#which i can understand; as someone who went through severe mental health crisis and depression while being the captain of a team sport
Text
An Autistic Analysis of Moon Knight (or, Why Having Good Autism Representation Is a Revolutionary Act)

Sooo I was rewatching Episodes 5 and 6 of Moon Knight as part of my analysis of the show from an autistic perspective. These episodes affected me profoundly in ways that I’m just starting to be able to process and articulate. The end of Episode 5 caused me to have an … existential crisis. But paired with Episode 6, it also helped me reframe my perception of myself as an autistic person. Basically, it caused me to have a paradigm shift. And I want to talk about that.
If you want to see my other autistic analyses of Moon Knight so far, you can read Part 1, Part 2, and Part 3.
PART 1: My Experiences with Autism-Specific Mental Health “Treatments”
So, Episode 5 is hard to watch. We all know this. I think everyone collectively wanted to send Marvel their therapy bills after it was over. What I’d like to talk about in this post is watching it from the perspective of someone who has intersected with autism-specific mental health treatment. Like many autistic people, I have had psychologists who attempted to reach into me and pull pieces of me out in some misguided attempt to make me “whole.”
I want to clarify that I am someone who has not had a particularly good experience within the mental health system. I know that there are some absolutely AMAZING therapists out there, and so I don’t want anyone to think that I’m knocking the profession. At all. Therapy is an essential resource. I know people whose lives have been saved because of therapy. I just happen to be someone who hasn’t really been helped by the “treatments” I have experienced.
I also feel that I need to disclose that I have generational trauma around psychological and psychiatric treatment — my mother went through periods of psychosis when she was young, and her experiences in 1970s psych wards were about as bad as you can imagine. I know little bits and pieces of what happened to her in those settings, and none of it was good. Luckily, her family doctor was able to keep her from being committed (her psychiatrist wanted to institutionalize her).
So, when I was growing up, I believed that I couldn’t tell anyone about my severe depression, my anxiety, or my periods of dissociation — all of which stemmed from my autistic neurology, as well as the unending daily torture of being bullied at school and neglected at home. I was terrified that I would be locked up if I let anyone know how bad it was inside my head.
When I did eventually seek out psychological treatment in my 20s, it didn’t resemble the psych wards of the 1970s, thank goodness, but it was insidious and destructive in its own way.
I’ve spoken before about getting my first set of diagnoses, which happened when I was in my late 20s. The psychologist who diagnosed me gave me a large packet with my autism diagnosis and a list of comorbid conditions. She then said, “Well, this gives us an idea of what’s been going on for you. Now you can look for some resources to help you.”
I decided to follow her advice and look for help, but I was still afraid to go to an actual talk therapist, because I believed that if I opened up too much about my internal experience, they would have me involuntarily committed. I now know that this would never have happened (unless they felt that I was a danger to myself or others), but it was a misperception that I had at the time.
So, instead of therapy, I started to look for autism-specific resources that could “fix” me. I want you to understand that at that point, deep down, I hated the fact that I was autistic. I also had a deep and entrenched sense of self-loathing for my masked self. I just wanted to be “normal” and to live a “normal” life. I wanted to be able to have regular friendships. I wanted to work a regular job. I just wanted to exist in society as a “regular” person.
Autism is characterized by extreme gifts, but also some pretty extreme “deficits” — at least, they are deficits when viewed in the context of modern neurotypical society.
The program that I found to “fix” me was called the Perspectives Program. It had been originally designed to “treat” schizophrenic people, but they were now revamping it to “treat” autistics. The name was based on an ableist (and false) idea that autistics and schizophrenics lack "theory of mind" (i.e., the ability to understand another person’s perspective). It was a well-funded research program that was part of a major university’s psychology department. It all was very “official.” They said that they could help me “manage” my autism. I signed up voluntarily.
In order to be part of the program, I had to have another psych eval, which was even more extensive (and uncomfortable) than my first one. After they confirmed my autism diagnosis, the head psych allowed me into the study.
At this time, there was a big push in the psychological and psychiatric communities to try to “cure” autistic people of their autism. What this meant in practice was attempting to somehow restructure our brains to “function” like neurotypical brains. That was the aim of the Perspectives Program. Every week, I would go in and do hours and hours of exercises that were supposedly designed to get rid of my autism.
This push to “cure” autism wasn’t just coming from the psychiatric community. Actual autistics were towing this neurotypical party line, as well. John Elder Robison (an autistic guy and the author of Look Me in the Eye) had very publicly tried to rid himself of his autism. Back then, he was working as a shill for Autism $peaks — he served on their board as the lone token autistic person. Through his connections with Autism $peaks in Massachusetts, he underwent an extremely experimental procedure called Transcranial Magnetic Stimulation. It uses powerful electromagnets to zap different parts of a person’s brain while they are still awake. This procedure left him with increased emotional lability (i.e., mood swings), but it definitely didn’t “cure” him of his autism. Still, the message that he sent to the autistic community was loud and clear: if you’re autistic, you should consider trying to cut the autism out of your brain.
Now, of course, it is not possible to “get rid” of autism. Autism is an epigenetic restructuring of the brain that is often first apparent by the age of 2 years old. Autistic brain wiring is extensive and life-long. There’s no way to “remove” it. Psychology, psychiatry, and other therapies can treat some of the comorbid conditions, like depression, anxiety, ADHD, and sensory processing issues, but there is no way to “treat” autism directly.
So, as much as the Perspectives Program would have liked to have “cured” me, what the program really did was teach me how to mask my autism even better than I had before. I had started developing my masked self when I was around eight years old (when shit really started going downhill), but it had always been a bit haphazard. The Perspectives Program taught me how to strengthen the mask so that it could hide me from sight.
I learned how to disguise my autistic traits from these psychologists, who chalked up my “progress” to the program “working.” Nope, I was still just as autistic; the only difference was that I was spending more and more spoons on hiding it.
So, why did I keep going back to the program? It wasn’t an inpatient program, so I could have found a way to leave. Psychological research programs are required to let you quit at any time. Honestly, I ask myself that a lot. I could have dropped out of the program. But back then, I was such a people-pleaser that I was afraid of the psychologists being upset at me. I also knew that they would have tried to talk me into finishing the program so that I wouldn’t mess up their data. I think I felt that it would have been worse to try to leave and then be coerced into staying. At least now, I could gaslight myself into thinking that I was contributing to “autism research.”
But there was another reason too. I had friends in the program, people that I cared about. There was one person in particular that I was very protective over. They were more “overtly” autistic than me, so they were always being singled out and picked on by the psychologists. Whenever the psychs started zeroing in on my friend, I would try to deflect their attention away from them. I was afraid of what would happen to my friend if I wasn’t there.
After a year, the program was done, and the psychologists gave us our final assessments. Based on my scores, my autism was declared to have been reduced. I was closer to being “normal.”
It took me a long time to process what happened to me. In a way, I’m still processing it. I know that the program dramatically increased the shame I felt about being autistic. It also increased the “mask” that I am, making it a stronger part of my being. The mask is me. But so is the autistic part. And the autistic part was suffering.
I remember talking to a psychologist around this time, someone who was a facilitator in one of the autism support groups that I attended (these support groups were led by neurotypicals and were very ableist). She asked me, “If Autism Speaks is able to find a cure, would you take it? Because I think that you’d really benefit from it. Just imagine how much you’d be able to accomplish if you didn’t have autism.”
I felt so sad when she said this. Because she thought that the only “real me” was the mask. She perceived my “autistic self” as an invader, something to be removed if possible. She didn’t know that I am both. I’ve been building my mask since I was a child (I wasn’t good at it back then, but I still tried), so if I somehow “removed” my autistic neurology, I would be half a person, maybe less.
Most of the psychologists that I’ve known view my autism like a tumor, something that in an ideal world could be “taken out.” For them, autism is a brain defect that prevents someone like me from being “normal.” If that part could just be excised, then I could be “happy.”
But for me, my autism is at the very core of who I am. Yes, there are “deficits,” but there are also tremendous strengths and gifts that I absolutely would not have if I weren’t autistic. My autism is my superpower. But we’ll get to that.
Okay, so now that I’ve given you some background on my autistic experience of psychological “treatment,” I want to return to Moon Knight.
PART 2: Steven’s “Death”
I want to emphasize that what I’m going to discuss next in relation to Episodes 5 and 6 is from the perspective of my autistic experience.
I’m not a system, and I don’t want what I’m about to write to overshadow the experiences that systems may have had while watching the following scenes. I know that the end of Episode 5 was painful for a lot of systems, but probably in a different way than it was for me.
I want to share my experience of Steven’s “death” from the vantage point of autism-related mental health “discourse.” As I’ve said, most of the interactions I’ve had with psychologists have been centered around “curing” or “removing” my autism. And so, this is the message that I believed the writers were giving at the end of Episode 5 when Steven fell into the Duat.
It was nearly 4:00 a.m. on a Wednesday morning (yes, I stayed up to watch every episode as soon as it dropped), and as Episode 5 ended, I began to have a mental health crisis.
Because, you see, Steven had been the more identifiably autistic alter in the system, the one that masked the least. Steven was just like me. Or rather, he was just like my fully embodied autistic self.
And now he was dead.
Now, I’m very familiar with Marvel. I know that unless a death is 150% confirmed, chances are, the character is coming back. The logical part of my brain told me that Steven would probably return. They wouldn’t feature Mr. Knight so heavily in the promo for the show and not have him fight in the final battle that had been teased.
But the part of me that had gone through decades of hating my autistic self, the part of me that had tried to cut out the autism from my brain (as if such a thing were possible) – I suddenly saw what I had been doing to myself.
It was captured in the stony expression on Steven’s face.
I had been trying to destroy a part of myself.
And I had allowed all those psychologists into my head. I had given them my permission to subject me to their treatments. And even though the treatments were unsuccessful at “curing” me of my autism, it didn’t diminish the fact that I had wanted them to work.
I might as well have thrown Steven into the Duat myself.
And I felt ashamed and guilty for what I had tried to do to myself.
And then I had a terrifying thought. What if the Moon Knight writers were taking the side of those psychologists? What if they were trying to say that it was “necessary” for Steven to “die” in order for Marc to be “balanced”?
Why did I think that? Because the hearts "balanced" as soon as Steven turned to stone. With a definitive clang, Marc’s and Steven’s hearts stopped moving. Taweret confirmed it. And a moment later, Marc found himself in the Field of Reeds.
I started sobbing. Were the writers parroting the same kind of “cure”-focused psychological discourse that I had experienced? Even though that’s not how any of this works! It certainly doesn’t work that way with DID. Alters can’t “die” like that. And it doesn’t work that way with autism. You can’t forcibly remove part of yourself like that. And from what I understand from systems who have undergone forced integration at the hands of psychiatrists, it is a harmful process and it doesn’t work.
So now, it was 5:00 in the morning. I had to be up in a few hours to start my editing work. But I had to know that Steven would be back. Because if he weren’t coming back, that meant that the writers were telling me that those psychologists were right: “If you are visibly autistic, you are expendable. Only those who mask shall find peace and happiness.”
I couldn’t bear the thought of this show that I had come to love so deeply telling me that Steven had to be sacrificed for Marc and Jake to survive.
Then I made the mistake of going online, desperately searching for Episode 6 spoilers. I looked for anything that indicated whether Mr. Knight would appear in the finale. No one on Reddit or Twitter had any information. But the ableist discourse online from uneducated singlets had already started to pour in.
These are what the most common opinions seemed to be.
TRIGGER WARNING for ableism, singlet asshattery, and just general bullshit:
“Steven was the one who was keeping Marc’s scales from balancing. That’s why he had to sacrifice himself.”
“Steven’s job was to protect Marc, and he died doing that.”
“Now that Steven is gone, Marc can begin to heal.”
“Steven was like Bing Bong. Marc didn’t need him anymore.”
At that point, I basically accepted that I wouldn’t get any work done on Wednesday. I was in full-on grieving mode.
I wasn’t just mourning the death of a character that I had come to love, I was mourning myself, because underneath all the masking I do, I am basically Steven. I have the same mannerisms, the same kinds of special interests, the same ways of infodumping, the same obsession with antiquity, the same compulsion to collect enough books to overflow my apartment, the same (charmingly!) foul mouth, the same drive to come up with idiosyncratic yet practical solutions to problems, the same literal thinking, the same obsessive need to learn languages, the same terrible driving skills (though I do have my license), the same answered rhetoricals in my speech, the same need to point out every animal that I see, the same kind of courage (being terrified of something but doing it anyway because it’s the right thing to do), the same social awkwardness, and the same desperate need to connect with people. Plus, when I was younger, I had a little goldfish with a stunted fin (I named him Cucchiaino, which means “teaspoon” in Italian). Dammit, Steven and I even have the same favorite French poet (Marceline Desbordes-Valmore).
And here I had been, trying to destroy that part of myself.
This is why GOOD REPRESENTATION MATTERS, folks.
Until I saw Oscar Isaac portray Steven on screen, I thought that all those qualities I possess made me weird, awkward, undesirable, and ultimately unlovable.
Because nearly every other intentional autistic portrayal that I’ve seen on screen is either pitiable, punchable, or pathological (think Rain Man, Sheldon Cooper, or Sam from Atypical). These characters are certainly not heroic. Or loveable.
And yet, here was Steven, on screen before me, and he was both loveable and heroic. And not only did I feel that way; practically the entire internet had fallen head over heels for him. Here was proof — if Steven is lovable, so am I. If Steven is worthy of love, so am I.
But now, he was gone. And I think I mentally went somewhere else for the next week. I have no memory of what happened for the next seven days. I have appointments, client calls, and work deadlines in my calendar that I must have kept, but I have no recollection of doing them.
The next thing that I solidly remember is telling myself that I really shouldn’t stay up to watch the finale, because I knew I couldn’t handle another tragedy happening at 3:40 in the morning. I tried to sleep, but I started to panic, and I knew that I had to watch the episode. Whether Steven lived or stayed dead, I had to find out.
I turned on the finale as soon as it dropped, and then several minutes in, Marc went back for Steven. I was pacing around my kitchen at the time, and I remember falling onto the floor. My cat was very worried about me, and he started licking my hand.
As I saw Steven frozen there, all alone in the Duat, I started to cry again. Because I knew that this was what I had been doing to myself. I had been trying to freeze the autistic part of me, the part of me that was like Steven. It was like when I was younger and I used to get ingrown nails. The doctor would freeze the nail first before cutting it out.
Then Marc gave his speech. The speech that ends in this line:
You are the only real superpower I’ve ever had.
That choice of the word "superpower" feels intentional here from a mental health standpoint. I believe that Oscar, Mohamed, and the writers were familiar with the kind of ableist discourse that my psychologists had used on me. And they were choosing to reject that discourse.
You see, that specific language is so important. Within the autistic community, as well as other neurodiverse communities, we often refer to our neurology as our superpower. I’d used this language, too, when talking with other autistics, but I’d never really believed it, not fully, because I still saw my autism as something that made me broken. But then Marc said it, and both he and Steven started coming back to life.
And I realized that, YES, this part of me that is like Steven, this un-masked autistic part of myself IS my superpower. Without qualification. Without the need to justify myself to anyone. And I started to thaw.
You see, I had already come to “accept” my autism years ago. But deep down, I had never reached the point where I could love myself BECAUSE I am autistic. It was an impasse, and I thought that “acceptance” was the best that I would ever experience.
But now, I saw Steven joyfully running with Marc, keeping his alter from stumbling, yelling “Hippo!” because (just like me) he needs to point out every animal he sees, and I realized, I love this character. And if I love this character, for all that he embodies, in all the ways that he is just like me, then I love myself too.
Moon Knight didn’t just help me embrace myself as autistic. It helped me celebrate myself as autistic. Because Moon Knight is, at its core, a celebration of a system, in which each alter has a different experience of autism.
And Steven, a canonical, intentional portrayal of an un-masked autistic person, is the hero of this show. And that is revolutionary.
Seeing Oscar Isaac talk about his love for Steven in every interview he gives about Moon Knight; seeing the internet fall in love with Steven and collectively mourn his “death” — because of this, for the first time in my life, I was able to see myself as an autistic person from an outside perspective that was loving and positive.
Watching Steven embody autistic experience so beautifully made me realize that I don’t have to mask so hard. I don’t have to hide who I am. I don’t have to constantly wear this costume of “performative normality.”
And yes, there will always be people like Donna that I work with — but fuck ‘em.
It is never worth compromising who I am to please other people for money, acceptance, or any other benefit that can be gotten.
The masking part of myself was designed around conformity, and so it has allowed me to blend in with neurotypical society. But in order to stay "safe," I bullied my autistic self into hiding. And then all the while, I profited off of my autistic strengths. I’ve held my autistic self captive, like an internal servant to do my work. I have masked as hard as I can to try and look “normal” to neurotypical eyes, and then when I get a work contract, I tell my autistic self, “Alright, nose to the grindstone, shoulder to the wheel.”
Because the "mask" of me can’t do this work. The mask of me can talk to neurotypicals, but it can’t do my editing and ghostwriting work. The autistic me is the one who writes books, which is what allows me to earn a living.
It’s time to be assertive and stand up for myself, just like Steven does. It’s time to allow myself to be. My autism is my superpower. Any accomplishments that I have made are BECAUSE of my autism, not in spite of it.
And maybe some of the neurotypicals that I work with will think that I'm weird and awkward, because I've definitely got some Donnas in my client base. One of my current business partners is a Donna. Who fucking cares. If they are really that put off by my autistic self, then I don't want to work with them. It's not worth the money if the money means that I have to deny the essence of who I am in order to earn it. If they can't see the amazingness of my autistic self, then they can piss off.
So Moon Knight really shifted my whole perspective on myself. I think I was already at a breaking point, but it was the catalyst I needed to get through that impasse. I’m in a very different place than I was just a couple of months ago.
So, I guess the ultimate lesson here is that representation matters. Good, positive autistic representation is vital. And it is revolutionary. Autistic people need to be able to see ourselves as heroes in our own narratives. No longer are we the pitiable, the punchable, or the pathological. We are courageous, we are heroic, and we are loveable.
If I’d had this show when I was younger, I think it would have helped me release that desperate need to “fix” myself. I know that I wouldn’t have let those psychologists get up into my head and try to rearrange me. Again, therapy in general is great, just not if the goal is to use shame to make you fundamentally change yourself. This show reminded me that I have many strengths and gifts. I’m going to focus on those now. And I’m going to stand up for myself as an autistic person in a neurotypical world. I now have a model of a heroic autistic self. I’ve got to protect that.
186 notes
·
View notes
Text

I don't understand you. I really don't. Why wouldn't you actively seek to make change after you scared your own friend out of a fandom they went into hoping to interact with you? I apologize, I don't know what they identify as so I'm using they. They were so excited and you posted an entire guilt-tripping essay about how no one interacts with you. You're still posting them. You've been posting them. That's why no one interacts with you. We don't want to interact with someone who's willing to emotionally manipulate like that. We just want to have fun. I'm sorry about your grandma, I really am. I hope you find peace and healing with time, but you've been doing this long before recently. We scrolled through your blog. We looked at the other ones to get an idea of how you rp. You've been through a lot. You have a lot of raw nerves. I don't think rping is a good space for you right now. I think you're hurting yourself and the people around you. That isn't fair to you. It isn't fair to them. I know this will upset you and I am sorry for that. I feel like someone needs to gently say something at this point after what happened with that nice Paimon rper. I hope they come back and I hope you do too some day when you're in a better place. Maybe we can be friends then. Maybe we can rp then.

Okay, so I do wanna address a few things. I'm not particularly upset, Im more taking this as you being upset you cannot rp with Vinny?
Vinny Uses he/they. (Below Vinny commentary)
he was recently hospitalized because he had a medical crisis that resulted in him coughing up blood. You can ask him at @reviviscencegruiform about it. I did talk to him in private about my feelings. I'll be honest, please do not tell me what's best for me. Vinny took a step back for a few reasons, we have already discussed. Vinny is like a grown-ass adult. Vinny is fine, he is my friend if I was to upset him in any way. Trust me he would tell me. Trust me He would.
I'm not entirely comfortable disclosing my mental health online but to be transparent, I'm just on an emotional rollercoaster. I think I'm doing fine, then I'm not! If you want a laundry list of what's wrong with me to have a better understanding of someone you've never talked to properly:
I am bipolar! Straight up, 99% of my problems rn. Especially since I am grieving! I have schizophrenia! I don't even know where to begin with that, so I won't. I am Autistic and have ADD/ADHD.
Also, a lot of my general discontent with 0 activity/interaction isn't like from anyone following me? 100% it's me projecting that I'm sad that my best friend jack isn't doing well, and we don't talk every day like we did. I'm sad! And so I turn to my like... coping mechanism which is btw usually RP! Lately, i have been feeling dissatisfied with it, not sure why but Im sure it has something to do with being severely depressed.
I do not appreciate you trying to "break it to me." If Vinny @hootfather/@rance-ed has an issue with me, he will tell me.
If you take someone going through an emotional crisis as emotional manipulation, I pity the people you are friends with. You are not seeing the background of what's happening in my life or with my friends. So what little trickles on my blog in this turbulent time in my life is currently just a fraction of what im dealing with.
I am currently not doing well, and I won't be for a long time, I don't know when things will settle for me, but if my friends ever get tired of dealing with the emotional chaos that comes from being friends with me, they will let me know.
I do not want you to interact with me, you are clearly putting yourself on a higher ground than me. I don't appreciate it. I appreciate people who are patient with me and the moments I am not well.


This isn't all of it a lot of this goes back to at least the first of this month?
Do not assume things about me. I am not doing well, usually, I'm like pretty okay? However life is falling apart around me, and the LITTLE control I have right now is my rp blogs.
If people do not want to interact with me because of my currently poor mental health. I understand, however, do not frame my instability AS anything other than just being that. Do not act like from a few cursory glances at my blogs that you know me.
Do not act like you know my friends and I's relationships based on a few interactions on the internet.
Also I don't want to be your friend, lmao! This was like kinda fucked up thing!
4 notes
·
View notes
Note
No offense bro, but why are you always so protective of Cloud? No disrespect to you or anything but I've heard quite a bit of different opinions and theories on Cloud myself and I do agree with the people who say that he takes Tifa for granted. Going through trauma in the past is not really an excuse for his behavior. He also does act like he's the only one who has suffered in his life. Do you have other reason to defend him other than the fact that you "relate" to him? Just wondering.
Sorry for the late reply, my life has basically left no room for hobbies these past months.
Your question is hard to reply to because I am not sure what you mean when you say I am protective of him.
I guess you mean I defend his actions? Specifically in ACC?
Firstly let me state that there is a difference between being a good character and being a nice character, there is also a difference between agreeing with someones actions, or just understanding them.
Personally, I never really liked Cloud, especially not when I was younger. A lot of my defense of Cloud doesn't come from me personally liking him, but from me thinking he's a good character. I also think Snape is a good character, but I don't like his actions, and I don't defend them, although I still understand them to a certain degree. I should also say that as I started to understand Clouds character more, I also started liking HIM a bit more, although I still don't like the things he did, and would very likely not be friends with him.
But I do understand why he did what he did and cannot be too critical of him because of that.
You've probably heard that before you judge someone, you should walk a mile in their shoes. That's great advice, if you want to judge someone, you should imagine what it would be like to be them, however, I've noticed that too often when people try to walk a mile in someone elses shoes, they refuse to take their own shoes off first.
They don't think "what would it be like to be him", they think "what would I do in that position". But Cloud is not you, and you cannot judge him by how you would act, you've not gone through the same things he has, your thought patterns aren't the same etc.
This matters because too often I see people judging Clouds actions in ACC, and establishing his motivations by saying things that boil down to "If I were in his position, I would only do those actions if I loved Aerith/didn't love Tifa/whatever". But they're not Cloud, and they're not understanding how Cloud thinks, and that it's different from how THEY think.
But like you said, I do see some recognizable elements of myself in Cloud, which is why I do understand his actions, and why I feel relatively certain in defending them, because I see them coming from a good place. It's common for me to react to things in a way that others find counter-intuitive. Let me give you an example, my brother once was mad at me because I had not told him my girlfriend of several years and I had broken up while I did tell a random stranger at the pub.
He said that he felt like he wasn't important to me if I told a random stranger but not him. The truth was the exact opposite, I love my brother, and could not bear to face him for some reason, as I told him: "if not caring enough was the problem, then I wouldn't have told a random stranger".
I see people exhibit that same lack of understanding when discussing Clouds actions, where they feel like his actions must be the sign of him just being a bad person, or not caring. But ask yourself what is more likely, that Square-enix wants their hero to be a bad person, or that you simply are misunderstanding the character?
I understand why people don't get Cloud, Cloud suffers from obvious mental health issues, and mental health issues simply are not something that the general public understands, even today. Not only that, but Cloud went through the most insane series of traumatic events anyone could ever imagine. He had an alien parasite in him, saw his entire town murdered before his eyes, then saw Zack murdered in front of his eyes, then saw Aerith murdered in front of his eyes, and just when he started living a peaceful life he is forced to watch his child succumb to sickness in front of his eyes, and then he finds he himself is dying. All this on the psyche of a man who had had a fear of failure ever since he was a child, spent most of his life essentially in war, and had a severe identity crisis as well.
Do you think you can honestly judge him by going "that's not what I would have done"? Would that not be incredibly
presumptuous?
Have you suffered from depression as a result of severe post-war PTSD and a lifelong feeling of inadequacy combined with a fear of failure and the belief that many of your loved ones died because you failed and were inadequate? Because that's the context in which you have to view Cloud when watching Advent Children.
Saying "Going through trauma in the past is not really an excuse for his behavior" is just incredibly short-sighted, your behavior is determined by who you are, and who you are is determined by what you go through in the past. You can't expect a broken child to become a well-adjusted adult when being a well-adjusted adult is the result of having a normal childhood.
I also don't want to cause offense, but this really is a mindset you should change, because this mindset is one of the most pervasive and damaging ones in our society, it's the one that probably bothers me most when I hear it because it makes zero sense. It's like breaking a robots self-repair unit, and then being angry at it on the grounds that the self-repair unit should have fixed it.
It's also very insensitive in general, it's the equivalent of saying "why are you depressed, just stop being depressed", people don't choose to be depressed, people don't choose to have a fear of failure. People don't choose their emotions, they're just there. They can be influenced by behavior over time, sure, but behavior is equally influenced by who you are and your emotions, which, as mentioned before, is determined for a large part by your past. People don't just "snap out of it". They fight and fight and fight, and sometimes they win and break out of the spiral, and sometimes they lose and it breaks them.
FFVII, and especially Advent children, is all about that struggle, and during those struggles you will have high-points, and low-points. FFVII shows all of those. It shows Cloud trying, it shows Cloud wanting, it shows Cloud failing, but it also, ultimately, shows Cloud prevailing.
Judging Cloud for not breaking out of the spiral by the time of Advent children, when he was mentally only barely 18 years old, and when he started at the worst place anyone could ever imagine, is just not reasonable. It's the modern day equivalent of "let them eat cake", something that can only be said from the place of privilege of not knowing what the struggles of the people you're critiquing are actually like.
So having that out of the way, lets look at Clouds actions from the perspective of Cloud.
Cloud is a young boy, and he's in love with the girl next door, he wants to get her to notice him. One day said girl walks up a mountain and he follows, she falls off a bridge and ends in a coma. Cloud followed her because he's in love with her, and he gets the blame from the adults. Cloud internalizes this, and its important to imagine what this must be like for a child, to have the adults all tell him it's his fault that the person he loves ended up hurt. "your fault", "your fault".
Afterwards Cloud starts thinking Tifa hates him and starts acting out. I think this is a good moment to point out btw that this child has no father figure. This is the start of his feelings of failure and inadequacy, he blames himself for not being able to protect Tifa, failure number 1, he thinks that if he were strong, he'd be able to protect her, he thinks that if he were like Sephiroth, then even Tifa would have to notice him.
Now until this time Cloud is not an asshole, he's a bit of a rebellious kid yes, but notice that he's not a bad kid as much as he's a kid who wants to protect someone, has no direction, and is acting out.
So Cloud thinks he's not good enough, but he leaves town confident that he'll become good enough, and even makes a promise to Tifa. All this follows logically from what we know about Cloud, and tells us a lot about how deeply seated these feelings are. Becoming Soldier wasn't a small thing, not some small passion project that he just came up with one day, it's the result of the things that happened in his childhood and he left everything behind make it so. He told the girl he loved, he promised, he boasted.
And then he failed. Failure number 2.
He comes back to Nibleheim and can't bear to look Tifa in the eye and admit that he couldn't do it, that he's a failure. His entire life so far has revolved around this and he wasn't good enough.
So here we have Cloud, not in a great mindset, thinking he's a failure, and what happens? His entire town is murdered by the person he admired, someone he worked with. His Mother is killed, and Tifa, the girl he PROMISED to protect, gets slashed open so badly that apparently she needed to have her ribcage reinforced with metal.
I think we can all agree that this by itself would be enough to potentially scar a person for life. (Cloud, not Tifa XD)
So what's next for the boy who left town in order to become a hero?
Well, he gets captured and experimented on for 4 years, during which his mind and sense of identity is bombarded with memories and knowledge of the lifestream in the form of mako, muddying up his thoughts. Cloud already had a weak sense of self as a result of his childhood, it's why he failed to enter Soldier and now this distaste for who he is makes him extra susceptible to Jenovas influence.
The next thing Cloud sees, (he didn't consciously experience the 4 years of mind-fuckery) is his best friend getting killed trying to protect him, because Cloud wasn't strong enough. Failure #3.
At this point, in Clouds mind the list of people dead because he could not protect them, because he's a failure, include his mother, his entire town, his best friend, and as far as he knows, the girl he loves. This is his life.
His mind is broken, he hates himself, he doesn't want to be himself,
he has a mind-altering parasite inside of him trying to adjust his identity and Clouds just goes "I reject this reality and constitute my own". And why wouldn't he? Why wouldn't he want to live in a fantasy world where he wasn't a failure, where he made it into soldier, where he was cool and successful and not a disappointing failure?
Zack tells him to be his living legacy and Cloud goes with it, then he runs into Tifa, Jenova adjusts Cloud further based on Tifas memories of them and rejoined with the girl for whom he joined Soldier Cloud is unconsciously all too willing to play the part.
FFVII starts and it doesn't take long for the cracks in his fake persona to show, he meets Aerith, and becomes her bodyguard. He gets to be the hero he always wanted to be. But then, even as "Cloud strife, soldier first class", Cloud is still a failure, the plate still drops, killing thousands, he gives Sephiroth the black materia, he beats up Aerith, and ultimately, fails to save her as well.
Tifa was the First Failure, and Aerith was the Final Failure.
Even as a soldier, Cloud still couldn't save anyone, he loses even more faith in himself, he doesn't know who he is, he doesn't trust himself, and then when he also loses Tifas trust in who he is, he just breaks and gives over to Jenova/Sephiroth. Even Hojo calls him a failure. Cloud feels like a nobody. Now mentally weakened, under the influence of jenova cells, he gives Sephiroth the black materia AGAIN, and meteor is summoned. Another entry on the long list of moments Cloud can look back on in shame later on in life.
He falls into the lifestream and again his psyche is under attack.
We know what happens afterwards, Tifa finds him, cares for him, and saves him through his feelings for her. Cloud realizes who he is, realizes he's weak, and goes after Sephiroth without lying to himself. In the end he defeats Sephiroth mentally and is supposedly rid of his direct influence.
But that doesn't mean that this mentally 17 year old is now fine, we should remember these events when analyzing ACC. Cloud has been in constant fighting/war/peril ever since he left home as a child, and is now a traumatized 17 year old in a 21 year olds body.
Novels and other materials give us an insight into how Cloud thinks during these times, and how he thinks about himself. We hear him say that he's going to live because that's the only way he can atone for his sins. He talks about wanting to change, and about believing he can change because he now has Tifa. He's a man (boy) who just exited war, and wants to be positive, but is still clearly blaming himself.
We see that this initially goes well, we are told that Cloud experiences peace and happiness that he's never experienced before. We're also told about the things that make it go badly, when he has to deliver flowers to the ancient city for instance. While Cloud regained the sense of who he was the belief that he wasn't good enough, that he was a failure, was never solved, if anything it was put on hold until he got his memories back, and now he is forced to deal with it.
While he is no longer directly manipulated by Sephiroth he's still suffering from PTSD and, most notably, survivors guilt. He blames himself for the deaths of Zack and Aerith in particular, and starts visiting the church. Now most people might think it's natural to avoid places that make you feel bad about yourself, but that's not how a depressed person thinks, Cloud thinks he deserves to feel badly he WANTS to punish himself, he WANTS to feel bad. He's ashamed of the moments where he's carefree and laughing with Tifa. Why should he get to be happy when Aerith and Zack are dead because of him? He shouldn't be happy, he should be in pain, he should remember them, not doing so would be an insult to their memories, he must never forget how he failed them!
That's how Cloud is thinking. We know of course that this is non-sense, Aerith and Zack wouldn't want this, if anything it's this mindset that is tarnishing the memories of Aerith and Zack, but that's not how a mentally unwell person thinks. Cloud wants to atone, and thinks he finds salvation in Denzel, whom he finds at Aeriths church. He thinks that by saving this life, he can, in some way, make up for all the death he caused. Tifa has a similar belief when she finds out Denzels parents died in the plate crash.
And when Denzel joins the family, and Cloud has path towards redemption in his mind, things start getting better again. Because this is the cause of the problems Cloud is having in ACC. When Nojima says:
first off, there’s the premise that things won’t go well between Tifa and Cloud, and that even without Geostigma or Sephiroth this might be the same
This is the conflict he's talking about, he's not saying "Tifa and Cloud are incompatible, it has nothing to do with Sephiroth", he's saying "if Sephiroth didn't show up during Advent children, Cloud and Tifa would still be having problems because Cloud is going through survivors guilt."
But the good times don't last, Denzel has Geostigma and Cloud cannot find a cure, Denzel....is going to die. Cloud, has failed again.
Not only that, but Cloud catches Geostigma....Cloud is going to die.
And THIS is why Cloud leaves in Advent children. And you have to look at this as Cloud. Cloud said he was going to live to atone for his sins, but instead he's going to die. He won't atone for his sins, even worse, he's going to leave Tifa and Marlene behind. He failed again. He couldn't protect Denzel, he potentially brought an infectious disease into their house as well. Literally all Cloud can think about is that literally everything he's ever tried has ended in failure, everyone he's ever tried to protect, he's failed at.
Do you understand how easy it would be for a person like this to fall into the trap of thinking "I deserve to die", "I don't want Tifa and Marlene to see me die", "Tifa and Marlene are better off without me anyway", "they'd be happier if I weren't here". Etc.
Now we know this is nonsense, but come on, how many instances have you heard of depressed people genuinely believing that their loved ones would be happier and better off if they just didn't exist?
However, throughout the movie, Zack, Tifa, and Aerith, all confront Cloud, and urge him to not give up. Cloud eventually does try again, and ultimately finds redemption not by being stuck in the past, but by letting the past rest and be beautiful (a lesson Cleriths unfortunately never learned).
"I never blamed you you know, not once"
"I want to be forgiven. By who?"
"Isn't it about time you did the forgiving?"
In the end, Cloud moves on, and therefore, so do Zack and Aerith. Aerith and Zack walk into the light, Cloud plants flowers on Zacks grave, and lets Zacks buster sword rest in Aeriths church, now no longer rusting, but shining. Instead of the past being a negative reminder, Cloud lets the past be beautiful.
Cloud was doing Aerith and Zack a disservice by remembering them the way he did, because it was ruining his life, it wasn't a good thing, but it did come from a good place, from a good man whose ashamed of not being good enough. Yes, it harmed Tifa, people going through these things often do hurt those around them, but it's not because they're bad people, or even weak, but because people are imperfect and Cloud has gone through hell, both internally, and externally.
Are his actions really that weird or deplorable?
"He didn't even go save the kids!"
Yes, he's hesitant about saving the kids, why shouldn't he be? Everyone Cloud tried to protect or save, ended up maimed or worse, or as Cloud puts it: "I can't even save myself".
"He left Tifa alone!"
Yes, he thinks he's going to waste away and die, can you blame him for not wanting to put Tifa through that and for thinking she'd be better off without him?
"He drinks!"
Wouldn't you?! Who wouldn't want to forget that stuff?
But in the end, He's only gone for about a week, he never intended to harm Tifa, he never physically harmed Tifa or cheated on her, his entire life revolved around wanting to be better for Tifa and blaming himself when he wasn't good enough, how is it reasonable to say this man takes Tifa for granted when the fact that he thinks he has to BE BETTER in order to be worthy of being with her has been a constant throughout his entire life and story? He DOESN'T take Tifa for granted, that's why he's beating himself up, that's why he leaves, not because he thinks he's better than her, or that he'll always have her, or that she'll follow him like a dog, or something like that. But because of the opposite, because he thinks HE is not good enough, that SHE would be better of without him.
Saying Cloud takes Tifa for granted, is honestly, simply, wrong. It's 180 degrees the opposite of what is happening in FFVII, the biggest constant in Clouds life, is that he doesn't take Tifa for granted, and I don't understand how anyone could argue otherwise.
103 notes
·
View notes
Link
Article from The Atlantic “This Is Not a Normal Mental Health Disaster” (posted July 7th, 2020). Excerpt:
In any case, the full extent of the fallout will not come into focus for some time. Psychological disorders can be slow to develop, and as a result, the Textbook of Disaster Psychiatry, which Morganstein helped write, warns that demand for mental-health care may spike even as a pandemic subsides. “If history is any indicator,” Morganstein says of COVID-19, “we should expect a significant tail of mental-health effects, and those could be extraordinary.” Taylor worries that the virus will cause significant upticks in obsessive-compulsive disorder, agoraphobia, and germaphobia, not to mention possible neuropsychiatric effects, such as chronic fatigue syndrome.
The coronavirus may also change the way we think about mental health more broadly. Perhaps, Schoch-Spana says, the prevalence of pandemic-related psychological conditions will have a destigmatizing effect. Or perhaps it will further ingrain that stigma: We’re all suffering, so can’t we all just get over it? Perhaps the current crisis will prompt a rethinking of the American mental-health-care system. Or perhaps it will simply decimate it.
Shared in entirety under the cut for those who can’t access it:
This Is Not a Normal Mental Health Disaster by Jacob Stern
If SARS is any lesson, the psychological effects of the novel coronavirus will long outlast the pandemic itself.
The SARS pandemic tore through Hong Kong like a summer thunderstorm. It arrived abruptly, hit hard, and then was gone. Just three months separated the first infection, in March 2003, from the last, in June.
But the suffering did not end when the case count hit zero. Over the next four years, scientists at the Chinese University of Hong Kong discovered something worrisome. More than 40 percent of SARS survivors had an active psychiatric illness, most commonly PTSD or depression. Some felt frequent psychosomatic pain. Others were obsessive-compulsive. The findings, the researchers said, were “alarming.”
The novel coronavirus’s devastating hopscotch across the United States has long surpassed the three-month mark, and by all indications, it will not end anytime soon. If SARS is any lesson, the secondary health effects will long outlast the pandemic itself.
Already, a third of Americans are feeling severe anxiety, according to Census Bureau data, and nearly a quarter show signs of depression. A recent poll by the Kaiser Family Foundation found that the pandemic had negatively affected the mental health of 56 percent of adults. In April, texts to a federal emergency mental-health line were up 1,000 percent from the year before. The situation is particularly dire for certain vulnerable groups—health-care workers, COVID-19 patients with severe cases, people who have lost loved ones—who face a significant risk of post-traumatic stress disorder. In overburdened intensive-care units, delirious patients are seeing chilling hallucinations. At least two overwhelmed emergency medical workers have taken their own life.
To some extent, this was to be expected. Depression, anxiety, PTSD, substance abuse, child abuse, and domestic violence almost always surge after natural disasters. And the coronavirus is every bit as much a disaster as any wildfire or flood. But it is also something unlike any wildfire or flood. “The sorts of mental-health challenges associated with COVID-19 are not necessarily the same as, say, generic stress management or the interventions from wildfires,” says Steven Taylor, a psychiatrist at the University of British Columbia and the author of The Psychology of Pandemics (published, fortuitously, in October 2019). “It’s very different in important ways.”
Most people are resilient after disasters, and only a small percentage develop chronic conditions. But in a nation of 328 million, small percentages become large numbers when translated into absolute terms. And in a nation where, even under ordinary circumstances, fewer than half of the millions of adults with a mental illness receive treatment, those large numbers are a serious problem. A wave of psychological stress unique in its nature and proportions is bearing down on an already-ramshackle American mental-health-care system, and at the moment, Taylor told me, “I don’t think we’re very well prepared at all.”
Most disasters affect cities or states, occasionally regions. Even after a catastrophic hurricane, for example, normalcy resumes a few hundred miles away. Not so in a pandemic, says Joe Ruzek, a longtime PTSD researcher at Stanford University and Palo Alto University: “In essence, there are no safe zones any more.”
As a result, Ruzek told me, certain key tenets of disaster response no longer hold up. People cannot congregate at a central location to get help. Psychological first-aid workers cannot seek out strangers on street corners. To be sure, telemedicine has its advantages—it eliminates the logistical and financial burdens of transportation, and some people simply find it more comfortable—but it complicates outreach and can pose problems for older people, who have borne the brunt of the coronavirus.
A pandemic, unlike an earthquake or a fire, is invisible, and that makes it all the more anxiety-inducing. “You can’t see it, you can’t taste it, you just don’t know,” says Charles Benight, a psychology professor at the University of Colorado at Colorado Springs who specializes in post-disaster recovery. “You look outside, and it seems fine.”
From spatial uncertainty comes temporal uncertainty. If we can’t know where we are safe, then we can’t know when we are safe. When a wildfire ends, the flames subside and the smoke clears. “You have an event, and then you have the rebuild process that’s really demarcated,” Benight told me. “It’s not like a hurricane goes on for a year.” But pandemics do not respect neat boundaries: They come in waves, ebbing and flowing, blurring crisis into recovery. One month, New York flares up and Arizona is calm. The next, the opposite.
That ambiguity could make it harder for people to be resilient. “It’s sort of like running down a field to score a goal, and every 10 yards they move the goal,” Benight said. “You don’t know what you’re targeting.” In this sense, Ruzek said, someone struggling with the psychological effects of the pandemic is less like a fire survivor than a domestic-violence victim still living with her abuser, or a traumatized soldier still deployed overseas. Mental-health professionals can’t reassure them that the danger has passed, because the danger has not passed. One can understand why, in a May survey by researchers at the University of Chicago, 42 percent of respondents reported feeling hopeless at least one day in the past week.
A good deal of this uncertainty was inevitable. Pandemics, after all, are confusing. But coordinated, cool-headed, honest messaging from government officials and public-health experts would have gone a long way toward allaying undue anxiety. The World Health Organization, for all the good it has done to contain the virus, has repeatedly bungled the communications side of the crisis. Last month, a WHO official claimed that asymptomatic spread of the virus is “very rare”—only to clarify the next day, after a barrage of criticism from outside public-health experts, that “we don’t actually have that answer yet.” In February, officials from the Centers for Disease Control and Prevention told Americans to prepare for “disruption to everyday life that may be severe,” then, just days later, said, “The American public needs to go on with their normal lives,” then went mostly dark for the next three months. Health experts are not without blame either: Their early advice about masks was “a case study in how not to communicate with the public,” wrote Zeynep Tufekci, an information-science professor at the University of North Carolina and an Atlantic contributing writer.
The White House, for its part, has repeatedly contradicted the states, the CDC, and itself. The president has used his platform to spread misinformation. In a moment when public health—which is to say, tens of thousands of lives—depends on national unity and clear messaging, the pandemic has become a new front in the partisan culture wars. Monica Schoch-Spana, a medical anthropologist at the Johns Hopkins Center for Health Security, told me that “political and social marginalization can exacerbate the psychological impacts of the pandemic.”
Schoch-Spana has previously written about the 1918 influenza pandemic. Lately, she says, people have been asking her how the coronavirus compares. She is always quick to point out a crucial difference: When the flu emerged in America at the end of a brutal winter, the nation was mobilized for war. Relative unity prevailed, and a spirit of collective self-sacrifice was in the air. At the time, the U.S. was reckoning with its enemies. Now we are reckoning with ourselves.
One thing that is certain about the current pandemic is that we are not doing enough to address its mental-health effects. Usually, says Joshua Morganstein, the chair of the American Psychiatric Association’s Committee on the Psychiatric Dimensions of Disaster, the damage a disaster does to mental health ends up costing more than the damage it does to physical health. Yet of the $2 trillion that Congress allocated for pandemic relief through the CARES Act, roughly one-50th of 1 percent—or $425 million—was earmarked for mental health. In April, more than a dozen mental-health organizations called on Congress to apportion $38.5 billion in emergency funding to protect the nation’s existing treatment infrastructure, plus an additional $10 billion for pandemic response.
Without broad, systematic studies to gauge the scope of the problem, though, it will be hard to determine with any precision either the appropriate amount of funding or where that funding is needed. Taylor told me that “governments are throwing money at this problem at the moment without really knowing how big a problem it will be.”
In addition to studies assessing the scope of the problem, which demographics most need help, and what kind of help they need, Ruzek told me researchers should assess how well intervention efforts are working. Even in ordinary times, he said, we don’t do enough of that. Such studies are especially important now because, until recently, disaster mental-health protocols for pandemics were an afterthought. By necessity, researchers are designing and implementing them all at once.
“Disaster mental-health workers have never been trained in anything about this,” Ruzek said. “They don’t know what to say.”
Even so, the basic principles will be the same. Disaster mental-health specialists often talk about the five core elements of intervention—calming, self-efficacy, connectedness, hope, and a sense of safety—and those apply now as much as ever. At an organizational level, the response will depend on extensive screening, which is to the mental-health side of the pandemic roughly what testing is to the physical-health side. In disaster situations—and especially in this one—the people in need of mental-health support vastly outnumber the people who can supply it. So disaster psychologists train armies of volunteers to provide basic support and identify people at greater risk of developing long-term problems.
“There are certain things that we can still put into place for people based on what we’ve learned about what’s helpful for PTSD and for depression and for anxiety, but we have to adjust it a bit,” says Patricia Watson, a psychologist at the National Center for PTSD. “This is a different dance than the dance that we’ve had for other types of disasters.”
Some states have moved quickly to learn the new steps. In Colorado, Benight is helping to train volunteer resilience coaches to support members of their community and, when necessary, refer them to formal crisis-counseling programs. His team has also worked with volunteers in 31 states, the United Kingdom, and Australia.
Colorado’s approach is not the sort of rigorously tested, evidence-based model to which Ruzek said disaster psychologists should aspire. Then again, “we’re sitting here with not a lot of options,” says Matthew Boden, a research scientist in the Veterans Health Administration’s mental-health and suicide-prevention unit. “Something is better than nothing.”
In any case, the full extent of the fallout will not come into focus for some time. Psychological disorders can be slow to develop, and as a result, the Textbook of Disaster Psychiatry, which Morganstein helped write, warns that demand for mental-health care may spike even as a pandemic subsides. “If history is any indicator,” Morganstein says of COVID-19, “we should expect a significant tail of mental-health effects, and those could be extraordinary.” Taylor worries that the virus will cause significant upticks in obsessive-compulsive disorder, agoraphobia, and germaphobia, not to mention possible neuropsychiatric effects, such as chronic fatigue syndrome.
The coronavirus may also change the way we think about mental health more broadly. Perhaps, Schoch-Spana says, the prevalence of pandemic-related psychological conditions will have a destigmatizing effect. Or perhaps it will further ingrain that stigma: We’re all suffering, so can’t we all just get over it? Perhaps the current crisis will prompt a rethinking of the American mental-health-care system. Or perhaps it will simply decimate it.
In 2013, reflecting on the tenth anniversary of the SARS pandemic, newspapers in Hong Kong described a city scarred by plague. When COVID-19 arrived there seven years later, they did so again. SARS had traumatized that city, but it had also prepared it. Face masks had become commonplace. People used tissues to press elevator buttons. Public spaces were sanitized and resanitized. In New York City, COVID-19 has killed more than 22,600 people; in Hong Kong, a metropolis of nearly the same size, it has killed seven. The city has learned from its scars.
America, too, will bear the scars of plague. Maybe next time, we will be the ones who have learned.
6 notes
·
View notes
Note
In short term 12, Grace shows Jaden her self-harm scars and discloses her past with abuse and self-harm. Is that something that happens and is okay (to share that kind of history with these kids) or is it another example of a lack of personal boundaries?
It’s… complicated, but I would say that the scene in the movie crosses the line into “poor boundaries” territory. That doesn’t mean that conversations like that don’t happen in these settings, it’s that that specific scene was not necessarily the preferred way to deal with that situation.
For those of you who haven’t seen the movie [spoiler and content warnings in effect] there is a scene where a deeply troubled girl has been placed in a sort of “cool down” room after a meltdown, and she begins attempting to self-harm by digging her thumbnails into the flesh of her hand. Her counselor, Grace - who has been struggling to connect with the hostile girl since she arrived - sees this as an opportunity to finally find some common ground with the girl, pulls up the leg of her pants to show her own self-harm scars, and discloses her own history of abuse.
Whenever a mental health worker tells a client personal information about themselves, we call it “self-disclosure”, and it’s not inherently a bad thing. Used properly, it can help you to establish trust and rapport with a client. When you work in mental health, clients will often assume that you can’t possibly understand where they are coming from, and that don’t have anything in common with them. This is especially true if you work with highly marginalized clients like the ones in the movie - they will often assume that your life is perfect and that you’ve never faced anything like the obstacles they have. Self-disclosing that you have had similar experiences can help you establish rapport and make the clients feel that you are talking to them as a peer who has been there, rather than a counselor talking down to them about things they’ve never experienced.
When it comes to self-harm, sometimes it can be better for a counselor who has visible scars to address that head-on, rather than trying to dodge the issue; many people who work in mental health have visible scars, and it can be an important opportunity to normalize having these scars and show that recovery is possible for people who have them. One of the best counselors I have ever known has a very obvious row of scars on his arm, and when kids asked him about it, he was honest about how he got them and what that recovery process was like for him, rather than trying to brush off the question. I certainly don’t think it’s inappropriate for mental health workers to have visible scars, or to answer honestly when asked how they got them.
When it comes to self-disclosure in general, though, there are a couple of big possible pitfalls, some of which Grace stumbles into in the movie. Self-disclosing to a client is always a risk, because:
It could make you look like an asshole. If you tell your counselor that you’re suicidal because your long-term partner just left you for the person they were cheating with and you think you lost the love of your life, and they respond with “yeah, I know how you feel, sometimes I feel like my husband doesn’t care about me because he never remembers to buy my favourite type of ice cream”, that’s not going to make you feel more connected to the counselor. It’s going to make you feel like the counselor is a self-centered asshole who isn’t taking you seriously and doesn’t understand what you’re going through at all. Self-disclosing when you don’t actually have any experiences that are similar to a client’s just makes you seem clueless and out-of-touch, especially if you have had a much more privileged upbringing than the client. New counselors make this mistake a lot. As someone from a relatively privileged upbringing, your parents’ divorce might genuinely be the worst thing that ever happened to you; trying to use it to connect with a kid who has been in neglectful and abusive foster care homes since age 2, however, just makes you sound like a rich jerk whining about having to have two Christmases.
It could be used against you. Counselors don’t always know their clients as well as they think they do. Sometimes, disclosing immensely personal information can be a mistake, because the client may share that information with other people, or try to use it as leverage against you. If you disclosed to a client that you were also a victim of sexual assault, they may cruelly throw that information in your face the next time they are upset with you, or they may share that information with your other clients without your consent. I currently work in a residential facility; anything that is told to one client usually spreads throughout the entire building, and staff are well aware that it’s only safe to disclose information that they are comfortable with every single client knowing. Even very casual information like “Oh, sorry I’m late, the 6 train was delayed today” can be dangerous - if you have a client who hates you (or likes you way, way too much), that’s information that they can use to track you down outside of work.
It can create an inappropriately personal relationship with the client. A counselor can have an amazing and close relationship with a client, but it’s important to remember that it’s still a client-counselor relationship. You are not friends, and in the case of teenage clients, you are not parent and child. If you’re going to be able to confide your darkest and most embarrassing secrets to a counselor and trust the advice they give you, there has to be a little bit of professional distance there. Otherwise, it’s impossible for the counselor to be impartial. A therapy session is a safe space for you to work through serious trauma and dysfunction, and learn healthier coping skills; it should not feel like a casual gossip session with your bestie. Therapists can definitely have a relaxed, fun, casual persona, but if the two of you are spending half your time together analyzing each other’s Tinder matches and swapping stories about drunk things you did in college, that’s a sign that professional boundaries are starting to break down. Counselors who over-disclose can cause their clients to start believing that the relationship is a genuine friendship, which sets the client up for shock and pain the first time the counselor tries to enforce boundaries. This is especially true of abused teens like the girl in the movie; they are often desperate for intimacy, and very quick to try to form inappropriately close or dependent relationships with their counselors.
It can make the counseling session all about you. Think about the last time you were having a mental health crisis - a panic attack, anxiety attack, depression wave, PTSD flashback, etc. In that moment, were you in a good place to listen to someone else’s darkest, most horrible experiences? Probably not. Self-disclosing your trauma or mental health issues - especially ones that are still ongoing - puts the client in a position where they suddenly have to comfort YOU, instead of the other way around. That’s not something that most people are prepared to take on when they are in the middle of a breakdown, and it can both damage the relationship between client and counselor, and leave the client feeling even more stressed-out than they were before. Many people who have experienced trauma need to be in a good headspace with advance notice to prepare themselves before they engage with potentially traumatic content - that’s why many people appreciate the inclusion of content warnings on media. For those people, having your mental health worker throw their own trauma in your lap when they are struggling to cope with their own is the stuff of nightmares.
That last one is the main error that Grace made in the movie, and it’s the biggest reason why I think this particular scene crossed boundaries. For one thing, she chose a pretty risky moment to have that kind of disclosure - not only was the girl in a bad place, she was actively self-harming. That girl was not in a place where she could even process her own emotions, and asking her to suddenly process someone else’s severe trauma - trauma that closely resembled her own - is too much. Perhaps when the girl was a little calmer, finding out that her counselor had been through similar experiences might have been helpful, but in the moment, it’s hard to see how that kind of disclosure would do anything but make the girl panic about the fact that she lives in a world rife with child abuse and self-harm. The description that Grace gives of the abuse she endured is quite explicit and quite graphic, and that girl already had enough horribly damaging images in her head at the time - it probably was not a good thing for Grace to add more. If anything, since Grace’s self-harm scars are much more prominent and numerous than the girl’s, the message that comes across is “I went through much worse than you did, why are you whining?”, even if that is not her intent.
Secondly, I think that Grace crossed the line because she was sharing abuse that she herself had neither worked through or resolved. The reason my counselor friend with the scars was helpful when he self-disclosed was because he was able to share a story of recovery - he would gloss over the bad things in his life that happened to cause the self-harm, and focused the narrative on the fact that he had successfully gotten help and that this kind of pain was no longer a part of his life. The message he was sending was “you can get better, and it’s possible to get to a place where you don’t feel the urge to do this anymore”. The trauma Grace is sharing, on the other hand, is unresolved. It is still very much affecting her life, and that is clear when she discusses it with the girl. Instead of presenting a message of hope or understanding, the narrative she inadvertently creates is “yeah, all this stuff is probably going to suck forever and you’re still going to be in pain as an adult”. It also really puts the teen in that counselling role - it’s clear that Grace is still very much in pain from her childhood experiences, and most people’s instinct would be to try to comfort her, which is the opposite of what should be happening here.
I do think that there are strong benefits to self-disclosure in mental health, but I don’t necessarily love how it was done here. This is reinforced by the fact that Grace later goes way too far in trying to personally take revenge on the girl’s father, something that points to some seriously blurry boundaries between the two women. In real life, that kind of breach of boundaries could get you fired and permanently barred from the profession, if not actually criminally charged if someone found out about it. A counselor who crosses boundaries like this is ultimately doing a disservice to their clients, and there are better ways to handle these kinds of situations.
5 notes
·
View notes
Text
“I existed in a world that never is – a prison of the mind.” (Gene Tierney)
As I am sure most of you are aware, the world is currently going through a health crisis regarding suicide and mental illness.
“The rate of suicide in the United States increased 28 percent from 1999 to 2016, according to a report last week from the Centers for Disease Control and Prevention.” [...] Suicide is the 10th leading cause of death in the United States. [x]
And that is just mentioning one country.
I wondered if I should approach such a delicate topic on my blog, and how. I decided though, that as someone who is mentally ill and has struggled with suicidal thoughts, I should have a word or two in the matter. For me, it is not only very important issue which concerns and saddens me deeply, but also a personal struggle.
I was diagnosed with depression (and later on, insomnia and generalized anxiety disorder) a few years ago at the tender age of 16. I’ve been in and out of therapy, and taking medication, ever since. I have struggled with self-harm, suicidal ideation, disordered eating, and (to a lesser extent) substance abuse. I saw, and still do, mental illness ruining what are supposed to be the happiest, most productive years of my life. April and May were particularly difficult months for me. If you struggle with depression and/or other disorder(s), you probably know it sort of comes in waves — you’re doing alright, going about your life, taking care of business. Sure there is a bit of struggle in living every single day, but overall you can manage it. It’s all right. Then something happens, or nothing happens, and it gets bad. And you find yourself going through one of those episodes. I swear... Feeling like you are actually losing your sanity is one very, very scary, and very, very real thing. If you have never experienced such a feeling, consider yourself one lucky human being. In early April I suffered a tragic family loss (which I briefly mentioned here on the blog) and obviously that didn’t help any. I went through one very difficult week, barely keeping myself together. It gets harder to eat, to sleep, to think, to shower, to not break down in tears several times during the day and (especially) during the night. I decided to drop out of college after only two months. I felt like my world was spiraling out of control. I eventually managed to get back on my feet — stumbling, but still. The calm before the storm.
On May 29, I suffered a nervous breakdown. I was taken to the hospital and checked into the psych ward as an emergency case because I was at the risk of committing suicide. I had said out loud: “I want to kill myself.” I talked to professionals (including my current therapist, who begged me to go to the hospital in the first place) and was given medication to reduce the physical symptoms — I was shaking and stuttering all over the place, literally falling apart. I spent about seven hours in the hospital, but felt safe enough to go back home with my family. Ever since that day, my family has been giving me a huge amount of support, even though they don’t quite understand why I am mentally ill. Well, I am none the wiser! But seeing the actual grief — and guilt and concern, too — in my parents’ faces was a life-changing thing, I can tell you that.
For what might have been the first time in my life, I actually realized that they care. That a lot of people care. From parents to distant relatives to online friends to complete strangers. They actually do. That was a mindblowing thing for me because, as it is known, depression and mental illness in general distorts your thoughts and doesn’t let you see things very clearly. Let me tell you, I am making this post because I care. I care about all the people committing suicide and I care about all the people thinking about it, all the people who are in unimaginable, debilitating pain, and are staying silent, making their plans to end it all. I care enough to open up about this to an online crowd of 40k+ people. And if one, or two, or ten of you are struggling right now, I want you to see this. And I want to tell you: get help.
Every person has a breaking point. Try as we might, it comes a time when we just can’t push any further. In my case, I could not go on feeling heavily depressed and suicidal, and just not say anything. Because I knew I was going to end my life if I didn’t say anything. That is not to say I am “cured”, mind you. I don’t think I will ever be. Every day is a battle. You ever heard the Fiona Apple song, “Every single night is a fight with my brain”? Yeah, that’s pretty much it. I actually had a nervous breakdown last night. But one thing has changed — I talk about it now. Obviously I don’t go out and say to every person I encounter: “Hey, I am suicidal!” But when I feel like I might break down and hurt myself, I turn to the person next to me — who is usually my mother — and say “I don’t feel so good. Actually, could you help me? Because I might die.”
It is one of the worst things in the world, hiding your feelings. Just pretending to be happy and that nothing is bothering you. And at one point, it becomes literally impossible to keep up the facade. It’s exhausting. Reading about the suicide increase rate all over the world, and seeing successful, billionaire people ending their own lives, and talking about it, and hearing from others, made me realize that I am not alone in this world of sorrow. You, who are reading this, are not alone. And I beg of you, if you are struggling, to get help. I know, from personal experience, how disappointing and unnerving the public health system can be. But even if you can’t get in touch with an actual professional, just talking about it with someone, anyone, is already a huge step. It could be a loved one, a relative, a friend, a complete stranger, me. My ask box and messaging system is always open for anyone who might want to say something to me. If you are struggling, I do not want you to go through this alone. You do not deserve to go through this alone. Mental illness and suicide are taboos in our society, and I know most of us feel like pariahs, but we don’t deserve to be. And if we talk about it, there are people — lots of people — who are willing to lend us a helping hand.
I know there are people who check and read this blog and the posts I make, so I felt like I could not stay silent about this subject. And as someone who is going through this and dealing with this pain right now at this very moment, I certainly don’t want any of you to feel like you are alone and uncared for, or that no one understands your pain. When I say “I understand what you’re feeling,” I literally do. I care about how you feel, I care about you living, and you can count on me.
#text post#mental health#tw: suicide#sorry about the huge wall of text and that is just like half of what's on my mind lol but i wanted to say something
48 notes
·
View notes
Text
maybe don’t read this if we’re close and you will worry about me. like, seriously. don’t. it will upset you. i promise that i will be okay, that i am okay right now. just some info i thought might be worth sharing about when you feel your worst, that might be helpful to others who are also struggling. but i imagine it will be very difficult to digest if you know me well.
so i broke down and contacted the suicide prevention hotline today. i was not on the brink of killing myself or anything, i was just stuck in the mindset of “why bother”. everything feels pointless so why bother? i don’t even like the things i say i like, i just do them to kill time. why bother? i am simply filling up space and time, for reasons i do not understand, and personally feel like an emotional drain on the people i love. why bother? would my sudden absence be upsetting to those same people? yes. but they are capable and would get over it. why delay what is inevitable, if my every errant thought is unhappy? so that’s where i was.
and i urge you to please seek help if you find yourself there. any kind of help. that’s why i went here.
they do have a web browser chat which is what i used. i am first off not great at articulating myself verbally, and i was sobbing so it wouldn’t have been great for me to try talking.
it took a long time to connect to someone, which could be bad for some, but it kept me hanging in there until someone finally connected. sort of in the sense of, okay just a couple more minutes and someone will be there to talk. okay, just a couple more minutes. and this went on for about 10 maybe 15 minutes with a little bar that updated telling me how many people were in line ahead of me.
once i was connected there was another queue to wait in for whatever reason. i imagined it sort of like a doctors office. where you wait in one room to get called in for your appointment, then you wait in another room for your doctor to actually show up. this took a little longer, i think. probably about 20 minutes. there were several occasions i thought about closing the window, or wondered if it was broken, but i didn’t and eventually someone messaged me.
at first it felt a little awkward and scripted. they asked why i was contacting them, and i said it was hard to summarize, and that generally speaking, it was depression. they told me i didn’t need to summarize and to just say whatever i was feeling. so i did. i don’t have a transcript of the conversation or i’d put it here, but more or less i explained that i feel empty. that i feel alone. that it feels like there is nothing ahead of me. i mentioned i had to go to work in a few hours at a job i hate.
he asked me where i worked. it felt irrelevant, but i answered. honestly don’t remember much of what he asked me after that for a bit, it all felt like it did’t matter, that he was just asking me things to keep me talking. which is a fine tactic, like i get it from a psychological standpoint. obviously this guy does not know me or what i know about mental health so he’s gotta just take a stab at it.
there was some delay in his responses, at which point i messaged a friend to more or less say what i was doing. said i wasn’t sure it would help. she urged me to message my regular therapist which i was hesitant about. if you have a regular therapist please don’t hesitate. if you don’t have one... well i don’t know if anyone will read this or not, but if you need help finding one, i would do anything i could to help. i kept talking to the hotline responder, he asked if i had anything positive in my life. at which point i struggled to think of anything in particular. i told him i’m not sure i enjoy the things that i say i do. that i feel like the friends i am closest to are exhausted by me and my inability to cope. that i went to college for seemingly no reason, and have been working at jobs i hate for the past 8 years, living paycheck to paycheck. that of my family the only one that i am really close to is my mother and that she tries but is not always... on the right track, when it comes to coping with mental illness. i told him i have pets and i love them, but there’s not a lot i can do with them.
he went through and framed everything i said in a more positive light. that i have friends who, despite my illness, are still my friends and care about me. that i succeeded in college, and that even though my degrees have not been useful yet, they’re proof of my success. stuff like that. it was nice, at least, to have someone outside my life make an effort to reframe some of the things that make me feel the worst.
my friend continued to urge me to text my therapist, and by that point i had calmed down a little to better consider it. i was, and still am a little bit, nervous she will have to have me committed. which sounds a lot worse than it is i’m sure. she is required to take action if she thinks i am a danger to myself. i don’t THINK i am. like, in this moment right now, i am not. but i can’t promise that in an hour or two things won’t be bad again. but i decided to text her. i told her it felt like i’d fallen down 15 flights of progress and didn’t know how to start climbing again. that i wished there was an elevator in my metaphor. she said she liked my metaphor and asked if i wanted to come see her tomorrow. so i made an early appt for tomorrow morning. i continued talking to the guy on the crisis line, told him i had contacted my therapist and he said that was a positive move towards recovery and he was glad. i contacted work, the two people there that i thought would understand my situation to any degree, to see if they could let me off work today.
by that point i was feeling a lot better just knowing i might not have to deal with work and that i had some place to be tomorrow.
anyway, all this to say. help IS available. and it can be awkward or weird. but stick it out. if you have a therapist, contact them. if you don’t, and you think you might benefit (which truly i think EVERYONE could benefit even if they’re not wallowing in negative feelings like me) please look for a directory near you. i promise it’s not as hard as it seems. and i don’t care if i don’t know you, if you’ve read this far and you want someone to help you, please feel free to contact me.
i don’t know if anyone will read this. but if it makes a difference to even one person i’m glad i wrote it.
#mental health#suicide tw#suicide HELP#idk how to tag this#mental health help#i just hope that if someone is sad and needs help they have the ability to find this post
1 note
·
View note
Text
Chloe's Petals for Hope, Pt. 2 - March 16th, 2021
Chloe’s Petals for Hope is a foundation to bring awareness to and normalize Mental Health issues. The foundation was started by Susan and Kent Rogers with daughters Courtney and Teagan along with support of family and friends after their daughter Chloe’ died by Suicide on June 16, 2020. Chloe was fun-loving and enjoyed life, however, she struggled with Mental Health issues including anxiety and depression.

This is our story:
Chloe was diagnosed with ADHD in the First grade. She began taking Adderall which managed her ADHD til her Freshman year in high school. She then wanted to stop taking her medication because she was very skinny and she said kids were making fun of her. We agreed she could stop taking the medication as long as her grades did not go down. She did well during high school and did not take ADHD meds again. She was concerned when she began college but again chose to not to take the meds. She struggled some with grades but worked really hard and was able to manage.
Then the end of Freshman year in college came and so began her real struggles. In January, she totaled her car in the dorm parking lot. She was so upset and distraught with herself. She then began serious negative self talk. She began a 3rd shift job at a nursing home and complained of being so tired, etc. When we talked about it, I told her it was probably her messed up sleep pattern working 3rd shift. Then she began having flu-like symptoms so went to the infirmary where she was diagnosed with Mononucleosis. It was hard for her to bounce back from these things happening within a short period of time.
She eventually began feeling better physically, but became so overburdened emotionally. She was constantly worried about student loans, money, grades, etc. She also felt like everyone wanted her to be a nurse because she enjoyed being a CNA and was really good with her patients. She did not want to be a nurse but was trying because she THOUGHT this is what others expected. In reality everyone else just wanted her to do what made her happy and she would enjoy doing everyday of her life. She finally realized that she was pursuing something she had no desire to continue with so she changed her major to Communications and Marketing.
She hid her worries and anxieties from most people. Only those who lived with her or spent days at a time with her truly knew her struggles. She wanted to be and do everything she thought was expected of her and do it while looking like she had it all together.
Her sophomore year of college was less hectic but she struggled with friendships, working and keeping her grades up. Her Junior year she transferred to UK and lived in Lexington. This year was easier but with its own challenges of a new school and becoming adapted to that environment. Then she transferred back to EKU and moved in with her cousin and stayed between there and home. She was working in Lexington at the time in retail and enjoyed this job and working with girls her age and a few older girls who became her “work moms”. In December of what was her 4th year, she moved home and commuted until she graduated as a 5th year Senior in May 2020. During this time she totaled another car on her way to school. When Kent got to the scene the officer told him she was pretty upset- Kent found her in a fetal position. She once again was so down on herself and didn’t know why she had to be so stupid. We repeatedly told her cars can be replaced, she can’t so it really was no big deal in the grand scheme of things. She was so worried about finding another car even though we were able to work out her using a family member's truck til she found something. It was just another stressor that she added to her list of faults.
In September 2019, her anxieties and depression were at an all time high and she was constantly moody and would say things like she didn’t want to be here and that she wanted to go HOME. She would say that she was a failure and that she wasn’t good enough for others. She didn’t feel like we loved her as much as we loved her sisters. She felt so inadequate. We tried talking with her and showing her ways that she was loved. We began asking her to please see a counselor. She had gone to the doctor for anxiety meds during the summer but did not like the way they made her feel so she stopped taking them. I kept pushing her to go to another doctor to try a different medication telling her medications work differently for different people. She agreed to try a different doctor, however this one was worse than before because the nurse practitioner told Chloe that all these things she was feeling were normal for young adults finding their way in the world. Chloe did not feel heard or taken seriously and refused to go anywhere else.
Then in October 2019, she came into our bedroom with Kent’s gun that she had taken at some point. We didn’t even know she knew where it was and had no idea she had gotten it. I believe she had tried to figure out how to load and shoot it but thankfully could not figure it out. That night we called the Sheriff’s office to come and talk with her. When they arrived Chloe was so mad at us for calling them, she had gotten a belt and wrapped around her neck yelling that we were trying to embarrass her. We tried calming her down and wanted her to understand how much we love her and want her to realize that getting help is okay. Thankfully, the officers on duty were very kind to her and one said that his daughter struggled also and saw a counselor. He even told Chloe that she may have to go through a few til she found one she liked.
After this, I tried to schedule counseling appointments with her because she wanted us to go together. However, when your child is an adult it is hard to schedule appointments for them. Chloe did schedule appointments with a counselor in Richmond and went several times. She also made an appointment with another nurse practitioner and began taking a new medication that she seemed to be okay with. This nurse practitioner told her they would keep trying til they found something that worked for her. She had also referred her to a specialist to check out her thyroid. Chloe did follow up on this and found that one of her numbers were low but not really what would cause her heightened anxiety. She had completed suicide before her follow up appointment.
I also made several appointments for us to go together for counseling but by the time the appointment date the crisis was over and she didn’t want to go. When she began to consider counseling her sophomore year of college she found many times she had to wait months and then she didn’t feel she needed it anymore. I feel like this is common for many with Mental Health issues, they make appointments when a crisis occurs but the wait time is weeks to months and by the time it comes around they don’t feel it is necessary anymore.
Then there was COVID-19! Her school shut down in person classes. Her work became more intense. Our spring break vacation got cancelled. Her birthday plans were cancelled. Her college graduation was cancelled. So many things she was excited about did not happen. Of course, we did celebrate her birthday with the usual homemade and decorated cake we made together since she was 3. We cooked her requested meal and played games. Then EKU decided to do an online graduation video to play on Graduation day. We celebrated at home with breakfast and champagne and tried to make it a big deal even though it was not what she had dreamed! So she did get some celebratory moments of these big achievements in life.
I thought she was happy and not struggling with everyday anxiety because we were home together and spending everyday she was off together watching tv, going through childhood memories in totes and closets as we cleaned out. I knew she still had school stress and was wanting to get her work done so she could be finished with this phase of life. She even won an award in the Communication Department for her last project.
Then June 16 came and she woke up in an ok mood I thought because we had been texting about her graduation party before she got out of bed and came downstairs. She was wanting to go to Simpsonville to the outlet mall and that was our plan for the day. Then she got upset about not having a pair of shorts and our day and lives changed forever.
She was excited to be graduating because she was planning to do an internship with the nursing home in which she was employed and working her way up in administration. She had a boyfriend and friends she loved spending time with as well as her family. She had places she wanted to visit and things she wanted to learn. She HAD PLANS!!!
In an instant she took away all those plans and dreams because she just couldn’t deal with the inner turmoil any longer. She made a decision to end her suffering but this decision left those that knew and loved her heartbroken and shattered.

Chloe’s Petals for Hope wants those suffering with Mental Health issues to realize you are not the only one. So many people need counselors and medication to cope and make it in this world of pressure and daily change. Please talk to someone, if not a professional remember Your friends and family love you and are willing to listen! Sometimes it is harder to talk with those closest to us so find a co-worker, an acquaintance, someone at church to talk with -- remember they will have a different perspective!!!
Most of all Remember this world will NEVER be the same WITHOUT YOU!
Susan Rogers, President for Chloe’s Petals for Hope Foundation
#children and family counseling associates inc#cafca#cafca inc#Chloe's Petals for Hope Foundation#Chloe's Petals for Hope#Susan Rogers#mental health#mental health resource#suicide awareness#mental health awareness#suicide prevention#march#march 16#2021
0 notes
Text
hello. welcome to my journey.
to give you a brief overview; I am a non-binary queer person with (currently) undiagnosed mental illness. I wanted to document my journey and find some communities who understand my struggles, and to have an anonymous place to vent.
current situation: I am in a mostly depressive episode. I say mostly because there are fleeting moments of okayness: where my partner has cheered me up, or someone makes me laugh. my moods are not fixed, though: they can change daily, or even through the course of a day. at present, I don’t have any highs, feelings of mania, or true happiness. it’s either an ocean of intense sadness, or a grey numbness: or both. I have had 2 serious instances of suicidality in the last week. I am prone to dipping very severely to feeling suicidal when I am upset, particularly if there’s an argument with someone I really love, but this has been more persistent. It wasn’t fleeting along with the situations, it was present and heavy and caused me to pour tablets into my hand and stare at them, or write my suicide notes and plan my wishes.
I was referred to secondary care after an initial assessment with the primary care mental health team, who deemed me slightly too complex for primary care. after an MDT meeting, I was contacted to be informed of my being placed on a waiting list for group DBT sessions; via online-video of course, because... well, COVID.
I have my assessment with secondary care in a fortnight.
after my first episode of severe suicidality this week, I contacted my GP to inform them that my depressive episode was worsening. the first offer was of medication and I am quick to hesitate; I have promazine (a low-dose anti-psychotic) on hand to take ad hoc, but due to my history with medications (which I will get to) I am very reluctant about them.
secondly, the GP offered to inform the mental health team to see if they could ‘speed up’ my assessment.
hours later, I was contacted by them. It was a brief conversation, basically telling me that my assessment cannot be brought forward, but that the team could be called any time and I could get a call back within a number of hours; or I could contact the crisis team, failing that. it was a comfort of sorts to know that there was someone there.
the next day of difficulty was 4 days later, with no particular trigger. the first was triggered by a heated argument with my partner; the second seemed to have no trigger. it was simply there. I felt incredibly sad and low for the entire day, having feelings of wanting to die or otherwise not be around. my partner’s family were due to come over, in part due to a sister needing some comfort in their own situation, and I hid in the bedroom for the entirety of the evening. crying regularly, and unable to concentrate on anything at all. I decided to contact the team, and I had a call back about 2 or so hours later. Bez and I talked for about 30 minutes, and he told me to buy a book: mindfulness for EUPD, and encouraged me to keep a gratefulness journal. he told me that the waiting list for DBT was 1-2 years, which both shocked me and left me in a bit of dismay. he did make me feel a little better, particularly around my guilt for needing my partner there when she needed to be elsewhere, and I wasn’t quite on the brink of suicidality anymore, but I still felt defeated, exhausted, and terribly sad. I took a promazine later in the evening at my partner’s encouragement, and I went to sleep a couple of hours later.
current symptoms: suicidal thoughts; feelings, loose plans, rapid mood changes, deep sadness, irritability, crying suddenly, quick to upset, low motivation, low concentration, isolation, lacking in logical thought, ‘black or white’ thinking, splitting, low opinion of self, critical of self and others, needing regular reassurance, mild paranoia, jealousy.
history: in brief;
- I had experienced panic attacks as a child which stemmed from my father driving very fast and unsafely on motorways. I experienced physical and mental abuse from my father and sexual abuse from my brother at around the ages of 8-10. my parents had been separated since I was 2. I lived with my mother, who I had a good relationship with, and my step-father, who I did not get on with and was quite strict.
- I was diagnosed with anxiety and depression at the age of 15 and was sent for counselling which I only attended briefly.
- I re-attended the GP later on in 2011, at 18. I was given citalopram to try and help my depressive/anxiety symptoms, which unfortunately didn’t help. I came off the medication a number of months later, shortly after my relationship had a breakdown. I self-referred to MIND for counselling and I engaged, but unfortunately my counsellor was very poor and kept cancelling our appointments, sometimes when I was literally on my way to an appointment with her.
- in early 2016, at age 23, I attended the GP again with high anxiety in the hope of trying something new. I was prescribed sertraline which only worsened my symptoms. I was unable to sleep, eat correctly, was self-harming in the form of cutting myself, and was feeling very low. I saw a private counsellor at my GP which helped somewhat in relation to my childhood trauma and having someone to ‘vent’ to.
- later on in 2016, I became very suicidal. my GP wondered if I might have bipolar disorder, and I was referred to the mental health team. after a number of A&E visits, discussions around admission, and a psychiatrist, my sertraline dose was increased. my mood changed very fast: I was high-energy, feeling paranoid, seeing things that were not there, had grand ideas, was engaging in risky behaviour, and felt urges to harm. I had never experienced this before and it was very new to me. during this time, I also spent a lot of money and engaged in drawing and painting, something I wasn’t normally interested in. I didn’t sleep a lot and I was unable to work. I was prescribed olanzapine to level my moods and the psychiatrist pondered the bipolar diagnosis alongside traits of eupd.
- I improved on olanzapine after a number of months, though it made me sleep too much to function. I ended up easing off it, and my psychiatrist discharged me without a firm diagnosis.
my current situation is the most severe in mental health issues since. I have had counselling privately online, and this helped some: I was active, eating well, and feeling okay. unfortunately, this didn’t last. I have very childish behaviours; screaming and sobbing when upset, irrational anger, fast and sudden mood changes, severe ‘splitting’ around myself and my partner especially; I react very strongly when voices are raised or if anything becomes remotely physical which I know is due to my childhood.
my gp, mental health team, and assessor all agree that I probably have eupd/bpd. unfortunately, of course, I need to see a psych to be *officially* diagnosed, which I suppose is my next movement.
if you read this far, well done...
& thank you for joining me in my journey.
0 notes
Note
I've been getting severe depression from knowing I can't come out because it's not safe and/or no one will accept me. Because of this I've been slacking off from school work (I do cyber schooling) and my mother just found out. She told me that if I don't make it all up in a day then I'll be punished but I can't just tell her that I'm depressed cause I'm basically forced to stay in the closet. Any ideas on how to cope?
hi love, here’s a link i found that could help you with ways to cope with depression due to being in the closet and not being able to come out. there’s also an ask I answered a few posts back with links to LGBTQ chat rooms/ forums that can help if you need people to talk to. another thing that can really help is The Trevor Project, which has a text and chat option and has trained professionals to help you out in a time of crisis. here’s both of the links:
https://everydayfeminism.com/2013/11/the-stress-of-being-in-closet/
https://www.thetrevorproject.org
as for the work that you have missed and need to make up, i know i say this a lot, but i went through exactly what you did last year and i struggled for a long time with depression. something that helped me was to make a to do list of all the assignments i had, and how long they would take me, and when i would do them and fitting them into my regular schedule.
i understand the way your chest feels tight with how anxious you are about that stuff. when you have a concrete list it helps unclench that fist a little bit.
divide all your tasks into tiny steps, and give yourself little rewards for accomplishing them. tell yourself you get a break after this question. move on to the next question and tell yourself you get a break after this question. keep doing that, and then eventually actually give yourself a break. take time during your break to do deep breathing, in fact, whenever you feel majorly depressed, listen to some music that makes you feel good and take deep breaths, and tell yourself everything is going to be ok. a grade doesn’t define you, sweetheart. you will overcome this obstacle in your life and every one after that.
practice trial and error with things that make you feel better. do you have a pet you can play with? a stuffed animal you can play with? a familiar book you can read? a significant other you can talk to or look at pictures of? anything that makes you happy, indulge in that when you reward yourself for getting your work done. make time to indulge yourself besides that too, because you’re going through a crucial time in your development as a human being and because you deserve it.
you’re going through a lot of shit and you’re so freaking strong for doing what you do every single day. don’t ever think your depression makes you weak or that it’s your fault. it’s not. it’s your situation and you can’t control that. figure out what you can’t control and learn to be okay with that, it does a lot of good, and helps you focus on the things you can control.
don’t underestimate the power of crying and a good nights sleep. if you overwork and over-stress yourself you WILL get less done. put on some calming instrumental music, take deep breaths, and take your assignments one manageable step at a time. pace yourself. you can do it.
in terms of telling your mother about your depression, it seems as though she’s not someone you really trust with that information. but remember that there’s a lot of reasons people can be depressed, and you don’t necessarily have to out yourself. you can say that your schoolwork is taking a huge toll on you, you can even make it really ambiguous and say that there are things going on in your social life that are causing you to spiral into depression. ask if you can see a therapist. if you can find the right person for you, i can’t even articulate how much good it can do you.
my therapist, Lori, got me through the most difficult time in my life. I saw her from the end of eighth grade to the end of sophomore year. those first two years of high school threw me for a god awful loop, my friend. i was depressed and anxious and suicidal and being harassed and bullied. sophomore year my parents got divorced, i went through five breakups, self harmed, and had constant panic attacks. i can say confidently that the only reason im still here is because of Lori and how she helped me. she was queer too, and i identified with her on that level even before i figured out i was gay. i remember our first meeting when we talked about BBC Sherlock and Dr. Who (i was a major geek then) and i fell in love with her. she moved away last year, but she left a lasting impression on my life and the way I cope and how i deal with shit. her voice is always in my head telling me everything’s ok when things get rough.
you deserve that kind of therapy too. this is a rough, awful time in your life, and the help of a professional therapist can do wonders. i promise. if there’s any way you can talk to your mother about it i think it’s extremely important to your mental health (always remember that your mental health matters just as much as physical).
if any other mods or any of our followers want to add on something i missed, please do. i love you, whoever you are, and i believe in you so much that you can do this. you can do it and you can finish your work and you can get better and someday you’ll be able to be safely out of the closet and you’ll be able to be open and happy and proud. childhood doesn’t last forever even if it seems like it does. hang in there my friend.
remember that all of us here love you and believe in you, and there are people who care and who will care about you in this world. hope this helped you in any infinitesimal way. -Mod Charlie
#answered#long post#homophobia tw#homophobic parents#depression //#depression tw#suicide //#tw suicude#transphobia tw#bullying tw#self harm tw#i overshared im sorrt
11 notes
·
View notes
Note
I have been diagnosed with bipolar type ll, gad, severe depression, insomnia, ptsd, and negative paranoid schizophrenia. I'm transgender and came out to my family and not a single person is really supportive. They are trying to convince me that it's my depression and anxiety and have also said they don't believe that I have bipolar type ll. They tried to kick me out and have given me a time limit to get out and my other family members all agree with what they are doing. Continued.... #kma
.... my only friends family wont let me stay with them for a bit either. And I'm trying really really hard to find a way to move out including trying to work a lot more but it's so expensive here and my surrounding areas. Im nearly 20 and after going to the doctor and getting put on T; my family refuses to let me transition and went as far as sneaking into my room and searching it to try to find the vial. Everythings become too much and Im getting to the point I just want to end it all. Idk #kma
Hi love,
I am sorry that you are having to deal with this array of mental health issues and that your family do not support or believe you, I can only imagine how hard this must be. I am so proud of you for reaching out for help though, that is a great step forwards and towards recovery
I do just need to start by saying, that if at any point you take any action to end your life, then please contact your local emergency services (e.g. 911) for immediate care. If you find yourself reaching a crisis point then please do your best to get yourself to a safe place and contact someone who can help to keep you safe and take you to hospital if necessary. You can also always contact a helpline or web counsellor for support. I think it might be a good idea for you to create a safety plan - this is a plan containing all of the things you can do whenever you feel yourself reaching a crisis point. For example, who you can call, grounding techniques and distractions that are effective for you. We have an outline for a plan on our printables page here. Something which you could incorporate into your plan, or make completely separate, is a list of your reasons to stay; this could be tiny things, all the way up to big reasons, but they all count towards why you deserve to stay and find happiness. Here is our list of reasons to stay, maybe somethings on here will give you some ideas. Whenever you feel like giving up, please try to remember the reasons that have made you stay for so long
Have you considered talking to your doctor about what is currently happening, and mentioning your thoughts of wanting to end everything? A doctor will be able to begin treatment with you, and refer you on for more specialist help - I think talk therapy may be a good options for you right now; a therapist can help you to understand your feelings and give you some great techniques to help you come with them. I know getting professional help can be really scary so here is our page about getting help, that should answer some of the concerns you may have.
I can imagine that you must feel quite alone and isolated right now, but please remember that you don’t have to do this alone and there are so many people out here who are happy to support you. Have you looked into any local or online support groups that you could maybe join/attend? I know there is a really large LGBTQ+ community on Tumblr, for example, and it is full of wonderful people who are ready to help and advise you - you may even find someone else who is going through the same things as you right now, and you can work together. When it comes to your housing situation, have you looked into any possible flat or house shares? Sharing a place with someone means that you can split the rent/costs so it would be cheaper for you to move out - is this something you could look into? Depending on where you live, your city may have some sort of organisation that helps trans youth who are facing homelessness. The Trevor Project also has some different resources that you might find useful. You can find their website here.
Again, I am so sorry that you are having to deal with all of this right now and that you are not being treated with the love and respect that you deserve - but I promise you, things will get better and you will be able to be the real you and be happy one day, and we’ll be here to support you every step of the way! Please don’t hesitate to get back in touch if there is anything else we can help you with.
Take care,
Rhiann xo
#kma#mha#advice#advice blog#mental health advice#mharhiann#transgender#unsupportive family#moving out#suicidal thoughts#suicide#lgbtq+#lgbtq+ community#getting help#transitioning#transgender issues
3 notes
·
View notes
Text
The Light Inside Me
I tried committing suicide.
And it all went dark.
I woke up in ICU with tubes all over my body. With an IV and tubes that went from the inside of my stomach through my nose.
It was bright, really bright. At first, I thought I was dead. But apparently, I was in a place where everyone was trying to avoid that.
After I blinked several times, I started to see my sister. She was holding my hand. I squeezed her hands as hard as if they were taking my blood for a test. She kept telling me that “everything is going to be okay”, but it felt like my world has fallen apart and I was hanging by a piece of thread.
I closed my eyes, and I took a breath. I was trying to remember what had happened, and why I was here - in this place. But my mind was as vague as myopia seeing the world without glasses. I still remembered having taken a handful of antidepressants, screams, emergency calls and panic attacks. And I remembered flashing lights shining at my eyes as I was lying in the back of a cab. I couldn't recall puking, but I saw stains on my shirt and it smelled like it.
After a few hours of intensive care trying to get the pills out of my digestive system, I was placed in a room filled with 15 other people - I still remember it clearly since I was placed in bed number 16. My dad came around 7 in the morning, 6 hours after the incident. His face was tired and pale, he had been working until midnight and fell asleep when my sister called him. Later on, my aunts came. They brought me so much food, of which I had no appetite to even take a bite.
As everyone was sitting around me, I heard doctors and patients talking about me. I was the youngest person in the room and probably the one without any ‘clinical disease’. Some of them were pitying me, some stared at me oddly - pondering on why I didn’t value life the way they fought for it. But I couldn’t explain why I did what I did because it would have been too complicated. I just closed my eyes and tried to fall asleep.
In my dream, the incident of the previous night was coming together like a puzzle. I saw myself, crying alone in my dark dorm room - holding a bunch of pills in my right palm as I tried to swallow them all at once. After I took them, I closed both ears with my palms and started to scream to god knows who. I was scared and terrified. Later, I was lying on the floor, calling my mother - telling her how much I love her while I was sobbing. And it all went dark.
I woke up in a room, this time all alone. Not with doctors, or nurses or 15 other patients. It was just me. I saw the clock, it said it’s 12:00 - I had been sleeping for 3 hours. I wiped the cold sweat from my forehead as I was thinking: Why?
It wasn’t my fault. It wasn’t anyone’s fault.
I was diagnosed with mental illness when I was 9 years old. The first diagnosis was ADHD. Around the tender age of 14, I was diagnosed with bipolar disorder. For those time period, I’ve been given therapies and medication - but most times I skipped them because I was afraid that my friends would find out that I am mentally ill.
The night I tried to commit suicide, I had been having a depression episode for more or less 4 straight days. I had been skipping my medicine since I was entering university at that time, and I didn’t know the impact it was having on me. I didn’t go out, nor tried to ask for help. I started to hear voices telling me that I am worthless and my life would be so much better if I’d end it. I was lacking support and interaction with other people - I surrendered myself to the voice.
It didn't take me long to understand why I did what I did. It was nobody’s fault. It was just a bad decision. And luckily, I survived.
If you’re currently on the Internet trying to browse “how to kill myself” or “how much antidepressants should I take to kill myself” - please, ask for help.
It is not worth it. You are beautiful inside and out and this world deserves an amazing person like you!
We all have our struggles, but I believe there are 101 ways to solve them - and trying to commit suicide is surely not one of them.
I was reckless for letting myself stay in the dark for too long. I never told anyone my problems, I was a self-restrained person who thought ‘things will be better if I acted happy’ - no. If you’re sad, then let it out - don’t let your feelings tie you down and make you lose your happiness.
There’s going to be someone out there to talk to. If you’re arguing with your family, there’s going to be a school friend, or college friend, or your pets or even things, for example, a diary.
Reach out for help if you ever feel depressed or sad. To anyone who’s reading this article, I would advise you saying “Hello, how are you?” to everyone you know, at least once a day. You might not know the impact of those words on someone else’s life. They might be going through a crisis and your simple act of sympathy might help.
I hope we can learn from my incident and lead a better life.
I am here with all of you, those who survived and those who didn’t. To those who ever thought of committing suicide, please reach out for help - in fact, I am here to help. Visit my blog to talk to me, or click this link to look for the international suicide hotline. I hope all goes well with you, don’t let the light inside you die.
This writing has appeared in Global Adolescent Health Conference in Ottawa, Canada. Click here to see more of my writings that have been featured by UNICEF’ Voice of Youth.
0 notes
Text
CHAPTER SEVEN : CONVERSION THERAPY

This one is going to be easy. This is an opinion piece. A inflammatory commentary of some monstrous practices. A pile of insults for a pile of shit : CONVERSATION THERAPY, the worst of humanity with genocides and Keeping Up with the Kardashians.
WHAT IS CONVERSATION THERAPY ?
“So-called Conversation Therapy is a range of dangerous and discredited practices that falsely claim to change a person’s sexual orientation or gender identity or expression” — Human Rights Campaign

I’ll let The Trevor Project explained it to you :
Conversion therapy, sometimes referred to as “reparative therapy,” is any of several dangerous and discredited practices aimed at changing an individual’s sexual orientation or gender identity. Conversion therapists use a variety of shaming, emotionally traumatic or physically painful stimuli to make their victims associate those stimuli with their LGBTQ identities. According to studies by the UCLA Williams Institute, more than 700,000 LGBTQ people have been subjected to the horrors of conversion therapy, and an estimated 80,000 LGBTQ youth will experience this unprofessional conduct in coming years, often at the insistence of well-intentioned but misinformed parents or caretakers.
A QUICK HISTORY OF CONVERSATION THERAPY
Early 20th Century. Sigmund Freud stated that homosexuality could sometimes be removed through hypnotic suggestion. In his paper “The Psychogenesis of a Case of Homosexuality in a Woman”, he wrote that changing homosexuality was difficult and possible only under unusually good conditions (fear of society’s disapproval was not considered one of those). Success meant making heterosexual feelings possible, not eliminating homosexual feelings.
Sure. Different time. Different ideas. Also, fuck you.
I will give points to Freud with his response to a letter from a mother whose son was gay :
“I gather from your letter that your son is a homosexual. … it is nothing to be ashamed of, no vice, no degradation; it cannot be classified as an illness; we consider it to be a variation of the sexual function, produced by a certain arrest of sexual development. … By asking me if I can help [your son], you mean, I suppose, if I can abolish homosexuality and make normal heterosexuality take its place. The answer is, in a general way we cannot promise to achieve it. In a certain number of cases we succeed in developing the blighted germs of heterosexual tendencies, which are present in every homosexual; in the majority of cases it is no more possible. It is a question of the quality and the age of the individual. The result of treatment cannot be predicted”.
When you think about it, the idea of curing homosexuality through therapy was kind of a step forward, as previous solutions were castration, frying one’s brain OR death.

One of the “great” minds behind modern conversation therapy was psychoanalytic theorist Edmund Bergler. His method could essentially be sum up to “BLAME THE VICTIM”. Bergler used confrontational therapy in which gay people were punished in order to make them aware of their masochism. He violated professional ethics to achieve this, breaking patient confidentiality in discussing the cases of patients with other patients, bullying them, calling them liars and telling them they were worthless. His studies and articles helped classify homosexuality as a mental disorder in 1952.
From this period until the Stonewall Riot in 1969, conversion therapy received approval from most of the psychiatric establishment in the United States.
AND THEN CAME THE MOVEMENT
After the Riots, conversion therapy came under increasing attack. In 1973, with pressure from numerous activists and newly formed LGBT groups, The American psychiatric Association removed homosexuality as a mental disorder. Then all were saved from trying to change and every Gay rights were approved by the government. Peace and harmony was finally here.
Oh, no. Wait.
AND THEN CAME THE CHRISTIANS

If the APA wasn’t going to treat homosexuals as mentally ill, the Religious Right would. Practicing aversion without any therapist licenses (which helps since they cannot be sued for malpractices), Gurus like Joseph Nicolosi and John Smid went on to create successful programs for years, persuading parents to involve their kids into weeks, months, years even, of costly and intense reconditionings.
Take for example Joseph Nicolosi. His website offers “psychological services to Men and Women whose Same-Sex attraction doesn’t define them”. He is described as a pioneer in the history of psychology, which he left as the profession was slowly abandoning the classic understanding of sexuality as being rooted in design and purpose (their words, not mine). He’s the author of masterpieces such as “Healing Homosexuality”, “A Parent’s Guide to Preventing Homosexuality” and “Shame and Attachment Loss : The Practical Work of Reparative Therapy”.
They don’t develop any specifics on how they reduce homosexual tendencies or how they cure the fags, but we can easily imagine.
YOU HAVE THE METHODS TO MAKE US STRAIGHT

The techniques that conversion therapy use are quite varied, but have one point that ties them all. They do not work.
Electroconvulsive Therapy (or Electroshock Therapy) : the art of sending electric charge into your brain, put together that the medical body before meds were like “hey! we’re here too!”. It was created in order to provide improvements in severe symptoms of mental health conditions such as depression, mania, catatonia, aggression and dementia. One that goes through ECT risks memory loss, physical side effects, medical complications, seizures, confusion.
Prayers : because God does not love you and you need to repent and be good. Be good. Be straight. Be what you were supposed to be.
Exorcism : when the prayers don’t work. in 2009 Manifested Glory Ministries came under fire for a youtube video showing a 16-year old being subjected to an exorcism to cure him of his homosexuality. Quote “Come on, you homosexual demon! You homosexual spirit ! We call you out right now ! Loose your grip, Lucifer” End quote.
Disconnection from exterior influences : That’s what happened to Mathew Shurka, who was forbidden from seeing his mother and sisters for over 3 years, to help him get rid of any “effeminate behavior”. He also went through extensive unlicensed therapy sessions and his father provided him with unprescribed viagra pills. Shurka is now a spokesman for the National Center for Lesbian Rights’s anti-conversion therapy campaign.
Aversive conditioning : the use of something unpleasant, or a punishment, to stop an unwanted behavior. For example, wire a homosexual to an electric machine, showing him porn and electrocuting him every time something sinful (aka gay porn) appears. You can also induce the patient with nausea or paralysis. Sometimes it’s not as drastic, with the use of elastic band to slap on you wrist.
Behavioral reconditioning : lessons about masculinity and femininity. Ways to improve posture, voice modification, walking patterns, etc.
The 12-step program : borrowed from the Alcoholics Anonymous program. As you try to manage your disease, you truly need to atone from your sins and ask for forgiveness.
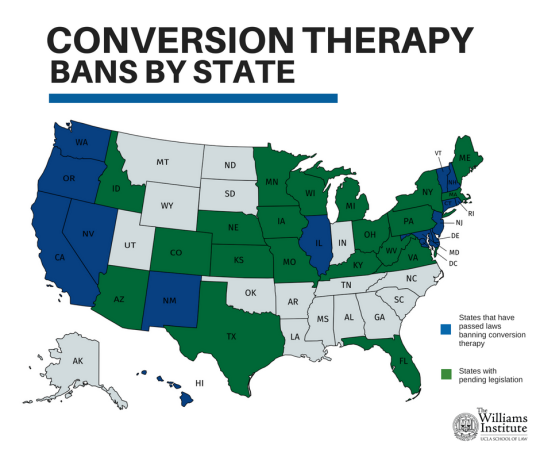
MEANWHILE IN FRANCE
As most of the rest of Europe, Conversation Therapy is not strictly banned by law. Malte was the first european country to outlaw CT, with a year in prison and a 10.000 euros fine. Worldwide, only Brazil, Canada and a couple of US states (including California) have laws to protect LGBT+ citizens from this mental genocide that is CT.
In France, though on the marginal side, there is a few groups that provide services to cure someone from the evil of gay life. The government, which doesn’t seem to really care that much about it, had a hard time evaluating how many of them exist. Gay activist and author Louis-George Tin gives an estimate number of five to six. He also warns that licensed therapists still try to heal homosexuality in secret sessions.

A first crisis of consciousness appeared in 2012 when an evangelical group called “Torrents de vie” offered services to reconnect with a saint heterosexuality, true femininity and true masculinity for the sweet deal of 410 euros. After the intervention of LGBT groups, the government started an investigation under the law that protects citizens against cults (as Conversation Therapy is a cult, don’t mistake it for anything else).
Since then, few cases went forward in the country but this year, Majority Deputy Laurence Vanceunebrock-Mailon announced her intentions to write an official text to outlaw groups that pretend to change sexual orientations from gay to straight. It is supposed to be available to the assembly before summer 2019.
A CURE FOR ILLNESS
Guys, I’m launching my own Conversion Therapy in a few weeks.

It’s called “Don’t give up, Sweet Bigot”. As a unlicensed medical expert in anything, I can only give what you can call “life advice” and offer “hang out” sessions to those who seek redemption from the path of bigotry.
You don’t like gay people ? You still they are sinful and worthy of burning in Hell ? The worst that society has to offer ? (thought we agreed the Kardashians were, but okay). This program is for YOU.
Come and join me (for the extraordinary start-up prize of my monthly rent) and I’ll will show you how to accept more people, all colors, sex, gender, choices, life goals.
Practices include midnight showings of my favorite gay porn on pornhub, going to ONE orgy (not multiple, I’m not that much of a party freak), having drinks by the Seine for our monthly Apero Queer, dancing time to the best of modern pop has to offer (see June 4th article, bigots), and off course, Electroconvulsive Therapy.
GO TO www.sweetbigot.org AND GET FREE GLITTER NOW !

You may not know what conversion therapy and it may not be as deadly as HIV or daily physical attacks on LGBT+ members around the world, but it kills. Those who went through that torture fest are eight times more likely to commit suicide in the years that follow. Garrard Conley wrote a wonderful memoir about his time at Love in Action. It was adapted in a very informative film also titled “Boy Erased”. There’s also “The Miseducation of Cameron Post”, check it out.

Don’t send your kids there. It’s not love to try and change someone. It’s abuse.
I’m gonna follow closely the events of this possible law against conversation therapy in France. We are painfully uninformed about what is going on around us.
Time to kick some Jesus Freaks’ butts.

0 notes
Photo

New Post has been published on https://fitnesshealthyoga.com/its-a-fentanyl-crisis-stupid-national-pain-report/
It’s a Fentanyl Crisis, Stupid! – National Pain Report
By Kaatje “Gotcha” van der Gaarden, PA-C, MPAS.
Editor’s Note: This story was originally published on Dec 17, 2018 on Medium Health.
Featured Image: TEDxABQ 2018 “A Working Parachute: spinal cord injuries, ketamine & comedy” which turned into a 9 min stand-up set! Photo credit Allen Winston Photography
In 2012, life was great: I proudly wore a white coat with a stethoscope around my neck and finally felt useful to humanity. Two decades earlier, as a stuntwoman, my parachute did not quite open, and I landed on my sacrum (tailbone) at 70 mph, crushing the sacral nerves. I had lost two inches of my spine, fractured several vertabrae, and would spend a year in ICU, hospitals, and a spinal cord clinic. I was left with traumatic cauda equina syndrome,¹ suffered from residual pain, and was left with a “sitting disability.” For my atrophied lower leg and foot muscles, I used leg braces, a cane or scooter and I sat on a padded office chair. I’ve schlepped pillows and camping mats with me ever since my skydiving accident. Frequently, lying down for a few minutes was the only way to deal with my disability.
Kaatje “Gotcha” van der Gaarden
As a Physician Assistant in primary care, I loved my job and providing a true provider-patient collaboration. I had ample opportunity to prescribe opioid medications. Responsibly, of course. In my toolbox, I had excellent interview skills, the State’s Prescription Monitoring Program (PMP), and a urine test. The PMP would let me know me if patients were doctor or pharmacy shopping, although it couldn’t take into account other states. A urinalysis would tell me if the patient was taking the opioids as prescribed, or diverting, or using other, illegal drugs, or medications that were not prescribed. Heck yeah, I even had my patients sign an Opioid Use Contract.
One patient’s husband worked for the Drug Enforcement Agency (DEA), and he told me one that opioids went for about 70 cents per milligram on the street, in 2012. However, I never assumed someone was gaming the system and tried to keep an open mind. Some patients did want me to refill their emergency room (ER) hydrocodone prescription, for complaints like a mildly strained knee. At that point, I would print out knee exercises instead. I always tried to understand my patients’ emotional and physical health and encouraged exercise and healthy habits (even if most days, I couldn’t prepare food so I ate LAY’S® Limón Potato Chips and gummi worms).
Another patient had just moved from Arizona, with a history of using 30 mg of MS-Contin, a long-acting morphine tablet, three times a day, plus another opioid, Percocet 10 mg instant relief (IR), one tablet every four to six hours for breakthrough pain. The patient was full-time employed, doing fairly intense labor, and was incensed when I wanted evidence of his “bad back.” The patient did not bring any records during his first visit, but he later returned with a lengthy health record — his pain deriving from five back surgeries, three of them revisions for the original surgeries.
I had never heard of “ultra-rapid” or “slow” opioid metabolizers² which affect adequate treatment, and still believed the Center for Disease Control (CDC) had society’s best interest at heart. The opioid crisis seemed far away, and I believed that did not affect my patients, or myself. Mistakenly, I thought there hardly would have been an “opioid epidemic” had medical providers only accompanied any opioid prescription with this warning: “Use your IR (instand relief) opioid medication when you truly have breakthrough pain, a 7–8 or higher, or it will no longer be as effective.”
Perhaps. But complicating matters was that opioid medications did seem to be prescribed for relatively mild to moderate pain, or in situations where acute pain would soon resolve. For example, to my patient with that strained knee, seen in a Colorado ER. In 1991, I’d fractured my lower leg above the ankle, after a car stunt gone awry, and wasn’t prescribed any opioid medication. The ER doc in Florida who applied the hot pink cast, from my toes to my knee, pointed me to a Walgreens to buy Tylenol (acetaminophen) for the simple, uncomplicated fracture.
Although I was in tremendous pain myself from the sky diving accident and crushed sacral nerves, I denied suffering from intractable pain. Yet I was battling worsening neuropathic (nerve) pain, as well as residual musculoskeletal pain from the sacral and vertebral fractures, on a daily basis. I made it through each workday by lying down on the exam table during lunch. Work gave me great happiness, but physically I had no energy left to cook, maintain friendships or even have a hobby.
That year I recall having to do five mandatory continuing medical education credits by the State on “responsible opioid prescribing.” This seemed ludicrous since I always looked at the PMP before going into the exam room. Especially with a patient that was on medications that fell under the Controlled Substances Act.³ As a non-contract employee, I also paid my own DEA license at $780 every three years for the privilege of writing controlled substance prescriptions. I was ticked off with the cost, but also with what I perceived as government encroachment on my medical decision making.
Sure enough, over the years, after the CDC Opioid Guidelines came out (which are voluntary, and not legally binding), I began to realize that there is no true opioid epidemic. There’s an epidemic alright, of people taking opioids with multiple medications and then adding alcohol and other illegal drugs on top. What we most certainly have is an alcohol epidemic, with 88,000 deaths⁴ annually, and this epidemic is starting to effect millennials. I blame those hipster beers with ridiculously high alcohol percentages, as millennials are dying of liver cirrhosis in record-breaking numbers.
Despite the ongoing alcohol epidemic, from 2012 to 2016, using opioid medication became synonymous with being a “drug seeker.” The “opioid crisis” narrative was perpetuated and fueled by mainstream media, whose culpability lies in using labels like “opioid overdose deaths” instead of the more appropriate “mixed drug intoxication.” True opioid deaths (opioid medications alone) range around five thousand deaths annually, according to Josh Bloom, writing for the American Council on Science and Health.⁵ New York City’s medical examiner’s office is unsurpassed when it comes to accurately determining cause of death: in 2016, 71 percent of all drug-related deaths involved heroin and/or fentanyl.⁶
Looking at the numbers, most of the so-called “opioid deaths” seemed to be people who did not take their medication as instructed, if opioids were legally prescribed in the first place. Seriously, because who cooks their Fentanyl patch and injects it? Not chronic pain patients, who need slowly titrated medication to bathe, cook, work, take care of kids, or go to school. Patients were indeed dying from respiratory depression, caused by taking legal or illegal opiates. But how many of those deaths are suicides? If patients with severe pain, on a stable regimen, are denied access, they may turn to suicide, or illegal opioids like heroin, now tainted by illegal fentanyl. That is not an opioid crisis, but another iatrogenic consequence of the “guidelines.” The Law of Unintended Consequences never fails.
How was it that the CDC took advice from an anti-opioid advocacy group, Physicians for Responsible Opioid Prescribing (PROP)⁸ in constructing the Opioid Guidelines? PROP had lobbied Federal officials and the FDA for years, to change opioid labels. When they were (mostly) rebutted, PROP got involved with the CDC, behind closed doors. The Washington Legal Foundation⁷ notified the CDC in 2015, as in their opinion, the CDC broke the 1972 Federal Advisory Committee Act (FACA) law. Washington Legal Foundation states that a Core Expert Group, advising the CDC, conducted their “research” and “Draft for Opioid Guidelines” in secret, without input from pain experts, pharmocologists, or patient groups.
Dr. Jane Ballantyne (current PROP President) was part of that Core Expert Group and is notorious for her anti-opioid stance. Another Core Expert Group member is PROP executive director, and founder, Dr. Andrew Kolodny, who refers to opiate medication as “heroin” pills and proclaimed that “oxycodone and heroin have indistinguishable effects.”⁹ Yet you oughtn’t compare a 5 mg tablet of oxycodone to IV heroin, without qualifiers on potency. Dr. Kolodny, an addiction expert, doesn’t even distinguish between “plain” heroin, and heroin cut with fentanyl, which is 100 times stronger than morphine. About 80 percent of fatal overdoses are now due to illegal fentanyl. By muddying the issues of opioid dependence, opioid addiction, and heroin use with either false or incomplete statements, PROP also does a disservice to people who are addicted to heroin or illegal fentanyl.
Research has found that 75% of heroin addicts have a mental health illness, and 50% have trauma from (sexual) abuse before age 16, something that gets drowned in Dr. Ballantyne’s simplified narrative of “continuous or increasing doses of opioids [… ] can worsen a person’s ability to function and his or her quality of life. It may also lead to opioid abuse, addiction, or even death.”¹⁰ Like many others, I argue that (illegal) fentanyl, and indirectly, profound loss of hope, is the main driver behind the current “mixed use overdose” deaths.
Dr. Kolodny was Chief Medical Officer of The Phoenix House, an addiction center, at the time he helped draft the CDC Guidelines. PROP also avoids mentioning the Millennium saliva,¹¹ or other DNA tests, to identify how individual patients metabolize opiate medication and that some are “ultrafast” metabolizers. PROP fails to mention opioid blood concentration measurements, no matter how imperfect.¹² However, no one doubts the conflict of interest: PROP Board members are involved with grants from the CDC, addiction centers, medical device companies to develop an opioid tapering mechanism, and even consulted with law firms investigating lawsuits against opiate pharmaceutical companies.
PROP was originally funded by Phoenix House, one of many addiction centers that prescribes buprenorphine. PROP is currently funded by the Steve Rummler HOPE Network,¹³ another anti-opioid group that lists Dr. Ballantyne and Dr. Kolodny on the medical advisory committee. Dr. Kolodny admitted in a 2013 New York Times article titled “Addiction Treatment with a Dark Side” that as a New York City Health official, he lobbied on behalf of the buprenorphine pharmaceutical industry. He was quoted as saying, “We had New York City staff out there acting like drug reps [with $10,000 incentives -KG].”¹⁴
Buprenorphine was the supposed miracle drug after methadone, but its known side effects include serious diversion, addiction, and possibly, lifelong treatment. Dr. Kolodny publicly promoted buprenorphine in various media outlets, despite evidence of buprenorphine overprescribing, pill mills, and overdoses. The true scale is not known, as most ERs and medical examiners do not test for the presence of buprenorphine. The CDC does not track buprenorphine deaths, despite a 2013 study¹⁵ that found a tenfold increase in buprenorphine-related ED visits, according to the Federally funded Substance Abuse and Mental Health Services Administration (SAMHSA). As “bupe” availability increased, so did diversion and overdose deaths.
Interestingly, that Dr. Kolodny promotes the idea that heroin and opioid medications are the same molecular compound. Actually, buprenorphine has a molecular profile¹⁶ that more closely resembles heroin, than hydrocodone. Dr. Kolodny indirectly claims that CDC “Guidelines” are effective, when the truth is that by the time PROP advised the CDC, prescriptions had already tapered off. This is evidenced in his statement as chief medical officer from a Phoenix House Q&A,¹⁷ dated December 2015: “It will take some time, but we’re already beginning to see a plateau in opioid prescribing.” Dr. Kolodny appears to take credit for a trend that had nothing to do with PROP, and he omits the fact that prescriptions are down since 2011, and yet overdoses are up.
Mainstream media occasionally, and accidentally, reveals the truth. CNN¹⁸ in 2018: “Fentanyl-related deaths double in six months; US government takes some action.” Then again, the echo of Dr. Kolodny’s statements, as reported by CNN: “The recent rise in popularity of these synthetics has been called the third wave of the opioid epidemic; the first wave was attributed to the overprescribing of painkillers like oxycodone and hydrocodone and the second to heroin. The drugs are all chemically similar and act on the same receptors in the brain.” Again, not one word about potency.
Few realize that when the CDC issued the Opioid Guidelines in 2016, there was inadequate research done ahead of time to determine the true cause of the rise in opioid-related deaths. There are no long-term studies on the effects of chronic opiate therapy. Very few, if any, pain management experts or pharmacologists were consulted to determine potential impacts on their practice. Neither veterans nor chronic pain patients were given a true opportunity to issue public comments to the CDC or any other Federal authority prior to the implementation of these new prescribing mandates. The CDC ended up targeting one of the most vulnerable groups, patients with intractable pain.
The CDC’s Guidelines also affect patients with cancer and patients who no longer receive cancer treatment because, unfortunately, both groups report similar pain levels. The guidelines allow the use of opioids during cancer treatment, but they are confusing when it comes to equally severe, post-cancer treatment pain. I fear this “opioid” crisis is far from over, and yet, trust me, this will go down as “reefer madness” in another hundred years. It is a manufactured tragedy that does real harm to patients with intractable pain. The “opioid” crisis also hurts human beings who suffer from heroin, opioids or other addictions by siphoning money, goodwill, and energy.
Few people realize that the CDC hired a PR agency to help sell the American people myths on the “opioid epidemic.” The agency, PRR, designed graphics to “educate” primary care providers that “one in four patients on opioids will develop addiction.” Even the National Institute of Health,¹⁹ another federal entity, estimates this to be 5 percent, not 25 percent. Another research team²⁰ concluded in Pain Medicine that opioid therapy for chronic pain patients (note: in absence of prior or current drug abuse) resulted in a 0.19 percent incidence of abuse.
The language used by the media as well as PROP contributes to misunderstanding; using words like addiction, tolerance, dependence, abuse or opioid use disorder as if they mean the same, directs the casual observer to bias. It’s clear that PROP never was an independent, neutral entity advising the CDC, yet they ended up dictating federal policy, based on flawed evidence. Dr. Ballantyne, Dr. Franklin, and Dr. Kolodny in Politico.com²¹ in March 2018: “We agree with Satel that the answer is not to force millions of chronic pain patients to rapidly taper off medications they are now dependent on (Italics mine). But then, neither is the answer to absolve overprescribing for pain.”
I’m not a linguist, but in that essay, PROP uses the word “addiction/addicted” 16 times, and “dependence” twice. The CDC could have ensured that patients with severe to intractable pain (no such distinction is made) would not lose access to their medications. And yet, that is exactly what happened. Stable patients on long-term opioids were tapered against their will, as the CDC “Guidelines” state it is undesirable to titrate above or equal to 90 morphine milligram equivalent²² daily (aka MME/day). But this was meant for opioid-naive patients, not those on long-term opiate therapy. Primary care providers, who were forced to follow these “Guidelines,” either stopped prescribing opioids altogether or forced patients to rapidly taper to below 90 MME.
Dr. Ballantyne is correct in her remarks that it isn’t realistic to expect zero pain levels, especially for acute pain that is expected to resolve quickly, like a sprain or an uncomplicated fracture. But people with severe to intractable pain are condemned to a world of suffering. Recall my patient with the five back surgeries? I wonder about him. He was working full time, on 180 MME a day, but in his mid-fifties, arthritis would worsen soon. My own story did not end well; I ended up with yet another spinal cord lesion, a benign hemangioma at chest level, which causes “central neuropathic pain syndrome.” My old cauda equina syndrome morphed into “severe, chronic adhesive arachnoiditis.” This is an incurable, intractable, progressive neuroinflammatory disorder whose pain is considered on par with having terminal cancer pain. Still, I try to make the best of it, see my essay, On Being Bedbound.
The CDC and PROP came for me: after using opioids exactly as prescribed, and less than 30 MME daily, my primary care clinic was forced to stop my opioid prescription, and that of all patients. I was not accepted in any pain management clinic, in an urban area of almost one million. Pain clinics here no longer provide “medical management,” yet perform epidural steroid injections ($3000 a pop), which may have contributed to, or worsened my adhesive arachnoiditis syndrome. I’m lucky to live in an urban area, where the academic hospital’s pain team took over my prescription.
But what about elderly and impoverished patients, or those in rural areas? PROP and the CDC claim primary care providers “overprescribe” and are responsible for most of the opioid prescriptions. But they fail to publicly acknowledge that pain management clinics no longer accept patients. This epidemic of undertreated patients will become known as one of the cruelest moves by a Federal agency on an already compromised population. I do feel for teenagers and adults who become addicted. Yet there ought to be a different, more sensible approach towards legitimate, chronic pain patients who need opioid medications, as well as people who develop a substance use disorder, who deserve our help and sympathy.
It is a conundrum of extraordinary proportions. At a time when managed care and Electronic Health Records dictate the length and quality of an office visit, there is less and less time to sit down and connect with a patient. Not just with chronic pain patients. Medicine and society would benefit greatly from the extra time clinicians deserve, to encourage exercise, eat healthier, lose weight, stop smoking and assess if a patient needs other support, like therapy.
In my opinion, it is loneliness, the feeling of not being connected to humanity in a meaningful way, combined with economic hardship, that leads to unhealthy lifestyle choices, as witnessed by the Rustbelt being hit hardest. Research shows that rats who were offered spring water or water laced with heroin, choose heroin. When those same rats were given ample toys, space, and other rats to play and have sex with, they did not choose the heroin laced water. That’s right, happy rats don’t need no heroin!
It cannot be denied that in previous decades, pain was both undertreated, and opioid medications prescribed for relatively minor, self-resolving aches and pains. Forget for a moment, the narrative that places blame on overprescribing, the opioid manufacturers, or the pharmaceutical distributors that, for example, flooded impoverished communities like those in West Virginia.²³ Forget all that, and focus on what is going on. Ultimately, patients with intractable pain pay the price of ignorance by scientists, journalists, politicians, and laypeople alike.
For this humanitarian crisis, there are no perfect answers. For example, as Red Lawhern, Ph.D. and prominent pain advocate²⁴ recently communicated with me (12/3/2018): “there is promise in genetic testing but hasn’t yet been fully reduced to routine practice and may not be covered by insurance.” Luckily my DNA testing was covered, on the condition it tested for depression. I also discovered that ketamine infusions help me most, but will leave that topic for my upcoming book, The Queen of Ketamine. Sadly, amidst the opioid paranoia, non-invasive alternatives like ketamine infusions aren’t mentioned for neuropathic or intractable backpain, which often has a neuropathic component. Research also shows that adding an anti-seizure medication to an opiate mediation provides better neuropathic pain contral, with less morphine²⁵.
In the end, I don’t think Tai Chi, Tylenol and Cognitive Behavioral Therapy is going to cut it for meningeal inflammation or other (neuropathic) pain syndromes. I believe the tide is turning. It will take time, and in that time, patients with intractable pain will choose to end their lives. But we are not alone, and it helps to know that courageous voices, notably the Alliance for Treatment of Intractable Pain, are speaking up for us. The print and online magazine Reason²⁶ has long been a voice of, well, reason. As Red Lawhern stated in a must-listen November 2018 radio interview,²⁷ “We must address underemployment, socioeconomic despair and hopelessness which are a vector for addiction. And end the War on Pain patients.”
Love, Kaatje
Kaatje Gotcha, model and stuntwoman-turned-Physician Assistant, found comedy, writing and advocacy after developing Adhesive Arachnoiditis. This spinal cord disease causes intractable neuropathic pain and leaves her mostly bedridden. Prior to that diagnosis, she’d survived a nighttime skydiving accident, landing at 70 mph. This caused Cauda Equina Syndrome; a subsequent lumbar puncture and epidural steroidal injections may have exacerbated her previous injuries.
Kaatje’s courageous spirit led to writing “The Queen of Ketamine,” available on Kindle in February. This is a comedic yet pragmatic memoir on adhesive arachnoiditis, the opioid “epidemic,” neuropathic pain, dating with a disability, while offering hope and practical advice. Kaatje’s 2018 TEDx talk and book publication will be posted on her Facebook page, at www.kaatjegotcha.com and Instagram @kaatjegotchacomedy. Find her essays on Medium, and follow her on twitter.
Cauda Equina Syndrome https://emedicine.medscape.com/article/1148690-overview
Opioid Metabolism https://www.medscape.com/viewarticle/771480
Controlled Substance Act https://www.dea.gov/controlled-substances-act
Alcohol Epidemic https://www.niaaa.nih.gov/alcohol-health/overview-alcohol-consumption/alcohol-facts-and-statistics
Opioid Epidemic Deception https://www.acsh.org/news/2017/10/12/opioid-epidemic-6-charts-designed-deceive-you-11935
Overdose Deaths by Heroin/Fentanyl 71percent https://www1.nyc.gov/assets/doh/downloads/pdf/epi/databrief89.pdf
Washington Legal Foundation and PROP https://www.forbes.com/sites/wlf/2015/12/15/cdc-bows-to-demands-for-transparency-and-public-input-on-draft-opioid-prescribing-guidelines/#c82eda135bc3
Physicians for Responsible Opioid Prescribing http://www.supportprop.org/
Dr Kolodny refers to “Heroin” Pills https://www.healthline.com/health-news/secondary-drug-industry-booming-amid-opioid-epidemic#2
Dr Ballantyne’s Narrative https://www.statnews.com/2015/11/30/chronic-pain-intensity-scale/
Millennium Opioid Metabolite DNA Test https://www.millenniumhealth.com/services/test-offerings/
Opioid Serum Measurements http://paindr.com/serum-opioid-monitoring-wheres-the-evidence/
Medical Advisory Committee https://steverummlerhopenetwork.org/our-team/
NYT: Addiction Treatment with a Dark Side https://www.nytimes.com/2013/11/17/health/in-demand-in-clinics-and-on-the-street-bupe-can-be-savior-or-menace.html
Sharp Rise in Buprenorphine ER Visits https://www.samhsa.gov/data/sites/default/files/DAWN106/DAWN106/sr106-buprenorphine.htm
Heroin and Buprenorphine Molecular Profile http://paindr.com/heroin-hydrocodone-buprenorphine-prop-aganda/#comment-334500]
Q&A with Dr. Kolodny, Phoenix House https://www.kolmac.com/2015/12/qa-dr-andrew-kolodny-chief-medical-officer-phoenix-house/
Fentanyl, as Reported by CNN https://www.cnn.com/2018/07/12/health/fentanyl-opioid-deaths/index.html
NIH Estimates Pain Patient “Addiction” 5 Percent https://medlineplus.gov/magazine/issues/spring11/articles/spring11pg9.html
Pain Patient “Opioid Use Disorder” without Risk Factors 0.19 percent https://academic.oup.com/painmedicine/article/9/4/444/1824073
Rebuttal by Dr. Kolodny and Dr. Ballantyne https://www.politico.com/magazine/story/2018/03/13/opioid-overprescribing-is-not-a-myth-217338
Morphine Equivalent Dosing https://www.wolterskluwercdi.com/sites/default/files/documents/ebooks/morphine-equivalent-dosing-ebook.pdf?v3
https://www.wvgazettemail.com/news/cops_and_courts/drug-firms-poured-m-painkillers-into-wv-amid-rise-of/article_99026dad-8ed5-5075-90fa-adb906a36214.html
Red Lawhern, PhD and nationally known Pain Patient Advocate http://face-facts.org/lawhern/
Combining epilepsy drug, morphine can result in less pain, lower opioid dose. https://www.sciencedaily.com/releases/2014/09/140915153613.htm
Jacob Sullum, Reason journalist and syndicated writer https://reason.com/archives/2018/03/08/americas-war-on-pain-pills-is#comment
“Unleashed” Matt Connarton Interviews Red Lawhern 11/28/18 https://www.spreaker.com/user/ipmnation/matt-connarton-unleashed-11-28-18
window.fbAsyncInit = function() FB.init( appId : 1443946719181573, autoLogAppEvents : true, xfbml : true, version : 'v3.2' ); ;
(function(d, s, id) var js, fjs = d.getElementsByTagName(s)[0]; if (d.getElementById(id)) return; js = d.createElement(s); js.id = id; js.src = "https://connect.facebook.net/en_US/sdk.js"; fjs.parentNode.insertBefore(js, fjs); (document, 'script', 'facebook-jssdk'));
Source link
0 notes
Last Seen Blogs

arceoptryx
mold drinker

sofiamp3
Untitled

nct-bliss
Kpop AU: NCT FEMALE SUBUNIT

kpopfan9991
Ellie :)

alinelie
aline