#Mental Health Clinic MD
Text
Tackle A Particular Mental Illness Or Life Stress.
Psychotherapy is a general term that is used to describe the process of treating psychological disorders and mental distress through the use of verbal and psychological techniques. During this process, a trained psychotherapist helps the client tackle specific or general problems such as a particular mental illness or a source of life stress.

Depending on the approach used by the therapist, a wide range of techniques and strategies can be used. Almost all types of psychotherapy involve developing a therapeutic relationship, communicating and creating a dialogue, and working to overcome problematic thoughts or behaviors.
Visit More: https://www.accesshealthservices.org/psychotherapy/
#Mental Health Clinic MD#MD Mental Health Services#Health Care Services MD#Mental Health Clinic Baltimore MD#MD Mental Health Clinic#Online Mental Health Services Baltimore#Mental Health Online Services Medication#Mental Health Services Online#Online Mental Health Services#Mental Health Online Services#Mental Health Clinic#Mental Health Service
0 notes
Note
Re your post about supplements: Totally agree, but can you clarify what a “Bruce Levine doctor” is? Thanks! Hope your bones become solid.
oh sorry i was just referencing this article by bruce levine about doctors (iconic) (to me)
Gaining acceptance into graduate school or medical school and achieving a PhD or MD and becoming a psychologist or psychiatrist means jumping through many hoops, all of which require much behavioral and attentional compliance to authorities, even to those authorities that one lacks respect for. The selection and socialization of mental health professionals tends to breed out many anti-authoritarians. Having steered the higher-education terrain for a decade of my life, I know that degrees and credentials are primarily badges of compliance. Those with extended schooling have lived for many years in a world where one routinely conforms to the demands of authorities. Thus for many MDs and PhDs, people different from them who reject this attentional and behavioral compliance appear to be from another world—a diagnosable one.
I have found that most psychologists, psychiatrists, and other mental health professionals are not only extraordinarily compliant with authorities but also unaware of the magnitude of their obedience. And it also has become clear to me that the anti-authoritarianism of their patients creates enormous anxiety for these professionals, and their anxiety fuels diagnoses and treatments.
In graduate school, I discovered that all it took to be labeled as having “issues with authority” was to not kiss up to a director of clinical training whose personality was a combination of Donald Trump, Newt Gingrich, and Howard Cosell. When I was told by some faculty that I had “issues with authority,” I had mixed feelings about being so labeled. On the one hand, I found it quite amusing, because among the working-class kids whom I had grown up with, I was considered relatively compliant with authorities. After all, I had done my homework, studied, and received good grades. However, while my new “issues with authority” label made me grin because I was now being seen as a “bad boy,” it also very much concerned me about just what kind of a profession that I had entered. Specifically, if somebody such as myself was being labeled with “issues with authority,” what were they calling the kids I grew up with who paid attention to many things that they cared about but didn’t care enough about school to comply there? Well, the answer soon became clear.
284 notes
·
View notes
Note
Riffing off of your recent post about Jordan Peterson, what IS the difference between counselling psychology and clinical psychology? I know it’s possible to get a PhD in either, but I’m fuzzy about the differences in approach.
My current therapist is a psychiatrist who is working with me on meds and also with Cognitive Behavioural Therapy (CBT) talk therapy. I’m perfectly happy with him, but if he ever got hit by a bus or something (or simply retired at some point), I’d be in the market for a new therapist. So I ought to know the difference between clinical psychologists and counselling psychologists.
Thank you.
In practical terms, on the client end, there's very little difference. The real divisions you need to know are:
Psychiatrist: Someone who went to medical school and specialized in psychiatry; can diagnose and prescribe medication. Usually designated MD.
Psychologist/Therapist/Counsellor: Someone who has gone to graduate school and focused on psychology or clinical social work; can sometimes diagnose, but usually cannot prescribe medication.
Psychiatrists do sometimes do talk therapy! I had a psychiatrist like that once. He was great. Sadly, this is mostly going out of fashion. Because they have so much extra training, they get higher salaries; administrators who care about increasing efficiency and cutting costs will therefore change them from seeing a patient for an hour each, to seeing a patient for only 15 minutes to talk about medication, and shunt the clients to cheaper therapists for talk therapy.
Within the field of psychologists/therapists /counselors, there are approximately eleventy squillion different variations in education format, theoretical basis, research background, and bragging rights. That's where the Counselling vs Clinical division lives. However, all the fields have similar aims (helping people reduce distress and become more healthy) and similar approaches (sit in a room and talk) and they freely poach any techniques or knowledge from each other that seem useful, so there's very little intrinsic difference that you would see.
The one big difference you would see is if you needed a formal diagnosis, more than just the person who treats you going, "Yeah, looks like [fill in the blank]". This is usually only needed if you're applying to something specific, like government benefits or special education accommodations. Assessment psychologists/neuropsychologists mostly tend to focus only on assessment, which is a whole different field in itself. Because of their expertise, and that someone who provides psychotherapy with you might be somewhat biased with their own ideas of what your deal is, formal assessments are generally done by someone who is not your therapist.
Anyway. The big difference between counselling and clinical psychology is basically historical. Clinical psychologists historically descend from the workers in hospitals, asylums, and mental health clinics, who focused on people with acute mental illnesses. They worked closely with psychiatrists and emulated psychiatry's popular methods at the time (mostly Freudian psychoanalysis) and focused specifically on treating mental health as a disease. This has generally been seen as a relatively more factual and sciencey field, since it's where a lot of the research on abnormal psychology and how to treat it has happened.
Counselling psychology, meanwhile, descends historically from pastors and school counsellors—people in churches or schools with "normal populations" who were the obvious go-to people for those in emotional distress or uncertainty about their lives. Counselling focused on training people who needed the skills to help somebody grieving the loss of a loved one, or who needed to figure out what they wanted to do with their lives. It has generally thus been seen as a fuzzier, less rigorous field, and less prestigious. It's also closely entangled with Social Work, which grew out of many of the same settings and focused on helping ease the lives of people affected by society's many ills.
But they were all of them decieved, for another Ring was made—
Counselling as a field got significantly transformed by Carl Rogers, who used scientific research to see what kinds of therapy approaches helped people—and to the shock and horror of many many people, the warm and gentle approaches used in Counselling and Social Work turned out to work better than Freudian impassivity—even in Clinical populations!
Because see, the division between these fields was based on a misapprehension. A hundred years ago, or even fifty, we thought that these fields focused on significantly different groups, and it turns out that's not really true. Freudian psychotherapy in its failure state was all about impersonal disconnection, pointing out the flaws and foibles of somebody's psyche and expecting them to fix it. Using Rogers' method of treating mentally ill people like human beings, looking them face-to-face and believing in their ability to better themselves as people, actually worked! Amazing!
And also, a lot of people with mental illnesses are really good at masking, compensating, and functioning as normal enough to avoid general detection and referral to medical treatment. Anyone dealing with the "general population" is inevitably going to deal with people with profound levels of depression, anxiety, psychosis, addiction, and every other mental disorder under the sun.
Therefore, anybody practicing in either field had to learn about both, because each required the skills the other had. These days, the difference is generally more about who your grad school was founded by fifty or a hundred years ago than your training recently. Counsellors get hired by mental hospitals, and clinical psychologists work in schools.
The differences still linger in little ways, like how in the Canadian Psychological Association, there are different "sections" that each organize their own newsletters and social media groups and parties during conferences. They discuss new research and issues relating to their areas of practice. Most people belong to three or four each, since they overlap—there's Counseling and Clinical, sure, but also Black Psychology, History and Philosophy, Psychology in the Military, and so on.
So I am mostly being petty and flippant when I say I'm glad not to be on the Clinical listserv, where there is, I imagine, a "Jordan Petetson is Making us Look Bad" Quarantine Thread, which will be locked after 9000 replies with no resolution in sight.
Anyway, that's all inside baseball and not useful to you. Onto the useful stuff.
Full disclosure: What I'm about to say may be unconsciously biased by my perspective, despite my efforts not to be so, because my Master's degree in Counseling means I have significantly less professional prestige than psychologists with doctorates, especially in Clinical Psychology. However, I earnestly believe that I am paying attention to the science and speaking the truth here.
All the best evidence states that what level of education someone has, what school they learned it in, and what therapeutic technique they are applying are not good predictors for whether therapy with them will help you.
And yet, therapy undeniably does work. It's just that, for all our trying, we still struggle to put our fingers on precisely what the difference is.
You are actually in the best position to predict success, because the best metric we can find is whether you, personally, feel that your counsellor is listening to you, understands and cares about you, and is helping you reach your goals. That's literally the most important thing. Does this counsellor seem like someone you could work with?
This means it's actively useful to provide feedback as you go, like, "I don't like that idea, what if I did it this way instead?" or "No, I think you're mistaken," or "I'm uncomfortable with this." Part of counselling is absolutely about sitting with discomfort and figuring out how to handle tough stuff, but your therapist should be someone you can at least discuss the whys and wherefores of the process with. They're a navigator on a journey with you, not a commander telling you where to march.
204 notes
·
View notes
Text
The MD and DVM; Chapter 1
Author’s note: hii omg this is the first fanfiction I’ve written in about five years now loool…I wrote this because I’ve never seen a harvey fic where the farmer is a veterinarian, and I have seen many questionable things said about farming. I work on a farm, and I am working towards going to veterinary school, so I felt my knowledge might contribute to a unique Harvey fic lol correct me if I’m wrong, tho, and please let me know if I should continue this! Crossposted on ao3 under xxdeaduniverse.
spring 1
You had always loved your grandfather’s property. His death almost broke you. However, you were delighted to find that he had left you his farm, Cinnamon Meadow. It was a quiet slice of heaven nestled away in Pelican Town. It still had all its old charm, just some added overgrowth and a lack of crops and animals.
You graduated from veterinary school a couple of years ago. Visiting your grandfather’s farm ignited your love for animals, and it only grew the older you became. After eight years, you earned a bachelor’s degree in animal science and were officially a doctor in veterinary medicine.
Since your veterinary school was near Zuzu City, you picked up a job offer at a clinic in the heart of the city and worked almost exclusively with dogs and cats. It was incredibly fun; however, you had forgotten your initial dream of working with farm animals instead of small ones. So when your grandfather died, you were happy to see he left you the farm in his will. While living in Zuzu City, you would visit Pelican Town every so often to say hello to your grandfather, but more so because Marnie was a client of yours. She called you whenever her animals were having the slightest of health issues. You were happy to answer her calls because it meant you would see cows, catch up with Marnie, and say hello to your grandfather.
You sighed while you stood on the porch of your grandfather’s old house, which was technically yours now. It was a beautiful spring day. You didn’t realize how much you had missed the sounds of birds chirping.
Marnie interrupted your peace by slamming the front door on her way out of the house.
“Whoops! Didn’t mean to let that door slam,” She chuckled. You smiled at her. You were so grateful she agreed to help you move your stuff today.
“Well, that was the last box,” She sighed in relief. “I’ve gotta run. Shane has to work a shift at JojaMart, and I need to watch Jas. You should stop by Robin’s house today so she can start building you a coop!” Marnie exclaimed, smiling at you.
“Yeah, I probably will. I want to get this place up and running as soon as possible,” You said, looking out onto the land again.
“I’ll be at the saloon Friday night. You should stop by and introduce yourself to everyone then,” suggested Marnie.
“That’s a good idea, actually. Gives me enough time to do some work and mentally prepare to meet all the new people,” You chuckled. Marnie rolled her eyes.
“They’ll love you. Just come by whenever you’re ready, okay?” She winked at you before walking off towards her farm.
You waved goodbye and groaned once you realized you would have to clear some overgrowth to build a chicken coop. You cracked your knuckles, grabbed your axe from the porch, and got to work.
A couple of hours of hard work later, you had a small clearing of land by the farmhouse. You decided that would be enough hard work for today, you weren’t sure when Robin would close up, and you haven’t unpacked anything in your house at all. You set the axe back on your porch and made yourself look somewhat presentable. You noticed your cat, Horace, had already taken a liking to the new digs. He had plopped himself on top of a pile of boxes. Horace was a fat, tuxedo tabby cat and essentially your best friend since you had adopted him your junior year of college. You gave him a pat on the head before heading out to Robin’s.
You admired the peace on your walk to the mountains. At some point, the hours must have melted away because three o’clock. You finally noticed how tired you were from moving in and doing physical work on the land. However, your dreams of dozing away were cut short. The walk to Robin’s was not as long as you had anticipated, though, as her house suddenly appeared hidden behind pine trees. You took a moment to admire her house, assuming she had built it herself. Wooden with a blue roof. You liked it. Once you spotted the telescope on the left, you immediately wondered how beautiful the skies must be here. You hadn’t seen a sky free of light pollution in years.
You cautiously opened the front door to see a counter with a ginger woman standing on the other side reading a newspaper. She looked up when the door opened, smiling at you.
“You must be Y/N! I’m so glad to meet you finally. I heard someone was moving into Cinnamon Meadow, but I didn’t know so soon. I’m Robin,” She said, coming out behind the counter to shake your hand. You shook it, happy to realize she wasn’t startled by some stranger entering her home. You smiled at her.
“Hi. Marnie said to come see you if I wanted anything built, so here I am,” You chuckled. Robin looked delighted.
“Well, sure! What were you wanting to have built?” She eagerly questioned. It was easy to see she was excited; not many villagers in Pelican Town needed new construction.
“I’m going to get Cinnamon Meadow up and running again, so I’ll need a new chicken coop. And then a barn. And probably house renovations. I need a lot done,” You sheepishly rubbed your neck, wondering if this was too much to request all at once. Robin defied you and lit up even more.
“Great! I can get started on the chicken coop tomorrow!” She exclaimed.
“Deal.”
~
After paperwork and settling payments, you returned to Cinnamon Meadow to continue yardwork. You felt so relieved that the coop wasn’t too expensive to build. You had been saving up since you paid off your tuition, and you were finally happy to invest some of the funds into your future. Around six o’clock, your exhaustion won over your ambition, and you decided to settle down for the night. You unpacked enough kitchen supplies to scrounge up some frozen dinner, took a hot shower, and promptly fell asleep with Horace in your small bed around eight.
You slept better than you had in ages. You even had a dream where your farm was complete, cows and all. But you knew something was missing. Or rather, a special someone. What was the farm if you had no one to share it with? You thought to yourself within your dream. You had always told yourself you didn’t need to be with someone, that as long as you made yourself happy, it was all that mattered. But you still ached for it. Your dream was cut short by a particular fat cat lightly smacking your cheek.
“What the–Horace!” You exclaimed.
“I was sleeping so well…” You sighed. You checked the time on your phone. 6 AM? Might as well get up now and get some yardwork done I guess… You thought to yourself with an elongated yawn. You realized you were a little sore from all the work yesterday. You groaned, knowing there would be more to come today. Slowly, you pulled yourself out of bed and organized some food for Horace. As expected, he flew to his breakfast and you figured you should do the same for yourself. A cup of coffee and one granola bar later, you pulled on your favorite pair of overalls and stretched. Today was going to be long. You intended to clear more of the land and buy and plant seeds.
You headed outside to start working and saw Robin hammering away at the coop. Her enthusiasm for her work made you smile.
“Morning, Robin! Any coffee for you?” You greeted.
“NO THANKS!” She yelled back with a smile. You wondered why she was screaming before noticing she was wearing headphones. You chuckled, grabbed your axe, and went straight to work.
Around one, you figured you should take a break to go to the store. You briefly recall Marnie mentioning a place called Pierre’s. After trading your axe for your wallet, you started heading in the general direction of town. It was another beautiful day. Are all the days here going to be as lovely as they have been? You wondered, smiling to yourself. You noticed that the change of scenery from moving here had already positively affected you.
You walked into town and focused on the square before you. It's small but adorable. Lamposts and trees lined the square, along with a few buildings. The one before you was the doctor’s clinic, with Pierre’s store on the other side. You briefly wondered about the town doctor for a moment. You knew you should get yourself checked up sooner rather than later. After doing farm research in your undergrad, you unfortunately found out the hard way that farm work was no joke. You filed away this thought for later and walked into Pierre’s.
The general store was small but had everything you could ever need. The older gentleman with glasses behind the single register smiled at you.
“You must be the new farmer! Y/N right? I’m Pierre. It’s so nice to have somebody new in town!” He exclaimed. You wondered when the last time somebody new moved into Pelican Town.
“Yeah, I’m Y/N. It’s nice to meet you,” You smiled back.
“I’m so sorry to hear about your grandfather. He was a great man. Sold me the best crops,” Pierre sighed. You felt a tinge of grief bite at you, pushing it away immediately.
“He was a good man. I fully intend to restore the farm, though, so I’ll have some crops for you,” You chuckled. Remembering what you came here for, you grabbed a bunch of random seed packets and essentials for your kitchen. You accidentally bumped into a woman with bright green hair in one of the aisles. You quickly learned she was Pierre’s wife, Caroline.
“You should come to the aerobics class here on Tuesdays! Great way to get to know everyone,” She smiled. The thought of any more exercise than you already had to do on the farm made you cringe.
“Maybe,” you tentatively said before mentioning it was good to meet her and heading to checkout. You went right home afterward, excited to plant your new seeds. You may have been a little ambitious when you started tilling the dirt; the field you created was large. You also knew if you wanted to make money anytime soon, it would be from crops.
It took forever to till, plant, and water the field. By the time it was 6, you were wiping sweat off your brow and decided that was all you could take today. You headed into your house to make a proper dinner from the groceries you picked up at Pierre’s today: homemade pizza. You savored every bite—your first meal in your first owned house. The thought made you smile. After a shower, you watched TV, cuddling Horace before finally falling asleep for the night.
The following two days seemed to blur together. At some point, you went to Marnie’s to catch up and buy chickens after Robin was done with the coop. You were overjoyed to finally have animals back on the farm and made a mental note to return to Robin’s on Monday to have her start building a barn. However, today was Friday. The day you were going to the saloon. You thought about it–stressed about it–while doing your farm chores that morning. Was everyone going to like you? Would they insist on kicking you out of Pelican Town? Or would you drink enough to forget these irrational thoughts and let go? You decided on the latter.
By the time five o’clock rolled around, you had showered and started getting ready for your first night out on the town. You threw on your favorite pair of jeans and a sweater with some jewelry. After a little makeup and tweaking your hair, you decided you were ready.
Walking out the door, you felt a cold spring breeze on your back. You were immediately grateful you picked a sweater. As you walked towards the saloon, you looked up at the sky. The sun had just begun to set. It was your favorite time of day. A part of you felt like having drinks on your porch alone instead of being crowded by strangers in a bar, but you knew better than to be a hermit tonight. You had told Marnie you would be there, so you would.
You could hear faint music and laughter inside as you approached the saloon. A warm glow of light emitted from the windows. You took a deep breath and walked in. The villagers were having so much fun not many even noticed you came in except Marnie. She sat in the center of the bar, smiling and waving at you. A wave of relief washed over you. You smiled and sat down
next to her.
“I’m so glad you came! I’ll have to introduce you to everyone,” She said, handing you a glass of wine—even more relief. You gulped to soothe your nerves. One by one, Marnie introduced you to some people in the town. You knew you would struggle to remember some of their names after tonight. You met Emily, tending the bar, along with Gus. Leah, an artist who had also moved to the valley from the city. Pam, who seemed like the local drunk. Willy, a sweet fisherman. Marnie pointed out other people; you determined Demetrius was married to Robin because they were dancing together. Some younger kids in the other room were Sebastian, Sam, and Abigail. A young woman with glasses suddenly sat herself next to you.
“Marnie, is this the new farmer we’ve all been hearing about?” She questioned, smiling at you.
“Yup! Y/N, meet Maru,” Marnie motioned to her.
“Hi,” you shyly said with a smile.
“Y/N is a veterinarian,” Marnie blurted out. You nodded.
“Good to have another scientist in town,” Maru giggled. “Dr. Y/N, then?” She asked. You laughed.
“Oh, no, please don’t call me doctor…except when I’m looking at your animals,” You winked, and they laughed. Maru looked in the other direction of the bar, and you saw something go off in her brain.
“I should introduce you to the only other doctor in town,” Maru giggled.
“Oh, sure, I’ve meant to meet them, actually,” You nodded. Maru took your hand and led you to a table near the jukebox. At the table sat two men having wine. One had long hair and wore a reddish coat, the other with glasses and a mustache wearing a green coat. Before you had time to think further, Maru set her hands down on the table.
“Gentlemen, this is Y/N. She just moved into Cinnamon Meadow. Harvey, she is also a doctor,” Maru said with a smirk. You briefly wondered which one she was talking to before the man in the glasses smiled.
“Is that right? I’m the town’s doctor, Harvey,” He introduced himself. You were taking him in. Handsome. Really handsome. It didn’t help you had a thing for mustaches, but he was also smart, evidently.
“I’m a veterinarian. I planned on getting my MD for a while but decided I liked animals more than people,” This raised a laugh out of them all.
“Good to meet you, doctor Y/N,” Harvey said, sipping his wine. The man with the long hair introduced himself as Elliott. You immediately let his name slip your mind because you were considering how you would further get to know Harvey. Marnie interrupted your thoughts by calling for you from the bar.
“Y/N! Come here, you gotta tell me what breed of cows you want to invest in!!” You blushed.
“I suppose I’ll see you later,” You said, mainly to Harvey. You could feel the alcohol working its way into your system, so it was probably best you get away from him now before you were completely drunk. Harvey looked a little disappointed.
“Be sure to come see me some time to get checked up,” He quickly mentioned. You nodded, smiling; maybe you weren’t just delusional, and he thought the same about you. You walked back to Marnie, but every fiber of your being wanted to stay and have another drink with him.
#stardew valley#sdv harvey#sdv harvey x reader#stardew harvey#harvey x reader#harvey x farmer#sdv farmer
7 notes
·
View notes
Note
hello ! i’m so glad i found your page, first of all. thank you po agad as your posts about psych have helped me get to know more about the /realities/ sa careers na kasama sa field. :))
i am currently taking up an undergrad degree in social science (sociology) in up as well ! i’ve wanted to shift to psych pero mukhang mahihirapan ako if i try as the slots are very limited. however, my envisioned career po eventually ay sa medical side talaga (i dream to either be a psychologist or a psychiatrist).
my question is, does it push me back sa psych path/career na i’m not an undergrad psych graduate? will it affect my goals to either proceed to clinical psych (and then take a psychologist licensure exam) or enroll in med school (become a psychiatrist)? is being a psych major a required step to pursue these careers? further, may advantages po ba na closely related naman ‘yung current program ko sa psych?
thank you very much ! ♡
Hello! I'm glad that my blog is somewhat helpful to you. 😊 Another person actually asked me a similar question, actually. You can check out my other responses to Asks on my page. But, anyway...
I wouldn't say that you're pushed back if the career you want is within psychology and your current program is sociology. However, having a psychology degree in college does afford you an advantage into some opportunities that can propel you into the field in psychology (e.g., jobs, grad school, etc.). But, that's not always the case in the real (adult) world. I have fellow classmates and peers who came from non-psychology college degrees, like fine arts, film, and business administration, just to name a few. I would even argue that other fields can also bring you advantages and creativity into how you will train yourself to become a psychologist. For example, at the top of my mind, I can imagine that sociological thoughts and ideas actually offer a lot of insight into how we look at mental health, psychotherapy, and the like.
When you step into grad school in psychology, many programs and schools will surely teach you the basics you may have missed from a bachelor's in psychology program (i.e., theories, research methods, etc.). Of course, having studied them back in college seems helpful, but ultimately it still depends on how you dedicate your effort and care into learning, no matter what college degree you have. Trust me, it will matter less as you journey further.
One thing though... I do notice that you seem to be considering two distinct paths: a psychologist OR a psychiatrist. These are two different roles/occupations but they do come with some similarities. While both overlap as a mental health professional, each requires a specific kind of training and timetable of formal education. At least in the Philippines, becoming a psychologist is faster on the average since it only requires you to complete a master's or doctorate degree (not MD!) before taking the licensure as a psychologist. On the other hand, becoming a psychiatrist requires you not only a medical degree, but also additional training and certification into specializing in psychiatry. Unfortunately, I cannot speak to how psychiatrists do training. I suggest looking for a psychiatrist you can ask about how they train. There are also some differences in approach to mental health as well but I won't elaborate them here for now (mas mahabang usapan na kasi yun hehe!). But, I do recommend that you learn more about each career path thoroughly.
My advice to you is to keep exploring your possibilities, even if you're in sociology, and decide to what you find is more important now and who you want to be in the future. Also, don't be afraid to take your chances no matter how small they are. I really don't want to tell you exactly what you should do -- and you're always free to disagree with me or take my words with a grain of salt -- but you will always miss all of the chances you never take. 😉
I hope this helps! Good luck!
3 notes
·
View notes
Text
Schizophrenia books x2!
I wrote two books on schizophrenia. Both can be found everywhere, Amazon included. Both of my books have been comprehensively reviewed including by some of the best in the world with expertise on schizophrenia i.e. certain MDs (psychiatrists) and PhDs (psychologists). If you are interested in the topic of schizophrenia, perhaps my books may well-suit.
My first book is “On Conquering Schizophrenia; From the Desk of a Therapist and Survivor; With Purview on Metaphysics, Philosophy, and Theology”. My second book is “The Essential Schizophrenia Companion; With Foreword by Elyn R Saks, PhD, JD”. I am a longtime mental health talk-therapist (a Licensed Clinical Social Worker- LCSW) who has lived with schizophrenia for 25+ years. Both books combine clinical perspective with lived experience perspective i.e. clinical psychology amid an otherwise first-person narrative.
Attached you will find some images of the books with some related reviews. More such editorial reviews can be found on the Amazon pages. Otherwise and most importantly, I wish you a great day, and tomorrow too! -Robert
My first book- “On Conquering Schizophrenia; From the Desk of a Therapist and Survivor; With Purview on Metaphysics, Philosophy, and Theology”
My second book- “The Essential Schizophrenia Companion; With Foreword by Elyn R. Saks, PhD, JD”



3 notes
·
View notes
Text
MADD and trauma
I got this comment on one of my posts

Remember, guys, Google is your friend
Below is a whole bunch of different sites and papers that say exactly what I said
Childhood traumatization and dissociative experiences among maladaptive and normal daydreamers
"The results revealed that certain types of childhood trauma occurred significantly more frequently in the group of maladaptive daydreamers."
British psychological society
"Maladaptive daydreaming usually occurs as a coping mechanism in response to trauma, abuse or loneliness."
Cleveland clinic
"These daydreams are usually a coping mechanism for other mental health conditions or circumstances. It's common — but not required — for people who have this to have a history of childhood trauma or abuse."
Maladaptive daydreaming: an escape from reality
"Maladaptive Daydreaming is the brain’s inventive way of coping with the anguish of trauma."
Childhood Trauma and Maladaptive Daydreaming: Fantasy Functions and Themes In A Multi-Country Sample
"Their reported childhood traumata were associated with the utilization of MD to distract from painful memories."
Top 5 Causes of Maladaptive Daydreaming
"The root causes of maladaptive daydreaming can be categorized as either trying to avoid something, trying to escape something, feeling a sense of boredom, feeling a sense of loneliness, or having difficulty grappling with a large life change of some kind."
Understanding the root cause of maladaptive daydreaming (this is a really good article and there's way too much to quote)
Maladaptive daydreaming
"The studies conducted by Eli Somer and many others have observed several commonalities concerning the onset of MD. Trauma, abuse, sexual assault, loneliness, or any kind of tragic experiences incites a strong urge to escape from all these problems."
Maladaptive daydreaming as a new form of behavioral addiction
"MD was developed as a strategy to cope with distress but led to uncontrollable absorption in fantasy, social withdrawal, and neglecting aspects of everyday life."
Maladaptive Daydreaming vs Hallucinations: Are They the Same?
"Early life trauma often plays a role in the development of both maladaptive daydreaming and psychosis, or the loss of touch with reality (of which hallucinations are a symptom)."
39 notes
·
View notes
Text
Adolescent Psychiatry Services : Mental Health Services
Adolescence is a critical period of development where individuals experience significant physical, emotional, and social changes. It is also a time when many mental health conditions emerge or worsen. Visit Now: www.accesshealthservices.org
#Adolescent Psychiatry Services#Mental Health Services#Adolescent Psychiatry Care#Access Health Services#Access Health Care Services#Psychiatric Clinic MD#Mental Health Clinic MD#MD Mental Health Services#Mental Health Clinic Baltimore MD#MD Mental Health Clinic#Psychiatrists in MD#Psychiatric Treatments in MD
0 notes
Text
By: Pamela Garfield-Jaeger
Published: Jun 22, 2023
On May 5th and 6th, 2023, I attended a training conference organized by the California Association of Marriage and Family Therapists (CAMFT). My aim was to gain an in-person perspective on the unfolding developments within my profession, particularly concerning gender ideology. I was eager to witness the current discourses imparted to my colleagues first-hand. Some striking revelations emerged from these sessions, some of which I will share, while primarily focusing on why I am convinced that gender activists feel their narrative is under threat.
In one of the sessions, Linda K. Reeves, a WPATH GEI Certified Gender Specialist, openly voiced her concerns, saying she was “afraid” of the new bills being passed in the Republican States, labeling them as “anti-trans.” The bills she referred to are designed to protect minors from irreversible medical interventions before they’re capable of informed consent. Reeves’ sentiment of fear was expressed twice during her 90-minute lecture, indicating the perception of losing legislative ground amid previous progress made by the trans community.
In another intriguing move, the workshop “Gender-Affirming Medical and Mental Health Care for Transgender Adolescents,” hosted by Aydin Olson-Kennedy, LCSW, and Johanna Olson-Kennedy, MD, requested that no filming take place due to a “tumultuous and hostile environment.” Ayden, a fully transitioned trans man, and Johanna, a Los Angeles Children’s Hospital pediatrician with 16 years of experience prescribing puberty blockers, were the sole workshop to issue such a request. This class “taught” me that puberty blockers are as harmless as a new haircut or clothing style. My question for them is: If you are an expert sharing important clinical information that you are certain of, why would you want your workshop to be hidden?
This workshop attempted, albeit clumsily, to debunk various gender-critical perspectives, signifying that opposing narratives are reaching their audience. For instance, the common question of a child's self-awareness at a young age was addressed. Both Ayden and Johanna asserted that children as young as three know their identities. They countered the prevalent concern about the internet’s influence on young people, stating that more time online is actually a good thing and indicates a healthy journey of self-discovery. Johanna advocated the transitioning of children since every trans adult was once a child, conveniently omitting that a majority of children with gender dysphoria, when not “affirmed,” ultimately desist.
According to a summary of multiple studies, about 80 percent of children desist.
Evidence from 10 available prospective follow-up studies from childhood to adolescence indicates that childhood gender dysphoria will recede with puberty in ~80% of cases. A Dutch paper notes that follow-up studies show the persistence rate of gender identity disorder to be about 15.8%, or 39 out of the 246 children who were reported on in the literature.
During the workshop, the Olson-Kennedys emphasized that gender dysphoria often causes other co-morbid mental health issues, contradicting what many therapists observe—distressed children clinging to trans identity with the misguided belief that it will resolve their underlying issues. “Depression treatment does not treat dysphoria. Gender Dysphoria for some folks is Depression. Gender Dysphoria = Depression,” stated Aydin Olson-Kennedy.
Unexpectedly, the instructors discredited the standard psychology manual, the Diagnostic Standard Manual-5 (DSM-5), which states a person must experience Gender Dysphoria for at least six months. Ayden described the DSM as a book smothered in cis-white privilege. Ayden stated the DSM was “colonized” due to its problematic binary language and its emphasis on Gender Dysphoria as distress. However, Ayden spent much of the lecture, including a video, showing the audience how distressing being trans is. Ayden even said it’s “normal” for dysphoric feelings to increase after receiving hormones and surgeries and, in fact, “There are pieces of dysphoria you can’t undo,” negating the prevailing thought that transition ameliorates distress. Nevertheless, the audience was assured that offering puberty blockers, hormones and surgeries is the compassionate form of treatment. Ayden rhetorically asked the audience: “At what point is it mean to let people suffer?”
Finally, Olson-Kennedy acknowledged the existence of detransitioners, a group often overlooked due to their narratives challenging the notion that those who claim to be trans are always know. The instructors downplayed the numbers of detransitioners but couldn’t entirely ignore their existence given the compelling stories increasingly being shared by individuals like Chloe Cole, Ritchie Herron, and many others who fell victim to “gender-affirming care.” “People are going to detransition, that’s OK, but we need not to organize our practice around it,” she said.
Shockingly, Olson-Kennedy also dismissed concerns about excessive prescription of puberty blockers, arguing legislation to be unnecessary given that “Only 5,000 children total are on puberty blockers in the U.S. That’s a small amount of kids to be writing legislation about.” However, most people would agree that 5,000 healthy children being medicalized for life is too 5,000 many. She also argued that puberty blockers are very helpful because they prevent future surgeries. Moreover, she failed to highlight potential side effects, like the inability to achieve a sexual orgasm later in life for those initiating puberty blockers before Tanner stage two (age 9-11), or the FDA’s warnings about brain swelling and blindness.
Another astonishing argument came when the detrimental effects of cross-sex hormones were downplayed, with the simplistic reasoning that “everyone has hormones.” Yes, that was the argument, from a credentialed medical professional nonetheless. A few side effects were mentioned but many serious ones, like early-onset menopause, urinary tract issues, mood instability, blood clots, and heart issues, were omitted. “At least the patient is alive”, she stated, alluding to the high suicide rates of trans people, but she did not share any data on that point.
Lastly, Linda Reeves addressed Lisa Littman’s research on Rapid Onset Gender Dysphoria (ROGD) in her presentation, claiming it had been “debunked” by WPATH due to its reliance on parental observations. It was dismissed based on the assumption that parents possess no real insight into their children’s emotions or histories. A slide from the presentation included an emotion-based argument claiming the report was “intended to cause fear” instead of revealing factual insights.
I see this as a win. WPATH knows this data is a threat to their questionable “standards of care” and they had to get their audience to hear about it with their spin first.
In summary, it was interesting to hear people who promote the sterilization of children and vulnerable adults attempt defend their faulty ideas. Most of what I heard were blatant lies and the bending or omission of truth. They openly said they were afraid of the “attacks” on trans people (which are simply bills to protect minors from high-risk procedures) and they tried unsuccessfully to discredit the thoughts, ideas, and experience of many outspoken critics of transgender medicine. Their quick-paced deliveries and limited question times further hinted at an awareness of growing scrutiny. For those opposed to the gender transition of minors and vulnerable adults, this means your voices are being heard and making a difference. Continue standing up for your beliefs; it's causing those pushing these transitions to reassess their stance.
==
Fear can make creatures dangerous, however. Especially when they no longer have anything to lose.
#Pamela Garfield Jaeger#gender ideology#queer theory#medical transition#sex trait modification#medical malpractice#medical scandal#medical corruption#puberty blockers#blockers#wrong sex hormones#cross sex hormones#blatant lies#WPATH#World Professional Association for Transgender Health#genderwang#religion is a mental illness
10 notes
·
View notes
Note
Idk if this is something you feel able to give advice on, but Seeing Wolves Where there are No Wolves is a big comfort to bc I know I too need help & its good to know that it's out there, but I don't know how to start. Like how the hell do you choose a therapist?! I google and still dont get the difference between lpc vs psyd, let alone what questions to ask or how to tell if they're a good fit. Feel free to say pass, but if you have tips I would so greatly appreciate it. thanks and sending love
hello, anon!
im actually able to help with this! im good at finding counselors! (and dentists!)
so, there are a couple of ways to go about this, but the truth of the matter is that if you've never been to therapy, or you're new to an area and are searching for a counselor, you may have to shop around a bit before you find the right fit. This can be emotionally taxing, so seeking out the right one will take some refining.
Acronyms To Know:
MSW: Master of Social Work
M.Ed: Master of Education / M.S.Ed: Master of Science in Education
M.S or M.A: Master of Science and Master of Arts, respectively.
LPC: Licensed Professional Counselor
LMHC: Licensed Mental Health Counselor
LCPC: Licensed Clinical Professional Counselor
LPCC / LCMHC: Licensed Professional Clinical Counselor of Mental Health / Licensed Clinical Mental Health Counselor
LMHP: Licensed Mental Health Practitioner
MFCC: Marriage, Family and Child Counselor
LCSW: Licensed Clinical Social Worker
DR is someone with a doctorate while MD is for Medical Doctor, and a Ph.D is someone with their doctorate of Philosophy - and all of these are people that are capable of obtaining certifications and licenses in a variety of counseling types, what it means to you is how much time this person has spent in school. In my experience, how much time a person has spent in school is not super indicative of how helpful they are, and it's much more informative to find out how many years they have spent in the field, and what their listed specialties are.
If you've been to counseling before, you may already be aware of what modes of therapy work best for you (Talk Therapy, DBT, CBT, EMDR, etc), but if you found Seeing Wolves to be comforting and that is the kind of therapy you're looking for, you will want to seek out a counselor that specializes in CBT (Cognitive Behavioral Therapy), DBT (Dialectic Behavioral Therapy) and/or Trauma Focused Therapy.
I highly recommend seeing counselors that have at least 5 years in the field, and in particular, at least 5 years of training or experience in dealing with trauma focused therapy. You may see counselors listing years of experience in rehabilitation centers with people who have substance abuse disorders, or working with veterans in VA hospitals and such - these are good indicators that they are aware of, and well practiced in trauma-informed approaches of therapy, even if they aren't specifically licensed or advertised as that.
Remember that your initial meeting with a new counselor is about you sussing THEM out, to see if they're a good fit. It's okay if you don't click right away, or if the vibes are off and you're like 'hmm :T i think im gonna keep looking.'
When picking a counselor, read their bios and work histories - determine if their field work feels relevant to the skills you want in a counselor, and look out for red flags, like 'faith-based approaches' as this can either be PRECISELY what you're looking for, OR it can be extremely limiting and unhelpful if the faith they're basing their practice on is only one, specific faith that does not align with yours.
That's all the advice I can really give on this without knowing what you're specifically struggling with. If you feel comfortable divulging more to me, I can help you narrow down your search more, but I hope this is helpful!!
#ask#anon#melanie answers stuff#psychology#mental health#it's a lot to keep track of i know#i hope u find what you're looking for!#you're v brave for starting the journey!!!! im proud of u!!!!!!
9 notes
·
View notes
Text
Psychopathology, Ch 2 pt. 3
Identify the major types of helping professionals and describe their training backgrounds and professional roles.
Clinical psychologists: have earned a doctoral degree in psychology, either a PhD (Doctorate of Philosophy), a PsyD (Doctorate of Psychology), or an EdD (Doctorate of Education) from an accredited college or university. Training in clinical psychology typically involves four years of graduate coursework, followed by a year-long internship and completion of a doctoral dissertation. Clinical psychologists specialize in administering psychological tests, diagnosing psychological disorders, and practicing psychotherapy. Until recently, they were not permitted to prescribe psychiatric drugs. However, as of this writing, five states (Idaho, Illinois, Iowa, Louisiana, and New Mexico) have enacted laws granting prescription privileges to psychologists who complete specialized training programs. The granting of prescription privileges to psychologists remains a hotly contested issue between psychologists and psychiatrists and within the field of psychology itself.
Counseling psychologists: also hold doctoral degrees in psychology and have completed graduate training preparing them for careers in college counseling centers and mental health facilities. They typically provide counseling to people with psychological problems falling in a milder range of severity than those treated by clinical psychologists, such as difficulties adjusting to college or uncertainties regarding career choices.
Psychoanalysts: typically are either psychiatrists or psychologists who have completed extensive additional training in psychoanalysis. They are required to undergo psychoanalysis themselves as part of their training.
Psychiatrists: have earned a medical degree (MD) and completed a residency program in psychiatry. Psychiatrists are physicians who specialize in the diagnosis and treatment of psychological disorders. As licensed physicians, they can prescribe psychiatric drugs and may employ other medical interventions, such as electroconvulsive therapy (ECT). Many also practice psychotherapy based on training they receive during their residency programs or in specialized training institutes.
Psychiatric nurses: typically are registered nurses (RNs) who have completed a master’s program in psychiatric nursing. They may work in psychiatric facilities or in group medical practices where they treat people suffering from severe psychological disorders.
Clinical or psychiatric social workers: have earned a master’s degree in social work (MSW) and use their knowledge of community agencies and organizations to help people with severe mental disorders receive the services they need. For example, they may help people with schizophrenia make a more successful adjustment to the community once they leave the hospital. Many clinical social workers practice psychotherapy or specific forms of therapy, such as marital or family therapy.
Counselors: have earned a master’s degree by completing a graduate program in a counseling field, such as mental health counseling or rehabilitation counseling. Counselors work in many settings, including private practices, schools, college testing and counseling centers, and hospitals and health clinics. Many specialize in vocational evaluation, marital or family therapy, rehabilitation counseling, or substance abuse counseling. Counselors may focus on providing psychological assistance to people with milder forms of disturbed behavior or those struggling with a chronic or debilitating illness or recovering from a traumatic experience. Some are clergy members who are trained in pastoral counseling programs to help parishioners cope with personal problems.
Describe the goals and techniques of the following forms of psychotherapy: psychodynamic therapy, behavior therapy, person-centered therapy, cognitive therapy, cognitive-behavioral therapy, eclectic therapy, group therapy, family therapy, and couples therapy.
Psychotherapy: a structured form of treatment derived from a psychological framework that consists of one or more verbal interactions or treatment sessions between a client and a therapist.
- used to treat psychological disorders, help clients change maladaptive behaviors or solve life’s problems, or to help them develop their unique potentials.
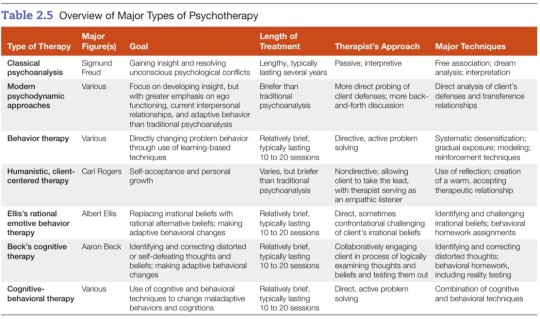
Psychoanalysis: the method of psychotherapy developed by Sigmund Freud.
Psychodynamic therapy: therapy that helps individuals gain insight into and resolve deep-seated conflicts in the unconscious mind.
Free association: the method of verbalizing thoughts as they occur without a conscious attempt to edit or censor them.
Transference relationship: in psychoanalysis, the client’s transfer or generalization to the analyst of feelings and attitudes the client holds toward important figures in their life.
Countertransference: in psychoanalysis, the transfer of the analyst’s feelings or attitudes toward other persons in their life onto the client.
Behavior therapy: the therapeutic application of learning-based techniques to resolve psychological disorders.
Systematic desensitization: a behavior therapy technique for overcoming phobias by means of exposure to progressively more fearful stimuli (in imagination or by viewing slides) while remaining deeply relaxed.
Gradual exposure: in behavior therapy, a method of overcoming fears through a stepwise process of exposure to increasingly fearful stimuli in imagination or in real-life situations.
Token economy: a behavioral treatment program that creates a controlled environment in which desirable behaviors are reinforced by dispensing tokens that may be exchanged for desired rewards.
Person-centered therapy: the establishment of a warm, accepting therapeutic relationship that frees clients to engage in self-exploration and achieve self-acceptance.
Empathy: the ability to understand someone’s experiences and feelings from that person’s point of view.
Genuineness: the ability to recognize and express one’s true feelings.
Congruence: the coherence or fit among one’s thoughts, behaviors, and feelings.
Cognitive therapy: a form of therapy that helps clients identify and correct faulty cognitions (thoughts, beliefs, and attitudes) believed to underlie their emotional problems and maladaptive behavior.
Rational emotive behavior therapy (REBT): a therapeutic approach that focuses on helping clients replace irrational, maladaptive beliefs with alternative, more adaptive beliefs.
Cognitive behavioral therapy (CBT): a form of psychotherapy incorporating cognitive and behavioral techniques.
Eclectic therapy: an approach to psychotherapy that incorporates principles or techniques from various systems or theories.

Group therapy: a form of therapy in which a group of clients with similar problems meets together with a therapist.
Family therapy: a form of therapy in which the family, not the individual, is the unit of treatment.
Couples therapy: a form of therapy that focuses on resolving conflicts in distressed couples.
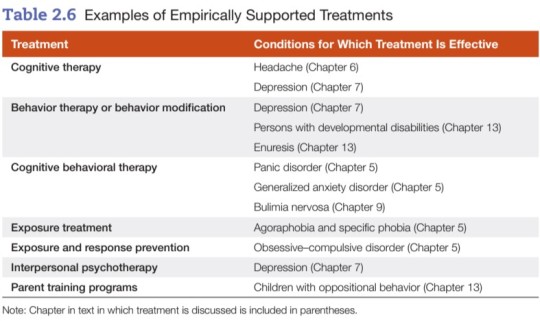
Evaluate the effectiveness of psychotherapy and the role of non-specific factors in therapy.
Nonspecific treatment factors: factors not specific to any one form of psychotherapy, including
empathy, support, and attention shown by the therapist
the therapeutic alliance = attachment the client develops toward the therapist and the therapy process
the working alliance = effective working relationship in which the therapist and client work together identifying and confronting the important problems and concerns the client faces
Telehealth: delivery or facilitation of treatment services via telecommunication or digital technology.
Evaluate the role of multicultural factors in psychotherapy and barriers to use of mental health services by ethnic minorities.
- Cultural sensitivity involves more than good intentions. Therapists must have accurate knowledge of cultural factors and the ability to apply that knowledge when developing culturally sensitive approaches to treatment.
- Just because a given therapy works with one population group does not mean that it will necessarily work with other groups. Therapists using established treatments should consider how they can incorporate culturally specific elements to boost treatment benefits in working with people from different ethnic or racial groups.
- Some of the barriers to mental health services for marginalized communities include...
Cultural mistrust: People from minority groups often fail to use mental health services because they don’t trust mental health institutions/professionals. Mistrust may stem from a cultural and/or personal history of oppression and discrimination, or experiences in which service providers were unresponsive to their needs. When minority clients perceive white therapists and white-dominated institutions to be cold or impersonal, they are less likely to place their trust in them.
Mental health literacy: A person may not make use of mental health services because they lack knowledge of mental disorders and how to treat them.
Institutional barriers: Facilities may be inaccessible to marginalized people because they are located at a considerable distance from their homes or because public transportation is lacking. Marginalized people are often overwhelmed or intimidated by bureaucratic red tape and/or protocol around health procedures.
Cultural barriers: Many recent immigrants have had little or no previous contact with mental health professionals. They may hold different conceptions of mental health problems or view mental health problems as less severe than physical problems. In some cultures, the family is expected to take care of members who have psychological problems and may resist outside assistance. Other cultural barriers include cultural differences between socio-economically disadvantaged clients and majority white + middle-class mental health staff, and the stigma often associated with seeking mental health treatment.
Language barriers: Mental health facilities may lack the resources to hire mental health professionals who are fluent in the languages of the communities they serve.
Economic and accessibility barriers: Financial burdens are often a major barrier to use of mental health services. Living in a rural or isolated area where mental health services may be lacking or inaccessible is also a big hurdle.
Psychopharmacology: the field of study that examines the effects of therapeutic or psychiatric drugs.
Identify the major categories of psychotropic or psychiatric drugs and examples of drugs in each type and evaluate their strengths and weaknesses.
Anti-anxiety drugs: drugs that combat anxiety and reduce states of muscle tension.
~ also called anxiolytics
~ examples include benzodiazepines (Valium, Xanax) as well as hypnotic sedatives (Halcion)
+ can be safe and effective in treating anxiety and insomnia
- potential for psychological and/or physical dependence, so they tend to be better for short term or occasional relief, not long term or daily use
Rebound anxiety: the experiencing of strong anxiety following withdrawal from a tranquilizer.
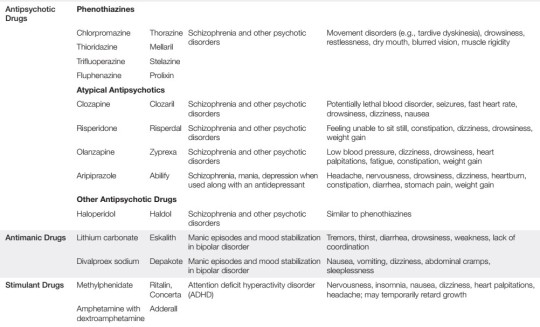
Antipsychotic drugs: drugs used to treat schizophrenia or other psychotic disorders.
~ also called neuroleptics
~ examples include Thorazine, Mellaril, Prolixin, Clozapil (atypical)
+ drastically reduced the need for long-term hospitalization, physical restraints, and confinement
- unpleasant side effects, such as muscular rigidity and tremors; long-term use of antipsychotic drugs (with exception of Clozapine) can produce tardive dyskinesia, a potentially irreversible and disabling motor disorder
Antidepressants: drugs used to treat depression that affect the availability of neurotransmitters in the brain.
~ four major classes: tricyclic antidepressants (TCAs), monoamine oxidase inhibitors (MAOIs), selective serotonin-reuptake inhibitors (SSRIs), and serotonin-norephinephrine reuptake inhibitors (SNRIs)
~ examples include Tofranil, Elavil, Sinequan (tricyclics), Nardil (MAOI), Prozac, Zoloft (SSRI), Effexor (SNRI)
+ antidepressants provide beneficial effects for a wide variety of psychological disorders
- however, there are side effects for each category, and in the case of MAOIs, a patient’s diet is heavily restricted

Electroconvulsive therapy (ECT): a method of treating severe depression by administering electrical shocks to the brain.
+ significant improvement for patients experiencing severe epileptic seizures or major clinical depression that has not responded to other treatment
- high relapse rates and memory loss for events occurring around the time of treatment; for these reasons, ECT is a last resort
Describe the use of psychosurgery and evaluate its effectiveness.
~ Previously, the prefrontal lobotomy was the most common form of psychosurgery. This procedure involved surgically severing nerve pathways linking the thalamus to the prefrontal lobes of the brain.
~ The premise of this operation was the belief that severing the connections between the thalamus and the frontal lobe of the cerebral cortex would control a patient’s violent or aggressive tendencies.
- This procedure was abandoned because (1) there was insufficient evidence of its effectiveness and (2) it often produced serious complications or even death.
- When anti-psychotic drugs became available during the 1950s, psychosurgery was all but eliminated.
+ In recent years, more sophisticated psychosurgery techniques have been introduced which target much smaller parts of the brain and produce far less damage than the prefrontal lobotomy. These techniques have been used to treat patients with severe OCD, bipolar, and/or major clinical depression who have failed to respond to other treatments.
~ Another experimental technique is deep brain stimulation (DBS), a surgical procedure in which electrodes are implanted in the brain and used to electrically stimulate deeper brain structures.
+ DBS shows promise in treating severe forms of depression and OCD that have failed to respond to more conservative treatments.
- However, DBS may have serious complications and its effectiveness needs to be investigated further. Thus, it is still an experimental treatment.
Evaluate biomedical treatment approaches.
~ Overall, a combination of medication and talk therapy seems to be more helpful for most mental health patients than either treatment alone.
~ The benefits and risks/side effects of each medication need to be carefully considered and discussed by the provider and the patient.
10 notes
·
View notes
Text
“Clinicians experience moral stress when they feel like they can’t provide good care because the systems they work in are working against them. Our findings make clear that the crisis of professional wellbeing facing our healthcare workforce is not only a mental health problem but also a moral one,” Buchbinder said.
“The STEPPS findings contribute to a more nuanced understanding of the health care worker’s perspective on every day and crisis situations arising in contemporary American hospitals,” said Berlinger. “Often, these frontline workers–in this case, physicians–are diagnosing what’s not working in their systems, and what they need to do their jobs well and to feel they are doing right by their patients. It is crucial for clinical leadership to listen to these insights and use them to build much more supportive environments for the work of healing and the relief of suffering.”
“Extreme burnout of our healthcare workforce was present before the pandemic and has been exacerbated in a most extreme way these past few years as we continue to move through this continuous crisis,” said Nadia E. Charguia, MD, director of UNC Health’s Taking Care of Our Own Program and a member of the STEPPS advisory board.
“We have an opportunity to learn and grow from all we have been through. We cannot continue to primarily focus on helping our workforce be more resilient when we are asking them to tolerate fractured and broken systems,” Charguia said.
8 notes
·
View notes
Text
I lost one notable follower after my previous post about my break-up. And as I reflect back on what I wrote, an item currently rubs me the wrong way:
I called my ex a "manchild." That was very disrespectful of me and I said it out of frustration. I apologize to to anyone who also struggles. Goodness knows I have my struggles too. (A lot more than I let on.)
Don't get me wrong, my ex is a very capable adult. He has built a career as a therapist in mental health care, working with clients who have HIV/AIDS. He has worked at a variety of LGBT clinics including Callen-Lorde in NYC, the Los Angeles LGBT Center, and now DAP Health in Palm Springs. These are all world-class healthcare organizations that provide specialized medical and mental health services to the LGBTQ+ community. His current role is leading a department responsible for handling patients who are in a mental health crisis. He's the one MD's call when a patient starts freaking out or talking about killing themself, because MDs are NOT trained to handle mental health situations.
My ex has a super-power, and it is empathy. He is a fantastic mental health therapist, and in his current role he works with some of the most difficult clients, those who are currently "in crisis."
As I mentioned above, RNs, LVNs, and MDs are not trained to handle these clients, to talk them off the ledge, to get them the help and resources they need.
My ex did it brilliantly and wonderfully. It is his gift. I am super proud of him and his successes. It would have been an honor to be by his side for the rest of our lives.
My frustration stems from other aspects of his life and personality.
(With the above information, hopefully my use of the word "manchild" makes more sense in the context of my post below.)
3 notes
·
View notes
Text
Yoga and Pilates
Weight Clinic MD is a weight loss clinic that offers a comprehensive approach to weight management and obesity medicine. They provide personalized treatment plans that are evidence-based and FDA-approved. Their multidisciplinary approach includes virtual consultations, telemedicine, and compassionate care. Their weight management program addresses obesity-related health conditions such as type 2 diabetes, hypertension, sleep apnea, high cholesterol, fatty liver disease, metabolic syndrome, heart disease, stroke, and cancer. The clinic uses prescription weight loss medications such as Contrave, Saxenda, Qsymia, Belviq XR, Xenical, Topamax, Tenuate, Adipex-P, Bontril, Wegovy, and Monjaro to help patients achieve their weight loss goals. Nutritional counseling is an essential component of their weight management program. The clinic's registered dietitians provide guidance on healthy eating habits, meal planning, portion control, macronutrient tracking, calorie counting, food diary, nutrient-dense foods, balanced diet, and dietary supplements. They also offer fitness and exercise programs that include personal training, group fitness classes, cardiovascular exercise, strength training, HIIT, yoga and pilates, fitness tracking, and physical therapy. Mental health and wellness are equally important, and the clinic offers stress reduction techniques, cognitive-behavioral therapy, motivational interviewing, support groups, behavioral therapy, positive psychology, meditation, mindfulness, sleep hygiene, and addiction recovery programs. They also provide digestive health, sleep, metabolism, and hormone-related treatments. Low-carb diets, keto diets, intermittent fasting, Mediterranean diet, vegan, and vegetarian diets are some of the weight loss plans that they offer. They also provide Weight Watchers, Jenny Craig, and Nutrisystem programs. The clinic is located in a convenient location, and their pricing is affordable. Patients can expect doctor-supervised weight loss, personalized treatment plans, and bariatric surgery if necessary.
2 notes
·
View notes
Note
Hello, sorry if this has already been answered but I have PTSD and ASD (both clinically diagnosed) but fit a lot of the diagnostic traits for MD. Is it possible to have both of these and MD or would it be overlapping traits only?
If it is just overlapping traits, what's the stance on certain terms? as I have what would be described as paras and a paracosm
It's possible that they are overlapping experiences. It's possible they are comorbid conditions. The best thing, of course, would be to get the opinion of a mental health professional to help you sort out what is what.
As for terms, this is a personal decision and I can't speak for the entire community on their usage. I do feel safe to say though that, if after careful deliberation you still identify as a maladaptive or immersive daydreamer then the characters which are included in that experience would be included in any IM or MD centric terminology.
4 notes
·
View notes
Text
a small breakdown of some of hucks issues , why they were chosen for the character.
Depression - VA estimated that about 1 in 3 Veterans visiting primary care clinics has some symptoms of depression; 1 in 5 has serious symptoms that suggest the need for further evaluation for major depression; and 1 in 8 to 10 has major depression, requiring treatment with psychotherapy or antidepressants. (2008 , VA.gov) - polls indicate rates haven risen
Body Dysmorphia - A survey of advanced individual training of tri-service personnel at Fort Sam Houston, Texas, was performed combining the dysmorphia concern questionnaire, a supplement questionnaire, and demographic factors. Our study shows a higher than expected prevalence rate of BDD and MD in service members. ( 2016 , MilMed ) - The U.S. Marine Corps' Body Composition and Military Appearance Program (BCMAP) standards were not developed from populations that reflect the current makeup of the force and the fitness requirements that they are subject to. Research suggests that the implementation of these standards could drive marines to adopt unhealthy behaviors, primarily those associated with disordered eating, to meet the standards. ( 2022 , RAND )
Alcoholism - The relationship between military personnel and alcohol has a long history of contention and difficulty. According to a recent survey conducted by the Department of Defense, one-third of service members meet the criteria for hazardous drinking as well as a possible alcohol misuse issue. Members of the armed forces are especially prone to binge and hazardous drinking: One Department of Defense health survey found that 42.6 percent of Marine Corps service members had engaged in binge drinking within the last 30 days ( 2019 , DELPHI )
PTSD - PTSD is 3 times more likely among Veterans who deployed compared to those who did not (of the same service era). Some factors in a combat situation may contribute to PTSD and other mental health problems, including military occupation or specialty, the politics around the war, where the war is fought, and the type of enemy faced. ( VA.gov ) Survivors of sexual assault have an increased likelihood of meeting criteria for posttraumatic stress disorder (PTSD). They are also comparatively more likely to exhibit higher levels of PTSD symptom severity ( 2018 , SAGE journals )
Internalized Homophobia - this man's a white texan man who comes form a very conservative 100% live red die red household do i really have to explain why he has internalized homophobia over the fact that he is bi ????? and how that affected his mental health ???
4 notes
·
View notes
Last Seen Blogs

pearlmethystisshit
Pearlmethyst is the biggest shit in the world

bkdk-merri
All for Deku

portal2maps
Portal 2 Map Submissions

hetaliahater69
fuck hetalia

pbiwa00
Building Inspections Perth WA