just...didn't.
And then when Ben died, I was sad, because I thought it would've been nice to tell him before that happened.
But looking back, I also feel like maybe if I had told him, then I'd be miserable because the one person I told died, and it, that...
It's like a damned if you do, damned if you don't sort of thing.
There was really no winning with that.
So when he died, I felt really guilty about him having not known about the powers, so every day I'd say to myself 'I have to tell someone, I have to tell someone,' but I knew Ned couldn't keep it a secret and May was having a hard time with Ben, and I didn't wanna stress her out.
Then I thought about the mutant school, Xavier's school, and thought about how my life might change and how I didn't want that.
Then I started fighting crime, and it was like...
Well I can't tell anyone now, because it wouldn't be safe for May or Ned, or anyone who got close to me.
And yeah, all this going on on top of puberty?
Fun stuff!
Loved that.
It was...it was a tough year.
But I figured it out, it's good now.
Everything's good, finally.
I feel good.
I'm really happy, I feel really...blessed, I guess?
It's good, I love my life now, hah."
--------------------------------------------------------------------------------------
--------------------------------------------------------------------
------------------------------------------------
(having Autism totally be like ^)
XD
Like the sensory thing but actually agonizing.
14 notes
·
View notes
Note
What are your headcannons for the kids from the four main All the Wrong Questions series?
oh geez there are so many
Lemony Snicket
Listen every character in the Snicketverse is autistic but Lemony? HIGH.KEY. This boy cannot stand sensory overload and also stims with verbal recitation.
After several months in Stain’d-by-the-Sea, the Associates got used to him just showing up and taking food. He eventually stopped asking, and then eventually stopped using the door. Moxie has, more than once, come downstairs to find him sitting on her counter eating cereal.
Beatrice snuck into town once to see how he was doing, saw him and Moxie trying to jump off the roof of the diner with a tablecloth parachute and Jake dragging them back and screaming, and she just turned right the fuck around and reported to their friends, “yeah he’s fine.”
Kit made him promise not to tell Jacques that she was almost in jail.
MODERN AU: Gets into twitter and tumblr fights with obvious trolls. Tried to call CPS on Theodora just to see what would happen. Can recite any “Unraveled” YouTube video on command. Has an extensive knowledge of Pokemon.
Moxie Mallahan
listen this girl is a lesbian in denial and she wrote Ellington Feint a note that said “get out of my town” because she didn’t know what else to do
She always kinda knew that her Mother was never coming back for her, but she didn’t admit it aloud until after Lemony left.
Moxie: I can eat ten marshmallows at once. Kellar: You are a hazard to yourself. Lemony: And a coward. Do twenty
Moxie knows how to pick every kind of lock, and how to break into every window. She takes her journalism very seriously and will get the truth even if she has to flip the world off as she does it.
MODERN AU: Blogger. Once spent a week straight putting together a project and then passed out for forty-eight hours. Still carries a typewriter with her everywhere. Had to physically stop Lemony from eating a tide pod.
Ellington Feint
Had literally no idea Lemony had a crush on her because she’s just that gay.
Actually popped up around town inbetween books constantly, mainly to chill with Cleo, Jake, the Bellerophons, and even Ornette. They just all neglected to mention this to Lemony.
She doesn’t remember anything about her mother. All she knows is what her father told her; that her mother used to make music boxes, loved coffee, and died in a fire.
Goes through a huge rebel/outlaw phase after escaping with Kit, because she’s completely lost and has no idea what to do or who to trust; her own father never gave a shit about her, as she now knows, so how could anyone care? Eventually she made her way back to Stain’d-by-the-Sea, where Moxie found her crying in the attic of Black Cat Coffee and awkwardly invited her to live in the lighthouse.
MODERN AU: Has been on the run from CPS for so fucking long. Quotes Gilmore Girls almost daily and will argue your ear off about why Rory/Paris should’ve been endgame. Once ate a tide pod. Cries while watching the Addams Family.
Kellar Haines
Even after the Train Incident, he basically lives with Moxie. He just can’t trust his Mom anymore, and while he claims otherwise, they didn’t really have a good relationship before then, either. Lizzie stays with him.
His special interest is in codemaking. He would’ve been really valuable to VFD if he’d gotten recruited. As is, Moxie kicks the ass of anyone who tries to kidnap him, so he’s fine.
He’s also super good at crafting, and can make really cool art projects whenever he has the time. Lizzie used to give him art supplies whenever she could, and still hangs his drawings on the lighthouse fridge.
He just gets so tired of his friends’ shit. He’d be a Mom Friend if he made any effort to stop them but as is he just kinda watches crap go down.
MODERN AU: Constantly goes to the movie theater just to chill. Addicted to YouTube. Is the only one of the squad not freaked out by the Watership Down movie. Asks existential questions at random to scare the squad and then immediately says “yeet” in a deadpan voice and throws Squeak across the room.
Pip and Squeak Bellerophon
They took over the taxi for their Dad when he fell ill. He died a few months later, and they kept claiming he was alive, in fear that they would get separated by whoever was in charge of their case. The only person they told is Jake, because he eventually followed them home to ask their Dad why the fuck he didn’t feed them and found that they were living alone, and Cleo, because Jake can’t keep secrets from her.
Pip and Squeak used to fight a lot, though they never intended any real harm. They slowly stopped after they started living alone, and Pip started kinda taking charge of keeping him and Squeak safe.
They used to be very tight with Qwerty, because they were constantly at the library. He suspected their situation, but never confirmed it and was alright just making sure the kids were okay. Squeak would sometimes climb on the bookshelves and knock them over, but thankfully Qwerty thought this was funny.
Squeak likes to “adopt” stray animals he finds in the backyard. Whenever he walks in going “gUESS WHO OUR NEW SIBLING IS,” Pip has to guess whether he’s going to bring in an injured baby bunny he can nurse back to health, or a squirrrel he just caught who is still struggling and about to destroy half the house.
MODERN AU: Pip has a Nintendo Switch that Squeak can only play Animal Crossing on. Squeak keeps posting photos on Instagram of him and Pip driving illegally but everyone thinks they’re edits. Squeak once very seriously told Pip that he would have to marry Jake so they could keep getting free food from him (before they found out he was dating Cleo). Have slept in library closets before and will again.
Cleo Knight
Identifies as Demi-bi. She and Jake met as preteens, when she wandered off and got lost, and went into the diner to use the phone and call Zada and Zora. Afterwards, she kept sneaking out to visit him.
Was much closer to Zada and Zora than her parents. She used to hang out in the kitchen with them, laying on the counter and practicing calculations or studying advanced chemistry while they cooked.
Also very very autistic. Can only eat certain things, because she has huge texture problems. Only Zada, Zora and Jake have ever gone out of their way to accommodate her without complaint.
Is incredibly reckless and never thinks anything through. While everyone knows she can take care of herself, it’s still nerve-wracking to see her run out the window, leaving only a note saying she’ll be back in three hours after trying to find a chemical, and coming back covered in blood that’s not her own.
MODERN AU: Was a Guardians of Ga’Hoole kid. Would exist on a diet of cheetos, cereal and sprite if not for her boyfriend. Once, Ornette helped her break out of the house to go to the movie theater to watch Lego Batman. Super into Stranger Things.
Jake Hix
Literally is the only reason the Associates are still alive. He gives them food and makes sure they don’t kill themselves doing some stupid reckless stuff.
Surprisingly, though, Cleo has had to physically stop him from fistfighting S Theodora Markson, who keeps forgetting to feed her fucking apprentice
Jake: As soon as I hit 18 I’m adopting you. Pip and Squeak, not even glancing over: Lit.
Has been in love with Cleo since they met. Since their relationship is technically “secret”, Hungry pretends not to notice, despite how increasingly obvious it gets. She knows she should technically discourage this, but he’s just. so in love. When he’s not working, he spends his time in him and Cleo’s garden.
MODERN AU: Has threatened to put parental locks on Lemony and Moxie’s phones multiple times. Keeps quoting The Princess Bride at Cleo, to the annoyance of the other Associates around them. Actually super into Doctor Who. Also keeps beating everyone’s ass in Mario Kart.
Ornette Lost
Has never once understood what was going on, but honestly she just rolls with it. “Guess we’re doing this now? Okay.”
Keeps bringing stray cats into her Uncles’ house and adopting them. She has twelve now. There is no stopping her.
Super close with Cleo and Jake. Mainly because she doesn’t mind third-wheeling, and will just fold origami when she gets bored, but also because she’s pretty good at dropping life advice and also is shockingly hilarious.
Lemony: Ornette. Why did the toaster blow up. Ornette: Hm?Lemony: Toaster. Blew up. Ornette: Oh. Yeah I blew it up Lemony: why Ornette: ¯\_(ツ)_/¯
MODERN AU: Very into anime, especially Fullmetal Alchemist. Lives on ice cream. Has OPINIONS on the Disney Reboots. She got expelled from school because she graffitied GAY RIGHTS on the side of the building, and then a couple of middle fingers.
Lizzie Haines
INCREDIBLY protective of Kellar. She had more part in raising him than their mother; she was reluctant to leave him for her apprenticeship, but he convinced her he’d be fine.
Sharon was a huge perfectionist in regards to Lizzie’s talents and studies, so Lizzie always felt very distant from her. When she left for her apprenticeship, she ended up bonding with Sally Murphy, to the point where Lizzie saw her as more of a parent figure.
Lizzie noticed suspicious activity going on around town, and started investigating, even though Sally didn’t think anything was wrong. Lizzie had a conspiracy board and everything. She was kidnapped just as she was piecing everything together.
It took her quite a few months to break out, but once she did, she immediately went hardcore and figured out how best to knock people out and keep them away from her. She had a lot of trauma that emerged after the Train Incident, but Kellar got very good at figuring out how to calm her down.
MODERN AU: Hangs Christmas lights around her room and glowing stars on her ceiling. Knows more about Sonic the Hedgehog lore than the other Associates could ever understand. Huge Marvel/Star Wars fan. She has memorized all of Chicago, Hairspray, Black Panther, The Empire Strikes Back and Mamma Mia.
#all the wrong questions#atwq#lemony snicket#moxie mallahan#ellington feint#kellar haines#pip bellerophon#squeak bellerophon#cleo knight#jake hix#ornette lost#lizzie haines#stain'd associates#mine#ask#anonymous
79 notes
·
View notes
Text
Caretaker
Summary: Autistic! Sides! Logan is a little too caught up with his work and Patton reminds him to look after himself first.
Pairing: Platonic logicality
Warnings: Food mention and that’s it I think!
Tag list: @mutechild @super-magical-wizard
A/N: I know this isn’t a whole lot on its own, but I wanted to do some autistic sides content so I thought (read: hoped) it was good enough. I was thinking I could (over time) write one for Patton taking care of/helping each of the sides in different ways and then one of them all helping Patton, cause I love stuff like that.
AO3 Link
"Logan? When was the last time you had something to eat?"
Logan looked up from his laptop blankly, blinking as his eyes adjusted to the dim light of the room. He was aware Patton had said something, but he wasn't 100% sure what exactly it was he had said, his mind far too caught up in his work.
He'd had the perfect idea for his astronomy paper earlier that morning, right in the middle of drinking his first cup of coffee, and had immediately wrapped himself up in getting it all written out and edited. The fact that the paper didn’t need to be handed in for another month was mostly irrelevant. It would certainly be useful to be a little bit ahead of the other students, plus this idea was far too good to let slip away regardless of the due date.
"I'm sorry, what was that, Patton?" Logan adjusted his glasses, semi-absentmindedly taking in his roommate’s form in the partially darkened room.
Patton was sitting upright in the armchair across from Logan—presumably indicating a serious discussion—leaning forward slightly—likely to show engagement in the present conversation, potentially also to appear less intimidating—and giving a—reassuring? kind? worried?—smile. All relatively common body language displays from him; nothing too out of the ordinary.
Logan wasn’t entirely sure when he’d arrived in the position he was in but, taking into account Patton’s almost constant sensory seeking and the lack of stim toys or blankets in his possession, Logan would assume it hadn’t been long.
"I asked when you'd last had something to eat, Lo," Patton said, tilting his head to the side—curiously? interestedly?
Logan hummed, returning his gaze to his paper, only vaguely continuing to pay attention to Patton. "Virgil brought me a chocolate bar not too long ago."
He skimmed the paragraph he’d just written, quickly refamiliarising himself with the point he was attempting to make.
"And did you eat it?"
There was something in Patton’s tone that made Logan pause. Of course, he'd eaten it! …hadn’t he? Chancing a look down at the table in front of him, Logan caught sight of the whole, still wrapped chocolate bar Virgil had brought him—sitting in plain view of Patton. Oh.
"It would appear not."
Logan watched as Patton sighed, scrunching up his face a little—in pain? annoyance? really, he had no idea—before speaking again. “Lo, I know you’re still kinda hyperfocusing but do you think you could come with me to grab some food?”
“Why would you require my companionship in order to eat?”
Patton screwed up his face again and Logan had a distinct feeling that he wasn’t grasping something that was vital to his understanding of this conversation. Truthfully, that was how Logan felt about most conversations, however, this was something beyond the realm of his regular confusion.
“Sorry, I didn’t phrase that well.” Patton began to scratch lightly at the chair he was sitting on. Logan’s mind immediately latched onto the sound, almost entirely blocking out Patton’s next words. “I meant, can you come with me so I can get you something to eat? Please?”
Logan blinked. He shut his laptop, recognising this was something he should appear slightly more involved in, even if he wasn’t entirely sure of the reasoning. He desperately wanted to continue working on his paper—he was halfway through a really interesting train of thought that he didn’t want to lose—but he owed Patton more than that.
“Why?”
Patton didn’t look offended by the question—he knew Logan wasn’t being snarky, he was genuine.
One of the best things about having entirely neurodivergent or autistic roommates was, despite them having their own difficulties and strengths, they were at least all aware of the things the others struggled with.
For example, Virgil had the most trouble with verbal communication, as well as having issues with becoming easily emotionally overwhelmed. Because they knew this, it resulted in the three of them being more cognizant of situations that could prove to be challenging to Virgil, or for that matter, any of them.
The level of communication in neurodivergent circles, Logan had found, was infinitely superior to the level of communication in neurotypical circles—something he personally appreciated a great deal. It was impossible to comprehend what people were trying to get across if they didn’t simply say what they meant; he didn’t understand this obsession neurotypicals had with making conversations more difficult than they needed to be.
“I’m worried about your wellbeing, that’s why,” Patton replied, pausing his scratching to pick up a stim toy from the table in front of him, “You haven’t eaten all day.”
“All day?”
Logan frowned. That seemed like a curious choice of words. After all, it could only be… What? 12 pm at the lates-
“Lo, it’s 8 pm.”
Ah, there it was.
At the revelation of the amount of time that had truly passed since he’d sat down to begin his paper, Logan abruptly became more aware of his surroundings, almost as if being pulled out of a dream. The appearance of the room, though once so hazy and unimportant, was forced into clarity and Logan had to take a second to process.
It was dark. He had noticed it was dark and yet he hadn’t until this exact moment realised the significance of that. It was also quiet—good for his focus, presumably not very good for his awareness—so he could assume that Virgil and Roman had retired to their own rooms.
His alarms had probably been going off all day and he hadn’t paid them any attention in the slightest. He couldn’t remember the last time he’d had something to drink. Was it that coffee this morning? His throat was so dry, he was lucky he didn’t have a headache.
Patton’s concern seemed infinitely more warranted now.
Logan furrowed his brow, sucking his bottom lip into his mouth. “I see.”
“Mmhmm,” Patton hummed. He threw the stim toy back onto the table before bouncing up out of the chair and over towards Logan. “So, you okay to come and get food with me now? I might even throw in some Crofter’s for dessert…”
If Logan wasn’t already prepared to accept Patton’s suggestion of food, the mention of his samefood certainly would have been enough to get him there.
He wondered, with enough convincing, whether Patton would make him Crofter’s waffles for dinner. Normally Logan felt very strongly about only eating breakfast foods for breakfast, but considering this entire day had been a disaster as far as routine was concerned—and if Logan thought about that for more than a second his chest started to tighten and his hands started to twitch—he supposed he might as well ask.
It would throw his whole week off, no doubt, but quite honestly, he felt like today was going to accomplish that whether he ate waffles for dinner or not. And at the present moment, Logan was willing to risk it regardless, solely to obtain a fraction of the comfort Crofter’s waffles brought him.
He stood up from the couch, wincing slightly at the way his muscles protested the movement. Despite all the work he’d managed to get done, staying in essentially one position for over ten hours definitely had its disadvantages. “Yes, Patton. That would be ideal.”
Logan threw in a, “thank you,” for good measure—it always paid to show gratitude to people when they were doing you a favour, and Patton appreciated good manners.
It was the kind of thing Logan had come to realise was quite important when sharing a living space with someone. He couldn’t say he had been all that polite in the past, but every time Virgil left his dirty dishes in the sink or Roman woke him up by singing Disney songs in the hallways, Logan understood Patton’s perspective just that little bit more.
Patton lit up at the response, his face breaking out into a grin and his whole body doing a small wiggle—happiness; that one Logan was absolutely sure of. He’d had enough exposure to Patton’s pleased stims to be able to recognise them when they happened.
Plus, he may or may not have whole sections of his notebooks dedicated to his roommates’ stimming habits—as well as sensory preferences, triggers and anything else Logan deemed important—but that was neither here nor there.
“Good,” Patton said brightly and before Logan even noticed he was moving he was grabbing a hold of Logan’s hand and pulling him into the kitchen.
#sanders sides#sanders sides fic#logan sanders#patton sanders#platonic logicality#logicality#autistic sides#lo can write#(also if I did continue it#which I probably will even if it takes a while#would y'all prefer I kept it platonic or made it lamp?#cause I'm cool with either)#I realised just as I was falling asleep that I forgot to add warnings#like there really weren't any I don't think but still#had to come back downstairs and boot everything up to do that hahah
373 notes
·
View notes
Text
beauty in the eye of the beholder (ugly in our own eyes)
My mother didn’t get married until she was 37 years old.
She went to school first. Had a career. She was one of the first female stockbrokers in Boston, you know. So smart. So amazing.
She met my father through a school project in business school. She didn’t go until her thirties. He’s younger than her. Three years.
My mother had me when she was 39 years old. A few months from 40. My younger brother is born a month and a half before her 43rd birthday. We are both happy, healthy babies. Full term. More than, in my case - I was 2 weeks late.
My mother is a small woman - 5’ 2”, a bit curvy. Thin, at least in my opinion. She works out religiously. Swims almost every morning. She swam a mile every day while pregnant - both times. She’s healthy as a horse.
My mother is in very good shape, but I have never seen her with abs. She has muscles - she’s strong - but her tummy is covered, no muscle showing through.
My mother dieted my whole childhood, trying to get the “perfect figure”.
Here’s the thing - my mother was never fat. Not even a little. Her stomach wasn’t soft because it had fat on it - it was skin. Stretched out, from two late-term pregnancies she had in her near-40s. A woman’s body is amazing. She made two people. From scratch. But the older you get, the less you can “bounce back” from pregnancy. She lost the weight. She didn’t lose the skin, the saggy breasts, the slightest of stretch marks.
I was always a really skinny kid. The smallest in my class for years - competing with Paige, the next smallest kid. Every once in a while, I would be a centimeter taller than her. She always overtook me again.
She was never skinnier than me. I was always the lightest.
I had trouble with food, growing up. Still do. But it’s not about fat, not for me. Some people have sensory issues. It’s common in people with autism. Less common in ADHD, but it’s seen. I don’t know if my ADHD is why I have food issues, but I suspect it’s a part.
When I was ten years old, I thought I was fat.
It’s ridiculous. I was the skinniest kid I have ever known. You could measure my body fat percentage in the single digits. (That’s an exaggeration. That would be malnourishment. I was not malnourished. I was just skinny.) But every child that age has a little bit of tummy. It’s partly weight gain preparing for puberty, partly just your organs, like, existing. Your diaphragm expanding so you can breath. Stuff like that.
But my mother had a tummy. It wasn’t fat, any more than mine was, but she hated her tummy. If mommy hated her tummy, so should I. I hated my tummy because I’d learned that tummies were a bad thing to have, no matter the reason.
About a year and a half ago, I spent two months living off cinnamon rolls. I should not have done that, obviously - it’s not healthy for all sorts of reasons - but I was coming off a bad few months and I liked the comfort in making and eating them. I got them from a can. Jumbo size. Extra flaky. I would make a bunch of extra icing for myself, because the amount they give you is never enough.
I ended up gaining about 30 pounds without noticing it. I finally realized right before an important photoshoot I had. I looked at my body for the first time in months and realized that I had stretch marks. I’d never had them before. They’re still there, on my thighs and ass. I like them, honestly. My mother hates them - I can’t wear shorts around her anymore. She’ll bring it up. No matter what.
I decided that, while I liked my stretch marks and didn’t mind gaining weight, for both health and career reasons I needed to lose some of the weight I’d put on. I went from 115 to 145. Looking back at myself, I decided that I liked how I’d looked and felt around 125. I didn’t push myself. I ate healthy again. (Mostly.) I worked out a little. Bit by bit, the weight came back off. In about 6 months, I’d gotten myself down to 130. I’m still there, trying to lose those last five pounds, but I’m okay. It’ll happen when it happens.
My mother was horrified to learn I’d gained weight. She immediately insisted I lose it immediately. I admitted I was at 145 - she told me I needed to lose 40 of it. I was a little shocked - I explained I hadn’t weighed that little since I was 17. I’d been at 115 for a few years by the time I gained the weight. I liked having a little extra, by the way, I didn’t want to lose all of it. Just some. I considered going to 135 just to spite her. I didn’t.
She never once used the word “fat”. Every time I tried to complain that I was uncomfortable with her bringing up my weight, encouraging me to lose it, that she made me feel like she thought I was fat - she’d always say, “I’ve never said you were fat!”
She still brings up those last five pounds every time she sees me. I’ve learned to ignore her. I’m comfortable in who I am - I learned to love my body (if not my mind) some time in high school. I had self-image issues in middle school, but they mostly stemmed not from being “fat” but “bald”. Actually - I shouldn’t even be using quotation marks there. I was half bald for a few years. Alopecia areata. My mother, thankfully, never made me feel bad about that. I eventually learned that I could be beautiful no matter what. That beauty itself shouldn’t always be the goal - healthy and happy is more important.
It still makes me uncomfortable when she brings up my weight. I didn’t learn to not be hurt by her comments - just to tune them out. It’s not the same thing.
If I had been a fat kid. If I had been chubby and overweight growing up, hearing my mother talk about all the diets she was on to get rid of her nonexistent belly when mine was twice her size, if she’d been pressuring me to not gain weight, lose a little, just five pounds, the whole time I was growing up… I’m not sure I would have handled it as well as I’m handling it now.
Actually, scratch that. I know I wouldn’t. I would have caved by the time I was 9.
I would have been dieting my whole childhood, trying to lose that weight, hearing how ugly I was without that word being used once, so it couldn’t be thrown back at anyone. Middle school, which was awful enough for me as a super skinny kid, would have been a complete disaster. I have no doubt my preexisting food issues would have morphed into a full-blown eating disorder. Probably anorexia - I hate throwing up.
There are so many little girls who are in that spot, right now. I skipped it due to pure luck - I was skinny because I had good genes and didn’t eat much and had a fast metabolism. Lots of girls don’t have that kind of luck. And my mother is not unusual. She isn’t the exception - she’s the rule. While she was dieting my whole childhood, so were all her friends. The mothers of my classmates. My female teachers. All of them, constantly trying to be thin.
I’m not sure where I was going with this in the beginning. I think my point was about little girls absorbing their mothers’ opinions on weight. How every time a mother talks about how fat she is, even when she isn’t, in front of her daughter, her daughter learns that being fat is bad. More than that - that being average is fat, and to be truly beautiful you have to be perfectly skinny.
There - that’s my point. That being average has become being fat, and as we all know, fat is bad, so being average is bad. It’s gotten to the point that little girls who aren’t fat, aren’t even average, but are skinny as hell still think it’s not good enough. They’re still fat.
Because they are here, and they are female, and they have a body, they are ugly.
I think there’s something wrong with that.
Don’t you?
31 notes
·
View notes
Text
Prompt by anon: Could you write something where virgil has disordered eating? (Like anorexia, bulimia, etc.) Only if you want to! (I know this is a triggering subject for some people)
(Hey, please be careful going into this. I don’t have an eating disorder but i do have several issues, mostly tied into anxiety and also sensory stuff. If any of this might be triggering or otherwise harmful to you I’d prefer you not reading it. Stay safe out there)
Virgil centric
Warning: Eating disorder, food talk, food issues, sensory issues, anxiety, nausea/vomiting
Wordcount: about 1k
Read on Ao3
---
Breakfast.
Just another chore for Virgil. Just another social function he has to attend.
He’s tired, he just wants to roll over and sleep the day away but sleep had eluded him that night. He couldn’t sleep no matter how hard he tried, kept awake by his nerves.
Every little noise seemed like a threat, every single heartbeat thundered in his ears, too loud and frantic. He couldn’t breathe.
The light of day made it easier, allowing him to finally draw a breath and calm down. But still he couldn’t sleep. So he got up when Patton called, joining the other sides in the kitchen. He got a mug of coffee, trying to choke down the single pancake he had taken to placate Patton.
Objectively, Virgil knew that the pancakes were great. Patton took his role of Dad friend serious and as such took pride in supplying his ‘sons’ with great food.
Subjectively, Virgil was too anxious to appreciate the taste. Paired with sleep deprivation, the food tasted bland.
There was so much Thomas had to do that day. So much responsibility. So many people to talk to. So many dangers to avoid.
So much Virgil had to protect him from. He couldn’t afford to take a nap even if he could.
He missed most of the meal, too absorbed in his own thoughts to listen to the others. He jumped to attention when the others got up and went back to his room as quickly as possible.
His stomach tied itself in knots as it always did on more anxious days and Virgil hoped that none of the others would notice that he’d lost his breakfast barely half an hour after he’d consumed it.
Lunch was usually just as bad but Virgil was lucky. Patton had accompanied Roman to the imagination after preparing some sandwiches for Logan and Virgil, letting them know that there was food ready and available.
Virgil stared at the food for a moment, alone in the kitchen. If he was honest, he was a little hungry, yes. But his stomach was still quite upset and he wasn’t keen on losing another meal.
So he left the sandwich in the fridge, instead grabbing a bottle of water. He had read somewhere that cold water could help with hunger. Time to put it to the test, it seemed.
He curled up into his beanbag chair in his room, using the calm of the day to listen to music. Maybe chilling out a little would help his nervous stomach enough to be able to handle dinner.
Of course he couldn’t completely sink into the music like he wished to do but he still had to keep an eye on Thomas. God knows what dangers were out there, VIrgil had to make sure Thomas noticed as many of them as possible or he’d be careless and get hurt.
Virgil had to admit it after a while. The cold water trick hadn’t helped, not really. So now he was still hungry and still vaguely nauseous and too nervous to talk about it with Logan who might have been able to give him some information that actually helped.
He sighed. Today was just bad.
All too soon it was time for Dinner.
By then Virgil felt less like a raging dumpster fire about to spew his insides everywhere so he braved the kitchen when Patton called, having returned with Roman.
The sight of the food almost made him turn back and cry. He was so hungry, he hadn’t eaten since morning and he wanted to sit and eat with his family now that he wasn’t bursting with anxiety anymore.
But Patton had made Brussel Sprouts.
Brussel Sprouts were bad.
Something about their smell repelled Virgil like nothing else and whenever he forced himself past that and ate some for Patton’s sake he almost threw up from the texture. Maybe it was just the way Patton prepared them but they were mushy but at the same time not but they weren’t crunchy either, they were in a horrible limbo of firmness and when he had one in his mouth and chewed on it it would almost disintegrate because the individual little leaves would come off the actual thing and it was just plain horrible.
He didn’t want to disappoint Patton though. He always put so much effort into the food he made. Virgil could force himself to eat some Brussel Sprouts for his best friend and he could chase them with the other foods on the plate, it was fine.
He was fine.
Edit: He was decidedly not fine.
The Brussel Sprouts were made with some sort of sauce and the sauce touched all of the other foods on his plate.
Virgil had nearly sobbed when Patton handed him his plate. He could ask to not have the sauce touch anything but everyone else already had their plates and Patton was already sitting down, it was too late to ask now. And regardless, it was liquid. There wasn’t much to be done about the fact that it was kinda running all over the plate, contaminating everything else.
He kept his head low, diligently shoveling bite after bite into his mouth until he had cleared at least a quarter of his portion. It wasn’t enough for him to be full but he nearly gagged at the taste and feel of the Brussel Sprouts so he stopped before he actually did throw up again.
He excused himself, claiming to be just not really hungry today Pat.
The lie settled heavier in his stomach than the food had and he went back to his room, laying down to try and sleep.
At least if he was asleep he couldn’t feel hungry. With the barest hint of luck he could eat tomorrow.
But then again, that’s what he had told himself yesterday.
And the day before that.
And many times before even that.
---
Taglist: @3-has-charm @adreamisadishyourmommakes @analogical-mess@bubbliee0 @iris-sanders-athena @letthefandomsbegin @emthetimelady@ilovereadingandilovebreathing @stormcrawler75 @soulwillriseinperfectlight
35 notes
·
View notes
Text
667.
1. If you found a baby turtle on the side of the road, would you pick it up and keep it?
>> If I found a baby of any species on the side of the road, I’m not going to pick it up and keep it, I’m going to call the appropriate authorities and let them handle it. The fuck am I doing with a baby anything?
2. Did you and your mum ever have a big fight that caused you to move out?
>> ---
3. Has the last person you kissed ever been to your house?
>> ---
4. Have you had a good day today or was yesterday better?
>> It was all right. At least the Sun was out a bit, and I managed to go out for once. Mostly I’m glad to be back in my bed now, lol.
5. Do you have any plans for the upcoming weekend?
>> No.
6. How about you, do you have a bf/gf?
>> Hm.
7. Could you date someone very attractive, but who thought they were better than everyone else?
>> I don’t date, period, but I also wouldn’t hang out with someone who had a superiority complex.
8. So do you have a best friend?
>> No.
9. What would you do if your best friend kissed the last person you kissed?
>> ---
10. Do you dislike anyone?
>> Not really. There are people I don’t really want to be around, of course, but I can’t think of anyone specific that I’m like “fuck that guy in particular” about except for people that have unapologetically hurt me (in which case it’s less “I dislike you” and more “I don’t even want to acknowledge your existence”).
11. Did you message your best friend today?
>> ---
12. Do you think you will be in a relationship two months from now?
>> I don’t see why not.
13. Do you always feel like you’re making mistakes?
>> Yeah, because I have Trauma Brain. But I also know that I don’t make any more mistakes than the average person and most of my mistakes are easily fixed.
14. How do you feel about your hair right now?
>> I’m going to need to buzz it again soon.
15. Does anybody have a tattoo with your name on it?
>> Maybe someone has a tattoo of my name, because my name doesn’t just belong to me. But no one has a tattoo of my name that is actually about me.
16. Who did you last see shirtless?
>> A couple of characters on Carnivale (before one of them got hanged with the word “HARLOT” carved into her forehead, of course. this is Carnivale after all).
17. How would you feel if you got the person you liked?
>> ---
18. Do you think you can last in a relationship for six months without cheating?
>> *sigh*
19. Do you like to make the first move?
>> The first move to what?
20. Do you think you will ever be married?
>> I am married.
21. Have you ever tried your hardest and then gotten disappointed in the end?
>> Sure.
22. Is it possible to be single and happy?
>> Duh?
23. Was the first person you talked to today male or female?
>> The first person I spoke to was the bartender at Gardella’s, who is female.
24. Do you remember who you liked on New Year’s?
>> ---
25. Are you a morning person or a night person?
I’m barely a person. <-- mood
26. Could you go the rest of your life without drinking alcohol?
>> Whether I “can” or not is irrelevant because I don’t fucking want to.
27. Have you ever felt like you weren’t good enough?
>> Sure.
28. Is there anyone who likes you?
>> ---
29. If the last person you kissed saw you kissing someone else, would they be mad?
>> ---
30. Do you understand football?
>> I understand American football. I don’t know anything about soccer football except the obvious bits.
31. What’s the first thing you heard this morning?
>> I don’t know.
32. Who last called you beautiful?
>> I don’t know.
33. Did you talk to someone until you fell asleep last night?
>> No.
34. How many kids do you want when you get older?
>> ---
35. Are you the type of person who has a new boyfriend/girlfriend every week?
>> Of course not.
36. Ever been called a jerk/bitch?
>> Yep.
37. Do you have feelings for anyone?
>> Bold of you to assume I have feelings--
38. If you fell pregnant to the last person you kissed, what would you think?
>> Falling while pregnant is dangerous, oof--
39. What’s your full name?
>> *eldritch screeching*
40. Are you young or old?
>> Depends on your perspective -- to a child I’m old, to a middle-aged person I’m young, etc.
41. What’s the gender?
>> Oh, the gender outside is frightful...
42. How’s your heart been lately?
>> You know. Beating and such.
43. Why aren’t you in bed?
>> I am, though.
44. Did you do laundry today?
>> No.
45. What kind of computer do you have?
>> I have an MSI Leopard Pro and a Lenovo Ideapad.
46. Are there always other fish in the sea?
>> Not if you overfish.
47. What can your tongue do?
>> You know. Lick stuff. Form phonemes. Get chemical burns when I eat too many sour candies in a row.
48. What do you think your mum does when she goes out?
>> ---
49. Do chickens have feelings?
>> I don’t know anything about chicken neurology/psychology.
50. Do you think the body is the most beautiful thing that was ever made?
>> No.
51. So how are you feeling today?
>> Neutral.
52. Where is your sister right now?
>> ---
53. Name five things you did today?
>> Took a bus, drank at a bar, briefly logged into ESO, watched an episode of Carnivale, ate mac n’ cheese with bacon.
54. What kind of phone do you have?
>> Moto g6.
55. What are you listening to?
>> Nothing.
56. What do you smell like?
>> A bit like my roll-on oil and a bit like my whipped shea butter. Mostly just like... clean skin or whatever.
57. What colour are your eyes?
>> Dark brown.
58. Have you ever done a Chinese fire drill?
>> No.
59. Do you know someone named Betsy?
>> No.
60. What colour is your mum’s hair?
>> ---
61. Do you have a dog? Breed? Name?
>> No.
62. Do you remember singing any songs as a kid?
>> I mean, yeah?
63. Are you married?
>> Yes.
64. When was the last time you talked to one of your siblings?
>> ---
65. Do you play an instrument?
>> No.
66. Do you like fire?
>> Sure, fire is nice. In moderation.
67. Are you allergic to anything?
>> No.
68. Have you ever been to a spa?
>> I’ve been to a nail spa because Sparrow works at one. I’ve also been to the Aveda spa that she did her training in years ago.
69. Do you miss someone?
>> No.
70. Views on premarital sex?
>> I have no views on it. I really can’t fathom having an opinion on whomst other people fuck and when.
71. What is a noise that you cannot stand?
>> Face sounds. Any of them. Eating, breathing, sniffling, lip-licking, eugh. Stay away. (Sometimes I can hear myself blinking and I want to rip my eyelids off. It’s bad.)
72. Do you know how to do a cartwheel?
>> Yeah.
73. What is the most you are willing to spend on a pair of sunglasses?
>> Not much.
74. Does your mum vacuum early in the morning while you’re asleep?
>> ---
75. Do you shower naked?
>> Do I look like Tobias Funke to you?
76. Does wearing glasses really make people look smart?
>> That’s not my interpretation. People with glasses just look like people with glasses.
77. Are you ADD or ADHD?
>> No.
78. Do your band-aids have cartoons on them?
>> I FUCKING WISH. I was so mad when I needed band-aids for my feet and none of the ones in the size I needed came in cartoon print. The only ones with fun designs were little baby band-aids. I think as an adult I should be able to buy whatever the fuck kind of band-aids I want, including ones with Stitch on them. Fuck you.
79. Have you ever kissed someone you shouldn’t have?
>> Probably.
80. In one word, how would you define yourself?
>> I wouldn’t.
81. Tell me about a dream you had recently?
>> I can’t, I can never remember them anymore. I get vague wispy impressions upon waking, and then even those disappear after a few minutes. I feel disconnected from dream!Mordred and I’m so curious at what it’s been up to.
82. Who’s the funniest drunk person you know?
>> ---
83. How did you feel when you woke up?
>> Fine, I guess.
84. What was the first thing you thought of when you woke up this morning?
>> I don’t know, probably something related to Sparrow knocking around as she got ready for work, because that’s my first sensory memory upon awakening.
85. Name something great that happened on Friday?
>> It’s Thursday, ask me on Saturday.
86. When was the last time you saw your father?
>> ---
87. Do you wish someone would call or text you right now?
>> No.
88. Have you ever been kissed by a person whose name starts with J?
>> Yeah.
89. Do you crack your knuckles?
>> Yeah.
90. What were you doing twenty minutes ago?
>> Probably still this survey, since it’s so long.
91. You’re thinking about someone, aren’t you?
>> No.
92. Have you held hands with anyone in the past twenty-four hours?
>> No.
93. What would you do if your partner still kept pictures of their ex?
>> Nothing? That doesn’t affect me.
94. What if your partner went through your cellphone?
>> I wouldn’t be with someone that went through my belongings without my express permission.
95. What if your partner was flirting with another girl/boy?
>> I’d be glad for her. I hope she gets whatever she’s looking for from that interaction.
96. Ever liked someone you thought you didn’t stand a chance with?
>> ---
97. You want someone/something?
>> Not really.
98. Is there really a difference between Coke and Pepsi?
>> Yeah, which is why many people have a preference.
99. Is there any emotion you’re trying to avoid right now?
>> No.
100. Are there any mistakes with your recent ex you wish you could have changed?
>> I’m pretty sure the entire situation in itself was a mistake, and it was changed, by us ending up having no contact with each other.
101. Has anyone ever been with you while you were throwing up?
>> I mean, sure.
102. Background on your computer?
>> Right now it’s a wallpaper with a scene from the movie Interstellar. (My desktop wallpaper is on a shuffle timer.)
103. Have you cried recently?
>> Like, within the last week, probably.
104. Who has hurt you the most?
>> I don’t know.
105. Are you happy with where you are relationship-wise now?
>> Sure.
106. What language do you want to learn?
>> ---
107. Your ex’s car breaks down and they ask you for a lift. Your response?
>> I mean, I don’t drive, dude. Also, we live in wildly different parts of the country. This is just so many layers of implausible.
108. Would you hit a member of the opposite sex?
>> ---
4 notes
·
View notes
Text
Friends in Dark Places [ch 12]
pairing: moxiety, eventual logince, background eventual remile, background eventual remy/emile/deceit
WARNINGS: sensory overload, panic attacks, self hate, school dances, swearing, food mentions, kissing, embarrassment, rumors, eating, possibly something else
tag list: @hufflepuffgirl01 @cocobearthe4th @cas-is-a-hunter @band-be-boss-blog @theunoriginaldaisy
a/n: so i have to repost all of these in a different format! yay fucking me!!!! please consider reblogging these if you’re a fan of this series because it’s all fucked up now
first - previous - next - companions
consider buying me a coffee (please)
-
“So, Virgil. Are you going to prom?” Roman casually asked before popping a french fry in his mouth.
“Um, I don’t know. I wasn’t planning on it.” Virgil absently dipped a chicken nugget into the pool of ranch on his tray. He really hadn’t thought about prom that much. Plus, the thought of a whole bunch of his peers stuck in one room together, probably grinding with their respective dates, was not a pleasant one.
“Awww, kiddo! You should go! You could come with us; we’re going to grab dinner and everything,” Patton whined.
“I mean, I guess?” Virgil grimaced as he weighed the options. “But don’t I have to rent a tux? I don’t have money for that, especially not after what happened on Monday. I’d be surprised to find my credit card still working with all of that in mind.”
Logan jumped into the conversation. “You would have to rent a tux, yes, but the three of us would be more than happy to help cover your expenses. We value you as a member of our friend group, and we wouldn’t exclude you from something just because you couldn’t afford it.”
Virgil opened his mouth to argue, but Roman interjected, “Dude, seriously. Just let us do this for you. It’ll be fun!”
“Plus, Ro already bought you a ticket,” Logan added and held out a small slip of cardstock. Westview Junior Prom.
Well, Virgil Thomas was now going to prom.
---
“Hey, Pat? Can you help me with my tie?” Virgil called from his bathroom. He had been struggling for the past five minutes trying to figure out the witchcraft behind ties, and he still had zero clue as to what he was supposed to be doing.
“Be right there, kiddo!” It was only a few moments before soft footsteps could be heard approaching, and Patton walked into the bathroom. He’d already mostly finished getting ready sans the fact that his hair was a catastrophic mess. Virgil could guess that he’d been trying to fix it when he’d been called into the other room.
“Alright. Work your magic,” Virgil smirked. In a matter of seconds, Patton had looped and pulled the tie into place, gently tightening it around Virgil’s neck. It was deep purple, picked out specifically because of his dislike of most other colors, and it went very well with the blues and reds of the others’ ties. The tie also matched the freshly dyed purple hair that Roman had forced his three friends to do along with him earlier that afternoon. What an ass.
Virgil admired his reflection. “Dude, what the fuck? How did you do that?” He felt oddly confident in his skin. The same feeling had come about a few times since he’d met Patton, and he had to admit that it was nice. Pat’s happy-go-lucky attitude somehow perfectly meshed with Virgil’s own doom-and-gloom one, forming a hilariously compatible friendship.
Patton smiled and ruffled Virgil hair, much to the other’s dismay. “Now that I helped you, will you please fix my hair.”
“Ugh, fine.”
“I mean it, Virge! Look at this.” Pat ran his fingers through his hair and aggressively tugged when he reached a clump of knots.
“Okay, yeah, we’re fixing that right now.”
---
“Dinner? Really, Patton? You guys couldn’t have told me about this before?” Virgil whined as the four walked into the diner. Yes, a diner, which meant that they were ridiculously overdressed; every other patron was wearing some sort of flannel and jeans combo. It smelled great, sure, but it was so unexpected that he couldn’t help but feel on edge.
“It’s our favorite restaurant,” Logan explained. “We always come here before school events. Roman has coined it as some sort of weird ritual, but it’s mostly tradition.” He led Virgil to the booth that Patton and Roman had already rushed to sit in.
“Plus, we’re friends with the staff,” Ro started with a smile. “You’ll love them; they’re all super nice. Speaking of, here comes Emilia.”
A young lady with brown hair walked up to their table, pulling out her small notepad. “Well, who do we have here? Another addition to our little group of customers of the month for every month since 2014?”
“Hey, Emilia!” Patton said. “This is Virgil; he’s a new friend of ours. He’s been living with me for a few weeks while his dad is out of the country on business.”
“That’s sweet, Patton. Now, what can I get for you guys?”
The three regulars spouted off their orders, clearly versed in what they wanted to eat. Suddenly, all eyes turned to Virgil. He’d barely been able to look over the menu in the time the others had taken to order.
“Uh… I… Um…” He stuttered. Every drop of intelligence that he had in his body was gone in an instant, and he was left a bumbling mess.
“He’ll have a cheeseburger and fries, thanks,” Patton cut in, saving his friend from any further embarrassment.
“Alright! I’ll be back in a few with your food and a pitcher of water!” Emilia gave the boys another smile before she walked back behind the counter to tend to other customers. Almost immediately, Patton and Roman launched themselves into a fast paced discussion about the upcoming festivities. Virgil, unsurprisingly, not only felt anxious, but he also felt like a complete idiot. He was just ordering dinner--there was no reason for him to have been so freaked out.
Virgil felt a hand rest on his left shoulder, turning to see Logan with a worried expression etched on his face. “Are you okay? Do you need to step outside for a moment to regain composure? I’d be willing to go with you if you don’t want to be alone.”
“Uh, no. I’m okay. I’m just a little worried. I mean, this is my first proper school event in, like, ever, and it’s freaking intimidating. You guys go to these things multiple times a year?” Virgil ran his hands through his hair, distressed.
“I understand. When Roman and Patton first made me come with them to homecoming, I was so nervous that I nearly passed out on the way here. Thankfully, I wasn’t driving us everywhere back then otherwise that would’ve ended in a disaster.” Logan gave Virgil a small smile, adding to the tiny--yet slowly growing--list of his outward displays of emotion. Virgil knew Lo wasn’t an emotionless android, but Roman and Patton were so all over the place that someone needed to play the calm and collected one.
“They can be pretty intense,” Virgil commented with a smile at the enthusiastic conversation across the table from them. Both of the teens were grinning and flinging their hands around in wild gestures, barely avoiding impact.
“Yeah, they sure can.” Logan glanced at the other side of the table with a fond expression, but he quickly snapped out of his reverie. “Don’t worry about the dance. Oh, here!” He pulled a pair of earbuds out of his inside jacket pocket and held them out to Virgil. “It gets pretty loud at these dances. I’ve observed that you put on headphones when it gets too noisy, so I brought these just in case you didn’t have your own.”
Virgil pocketed them just as Emilia finally returned with their food. The other three immediately began to dig in while he hesitantly poked at his burger. He picked up a fry and lazily popped it into his mouth.
He picked at his fries for a few minutes, but he eventually worked his way up to taking a bite of his burger. “Holy shit! This stuff is great--wait, why haven’t you taken me here yet?”
“I was trying to ease you into our friend group, so I thought eating dinner at my house would save you some unnecessary interaction,” Pat explained. “Obviously, that was a crime against your taste buds.”
“Of course it was, Patton. Depriving anyone of this blessed food is practically a war crime!” Roman dramatically stated, throwing out his arms. Virgil snorted at the theatrics.
They continued to eat, and all but Virgil had finished their dinner when Emilia returned to their table for dessert orders. Logan ordered a slice of pecan pie for himself, a chocolate lava cake for Roman, a hot fudge sundae for Patton, and a caramel shake for Virgil. Patton, of course, began to spout off a review of all of the desserts they’d ordered, even though Virgil wouldn’t be eating most of them. They all listened politely, not really absorbing any of the information, until their orders arrived. Within a nanosecond, Pat’s face was stuffed full of vanilla ice cream and fudge sauce, easily and efficiently shutting him up.
They ate in near silence, save for the “light” discussion of whether cake or pie was better (Patton eventually had to cut in when Roman threatened Logan with a butterknife). Pat covered the whole bill once they’d finished, claiming “it’s my way of thanking you guys for putting up with my shenanigans.”
---
“Three, two, one!” Roman dramatically counted as he threw the doors to the venue open. Time seemed to freeze as the four friends stepped in; all eyes snapped to them. It had been days since they’d been the topic of gossip at school, but that didn’t mean the student body had lost their interest in the boys.
Roman was at the front of the group, confidently striding to the grand staircase and adjusting his red tie. Logan followed close behind, who looked absolutely stunning in the sharp suit and deep blue tie. Then was Patton, who was marveling at the cascading flower vines and glittering fairy lights. And last but certainly not least…
Virgil. He had a wary smile on his face, shoving his hands deep into the pockets of his slacks. The boy made absolutely sure that he didn’t get lost; he kept eyes on Patton the entire time they descended the stairs.
Logan had been right; it was fucking loud. People were screaming left and right, and the music was so loud that Virgil could feel every beat vibrate in his chest. He was lucky that he’d put the earbuds in before they’d arrived, or he never would have stepped inside the venue.
Patton turned around to check on Virgil, obviously sensing the tension building in his friend. He held out his hand for Virgil, who hesitated for just a moment before gently taking it. If people wanted to believe they were together, that wasn’t his problem. It was no skin off his back.
They talked and danced for what felt like hours, and Virgil even joined in on a few of the dances he knew. He was having fun. He smiled and laughed, and it was all genuine! In just a few short weeks, Patton had actually transformed him from a suicidal nightmare into someone who found joy in life. It was a stupid sentiment, and he knew it, but it still brought Virgil a bit of warmth in his chest.
The DJ announced a slow dance. Ugh, how awful. He had nobody to dance with; it was just—
Oh.
Patton tugged Virgil’s hand lightly, pulling their bodies closer together. “Wanna dance? We don’t have to, of course, but it would be a fun first experience for both of us!”
“I—Uh, sure,” Virgil mumbled, trying to hide his gently growing blush. Pat gently guided Virgil’s hands around his neck and placed his own on Virgil’s waist. For the first time, Virgil noticed that he was just an inch or so taller than his friend. Reveling in the warmth and closeness, the two swayed together to the gentle rhythm.
The song ended, and Virgil stepped back, shoving his hands into his pockets. He was extremely grateful that the low light hid his pink cheeks. The screaming resumed as couples broke apart, and early 2000s rap boomed out of the speakers.
And then just like that, Virgil was attacked by anxiety. His hands started shaking, and he rushed away from the small group he was in, mumbling something about going to the bathroom. He calmed slightly when he had made it outside, where he simply collapsed to the ground, but then his panic picked up again when he realized how fucking alone he was always going to be.
Nobody would love the weird guy who rushes out on social gatherings for no fucking reason! Why should they? Virgil had nothing to offer; he was just a guy who had snark to rival Roman and barely two cents to his name.
Tears streamed down his face, running in dark gray streaks as they mixed with his black eye makeup. He could feel his chest heaving, but little air actually made it into his body. Everything was working overtime yet nothing actually happened. Virgil stayed sobbing on the ground. Nothing. Changed.
“Virge, honey? Do you need me to call my mom and have her pick us up?” Patton slowly lowered himself next to Virgil, talking softly so that he woudn’t stir up anything worse.
“N-No! I’ll… I’ll… Fuck!” Virgil cried as he ripped the earbuds out of his ears. He threw the cord a few feet away, instantly regretting it as the sound of shattering plastic reached his ears. He’d have to buy Logan new ones. He couldn’t afford to replace them.
“Goodness gracious, Virgil. It’s okay. I’m going to call Logan, and we’re going to get you out of here—“
“I-I-I don’t… want t-t-to… ruin… night…” Virgil sputtered. He was having trouble pushing the words out; all of them got stuck in his throat.
Patton carefully began to comb through Virgil’s hair with his fingers in an attempt to soothe the attack. “Don’t worry about that, kiddo. There isn’t much more fun to be had, anyway. We still love you—I still love you.”
That’s it. That’s what he felt. Love. He loved Patton.
All of the impulse control he had—though, truthfully, there was very little to begin with—left his body. He reached out and brought Pat’s face to his own, lightly kissing him. Patton stiffened for a fraction of a second before relaxing into the kiss. They were both going to regret this later, but what did that matter in the moment?
next
#sanders sides fic#moxiety#logince#m writes things#virgil sanders#logan sanders#patton sanders#roman sanders
15 notes
·
View notes
Text
The Bestiary Revamped: Vampire Squid (HALLOWEEN SPECIAL)
Disclaimer: While this article is founded in scientific fact, it contains hyberbole and conscious exaggerations for the sake of comedy. Do not take my ramblings at face value. You can find the sources at the end of the article and tools for scientific fact-checking under the “Learn more” link on my blog.
The old article can be read here.
(I intended to post this yesterday but stuff came up. Anyway.)
Ahem.
Cue the spooky music.

*threatening organ music plays at unbearable volumes*
That’s right, dear readers, the Spooky Gourd Day has finally, finally come, and with it the nigh-endless Halloween shitposting that permeates this website every October like the smell of pumpkin pie did my house just a few hours ago, immediately before I ate most of it. (I still have like half of it left, but it’s cold now so it doesn’t have that mouthwatering smell unless I reheat it. And I was too busy watching old Betty Boop Halloween cartoons to reheat it. Anyway, I’m getting off track.)
Frankly, the obsession of internet culture with this innocuous holiday has always fascinated me. What it is about a day when you get to dress up all funky-like, go from house to house acting like an idiot, horf down all the candy you can get away with and watch scary movies all night that is so attractive to them youngsters? I simply cannot wrap my head around it.
However, it is a day of great significance to this blog, since this is the day when we celebrate the utter freakiest of the freakiest that can be pulled up from the stygian waves of the planet’s oceans. This is the third Halloween of the Terrible Tentacle Theatre, and for this notable occasion, I have decided to give one of my earliest poster children a much-needed revisit.
Back in the early days of the blog, when it was still called Hectocotylus and my content mainly consisted of spicing up Wikipedia and Cracked articles with swearing for the sick enjoyment of some 30 followers, the article in question was my first big hit among the people of the Digital Blue Hills of Hell. In the days when most of my articles didn’t go above 20 notes, this beast gathered up 300 notes by using its nebulous tendrils to reach into the deepest corners of the ole ‘web. Not only was this creature my first big hit in my career as a marine biology blogger with tone moderation issues, it would also fit in great as the main monster in a theoretical Universal Horror/Syfy teamup, which would be the Halloweeniest shit ever.
Ladies, gentlemen and other fellows, the vampire squid.
Before you even see this thing in full detail you can already gather that I didn’t choose it for this year’s Halloween special for nothing. Everything from the ghoulish dark red color scheme to the bat-like webbing between eldritch tentacles screams “cheesy Hammer Horror movies written by good ol’ Howard Philips”. And it will become even more evident when you see it in its full, glowy, betentacled glory.

This is how it looks like when you stare down a squishy, floppy incarnation of doom. This thing looked so freaky that the dude who discovered it, a certain German biologist called Karl Chun, decided to name it Vampyroteuthis infernalis. That’s Latin for “vampire squid from Hell”. Yep, that’s right. Remember the part where science is hard fact unaffected by emotion? Well you can throw that right out the window, because this fucker freaked its discoverer out so hard that he named it the vampire squid from Hell.
“The shit I’ve seen, kiddo. You wouldn’t believe.”
Even descriptions of this guy sound like they escaped straight from a 19th century gothic horror novel. For example, in 1925 the Arcturus expedition caught one near the Galapagos Islands and described it as “a very small but very terrible octopus, black as night, with ivory white jaws and blood-red eyes.” Even in the years of the Roaring Twenties, merely seeing the vampire squid was enough to bring out anyone’s inner Poe or Bram Stoker, apparently, which isn’t very surprising considering that it looks like Béla Lugosi had an illicit affair with one of the Star-Spawn of Cthulhu.
You’re welcome for that mental image.
While calling it a vampire is more than appropriate, the names “squid” or “octopus” are much less fitting. While intially appearing to be something of an octopus, it’s actually not one of them; and it isn’t a squid either, which left the confused scientists to place it within its own little private taxon, the order Vampyromorphida. If you know a little bit of Latin, that means “vampire-shaped”, which would imply that this is the general shape for vampires. So next time you read Twilight, imagine Edward as a vampire squid flopping around on the ground the entire time and I guarantee you’ll have a blast reading through several hundred pages of sweaty bloodsucker romance.
Unlike Edward however, the vampire squid doesn’t actually feed on blood. Dashing from shadow to shadow in the cover of a snappy opera cape and hunting for innocent young maidens in the night is the kind of energy expenditure that this malevolent mollusk cannot afford. Mainly because it lives (you guessed it) in the darkest, deepest excesses of the oceans, where the eternal darkness creates an all-year-round Halloween mood. In these waters, even beginners have a hard time finding the tiniest scraps of food, and have to resort to drastic measures to get by. But the vampire squid looks at those beginners and goes “yall are scrubs git gud lmao”. Compared to the vampire squid’s lifestyle, virtually any other denizen of the deep sea lives right in the middle of a goddamn cornucopia.

See, the vampire squid doesn’t just live in the deep ocean. It specifically prefers places called Oxygen Minimum Zones (OMZ), which sounds more like the hardest Sonic level ever than any serious place which can support life. OMZs are vast sheet-like expanses of water in the deep sea which barely contain any breathable oxygen. Some of these zones can contain as little as 5% of the oxygen that saturates air, and barely anything survives here.
And guess what? The vampire squid lives here. Not only lives, but thrives.

This is the game the vampire squid plays, every day of its life. On hard difficulty.
Obviously, living in a dead wasteland of suffocating water has required the squid to adopt some nifty tools of survival. Do not do so would be like entering the final dungeon of a video game with early game gear.
First off is a pair of sensory filaments, which the vampire squid extends through the water much like a spider does its web. They are super long and flexible, and probably the source of so many dick jokes that the squid will choke a bitch if anyone tells one more.

“No, I’ve never heard that one ever. Ha ha ha. Real fuckin’ original.”
Next up is a pair of membranous wings, used by the squid to travel through the aether of space to “fly” through the water, it’s cape-like arm web billowing behind it. The vampire parallels are getting more and more accurate.
Interestingly this wing isn’t the same in adults and juveniles. At one point in their devlopment they start growing a second pair of fins which eventually fully substitutes the first pair, which then atrophies back into the flesh. Thus if you’re lucky enough to catch a vampire squid, it’s not impossible that it will have four fins. The biologists who first found these four-finned squid nearly went insane trying to describe it (and several other developmental stages) as separate species. It was such a mess it took years to sort out, and nowadays the vampire squid is the sole surviving species of its order. He’s standing in the darkness. Alone.

WAKE ME UP INSIDE
The fins and the filaments aren’t just decorative elements the squid picked out at Hot Topic, either. Used in tandem, they’re a fearsomely effective netting tool and the way this crafty cephalopod earns its daily bread. You think spiders are cool with their webs? Nah, Spiders ain’t shit. They’re lazy idiots and their web does all the work for them. the vampire squid’s filaments is where it’s REALLY at.
See, the vampire squid’s main diet is thankfully not blood but something called “marine snow”. This is basically the shower of discarded tissue, shit and corpses that rains down upon the lower layers of the deep ocean from the upper layers all year round. Having this fall from the sky for “White Christmas” would probably be quite traumatizing.

DECK THE HALLS WITH BALLS OF FECES SHALALALALALALALALAAAAARGH
The vampire squid, however, has had its resolve steeled by years of isolation in the darkness of the deep ocean, and is willing to chug down anything to survive. Bear Grylls is a picky gourmet chef compared to this guy.
That said, it needs to eat something that’s actually of some nutritional worth. It could spend its life scarfing down every chunk of marine snow it comes across, but that would be a waste of muscle movements since most of it does exactly nil to fill up its stomach. That’s where the filaments/fins combo come in, turning the vampire squid into an angry little tripwire trap ready to snap at any moment.

Note the filament. That’s not a parasite, that’s legit a part of the animal. Nobody knows where it evolved from, it’s not a modified arm or tentacle and it’s a fucking enigma.
Mystery tentacles: the quintessential Terrible Tentacle Theatre experience.
Extending its filaments (one at a time) into the mucky waters around, it waits more still then I do when I go to the kitchen for a glass of water during the night and I hear a sudden noise. The filaments come with a plethora of sensitive nerve endings, ensuring that anything bigger than a flea’s asscheeks landing on them will elicit an immediate response from the squid. And if said asscheeks touch the filaments, responds the squid it does. Specifically, it exhibits a surprising burst of speed (considering it just drifts around all day and it is effectively the consistency of Jell-O), pulled entirely by its fins to perform an acrobatic fucking pirouette off the handle, whipping around in a loose loop and catching its own filament. Millions of dogs around the world enviously sigh in unison.
After this, the squid pulls off its prey from the filament using its arms, which generate a solid slime-like material. The collected chunks of edible whatnot are rolled into a ball of slime, and horfed down by the squid at once. You probably cannot tell but there’s a Michelin star underneath its mantle. “Slimeball à la Vampire Squid” is one gourmet-ass dish.

Molto bene!
Of course, all this fine dining makes the vampire squid itself tasty as all hell. You are what you eat, afterall. But in the deep sea, you do NOT want to be tasty, because everyone is hungry on top of being the most light-deficient gourmet motherfuckers on the planet. So naturally, our subject needs some sort of way to evade the raving food critics hunting him in the deep. And he has this way in the form of a very unlikely tool: bioluminescence.
“But Admin”, I hear you say, “didn’t you just get done telling us last week that glowing in the deep sea will attract everything around you?” That I did, young padawan, and it still stands. However, just like last week’s subject, the vampire squid uses its built-in glowsticks with a very express purpose and doesn’t just flash into the sunset willy-nilly. The glowy parts of this beast have very well-defined places and usages, exquisitely located and timed, just like a laugh track in a sitcom. Underneath its dark-red skin the vampire squid carries clusters of glowing photophores mainly on the tip of its arms as well as in two fake eye-spots on the top of its mantle, ready to flare up in a blue burst of light on demand. The fake eyes even come with their own built-in eyelids, opening and closing as Dracula Jr. sees fit.
Imagine you’re a predator and you see this glowing collection of random bullshit. Now figure out where to bite. Good fucking luck.
These lights are used with great care and consideration in order to troll the fuck out of anybody who is foolish enough to make an attempt on the vampire squid’s life. Upon attack, the squid whips its arms around with the lights on full luminosity, creating a confusing dance of light spots in the otherwise total darkness and messing up the predator’s perception. The false eyes only make things worse, finally creating the illusion that the vampire squid possesses unlimited godlike control over space and time, which may damn well be true.

Question: What way is this vampire squid going? Hint: It’s not facing toward you.
The appearance of the squid as a godlike psychic is surprisingly in line with the whole vampire angle, since Dracula has reknownedly had the ability to charm and hypnotize people. The effect is further accentuated by the squid’s eyes, proportionally the largest of any animal ever discovered. With a diameter a whopping one sixth of the animal’s whole body, this thing's oculars are like if you were walking around with eyes the size of your head. Each.
And for added effect, they glow and change color depending on which angle you’re looking at them from.

DISCO CTHULHU
And finally, if a spooky vampire-looking-ass dark red glowing octopus-squid-thing with hypnotic powers isn’t Halloweeny enough for you, the vampire squid has a final trick up its sleeve that catapults it right into the realm of body horror. This is suspected to be a defensive tactic but who the fuck knows, really. Deep sea creatures are enigmatic as shit, and they guard their secrets jealously.
Alright, I’ll quit beating around the bush and say it outright. Basically the final defensive measure of the vampire squid is turning itself inside out.

Yep.
Of all the stupid shit that Mother Nature could have come up with, she went and decided “alright, it just up and turns itself inside the fuck out. What are you gonna do about it?”
This behavior is known to science as “pineappling” or even more Halloweeny-ly “pumpkin posture” (no, seriously) and it involves the squid taking the webbing between its arms and turning it upside to shield its head and body from harm. Now folded comfortably into a spiky little footbal, the vampire squid knows itself free from harm. The webbings are thin enough for it to see through, but also don’t let its lights to shine around, so doing this effectively means the vampire squid switches into stealth mode. Plus it looks stylishly similar to Dracula popping the collar on his cape.
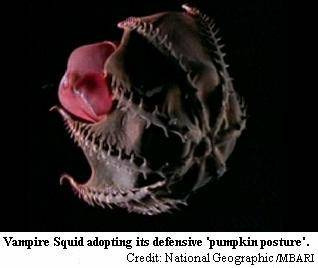

The vampire squid is every Monster Mash horror cliché come to life and smushed into a vaguely cephalopod shaped package for best user experience. When the stars are right and Cthulhu and his Star-Spawn emerge from the sunken city of R’lyeh to bring the world to ruin once more, these guys will be the first living things they encounter. And then they’ll fuck off back to their stupid city, mumbling things like “what the hell man, that’s plagiarism” and “that’s way too extra, even for us”. The apocalypse is postponed once again, thanks to the vampire squid’s vailant efforts of looking weird as fuck.
Happy Halloween, everybody! I was a day late due to the length of this article, but I hope you don’t mind. Until next Tuesday’s article, have a wonderful time with the aftermath of the day of cheesy horror and confectioneries.
Sources:
Encyclopedia of Life
Tree of Life Web Project
Animal Diversity Web
Ocean Biogeographic Information System (OBIS)
Ellis, Richard. “Introducing Vampyroteuthis infernalis, the vampire squid from Hell”. The Cephalopod Page. Dr. James B. Wood.
Seibel, Brad. “Vampyroteuthis infernalis, Deep-sea Vampire squid”. The Cephalopod Page. Dr. James B. Wood. Retrieved 3 July 2011.
Hoving, H. J. T.; Robison, B. H. (2012). “Vampire squid: Detritivores in the oxygen minimum zone”. Proceedings of the Royal Society B: Biological Sciences.
#bestiary#bestiary revamped#halloween#halloween special#cephalopod#deep sea creatures#bioluminescence#marine snow#vampire squid#spoopy#bela lugosi is spinning in his grave somewhere
988 notes
·
View notes
Text
RHR: A Three-Step Plan to Fix Conventional Healthcare
In this episode we discuss:
The patient case that inspired the book
Who is this book for?
The mismatch between our medical paradigm and chronic disease
Drug companies and conflicts of interest
How clinicians can help create a new paradigm
The three core problems and how to solve them
What this new paradigm looks like
How do we pay for this? Is it scalable?
How allied providers are the key
Show notes:
Unconventional Medicine by Chris Kresser
Special offer for RHR podcast listeners - get the audiobook free if you buy the book by November 12th.
NaturalForce.com - use coupon “unconventional” and get $10 plus free shipping
[smart_track_player url="http://ift.tt/2yiM0Yd" title="A Three-Step Plan to Fix Conventional Healthcare" artist="Chris Kresser" ]
youtube
Chris Kresser: Hey, everybody, Chris Kresser here. Welcome to another episode of Revolution Health Radio. Today we’re going to do something a little different. I am bringing on a guest host, Tony Federico, he’s the VP of marketing for Natural Force Nutrition, a physiology editor for the Journal of Evolution and Health, and a longtime contributor to Paleo Magazine, and also at Paleo f(x), which is where I met Tony, I think, originally, and I have interacted with him the most. And he’s moderated several panels that I’ve been on and I’ve always been impressed with the way he’s done that, the intelligent questions that he asks and just his balanced perspective on ancestral health and Functional Medicine, and this movement overall. Today is the day that my new book, Unconventional Medicine, comes out. It’s now available on Amazon, and I wanted to ask Tony to come take over the podcast and talk with me about the book because I know he’s really interested in all these topics and he’s read quite a bit of the book himself, and I thought it would be more interesting to have a conversation about it than for me to just sit here and do a monologue. So Tony welcome to the show and thanks for being here. Tony Federico: Yeah, thanks for inviting me on, Chris. It’s always fun, when we’ve had the chance to chat, as you said. Whether in person or on podcast, I’m always happy to jump in and dish on health with you. Chris: Fantastic. So, you have read a little bit of the book and we chatted a little bit about it via email, so let’s dive in. Let’s talk a little bit about this book. And for me it was really, it felt like the most important next step that I could take in order to get this message out about ending chronic disease. Tony: Yeah, I got my copy of Unconventional Medicine a couple days ago. I just so happened to have some time off yesterday, and the next thing I knew I was 80 pages in. Chris: Nice. Tony: So, I have to say that, as somebody who’s been in the trenches, I worked as a personal trainer for 10 years, I could really relate to a lot of the things that you were saying in the book, and we’ll get into why a little bit later on in the interview. But you know I just am really impressed with what you put together here, Chris. So let's just, let's get into it, and the first thing that I actually wanted you to maybe tell me a little bit about was how you open the book, which I think is a really great story about a patient named Leo. So I wanted to talk a little bit about Leo and his story and kind of how that inspired you to go down this particular path of unconventional medicine.
The patient case that inspired the book
Chris: Sure, yeah. So, Leo was an eight-year-old boy that I treated in my clinic a few years back, and I wanted to start with his story because it's, unfortunately, a typical story, much more common than, of course, we would like. And it was powerful for me, it was a powerful experience. It's what actually led to me writing this book. So, like way too many other kids of his age, he was suffering from a number of behavioral issues. He was initially diagnosed on the autism spectrum. Eventually they settled on OCD and sensory processing disorder. He would throw these just crazy tantrums where he'd end up crying or screaming inconsolably, writhing on the floor, and this would happen for seemingly the simplest of reasons. Like trying to get his shoes tied as they were going out the door, not cutting the crust off his sandwich in just the right way or getting a stain on his favorite T-shirt. And he was really rigid around his behavior and its environment, everything had to be just right, just the way he wanted it to be, or else he would fly off the handle.
Is a new healthcare paradigm affordable? Scalable? You bet.
His diet was extremely limited, he only ate a handful of foods, pretty much all of which were processed and refined. So crackers, bread, toaster waffles, that sort of thing, and this is part of the kind of OCD-like tendencies. And any time his parents would try to introduce new food, he would go totally ballistic. And they were worried about nutrient deficiency, but they didn't feel like they ... they were just worn down. Any parent who has a kid like this will understand that. It's just they didn’t feel like they had the resources to battle him at every meal. And they took him to a bunch of doctors locally, and that’s where they got those diagnoses. Initially they were kind of relieved to have those, but then after a while they realized that they were just simply labels for symptoms. And when they asked what the treatment was, you can probably guess the answer: medication. Tony: Something to do with drugs. Chris: Something to do with drugs. Yeah. And when they asked how long he would be on that treatment, you can probably also guess the answer. Tony: The rest of your life. Chris: Yeah. Shrug of the shoulders, indefinitely, maybe he'll grow out of it, that sort of thing. And they weren't excited about the idea of of medicating their son, but they were also aware of how much he was suffering, and they were suffering, frankly, too. They decided to give them a try, starting with Adderall, and then they progressed to Ritalin and then antidepressants. And certainly the drugs did seem to help with at least some of the symptoms, but there were a couple issues. Number one, they also caused some very intractable side effects like headache, abdominal pain, irritability, and most significantly, severe sleep disruption. And they had a couple of other kids that were younger than Leo. So they were not happy about the sleep disruption. Nobody was because it was brutal for them and also brutal for Leo. Kids need a lot of sleep, and if they’re waking up throughout the night, that’s going to make ... So that was in some ways worse than the original symptoms they were trying to treat. And then Leo's mom had done quite a bit of research on the effects of these medications and she was scared. Particularly for children and adolescents, some of these drugs have some pretty scary side effects and long-term risks. So what really stood out to me, and I mentioned this in the book, is that not once during this entire process of seeing all these different doctors, primary care provider, psychiatrist, eventually behavioral disorder specialists, did anybody even hint at the possibility that something in Leo's diet or some other underlying issue like a gut problem or nutrient deficiency or heavy metal toxicity or something like that could be contributing to his symptoms. It wasn't even broached as a possibility at any time. Fortunately, Leo's mom, one of her friends followed my work and sent her a couple of articles from my blog. One was on the gut–brain–axis, and I think the other one was on the underlying root causes of behavioral disorders. And so that's what led them to bring Leo to see me, and long story short, we were able to ... we did a bunch of testing, found issues that you might guess at. So, disrupted gut microbiome, SIBO, fungal overgrowth, gluten intolerance, but also intolerance of soy and corn and rice and buckwheat, which were major ingredients in a lot of the processed and refined food products that he ate, and arsenic toxicity because rice milk was the only other beverage he would drink aside from water. And we know that rice products can be high in arsenic. So, we, over several months, it definitely wasn't easy to address these problems because of his OCD-like tendencies and his picky eating habits. But after several months he was like a different kid. His teacher even called home and was like, “What have you done with Leo and who’s this kid that you’re sending in?” Because it was a big issue for her. They often had to come to school and pick him up early because of the behavioral problems. And his diet expanded; he was eating foods he would've thrown against the wall just months before, he was more tolerant of disorder, more relaxed in his environment. They were able to travel for the first time in a long time because he wasn't so anxious in unfamiliar environments. His physical symptoms had improved significantly. So they were just over the moon. They couldn't believe it, and toward the end of our treatment together, she said something that really struck me, which was there’s so many kids out there that are like Leo and they’re suffering, they’re not finding help in the conventional system. Tony: Sure. Chris: And their doctors and parents are not even thinking about this stuff. Like it’s not even in most people’s consciousness that if a kid has a behavioral disorder that you should look at these physiological issues. It’s not, for 99 percent of people they don't even go there because they don't know. Tony: Yeah, I mean I think that that was—reading about Leo and reading about a story and certainly there's people that I've known, myself included, who have had very similar experiences—I think it's great to have a narrative like this that you can really connect to because then when you tease it apart, all the pieces really make sense. It makes sense why having doctors treat symptoms has failed, it makes sense why a lack of communication between the health provider network that was supposed to be serving Leo failed. It makes sense why it didn't work when you actually start to tease it out. But then we’re still all, well not all, but most of us are still going down this path and it's an exercise in futility, really. You have an eight-year-old kid who's on powerful stimulant medications, he’s on antidepressants, and it was bad enough for his parents to reach out and to seek those interventions as solutions, and then the side effects are even worse. And that’s just something that just gets you right in the heart. And like you said, he’s not the only one, he’s not the only kid. His parents are not the only parents. And frankly, his doctors are not the only doctors because I can guarantee you that that probably doesn’t really feel good for the practitioner, for the healthcare provider to not get results as well. And they’re working with what they’ve got. Chris: Absolutely. Tony: And trying to use the tools they have. Chris: Yeah, I mean, let’s be clear about this. Everybody is doing the best they can in this situation. The parents are doing the best they can, in the vast majority of situations, parents just love their kids and do everything possible that they can to help their kids thrive. I’m a parent, I know that that’s how I relate to my kid. I know that every parent I know, that’s how they relate to their kids. And I would even, I would say that’s true for doctors too. The vast majority of them are trying to do the best they can with the tools that they have and in the system that they’re working within. And that’s the rub. Tony: Right. Chris: It’s like most doctors I’ve seen have been caring and they’ve wanted to do the right thing, but the question is, can they do the right thing in the conventional medical system as it exists today? And, of course, that’s largely what the book is about.
Who is this book for?
Tony: Yeah, so let’s kind of speak to that specifically. And we’re talking about doctors, we’re talking about medical professionals, we’re talking about patients, and then we didn’t mention it, but where I fit into this formula or potential formula as an allied healthcare provider, as a personal trainer/health coach, is that your audience for this book, do you really see that kind of triad is who you're speaking to here? Chris: Yeah, definitely. I think if you look at the cover of the book, the subtitle is “join the revolution to reverse chronic disease, reinvent healthcare, and create a practice you love.” So that last bit would suggest that it's mostly for practitioners, but that's not true. It is really for anybody that is interested in the ideas of reinventing healthcare and reversing chronic disease. And, in fact, I would argue that that change is going to be initiated by people, primarily by people that are not practitioners. So it's like a grassroots, bottom-up approach, where a good example is with my training program, my ADAPT training program, now that we've been training practitioners in this approach for the last couple years, we always ask people how they learned about my work or how they learned about the training program. And in a surprising number of cases, the answer is from their patients. So these doctors or other practitioners, their patient brings an article in that I wrote or brings something in, tells them about me, and to their credit they’re open-minded enough to go and check it out. And then they like what they see and they end up taking the next step. So people even who have no intention of ever becoming a healthcare practitioner, I think would really benefit from this book if they're interested in these ideas. And then certainly, as you mentioned, licensed healthcare providers like medical doctors or nurse practitioners or physician assistants that are currently working within the conventional paradigm but have already seen its limitations and want to do something different but don't yet know what that might look like. And then people who are outside of the conventional paradigm but are already practitioners, so acupuncturists, chiropractors, naturopathic physicians, etc., in many cases they’re already well aware of the limitations of conventional medicine, which is why they chose to go down a different path. But speaking personally as an acupuncturist myself, I also saw some limitations in the traditional Chinese medicine approach, or at least some differences in the way that I wanted to practice it. I was looking for something that could incorporate modern diagnostic testing and create a more systematic approach that included ancestral diet and lifestyle and some of the other things we talk about in the book. So, I think many of those practitioners can benefit from the book from that perspective. And then you have the growing and already large number of people like yourself who are personal trainers, health coaches, nutritionists, etc., who I really think are going to play an increasingly important role in this revolution to reinvent healthcare. Tony: Yeah, it so important now for people to really, for patients to be their own advocate, and I don't think we’re living in a time where I remember with my grandparents—if your doctor said something, it was basically gospel and you didn’t question it and you didn't think about it. Now, the first thing people do when they experience a symptom, it's Dr. Google first. So it's super important to equip and arm patients with good information, which I think this book does. Here's a path, here's a path forward for you as a patient. But then it's respectful of the role of doctors, and you highlight many situations where conventional medicine is great. If you break your arm or get in a car accident or have a heart attack or whatever the case may be, yeah, you need a doctor, and you need to go to an emergency room and you need those types of interventions. But it's really in this kind of gray area, it’s really not gray, it’s actually quite clear. And we could probably specify a little bit more, but there’s this middle zone where somebody’s not acutely injured, they’re not acutely in a disease state. They’re in a chronic disease state, or they’re just unwell. And it’s hard for a system that is all about pharmacological interventions, surgical interventions, to deal with a more subtle approach. And that’s where that whole middle ground and acupuncturists and massage therapists and everybody who's in that middle zone. I had clients constantly when I was actively training, constantly asking me questions where I was like, you know what? This is really something they maybe should be taking to their doctor. But guess what? The doctor only has 15 minutes under pressure to see as many patients as they can. I had a friend who was a physician in France. And he was telling me about their medical model, and he would spend tons of time with his patients. And it was actually incentivized for prevention. And here we see some maybe misplaced incentives, and perhaps you can speak a little bit more about that.
The mismatch between our medical paradigm and chronic disease
Chris: Yeah, so, going back to your original comments, I think that the most important thing for people to understand is that our medical model, when it comes to our medical paradigm, is that it evolved during a time when acute problems were the biggest issues. So in 1900, the top three causes of death were all infectious diseases, tuberculosis, typhoid, and pneumonia. And the other reasons people would see the doctor were among those you mentioned, like a broken bone or a gallbladder attack or appendicitis. Tony: War. Chris: Right, injuries, trauma, etc. And so the treatment for that's pretty straightforward. It wasn't always successful, of course, but it was straightforward. You know, if the bone was broken, you set it in a cast. If the gallbladder was swelling, you would take it out. If someone was having appendicitis, you’d remove the appendix. So that's pretty ... it's one problem, one doctor, one treatment. Pretty straightforward. But you fast-forward to today, it's a totally different healthcare landscape. Seven of the top 10 causes of death are chronic disease rather than acute problems now, and 86 percent of the healthcare dollars we spend go toward treating chronic disease. And unlike acute problems, chronic diseases are expensive, difficult to manage and usually last for a lifetime. They don't lend themselves to that one doctor, one problem, one treatment kind of approach. The average chronic disease patient requires multiple doctors, usually one for every different part of the body in our system, and is taking ... Tony: Specialists. Chris: Right, specialists, they’re taking multiple medications in many cases, and they're going to be taking those medications for the rest of their life. So far, it's really, our conventional medical system is amazing for these acute problems. But it's the wrong tool for the job for chronic problems. So that's one issue, and it’s really important to point that out, because we just went through the whole healthcare debate again with the Affordable Care Act and the current administration’s proposal for a replacement, which has not come to fruition. But throughout that entire discussion, it really bothered me that there was an elephant in the room. All the discussion was around insurance. Like, who gets insurance and who doesn’t. And that’s important, it’s important to talk about that. But we have to recognize that health insurance is not the same thing as healthcare. Tony: Yeah. Chris: Health insurance is a method of paying for healthcare. And that’s really crucial to get that difference. Because my argument in the book is that there is no method of paying for healthcare, whether it’s the government, corporations, or individuals, that will be adequate and will be sustainable under the pressure of growing prevalence of chronic disease. It will bankrupt all of us. Government, the corporations, individuals, whoever is responsible for paying for the care will not be able to do it unless we can actually prevent and reverse chronic disease instead of just slapping Band-Aids on it. Tony: I think the analogy you gave in the book was rearranging the deck chairs on the Titanic. “Making a few small tweaks to our current system and expecting that to work is like rearranging the deck furniture on the Titanic as it inexorably sinks into the ocean. Too little, too late.” Chris: Yeah, exactly. That’s the argument about insurance. As the whole ship goes under, sinks under. The other problems you mentioned are very real also. So we have a misalignment of incentives, like the insurance industry, for example, doesn't benefit when the cost of care shrinks because they only make more money when the overall expenditures rise. So it's actually not in their best interest necessarily to seek out the most cost-effective solutions.
Drug companies and conflicts of interest
Chris: And then of course, we have drug companies. People are pretty well aware of the conflicts of interest there. It’s in their interest to sell drugs, and even when that’s not in the interests of the general public or the patients or the doctors. In many cases, it’s not in their interest either. So the best example of this is a recent one. We’re in the midst of an opioid crisis, the worst we’ve ever seen by far, and the DEA has been wanting to create new regulations that restrict a pharmacy’s ability to sell opioids in ways that will protect people. So, for example, there was a pharmacy in West Virginia in a town that was tiny. It had like 30,000 people in this town, and they had ordered something like nine million opioid pills in the last year. It was clearly a front, like there’s clearly something shady going on there. There's no way that 30,000 people in that town needed nine million opioid pills, and yet there are no regulations to actually prevent that from happening. And so, the DEA had proposed some regulations to just safely protect people from that kind of thing. And the Big Pharma lobby basically shut that down and they played a big role in writing a law that limits the DEA's ability to do that kind of regulation in the midst of the worse opioid crisis ever. And to put this in perspective, we hear a lot about the gun lobbies and their control. They spend about $10.5 million lobbying Congress, I think, per year. And Big Pharma, they spent $250 million. Tony: Wow. Chris: Twenty-five-fold higher. Tony: It's really tragic. I actually, I don’t think we’ve ever talked about this, but I grew up in South Florida, which was kind of ground zero for the opioid epidemic. And I remember in high school down in Miami and West Palm Beach, and kids would get a hold of a contact or whatever, somebody that had a prescription and basically would end up being a de facto drug dealer vis-à-vis a pill mill, etc. The kid across the street from me died, multiple kids in my high school died, multiple kids went into in-treatment programs, some of them battled addictions for decades. Some of them got out of it. Very few got out of it. Some of them didn't and have continued to be plagued with either switching from pharmaceuticals to street drugs like heroin, etc., and then we can see what's happening there. And that's just one example. If we look at drug consumption in the United States, is it that Americans are just that much sicker and we’re in that much more pain than people in other countries? Because we’re consuming far and away more painkillers than any other country on the planet. And I would venture to guess that you could say the same about antidepressants or ADD medication. It's very much a case of misaligned incentives. And incentives are working in the sense of the pharmaceutical companies are doing very well. Chris: Yeah. Who are they working for is the question. Tony: Exactly. Chris: We’re the only country aside from New Zealand that allows direct-to-consumer drug advertising, and I think that's a big part of the problem. But it's not just Big Pharma. We also have conflicts in medical research that, of course, are related to Big Pharma because they pay for two-thirds of all medical research. We have broken payment models, where there's no real incentive or reward for good performance, and in fact, you could argue it's the other way around because doctors are compensated for, usually based on the number of procedures they order and the number of patients they see. So to your point about the doctor in France who is actually incentivized to prevent, rather than just treat disease, we don't have that at all, it's the opposite. And so there are a lot of deeply entrenched issues that we certainly need to address, and that's not essentially what this book is about. There are other books that cover that material really well, and frankly many of those issues are outside of our individual control as clinicians or practitioners.
How clinicians can help create a new paradigm
Chris: We can work toward addressing them, and I think we should, but the good news is that I think that the bigger changes that we need to focus on individually and collectively are addressing the medical paradigm which we’ve talked about, creating a medical paradigm that’s better suited to tackle chronic disease. Addressing the mismatch between our modern diet and lifestyle, and our genes and our biology, which we've, of course, talked a lot about on the show before. And then creating a new way of delivering healthcare that actually supports this new medical paradigm and this more preventative approach. Because those things are all within our control as clinicians. Tony: Yeah. I like how you posed the question, and it was kind of a cool little, I think it was, not Hiroshi, but the person who is in charge of cooking at a Buddhist monastery. And basically a young monk comes up to this older man. He’s like, why are you doing the grunt work, basically washing rice out in the courtyard? And he says, it was like, what was it? “If not me, who? And if not now, when?” And I think that that’s really kind of the core of setting all this stuff up. Talking about the problem is really in the service of pivoting to the solution, and I’m a big believer in thinking globally, thinking big, but acting locally, hyper-locally, like yourself. Chris: Yeah. Tony: And then the people around you and who you can touch and impact. That’s ultimately where the power comes from. So let’s talk about that. What is in people’s power. And you started to describe some of those pillars of a new model. And you describe it as the ADAPT framework. And I don’t know how much you get into this on your regular podcast episodes, but to just kind of lay it out, ADAPT from a big-picture perspective. How does that actually address some of these systemic issues from an individually empowered stance? Chris: Yeah, great question, and before I even go into that, I just want to say I agree that I think the change is going to happen on different levels. So, because a lot ... we’ve talked about this stuff at conferences or even some people who’ve already read the book. They say, oh, this is fantastic. I’m so excited. But how are we going to deal with Big Pharma and the insurance industry and these misaligned incentives and all of that? And can we ever deal with that? The answer is we’re not going to deal with that overnight and it’s going to take a while to unwind those things. Tony: It’s the chronic disease, is what you call... Chris: Exactly, exactly. And I use that analogy in the book. But the good news is that changes can happen very quickly on an individual and local level. And there’s already a lot of evidence of that happening. So my own clinic, CCFM, tripled in size in the last three years alone. We have Cleveland Clinic Center for Functional Medicine, launched by Dr. Mark Hyman, has just blown up like crazy. I mean they started in this tiny space. Now their 17,000-square-foot space, it takes up the whole second floor of the Glickman Tower at Cleveland Clinic. They've got a waitlist of 2,500 patients from nine countries around the world. This is really exciting! The Cleveland Clinic is always on the forefront of the newest trends in medicine, and the fact that they've invested that much money in this speaks volumes. Then we have groups like Iora Health, an organization based in the Rocky Mountain area that’s reversing diabetes using health coaches. So there are lots of really interesting produced concepts, and there's going to be more and more of these. Like we’re doing a pilot program with the Berkeley Fire Department where we’re working with their new recruits to help, we’re implementing a wellness program. Tony: That’s awesome. Chris: To reduce injuries and help with recovery and optimize their performance. And if that goes well, there’s been interest from the wider fire department and in the city of Berkeley as a whole. Robb Wolf’s done some incredible work with Reno that we’ve talked about before. So I think the change is going to happen more quickly on this local grassroots level, and then that's going to start to get the attention of people on a state and federal level. And then it will start to get really interesting.
The three core problems and how to solve them
To answer your question, in my book I basically lay out three core fundamental problems with the healthcare system in the US. And these, I argue, go even deeper than the misaligned incentives and Big Pharma and all of that stuff, although they’re, of course, connected. The first is that there is a profound mismatch between our genes and our biology and our modern diet and lifestyle. And I'm not going to say more about that now because almost everyone listening to this podcast knows exactly what I mean. The second problem is the mismatch between our medical paradigm and chronic disease, which we just talked about. We need a new medical paradigm that is better suited for chronic disease. And then the third is that the way we deliver care in this country is also, it's not set up to support the most important interventions. And we’ve touched on that too, where the average visit with the primary care provider is just actually eight to 12 minutes. Tony, you were talking about 15 minutes. That’s luxurious in our current model. The average amount of time a patient gets to speak before they’re interrupted by the doctor is 12 seconds. Tony: Wow. Chris: So I think it’s pretty clear that if a patient has multiple chronic diseases, which one in four Americans now do, one in two has one chronic disease, and they show up to the doctor’s office and they're on multiple medications, and they had been presenting with a whole set of new symptoms, there’s absolutely no way to provide high-quality care in a 10-minute visit. So we have to change our, not only the paradigm, but also the way that care is delivered. So that was my premise. So it follows then that my solution would address, I would hope at least those three points, right? Each of those three deficiencies. So the ADAPT framework combines an ancestral diet and lifestyle, which addresses that mismatch between our genes and biology in our modern diet and lifestyle. And then Functional Medicine is the new paradigm of medicine that is based on addressing the root cause of health problems, so we can prevent and reverse them instead of just suppressing symptoms. And then the third component is what I call a collaborative practice model, which links licensed providers like medical doctors, nurse practitioners, with what I call allied providers, which include folks like yourself, Tony, health coaches, nutritionists, personal trainers, etc., to provide a much, much higher level of care than what doctors are able to provide on their own. So, again, we're not trying to replace doctors in any, or even conventional medicine. We need people to do colonoscopies and remove cancerous tumors and use all of the incredible amount of training and expertise and skill that they’ve acquired over a lifetime of practice and study. We absolutely want that, but we need to add stuff to that that's not available now. Tony: What that really says to me is, emphasize the importance of community, of connection, of collaboration. We’re social creatures, we’re tribal by nature. That’s another kind of Paleo/ancestral health part of the puzzle. And it would be foolish to think that we can dissect out and silo out all these different aspects of our lives without consequence. I really like this idea of bringing everybody into the fold, and it’s not saying that you can go to just the naturopath, or you can go to just the health coach. Because like I mentioned already, I certainly would’ve been ill-equipped to handle plenty of issues that a client would’ve brought to mind or brought up in conversation during a training session. But it would’ve been really great to say, ah, here's the Functional Medicine practitioner that I recommend you speak with, and to have a good relationship with that person and to be able to, as a health coach, help my clients better by getting them in touch with the right person. And that’s having this network that can really support people throughout their health journey whether it’s just feeling better and more energy, or addressing something like diabetes or hypertension. Which certainly there’s a place for all the players in that kind of scenario.
What this new paradigm looks like
Chris: Absolutely. And let’s use an example just to bring this to life for people. So, imagine you go to the doctor and they do some blood testing for your annual physical. And they find that your fasting blood sugar is 96 or 97. Your hemoglobin A1c is 5.5, and you’ve got triglycerides that are 110, 120, maybe 130. Currently, what would happen is nothing, usually. Tony: You’re not sick enough yet. Chris: Yeah, all of your markers are within the lab range, they say, and that means you’re normal, and so you might get some vague advice about make sure to exercise and follow a good diet. And thank you very much, that’s it. Certainly there are exceptions to the rule, of course. There’s some practitioners who can get a lot more proactive about that. But I can’t tell you how many people, patients I’ve had that have been given that basic line with those kinds of lab results. What could happen is this. The doctor says, “Well, you know, if we think of blood sugar disorders on a spectrum, on the left you’ve got perfect blood sugar. On the right you’ve got full-fledged type 2 diabetes. You’re not on the right yet, you don’t have type 2 diabetes or even technically prediabetes, but you’re progressing along that spectrum. And what we know from a lot of research is that if we don’t intervene now, that you’re going to continue progressing. And in fact, we have studies that show that the average patient who has prediabetes, will progress to full-fledged type 2 diabetes in just five years if it’s not addressed.” So what we want to do is be proactive here. We want to intervene now because it’s much easier to prevent a disease before it occurs than it is to treat it after it’s already occurred. So here’s what we’re going to do. We’re going to set you up with our staff health coach, and they’re going to give you all the support you need to adopt a better diet. They’re actually even going to take you shopping, they’re going to come to your house and clean out your pantry with you, and they're going to give you recipes and meal plans and give you ... totally hold your hand and do everything that they need to to get you on this diet. Because we know that information is not enough. We’ve got lots of studies. I can tell you as a doctor, go eat a healthy diet, and hey, we know that that’s probably not going to happen. Most people know what they should be doing, but they’re not doing it, and it’s not because of lack of information. It’s because they need support, and we’re here to support you. We’ve got this health coach. Furthermore, we've got this great personal trainer named Tony. We’re going to set you up with him and we’re also going to set you up with a gym membership. And the good news is, your insurance is going to pay for all this. They’re going to pay for the health coach, they’re going to pay for the gym membership, they’re going to pay for your sessions with Tony. And in six months’ time, you’re going to come back here and we’re going to retest your blood markers and I can almost guarantee that if you stick with the program, you’re going to have normal blood sugar by that time. And throughout that period you’re going to have weekly check-ins with a health coach, you’re going to have training sessions. And not only will your blood sugar be normal, you’re going to lose weight, your energy levels are going to go up, your sleep’s going to get better, you’re going to feel more confident and empowered because you’re making these changes, and you’re going to feel like a different person. Now that’s totally possible.
How do we pay for this? Is it scalable?
Chris: I can hear some people saying, “Oh, how are we going to pay for that? That’s ridiculous.” Tony: Is it scalable? Chris: The question we should be asking is, is treating type 2 diabetes scalable? Because I mentioned this in the book, it costs $14,000 a year to treat a single patient with type 2 diabetes. So let’s imagine that this patient progresses. We don’t intervene, five years later they have type 2 diabetes. All of a sudden the healthcare system is spending $14,000 a year paying for that person’s care. And let’s say that that person gets diagnosed at age 40, which is still reasonable these days. The age of diagnosis is dropping more and more, and then let’s say that they live until they’re 85 years old, which is also possible because of our heroic medical interventions that keep people alive a lot longer than they might have been otherwise. So 45 years living with type 2 diabetes, that’s a cost of almost $650,000 for one patient to the healthcare system. Tony: And that doesn’t even touch on the lost wages, cost to employers, when someone’s on leave, loss of productivity. And then the cost to the family members. Chris: Absolutely. Tony: People that are actually, are helping the patient, their health is going to be going down too. Chris: Yeah. Nor does it touch on the qualitative aspects. Being immobilized, not being able to play with your grandkids, all of that stuff. But let’s just even forget about that for a second—$650,000, okay? And then the CDC recently came out with statistics saying that 100 million Americans have either prediabetes or diabetes, and 88 percent of people with prediabetes don’t even know that they have it. Which means they're almost certainly going to progress, right? If you do the math and you multiply 100 million people times even $14,000 for one year, you get a number that’s so large, I don’t even know what it is. It’s like a google something. It’s like, it has so many zeros after it, I don’t even know how to characterize it. But then if you multiply 100 million times like 20 or 30 years, it’s more money than there is in the world. It's like it's not going to happen. Tony: Not sustainable, not scalable. Chris: Not sustainable, not scalable. So let’s say in our example that we ... the healthcare system spends $10,000, which is way more than would be necessary, but let’s even say we buy the person’s groceries for three months. And their gym membership and their trainer, and their health coach, and those weekly, let’s say we spend $10,000. We’re just super generous and we spend $10,000 for that six-month period. Again, the research and my clinical experience indicates with near certainty that if the person is at that stage of not even prediabetic and we intervene, there’s like almost no chance that it’s not going to, we’re not going to be able to normalize that person’s blood sugar. And if they do that and they stick with it and they are able to do that because they now have support rather than just information, we’ve just saved the healthcare system $640,000 over the course of that patient’s lifetime. And that’s a conservative estimate, as you say. We're not including even the indirect costs. Tony: Right, right. Chris: I think that this is not only possible, it's going to become necessary. And whether we get there with a proactive approach where we decide to move in this direction and we make these changes or whether we get there because we absolutely have no choice, we’re going to get there. Tony: Yeah. I mean it really sounds like we can’t afford to not do this. Chris: Exactly. Tony: And if we get to that point where we continue down the reactive path and we wait until there’s a total collapse, it might be too late, just to put it frankly. And it’s going to come out at a huge, not just financial cost, a huge human cost. Chris: Yeah, it’s going to be, we can use the chronic disease metaphor again, it’s a lot easier to prevent a problem or reverse it at an earlier stage than it is to wait until the patient is essentially on life support or the healthcare system is on life support. It’s harder to reverse it at that time. And that’s of course why I’m writing the book now because I want to get this message out as far and wide as I can. Tony: Yeah. If not now, when? If not you, who? Go right back to there.
How allied providers are the key
Chris: Exactly. And one more thing about that is the amazing thing, the beauty of this is that it takes about eight years and hundreds of thousands of dollars to train a doctor. And it takes a certain kind of personality and a certain kind of comfort level with science, and a lot of prerequisites. It’s not for everybody. And there’s a ... already we have a shortage of doctors, and that’s predicted to get worse. I’ve seen estimates that suggest by 2025 we’ll have a shortage of 52,000 primary care physicians. So that’s a big deal. [insert image] So we already don’t have enough doctors, it’s already going to get worse, but if you think of healthcare as like a ... I have something in the book called the healthcare population pyramid. And you were referring to it earlier, Tony, where at the very top of that pyramid you’ve got 5 percent of people who are in really acute situations. So they’re in the hospital or they’re in an intensive outpatient care setting. They need the conventional medicine paradigm as it exists, and it’s fantastic for those situations. Then you’ve got another 25 percent of people in that kind of high middle of the pyramid who are dealing with some pretty serious chronic health challenges. So they require more regular care, but they’re not sick enough to be in the hospital or in any kind of ... they’re living their lives, but they’re struggling a lot. A Functional Medicine practitioner/clinician usually working in concert possibly with the conventional specialist of some kind is a really great option for that 25 percent of the pyramid. But then you’ve got the 70 percent at the bottom. So these are people who do, may have health issues, but they’re more minor, so they might have skin problems, or a little bit of brain fog, some difficulties sleeping, some GI issues. And these can be definitely debilitating and total pain, but they’re not at the level of that 25 percent. My argument is that in many cases these people could be very well served by a health coach or nutritionist with good training. And possibly seeing a Functional Medicine provider once or twice a year, or something like that. And the thing is, we can train people in a year or two without an extensive science background to be very, very objective in this role. Because they’re mostly working with patients on changing their behavior. If you think about it, most of the risk factors for chronic disease come down to the wrong behaviors. Eating the wrong diet, not getting enough sleep, not exercising, or exercising too much, or any number of things that come down to choices that we’re making. And so if a skilled health coach who’s trained in things like motivational interviewing and coaching to strengths and other evidence-based principles of facilitating behavior change which we have a ton of research on, they can be incredibly effective for that 70 percent of the population. That's the majority of the population. So we’re totally underutilizing these practitioners, and my argument is that they’re going to play a huge role in this future of medicine. And that's of course one reason why we're launching an ADAPT Health Coach Training Program next year to complement the practitioner training program that we've been doing. Because I want to create this ecosystem we've been talking about where you have all of these different types of practitioners working to the maximum of their training and ability and scope of practice and supporting each other and therefore providing the highest level of care to patients. Tony: That certainly kind of perks my ears up hearing about the ADAPT health coach option and something that I’m personally interested in. So who knows? Maybe I can get in on that. We can talk about it again in the future. Chris: Yeah, for sure. For sure. Tony: So, for this particular book, for Unconventional Medicine, people are fired up, they’re hearing about it, they’re like, “Okay, this resonates with me. I’m a practitioner, I’m an allied health provider, I’m a patient, I’m ready. Now’s the time. This is it. We’re going to do this.” What’s the best way for people to get their hands on this thing? Chris: Well not surprisingly, Amazon. They have the best way to get your hands on anything. So it’s available in paperback, Kindle, and audiobook. We’re hoping [the audiobook] is going to be out today, the day this podcast is released. But it might be another two or three days. They’re just taking their sweet time to approve it. I narrated the audiobook myself. So you podcast listeners, I figured you might be into that, since you like to listen. Tony: They know your voice. Chris: Yeah, and just listening to something instead of reading it perhaps. So to that end, we have a special offer for podcast listeners, because I appreciate your support and I know many of you are already part of this movement, and some are wanting to get involved. So if you buy that paperback or Kindle version between now and Sunday night, you’ll get some really cool bonuses. The first is a free copy of the audiobook. So again, we wanted to include that for podcast listeners, since we figured you guys and gals are probably interested in audio. But there are two other things that are really, I think, fantastic. And one, they’re both tools to help you be more confident and persuasive and factual when you share your passion for Functional Medicine and an ancestral diet and lifestyle. Because we’ve had a lot of questions from people, both practitioners and non-practitioners alike. They say, “Oh, how do I talk about this stuff to my sister at Thanksgiving?” Tony: “Isn’t that that caveman diet?” Chris: Yeah, exactly. All of our ancestors died when they were 30, so why should we even care? How do you respond to those arguments? Or if you start talking about Functional Medicine and maybe one of your conventional medicine colleagues says, “Oh, that’s just, I saw something on Science-based Medicine that said that was all just hooey. There’s nothing to it. How do you respond to that?” So what we wanted to do is give people the ammunition they needed in a respectful way. You know, this isn’t about getting the better of somebody. It’s about responding in a factual and convincing but respectful way. So we’ve got two different, we’re calling these the Power Packs. And one is for practitioners, so clinicians, health coaches, nutritionists, trainers, etc., and these are facts, research that you can reference and persuasive reasons for your clients or patients or colleagues to consider this Functional Medicine and ancestral diet and lifestyle approach. And then we have one for non-practitioners called the Supporter Power Pack. And these are smart answers and compelling comebacks, again respectful, for those common objections that you hear when you start talking about this stuff with your friends and family. So these bonuses are available until Sunday night [November 12, 2017] at 11:59 p.m. Pacific Time. So you’ve got a few days to act on that, and you can go to ... we set up a special link for you to get these and that’s Kresser.co/bonus. That’s Kresser.co/bonus. So head over there to get your Power Packs and your free audiobook, and that’s after you purchase either the paperback or Kindle. There’ll be a place where you enter your order number and we ask for some information just to verify, and I hope you enjoy those and get a lot out of them. Because they were actually really fun to put together. Tony: Yeah, I think the audiobook is huge. I like to listen to audiobooks when I’m driving around town or outside getting some exercise. Chris: Yeah. Tony: So, no excuses when you make it that easy. Chris: Yeah, yeah. So, Tony, thanks so much for doing this. This has been really fun to talk to you, as it always is. And I appreciate it. Tony: Actually, I wanted to throw in one extra little special thing, as we mentioned, at the top of the show. I spent 10 years as a personal trainer in the trenches, I was involved with Paleo Magazine for many, many years, going to all the events, and for me kind of an evolution in my professional life was, how do I impact more people? How do I help more people? And at first I was working one on one, and then it was as a facility manager helping other trainers and coaches get better. And then I was able to scale it up that way. And last year I had an opportunity to join the team over at Natural Force, which is all-natural, nutritional products, and I basically said, “You know what? I’m going to go all in on this because if I can touch a million people through really good, high-quality nutrition, that’s me maximizing my impact and really kind of living my purpose.” So one of the things I wanted to do today is put it out there for anyone listening who maybe uses collagen or MCT oil or whey protein. We really bend over backwards to source the best ingredients in the world, no additives, all that stuff. Everything is as clean as we can possibly make it. It takes a lot of work, working with manufacturers. Kind of like what you were saying, how patients have to know how to talk to their doctor. I don’t think people really realize, and I didn’t realize until I got on the inside, how much work it is for a brand to work with their manufacturers to convince them to get outside of the conventional mold. So it’s the kind of unconventional nutrition is really what we’re pushing here. So I set up a discount code for any Revolution Health listeners. Go to NaturalForce.com, use coupon code “unconventional” and get $10 off plus free shipping on your order. So I just want to put that out there as just a little extra bonus for anybody, and I would certainly love to help in that way and really get some good, high-quality nutrition into people’s hands. Chris: Awesome. Yeah, and there’s so many ways people can help, and I ... at Paleo f(x) we’ve see the growth of companies that are serving this space, and it's amazing. Like the products that are available now. I had breakfast this morning, I had some eggs and kale and parsley and a little bit of bacon in a couple of cassava flour tortillas. Breakfast burritos. Whoever thought I’d be having a breakfast burrito again? Tortillas are made from completely cassava flour. They’re autoimmune friendly and they’re grain-free tortillas. It’s incredible. Tony: I think I might have some of those in my fridge as well. Chris: Yeah. I mean there’s so many things. And these people, they’re serving this movement with that kind of work. So it’s great to see. Tony: It takes a village, man. Chris: It does. Thanks again, Tony. I really appreciate it. Thank you, everybody. So again, Kresser.co/bonus to pick up your free audiobook and the other bonuses, and I hope you can all join me in this revolution to reinvent healthcare. We need you, whatever your background and goals. Take care, everybody.
Source: http://chriskresser.com
November 08, 2017 at 04:12PM
1 note
·
View note
Text
Every parent at some point in their children’s lives with deal with picky eaters. Children’s palates change so much during their first years that is hard as a parent to know what a toddler will or will not eat on a weekly basis.
Currently in our household, we are dealing with a fussy or picky eater. My otherwise food-loving toddler decided a few months ago that he no longer loves vegetables and that he would only eat fruit, eggs, chicken strips, pasta, bread, potatoes and rice. You know, the toddler favorites. He still eats most fruits I put in front of him, but as a concerned parent, I wanted him to branch out and eat more vegetables as well. So I started trying out different strategies to get him to eat more of the good stuff.
Over these past few months, there were some things that resonated with me and also some valuable finds! So I thought I would share with you in case you are also dealing with a picky eater.
For those who prefer videos, check out my collaboration with Beech-Nut® Naturals™ on YouTube.
Tips on how to deal with a picky eater
[ 1 ] Be a role model
Kids will emulate what their parents do, so it’s only natural they will want to eat what you eat. Any good habits that you want your kids to have will have to be learned from you. Eat as many vegetables you can during meals and snacks and let them see you.
[ 2 ] Serve vegetables with every meal
Even if your kids don’t eat certain vegetables or are stuck in the “white foods”(bread, pasta, potatoes) phase, serve it with every meal. If kids see it on the table, it’s more likely they will associate that as a normal event and consider vegetables an essential part of every meal.
[ 3 ] Don’t stick with what they will eat
I made this mistake, because it was much easier and I thought my son would starve if he didn’t eat anything, but kids won’t starve. If they are hungry, they will eat. By giving them just things they will eat, you are perpetuating those bad habits and possibly raising even pickier eaters.
These days, I serve 1/3 of food I know he will eat, 1/3 of food he eats sometimes and 1/3 of food that he doesn’t eat.
Of course, if you notice your child is loosing weight or shows signs of hunger, it’s time to talk to a pediatrician. There are other things that can be happening such as sensory issues or problems with chewing.
[ 4 ] Hide vegetables
Some people say you shouldn’t do this, because 1) you can create distrust in your children and 2) children should learn to eat vegetables in their natural form so they know where they come from.
I disagree with these points, because 1) food is complex – we don’t eat vegetables by itself all the time. Some of the best dishes are combinations of flavors, so if I want my child to be exposed to a diverse world of food, I need to introduce it early and 2) children can, should and will learn where food comes from with other activities such as grocery shopping, gardening, field trips and books.
My philosophy is if hiding veggies gets them to eat it, then so be it. My son doesn’t eat carrots by itself. I’ve tried raw, steamed, mashed, puree, roasted… He just doesn’t like it. But he loves my carrot applesauce muffins, which are packed with carrots.
Most adults have likes and dislikes and I don’t think it is different for children, which brings me to the next point.
[ 5 ] Don’t stress
I used to have that dreaded mom guilt and feel like I was failing, because my child had suddenly decided that chicken fingers was the only thing he would eat. Or so I thought.
Once I started really paying attention, I realized he eats a lot more. He will eat virtually any fruit and there are some vegetables he never says no to. This kid can eat his weight in tomatoes, corn, peas, beans and cucumbers. So, why should I be stressing out if he doesn’t like broccoli and carrots? I shouldn’t and neither should you.
[ 6 ] Try different preparations
As I mentioned before, I tried every preparation for carrots there is and my son still doesn’t like it, but he will eat some vegetables raw or cooked better. It’s about texture. So if your child is not eating green beans one way, try another. You might be surprised.
[ 7 ] Be consistent
Don’t overwhelm you child with every vegetable you see in the store, but continue to present it with every meal. Consistency is key. Even if they don’t eat, make it available. I put small amounts in his tray and if he doesn’t eat it, that is fine. It feels like a waste, but sometimes a few pieces make it in and internally I do a happy dance.
[ 8 ] Act like it’s no big deal
I used to make such a fuss if he ate or didn’t eat something. Then I realized that my son was starting to use food to manipulate me. He would bring things to his mouth and wait for my reaction and either spit it out or throw it on the floor. Now, I act like it doesn’t affect me one way or the other. I keep the celebrations internal so he doesn’t associate any food with my reaction. Sometimes, when introducing him to something new I will serve it to him and walk away and watch him from a distance. That way he is free to form his own judgement on a new food.
[ 9 ] Go back to puree
This was so surprising to me. Recently I was working with Beech-Nut, a brand I used when introducing Roark to solids. One day, I had a thought while looking at the jars- will he eat it if I gave it to him now?
I used a jar with vegetables that he usually doesn’t eat and lo and behold, he ate it – the whole jar and asked for more. I was stunned and of course elated, but how didn’t I think of that before?
[ 10 ] Remove distractions
You know that first point of being a role model and that kids will emulate what you do? Well, my husband and I were a childless couple for over 10 years of marriage and we developed some bad habits – watching tv during dinner was one of them. Naturally, our son picked up on this and became hooked as well. He would take ages to eat, because he was so distracted.
Now, I remove all distractions and the only thing to entertain him is his food and our conversations. No more TV or phones are allowed at dinnertime. R eats much faster and is more deliberate on how he eats. He likes to use utensils and that takes concentration at his age.
[ 11 ] Serve vegetables with a dip
R loves humus and will eat almost anything dipped in it. Most times he will just lick it off the vegetable, but sometimes he will take a bite. Humus is super healthy so either way, I see that as a win. He also loves tomato sauce, so I give him vegetables to dip in it. Other dips could be yogurt, peanut butter or even dressing.
[ 12 ] Get kids involved if they are old enough
R is too young for cooking. He likes to watch, but can’t quite help yet. However, he loves grocery shopping. I let him pick fruit and when we get home, I let him try it. Recently he picked some plums and loved them.
[ 13 ] Remember it’s just phase
Children’s palates change a lot faster than ours. What your child liked or disliked a month ago, may not be what he/she likes now. That’s ok. Just keep introducing the same things and also new foods, and eventually they will find foods they love.
Sure, some people never grow out of being a picky eater, but most of us eat more than 5 foods, right?
[ 14 ] Don’t force it
It causes trauma when you try to force feed a child. I know this from first hand experience. I was a picky eater and when I 4-6 years old, a family member tried to make me eat raw tomatoes by force feeding it to me.
I didn’t eat raw tomatoes until I was in my late twenties and I only eat it now when it’s mixed with other things like bruschetta or salsa. So please, don’t force feed your children.
I hope these tips on how to deal with a picky eater help you find a trick that works for your child. Remember, parenting is hard work and although there are many books on the subject, every child is different. Listen to your gut and do whatever works for you!
If you have any more tips, I would love to hear it. Please leave them in the comments below!
Jana
Tips on how to deal with picky eater #tips #parenting #blogger #toddler #momlife #motherhood Every parent at some point in their children's lives with deal with picky eaters. Children's palates change so much during their first years that is hard as a parent to know what a toddler will or will not eat on a weekly basis.
#fussy eater#hacks#how to deal with picky eaters#how to get kids to eat more vegetables#motherhood#parenting#tips#toddlers
0 notes
Text
RHR: A Three-Step Plan to Fix Conventional Healthcare
In this episode we discuss:
The patient case that inspired the book
Who is this book for?
The mismatch between our medical paradigm and chronic disease
Drug companies and conflicts of interest
How clinicians can help create a new paradigm
The three core problems and how to solve them
What this new paradigm looks like
How do we pay for this? Is it scalable?
How allied providers are the key
Show notes:
Unconventional Medicine by Chris Kresser
Special offer for RHR podcast listeners - get the audiobook free if you buy the book by November 12th.
NaturalForce.com - use coupon “unconventional” and get $10 plus free shipping
[smart_track_player url="http://traffic.libsyn.com/thehealthyskeptic/RHR_-_A_Three-Step_Plan_to_Fix_Conventional_Healthcare.mp3" title="A Three-Step Plan to Fix Conventional Healthcare" artist="Chris Kresser" ]
youtube
Chris Kresser: Hey, everybody, Chris Kresser here. Welcome to another episode of Revolution Health Radio. Today we’re going to do something a little different. I am bringing on a guest host, Tony Federico, he’s the VP of marketing for Natural Force Nutrition, a physiology editor for the Journal of Evolution and Health, and a longtime contributor to Paleo Magazine, and also at Paleo f(x), which is where I met Tony, I think, originally, and I have interacted with him the most. And he’s moderated several panels that I’ve been on and I’ve always been impressed with the way he’s done that, the intelligent questions that he asks and just his balanced perspective on ancestral health and Functional Medicine, and this movement overall. Today is the day that my new book, Unconventional Medicine, comes out. It’s now available on Amazon, and I wanted to ask Tony to come take over the podcast and talk with me about the book because I know he’s really interested in all these topics and he’s read quite a bit of the book himself, and I thought it would be more interesting to have a conversation about it than for me to just sit here and do a monologue. So Tony welcome to the show and thanks for being here. Tony Federico: Yeah, thanks for inviting me on, Chris. It’s always fun, when we’ve had the chance to chat, as you said. Whether in person or on podcast, I’m always happy to jump in and dish on health with you. Chris: Fantastic. So, you have read a little bit of the book and we chatted a little bit about it via email, so let’s dive in. Let’s talk a little bit about this book. And for me it was really, it felt like the most important next step that I could take in order to get this message out about ending chronic disease. Tony: Yeah, I got my copy of Unconventional Medicine a couple days ago. I just so happened to have some time off yesterday, and the next thing I knew I was 80 pages in. Chris: Nice. Tony: So, I have to say that, as somebody who’s been in the trenches, I worked as a personal trainer for 10 years, I could really relate to a lot of the things that you were saying in the book, and we’ll get into why a little bit later on in the interview. But you know I just am really impressed with what you put together here, Chris. So let's just, let's get into it, and the first thing that I actually wanted you to maybe tell me a little bit about was how you open the book, which I think is a really great story about a patient named Leo. So I wanted to talk a little bit about Leo and his story and kind of how that inspired you to go down this particular path of unconventional medicine.
The patient case that inspired the book
Chris: Sure, yeah. So, Leo was an eight-year-old boy that I treated in my clinic a few years back, and I wanted to start with his story because it's, unfortunately, a typical story, much more common than, of course, we would like. And it was powerful for me, it was a powerful experience. It's what actually led to me writing this book. So, like way too many other kids of his age, he was suffering from a number of behavioral issues. He was initially diagnosed on the autism spectrum. Eventually they settled on OCD and sensory processing disorder. He would throw these just crazy tantrums where he'd end up crying or screaming inconsolably, writhing on the floor, and this would happen for seemingly the simplest of reasons. Like trying to get his shoes tied as they were going out the door, not cutting the crust off his sandwich in just the right way or getting a stain on his favorite T-shirt. And he was really rigid around his behavior and its environment, everything had to be just right, just the way he wanted it to be, or else he would fly off the handle.
Is a new healthcare paradigm affordable? Scalable? You bet.
His diet was extremely limited, he only ate a handful of foods, pretty much all of which were processed and refined. So crackers, bread, toaster waffles, that sort of thing, and this is part of the kind of OCD-like tendencies. And any time his parents would try to introduce new food, he would go totally ballistic. And they were worried about nutrient deficiency, but they didn't feel like they ... they were just worn down. Any parent who has a kid like this will understand that. It's just they didn’t feel like they had the resources to battle him at every meal. And they took him to a bunch of doctors locally, and that’s where they got those diagnoses. Initially they were kind of relieved to have those, but then after a while they realized that they were just simply labels for symptoms. And when they asked what the treatment was, you can probably guess the answer: medication. Tony: Something to do with drugs. Chris: Something to do with drugs. Yeah. And when they asked how long he would be on that treatment, you can probably also guess the answer. Tony: The rest of your life. Chris: Yeah. Shrug of the shoulders, indefinitely, maybe he'll grow out of it, that sort of thing. And they weren't excited about the idea of of medicating their son, but they were also aware of how much he was suffering, and they were suffering, frankly, too. They decided to give them a try, starting with Adderall, and then they progressed to Ritalin and then antidepressants. And certainly the drugs did seem to help with at least some of the symptoms, but there were a couple issues. Number one, they also caused some very intractable side effects like headache, abdominal pain, irritability, and most significantly, severe sleep disruption. And they had a couple of other kids that were younger than Leo. So they were not happy about the sleep disruption. Nobody was because it was brutal for them and also brutal for Leo. Kids need a lot of sleep, and if they’re waking up throughout the night, that’s going to make ... So that was in some ways worse than the original symptoms they were trying to treat. And then Leo's mom had done quite a bit of research on the effects of these medications and she was scared. Particularly for children and adolescents, some of these drugs have some pretty scary side effects and long-term risks. So what really stood out to me, and I mentioned this in the book, is that not once during this entire process of seeing all these different doctors, primary care provider, psychiatrist, eventually behavioral disorder specialists, did anybody even hint at the possibility that something in Leo's diet or some other underlying issue like a gut problem or nutrient deficiency or heavy metal toxicity or something like that could be contributing to his symptoms. It wasn't even broached as a possibility at any time. Fortunately, Leo's mom, one of her friends followed my work and sent her a couple of articles from my blog. One was on the gut–brain–axis, and I think the other one was on the underlying root causes of behavioral disorders. And so that's what led them to bring Leo to see me, and long story short, we were able to ... we did a bunch of testing, found issues that you might guess at. So, disrupted gut microbiome, SIBO, fungal overgrowth, gluten intolerance, but also intolerance of soy and corn and rice and buckwheat, which were major ingredients in a lot of the processed and refined food products that he ate, and arsenic toxicity because rice milk was the only other beverage he would drink aside from water. And we know that rice products can be high in arsenic. So, we, over several months, it definitely wasn't easy to address these problems because of his OCD-like tendencies and his picky eating habits. But after several months he was like a different kid. His teacher even called home and was like, “What have you done with Leo and who’s this kid that you’re sending in?” Because it was a big issue for her. They often had to come to school and pick him up early because of the behavioral problems. And his diet expanded; he was eating foods he would've thrown against the wall just months before, he was more tolerant of disorder, more relaxed in his environment. They were able to travel for the first time in a long time because he wasn't so anxious in unfamiliar environments. His physical symptoms had improved significantly. So they were just over the moon. They couldn't believe it, and toward the end of our treatment together, she said something that really struck me, which was there’s so many kids out there that are like Leo and they’re suffering, they’re not finding help in the conventional system. Tony: Sure. Chris: And their doctors and parents are not even thinking about this stuff. Like it’s not even in most people’s consciousness that if a kid has a behavioral disorder that you should look at these physiological issues. It’s not, for 99 percent of people they don't even go there because they don't know. Tony: Yeah, I mean I think that that was—reading about Leo and reading about a story and certainly there's people that I've known, myself included, who have had very similar experiences—I think it's great to have a narrative like this that you can really connect to because then when you tease it apart, all the pieces really make sense. It makes sense why having doctors treat symptoms has failed, it makes sense why a lack of communication between the health provider network that was supposed to be serving Leo failed. It makes sense why it didn't work when you actually start to tease it out. But then we’re still all, well not all, but most of us are still going down this path and it's an exercise in futility, really. You have an eight-year-old kid who's on powerful stimulant medications, he’s on antidepressants, and it was bad enough for his parents to reach out and to seek those interventions as solutions, and then the side effects are even worse. And that’s just something that just gets you right in the heart. And like you said, he’s not the only one, he’s not the only kid. His parents are not the only parents. And frankly, his doctors are not the only doctors because I can guarantee you that that probably doesn’t really feel good for the practitioner, for the healthcare provider to not get results as well. And they’re working with what they’ve got. Chris: Absolutely. Tony: And trying to use the tools they have. Chris: Yeah, I mean, let’s be clear about this. Everybody is doing the best they can in this situation. The parents are doing the best they can, in the vast majority of situations, parents just love their kids and do everything possible that they can to help their kids thrive. I’m a parent, I know that that’s how I relate to my kid. I know that every parent I know, that’s how they relate to their kids. And I would even, I would say that’s true for doctors too. The vast majority of them are trying to do the best they can with the tools that they have and in the system that they’re working within. And that’s the rub. Tony: Right. Chris: It’s like most doctors I’ve seen have been caring and they’ve wanted to do the right thing, but the question is, can they do the right thing in the conventional medical system as it exists today? And, of course, that’s largely what the book is about.
Who is this book for?
Tony: Yeah, so let’s kind of speak to that specifically. And we’re talking about doctors, we’re talking about medical professionals, we’re talking about patients, and then we didn’t mention it, but where I fit into this formula or potential formula as an allied healthcare provider, as a personal trainer/health coach, is that your audience for this book, do you really see that kind of triad is who you're speaking to here? Chris: Yeah, definitely. I think if you look at the cover of the book, the subtitle is “join the revolution to reverse chronic disease, reinvent healthcare, and create a practice you love.” So that last bit would suggest that it's mostly for practitioners, but that's not true. It is really for anybody that is interested in the ideas of reinventing healthcare and reversing chronic disease. And, in fact, I would argue that that change is going to be initiated by people, primarily by people that are not practitioners. So it's like a grassroots, bottom-up approach, where a good example is with my training program, my ADAPT training program, now that we've been training practitioners in this approach for the last couple years, we always ask people how they learned about my work or how they learned about the training program. And in a surprising number of cases, the answer is from their patients. So these doctors or other practitioners, their patient brings an article in that I wrote or brings something in, tells them about me, and to their credit they’re open-minded enough to go and check it out. And then they like what they see and they end up taking the next step. So people even who have no intention of ever becoming a healthcare practitioner, I think would really benefit from this book if they're interested in these ideas. And then certainly, as you mentioned, licensed healthcare providers like medical doctors or nurse practitioners or physician assistants that are currently working within the conventional paradigm but have already seen its limitations and want to do something different but don't yet know what that might look like. And then people who are outside of the conventional paradigm but are already practitioners, so acupuncturists, chiropractors, naturopathic physicians, etc., in many cases they’re already well aware of the limitations of conventional medicine, which is why they chose to go down a different path. But speaking personally as an acupuncturist myself, I also saw some limitations in the traditional Chinese medicine approach, or at least some differences in the way that I wanted to practice it. I was looking for something that could incorporate modern diagnostic testing and create a more systematic approach that included ancestral diet and lifestyle and some of the other things we talk about in the book. So, I think many of those practitioners can benefit from the book from that perspective. And then you have the growing and already large number of people like yourself who are personal trainers, health coaches, nutritionists, etc., who I really think are going to play an increasingly important role in this revolution to reinvent healthcare. Tony: Yeah, it so important now for people to really, for patients to be their own advocate, and I don't think we’re living in a time where I remember with my grandparents—if your doctor said something, it was basically gospel and you didn’t question it and you didn't think about it. Now, the first thing people do when they experience a symptom, it's Dr. Google first. So it's super important to equip and arm patients with good information, which I think this book does. Here's a path, here's a path forward for you as a patient. But then it's respectful of the role of doctors, and you highlight many situations where conventional medicine is great. If you break your arm or get in a car accident or have a heart attack or whatever the case may be, yeah, you need a doctor, and you need to go to an emergency room and you need those types of interventions. But it's really in this kind of gray area, it’s really not gray, it’s actually quite clear. And we could probably specify a little bit more, but there’s this middle zone where somebody’s not acutely injured, they’re not acutely in a disease state. They’re in a chronic disease state, or they’re just unwell. And it’s hard for a system that is all about pharmacological interventions, surgical interventions, to deal with a more subtle approach. And that’s where that whole middle ground and acupuncturists and massage therapists and everybody who's in that middle zone. I had clients constantly when I was actively training, constantly asking me questions where I was like, you know what? This is really something they maybe should be taking to their doctor. But guess what? The doctor only has 15 minutes under pressure to see as many patients as they can. I had a friend who was a physician in France. And he was telling me about their medical model, and he would spend tons of time with his patients. And it was actually incentivized for prevention. And here we see some maybe misplaced incentives, and perhaps you can speak a little bit more about that.
The mismatch between our medical paradigm and chronic disease
Chris: Yeah, so, going back to your original comments, I think that the most important thing for people to understand is that our medical model, when it comes to our medical paradigm, is that it evolved during a time when acute problems were the biggest issues. So in 1900, the top three causes of death were all infectious diseases, tuberculosis, typhoid, and pneumonia. And the other reasons people would see the doctor were among those you mentioned, like a broken bone or a gallbladder attack or appendicitis. Tony: War. Chris: Right, injuries, trauma, etc. And so the treatment for that's pretty straightforward. It wasn't always successful, of course, but it was straightforward. You know, if the bone was broken, you set it in a cast. If the gallbladder was swelling, you would take it out. If someone was having appendicitis, you’d remove the appendix. So that's pretty ... it's one problem, one doctor, one treatment. Pretty straightforward. But you fast-forward to today, it's a totally different healthcare landscape. Seven of the top 10 causes of death are chronic disease rather than acute problems now, and 86 percent of the healthcare dollars we spend go toward treating chronic disease. And unlike acute problems, chronic diseases are expensive, difficult to manage and usually last for a lifetime. They don't lend themselves to that one doctor, one problem, one treatment kind of approach. The average chronic disease patient requires multiple doctors, usually one for every different part of the body in our system, and is taking ... Tony: Specialists. Chris: Right, specialists, they’re taking multiple medications in many cases, and they're going to be taking those medications for the rest of their life. So far, it's really, our conventional medical system is amazing for these acute problems. But it's the wrong tool for the job for chronic problems. So that's one issue, and it’s really important to point that out, because we just went through the whole healthcare debate again with the Affordable Care Act and the current administration’s proposal for a replacement, which has not come to fruition. But throughout that entire discussion, it really bothered me that there was an elephant in the room. All the discussion was around insurance. Like, who gets insurance and who doesn’t. And that’s important, it’s important to talk about that. But we have to recognize that health insurance is not the same thing as healthcare. Tony: Yeah. Chris: Health insurance is a method of paying for healthcare. And that’s really crucial to get that difference. Because my argument in the book is that there is no method of paying for healthcare, whether it’s the government, corporations, or individuals, that will be adequate and will be sustainable under the pressure of growing prevalence of chronic disease. It will bankrupt all of us. Government, the corporations, individuals, whoever is responsible for paying for the care will not be able to do it unless we can actually prevent and reverse chronic disease instead of just slapping Band-Aids on it. Tony: I think the analogy you gave in the book was rearranging the deck chairs on the Titanic. “Making a few small tweaks to our current system and expecting that to work is like rearranging the deck furniture on the Titanic as it inexorably sinks into the ocean. Too little, too late.” Chris: Yeah, exactly. That’s the argument about insurance. As the whole ship goes under, sinks under. The other problems you mentioned are very real also. So we have a misalignment of incentives, like the insurance industry, for example, doesn't benefit when the cost of care shrinks because they only make more money when the overall expenditures rise. So it's actually not in their best interest necessarily to seek out the most cost-effective solutions.
Drug companies and conflicts of interest
Chris: And then of course, we have drug companies. People are pretty well aware of the conflicts of interest there. It’s in their interest to sell drugs, and even when that’s not in the interests of the general public or the patients or the doctors. In many cases, it’s not in their interest either. So the best example of this is a recent one. We’re in the midst of an opioid crisis, the worst we’ve ever seen by far, and the DEA has been wanting to create new regulations that restrict a pharmacy’s ability to sell opioids in ways that will protect people. So, for example, there was a pharmacy in West Virginia in a town that was tiny. It had like 30,000 people in this town, and they had ordered something like nine million opioid pills in the last year. It was clearly a front, like there’s clearly something shady going on there. There's no way that 30,000 people in that town needed nine million opioid pills, and yet there are no regulations to actually prevent that from happening. And so, the DEA had proposed some regulations to just safely protect people from that kind of thing. And the Big Pharma lobby basically shut that down and they played a big role in writing a law that limits the DEA's ability to do that kind of regulation in the midst of the worse opioid crisis ever. And to put this in perspective, we hear a lot about the gun lobbies and their control. They spend about $10.5 million lobbying Congress, I think, per year. And Big Pharma, they spent $250 million. Tony: Wow. Chris: Twenty-five-fold higher. Tony: It's really tragic. I actually, I don’t think we’ve ever talked about this, but I grew up in South Florida, which was kind of ground zero for the opioid epidemic. And I remember in high school down in Miami and West Palm Beach, and kids would get a hold of a contact or whatever, somebody that had a prescription and basically would end up being a de facto drug dealer vis-à-vis a pill mill, etc. The kid across the street from me died, multiple kids in my high school died, multiple kids went into in-treatment programs, some of them battled addictions for decades. Some of them got out of it. Very few got out of it. Some of them didn't and have continued to be plagued with either switching from pharmaceuticals to street drugs like heroin, etc., and then we can see what's happening there. And that's just one example. If we look at drug consumption in the United States, is it that Americans are just that much sicker and we’re in that much more pain than people in other countries? Because we’re consuming far and away more painkillers than any other country on the planet. And I would venture to guess that you could say the same about antidepressants or ADD medication. It's very much a case of misaligned incentives. And incentives are working in the sense of the pharmaceutical companies are doing very well. Chris: Yeah. Who are they working for is the question. Tony: Exactly. Chris: We’re the only country aside from New Zealand that allows direct-to-consumer drug advertising, and I think that's a big part of the problem. But it's not just Big Pharma. We also have conflicts in medical research that, of course, are related to Big Pharma because they pay for two-thirds of all medical research. We have broken payment models, where there's no real incentive or reward for good performance, and in fact, you could argue it's the other way around because doctors are compensated for, usually based on the number of procedures they order and the number of patients they see. So to your point about the doctor in France who is actually incentivized to prevent, rather than just treat disease, we don't have that at all, it's the opposite. And so there are a lot of deeply entrenched issues that we certainly need to address, and that's not essentially what this book is about. There are other books that cover that material really well, and frankly many of those issues are outside of our individual control as clinicians or practitioners.
How clinicians can help create a new paradigm
Chris: We can work toward addressing them, and I think we should, but the good news is that I think that the bigger changes that we need to focus on individually and collectively are addressing the medical paradigm which we’ve talked about, creating a medical paradigm that’s better suited to tackle chronic disease. Addressing the mismatch between our modern diet and lifestyle, and our genes and our biology, which we've, of course, talked a lot about on the show before. And then creating a new way of delivering healthcare that actually supports this new medical paradigm and this more preventative approach. Because those things are all within our control as clinicians. Tony: Yeah. I like how you posed the question, and it was kind of a cool little, I think it was, not Hiroshi, but the person who is in charge of cooking at a Buddhist monastery. And basically a young monk comes up to this older man. He’s like, why are you doing the grunt work, basically washing rice out in the courtyard? And he says, it was like, what was it? “If not me, who? And if not now, when?” And I think that that’s really kind of the core of setting all this stuff up. Talking about the problem is really in the service of pivoting to the solution, and I’m a big believer in thinking globally, thinking big, but acting locally, hyper-locally, like yourself. Chris: Yeah. Tony: And then the people around you and who you can touch and impact. That’s ultimately where the power comes from. So let’s talk about that. What is in people’s power. And you started to describe some of those pillars of a new model. And you describe it as the ADAPT framework. And I don’t know how much you get into this on your regular podcast episodes, but to just kind of lay it out, ADAPT from a big-picture perspective. How does that actually address some of these systemic issues from an individually empowered stance? Chris: Yeah, great question, and before I even go into that, I just want to say I agree that I think the change is going to happen on different levels. So, because a lot ... we’ve talked about this stuff at conferences or even some people who’ve already read the book. They say, oh, this is fantastic. I’m so excited. But how are we going to deal with Big Pharma and the insurance industry and these misaligned incentives and all of that? And can we ever deal with that? The answer is we’re not going to deal with that overnight and it’s going to take a while to unwind those things. Tony: It’s the chronic disease, is what you call... Chris: Exactly, exactly. And I use that analogy in the book. But the good news is that changes can happen very quickly on an individual and local level. And there’s already a lot of evidence of that happening. So my own clinic, CCFM, tripled in size in the last three years alone. We have Cleveland Clinic Center for Functional Medicine, launched by Dr. Mark Hyman, has just blown up like crazy. I mean they started in this tiny space. Now their 17,000-square-foot space, it takes up the whole second floor of the Glickman Tower at Cleveland Clinic. They've got a waitlist of 2,500 patients from nine countries around the world. This is really exciting! The Cleveland Clinic is always on the forefront of the newest trends in medicine, and the fact that they've invested that much money in this speaks volumes. Then we have groups like Iora Health, an organization based in the Rocky Mountain area that’s reversing diabetes using health coaches. So there are lots of really interesting produced concepts, and there's going to be more and more of these. Like we’re doing a pilot program with the Berkeley Fire Department where we’re working with their new recruits to help, we’re implementing a wellness program. Tony: That’s awesome. Chris: To reduce injuries and help with recovery and optimize their performance. And if that goes well, there’s been interest from the wider fire department and in the city of Berkeley as a whole. Robb Wolf’s done some incredible work with Reno that we’ve talked about before. So I think the change is going to happen more quickly on this local grassroots level, and then that's going to start to get the attention of people on a state and federal level. And then it will start to get really interesting.
The three core problems and how to solve them
To answer your question, in my book I basically lay out three core fundamental problems with the healthcare system in the US. And these, I argue, go even deeper than the misaligned incentives and Big Pharma and all of that stuff, although they’re, of course, connected. The first is that there is a profound mismatch between our genes and our biology and our modern diet and lifestyle. And I'm not going to say more about that now because almost everyone listening to this podcast knows exactly what I mean. The second problem is the mismatch between our medical paradigm and chronic disease, which we just talked about. We need a new medical paradigm that is better suited for chronic disease. And then the third is that the way we deliver care in this country is also, it's not set up to support the most important interventions. And we’ve touched on that too, where the average visit with the primary care provider is just actually eight to 12 minutes. Tony, you were talking about 15 minutes. That’s luxurious in our current model. The average amount of time a patient gets to speak before they’re interrupted by the doctor is 12 seconds. Tony: Wow. Chris: So I think it’s pretty clear that if a patient has multiple chronic diseases, which one in four Americans now do, one in two has one chronic disease, and they show up to the doctor’s office and they're on multiple medications, and they had been presenting with a whole set of new symptoms, there’s absolutely no way to provide high-quality care in a 10-minute visit. So we have to change our, not only the paradigm, but also the way that care is delivered. So that was my premise. So it follows then that my solution would address, I would hope at least those three points, right? Each of those three deficiencies. So the ADAPT framework combines an ancestral diet and lifestyle, which addresses that mismatch between our genes and biology in our modern diet and lifestyle. And then Functional Medicine is the new paradigm of medicine that is based on addressing the root cause of health problems, so we can prevent and reverse them instead of just suppressing symptoms. And then the third component is what I call a collaborative practice model, which links licensed providers like medical doctors, nurse practitioners, with what I call allied providers, which include folks like yourself, Tony, health coaches, nutritionists, personal trainers, etc., to provide a much, much higher level of care than what doctors are able to provide on their own. So, again, we're not trying to replace doctors in any, or even conventional medicine. We need people to do colonoscopies and remove cancerous tumors and use all of the incredible amount of training and expertise and skill that they’ve acquired over a lifetime of practice and study. We absolutely want that, but we need to add stuff to that that's not available now. Tony: What that really says to me is, emphasize the importance of community, of connection, of collaboration. We’re social creatures, we’re tribal by nature. That’s another kind of Paleo/ancestral health part of the puzzle. And it would be foolish to think that we can dissect out and silo out all these different aspects of our lives without consequence. I really like this idea of bringing everybody into the fold, and it’s not saying that you can go to just the naturopath, or you can go to just the health coach. Because like I mentioned already, I certainly would’ve been ill-equipped to handle plenty of issues that a client would’ve brought to mind or brought up in conversation during a training session. But it would’ve been really great to say, ah, here's the Functional Medicine practitioner that I recommend you speak with, and to have a good relationship with that person and to be able to, as a health coach, help my clients better by getting them in touch with the right person. And that’s having this network that can really support people throughout their health journey whether it’s just feeling better and more energy, or addressing something like diabetes or hypertension. Which certainly there’s a place for all the players in that kind of scenario.
What this new paradigm looks like
Chris: Absolutely. And let’s use an example just to bring this to life for people. So, imagine you go to the doctor and they do some blood testing for your annual physical. And they find that your fasting blood sugar is 96 or 97. Your hemoglobin A1c is 5.5, and you’ve got triglycerides that are 110, 120, maybe 130. Currently, what would happen is nothing, usually. Tony: You’re not sick enough yet. Chris: Yeah, all of your markers are within the lab range, they say, and that means you’re normal, and so you might get some vague advice about make sure to exercise and follow a good diet. And thank you very much, that’s it. Certainly there are exceptions to the rule, of course. There’s some practitioners who can get a lot more proactive about that. But I can’t tell you how many people, patients I’ve had that have been given that basic line with those kinds of lab results. What could happen is this. The doctor says, “Well, you know, if we think of blood sugar disorders on a spectrum, on the left you’ve got perfect blood sugar. On the right you’ve got full-fledged type 2 diabetes. You’re not on the right yet, you don’t have type 2 diabetes or even technically prediabetes, but you’re progressing along that spectrum. And what we know from a lot of research is that if we don’t intervene now, that you’re going to continue progressing. And in fact, we have studies that show that the average patient who has prediabetes, will progress to full-fledged type 2 diabetes in just five years if it’s not addressed.” So what we want to do is be proactive here. We want to intervene now because it’s much easier to prevent a disease before it occurs than it is to treat it after it’s already occurred. So here’s what we’re going to do. We’re going to set you up with our staff health coach, and they’re going to give you all the support you need to adopt a better diet. They’re actually even going to take you shopping, they’re going to come to your house and clean out your pantry with you, and they're going to give you recipes and meal plans and give you ... totally hold your hand and do everything that they need to to get you on this diet. Because we know that information is not enough. We’ve got lots of studies. I can tell you as a doctor, go eat a healthy diet, and hey, we know that that’s probably not going to happen. Most people know what they should be doing, but they’re not doing it, and it’s not because of lack of information. It’s because they need support, and we’re here to support you. We’ve got this health coach. Furthermore, we've got this great personal trainer named Tony. We’re going to set you up with him and we’re also going to set you up with a gym membership. And the good news is, your insurance is going to pay for all this. They’re going to pay for the health coach, they’re going to pay for the gym membership, they’re going to pay for your sessions with Tony. And in six months’ time, you’re going to come back here and we’re going to retest your blood markers and I can almost guarantee that if you stick with the program, you’re going to have normal blood sugar by that time. And throughout that period you’re going to have weekly check-ins with a health coach, you’re going to have training sessions. And not only will your blood sugar be normal, you’re going to lose weight, your energy levels are going to go up, your sleep’s going to get better, you’re going to feel more confident and empowered because you’re making these changes, and you’re going to feel like a different person. Now that’s totally possible.
How do we pay for this? Is it scalable?
Chris: I can hear some people saying, “Oh, how are we going to pay for that? That’s ridiculous.” Tony: Is it scalable? Chris: The question we should be asking is, is treating type 2 diabetes scalable? Because I mentioned this in the book, it costs $14,000 a year to treat a single patient with type 2 diabetes. So let’s imagine that this patient progresses. We don’t intervene, five years later they have type 2 diabetes. All of a sudden the healthcare system is spending $14,000 a year paying for that person’s care. And let’s say that that person gets diagnosed at age 40, which is still reasonable these days. The age of diagnosis is dropping more and more, and then let’s say that they live until they’re 85 years old, which is also possible because of our heroic medical interventions that keep people alive a lot longer than they might have been otherwise. So 45 years living with type 2 diabetes, that’s a cost of almost $650,000 for one patient to the healthcare system. Tony: And that doesn’t even touch on the lost wages, cost to employers, when someone’s on leave, loss of productivity. And then the cost to the family members. Chris: Absolutely. Tony: People that are actually, are helping the patient, their health is going to be going down too. Chris: Yeah. Nor does it touch on the qualitative aspects. Being immobilized, not being able to play with your grandkids, all of that stuff. But let’s just even forget about that for a second—$650,000, okay? And then the CDC recently came out with statistics saying that 100 million Americans have either prediabetes or diabetes, and 88 percent of people with prediabetes don’t even know that they have it. Which means they're almost certainly going to progress, right? If you do the math and you multiply 100 million people times even $14,000 for one year, you get a number that’s so large, I don’t even know what it is. It’s like a google something. It’s like, it has so many zeros after it, I don’t even know how to characterize it. But then if you multiply 100 million times like 20 or 30 years, it’s more money than there is in the world. It's like it's not going to happen. Tony: Not sustainable, not scalable. Chris: Not sustainable, not scalable. So let’s say in our example that we ... the healthcare system spends $10,000, which is way more than would be necessary, but let’s even say we buy the person’s groceries for three months. And their gym membership and their trainer, and their health coach, and those weekly, let’s say we spend $10,000. We’re just super generous and we spend $10,000 for that six-month period. Again, the research and my clinical experience indicates with near certainty that if the person is at that stage of not even prediabetic and we intervene, there’s like almost no chance that it’s not going to, we’re not going to be able to normalize that person’s blood sugar. And if they do that and they stick with it and they are able to do that because they now have support rather than just information, we’ve just saved the healthcare system $640,000 over the course of that patient’s lifetime. And that’s a conservative estimate, as you say. We're not including even the indirect costs. Tony: Right, right. Chris: I think that this is not only possible, it's going to become necessary. And whether we get there with a proactive approach where we decide to move in this direction and we make these changes or whether we get there because we absolutely have no choice, we’re going to get there. Tony: Yeah. I mean it really sounds like we can’t afford to not do this. Chris: Exactly. Tony: And if we get to that point where we continue down the reactive path and we wait until there’s a total collapse, it might be too late, just to put it frankly. And it’s going to come out at a huge, not just financial cost, a huge human cost. Chris: Yeah, it’s going to be, we can use the chronic disease metaphor again, it’s a lot easier to prevent a problem or reverse it at an earlier stage than it is to wait until the patient is essentially on life support or the healthcare system is on life support. It’s harder to reverse it at that time. And that’s of course why I’m writing the book now because I want to get this message out as far and wide as I can. Tony: Yeah. If not now, when? If not you, who? Go right back to there.
How allied providers are the key
Chris: Exactly. And one more thing about that is the amazing thing, the beauty of this is that it takes about eight years and hundreds of thousands of dollars to train a doctor. And it takes a certain kind of personality and a certain kind of comfort level with science, and a lot of prerequisites. It’s not for everybody. And there’s a ... already we have a shortage of doctors, and that’s predicted to get worse. I’ve seen estimates that suggest by 2025 we’ll have a shortage of 52,000 primary care physicians. So that’s a big deal. [insert image] So we already don’t have enough doctors, it’s already going to get worse, but if you think of healthcare as like a ... I have something in the book called the healthcare population pyramid. And you were referring to it earlier, Tony, where at the very top of that pyramid you’ve got 5 percent of people who are in really acute situations. So they’re in the hospital or they’re in an intensive outpatient care setting. They need the conventional medicine paradigm as it exists, and it’s fantastic for those situations. Then you’ve got another 25 percent of people in that kind of high middle of the pyramid who are dealing with some pretty serious chronic health challenges. So they require more regular care, but they’re not sick enough to be in the hospital or in any kind of ... they’re living their lives, but they’re struggling a lot. A Functional Medicine practitioner/clinician usually working in concert possibly with the conventional specialist of some kind is a really great option for that 25 percent of the pyramid. But then you’ve got the 70 percent at the bottom. So these are people who do, may have health issues, but they’re more minor, so they might have skin problems, or a little bit of brain fog, some difficulties sleeping, some GI issues. And these can be definitely debilitating and total pain, but they’re not at the level of that 25 percent. My argument is that in many cases these people could be very well served by a health coach or nutritionist with good training. And possibly seeing a Functional Medicine provider once or twice a year, or something like that. And the thing is, we can train people in a year or two without an extensive science background to be very, very objective in this role. Because they’re mostly working with patients on changing their behavior. If you think about it, most of the risk factors for chronic disease come down to the wrong behaviors. Eating the wrong diet, not getting enough sleep, not exercising, or exercising too much, or any number of things that come down to choices that we’re making. And so if a skilled health coach who’s trained in things like motivational interviewing and coaching to strengths and other evidence-based principles of facilitating behavior change which we have a ton of research on, they can be incredibly effective for that 70 percent of the population. That's the majority of the population. So we’re totally underutilizing these practitioners, and my argument is that they’re going to play a huge role in this future of medicine. And that's of course one reason why we're launching an ADAPT Health Coach Training Program next year to complement the practitioner training program that we've been doing. Because I want to create this ecosystem we've been talking about where you have all of these different types of practitioners working to the maximum of their training and ability and scope of practice and supporting each other and therefore providing the highest level of care to patients. Tony: That certainly kind of perks my ears up hearing about the ADAPT health coach option and something that I’m personally interested in. So who knows? Maybe I can get in on that. We can talk about it again in the future. Chris: Yeah, for sure. For sure. Tony: So, for this particular book, for Unconventional Medicine, people are fired up, they’re hearing about it, they’re like, “Okay, this resonates with me. I’m a practitioner, I’m an allied health provider, I’m a patient, I’m ready. Now’s the time. This is it. We’re going to do this.” What’s the best way for people to get their hands on this thing? Chris: Well not surprisingly, Amazon. They have the best way to get your hands on anything. So it’s available in paperback, Kindle, and audiobook. We’re hoping [the audiobook] is going to be out today, the day this podcast is released. But it might be another two or three days. They’re just taking their sweet time to approve it. I narrated the audiobook myself. So you podcast listeners, I figured you might be into that, since you like to listen. Tony: They know your voice. Chris: Yeah, and just listening to something instead of reading it perhaps. So to that end, we have a special offer for podcast listeners, because I appreciate your support and I know many of you are already part of this movement, and some are wanting to get involved. So if you buy that paperback or Kindle version between now and Sunday night, you’ll get some really cool bonuses. The first is a free copy of the audiobook. So again, we wanted to include that for podcast listeners, since we figured you guys and gals are probably interested in audio. But there are two other things that are really, I think, fantastic. And one, they’re both tools to help you be more confident and persuasive and factual when you share your passion for Functional Medicine and an ancestral diet and lifestyle. Because we’ve had a lot of questions from people, both practitioners and non-practitioners alike. They say, “Oh, how do I talk about this stuff to my sister at Thanksgiving?” Tony: “Isn’t that that caveman diet?” Chris: Yeah, exactly. All of our ancestors died when they were 30, so why should we even care? How do you respond to those arguments? Or if you start talking about Functional Medicine and maybe one of your conventional medicine colleagues says, “Oh, that’s just, I saw something on Science-based Medicine that said that was all just hooey. There’s nothing to it. How do you respond to that?” So what we wanted to do is give people the ammunition they needed in a respectful way. You know, this isn’t about getting the better of somebody. It’s about responding in a factual and convincing but respectful way. So we’ve got two different, we’re calling these the Power Packs. And one is for practitioners, so clinicians, health coaches, nutritionists, trainers, etc., and these are facts, research that you can reference and persuasive reasons for your clients or patients or colleagues to consider this Functional Medicine and ancestral diet and lifestyle approach. And then we have one for non-practitioners called the Supporter Power Pack. And these are smart answers and compelling comebacks, again respectful, for those common objections that you hear when you start talking about this stuff with your friends and family. So these bonuses are available until Sunday night [November 12, 2017] at 11:59 p.m. Pacific Time. So you’ve got a few days to act on that, and you can go to ... we set up a special link for you to get these and that’s Kresser.co/bonus. That’s Kresser.co/bonus. So head over there to get your Power Packs and your free audiobook, and that’s after you purchase either the paperback or Kindle. There’ll be a place where you enter your order number and we ask for some information just to verify, and I hope you enjoy those and get a lot out of them. Because they were actually really fun to put together. Tony: Yeah, I think the audiobook is huge. I like to listen to audiobooks when I’m driving around town or outside getting some exercise. Chris: Yeah. Tony: So, no excuses when you make it that easy. Chris: Yeah, yeah. So, Tony, thanks so much for doing this. This has been really fun to talk to you, as it always is. And I appreciate it. Tony: Actually, I wanted to throw in one extra little special thing, as we mentioned, at the top of the show. I spent 10 years as a personal trainer in the trenches, I was involved with Paleo Magazine for many, many years, going to all the events, and for me kind of an evolution in my professional life was, how do I impact more people? How do I help more people? And at first I was working one on one, and then it was as a facility manager helping other trainers and coaches get better. And then I was able to scale it up that way. And last year I had an opportunity to join the team over at Natural Force, which is all-natural, nutritional products, and I basically said, “You know what? I’m going to go all in on this because if I can touch a million people through really good, high-quality nutrition, that’s me maximizing my impact and really kind of living my purpose.” So one of the things I wanted to do today is put it out there for anyone listening who maybe uses collagen or MCT oil or whey protein. We really bend over backwards to source the best ingredients in the world, no additives, all that stuff. Everything is as clean as we can possibly make it. It takes a lot of work, working with manufacturers. Kind of like what you were saying, how patients have to know how to talk to their doctor. I don’t think people really realize, and I didn’t realize until I got on the inside, how much work it is for a brand to work with their manufacturers to convince them to get outside of the conventional mold. So it’s the kind of unconventional nutrition is really what we’re pushing here. So I set up a discount code for any Revolution Health listeners. Go to NaturalForce.com, use coupon code “unconventional” and get $10 off plus free shipping on your order. So I just want to put that out there as just a little extra bonus for anybody, and I would certainly love to help in that way and really get some good, high-quality nutrition into people’s hands. Chris: Awesome. Yeah, and there’s so many ways people can help, and I ... at Paleo f(x) we’ve see the growth of companies that are serving this space, and it's amazing. Like the products that are available now. I had breakfast this morning, I had some eggs and kale and parsley and a little bit of bacon in a couple of cassava flour tortillas. Breakfast burritos. Whoever thought I’d be having a breakfast burrito again? Tortillas are made from completely cassava flour. They’re autoimmune friendly and they’re grain-free tortillas. It’s incredible. Tony: I think I might have some of those in my fridge as well. Chris: Yeah. I mean there’s so many things. And these people, they’re serving this movement with that kind of work. So it’s great to see. Tony: It takes a village, man. Chris: It does. Thanks again, Tony. I really appreciate it. Thank you, everybody. So again, Kresser.co/bonus to pick up your free audiobook and the other bonuses, and I hope you can all join me in this revolution to reinvent healthcare. We need you, whatever your background and goals. Take care, everybody.
0 notes
Text
RHR: A Three-Step Plan to Fix Conventional Healthcare
In this episode we discuss:
The patient case that inspired the book
Who is this book for?
The mismatch between our medical paradigm and chronic disease
Drug companies and conflicts of interest
How clinicians can help create a new paradigm
The three core problems and how to solve them
What this new paradigm looks like
How do we pay for this? Is it scalable?
How allied providers are the key
Show notes:
Unconventional Medicine by Chris Kresser
Special offer for RHR podcast listeners - get the audiobook free if you buy the book by November 12th.
NaturalForce.com - use coupon “unconventional” and get $10 plus free shipping
[smart_track_player url="http://traffic.libsyn.com/thehealthyskeptic/RHR_-_A_Three-Step_Plan_to_Fix_Conventional_Healthcare.mp3" title="A Three-Step Plan to Fix Conventional Healthcare" artist="Chris Kresser" ]
youtube
Chris Kresser: Hey, everybody, Chris Kresser here. Welcome to another episode of Revolution Health Radio. Today we’re going to do something a little different. I am bringing on a guest host, Tony Federico, he’s the VP of marketing for Natural Force Nutrition, a physiology editor for the Journal of Evolution and Health, and a longtime contributor to Paleo Magazine, and also at Paleo f(x), which is where I met Tony, I think, originally, and I have interacted with him the most. And he’s moderated several panels that I’ve been on and I’ve always been impressed with the way he’s done that, the intelligent questions that he asks and just his balanced perspective on ancestral health and Functional Medicine, and this movement overall. Today is the day that my new book, Unconventional Medicine, comes out. It’s now available on Amazon, and I wanted to ask Tony to come take over the podcast and talk with me about the book because I know he’s really interested in all these topics and he’s read quite a bit of the book himself, and I thought it would be more interesting to have a conversation about it than for me to just sit here and do a monologue. So Tony welcome to the show and thanks for being here. Tony Federico: Yeah, thanks for inviting me on, Chris. It’s always fun, when we’ve had the chance to chat, as you said. Whether in person or on podcast, I’m always happy to jump in and dish on health with you. Chris: Fantastic. So, you have read a little bit of the book and we chatted a little bit about it via email, so let’s dive in. Let’s talk a little bit about this book. And for me it was really, it felt like the most important next step that I could take in order to get this message out about ending chronic disease. Tony: Yeah, I got my copy of Unconventional Medicine a couple days ago. I just so happened to have some time off yesterday, and the next thing I knew I was 80 pages in. Chris: Nice. Tony: So, I have to say that, as somebody who’s been in the trenches, I worked as a personal trainer for 10 years, I could really relate to a lot of the things that you were saying in the book, and we’ll get into why a little bit later on in the interview. But you know I just am really impressed with what you put together here, Chris. So let's just, let's get into it, and the first thing that I actually wanted you to maybe tell me a little bit about was how you open the book, which I think is a really great story about a patient named Leo. So I wanted to talk a little bit about Leo and his story and kind of how that inspired you to go down this particular path of unconventional medicine.
The patient case that inspired the book
Chris: Sure, yeah. So, Leo was an eight-year-old boy that I treated in my clinic a few years back, and I wanted to start with his story because it's, unfortunately, a typical story, much more common than, of course, we would like. And it was powerful for me, it was a powerful experience. It's what actually led to me writing this book. So, like way too many other kids of his age, he was suffering from a number of behavioral issues. He was initially diagnosed on the autism spectrum. Eventually they settled on OCD and sensory processing disorder. He would throw these just crazy tantrums where he'd end up crying or screaming inconsolably, writhing on the floor, and this would happen for seemingly the simplest of reasons. Like trying to get his shoes tied as they were going out the door, not cutting the crust off his sandwich in just the right way or getting a stain on his favorite T-shirt. And he was really rigid around his behavior and its environment, everything had to be just right, just the way he wanted it to be, or else he would fly off the handle.
Is a new healthcare paradigm affordable? Scalable? You bet.
His diet was extremely limited, he only ate a handful of foods, pretty much all of which were processed and refined. So crackers, bread, toaster waffles, that sort of thing, and this is part of the kind of OCD-like tendencies. And any time his parents would try to introduce new food, he would go totally ballistic. And they were worried about nutrient deficiency, but they didn't feel like they ... they were just worn down. Any parent who has a kid like this will understand that. It's just they didn’t feel like they had the resources to battle him at every meal. And they took him to a bunch of doctors locally, and that’s where they got those diagnoses. Initially they were kind of relieved to have those, but then after a while they realized that they were just simply labels for symptoms. And when they asked what the treatment was, you can probably guess the answer: medication. Tony: Something to do with drugs. Chris: Something to do with drugs. Yeah. And when they asked how long he would be on that treatment, you can probably also guess the answer. Tony: The rest of your life. Chris: Yeah. Shrug of the shoulders, indefinitely, maybe he'll grow out of it, that sort of thing. And they weren't excited about the idea of of medicating their son, but they were also aware of how much he was suffering, and they were suffering, frankly, too. They decided to give them a try, starting with Adderall, and then they progressed to Ritalin and then antidepressants. And certainly the drugs did seem to help with at least some of the symptoms, but there were a couple issues. Number one, they also caused some very intractable side effects like headache, abdominal pain, irritability, and most significantly, severe sleep disruption. And they had a couple of other kids that were younger than Leo. So they were not happy about the sleep disruption. Nobody was because it was brutal for them and also brutal for Leo. Kids need a lot of sleep, and if they’re waking up throughout the night, that’s going to make ... So that was in some ways worse than the original symptoms they were trying to treat. And then Leo's mom had done quite a bit of research on the effects of these medications and she was scared. Particularly for children and adolescents, some of these drugs have some pretty scary side effects and long-term risks. So what really stood out to me, and I mentioned this in the book, is that not once during this entire process of seeing all these different doctors, primary care provider, psychiatrist, eventually behavioral disorder specialists, did anybody even hint at the possibility that something in Leo's diet or some other underlying issue like a gut problem or nutrient deficiency or heavy metal toxicity or something like that could be contributing to his symptoms. It wasn't even broached as a possibility at any time. Fortunately, Leo's mom, one of her friends followed my work and sent her a couple of articles from my blog. One was on the gut–brain–axis, and I think the other one was on the underlying root causes of behavioral disorders. And so that's what led them to bring Leo to see me, and long story short, we were able to ... we did a bunch of testing, found issues that you might guess at. So, disrupted gut microbiome, SIBO, fungal overgrowth, gluten intolerance, but also intolerance of soy and corn and rice and buckwheat, which were major ingredients in a lot of the processed and refined food products that he ate, and arsenic toxicity because rice milk was the only other beverage he would drink aside from water. And we know that rice products can be high in arsenic. So, we, over several months, it definitely wasn't easy to address these problems because of his OCD-like tendencies and his picky eating habits. But after several months he was like a different kid. His teacher even called home and was like, “What have you done with Leo and who’s this kid that you’re sending in?” Because it was a big issue for her. They often had to come to school and pick him up early because of the behavioral problems. And his diet expanded; he was eating foods he would've thrown against the wall just months before, he was more tolerant of disorder, more relaxed in his environment. They were able to travel for the first time in a long time because he wasn't so anxious in unfamiliar environments. His physical symptoms had improved significantly. So they were just over the moon. They couldn't believe it, and toward the end of our treatment together, she said something that really struck me, which was there’s so many kids out there that are like Leo and they’re suffering, they’re not finding help in the conventional system. Tony: Sure. Chris: And their doctors and parents are not even thinking about this stuff. Like it’s not even in most people’s consciousness that if a kid has a behavioral disorder that you should look at these physiological issues. It’s not, for 99 percent of people they don't even go there because they don't know. Tony: Yeah, I mean I think that that was—reading about Leo and reading about a story and certainly there's people that I've known, myself included, who have had very similar experiences—I think it's great to have a narrative like this that you can really connect to because then when you tease it apart, all the pieces really make sense. It makes sense why having doctors treat symptoms has failed, it makes sense why a lack of communication between the health provider network that was supposed to be serving Leo failed. It makes sense why it didn't work when you actually start to tease it out. But then we’re still all, well not all, but most of us are still going down this path and it's an exercise in futility, really. You have an eight-year-old kid who's on powerful stimulant medications, he’s on antidepressants, and it was bad enough for his parents to reach out and to seek those interventions as solutions, and then the side effects are even worse. And that’s just something that just gets you right in the heart. And like you said, he’s not the only one, he’s not the only kid. His parents are not the only parents. And frankly, his doctors are not the only doctors because I can guarantee you that that probably doesn’t really feel good for the practitioner, for the healthcare provider to not get results as well. And they’re working with what they’ve got. Chris: Absolutely. Tony: And trying to use the tools they have. Chris: Yeah, I mean, let’s be clear about this. Everybody is doing the best they can in this situation. The parents are doing the best they can, in the vast majority of situations, parents just love their kids and do everything possible that they can to help their kids thrive. I’m a parent, I know that that’s how I relate to my kid. I know that every parent I know, that’s how they relate to their kids. And I would even, I would say that’s true for doctors too. The vast majority of them are trying to do the best they can with the tools that they have and in the system that they’re working within. And that’s the rub. Tony: Right. Chris: It’s like most doctors I’ve seen have been caring and they’ve wanted to do the right thing, but the question is, can they do the right thing in the conventional medical system as it exists today? And, of course, that’s largely what the book is about.
Who is this book for?
Tony: Yeah, so let’s kind of speak to that specifically. And we’re talking about doctors, we’re talking about medical professionals, we’re talking about patients, and then we didn’t mention it, but where I fit into this formula or potential formula as an allied healthcare provider, as a personal trainer/health coach, is that your audience for this book, do you really see that kind of triad is who you're speaking to here? Chris: Yeah, definitely. I think if you look at the cover of the book, the subtitle is “join the revolution to reverse chronic disease, reinvent healthcare, and create a practice you love.” So that last bit would suggest that it's mostly for practitioners, but that's not true. It is really for anybody that is interested in the ideas of reinventing healthcare and reversing chronic disease. And, in fact, I would argue that that change is going to be initiated by people, primarily by people that are not practitioners. So it's like a grassroots, bottom-up approach, where a good example is with my training program, my ADAPT training program, now that we've been training practitioners in this approach for the last couple years, we always ask people how they learned about my work or how they learned about the training program. And in a surprising number of cases, the answer is from their patients. So these doctors or other practitioners, their patient brings an article in that I wrote or brings something in, tells them about me, and to their credit they’re open-minded enough to go and check it out. And then they like what they see and they end up taking the next step. So people even who have no intention of ever becoming a healthcare practitioner, I think would really benefit from this book if they're interested in these ideas. And then certainly, as you mentioned, licensed healthcare providers like medical doctors or nurse practitioners or physician assistants that are currently working within the conventional paradigm but have already seen its limitations and want to do something different but don't yet know what that might look like. And then people who are outside of the conventional paradigm but are already practitioners, so acupuncturists, chiropractors, naturopathic physicians, etc., in many cases they’re already well aware of the limitations of conventional medicine, which is why they chose to go down a different path. But speaking personally as an acupuncturist myself, I also saw some limitations in the traditional Chinese medicine approach, or at least some differences in the way that I wanted to practice it. I was looking for something that could incorporate modern diagnostic testing and create a more systematic approach that included ancestral diet and lifestyle and some of the other things we talk about in the book. So, I think many of those practitioners can benefit from the book from that perspective. And then you have the growing and already large number of people like yourself who are personal trainers, health coaches, nutritionists, etc., who I really think are going to play an increasingly important role in this revolution to reinvent healthcare. Tony: Yeah, it so important now for people to really, for patients to be their own advocate, and I don't think we’re living in a time where I remember with my grandparents—if your doctor said something, it was basically gospel and you didn’t question it and you didn't think about it. Now, the first thing people do when they experience a symptom, it's Dr. Google first. So it's super important to equip and arm patients with good information, which I think this book does. Here's a path, here's a path forward for you as a patient. But then it's respectful of the role of doctors, and you highlight many situations where conventional medicine is great. If you break your arm or get in a car accident or have a heart attack or whatever the case may be, yeah, you need a doctor, and you need to go to an emergency room and you need those types of interventions. But it's really in this kind of gray area, it’s really not gray, it’s actually quite clear. And we could probably specify a little bit more, but there’s this middle zone where somebody’s not acutely injured, they’re not acutely in a disease state. They’re in a chronic disease state, or they’re just unwell. And it’s hard for a system that is all about pharmacological interventions, surgical interventions, to deal with a more subtle approach. And that’s where that whole middle ground and acupuncturists and massage therapists and everybody who's in that middle zone. I had clients constantly when I was actively training, constantly asking me questions where I was like, you know what? This is really something they maybe should be taking to their doctor. But guess what? The doctor only has 15 minutes under pressure to see as many patients as they can. I had a friend who was a physician in France. And he was telling me about their medical model, and he would spend tons of time with his patients. And it was actually incentivized for prevention. And here we see some maybe misplaced incentives, and perhaps you can speak a little bit more about that.
The mismatch between our medical paradigm and chronic disease
Chris: Yeah, so, going back to your original comments, I think that the most important thing for people to understand is that our medical model, when it comes to our medical paradigm, is that it evolved during a time when acute problems were the biggest issues. So in 1900, the top three causes of death were all infectious diseases, tuberculosis, typhoid, and pneumonia. And the other reasons people would see the doctor were among those you mentioned, like a broken bone or a gallbladder attack or appendicitis. Tony: War. Chris: Right, injuries, trauma, etc. And so the treatment for that's pretty straightforward. It wasn't always successful, of course, but it was straightforward. You know, if the bone was broken, you set it in a cast. If the gallbladder was swelling, you would take it out. If someone was having appendicitis, you’d remove the appendix. So that's pretty ... it's one problem, one doctor, one treatment. Pretty straightforward. But you fast-forward to today, it's a totally different healthcare landscape. Seven of the top 10 causes of death are chronic disease rather than acute problems now, and 86 percent of the healthcare dollars we spend go toward treating chronic disease. And unlike acute problems, chronic diseases are expensive, difficult to manage and usually last for a lifetime. They don't lend themselves to that one doctor, one problem, one treatment kind of approach. The average chronic disease patient requires multiple doctors, usually one for every different part of the body in our system, and is taking ... Tony: Specialists. Chris: Right, specialists, they’re taking multiple medications in many cases, and they're going to be taking those medications for the rest of their life. So far, it's really, our conventional medical system is amazing for these acute problems. But it's the wrong tool for the job for chronic problems. So that's one issue, and it’s really important to point that out, because we just went through the whole healthcare debate again with the Affordable Care Act and the current administration’s proposal for a replacement, which has not come to fruition. But throughout that entire discussion, it really bothered me that there was an elephant in the room. All the discussion was around insurance. Like, who gets insurance and who doesn’t. And that’s important, it’s important to talk about that. But we have to recognize that health insurance is not the same thing as healthcare. Tony: Yeah. Chris: Health insurance is a method of paying for healthcare. And that’s really crucial to get that difference. Because my argument in the book is that there is no method of paying for healthcare, whether it’s the government, corporations, or individuals, that will be adequate and will be sustainable under the pressure of growing prevalence of chronic disease. It will bankrupt all of us. Government, the corporations, individuals, whoever is responsible for paying for the care will not be able to do it unless we can actually prevent and reverse chronic disease instead of just slapping Band-Aids on it. Tony: I think the analogy you gave in the book was rearranging the deck chairs on the Titanic. “Making a few small tweaks to our current system and expecting that to work is like rearranging the deck furniture on the Titanic as it inexorably sinks into the ocean. Too little, too late.” Chris: Yeah, exactly. That’s the argument about insurance. As the whole ship goes under, sinks under. The other problems you mentioned are very real also. So we have a misalignment of incentives, like the insurance industry, for example, doesn't benefit when the cost of care shrinks because they only make more money when the overall expenditures rise. So it's actually not in their best interest necessarily to seek out the most cost-effective solutions.
Drug companies and conflicts of interest
Chris: And then of course, we have drug companies. People are pretty well aware of the conflicts of interest there. It’s in their interest to sell drugs, and even when that’s not in the interests of the general public or the patients or the doctors. In many cases, it’s not in their interest either. So the best example of this is a recent one. We’re in the midst of an opioid crisis, the worst we’ve ever seen by far, and the DEA has been wanting to create new regulations that restrict a pharmacy’s ability to sell opioids in ways that will protect people. So, for example, there was a pharmacy in West Virginia in a town that was tiny. It had like 30,000 people in this town, and they had ordered something like nine million opioid pills in the last year. It was clearly a front, like there’s clearly something shady going on there. There's no way that 30,000 people in that town needed nine million opioid pills, and yet there are no regulations to actually prevent that from happening. And so, the DEA had proposed some regulations to just safely protect people from that kind of thing. And the Big Pharma lobby basically shut that down and they played a big role in writing a law that limits the DEA's ability to do that kind of regulation in the midst of the worse opioid crisis ever. And to put this in perspective, we hear a lot about the gun lobbies and their control. They spend about $10.5 million lobbying Congress, I think, per year. And Big Pharma, they spent $250 million. Tony: Wow. Chris: Twenty-five-fold higher. Tony: It's really tragic. I actually, I don’t think we’ve ever talked about this, but I grew up in South Florida, which was kind of ground zero for the opioid epidemic. And I remember in high school down in Miami and West Palm Beach, and kids would get a hold of a contact or whatever, somebody that had a prescription and basically would end up being a de facto drug dealer vis-à-vis a pill mill, etc. The kid across the street from me died, multiple kids in my high school died, multiple kids went into in-treatment programs, some of them battled addictions for decades. Some of them got out of it. Very few got out of it. Some of them didn't and have continued to be plagued with either switching from pharmaceuticals to street drugs like heroin, etc., and then we can see what's happening there. And that's just one example. If we look at drug consumption in the United States, is it that Americans are just that much sicker and we’re in that much more pain than people in other countries? Because we’re consuming far and away more painkillers than any other country on the planet. And I would venture to guess that you could say the same about antidepressants or ADD medication. It's very much a case of misaligned incentives. And incentives are working in the sense of the pharmaceutical companies are doing very well. Chris: Yeah. Who are they working for is the question. Tony: Exactly. Chris: We’re the only country aside from New Zealand that allows direct-to-consumer drug advertising, and I think that's a big part of the problem. But it's not just Big Pharma. We also have conflicts in medical research that, of course, are related to Big Pharma because they pay for two-thirds of all medical research. We have broken payment models, where there's no real incentive or reward for good performance, and in fact, you could argue it's the other way around because doctors are compensated for, usually based on the number of procedures they order and the number of patients they see. So to your point about the doctor in France who is actually incentivized to prevent, rather than just treat disease, we don't have that at all, it's the opposite. And so there are a lot of deeply entrenched issues that we certainly need to address, and that's not essentially what this book is about. There are other books that cover that material really well, and frankly many of those issues are outside of our individual control as clinicians or practitioners.
How clinicians can help create a new paradigm
Chris: We can work toward addressing them, and I think we should, but the good news is that I think that the bigger changes that we need to focus on individually and collectively are addressing the medical paradigm which we’ve talked about, creating a medical paradigm that’s better suited to tackle chronic disease. Addressing the mismatch between our modern diet and lifestyle, and our genes and our biology, which we've, of course, talked a lot about on the show before. And then creating a new way of delivering healthcare that actually supports this new medical paradigm and this more preventative approach. Because those things are all within our control as clinicians. Tony: Yeah. I like how you posed the question, and it was kind of a cool little, I think it was, not Hiroshi, but the person who is in charge of cooking at a Buddhist monastery. And basically a young monk comes up to this older man. He’s like, why are you doing the grunt work, basically washing rice out in the courtyard? And he says, it was like, what was it? “If not me, who? And if not now, when?” And I think that that’s really kind of the core of setting all this stuff up. Talking about the problem is really in the service of pivoting to the solution, and I’m a big believer in thinking globally, thinking big, but acting locally, hyper-locally, like yourself. Chris: Yeah. Tony: And then the people around you and who you can touch and impact. That’s ultimately where the power comes from. So let’s talk about that. What is in people’s power. And you started to describe some of those pillars of a new model. And you describe it as the ADAPT framework. And I don’t know how much you get into this on your regular podcast episodes, but to just kind of lay it out, ADAPT from a big-picture perspective. How does that actually address some of these systemic issues from an individually empowered stance? Chris: Yeah, great question, and before I even go into that, I just want to say I agree that I think the change is going to happen on different levels. So, because a lot ... we’ve talked about this stuff at conferences or even some people who’ve already read the book. They say, oh, this is fantastic. I’m so excited. But how are we going to deal with Big Pharma and the insurance industry and these misaligned incentives and all of that? And can we ever deal with that? The answer is we’re not going to deal with that overnight and it’s going to take a while to unwind those things. Tony: It’s the chronic disease, is what you call... Chris: Exactly, exactly. And I use that analogy in the book. But the good news is that changes can happen very quickly on an individual and local level. And there’s already a lot of evidence of that happening. So my own clinic, CCFM, tripled in size in the last three years alone. We have Cleveland Clinic Center for Functional Medicine, launched by Dr. Mark Hyman, has just blown up like crazy. I mean they started in this tiny space. Now their 17,000-square-foot space, it takes up the whole second floor of the Glickman Tower at Cleveland Clinic. They've got a waitlist of 2,500 patients from nine countries around the world. This is really exciting! The Cleveland Clinic is always on the forefront of the newest trends in medicine, and the fact that they've invested that much money in this speaks volumes. Then we have groups like Iora Health, an organization based in the Rocky Mountain area that’s reversing diabetes using health coaches. So there are lots of really interesting produced concepts, and there's going to be more and more of these. Like we’re doing a pilot program with the Berkeley Fire Department where we’re working with their new recruits to help, we’re implementing a wellness program. Tony: That’s awesome. Chris: To reduce injuries and help with recovery and optimize their performance. And if that goes well, there’s been interest from the wider fire department and in the city of Berkeley as a whole. Robb Wolf’s done some incredible work with Reno that we’ve talked about before. So I think the change is going to happen more quickly on this local grassroots level, and then that's going to start to get the attention of people on a state and federal level. And then it will start to get really interesting.
The three core problems and how to solve them
To answer your question, in my book I basically lay out three core fundamental problems with the healthcare system in the US. And these, I argue, go even deeper than the misaligned incentives and Big Pharma and all of that stuff, although they’re, of course, connected. The first is that there is a profound mismatch between our genes and our biology and our modern diet and lifestyle. And I'm not going to say more about that now because almost everyone listening to this podcast knows exactly what I mean. The second problem is the mismatch between our medical paradigm and chronic disease, which we just talked about. We need a new medical paradigm that is better suited for chronic disease. And then the third is that the way we deliver care in this country is also, it's not set up to support the most important interventions. And we’ve touched on that too, where the average visit with the primary care provider is just actually eight to 12 minutes. Tony, you were talking about 15 minutes. That’s luxurious in our current model. The average amount of time a patient gets to speak before they’re interrupted by the doctor is 12 seconds. Tony: Wow. Chris: So I think it’s pretty clear that if a patient has multiple chronic diseases, which one in four Americans now do, one in two has one chronic disease, and they show up to the doctor’s office and they're on multiple medications, and they had been presenting with a whole set of new symptoms, there’s absolutely no way to provide high-quality care in a 10-minute visit. So we have to change our, not only the paradigm, but also the way that care is delivered. So that was my premise. So it follows then that my solution would address, I would hope at least those three points, right? Each of those three deficiencies. So the ADAPT framework combines an ancestral diet and lifestyle, which addresses that mismatch between our genes and biology in our modern diet and lifestyle. And then Functional Medicine is the new paradigm of medicine that is based on addressing the root cause of health problems, so we can prevent and reverse them instead of just suppressing symptoms. And then the third component is what I call a collaborative practice model, which links licensed providers like medical doctors, nurse practitioners, with what I call allied providers, which include folks like yourself, Tony, health coaches, nutritionists, personal trainers, etc., to provide a much, much higher level of care than what doctors are able to provide on their own. So, again, we're not trying to replace doctors in any, or even conventional medicine. We need people to do colonoscopies and remove cancerous tumors and use all of the incredible amount of training and expertise and skill that they’ve acquired over a lifetime of practice and study. We absolutely want that, but we need to add stuff to that that's not available now. Tony: What that really says to me is, emphasize the importance of community, of connection, of collaboration. We’re social creatures, we’re tribal by nature. That’s another kind of Paleo/ancestral health part of the puzzle. And it would be foolish to think that we can dissect out and silo out all these different aspects of our lives without consequence. I really like this idea of bringing everybody into the fold, and it’s not saying that you can go to just the naturopath, or you can go to just the health coach. Because like I mentioned already, I certainly would’ve been ill-equipped to handle plenty of issues that a client would’ve brought to mind or brought up in conversation during a training session. But it would’ve been really great to say, ah, here's the Functional Medicine practitioner that I recommend you speak with, and to have a good relationship with that person and to be able to, as a health coach, help my clients better by getting them in touch with the right person. And that’s having this network that can really support people throughout their health journey whether it’s just feeling better and more energy, or addressing something like diabetes or hypertension. Which certainly there’s a place for all the players in that kind of scenario.
What this new paradigm looks like
Chris: Absolutely. And let’s use an example just to bring this to life for people. So, imagine you go to the doctor and they do some blood testing for your annual physical. And they find that your fasting blood sugar is 96 or 97. Your hemoglobin A1c is 5.5, and you’ve got triglycerides that are 110, 120, maybe 130. Currently, what would happen is nothing, usually. Tony: You’re not sick enough yet. Chris: Yeah, all of your markers are within the lab range, they say, and that means you’re normal, and so you might get some vague advice about make sure to exercise and follow a good diet. And thank you very much, that’s it. Certainly there are exceptions to the rule, of course. There’s some practitioners who can get a lot more proactive about that. But I can’t tell you how many people, patients I’ve had that have been given that basic line with those kinds of lab results. What could happen is this. The doctor says, “Well, you know, if we think of blood sugar disorders on a spectrum, on the left you’ve got perfect blood sugar. On the right you’ve got full-fledged type 2 diabetes. You’re not on the right yet, you don’t have type 2 diabetes or even technically prediabetes, but you’re progressing along that spectrum. And what we know from a lot of research is that if we don’t intervene now, that you’re going to continue progressing. And in fact, we have studies that show that the average patient who has prediabetes, will progress to full-fledged type 2 diabetes in just five years if it’s not addressed.” So what we want to do is be proactive here. We want to intervene now because it’s much easier to prevent a disease before it occurs than it is to treat it after it’s already occurred. So here’s what we’re going to do. We’re going to set you up with our staff health coach, and they’re going to give you all the support you need to adopt a better diet. They’re actually even going to take you shopping, they’re going to come to your house and clean out your pantry with you, and they're going to give you recipes and meal plans and give you ... totally hold your hand and do everything that they need to to get you on this diet. Because we know that information is not enough. We’ve got lots of studies. I can tell you as a doctor, go eat a healthy diet, and hey, we know that that’s probably not going to happen. Most people know what they should be doing, but they’re not doing it, and it’s not because of lack of information. It’s because they need support, and we’re here to support you. We’ve got this health coach. Furthermore, we've got this great personal trainer named Tony. We’re going to set you up with him and we’re also going to set you up with a gym membership. And the good news is, your insurance is going to pay for all this. They’re going to pay for the health coach, they’re going to pay for the gym membership, they’re going to pay for your sessions with Tony. And in six months’ time, you’re going to come back here and we’re going to retest your blood markers and I can almost guarantee that if you stick with the program, you’re going to have normal blood sugar by that time. And throughout that period you’re going to have weekly check-ins with a health coach, you’re going to have training sessions. And not only will your blood sugar be normal, you’re going to lose weight, your energy levels are going to go up, your sleep’s going to get better, you’re going to feel more confident and empowered because you’re making these changes, and you’re going to feel like a different person. Now that’s totally possible.
How do we pay for this? Is it scalable?
Chris: I can hear some people saying, “Oh, how are we going to pay for that? That’s ridiculous.” Tony: Is it scalable? Chris: The question we should be asking is, is treating type 2 diabetes scalable? Because I mentioned this in the book, it costs $14,000 a year to treat a single patient with type 2 diabetes. So let’s imagine that this patient progresses. We don’t intervene, five years later they have type 2 diabetes. All of a sudden the healthcare system is spending $14,000 a year paying for that person’s care. And let’s say that that person gets diagnosed at age 40, which is still reasonable these days. The age of diagnosis is dropping more and more, and then let’s say that they live until they’re 85 years old, which is also possible because of our heroic medical interventions that keep people alive a lot longer than they might have been otherwise. So 45 years living with type 2 diabetes, that’s a cost of almost $650,000 for one patient to the healthcare system. Tony: And that doesn’t even touch on the lost wages, cost to employers, when someone’s on leave, loss of productivity. And then the cost to the family members. Chris: Absolutely. Tony: People that are actually, are helping the patient, their health is going to be going down too. Chris: Yeah. Nor does it touch on the qualitative aspects. Being immobilized, not being able to play with your grandkids, all of that stuff. But let’s just even forget about that for a second—$650,000, okay? And then the CDC recently came out with statistics saying that 100 million Americans have either prediabetes or diabetes, and 88 percent of people with prediabetes don’t even know that they have it. Which means they're almost certainly going to progress, right? If you do the math and you multiply 100 million people times even $14,000 for one year, you get a number that’s so large, I don’t even know what it is. It’s like a google something. It’s like, it has so many zeros after it, I don’t even know how to characterize it. But then if you multiply 100 million times like 20 or 30 years, it’s more money than there is in the world. It's like it's not going to happen. Tony: Not sustainable, not scalable. Chris: Not sustainable, not scalable. So let’s say in our example that we ... the healthcare system spends $10,000, which is way more than would be necessary, but let’s even say we buy the person’s groceries for three months. And their gym membership and their trainer, and their health coach, and those weekly, let’s say we spend $10,000. We’re just super generous and we spend $10,000 for that six-month period. Again, the research and my clinical experience indicates with near certainty that if the person is at that stage of not even prediabetic and we intervene, there’s like almost no chance that it’s not going to, we’re not going to be able to normalize that person’s blood sugar. And if they do that and they stick with it and they are able to do that because they now have support rather than just information, we’ve just saved the healthcare system $640,000 over the course of that patient’s lifetime. And that’s a conservative estimate, as you say. We're not including even the indirect costs. Tony: Right, right. Chris: I think that this is not only possible, it's going to become necessary. And whether we get there with a proactive approach where we decide to move in this direction and we make these changes or whether we get there because we absolutely have no choice, we’re going to get there. Tony: Yeah. I mean it really sounds like we can’t afford to not do this. Chris: Exactly. Tony: And if we get to that point where we continue down the reactive path and we wait until there’s a total collapse, it might be too late, just to put it frankly. And it’s going to come out at a huge, not just financial cost, a huge human cost. Chris: Yeah, it’s going to be, we can use the chronic disease metaphor again, it’s a lot easier to prevent a problem or reverse it at an earlier stage than it is to wait until the patient is essentially on life support or the healthcare system is on life support. It’s harder to reverse it at that time. And that’s of course why I’m writing the book now because I want to get this message out as far and wide as I can. Tony: Yeah. If not now, when? If not you, who? Go right back to there.
How allied providers are the key
Chris: Exactly. And one more thing about that is the amazing thing, the beauty of this is that it takes about eight years and hundreds of thousands of dollars to train a doctor. And it takes a certain kind of personality and a certain kind of comfort level with science, and a lot of prerequisites. It’s not for everybody. And there’s a ... already we have a shortage of doctors, and that’s predicted to get worse. I’ve seen estimates that suggest by 2025 we’ll have a shortage of 52,000 primary care physicians. So that’s a big deal. [insert image] So we already don’t have enough doctors, it’s already going to get worse, but if you think of healthcare as like a ... I have something in the book called the healthcare population pyramid. And you were referring to it earlier, Tony, where at the very top of that pyramid you’ve got 5 percent of people who are in really acute situations. So they’re in the hospital or they’re in an intensive outpatient care setting. They need the conventional medicine paradigm as it exists, and it’s fantastic for those situations. Then you’ve got another 25 percent of people in that kind of high middle of the pyramid who are dealing with some pretty serious chronic health challenges. So they require more regular care, but they’re not sick enough to be in the hospital or in any kind of ... they’re living their lives, but they’re struggling a lot. A Functional Medicine practitioner/clinician usually working in concert possibly with the conventional specialist of some kind is a really great option for that 25 percent of the pyramid. But then you’ve got the 70 percent at the bottom. So these are people who do, may have health issues, but they’re more minor, so they might have skin problems, or a little bit of brain fog, some difficulties sleeping, some GI issues. And these can be definitely debilitating and total pain, but they’re not at the level of that 25 percent. My argument is that in many cases these people could be very well served by a health coach or nutritionist with good training. And possibly seeing a Functional Medicine provider once or twice a year, or something like that. And the thing is, we can train people in a year or two without an extensive science background to be very, very objective in this role. Because they’re mostly working with patients on changing their behavior. If you think about it, most of the risk factors for chronic disease come down to the wrong behaviors. Eating the wrong diet, not getting enough sleep, not exercising, or exercising too much, or any number of things that come down to choices that we’re making. And so if a skilled health coach who’s trained in things like motivational interviewing and coaching to strengths and other evidence-based principles of facilitating behavior change which we have a ton of research on, they can be incredibly effective for that 70 percent of the population. That's the majority of the population. So we’re totally underutilizing these practitioners, and my argument is that they’re going to play a huge role in this future of medicine. And that's of course one reason why we're launching an ADAPT Health Coach Training Program next year to complement the practitioner training program that we've been doing. Because I want to create this ecosystem we've been talking about where you have all of these different types of practitioners working to the maximum of their training and ability and scope of practice and supporting each other and therefore providing the highest level of care to patients. Tony: That certainly kind of perks my ears up hearing about the ADAPT health coach option and something that I’m personally interested in. So who knows? Maybe I can get in on that. We can talk about it again in the future. Chris: Yeah, for sure. For sure. Tony: So, for this particular book, for Unconventional Medicine, people are fired up, they’re hearing about it, they’re like, “Okay, this resonates with me. I’m a practitioner, I’m an allied health provider, I’m a patient, I’m ready. Now’s the time. This is it. We’re going to do this.” What’s the best way for people to get their hands on this thing? Chris: Well not surprisingly, Amazon. They have the best way to get your hands on anything. So it’s available in paperback, Kindle, and audiobook. We’re hoping [the audiobook] is going to be out today, the day this podcast is released. But it might be another two or three days. They’re just taking their sweet time to approve it. I narrated the audiobook myself. So you podcast listeners, I figured you might be into that, since you like to listen. Tony: They know your voice. Chris: Yeah, and just listening to something instead of reading it perhaps. So to that end, we have a special offer for podcast listeners, because I appreciate your support and I know many of you are already part of this movement, and some are wanting to get involved. So if you buy that paperback or Kindle version between now and Sunday night, you’ll get some really cool bonuses. The first is a free copy of the audiobook. So again, we wanted to include that for podcast listeners, since we figured you guys and gals are probably interested in audio. But there are two other things that are really, I think, fantastic. And one, they’re both tools to help you be more confident and persuasive and factual when you share your passion for Functional Medicine and an ancestral diet and lifestyle. Because we’ve had a lot of questions from people, both practitioners and non-practitioners alike. They say, “Oh, how do I talk about this stuff to my sister at Thanksgiving?” Tony: “Isn’t that that caveman diet?” Chris: Yeah, exactly. All of our ancestors died when they were 30, so why should we even care? How do you respond to those arguments? Or if you start talking about Functional Medicine and maybe one of your conventional medicine colleagues says, “Oh, that’s just, I saw something on Science-based Medicine that said that was all just hooey. There’s nothing to it. How do you respond to that?” So what we wanted to do is give people the ammunition they needed in a respectful way. You know, this isn’t about getting the better of somebody. It’s about responding in a factual and convincing but respectful way. So we’ve got two different, we’re calling these the Power Packs. And one is for practitioners, so clinicians, health coaches, nutritionists, trainers, etc., and these are facts, research that you can reference and persuasive reasons for your clients or patients or colleagues to consider this Functional Medicine and ancestral diet and lifestyle approach. And then we have one for non-practitioners called the Supporter Power Pack. And these are smart answers and compelling comebacks, again respectful, for those common objections that you hear when you start talking about this stuff with your friends and family. So these bonuses are available until Sunday night [November 12, 2017] at 11:59 p.m. Pacific Time. So you’ve got a few days to act on that, and you can go to ... we set up a special link for you to get these and that’s Kresser.co/bonus. That’s Kresser.co/bonus. So head over there to get your Power Packs and your free audiobook, and that’s after you purchase either the paperback or Kindle. There’ll be a place where you enter your order number and we ask for some information just to verify, and I hope you enjoy those and get a lot out of them. Because they were actually really fun to put together. Tony: Yeah, I think the audiobook is huge. I like to listen to audiobooks when I’m driving around town or outside getting some exercise. Chris: Yeah. Tony: So, no excuses when you make it that easy. Chris: Yeah, yeah. So, Tony, thanks so much for doing this. This has been really fun to talk to you, as it always is. And I appreciate it. Tony: Actually, I wanted to throw in one extra little special thing, as we mentioned, at the top of the show. I spent 10 years as a personal trainer in the trenches, I was involved with Paleo Magazine for many, many years, going to all the events, and for me kind of an evolution in my professional life was, how do I impact more people? How do I help more people? And at first I was working one on one, and then it was as a facility manager helping other trainers and coaches get better. And then I was able to scale it up that way. And last year I had an opportunity to join the team over at Natural Force, which is all-natural, nutritional products, and I basically said, “You know what? I’m going to go all in on this because if I can touch a million people through really good, high-quality nutrition, that’s me maximizing my impact and really kind of living my purpose.” So one of the things I wanted to do today is put it out there for anyone listening who maybe uses collagen or MCT oil or whey protein. We really bend over backwards to source the best ingredients in the world, no additives, all that stuff. Everything is as clean as we can possibly make it. It takes a lot of work, working with manufacturers. Kind of like what you were saying, how patients have to know how to talk to their doctor. I don’t think people really realize, and I didn’t realize until I got on the inside, how much work it is for a brand to work with their manufacturers to convince them to get outside of the conventional mold. So it’s the kind of unconventional nutrition is really what we’re pushing here. So I set up a discount code for any Revolution Health listeners. Go to NaturalForce.com, use coupon code “unconventional” and get $10 off plus free shipping on your order. So I just want to put that out there as just a little extra bonus for anybody, and I would certainly love to help in that way and really get some good, high-quality nutrition into people’s hands. Chris: Awesome. Yeah, and there’s so many ways people can help, and I ... at Paleo f(x) we’ve see the growth of companies that are serving this space, and it's amazing. Like the products that are available now. I had breakfast this morning, I had some eggs and kale and parsley and a little bit of bacon in a couple of cassava flour tortillas. Breakfast burritos. Whoever thought I’d be having a breakfast burrito again? Tortillas are made from completely cassava flour. They’re autoimmune friendly and they’re grain-free tortillas. It’s incredible. Tony: I think I might have some of those in my fridge as well. Chris: Yeah. I mean there’s so many things. And these people, they’re serving this movement with that kind of work. So it’s great to see. Tony: It takes a village, man. Chris: It does. Thanks again, Tony. I really appreciate it. Thank you, everybody. So again, Kresser.co/bonus to pick up your free audiobook and the other bonuses, and I hope you can all join me in this revolution to reinvent healthcare. We need you, whatever your background and goals. Take care, everybody.
RHR: A Three-Step Plan to Fix Conventional Healthcare published first on https://chriskresser.com
0 notes
Text
Friends in Dark Places [remastered, ch 12]
pairing: moxiety, eventual logince, background eventual remile, background eventual remy/emile/deceit
WARNINGS: sensory overload, panic attacks, self hate, school dances, swearing, food mentions, kissing, embarrassment, rumors, eating, possibly something else
tag list: @hufflepuffgirl01 @cocobearthe4th @cas-is-a-hunter @band-be-boss-blog @theunoriginaldaisy
a/n: jsyk, it’s totally okay to ask for a modified chapter if you need it or if i need to add tags! i get it, and it’s no problem for me to quick edit a chapter or whatever :) also, feel free to send requests or questions that you have!
a/n 2: :)
chapter 1 - chapter 2 - chapter 3 - chapter 4 - chapter 5 - chapter 6 -chapter 7 - chapter 8 - chapter 9 - chapter 10 - chapter 11 - chapter 13
companion fics: exes and ‘oh’s
consider buying me a coffee
-
“So, Virgil. Are you going to prom?” Roman casually asked before popping a french fry in his mouth.
“Um, I don’t know. I wasn’t planning on it.” Virgil absently dipped a chicken nugget into the pool of ranch on his tray. He really hadn’t thought about prom that much. Plus, the thought of a whole bunch of his peers stuck in one room together, probably grinding with their respective dates, was not a pleasant one.
“Awww, kiddo! You should go! You could come with us; we’re going to grab dinner and everything,” Patton whined.
“I mean, I guess?” Virgil grimaced as he weighed the options. “But don’t I have to rent a tux? I don’t have money for that, especially not after what happened on Monday. I’d be surprised to find my credit card still working with all of that in mind.”
Logan jumped into the conversation. “You would have to rent a tux, yes, but the three of us would be more than happy to help cover your expenses. We value you as a member of our friend group, and we wouldn’t exclude you from something just because you couldn’t afford it.”
Virgil opened his mouth to argue, but Roman interjected, “Dude, seriously. Just let us do this for you. It’ll be fun!”
“Plus, Ro already bought you a ticket,” Logan added and held out a small slip of cardstock. Westview Junior Prom.
Well, Virgil Thomas was now going to prom.
---
“Hey, Pat? Can you help me with my tie?” Virgil called from his bathroom. He had been struggling for the past five minutes trying to figure out the witchcraft behind ties, and he still had zero clue as to what he was supposed to be doing.
“Be right there, kiddo!” It was only a few moments before soft footsteps could be heard approaching, and Patton walked into the bathroom. He’d already mostly finished getting ready sans the fact that his hair was a catastrophic mess. Virgil could guess that he’d been trying to fix it when he’d been called into the other room.
“Alright. Work your magic,” Virgil smirked. In a matter of seconds, Patton had looped and pulled the tie into place, gently tightening it around Virgil’s neck. It was deep purple, picked out specifically because of his dislike of most other colors, and it went very well with the blues and reds of the others’ ties. The tie also matched the freshly dyed purple hair that Roman had forced his three friends to do along with him earlier that afternoon. What an ass.
Virgil admired his reflection. “Dude, what the fuck? How did you do that?” He felt oddly confident in his skin. The same feeling had come about a few times since he’d met Patton, and he had to admit that it was nice. Pat’s happy-go-lucky attitude somehow perfectly meshed with Virgil’s own doom-and-gloom one, forming a hilariously compatible friendship.
Patton smiled and ruffled Virgil hair, much to the other’s dismay. “Now that I helped you, will you please fix my hair.”
“Ugh, fine.”
“I mean it, Virge! Look at this.” Pat ran his fingers through his hair and aggressively tugged when he reached a clump of knots.
“Okay, yeah, we’re fixing that right now.”
---
“Dinner? Really, Patton? You guys couldn’t have told me about this before?” Virgil whined as the four walked into the diner. Yes, a diner, which meant that they were ridiculously overdressed; every other patron was wearing some sort of flannel and jeans combo. It smelled great, sure, but it was so unexpected that he couldn’t help but feel on edge.
“It’s our favorite restaurant,” Logan explained. “We always come here before school events. Roman has coined it as some sort of weird ritual, but it’s mostly tradition.” He led Virgil to the booth that Patton and Roman had already rushed to sit in.
“Plus, we’re friends with the staff,” Ro started with a smile. “You’ll love them; they’re all super nice. Speaking of, here comes Emilia.”
A young lady with brown hair walked up to their table, pulling out her small notepad. “Well, who do we have here? Another addition to our little group of customers of the month for every month since 2014?”
“Hey, Emilia!” Patton said. “This is Virgil; he’s a new friend of ours. He’s been living with me for a few weeks while his dad is out of the country on business.”
“That’s sweet, Patton. Now, what can I get for you guys?”
The three regulars spouted off their orders, clearly versed in what they wanted to eat. Suddenly, all eyes turned to Virgil. He’d barely been able to look over the menu in the time the others had taken to order.
“Uh… I… Um…” He stuttered. Every drop of intelligence that he had in his body was gone in an instant, and he was left a bumbling mess.
“He’ll have a cheeseburger and fries, thanks,” Patton cut in, saving his friend from any further embarrassment.
“Alright! I’ll be back in a few with your food and a pitcher of water!” Emilia gave the boys another smile before she walked back behind the counter to tend to other customers. Almost immediately, Patton and Roman launched themselves into a fast paced discussion about the upcoming festivities. Virgil, unsurprisingly, not only felt anxious, but he also felt like a complete idiot. He was just ordering dinner--there was no reason for him to have been so freaked out.
Virgil felt a hand rest on his left shoulder, turning to see Logan with a worried expression etched on his face. “Are you okay? Do you need to step outside for a moment to regain composure? I’d be willing to go with you if you don’t want to be alone.”
“Uh, no. I’m okay. I’m just a little worried. I mean, this is my first proper school event in, like, ever, and it’s freaking intimidating. You guys go to these things multiple times a year?” Virgil ran his hands through his hair, distressed.
“I understand. When Roman and Patton first made me come with them to homecoming, I was so nervous that I nearly passed out on the way here. Thankfully, I wasn’t driving us everywhere back then otherwise that would’ve ended in a disaster.” Logan gave Virgil a small smile, adding to the tiny--yet slowly growing--list of his outward displays of emotion. Virgil knew Lo wasn’t an emotionless android, but Roman and Patton were so all over the place that someone needed to play the calm and collected one.
“They can be pretty intense,” Virgil commented with a smile at the enthusiastic conversation across the table from them. Both of the teens were grinning and flinging their hands around in wild gestures, barely avoiding impact.
“Yeah, they sure can.” Logan glanced at the other side of the table with a fond expression, but he quickly snapped out of his reverie. “Don’t worry about the dance. Oh, here!” He pulled a pair of earbuds out of his inside jacket pocket and held them out to Virgil. “It gets pretty loud at these dances. I’ve observed that you put on headphones when it gets too noisy, so I brought these just in case you didn’t have your own.”
Virgil pocketed them just as Emilia finally returned with their food. The other three immediately began to dig in while he hesitantly poked at his burger. He picked up a fry and lazily popped it into his mouth.
He picked at his fries for a few minutes, but he eventually worked his way up to taking a bite of his burger. “Holy shit! This stuff is great--wait, why haven’t you taken me here yet?”
“I was trying to ease you into our friend group, so I thought eating dinner at my house would save you some unnecessary interaction,” Pat explained. “Obviously, that was a crime against your taste buds.”
“Of course it was, Patton. Depriving anyone of this blessed food is practically a war crime!” Roman dramatically stated, throwing out his arms. Virgil snorted at the theatrics.
They continued to eat, and all but Virgil had finished their dinner when Emilia returned to their table for dessert orders. Logan ordered a slice of pecan pie for himself, a chocolate lava cake for Roman, a hot fudge sundae for Patton, and a caramel shake for Virgil. Patton, of course, began to spout off a review of all of the desserts they’d ordered, even though Virgil wouldn’t be eating most of them. They all listened politely, not really absorbing any of the information, until their orders arrived. Within a nanosecond, Pat’s face was stuffed full of vanilla ice cream and fudge sauce, easily and efficiently shutting him up.
They ate in near silence, save for the “light” discussion of whether cake or pie was better (Patton eventually had to cut in when Roman threatened Logan with a butterknife). Pat covered the whole bill once they’d finished, claiming “it’s my way of thanking you guys for putting up with my shenanigans.”
---
“Three, two, one!” Roman dramatically counted as he threw the doors to the venue open. Time seemed to freeze as the four friends stepped in; all eyes snapped to them. It had been days since they’d been the topic of gossip at school, but that didn’t mean the student body had lost their interest in the boys.
Roman was at the front of the group, confidently striding to the grand staircase and adjusting his red tie. Logan followed close behind, who looked absolutely stunning in the sharp suit and deep blue tie. Then was Patton, who was marveling at the cascading flower vines and glittering fairy lights. And last but certainly not least…
Virgil. He had a wary smile on his face, shoving his hands deep into the pockets of his slacks. The boy made absolutely sure that he didn’t get lost; he kept eyes on Patton the entire time they descended the stairs.
Logan had been right; it was fucking loud. People were screaming left and right, and the music was so loud that Virgil could feel every beat vibrate in his chest. He was lucky that he’d put the earbuds in before they’d arrived, or he never would have stepped inside the venue.
Patton turned around to check on Virgil, obviously sensing the tension building in his friend. He held out his hand for Virgil, who hesitated for just a moment before gently taking it. If people wanted to believe they were together, that wasn’t his problem. It was no skin off his back.
They talked and danced for what felt like hours, and Virgil even joined in on a few of the dances he knew. He was having fun. He smiled and laughed, and it was all genuine! In just a few short weeks, Patton had actually transformed him from a suicidal nightmare into someone who found joy in life. It was a stupid sentiment, and he knew it, but it still brought Virgil a bit of warmth in his chest.
The DJ announced a slow dance. Ugh, how awful. He had nobody to dance with; it was just—
Oh.
Patton tugged Virgil’s hand lightly, pulling their bodies closer together. “Wanna dance? We don’t have to, of course, but it would be a fun first experience for both of us!”
“I—Uh, sure,” Virgil mumbled, trying to hide his gently growing blush. Pat gently guided Virgil’s hands around his neck and placed his own on Virgil’s waist. For the first time, Virgil noticed that he was just an inch or so taller than his friend. Reveling in the warmth and closeness, the two swayed together to the gentle rhythm.
The song ended, and Virgil stepped back, shoving his hands into his pockets. He was extremely grateful that the low light hid his pink cheeks. The screaming resumed as couples broke apart, and early 2000s rap boomed out of the speakers.
And then just like that, Virgil was attacked by anxiety. His hands started shaking, and he rushed away from the small group he was in, mumbling something about going to the bathroom. He calmed slightly when he had made it outside, where he simply collapsed to the ground, but then his panic picked up again when he realized how fucking alone he was always going to be.
Nobody would love the weird guy who rushes out on social gatherings for no fucking reason! Why should they? Virgil had nothing to offer; he was just a guy who had snark to rival Roman and barely two cents to his name.
Tears streamed down his face, running in dark gray streaks as they mixed with his black eye makeup. He could feel his chest heaving, but little air actually made it into his body. Everything was working overtime yet nothing actually happened. Virgil stayed sobbing on the ground. Nothing. Changed.
“Virge, honey? Do you need me to call my mom and have her pick us up?” Patton slowly lowered himself next to Virgil, talking softly so that he woudn’t stir up anything worse.
“N-No! I’ll… I’ll… Fuck!” Virgil cried as he ripped the earbuds out of his ears. He threw the cord a few feet away, instantly regretting it as the sound of shattering plastic reached his ears. He’d have to buy Logan new ones. He couldn’t afford to replace them.
“Goodness gracious, Virgil. It’s okay. I’m going to call Logan, and we’re going to get you out of here—“
“I-I-I don’t… want t-t-to… ruin… night…” Virgil sputtered. He was having trouble pushing the words out; all of them got stuck in his throat.
Patton carefully began to comb through Virgil’s hair with his fingers in an attempt to soothe the attack. “Don’t worry about that, kiddo. There isn’t much more fun to be had, anyway. We still love you—I still love you.”
That’s it. That’s what he felt. Love. He loved Patton.
All of the impulse control he had—though, truthfully, there was very little to begin with—left his body. He reached out and brought Pat’s face to his own, lightly kissing him. Patton stiffened for a fraction of a second before relaxing into the kiss. They were both going to regret this later, but what did that matter in the moment?
chapter 13
#sanders sides fic#moxiety#logince#m writes things#virgil sanders#logan sanders#patton sanders#roman sanders
12 notes
·
View notes
Last Seen Blogs

lollyloopsart
_lollyloops_

earl-grey-love
So few pleasures in life as fine as your company

kairaasiijewellers
Kairaasii Jewellers

alonysart
Somewhere Under The Sun, Moon, and Stars

rogersreubenrater-blog
Roger's Reuben Rater