#2. the ableism
Text
been reading a run of horror/thriller novels lately. i've specifically been looking for ones that aren't too intense, ones that are a bit generic or not intended to be especially earthshattering. and i've been largely enjoying it, but, for anyone else who also enjoys reading horror/supernaturaly thrillers, i just wanna stake a quick red flag over J. H. Markert's The Nightmare Man. Not gonna say "don't read". however. AM going to say two things: thought it was a first novel until i saw the six other titles at the back; was astonished at the amount of gratuitous ableism throughout. Also felt it was a bit racist and sexist but not in an overt way, in a nagging uncomfy way.
#details in tags bc i hate to openly hate on things#please allow me this sotto vocce bitching#so 1: the first novel thing.#i noticed a few typos - more than normal - and there were a lot of extremely confusing sentences that i felt an editor should have caught#there were a lot of just Off phrasings#and very little concrete character descriptions and connective action descriptions#so a lot of things were like - oh that happened already?#the plot was also really oddly paced and overly complex#the worldbuilding was also dripped in a way that was like. just uneven#so on that level i was just feeling like it's Okay but just not experienced#2. the ableism#so there's a central background semi-villanous psychiatrist who builds an asylum.#that CAN be done less horribly#i lately read the children on the hill which had the same conceit but was much more sympathetic#anyway. the portrayal of the many mentally ill (actually possessed by nightmares) people we encounterer was so ridiculously flat and cliche#like. to a point that was distinctly uncomfortable over and above the inherent bullshit#because these were. people who were literally supernaturally not in control of their actions. and they were described so animalistically#with ZERO sympathy#except for one woman who was young and hot and whose ridealong nightmare demon just seduced married men rather than kill anyone#and then the ultimate villain came from a deeply toxic family environment and was like the most stereotypical#bad criminal minds episode quote unquote psychopath#and there was ZERO narrative reflection on anything - the kid was just born evil apparently#the father of that kid also had a limb difference and a cleft palate and there was like. so much made of this#but nothing done with it except the guy's wife was cheating on him with his dad#and the narrative essentially justified it bc of this guy's differences#it was just sort of like. a really bad criminal minds episode meets arkham asylum meets what i think nightmare on elm street is about#it was also just blandly racist and sexist#ran out of tags. know i am fuming.
4 notes
·
View notes
Text
Can we stop using "still lives with their parents" or "unemployed" or "doesn't have a drivers license" or "didn't graduate high school" as an insult or evidence that someone is a bad person? Struggling with independence or meeting milestones is not a moral failing.
#autism#autistic#neurodivergent#actually autistic#asd#level 2 autism#medium support needs#low support needs#high support needs#level 1 autism#level 3 autism#disability#ableism
25K notes
·
View notes
Text
Everybody let's not sleep on the fact that Claudia's *entire* arc is not only about her discovering her queerness, but it's also an allegory about disability and ableism.
Claudia is "disabled" in a vampire sense. She has a weaker, slighter body, and looks younger than she is. She can't physically turn vampires, and must rely on help, having to beg for something other vampires can do freely.
She is sexually abused because of her percieved weakness by Bruce, a sad fact that the disabled are more likely to be.
But when she wishes to express her own sexuality she is mocked and patronized by her inability to control herself and not kill doing the act (something the physically older vampires are able to do), and again not able to turn one she wishes for her companion, and have to humiliate herself in the process (having to endure Louis calling her a burden in an attempt to convince Armand).
She just have to shut up and take it, just have so many disabled people have to endure abuse from the caregivers they rely on.
Her ability to decide for her own life, are constantly questioned, as are those with disabilities.
She is patronized, disregarded and systematically ridiculed just for wanting to be a part of a group.
Only Madeleine view her as an equal, and neither coddle her and patronize her.
So remember, when you write about Claudia, and how her relationship with Madeleine gives you "the ick" despite Claudia being a mature woman mentally, just because she has a physically slighter, younger body, remember that many disabled people, physically or mentally, can appear much younger than we are, yet still have fully formed sexual desires, and inner lives. Remember the people who's bodies outside of fiction who's sexual desires gives you "the ick" because they fall out of social norms.
And remember, that Claudia in this series is not only a sapphic woman of color, she's a *disabled* sapphic woman of color (and I love her for it).
549 notes
·
View notes
Text
I love you, trans people with intellectual disabilities. You deserve to have the same opportunities as everybody else, and that's because you are a person. You deserve to be happy. Intellectually disabled trans people deserve the exact same respect, recognition, and love that (should be) afforded to everybody else.
Intellectually disabled trans people, you deserve to make your own decisions about your transness. You are allowed to want for transition or to change your name, clothes, hair, pronouns, or anything else. You deserve support and understanding. I hope you are able to receive that. You belong in this world as your true self. Your transness and your disability/disabilities are not bad things - they are good, and they are important.
#trans#transgender#lgbt#lgbtq#ftm#mtf#nonbinary#intellectual disability#disability#disability positivity#trans positivity#absolutely *so* tired of people 'forgetting' that intellectually disabled trans people; 1) exist and 2) are autonomous human beings#absolutely hate hate hate the ableism of 'but we have to protect ID trans people from themselves :('#no. YOU deserve to have a say in your life intellectually disabled trans person. you are a person first and foremost#you don't need to be 'saved' from the 'tragedy' of having an ID or from being trans...#...these things are neutral at worst. you deserve whatever support you want and/or need...#...but you aren't ever a bad person for that. you are loved. you are worthy. you are cherished. you deserve to be you
3K notes
·
View notes
Text
the way this website treats disabled people is actually horrendous
#yes even the ''progressive'' types always love to imply that literal symptoms of disability#means someone is lazy or that its a moral failing or that they should simply just stop#and the sheer NUMBER of autistic people shitting on other autistic people with higher support needs than them#or who ''act'' more autistic or just have more unpalatable inconvenient or annoying symptoms than them#that cannot be treated like just a quirky trait that makes them more interesting or cute or whatever#i think i wrote like. 2 posts on that where its more coherent than here idk#''this is the autism website'' no. i don't think i feel very welcome here.#mine#yomipost#ableism#actually autistic#i guess other people can add on if they want cause im not gonna be able to articulate much else than that
253 notes
·
View notes
Text
If your activism for diabetics stops as soon as you have to include type 2 diabetics, then not only is your "activism" ableist and almost certainly fatphobic, your efforts are also useless. You will never improve how society treats diabetic people if you only care about the diabetic people who are viewed more favorably in this fatphobic, ableist, and dieting-obsessed world.
-Mod Worthy
#fatphobia#t2d#type 2 diabetes#t1d#ableism#diet culture#diabetes#type 1 diabetes#healthism#Mod Worthy
1K notes
·
View notes
Text
Love it when a modern "progressive" show makes all the evildoers physically disabled.
Larys has a Clubfoot, Aemond gets his eye cut out, and now Aegon is burnt and missing appendages.
Isn't it convenient that we can immediately tell a person is bad because their body looks different?
And of course, we don't explore any discrimination against these characters because they're horrible, and we shouldn't feel bad for horrible people.
People were mean to Larys because of his Clubfoot? But don't you know he has a gross foot fetish?
Aemond has impaired vision? But his eyepatch looks cool, and he is still a good fighter, so what is he even complaining about?
Aegon has been severely burnt? But he is a rapist and so let's make jokes about his dick burning off, lol.
#adding Helaena as neurodivergent and Alicent as an SA victim makes it even more fucking jarring that all these characters are on TG#Because of the obvious moral whitewashing of TB and Rhaenyra specifically#it is really gross how when you put the 2 factions next to each other you have the morally superior side all be pretty able-bodied people#and the other side is full of disabled people and victims who handle their trauma in unpalatable ways#in f&b this was less of an issue because no side was morally superior and the TG disabilities made an interesting sort of balance#book!Rhaenyra had to struggle because of her gender book!Aegon and Aemond because of their disabilities#but by tipping the scales the show created ruin their chance to create compelling disabled characters#they could have had their version of Tyrion Jaime and Bran instead they wrote a bunch of gross stereotypes#house of the dragon#ableism#hotd critical#anti hotd#aemond targaryen#larys strong#aegon ii targaryen
236 notes
·
View notes
Text
PSA to abled people
don't ask how a disabled person became disabled
because chances are, the answer is just "I was born"
which is awkward to say
or worse, the answer is something traumatic that is difficult to talk about
either way, don't
#just wait until I tell y'all about the lady who was sitting in front of me on the plane#she thought it was an appropriate thing to ask 2 hours into being stuck on the tarmac#disability#chronic pain#chronic illness#spoonie#ableism
2K notes
·
View notes
Text
giggling, twirling my hair, kicking my feet, etc
#thought about anders dragonage incident. many dead many injured#fuck jennifer heplar forever and ever for the blatant ableism that went into writing anders and the general hatred she has for him. but also#thank you jennifer heplar. for this paragraph. the sexiest words that have ever been written.#your daily dose of idiocy#dragon age 2#anders my beloved
272 notes
·
View notes
Text
“You may now become who you thought was disposable”: COVID-19 Politics and Ableism - Published July 4, 2024
Unpaywalled link available in the link to our archive! A taste below!
“You may now become who you thought was disposable”:
COVID-19 Politics and Ableism
Andrea Kitta
Journal of American Folklore, Volume 137, Number 545, Summer 2024,
pp. 321-330 (Article)
Published by American Folklore Society
For additional information about this article
muse.jhu.edu/article/931461[37.228.238.33] Project MUSE (2024-07-09 12:59 GMT) American Folklore Society
This essay critically examines the intersection of COVID-19, Long COVID, ableism, and health care disparities in the United States, emphasizing the transformative impact of COVID-19 as a mass disabling event with a disproportionate impact on marginalized communities. I also bring an autoethnographic lens to my experi-
ence of COVID-19 and Long COVID, underscoring the importance of recognizing the diverse and often untellable experiences of individuals with disabilities and challenging the prevailing ableist perspectives embedded in society. I raise ethical considerations of storytelling in the context of Long COVID and urge researchers to
embrace empathy and a more inclusive approach that challenges traditional notions of objectivity and distancing within academic research. I call for a collaborative approach between disability studies and folklore studies, encouraging scholars to interrogate and explore the traditions shaped by experiences of disability.
On December 13, 2020, disability advocate Imani Barbarin created a TikTok where she stated in the caption: “COVID is a mass disabling event. Things will never
be the same. Never. You may now become who you thought was disposable” (Barbarin 2020). Barbarin was not overstating what is happening in the United States. In addition to the overwhelming number of US-based COVID-19 deaths (1.07 million as of November 1, 2022, according to the New York Times COVID-19 Tracker [New
York Times 2023]), there is also an alarming number of cases of post-acute sequelae SARS-CoV-2 infection (PASC) or, as it’s more commonly known, Long COVID. Long COVID happens in anywhere from 5 percent to 50 percent of COVID-19 infections (although most medical experts agree the rate of Long COVID is somewhere around 20–30 percent of all infections). Long COVID affects women at a 22 percent higher rate than men (Sylvester et al. 2022:1391), and one study of Long COVID listed over 200 symptoms (Davis et al. 2021). The most common symptoms are fatigue, shortness of breath, cough, chest pain, brain fog, sleep disturbances, depression, joint pain, and dysautonomia (a dysfunction of the autonomic nervous system that typically
presents as the inability to control temperature, breathing issues, and other things the body normally controls automatically).
Current estimates of those affected by Long COVID in the United States are between twenty and forty million. COVID-19 has
also been shown to reactivate other viruses (Gold et al. 2021; Chen et al. 2022; Su et al. 2022), and one current theory is that Long COVID is the result of the COVID-19 virus continually being reactivated in the body (Klein et al. 2022). The latest research
out of Yale University shows that COVID-19 cases entail cellular changes to the B and T cells, lower levels of cortisol, and that the virus can reactivate other viruses (Su et al. 2022:891–2). A recent study with more than 154,068 participants showed that “in the post-acute phase of COVID-19, there was increased risk of an array of incident neurologic sequelae including ischemic and hemorrhagic stroke, cognition and memory disorders, peripheral nervous system disorders, episodic disorders (for example, migraine and seizures), extrapyramidal and movement disorders, men tal health disorders, musculoskeletal disorders, sensory disorders, Guillain–Barré syndrome, and encephalitis or encephalopathy” (Xu, Xie, and Al-Aly 2022:2406).
Both COVID-19 and Long COVID exposed inequities in the US health care system, with Black, Indigenous, and people of color (BIPOC) populations dying from COVID-19 at much higher rates than White people at the beginning of the pandemic. Compared to White people, Alaskan Indian or Alaskan Natives died at 2.1 times the rate, Black people at 1.7 times the rate, Hispanic or Latinx people at 1.8 the rate, and Asian Americans at 0.8 times the rate (CDC 2023). According to the Washington Post’s analysis of CDC’s statistics, the rate of White people dying from COVID-19
became equal to the rate of other groups beginning in October 2021, then (except for the Omicron wave) increased, primarily due to White people being unvaccinated. Strangely enough, the equalizing trend wasn’t because death rates dropped for BIPOC
people, but rather was due to the rise of the White death rate. Tasleem Padamsee, Assistant Professor at The Ohio State University who researched vaccine use and who is a member of the Ohio Department of Health’s work group on health equity, stated:
“Usually, when we say a health disparity is disappearing, what we mean is that . . . the worse-off group is getting better. . . . We don’t usually mean that the group that had a systematic advantage got worse” (quoted in Johnson and Keating 2022).
Additionally, at the time of this writing in Spring 2023, the pandemic has been declared as “over” despite the fact that around 400 people are still dying per day in the United States and that those dying tend to be people with disabilities and the
elderly (New York Times 2023). It’s difficult to imagine a situation where 400 deaths a day are deemed acceptable, yet here we are. Many people are desperate to “get back to normal” and seem to care more about going maskless or dining indoors than they do about those who are dying of COVID-19. Those who are unvaccinated and unmasked also seem to not understand (or not care) that the longer they continue on that path, the longer the pandemic will take to dissipate. Simply put, the majority
of people do not seem to care about people with disabilities, including those who are immunocompromised, and their increased health risks due to the pandemic.
People with disabilities are an unrecognized health disparity population, and they died at much higher rates during COVID-19 (Krahn, Walker, and Correa-de-Araujo 2015). The National Council on Disability found that 181,000 people with disabilities in long-term care facilities died from COVID-19 in the first year of the pandemic, making up one-third of COVID-19 deaths at that time (National Council of Disabilities 2021). The report is worth quoting at length.
In addition to disproportionate fatalities, key findings of the report include:
People with disabilities faced a high risk of being triaged out of COVID-19 treatment
when hospital beds, supplies, and personnel were scarce; were denied the use of their
personal ventilator devices after admission to a hospital; and at times, were denied the
assistance of critical support persons during hospital stays. Informal and formal Crisis
Standards of Care (CSC), pronouncements that guided the provision of scarce health
care resources in surge situations, targeted people with certain disabilities for denial of
care (National Council of Disabilities 2021).
Students with disabilities were denied necessary educational services and supports during
the pandemic and have experienced disruption and regression in their behavioral and
educational goals (National Council of Disabilities 2021).
The growing shortage of direct care workers in existence prior to the pandemic became
worse during the pandemic. Many such workers, who are women of color earning less
than a living wage and lacking health benefits, left their positions for fear of contracting
and spreading the virus, leaving people with disabilities and their caregivers without
aid and some at risk of losing their independence or being institutionalized (National
Council of Disabilities 2021).
Deaf, Hard of Hearing, Deaf-Blind, and Blind persons faced a profound communication
gulf as masks became commonplace, making lip-reading impossible and sign language
harder (National Council of Disabilities 2021).
#disability justice#disability politics#covid pandemic#covidー19#mask up#covid#pandemic#covid 19#coronavirus#wear a mask#sars cov 2#still coviding#public health#wear a respirator#ableism#covid eugenics
133 notes
·
View notes
Text
hate hate HATE people's reaction to me being a type 1 diabetic being "oh so you didn't do this to yourself" essentially. Type 2 diabetics didn't do anything to themselves either + fuck off i hate you.
#and even if they did they would still deserve help and kindness#type 1 diabetes#diabetic#type 1 diabetic#t1d#t2d#type 2 diabetes#ableism#fatphobia
140 notes
·
View notes
Text
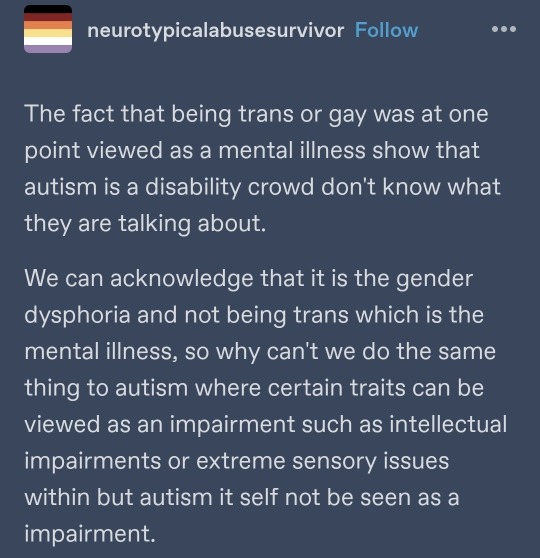
This is the DUMBEST SHIT I have ever seen, so congratulations! You win a prize and the prize is apparently "myling unwisely picking fights".
AS A LEVEL 1 autistic person I say this unto you: Shut up. Sit down. Listen to higher support autistics. If you're so scared to be seen as disabled that you have to deny how autism is the direct cause of people's disability, there's always just the possibility of masking. I don't like saying that, because I think it's perfectly possible to both be autistic and to not be disabled in any way, but I despise these attempts from fellow low support autistic people to distance the disorder from those who are actually disabled. It stinks of ableism.
ASD isn't a mental illness. It is a developmental disorder. Feel free to explain how homosexuality being seen historically as a mental illness maps onto a developmental disorder that is frequently both intellectually and physically disabling.
Sometimes, there's actually a good reason to have a name for a group of symptoms! Such as the fact it makes it easier to get help.
#autism#actually autism#asd#autism spectrum disorder#level 1 autism#level 2 autism#level 3 autism#disability#ableism#high functioning autism#autism spectrum#autism community#THE FUCKING SHIT PEOPLE WILL JUST PUT OUT THERE#GODDAMMIT I'm angry
225 notes
·
View notes
Text
Add one to the list of Insulting Euphemisms for Autistic People

I'm going to add "Booksmart Emotional Idiot" to our collection of fetching Offensive Nicknames for Aziraphale t-shirts (alongside such noteworthies as "Little Miss Religious Trauma"). You get one for free if you're Autistic.
😘
189 notes
·
View notes
Text
generalizing statements like 'all men are evil' are for sure wrong but also i think its important not to cut discussions of gender out of the picture esp bc they are extremely relevant in this case as misogyny is a big part of wilbur's abusive actions and the wider discussion of the. social environment of cc spaces that enables things like this. so.
#also i think its important 2 watch how we talk abt this wrt rhetoric abt gender thats veering in2 radfem territory and ableism#but wrt to the gender stuff it feels like some of the stuff on my dash is also touching on being an overcorrection? like. yeah cis men are#not singularly capable of doing abuse but also this is a conversation abt a space wherein cis men are particularly#empowered and protected 2 abuse their power#so.#and also its worth having grace for ppl who may feel particularly sensitive abt this topic and not aggressively police every part of#how theyre responding to this. .um#yens
155 notes
·
View notes
Text
I hope it turns out that Maggie is "just" a human. I hope it turns out that there is absolutely nothing supernatural or occult or celestial or whatnot about her, fuck, I hope it turns out it's NINA instead.
Fuck, I'm trying very hard not to be frustrated and upset, but I am. I am because it's been over a month and people are still taking Maggie's clearly neurodivergent, and more specifically autistic, behaviour and twist it into "oh look no normal human is like this she's so creepy she must be a demon or an angel" like are you LISTENING to yourselves?
YES she talks differently sometimes, yes she's emotional, yes she did ONE FUCKING SPELLING MISTAKE while she was literally sobbing her eyes out. People are like that, you know. People that don't drink and that didn't go to parties and don't socialize well exist. I'm that person.
I had absolutely ZERO thoughts about Maggie being a celestial because to me, she isn't weird. There is nothing off about her. She's like me, I felt SEEN, I felt recognized and acknowledged.
The worst part is that people LOVE headcanoning Muriel or Aziraphale or Crowley as autistic but as soon as it's not something people can either infantilize or twist into something else, they hate it. Muriel gets praised for the same traits that have people calling Maggie a villain.
Can we stop doing that? Can we stop taking people who are weird or visibly disabled or different and shoving them into the non-human box? Do you have any idea how dehumanizing that is for people who are like those characters?
We had canonically non-binary characters this season that are human, so why, and please fucking tell me WHY, is it impossible in your minds to have disabled humans around? Why does anyone slightly weird have to be a supernatural being?
Just because Maggie's behaviour isn't played off as a joke? Because she is allowed to be a middle-aged, lesbian autistic woman? Because you cannot infantilize her like you can with Muriel?
Please tell me because I don't fucking know.
#alex talks good omens#good omens#good omens season 2#maggie good omens#maggie and nina#literally i am so fucking tired of this i cant#if anyone tries to start shit they'll be blocked#vent post#fucking hell#im so tired of the casual ableism people don't even know they're playing into
294 notes
·
View notes
Text
aroace hate in the ace tag (aro poster), very cool very awesome, love that for you bud, have a wonderful day
this exact behaviour is what drove me away from r/aaaaaaaarrrrro and then r/aaaaaaacccccccce, very nice to see it persist onto tumblr dot com
all this behaviour does is splits up the community, we should be connected and together, not infighting bc aroallos and alloaces and aroaces exist, what does aspec mean, remind me?
#asexual#aro#aromantic#ace#:)#cope seethe and mald#im aro and ace and aroace#i added tags into main body#you have to be a troll#or like 12#who would have thought AROaces would exist in ARO spaces#put me on your blog for mistagged aro posts i dont care#you come into the asexual tag with your aroace hate as an aro kind of makes it an aro focused topic#also you say you will be uploading screenshots with urls intact so free real estate#angry-ar0#from their pinned:#I won't ask you to not arrass these blogs because#let's face it#I don't care#<- do with that info what you will#what a pathetic human you are#your account is just reeking toxicity#its also in the aroace tag#wowee what a nice bean you are#upon further investigation they believe Rword should be normalised like imbecile#gatekeep aroacephobia and ableism 3in1#oh its an alt account because of course it is#drop your main :) you wouldnt#blocked and reported both angry-ar0 and angry-aro-2-2
57 notes
·
View notes
Last Seen Blogs


critical--error
CRITICAL ERROR

hunting-evolution
Pokemon

chavesdaliberdade
Marcello Broke

allofthequeer
all of the queer