#the cass report
Text
If you are a trans person in the UK either under the care of a gender clinic, or even on the wait list for one, please do send them an email or letter opting out of your patient records and data being used for 'research', like the clearly transphobic review that's coming for adult services next.
This is especially important if you are under 30 years old.
There's a great template letter you can use here, it took me less than five minutes to copy stuff and send off an email.
871 notes
·
View notes
Text
Fuck the Cass report
Fuck the Tories
Fuck Labour
Fuck TERFs
256 notes
·
View notes
Text
Breaking Down Cass Review Myths and Misconceptions: What You Need to Know.
An answer when some tranny or handmaiden disputes the review. (long post with lots of facts!)
Via The Quakometer:
It has now been just little under a week since the publication of the long anticipated NHS independent review of gender identity services for children and young people, the Cass Review.
The review recommends sweeping changes to child services in the NHS, not least the abandonment of what is known as the “affirmation model” and the associated use of puberty blockers and, later, cross-sex hormones. The evidence base could not support the use of such drastic treatments, and this approach was failing to address the complexities of health problems in such children.
Many trans advocacy groups appear to be cautiously welcoming these recommendations. However, there are many who are not and have quickly tried to condemn the review. Within almost hours, “press releases“, tweets and commentaries tried to rubbish the report and included statements that were simply not true. An angry letter from many “academics”, including Andrew Wakefield, has been published. These myths have been subsequently spreading like wildfire.
Here I wish to tackle some of those myths and misrepresentations.
Myth 1: 98% of all studies in this area were ignored.

Fact
A comprehensive search was performed for all studies addressing the clinical questions under investigation, and over 100 were discovered. All these studies were evaluated for their quality and risk of bias. Only 2% of the studies met the criteria for the highest quality rating, but all high and medium quality (50%+) studies were further analysed to synthesise overall conclusions.
Explanation.
The Cass Review aimed to base its recommendations on the comprehensive body of evidence available. While individual studies may demonstrate positive outcomes for the use of puberty blockers and cross-sex hormones in children, the quality of these studies may vary. Therefore, the review sought to assess not only the findings of each study but also the reliability of those findings.
Studies exhibit variability in quality. Quality impacts the reliability of any conclusions that can be drawn. Some may have small sample sizes, while others may involve cohorts that differ from the target patient population. For instance, if a study primarily involves men in their 30s, their experiences may differ significantly from those of teenage girls, who constitute the a primary patient group of interest. Numerous factors can contribute to poor study quality.
Bias is also a big factor. Many people view claims of a biased study as meaning the researchers had ideological or predetermined goals and so might misrepresent their work. That may be true. But that is not what bias means when we evaluate medical trials.
In this case we are interested in statistical bias. This is where the numbers can mislead us in some way. For example, if your study started with lots of patients but many dropped out then statistical bias may creep in as your drop-outs might be the ones with the worst experiences. Your study patients are not on average like all the possible patients.
If then we want to look at a lot papers to find out if a treatment works, we want to be sure that we pay much more attention to those papers that look like they may have less risk of bias or quality issues. The poor quality papers may have positive results that are due to poor study design or execution and not because the treatment works.
The Cass Review team commissioned researchers at York University to search for all relevant papers on childhood use of puberty blockers and cross-sex hormones for treating “gender dysphoria”. The researchers then graded each paper by established methods to determine quality, and then disregarded all low quality papers to help ensure they did not mislead.
The Review states,
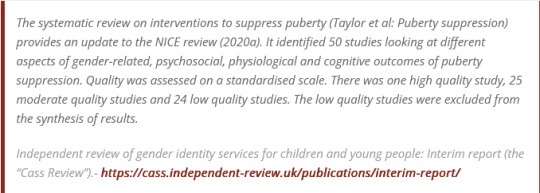
As can be seen, the conclusions that were based on the synthesis of studies only rejected 24 out of 50 studies – less than half. The myth has arisen that the synthesis only included the one high quality study. That is simply untrue.
There were two such literature reviews: the other was for cross-sex hormones. This study found 19 out of 53 studies were low quality and so were not used in synthesis. Only one study was classed as high quality – the rest medium quality and so were used in the analysis.

Again, it is myth that 98% of studies were discarded. The truth is that over a hundred studies were read and appraised. About half of them were graded to be of too poor quality to reliably include in a synthesis of all the evidence. if you include low quality evidence, your over-all conclusions can be at risk from results that are very unreliable. As they say – GIGO – Garbage In Garbage Out.
Nonetheless, despite analysing the higher quality studies, there was no clear evidence that emerged that puberty blockers and cross-sex hormones were safe and effective. The BMJ editorial summed this up perfectly,

Myth 2: Cass recommended no Trans Healthcare for Under 25s.

Fact
The Cass Review does not contain any recommendation or suggestion advocating for the withholding of transgender healthcare until the age of 25, nor does it propose a prohibition on individuals transitioning.
Explanation
This myth appears to be a misreading of one of the recommendations.
The Cass Review expressed concerns regarding the necessity for children to transition to adult service provision at the age of 18, a critical phase in their development and potential treatment. Children were deemed particularly vulnerable during this period, facing potential discontinuity of care as they transitioned to other clinics and care providers. Furthermore, the transition made follow-up of patients more challenging.
Cass then says,
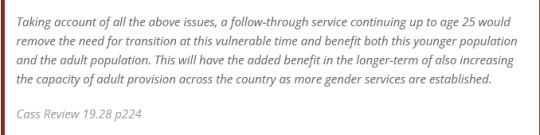
Cass want to set up continuity of service provision by ensure they remain within the same clinical setting and with the same care providers until they are 25. This says nothing about withdrawing any form of treatment that may be appropriate in the adult care pathway. Cass is explicit in saying her report is making no recommendations as to what that care should look like for over 18s.
It looks the myth has arisen from a bizarre misreading of the phrase “remove the need for transition”. Activists appear to think this means that there should be no “gender transition” whereas it is obvious this is referring to “care transition”.
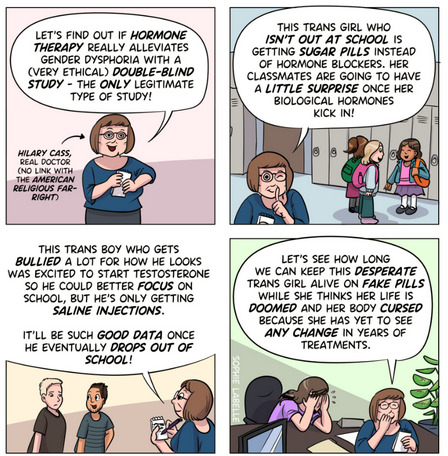
Myth 3: Cass is demanding only Double Blind Randomised Controlled Trials be used as evidence in “Trans Healthcare”.

Fact
While it is acknowledged that conducting double-blind randomized controlled trials (DBRCT) for puberty blockers in children would present significant ethical and practical challenges, the Cass Review does not advocate solely for the use of DBRCT trials in making treatment recommendations, nor does it mandate that future trials adhere strictly to such protocols. Rather, the review extensively discusses the necessity for appropriate trial designs that are both ethical and practical, emphasizing the importance of maintaining high methodological quality.
Explanation
Cass goes into great detail explaining the nature of clinical evidence and how that can vary in quality depending on the trial design and how it is implemented and analysed. She sets out why Double Blind Randomised Controlled Trials are the ‘gold standard’ as they minimise the risks of confounding factors misleading you and helping to understand cause and effect, for example. (See Explanatory Box 1 in the Report).
Doctors rely on evidence to guide treatment decisions, which can be discussed with patients to facilitate informed choices considering the known benefits and risks of proposed treatments.
Evidence can range from a doctor’s personal experience to more formal sources. For instance, a doctor may draw on their own extensive experience treating patients, known as ‘Expert Opinion.’ While valuable, this method isn’t foolproof, as historical inaccuracies in medical beliefs have shown.
Consulting other doctors’ experiences, especially if documented in published case reports, can offer additional insight. However, these reports have limitations, such as their inability to establish causality between treatment and outcome. For example, if a patient with a bad back improves after swimming, it’s uncertain whether swimming directly caused the improvement or if the back would have healed naturally.
Further up the hierarchy of clinical evidence are papers that examine cohorts of patients, typically involving multiple case studies with statistical analysis. While offering better evidence, they still have potential biases and limitations.
This illustrates the ‘pyramid of clinical evidence,’ which categorises different types of evidence based on their quality and reliability in informing treatment decisions

The above diagram is published in the Cass Review as part of Explanatory Box 1.
We can see from the report and papers that Cass did not insist that only randomised controlled trials were used to assess the evidence. The York team that conducted the analyses chose a method to asses the quality of studies called the Newcastle Ottawa Scale. This is a method best suited for non RCT trials. Cass has selected an assessment method best suited for the nature of the available evidence rather than taken a dogmatic approach on the need for DBRCTs. The results of this method were discussed about countering Myth 1. Explainer on the Newcastle Ottawa Scale
As for future studies, Cass makes no demand only DBRCTs are conducted. What is highlighted is at the very least that service providers build a research capacity to fill in the evidence gaps.
Myth 4: There were less than 10 detransitioners out of 3499 patients in the Cass study.

Fact
Cass was unable to determine the detransition rate. Although the GIDS audit study recorded fewer than 10 detransitioners, clinics declined to provide information to the review that would have enabled linking a child’s treatment to their adult outcome. The low recorded rates must be due in part to insufficient data availability.
Explanation
Cass says, “The percentage of people treated with hormones who subsequently detransition remains unknown due to the lack of long-term follow-up studies, although there is suggestion that numbers are increasing.”
The reported number are going to be low for a number of reasons, as Cass describes:

Damningly, Cass describes the attempt by the review to establish “data linkage’ between records at the childhood gender clinics and adult services to look at longer term detransition and the clinics refused to cooperate with the Independent Review. The report notes the “…attempts to improve the evidence base have been thwarted by a lack of cooperation from the adult gender services”.
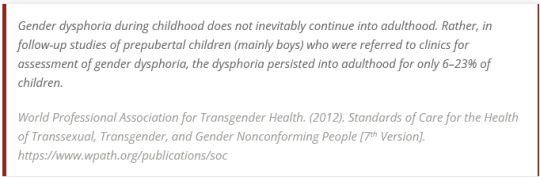
We know from other analyses of the data on detransitioning that the quality of data is exceptionally poor and the actual rates of detransition and regret are unknown. This is especially worrying when older data, such as reported in WPATH 7, suggest natural rates of decrease in dysphoria without treatment are very high.
This suggests that active affirmative treatment may be locking in a trans identity into the majority of children who would otherwise desist with trans ideation and live unmedicated lives.
I shall add more myths as they become spread.
#Cass report#the cass report#cass review#the cass review#trans lies#gender critical#tras#medical malpractice#the tide is turning
100 notes
·
View notes
Text
Okay this ain't even my country and I know that I'm preaching to the choir but "Dr" Hilary Cass' report on how trans youth in Britain are totally fine without transitioning and hey maybe we should just ban it all entirely is one of the most glaring examples of bad faith science I've seen and I want to dress down exactly why it's horseshit.
She did not conduct any research herself. She has never so much as interacted with a trans youth. What she did was cherrypick a bunch of publications, say that they "weren't conducted properly", and then read that as a "lack of evidence" for the benefits of transitioning. (Note: All of the studies she looked at were UK. Ergo every other country that has found that transitioning helps people can get fucked I guess because the laws of science only apply to Britain.) There were plenty of publications that did pass her narrow view for scientific rigor, and she deliberately left them all out. She can't even say they were wrong, she just says "they weren't good enough" and takes that as "proof" there was no real evidence to begin with.
If she was a scientist and not a TERF with a political agenda, she would be asking for these studies to be redone with her new standard. But she's not. She just wants all trans science to stop before it shows her something she doesn't want to hear, and for all trans youth to kill themselves quietly so she can say they were "just" suicidal and there was nothing that transitioning could have done for them. And the fact that the government and even other scientists are supporting her in this endeavor makes me sick.
34 notes
·
View notes
Text
the idea that you have to be 25 to make a huge life decision is incredibly dangerous. And it won't just affect Trans people. It will affect disabled people, people of color and other queer people.
36 notes
·
View notes
Text
A recent review of the Cass report by experts with experience with GIDS has been released, and it's a very interesting read
But if there's one thing I really want to point out, it's this: Cass notably during the report brought up the notion that "97% of kids who take puberty blockers go onto take gender affirming hormones" and suggested it was a bad thing, rather than evidence that puberty blockers were being assigned correctly in the vast, vast majority of cases. Yet it didn't really elaborate on why this was supposedly a negative.
Well, according to Dr Max Davie, Cass certainly had a motive here:
Towards the end of 2020, I was called by Dr Cass, to discuss potential involvement in her review, which had just been announced. This is my recall of that conversation.
We had worked together on a NICE working group looking at medical transition, which was a separate piece of work with a different governance structure to the subsequent review.
During this NICE exercise, I had become aware of Dr Cass’s scepticism about the GiDs model.
During the call, she expressed concerns about GiDs practice. She expressed the view that it was shocking that 97% of children who went onto puberty blockers then progressed to gender affirming hormones in the GiDs service. I suggested that this might have been due to accurate triage. She recommended that I read Irreversible Damage.
The call ended and I never heard anything about involvement in the review.
So yeah, anyone who argues Cass was a "neutral party" was entirely wrong. While Cass has denied Dr Davie's accusation, the fact that she follows hate group TransgenderTrend on twitter, the fact that she most definitely did argue that the 97% figure was a bad thing, and everything else she's said and done, I believe Dr Davie on this part.
13 notes
·
View notes
Text
Brilliantly restrained roundup of the slew of evidence that the Cass report is an horrendous, ideologically-driven, transphobic mess
#transphobia#trans#the cass report#oh dear oh dear oh dear#it would be funny if it wasn’t so fucking tragic and so likely to fuck trans people even more#especially vulnerable trans kids
13 notes
·
View notes
Text

#id in alt text#star control 2#star control#Commander hayes#the cass report#cass report#cass review#nhs#gender affirming care
10 notes
·
View notes
Text
the Cass report is fucking evil and should never have been allowed.
15 notes
·
View notes
Text
TW: Transphobia, Forced outting, Abuse (Emotional and medical), Childhood trauma
I am so sick of hearing transphobes talk about all these traumatised, detransitioning kids. What about me? What about my trauma? I have been told all my life I am not who I say I am. That I am confused and a liar. I have been forced to sit back and watch my body change in ways I can only hope are reversible. And ostracised from society as it happens.
Where is the love for the 10-year-old who sobbed in his seat as his loved ones shouted at him for attempting to bind his chest? Where is the love for the 11-year-old who hugged his knees and cried as he had to explain to his teacher he hated being made to feel like a girl? Where is the love for the 12-year-old who wandered around depressed because he knew that nobody around him could be his friend and respect him for who he is? Where is the love for the 13-year-old that tore into his body because it was not his and he hated it for betraying him? Where is the love for the 14-year-old who does not know if his family will one day look upon his body in disgust?
I have been hurt and harassed and abused because of who I am, or in the eyes of transphobes, who I think I am. All I have ever asked is for people to call me my name, and not call me a she – and somehow that has been deserving of the things I have endured. I feel really, really sorry for all the kids who were put on hormone blockers they regret taking – but what about me? What about my trauma? I will never look at my body with love, I will never get to in my youth. In case I “make the wrong decision.” All I want is to feel safe, loved and accepted. I do not get that. Because you do not care about my pain. You do not care about trans kids. You just care about protecting your own sense of reality, even if it is hurting me
8 notes
·
View notes
Text

TransActual has a good briefing on the issues with the Cass Report in case you're like me and can't stand to read the whole horrible thing
One of the recommendations they are making is to basically screen for neurodiversity, because they want to deny autistic trans people the right to transition so badly.

And the NHS is already putting things into motion to make things worse for adult trans people in this country too.
The overall Ableism in this is absolutely despicable. They are making a new "research oversight board" and putting this fucking guy in charge of it, that despite all scientific evidence to the contrary still insists ME/Chronic Fatigue Syndrome is a "psychosocial" condition - Not real, all in people's heads, etc.
Someone like this being given this level of legitimacy is sick, and will continue to promote the horrible treatment of chronically ill and disabled people in this country.
350 notes
·
View notes
Text
Can't believe that people want me to spend a quarter of my life in the wrong body :/
that's it
9 notes
·
View notes
Text
The Courage to Follow the Evidence on Transgender Care.
(WOW, the New York Times -- which a couple years ago had an ad about a qu**r girl who wished for a world in which J.K. Rowling wasn't the author of Harry Potter -- has published yet another opinion piece about trans, this one about the Cass Review. Personally, I think he's too lenient, but at least he's bringing attention to the review to Americans. )
(For those who can't read the NYT page, here's the text.)

Opinion, David Brooks, April 18, 2024.
Hilary Cass is the kind of hero the world needs today. She has entered one of the most toxic debates in our culture: how the medical community should respond to the growing numbers of young people who seek gender transition through medical treatments, including puberty blockers and hormone therapies. This month, after more than three years of research, Cass, a pediatrician, produced a report, commissioned by the National Health Service in England, that is remarkable for its empathy for people on all sides of this issue, for its humility in the face of complex social trends we don’t understand and for its intellectual integrity as we try to figure out which treatments actually work to serve those patients who are in distress. With incredible courage, she shows that careful scholarship can cut through debates that have been marked by vituperation and intimidation and possibly reset them on more rational grounds.
Cass, a past president of Britain’s Royal College of Pediatrics and Child Health, is clear about the mission of her report: “This review is not about defining what it means to be trans, nor is it about undermining the validity of trans identities, challenging the right of people to express themselves or rolling back on people’s rights to health care. It is about what the health care approach should be, and how best to help the growing number of children and young people who are looking for support from the N.H.S. in relation to their gender identity.”
This issue begins with a mystery. For reasons that are not clear, the number of adolescents who have sought to medically change their sex has been skyrocketing in recent years, though the overall number remains very small. For reasons that are also not clear, adolescents who were assigned female at birth are driving this trend, whereas before the late 2000s, it was mostly adolescents who were assigned male at birth who sought these treatments.
Doctors and researchers have proposed various theories to try to explain these trends. One is that greater social acceptance of trans people has enabled people to seek these therapies. Another is that teenagers are being influenced by the popularity of searching and experimenting around identity. A third is that the rise of teen mental health issues may be contributing to gender dysphoria. In her report, Cass is skeptical of broad generalizations in the absence of clear evidence; these are individual children and adolescents who take their own routes to who they are.
Some activists and medical practitioners on the left have come to see the surge in requests for medical transitioning as a piece of the new civil rights issue of our time — offering recognition to people of all gender identities. Transition through medical interventions was embraced by providers in the United States and Europe after a pair of small Dutch studies showed that such treatment improved patients’ well-being. But a 2022 Reuters investigation found that some American clinics were quite aggressive with treatment: None of the 18 U.S. clinics that Reuters looked at performed long assessments on their patients, and some prescribed puberty blockers on the first visit.
Sign up for the Opinion Today newsletter Get expert analysis of the news and a guide to the big ideas shaping the world every weekday morning. Get it sent to your inbox.
Unfortunately, some researchers who questioned the Dutch approach were viciously attacked. This year, Sallie Baxendale, a professor of clinical neuropsychology at the University College London, published a review of studies looking at the impact of puberty blockers on brain development and concluded that “critical questions” about the therapy remain unanswered. She was immediately attacked. She recently told The Guardian, “I’ve been accused of being an anti-trans activist, and that now comes up on Google and is never going to go away.”
As Cass writes in her report, “The toxicity of the debate is exceptional.” She continues, “There are few other areas of health care where professionals are so afraid to openly discuss their views, where people are vilified on social media and where name-calling echoes the worst bullying behavior.”
Cass focused on Britain, but her description of the intellectual and political climate is just as applicable to the U.S., where brutality on the left has been matched by brutality on the right, with crude legislation that doesn’t acknowledge the well-being of the young people in question. In 24 states Republicans have passed laws banning these therapies, sometimes threatening doctors with prison time if they prescribe the treatment they think is best for their patients.
The battle lines on this issue are an extreme case, but they are not unfamiliar. On issue after issue, zealous minorities bully and intimidate the reasonable majority. Often, those who see nuance decide it’s best to just keep their heads down. The rage-filled minority rules.
Cass showed enormous courage in walking into this maelstrom. She did it in the face of practitioners who refused to cooperate and thus denied her information that could have helped inform her report. As an editorial in The BMJ puts it, “Despite encouragement from N.H.S. England,” the “necessary cooperation” was not forthcoming. “Professionals withholding data from a national inquiry seems hard to imagine, but it is what happened.”
Cass’s report does not contain even a hint of rancor, just a generous open-mindedness and empathy for all involved. Time and again in her report, she returns to the young people and the parents directly involved, on all sides of the issue. She clearly spent a lot of time meeting with them. She writes, “One of the great pleasures of the review has been getting to meet and talk to so many interesting people.”
The report’s greatest strength is its epistemic humility. Cass is continually asking, “What do we really know?” She is carefully examining the various studies — which are high quality, which are not. She is down in the academic weeds.
She notes that the quality of the research in this field is poor. The current treatments are “built on shaky foundations,” she writes in The BMJ. Practitioners have raced ahead with therapies when we don’t know what the effects will be. As Cass tells The BMJ, “I can’t think of another area of pediatric care where we give young people a potentially irreversible treatment and have no idea what happens to them in adulthood.”
She writes in her report, “The option to provide masculinizing/feminizing hormones from age 16 is available, but the review would recommend extreme caution.” She does not issue a blanket, one-size-fits-all recommendation, but her core conclusion is this: “For most young people, a medical pathway will not be the best way to manage their gender-related distress.” She realizes that this conclusion will not please many of the young people she has come to know, but this is where the evidence has taken her.
You can agree or disagree with this or that part of the report, and maybe the evidence will look different in 10 years, but I ask you to examine the integrity with which Cass did her work in such a treacherous environment.
In 1877 a British philosopher and mathematician named William Kingdon Clifford published an essay called “The Ethics of Belief.” In it he argued that if a shipowner ignored evidence that his craft had problems and sent the ship to sea having convinced himself it was safe, then of course we would blame him if the ship went down and all aboard were lost. To have a belief is to bear responsibility, and one thus has a moral responsibility to dig arduously into the evidence, avoid ideological thinking and take into account self-serving biases. “It is wrong always, everywhere, and for anyone, to believe anything upon insufficient evidence,” Clifford wrote. A belief, he continued, is a public possession. If too many people believe things without evidence, “the danger to society is not merely that it should believe wrong things, though that is great enough; but that it should become credulous, and lose the habit of testing things and inquiring into them; for then it must sink back into savagery.”
Since the Trump years, this habit of not consulting the evidence has become the underlying crisis in so many realms. People segregate into intellectually cohesive teams, which are always dumber than intellectually diverse teams. Issues are settled by intimidation, not evidence. Our natural human tendency is to be too confident in our knowledge, too quick to ignore contrary evidence. But these days it has become acceptable to luxuriate in those epistemic shortcomings, not to struggle against them. See, for example, the modern Republican Party.
Recently it’s been encouraging to see cases in which the evidence has won out. Many universities have acknowledged that the SAT is a better predictor of college success than high school grades and have reinstated it. Some corporations have come to understand that while diversity, equity and inclusion are essential goals, the current programs often empirically fail to serve those goals and need to be reformed. I’m hoping that Hilary Cass is modeling a kind of behavior that will be replicated across academia, in the other professions and across the body politic more generally and thus save us from spiraling into an epistemological doom loop.
#cass review#the cass review#cass report#the cass report#transgender#trans#trans insanity#the tide is turning#gender critical#gender ideology#gender identity#gender cult#gender madness
51 notes
·
View notes
Text
When I was a teenager, my father passed away from years of chronic illness and I got very depressed
I don't remember much for about a year, other than being in bed, crying. Life paused for a year or two, so that although time went on, my life didn't. Effectively ending it would've merely been a physical affirmation of what was already true: I was dead, at least, inside.
My father and I had a very close relationship. It wasn't like we got to do that many father-daughter things together, but mostly it was just that we were two faces of the same coin; similar enough to understand each other without a need for words, and to feel understood by each other, but different enough not to rub each other off the wrong way. I am far more different from my mother, and yet, the mother-daughter bond being as legendary as it is, we've always been attached to each other's hip and we have a deeply affectionate relationship. But after my father died, I felt abandoned, left out, alone. I felt like the black sheep of the family, the different one, because the one person who got me, who I was like, was gone forever. If only I'd known then what I know now: everybody tends to feel the same way at some point.
It affected my relationship with my father's side of the family. My parents were together until the end, so I'd always spent the most time with his side of the family, which lived near us, rather than my mum's, which lived farther away. My dad had been the best of his family, so I was never particularly close with anyone there except my, by then, very elderly grandparents. Without my dad, I experienced an odd feeling of disconnection; like a cable that's cut in the middle. Like, the thing that united me to them was gone, so was I even one of them any more? And it might seem strange, but actually, the fact that I had my dad's surname there was something I held onto firmly to remind myself I was still part of my family. Still, even a decade later, it's my mother's family I feel more united to.
Losing a parent at a young age was, to me, like being blown away by a bloody tornado when you were just beginning to learn how to walk on your own. And suddenly you're all alone, waking up in unknown turf, standing in the ruins of your family, your home... whatever remains when a chronic illness has been punching everyone where it hurts the most for years and years. And it took me years, and actually leaving my country, to find my footing again and stand strong again.
My point is that, for many years, I was in a deeply vulnerable and fragile mental state. I didn't seek refuge in drugs, but I did start to drink for the first time, even when I've always despised the taste of alcohol. In my late teens, it was trendy to be dark, mysterious, depressed... and none is that more than someone going through the kind of grief and heartbreak you can't make your friends understand. So my sudden drinking (not to drunkenness, but certainly completely out of my normal behaviour), my quietness, my self-isolation, were seen not as warning signs, but as cool behaviour, among my friends.
And then things got weird. I was seventeen, bursting into tears in high school, in front of everyone, because I'd misplaced something my dad had gifted me and couldn't find it. It wasn't even something important, just a pouch where to put money... but it was my dad's gift to me, and I could only find one friend who understood why it mattered to me, and helped me find it even if I was making a huge thing out of a grain of salt. And for a decade, I've been lashing out. A small feeling of discontentment or annoyance suddenly bursts into flames of fury, and I screamed at my mother, even though I'd never done it. I still go from 0 to 100 with tremendous ease; in sadness, in happiness, in anger, in laughter. Every feeling starts dull and is suddenly overwhelming. And so in the middle of these years of grief, I fell in love, went from 0 to a 100 in five minutes, and if I hadn't stopped myself right on time, I would've agreed to marry someone who simply wasn't right for me. Someone who loved me 80%, when I was there 100%. By now I've accepted that everything is always going to feel too much, too suddenly. That tears will burst out of my eyes for no particular reason, but so will laughter from my chest, and love from my heart. It is both a super power and a dangerous thing, but I'm treating it as a super power, and doing my best to control it when I can, without eradicating it.
One of the things I did in my grief was cross-dress as a man. I put on a three-piece suit that didn't really suit me, and cut my hair from long to zero, and even tried to use fake beards.
I wasn't a man. I never identified as such. I was always clear on the fact that I was seventeen and I just wanted to know "what it's like". But deep inside, it was about control. You see, I'd been left shattered, I was scrambling to keep my head above water, I had no control - and I longed for the power of being a man.
I wanted to stand strong as a man. I wanted to be like my late dad. To be a good man in the storm. To fight, to be strong, to be tough, to dress however I wanted, to stop being whistled at and catcalled, to have a man's salary, a man's work opportunities, a man's power.
It was just a period of my life. The closer to thirty I've gotten, the more comfortable I've felt as a woman, the more I've loved being a woman, the more I've remembered my father's happy eyes on me, watching me speechless the first time I put on a dress, make-up and heels, telling me how beautiful I was, taking photos non-stop with his professional camera and making me feel like a gorgeous princess. And damn it, I've never given a shit about male admiration, I've never fancied dressing "to impress", but my dad had such a way of looking at me with eyes full of wonder, not in a sexualised way, but in a "my god, you're a grown-up woman!" way, that I'd happily fight to have that back. This was the same man who, when I first got my period and was in a mood, cracked a smile on my face by grinning at me and saying "you're all grown-up now!", the same man who when I was just born, was the only one who said I was beautiful, and was too afraid of hurting me to even hold me for a wee bit, the same man who, if I was sitting alone with my head on the table going through whatever, would sit next to me and put his head on the table too, without saying anything, just so I wouldn't be alone, and the same man who'd go above and beyond to do things with me and get to know me. I don't look back on my dad as a dad, I look back on my dad as a best friend. I used to want to be just like him - now I just want to be like myself, and see in me the wonders that he saw. Now I stand proud as a woman, the woman I know he would've been stocked to know.
The Cass Report has brought back into the forefront of my mind what a pain it was to be a teenager and a young adult. In my case, it was because of Earth-shattering grief. In my case, I could want to have male things for a bit, and I got to experiment, to cross-dress, to kiss boys and girls, to make mistakes, and to, over the course of a decade, find my way back.
That is what I wish for children to be given back: the space and the time to figure things out without having to deal with more life-changing procedures.
Teens were in a mental health crisis a decade ago and it's only gotten worse since. And if my friends had seen what I was doing in my grief as alarming signs of mental health problems, instead of as a cool, trendy behaviour, then maybe I would've gone to therapy instead of opening a bottle of Vodka. I probably would've taken it wrong to be told I had mental health problems - and I would've rebelled, fought, argued, and in fact I did, the one time my mum insisted I saw somebody. God how I hated psychologists then, and now it's one of my main fields of study. I didn't want to be told I was sick any more than these kids do. But I needed to hear that. I needed my problems validated, even if I didn't want to hear it. I needed to be forced to accept help. I needed to be told grief is one thing, and feeling like you can't possibly go on is another. I NEEDED PROFFESSIONAL HELP.
That is all the Cass Report shows. That children need professional help. That children go through hell and back because they're barely equipped to deal with big shocks to the system, and the world has never been more hostile to them. And that just because alarming behaviour that points to mental health issues can be perceived as "cool" or "trendy", and become fashionable, it doesn't make it less of a mental health problem.
#the cass report#bbc#bbc news#personal#mental health#psychology#therapy#grief#mourning#father loss#parental loss#personal loss#death#depression#teens#teenager#women#feminism#feminist#transgender#children#children's rights#trans rights
7 notes
·
View notes
Text
Big news for The Cass Review.
The peer reviews are starting to come in and its not looking good for Dr Cass. The article above, written by Mira Lazine, provides whats essentially a sparknotes version of the documentation releases by Yale.
I'm not going to pretend I understand the majority of the terminology used in the document and if anyone out there does then please your insight if you'd like.
Here is a link to the full paper.
#trans rights#trans liberation#trans healthcare#uk#the cass report#the cass review#terfs will be automatically blocked I am not interested in engaging with you#yale university#protect trans kids
3 notes
·
View notes
Text
Hormone blockers would have saved me so much distress in my body. If I had figured out I was trans at a younger age hormone blockers would have saved so much stress and panic and pain. And now kids aren't getting them.
The Cass report is fucking bullshit, it has been proved they've used AI generated images. It is bullshit and harmful and this is fucking bullshit and I'm emotional rn because I shouldn't be this worried about my safety as a trans person in this god forsaken country
2 notes
·
View notes
Last Seen Blogs

losergames
crime, cars, cash.

glimmerkey
lofty castle

jutetower8-blog
New York City Finds

alendesy
Lost In The Storm
firmament00000
00000