#and then I had to do a subcutaneous injection
Explore tagged Tumblr posts
Visit Tumblr Blog
Explore Tumblr blogs with no restrictions, modern design and the best experience.
Last Seen Tumblr Blogs





Fun Fact
When “GIF” was named word of the year in 2012, Oxford Dictionaries U.S.A. credited Tumblr for pushing the word.
Text
2nd day of class and we're already helping during surgeries lmaooooo
#i mean she sid warn us that they were SHORT on staff and that the sooner we help the better#i just wasn't expecting actually having to do things during surgeries lol#the cat was super super good so that made having to restrain her easy thank fuck#and then I had to do a subcutaneous injection#and the girl is already filling us on the clinics drama lmaoo#it was a simple surgery though removing a tumour#we also did some blood and urine analysis#fun day tbh
0 notes
Text
Alright, we’re going to start with the Lucy update. The whole thing is long so I’m going to put it under a read more. But the short story is she has gone into heart failure and I’m unfortunately having to have her euthanized today.
Wednesday night I got home from work and saw that Lucy had vomited. She was lethargic and just generally didn’t seem like she felt good. It didn’t seem like a dire situation so I figured I’d see how she was in the morning and go from there.
Thursday morning she seemed to have rallied some. Her breathing was “off” and she sounded a little congested, but she was much more alert and seemed more comfortable. She didn’t eat a ton on Thursday but she pick at her food some. She also vomited a few more times. I felt good about her condition though because she seemed so much more alert and comfortable than Wednesday. I figured it wasn’t an emergency and I’d just bring her to work with me today.
This morning I woke up and she had no interest in breakfast at all. Her breathing was significantly worse from the night before. She was 100x more lethargic than she had been on Wednesday night.
We did a full work up this morning at the clinic and found that she had gone into heart failure. I discussed options with Doc and he said it was possible that we could get her through the worst of it and then with some medication she could be comfortable and happy for awhile yet.
She seemed to rally a little again after getting some injections and subcutaneous fluids. I tried to take her back home on my lunch period but she ended up vomiting blood and then becoming extremely weak and lethargic again. So we turned around and went right back to the clinic.
This is another one that I feel a little guilty about, like maybe I should have taken her to an emergency clinic earlier. Or maybe I should have realized her heart was failing sooner and then we could have started her on meds sooner and given her more time. But I also know she was very old and sometimes these things just happen so quickly. I did the best I could and I did what I thought was right, and that’s all you can do.
#my post#Lucy#was really not expecting this at all when I went to bed last night#also the ‘we had a doozy of a morning’ post was made before she vomited up blood#otherwise I probably would have worded that in a better / more appropriate way#but at the point I thought she was still coming home
199 notes
·
View notes
Text
A little bit about IVF:
In honour of my impending IVF cycles, I thought I'd talk you guys through an antagonist protocol, because that's what I'm on. It's considered one of the more short and minimal protocols in terms of injections. Needless to say, this is just a rough summary of one way IVF is done, there are several kinds of protocol that work a little differently.
This will be a politics-lite post - as anyone who follows me knows I'm very pro choice and anti- misinformation about IVF, but we're going to be focusing on the science and my journey here.
How does IVF start?
Ordinarily in a normal unmedicated menstural cycle, our body would be developing multiple follicles, but only one will mature enough to be released as a mature egg. The rest were backups and just die. Which is fine, because you don't normally want to be releasing more than one (that's how fraternal twins happen!) but it's kind of inefficient.
And given how we know a lot of eggs don't develop into embryos, and how lots of embryos stall and die, you can't really do IVF one egg at a time. So, we want to find a way to get more eggs at once. That's where IVF meds come in. At the start of an IVF cycle, we start using a stimulating agent - this makes the ovaries develop all the follicles that would have developed this cycle - it basically does the job of the hormones FSH and sometimes LH as well.
You start your stims on day 2 of your cycle and continue it until they tell you to stop it, but I've been given enough to take me up to egg retrieval. The team can and will tweak the plan as the cycle progresses, so IVF is the kind of treatment where you have to be prepared to pivot if things do not go to plan. Which, yknow, is hard as the kind of person who works in medicine.
From about day 6 onwards (it can depend on your estrogen level), I've been told to add in my GnRH antagonist - this should stop me from ovulating unexpectedly early, so we can collect more eggs. Effectively, you want as many eggs to grow and then ripen around the same time.
This graphic from the alife blog sums up the typical timeline:
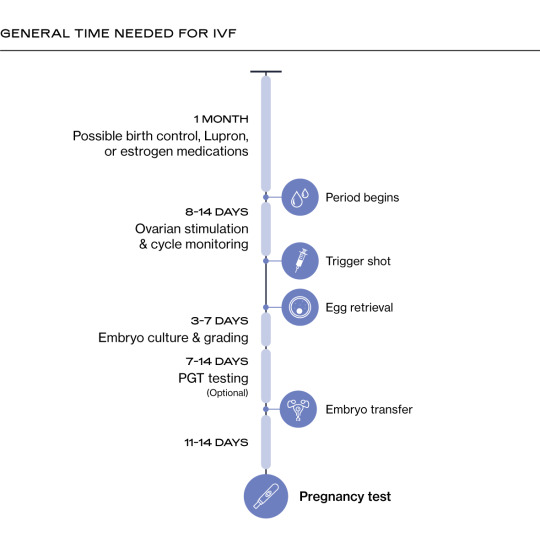
As it states, some people may be given birth control or other treatments before their IBF cycle - for example, to get their endometriosis or PCOS under control. It's also normal to have a transvaginal scan in the cycle before, just to make sure there aren't any new cysts or other issues that may need to delay treatment.
Once we have reached day 5/6 onwards, you're expected to have plenty of trans vaginal ultrasound scans (I've been warned these will be every other day) and often blood tests as well, to assess how the egg follicles are developing and when we should take the eggs out. I've had to be open with my work about undergoing IVF as I will likely have to cancel clinics at the last minute, and this was one of the things I've had the most nerves about - but you don't really get to choose when you are ready, there may be a bit of wiggle room, but really it's down to how your body responds to medication. Unfortunately when you're doing IVF, your timetable has to fit around the treatment, rather than vice versa.
The practicalities of IVF can be annoying - you get given a big bag with several medications in them, some of which need to be kept in the fridge, and most of which you need to self-inject into your tummy or thigh fat via subcutaneous injection. It seems like I won't need to do more than two injections once a day most days, but that's still a time commitment - especially as it needs to be at the same time of day if possible.
There's a large amount of variation in terms of how many eggs different people will be able to collect. For example, a person with low ovarian reserve may only make a couple of eggs- in rare occasions some people make none at all! On the other hand people with PCOS can make many but the quality of the eggs (and therefore their odds of fertilising and developing) may be lower. Either way, it's likely for someone undergoing IVF to feel uncomfortable as your ovaries can potentially become pretty swollen. I've made sure I have plenty of flowy dresses and unrestrictive clothing so I hope I can stay comfortable.
I've been told certain kinds of physical activity are not OK due to increased chances of injuring your ovaries, however protected sex is OK. Unprotected sex is not - because you're brewing a whole bunch of eggs and there's a small chance you can accidentally octomom yourself if you accidentally fertilise a bunch of them at once.
There is also the risk of ovarian hyperstimulation syndrome - a potentially life threatening complication, though this is rarer now thanks to treatment protocols being improved.
Egg collection and waiting:
Once we've reached the point that the eggs are done cookin', I take the trigger shot (which does the last bit of maturing the eggs prepping them for removal), and then the procedure to remove them is organised around 36 hours after that.
Collecting them is the riskiest part of IVF -you go under sedation or anaesthetic, because the preferred way of taking them out, usually, is via a guided needle inserted into the vagina. Ideally you want to get as many eggs as possible - so that you don't need to undergo another stimulation cycle if you can avoid it.
The reason you want more eggs is because of what they call the IVF funnel - at each stage some eggs will probably not develop or will die. These graphics from Alife (left) and Natalist (right) explains it better visually:

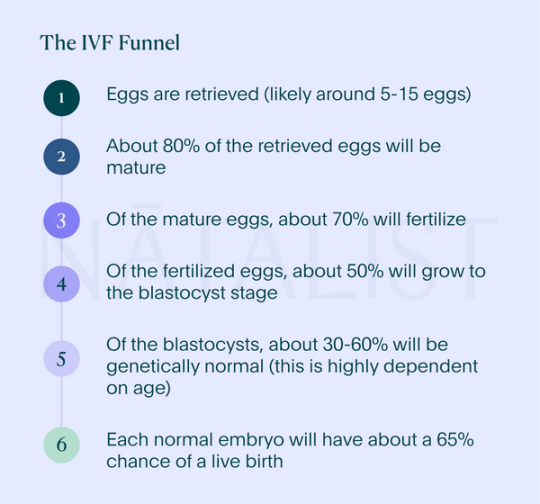
We can see that each step of the process can potentially result in eggs or embryos that will not work out.
Not all eggs that get collected mature adequately or fertilise - those that don't cannot be used for IVF and must be discarded or used for research.
Not all fertilised eggs will grow into a blastocyst that can be implanted. Some of those will develop abnormally or show chromosomal abnormalities that are not compatible with a successful pregnancy. These numbers are a rough guide - it's possible to collect a low number of eggs but have more of them turn out into viable embryos, or collect a ton of eggs (especially with PCOS) but lose a lot more along the way. There's really no way to tell.
I remember seeing this graphic by reddit user greenishbluish explaining their wife's IVF treatment (which I've shared before as they explicitly were hoping to raise awareness) - it demonstrates that you can get a lot of eggs, but sometimes a lot of them just won't make it:

It's easy to look at these figures and feel stressed out - there's potential to get 0 viable embryos after all that effort. But I feel like all you can do is try your best. I'm nervous but I'm excited - and for the first time in a long while, kind of hopeful.
Now, after the eggs have been collected and cooked for 3-5 days in the lab under the care of the embryologists, there are two options : freeze them, or implant one of them as part of a fresh cycle.
The NHS usually funds a fresh cycle during your collection cycle - basically, since you're already sort of primed to be pregnant, they put one of the embryos back in 3-5 days after it was taken out. If this is successful, great!
You continue after this as if you are pregnant, take your antenatal vitamins and progesterone (for me it's going to be vaginal pessaries, which is a relief as I don't relish the idea of intramuscular injections). You are normally advised to wait around 2 weeks before you test - in my case they've advised waiting 16 days, both to make sure that my HCG trigger shot has washed out of my system, and to give the test more than enough time to be positive. Whether you are pregnant or not, you have to call them up and let them know, so you can work on the next step.
The rest of the embryos are frozen around day 3-5 after they were retrieved and fertilised, and can then be used in subsequent cycles if they are needed. They have to be frozen to be used, because eggs can't develop for too long outside the body without complications and realistically you can't gestate them for months in a petri dish.
Now, frozen cycles can often have higher success rates - because rather than trying to optimise the hormones for both getting eggs and then implantation after, you can focus on just getting the lining right for implantation.
But most importantly, they are often needed because the success rates for each cycle aren't 100% - I'm hoping for about a 1 in 4 chance of getting a live birth from each cycle. That means each cycle you're rolling the dice and hoping for the best. Even with the best edical assistance, that only brings us in line with the odds of your average fertile person conceiving through regular PIV sex each month. However, given my odds are probably something like 1-2% trying unassisted at this point, I'll take those odds!
This is what I mean when I say that people going through IVF aren't (or at least shouldn't) be going into it with the idea that they are buying a child - there's no certainty. There's no guarantee. The NHS only covers IVF a limited number of times (set by your local health authority where you live), and after that if it didn't work you have to go private or give up.
We'll see what happens. One step at a time.
20 notes
·
View notes
Note
how quick did u start seeing changes on t? also as someone who is. Not a fan of needles how did/do you deal with injecting yourself?
Internally: immediately. possibility placebo, but I think hormonally T does impact uh, "arousal" immediately, and "arousal" is not something exclusively reserved for Being Horny. It's also like, mood and energy and such things. YMMMV
Physically: pretty quickly honestly, my voice dropped really fast (one of my only big "hm i dont like this" moments) and I had to start shaving my face at 2 months. I think I am a bit of an outlier in this respect though, and it largely depends on your genetics.
I am not sure how much I can help with needle phobia, I have never had a signifigant problem with needles. Injecting myself the first time vs just getting stabbed was kind of intimidating but I have learned how to do more difficult things over youtube before, and planned parenthood's video tutorials are very helpful.
The good thing is injection/needle anxiety is incredibly common, and lots of people with needle anxiety still need to self inject (i.e. diabetics), so there IS a lot of advice/help/devices out there if you are in that "physically able to inject yourself but it is still scary" zone.
They make auto injector attachments that help you inject (they're not actually 100% automatic but they usually hide the needle so you dont see it at least), and there's also a special perscription type of T (XYOSTED, iirc it is more expensive/harder to get) that comes in pre-fulled syringes, but you still have to hold it against your body and press a button to make it inject. For whatever it is worth, in my experience, I actually had MORE pain with subcutaneous injections (tiny needle), because the skin/fat is where it hurt the most, wheras with intramuscular injections (BIG needle) it goes past the skin/fat really quickly and into muscle which just isn't as sensitive. YMMV
They also make like, "prickle pads" I think? I've never used them but they help disperse the feeling of the poke. I think there are other tricks out there too, like numbing the area with ice or similar.
If you definitely can't do needles there is the option of gel (depending on your insurance or financial status), or having someone else inject it for you, be that a nurse or friend/family member.
20 notes
·
View notes
Note
i have trouble with doing my shots and gel does not work and is not an option for me; do you have any advice for doing them? the only way i can do it without getting the yips is a slow needle insertion, but my easier leg to access has such a build up of subcutaneous scar tissues that even doing it quickly is difficult.
hey good question!
i can relate to the subcutaneous scar tissue, i've had to be mindful of that lately. does anyone have suggestions for this anon? i do not have any sort of strong reactions to injections so i can't think of much advice but i hope some other people can help!
18 notes
·
View notes
Text
Testosterone HRT journey so far: an overview
Note: If you are below the age of 18 and reading this, please scroll past this post and blog as a whole. My channel is made by an adult for adults and some of the topics in my post may be (educationally) nsfw in nature. I believe everyone deserves resources & information to research, but I do not feel comfortable if this post were to be read by minors.
With that out of the way, some info about my hrt. I currently take 50 mg of testosterone every week through subcutaneous injection and have been doing so for 3 weeks. I wanted to make this post to give an overview of the changes and such I experienced to give other (pre) t trans/nb folks an idea of what they can expect in their first month of t.
First week
Big emotional confidence boost. Although there were no clear physical changes, it helped to know I was no longer waiting to finally get on t and that the thing that would change my body and life was actively inside my body.
First thing I noticed (a few days in) was an oilier skin. I've always had a greasy skin, but the consistency of the "grease" was definitely more oily than before. I could wipe my forehead with a tissue and oil would visibly be wiped off.
I had my first hot flash within a few days. I started getting "overheated" easier than before, but it calms down fairly quickly afterwards.
Second week
I noticed my libido started increasing at the end of the second week. Nothing dramatic or distracting during daily activities, but it's easier to get turned on and rub one out more than once a day if I wanted to.
Something about my voice changed. My voice itself still sounds pretty much the same, but it has started coming more from my chest than it did before and "vibrates" differently than it used to. I can talk comfortably in a slightly lower voice without it feeling forced, although this can't be considered a significant voice drop.
It has gotten easier for me to get frustrated by smaller, insignificant things. I'm a person with a lot of self control, so taking a deep breath and telling myself it's not that deep is enough to handle those emotions. But it's definitely something I noticed.
Third week
I started showing the beginning of what I believe is bottom growth. The bean has gotten significantly bigger and while it doesn't really protrude from the rest of my anatomy yet, it's a start.
Libido further increased, but can still manage it as well as before.
I think my sweat has started changing smell a little bit.
If anything else changes by the 1 month mark, I will post a new update! If not I may wait a few more weeks until I notice any other significant changes.
#hrt journey#hrt ftm#diy hrt#testosterone#trans#transmasc#trans man#hrt#trans hrt#trans healthcare#minors dni
10 notes
·
View notes
Note
i saw your post about "testosterone" puberty and while i appreciate the sentiment, i think you're wrong. and i say this as someone who is amab and went through an amab puberty.
i didn't sweat that much at all. and even when i did in summer, it was nothing a shower, soap and deodorant couldn't fix. my hair never got greasy, even when i was depressed and went for a week without showering or washing it. in fact, it was the opposite: it was unusually dry. my skin also never got oily and was always dry.
very few of my peers stinked because we practiced proper hygiene. it's your own responsibility as a teenager to clean yourself and practice proper hygiene, no matter how much testosterone you make. it's not a valid excuse to be dirty.
the reason you're sweating so much is probably because you're overdosing on testosterone. most transmascs on t take doses WAY HIGHER that what the average cis boy/man produces. the average cis boy/man has levels of 400-500, meanwhile the average ftm dosage is around 800-1000.
also, the timing of testosterone production is different. cis boys/men produce it daily (every morning), meanwhile you guys get it weekly (whenever you take your shots). so it's more evenly spread out amongst cis boys/men.
if you're bothered by the symptoms you're experiencing, you should talk to your doctor about lowering your dosage.
Oh yay unsolicited health advice
My levels are round 400 as of my last blood test, thanks though.
I’m gonna stop you right there at my injections - testosterone injections are not done into veins. They’re done intramuscularly (into a large muscle) or subcutaneously (into the layer of fat that sits under the skin). This is because injectable testosterone is oil based, because it is meant to absorb slowly through the week, similarly to how it’s produced.
Not to mention, my body also… does make testosterone. Like on its own. Not enough to masculinize me, but testosterone is a hormone that regulates things like ovarian function and bone density in afab folks. All this to say that my body knows what to do with it, and if my levels were too high, my dose would have been lessened when my blood was tested. In fact I seem to struggle to absorb it properly - I originally started on low-dose T and had to increase it because it barely raised my levels at all.
With that out of the way, I’ll address the rest;
That… doesn’t change the fact that while you personally may not have sweat much or had oily skin, a lot of my classmates the first time I had puberty did. And a lot of them were my friends, because I was the only person who didn’t treat them like dirty and gross for struggling to adapt to their bodies changing.
Going through puberty the first time for me meant almost no change in how much I sweat, stank, or how comfortable I was. A week out of the month I had to deal with smelling like blood and dealing with pads and being extremely uncomfortable - im not saying it was a breeze, but what I am saying is I didn’t have to worry about gym class leaving a smiley face in sweat on my shirt, or being unpresentable in general unless I was on my period. And even then - if someone called me on it I could always say I was on my period and people would fuck off about it. Besides that, I’m saying I didn’t have to change my hygiene as a teen whatsoever. No changes. No increase in showers. No extra deodorant.
What I experience now is similar to what I saw my friends experience, and what I saw them catch absolute hell for.
Something that I, as an adult, do have the tools and knowledge to handle. But as a child, I would have struggled immensely.
I said it before and I will say it again. Sweaty, stinky, disheveled teenage boys are learning entirely new routines in order to be presentable. They’re fucking kids, and I personally think if you make fun of kids for not being able to adjust to a change that is so huge, I think that’s pretty shitty tbh.
They deserve a break.
#the bell tolls for you#I’m not mad at you to be clear. i don’t know if this sounds mad#but I’m really not. i just firmly believe that picking on boys struggling with being presentable in public does a lot of uneccessary harm
33 notes
·
View notes
Text
Slime HRT - First Step (Part Two)
“…and this last drug is Vasopressin, which is a standard water retention drug. Usually patients are plagued by constant thirst on this regimen, so we’ve started to prescribe this to combat it.”
This owl sure knew his stuff.
The appointment had gone perfectly, all things considered. After securing a follow-up appointment for a month in the future, Elise was walking out of the clinic with a copy of her prescription. Some of these medicines were vaguely familiar – she’d heard of salicylic acid in a chemistry class – but some of these drugs were of a fantastical nature. Myochitinase, homolipastat? These weren’t real things. You couldn’t get slime estradiol at a pharmacy.
Though…was there much use in thoughts like those anymore? She was in a city that didn’t exist, drawn by a promise from a made up company, and had been prescribed four different make-believe drugs by a six-foot-four bird in a labcoat. Reality had been blurred in the past four-ish hours, so maybe it was time to accept what she had just been given.
Plus, it wasn’t as though this city was strictly human, either. Granted, that was a majority of the population, but there were others who didn’t fit the label, not by any sense. Dragons, centaurs, other creatures of myth, and just about any kind of animal in the kingdom. Even things outside of animals, evident by the occasional dryad(?) that happened to pass her by.
Though, in spite of it all, no slimes. They could’ve just been inside, it was something like 85 degrees even here in the city. Which begged the question: what was going to change as the changes began and progressed? She’d done her research, and had asked around for advice, but the unfortunate truth was that slimes were a bit rare in this world of exotic creatures and their transspecies equivalents.
Basically, fat chance that Elise would meet someone like herself.
Such thoughts were muted as the day went on. The pharmacy in the city had the set of drugs she was in search of, and was able to set up a delivery schedule for her refills. Her medicines all looked uncannily similar to her existing HRT, but Elise could not deny that something was different about the drugs themselves, and it was hard not to describe them as ‘slimy.’
‘Well,’ she thought later that night as she took her first dose, ‘here goes nothing.’
PART TWO PART TWO GET YOUR COPY NOW
So I didn't do as much writing as part 1 (damn you writers block ;~;) so instead!!! Information Pamphlet!!
Human Replacement Therapy for Transspecies Slimefolk
Drug #1 - Myochitinase: 1mL intramuscular injection once weekly
The primary drug in slime human replacement therapy. The drug chemically changes the present myocytes (muscle cells) into chitin. Effects include increased translucence and thinning of skin, decreased muscle mass to make way for gel matrix mass, and decreased resistance to illness due to increased permeablility of the skin.
Drug #2 - Homolipastat: 100mg gel capsules once daily
The auxiliary drug in slime HRT. Similar in concept to human feminising HRT drug spironolactone and its alternatives, where homolipastat is utilised in preventing the reproduction of present myocetes. Further decreases muscle mass during conversion of muscle to gel matrix.
Drug #3 - Salicylic Acid: 30g ointment tube once weekly
Non-specific drug used to assist in the breakdown of skin cells in preparation for conversion to surface membrane.
Drug #4 - Vasopressin: 1 μL subcutaneous injection once daily
Optional antidiuretic used for water retention during initial stages of transition.
Affirming Treatments for Transspecies Slimefolk
Slime Stem Cell Therapy - Advised after one year of medical transition
Regular series of stem cell injections promoting transformation of organs to a core. Treatment includes pain relief and at-home assistance is strongly recommended.
Pigment Alteration Therapy - Optional as medical transition progresses
Pigment drugs such as melanin or other compounds may be started to change the colour of the individual later on in transition.
I LOVE YOU ALL STAY SLIMY :3 :3 :3
Last || Next
#slime girl#slime hrt#animal hrt#transgender#my writing#my gender#my hyperfixations#I can't wait for elise to get some tangible results and reveal my plans for her >:3
29 notes
·
View notes
Text
cat health update, as positive an outcome as possible
so her kidney levels (BUN and creatinin) are off the chart they’re so bad, literally. her urine gravity is bad, which tracks with the above. her kidneys are also apparently very small. by the numbers I think she’s lost 90% of her kidney function.
but, her blood pressure is okay. her potassium is creeping toward too low but is still in range so far. her phosphorus is also okay. these are things to keep an eye on. she has no problem eating and in fact with the appetite stimulant she is on (bc eating is crucial and she’s lost 7lbs) I feel like all she does is eat. she’s even eating the renal food so far okay.
we took her to a new vet today that tried more soothing approaches. she hated every second of it but allowed them to do things including show us how to do subcutaneous fluids at home. we’ll see how that goes long term. I need to acquire a supplement for her and we also need to give her two pouches of what looks like straight up soup every day to improve her water intake.
we did drug her for this appt, the first time using something called bonqat. I can’t say how much it helped at the appt but boy was she like a fun drunk when we got home. Like heyyyy what’s in here!!!!! And trying to GO OUT THE FRONT DOOR which is insane. she has now progressed to sleepy drunk which includes walking across my keyboard, something she hasn’t done in nearly 14 years bc she’s usually picky about what she walks on. Not now.
upsettingly she only had a few bites of her soupy food mixture before rejoining me on the couch where she is now face down passed out.
I am glad we took her to a new vet bc they did everything in the room with us and will strive to do that where possible in the future. I do think that helped her a LOT bc she didn’t pee or poop herself which she has so far every time the old vet would take her in the back. this place took their time to be gentle with her and had ocean sounds and feliway soaked things, and they brought the blood pressure machine into the room and let me try to smoosh her head into my hand to distract her while the tech tried to get a cuff around her leg (which was quite close to her mouth, an understandable danger zone).
we’re at that point where we had several travel plans set up and now I don’t know if we can do any of them. how can I leave her? she’s going to need food constantly, and kidney disease can just swoop in and take a cat whenever, or she could live another few years. she’s going to need subq fluid injection/infusions twice a week. she needs two medicines smeared in her ears every day.
here is the cat face down passed out.

14 notes
·
View notes
Text
so idk if i mentioned it here, but my insurance stopped covering my xyosted, the subcutaneous testosterone i'm always raving about because it's so easy and pain-free to inject. it's over $400/month without insurance, even with goodrx.
however, my insurance WILL cover it with a PA, BUT i need to try and fail first on testosterone cypionate, which i did because of my low T levels, and then on enanthate, which i'm using right now.
we learned that i wasn't injecting the IM shots properly as i wasn't getting the needle all the way into the muscle, so the T wasn't going into the muscle. so i scheduled a nurse visit to show me how to do it right. well, i'm too fuckin scared to do it. i can't do it. 🤷 i've tried twice with the nurse helping, and she had to guide my hand and i can't do it on my own.
the second time, i pushed the plunger down and it took FOREVER to go in, and it bled a lot after i took the needle out. also, my thigh still hurts, and i did the shot yesterday. not the injection site, my whole thigh muscle.
so i messaged my doctor and i'm hoping that between the injection anxiety and the pain/bleeding, she'll think that's enough to consider this a "failure" so we can try the PA for xyosted again lmao.
keep ur fingers crossed for me y'all 🤞
7 notes
·
View notes
Text
gave dad his first injection. uh. hated that btw
he was fine but i suddenly realized i didn't really know what i was doing bc the instructions didn't help. it says "subcutaneous or intravenous" while im pretty sure the doctor said intramuscular?? It had a short needle so just. poked it in all the way?
it said "single dose" so i just injected all of it?? because nothing said not to??
mom says if it was more complicated they wouldn't let us just do it at home without better instructions but idk man
10 notes
·
View notes
Text
"Let me do this for you." (Solomon Injection Comfort)
Solomon offers to give you your HRT injections when you show a bit of hesitation. Just a bit of fluff for my trans readers. (It's gender neutral so this works for trans men, trans women, and nonbinary people) I hope you like it! 🩵🩷🤍🩷🩵
(Solomon x trans!MC) (intimate, but could be read as platonic) (SFW)
Word Count: +1,300
Solomon had been right alongside you at the Demon Lord’s Castle when you told Diavolo that you wanted access to hormonal medication in the Devildom. It went much easier than you hoped, but it was still a comfort to have him there. He even held your hand.
You expected his support to stop there, but it didn’t. Solomon waited outside of the office during your consultation with the human doctor Diavolo employed to ensure you and Solomon would have adequate healthcare. When you were cleared for your prescription, Solomon went with you to the pharmacy to pick up your medication and supplies.
The doctor had informed you that the needle for your intramuscular injection would be larger than for subcutaneous ones, but they wanted to start with IM and see how you reacted to it. They also warned that injections would take a bit longer – due to the consistency of the hormones. Unfortunately, they didn’t show you a sample of the needle they prescribed for you.
When you and Solomon got home from the pharmacy, you decided now was as good of a time as any for your first dose. You pulled out your supplies. The syringe needle was intimidating. Despite the doctor having told you how to give yourself the injection at the office, when you stared at the needle that was supposed to go into you – which was, luckily, slightly smaller than the needle used to draw out your medication – suddenly, everything left your mind. The color drained from your face.
“Are you okay?” Solomon asked.
“Yeah.” You tried to sound nonchalant, but you couldn’t cover up the nervousness.
Solomon crossed his arms and let out a soft sigh. He took the bottle from your hands and smiled at you sweetly. “Do you want to change into shorts or just take off your pants?”
You knew what he was suggesting, but the words still flustered you. Besides, it wasn’t every day that a cute sorcerer asked you to take off your pants. That kind of stuff shocks people.
You left him to change into a pair of shorts; maybe next time, if your comfort levels allowed it, you would take your pants off in front of him. You were home, after all.
When you returned, Solomon sat you down on the couch. All your supplies were laid out on the side table. Solomon excused himself to wash his hands. He came back with a Ruri-chan themed bandage. You couldn’t hold back a self-deprecating laugh. This was so embarrassing.
“Are you sure you want to do this for me? I can do it. I just want to double check that I’m doing it right first.” You pulled out your D.D.D. and started to unlock it, but Solomon put his hand over your thigh and squeezed slightly.
“I promise it’s alright. I can do this – I want to do this. The doctor gave me a pamphlet with all the instructions, and I watched multiple instructional videos from nurses, doctors, and people who inject hormones into themselves. Just trust me with this.”
And you did.
Even after weeks of injections, Solomon hadn’t let you down, yet. The only thing that had changed was that you decided it was more comfortable to take your injections in your room. So, every few days, Solomon sat you down in your bed and started the process. By now, you were getting used to it. Sure, the needle was still a little bit intimidating, but you were confident that you could do it yourself if you had to.
“Solomon,” you started as you sat on your bed in your underwear, “I can do it this time.”
“Please,” Solomon stroked your cheek gently, “let me do this for you.”
“But –” you called out to Solomon as he stepped into the bathroom attached to your room to wash his hands. The way he smiled at you when he returned dammed the protest up in your throat. You swallowed it back down. “Alright. Thank you.”
Solomon pulled the cap on the hormones off to the side and set it down. Then, he disinfected it with an alcohol wipe. As he waited for it to dry, Solomon attached the larger needle to the syringe and added some air. He pierced the vial, turned it upside down, injected the air into it, and drew in your exact dose. Something about how intensely he stared at the syringe reminded you of the concentration he held when he was studying or working on an experimental potion – grave and careful. His handsome face was calm as the medication slowly drained, and you couldn’t help but wonder why doing this was so important to him. When he hit the right dosage fill line, Solomon turned to face your gaze. In response to your prodding stare, he gave you an innocent grin that brought heat to your cheeks. Solomon, then, discarded the needle in your sharps bin and secured your injection needle.
By now, Solomon had memorized the area on your thigh that he needed to inject, but as he gently rubbed an alcohol wipe over the spot, you remembered the shyness you had felt the first few times. Solomon had asked you to put your hand at the top of your thigh before he placed his hand just above your knee – locating the middle third and then the outer half. His hands were so warm then.
With the alcohol fully dried, Solomon stretched your skin. He looked up at you and asked, “You know the drill, right?”
“Cough after the countdown,” you affirmed the process. You weren’t sure where Solomon had heard that trick, and it sounded kind of silly when he first asked you to cough, but for some reason, it didn’t really hurt when you tried it. You didn’t know why. Maybe it was just a good distraction or maybe it was a placebo. Either way, you kept with the process.
“Wonderful.” Solomon gave you an approving smile. “Now, 3, 2, 1.”
You coughed as he jabbed the needle straight down. Solomon aspirated the syringe to check for blood, but you were clear. Thank goodness. The only time that happened, Solomon had to get a new needle and you had to go through the process again in a different spot. Solomon slowly pushed the medication in before he pulled the needle out. A speck of blood pooled up at the injection sight, and he cleaned it for you.
“There we are,” Solomon added. He started to gently massage your thigh. Why was he so sweet to you during such mundane moments? Still massaging your leg, Solomon looked up at you and opened his mouth. There was some hesitation – as if he wasn’t sure if he should let the words out. Maybe he was too honest when it came to you because he gave them life. “I’m grateful that love is not some fleeting emotion that withers in your heart. Instead, like this, you inject it with an appropriate dose consistently. It’s coursing through you – a part of you, helping you become the person you are. I don’t want you to ever stop feeling cherished.”
“Solomon.” His name was the only thing that pushed through the initial shock.
“You know, the love you’ve given me has helped me become the person I am now. Let me return the favor.”
“Is that why you’ve been so insistent?”
“I guess so. I just want you to know that you’re loved and cared for every step of the way. It’s sort of intimate, too, isn’t it? I’m proud to be the one who can do this for you.” Solomon’s cheeks burned, and he averted his gaze to your bare thigh. He almost couldn’t believe that he was able to admit that.
“If you could cook without killing me, I would marry you right now,” you muttered to yourself.
“What was that?” Solomon looked up at you quizzically.
“Nothing. Love you. Appreciate you. Stay out of the kitchen, and I’ll love you even more.”
“I think you’d love me more if you’d let me cook for you – if it’s even possible to love me anymore than you do now, right?” Solomon chuckled.
No.
34 notes
·
View notes
Note
heya! baby-ish tgirl here. i've been on E since dec now (current regimen 6mg E sublingual/100mg spiro per day). anyway i have a nasty needle phobia but i also really kinda want to switch to injections and i think i might be stubborn enough to overcome it. what do you think? worth doing?
Well, I'm not an endocrinologist, and this is very much a conversation you should be having with one. With that caveat out of the way though I'd say it depends. First of all, if you're Estrogen levels and testosterone levels are in the ideal ranges and you're feeling good about the results you’ve been seeing thus far, I would say there's no real reason to make that change. If you’re levels are good and your mostly satisfied but just want to get a lil extra juice out of your regimen, you may want to consider just adding in Progesterone.
Many trans women swear by injectable but obviously there's nuances here. The old axiom "your mileage may vary" absolutely applies. The big advantage you have with injectable estrogen is that you bypass the stomach and the liver and thus you don't have to worry as much about how much estrogen is actually available for your body to use or your body's receptors' ability to bind to the estrogen. When I first started I took oral estrogen, but it was really challenging to get my T and E levels in the correct ranges (for context I had incredibly high levels of testosterone before HRT, even by cis male standards). After trying a few different dosages of Estradiol and Spiro (and eventually progesterone as well) and still not getting the levels right, I made the switch to injectable. Once I made the switch it felt like I was cooking with gas. So I very well may have been one of those people who wasn't effectively binding to the estrogen taken orally.
The main disadvantage to injectable estrogen is really just the needles if you’re someone who feels nervous about that. Now with injectable there’s two formats, intramuscular and subcutaneous. Both are equally effective, the only big difference between the two is that intramuscular comes with a slight risk of scarring. Both are pretty easy, and you’ll get the hang of it fairly quickly. As far as avoiding pain and scarification my main advice is: 1. don’t do your injections when you are tired, in a rush, inebriated, or under any other condition that might cause your hand to be less than steady and 2. Be swift with the needle.
Another big difference, that is neither better or worse just different, is that your hormone levels will fluctuate differently. When you take hormones orally, you get your initial E spike and it tapers off over the course of the day, which is why you generally take two doses per day. With injectable you get your initial estrogen spike after injecting, and it slowly tapers off over the course of the week until your next does (this is why it's recommended you get your bloodwork done halfway between doses). So if/when you make the switch, you may experience some mild mood swings (not everyone does though, I only experienced noticeable mode swings during the first 3 months of progesterone) and you may experience a few other signs of hormonal fluctuation such as mild non-inflammatory acne on the sides of your nose (if you experience this talk to your end, you may need the dosage adjusted and definitely re-evaluate your skin-care routine as you may need to start treating the nose with salicylic acid).
Now there are a few other delivery methods to consider, such as the Patch and the Pellet, but I don't know as much about them so I'm not as comfortable speaking on them.
I hope that info is helpful baby-girl! But definitely take all of that with a grain of salt and go talk to an actual endocrinologist!
Love,
🌷Mother Calamity🌷
7 notes
·
View notes
Text
FIRST T SHOT: COMPLETE✅✅✅‼️‼️‼️‼️‼️‼️
details under the cut!! :-)
oh GOD i am so happy. oh god. oh i am losing my mind. years of agony every waking moment is gonna be over soon enough. even though i won’t see changes for a while, i already feel better.
it came a day early and they accidentally sent me testosterone cypionate instead of enanthate which, longer half-life + 8 carbon fucks severely so i’m not complaining!!! i don’t think i’m allergic, i got a little itchy immediately after injecting but i think it was mostly nerves/putting on my pajamas that had dog hair on them (i’m allergic to my dog), and it went away. i also feel nauseous ~2 hours after injection but i don’t know if it’s an issue with the T or just nerves or something unrelated. i was scrolling on tiktok for a bit which always makes me feel super nauseous so maybe that’s why
this was really, really, really scary. i did it on call with one of my best friends in the world (also trans, on e) and she really helped me. she’s the only person in my life who knows i’m on t, major shoutout, cannot express how much i love her
it’s been 2.5 hours since injecting about 25mg. i fucked up and am not quite sure how much i actually got in there cause the t got all stuck in the syringe plunger??? but the second time it worked i think. may have been more or less then 25mg…but…about? oops!
it didn’t hurt at all the first time but i fucked up and had to start over. the second time hurt a little because i forgot to turn the needle’s long side closer to my body, also the adrenaline had calmed down a little so i felt it more!!! but it was all very lovely and chill. i do subcutaneous (subq) and the needle was tiiiiiny tiny tiny so it really was nothing
i generally just feel Weird. everything feels sharper, i’m very very aware of my body right now. i was in absolute fight or flight panic defense mode while doing the injection because it was 1. just kinda a scary thing! 2. scared someone in my house was gonna catch me (they didn’t, we are all good). so i don’t know if my current Weird feeling is from T or from coming down from my crazy defense mode.
it feels like yesterday it was early august and i first heard of diy, it feels like yesterday i was holding my breath wondering if this was something i could really do. it feels like yesterday i, a trans kid in the south with no resources and no trans community, all on my own besides for a few friends up north, tasted real, tangible hope for the first time. and now i’m here and i did it. i started hrt. i finally did it
it’s Weird but really nice. i looked in the mirror and i feel different, i feel like me but also like a different person and i think i really like it and only time will tell how this all goes!!! i thank god and the universe and whatever divine luck brought me here because oh lord i have been so lucky. i am so lucky and have been so protected. i am so immeasurably grateful
6 notes
·
View notes
Note
For the person scared of needles, if it’s a more minor fear, you absolutely can work yourself up to it. I was scared of them, too, but worked myself up to it with exposure. Needles feel like this Big Thing since most people don’t come into contact with them often. But I had to get my blood drawn a few times in one year for health reasons after I’d decided to start T and used it as a time to desensitize myself. When you pull all the mystique away, it’s just a little pinch and you’re ok. Injecting T hurts less than blood drawing imo, since there’s no one wiggling the needle around to switch vials. It’s also a smaller needle and pretty quick.
There’s subcutaneous (injecting into fat under skin) and intramuscular (injecting into muscle). Subcutaneous is what I do, it supposedly hurts less. All you need to do is pinch some skin on your stomach and push the needle all the way in. If you hold the needle still, it won’t hurt very much at all.
Testosterone also comes in a gel and a patch that do the same thing. You don’t have to stress yourself. I didn’t go that path because I didn’t want to worry about residue but it’s a real option.
.
17 notes
·
View notes
Text
I have a very rare disease, hooray! Under a cut in case I ramble, not for content warning. I won't be talking about anything explicit.
It's official: I have hypophosphatasia, which is a genetic mutation that causes a deficiency of alkaline phosphatase (ALP) which is used for building bones and metabolizing vitamin B6 into energy, among other things.
Ever since I started getting my lab results mailed to me as an adult, I've had low ALP. But most doctors either only know about the more severe infantile form of HPP, or they don't know about it at all. So it's understandable that they always wrote something like "Low ALP isn't a concern", because most doctors only look for high ALP (which indicates liver problems). I'm accustomed to doing research into medical things, but even I didn't have reason to suspect HPP because most of the information (at least in the past) focused on the severe form.
I didn't look hard enough. Childhood-onset HPP is a thing and it isn't fatal, just painful and annoying. And that's what I have. The signs were there as a kid: disliking standing, finding it easier to walk than stand, difficulty with stairs, "growing pains", less energy and muscle strength than my peers. But none severe enough to catch the attention of teachers or pediatricians. In the US you can only get treatment if symptoms presented before 18 (adult-onset is also a thing but the FDA doesn't care about those people*), so when I was gathering data for the endocrinologist I thought back to my childhood for anything out of the ordinary. One memory that stood out to the doctor and my case managers was the time my classmate broke his leg in fourth grade. He had crutches, and - as our rural school somehow managed to be fairly progressive and inclusive in 1993 - he chose to allow the rest of us to try them, so we could have empathy for him. When I tried them, I remember feeling relief. I though this was cool, there was less weight on my legs but I could still move! It did not occur to me that that isn't a normal thing for a ten-year-old to think. I think it was the pharmacy case manager that went "OH" at this memory.
So HPP is at least a major contributor to my ongoing struggles with chronic fatigue and weakness. It may not be the only one, but it needs to be treated even if only to protect my bones as I get older. ALP is needed to metabolize vitamin B6 as well as make bones though, and Strensiq (a lab-created form of ALP) is known to break down B6. It's so good at it in fact that you can't really get a B6 blood test to be accurate if you're on Strensiq, because the drug will keep eating the B6 in the vial! So we're hopeful that Strensiq will make me feel better, even though it's really made with people with soft bones in mind. The fact that I haven't broken a bone going up the stairs like many people do may make it difficult to get Medicare to approve the prescription. Thankfully, not only am I perfectly willing to fight about it, I have a team to fight alongside me. HPP is so rare that the manufacturer and pharmacy for Strensiq have enough resources to assign each patient case managers to assist with everything from insurance to learning about the drug and how to take it (it's a subcutaneous injection), and also there's Soft Bones, the largest patient advocacy group for HPP in the US. I've already touched base with them and they're standing ready to assist if needed.
Also Alexion sent me this frickin adorable kids' book with the information packet:
*Forgot the note I was going to add about this. The reason the FDA doesn't authorize Strensiq for adult-onset is probably because studies didn't show as dramatic an improvement for adults compared to kids. But I think that's stupid. For one thing the disease is rare so studies are always small and there aren't very many of them. For another, of course the improvement in kids is more dramatic, their disease is more severe. Japan is the only country that allows Strensiq for adult-onset, as far as I'm aware.
6 notes
·
View notes